Embed Size (px)
Citation preview

Manuscript Accepted Peer Reviewed | Early View Article
Page 1 of 16
Early View Article: Online published version of an accepted article before publication in the
final form.
Journal Name: Journal of Case Reports and Images in Obstetrics and Gynecology
Type of Article: Case Report
Title: Hysteroscopcally-Guided Subchorionic Methotrexate Administration, a New
Technique for Termination of Cesarean Scar Pregnancy
Authors: Giancarlo Garuti, Stefania Calabrese, Lorenzo Quirino, Marco Di Mario
doi: To be assigned
Early view version published: December 2, 2015
How to cite the article: Garuti G, Calabrese S, Quirino L, Mario M D. Hysteroscopcally-
Guided Subchorionic Methotrexate Administration, a New Technique for Termination of
Cesarean Scar Pregnancy. Journal of Case Reports and Images in Obstetrics and
Gynecology. Forthcoming 2015.
Disclaimer: This manuscript has been accepted for publication. This is a pdf file of the
Early View Article. The Early View Article is an online published version of an accepted
article before publication in the final form. The proof of this manuscript will be sent to the
authors for corrections after which this manuscript will undergo content check,
copyediting/proofreading and content formatting to conform to journal’s requirements.
Please note that during the above publication processes errors in content or presentation
may be discovered which will be rectified during manuscript processing. These errors may
affect the contents of this manuscript and final published version of this manuscript may
be extensively different in content and layout than this Early View Article.
Manuscript Accepted Peer Reviewed | Early View Article
Page 2 of 16
TYPE OF ARTICLE: Case Report 1
2
TITLE: Hysteroscopcally-Guided Subchorionic Methotrexate Administration, a New 3
Technique for Termination of Cesarean Scar Pregnancy 4
5
AUTHORS: 6
Giancarlo Garuti1, Stefania Calabrese1, Lorenzo Quirino1, Marco Di Mario1 7
8
AFFILIATIONS: 9
1MD, Obstetrics and Gynecology Department, Public Hospital of Lodi, Via Savoia 1, 10
26900-Lodi, Italy 11
12
CORRESPONDING AUTHOR DETAILS 13
Giancarlo Garuti (MD), Obstetrics and Gynecology Department, Lodi Hospital, via 14
Savoia n° 1, 26900-Lodi, Italy 15
Phones: 39.371.372349, 39.338.2702675 16
Email: [email protected] 17
18
Short Running Title: CSP treatment by hysteroscopically-guided MTX 19
administration 20
21
Guarantor of Submission : The corresponding author is the guarantor of 22
submission. 23
24
25
26
27
28
29
30
31

Manuscript Accepted Peer Reviewed | Early View Article
Page 3 of 16
TITLE: Hysteroscopcally-Guided Subchorionic Methotrexate Administration, a New 32
Technique for Termination of Cesarean Scar Pregnancy 33
34
ABSTRACT 35
36
Introduction 37
Cesarean Scar Pregnancy (CSP) is a rare but life-threatening condition, due to the 38
risk of uterine rupture or for the development of placenta previa/accreta. The 39
mainstay of management to spare fertility is early diagnosis and pregnancy 40
termination. Although several conservative treatments have been experienced, no 41
consensus on the best therapeutic approach is currently shared. The medical 42
therapy for CSP termination is based on systemic or local Methotrexate (MTX) 43
administration. Hysteroscopy allows the precise visualization of placental 44
implantation and it can be used to drive MTX injection selectively within the 45
intervillous placental spaces. This procedure increases drug concentration delivered 46
to the target tissue, potentially improving its therapeutic index. 47
48
Case Report 49
A 36-years-old patient with history of cesarean section was admitted to our 50
Department with a diagnosis of viable 7th weeks CSP. The patient gave her consent 51
to pregnancy termination by a hysteroscopically-guided MTX administration within 52
the cervico-isthmic placental implantation site, followed by its resectoscopic removal. 53
In an office setting, 80 mg of MTX were injected through a needle adaptable to the 5-54
Fr operative channel of hysteroscope, under the chorionic membrane of placental 55
implantation site. The duration of the procedure took 3 minutes and it resulted easy, 56
painless and uneventful. An early embryo demise was obtained; the human 57
Chorionic Gonadotropin-beta subunit (beta-hCG) serum trend showed a rapid 58
pregnancy termination and no patient complaints were recorded. After 28 days, a 59
resectoscopic removal of the gestational sac and placenta was safely accomplished. 60
61
62
63

