Embed Size (px)
DESCRIPTION
Journal for Patient Compliance - Strategies to enhance Adherence & Health Outcomes
Citation preview

ww
w.JforPC
.com
Journal For Patient Com
pliance Strategies to enhance Adherence and H
ealth Outcom
esV
olume 2 - Issue 4
JOURNAL FOR
Strategies to enhance Adherence and Health OutcomesPATIENT COMPLIANCE✓
Volume 2 - Issue 4
www.JforPC.com
An all-in-one personal point-of-careDream or Reality?
The Impact of Selected Legal FactorsOn Pan-European patient-centric programs
A Linguistic Approach To Improving Self-Care And Compliance
Adherence in Chronic Myeloid LeukemiaResults of a Patient-driven Pilot Survey
PEER REVIEWED


DIRECTORS Martin Wright
PUBLISHERMark A. Barker
MANAGING EDITOR Mark A. Barker
EDITORIAL MANAGERJaypreet Dhillon
EDITORIAL ASSISTANTSNick Love, Kevin Cross, Lanny McEnzie
DESIGN DIRECTOR Ricky Elizabeth
RESEARCH & CIRCULATION MANAGERDorothy Brooks
BUSINESS DEVELOPMENTRoss [email protected]
ADMINISTRATOR Petya Stefanova
FRONT COVER © iStockphoto
PUBLISHED BY Pharma PublicationsUnit J413, The Biscuit Factory Tower Bridge business complex 100 clements road, London SE16 4DGTel: +44 (0)20 7237 2036 Fax: +0014802475316Email: [email protected]
Journal For Patient Compliance – Strategies to enhance Adherence and Health Outcomes. ISSN 2045-9823 is published quarterly by PHARMAPUBS.
The opinions and views expressed by the authors in this magazine are not necessarily those of the Editor or the Publisher. Please note that although care is taken in preparation of this publication, the Editor and the Publisher are not responsible for opinions, views and inaccuracies in the articles. Great care is taken with regards to artwork supplied, the Publisher cannot be held responsible for any loss or damage incurred. This publication is protected by copyright.
2012 PHARMA PUBLICATIONSVolume 2 issue 4
JOURNAL FOR
Strategies to enhance Adherence and Health OutcomesPATIENT COMPLIANCE✓
Contents
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 1www.JforPC.com
6 FOREWORD
THINk TANk
8 A Different Approach to Changing Health Behaviour Our behaviour is heavily influenced by what we see other
people doing. Research has shown that the proportion of people dropping a leaflet on the ground rose from 10 per cent to 40 per cent when the number of similar pieces of litter already on the ground was increased from one to eight or more. Carole North co-founder and Joint Managing Director of 90TEN Healthcare looks into a Case Study – Reducing ‘Did Not Attend’ Rates in GP Surgeries, Changing Behaviour in Young People can be More Challenging and provided examples of where the Nudge theory was successfully incorporated into healthcare campaigns to change the health behaviour of a specific segment of a community.
WATCH PAGES
10 The Motivation to Change Dr Anna Baker of Atlantis Healthcare has a closer look at
Motivational interviewing. Motivational interviewing (MI) is based on the premise that the motivation to change should not be imposed from outside, but elicited from within the individual. Rather than a form of therapy, it is a series of principles, backed by techniques, which can be used by healthcare professionals (HCPs) to support patients to explore their unhelpful beliefs about medication and work towards better adherence. Dr Baker answers the questions, How Would a Typical MI Session Take Place? And why does it Work? When is Motivational interviewing Most Effective?
12 Helping Patients Take Their Medication: Lessons from Helping Patients Quit Smoking
The interesting thing about smoking cessation is that we as a society often treat this as a social problem. For example, to get dad to quit, we solicit the help of his family (wife, kids, and friends). We suggest aids that may help, like exercise and diet. We recommend that he see his doctor and try nicotine replacement therapy. Surrounding the patient with the necessary support that he needs to quit (and not what we want) is critical. Michael Wong, the founder of the Physician-Patient Alliance for Health & Safety (PPAHS) argues that, the next time you start to think about an adherence programme, take a page from smoking cessation – make sure it listens to patients and responds to their individual needs in improving medication adherence. This patient centric approach should be a part of each and every strategic decision.

Contents
Volume 2 - Issue 42 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
REGULATORY & MARkETPLACE
14 The Impact of Selected Legal Factors on Pan-European Patient-centric Programmes: A comparison between four European countries
Whilst today there exists a common understanding in the pharmaceutical industry and amongst payors that non-adherence poses a tremendous problem, and numerous programmes to overcome this challenge have been developed and implemented, Pan-European approaches to increase patient adherence are still rare. Issues examined by Kathrin Heinritz, Global Business Development Manager, Health Management Services at Pharmexx GmbH includes a Patient centric Service Including a Nurse at the Patient’s Home or a Medical Dialogue Centre per se a Promotion of the Product to the Patient? If the Patient can successfully be approached and is Happy to join the programme, the Question of Patient Consent comes into Play. The detailed article concludes that pharmaceutical companies should consider centralising a “core” part of their patient support approach in order to raise standards and make programmes amongst countries comparable. In terms of the legal requirements evaluated, they do not differ that much between the countries analysed, and therefore, there is no immovable hurdle in the way of providing ground-breaking services that make a real difference to patient outcomes.
BEHAVIOUR PROGRAMMES
20 A Linguistic Approach to Improving Self-care and Compliance
In the adherence literature, over 200 variables have been examined to determine their association with patient adherence to self-care behaviours. Previous approaches have had either little predictive power or were dependent on epidemiologic variables that were not amenable to intervention. Ideally an adherence questionnaire should be simple to administer and provide a reliable classification that predicts individual adherence and generates actionable information. Herein the authors provide evidence that the CoMac Descriptor™, based upon linguistic analyses of patient statements regarding their disease, meets these criteria. The authors of this work, Charles Clark Jr.,Professor Emeritus of Medicine Indiana University School of Medicine; Ulla Connor, Chancellor’s Professor of English, Zimmer Endowed Chair in Intercultural Communication, and Director of the Indiana Center for Intercultural Communication at Indiana University School of Liberal Arts; Kathryn Lauten, Associate Director, Indiana Center for Intercultural Communication at Indiana University School of Liberal Arts Principal, CoMac Analytics, Inc; Robert Mac Neill Jr., CEO of CoMac Analytics, Inc.; and Robert Sandy chief statistician at CoMac Analytics, Inc. conclude that patients see the world differently and those differences are important both in predicting behaviour and in changing it.
24 An All-in-One Personal Point-of-Care: Dream or Reality? Behavioural change, and treatment plan adherence in
particular, is a multi-faceted phenomenon that requires an equally diverse and constant process of intervention, that must be adapted to the individual needs of each patient. Based on
this approach, a personal point-of-care can become a useful tool in strengthening the therapeutic physician patient alliance, aiming above all to provide optimal healthcare services and improve patients’ quality of life. Zoe Tziakou, Operations Manager, PCC HELLAS and Constantina Georgaki, Clinical Psychologist, PCC HELLAS examine aspects such as Educating the Patient, Patient Reminders, Analysing and Evaluating, People Behind the Adherence Plan, Better Communication, Feeling Included, Real-world Data. The authors conclude that a personal point-of-care will enable healthcare providers to render better patient management and pass crucial messages to their patients in order to achieve behaviour changes. Employing the right approach, the right people and the right tools, we will be there to effectively cover those needs.
THERAPEUTIC
28 Improving Adherence to Inhaled Therapies; Telemonitoring of Dosing Frequency and Technique
John Pritchard, CTO for Philips Respironics Drug Delivery examines Telemedicine, which in its most general sense the practice of “medicine at a distance”, was hailed in the mid-1990s as a potentially time- and cost-effective means of providing patient care. Today telemedicine utilises electronic communication and information technologies which encompass the electronic transmission, storage, and retrieval of digital data. Telemedicine-based approaches offer an opportunity to address aspects of patient care which have traditionally proven difficult to monitor and improve. John concludes that Monitoring vital signs may be seen as a reactive “firefighting” approach to telemedicine, which clearly differs from I-neb Insight Online’s more proactive focus on True Adherence. However, combining the use of I-neb Insight Online with the monitoring of vital signs for the early detection of exacerbations, and other facets of CF treatment such as diet and physiotherapy, may offer an opportunity for optimising the integrated management of the major complications.
32 Adherence in Chronic Myeloid Leukemia: Results of a Patient-driven Pilot Survey
Jan Geissler and Giora Sharf the co-founders of the global CML Advocates Network examine present results of a patient-driven pilot survey on adherence in chronic myeloid leukemia. Optimal adherence to oral cancer therapy is of key importance to maximise treatment effectiveness in patients. With the advance of molecular target therapies, cancer treatment in more and more indications is transforming from in-hospital care towards oral treatment in an outpatient setting. With cancer becoming a chronic disease, patients are often required to take the drug indefinitely on a daily basis. Ensuring an optimal adherence to treatment over the long-term period could be a challenge. As data on the driving factors of nonadherence in oncology is scarce, a pan-European workgroup of the CML Advocates Network has conducted a pilot study which has unveiled differences of non-adherence between countries, administration types and use of adherence tools in Chronic Myeloid Leukaemia.


Contents
Volume 2 - Issue 44 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
36 Why Illness Perceptions Count in Heart Health Half of all patients hospitalised with a serious heart condition
will make mistakes with their medications within a month of checking out of the hospital, says the latest research from Vanderbilt University Hospital and Brigham and Women’s Hospital in Boston. To investigate this issue, Clare Moloney of Atlantis Healthcare in the UK, a Health Psychology Specialist with a focus on cardiovascular health, explains the ‘patient perspective’ and tells us why – and how – we can help to tackle this issue.
40 Practical Pain Management in Older People Pain relief, whether acute, chronic or related to surgery, is
an issue throughout the world. However, as a result of a changing population demographic in countries like the UK, the proportion of older patients is increasing, which poses unique challenges when considering analgesia. We have a potential aging ‘time bomb’ and we need to prepare our services to meet the needs of this older age group ensuring their dignity and their well-being not compromised. Hence, five years ago the British Pain Society worked with the British Geriatrics Society & the Royal College of Physicians, reviewed the evidence and produced national guidance to help all practitioners in assessing pain in older people with a simple algorithm in October 2007. The purpose was to provide professionals with a set of practical skills to assess pain as the first step towards its effective management. Based on recent experience & developments locally Dr. BalMukund Bhala and Dr. Neeraj Bhala recommends the steps will help us move in the right direction for better pain management in older people.
MODERN TECHNOLOGY
44 Direct to the ePharma Consumer – In the Age of Connectivity
Pharmaceutical and Medical Device companies must adapt to the new digital environment says Liz Moench, President and CEO of MediciGroup. While change is inevitable in any industry, this may be the first time that neither industry nor regulators but rather patients are driving this shift. To understand the hesitancy of the pharma industry and FDA toward direct-to ePharma consumers, it is helpful to look back 30 years ago to the advent of direct-to-patient advertising in 1983 in the US, by British-based Boots Pharmaceuticals. At the time, US regulators and major pharma companies resisted the direct-to-consumer approach. A two-year moratorium was immediately enacted by the Food and Drug Administration (and initially supported by most major pharma companies). The moratorium was intended to allow regulators time to more fully explore the ‘risks and benefits’ of going direct to consumer. While industry and FDA viewed it as risky, patients on the other hand viewed it as necessary.
DRUG DELIVERY, DRUG PACkAGING, LABELLING & DISPENSING
48 A Tool for Designing and Evaluating Packaging for Healthcare Products
Although significant resources are devoted to developing healthcare products that are safe and effective pharmacologically, significantly less effort is devoted to ensuring products perform as intended in the hands of providers and patients. Poor designs result in user confusion and frustration, and have the potential to lead to errors and adverse events. The interaction that occurs between people and healthcare products is an area in need of study. The human-package interaction framework introduced by this paper is an analysis tool to support decision-making while designing and evaluating healthcare products. According to this model, any healthcare product has: a set of intended users, varied contexts of use, and a series of tasks that users must accomplish (selection of the correct product, opening, administration, reclosing, disposal, etc.). Javier de la Fuente & Laura Bix, at the school of packaging, Michigan State University discusses how this model provides designers with a structured consideration set with regard to the interactions between people and healthcare products. Considerations to the interface are critically needed in order to reduce the occurrence of medication errors and increase adherence.


Quality healthcare outcomes depend upon patients’ adherence to recommended treatment regimens. Patient non-adherence can be a pervasive threat to health and wellbeing and can carry an appreciable economic burden as well. In some disease conditions, more than 40% of patients sustain significant risks by misunderstanding,
forgetting, or ignoring healthcare advice. While no single intervention strategy can improve the adherence of all patients, decades of research studies agree that successful attempts to improve patient adherence depend upon a set of key factors. These include realistic assessment of patients’ knowledge and understanding of the regimen, clear and effective communication between health professionals and their patients, and the nurturance of trust in the therapeutic relationship. Patients must be given the opportunity to tell the story of their unique illness experiences. Knowing the patient as a person allows the health professional to understand elements that are crucial to the patient’s adherence: beliefs, attitudes, subjective norms, cultural context, social supports, and emotional health challenges, particularly depression. Physician-patient partnerships are essential when choosing amongst various therapeutic options to maximise adherence. Mutual collaboration fosters greater patient satisfaction, reduces the risks of non-adherence, and improves patients’ healthcare outcomes. For most medical conditions, correct diagnosis and effective medical treatment are essential to a patient’s survival and quality of life. A significant barrier to effective medical treatment, however, is the patient’s failure to follow the recommendations of his or her physician or other healthcare provider. Patient non-adherence (sometimes called non-compliance) can take many forms; the advice given to patients by their healthcare professionals to cure or control disease is too often misunderstood, carried out incorrectly, forgotten, or even completely ignored. Non-adherence carries a huge economic burden.
Journal for Patient Compliance gives you these specific step-by-step, practical guidelines to achieve better adherence levels.
We bring you another array of very interesting articles. Carole North, co-founder and Joint Managing Director of 90TEN Healthcare, looks into a different approach to changing health behaviour. Dr Anna Baker of Atlantis Healthcare has a closer look at motivational interviewing, and Michael Wong, the founder of the Physician-Patient Alliance for Health & Safety (PPAHS) argues that, the next time you start to think about an adherence programme, take a page from smoking cessation – make sure it listens to patients and responds to their individual needs in improving medication adherence. This patient-centric approach should be a part of each and every strategic decision.
In the Regulatory section, Kathrin Heinritz of Pharmexx GmbH looks into the impact of selected legal factors on pan-European patient-centric programmes.
In the Behaviour section, Charles Clark and his team look into a linguistic approach to improving self-care and compliance, and Zoe Tziakou and Constantina Georgaki of PCC HELLAS discuss whether an all-in-one personal point-of-care is a dream or reality.
I hope you all enjoy this issue of JPC, and I wish you all a Very Merry Christmas and a wonderful New Year.
See you all in 2013.
Mark A. Barker
Editorial Advisory Board
Andree Bates, Managing Director, Eularis
Anna Dirksen, Senior Manager, PSI Behavior Change
Chris Penfold, Vice Chairman - East Midlands Packaging
Society, Consultant, Freelance Packaging Specialist
Carole North, Managing Director, 90 TEN Healthcare
Dyan Bryson, Managing Partner/VP Patient Strategy
& Outcomes for Inspired Health Strategies
Elisabeth Moench, President & CEO of Medici Global
Helen Lawn, Managing Director, Helen Lawn & Associates
a healthcare PR and communications agency
Isabelle Moulon, Head of Medical Information
Sector, European Medicines Agency
Jay H. Bolling, President and CEO,
Roska Healthcare Advertising
Joseph Bedford, Director of Marketing
Almac Clinical Technologies
Laura Bix, Assoc. Prof. School of Packaging
Michigan State University
Louis A. Morris, Ph.D., is President of Louis
A. Morris and Associates, Inc
Mark Duman, Managing Director ,
MD Healthcare Consultants
Michael Wong is Managing Director at hcCatalyst
Peter van Iperen, Experienced Pharmaceutical Professional
Phill Marley, Packaging Account Manager,
Global Quality Operations AstraZeneca
Ronald E. Weishaar, Executive Director, Observational
Research, PharmaNet Development Group
Saurabh Jain, Director of Patient Value
Services and CME Solutions at Indegene.
Steve Kemp, Business Development Director at Brecon
Pharmaceuticals and Chairman of HCPC Europe
Tassilo Korab, Co-founder of HCPC Europe
(Healthcare Packaging Council)
Vassilis Triantopoulos, CEO of BIOAXIS Healthcare
Walter Berghahn, Executive Director, The
Healthcare Compliance Packaging Council
Foreword
Volume 2 - Issue 46 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes


Think Tank
Our behaviour is heavily influenced by what we see other people doing. Research has shown that the proportion of people dropping a leaflet on the ground rose from 10 per cent to 40 per cent when the number of similar pieces of litter already on the ground was increased from one to eight or more.1
Further research, about to be published in the Journal of Applied Social Psychology, shows that smokers were more interested in cigarettes after being shown a series of images which contained ‘no smoking’ signs in the background. The results suggest that campaigns against smoking and other unhealthy behaviour could ironically trigger the very behaviours they are meant to discourage’.2
Drawing attention to the frequency of this unwanted behaviour therefore often ‘normalises’ it and results in a subsequent increase in its incidence. This trait can also be successfully used to normalise ‘good’ social behaviour, by incorporating the thinking of the Nudge theory.
This theory holds that if we’re fat, smoke too much, or practice risky sexual behaviour, this is largely because we’re lazy or have made stupid choices. These choices are centered in the automatic part of our brains (which dictates our behaviour far more than we are aware of) and ‘nudge’ takes advantage of this to encourage desirable social norms.3
Trials of the theory, which has been adopted by the both the Obama and Cameron administrations, reveal that placing greater emphasis on the norm and making relatively minor changes to language and processes can have a positive impact on behaviour.4
Case Study – Reducing ‘Did Not Attend’ Rates in GP SurgeriesIn the UK, GP practices routinely highlight the large number of patients who fail to cancel an appointment on a large handwritten poster, an electronic notice board or plasma screen. This approach was flawed for a number of reasons, one of which was that the signs targeted the patients who actually attended their appointments and not those who were Did Not Attends (DNAs).
As most of the appointment booking was done over the telephone, the patient’s role was a passive one, and yet behavioural science shows that the more an individual is actively involved, especially in the early stages of making a commitment, the more likely they are to keep to that commitment.
During the study, patients calling to make a GP appointment were asked to repeat back the details of their appointment before ending the call, which led to an immediate reduction of 6.7% in DNA rates. Patients making appointments during clinics were asked to write down the details on a blank card,
which, over a two-month period, led to an 18% reduction in DNAs.
The sign was replaced with a message that conveyed the number of patients who typically do turn up to their appointment in a timely manner (around 95%), normalising the ‘good’ behaviour. This sign, when used in combination with the active and written commitments, resulted in a 31.4% reduction in actual DNAs compared with the 12-month average.5
Changing Behaviour in Young People can be More ChallengingUsing this approach with young people, however, needs to take into consideration what psychologists call the ‘Romeo and Juliet’ effect – the tendency to actively react against what they are being told to do. It then becomes clear why sending teenage mothers into schools to discourage teenage pregnancy can be counter-productive.
In this context, if young people are seeing media stories that normalise teenage pregnancy, and are ‘hanging out’ with friends who have babies, while being told by ‘figures of authority’ that they shouldn’t drink, take drugs or have sex, the explanation as to why teen pregnancy has been increasing becomes apparent.
This is where utilising social marketing principles and creating social norms has had a proven impact on behaviour change.
A Different Approach to Changing Health Behaviour
Volume 2 - Issue 48 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes

Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 9www.JforPC.com
Think Tank
Social marketing is the application of marketing principles in campaigns that seek to achieve social change. It is used to advance a social cause, idea or behavioural change. There are some key principles involved in the use of social marketing; namely, that it:• Targets specific groups of people• Utilises research to build effective strategies• Segments audiences within those target groups and then
tailors strategies to their needs, wants, resources and behaviours
England and Wales have some of the highest rates of teenage pregnancy in Western Europe. In 2010, 90TEN Healthcare was commissioned to encourage young people (YP) to use contraception and attend local sexual health service centers, with the aim of reducing teenage pregnancy by 5% across a 12-month period.
Extensive consultations were undertaken with all the stakeholders involved (including young people and staff directly engaging with them at local sexual health services and pharmacists, and through youth engagement teams).
This consultation process not only provided the necessary research outcomes to inform our strategy, but also fully engaged some stakeholder champions, which included a large group of young people who felt empowered and had a sense of ownership in the campaign.
The campaign resulted in an 11% reduction in teen
pregnancy by March 2010, and 61% of YP surveyed said they would discuss the campaign’s safe sex message with friends, or visit a GP or sexual health service provider for contraception and STI advice.
These are just a few examples of where the Nudge theory was successfully incorporated into healthcare campaigns to change the health behaviour of a specific segment of a community. Crucially, the approach should be targeted rather than blanket; a core part of the initial Nudge-informed social marketing process is not only to define types of behaviour but also identify potential advocates to help promote change. The principle can be incorporated into adherence programmes, to both standardise anticipated levels of acceptable medication adherence among healthcare professionals, and to place greater responsibility on, and thereby empower, the patient.
References 1. Cialdini RB, Reno RR and Kallgren CA (1990). A focus theory
of normative conduct: Recycling the concept of norms to reduce littering in public places. Journal of Personality and Social Psychology 58(6): 1015–1026.
2. Earp BD, Dill B, Harris JL, Ackerman JM & Bargh JA (2012). No sign of quitting: Incidental exposure to no-smoking signs ironically boosts cigarette-approach tendencies in smokers. http://www.yale.edu/acmelab/articles/Earpetal2012JAPS.pdf
3. The Guardian. http://www.guardianpublic.co.uk/nudge-theory-can-effect-behaviour-change-but-care-is-needed
4. Applying behavioural insights to reduce fraud, error and debt. The Cabinet Office. http://www.cabinetoffice.gov.uk/sites/default/files/resources/BIT_FraudErrorDebt_accessible.pdf
5. GP Online. http://www.gponline.com/Medeconomics/article/1092121/reducing-missed-appointments/
Carole North is co-founder and Joint Managing Director of 90TEN Healthcare. She has over 11 years’ experience delivering programmes that increase adherence to treatment by empowering patients to change their health beliefs and behaviours, supporting HCPs
to manage those patients, and developing initiatives that help reduce acute hospital admissions. 90TEN Healthcare consistently wins awards for its adherence, concordance, and experiential and social marketing campaigns, and is currently delivering patient adherence programmes in 23 countries.Email: [email protected]

Volume 2 - Issue 410 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Watch Pages
Motivational interviewing (MI) is based on the premise that the motivation to change should not be imposed from outside, but elicited from within the individual. Rather than a form of therapy, it is a series of principles, backed by techniques, which can be used by healthcare professionals (HCPs) to support patients to explore their unhelpful beliefs about medication and work towards better adherence.
A Closer Look at MIMotivational interviewing requires that the HCP work with the principles of expressing empathy, supporting self-efficacy, rolling with resistance and developing discrepancy. These are about seeing the issues from the patient’s perspective and allowing them to identify the barriers and ways to overcome these to enable change. For example, it allows the patient to highlight or identify ways of moving towards a goal, rather than the HCP trying to provide the immediate solution.
It also requires using patient-centred communication techniques such as asking open-ended questions; using affirmations to acknowledge use of positive change talk from the patient and to encourage the patient to engage in constructive dialogue and explore their own thinking. In addition, MI involves being able to listen in detail to what the patient is saying and to identify the key points. Finally, it uses reflective listening to offer back to the patient what they have said to the HCP. This shows that not only they are heard, but also that they are understood.
How Would a Typical MI Session Take Place?MI sessions can take any form – face-to-face, online or by phone, in small groups – as long as there is open communication whereby patients can break down their personal barriers to change by developing their own solutions. The focus here is on creating a stronger and more productive relationship between the HCP and the patient. It is about enabling the patient to take responsibility for their own issues and to collaboratively work through solutions.
And Why does it Work?MI allows the HCP to view the therapeutic relationship as more of a partnership, and less of a structured hierarchy. This allows for a more equal balance within a patient’s relationship with their HCP. These principles and techniques can be used to help patients to take ownership of their disease and make effective decisions to manage it.
When is MI the Most Effective?MI is particularly useful for new patients or those changing medication, as it is effective when helping patients to identify the pros and cons of changing treatment compared to staying with usual care.
MI in PracticeAs an example, in patients living with diabetes, MI could be used to help support their motivation to change to a different form of treatment. A patient who has previously managed their illness through oral medication and diet may have concerns about changing to injections even though they may know it is the right thing to do.
While acknowledging the benefits to their physical health, they may have relevant concerns about the impact on their day-to-day living and personal relationships. By using MI techniques, an HCP could support them to make the decision to change their behaviour as well as helping inform strategies to implement goals for change. The techniques could also be used to develop a personal self-management programme that builds confidence and ultimately supports better adherence.
This is a valuable approach to enhancing the HCP/patient relationship as well as a patient’s motivation to change their behaviour. It can be effectively used to support patients developing strategies for better adherence and self-management. However, appropriate training and follow-up of HCPs is needed to ensure proper implementation of the approach, in order to get the best outcomes for both parties.
Dr Anna Baker (C Psychol AFBPsS) has a PhD in Health Psychology from University College London. She has worked as a Clinical Strategist for Atlantis Healthcare involved in developing and implementing the psychological components of patient-
centric solutions worldwide. Prior to working at Atlantis she was Course Leader for the MSc and Professional Doctorate Health Psychology programmes at London Metropolitan University. Anna has over 19 years of research and clinical expertise in health professionals training, behaviour change techniques, tailored interventions and chronic disease prevention with a special emphasis on ethnic minority populations. She is also a Registered Health Psychologist and trained Cognitive Behavioural Therapist who has worked with mental and physical health issues. Email: [email protected]
The Motivation to Change

Volume 2 - Issue 412 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Watch Pages
Smokers are not patients -- or, at least, that’s the view that most people have of smokers. Like most “self-inflicted” health risks, like drinking too much alcohol and sharing needles, the stigma attached to smoking and smokers is pervasive1.
Unfortunately, not treating smokers as “patients” and seeing smoking as a “disease” can lead us to not apply valuable lessons from quit smoking programmes to help patients take their medication.
The interesting thing about smoking cessation is that we as a society often treat this as a social problem. For example, to get dad to quit, we solicit the help of his family (wife, kids, and friends). We suggest aids that may help, like exercise and diet. We recommend that he see his doctor and try nicotine replacement therapy. Surrounding the patient with the necessary support that he needs to quit (and not what we want) is critical.
With that in mind, I, together with the Vietnamese American Cancer Foundation (VACF) and GlaxoSmithKline (GSK) developed a programme directed towards the Vietnamese American community, targeting “Little Saigon” in Orange County, California. Little Saigon has the largest number of Vietnamese outside of Vietnam. Unfortunately, this community was facing a number of enormous challenges. It had one of the US market’s highest smoking rates (36 per cent)2 and had therefore been deeply impacted by the scars of this addiction – death, disease and their consequences on family wellbeing and livelihood. Moreover, entrenched cultural and social acceptance of smoking made it an even more difficult task, with smoking for example still occurring in restaurants and offices with social impunity.
We purposely engaged the entire community in the programme (doctors, a community patient advocate, and a pharmaceutical company). Local doctors were asked to actively speak with their smoking patients about the need to quit. As Dr Loc D. Bui (a Little Saigon doctor) urged his fellow colleagues at the start of the campaign, “As physicians, we know the danger of smoking. I would like to see all the physicians in our community talk to their patients about smoking and strongly encourage them to quit.”
The pharmaceutical GSK, although a manufacturer of nicotine replacement products, was content to fund these activities without active product promotion. For example, in a survey of local physicians, doctors’ attitudes and beliefs about nicotine replacement therapies involving gums, patches and lozenges were explored along with “cold turkey”, herbal supplements, diet, exercise, or anything else they might recommend to their patients.
These patients were made aware of the cadre of healthcare experts, quit lines, and volunteers at the VACF that stood ready to assist them. “People don’t realise that it is not just their health, it is the health and welfare of their whole family that the smoker puts at risk,” said Leonard Tran (then
Executive Director of VACF). “Men who develop smoking-related diseases often leave their families without means for support. By quitting smoking, men can give themselves their best chance of being able to be there for their families in the long term.”
The community responded to VACF’s message. A young widow, for example, spoke on community radio to tell her heart-wrenching story of not getting her husband to quit soon enough. Sadly, he had recently died, leaving his wife and kids to deal with bills and payments, and continuing to live their lives without him.
The results? Activity on the quit lines and at VACF increased dramatically. As one doctor observed, epitomising the programme results, “Since the programme started, I have had 4-5 patients per month quit smoking which is 4-5 times more than I usually have.”
However, what the programme had really done is motivational counselling at its best -- doctors intervened as the medical authority, the community provided stories and emotional support, and the local cancer foundation (VACF)
Helping Patients Take Their Medication: Lessons from Helping Patients Quit Smoking

Watch Pages
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 13www.JforPC.com
gave individualised and group counselling and advice.More importantly, we applied techniques that we knew
would work. We were not encumbered with the need and desire to wait for clinical trial data, or have confirmed and documented returns on investments from other smoking cessation programmes before starting the Little Saigon programme.
Waiting for this data before acting is truly regrettable. Recently, for example, the Archives of Internal Medicine reported on the results of a study to examine whether a
telephone-based counselling programme rooted in motivational interviewing would improve adherence to osteoporosis medication.
For this study, more than 1000 Medicare patients who had been newly prescribed osteoporosis medication were divided into a control group, who were mailed educational materials, and an intervention group, who received telephone-based counselling.
Median medication adherence was 49% in the telephone group and 41% in the control group. In short, as the
osteoporosis researchers concluded, “In this randomised controlled trial, we did not find a statistically significant improvement in adherence to an osteoporosis medication regimen using a telephonic motivational interviewing intervention.”
Unfortunately, the results of studies like these may result in programmes like these never starting. As Dr Jon Ebbert (Professor of Medicine at Mayo Clinic) emailed us:
Tragically, this may mean that stakeholders may not pay attention to what may be a very promising and innovative strategy to improve medication adherence. Behavioural strategies have been used very successfully in getting patients to quit smoking and can be a great tool in getting patients to take their physician-prescribed medication. So, the next time you start to think about an adherence
programme, take a page from smoking cessation – make sure it listens to patients and responds to their individual needs in improving medication adherence.
This patient-centric approach should be a part of each and every strategic decision.
Why? Because the old marketing adage that the customer is always right applies even to the healthcare industry. Don’t discount such things as complaints of side-effects, lifestyle inconveniences, and forgetfulness -- listening and responding may be the difference between an adherent patient and a non-adherent patient.
References 1. Jennifer Stuber et al., “Smoking and the emergence
of a stigmatized social status” Social Science and Medicine (May 2008) http://deepblue.lib.umich.edu/bitstream/2027.42/60953/1/stuber_smoking%20and%20stigma_2008.pdf (accessed April 8, 2012).
2. A Provider’s Handbook on Culturally Competent Care, Smoking Among Asian Americans: A National Tobacco Survey
Michael Wong is the founder of the Physician-Patient Alliance for Health & Safety (PPAHS). PPAHS is an advocacy group devoted to improving patient health and safety; and is composed of physicians, patient advocates, and professional healthcare organizations,
and can be found at www.ppahs.org Like a serial entrepreneur, Mike has been behind many healthcare initiatives, including encouraging people to quit smoking, get tested and treated for hepatitis, and take their medications as prescribed by their physicians. As well, he has helped improve access to healthcare.Email: [email protected]

Volume 2 - Issue 414 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Whilst today there exists a common understanding in the pharmaceutical industry and amongst payors that non-adherence poses a tremendous problem, and numerous programmes to overcome this challenge have been developed and implemented, Pan-European approaches to increase patient adherence are still rare.
One reason for the rarity of Pan-European patient-centric programmes could be that these programmes are still decided by the country affiliate of a pharmaceutical company and not centrally, with the role of paying for such a Pan-European service residing with the pharmaceutical industry and not the payors.
Does the pharmaceutical industry still see patient-centric services as a component of local commercialisation (nationally driven) initiatives and not a core marketing (centrally driven) activity? Should a pharmaceutical company let individual countries decide on what is appropriate, or is the decision due to the fact that marked differences between countries in terms of legal issues, healthcare markets or other factors like technological development and cultural variations are present?
Due to the targeted scope of the article, we shall focus in this paper on the differences between countries in the area of legal issues whilst acknowledging that there might be other factors impacting the decentralism of patient-centric services, too. The evaluation of the legal differences represents an assessment of the current frameworks based on an analysis carried out in the countries observed in this article. We acknowledge that there is permanent change in this field and as such the situation may change rapidly in some countries. It is therefore indispensable to verify the current legal framework in each market for each specific project! The author has written this article to the best of her knowledge and on availability per country but does not take any liability for the legal statements made.
Four different European countries, including a Scandinavian (Denmark), a middle European (Germany), a Western European (Belgium) and a Southern European country (Spain) have been chosen to compare.
If we consider health management services in this article, the definition “nursing service” (nurse or other adequate HCP visits the patient at home to inform, educate, train and support the patient) and “medical dialogue centre” (nurse or other adequate HCP calls the patient to inform, educate, train and support) shall apply. These services are directly targeted at patients in order to increase adherence – and are not classical homecare services.
In order to evaluate the legal framework for patient-centric services and their implementation, four important steps have been analysed according to the set-up of a patient-centric programme: first of all, the question if a patient-centric service per se is a promotion by the pharmaceutical company
to the patient; second, how the patient can actually be accessed; third, if we need any consent of the patient in order to implement the patient programme with him or her; and last but not least, what actually can be done by a nurse (since it is assumed in this article that usually these are nurses) at the patient’s home.
Is a Patient-centric Service Including a Nurse at the Patient’s Home or a Medical Dialogue Centre per se a Promotion of the Product to the Patient?Contrary to the US, we can anticipate that in none of the four European countries selected is any kind of promotion allowed from pharmaceutical company to patients for Rx products or in general for Rx products to patients. The legal framework in the countries is similar since it is based on an EU directive1. In Germany, for example, it is stated: “Pharma companies are not allowed to promote Rx-products directly to patients / consumers”, “Pharma companies are not allowed to pro-actively and directly contact patients for product-related informational purposes” or “Pharma companies are not allowed to pro-actively and directly contact patients for further support with the product”.
Similar statements can be found in the three other countries2.
However, the Spanish and Danish laws foresee a clause where “Pharma companies are allowed to prepare informational materials, that the doctor may provide to a patient, regarding Rx-products which, due to the complexity of their dosage, route of administration, etc., require the provision of additional information”, provided that:• This information is only intended to improve compliance
with treatment.• The material does not include promotional information
on the product.
In Belgium, for example, it is similarly not considered as a promotion if they do not contain any product promotion and / or answer a specific question about a particular product: “correspondence, possibly accompanied by material of a non-promotional nature, needed to answer a specific question about a particular medicinal product” and “factual, informative announcements and reference material relating, for example, to pack changes, adverse-reaction warnings as part of general drug precautions, trade catalogues and price lists, provided they include no product claims3.”
Already in this statement, it can be concluded that material aimed at improving compliance without any promotional content can be used in order to support the patient – can that be viewed in the same way for a nurse who visits a patient, or might a medical dialogue centre call not be seen as a promotion, but rather as the trial supporting the patient?
If we consider that the usual procedure of a patient-
The Impact of Selected Legal Factors on Pan-European Patient-centric ProgrammesA comparison between four European countries
Regulatory & Market Place


Volume 2 - Issue 416 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Regulatory & Market Place
centric service in reality foresees that the patient is only informed about the patient-centric service after a product has been prescribed by a physician, the promotional sense of this service is already negated in the first place. It must, however, be ensured that the nurse or HCP is well trained to not “promote” the product at the patient’s home in any way.
In order to NOT trespass on the promotional factor that the information on the programme could have, it is therefore advisable to use the pharmaceutical company’s own sales force, or that of a third party, to inform the physicians and / or pharmacists about the programme, who then in turn inform the patients after prescription of the product.
Concluding that no promotional support of the drug is possible as the patient-centric programme only starts when the patient is already on the drug following the prescription of the physician, the ways in which the patient can be accessed shall now be analysed.
We have already seen that patients can be informed by the treating physician about a patient-centric programme if the product has already been prescribed to the patient and the information is non-promotional as regards the product.
However, is there any supporting way to access the patient for a programme? There seem to be alternative ways!
In Germany, Denmark and Belgium, for example, package inserts as regards the programme, and also flyers or brochures at the physician and / or at the pharmacy, can be used in order to inform about the patient-centric programme (only after the product has been prescribed).
Moreover, the pharmacist could also be used in order to transfer the message of the patient-centric programme to the patient. In Spain, the optimal and legal way to approach the patients would also be via the physicians, and non-promotional materials can be used as discussed above.
If the Patient can Successfully be Approached and is Happy to Join the programme, the Question of Patient Consent comes into Play In all of the four countries, the patient has to provide consent!4 Except for Denmark, in the three other countries, contact with the patient has to be in writing. It should also be possible to express consent via registration on a homepage.
In Denmark, even if it is not mandatory to receive the consent in writing, it is definitely recommended to do so in order to avoid any doubt.
According to Article 5 of Organic Law 15/1999 in Spain, the
patient whose personal data are collected must previously be informed, in an express, precise and unmistakable way, of the following matters:• Of the existence of a personal data filing system or the
processing of personal data, of the purposes of the collection of the personal data, and of the recipients of the information;
• Of the mandatory or optional character of his or her response to the questions asked;
• Of the consequences of the collection of the data or of the refusal to provide the data;
• Of the possibility to exercise at any time the rights of access, rectification, cancellation and opposition;
• Of the identity and address of the processor, or, if applicable, of its representative.
In Denmark, with the consent of the patient, healthcare personnel can pass on information about the patient health, private information, or other confidential information to other healthcare personnel. Moreover, physicians who are treating a patient are then, in the case of a patient-centric programme, allowed to obtain information about a patient’s health, private information or other confidential information from electronic systems when it is necessary in connection to an ongoing treatment of the patient from the HMS nurse5.
In Germany and Belgium, moreover, there has to be written consent by the patient to store and process his/her data. The patient data has to be separated from the pharmaceutical entrepreneur. The staff involved in the project have to be instructed about data protection6.
Under no circumstances should the reporting to the pharmaceutical manufacturer, or a third party involved in the programme, include any personal data or any medical personal data, but only anonymous data.
Which Tasks can be Performed at Home for Patients by an HCP in the Framework of a Health Management Service?After having passed the three challenges prior to the beginning of the programme, it is indispensable to know what tasks and interventions can be performed with the patient at home by a nurse (we assume that it is a nurse who visits the patient at home. If it is another HCP, the facts might be different).
In Germany, for example, nurses are allowed to inform the patient at home about the disease, treatment and the application of a product as well as to show the patient how to use the product; they are not allowed to set infusions or injections themselves at home of a patient due to the regulations of the BÄK (Bundesärztekammer = Federal medical council) – a physician would have to be within earshot7. As outlined in point number one, they are not allowed to promote the product in any way, but only to neutrally discuss it and its usage.
It has to be taken into account, however, that in Spain, for injections and infusions, the home-setting scenario can only be fulfilled if the use of the product has not been restricted to the premises of the hospital. If this is the case, the nurse is allowed to carry out injections and infusions.
In all of the countries, no other HCP (except an alternative practitioner for OTC drugs in Germany) other than a physician can carry out injections into the patient on own responsibility.
Graph: possible way of approaching the patient for a patient-centric programme
Regulatory & Market Place
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 17www.JforPC.com
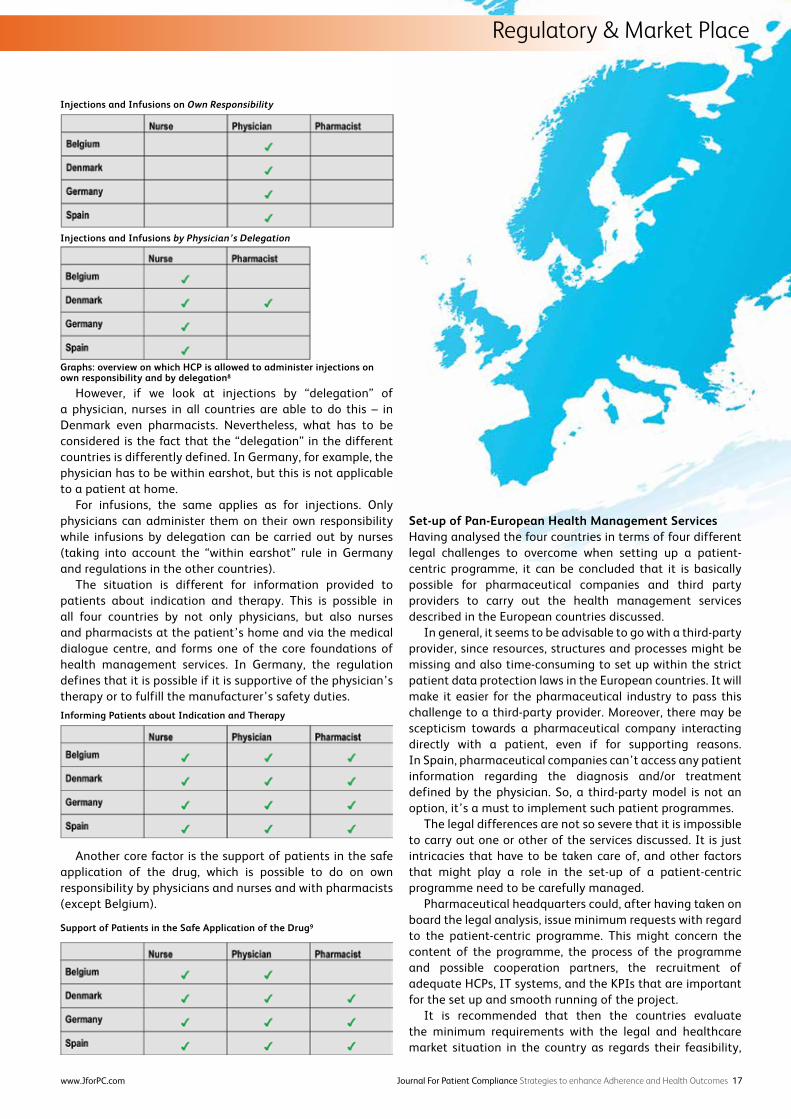
However, if we look at injections by “delegation” of a physician, nurses in all countries are able to do this – in Denmark even pharmacists. Nevertheless, what has to be considered is the fact that the “delegation” in the different countries is differently defined. In Germany, for example, the physician has to be within earshot, but this is not applicable to a patient at home.
For infusions, the same applies as for injections. Only physicians can administer them on their own responsibility while infusions by delegation can be carried out by nurses (taking into account the “within earshot” rule in Germany and regulations in the other countries).
The situation is different for information provided to patients about indication and therapy. This is possible in all four countries by not only physicians, but also nurses and pharmacists at the patient’s home and via the medical dialogue centre, and forms one of the core foundations of health management services. In Germany, the regulation defines that it is possible if it is supportive of the physician’s therapy or to fulfill the manufacturer’s safety duties.
Another core factor is the support of patients in the safe application of the drug, which is possible to do on own responsibility by physicians and nurses and with pharmacists (except Belgium).
Set-up of Pan-European Health Management ServicesHaving analysed the four countries in terms of four different legal challenges to overcome when setting up a patient-centric programme, it can be concluded that it is basically possible for pharmaceutical companies and third party providers to carry out the health management services described in the European countries discussed.
In general, it seems to be advisable to go with a third-party provider, since resources, structures and processes might be missing and also time-consuming to set up within the strict patient data protection laws in the European countries. It will make it easier for the pharmaceutical industry to pass this challenge to a third-party provider. Moreover, there may be scepticism towards a pharmaceutical company interacting directly with a patient, even if for supporting reasons. In Spain, pharmaceutical companies can’t access any patient information regarding the diagnosis and/or treatment defined by the physician. So, a third-party model is not an option, it’s a must to implement such patient programmes.
The legal differences are not so severe that it is impossible to carry out one or other of the services discussed. It is just intricacies that have to be taken care of, and other factors that might play a role in the set-up of a patient-centric programme need to be carefully managed.
Pharmaceutical headquarters could, after having taken on board the legal analysis, issue minimum requests with regard to the patient-centric programme. This might concern the content of the programme, the process of the programme and possible cooperation partners, the recruitment of adequate HCPs, IT systems, and the KPIs that are important for the set up and smooth running of the project.
It is recommended that then the countries evaluate the minimum requirements with the legal and healthcare market situation in the country as regards their feasibility,
Injections and Infusions by Physician’s Delegation
Graphs: overview on which HCP is allowed to administer injections on own responsibility and by delegation8
Injections and Infusions on Own Responsibility
Informing Patients about Indication and Therapy
Support of Patients in the Safe Application of the Drug9

