Embed Size (px)
Citation preview
EDITORJEAN LEA SPITZ, MPH, RDMSCollege of Allied HealthUniversity of Oklahoma Health Sciences Ctr.PO Box 26901Oklahoma City, Oklahoma 73190
Contributing EditorsMARVEEN CRAIG, RDMS, FSDMSTucson, AZ
SANDY HAGEN–ANSERT, MS, RDMS, RDCS, FSDMSMt. Pleasant, SC
Editors EmeritusJULIA A. DROSE, BA, RDMS, RDCS, RVT, FSDMSDALE CYR, MBA, RDMSMIMI BERMAN-SANDLER, PHD, RDMS
Editorial BoardCatherine Carr-Hoefer, RT, RDMS, RDCS, RVT, FSDMSCorvallis, OR
Mark S. Cartier, BS, RDMS, RTNorth Conway, NH
Carolyn T. Coffin, MPH, RT, RDMS, RVT, RDCS, FSDMSDenver, CO
Harris L. Cohen, MDBaltimore, MD
Peter L. Cooperberg, MD, FRCPCVancouver, BC
Joshua A. Copel, MDNew Haven, CT
Reva Curry, PHD, RDMS, RT(R), FSDMSSicklerville, NJ
Marie DeLange, BS, RT, RDMS, RDCS, FSDMSRedlands, CA
Rich Dempsey, RDMS, RVTRiverton, WY
Janice D. Dolk, MA, RT(R), RDMSOwings Mills, MD
Terry DuBose, MS, RDMS, FSDMSLittle Rock, AR
Stephanie Ellingson, BA, RDMS, RVT, RDCS, RT(R)Iowa City, IA
Steven Goldstein, MDNew York, NY
Joyce Grube, MS, RDMSKettering, OH
Rebecca J. Hall, PHD, RDMS, FSDMSAlbuquerque, NM
Jay Harolds, MDOklahoma City, OK
Lois Hart, RDMSQuincy, MA
W. R. Hedrick, PHDCanton, OH
Diane M. Kawamura, PHD, RDMS, RT(R), FSDMS, FAIUMOgden, UT
Harry J. Khamis, MS, PHDDayton, OH
Lori A. Koziol, RDMS, FSDMSHamilton, ON
E. A. Lyons, MD, FRCP(C), FACRWinnipeg, MAN
Daniel A. Merton, BS, RDMSPhiladelphia, PA
William O’Brien, Jr., PHDUrbana, IL
Wayne H. Persutte, BS, RDMS, FAIUM, FSDMSDenver, CO
John C. Pope, BS, PAC, RDMS, RDCS, RVTAugusta, GA
Dana Salim, BS, RDCSNorman, OK
William Schroedter, BS, RVTVenice, FL
Terry M. Silver, MD, FACRAnn Arbor, MI
Terrence L. Tye, MS, RDMS, RDCSPalo Alto, CA
Alan Waggoner, MHS, RDCSSt. Louis, MO
Larry Waldroup, BS, RDMSPhiladelphia, PA
Paula Woletz, MPH, RDMS, RDCSLaurel, MD
James A. Zagzebski, PHDMadison, WI
SDMS Board of Directors
PresidentKEVIN EVANS, MS, RT(R)(M), RDMS, FSDMS
President-ElectLAURINDA S. ANDRIST, BS, RDMS, RDCS, FSDMS
Vice PresidentREBECCA HALL, PHD, RDMS, FSDMS
SecretaryLORI KOZIOL, RDMS, FSDMS
TreasurerCAROLYN COFFIN, MPH, RT, RDMS, RVT, RDCS, FSDMS
Past PresidentSTEPHEN M. MCLAUGHLIN, BS, RT, RDMS, FSDMS
Regional Directors
Region 1CATHERINE CARR-HOEFER, RT, RDMS, RDCS, RVT, FSDMSRegion 2CINDY RAPP, BS, RDMS, RDCS, FSDMS, FAIUMRegion 3TERRY J. DUBOSE, MS, RDMS, FSDMSRegion 4LYNNE SCHREIBER, MS, RT(R), RDMSRegion 5KERRY WEINBERG, MPA, RT, RDMS, RDCSRegion 6ANNE CONNER-DAY, BS, RT(R), RDMSRegion 7LORRIE SCHERER, RDMS, RDCS
Ex Officio Commercial RepresentativeMARY RENDER, RDMS, RVT
Executive DirectorDONALD F. HAYDON, CAE
Advertising Account ManagerDIANE [email protected](215) 675-9133 ext. 105
The statements and opinions expressed in correspondence,editorials, articles, and symposia are those of the authors anddo not necessarily reflect positions of the Journal of DiagnosticMedical Sonography or the Society of Diagnostic MedicalSonography. Acceptance of advertising does not constituteendorsement. Neither the Journal of Diagnostic MedicalSonography nor the Society of Diagnostic Medical Sonographywarrants or guarantees any product or service advertised inthis journal.
Journal of Diagnostic Medical SonographyOfficial Journal of The Society of Diagnostic Medical Sonography
November/December 2001 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY VOL. 17, NO. 6
November/December 2001 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY VOL. 17, NO. 6
EDITORIAL
Standards for Assurance of Minimum Entry-LevelCompetence for the Diagnostic UltrasoundProfessional 307
INTRODUCTION BY LAURINDA S. ANDRIST, BS, RDMS, RDCSWILLIAM SCHROEDTER, BS, RVT
ARTICLES
Sonographers and Occupational Overuse Syndrome:Cause, Effect, and Solutions 312
CATHY JAKES, BS
SDMS-JDMS CME Test 321
Ultrasound of the Carpal Tunnel and Median Nerve: AReproducibility Study 323
MAUREEN WILKINSON, DCR(R), DMU, AMSKAREN GRIMMER, PHDNICOLA MASSY-WESTROPP, BAPPSC(OT)
SDMS-JDMS CME Test 329
The Use of Sonography in the Detection of Bony andCalcific Disorders of the Shoulder 331
MARK A. STIELER, MS
CASE STUDIES
Sonographic Evaluation of IntraocularCysticercosis 339
R. SIDHU, MDR. GUPTA, MDSUMEET MALHOTRA, MS
Sonographic Appearance of Klippel-Trénaunay-WeberSyndrome Diagnosed at 18 Weeks Gestation 342
DEBORAH A. HUBACZ, BA, RDMS
Carotid Anomaly in a Patient With Holt-OramSyndrome 347
LES B. FORGOSH, MD, FACC, FACPRHONDA POORE, RDMS, RDCS
Ultrasound Evaluation and Clinical Managementof Persistent Gestational Sac in a Cervical EctopicPregnancy 350
VICKI L. MAUK, RDMSGARY L. FORCIER, MD
Hypochondrogenesis: A Rare Lethal SkeletalDysplasia 354
JEAN M. PANTALEO, RT, RDMSMARVEEN CRAIG, RDMSDONALD M. EHMAN, MD
Sonographic Findings in Fetal Alpha ThalassemiaMajor 358
MARIANA KOZIROVSKY, BS, RDMS, RDCSJULIA SHVETSOVA, BS, RDMS, RVT
DIAGNOSTIC CHALLENGE 362
BRIANNA M. WHITWORTH
FOCUSING ON THE ISSUES
A Gathering of Angels 363MARVEEN CRAIG, RDMS
LETTER TO THE EDITOR 368
Subject Index 369
Author Index 372
Information for Authors 374
The Journal of Diagnostic Medical Sonography (ISSN 8756-4793) is published bimonthly for the Society of Diagnostic Medical Sonography by Sage SciencePress, an imprint of Sage Publications, 2455 Teller Road, Thousand Oaks, CA 91320; telephone (800) 818-SAGE (7243) and (805) 499-9774; fax/order line (805)499-0871; e-mail [email protected], http://www.sagepub.com. Printed in the U.S.A. Periodicals postage paid at Thousand Oaks, CA and additional mailingoffices. Outside U.S. subscription rates include shipping via air-speeded delivery. U.S.: individual $111 per year, $35 single issue; institution $270 per year, $56single issue. All other countries: individual $161 per year, $35 single issue; institution $303 per year, $56 single issue. Annual subscription rates for institutionsand individuals are based on the current frequency. Prices quoted are in U.S. dollars and are subject to change without notice. Canadian subscribers add 7%GST (and HST as appropriate). Disclaimer: The authors, editors, and publisher will not accept any legal responsibility for any errors or omissions that may bemade in this publication. The publisher makes no warranty, expressed or implied, with respect to the material contained herein.
