Embed Size (px)
Citation preview
Journal of Abnormal Psychology
Predictive Validity of Childhood Oppositional Defiant Disorder andConduct Disorder: Implications for the DSM–VJeffrey D. Burke, Irwin Waldman, and Benjamin B. Lahey
Online First Publication, September 20, 2010. doi: 10.1037/a0019708
CITATION
Burke, J. D., Waldman, I., & Lahey, B. B. (2010, September 20). Predictive Validity of Childhood
Oppositional Defiant Disorder and Conduct Disorder: Implications for the DSM–V. Journal of
Abnormal Psychology. Advance online publication. doi: 10.1037/a0019708

Predictive Validity of Childhood Oppositional Defiant Disorder andConduct Disorder: Implications for the DSM–V
Jeffrey D. BurkeUniversity of Pittsburgh
Irwin WaldmanEmory University
Benjamin B. LaheyUniversity of Chicago
Data are presented from 3 studies of children and adolescents to evaluate the predictive validity ofchildhood oppositional defiant disorder (ODD) and conduct disorder (CD) as defined in the Diagnosticand Statistical Manual of Mental Disorders, 4th edition (DSM–IV; American Psychiatric Association,1994) and the International Classification of Diseases, Version 10 (ICD-10; World Health Organization,1992). The present analyses strongly support the predictive validity of these diagnoses by showing thatthey predict both future psychopathology and enduring functional impairment. Furthermore, the presentfindings generally support the hierarchical developmental hypothesis in DSM–IV that some children withODD progress to childhood-onset CD, and some youth with CD progress to antisocial personalitydisorder (APD). Nonetheless, they reveal that CD does not always co-occur with ODD, particularlyduring adolescence. Importantly, the present findings suggest that ICD-10 diagnostic criteria for ODD,which treat CD symptoms as ODD symptoms when diagnostic criteria for CD are not met, identify morefunctionally impaired children than the more restrictive DSM–IV definition of ODD. Filling this “hole”in the DSM–IV criteria for ODD should be a priority for the DSM–V. In addition, the present findingssuggest that although the psychopathic trait of interpersonal callousness in childhood independentlypredicts future APD, these findings do not confirm the hypothesis that callousness distinguishes a subsetof children with CD with an elevated risk for APD.
Keywords: oppositional defiant disorder, conduct disorder, antisocial personality disorder, interpersonalcallousness
Since the publication of the Diagnostic and Statistical Manualof Mental Disorders, 4th edition (DSM–IV; American PsychiatricAssociation, 1994), the emerging empirical evidence has providedstrong support for the DSM–IV’s taxonomic model of attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disor-der (ODD), and conduct disorder (CD). Both exploratory andconfirmatory factor analyses have consistently shown that thesymptoms of ODD and CD, and the inattention and hyperactivity-impulsivity dimensions of ADHD, load onto separate factors (fora review, see Loeber, Burke, & Pardini, 2009). Consistent with thegrouping of these disorders under the rubric of “Attention-Deficitand Disruptive Behavior Disorders” in the DSM–IV, however,these four dimensions of symptoms are highly correlated with oneanother (Lahey et al., 2008).
Nonetheless, there remain a number of significant unresolvedissues that need to be empirically addressed before the the DSM–VTask Force concludes its review and possible revisions of diag-
nostic criteria for ODD and CD (Moffitt et al., 2008). In thepresent article we reports analyses of data from three samples toaddress three of these issues.
1. Hierarchical developmental relations among disorders. TheDSM–IV hypothesized a developmental pathway from ODD to CDto antisocial personality disorder (APD). These developmentalrelations are hypothesized to be hierarchical, with only somechildren with ODD progressing to CD and only some youth withCD progressing to APD (Lahey & Loeber, 1994; Lahey, Loeber,Burke, & Applegate, 2005; Loeber, Burke, et al., 2000; Loeber,Lahey, & Thomas, 1991; Moffitt et al., 2008). Indeed, in theDSM–IV, when criteria for CD are met, the diagnosis of ODDcannot also be assigned because it is assumed to always be present.Furthermore, the diagnosis of APD cannot be given unless there isevidence that the individual exhibited significant CD behaviorsbefore age 15.
Because the extent to which a diagnosis predicts a later, moreserious diagnosis is a fundamental aspect of predictive validity, itis important to know whether ODD, CD, and APD are, in fact,nested developmentally. The limited new evidence emerging since1994 from longitudinal studies is consistent with the hypothesisthat childhood ODD is a developmental precursor to CD, giventhat ODD usually has an earlier onset and a greater prevalence, andchildren with ODD are at increased risk for developing CD (Burke,Loeber, & Birmaher, 2002; Lahey & Loeber, 1994; Lavigne et al.,
Jeffrey D. Burke, Western Psychiatric Institute and Clinic, University ofPittsburgh; Irwin Waldman, Department of Psychology, Emory University;Benjamin B. Lahey, Department of Health Studies, University of Chicago.
Correspondence concerning this article should be addressed to Jeffrey D.Burke, Western Psychiatric Institute and Clinic, University of Pittsburgh, 3811O’Hara Street, Pittsburgh, PA 15213. E-mail: [email protected]
Journal of Abnormal Psychology © 2010 American Psychological Association2010, Vol. ●●, No. ●, 000–000 0021-843X/10/$12.00 DOI: 10.1037/a0019708
1

2001; Loeber, Burke, et al., 2000). Similarly, there is recentevidence confirming the hypothesis that child and adolescent CDas defined in the DSM–IV is a developmental precursor to APD(Lahey et al., 2005; Loeber, Burke, & Lahey, 2002).
The DSM–IV assumes that ODD is always present in youth whomeet diagnostic criteria for CD. Previous studies suggest that theextent to which ODD is always present in youth who meet diag-nostic criteria for CD appears to vary with the type of sample.Although the proportion of children with CD who meet or haveever met criteria for ODD tends to be high in clinic samples, it iscommon to identify youth who meet criteria for CD in samplesrepresentative of the general population who do not also exhibitODD (see Burke, in press). This discrepancy in findings mayreflect two kinds of sampling biases. First, consistent with theconcept of Berkson’s (1946) bias, there is evidence that childrenand adolescents who receive clinical services are more likely tomeet criteria for multiple mental disorders than children and ado-lescents identified in population-based samples who have notreceived clinical services (Goodman et al., 1997). Indeed, there isevidence that comorbid ODD could particularly lead to clinicreferral because a diagnosis of ODD, but not CD, has been foundto be associated with caregiver strain (Bussing, Gary, et al., 2003;Bussing, Zima, et al., 2003), and similarly is associated withinvolvement in mental health treatment during the prior year(Bussing, Zima, et al., 2003). Thus, clinic samples may be morelikely to include higher rates of children with CD who also havemet criteria for ODD because parents are motivated to seek clinicalservices. Nonetheless, it is important to determine how commonODD is among children who meet criteria for CD even in clinicsamples to evaluate this hierarchical diagnostic rule. We report theresults of analyses of this association using a longitudinal clinicsample to assess the nesting of the diagnosis of ODD within CD.
Second, there is evidence that children and adolescents whomeet criteria for CD with later ages of onset are less likely toreceive mental health services (Lahey et al., 1999). This is impor-tant because there is strong evidence that youth who follow dif-ferent developmental trajectories of antisocial behavior exhibitdifferent childhood characteristics, including substantially greateroppositional behavior among youth with childhood-onset antiso-cial behavior (Lahey et al., 2006; Moffitt, Caspi, Harrington, &Milne, 2002). Thus, the DSM–IV presumption that ODD is alwayspresent when criteria for CD are met is unlikely to be literallycorrect, but may be generally accurate in clinical settings. In thepresent article, we report new data from a 13-year longitudinalstudy on the extent to which clinic-referred children with CDconcurrently meet criteria for ODD.
2. Predictive validity of ODD. As noted by Moffitt et al. (2008),predictive validity is a sine qua non for diagnostic criteria formental disorders that are applied to children and adolescents. Thatis, although functional impairment and distress that is concurrentlyassociated with mental disorders may provide sufficient justifica-tion for treatment, it is essential that diagnostic criteria used withchildren predict future adaptive and maladaptive outcomes toimprove treatment planning and prognosis. Although considerableexisting research supports the predictive validity of ODD and CD(Moffitt et al., 2008), more remains to be learned about thepredictive validity of ODD. In particular, it is not yet clear thatODD is associated with future adverse outcomes if it does not leadto CD, which is the case for many children with ODD. That is, is
ODD a challenging and impairing condition during childhood, butnot one associated with lasting dysfunction in those children withODD who do not develop CD? To better understand the predictivevalidity of childhood ODD, we compare both the persistence ofODD symptoms and functional impairment of children with ODDwho do and do not ever meet criteria for CD over a 13-year period.
Furthermore, there remains a controversy as to the role ofADHD in the prediction of CD after accounting for ODD (Lahey,McBurnett, & Loeber, 2000; Lahey et al., 2009; Mannuzza, Klein,Abikoff, & Moulton, 2004; Mannuzza et al., 1991). Some theoristshypothesize that ADHD is a direct developmental precursor to CDand APD (Mannuzza et al., 2004), whereas others suggest thatapparent links between ADHD and later antisocial behavior havebeen observed due to the failure to account fully for the presenceof childhood ODD (Lahey et al., 2000). For example, in a clinicsample of boys using DSM-based clinical interview measures fromages 7 to 17, annual increases in CD symptoms were predicted byODD and not ADHD, but ADHD predicted increases in ODD overtime (Burke, Loeber, Lahey, & Rathouz, 2005). Nonetheless, thereis evidence that early oppositional behaviors do not predict laterconduct problems when early conduct problems are controlled(Lahey et al., 2009). These data were not based on DSM–IVsymptom lists, but raise concerns about the importance of ODD asa developmental precursor to later CD that must be addressedusing DSM–IV criteria. In the present article, questions regardingchildhood ADHD and ODD as precursors to CD are addressedusing data from a longitudinal study that has followed childrenwho met criteria for ADHD at 4–6 years and demographicallymatched comparison children. We test the hypothesis that ODD inYear 1 is a developmental precursor to new cases of CD overthe next 12 years, even when subthreshold symptoms of CD inYear 1 are controlled, but ADHD is not an independent predic-tor of future CD.