Manuscript Accepted Peer Reviewed | Early View Article
Page 4 of 16
Conclusion 64
Selective hysteroscopic administration of MTX within intervillous spaces of the 65
ectopic placental implantation is effective and it can be considered for CSP 66
termination. 67
68
Keywords: Cesarean Scar Pregnancy, Methotrexate, Hysteroscopy, Ectopic 69
pregnancy, Office hysteroscopy, Resectoscopy 70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94

Manuscript Accepted Peer Reviewed | Early View Article
Page 5 of 16
TITLE: Hysteroscopically-Guided Subchorionic Methotrexate Administration, a New 95
Technique for Termination of Cesarean Scar Pregnancy 96
97
INTRODUCTION 98
Cesarean Scar Pregnancy (CSP) is a rare but potentially life-threatening condition, 99
caused by a placental implantation within a retracted scar of cervico-isthmic uterine 100
junction, deriving from a previous Cesarean Delivery (CD) [1]. Firstly described in 101
1978, CSP was more frequently reported in the last decades, due to the increasing 102
rates of CD. In patients with history of CD, the CSP incidence varies from 1:500 to 103
1:1500 [1, 2, 3]. If untreated, CSP exposes the patient to the risk of uterine rupture 104
and hemorrhage during the first pregnancy months or to the development of a 105
placenta previa/accreta near pregnancy termination [4, 5]. The mainstay 106
management aimed to spare fertility and to reduce maternal morbidity, is an early 107
diagnosis and pregnancy termination [6]. The current treatment of CSP is based on 108
case reports and small case series, with more than 30 therapeutic options described 109
[1, 3]. Even if recent studies compared different managements of CSP, no guidelines 110
have been given until now [7, 8]. The dihydrofolate-reductase (DHFR) enzyme 111
inhibitor, Methotrexate (MTX), administered by systemic, loco-regional or 112
intragestational-sac routes, is the cornerstone of medical therapy, followed or not by 113
surgical removal [1, 3, 6, 9]. Due to the reversible and competitive nature of MTX 114
binding to DHFR, drug concentration within target-cell is a major determinant of 115
cytotoxicity [10]. Among the surgical techniques suggested for CSP removal (uterine 116
dilatation and curettage, laparotomy, laparoscopy, vaginal excision and 117
hysteroscopy), hysteroscopy resulted to be effective and showed a low morbidity-118
rate [3, 11, 12]. Based on the knowledge of MTX pharmacokinetics [10] and 119
assuming that its selective administration within the placental intervillous spaces can 120
enhance its cytocidal effects, we report the case of a patient with a viable CSP 121
managed by hysteroscopically-guided sub-chorionic MTX administration, delivered at 122
the placental implantation. The procedure was completed by the resectoscopic 123
removal of the terminated pregnancy. 124
125
126

Manuscript Accepted Peer Reviewed | Early View Article
Page 6 of 16
CASE REPORT 127
In April, 2015, a 36-years-old woman with a positive urine pregnancy test and 8 128
weeks of amenorrhea, was admitted to our Department due to pelvic cramping pain 129
and ultrasound evidences of a viable CSP. No gynecological complaints were 130
recorded; her past obstetric history revealed a CD due to breech presentation and a 131
vaginal delivery 11 and 3 years before, respectively. Pelvic examination detected a 132
movable uterus with a smooth, painless and soft mass measuring about 2.5 cm, 133
arising from the cervico-isthmic area and expanding toward the bladder base. Serum 134
beta-subunit of human Chorionic Gonadotropin (beta-hCG) concentration was of 135
18000 mUI/ml. Transvaginal Ultrasonography revealed empty endometrial cavity and 136
empty cervical canal, the gestational sac measuring 17x14 mm was embedded 137
deep within the uterine wall at the level of the cervico-isthmic junction, bulging 138
ventrally towards the bladder (Figure 1). It contained an embryonic pole showing 139
heart activity and measuring 4.6 mm, corresponding to 7th pregnancy weeks (Figure 140
2). The measurement of myometrial thickness between gestational sac and bladder 141
base was 1.5 mm. Color-Doppler and spectral analysis showed a high blood-flow 142
with low resistances around the cervico-isthmic area. Based on these findings and 143
according to published data, a diagnosis of viable CSP was made [6]. With the 144
assumption that pregnancy termination was indicated and no guidelines were 145
provided to treat CSP, we proposed to the patient local MTX administration through 146
hysteroscopy guidance, followed by the resectoscopic removal of pregnancy. The 147
patient signed an informed consent and an informative chart about the risk of 148
hemorrhage. The first procedure was carried out in an office setting. By the 149
vaginoscopic technique without analgesia or anesthesia, a double-flow 5-mm 150
hysteroscope (Karl Storz, Tuttlingen, Germany) was used to administer 50 mg/m2 of 151
MTX in 2 cc of saline, through a 17-gauge needle adaptable to the 5Fr operative 152
channel. Continuous saline flow was delivered at working pressure set at 60 mm/Hg 153
by an electronic irrigation-suction device. After the visual confirmation of a ventral 154
uterine pregnancy implantation within the cesarean scar, we entered the chorionic 155
sac by using hysteroscopy scissors, opening sequentially capsular decidua, chorion 156
leave and chorionic membrane. After needle insertion within the operative channel, 157
MTX has been injected 2-3 mm deep the chorionic membrane at the level of anterior 158