Copyright 2001 by the Society of Diagnostic Medical Sonography.Send member changes of address to the SDMS, 12770 Colt Road, Suite 708, Dallas, TX 75251.The Journal of Diagnostic Medical Sonography is indexed in the CINAHL database, CUMULATIVE INDEX TO NURSING AND ALLIED HEALTH LITERATURE,
and EMBASE/Excerpta Medica.POSTMASTER: Send address changes to Journal of Diagnostic Medical Sonography, c/o Sage Science Press, 2455 Teller Road, Thousand Oaks, CA 91320.
Contents
JDMS 17:307-311 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
EDITORIAL / Andrist, Schroedter
EDITORIAL
Standards forAssurance ofMinimum Entry-Level Competencefor the DiagnosticUltrasoundProfessional
The document presented below is the result of a 14-month collaborative effort between the Society ofDiagnostic Medical Sonography (SDMS) and theSociety of Vascular Technology (SVT). During thedrafting of this document, multiple persons wereinvolved in the evolution of these standards includinglegal council, educators, clinical sonographers of allspecialties, and vascular technologists. The purpose ofthe document is to establish the minimum entry-leveleducational and clinical standards to enter the field ofdiagnostic ultrasound for all subspecialties. Thisdocument will be used in tandem with the Scope ofPractice for the Diagnostic Ultrasound Professional toreinforce the parameters of our profession witheducational institutions, establishments of clinicalpractice, and legislative and regulatory agencies. It isanticipated this document will be periodically revisedas our profession continues to change. Theendorsement from other ultrasound organizations willbe sought, as was done with the Scope of Practice.
We wish to acknowledge the presidents of theultrasound professional associations under whoseterms of office and leadership direction this documentwas created: Pat Marques, RN, RVT (Society ofVascular Technology) and Stephen M. McLaughlin,BS, RT, RDMS (Society of Diagnostic MedicalSonography). Special thanks go to Bill Sarraille, JD;Anne Jones, RN, RVT, RDMS; Margaret Nix, RN,BSN, RVT; Frank West, BSN, RVT, CVN; JeanetteBurlbaw, BS, RDMS; Cara Case, RT, RDMS, RDCS;Beth Anderhub, MEd, RDMS; the SDMS Board ofDirectors; and the SVT Board of Directors.
Laurinda S. Andrist, BS, RDMS, RDCS
William Schroedter, BS, RVT
PREAMBLE
The purpose of this document is to define thequalifications necessary to become certified andpractice as a Diagnostic Ultrasound Professional,which includes Diagnostic Cardiac Sonographers,
JDMS 17:307-311 November/December 2001 307

Diagnostic Medical Sonographers, and VascularTechnologists. It is expected that this document willchange as the needs of the profession evolve in thefuture. The minimum standards established in thisdocument are to be used in conjunction with the Scopeof Practice for the Diagnostic Ultrasound Professional1
and represent the entry-level threshold for persons toenter the field of diagnostic ultrasound. The Scope ofPractice of the Diagnostic Ultrasound Professionalincludes those procedures, acts, and processespermitted by law for which the individual has receivededucation and clinical experience and in which he orshe has demonstrated competency. The field ofdiagnostic medical ultrasound includes the specialtiesof Vascular Technology, which encompasses vascularsonology and physiologic testing; Diagnostic CardiacSonology, with subspecialties in adult echocardiog-raphy and pediatric echocardiography; and DiagnosticMedical Sonology, with subspecialties in breastsonology, general medicine sonology, neurosonology,obstetrics and gynecology, and ophthalmology.
Standards, as described in the Scope of Practice, aredesigned to reflect behavior and performance levelsexpected in clinical practice. Clinical practicestandards and personnel certification are paramount toensure quality ultrasound examinations and maximumpatient protection.
It is clear that a wide range of both academic andclinical training is prerequisite in order for individualsto meet these standards. The increasing sophisticationof ultrasound technologies coupled with the currentenvironment and the level of practice required of theDiagnostic Ultrasound Professional renders on-the-jobtraining inadequate as an educational pathway. Whileno mechanism exists to unquestionably assuretechnical competence, national board certification isthe standard of practice in ultrasound. The purpose ofcertification is to provide assurance to the public thatpersons practicing diagnostic ultrasound have com-pleted specified didactic course work, clinicalexperience, and possess the knowledge, skills, andexperience to deliver high-quality patient care.
DESCRIPTION OF THE PROFESSION
Diagnostic Ultrasound Professionals use a variedintellect that requires advanced education specific tothe multiple specialties of diagnostic ultrasound.Individuals exercise independent judgment in thepractice of diagnostic ultrasound, making the outcome
of the examination unique to each patient and not aroutine process.
According to the Scope of Practice, DiagnosticUltrasound Professionals
• perform patient assessments;• acquire and analyze data obtained using
ultrasound and related diagnostic technologies;• provide a summary of findings to the physician to
aid in patient diagnosis and management;• use independent judgment and systematic
problem-solving methods to produce high-quality diagnostic information and optimizepatient care.
Competency in performing these critical patient carefunctions requires advanced education specific to themultiple specialties of diagnostic ultrasound.
Minimum Standards for the Profession
I. DIAGNOSTIC ULTRASOUNDMINIMUM ACADEMIC STANDARDS2
These represent the minimum educationalrequirements identified as necessary for an individualto enter the Diagnostic Ultrasound Profession. Theeducational structure for the Diagnostic UltrasoundProfessional has been evolving over the past 2decades. It is anticipated that all persons will enter thefield with a minimum of an associate degree in ultra-sound, other allied health or life sciences and have, at aminimum, the clinical requirements outlined inSection II of this document by 2006; a bachelor ofscience degree in allied health or life sciences andhave, at a minimum, the clinical requirements outlinedin Section II of this document by 2008; and a bachelorof science degree in diagnostic ultrasound or one of itsspecialties by 2012.
Standard: Educational Program Accreditation
• All established ultrasound educational programsin the United States must be accredited by theCommission on Accreditation of Allied HealthEducation Programs (CAAHEP)3,4 by 2006.