Perhaps the most important unresolved question regarding theDSM–IV model of ODD and CD is whether the InternationalClassification of Diseases, Version 10 (ICD-10; World HealthOrganization, 1992) definition of ODD is more valid in the ICD-10than in the DSM–IV. In the DSM–IV, children can have up to threesymptoms of ODD and two symptoms of CD and not meet criteriafor either ODD or CD. In the ICD-10, which takes a developmen-tal approach to ODD and CD, both symptoms of ODD and CD areconsidered in making the diagnosis of ODD when criteria for CDare not met; thus, these children would meet criteria for ODD.Rowe, Maughan, Costello, and Angold (2005) found the preva-lence of DSM–IV ODD to be 3.9%, whereas the prevalence ofICD-10 ODD was 5.4%. Moreover, children who met criteria forICD-10 ODD but not DSM–IV ODD were found to show levels ofimpairment and comorbidity equal to children who met DSM–IVcriteria for ODD (Rowe et al., 2005).
In this article, we compare the validity of the ICD-10 andDSM–IV definitions of ODD in both a longitudinal study ofclinic-referred children and controls and a large representativesample of twins (Lahey et al., 2008). We test the hypothesis thatICD-10 ODD identifies children with impairing disruptive behav-ior problems who do not meet criteria for either ODD or CD in theDSM–IV.
3. The role of psychopathic characteristics in the predictivevalidity of CD. It is clear that many children and adolescents whomeet diagnostic criteria for CD do not progress to APD (Burke,
2 BURKE, WALDMAN, AND LAHEY

Loeber, & Lahey, 2003). Although CD is the best predictor ofAPD, CD is defined solely by discrete antisocial behaviors and notby the personality characteristics that are part of the definition ofAPD (Burke, 2007). Therefore, there is great interest in the po-tential role of personality features in childhood in predicting laterAPD. For example, a construct measuring callous and unemotionaltraits has been found to predict CD and other psychopathology(Rowe et al., in press), as well as predicting a more severe andaggressive pattern of later conduct problems (Frick, Cornell,Barry, Bodin, & Dane, 2003). Adolescent interpersonal callous-ness (IC; Burke, Loeber, & Lahey, 2007) and adolescent psychop-athy (Lynam, Caspi, Moffitt, Loeber, & Southamer-Loeber, 2007)predict psychopathy in young adults. However, IC was not foundto predict future delinquency after accounting for existing conductproblems in two of three cohorts of the Pittsburgh Youth Study(Pardini, Obradovic, & Loeber, 2006). Similarly, in a largepopulation-based sample, controlling for concurrent CD renderedthe prediction from callous and unemotional traits to other disor-ders nonsignificant (Rowe et al., in press). To provide evidencerelevant to the proposal to use callousness as a subtyping dimen-sion for CD in the DSM–V, we test the hypothesis that IC improvesthe prediction of APD in the clinic-referred Developmental TrendsStudy (DTS; Loeber, Green, Lahey, Frick, & McBurnett, 2000)sample.
Method
Growing Up With ADHD Study (GUWAS)
Participants. In the GUWAS (Lahey et al., 2007; Lee, Lahey,Owens, & Hinshaw, 2008), two cohorts of 3.8- to 7.0-year-oldchildren were recruited in consecutive years at two sites, Chicagoand Pittsburgh. Participants all lived with their biological mothers,and half initially met DSM–IV diagnostic criteria for ADHD. InChicago, children with ADHD were recruited from a universitychild psychiatry clinic. In Pittsburgh, 42% of the children withADHD were recruited from a university child psychiatry clinic,and 58% were recruited through advertisements, but no differenceswere found between recruitment methods. Five potential partici-pants were excluded because of pervasive developmental disorder,mental retardation, or seizure disorder. Comparison children wererecruited from similar schools and neighborhoods as probands andapproximately matched probands on sex, ethnicity, and age. Theyhad never been referred for mental health problems but were notexcluded if they met criteria for a disorder other than ADHD. Of310 eligible participants, 259 parents gave consent and partici-pated. The present analyses are based on approximately annualstructured diagnostic assessments conducted during Years 1–4,6–9, and 12–13. Assessments were not conducted during Years 5,10, and 11 due to insufficient funding.
Measures. Beginning with the initial assessment when thechildren were 4–6 years old, approximately annual assessmentswere conducted by trained lay interviewers. The Diagnostic Inter-view Schedule for Children (DISC; Shaffer, Fisher, Piacentini,Schwab-Stone, & Wicks, 1993) was administered to mothers ineach assessment. Information was obtained from mothers onDSM–IV diagnostic criteria for a range of disorders, includingsymptoms of ADHD, ODD, and CD symptoms during the last 12months (Lahey al., 1998). In addition, the DISC was administered
to the youth in Years 6–13 to query DSM–IV diagnostic criteria forCD and internalizing disorders. In each assessment, the child’sprimary teacher completed the DSM–IV version of the DisruptiveBehavior Disorder Rating Scale (Pelham, Gnagy, Greenslade, &Milich, 1992) by mail. Following standard procedures, teacher-reported ADHD symptoms rated “pretty much” or “very much”were scored as present. Symptoms of CD were considered to bepresent if reported by either the parent or the youth using thesimple “or” rule as in the DSM–IV field trials (Lahey et al., 1994).Because both parent and youth reports of CD symptoms accountfor independent variance in functional impairment (E. L. Hart,Lahey, Loeber, & Hanson, 1994), the combination of parent andyouth reports provides the most valid measure of CD symptoms.
In each assessment, the nonclinician version of the Children’sGlobal Assessment Scale (CGAS; Setterberg, Bird, & Gould,1992) was used to obtain ratings of the child’s lowest level ofoverall functioning during the past 6 months. CGAS ratings werecollected independently from the mother and interviewer whoadministered the DISC to the mother. In each assessment, thechild’s primary or English teacher estimated the proportion of thechild’s classmates who like, dislike, and ignore the child on threeseparate 5-point scales each year (Dishion, 1990). A social pref-erence score was created by subtracting dislike ratings from likeratings. These scores were reversed to yield a negative socialpreference score with approximately Poisson distributions in eachyear.
Sample 2: Tennessee Twin Study (TTS)
Participants. The TTS sample is representative of all 6- to17-year-old twins who were born in Tennessee and living in one ofthe state’s five metropolitan statistical areas in 2001 (Lahey et al.,2008). These include the 28 urban, suburban, and rural countiessurrounding Nashville, Memphis, Knoxville, Chattanooga, andBristol. A random sample of families with twins was selected andstratified on the age of the twins, proportional to the population of35 geographic subareas. Ninety percent of families were locatedand screened, with 2,646 families being eligible. Twins wereeligible if (a) both twins coresided with the adult caretaker at leasthalf of the time during the past 6 months, (b) both twins and thecaretaker spoke English, and (c) the twins were 6–17 years old.Only 12 families were ineligible because of language. Interviewswere completed with 2,063 adult caretakers (91% biological moth-ers, 8% biological fathers). The response rate for caretaker inter-views was 70%; when the caretaker was interviewed, 98% of thetwin pairs were interviewed. Consistent with the population ofTennessee in 2001, caretakers classified 72% of the twin pairs asnon-Hispanic White, 23% as African American, 2% as Hispanic,and 3% as other race/ethnic groups. Youth were excluded from theTTS if they had a diagnosis of psychosis or autism. This resultedin 2,023 twin pairs (4,046 youth). The TTS consists of approxi-mately equal numbers of monozygotic (MZ; n � 752 pairs; 51%female pairs), same-sex dizygotic (DZ; n � 670 pairs; 51% femalepairs), and mixed-sex DZ pairs (n � 601 pairs).
Measures. Adult caretakers and youth were interviewed sep-arately using the Child and Adolescent Psychopathology Scale(CAPS; Lahey et al., 2008). Interviewers read each CAPS itemaloud to the respondent from a laptop computer and entered
3SPECIAL SECTION: PREDICTIVE VALIDITY OF ODD AND CD

responses. The CAPS covers all DSM–IV and ICD-10 symptomsof ADHD, ODD, CD, major depression (MDD), generalized anx-iety disorder, separation anxiety disorder, agoraphobia, social pho-bia, specific phobia, and obsessive-compulsive disorder (OCD).The CAPS was developed by primary investigator Lahey withNational Insitute of Mental Health funding to create a structureddiagnostic interview that yields both categorical diagnoses andcontinuous ratings of dimensions of child and adolescent psycho-pathology. CAPS items covering DSM–IV symptoms were basedon the “stem questions” of the DISC–IV (Shaffer et al., 1996),modified from “yes or no” questions to fit a 4-point response scale,where1 � not at all, 2 � just a little, 3 � pretty much, and 4 �very much. Respondents were asked to respond by thinking abouthow well each item described the youth’s emotion or behavior,how often it occurred, and how serious it was during the last 12months. Algorithms based on relations with DISC categoricaldiagnoses allow categorical diagnoses to be made on the basis ofthe CAPS.
The optimal informants on mental disorders in children andadolescents are different at different ages and for different disor-ders. Children � 9 years have been found to be unreliable infor-mants on all types of symptoms in structured interviews, but 9-to17-year-old youth can report reliable and valid information on CDand internalizing symptoms.(Jensen et al., 1999). In a separatelarge population-based sample of 4- to 17-year-olds (Lahey et al.,2004), a subset of participants (290 adult caretakers and 196 youth)stratified by age and numbers of symptoms was selected for asecond interview 7–14 days later. Test–retest intraclass correla-tions for unit-weighted mean ratings of the symptoms of eachDSM–IV disorder using the CAPS ranged from .65 to .89 caretakerreports and from .62 to .83 for youth reports of symptoms. Robustcorrelations with measures of functional impairment providestrong external validation of the CAPS (Lahey et al., 2004).