Manuscript Accepted Peer Reviewed | Early View Article
Page 7 of 16
implantation of the placenta, i.e. directly within the placental intervillous spaces 159
(Figure 3). The procedure lasted 3 minutes, it was painless, and the patient was 160
discharged after 2 hours of uneventful observation. Clinical, sonographic and beta-161
hCG monitoring were recommended after 4, 7, 14 and 21 days from MTX 162
administration. During the follow-up period a light vaginal bleeding was the only 163
complaint recorded. No embryonic heart activity was found after 4 days while the 164
persistence of gestational sac within the cesarean scar was found until the 21th day. 165
Beta-hCG increased to 29000 mUI/ml after 4 days, decreasing to 18000 mUI/ml, 166
5000 mUI/ml and 3000 mUI/ml after 7, 14 and 21 days, respectively. After 28 days, 167
observing a further drop of beta-hCG to 500 mUI/ml, the hysteroscopy removal of 168
CSP was planned. The intervention was carried-out under conscious sedation, using 169
a 27Fr resectoscope armed with a 4mm bipolar loop (Versapoint Bipolar System, 170
Gynecare, Ethicon Inc., Menlo Park, CA, USA) set at 100w power. Due to the soft 171
consistency of the cervix, its dilatation was avoided. Saline solution was delivered as 172
uterine distension medium at 60 mm/Hg working pressure. After CSP identification 173
(Figure 4 and 5) the intervention was almost entirely managed by using the cold loop 174
to separate villous trophoblast from the cervico-isthmic niche, following a loose 175
cleavage plane maintained between tissues (Figure 6). The application of 176
coagulating current for bleeding control was not necessary. The intervention lasted 8 177
minutes, an uneventful recovery followed and the patient was discharged on first 178
post-operative day. Villous trophoblast and embryonic tissues were found at 179
pathology assessment. After intervention, beta-hCG decreased to a non-pregnancy 180
range after 15 days. The first menstrual period was recorded after 32 days and no 181
abnormalities were found both at physical and ultrasound examination after 40 days 182
from intervention. 183
184
DISCUSSION 185
The main metabolic pathway leading to MTX cytotoxicity is represented by a tight but 186
reversible inhibition of DHFR. The DHFR enzyme plays a key role in maintaining 187
intracellular folate homeosthasis and it is responsible for the conversion of 188
dihydrofolate substrates to tetrahydrofolates. Tetrahydrofolates play an essential role 189
in synthesis of DNA and RNA precursors such as purine and pirimidine rings. With 190