• All newly established ultrasound educationalprograms in the United States must be accreditedby the CAAHEP within 5 years of initiation.
308 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
EDITORIAL / Andrist, Schroedter 309
• Standards for the accreditation of an educationalprogram for the Diagnostic UltrasoundProfessional should be in conjunction withSection I (Requirements for Accreditation) andIII (Maintaining and Administering Accredi-tation) of the CAAHEP Standards andGuidelines for an Accredited EducationalProgram.5,6
• Multispecialty programs must ensure that allrequisite standards for each specialty are met. Inthe case of diverse specialties, this may requirean additional year of didactic training.
Standard: Prerequisite Education perCAAHEP Standards Section IC1(Admission Policies and Procedures)
Standard: Curriculum per CAAHEP StandardsSection IIB
The entry-level curriculum for diagnosticultrasound provides the foundation of knowledge thatwill be used before a student enters into clinicaltraining.
Standard: Required Competencies Common toEach Learning Concentration (Section IIC).
• Curriculum should be reviewed to ensurecurrency of content every 2 years.
• Competencies should be outcomes based.• Code of Ethics as created by the Sonography
Coalition should be adopted.• Code of Professional Conduct should be
established.• Professional society participation should be
promoted.
A. Cardiac Sonology Learning Concentration5,6
• Competencies specific to the cardiac sonologylearning concentration (Section IIE)
B. Vascular Technology Learning Concentration5,7
Competencies specific to the vascular technologylearning concentration (Section IIF)
C. General Medicine SonologyLearning Concentration5
• Competencies specific to the general medicinelearning concentration (Sections IID1-3 and 8)
D. Obstetrics and GynecologyLearning Concentration5
• Competencies specific to obstetrics andgynecology learning concentration (SectionsIID4-8)
E. Neurosonology Learning Concentration8
F. Breast Sonology Learning Concentration8
G. Ophthalmology Learning Concentration8
II. DIAGNOSTIC ULTRASOUNDCLINICAL EDUCATION STANDARDS
Clinical education should be an adjunct to didacticeducation. The cognitive and psychomotor skillsnecessary to competently perform any ultrasoundspecialty require extensive clinical experience. Asignificant component of any ultrasound educationalprogram is clinical practice. Exposure to a highvolume and variance of sonographic procedures isnecessary, which permits exposure to a variety ofpathologic conditions. Clinical education should bespecific for each specialty practiced. Clinicaleducation must be accomplished under the directsupervision of a certified Diagnostic MedicalSonographer, Diagnostic Cardiac Sonographer, orVascular Technologist experienced in the specialty ofclinical focus. The cardiac concentration requires aminimum of 800 procedures annually in the lab ofclinical internship. The vascular concentrationrequires a minimum of 1000 procedures annually inthe lab of clinical internship, including bothsonographic and indirect physiologic procedures.Multispecialty programs require a minimum of 1500clinical procedures annually in the lab of clinicalinternship.9 This allows for overlap of skilldevelopment in clinical education that occurs inthe first 4 to 6 months for any single learningconcentration.
III. DIAGNOSTIC ULTRASOUND MINIMUMCERTIFICATION STANDARDS
Definition of Certification: Successful completion of anational objective written certification examinationthat has been independently validated and meets thestandards of the National Commission for CertifyingAgencies (see Appendix, Part III)
Standard: National Board Certification IsMandatory to Ensure
• Public protection• Quality of care
The purpose of certification is to provide assurance tothe public that the Diagnostic Ultrasound Professionalhas completed specified didactic courses, and clinicalexperience, and possesses the knowledge, skills, andexperience to deliver high-quality patient care.Additionally, the provider is able to appropriatelyevaluate normal and abnormal anatomy withultrasound images or related technologies, assesspatient clinical history, optimize establishedexamination procedures, and communicate findingswith physicians.
Competence in one specialty can not, and shouldnot, be construed as competence in any other.Certification in each area of clinical work is required.
Standard: PostcertificationContinuing Education
Diagnostic Ultrasound Professionals must adhere tothe specific continuing education and/or recertificationguidelines as mandated by the organization fromwhich the certification is obtained. Due to rapidadvancement in ultrasound practice, the need forcontinually staying abreast of evolving standards,techniques, and technology is imperative. Withoutcontinuing education and exposure to knowledgebeyond the undergraduate experience, no professionalcan stay current in information and skills necessary toprovide high-quality care to patients. Ongoingcertification is based on a standard that includessuccessful attainment of continuing professionaleducation and experience with new technologies andmodalities. In order to remain current with thedevelopment of the field, persons who have passedtheir certification examinations for ultrasound mustdemonstrate completion of at least 30 hours ofqualified CME every 3 years and a minimum of 15hours in each specialty in which they are certified.
Standard: Types of Continuing Education
Standards of practice will continue to evolve astechnology advances and new procedures and tech-
niques are developed. Ongoing education of currentpractice is necessary to remain abreast of thesechanges. Participation in research, scientificpublication, and completion of advanced degrees mayalso be a means of staying current with the professionand/or contributing to continuing professionaldevelopment.
Standard: Institutional Orientation
Current practice dictates persons practicing diag-nostic medical ultrasound assume significantresponsibility for obtaining a complete and accurateexamination, pertinent to each patient’s condition.Institutional and laboratory-specific protocols and pro-cedures cannot be taught prior to being employed at aninstitution. Every employer of ultrasound profes-sionals must provide comprehensive institutionalorientation about its philosophy, standards andmethods of practice, the range of patients to beencountered, and all protocols and procedures. Thelength of this orientation will vary depending on manyfactors, including the size of the institution, but wouldgenerally be a minimum of 6 months.
Standard: Continuing Professional Development
Participation in research, scientific publication, andcompletion of advanced degrees in order to staycurrent with the profession is strongly encouraged andsupported by the field. However, clinically relevantcontinuing education is still mandatory.
Appendix
I. Commission on Accreditation of Allied HealthEducation Programs (CAAHEP), Standards andGuidelines for an Accredited Education Programfor the Diagnostic Medical Sonographer,www.caahep.org/standards/dms-st.htm
II. CAAHEP, Standards and Guidelines for anAccredited Program for the Cardiovascular Tech-nologist, www.caahep.org/standards/cvt-st.htm
III. National Organization for Competency AssuranceStandards for National Commission for CertifyingAgencies Accreditation, www.noca.orgs
310 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6

EDITORIAL / Andrist, Schroedter 311
Notes
1. “Scope of Practice for the Diagnostic UltrasoundProfessional” (Journal of Diagnostic Medical Sonography2000;16:206–211, Journal of Vascular Technology2000;24:151–156).
2. The minimum educational and clinical standards within thisdocument are supported by the precedent set in the U.S.district court for the eastern district of Pennsylvania (CivilAction No. 98-CV-4076).
3. Commission on Accreditation of Allied Health EducationPrograms (CAAHEP), Standards and Guidelines for anAccredited Education Program for the Diagnostic MedicalSonographer, www.caahep.org/standards/dms-st.htm.
4. Commission on Accreditation of Allied Health EducationPrograms (CAAHEP), Standards and Guidelines for anAccredited Program for the Cardiovascular Technologist,www.caahep.org/standards/cvt-st.htm.
