Embed Size (px)
Citation preview

C
Aod
THD
a
ARR2A
KAEC
I
sscfewvclR
NK
(
1h
Journal of Cardiology Cases 9 (2014) 67–70
Contents lists available at www.sciencedirect.com
Journal of Cardiology Cases
journa l h om epage: www.elsev ier .com/ locate / j ccase
ase Report
cute myocardial infarction caused by left anterior descending arterycclusion presenting as inferior ST elevation and anterior STepression
suyoshi Honda (MD) ∗, Kazuteru Fujimoto (MD), Yuji Miyao (MD),idenobu Koga (MD), Masanobu Ishii (MD)
epartment of Cardiology, Cardiovascular Center, National Hospital Organization Kumamoto Medical Center, Kumamoto, Japan
r t i c l e i n f o
rticle history:eceived 29 August 2013eceived in revised form4 September 2013ccepted 5 October 2013
eyword:cute myocardial infarctionlectrocardiogramollaterals
a b s t r a c t
We report a case of acute myocardial infarction caused by left anterior descending artery occlusionpresenting as ST elevation in the inferior leads and ST depression in the precordial leads, suggestingan involvement of the right coronary artery (RCA). However, coronary angiography (CAG) showed acomplete occlusion of the proximal left anterior descending (LAD) coronary artery and collaterals fromthe left circumflex coronary artery and the RCA. Although he underwent primary percutaneous coro-nary intervention (PCI), he had chest pain at four days after primary PCI. His electrocardiogram (ECG)showed precordial ST elevation, suggesting an involvement of the LAD. Emergent CAG showed a completeocclusion of the proximal LAD without collaterals, but his ECG showed precordial ST elevation that wasdifferent from ST changes seen on admission. These unusual ST-segment changes might be associated
with a weaker anterior ischemia due to collaterals and a strong inferior ischemia due to wrapped LADartery.<Learning objective: Inferior ST elevation and anterior ST depression generally indicate inferior myocar-dial infarction. However, the unusual ST-segment changes seen in this patient with anterior myocardialinfarction might be associated with a weaker anterior ischemia due to collaterals and a strong inferiorleft a3 Jap
ischemia due to wrapped© 201
ntroduction
Acute ST-segment elevations in the inferior leads generallyuggest acute occlusion of the right coronary artery (RCA). Occlu-ion of the left anterior descending coronary artery (LAD) mayause infarction of the anterior wall of the left ventricle, mani-ested as precordial ST-segment elevations. Inferior ST-segmentlevations due to occlusion of a LAD may reflect an ischemia ofrapped LAD artery [1,2]. We describe a patient with ST ele-
ation in inferior leads and ST depression in precordial leadsaused by acute occlusion at the proximal segment LAD with col-ateral flow from the left circumflex (LCx) coronary artery andCA.
∗ Corresponding author at: Department of Cardiology, Cardiovascular Center,ational Hospital Organization Kumamoto Medical Center, 1-5 Ninomaru, Chuo-ku,umamoto 860-0008, Japan. Tel.: +81 96 353 6501; fax: +81 96 325 2519.
E-mail addresses: [email protected], [email protected]. Honda).
878-5409/$ – see front matter © 2013 Japanese College of Cardiology. Published by Elsettp://dx.doi.org/10.1016/j.jccase.2013.10.003
nterior descending artery.>anese College of Cardiology. Published by Elsevier Ltd. All rights reserved.
Case report
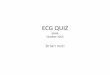
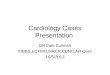
A 53-year-old man was referred to our hospital for chest painhe had experienced for a few hours. His electrocardiogram (ECG)showed ST-segment elevation in the inferior leads and ST-segmentdepression in the V2–V4 leads (Figs. 1 and 2A), suggesting aninvolvement of the RCA. However, emergent coronary angiography(CAG) showed a complete proximal occlusion of the LAD coronaryartery (Fig. 3A, arrow 1) and collaterals from the LCx coronary artery(Fig. 3A and B, arrows 2–3) and the RCA (Fig. 3C, arrows 4–5). Heunderwent primary percutaneous coronary intervention (PCI) withcoronary artery stenting to the infarct-related LAD. Four days afterprimary PCI, he had chest pain again. His ECG showed precordial STelevation (Figs. 1B and 2), suggesting an involvement of LAD. Emer-gent CAG showed a complete proximal occlusion of the LAD withoutcollaterals (Fig. 3D, arrow 6). He underwent PCI for subacute stentthrombosis (SAST) (Fig. 3E and F).
Discussion
We report for the first time that coronary artery occlusion atthe same segment in a patient showed different ECG changes.
vier Ltd. All rights reserved.