Manuscript Accepted Peer Reviewed | Early View Article
Page 8 of 16
respect to natural dihydrofolates substrates, the competitive reversible nature of the 191
MTX binding to DHFR, leads to two critical determinants of cytotoxicity: drug cell 192
concentration and duration of drug cell exposure [10]. These pharmacokinetic 193
principles, combined with the short drug half-life and the poor blood supply to scar 194
tissue surrounding a CSP, are the main causes of the low therapeutic index 195
associated with systemic MTX administration [1, 3, 10]. Driving MTX directly to the 196
target tissue may lead to an excess of free drug cell concentration required to fully 197
inhibit the enzyme, potentially enhancing its clinical effectiveness. Accordingly, 198
ultrasound-guided MTX administration within the gestational sac showed an 199
improvement of clinical results with respect to systemic MTX and it is now 200
considered the first choice for CSP conservative treatment [3, 4, 13, 14]. However, 201
as reported in 26%-39% of cases [13, 14] pregnancy absorption takes long time and 202
possible failures require additional treatments. The target tissue of MTX is the villous 203
trophoblast of the blastocyst implantation site, leading to the placental differentiation 204
within the cesarean scar niche. The placental growth inhibition leads to pregnancy 205
termination and it represents the key measure to reduce the risks of uterine wall 206
rupture and hemorrhage. Previous reports related to hystero-embryoscopy settings 207
showed that miniaturized hysteroscopes enable an easy access to the gestational 208
sac [15]. Based on these assumptions, we believed that MTX administration in 209
subchorionic space at placental implantation site (i.e. directly within the intervillous 210
spaces), may optimize the cytotoxicity, enhancing the drug concentrations delivered 211
to the target tissues. In the case here presented, hysteroscopy easily assessed the 212
CSP anatomy and it allowed a selective MTX administration to the underlying villous 213
trophoblast by identifying the placental implantation site. With regard to hysteroscopy 214
guidance, ultrasound techniques of intra-gestational and/or peri-gestational sac MTX 215
administration may be less specific in driving selectively the drug. This is mainly due 216
to the possible difficulty in positioning precisely the needle tip within the placental 217
implantation site [3, 13]. Subchorionic hysteroscopic MTX administration resulted 218
technically easy, quick, painless, safe and effective; moreover, it can be 219
accomplished as outpatient procedure. The effectiveness of this technique was 220
demonstrated by the early loss of embryonic cardiac activity and the early increase 221
of beta-hCG (due to trophoblast cells necrosis) followed by its fast and progressive 222

Manuscript Accepted Peer Reviewed | Early View Article
Page 9 of 16
fall [6, 13]. In current literature, only one report describes a hysteroscopy-guided 223
MTX administration for treatment of viable CSP. After systemic MTX failure and 224
under hysteroscopy guidance the Authors injected MTX within the gestational sac, 225
obtaining an embryo’s demise but observing a persistent increase of beta-hCG 226
levels [16]. Although no guidelines provided preferential options in CSP 227
management, the recent literature suggests a combined sequential approach. The 228
first measure is aimed to pregnancy termination by MTX administration or by acute 229
reduction of placental blood supply by Uterine Artery Embolization. Subsequently, an 230
appropriate timing for surgical pregnancy removal is advised [7, 8, 9, 17]. Based on 231
literature data, the hysteroscopic CSP removal appears to be the safest surgical 232
therapy. Hysteroscopy allows a precise assessment of pregnancy topography and 233
placental implantation, a bleeding control by use of coagulating current and a 234
selective pregnancy removal under vision [3, 8, 11, 12, 16, 17]. As previously 235
reported, based on the significant decrease of beta-hCG levels after MTX 236
administration and demonstrating the pregnancy termination, we safely removed the 237
CSP by resectoscope, accordingly [11, 12, 16]. 238
239
CONCLUSION 240
A successful and never described technique to manage a viable CSP by the 241
selective administration of MTX under hysteroscopy guidance, within the placental 242
intervillous space of the ectopic implantation, has been reported. An eye-driven MTX 243
administration within the target tissue, leading to high drug cell concentrations, may 244
optimize its cytotoxicity. When hysteroscopy facilities are available, this technique 245
can be considered as an option for CSP termination. 246
247
CONFLICT OF INTEREST 248
All Authors declare no conflict of interest 249
250
AUTHOR’S CONTRIBUTIONS 251
Giancarlo Garuti (MD) 252
Group 1- Conception and design, acquisition of data, analysis and interpretation of 253
data 254