Volume 2 - Issue 418 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Regulatory & Market Place
and present their findings to the central department that is responsible for such programmes.
Together, it can then be decided what kind of adaptation has to be undertaken to adhere to the required standards, without neglecting country regulations and framework conditions.
The projects are then agreed upon by headquarters and affiliates and KPIs tracked.
Eventually, the project outcomes will be evaluated and compared against each other.
Best practice examples can be discussed, and lessons learned in the project might be taken on board in other countries as well.
Conclusion For the time being, there does not seem to be an official stance on the provision of health management services of this type, on the part of a pharmaceutical company in many countries in Europe. This situation can be explained, in part, by the fact that EU legislation has not yet established a clear frontier to define when we are in the presence of a merely informative activity in connection with a certain medicinal product, and when we are facing an activity of a promotional nature.
In terms of health management services that support patients therapy adherence and therapy outcome, that complement physician’s work, and that are beneficial for the whole healthcare systems as regards cost burden, one has to consider the neutrality and non-promotional touch and the tasks that can be carried out by an HCP at a patient’s home and via telephone – then, there is a win-win situation for everybody involved.
Pharmaceutical companies should consider centralising a “core” part of their patient support approach in order to raise standards and make programmes amongst countries comparable. In terms of the legal requirements evaluated, they do not differ that much between the countries analysed, and therefore, there is no immovable hurdle in the way of providing groundbreaking services that make a real difference to patient outcomes.
Footnotes 1. EU Directive 92/28/EEC of March 31, 19922. Spain: Art. 78.1 Law 29/2006; Art. 3.6 Law 29/2006;
Belgium: Article 9 Law of March 25, 1964; Royal Decree of 7 April 1995; Denmark: Danish Medicines Act no. 1180 of 12.12.2005, Clauses 63 and 66)
3. Article 9 § 1 Law of March 25, 19644. Germany: §4a, 5 and 11 BDSG, Denmark: The Act on
Processing Personal Data, Spain: Article 7.3 of Organic Law 15/1999 on personal data protection, Belgium: Law of 8 December 2002 on Privacy Protection and duty of medical secrecy.
5. To follow6. Bundesdatenschutzgesetz (BDSG), Belgium: Law of 8
December 20027. Bundesärztekammer, Persönliche Leistungserbringung,
29.08.20088. Country analysis 2010 by Pharmexx9. Country analysis 2010 by Pharmexx
References1. Germany: Bundesärztekammer, Persönliche
Leistungserbringung, 29.08.2008, in: http://www.bundesaerztekammer.de/page.asp?his=0.7.47.3225, 05.11.2012
2. Council Directive 92/28/EEC of 31 March 1992 on the advertising of medicinal products for human use and “Advertising of medicinal products for human use” in http://europa.eu/legislation_summaries/other/l21143_en.htm, 05.11.2012
3. Spain: Law 29 of 26.07.2006 on the guarantees and rational use of medicines and health products
4. Belgium: Belgian Act on Medicines of 25.03.19645. Denmark: Danish Medicines Act no. 1180 of 12.12.2005,
Clauses 63 and 666. Belgium: Clause 54 in Act. No. 1350 of 17.12.2008 on
authorization of health-care professionals and on health-care activities in Belgium, Royal Decree of 11.03.1985
7. Germany: Bundesdatenschutzgesetz (BDSG, § 4 a and 5)8. Denmark: Danish Data protection law in: http://www.
datatilsynet.dk/english/the-act-on-processing-of-personal-data/ read-the-act -on-process ing-of -personal -data/compiled-version-of-the-act-on-processing-of-personal-data/, 05.11.2012
9. Spain: Ley Orgánica 15/1999, de 13 de Diciembre, de Protección de Datos de Carácter Personal. (LOPD) in: http://www.agpd.es/portalwebAGPD/english_resources/regulations/index-iden-idphp.php, 06.11.2012
Kathrin Heinritz graduated from the University of Applied Sciences Furtwangen, Germany, in 2004 with a degree in International Business Administration. She later earned her Masters Degree in International Management at the Northeastern
University in Boston, USA, and Università Cattolicà del Sacro Cuore in Piacenza, Italy, in 2009. Between 2005 and 2008, Mrs. Heinritz worked as Project Manager international projects in Service, Sales and Auditing projects for several blue chips in a specialised consulting company serving the automative industry. Here, she was responsilbe for the conceptual set up of the projects as well as their implementation and evaluation worldwide. She joined Celesio Group (Pharmexx’s parent company) in 2009 and worked as Portfolio Manager for Pharmexx between 2009 and 2011 concentrating on harmonization and development of the Pharmexx service portfolio on international level. Pharmexx is a leading international outsourcing partner for companies within the area of Life Science.
Since May 2011, she is working as Manager Global Projects being responsible for the roll-out of patient-centric services internationally across Pharmexx which includes the development of service blueprints, customer visits, workshop gearance and the development of tailor-made solutions in this area. Mrs. Heinritz also coordinated the processes of a big patient-centric project in Germany. She has also held speeches on Health Management Services on several pharma conferences on international level.Email: [email protected]

Volume 2 - Issue 420 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Behaviour Programmes
In the adherence literature, over 200 variables have been examined to determine their association with patient adherence to self-care behaviours1-3. Previous approaches have had either little predictive power or were dependent on epidemiologic variables that were not amenable to intervention. Ideally an adherence questionnaire should be simple to administer and provide a reliable classification that predicts individual adherence and generates actionable information. Herein we provide evidence that the CoMac Descriptor™, based upon linguistic analyses of patient statements regarding their disease, meets these criteria.
Main body Paragraphs:Over the past several years, an interdisciplinary research group at Indiana University, consisting of linguists and healthcare professionals, has identified linguistic indicators in three domains related to adherence: control orientation, based on locus of control research4; agency, based on self-efficacy5; and affect or attitude and emotion6. Based upon this linguistic research7-10 and using the language that reveals a subject’s worldviews on each of the domains, we have developed a questionnaire, the CoMac Descriptor™. The CoMac Descriptor™ relies on patient’s self-identification with the actual words used by other patients with the same worldview. The instrument categorises patients into one of eight bins: internal or external control orientation, high or low agency, and positive or negative affect (Table 1). The questionnaire can be administered in 10 to 15 minutes. The data presented below describe the research that led to the development of the CoMac Descriptor™. Data are provided to show that the Descriptor™ can reliably predict self-care behaviour compliance in persons with type 2 diabetes and hypertension.
Recognising the importance of understanding the patient, the interdisciplinary research group at Indiana University conducted in-depth interviews of 43 English-speaking subjects with type 2 diabetes. They were analysed by domain by two to four coders into one of the eight bins (internal and external control, high and low agency and negative emotions). The linguistic feature systems (word use, sentence structure, and other expressions) for agency and control domains were generated using grounded theory analysis that has been extensively used in qualitative analyses of health communication. The linguistic features of affect expressions that were tested in this sample of diabetes patients came from a well-established linguistic theory of affect appraisal6.
The initial CoMac Descriptor™, based upon the results of these analyses, was a 35-item survey. Its validity was tested in 20 persons with diabetes as compared to the in-depth interviews of the same persons. The CoMac Descriptor™ responses and interviews were analysed independently from each other. The results from the CoMac Descriptor™ coding were compared to those of the interview coding to determine the concurrence of the domain placement of the interviews versus the CoMac Descriptor™. In this administration of the 35-item version, there was 75% agreement between CoMac Descriptor™ results and the linguistic analysis of individual interviews; the agreements between the CoMac Descriptor™ and control orientation, agency, and affect were 75%, 70%, and 80%, respectively. There was also 100% agreement on content validity arrived at through inter-rater reliability assessment by three content specialists in linguistics and test development.
After dropping the questions below r=0.7, the CoMac Descriptor™ was revised to a 28-item survey. The resultant 28-item CoMac Descriptor™ was administered in a similar study to 16 new subjects. There was a 74% agreement between CoMac Descriptor™ results and individual interview linguistic analysis as well as 100% agreement on content validity arrived at through inter-rater reliability assessment by content specialists in linguistics and test development.
Thus, our initial testing demonstrated that a brief questionnaire yielded reliable information in three domains known to explain compliance in over 70 per cent of the subjects tested. We concluded that such a questionnaire is useful for individualising the educational approach to initiating or improving self-care adherence behaviours.
For example, persons in the most favourable domains (internal control, high agency and positive emotion) would receive positive reinforcement to continue their successful behaviours. For persons in the least favourable domains (external control, low agency and negative emotions) extensive intervention would be necessary beginning with analysis of the specific negative emotion (e.g. fear, anxiety, depression, etc.). Each of the eight placements would generate actionable approaches most likely to be consistent with the individual’s control orientation, agency and emotion.
Control orientation is a strong perception and the least likely of the three domains to be mutable. Nevertheless, the terms the clinician would use in approaching persons with internal or external control orientation would be quite different. For those individuals with an external control orientation, the clinician would couch his or her advice in terms of “Your provider holds the key to your health” or “9 out of 10 persons with diabetes have benefited from taking this medication.” In contrast, internal control oriented individuals would receive advice beginning with such statements as “You are in the driver’s seat” or “Consider the benefits of this medication -- you may find out that it addresses your health concerns.”
A Linguistic Approach to Improving Self-care and Compliance
Table 1: DescripterTM Clusters

Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 21www.JforPC.com
Behaviour Programmes
For an individual, neither agency nor emotion levels are immutable. Yet, there are a number of studies that report negative emotions, especially depression and anxiety, to be common in chronic disease and lead to low levels of patient compliance with self-care behaviours. Therefore, our approach to patients with negative emotions could take priority over agency until the negative emotions have been addressed. After addressing emotion, the healthcare professional can begin to address low agency; that is, infrequently engaging in self-care behaviours. The healthcare professional can approach persons with internal control, but low agency, by suggesting that they decide on their own what small steps they would take to increase self-care behaviours. For those with low agency and external control, the approach would be for the healthcare provider to suggest a specific small step toward enhancing the ability and confidence of the individual with each step.
Our next step in the development of the CoMac Descriptor™ was to compare the results generated by the CoMac Descriptor™ with the impressions of a clinician actively engaged in the care of the patients being studied. In order to accomplish this we engaged the collaboration of a nurse practitioner caring for the patients with type 2 diabetes in our validation studies. She had extensive experience with these individuals and knowledge of their self-care behaviours. We familiarised the nurse practitioner with the domains being studied and how she might recognise them. Of the 16 patients with diabetes, there was complete concordance between the nurse practitioner’s classification of the patients and that derived from the CoMac Descriptor™ in all but three cases. Of the three in which there was not concordance, one did not complete the questionnaire and one was clearly gaming the questionnaire. This study, therefore, assured us that we were dealing with a questionnaire that yielded clinically meaningful and actionable information. Our next developmental step addressed the generalisability of the linguistic approach that we had developed. Specifically: would a modification of the CoMac Descriptor™ directed at hypertension yield comparable results to those seen in diabetes and would such a modification for hypertension in a different culture or language yield comparable results to those seen with the questionnaire in English?
To address these questions we administered a modified CoMac Descriptor™ focused on self-care behaviours in hypertension to over 358 persons with hypertension in English, Spanish, German, and Italian. We then compared results to a widely used questionnaire to predict compliance, the MARS-5. Our a priori hypotheses were that those subjects who were internally oriented, and had high agency and positive emotions would be the most compliant, and that those who were externally oriented, and had low agency and negative emotions would be the least compliant. The data generated in this study supported these hypotheses11. Further, we were able to detect differences in the clustering results obtained in different populations with different native languages. While we will need further study to characterise completely intercultural and inter-linguistic issues in our approach, we believe the data generated thus far support our contention that a linguistic approach to predicting self-care behaviours is both reliable and generalisable.
We believe that our linguistic approach yields information that both predicts self-care behaviour and provides avenues or approaches to improve self-care behaviours when such improvement is necessary. First let us begin with two questions: “Does the CoMac Descriptor™ yield information that predicts compliance to self-care behaviour as well as current questionnaires?” and “Does the CoMac Descriptor™ yield information that is more useful and actionable than that provided by current questionnaires?” Table 2 summarises the most common variables used to predict adherence to self-care behaviours. They are demographic and medical/epidemiological in nature.
While demographic and medical information is interesting, it is not really useful to the clinician as the variables are not mutable. Table 3 shows the significant variables generated from the study discussed in the previous paragraph. While they give the clinician direction on how he or she might change the regimen, if that seems clinically appropriate, they are not particularly useful in developing an educational approach for the individual patient. The table also shows that the significant variables predicted somewhat over 65% of the variation.
Table 4 summarises the results from the CoMac Descriptor™ in the same study. Predictability of compliance was slightly better than for the demographic and medical variables. More importantly, as discussed above, the information provides useful information that the healthcare provider can use in his or her approach to the patient.
We conclude that patients see the world differently and those differences are important both in predicting behaviour and in changing it. For addressing adherence, knowing how patients think is more important than their demographics or attitudes toward their medical regimen. The CoMac
Table 4: Results for the linguistic clusters in predicting adherence
Correctly classified when using only linguistic variables: 66.86%
Correctly classified when using all medical, demographic and linguistic variables: 70.37%
Data provided by Quintiles/MediGuard
Table 3: Results for all demographic and medical variablesCorrectly classified into an adherence category: 65.24%Significant variables• Had severe side effects• Avoiding side effects• Employed• Stopped medicine because I got betterData provided by Quintiles/MediGuard
Table 2: Conventional explanatory variables and descriptive statisticsAge, mean = 52, S.D. = 12Demographic variables• Employed: 54%• Any college education: 48%• Stopped medicine because I got better: 11%Medical variables• Cost of the medication: 6%• Avoiding side effects: 10%• Had severe side effects: 8%• Medication not effective: 2%Data provided by Quintiles/MediGuard

Volume 2 - Issue 422 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Behaviour Programmes
Descriptor™ provides information on how the patient thinks that is useful to the clinician in the development of an educational approach to improve self-care behaviour and eventually outcomes. We summarise our conclusions in Table 5.
References1. Morris LS, Schulz RM. Patient compliance—An overview. J
Clin Pharm Ther. 1992; 17: 283-295. 2. Vermeire E, Hearnshaw H, Van Royen P, Denekens J. Patient
adherence to treatment: Three decades of research. A comprehensive review. J Clin Pharm Ther. 2001; 26: 331-342.
3. van Dulmen S, Sluijs E, van Dijk L, de Ridder D, Heerdink R, Bensing J, et al. Furthering patient adherence: A position paper of the international expert forum on patient adherence based on an internet forum discussion. BMC Health Serv Res, 2008; 8(1): 47
4. Wallston KA, Wallston BA, DeVellis R. Development of the multidimensional health locus of control (MHLC) scales. Health Educ Behav. 1978; 6: 160-170.
5. Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. 1977; 84: 191-215.
6. Martin JR, White PRR. The language of evaluation: Appraisal in English. New York: Palgrave Macmillan; 2005.
7. Connor U, Lauten K. (invited submission). A multi-method analysis of diabetes patients’ health beliefs and actions. In: Hamilton H, Chou WS, eds. Handbook of Language and Health Communication. New York: Routledge.
8. Lauten K, Connor U, Antón M, Balunda S, Goering E, Hayat A, Roach P. (2010, November). “You are what you talk” – patient-centered interactions. Paper presented at the ICADE Diabetes Conference 2010, Indianapolis, IN.
9. Lauten K, Connor U, Antón M, Balunda S, Goering E, Hayat A, Roach P. Patient-centered adherence improvement. Paper presented at: International Conference on Communication in Healthcare; 2010 September; Verona, Italy.
10. Connor U, Cortes V. A Corpus linguistic analysis of diabetes patients’ health beliefs and action. Paper presented at: American Association of Applied Linguistics (AAAL) Conference; 2010 March; Atlanta, GA.
11. Sandy R, Clark C, Connor U, Lauten K, Mac Neill R. Determinants of adherence: a comparison of commonly used variables to linguistically identified worldviews. Presented at: Patient Adherence, Communication and Engagement USA 2011 Conference; 2011 October; Philadelphia, PA.
Charles M. Clark Jr., M.D.; Professor Emeritus of Medicine Indiana University School of Medicine. Dr Clark is former Director of the Diabetes Research and Training Center; Associate Dean for Continuing Medical Education at Indiana University and Editor in Chief
of Diabetes Care. He has published extensively on facilitating patient education and compliance. He is the Medical Director of CoMac. Email: [email protected]
Ulla Connor, Ph.D.; Chancellor’s Professor of English, Zimmer Endowed Chair in Intercultural Communication, and Director of the Indiana Center for Intercultural Communication at Indiana University School of Liberal Arts. Dr Connor has 30 years of experience in the
sociolinguistic and ethnographic analysis of communication, most recently applied to patient-centric adherence through communication strategies based on the patient perspective. The author of more than 100 publications, including 10 books, Dr Connor has lectured globally about intercultural communication and applied linguistics. She is the Chief Scientific Officer of CoMac. Email: [email protected]
Kathryn Lauten, PhD; Associate Director, Indiana Center for Intercultural Communication at Indiana University School of Liberal Arts Principal, CoMac Analytics, Inc. Kathryn Lauten is a specialist in health literacy and models of health behaviour. Her current research
involves combining her background in education, linguistics and intercultural communication with her work in health communication in order to improve patient outcomes. She received her BA from Dartmouth College and her PhD from the University of Michigan.Email: [email protected]
Robert Mac Neill Jr., MBA; CEO, CoMac Analytics, Inc. Mr Mac Neill has more than 30 years of progressive experience in the pharmaceutical and health service industries, including roles at Eli Lilly & Co. and Areks, Inc. Mr Mac Neill earned a BA at Brown University and an MBA at
Harvard University. Email: [email protected]
Robert Sandy PhD; Principal, CoMac Analytics, Inc. is chief statistician at CoMac Analytics, Inc. He has authored two books and 16 journal articles, and been the principal investigator of an NIH-funded study of childhood obesity. His research focus is occupational safety
and health, e.g., the consequences of workplace illnesses. Email: [email protected]
Table 5: CoMac ConclusionsPatients perceive the world differently For addressing adherence, knowing how patients think is more valuable than knowing their demographics and their concerns about medicine
The CoMac Descriptor™ provides what you need to approach the individual patient in a tailored patient-centric manner that is consistent with their worldviews

Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 23www.JforPC.com
Behaviour Programmes

Behaviour Programmes
Volume 2 - Issue 424 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Behavioural change, and treatment plan adherence in particular, is a multi-faceted phenomenon that requires an equally diverse and constant process of intervention, that must be adapted to the individual needs of each patient. Based on this approach, a personal point-of-care can become a useful tool in strengthening the therapeutic physician-patient alliance, aiming above all to provide optimal healthcare services and improve patients’ quality of life.
Targeting adherence effectively is a daunting task. Drawing from studies that examine the success of adherence interventions, it has been found that multi-faceted interventions are the most effective 1,2.
The idea behind a promising patient compliance programme must be based on an approach to patient adherence that is both holistic and tailored to individual needs, that is grounded in the principles of behavioural change theory and the use of interactive technology. It aims to be an efficient means of providing information, education, reminders, monitoring, communication, evaluation and support, along with the patient’s and the physician’s active participation in the process of adhering to a care plan and managing a disease.
Tailoring a programme to each patient’s individual needs is the most encouraging form of intervention. Evaluation is an important means of defining the patient’s unique, individual characteristics. The main attributes that should be considered when tailoring a programme to a patient’s needs are presented here (Table 1):
Educating the PatientOne of the basic factors involved in adherence and, by extension, a programme that aims at reinforcing adherence is keeping the patient informed on his or her disease and treatment. The tasks patients need to undertake in managing their illness are often complicated and can be difficult to perform consistently. As many as 50% of patients do not know what they are supposed to do to take care of themselves after their visit to the doctor’s office3.
A point-of-care solution should provide up-to-date information regarding the disease (causes, symptoms and clinical signs, management of its psychosocial impact) and the treatment (nature, duration, side-effects, management of side-effects etc). Providing information to the patient creates a sense of security and confidence in better managing his or her condition, and helps the patient meet his or her goals more easily.
Anastasia, 60: “I enjoyed going through the educational material on my disease. There were a lot of things I had never heard about before. After I read it, I called my friends to read it together.”
At the same time, such a solution should provide detailed instructions on the proper use of treatment, thus ensuring that the medication is safely and appropriately used, with a focus on boosting patient self-confidence and independence. Specifically, patient training can lead to lower risk of drug misuse due to multipharmacy, and fewer adverse reactions, drug interactions and health complications.
Danae, 39: “I was given the chance to train myself on administering the drug and now I can help my mother-in-law with her medication. This way, it takes less effort and less time, and I can always rest assured that we follow her treatment plan according to the doctor’s instructions. We used to visit her doctor every time she had an injection scheduled - commuting was difficult for both of us.”
Patient RemindersReminders for medication-taking and a timely scheduling of prescribing and obtaining medication are essential and practical ways of facilitating and motivating the patient’s adherence to a treatment plan. An ideal personal point-of-care provides all necessary reminders, while personalised reminders are able to cover every need of the patient’s everyday schedule.
Medication reminders can be interactive, since they require confirmation from the patient that the treatment was followed. This way, patient behaviour is recorded with every scheduled dose.
Helen, 32: “I don’t have to struggle to remember the dates that I have to take my medicine. PCC HELLAS provides reminders for the next scheduled injection. That’s a great help for me, because I tend to forget, it’s my condition that makes me really forgetful.”
Evaluation of one of our company’s patient adherence plans
An All-in-One Personal Point-of-Care: Dream or Reality?

– which includes, among other things, sending reminders in the form of text messages and requests for call-back confirmation from patients after medication-taking – has shown that the majority of patients had a positive opinion of the programme’s interactive nature. The call-back confirmation as a means of monitoring the adherence programme was considered a positive feature by the majority of patients and was seen as a form of communication and collaboration between themselves and our service. It must be noted that none of the patients considered the calls they had to perform as a tiresome or dull process. Some patients evaluated this feature as their own “giving back”, a sort of “contribution” to the services offered by the programme, while others saw it as an extra motivation to maintain adherence.
Based on the above results, it is obvious that when it comes to a programme built on respect for the patient and his or her needs, on open communication, trust and the provision of satisfactory services, the presence of interactivity and active involvement is highly beneficial. Instead of patients acting as passive spectators, they are being asked to take up an active role in their treatment. Patient engagement is increasingly recognised as a key component of treatment. We believe that it would be interesting to further investigate the role of interactive participation in adherence programmes, how it interrelates with other factors, and how this interrelation affects adherence.
Analysing and Evaluating The features of a well-designed personal point-of-care allow for an initial evaluation of the patient’s state (e.g. through questionnaires) and a regular evaluation of the patient’s progress (through regular follow-up interviews and/or questionnaires). On top of that, it is possible to further analyse and statistically process this data in order to extract useful and definite conclusions concerning the treating physicians and the medical community in general or healthcare providers (national organisations for healthcare) and pharmaceutical control services (EMEA etc.).
It is also possible to create assessment questionnaires on the patient’s clinical status and progress through treatment. In the hands of healthcare professionals, these questionnaires can become valuable tools for appraising the course of the disease and treatment. Since time restrictions rarely allow for the collection and practical application of this data, the physician is now given the ability to receive such important information, save it for later use and then statistically process it through integrated applications. Patients are no longer required to fill in time-consuming questionnaires and assessment forms at the doctor’s office; online completion provides a major workload relief for the healthcare professional.
People Behind the Adherence PlanAside from making good use of all technology has to offer, it is necessary for the design, implementation and evaluation of multi-component, patient-centred adherence programmes to enjoy the support of a dedicated, inter-disciplinary support team consisting of highly-trained personnel. Expertise in behavioural science, interpersonal communication and motivational interviewing is necessary in order to deploy appropriate behavioural strategies and enhance intrinsic motivation that affects adherence.
A 2006 study observed HIV patients using a tablet PC-based counselling tool designed to support medication adherence and secondary HIV prevention. The study’s findings suggest that such a tool may reduce social bias and embarrassment, and encourage patients answering honestly. Nevertheless, participants identified important qualities that a computer cannot provide, such as empathy, compassion, and caring4. The study results stress that a computer-based solution can be a valuable solution when coupled with skilled healthcare providers.
Better Communication What a personal point-of-care effectively does is communicate information regarding the patient’s behaviour within his or her treatment plan to the physician or any other healthcare professional. Constant monitoring of the patient’s behaviour provides the physician with a flexible system that allows for evaluation, guidance, and both timely and direct intervention in the patient’s treatment plan. At the same time, it gives us the ability to identify the patient’s needs and match all action taken within the adherence programme to those needs.
Adam, 42: “Lying to your doctor is lying to yourself.”Using a personal point-of-care takes advantage of direct
communication technology capabilities (video or voice calls), reinforcing collaboration and the therapeutic physician-patient relationship. This results in creating optimal conditions for a more effective and meaningful communicative exchange.
Feeling IncludedTaking things a step further, patients can be connected with the patient community and kept up-to-date by receiving relevant health news, information about their doctor’s practice and updates on an ongoing basis. Patient groups, health organisations and even pharma corporate communications can be brought into this concept; this sort of interaction can benefit patients considerably.
Anastasia, 60: “I received a news bulletin about the World Arthritis Day. I was moved; there’s actually an observance dedicated to patients like me!”
Real-world DataSince September 2012, we have been running a pilot project where patients receive a personal point-of-care, which is actually a tablet PC that includes all of the previously-discussed features. Participating patients were chosen by their treating doctors and they will be keeping their tablet until the end of the project, in a few months from now.
Participants include both male and female patients of a varying age range: 50% are people aged 31-40, 17% are people aged 41-50 and 33% are people aged over 60. In order to better understand the expectations and the impact a compliance tool of this sort can carry, we have designed questionnaires that are being given to patients and doctors within a specific timeframe. Most of the patients involved in the pilot project stated that they feel well-informed about their medication and their illness; 83% of participants said that they know exactly how their medication helps them battle their illness and 66% feel that they are fully educated about their illness.
In the beginning of the project, however, all participants stated that they expect a personal point-of-care to provide much-
Behaviour Programmes
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 25www.JforPC.com

Volume 2 - Issue 426 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Behaviour Programmes
needed information on disease and medication. Moreover, over the course of the pilot project we have been noticing that many patients frequently ask for additional educational and training materials. Some of them also said that they often share the educational content with their friends and family.
All patients said that they receive information concerning their disease and drugs from their doctor. Roughly 80% of participants also look up relevant information on the internet, while a small percentage obtains information from books, leaflets and/or other patients suffering from the same disease. According to research, doctors overestimate the amount of information they provide to their patients and underestimate the amount of information patients actually want5. During doctor’s visits, a mean of 49 seconds was spent discussing all aspects of newly-prescribed medications6.
Our findings highlight how crucial the doctor’s role can be in educating his or her patients. By extension, a personal point-of-care that contains educational materials can lead to a decrease in the doctor’s office workload and eliminate the possibility that paatients forget or misunderstand a specific piece of information. Most importantly, these materials are selected and approved by the treating doctor; no more hearsay and dubious information of questionable value.
Some findings on patient beliefs are contradictory as well. The patients believe that their doctor chose them to participate in the project based on their familiarity with technology and their positive pre-existing personal relationship. On the other hand, when the doctors were asked what their criteria were for registering a patient for the pilot project, the answers we received were quite different. The doctors chose each participant based mostly on his or her health condition, low compliance rates and age.
Regarding the medication reminder system, 50% of patients stated that they use mobile phone reminders (mostly patients aged between 30 and 50). 33% said that they use no reminders and just rely on memory, while 16% use a printed calendar. About 85% of patients expect that a personal point-of-care will significantly help in reminding them when to take their medication.
Apart from obtaining information and receiving reminders, some other expectations the patients had are presented in Table 2:
Doctors have more or less similar expectations, but believe that such a personal point-of- care will help them in retrieving and analysing important data as well. According to our findings, patients were worried mostly about the progression of their disease and their therapy’s outcome. A high number of patients also stated that they have to take too many drugs.
Roughly 80% of the patients have no contact at all with patient groups and related health organisations. Underlying reasons vary. What a personal point-of-care could do is bridge the gap between patients and associated groups via a constant flow of information and messages (e.g. announcements, newsletters, bulletins).
A statement coming from one of the patients vividly sums up his experience of using his personal point-of-care: “We have become inseparable”.
Changing Lives In the words of Heraclitus, it is in changing that we find purpose. Very often people avoid change because they do not know how to go about it; a well-designed personal point-of-care can show them the way. As we move forward, technology becomes more and more involved in our lives, resulting in the emergence of new needs and new ideas. A personal point-of-care will enable healthcare providers to render better patient management and pass crucial messages to their patients in order to achieve behaviour changes. Employing the right approach, the right people and the right tools, we will be there to effectively cover those needs.
References 1. McDonald HP, Garg AX and Haynes RB. Interventions to enhance patient adherence
to medication prescriptions: scientific review. JAMA. 2002;288:2868–79.2. Haynes RB, Ackloo E, Sahota N, McDonald HP and Yao X. Interventions for
enhancing medication adherence. Cochrane Database Syst Rev. 2008 Apr 16: CD000011.
3. Heisler M, Bouknight R, Hayward R, Smith D and Kerr E. The Relative Importance of Physician Communication, Participatory Decision Making, and Patient Understanding in Diabetes Self-management. J Gen Intern Med. 2002 April; 17(4): 243–252.
4. Skeels M, Kurth A, Clausen M, Severynen A, and Garcia-Smith H. CARE+ User Study: Usability and Attitudes Towards a Tablet PC Computer Counseling Tool for HIV+ Men and Women. AMIA Annu Symp Proc. 2006; 2006: 729–733.
5. Street RL Jr. Information-giving in medical consultations: the influence of patients’ communicative styles and personal characteristics. Soc Sci Med. 1991; 32(5):541-8.
6. Tarn DM, Paterniti DA, Kravitz RL, Heritage J, Liu H, Kim S, Wenger NS. How much time does it take to prescribe a new medication? Patient Educ Couns. 2008 Aug; 72(2):311-9. Epub 2008 Apr 11.
Zoe Tziakou, Operations Manager, PCC HELLAS. Zoe has been dealing with patient adherence management problems and solutions on a daily basis. She has been an active participant in the design and management of patient adherence programs carried out by PCC HELLAS,
supervises all personnel involved in patient support, and receives daily feedback from patients and healthcare professionals. Email: [email protected]
Constantina Georgaki, Clinical Psychologist, PCC HELLAS. Constantina is involved in the development and implementation of patient adherence interventions for populations facing a variety of health conditions. She is also involved in the patient support centre,
conducting one-to-one communication with patients and caregivers. Her other areas of special interest include relaxation training and crisis intervention. Email: [email protected]

Regulatory & Market Place
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 23www.JforPC.com

Therapeutic
Volume 2 - Issue 428 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Telemedicine, in its most general sense the practice of “medicine at a distance”, was hailed in the mid-1990s as a potentially time- and cost-effective means of providing patient care. Today telemedicine utilises electronic communication and information technologies which encompass the electronic transmission, storage, and retrieval of digital data. Telemedicine-based approaches offer an opportunity to address aspects of patient care which have traditionally proven difficult to monitor and improve.
Patient adherence is one such aspect; the World Health Organisation (WHO) suggests “improving adherence might be the best investment for tackling chronic conditions effectively”, implying that non-adherence to prescribed medication is amongst the most influential factors affecting health status1. Respiratory therapies present a particular challenge, given the demand for adherence, and also compliance with correct technique; it is not difficult to appreciate that administering aerosol via a nebuliser, pressurised metered dose inhaler (pMDI), or dry powder inhaler (DPI) is more complex than simply swallowing a pill. The use of a respiratory device is often not intuitive, and while an average patient’s compliance errors may be less extreme than firing the pMDI directly onto the chest, or swallowing capsules intended for a DPI, basic errors in technique remain common, and can dramatically reduce drug delivery. For this reason, True Adherence ([% adherence to prescribed regimen x % compliance with correct use] / 100) is proposed as a preferable global measure of medication delivery in respiratory patients2.
Factors underlying poor True Adherence are likely to be multiple, and involve an interaction between aspects “extrinsic” to patients – relating to the healthcare system or therapy itself – and more “intrinsic” influences, such as the patients’ attitudes and demographics. Notably, those patients who are “unwitting” or have low levels of literacy may be unaware of their poor True Adherence.
Interventions designed to empower patients in the practice of self-management are likely to be more beneficial than more paternalistic approaches to adherence promotion.
A prerequisite for assessing True Adherence is the ability to accurately monitor medication use; today, electronic monitors represent the “gold-standard” for such monitoring. In respiratory patients the feedback derived from monitoring may also be a valuable method for improving adherence, while providing a key to unlocking the complex reasons underlying an individual’s adherence behaviours. Telemedicine-based interventions, which monitor whilst also providing adherence and compliance-related feedback, have the potential to improve poor True Adherence and, ultimately, disease control. This article reviews current methods designed to monitor and promote True Adherence, and explores the potential of telemedicine-based systems. We discuss the evidence for the benefits of systems such as I-neb Insight Online, a True Adherence focused telemedicine-based system, which
combines real-time feedback with the opportunity to promote and improve adherence in respiratory patients.
Historically, interventions aimed at addressing patients’ self-management and medication use have focused on adherence alone. It is only recently that reliable compliance monitors have been developed and many of these devices are not commercially available outside of clinical trials.
Assessing the impact of an adherence intervention on recorded adherence alone is arguably meaningless, given that the intention of improving adherence is to demonstrate measurable benefits in health outcomes. In view of this, a 2007 systematic review assessed longer-term (minimum six months follow-up) randomised controlled trials which attempted to correlate adherence with clinical outcomes in chronic non-psychiatric conditions3. A total of 37 clinical trials met the inclusion criteria; these trials assessed 12 different chronic conditions including HIV, rheumatoid arthritis, diabetes, and cardiovascular disease. Eleven studies focused on respiratory disease, the majority of which concerned asthma alone, while two covered both asthma and chronic obstructive pulmonary disease (COPD). The interventions assessed were grouped broadly into behavioural, informational, and combined behavioural and informational.
The provision of monitoring and feedback, or reductions in dosing demands, were associated with improved adherence across the different disorders. However, many studies declined to use electronic monitoring to assess adherence, instead opting for the cheaper, though far less reliable, method of self-report. This may explain why results differed from those of a more recent review of studies utilising electronic adherence monitoring in respiratory patients,
Improving Adherence to Inhaled Therapies; Telemonitoring of Dosing Frequency and Technique
Table 1. Factors which may underlie poor True Adherence