Sample 3: The DTS
Participants. Participants in the DTS were 177 boys recruitedin 1987 from clinics in Pittsburgh, Pennsylvania and in Athens andAtlanta, Georgia. Boys had to be living with at least one biologicalparent and were excluded if they had a history of mental retarda-tion or psychosis, inpatient psychiatric treatment within the last 6months, or could not discontinue taking psychotropic medicationfor 2 days prior to their scheduled assessment. Further detailsregarding participant recruitment can be found in Loeber, Green, etal., 2000.
Participants in the DTS were 7–12 years of age at the beginningof the study, and were followed up with parent and child assess-ments until the age of 17. These interviews were conducted on anannual basis, except in Year 5, due to a funding cut. Young adultfollow-up interviews were conducted with the youth alone at 18,19, and 24 years of age. Retention rates for the childhood throughadolescent data collection ranged from a high of 100% in Year 2to 87.1% in Year 10, with an average across all years of 93.4%.There were 164 participants (93%) who completed at least oneyoung adult follow-up interview at 18, 19, or 24 years of age; with162 assessed at age 18, 153 assessed at age 19, and 143 assessedat age 24. The sample was composed of non-Hispanic White(70%) and African American boys (30%).
Measures. A modified version of the DISC (Costello, Edel-brock, Dulcan, Kalas, & Klaric, 1987) was developed on the basisof DSM–III–R criteria (Loeber et al., 1989). Parallel versions forparents, children, and teachers were administered at each assess-ment to assess symptoms of CD, ODD, and ADHD. In the presentanalyses, both parent and child reports were used, combined at thesymptom level using an either/or strategy, so that a positive symp-tom endorsement from either the parent or the child was consid-ered to denote the presence of that symptom.
Although the DISC assessed DSM–III–R symptoms, we wereable to create CD constructs using criteria similar to the DSM–IV.The primary distinction is the addition of “often bullies, threatensor intimidates others” and “often stays out at night despite parentalprohibitions,” which we had within our parent report for all phases.For child report, we also had “bullying” for all phases. However,we queried “stay out late” with children in only the first andsecond assessment waves. Finally, the DSM–IV specifies “lying tocon,” whereas the DSM–IV included “lying” without any qualifi-cation. Our assessment did not include the specification of “lyingto con” at any phase.
IC. Parents and teachers completed an extended version of theChild Behavior Checklist (CBCL; Achenbach & Edelbrock, 1983)annually through assessments at age 17. This was modified toinclude 88 items regarding delinquent and covert antisocial behav-iors (Loeber, Farrington, Stouthamer-Loeber, & Van Kammen,1998). Eight items from these measures regarding manipulative,sneaky behavior and an absence of guilt were summed to createseparate parent and teacher constructs of IC behaviors. The devel-opment of this construct and its psychometric properties are de-scribed in more detail elsewhere (Burke et al., 2007; Pardini et al.,2006). Across the 10 waves of the present data set, the internalconsistency reliability alpha for the construct ranged from .87 to.93. The extent to which this measure is correlated with relatedconstructs, such as callous unemotional (CU) traits (e.g., Frick etal., 2003) and childhood psychopathy (e.g., Lynam et al., 2007) isnot well established, although parent-rated IC has been shown tocorrelate with the interpersonal/affective factor of the Child Psy-chopathy Scale (r � .78; Pardini & Loeber, 2008). CU items taplargely overlapping items, although CU also includes affectivelyoriented items, and psychopathy includes impulsive, irresponsible,and antisocial behavior (see Loeber, Burke, & Pardini, 2009, forfurther discussion).
APD. At 18, 19, and 24 years of age, participants were as-sessed using the Computerized Diagnostic Interview ScheduleRevised (DIS; Robins & Helzer, 1988). The temporal stability ofDIS-based measurement of APD has been shown to be good (�s �.60 and .58 for 6- and 12-month follow-up assessments; Vandiver& Sher, 1991).
This included an assessment of DSM–III–R criteria for APD,whereas DSM–IV criteria for APD did not include items regardingability to function as a responsible parent and sustaining a monog-amous relationship for 1 year. Additionally, in DSM–IV, two itemspertaining to inconsistent work behavior and failure to honorfinancial obligations were combined. DSM–IV APD scoring wasdeveloped by excluding DIS data on the two items that weredropped and defining the item on work behavior and financialobligations by combining items for these criteria. Because wewished to examine CD as an antecedent to APD, we did not requirechildhood CD to have been present to give the diagnosis of APD.
4 BURKE, WALDMAN, AND LAHEY

Preliminary analyses showed that the diagnosis of APD was notalways stable across assessment waves in the DTS. Therefore,because APD is conceptualized as a chronic mental disorder, APDwas conservatively considered to be present only if criteria weremet in at least two of the three adult assessments at 18, 19, or 24years. Of the 164 participants assessed at least once during adult-hood, these scoring procedures led to five missing cases, or a totalof 159 participants available for analyses predicting APD.
To validate this measure of APD based on at least two positivediagnoses, the association between our definition of APD andseveral external criterion variables related to the construct of APDwas tested. Participants meeting criteria for APD in adulthood had,on average, twice as many criminal charges (M � 6.35 vs. M �2.5) and approximately four times as many violent charges (M �0.92 vs. M � 0.23) as other participants, according to officialrecords (both differences significant at p � .01). Similarly, par-ticipants with APD were 2.6 times more likely than those withoutAPD to report having been fired from a job ( p � .001) and were3.3 times as likely to report causing injury to a romantic partner( p � .04). They also had Psychopathy Checklist scores (Hart, Cox,& Hare, 1995) that were, on average, 2.3 times greater than thosewithout APD ( p � .001).1
Data analyses. In the GUWAS sample, all longitudinal dataanalyses were conducted using general estimating equations(GEEs; Zeger & Liang, 1986). GEEs account for the clustering ofmultiple repeated observations over time within each participantand allows the specification of a within-person correlation struc-ture to account for correlations in the outcome variable over time.Given that GEEs were used within generalized linear models, thepresent analyses allow for nonnormally distributed outcomes, suchas count or dichotomous variables. In all of these analyses, anautoregressive correlation structure was specified.
For repeated measures of dichotomous outcome variables, bi-nomial regression was specified in the present analyses. For con-tinuous data, working distributions that approximate the data werespecified on the basis of their empirical distributions. Specifically,when GEE was used with count variables in the GUWAS, aPoisson distribution was specified. Because population-averagedGEE regressions model the average value of the outcome for eachsubset of participants who share the same value of the predictorvariable, and not the entire distribution of outcome values, they areless restricted by distributional assumptions than other approachesto longitudinal data analysis. The z statistic was used in all statis-tical tests, which were based on the robust (“empirical”) standarderror that adjusts for dispersion and minimizes the effect of incor-rect specification of the within-person covariance structure.
GEE was also used for dichotomous and count outcomes in thecross-sectional analyses of the TTS data. In this case, the GEE wasused to account for the clustering of participants within twin pairs.This allowed all individual twins to be included in the sameanalysis without violating the assumption of observational inde-pendence.
To examine the prediction of APD in adulthood from CD to ICthrough adolescence in the DTS, logistic regression models wereconducted in which participants were clustered to account forcorrelated observations, which allow for all waves of predictors tobe included in the model.
Results
Issue 1: Are There Hierarchical DevelopmentalRelations Among ODD, CD, and APD?
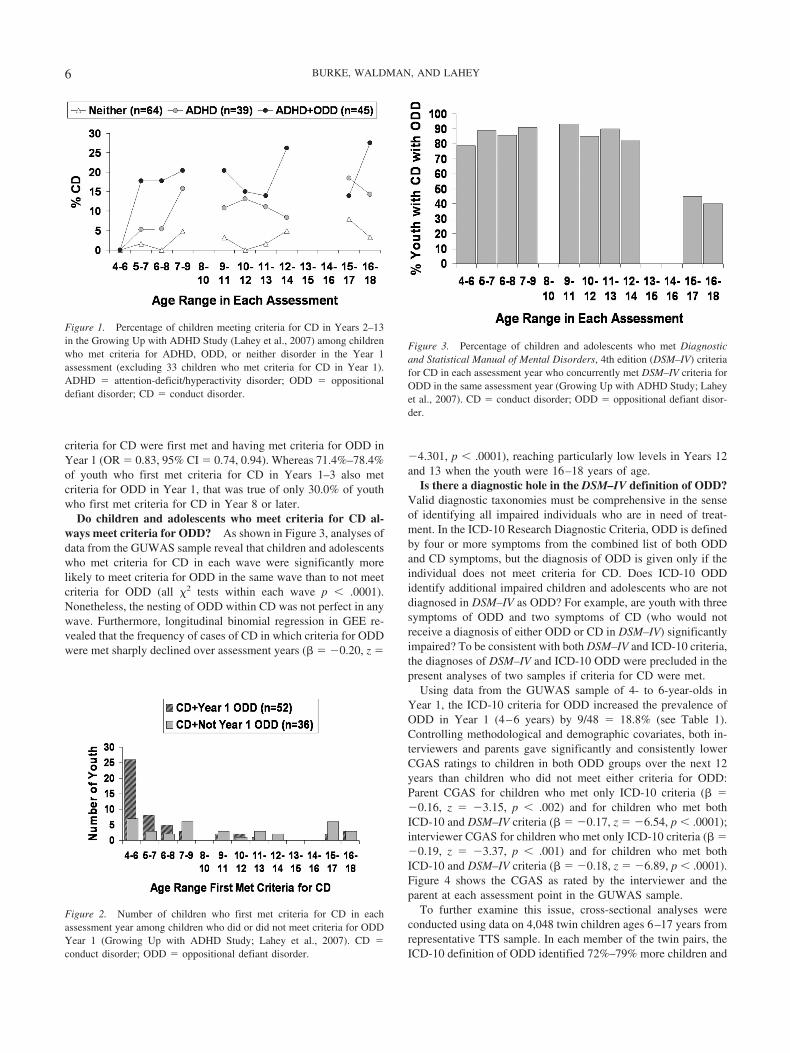
Does childhood ODD predict later CD? Using data from theGUWAS sample, groups of children were created based on meet-ing DSM–IV diagnostic criteria for ADHD, both ADHD and ODD,or neither disorder in Year 1 (at 4–6 years of age). These analysesused data from the 184 children who were assessed throughassessment Years 12 and/or 13 (Note: half of non-ADHD com-parison children were dropped from the study before Year 12 forbudgetary reasons), but not including 33 children who already metcriteria for CD in Year 1. Figure 1 shows the percentage ofchildren meeting criteria for CD within each group in each assess-ment year. In addition, four children with ODD in the absence ofADHD were not included in these analyses, but including themhad essentially no effect on the results.