Manuscript Accepted Peer Reviewed | Early View Article
Page 10 of 16
Group 2- Drafting the article, critical revision of the article 255
256
Stefania Calabrese (MD) 257
Group 1- Conception and design, acquisition of data, analysis and interpretation of 258
data 259
260
Lorenzo Quirino (MD) 261
Group 1- Conception and design, acquisition of data, analysis and interpretation of 262
data 263
264
Marco Di Mario (MD) 265
Group 3- Final approval of the version to be published 266
267
ACKNOWLEDGEMENTS 268
We thank Mrs.Elena Bosoni for language revision of the Manuscript 269
270
REFERENCES 271
1. Ash A, Smith A, Maxwell D. Cesarean scar pregnancy. BJOG 2007;114:253-263 272
2. Larsen JV, Solomon MH. Pregnancy in a uterine scar sacculus: an unusual 273
cause of postabortal haemorrhage. S Afr Med J 1978;53:142-143 274
3. Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing 275
rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. 276
A review. Am J Obstet Gynecol 2012;207:14-29 277
4. Timor-Tritsch IE, Khatib N, Monteagudo A, Ramos J, Berg R, Kovacs S. 278
Cesarean scar pregnancies: experience of 60 cases. J Ultrasound Med 279
2015;34:601-610 280
5. Jurkovic D. Cesarean section scar ectopic pregnancy: a new problem or new 281
name for an old one? Aus J Ultrasound Med 2009;12:22-23 282
6. Timor-Tritsch IE, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The 283
diagnosis, treatment, and follow-up of cesarean scar pregnancy. Am J Obstet 284
Gynecol 2012;207:44e1-13 285

Manuscript Accepted Peer Reviewed | Early View Article
Page 11 of 16
7. Gao L, Huang Z, Gao J, Mai H, Zhang Y, Wang X. Uterine artery embolization 286
followed by dilatation and curettage within 24 hours compared with systemic 287
methotrexate for cesarean scar pregnancy. Int J Gynaecol Obstet 2014;127:147-288
151 289
8. Li YR, Xiao SS, Wan YJ, Xue M. Analysis of the efficacy of three treatment 290
options for cesarean scar pregnancy management. J Obstet Gynaecol Res 291
2014;11:2146-2151 292
9. Huang Y, Li Y, Xi R, Chen Z, Ying D, Li Z, Yang Y. An application of uterine 293
artery chemoembolization in treating cesarean scar pregnancy. Int J Clin Exp 294
Med 2015;8:2570-2577 295
10. Stika CS. Methotrexate: the pharmacology behind medical treatment for ectopic 296
pregnancy. Clin Obstet Gynecol 2012;55:433-439 297
11. Yang Q, Piao S, Wang G, Wang Y, Liu C. Hysteroscopic surgery of ectopic 298
pregnancy in the cesarean section scar. J Minim Inv Gynecol 2009;16:432-436 299
12. Deans R, Abbott J. Hysteroscopic management of cesarean scar ectopic 300
pregnancy. Fertil Steril 2010;93:1735-1740 301
13. Cok T, Kalayci H, Ozdemir H, Haydardedeoglu B, Parlakgumus AH, Tarim E. 302
Transvaginal ultrasound-guided local methotrexate administration as the first-line 303
treatment for cesarean scar pregnancy. Follow-up of 18 cases. J Obstet Gynecol 304
Res 2015;41:803-808 305
14. Cheung VY. Local methotrexate injection as first-line treatment for cesarean scar 306
pregnancy: review of the literature. J Minim Invasive Gynecol 2015; 22: 753-758 307
15. Ferro J, Martinez C, Love C, Pellicer A, Remohi J, Serra V. Improved accuracy of 308
hysteroembrioscopic biopsies for karyotyping early missed abortions. Fertil Steril 309
2003;80:1260-1264 310
16. Di Spiezio Sardo A, Alviggi C, Zizolfi B, Spinelli M, De Rosa P, De Placido G, 311
Nappi C. Cervico-isthmic pregnancy successfully treated with bipolar resection 312
following methotrexate administration: case report and literature review. Reprod 313
Biomed Online 2013;26:99-103 314
17. Wu X, Xue X, Wu X, Lin R, Yuan Y, Wang Q, Xu C, He Y, Hu W. Combined 315
laparoscopy and hysteroscopy vs uterine curettage in the uterine artery 316