5. Commission on Accreditation of Allied Health EducationPrograms (CAAHEP), Standards and Guidelines for an
Accredited Education Program for the Diagnostic MedicalSonographer, www.caahep.org/standards/dms-st.htm.
6. Commission on Accreditation of Allied Health EducationPrograms (CAAHEP), Standards and Guidelines for anAccredited Program for the Cardiovascular Technologist,www.caahep.org/standards/cvt-st.htm.
7. SVT Guidelines for Educational Programs in VascularTechnology.
8. Because the standards for the learning concentrations relatedto neurosonology, breast sonology, and ophthalmology havenot been created by the CAAHEP, the SDMS and SVT willjointly approach the CAAHEP to request creation of thesestandards. The SDMS and SVT seek endorsement from theAmerican Society of Ophthalmology.
9. Commission on Accreditation of Allied Health EducationPrograms (CAAHEP), Standards and Guidelines for anAccredited Education Program for the Diagnostic MedicalSonographer, www.caahep.org/standards/dms-st.htm.

312 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
JDMS 17:312-320 November/December 2001
JDMS 17:312-320 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
OCCUPATIONAL OVERUSE SYNDROME / Jakes
Sonographers andOccupationalOveruseSyndrome:Cause, Effect,and Solutions
CATHY JAKES, BS
Due to remarkable advances in technology,sonographers today are working more efficiently,serving considerably more patients per day. Onewould assume this to be a benefit, when in fact anew problem has surfaced directly related to theseachievements. Ultrasound exams require a peculiartype of muscular effort on the part of thesonographer. Tiny muscle tears that are the result ofrepetitive manipulations of the transducer, withoutadequate rest between exams, progress to moreextensive muscular damage. The muscular damagecan lead to career-ending injury. The purpose of thisarticle is to examine the causes of overuse injuriesbrought on by repetitive muscle stresses associatedwith the performance of ultrasound exams and todiscuss the changes necessary to combat thisergonomic crisis. Change is difficult, but with thecombined efforts of equipment designers,employers, and sonographers, change is possibleand an auspicious future can be envisioned.
Key words: ultrasound, sonographer, overuse,musculoskeletal, injury, ergonomics
The technology of ultrasound is improvingexponentially. The advantages of real time plusimproved imaging capabilities of ultrasound havemade ultrasound the diagnostic tool of choice fordetecting a variety of medical conditions. It is anexciting field to be in, and one with growingopportunity. A student of ultrasound has much to lookforward to.
Unfortunately, there is a down side to theseadvances. The improved technology not only provideshigher quality images but also faster processing ofthose images. This means more time spent scanningpatients and less time in between patients. Althoughseemingly advantageous, this is ultimately detrimentalto both the employer and the sonographer. Morescanning time means more time in damaging activity,and less time between patients means less time fordamaged muscle fibers to repair.1,2 Eventually, thesonographer misses work due to work-related injury,
312 JDMS 17:312-320 November/December 2001
From the Diagnostic Ultrasound Program, Bellevue CommunityCollege, Bellevue, Washington.
Reprint requests: Cathy Jakes, 3736 SE Henry Street, Portland, OR97202. E-mail: [email protected].
OCCUPATIONAL OVERUSE SYNDROME / Jakes 313
which has a dramatic impact on the sonographer, theemployer, and the quality of care available to patients.
Eighty percent of sonographers are working in pain;40% label their pain as severe, and 20% have lost theircareers due to this insidious process. Unfortunately,the incidence of overuse injuries in the profession isincreasing.1,3,4 The purpose of this article is to examinethe causes and physiological processes of overuseinjuries brought on by repetitive muscle stressesassociated with the performance of ultrasound exams,and to discuss the changes necessary to combat thisergonomic crisis. Solutions and preventative measureshave been offered, but it will take the combinedcooperation of equipment manufacturers, employers,and sonographers to implement those solutions.
Causes of OveruseInjury in Sonographers
There is a tapestry of factors (involving both thesonographer and the workplace ergonomics) that, incombination and over time, lead to musculoskeletalinjury. Numerous researchers2,3,5-7 agree on thefollowing causes:
1. Minute movements of the transducer (the instrumentheld against the patient’s skin during the exam) andgripping the transducer tightly cause insult to thesmall muscle fibers of the fingers, hand, andforearm.
2. Twisting and bending the wrist while applyingpressure against the patient’s skin exacerbates thestrain in the wrist.
3. Holding the elbow away from the body (shoulderabduction) while pressing against the skin for asustained period of time compromises the musclesof the shoulder joint, neck, and back. According toGregory, “The arm should not be abducted morethan 20 degrees and ideally no more than 8 degrees.Sonographers nearly always exceed this angle ofabduction.”3(p3)
4. Performing these muscular activities in acompromised posture, such as leaning over thepatient and twisting the torso and neck to see themonitor, leads to back and neck strain.
5. Poor workplace ergonomics (height of systemkeyboard, height and direction of monitor,sonographer’s chair height, exam table height andwidth, transducer shape and size, and improper roomlighting) contribute significantly to forcingsonographers into compromising positions whileperforming exams.
6. Increased number of exams and less time betweenexams leads to the slow progressive process ofmuscle strain referred to as overuse injury.
7. Height, age, and gender of the sonographer as theyrelate to shoulder abduction and muscle strength,respectively.
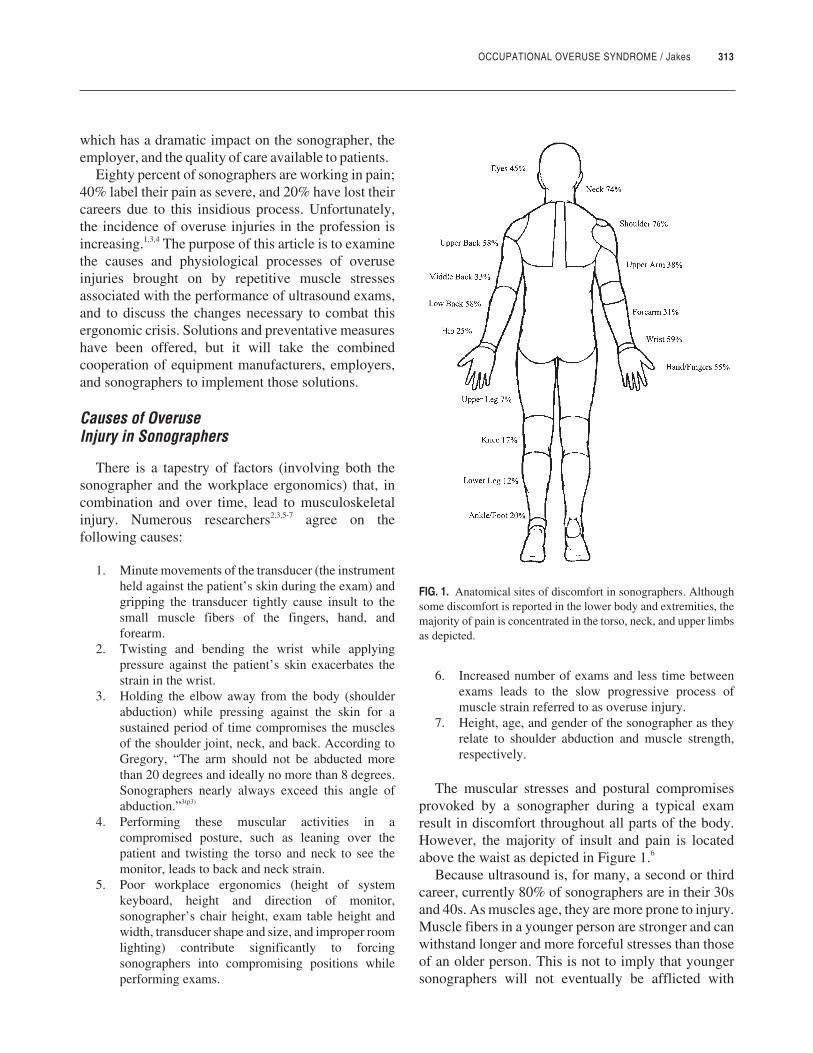
The muscular stresses and postural compromisesprovoked by a sonographer during a typical examresult in discomfort throughout all parts of the body.However, the majority of insult and pain is locatedabove the waist as depicted in Figure 1.6
Because ultrasound is, for many, a second or thirdcareer, currently 80% of sonographers are in their 30sand 40s. As muscles age, they are more prone to injury.Muscle fibers in a younger person are stronger and canwithstand longer and more forceful stresses than thoseof an older person. This is not to imply that youngersonographers will not eventually be afflicted with
FIG. 1. Anatomical sites of discomfort in sonographers. Althoughsome discomfort is reported in the lower body and extremities, themajority of pain is concentrated in the torso, neck, and upper limbsas depicted.