Therapeutic
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 29www.JforPC.com
which found the provision of feedback to be associated with significant improvements in adherence, whilst regimen simplification was not4. The beneficial effect of monitoring and feedback reflects the opinion of the WHO which suggests that “ongoing communication efforts - may be the simplest and most cost-effective strategy for improving adherence”1.
Overall, results of the review indicated that studies employing informational interventions in respiratory patients were less successful in improving adherence, compared with those using combined informational-behavioural interventions.
Studies of behavioural interventions alone were generally limited by the use of poor quality adherence monitoring techniques; although previously shown to be one of the most unreliable means of monitoring, self-reported adherence was the most commonly used method. More objective measures, including pharmacy records and canister weights, were used by some of the studies included in the review, although neither of these offers any means of detecting whether a patient has incorrectly administered their medication - either unwittingly, due to poor compliance, or through “canister dumping”, wherein patients perform multiple, perhaps hundreds, of consecutive actuations prior to a clinic visit, with the intention of emptying the canister, thereby disguising non-adherence. The lack of objective measures of adherence may be interpreted as a cost-saving issue; it is however unfortunate, given that highly accurate adherence monitors are commercially available.
It is plausible that the inconsistencies in the relationship between adherence and clinical outcomes were influenced by the variable definitions of “adherent behaviour” and the low accuracy of the commonly utilised method of self-report.
Studies employing validated electronic adherence monitors have shown some promise. For example, use of Chronolog (Medtrac, Colorado), an early electronic adherence monitor capable of recording the date and time of pMDI actuations, was associated with an improvement in adherence to inhaled corticosteroids; from week two onwards the intervention group showed a significantly higher mean adherence, compared with the control group5. However, there was no demonstrable difference in clinical outcomes over the 10-week study period. The Smartinhaler (Nexus6, New Zealand) is a more recent adherence monitor which also records the date and time of pMDI actuation, in addition to providing audible medication reminders and visual cues. When adherence levels, obtained via monitoring with the Smartinhaler, were fed back to paediatric asthma patients and their carers, a 21 percentage point improvement in adherence was observed, compared with those patients who were unaware of their adherence level6. Improvements in FEV1 were also greater in the feedback group; however, baseline differences in lung function meant that these changes did not reach statistical significance6. Thus, while the use of electronic adherence monitors undoubtedly aids recognition of poor adherence, devices which record adherence alone do not necessarily improve True Adherence or result in clinically meaningful changes in outcome measures.
As noted above, to assess True Adherence it is necessary to also measure patients’ compliance, requiring the use of more sophisticated monitoring devices. Several such
devices have been developed over the last decade; however, while these have generally been validated, few have been assessed in clinical trials designed to correlate increased inhaler competence with disease control, and fewer still are commercially available. Taken together, these results indicate that monitoring and feedback cannot be seen as the solution to poor True Adherence, but rather, an important part of an otherwise multifactorial approach to what is recognised as a multifactorial problem7.
Telemedicine-based systems, which monitor both adherence and compliance, and also provide problem-oriented feedback based on that monitoring, may offer a means by which to address True Adherence in a suitably multifactorial way. While various products such as the Smartinhaler, and more recent SmartTrak device (Nexus6) offer reminders, these can address only unconscious non-adherence, and make no attempt to improve compliance. The most sophisticated monitors permit automated, and in most cases, remote tracking of adherence. However, of devices capable of monitoring compliance, many are limited by the generalisability of their use (the Electronic Diskhaler for example is device-specific, while the MDILog (WestMed, Inc., USA) requires the purchase of modified components). The V3 Datalogger (Philips Respironics, USA) is a compliance monitor designed for use with pMDI accessory devices. The V3 Datalogger has shown promise, in terms of providing detailed and accurate information on patients’ compliance, and has been used alongside radiolabelling studies assessing lung deposition8. This offers great potential in terms of investigating the relationship between objectively assessed aspects of inhaler technique, and the adequacy of drug delivery to the target tissue. However, the Datalogger remains at the development stage, and is currently not available for remote use. Figure 1.True Adherence; a global indicator of patients’ device use

Volume 2 - Issue 430 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Therapeutic
Of all the available devices, the I-neb Insight Online system is unique. I-neb Insight Online is designed for use with the I-neb Adaptive Aerosol Delivery (AAD) nebuliser (Philips Respironics, UK), and contains a data logger that can be connected to a computer9. The system can monitor adherence and compliance, facilitate access to this data for physicians, patients, and homecare providers, and provide treatment-related feedback and support. The previously discussed review did not include any studies of True Adherence in patients with cystic fibrosis (CF)3. This is concerning, given the complexity of CF treatment regimens, the notoriously poor True Adherence reported in these patients, and the likely impact on morbidity and mortality. True Adherence
data obtained through the use of I-neb Insight Online is therefore also likely to provide an important contribution to our understanding of electronic monitoring, feedback, and True Adherence in this population.
Patients using I-neb Insight Online can also utilise a breathing trainer within the software, which enables the interactive practice of long, slow inhalations, thereby minimising treatment times. A recent randomised controlled trial in CF patients using I-neb Insight Online indicated that longer, slower inhalations were associated with a reduction in treatment times of more than 40%10. In the same study, the shorter treatment times also had a positive impact on adherence. Shorter treatment times using I-neb Insight Online have also been shown to correlate with higher levels of True Adherence11, providing evidence that the patient may be more likely to take a treatment if the associated intrusion into day-to-day activities is lessened.
Data collected via the system is uploaded to a central server, where it is accessible to the patient, the patient’s healthcare provider, and a dedicated patient support team9. The patient support team is able to monitor compliance with inhalation technique and aspects of device performance. At a subsequent consultation the physician can examine patterns of dosing, for example frequently missed doses at a particular time of day, or on specific days of the week. The transparency of information provided by I-neb Insight Online not only offers an opportunity for the physician to engage in a more informed discussion with the patient regarding behavioural modification aimed at improving adherence, but may facilitate modification of the treatment burden to a mutually agreeable level. It may also help the physician make more informed clinical decisions on the relative efficacy of prescribed medication against the patient’s True Adherence
Figure 2. I-neb Insight Online infrastructure

levels. Clinicians have reported that open routine monitoring can help support patients in maintaining long-term inhalation therapy, while use of the information recorded can facilitate the tailoring of treatment regimens to the individual, which can also improve adherence12. As such, I-neb Insight Online can be seen as uniquely multifaceted, reflecting the needs of the patient, identified from real-time adherence and compliance data. This system is currently available in the UK, and will be rolled out across Europe over the coming months.
In the previously mentioned handling study, use of I-neb Insight Online in adult CF patients was associated with 98% compliance, and 69.4% adherence, resulting in a mean True Adherence of 68%9. This compares favourably with the recently reported adherence level of 36%, also recorded in adult CF patients using data downloads obtained from the I-neb AAD System13. While such a comprehensive telemedicine system has not yet been developed and trialled for use in other respiratory disorders, the potential impact of I-neb Insight Online on True Adherence in CF suggests that similar systems may also aid treatment optimisation in conditions such as asthma and COPD.
Further indication for the potential of telemedicine solutions in chronic conditions is derived from the UK’s Whole System Demonstrator (WSD). The WSD, the largest randomised controlled trial of telehealth to date, involved the remote monitoring of vital signs in patients with COPD, coronary heart disease, and diabetes. Recent results were promising, claiming significant reductions in mortality, hospitalisations, length of hospital stay, and overall healthcare costs14.
Monitoring vital signs may be seen as a reactive “firefighting” approach to telehealth, which clearly differs from I-neb Insight Online’s more proactive focus on True Adherence. However, combining the use of I-neb Insight Online with the monitoring of vital signs for the early detection of exacerbations, and other facets of CF treatment such as diet and physiotherapy, may offer an opportunity for optimising the integrated management of the major complications of CF. Depending on health status and behaviours of the individual, certain patients may benefit from specific aspects of telemedicine alone. However, for those patients with complex multisystem disorders, or multiple comorbidities, a combined approach has tremendous potential to address this highly challenging area of disease management.
References 1. Sabate, E. Adherence to long-term therapies: evidence for
action. Geneva: World Health Organization (2003). http://www.who.int/chronic_conditions/en/adherence_report.pdf, visited 13 November 2012.
2. Nikander, K., Arheden, L., Denyer, J. & Cobos, N. Parents’ adherence with nebulizer treatment of their children when using an Adaptive Aerosol Delivery (AAD) system. J. Aerosol Med. 16;3, 273-281 (2003).
3. Kripalani, S., Yao, X. & Haynes, R.B. Interventions to enhance medication adherence in chronic medical conditions. Arch. Intern. Med. 167;6, 540-550 (2007).
4. Nikander, K., Pearce, L.J., Smith, N.J. & Pritchard, J.N. The impact of electronic monitors on patients’ adherence to inhaled medications. Dalby, R.N., Byron, P.R., Peart, J.,
Suman, J.D. & Young, P.M. (Eds) Respiratory Drug Delivery, 2012. Phoenix, Arizona., Davis Healthcare International Publishing, River Grove, Illinois. 3, 673-678 (2012).
5. Onyirimba, F., Apter, A., Reisine, S., Litt, M., McCusker, C., Connors, M. & ZuWallack, R. Direct clinician-to-patient feedback discussion of inhaled steroid use: its effect on adherence. Ann. Allergy Asthma Immunol. 90;4, 411-415 (2003).
6. Burgess, S.W., Sly, P.D. & Devadason, S.G. Providing feedback on adherence increases use of preventive medication by asthmatic children. J. Asthma. 47, 198-201 (2010).
7. Lareau, S.C. & Yawn, B.P. Improving adherence with inhaler therapy in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 5, 401-406 (2010).
8. Devadason, S., Murdzoska, J., Ditcham, W., Roller, C., von Hollen, D. & Nikander, K. Lung deposition of 99mTc-DTPA from a pressurised metered dose inhaler and valved holding chamber, used with facemask or mouthpiece in children with stable asthma - A pilot study. (2012). http://www.rcjournal.com/abstracts/2012/?id=1433375, visited 16 November 2012.
9. Spencer, T., Daniels, T., Pollard, K., Agent, P., Morgan, G., Madge, S., Bilton, D. & Peckham, D. I-neb Insight Online - A telemedicine option in the treatment of cystic fibrosis. J. Cystic Fibrosis. 11(Suppl 1), S78 (2012).
10. McCormack, P., McNamara, P.S. & Southern, K. A randomised controlled trial of breathing modes for adaptive aerosol delivery in children with cystic fibrosis. J. Cystic Fibrosis. 10;5, 343-349 (2011).
11. Spencer, T., Dyche, T., Nikander, K., Smith, N.J. & Pritchard, J.N. The association of true adherence, inhalation time and treatment time for patients using the I-neb AAD system in either TBM or TIM. Dalby, R.N., Byron, P.R., Peart, J., Suman, J.D. & Young, P.M. (Eds) Respiratory Drug Delivery, 2012. Phoenix, Arizona., Davis Healthcare International Publishing, River Grove, Illinois. 3, 679-684 (2012).
12. McCormack, P., Southern, K. & McNamara, P. New nebulizer technology to monitor adherence and nebulizer performance in cystic fibrosis. J. Aerosol Med. Pulm. Drug. Deliv. 25, 307-309 (2012).
13. Daniels, T., Goodacre, L., Sutton, C., Pollard, K., Conway, S. & Peckham, D. Accurate assessment of adherence: Self-report and clinician report vs electronic monitoring of nebulizers. Chest. 140;2, 425-432 (2011).
14. Department of Health. Whole system demonstrator programme: Headline findings - December 2011. (2011). Gateway ref. 16972 http://www.dh.gov.u k / e n / P u b l i c a t i o n s a n d s t a t i s t i c s / P u b l i c a t i o n s /PublicationsPolicyAndGuidance/DH_131684, visited 16 November 2012.
John Pritchard, PhD, is CTO for Philips Respironics Drug Delivery, with global accountability for the development of advanced delivery systems for the monitoring and treatment of respiratory diseases. He has published widely in the respiratory drug delivery field, been
editor to several journals, as well as having served on the boards of two International Scientific Committees and on International Government Advisory Panels.
Therapeutic
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 31www.JforPC.com

Therapeutic
Volume 2 - Issue 432 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Optimal adherence to oral cancer therapy is of key importance to maximise treatment effectiveness in patients. With the advance of molecular target therapies, cancer treatment in more and more indications is transforming from in-hospital care towards oral treatment in an outpatient setting. With cancer becoming a chronic disease, patients are often required to take the drug indefinitely on a daily basis. Ensuring an optimal adherence to treatment over the long-term period could be a challenge. As data on the driving factors of non-adherence in oncology is scarce, a pan-European workgroup of the CML Advocates Network has conducted a pilot study which has unveiled differences of non-adherence between countries, administration types and use of adherence tools in Chronic Myeloid Leukemia. This pilot study has provided the groundwork for a larger global adherence study that is currently ongoing in 12 languages.
BackgroundChronic Myeloid Leukemia (CML) has been pioneering targeted therapies in cancer, and since Imatinib’s broad availability in 2001, the effect of intentional and non-intentional non-adherence has been observed. Noens et al. (2009) first demonstrated that non-adherence to Imatinib is very common and associated with poorer response to treatment. More recently, Marin et al. (2010) found a correlation between low adherence rate (less than 90%) and the six-year probability of achieving a major molecular response (MMR). In addition, non-adherence was found to be the main reason for losing response to CML treatment. These studies emphasise that strict adherence to the prescribed Imatinib dose is key to ensuring treatment effectiveness in patients with CML.
There is not much literature on potential reasons for non-adherence to oral anti-cancer treatments (Ruddy, 2009). Even less data is available on reasons why CML patients might be non-adherent to Imatinib therapy (Breccia, 2011; Eliasson, 2011). A number of factors may influence compliance to oral medication regimens (Partridge et al., 2002). These not only include treatment-related aspects but also individual patient characteristics and personal factors (Ruddy et al., 2009) as well as patient education, supporting self-management of patients and engaging their social network (EBMT Nurses Group, 2011). A recent study has also revealed that only 53% of CML patients reported strict adherence, with adherence being influenced by the availability of patient information, social support and concomitant drug burden (Efficace et al., 2012).
Both intentional and non-intentional non-adherence in CML are very common, but so far, the reasons, as well as the feasibility of supportive adherence tools, have not been investigated in depth.
For this reason, the CML Advocates Network, a global network of 68 leukemia patient advocacy groups in 55 countries, has run a pilot survey to gain greater understanding of CML patients’ attitudes and behaviours surrounding adherence, and to develop the questionnaire for a larger study to ultimately support physicians and patients to improve compliance and to develop adherence tools. Given the limitations of a pilot survey with small participant numbers, the primary objective was to confirm the accessibility and usability of the questionnaire in anticipation of a broader, global survey.
MethodologyThe pilot survey was provided in eight languages: Czech, Dutch, English, French, German, Hebrew, Italian and Polish. The questionnaire was developed by patient advocates and CML experts with in-kind logistical support from Bristol-Myers Squibb. Local CML patient advocacy groups disseminated the online questionnaire, based on a SNAP Surveys technical survey platform, to 10-20 CML patients per country. The survey data was compiled and analysed by an independent statistician. To determine whether the pilot survey measures are reliable, Cronbach’s alpha was employed to assess the consistency and reliability of the data results across the survey. A Cronbach’s alpha of 0.81 was produced, indicating an expectation of CML duration to be strongly associated with CML medication duration. This suggests that there is some level of reliability and consistency within the survey. Given the pilot survey’s design and distribution methods, the results are biased as the recruitment addressed rather educated, informed, younger, active patients who are online.
DemographicsIn total 150 total online responses from 10 different countries were received over a period of two weeks. Austria (n=1), Czech Republic (24), France (21), Germany (25), Israel (25), Italy (19), Netherlands (18), Poland (11), Switzerland (1) and United Kingdom (5). The responses reflect the general CML patient demographics, with the majority (96%) of patients having CML in chronic phase, a relatively even split between male (46.3%) and female (53.7%). The average age of respondents was 51 years.
ResultsOf note is that the pilot survey was not powered to be statistically significant. The pilot was designed to confirm the usefulness of the questionnaire and to develop indicators for an upcoming broader, statistically significant research work.
However, the pilot survey already indicates that there might be substantial differences in adherence across countries. When asked whether patients missed at least one dose within the past month, non-adherence rates varied from
Adherence in Chronic Myeloid Leukemia: Results of a Patient-driven Pilot Survey


Volume 2 - Issue 434 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Therapeutic
18% (Poland) to 33% (Netherlands). Self-reported overall adherence in general was even lower in most countries, with 8% (Germany) to 36% (Poland) of patients claiming to take their medicines strictly as prescribed (see Figure 1). Interestingly, patients tend to wrongly estimate their own adherence, as evidenced in the difference between patients’ reported perception of their own adherence behaviour and the reported instances of actual missed doses.
In 2009, three tyrosine kinase inhibitors were approved therapies: Imatinib, which was the gold standard for first-line CML treatment and is usually administered once daily without having any food effects. So-called approved second-generation drugs were Nilotinib, which is taken twice daily with two hours fasting before and one hour after, and Dasatinib, a once-daily oral drug without food effects. By the time of the survey, the second-generation drugs Nilotinib and Dasatinib were usually administered as a second-line treatment after Imatinib failure or intolerance, but not as a first-line treatment. Given administration regimen, side-effect profiles and the psychological impact of first-line failure may both be interesting influence factors of adherence, so the survey looked at differences in adherence between these types of treatments.
The majority of respondents were taking Imatinib (72%), while fewer were taking a second-generation tyrosine kinase inhibitor (26%). There was no difference in overall adherence between the medications (25% adherence on Imatinib, 23% on second-generation treatment). However, the reasons for missing doses appear to vary by treatment and intention: 24% of Imatinib patients missed the doses accidentally, while only 15% of patients treated with second-generation drugs forget to take their pills. In contrast, only 7% of Imatinib patients but 21% of patients with second-generation drugs consciously decided not to take their drug as prescribed.
As forgetting to take the medication is the most common reason for non-intentional non-adherence, a large proportion of patients is interested in tools to improve their adherence. Patients were asked whether they use, or would use if available, alarm clock reminders, mobile phone-based reminders, reminder phone calls, email reminders, reminders from doctors during appointments, reminders from family members, magnets at refrigerators or medication dispensers.
As Figure 2 reveals, family members reminding patients to take their medicine (41%), medication dispenser boxes (36%) and SMS reminders (19%) are the most frequently used tools today. An additional 11-20% of patients would want to use these reminder tools if they were available to them. At the same time, there is a large proportion of patients that reject these tools, with email reminders (92%), phone calls (83%), health professionals and alarm clocks (76%) being least popular. This may indicate that a significant proportion of patients do not want to be reminded in their daily life that they have cancer.
DiscussionThe pilot survey indicates that a significant proportion of patients tend to overestimate their own adherence to therapy. In other words, their perceived adherence differs from how often they report missing or skipping doses. Also, the difference on intentional and non-intentional non-adherence between first- and second-generation CML drugs, and subsequently the different motivation for adherence between first- and second-line treatment, prove the need for further needs for research on the drivers of non-adherence. A significant proportion of patients use tools to increase their adherence, but there is a large group that feels these
Figure 1: Missed dose (for any reason) and self-reported adherence level by country
Figure 2: Actual use, willingness to use and rejection of adherence tools
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 35www.JforPC.com
tools are not yet available to them. However, there is no single adherence tool for everyone, which is demonstrated by a large rejection rate of all tools in some groups. A more statistically significant survey may provide insights into which tools might work best for certain subpopulations within the patient community.
Overall, the pilot survey has strengthened our thinking that there are certain country-specific characteristics, drug- and disease-phase-related factors, as well as different drivers and tools influencing intentional and non-intentional non-adherence.
The next phase of this research work, run by a workgroup of eight European CML patient advocates and two CML experts from European countries, is currently underway. The survey is conducted online and offline and intends to have at least 2000 respondents. The questionnaire was deployed on 22 September 2012 in 12 languages (English, Spanish, German, French, Italian, Portuguese, Finnish, Dutch, Czech, Hebrew, Polish and Russian), with more than 1600 patients from 73 countries having responded in the first eight weeks. To minimise the online recruitment bias, clinicians in three national CML research groups - GIMEMA in Italy, FI LMC in France and the German CML Study Group - are cooperating with the CML Advocates Network to distribute hard-copy questionnaires to CML patients in addition to the online survey. Results of the study are expected to become available in spring 2013.
ReferencesAerts E, Kellerhals SD, Fliedner M (2011): Adherence to oral anti-tumour therapies. EBMT Swiss Nurses Group
Breccia M, Efficace F, Alimena G (2011): Imatinib treatment in chronic myelogenous leukemia: What have we learned so far? Cancer Lett 300(2): 115–121
Efficace F, Baccarani M, Rosti G, Cottone F, Castagnetti F, Breccia M, Alimena G, Iurlo A, Rossi AR, Pardini S, Gherlinzoni F, Salvucci M, Tiribelli M, Vignetti M, Mandelli F (2012): Investigating factors associated with adherence behavior in patients with chronic myeloid leukemia: an observational patient-centered outcome study. British Journal of Cancer: 2012.348
Eliasson L, Clifford S, Barber N, Marin D (2011): Exploring chronic myeloid leukemia patients’ reasons for not adhering to the oral anticancer drug imatinib as prescribed. Leuk Res 35: 626–630
Marin D, Bazeos A, Mahon FX, Eliasson L, Milojkovic D, Bua M, Apperley JF, Szydlo R, Desai R, Kozlowski K, Paliompeis C, Latham V, Foroni L, Molimard M, Reid A, Rezvani K, de Lavallade H, Guallar C, Goldman J, Khorashad JS (2010): Adherence is the critical factor for achieving molecular responses in patients with chronic myeloid leukemia who achieve complete cytogenetic responses on imatinib. J Clin Oncol 28: 2381–2388
Noens L, van Lierde MA, De Bock R, Verhoef G, Zachee P, Berneman Z, Martiat P, Mineur P, Van Eygen K, MacDonald K, De Geest S, Albrecht T, Abraham I (2009): Prevalence, determinants, and outcomes of nonadherence to imatinib
therapy in patients with chronic myeloid leukemia: the ADAGIO study. Blood 113: 5401–5411
Ruddy K, Mayer E, Partridge A (2009): Patient adherence and persistence with oral anticancer treatment. CA Cancer J Clin 59: 56–6
AcknowledgementsThe pilot survey on CML Adherence was developed and run by a workgroup of the following CML patients and experts:• Giora Sharf, Chair of the Adherence Workgroup / CML
Advocates Network / Leukemia Patient Advocates Foundation, Switzerland / Israeli CML Patients Organisation
• Jan Geissler, CML Advocates Network / Leukemia Patient Advocates Foundation, Switzerland / LeukaNET, Germany
• Felice Bombaci, Gruppo AIL Pazienti Leucemia Mieloide Cronica (Italy)
• Mina Daban, President, Leucémie Myéloide Chronique France (France)
• Anna Span, Editor LeukoNiews, Stichting Contactgroep Leukemie (Netherlands)
• Audrey Denis, Secretary, Vivre Avec La LMC (France)• Tony Gavin, Director of Campaigning and Advocacy,
Leukaemia CARE (UK)• Dr Lina Eliasson, Research Associate, Centre for Haematology,
Division of Experimental Medicine, Imperial College London (UK)
• Dr Fabio Efficace, Chairman GIMEMA Working Party on Quality of Life (Italy)
• Dr Joëlle Guilhot, Biostatistics, INSERM CIC 802, University Hospital of Poitiers (France)
The workgroup received in-kind logistical support from Bristol-Myers Squibb.
Jan Geissler is co-founder of the global CML Advocates Network, co-founder and vice president of the Leukemia Patient Advocates Foundation, and chair of Leukaemie-Online in Germany. He is Director of the European Patients’ Academy on Therapeutic Innovation,
and is acting as a patients’ representative in various steering committees and advisory boards. Email: [email protected]
Giora Sharf is co-founder of the global CML Advocates Network, co-founder and treasurer of the Leukemia Patient Advocates Foundation, and chair of the Israeli CML Patients Organization. Email: [email protected]
The patient-run CML Advocates Network connects 68 leukemia patient organisations in 55 countries on all continents. The network facilitates the sharing of best practice in CML patient advocacy, organizes an annual Global CML Advocacy Summit, and collaborates with researchers and clinicians.
Therapeutic