68 T. Honda et al. / Journal of Cardiology Cases 9 (2014) 67–70
stent
At(ci
miswlisea
Fig. 1. Electrocardiogram (ECG) on admission and at the time of subacute
lthough his ECG on admission showed ST-segment elevation inhe inferior leads and ST-segment depression in the V2–V4 leadsFigs. 1A and 2), his ECG at four days after primary PCI showed pre-ordial ST elevation (Figs. 1B and 2). Interestingly, the culprit lesionn these coronary events was the same segment, proximal LAD.
Inferior ST-segment elevation during anterior wall acuteyocardial infarction (AMI) due to LAD coronary artery occlusion
s uncommon [3,4]. Usually, 2 conditions are thought to be neces-ary for these findings: relatively small mass of ischemic anteriorall myocardium, resulting in a weaker anterior injury current and
ess reciprocal inferior ST-segment depression, and a concomitant
nferior wall transmural ischemia that further shifts the inferior STegments upward. According to other studies, inferior ST-segmentlevation was related to a distal LAD stenosis or a wrapped LADrtery [1,2].thrombosis (SAST). (A) ECG on admission and (B) ECG at the time of SAST.
In our case report, first ECG might be associated with a weakeranterior ischemia due to collaterals and a strong ischemia due toa wrapped LAD artery. It might be associated with rich collateralsfrom RCA and LCx to middle segment of LAD and diagonal branchand fewer collaterals to apical segment of LAD. This unusual patternwas previously presented by Brunetti et al. However, a pathophy-siological explanation for this peculiar ECG pattern was explainedwith distal embolization into the distal, inferior part either of theLAD or LCx, or a concomitant spasm of the RCA because they didnot undertake emergent coronary angiography [5]. In our patient,rich collaterals from the LCx and RCA supplied the anterior wall and
the total occlusion of the wrapped LAD caused an ischemia of theinferior wall.The second ECG shows the complete occlusion of the proximalLAD. This was explained with an ischemia of anterior wall, because

T. Honda et al. / Journal of Cardiology Cases 9 (2014) 67–70 69
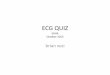
Fig. 2. Electrocardiogram (ECG) evolution. ECG after admission in emergency room demonstrated ST-elevation in II, III, aVF leads with combined ST-depression in V2–V4l 4 dayn
tsoSi
eads. After primary PCI, ST was normal with abnormal Q wave in V1–V3 leads. Atormal. Negative T waves were present before discharge in V1–V4, aVL leads.
here were not collaterals from other coronary arteries. First, past
tudy showed that coronary collaterals accompanied with coronarycclusion in dogs disappeared within 24 h after reperfusion [6].econd, a previous study demonstrated that collateral flow mightncrease considerably over time even in the first 6 h following acutes after primary PCI, ST-elevation in V1–V4 leads was detectable. After PCI, ST was
coronary occlusion [7]. In this case, the time from chest pain to
angiography was only 25 min at the time of SAST although it was3.3 h on admission. The collaterals to LAD might not work at SAST,because they had already disappeared after primary PCI and therewas not enough time for the collaterals to LAD to develop again.
70 T. Honda et al. / Journal of Cardiology Cases 9 (2014) 67–70
F thromf nal brf l LAD
v
C
ii
R
[
[
[
[
[
[
ig. 3. Coronary angiography (CAG) on admission and at the time of subacute stentrom LCx to diagonal branch, (B) CAG on admission, 3: collaterals from LCx to diagorom RCA to the distal LAD, (D) CAG at the time of SAST, 4: occlusion of the proxima
In summary, this is an exceptional ECG showing inferior ST ele-ation and anterior ST depression, secondary to occlusion of LAD.
onflict of interest
We do not have a direct financial relation with the commercialdentities mentioned in our paper that might lead to conflict ofnterest for any of the authors.
eferences
1] Sapin PM, Musselman DR, Dehmer GJ, Cascio WE. Implication of inferior ST-
segment elevation accompanying anterior wall acute myocardial infarction forthe angiographic morphology of the left anterior descending coronary arterymorphology and site of occlusion. Am J Cardiol 1992;69:860–5.2] Sasaki K, Yotsukura M, Sakata K, Yoshino H, Ishikawa K. Relation of ST-segmentchanges in inferior leads during anterior wall acute myocardial infarction to
[
bosis (SAST). (A) CAG on admission, 1: occlusion of the proximal LAD, 2: collateralsanch, (C) CAG on admission, 4: collaterals from RCA to septal branch, 5: collaterals, (E) CAG at the time of SAST, and (F) CAG at the time of SAST, 7: wrapped LAD.
length and occlusion site of the left anterior descending coronary artery. Am JCardiol 2001;87:1340–5.
3] Kosuge M, Kimura K. Clinical implication of electrocardiograms for patients withanterior wall ST-segment elevation acute myocardial infarction in the interven-tional era. Circ J 2012;76:32–40.
4] Kosuge M, Ebina T, Hibi K, Iwahashi N, Tsukahara K, Endo M, Maejima N,Nagashima Z, Suzuki H, Morita S, Umemura S, Kimura K. Differences in nega-tive T waves between Takotsubo cardiomyopathy and reperfused anterior acutemyocardial infarction. Circ J 2012;76:462–8.
5] Brunetti ND, Correale M, Ieva R, De Gennaro L, Pellegrino PL, Cucclo A,Di Biase M. An usual case of left anterior descending coronary artery occlusion-anterior ST depression and inferior ST elevation. J Electrocardiol 2009;42:449–52.
6] Khouri EM, Greqq DE, McGranahan Jr GM. Regression and reappearance of coro-nary collaterals. Am J Physiol 1971;220:655–61.
7] Elsman P, van‘t Hof AW, de Boer MJ, Hoorntje JC, Suryapranata H, DambrinkJH, Zijlstra F, Zwolle Myocardial Infarction Study Group. Role of collateralcirculation in the acute phase pf ST-segment-elevation myocardial infarc-tion treated with primary coronary intervention. Eur Heart J 2004;25:854–8.