occupational overuse injuries, just that it may take alittle longer. The benefits of strength training toincrease muscle strength will be discussed later.
Reflecting on why women tend to experience moreinjuries than men, Vanderpool et al explained, “Astronger person may be able to hold the ultrasoundtransducer against the patient with less perceivablehand grip pressure than a weaker person.”2(p609)
Another factor contributing to the problem ofoveruse injury in the ultrasound profession is thetypical nature, or personality, of most sonographers. Ithas been my observation as a student of diagnosticultrasound that sonographers are more concerned withserving the patient than they are with their own well-being. I have heard sonographers refer to work-relatedinjury as just part of the job, something you endurebecause you love your work.
But testimonies from those who have lost their jobsdue to work-related injury exposes the destructivenature of such devotion. The testimony of Susan L.Murphey, who worked 18 years as a sonographer,reveals some of the brutal realities of the currentprofession:
The practice of medicine has changed dramatically,too. The focus has shifted to issues concerningreimbursement, increased productivity and minimiz-ing expenses. . . . Many recommendations were madeto improve the ergonomic situation. . . . Instead,managers were pressured to increase the number ofscanned. . . . As a result, our patient volumes went up,and our rest breaks between exams went down.Sonographers were now increasing the time spent inpositions of postural dysfunction with little or no restbreak available throughout the day.1(pp6-7)
Susan shared that these work-related injuries becameso bad that she was unable to perform simple dailytasks such as laundry, cooking, and cleaning. The fearof losing her job was compounded with the fear oflosing her ability to care for her family.
Another woman who lost her career to overusework-related injury had a testimony similar to Susan’s.This woman, who asked to remain anonymous, feltcompelled to share her experience for the purpose ofhelping other sonographers avoid the same fate: “Iloved being a sonographer; I am so very sad to havelost something that I loved so deeply. . . . My physicianhas told me that these conditions are the permanentresult of attempting to compensate [for] the pain,
rotator cuff tear and the impingement that Iexperienced.” Similar to Murphey’s testimony, shereveals, “We often scanned 10 to 12 hours a daywithout breaks or lunch.” And, like Susan, this womangrieved not only the loss of her job but also the loss ofvalued family activities: “Even the gentle tug of mygrandchildren’s hand was very painful.”1(pp8-10)
Physiology and Symptoms: TheProgressive Nature of Overuse Injury
The type of injury that sonographers experiencedoes not happen after one day or one week of work. Itis the result of the accumulation of small, repetitivestresses on muscle fibers over time. When repetitivelow-level muscle strain is sustained beyond a muscle’scapability, damage occurs. The initial damage may gounnoticed, producing no symptoms. These smallmuscle fiber tears will heal if given adequate rest time.But small muscle fiber tears, in the absence ofadequate rest time, progress to larger groups of fibersbeing injured. These larger insults to the musclerequire longer periods of rest to heal. If not given therequired rest time, more serious injuries are incurred.3
Another physiologic response to repetitive motionand cumulative trauma is obstruction of venous return,swelling, and compression and demyelination of thenerves supplying the muscles.3
Repetitive strain injury will be felt by thesonographer in a variety of ways. Recall that theoriginal insult will most likely not present noticeablesymptoms. But, as time passes, the followingsymptoms are felt: tingling, numbness, shootingsensations, weakness, itching and burning sensations,clumsiness of fingers, swelling, and changes in musclebulk. Pain is felt in the neck, back, arms, hands, andfingers, as well as shoulder, elbow, and wrist joints.Reduced mobility, freezing of joints, and, eventually,total loss of function are the end stages of thisprogression.2,3
The fast pace and multiple exams performed dailyby the sonographer, plus the “add ons” being squeezedinto an already heavy schedule, is a recipe for disaster.1
If this pace is allowed to continue, the absolute result issevere debilitating pain that will incapacitate the mostvalued players on the sonographic team.
The industry is losing the most qualifiedsonographers to this occupational overuse syndrome.The new sonographers miss diseased processes that
314 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6

OCCUPATIONAL OVERUSE SYNDROME / Jakes 315
the experienced eye can detect. Losing valuedsonographers is a price the health care industry shouldnot be willing to pay. Solutions have been offered.Unfortunately, only some are aggressively imple-menting those solutions.
Solutions: It Is Up to the Equipment Designers,Employers, and Sonographers to Work Together
Many are speaking out passionately for the need forchanges to occur to stop this ergonomic crisis. Thegood news is that solutions do exist. The success ofthose solutions requires the cooperation and combinedefforts of the equipment designers, the employers, andthe sonographers—each doing his or her part inimplementing the proposed remedies. Joan P. Bakersupports the projected solutions, stating that “all this isdoable, and is not too expensive. In fact it is cheapwhen compared to the cost of claims and injuries indollars as well as emotional trauma from loss ofcareers.”1(p5)
RESPONSIBILITIES OF THE EQUIPMENT DESIGNERS
Addressing the equipment designers, Baker pro-posed that “the technology and know-how exists tomake ultrasound equipment ‘sonographer friendly.’”1(p4)
Transducer design has been tagged as a majorcontributing factor to hand-wrist strains.6 The newer,smaller transducers provide improved imaging butrequire additional finger and hand strength to grip andapply the necessary forces. Proposed changes intransducer design include incorporating a smallfaceplate onto a large transducer or “developing atransducer that has a handle portion ‘detached’ fromthe ‘functioning’ portion, as is the case with mosttools.”5(p6) Additionally, thinner, lighter-weight trans-ducer cords would substantially alleviate strain andtorque associated with transducer use.