Volume 2 - Issue 436 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Therapeutic
Half of all patients hospitalised with a serious heart condition will make mistakes with their medications within a month of checking out of the hospital, says the latest research from Vanderbilt University Hospital and Brigham and Women’s Hospital in Boston.1 To investigate this issue, Clare Moloney, a Health Psychology Specialist with a focus on cardiovascular health, explains the ‘patient perspective’ and tells us why – and how – we can help to tackle this issue.
The Cost of Poor Heart HealthThe economic impact of coronary heart disease (CHD) in the UK alone is huge, costing taxpayers an average of £1.7 billion each year. Loss of productivity has even greater consequences: more than £3.9 billion in 2006, with 65% attributed to death and 35% to CHD-related illness.2
There is evidence to demonstrate that adherence to prescribed medication in conjunction with lifestyle modification greatly improves patient outcomes.3 Conversely, non-adherence has the opposite effect. So it is important to understand what holds patients back from taking their medications as prescribed.
Discovering What Really Drives Patients Research that considers the real issues around treatment non-adherence in Acute Coronary Syndrome (ACS) – which is an umbrella term used for patients who have had a heart attack or episode of unstable angina, has revealed insights into how patients cope with this condition, and how we can aim to support them. This research involved a literature review that was commissioned, alongside patient and Healthcare Provider (HCP) research, to uncover the real drivers of non-adherence in this patient group.
Adherence Challenges in Heart Health - RevealedThe research uncovered some interesting findings, and as with all illnesses there were a variety of patient perceptions and beliefs that led to non-adherence:
• “I was only in hospital for a couple of days; it can’t be that bad”
Although the implications of having a heart condition are very serious, advances in treatment means that many patients may now only spend a short time in hospital following an episode, leading to a misunderstanding about the seriousness of the condition.
• “Well, that’s it for me…” Research found that patients who feel a lack of control following hospitalisation and diagnosis could be ‘fatalistic’, taking the view that nothing can help their condition: either medical treatment or lifestyle changes.
• “Who are you to tell me?”
Other patients may find it hard to accept their diagnosis (particularly those who are largely asymptomatic) and therefore find it hard to accept their diagnosis or choose to rebel against the advice given as a way of avoiding facing the ‘truth’ about what has happened to them.
• ‘I was so shocked, everything’s just a blur”
For many people, receiving information at hospital discharge or in the very first recovery phases is too early.4 Patients who have very recently had a myocardial infarction (MI) or received a CHD diagnosis may not be able to absorb important information fully due to post-traumatic stress or an emotional response to their illness.
This can impair their cognitive ability to the extent that they cannot understand how to manage their medicine and lifestyle changes.5
Why Illness Perceptions Count in Heart Health

Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 37www.JforPC.com
Helping Patients get Improved OutcomesTo empower a patient to better self-manage their condition and achieve better long-term health, these underlying beliefs must be targeted. To change their behaviour, the key thing to do initially is to understand the current beliefs patients hold in relation to their illness and their treatment. Then you can work to appropriately increase their understanding about their condition by providing targeted information and getting them to objectively evaluate the reasons they hold these beliefs.
Most patients with chronic conditions must come to terms with their diagnosis, and that they are likely to be on medication ‘for the rest of their lives’, which can lead to grieving as they come to terms with the ‘death of wellbeing’.6 Other interconnected psychological effects include depression and anxiety, as well as distress at time spent away from work.
Effective adherence patient programmes should encourage patients to seek social support to help them through this process of readjustment, and provide information to share with family and caregivers, as well as giving patients strategies on how to begin to widen their support circle.
Family and Friends can Play a Vital RoleCaregivers and family have a key role to play, not only through offering support, but also by influencing beliefs. Poor social support has been linked with greater risk of recurrent cardiac events following ACS,7 while positively perceived social support leads to better long-term outcomes after MI.8 In the case of MI, congruent positive beliefs between the patient and their partner predict better outcomes and recovery.9
How HCPs can Make a DifferenceHCPs can make a real difference in addressing patients’ unhelpful beliefs about their medication. I’d say to check levels of understanding in recently diagnosed and discharged patients who may not have been able to ‘take everything in’ when they are first told. Then, further along the line, try to understand how the patient is feeling about their treatment and condition to ensure they still understand the long-term nature of ACS and the importance of appropriate adherence to help them enjoy not only day to day quality of life, but hopefully a lengthier life, too. The positive message for patients is that they can have a positive effect on their own health.
References1. Annals of Internal Medicine, July 3rd 20122. British Heart Foundation, 20103. De Backer et al., 20034. Royal College of Physicians, 2010; Timmins, 20055. Timmins, 20056. Royal College of Physicians, 20107. Lett, Blumenthal, Babyak et al., 20058. ibid. 20079. Figueiras & Weinman, 2003
Clare Moloney is the Lead Health Psychology Specialist at Atlantis Healthcare in the UK. She has an MSc in Health Psychology and is working towards her Doctorate in Health Psychology: investigating Illness Perceptions and Health Behaviour
Change in Patients with Intellectual Disabilities. She has developed behaviour change interventions across a range of disease areas, and has a keen interest in telecare and telehealth, the link between emotional wellbeing and health, and the role of music therapy within medicine. Email: [email protected]
Therapeutic


Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 35www.JforPC.com
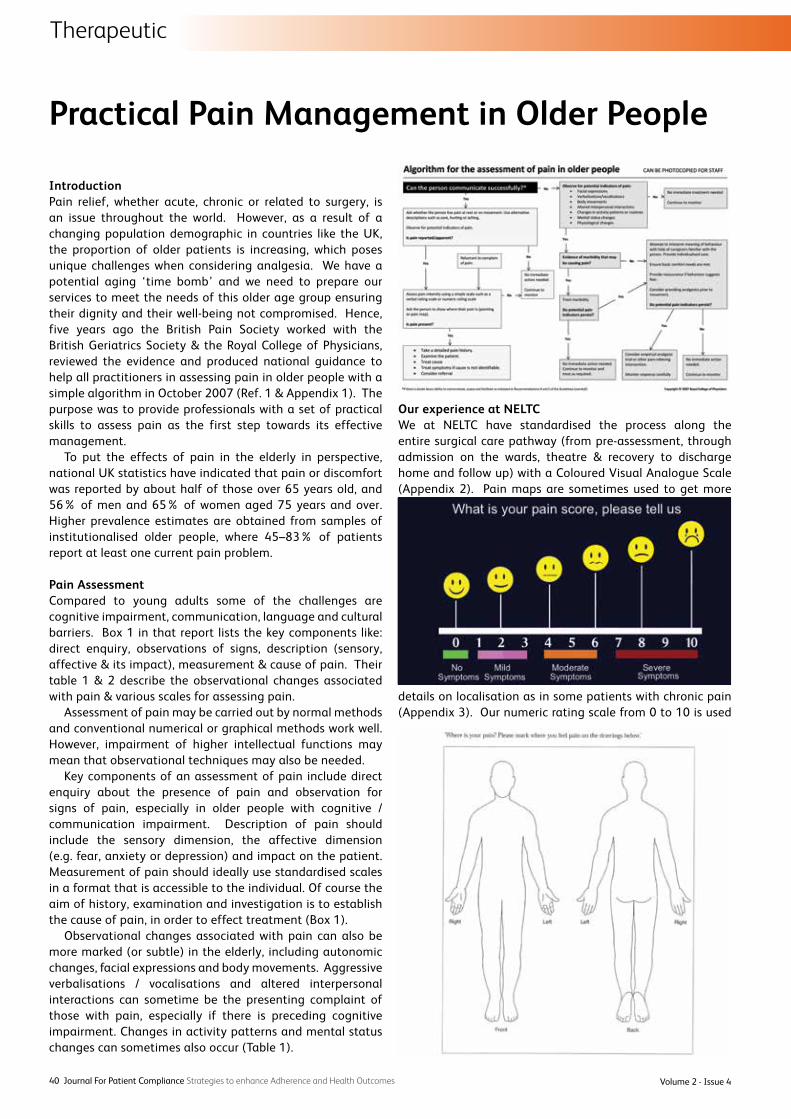
Volume 2 - Issue 440 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Practical Pain Management in Older People
IntroductionPain relief, whether acute, chronic or related to surgery, is an issue throughout the world. However, as a result of a changing population demographic in countries like the UK, the proportion of older patients is increasing, which poses unique challenges when considering analgesia. We have a potential aging ‘time bomb’ and we need to prepare our services to meet the needs of this older age group ensuring their dignity and their well-being not compromised. Hence, five years ago the British Pain Society worked with the British Geriatrics Society & the Royal College of Physicians, reviewed the evidence and produced national guidance to help all practitioners in assessing pain in older people with a simple algorithm in October 2007 (Ref. 1 & Appendix 1). The purpose was to provide professionals with a set of practical skills to assess pain as the first step towards its effective management.
To put the effects of pain in the elderly in perspective, national UK statistics have indicated that pain or discomfort was reported by about half of those over 65 years old, and 56% of men and 65% of women aged 75 years and over. Higher prevalence estimates are obtained from samples of institutionalised older people, where 45–83% of patients report at least one current pain problem.
Pain AssessmentCompared to young adults some of the challenges are cognitive impairment, communication, language and cultural barriers. Box 1 in that report lists the key components like: direct enquiry, observations of signs, description (sensory, affective & its impact), measurement & cause of pain. Their table 1 & 2 describe the observational changes associated with pain & various scales for assessing pain.
Assessment of pain may be carried out by normal methods and conventional numerical or graphical methods work well. However, impairment of higher intellectual functions may mean that observational techniques may also be needed.
Key components of an assessment of pain include direct enquiry about the presence of pain and observation for signs of pain, especially in older people with cognitive / communication impairment. Description of pain should include the sensory dimension, the affective dimension (e.g. fear, anxiety or depression) and impact on the patient. Measurement of pain should ideally use standardised scales in a format that is accessible to the individual. Of course the aim of history, examination and investigation is to establish the cause of pain, in order to effect treatment (Box 1).
Observational changes associated with pain can also be more marked (or subtle) in the elderly, including autonomic changes, facial expressions and body movements. Aggressive verbalisations / vocalisations and altered interpersonal interactions can sometime be the presenting complaint of those with pain, especially if there is preceding cognitive impairment. Changes in activity patterns and mental status changes can sometimes also occur (Table 1).
Our experience at NELTCWe at NELTC have standardised the process along the entire surgical care pathway (from pre-assessment, through admission on the wards, theatre & recovery to discharge home and follow up) with a Coloured Visual Analogue Scale (Appendix 2). Pain maps are sometimes used to get more
details on localisation as in some patients with chronic pain (Appendix 3). Our numeric rating scale from 0 to 10 is used
Therapeutic

Therapeutic
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 41www.JforPC.com
in those patients, with some difficulties, who are able to use verbal descriptor 0 to 5 scale by converting it to 0 to 10 while recording it (Appendix 4). We found this standardisation to
be very helpful in doing our routine recording of pain scores by our nurses on the wards, and also in the Pain & Sickness Audit carried out by us based on their records. This audit showed us excellent pain & sickness scores, with a high patient satisfaction rate, compared to world literature & was presented at various conferences in Birmingham (BAPIO), Wembley (BAOIA), Tel Aviv (ISA), Mumbai (ISA) & Granada (WSPC) and well received by the audience2. We followed the recommendations of the National Guidelines which are summarised (Appendix 5) along with the algorithm (Appendix 1).
Management of Acute Postoperative PainThree years ago European Society of Regional Anaesthesia and Pain Therapy produced general recommendations and principles for successful pain management postoperatively3. Effective pain management is a very important part of modern surgical practice. The goals are to: improve quality of
life, rapid recovery & early discharge with minimum morbidity. Listening to and believing in patient is the first step. Use of one scale within a hospital ensures that everyone in the team ‘speaks the same language’ of intensity of pain, from pre-assessments, wards, recovery to discharge time. This also helps in adjusting drugs for better pain management4.
Informed consent ensures detailed discussion about pain and its treatment. To keep realistic expectations of care patient participation is important and they need to know about ‘pain relief’, not a ’pain free status’. In addition to verbal information wall posters in the clinics / wards and patient leaflets are useful.
As the mechanism of pain is multi-factorial these days multimodal analgesia is recommended for a balanced combination of analgesics, co-analgesics & local anaesthetic (LA) blocks or infiltrations. Surgeons routinely use local anaesthetics before or after (preferably both), with or without other form of anaesthesia to improve pain control. Using LA before incision means patient’s analgesic requirements & side-effects are reduced, especially in those older patients with multiple co-morbidities.
The elderly present special problems in the provision of analgesia. As a general rule, the elderly report pain less frequently and require smaller doses of analgesic drugs to achieve adequate pain relief. Many patients are anxious, which may be associated with increased pain postoperatively.
Commonest drugs in use are Paracetamol, NSAIDs, Gabapentin / Pregabalin, Codeine, Tramadol, Oxycodone, Morphine in various combinations, through a step by step approach depending on the severity of pain & patient’s tolerance / intolerance of drugs. Drug dose for each drug prescribed needs to be tailored to patient requirements especially taking their age and age-related metabolic changes in consideration. Coxib or NSAIDs are used with caution in older people usually with proton pump inhibitor and routinely monitored for drug interactions, gastrointestinal, renal & cardiovascular side effects.
NSAIDs (e.g. diclofenac, ibuprofen and naproxen are amongst the most widely used medications globally for analgesia, particularly in patients with rheumatological conditions, but they can have serious side effects. Upper gastrointestinal disorders ranging from heartburn and dyspepsia are more common to peptic ulceration and gastrointestinal bleeding. Care should also be taken in patients with compromised hepatic or renal function. These drugs can also cause raised blood pressure, as well as leading to heart failure and myocardial infarction in high-risk patients, first detected in studies of selective cyclo-oxygenase inhibitors.
Self-medication with opioids is not always wise in elderly patients and thus the role of patient-controlled analgesia may be limited. The elderly may be particularly sensitive to opioids and side effects such as confusion, sedation and respiratory depression assume greater importance. Because of changes in hepatic and renal function lower doses of opioids are needed and the expected length of action may be longer.
Only one analgesic drug should be used at a time in the elderly. In general about half the normal adult dose, even less in very old, should be given at first, especially if the drug is being given intravenously. Small doses should be given regularly to anticipate pain where appropriate.

When analgesic drugs are given they may not be absorbed as well or metabolised as efficiently. In practical terms, doses of drugs such as NSAIDs and opioids in the elderly should be reduced because of a decrease in liver metabolism. In addition, since the metabolites of drugs such as morphine and pethidine are excreted by the kidneys, any decrease in renal function may lead to accumulation with repeated doses. The elderly are more likely to be receiving more than one drug for underlying medical conditions and the possibility of drug interaction is also greater.
Spinal anaesthetic (LA + opioid) is now generally more popular than Epidural, and LA infiltrations are becoming more common than Nerve Blocks. For intra-articular LA infiltrations some adrenaline, NSAID & opioids maybe indicated for better results than LA alone. Some of these drugs also help in reducing the incidence of the pain becoming chronic (beyond 3 months after surgery).
Nerve blocks are a most effective way of giving postoperative pain relief. Intercostal nerve block can aid pulmonary function after chest or upper abdominal surgery and pain below the waist can be abolished by epidural blockade aiding the return of gastrointestinal function after surgery. However, blocks spread more widely in the elderly and there may be compromise of respiratory function due to intercostal paralysis. In addition, a greater sympathetic block may occur with a consequent fall in blood pressure. With care, local anaesthetic blocks can be very useful in the elderly and give excellent pain relief whilst permitting mobilisation and rehabilitation by physiotherapists.
Non-pharmacological treatments like cold therapy with iced water bag on the joints seem to help reducing the swelling as well as pain. Fewer analgesic drugs are required, as we move towards enhanced recovery from surgery.
We have regular meetings of Anaesthetists Group and Pain Group to continue to update and improve with latest evidence and mutual agreements. Daily multi-disciplinary ward rounds headed by an anaesthetist (with overall responsibility) have been valuable for some of the improvements in quality of life, reduced morbidity, rapid enhanced recovery and early discharges. Older patients in particular may need more time commitments and mutual co-operation from all staff in a multi-disciplinary set up.
Management of Chronic PainProfessor Schofield and colleagues produced a paper reviewing the main recommendations within the guidelines by the BPS & BGS4.
Any pain beyond three months by definition is chronic. Prevalence of any pain in older persons is 0 to 93% by various estimates carried out, according to this joint report. Current pain ranged from 20-46% in the community & 28-73% in residential care. Chronic pain prevalence ranged from 25-76% in community & 83-93% in residential care. Women have a higher prevalence than men.
The three most common sites of pain in older people were: back, lower limb and other joints. This shows that millions of people live with chronic pain as if it is ‘expected to be part of ageing’ that they are ‘learning to live with’.
In addition to the drugs for acute pain these patients might need the following, initially in lowest doses: Tricyclic
antidepressants, anti-epileptics, gabapentin / pregabalin, with prophylactic anti-emetics and laxatives.
Interventional therapies showing benefits in well selected cases by Pain Clinicians include facet joint radiofrequency lesioning and intra-articular corticosteroids or hyaluronic acid injections. In acute herpes zoster & post-herpetic neuralgia LA infiltration or nerve block with LA & corticosteroids is effective. In trigeminal neuralgia in older people percutaneous procedures are preferred over microvascular decompression.
Psychological approaches like cognitive behaviour therapy (CBT) has some role and maybe relaxation, meditation, mindfulness etc.
Therapeutic
Volume 2 - Issue 442 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes

Therapeutic
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 43www.JforPC.com
Ethical & Legal Aspects of Pain managementWhile assessing & managing pain in older people some important aspects of ethics and law need to be kept at the back of our minds5&6.
Firstly, it is now important that the consent is as informed as possible, with patients having rights to refuse. Consent in various situations and in different age groups, from cradle to grave, is discussed.7&8 On the basis of the Data Protection Act 1998, Confidentiality is considered along with express consent. Risk Management includes statutes such as the Medical Acts, NHS Acts and the Health & Safety at Work Act.
It is suggested that we use Complaints Management from local resolutions to legal proceedings and ADR, in the light of Lord Woolf’s Reforms. Importance of good quality (Medical / Anaesthetic / ICU / Pain / Clinic / Hospice / Hospital) records is stressed in medical defence of any unfortunate incidents9&10. From Bolam to Bolitho is the consideration on Clinical Negligence. Here the importance of practising within the issued guidelines from public authorities, like NICE, GMC, Royal Colleges or Boards, WHO, UN and international evidence based medical (EBM) practice, is stressed. Over 40 years of practice and experiences from the USA, Canada, Europe, Balkans, Australia, New Zealand and India help us do a global comparison but we still need to tune into national guidelines, especially those drawn up by experts like BPS,BGS, RCP.
If we visit a virtual courtroom to study civil, military and criminal cases and the law governing those Medical Witnesses and Medical Experts we will see various types and grounds of Discrimination including the latest developments in this highly prevalent, but preventable, area of Employment Law. An LLM project on ‘Race Laws in the NHS’, and experience in the BMA Medical Ethics Committee are briefly mentioned.
A very significant shift in English Law, due to a European introduction (from October 2000) of the Human Rights Act 1998, is highlighted11,12,13. With this knowledge we then try to predict the likely impact on the Pain Practice with all its sub-specialties. We will certainly be looking forward to any suggestions for tackling information overload while continuing to practice evidence-based, safe pain management, anaesthesia and critical care for our older patients! Let the Medical Law continue to evolve in the West and be lead by Ethics from the East, based on Bhagavad-Gita14.
Recommendations & ConclusionBased on our recent experience & developments locally we recommend that the following steps will help us move in the right direction for better pain management in older people:1. Institutions to have Strategic Pain Groups for those
interested in the topic with a commitment for updates & continuous improvement leading to creating local champions everywhere.
2. To standardise Pain Scales with Pain Maps for better assessing pain localization & pain intensity.
3. On surgical side, to give more emphasis on acute pain management including safe use of LA in almost all patients & utilizing the skills of Anaesthetist colleagues.
4. On Medical side, to use balanced analgesic combinations mainly, seeking expert advice from Pain Clinics in chronic or acute on chronic pains or from Psychologists in selected cases.
5. Not to forget the Ethical & Legal issues in pain practice while using our National Guidelines.
In conclusion, ‘Sarve Bhavantu sukhinah, Sarve santu niramayaah’ meaning let everybody be happy, free of pain & suffering. Let’s aspire to make the world of older people free of pain so we can all look forward to a long & happy retirement too!
References1. The assessment of pain in older people National Guidelines
(October 2007) by RCP, BGS & BPS.2. Bhala B & Kozma Z, Pain & Sickness Audit in Joint
Replacement Surgery at NEL NHS TC, Ilford IG3 8YY. Presented at various conferences (2011).
3. Postoperative Pain Management – Good Clinical Practice, General recommendations and principles for successful pain management: by European Society of Regional Anaesthesia & Pain Therapy (2009).
4. Pat Schofield et al, Pain in older adults – guidelines for the management (Pain News, June 2012) by, Vol 10 No 2 p. 120-122.
5. Bhala B, Ethical & Legal Aspects of Pain Management presented at various updates & conferences (2011).
6. Giordano J. Moral Agency in Pain Medicine, Pain Physician 2006:9:41-46
7. Meisel A. et al. Seven Legal Barriers to End-of-Life Care, JAMA 2000:284:19
8. Byock I. End of life decisions and quality of care before death, BMJ 2009:339:357
9. Shapiro R.S. Healthcare providers’ liability exposure for inappropriate pain management, Journal of Law, Medicine & Ethics 1996:24:360-4
10. Furrow B.R. Pain Management and Provider Liability: No more excuses, Journal of Law, Medicine & Ethics 2001:29:28-51
11. Brennan F. et al. Pain Management: A Fundamental Human Right, Anesth Analg 2007:105:205-221
12. Schatman M.E. Ethical Issues in Chronic Pain Management 2006
13. Blacksher E. Hearing from Pain, Pain Medicine 2001:2:169-175
14. BHAGAVAD-GITA (www.yatharthgeeta.com).
Dr BalMukund Bhala TD, RAMC (V) MD (Anaesthesiology), FFARCSI, MBA (OUBS), LLM in Medical Law (UNN) Care UK Consultant Anaesthetist & Chair, Anaesthetists Group & Pain Group, North East London NHS Treatment Centre, near KGH, Ilford, Essex IG3 8YY. Member of Pain in Older Adults Special Interest Group of British Pain Society.
Dr Neeraj Bhala MBChB, MRCP, MSc(Epi.), DLSHTM, FRSPH Specialist Registrar in Gastroenterology and General MedicineQueen Elizabeth Hospital, University Hospitals Birmingham NHS Trust, B15 2TH. MRC Health of the Public Fellow Clinical Trial Service Unit, University of Oxford, OX3 7LF.
Volume 2 - Issue 444 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Modern Technology
It is not a passing fad but a permanent shift. ePharma consumers are here to stay. It means that pharmaceutical and medical device companies must adapt to the new digital environment. While change is inevitable in any industry, this may be the first time that neither industry nor regulators but rather patients are driving this shift. To understand the hesitancy of the pharma industry and FDA toward direct-to-ePharma consumers, it is helpful to look back 30 years ago to the advent of direct-to-patient advertising in 1983 in the US, by British-based Boots Pharmaceuticals. The campaign was for its prescription brand of ibuprofen [Rufen]. At the time, US regulators and major pharma companies resisted the direct-to-consumer approach. A two-year moratorium was immediately enacted by the Food and Drug Administration (and initially supported by most major pharma companies). The moratorium was intended to allow regulators time to more fully explore the ‘risks and benefits’ of going direct to consumer. While industry and FDA viewed it as risky, patients on the other hand viewed it as necessary. AIDS and breast cancer activists at the time were the most vocal patients in voicing their demands for the right to become actively involved in their healthcare knowledge and decision-making, and ironically the then US Surgeon General, C. Everett Koop, publicly called for patients to become “empowered healthcare consumers”.
Today, three decades later, in the face of digital marketing, some of the same hesitancy by regulators and industry surrounds the direct-to-ePharma consumer approach in Europe and the US. But this time in the US and Europe there is a major difference: while FDA deliberates, European agencies dismiss it, and industry’s legal, regulatory and compliance teams take time to garner institutional knowledge about digital media, patients are already leading the charge and doctors, medical centres and clinical researchers across the globe are joining them.
Technology is also propelling the broader adoption of direct-to consumer strategies globally through the use of portable digital devices, and it’s happening at warp speed, leaving industry to catch up. Today, internet penetration is over 70% in the majority of countries, enabling over 90% of patients and/or their families to conduct online research before seeking medical intervention. Furthermore, over two-thirds of adults go online looking for broader health- and pharmaceutical-related information.
This trend requires industry and more doctors to embrace the most empowered ePharma consumers that either has ever encountered. Constant internet connectivity – together with the rapid adoption of mobile devices – is changing how we market prescription products and clinical trials direct to ePharma consumers, care-givers and others.
It’s not a question of if, but when … and the answer is now.
While direct selling to patients through multiple channels has been around since the US Boots’ TV and print campaign in 1983, recent technology advances have had a significant impact on consumer behaviour, not only in healthcare but in daily living as well. By 2015, it is estimated that more than 50% of all retail sales will be either online or influenced by the online channel, demonstrating the integral use of the internet in all aspects of daily living including healthcare.
In the traditional model, industry’s principal ‘customer’ remains the doctor, who serves as gatekeeper, prescriber and learned intermediary. However, as other industries have found, their customers - consumers of all ages - are leveraging the benefits of an integrated, multi-channel approach, offering mobile applications and online options that make it easy and convenient for customers to execute transactions, access information, and make informed decisions, regardless of location.
Given how quickly patient expectations are rising, direct to consumer models that include mobile-enabled digital strategies in a constantly connected future will help differentiate a product or clinical trial from competitors. Tailored messages and information are delivered by a patient’s choice of communication: SMS, email, automated voicemail, direct mail, or a combination. On the commercial side, marketers are finding success in integrating co-pay benefit programmes to individual patient needs, on-demand access to experts, and community support.
The most successful direct-to-ePharma consumer campaigns are those that foster a more effective dialogue with patients. Engaging patients online as they are looking for information, and integrating that information with programmes that are accessible offline and through mobile, is the new model for both the commercial and clinical trial sides of the industry.
It’s not just a US phenomenon either. It’s a global one, as empowerment is occurring in countries with traditional social hierarchies. And while some doctors might prefer patients not to be well-informed, patients on the other hand expect to be able to research and obtain product information any time and anywhere, using whichever channel (or combination of channels) they find most convenient. The same goes for clinical trials as well.
Direct-to-ePharma consumer marketing requires an integrated business model where all channels – digital and physical – work together seamlessly to connect with patients and guide them to diagnosis, medical specialists, treatments and or clinical trials.
Today, ePharma consumers want access to condition education in innovative and engaging formats with personalised assessments. Condition-specific online videos for example, bring to life the experiences of real people living
Direct to the ePharma Consumer – In the Age of Connectivity

Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 45www.JforPC.com
Modern Technology
with real conditions — from allergies to Alzheimer’s — as well as care-givers and expert insights. Videos showcase challenges, questions, struggles, humour, relationships, and everyday issues of the patient and care-giver journey. For clinical trials, they ease anxiety and address concerns. Importantly, users can come back at their convenience, bookmark it, create their own playlists, rate videos, or send to a friend or family member, further expanding the reach of a direct-to-ePharma consumer campaign.
Reaching the ‘connected consumer’, today’s digital campaigns must incorporate strategies that address fundamental behaviours. These ePatient consumers are increasingly connected
• Technically through a wide array of devices,• Socially through ever-expanding social networks,• Medically through online communities of ‘consequential
strangers’ where ePatients leverage their knowledge with information exchange, and
• Economically through memberships to online pharmacies that offer discounted prescriptions and medical supplies.
The rapid growth of ePharma consumers has created new opportunities to tap into well-defined online patient communications channels for pharmaceutical marketers of prescription drugs and those promoting clinical trials directly to patients. A number of factors are driving the growth of the ePharma consumer population. Older consumers are increasingly using the internet as a search tool, with prescription drug information of particular interest in this population. In addition, many people now take multiple prescription medications; in the current economic climate ePharma consumers are carefully considering their therapeutic options. In the US, where medical costs for many are not paid for by the government, cost-conscious older consumers are heading online in search of money-saving coupons and free trials for FDA-approved treatments, while other consumers intentionally or by chance seek out clinical trials that offer free study-related medical care and treatment, and reimbursement for participation.
The rise in online direct advertising has been accompanied by a decline in offline advertising, with advertisers looking for
Guide to developing a successful direct-to-ePharma consumer strategy

Volume 2 - Issue 446 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Modern Technology
more innovative, lower-cost alternatives, and the ability to more precisely reach specific patient populations, especially for clinical trial marketing. For clinical trials, marketers must find and connect with very specific subsets of patients that meet very specific medical criteria. On the commercial side this specificity is generally not required, and direct-to-consumer campaigns target patients therapeutically – diabetes, rheumatoid arthritis, irritable bowel patients. Clinical study teams who have embraced eMarketing as an integral part of their patient recruitment strategies have generally found online media costs to be significant lower, with per-patient recruitment costs up to six times less than offline advertising. But online marketing success for clinical trials requires the artful use of market data.
Succeeding at online marketing is more than simple arithmetic. Instead, a digital marketing team that is well-versed in web-based outreach must interpret various search engine analytics, and be able to translate that information into a nuanced understanding of various search engine capabilities. Even details such as the direction in which advertisements are positioned on a web page can influence the effectiveness of outreach campaigns. An effective eMarketing campaign requires constant and daily attention and assessment of performance metrics. Dedicated digital marketing managers bring a highly-defined skill set that is required to truly launch successful digital ePharma consumer campaigns that expeditiously deliver patients to clinical trials or to a branded product.
We have learned over the past several decades of launching and implementing deeply engaging, supportive, and authentic patient activation programmes, branded products and clinical trials that a continuous supply of resources needs to be readily available for patients at every decision point, from online assessment tools, to call centre support and accessing clinical research centres on demand. We also know that different types of patients behave differently. Online patient communities have provided a window into the lives of patients, providing depth of knowledge that was not possible before. Harnessing the power of digital media, data and portable technologies can take direct-to-ePharma consumer campaigns to new heights.
Liz Moench, President and CEO of MediciGroup® Inc, has developed groundbreaking patient-centric prog-rammes for marketed products and clinical trials. Her achievements include launching industry’s first direct to consumer advertising campaign [1983],
pioneering patient recruitment for clinical trials, [1991] and optimising digital and social media for clinical recruitment, including creating some of the largest online patient comunities; Team Epilepsy, Gout Study, Lupus Team to promote clinical research. Email: [email protected]


Drug Delivery, Drug Packaging, Labelling & Dispensing
Volume 2 - Issue 448 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
AbstractAlthough significant resources are devoted to developing healthcare products that are safe and effective pharmacologically, significantly less effort is devoted to ensuring products perform as intended in the hands of providers and patients. Poor designs result in user confusion and frustration, and have the potential to lead to errors and adverse events. The interaction that occurs between people and healthcare products is an area in need of study.
The human-package interaction framework introduced by this paper is an analysis tool to support decision-making while designing and evaluating healthcare products. According to this model, any healthcare product has: a set of intended users, varied contexts of use, and a series of tasks that users must accomplish (selection of the correct product, opening, administration, reclosing, disposal, etc.). The model provides designers with a structured consideration set with regard to the interactions between people and healthcare products. Considerations to the interface are critically needed in order to reduce the occurrence of medication errors and increase adherence. Two examples are described to illustrate the concepts.
kEYWORDS: packaging, usability, adherence, non-compliance, medication error
IntroductionThe American National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP) defines a medication error as “any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the health care professional, patient, or consumer. Such events may be related to professional practice, health care products, procedures, and systems, including prescribing; order communication; product labeling, packaging, and nomenclature; compounding; dispensing; distribution; administration; education; monitoring; and use.”1
One way that medication errors manifest themselves is as an adverse drug event (ADE), defined as “injury due to medication.”2 By their nature, ADEs can be either preventable or unpreventable. Events that are attributable to product quality defects, medication errors or issues of non-compliance are examples of preventable events, while things that cannot be foreseen or avoided are unpreventable. Examples of unpreventable events include things like an unknown allergic reaction to a medication, or unavoidable side-effects, such as nausea and fatigue induced by chemotherapy.
Medication errors and non-compliance events are closely interrelated. Some researchers have even argued that some non-compliance events could be considered medical errors.3 Irrespective of how they are classified, both medication errors
and non-compliance issues are, many times, related to poor design. Consider, for example, the Office of Post-Marketing Drug Risk Assessment (OPDRA, a division of the US Food and Drug Administration), recommends interventions which include changes in the naming, labelling, or packaging of a drug product.4
Regardless of whether the product is administered by a healthcare professional, or the patient, there is an important interaction which must occur between the human and the product. However, while a significant amount of time and resources are devoted to ensuring safety and efficacy pharmacologically, the degree to which design impacts the product’s performance in the hands of patients and care-givers is given considerably less attention.5 Healthcare products that are designed and evaluated such that they catalyse medication adherence and minimise errors are sorely needed.
The correct and effective use of a drug does not simply depend on the written information of its labelling and the verbal information given by healthcare professionals; it is supported by a system of physical components such as packaging, measuring devices, applicators, dosing devices, closure systems, and the drug itself.6 All these different parts convey crucial information to patients, and their poor design is known to be a contributing factor to patient non-compliance6 and subsequent adverse events.7,8 In fact, according to the Medication Error Reporting Program (MERP) operated by US Pharmacopeia (USP) and the Institute for Safe Medication Practices (ISMP), labelling and packaging issues were cited as the primary cause of 33% of medication errors, and incited 30% of reported fatalities.
A review of the literature suggests that patient confusion and lack of accessibility are at the core of usability problems with medications:
• Confusion due to packaging similarity.6,8,9
• Confusion due to flawed dosing devices.10
• Confusion due to physical drug appearance (e.g., tablet similarity).6
• Confusion because of labelling issues: distorted text, non-flat labels, small print, lack of contrast, etc.6,8
• Confusion due to drug naming issues.8,9,11-13
• Non-accessible packaging.6,14
One critical reason for these problems is that the scientists and regulators who have historically made decisions regarding the design of these systems frequently do not understand the complexities of human ability and behaviour. The approach has generally been product-centered (PCD) in nature. That is, traditional decisions have been driven by the technical needs of the product (i.e., a drug) and manufacturing. Decisions tend to be focused on the manufacturer’s ability to maintain
A Tool for Designing and Evaluating Packaging for Healthcare Products

the product’s safety and efficacy throughout the stated shelf life, as well as the need to produce, fill and distribute the drug efficiently. User considerations and abilities generally play a secondary role in terms of importance.
We believe a more user-centred design (UCD) approach is needed. This shift is already beginning, and will likely grow, as the result of: • the costs associated with non-compliance, • global population aging, • changes in the social construct through which we view
disability, • the need for product differentiation in an increasingly
competitive marketplace, and• the social dimension of the sustainability movement.
A Comprehensive Interaction FrameworkClearly, the interaction that occurs between people (i.e., users: patients and healthcare professionals) and healthcare products is an area in need of study. To provide a framework for creating and evaluating how products perform in the hands of patients and healthcare professionals, we have adapted and combined commonly accepted models from the fields of cognitive psychology and human factors; Human Processor Model15 and Usability Theory.16
The Human Processor Model is a simplified representation of the human mind. It postulates that, in order to process information and then act upon it, humans employ three systems: a) The perceptual system: which handles sensory stimulus
from the outside world (i.e., the five senses).b) The motor system: which controls actions. c) The cognitive system: which supplies the processing to
connect the perceptual system (input) and motor system (output).
The interaction between an object (e.g., warning, label, package, etc.) and a person can be described as a cyclic information flow17 consisting of five stages (see Table 1): 1. Exposure: the user is exposed to necessary information.
Information may be in the form of the pack, features, labelling, or other components of interest.
2. Perception: information is input into one or more of the five senses.
3. Encodation: the external information gathered through perception is transformed into an internal representation. This may be associated with perceived affordances stored in the long term memory (e.g., information from other sources, previous experiences, etc.). Perceived affordances provide cues about the operation of things. They refer to the object’s characteristics that are perceived by their users regarding their potential use.18 Form, colour, texture, material, and weight of a package incite certain user’s actions.
4. Comprehension: the user recognises and assigns meaning to the encoded information, thinks about the effects of using the package features, and compares the effect of the action with the user’s goals (intentions). Goals may condition recognition and vice versa.
5. Execution: thought is then translated into actions by
activating voluntary muscles. In the case of packaging manipulations, the most important effectors are the arm-hand-finger and the head-eye systems. User’s actions, or reactions, may be instrumental or non-instrumental. Instrumental reactions include the use of a packaging feature to accomplish a goal (e.g., opening). Non-instrumental actions include things like touching a surface, etc. The user’s actions may cause a new state of things (e.g., opening accomplished, now dispensing must occur) and the cycle repeats until the user’s goals are accomplished.
According to Usability Theory, there are four principal components in a “human-machine” system, namely: user, task, tool, and environment;16 in our argument the “tool” is represented by the design of the packaged product. Since human-package interactions can be described by means of information flow, it can be inferred that success or failure at each step of the Human Processor Model (see Table 1) is dependent on the four components of Usability Theory (see Figure 1)
1. The user: the characteristics of the person, including perceptual, cognitive, and physical capabilities, beliefs, habits, previous experience, etc.
2. The task: the series of actions and goals to be accomplished, such as identifying, following instructions and directions, opening, dosing, reclosing, storing, disposing, etc.
3. The pack: the object of the interaction; the design of the package and product.
4. The context: the physical and social environment in which the interaction takes place. This includes characteristics like lighting, seating, distractions, temperature, pressures, other people, etc.
Drug Delivery, Drug Packaging, Labelling & Dispensing
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 49www.JforPC.com
Table 1 – The five stages of human-package interactions
Figure 1: The four components affecting the five stages of human-package interactions. Adapted from Shackel 16

