BioMed Central
Journal of Cardiovascular Magnetic Resonance
ss
Open AcceOral presentation12-lead ECG in a 1.5 Tesla MRI:
Separation of real ECG and MHD voltages with adaptive filtering for
gating and non-invasive cardiac outputZion Tsz Ho Tse*1, Charles L
Dumoulin2, Gari Clifford3, Michael Jerosch-Herold1, Daniel Kacher1,
Raymond Kwong4, William Gregory Stevenson4 and Ehud Jeruham
Schmidt1
Address: 1Radiology, Brigham and Women's Hospital, Boston, MA,
USA, 2University of Cincinnati College of Medicine, Cincinnati, OH,
USA, 3Health Sciences and Techology, Massachusetts Institute of
Technology, Boston, MA, USA and 4Cardiology, Brigham and Women's
Hospital, Boston, MA, USA
* Corresponding author
IntroductionThe Magneto-Hydro-Dynamic (MHD) effect arises
whenconductive blood flows in the MRI magnetic field (B0).MHD
generates a voltage which distorts the real electro-cardiogram
(ECGreal), especially during the S-T segmentwhere flow from the
left ventricle (LV) into the aorta con-tributes to a large MHD
voltage [1]. A dominant QRS andundistorted S-T segment are
important for MRI gating andphysiological monitoring for ischemia
during cardiacimaging/interventions [2].
PurposeWe hypothesized that adaptive filtering could
separatebetween MHD and ECGreal, and that the MHD signalcould
non-invasively estimate cardiac output.
MethodsMRI-compatible 12-lead ECGs were acquired with a
mod-ified ECG-recording system [3] from three healthy volun-teers
and one patient with idiopathic outflow tractPremature Ventricle
Contractions (PVCs) (Ejection Frac-tion 20-25%, LV wall thickening,
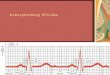
mitral regurgitation).Three sets of 20-sec breath-held ECGs (Fig.
1), were meas-ured in a 1.5 scanner with subjects placed (i)
outside thescanner with their head-in (ECG = ECGreal), (ii) at
iso-cen-
tre with their head-in (ECG = ECGreal+MHDhead-in), and(iii) at
iso-centre with their feet-in (ECG = ECGreal+MHD-
feet-in), which reverses B0 polarity (MHDfeet-in~-1 × MHD-
head-in). Data processing (Fig. 2) involved application of
anadaptive Least-Mean-Square filter to (ii) and (iii), whilst(i)
was used to train the filter to decouple the MHD signalfrom
ECGreal.
ResultsFig. 3(a-d) show processing of the patient's V6 ECGs
inpositions (ii) and (iii). MHD signals are effectively
from 13th Annual SCMR Scientific SessionsPhoenix, AZ, USA. 21-24
January 2010
Published: 21 January 2010
Journal of Cardiovascular Magnetic Resonance 2010, 12(Suppl
1):O95 doi:10.1186/1532-429X-12-S1-O95
Abstracts of the 13th Annual SCMR Scientific Sessions - 2010
Meeting abstracts - A single PDF containing all abstracts in
this Supplement is available here.
http://www.biomedcentral.com/content/files/pdf/1532-429X-11-S1-info
This abstract is available from:
http://jcmr-online.com/content/12/S1/O95
© 2010 Tse et al; licensee BioMed Central Ltd.
Unprocessed PVC patient ECGsFigure 1Unprocessed PVC patient
ECGs.
Page 1 of 3(page number not for citation purposes)
http://jcmr-online.com/content/12/S1/O95http://www.biomedcentral.com/http://www.biomedcentral.com/info/about/charter/
Journal of Cardiovascular Magnetic Resonance 2010, 12(Suppl
1):O95 http://jcmr-online.com/content/12/S1/O95
Publish with BioMed Central and every scientist can read your
work free of charge
"BioMed Central will be the most significant development for
disseminating the results of biomedical research in our
lifetime."
Sir Paul Nurse, Cancer Research UK
Your research papers will be:
available free of charge to the entire biomedical community
peer reviewed and published immediately upon acceptance
cited in PubMed and archived on PubMed Central
yours — you keep the copyright
Submit your manuscript
here:http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
ment preserved. The MHD signals, Fig. 3(e-f), are maxi-mal
during the S-T segment. Oscillating positive andnegative MHD
voltages during systole in each PVC cyclecan be explained by flow
eddies, consistent with thepatient's mitral regurgitation. Fig.
3(g-h) show the cardiacoutput, calculated from the systolic
time-integrated MHD.Cardiac output during PVC cycles is much
smaller thanduring normal beats. Fig. 3(i) indicates that the
PVCpatient's average cardiac output is 44-54% of the
healthyvolunteers', due to less effective PVC beats.
ConclusionThe filtering procedure separates the ECGreal and
MHDsignals in 12-lead ECGs acquired within the MRI. The QRScomplex
becomes dominant, as required for good MRIgating, while preserving
S-T segment fidelity for physio-logical monitoring during
imaging/interventions. MHDsignals allow for non-invasive monitoring
of beat-to-beatcardiac output.
References1. Gupta : IEEE Trans BioMed Eng 2008.2. Haberl : ECG
pocket, Borm Bruckmeier Publishing; 2006. 3. Dukkipati :
Circulation 2008.
Page 3 of 3(page number not for citation purposes)
http://www.biomedcentral.com/http://www.biomedcentral.com/info/publishing_adv.asphttp://www.biomedcentral.com/
IntroductionPurposeMethodsResultsConclusionReferences