Another suggestion is to design adjustable chairs,keyboards, and monitors so that the sonographer canmanipulate their heights to appropriate levels.Additionally, “Ultrasound equipment should be fittedwith a high resolution screen that has a high refreshrate (85 Hertz or higher), a non-interlaced monitor andan easily adjustable brightness control” to reduce eyestrain.3
But the best that equipment designers have to offercannot help the vulnerable sonographer unless theemployer is willing to purchase the equipment.
RESPONSIBILITIES OF THE EMPLOYER
It is the employer’s responsibility to provide a safework environment for the sonographer and to supplyadequate rest periods to insure that muscle recoverytime matches muscle trauma. Jonathan Batchelor ofAuntMinnie.com shares statements from Joan Bakerconcerning the cost effectiveness of purchasingergonomically sound equipment: “An ultrasoundmachine that lies idle for one week due to sonographerinjury looses an estimated $10,000 (U.S.) in charge-able revenue, and 4 weeks of chargeable revenue lossis equivalent to the average annual salary of asonographer”.8 Baker continues to inculcate that thecost of support cushions is no more than the cost of asingle exam and that an ergonomic exam table is paidfor in two to three typical work days8. Anothersuggestion is to provide a separate viewing monitor forthe patient. This addition would alleviate the neckstrain associated with sharing the monitor with thepatient. 8
Lastly, it is recommended that employers have theirsite evaluated by ergonomic professionals followed bymaking necessary adjustments, and provide educationto their staff about safe postures and work habits.8
RESPONSIBILITIES OF THE SONOGRAPHER
Indeed, it has been noted that most of the power toreduce the incidence of repetitive strain to workingsonographers seems to lie in equipment design andworkplace setups.5,9 But does this mean that thesonographer is powerless to do anything to reduce theincidence of his or her own injury? There are in factmany things the sonographer can do, both on and offthe job, to decrease the likelihood of overuse injury.Recall, the culprits are poor posture, shoulderabduction, repetitive movements, gripping thetransducer tightly for long periods of time, andapplying static forces with the transducer against thepatient’s body. Sonographers need to focus on theseproblems and change their habits. A new sonographerneeds to anticipate how to avoid these injury traps byestablishing good habits to begin with.
On the job, sonographers should do the following3,6:
1. Seek employment at a facility that has height-adjustable chairs, exam beds, keyboards, andmonitors (with a separate monitor for patientviewing). Additionally, the chair should rotate freelyand offer easy access to a footrest. Ideally, there are
separate exam rooms for alternating between right-and left-handed scanning. Also, support cushions orpads for arm and elbow should be available.
2. Seek employment at a facility that does notoverwork its sonographers but allows time forminibreaks and regular breaks to accommodatemuscle recovery.
3. Maintain an upright posture and avoid leaning overthe patient as much as possible. Ask patients to moveto the edge of the bed so they are closer to you rightfrom the start. Throughout the exam, you may askthem to change positions as needed to scan variousparts of the body. When reaching is unavoidable, usea support cushion or a specially designed saddle-type pad to rest the elbow on.
4. Keep updated on new, ergonomically designedequipment and ask employers to provide it if they donot already. Suspended slings for elbow support arecurrently being developed.5
5. Vary your posture so that different muscles are usedthroughout the day. This could involve standing forsome exams and sitting for others. Be sure to adjustthe exam bed, keyboard, and monitor accordingly.
6. The keyboard should ideally be at a level that keepsthe elbow at a 90° angle and allows the upper arm tohang freely near your side. Monitor viewing heightshould be slightly lower than looking straight ahead.
7. Alternate between right- and left-handed scanning.This is most easily done if there are separate roomsset up for it. The amount of time spent learning toscan with the untrained hand is well worth reducingmuscle strain by one half.
8. Try to do a variety of exams throughout the day sothat the muscles are stressed in different ways. Thiswill need to be discussed with the scheduling staff.
9. Keep the elbow as close to the body as possible toreduce shoulder strain caused from abduction. Thismay require adjusting chair and bed height.
10. Put feet on a footrest to increase stability. Anunbalanced posture puts strain on support musclesover time.
11. Lighten your grip on the transducer and periodicallyrelease grip to allow muscles short rest periodsthroughout exam. Wear gloves with a specializedtexture that assists gripping the transducer.
12. Reduce the amount of time in sustained downwardforces against the patient’s skin. Only press as longas is necessary to get the image, and then release.
13. Keep wrist and neck in a straight position. (Pretendyou have a cast on your wrist and you cannot bendit.)
14. Take minibreaks during the exam to stretch and restmuscles. Complete rest, lasting as little as 2 to 3seconds, can be of tremendous benefit.6 Ideally, the
rest time should at least match the exertion time. Asexplained by Habes and Baron, “If a sonographerpushes down on the abdomen for a period of 15seconds to obtain a necessary fetal view, he/sheshould release the scan head and recover for 15seconds before proceeding with the examination.For exertion times lasting 1 minute, recovery timesof 100 seconds are required.”5(p6) Also, stretching theneck, upper back, lower back, chest, shoulder, arm,and wrist muscles during minibreaks is effective.Periodically looking away from the monitor willreduce eye strain.
15. Be aware of how your muscles are feeling. Do notignore early signs of overuse strain. Recall, minutemuscle tears will heal with small rest breaks.6
16. As a staff, work together to reduce overuse injury.Brainstorm together and share creative ideas forreducing occupational overuse strain.
17. As a group, or individually, learn as much as you canabout workplace ergonomics by attending seminars,watching educational video tapes, seeking Internetsources (www.soundergonomics.com), and so on.The more you understand how the muscles arestressed in various positions, the more likely youwill discover creative ways to avoid self-injury.
18. Support each other in reporting injury as soon as it isincurred, and do not delay getting immediate helpwith rehabilitation.
Off the job, sonographers should do the following:
1. Eat a healthy diet including lots of fruits andvegetables.
2. Increase muscle strength and improve overallfitness.3
3. Investigate new exercise equipment designed forsonographers (i.e., grip strength putty, available atwww.soundergonomics.com).
4. Get adequate rest.5. Learn effective relaxation exercises and ways to
reduce overall stress. Muscle tension due to mentalstress will not be noticed unless you are consciouslymaking an effort to check for it. (A good exercise todo periodically is to shrug the shoulders toward theears. Hold the tension there for a few seconds. Then,slowly relax the neck, allowing the shoulders tolower, until all tension is gone.)
About Exercise
The bottom line for sonographers is that strongmuscles hold up under the pressure better than weakmuscles.
316 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
OCCUPATIONAL OVERUSE SYNDROME / Jakes 317
This should be of particular interest to the oldersonographers as they have been targeted as an at riskpopulation. The good news is that at any age, one canimprove their endurance, flexibility, strength andresilience. In other words, given that all other lifestylehabits are similar, an active and fit 40-year-old is atlower risk for occupational overuse injury than asedentary 30-year-old.
A sonographer from Canada stated that the facilityshe worked at had set up exercise stations for theemployees, and had been working with aphysiotherapist to incorporate passive stretchingexercises. She further professed that many were takingup strength training to improve upper body strength.3
Specific exercises for sonographers designed bySDMS are available at www.sdms.org (select“workzone” and then “exercises”). Taking the nextstep and adopting a generalized exercise program intoone’s daily routine will substantially reduce theincidence of any type of injury as well as improveoverall health and work productivity.