Longitudinal binomial regression in the GEE was used to testthe extent to which Year 1 ADHD and ODD entered as simulta-neous predictors predicted the prevalence of the diagnosis of CDover the next 12 years. Among children who did not already meetdiagnostic criteria for CD in Year 1, both the diagnoses of ADHD(� � 0.91, z � 2.09, p � .04) and ODD (� � 1.41, z � 4.51, p �.0001) predicted meeting criteria for CD during Years 2–13, con-trolling methodological and demographic covariates. When thenumber of subthreshold CD symptoms in Year 1 were added as athird simultaneous predictor, however, Year 1 CD symptoms (� �0.90, z � 4.62, p � .0001) and the diagnosis of ODD in Year 1(� � 0.97, z � 3.22, p � .002) both predicted the prevalence ofCD over the next 12 years, but the diagnosis of ADHD in Year 1did not (� � 0.64, z � 1.43, p � .15). Thus, both ODD andsubthreshold symptoms of CD independently predicted new (i.e.,incident) cases of CD over the next 12 years in this sample.
It is important to examine further the developmental sequencesof ODD and CD in the 19 of the 48 children who met criteria forADHD but not ODD or CD in Year 1, but who later met criteriafor CD at least once during Years 2–13. Among these 19 children,nine met criteria for ODD at least once before criteria for CD weremet during Years 2–13, and six met criteria for ODD in the sameyear as criteria for CD were first met. Only four of these 19children met criteria for CD without meeting criteria for ODD inan earlier year or in the same year.
Early ODD and the early emergence of CD. Because theGUWAS sample was ascertained at 4–6 years of age, it would bereasonable to assume that most children with CD in this samplewould first meet criteria for CD during childhood. Consistent withthis view, Figure 2 shows that 70.0% of the 86 children who evermet criteria for CD during Years 1–13 did so for the first timeduring the first 4 years of the study (spanning ages 4–9 years ofage). Consistent with previous studies showing a link betweenearly ODD behavior and early-onset conduct problems (Lahey etal., 1998, 2006), ordinal logistic regression showed that amongchildren who met criteria for CD at least once during the study,there was a robust inverse relation between the year in which
1 Additional details on these validation analyses are available fromJeffrey D. Burke upon request.
5SPECIAL SECTION: PREDICTIVE VALIDITY OF ODD AND CD
criteria for CD were first met and having met criteria for ODD inYear 1 (OR � 0.83, 95% CI � 0.74, 0.94). Whereas 71.4%–78.4%of youth who first met criteria for CD in Years 1–3 also metcriteria for ODD in Year 1, that was true of only 30.0% of youthwho first met criteria for CD in Year 8 or later.
Do children and adolescents who meet criteria for CD al-ways meet criteria for ODD? As shown in Figure 3, analyses ofdata from the GUWAS sample reveal that children and adolescentswho met criteria for CD in each wave were significantly morelikely to meet criteria for ODD in the same wave than to not meetcriteria for ODD (all �2 tests within each wave p � .0001).Nonetheless, the nesting of ODD within CD was not perfect in anywave. Furthermore, longitudinal binomial regression in GEE re-vealed that the frequency of cases of CD in which criteria for ODDwere met sharply declined over assessment years (� � �0.20, z �
�4.301, p � .0001), reaching particularly low levels in Years 12and 13 when the youth were 16–18 years of age.
Is there a diagnostic hole in the DSM–IV definition of ODD?Valid diagnostic taxonomies must be comprehensive in the senseof identifying all impaired individuals who are in need of treat-ment. In the ICD-10 Research Diagnostic Criteria, ODD is definedby four or more symptoms from the combined list of both ODDand CD symptoms, but the diagnosis of ODD is given only if theindividual does not meet criteria for CD. Does ICD-10 ODDidentify additional impaired children and adolescents who are notdiagnosed in DSM–IV as ODD? For example, are youth with threesymptoms of ODD and two symptoms of CD (who would notreceive a diagnosis of either ODD or CD in DSM–IV) significantlyimpaired? To be consistent with both DSM–IV and ICD-10 criteria,the diagnoses of DSM–IV and ICD-10 ODD were precluded in thepresent analyses of two samples if criteria for CD were met.
Using data from the GUWAS sample of 4- to 6-year-olds inYear 1, the ICD-10 criteria for ODD increased the prevalence ofODD in Year 1 (4–6 years) by 9/48 � 18.8% (see Table 1).Controlling methodological and demographic covariates, both in-terviewers and parents gave significantly and consistently lowerCGAS ratings to children in both ODD groups over the next 12years than children who did not meet either criteria for ODD:Parent CGAS for children who met only ICD-10 criteria (� ��0.16, z � �3.15, p � .002) and for children who met bothICD-10 and DSM–IV criteria (� � �0.17, z � �6.54, p � .0001);interviewer CGAS for children who met only ICD-10 criteria (� ��0.19, z � �3.37, p � .001) and for children who met bothICD-10 and DSM–IV criteria (� � �0.18, z � �6.89, p � .0001).Figure 4 shows the CGAS as rated by the interviewer and theparent at each assessment point in the GUWAS sample.
To further examine this issue, cross-sectional analyses wereconducted using data on 4,048 twin children ages 6–17 years fromrepresentative TTS sample. In each member of the twin pairs, theICD-10 definition of ODD identified 72%–79% more children and
Figure 1. Percentage of children meeting criteria for CD in Years 2–13in the Growing Up with ADHD Study (Lahey et al., 2007) among childrenwho met criteria for ADHD, ODD, or neither disorder in the Year 1assessment (excluding 33 children who met criteria for CD in Year 1).ADHD � attention-deficit/hyperactivity disorder; ODD � oppositionaldefiant disorder; CD � conduct disorder.
Figure 2. Number of children who first met criteria for CD in eachassessment year among children who did or did not meet criteria for ODDYear 1 (Growing Up with ADHD Study; Lahey et al., 2007). CD �conduct disorder; ODD � oppositional defiant disorder.
Figure 3. Percentage of children and adolescents who met Diagnosticand Statistical Manual of Mental Disorders, 4th edition (DSM–IV) criteriafor CD in each assessment year who concurrently met DSM–IV criteria forODD in the same assessment year (Growing Up with ADHD Study; Laheyet al., 2007). CD � conduct disorder; ODD � oppositional defiant disor-der.
6 BURKE, WALDMAN, AND LAHEY

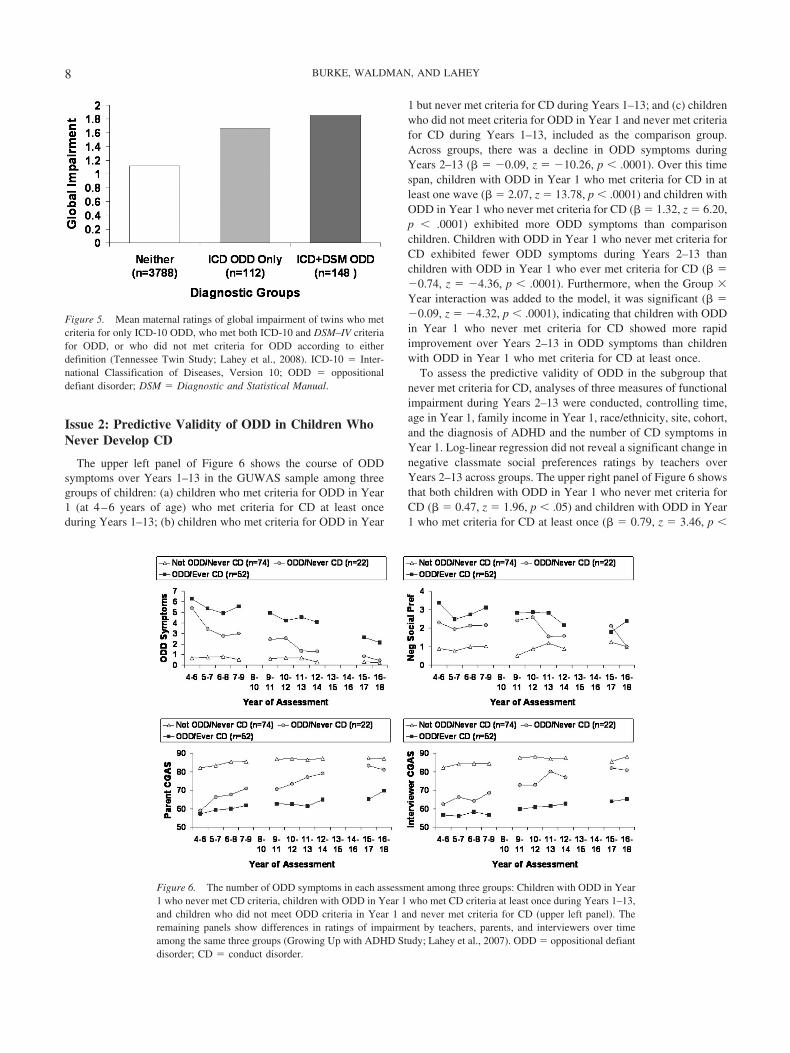
adolescents with ODD in this sample (see Table 1). The twogroups of children and adolescents who met criteria for ODD(according to ICD-10 only, or according to both ICD-10 andDSM–IV) were compared with children who met neither set ofcriteria for ODD on a measure of global impairment completed bymothers that combined impaired functioning with peers, withparents, with teachers, difficulties in completing homework orwork at home, and difficulties in completing classroom academicwork or work outside the home (Lahey et al., 2004). Figure 5shows the mean global impairment score by diagnostic group.GEE was used to account for clustering within twin pairs to allowdata on all twins to be analyzed in the same model. Controlling forage, sex, race/ethnicity, and family income, both the ICD-onlygroup (� � 0.30, z � 8.43, p � .0001) and the ICD � DSM–IV group(� � 0.44, z � 15.87, p � .0001) exhibited significantly greaterimpairment than the ODD group. The both ICD � DSM–IV group(� � 0.14, z � 3.36, p � .001) exhibited slightly but significantlygreater impairment than the ICD-only group.