Manuscript Accepted Peer Reviewed | Early View Article
Page 12 of 16
embolization-based management of cesarean scar pregnancy: a cohort study. Int 317
J Exp Med 2014;7:2793-2803 318
319
FIGURE LEGENDS 320
Figure 1: Gray Scale Transvaginal Sonography showing a 7 weeks gestational sac 321
embedded in the anterior wall of uterine cervico-isthmic junction. Both endometrium 322
and cervical canal are empty 323
324
Figure 2: Gray Scale Transvaginal Sonography showing a viable embryo and yolk 325
sac within the CSP 326
327
Figure 3: Office intervention. Few seconds before MTX injection, with the 328
hysteroscope positioned within the gestational sac we show the tip of the needle 329
(white arrow) inserted few millimeters under the ventral aspect of chorionic 330
membrane of the CSP, i.e. within the intervillous spaces of placental implantation 331
site 332
333
Figure 4: Resectoscopic removal of CSP. A panoramic view of uterine cavity 334
showing an empty endometrial cavity, the upper limit of cervico-isthmic niche and a 335
cranial portion of the CSP capsular decidua (at the top of Figure, on the left, 336
indicated by the arrow) 337
338
Figure 5: Resectoscopic CSP removal. We show the caudal extension of gestational 339
sac demonstrating the break of the capsular decidua resulting from the previous 340
office intervention 341
342
Figure 6: Resectoscopic CSP removal. Using the 4 mm bipolar loop, a cold 343
separation of villous trophoblast from the cervico-isthmic placental bed is in progress 344
345
346
347
348

Manuscript Accepted Peer Reviewed | Early View Article
Page 13 of 16
FIGURES 349
350
351
352
Figure 1: Gray Scale Transvaginal Sonography showing a 7 weeks gestational sac 353
embedded in the anterior wall of uterine cervico-isthmic junction. Both endometrium 354
and cervical canal are empty 355
356
357
358
Figure 2: Gray Scale Transvaginal Sonography showing a viable embryo and yolk 359
sac within the CSP 360

Manuscript Accepted Peer Reviewed | Early View Article
Page 14 of 16
361
362
Figure 3: Office intervention. Few seconds before MTX injection, with the 363
hysteroscope positioned within the gestational sac we show the tip of the needle 364
(arrow) inserted few millimeters under the ventral aspect of chorionic membrane of 365
the CSP, i.e. within the intervillous spaces of placental implantation site 366
367
368
369
370
371
372
373