The key to attaining desired results from an exerciseprogram is to start slowly and gradually increaseintensity and duration as personal fitness and timeallows. Exercise does not need to be intense, neithershould it take up all your free time (unless you want itto). Moderation is very effective and consistency is thekey.3 Only do what fits into your lifestyle andaccommodates your other responsibilities. It is betterto be consistent with a little than inconsistent with alot. Joining a fitness center or getting help initiallyfrom a fitness specialist is highly recommended. At thevery least, follow these guidelines.
AEROBIC EXERCISE
Aerobic exercise should be performed 3 to 5 daysper week for a duration of 20 to 40 minutes at amoderate pace (a pace that allows you to hold aconversation). Examples of aerobic exercise, from lowto high impact, are as follows: swimming, aerobicrowing machine, water aerobics, bicycling, crosscountry skiing, elliptical machine, aerobic slide, rollerskating, ice skating, roller blading, stair master, hiking,treadmill, walking, jazzercise, floor or step aerobics,jogging, and running (Fig. 2).
FLEXIBILITY
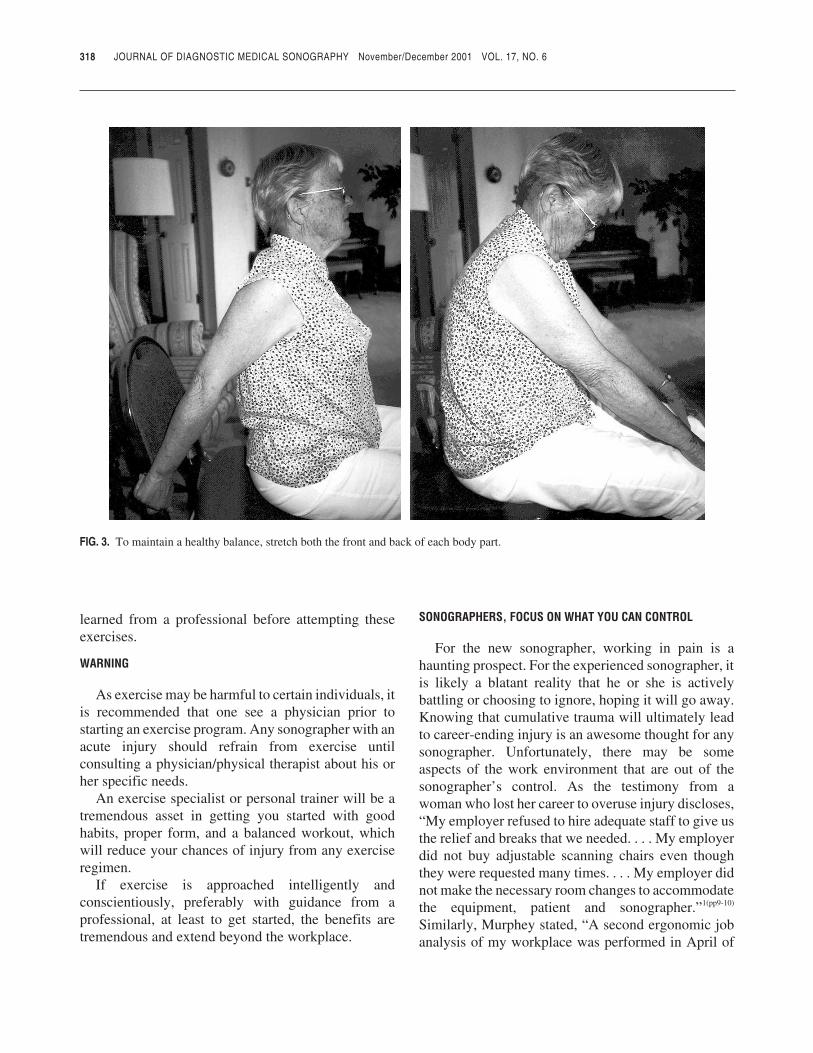
Hold each stretch for approximately 15 seconds.Stretching is gentle and pain free and is most effective
following a general, whole body warm-up. If you are atyour work station and unable to warm up prior tostretching, be especially careful about moving in andout of the stretch slowly and keeping the stretch wellwithin your comfort level (Fig. 3).
STRENGTH TRAINING
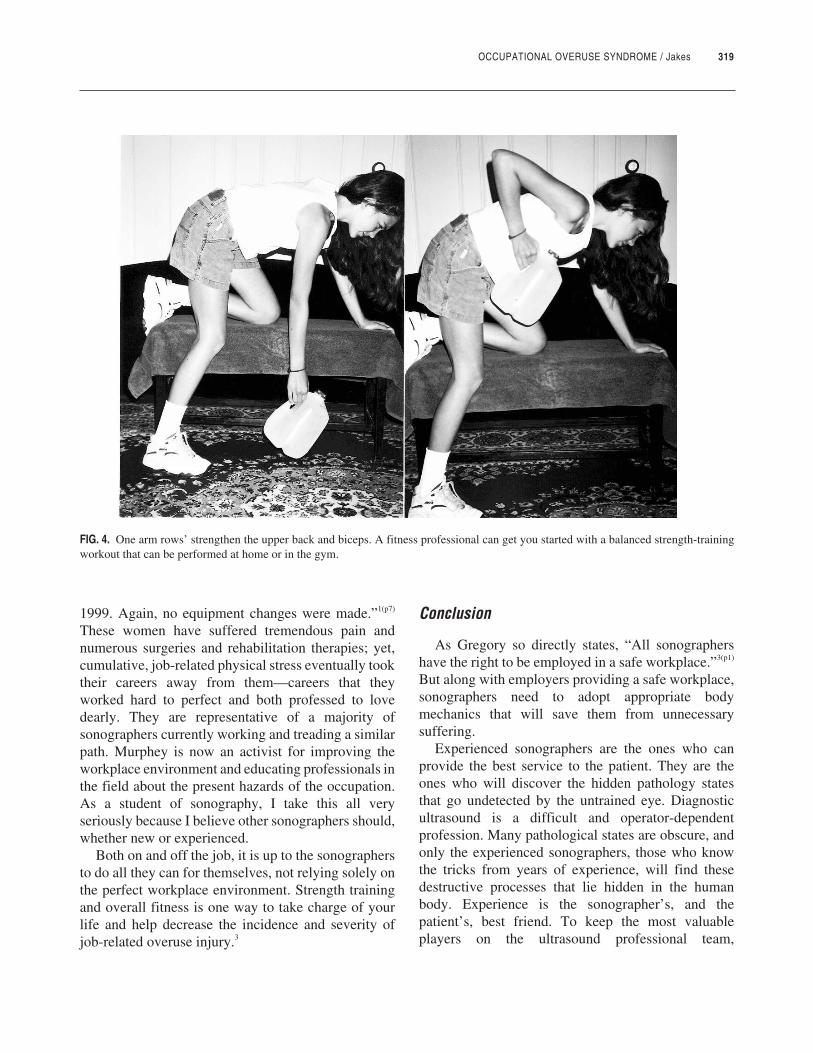
Work each muscle group 2 to 3 days per week.Never work the same muscle 2 days in a row. One wayto avoid working the same muscle 2 days in a row is todo upper-body strength exercises one day followed bylower-body strength exercises the next (Fig. 4).