To determine whether the much greater percent difference in thenumber of identified cases of ODD using the ICD-10 and DSM–IVdefinitions in the TTS sample than in the GUWAS was due to themuch greater number of older children and adolescents (6–17 vs.4–6 years) at the time of the diagnosis of ODD in the TTS, or thegreater proportion of females in the TTS (50% vs. 20%), the
association of the prevalence of ICD-only cases of ODD with ageand sex was tested in binomial regression in GEE. There was nota significant sex difference in the prevalence of cases of ODDdiagnosed only in the ICD-10 (� � 0.25, z � 1.38, p � .17). Therewas a nonsignificant trend toward an association between age andthe number of cases of ODD diagnosed only in the ICD-10 (� ��0.05, z � �1.84, p � .066), but the trend was in the oppositedirection (i.e., more ICD-only cases at younger ages). Thus, thedifference in the relative prevalence of the ICD-10-only cases inthe TTS and GUWAS sample appears to be due to factors otherthan age or sex differences, such as differences in clinic andrepresentative samples.
Does CD predict future APD? Forty-eight participants(30.2%) in the DTS met criteria for APD two or more times amongthe 159 who were assessed at least twice over ages 18, 19, and 24.Of those 159 young men, 109 had met criteria for CD at least oncebetween ages 7 and 17, and 39.5% of those with CD went on tomeet criteria for APD more than once (OR � 1.77, SE � 0.51, p �.001). Also of interest, 10% of young men who met criteria forAPD never met criteria for CD (n � 5). All five had shown twosymptoms of CD during at least one previous assessment, how-ever. These findings are consistent with previous reports based onthe age 18- and 19-year assessments in the DTS (Lahey et al.,2005; Loeber et al., 2002).
Table 1Numbers of 4- to 6-Year-Old Children in the Growing Up With ADHD Study (GUWAS) and The Tennessee Twin Study (TTS) WhoMet Diagnostic Criteria for Oppositional Defiant Disorder According to DSM–IV and ICD-10 Criteria
Not DSM–IV ODD DSM–IV ODD
GUWAS TTS (Twin 1) TTS (Twin 2) GUWAS TTS (Twin 1) TTS (Twin 2)
Not ICD ODD 94 1893 1895ICD ODD, but not DSM–IV ODD 9 55 57ODD in both ICD and DSM–IV 48 76 72
Note. ADHD � attention-deficit/hyperactivity disorder; DSM–IV � Diagnostic and Statistical Manual of Mental Disorders, 4th edition; ICD-10 �International Classification of Diseases, Version 10; ODD � oppositional defiant disorder.
Figure 4. Children’s Global Assessment Scale (CGAS; Setterberg, Bird, & Gould, 1992) ratings by inter-viewers and parents during each year of assessment among children who met criteria for only ICD-10 ODD, whomet both ICD-10 and DSM–IV criteria for ODD, or who did not met criteria for ODD according to eitherdefinition (Growing Up with ADHD Study; Lahey et al., 2007). ICD-10 � International Classification ofDiseases, Version 10; ODD � oppositional defiant disorder; DSM–IV � Diagnostic and Statistical Manual ofMental Disorders, 4th edition.
7SPECIAL SECTION: PREDICTIVE VALIDITY OF ODD AND CD
Issue 2: Predictive Validity of ODD in Children WhoNever Develop CD
The upper left panel of Figure 6 shows the course of ODDsymptoms over Years 1–13 in the GUWAS sample among threegroups of children: (a) children who met criteria for ODD in Year1 (at 4–6 years of age) who met criteria for CD at least onceduring Years 1–13; (b) children who met criteria for ODD in Year
1 but never met criteria for CD during Years 1–13; and (c) childrenwho did not meet criteria for ODD in Year 1 and never met criteriafor CD during Years 1–13, included as the comparison group.Across groups, there was a decline in ODD symptoms duringYears 2–13 (� � �0.09, z � �10.26, p � .0001). Over this timespan, children with ODD in Year 1 who met criteria for CD in atleast one wave (� � 2.07, z � 13.78, p � .0001) and children withODD in Year 1 who never met criteria for CD (� � 1.32, z � 6.20,p � .0001) exhibited more ODD symptoms than comparisonchildren. Children with ODD in Year 1 who never met criteria forCD exhibited fewer ODD symptoms during Years 2–13 thanchildren with ODD in Year 1 who ever met criteria for CD (� ��0.74, z � �4.36, p � .0001). Furthermore, when the Group �Year interaction was added to the model, it was significant (� ��0.09, z � �4.32, p � .0001), indicating that children with ODDin Year 1 who never met criteria for CD showed more rapidimprovement over Years 2–13 in ODD symptoms than childrenwith ODD in Year 1 who met criteria for CD at least once.
To assess the predictive validity of ODD in the subgroup thatnever met criteria for CD, analyses of three measures of functionalimpairment during Years 2–13 were conducted, controlling time,age in Year 1, family income in Year 1, race/ethnicity, site, cohort,and the diagnosis of ADHD and the number of CD symptoms inYear 1. Log-linear regression did not reveal a significant change innegative classmate social preferences ratings by teachers overYears 2–13 across groups. The upper right panel of Figure 6 showsthat both children with ODD in Year 1 who never met criteria forCD (� � 0.47, z � 1.96, p � .05) and children with ODD in Year1 who met criteria for CD at least once (� � 0.79, z � 3.46, p �
Figure 5. Mean maternal ratings of global impairment of twins who metcriteria for only ICD-10 ODD, who met both ICD-10 and DSM–IV criteriafor ODD, or who did not met criteria for ODD according to eitherdefinition (Tennessee Twin Study; Lahey et al., 2008). ICD-10 � Inter-national Classification of Diseases, Version 10; ODD � oppositionaldefiant disorder; DSM � Diagnostic and Statistical Manual.
Figure 6. The number of ODD symptoms in each assessment among three groups: Children with ODD in Year1 who never met CD criteria, children with ODD in Year 1 who met CD criteria at least once during Years 1–13,and children who did not meet ODD criteria in Year 1 and never met criteria for CD (upper left panel). Theremaining panels show differences in ratings of impairment by teachers, parents, and interviewers over timeamong the same three groups (Growing Up with ADHD Study; Lahey et al., 2007). ODD � oppositional defiantdisorder; CD � conduct disorder.
8 BURKE, WALDMAN, AND LAHEY

.0005) were given more negative social preference scores thancomparison children. The difference between these two ODDgroups was not significant at p � .05 (� � �0.32, z � �1.70, p �.09), and when the interaction with time was added to the model,there was not a significant difference in the rate of decline innegative social preference scores over years between the two ODDgroups (� � 0.00, z � 0.07, p � .94).
Linear regression revealed that parent CGAS ratings improvedover years across groups (� � 0.62, z � 5.49, p � .0001). Thelower left panel of Figure 6 shows that both children with ODD inYear 1 who never met criteria for CD (� � �5.08, z � �2.11, p �.05) and children with ODD in Year 1 who met criteria for CD atleast once (� � �13.94, z � �5.29, p � .0001) were given lowerCGAS ratings by parents than comparison children during Years2–13. Children with ODD in Year 1 who never met criteria for CDreceived higher CGAS ratings than children with ODD in Year 1who did meet criteria for CD (� � 8.85, z � 3.18, p � .005), butwhen the interaction with time was added to the model, there wasnot a significant difference in the rate of decline in CGAS im-provement over years between the two ODD groups (� � 0.62,z � 1.56, p � .12).
Linear regression also showed that interviewer CGAS ratingsimproved over years across groups (� � 0.85, z � 4.13, p �.0001). The lower right panel of Figure 6 shows that children withODD in Year 1 who met criteria for CD at least once (� � �14.15,z � �5.66, p � .0001), but not children with ODD in Year 1 whonever met criteria for CD (� � �3.94, z � �1.69, p � .09), weregiven lower CGAS ratings by interviewers than comparison chil-dren. Children with ODD in Year 1 who never met criteria for CDreceived higher interviewer CGAS ratings during Years 2–13 thanchildren with ODD in Year 1 who did meet criteria for CD (� �10.21, z � 3.88, p � .0001). Furthermore, when the interactionwith time was added to the model, children with ODD in Year 1who never met criteria for CD were found to exhibit more rapidincreases in CGAS scores over time than children who met withODD who met criteria for CD at least once (� � 0.70, z � 2.26,p � .05).