Manuscript Accepted Peer Reviewed | Early View Article
Page 15 of 16
374
375
Figure 4: Resectoscopic removal of CSP. A panoramic view of uterine cavity 376
showing an empty endometrial cavity, the upper limit of cervico-isthmic niche and the 377
cranial portion of the CSP capsular decidua (at the top of Figure, on the left, 378
indicated by the arrow) 379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
Manuscript Accepted Peer Reviewed | Early View Article
Page 16 of 16
396
397
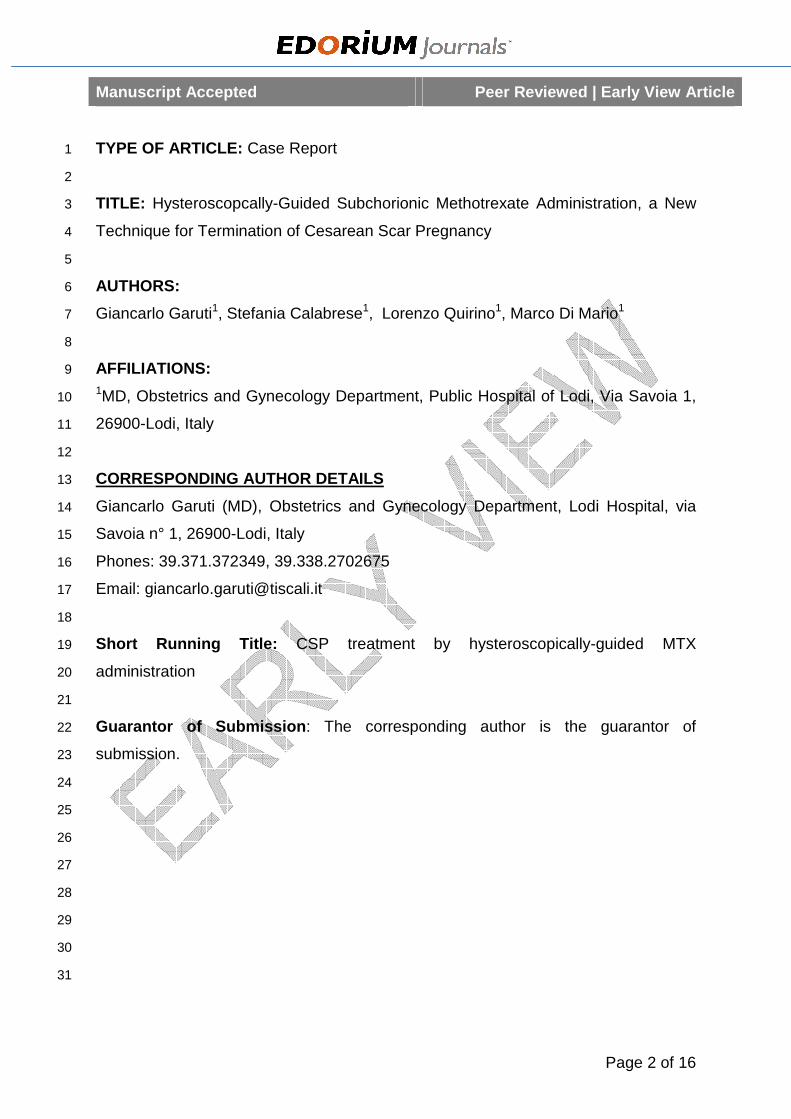
Figure 5: Resectoscopic CSP removal. We show the caudal extension of gestational 398
sac demonstrating the break of the capsular decidua resulting from the previous 399
office intervention 400
401
402
403
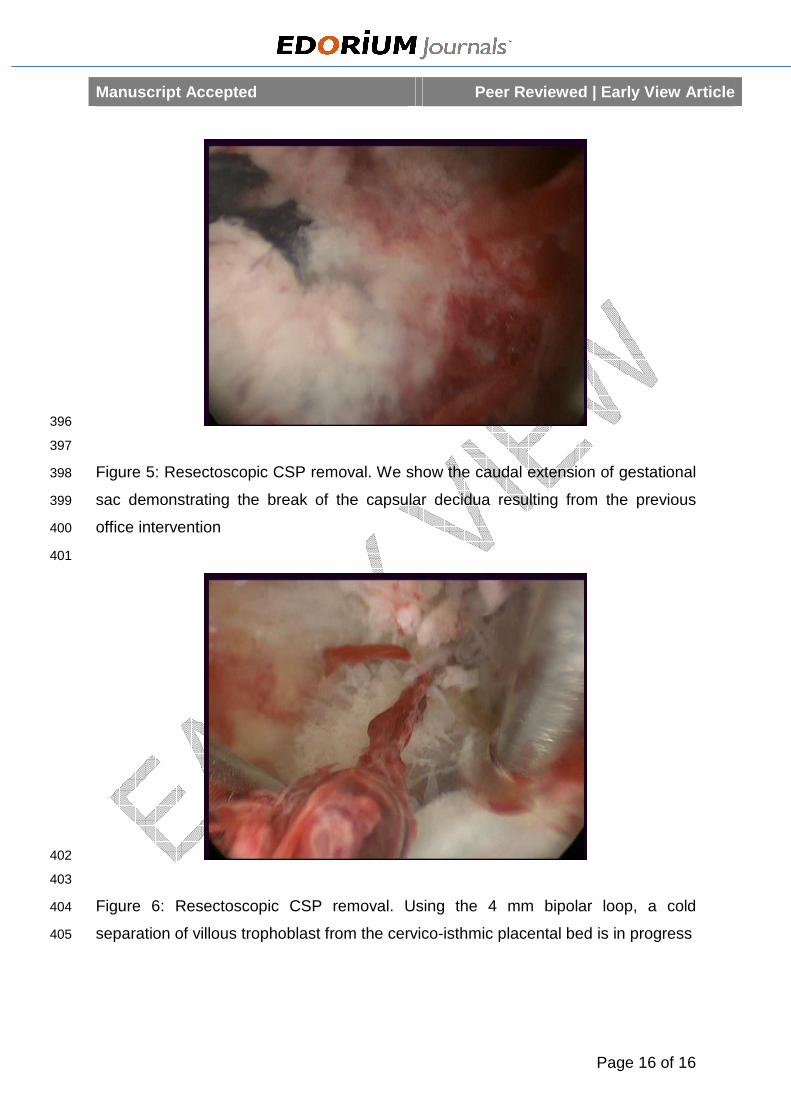
Figure 6: Resectoscopic CSP removal. Using the 4 mm bipolar loop, a cold 404
separation of villous trophoblast from the cervico-isthmic placental bed is in progress 405