Drug Delivery, Drug Packaging, Labelling & Dispensing
Volume 2 - Issue 450 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
The combination and adaptation of the existing models provides a framework regarding the needs, abilities, and desires of users with diverse goals in varied contexts. It can be used to inform the consideration set of variables which have the potential to influence adherence when designing for, or evaluating, package performance.
Further, these interactions can be described as an iterative loop that consists of perception, mental processing, and action that occurs within a particular context when an individual needs to perform a specific task (or series of tasks) with a packaged product (see Figure 2). The interaction is a cyclic process in which user’s actions may cause effects leading to a new state of things, and perception is then re-evaluated in terms of user’s goals.
Application to Healthcare ProductsDesigners that employ a user-centred design approach will identify users’ characteristics, contexts of use, and tasks associated with a healthcare product in order to optimise performance. For evaluation and testing purposes, this tool can be used to define testing conditions and compose user panels. Contextual conditions for testing include: the physical environment, lighting, temperature, noise, and distractions, for example.
For design and development, the framework can support several design research activities such as user observation, ethnography, task analysis, context of use analysis, product benchmarking, and so on. During design phases like concept generation, prototyping, and testing, designers and engineers have the potential to account for a variety of factors affecting the usability of healthcare products. Furthermore, key design strategies are likely to be generated by analysing and prioritising such factors.
The model can be used to guide and verify assumptions regarding the product and the target audience. Designers should observe and interview actual users carefully in order to incorporate insights about product use and verify their assumptions in an ecologically valid context. The next sections illustrate potential problems of adherence and medication errors that would benefit from a more user-centred approach to design.
To accomplish this, we use two healthcare products (see Table 2)
a) Infant’s and children’s ibuprofen: a situation dealing with dosing and drug identification issues.
b) Epinephrine injection: a situation of emergency use.
Infant’s and Children’s IbuprofenIbuprofen is a non-steroidal anti-inflammatory (NSAID) analgesic antipyretic (lowers body temperature without impairing consciousness) that, at higher doses, reduces inflammation. Our example utilises two formulations, one for infants and a second for children, both with the active ingredient ibuprofen. The infant formulation consists of a concentrated liquid oral (50 mg per 1.25 mL)19 and is intended for infants aged up to 23 months. Children’s ibuprofen is also an oral suspension. Its concentration is 100 mg of active per 5 mL19 and it is intended for children between 2 and 11 years of age. Both products are supplied in bottles. Each product has a specific dosing device: a standard syringe for the infant product and a thermoformed plastic cup for the children’s version.
The user of either product is not likely to be the actual patient. It may be a parent, a grandparent, a babysitter, or a healthcare professional. Designers will have to consider users with different levels of education, and a broad range of abilities (i.e., perceptual, cognitive, and physical) and experience.
Varied contexts of use include different rooms of a house (e.g., bathroom, kid’s bedroom, kitchen, and so on) or even an on-the-go situation (e.g., car, other house, a public place, etc). In the worst case scenarios, light might be inadequate, for example, because it’s late at night and parents simply do not want to awaken the child.
Typical tasks include storing, identifying the correct product from among many, locating and understanding correct dosage information, opening child-resistant packages, dispensing and measuring by means of a dosing device, reclosing, and, eventually, disposal. The challenge is to simultaneously consider the factors presented in the model in order to optimise the likelihood of successful administration of the product. For instance, locating and comprehending the correct dose might be particularly challenging for users not familiar with metric units or not formally trained regarding medications, but may be readily understood by those who are.
If the dosing device is designed in such a fashion that it is difficult to perceive (e.g. poor contrast, inadequate
Figure 2: Human-package interaction framework. Adapted from Shackel, Card, and Monk. 15-17
Table 2: Summary breakdown of users, contexts of use and tasks for two common healthcare products

Journal For Patient Compliance Strategies to enhance Health Outcomes 51www.JforPC.com
embossing of units or text that is too small), mistakes could be made even if the care-giver thoroughly understands the dosing instructions. These difficulties can be further exacerbated by the context undergirding the interaction, such as the lighting of the environment and the condition, location and behaviour of the child, which have the potential to add stress to the difficulty.
A specific combination of events may conspire to confuse the user, inducing them to dose a child with the more concentrated infant product using the wrong dosing device, ultimately resulting in a medication error. For instance, different standard syringes might be available to the user, with no markings identifying their respective drug product. As such, a child could receive the right drug at the right dose but in the wrong concentration because of an identification problem related to the packaging and dosing device.
Inconsistencies in the measuring devices for children’s liquid oral dosages that are likely to lead to care-giver confusion are documented.10 In fact, largely as the result of numerous, documented, unintentional overdoses involving liquid oral formulations, both the industry20 and the US Food and Drug Administration (FDA) have released guidances regarding the inclusion, markings and abbreviations appropriate to these devices.21
Epinephrine Injection Epinephrine is generally administered parenterally; typically in the form of an injection used to treat life-threatening allergic reactions caused by insect bites, foods, medications, latex, and other causes.22 It is packaged in varied forms, which include a single-dose pre-filled automatic injection device that is applied in a “swing and stab motion” into the thigh. Patients and their care-givers are instructed to administer epinephrine at the early signs of a serious allergic reaction (as indicated by swelling redness, etc.).
Users of epinephrine injections have a wide range of abilities, as they include children to older adults, and the drug
may be self-administered or administered by a care-giver (e.g. healthcare professional, parent, teacher, babysitter, etc.). Care-givers, in particular, may or may not be familiar with the appropriate use of the device that delivers the drug. Given the critical context of use (time is of the essence in a potentially life-threatening situation) and the varied experience levels of those likely to administer the drug, clear and simple directions regarding this product are paramount.
This product will always be used under a high level of stress and rush induced by the emergency nature of the need for it. Other characteristics of the context of use are incredibly varied and will likely include: outdoors, indoors, public places, homes, schools, vehicles, etc. A usage scenario can be conjured for literally any place.
The set of tasks include carrying the device (some users may actually “holster” this drug to themselves due to the time-critical nature of its use), identifying the needle tip, removing its safety feature, holding the device in the right position, and administering the drug successfully (which in and of itself has a series of steps). These steps may look easy to replicate, but the combination of poorly designed devices, untrained users, limited time for reasoning, and a stressful context complicate the process, making clear and straightforward design requisite for success, with potential life-threatening implications resulting from poor designs.
ConclusionsA majority of efforts regarding the design and evaluation and drugs is devoted to understanding the chemical aspects of the packaged product so that it is assured to be safe and efficacious throughout its stated shelf life. Yet, in virtually every instance of healthcare, there are people (be they the patient themselves or a care-giver – trained or untrained) who must interact with the packaged product such that it is administered safely and effectively. As a result, the safety of patients is partially dependent on a system of physical components such as packaging, measuring devices,
Drug Delivery, Drug Packaging, Labelling & Dispensing

applicators, dosing devices, closure systems, and the drug itself.6 These components convey important information regarding the safe and effective use of the products.
The human-package interaction framework (presented herein) indicates that any healthcare product has a set of intended users, a set of contexts of use, and a series of specific tasks that must be accomplished. The framework serves to support the design and evaluation of products in an attempt to reduce the occurrence of medications error and increase adherence.
References 1. National Coordinating Council for Medication Error
Reporting and Prevention. About medication errors: What is a medication error? 2007; http://www.nccmerp.org/aboutMedErrors.html. Accessed March 16, 2011.
2. Bates DW, Cullen DJ, Laird N, et al. Incidence of adverse drug events and potential adverse drug events. JAMA: The Journal of the American Medical Association. 1995;274(1):29-34.
3. Barber N. Should we consider non-compliance a medical error? Quality and Safety Health Care. 2002;11:81–84.
4. US FDA. FDA 101: Medication Errors. 2009; http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm048644.htm. Accessed March 18, 2011.
5. DeWalt DA. Ensuring safe and effective use of medication and health care. JAMA: The Journal of the American Medical Association. 2010;304(23):Published online November 30, 2010.
6. Ward J, Buckle P, Clarkson JP. Designing packaging to support the safe use of medicines at home. Applied Ergonomics. 2010;41(5):682-694.
7. Food and Drug Administration. Guidance for industry. Dosage delivery devices for OTC liquid drug products. November, 2009; http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM188992.pdf. Accessed December 6, 2010.
8. Berman A. Reducing medication errors through naming, labeling, and packaging. Journal of Medical Systems. 2004;28(1):9-29.
9. McCoy LK. Look-alike, sound-alike drugs review: include look-alike packaging as an additional safety check. Joint Commission Journal on Quality and Patient Safety. 2005;31(1):47-53.
10. Yin HS, Wolf MS, Dreyer BP, Sanders LM, Parker RM. Evaluation of consistency in dosing directions and measuring devices for pediatric nonprescription liquid medications. JAMA: The Journal of the American Medical Association. 2010;304(23):Published online November 30, 2010.
11. Kenagy JW, Stein GC. Naming, labeling, and packaging of pharmaceuticals. American Journal of Health-System Pharmacy. 2001;58(21):2033.
12. Lambert BL, Lin SJ, Chang KY, Gandhi SK. Similarity as a risk factor in drug-name confusion errors: the look-alike (orthographic) and sound-alike (phonetic) model. Medical Care. 1999;37(12):1214-1225.
13. US Pharmacopeia. Look-alike/sound-alike drug products affect cognition. 2004; http://www.usp.org/pdf/EN/patientSafety/capsLink2004-05-01.pdf. Accessed
December 21, 2010.14. de la Fuente J. The use of a universal design methodology
for developing child resistant drug packaging. East Lansing: School of Packaging, Michigan State University; 2006.
15. Card SK, Moran TP, Newell A. The psychology of human-computer interaction. Mahwah: Lawrence Erlbaum Associates, Inc.; 1983.
16. Shackel B. Usability - Context, framework, definition, design and evaluation. Interacting with Computers. 2009;21(5-6):339-346.
17. Monk A. Cyclic interaction: a unitary approach to intention, action and the environment. Cognition. 1998;68(2):95-110.
18. Norman DA. The psychology of everyday things. New York, NY, USA: Basic Books.; 1988.
19. All about kids Pediatrics. Ibuprofen dosage. 2011; http://www.allaboutkidspediatrics.com/parents/dosage.html. Accessed March 19, 2011.
20. Consumer Healthcare Products Association. Guideline Volumetric Measures for Dosing of Over-the-Counter Liquid Oral Drug Products for Children ≤ 12 Years of Age. 2010; http://www.chpa-info.org/scienceregulatory/Voluntary_Codes.aspx#volumetricmeasure. Accessed March 21, 2011.
21. US Department of Health and Human Services US Food and Drug Administration. Guidance for Industry: Dosage Delivery Devices for OTC Liquid Drug Products. In: (CDER) CfDEaR, ed2009.
22. PubMed Health. Epinephrine Injection. 2008; http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0000211/. Accessed March 19, 2011.
Javier de la FuenteJavier is co-director of Factor IDD, a design consulting company specializing in packaging and product design. He is pursuing a doctorate at the Michigan State University School of Packaging. His current research focuses on usability
issues of flexible packaging. He earned his Master of Science degree from the same school and holds a five-year degree in Industrial Design from the University of Buenos Aires, Argentina. Email: [email protected]
Laura Bix, Ph.D. Dr. Bix is an Associate Professor at the School of Packaging at Michigan State University. She was appointed, and currently serves as the US delegate to ISO TC122 WG 9, a group which is developing a standard for measuring
the accessibility of packages. Bix served as the Vice-Chair of Committee D10.32, the Committee on Consumer, Pharmaceutical and Medical Packaging, from 2004-2007, and as a member of Committee F-02, the flexible barrier material committee, from 2002-2008. In 2008 she was named one of the 100 most notable people in the medical device industry by Medical Devices and Diagnostics Industry. Email: [email protected]
Drug Delivery, Drug Packaging, Labelling & Dispensing
Volume 2 - Issue 452 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes

Drug Delivery, Drug Packaging, Labelling & Dispensing
Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 53www.JforPC.com

Volume 2 - Issue 454 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Pharma patient adherence budgets have increased 281 percent in four yearsPatient adherence is a hot topic for the healthcare industry because it can impede or undermine patients’ recovery or a chronic condition. Non adherence costs an estimated $290 billion in hospitalization stemming from complications. For the pharmaceutical industry, improving it could provide a way to save millions in lost revenue. An effective plan by a pharmaceutical company could pave the way to a favorable spot on a formulary.
As startups, providers and pharmaceutical firms develop ways to solve this critical problem, a new report has highlighted some interesting trends. Pharmaceutical companies are devoting more budget spend to patient adherence teams and allocations to digital programs have spiked in the past year.
In the past four years US pharmaceutical companies’ patient adherence budget allocations have jumped 281 percent from $400,000 in 2009 to $1.5 million in 2012. But more importantly there is an increasing recognition that understanding patients and their motivations will help pharmaceutical companies better engage them and make adherence programs more successful. Here are some of the most interesting findings in a patient adherence survey by Cutting Edge Information in Durham, North Carolina. JCS – Staff Writer – Maria Alvarez
Patient Portals – From Doctor to PatientWith the advent of social media platforms such as Facebook and Twitter, a tremendous hype was generated by being in constant touch with one another. By virtue of this phenomenon, staying in touch round the clock via instant messaging where any physical boundaries or restrictions were absent became the new norm. This simple and effective means of communication delivered a great value for all business entities alike. The absence of employing such useful technology would project a negative image into the mind of your clients. Health IT vendors could not afford to lose in this department; hence, to provide a solution to this predicament patient portals emerged. Through the introduction of patient portals by established EMR vendors, hassle for patients along with physicians was significantly reduced.
’Patient Portals provide a platform for patients to stay connected with their providers. Instantaneous access to all the patients’ reports, scheduling appointments etc. has made life easy for patients comprehensively. These portals eliminate the requirement for making phone calls every time a patient might have a health related query. It was never as simplistic to manage your patients’ health prior to patient portals’, says an Ohio based physician.
For the healthcare industry today, the Patient Portal
has emerged as the definitive platform for better patient engagement. The technology is so simplistic in nature that patients find it very user friendly to utilize and can operate it almost immediately with little or no training. All any patient has to do is simply login to the online web based portal in order to remain connected with their doctor.
They can do this from any place and at any time; needless to say that this freedom of mobility ensued in numerous benefits. Now both patients and doctors didn’t have to incur the unnecessary costs on lengthy phone calls to one another. Reports could be obtained online, alongside other relevant medical information. Even requesting refills and scheduling appointments was made simple, at the convenience of just a few clicks away.Source: Cutting Edge
Online survey on the management of patient adherenceResearchers at Keele University have launched an online survey to learn about health care professionals’ (doctors, pharmacists and nurses) approach to supporting patients with taking medicines and promoting adherence.
Dr Wendy Clyne and colleagues at NPC Plus, Keele University, are coordinating the survey which is part of a larger project on medicines adherence called the ‘ABC project’ (www.abcproject.eu/) funded by the European Commission. The survey is taking place in countries across Europe including Austria, Belgium, France, Germany, Greece, Hungary, Italy, Portugal, Poland, Switzerland, The Netherlands and England. The survey will run until the end of March 2012.
The survey aims to investigate health care professionals’ perceptions of the extent and nature of non-adherence, as well as the things that health care professionals do to support patients with medication taking.
JOURNAL FOR
Strategies to enhance Adherence and Health OutcomesPATIENT COMPLIANCE✓

Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes 55www.JforPC.com
JPC News
The study also aims to find out about any barriers to supporting adherence as reported by doctors, pharmacists and nurses. Dr Clyne, Head of the Medicines Partnership Programme at NPC Plus, said ‘With more patients taking medicines than ever before, encouraging patients to get the most out of their medicines is essential to avoid unnecessary ill health as well as reduce waste and unnecessary cost. We are really interested to find out what healthcare professionals do to support patients with medicine taking, and how effective they think their actions are. At the end of the study we should have a really clear picture of the role of these three key professional groups in supporting patients with medicines, how that support fits together, and whether we have a consistent picture across Europe, or whether there are variations in practice from one country to another.’Source: Cutting Edge
Patient adherence predicts ankle surgery healingFocusing on postoperative care may be the optimal way of reducing healing complications following ankle fracture surgery, say US researchers.
The team from the Thomas Jefferson University Hospital in Philadelphia, Pennsylvania, reports that surgical debridement was required by just six (1.25%) of 478 patients who underwent open ankle reduction and internal fixation between 2003 and 2010. A further 14 (2.9%) patients needed additional wound dressing or oral antibiotics during healing.
Nevertheless, multivariate analysis identified several risk factors for postoperative wound complications among this population.
Specifically, patients were significantly more likely to have wound complications if they had diabetes (odds ratio [OR]=3.61) or an open fracture (OR=13.43), and if they used wound-compromising medications (OR=6.75), such as corticosteroids.
Furthermore, delayed wound healing was a significant 3.66 times more common in patients who were nonadherent to postoperative instructions, such as avoidance of weight bearing for at least 6 weeks, compared with patients who followed their physician’s advice.
The risk for wound complications also rose significantly with increasing patient age, say Adam Miller and co-authors.
“While most risk factors cannot be controlled, postoperative care is an area of importance for wound-healing,” writes the team. “The adherence to postoperative instructions should be emphasized, and the treating surgeon should remain vigilant to the potential effect that noncompliance may have on wound-healing after surgical intervention.”
The researchers note in the US edition of the Journal
of Bone and Joint Surgery that there was a trend toward an increased risk for wound complications in patients who underwent surgery within 5 days of injury compared with at a later date, but that this did not reach significance.They were also unable to demonstrate any impact of preoperative swelling on the risk for wound complications in their study due to the subjective nature of the analysis.Believing these two factors may nevertheless have significance in wound healing, they add: “This conjecture needs to be confirmed in a future randomized comparative study.”JCS – Staff Writer – Maria Alvarez
Attitudes Predict Ability To Follow Post-Treatment AdviceWomen are more likely to follow experts’ advice on how to reduce their risk of an important side effect of breast cancer surgery - like lymphedema - if they feel confident in their abilities and know how to manage stress, according to new research from Fox Chase Cancer Center presented at the 2012 CTRC-AACR San Antonio Breast Cancer Symposium on Saturday, December 8, 2012.
These findings suggest that clinicians must do more than just inform women of the ways they should change their behavior, says Suzanne M. Miller, PhD, Professor and Director of the Psychosocial and Biobehavioral Medicine Program at Fox Chase and study author. Doctors and nurses should also provide strategies for women who feel less empowered to make those changes, and have fewer skills for reducing their stress.
“Women are in charge of their future, because there are things they can do to minimize the effects of treatment,” says Miller. “If they get into a routine of doing them, it will reduce their stress and vulnerability.”
The study, funded by the U.S. Department of Defense, focused on the side effect of surgery known as lymphedema - an incurable build up of fluid in the lymph nodes that can cause swelling and affect range of motion. In more severe cases, it can be quite painful. The rate of lymphedema can vary, but a significant proportion - perhaps as many as half - of women will develop it after undergoing surgery to remove breast cancer.
“That advice may sound easy to follow, but the reality is quite different,” says Miller. To truly follow these recommendations, she says, women have to forever change and monitor their behavior - moisturize the arm on the side of surgery several times per day, use an electric shaver instead of a razor, wear gloves when doing housework or physical activity, avoid tight jewelry or clothes, stop carrying heavy objects, and constantly protect the arm from being jostled or squeezed, for instance. “These changes are going to be very intrusive into a woman’s everyday life,” says Miller.Source: NHS Health News

Volume 2 - Issue 456 Journal For Patient Compliance Strategies to enhance Adherence and Health Outcomes
Drug Delivery, Drug Packaging, Labelling & Dispensing
Advertisers IndexPage 29 9th Annual Patient Summit Europe 2012 - EyeforPharma
Page 33 10th Annual Conference on Controlled Release
Page 53 11th Annual Eyeforpharma Barcelona 2013
Page 3 90 Ten Healthcare
IFC Atlantis Healthcare
Page 23 Bobst
Page 38 & 39 CRF Health
IBC Health Window
Page 11 Memotext
OBC MediciGlobal
Page 19 Mobile PRM
Page 47 Patient Summit USA 2013
Page 7 PCC Hellas
Page 27 Pharma Publications
Page 5 Pharmexx
Page 15 Vitaphone Nederland BV
JOURNAL FOR
Strategies to enhance Adherence and Health OutcomesPATIENT COMPLIANCE✓
Subscription offerGuarantee you receive your copy of JPC:4 issues per year. Pharma Publications is delighted to be able to offer it’s readers a great one year’s subscription offer.
Subscribe now to receive your 20% discount
Post: Complete form below, detach and post to: Pharma Publications, Unit J413, The Biscuit Factory Tower Bridge business complex 100 clements road, London SE16 4DG
Tel: +44 (0)20 7237 2036 Fax: Complete and fax this form to +44 0014802475316
Email: Your details to [email protected]
Please tick the relevant boxes below:
UK & N. Ireland £120 inc p&pEurope €130 inc p&pUSA $200 inc p&pI enclose a cheque made payable to Pharmapubs
I wish to pay by credit card (Mastercard or Visa)
Card number
Valid from Expiry date
Security code
Name:
Job title:
Company:
Address:
Postcode
Tel:
Fax:
Email:
Signature