Outcomes of CD
Issue 3: Role of Psychopathylike Characteristicsin the Predictive Validity of CD
Analyses of the DTS data were conducted to assess the role ofIC in predicting APD using logistic regression models with APDas the outcome, clustered on participants to allow for all waves ofpredictors to be included in the model. When tested in separatemodels, both parent-reported (OR � 1.09, 95% CI � 1.03, 1.16,p � .004) and teacher-reported (OR � 1.11, 95% CI � 1.06, 1.16,p � .001) IC predicted APD, and both remained significant whentested simultaneously in a joint model with age as a covariate.Including the diagnosis of CD (OR � 2.12, 95% CI � 1.30, 3.47,p � .003) in the model rendered parent-reported IC nonsignificant(OR � 1.03, 95% CI � 0.96, 1.11, p � .38), whereas teacher-reported IC remained significant (OR � 1.08, 95% CI � 1.03,1.14, p � .002). When other measures of psychopathology weretested for entry into the model, only a diagnosis of ODD (OR �1.71, 95% CI � 1.05, 2.79, p � .03) entered the model. Testing forinteractions found that the interaction between CD and IC was
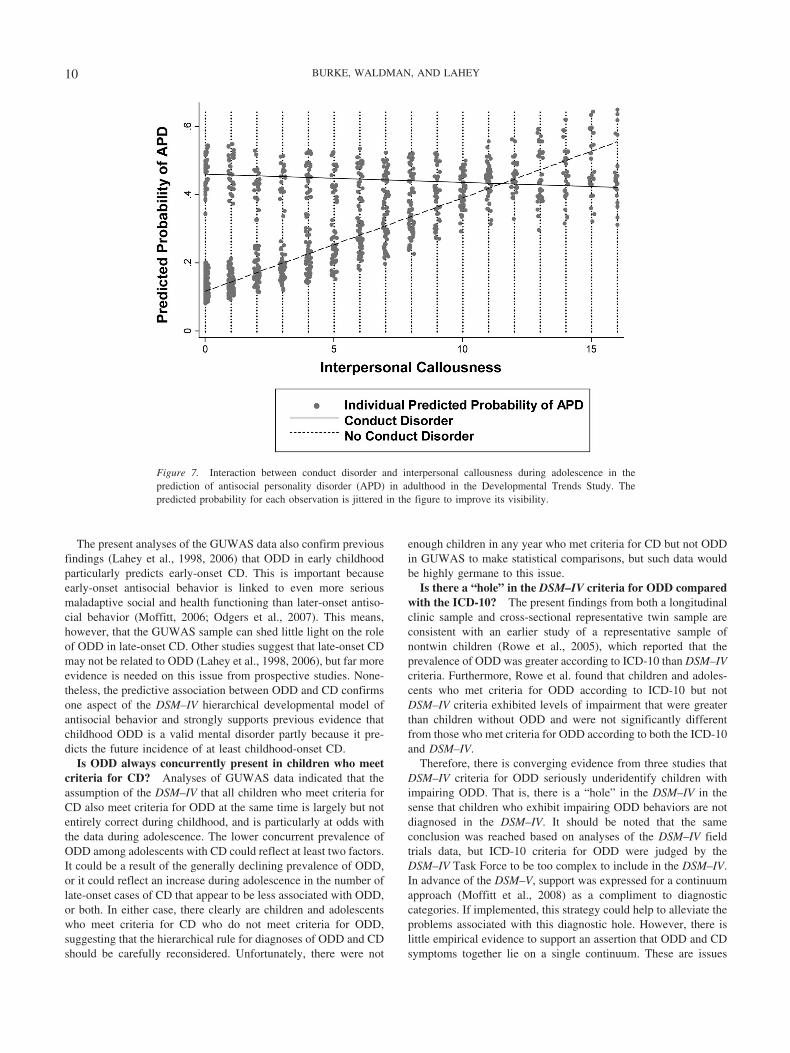
significant (OR � 0.86, 95% CI � .80, .93, p � .001) and renderedODD nonsignificant (see Table 2). The interaction term indicatedthat when CD was present, the level of concurrent IC made nodifference for the probability of APD in adulthood, whereas whena diagnosis of CD was absent, increasing IC led to an increasingprobability of APD (see Figure 7). IC scores approximately 1.5standard deviations above the mean and greater were associatedwith a probability of APD that was equal to CD. In fact, four of thefive young men who met criteria for APD without ever meetingcriteria for CD had IC scores in at least one year that were equalto or greater than 1.5 standard deviations above the mean IC score.
Discussion
The present analyses provide strong support for many aspects ofthe DSM–IV developmental model of ODD, CD, and APD butreveal important taxonomic problems, particularly regarding themore comprehensive coverage of the ICD-10 versus the DSM–IVODD and the role of callous interpersonal behavior in regardsto CD.
Hierarchical Developmental Relations Among ODD,CD, and APD
In order to evaluate the predictive validity of ODD, CD, andAPD, it is necessary to know whether they are related to oneanother developmentally in the hierarchical manner described inthe DSM–IV.
Is ODD in early childhood a developmental precursor toCD? The present findings suggest that ODD is a robust predictorof at least early-onset CD. In the longitudinal GUWAS sample, thediagnosis of ODD at 4–6 years of age predicted incident cases ofCD over the next 12 years, controlling for both the diagnosis ofADHD and the number of subthreshold CD symptoms at 4–6years of age. Indeed, among children who did not meet criteria forODD at 4–6 years but later met criteria for CD, diagnostic criteriawere first met for ODD in a preceding wave or in the same waveas criteria were first met for CD in 79% of cases. Thus, criteria forODD were met before or at about the same time as CD in nearlyall cases. These findings are important because the GUWAS beganwhen participating children were young enough to capture most ofthe developmental transition from ODD to childhood-onset CD.Nonetheless, such developmental relations remain hidden from usfor the children who already met criteria for CD at 4–6 years ofage.
Table 2Interpersonal Callousness and Conduct Disorder in thePrediction of APD in the Developmental Trends Study (DTS)
Odds ratio SE p 95% CI
Teacher-rated IC 1.15 0.03 �.001 1.08, 1.22CD 2.37 0.57 �.001 1.48, 3.80CD � IC interaction 0.86 0.03 �.001 0.80, 0.93ODD 1.56 0.40 .08 0.95, 2.56Age 1.06 0.03 .04 1.00, 1.11
Note. IC � interpersonal callousness; CD � conduct disorder; ODD �oppositional defiant disorder.
9SPECIAL SECTION: PREDICTIVE VALIDITY OF ODD AND CD
The present analyses of the GUWAS data also confirm previousfindings (Lahey et al., 1998, 2006) that ODD in early childhoodparticularly predicts early-onset CD. This is important becauseearly-onset antisocial behavior is linked to even more seriousmaladaptive social and health functioning than later-onset antiso-cial behavior (Moffitt, 2006; Odgers et al., 2007). This means,however, that the GUWAS sample can shed little light on the roleof ODD in late-onset CD. Other studies suggest that late-onset CDmay not be related to ODD (Lahey et al., 1998, 2006), but far moreevidence is needed on this issue from prospective studies. None-theless, the predictive association between ODD and CD confirmsone aspect of the DSM–IV hierarchical developmental model ofantisocial behavior and strongly supports previous evidence thatchildhood ODD is a valid mental disorder partly because it pre-dicts the future incidence of at least childhood-onset CD.
Is ODD always concurrently present in children who meetcriteria for CD? Analyses of GUWAS data indicated that theassumption of the DSM–IV that all children who meet criteria forCD also meet criteria for ODD at the same time is largely but notentirely correct during childhood, and is particularly at odds withthe data during adolescence. The lower concurrent prevalence ofODD among adolescents with CD could reflect at least two factors.It could be a result of the generally declining prevalence of ODD,or it could reflect an increase during adolescence in the number oflate-onset cases of CD that appear to be less associated with ODD,or both. In either case, there clearly are children and adolescentswho meet criteria for CD who do not meet criteria for ODD,suggesting that the hierarchical rule for diagnoses of ODD and CDshould be carefully reconsidered. Unfortunately, there were not
enough children in any year who met criteria for CD but not ODDin GUWAS to make statistical comparisons, but such data wouldbe highly germane to this issue.
Is there a “hole” in the DSM–IV criteria for ODD comparedwith the ICD-10? The present findings from both a longitudinalclinic sample and cross-sectional representative twin sample areconsistent with an earlier study of a representative sample ofnontwin children (Rowe et al., 2005), which reported that theprevalence of ODD was greater according to ICD-10 than DSM–IVcriteria. Furthermore, Rowe et al. found that children and adoles-cents who met criteria for ODD according to ICD-10 but notDSM–IV criteria exhibited levels of impairment that were greaterthan children without ODD and were not significantly differentfrom those who met criteria for ODD according to both the ICD-10and DSM–IV.
Therefore, there is converging evidence from three studies thatDSM–IV criteria for ODD seriously underidentify children withimpairing ODD. That is, there is a “hole” in the DSM–IV in thesense that children who exhibit impairing ODD behaviors are notdiagnosed in the DSM–IV. It should be noted that the sameconclusion was reached based on analyses of the DSM–IV fieldtrials data, but ICD-10 criteria for ODD were judged by theDSM–IV Task Force to be too complex to include in the DSM–IV.In advance of the DSM–V, support was expressed for a continuumapproach (Moffitt et al., 2008) as a compliment to diagnosticcategories. If implemented, this strategy could help to alleviate theproblems associated with this diagnostic hole. However, there islittle empirical evidence to support an assertion that ODD and CDsymptoms together lie on a single continuum. These are issues
Figure 7. Interaction between conduct disorder and interpersonal callousness during adolescence in theprediction of antisocial personality disorder (APD) in adulthood in the Developmental Trends Study. Thepredicted probability for each observation is jittered in the figure to improve its visibility.
10 BURKE, WALDMAN, AND LAHEY

with serious consequences that must be revisited by the DSM–Vwork groups and Task Force.
Does CD predict APD? The present analyses of the DTSelaborate on early assessments of the predictive association ofchildhood and adolescent CD with APD at ages 18 or 19 years(Lahey et al., 2005; Loeber et al., 2002). The present findingssuggest that, when APD is defined as meeting diagnostic criteriafor APD in at least two assessments over 18, 19, and 24 years,approximately one third of those with CD progress to APD. Thisis roughly consistent with the proportion of children who progressfrom ODD to CD in the DTS. For a small group, APD emerged inyoung adulthood without ever having met criteria for CD, althoughno youth in the DTS who met APD criteria in at least twoassessments was completely absent of a history of CD symptoms.Recent evidence from a large population-based study are consis-tent, finding that CD measured in childhood or adolescence is thesingle strongest predictor of young adult APD among mentalhealth disorders (Copeland, Shanahan, Costello, & Angold, 2009).
The present analyses of the DTS are the first to report on APDas an outcome of CD when APD was assessed repeatedly over a6-year period. These results suggest on the whole that the hierar-chical developmental model of ODD, CD, and APD assumed bythe DSM–IV reflects the progression in antisocial behavior of somechildren. Two important caveats to this hierarchical model shouldbe emphasized, however. First, the findings of the DTS are likelyrelevant only to early-onset CD and may not be relevant to later-onset CD. Second, it is clear that not all children with ODD willprogress to CD and then to APD in young adulthood; indeed, themajority of children with ODD do not. Much remains to be learnedfrom longitudinal studies about the development of disruptive andantisocial behavior, particularly using studies of population-basedsamples in addition to clinic samples.
Predictive Validity of ODD Among Children WhoNever Develop CD
In the GUWAS sample, children who met diagnostic criteria forODD in Year 1 (at 4–6 years of age) continued to exhibit sub-stantial numbers of ODD symptoms and significant levels offunctional impairment over many years, even though there was ageneral trend for symptoms and impairment to improve over the12-year follow-up period. The long-term GUWAS longitudinaldatabase affords a unique opportunity to determine whether ODDat 4–6 years exhibits predictive validity even in those childrenwho never develop CD. Children with ODD in Year 1 who nevermet criteria for CD continued to exhibit atypical numbers of ODDsymptoms for at least 6–7 years, even though they showed a morerapid decline in ODD symptoms than children diagnosed withODD in Year 1 who did meet criteria for CD. Nonetheless, bothODD groups continued to exhibit substantial levels of functionalimpairment relative to comparison children over at least 6–7 yearsafter the diagnosis. Thus, the diagnosis of ODD in young childrenhas clear predictive validity both in the sense that ODD oftenprecedes the more impairing disorder of CD and because evenchildren with ODD who never meet criteria for CD continue toexhibit marked levels of functional impairment both at the time ofdiagnosis and for many years to come. It is encouraging that somechildren recover from early ODD, but they do so very gradually
and continue to exhibit impairment over the long period in whichthey continue to exhibit symptoms.
Does IC Improve the Prediction of APD AmongChildren With CD?
Are children with CD who exhibit early psychopathylike char-acteristics more likely to meet diagnostic criteria for APD? In theDTS, teacher-reported IC from childhood through adolescencesignificantly predicted APD, along with CD and ODD diagnoses.As with the prediction of young adult psychopathy in the samesample (Burke et al., 2007), parent-reported IC was not signifi-cantly predictive after accounting for other covariates, notably CD,but teacher-reported IC was a significant independent predictor offuture APD.
It is important to note that the significant interaction between ICand CD did not mean that children with CD who have higher levelsof IC are at greater risk of developing APD. Rather, the significantinteraction indicated that when CD was present, the level of ICmade little difference in the probability of future APD. In contrast,when CD was absent, greater IC was associated with a greater riskfor APD in young adulthood. The possibility that callous interper-sonal traits should be used instead of age of onset as the basis forsubtyping CD to reduce its heterogeneity is under consideration forthe DSM–V. Our findings suggest that IC features do not improvethe prediction of APD when CD is present, which does not supportusing IC as the basis for subtyping CD in the DSM–V to improvethe prediction of APD.
The results of the present analyses are at odds with previousanalyses from the DTS (Loeber et al., 2002), however, whichfound that callousness did distinguish those who went on to meetcriteria for APD from those who did not over and above thepresence of CD. Several key differences between the presentanalyses and the prior findings explain these differences. First andforemost, the previous analyses generated predictors by collapsingacross all waves of predictors to conduct a simple logistic regres-sion model. In contrast, the present analyses maintain all waves ofdata while accounting for clustering by participant, which allowsfor the evaluation of the relative strength of CD and callousnesscontemporaneously at each wave. The present analyses also in-cluded the additional assessment of APD at age 24, and requiredAPD to be present over multiple assessments.
In addition, the prior analyses used an ad hoc measure ofcallousness rather than the somewhat more established constructused here. Thus, although the present findings do not support theoption of using callousness to subtype CD, the overall evidenceacross studies with differing constructs and during differing de-velopmental periods remains mixed.
Limitations
The longitudinal studies used in the present analyses have theadvantage of covering large spans of development but were rela-tively small and not well powered statistically. Although a strongargument can be made for testing diagnostic criteria in the kinds ofclinic samples for which the DSM–V is intended, these samplescannot be said to be representative of all clinic-referred children,but were selected to oversample children with ADHD (theGUWAS) or children with CD (the DTS). There are a few more
11SPECIAL SECTION: PREDICTIVE VALIDITY OF ODD AND CD

useful longitudinal studies of clinic samples that used DSM–IVcriteria, but these limitations must be acknowledged. Furthermore,the fact that the DTS included only boys and the GUWAS includedonly a minority of girls is an important limitation of the presentanalyses. Fortunately, longitudinal studies of disruptive behaviordisorders in girls are now available to test the generality of thepresent findings (e.g., Loeber, Hipwell, Battista, Sembower, &Stouthamer-Loeber, 2009; Odgers et al., 2008).
References
Achenbach, T. M., & Edelbrock, C. (1983). Manual for the Child BehaviorChecklist and revised Child Behavior Profile. Burlington: University ofVermont.
American Psychiatric Association. (1994). Diagnostic and statistical man-ual of mental disorders (4th ed.). Washington, DC: Author.
Berkson, J. (1946). Limitations of the application of fourfold table analysisto hospital data. Biometrics Bulletin, 2, 47–53.
Burke, J. D. (2007). Antisocial personality disorder. In A. Bell & M.Reinecke (Eds.), Personality disorders in childhood (pp. 429–494).New York, NY: Wiley.
Burke, J. D. (in press). The relationship between conduct disorder andoppositional defiant disorder and their continuity with antisocial behav-iors: Evidence from longitudinal clinical studies. In D. Shaffer, E.Leibenluft, & L. A. Rohde (Eds.), Externalizing disorders of childhood:Refining the research agenda for DSM–V. Arlington, VA: AmericanPsychiatric Association.
Burke, J. D., Loeber, R., & Birmaher, B. (2002). Oppositional defiantdisorder and conduct disorder: A review of the past 10 years, part II.Journal of the American Academy of Child and Adolescent Psychiatry,41, 1275–1293.
Burke, J. D., Loeber, R., & Lahey, B. B. (2003). Course and outcomes ofoppositional defiant disorder and conduct disorder. In C. Essau (Ed.),Conduct and oppositional defiant disorders: Epidemiology, risk factorsand treatment (pp. 61–94). Mahwah, NJ: Erlbaum.
Burke, J. D., Loeber, R., & Lahey, B. B. (2007). Adolescent conductdisorder and interpersonal callousness as predictors of psychopathy inyoung adults. Journal of Clinical Child and Adolescent Psychology, 36,334–346.
Burke, J. D., Loeber, R., Lahey, B. B., & Rathouz, P. J. (2005). Develop-mental transitions among affective and behavioral disorders in adoles-cent boys. Journal of Child Psychology and Psychiatry, 46, 1200–1210.
Bussing, R., Gary, F. A., Mason, D. M., Leon, C. E., Sinha, K., & Garvan,C. W. (2003). Child temperament, ADHD and caregiver strain: Explor-ing relationships in an epidemiological sample. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 42, 184–192.
Bussing, R., Zima, B. T., Gary, F. A., Mason, D. M., Leon, C. E., Sinha,K., & Garvan, C. W. (2003). Social networks, caregiver strain, andutilization of mental health services among elementary school studentsat high risk for ADHD. Journal of the American Academy of Child &Adolescent Psychiatry, 42, 842–850.
Copeland, W. E., Shanahan, L., Costello, E. J., & Angold, A. (2009).Childhood and adolescent psychiatric disorders as predictors of youngadult disorders. Archives of General Psychiatry, 66, 764–772.
Costello, A. J., Edelbrock, C., Dulcan, M. K., Kalas, R., & Klaric, S.(1987). Diagnostic Interview Schedule for Children (DISC). Pittsburgh,PA: Western Psychiatric Institute and Clinic.
Dishion, T. (1990). The peer context of troublesome child and adolescentbehavior. In P. E. Leone (Ed.), Understanding troubled and troublingyouth. Newbury Park, CA: Sage.
Frick, P. J., Cornell, A. H., Barry, C. T., Bodin, S. D., & Dane, H. E.(2003). Callous-unemotional traits and conduct problems in the predic-tion of conduct problem severity, aggression, and self-report of delin-quency. Journal of Abnormal Child Psychology, 31, 457–470.
Goodman, S. H., Lahey, B. B., Fielding, B., Dulcan, M., Narrow, W., &Regier, D. (1997). Representativeness of clinical samples of youth withmental disorders: A preliminary population-based study. Journal ofAbnormal Psychology, 106, 3–14.
Hart, E. L., Lahey, B. B., Loeber, R., & Hanson, K. S. (1994). Criterionvalidity of informants in the diagnosis of disruptive behavior disorders inchildren: A preliminary study. Journal of Consulting and Clinical Psy-chology, 62, 410–414.
Hart, S. D., Cox, D. N., & Hare, R. D. (1995). The Hare PsychopathyChecklist: Screening version (PCL:SV). North Tonawanda, NY: Multi-Health Systems.
Jensen, P. S., Rubio-Stipec, M., Canino, G., Bird, H. R., Dulcan, M. K.,Schwab-Stone, M. E., & Lahey, B. B. (1999). Parent and child contri-butions to diagnosis of mental disorder: Are both informants alwaysnecessary? Journal of the American Academy of Child & AdolescentPsychiatry, 38, 1569–1579.
Lahey, B. B., Applegate, B., Barkley, R. A., Garfinkel, B., McBurnett, K.,Kerdyk, L., . . . Newcorn, J. (1994). DSM–IV field trials for oppositionaldefiant disorder and conduct disorder in children and adolescents. Amer-ican Journal of Psychiatry, 151, 1163–1171.
Lahey, B. B., Applegate, B., Waldman, I. D., Loft, J. D., Hankin, B. L., &Rick, J. (2004). The structure of child and adolescent psychopathology:Generating new hypotheses. Journal of Abnormal Psychology, 113,358–385.
Lahey, B. B., Goodman, S. H., Waldman, I. D., Bird, H., Canino, G.,Jensen, P., . . . Applegate, B. (1999). Relation of age of onset to the typeand severity of child and adolescent conduct problems. Journal ofAbnormal Child Psychology, 27, 247–260.
Lahey, B. B., Hartung, C. M., Loney, J., Pelham, W. E., Chronis, A. M.,& Lee, S. S. (2007). Are there sex differences in the predictive validityof DSM–IV ADHD among younger children? Journal of Clinical Childand Adolescent Psychology, 36, 1–14.
Lahey, B. B., & Loeber, R. (1994). Framework for a developmental modelof oppositional defiant disorder and conduct disorder. In D. K. Routh(Ed.). Disruptive behavior disorders in childhood (pp. 139–180). NewYork, NY: Plenum Press.
Lahey, B. B., Loeber, R., Burke, J. D., & Applegate, B. (2005). Predictingfuture antisocial personality disorder in males from a clinical assessmentin childhood. Journal of Consulting and Clinical Psychology, 73, 389–399.
Lahey, B. B., Loeber, R., Quay, H. C., Applegate, B., Shaffer, D., Wald-man, I., . . . Bird, H. (1998). Validity of DSM–IV subtypes of conductdisorder based on age of onset. Journal of the American Academy ofChild & Adolescent Psychiatry, 37, 435–442.
Lahey, B. B., McBurnett, K., & Loeber, R. (2000). Are attention-deficithyperactivity disorder and oppositional defiant disorder developmentalprecursors to conduct disorder? In A. Sameroff, M. Lewis, & S. Miller(Eds.), Handbook of developmental psychopathology (2nd ed., pp. 431–446). New York, NY: Plenum Press.
Lahey, B. B., Rathouz, P. J., Applegate, B., Van Hulle, C. A., Garriock,H. A., Urbano, R. C., . . . Waldman, I. D. (2008). Testing structuralmodels of DSM–IV symptoms of common forms of child and adolescentpsychopathology. Journal of Abnormal Child Psychology, 36, 187–206.
Lahey, B. B., Van Hulle, C. A., Rathouz, P. J., Rodgers, J. L., D’Onofrio,B. M., & Waldman, I. D. (2009). Are oppositional-defiant andhyperactive-inattentive symptoms developmental precursors to conductproblems in late childhood? Genetic and environmental links. Journal ofAbnormal Child Psychology, 37, 45–58.
Lahey, B. B., Van Hulle, C. A., Waldman, I. D., Rodgers, J. L., D’Onofrio,B. M., Pedlow, S., . . . Keenan, K. (2006). Testing descriptive hypoth-eses regarding sex differences in the development of conduct problemsand delinquency. Journal of Abnormal Child Psychology, 34, 737–755.
Lavigne, J. V., Cicchetti, C., Gibbons, R. D., Binns, H. J., Larsen, L., &DeVito, C. (2001). Oppositional defiant disorder with onset in preschool
12 BURKE, WALDMAN, AND LAHEY

years: Longitudinal stability and pathways to other disorders. Journal ofthe American Academy of Child & Adolescent Psychiatry, 40, 1393–1400.
Lee, S. S., Lahey, B. B., Owens, E. B., & Hinshaw, S. P. (2008). Fewpreschool boys and girls with ADHD are well-adjusted during adoles-cence. Journal of Abnormal Child Psychology, 36, 373–383.
Loeber, R., Burke, J. D., & Lahey, B. B. (2002). What are adolescentantecedents to antisocial personality disorder? Criminal Behaviour andMental Health, 12, 24–26.
Loeber, R., Burke, J. D., Lahey, B. B., Winters, A., & Zera, M. (2000).Oppositional defiant and conduct disorder: A review of the past 10 years,part I. Journal of the American Academy of Child & Adolescent Psy-chiatry, 39, 1468–1484.
Loeber, R., Burke, J. D., & Pardini, D. A. (2009). Oppositional defiantdisorder, conduct disorder and psychopathy. Journal of Child Psychol-ogy and Psychiatry, 50, 133–140.
Loeber, R., Farrington, D. P., Stouthamer-Loeber, M., & Van Kammen,W. B. (1998). Multiple risk factors for multi-problem boys: Co-occurrence of delinquency, substance use, attention deficit, conductproblems, physical aggression, covert behavior, depressed mood, andshy/withdrawn behavior. In R. Jessor (Ed.), New perspectives on ado-lescent risk behavior (pp. 90–149). Cambridge, England: CambridgeUniversity Press.
Loeber, R., Green, S. M., Lahey, B. B., Frick, P. J., & McBurnett, K.(2000). Findings on disruptive behavior disorders from the first decadeof the developmental trends studies. Clinical Child and Family Psychol-ogy Review, 3, 37–60.
Loeber, R., Green, S. M., Lahey, B. B., & Stouthamer-Loeber, M. (1989).Optimal informants on childhood disruptive behaviors. Developmentand Psychopathology, 1, 317–337.
Loeber, R., Hipwell, A., Battista, D., Sembower, M., & Stouthamer-Loeber, M. (2009). Intergenerational transmission of multiple problembehaviors: Prospective relationships between mothers and daughters.Journal of Abnormal Child Psychology, 37, 1035–1048.
Loeber, R., Lahey, B. B., & Thomas, C. (1991). The diagnostic conundrumof oppositional defiant disorder and conduct disorder. Journal of Ab-normal Psychology, 100, 379–390.
Lynam, D. R., Caspi, A., Moffitt, T. E., Loeber, R., & Stouthamer-Loeber,M. (2007). Longitudinal evidence that psychopathy scores in earlyadolescence predict adult psychopathy. Journal of Abnormal Psychol-ogy, 116, 155–165.
Mannuzza, S., Klein, R. G., Abikoff, H., & Moulton, J. L. (2004). Signif-icance of childhood conduct problems to later development of conductdisorder among children with ADHD: A prospective follow-up study.Journal of Abnormal Child Psychology, 32, 565–573.
Mannuzza, S., Klein, R. G., Bonagura, N., Malloy, P., Giampino, T. L., &Addalli, K. A. (1991). Hyperactive boys almost grown up: Replicationof psychiatric status. Archives of General Psychiatry, 48, 77–83.
Moffitt, T. E. (2006). Life-course persistent and adolescence-limited anti-social behavior. In D. Cicchetti & D. Cohen (Eds.), Developmentalpsychopathology (2nd ed., pp. 570–598). New York, NY: Wiley.
Moffitt, T. E., Arseneault, L., Jaffee, S. R., Kim-Cohen, J., Koenen, K. C.,Odgers, C. L., . . . Viding, E. (2008). DSM–V conduct disorder: Researchneeds for an evidence base. Journal of Child Psychology and Psychiatryand Allied Disciplines, 49, 3–33.
Moffitt, T. E., Caspi, A., Harrington, H., & Milne, B. J. (2002). Males on
the life-course-persistent and adolescence-limited antisocial pathways:Follow-up at age 26 years. Development and Psychopathology, 14,179–207.
Odgers, C. L., Caspi, A., Broadbent, J. M., Dickson, N., Hancox, R. J.,Harrington, H., . . . Moffitt, T. E. (2007). Prediction of differential adulthealth burden by conduct problem subtypes in males. Archives of Gen-eral Psychiatry, 64, 476–484.
Odgers, C. L., Moffitt, T. E., Broadbent, J. M., Dickson, N., Hancox, R. J.,Harrington, H., . . . Caspi, A. (2008). Female and male antisocial trajec-tories: From childhood origins to adult outcomes. Development andPsychopathology, 20, 673–716.
Pardini, D. A., & Loeber, R. (2008). Interpersonal callousness trajectoriesacross adolescence: Early social influences and adult outcomes. Crimi-nal Justice and Behavior, 35, 173–196.
Pardini, D. A., Obradovıc, J., & Loeber, R. (2006). Interpersonal callous-ness, hyperactivity/impulsivity, inattention, and conduct problems asprecursors to delinquency persistence in boys: A comparison of threegrade-based cohorts. Journal of Clinical Child and Adolescent Psychol-ogy, 35, 46–59.
Pelham, W. E., Gnagy, E. M., Greenslade, K. E., & Milich, R. (1992).Teacher ratings of DSM–III–R symptoms of the disruptive behaviordisorders. Journal of the American Academy of Child & AdolescentPsychiatry, 31, 210–218.
Robins, L. N., & Helzer, J. E. (1988). The Diagnostic Interview Schedule:Its development, evolution, and use. Social Psychiatry and PsychiatricEpidemiology, 23, 6–16.
Rowe, R., Maughan, B., Costello, E. J., & Angold, A. (2005). Definingoppositional defiant disorder. Journal of Child Psychology and Psychi-atry and Allied Disciplines, 46, 1309–1316.
Rowe, R., Maughan, B., Moran, P., Ford, T., Briskman, J., & Goodman, R.(2010). The role of callous and unemotional traits in the diagnosis ofconduct disorder. Journal of Child Psychology and Psychiatry andAllied Disciplines, 51, 688–695.
Setterberg, S., Bird, H., & Gould, M. (1992). Parent and interviewerversion of the Children’s Global Assessment Scale. New York: NewYork State Psychiatric Institute.
Shaffer, D., Fisher, P., Dulcan, M., Davies, M., Piacentini, J., Schwab-Stone, M., . . . Regier, D. A. (1996). The NIMH Diagnostic InterviewSchedule for Children (DISC 2.3): Description, acceptability, preva-lences, and performance in the MECA study. Journal of the AmericanAcademy of Child & Adolescent Psychiatry, 35, 865–877.
Shaffer, D., Fisher, P., Piacentini, J., Schwab-Stone, M., & Wicks, J.(1993). Diagnostic Interview Schedule for Children. New York, NY:Columbia University.
Vandiver, T., & Sher, K. J. (1991). Temporal stability of the DiagnosticInterview Schedule. Psychological Assessment, 3, 277–281.
World Health Organization. (1992). International Statistical Classificationof Diseases and related health problems (10th rev.). Geneva, Switzer-land: Author.
Zeger, S. L., & Liang, K. L. (1986). Longitudinal data analysis for discreteand continuous outcomes. Biometrics, 42, 121–130.
Received June 13, 2009Revision received March 2, 2010
Accepted March 2, 2010 �
13SPECIAL SECTION: PREDICTIVE VALIDITY OF ODD AND CD