Always exhale while lifting and inhale whilelowering the weight. If standing, keep knees bentslightly and hold abdominals tight. Hips should bedirectly below shoulders—never sway the hips toassist the lift. Squats and lunges are the highest riskstrength exercises; therefore, proper form should be
FIG. 2. Jogging is an example of high-impact aerobic exercise. Abeginner may want to start out with a low-impact choice such aswalking.
learned from a professional before attempting theseexercises.
WARNING
As exercise may be harmful to certain individuals, itis recommended that one see a physician prior tostarting an exercise program. Any sonographer with anacute injury should refrain from exercise untilconsulting a physician/physical therapist about his orher specific needs.
An exercise specialist or personal trainer will be atremendous asset in getting you started with goodhabits, proper form, and a balanced workout, whichwill reduce your chances of injury from any exerciseregimen.
If exercise is approached intelligently andconscientiously, preferably with guidance from aprofessional, at least to get started, the benefits aretremendous and extend beyond the workplace.
SONOGRAPHERS, FOCUS ON WHAT YOU CAN CONTROL
For the new sonographer, working in pain is ahaunting prospect. For the experienced sonographer, itis likely a blatant reality that he or she is activelybattling or choosing to ignore, hoping it will go away.Knowing that cumulative trauma will ultimately leadto career-ending injury is an awesome thought for anysonographer. Unfortunately, there may be someaspects of the work environment that are out of thesonographer’s control. As the testimony from awoman who lost her career to overuse injury discloses,“My employer refused to hire adequate staff to give usthe relief and breaks that we needed. . . . My employerdid not buy adjustable scanning chairs even thoughthey were requested many times. . . . My employer didnot make the necessary room changes to accommodatethe equipment, patient and sonographer.”1(pp9-10)
Similarly, Murphey stated, “A second ergonomic jobanalysis of my workplace was performed in April of
318 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 3. To maintain a healthy balance, stretch both the front and back of each body part.
OCCUPATIONAL OVERUSE SYNDROME / Jakes 319
1999. Again, no equipment changes were made.”1(p7)
These women have suffered tremendous pain andnumerous surgeries and rehabilitation therapies; yet,cumulative, job-related physical stress eventually tooktheir careers away from them—careers that theyworked hard to perfect and both professed to lovedearly. They are representative of a majority ofsonographers currently working and treading a similarpath. Murphey is now an activist for improving theworkplace environment and educating professionals inthe field about the present hazards of the occupation.As a student of sonography, I take this all veryseriously because I believe other sonographers should,whether new or experienced.
Both on and off the job, it is up to the sonographersto do all they can for themselves, not relying solely onthe perfect workplace environment. Strength trainingand overall fitness is one way to take charge of yourlife and help decrease the incidence and severity ofjob-related overuse injury.3
Conclusion
As Gregory so directly states, “All sonographershave the right to be employed in a safe workplace.”3(p1)
But along with employers providing a safe workplace,sonographers need to adopt appropriate bodymechanics that will save them from unnecessarysuffering.
Experienced sonographers are the ones who canprovide the best service to the patient. They are theones who will discover the hidden pathology statesthat go undetected by the untrained eye. Diagnosticultrasound is a difficult and operator-dependentprofession. Many pathological states are obscure, andonly the experienced sonographers, those who knowthe tricks from years of experience, will find thesedestructive processes that lie hidden in the humanbody. Experience is the sonographer’s, and thepatient’s, best friend. To keep the most valuableplayers on the ultrasound professional team,
FIG. 4. One arm rows’ strengthen the upper back and biceps. A fitness professional can get you started with a balanced strength-trainingworkout that can be performed at home or in the gym.

320 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
sonographers must practice safe postures and scanninghabits and employers must provide state-of-the-art,ergonomically designed equipment. As Baker, apioneer in the field, stated, “In order for patients tohave the benefit of this wonderful nonionizing modal-ity, we have to make the changes that will guarantee aproductive future for all sonographers.”4(p25)
References
1. Society of Diagnostic Medical Sonography: SDMS SpeaksOut for Sonographers at OSHA Hearings on ErgonomicInjury Rules. 2000-2001. Available at: http://www.sdms.org/msi/osha.asp. Accessed March 8, 2001.
2. Vanderpool HE, Friis EA, Smith BS, Harms KL: Prevalenceof carpal tunnel syndrome and other work-relatedmusculoskeletal problems in cardiac sonographers. J OccupMed 1993;35:604–610.
3. Gregory V: Musculoskeletal injuries: an occupational healthand safety issue in sonography. Sound Effects Sep 1998.
4. Wursta C: Sound advice: interview with Joan P. Baker.Radiology Today Feb 2001:24–25.
5. Habes DJ, Baron S: Health Hazard Evaluation Report No. 99-0093. University of Medicine and Dentistry of New Jersey;National Institute for Occupational Safety and Health;Piscataway, New Jersey. August 1999. Available at: http://proquest.umi.com/pqdweb?TS=984096851&Did=000000066652511&Mtd=1&Fmt=3. Accessed August 1999.
6. Murphy C, Russo AB: An update on ergonomic issues insonography: report. Healthcare Benefit Trust. EmployeeHealth and Safety Services 2000.
7. Mercer RB, Marcella CP, Carney DK, McDonald RW:Occupational health hazards to the ultrasonographer and theirpossible prevention. J Am Soc Echocardiography 1997;10:363–366.
8. Batchelor J: Employers can reduce repetitive strain injuriesamong sonographers. AuntMinnie.com 2001. Available at:http://www.soundergonomics.com/PageHtm/auntminnie.htm.Accessed March 8, 2001.
9. Mirk P, Magnavita N, Masini L, Bazzocchi M, Fileni A:Frequency of musculoskeletal symptoms in diagnosticmedical sonographers: results of a pilot survey. RadiologyMedicine (Torino) 1999;98:236–241.
JDMS 17:321-322 November/December 2001
SDMS-JDMS CME TEST
Article: Sonographers and Occupational Overuse Syndrome:Cause, Effect, and Solutions
Author: Cathy Jakes
Category: Other
Objectives: After reading the article, the sonographer will be ableto
1. List strategies to avoid hand, wrist, and back injuries.2. Describe key components of exercise and resources for
sonographer-designed exercises.3. Describe the causes of work-related sonographer injury and
the impacts on patient care.4. Specify the percentage of sonographers reporting career-
ending injuries.5. Specify employer strategies for reducing sonographer injury.6. Specify actions to take when injury occurs.7. Describe the physiologic causes of injury.
1. More time spent scanning and less time between patients is theresult of all of the following excepta. technical advancesb. sonographer shortagesc. expanding ultrasound usesd. injury prevention strategies
2. The percentage of sonographers who have lost their career dueto work-related injury isa. 10b. 20c. 40d. 80
3. Physiologic responses to repetitive strain injury include all ofthe following excepta. venous obstructionb. muscle tearsc. nerve myelinationd. swelling
4. Hand and wrist strains can be minimized by all of thefollowing excepta. selecting thinner and lighter transducer cordsb. using smaller transducersc. buying textured glovesd. holding the wrist in a straight position
5. Sonographers who are concerned about work-related injuryshould encourage employers to provide all of the followingexcepta. assistants to perform functions between examinationsb. height-adjustable chairs with footrestsc. separate monitors for patient viewingd. support cushions and pads
6. With respect to exercise, the author emphasizes the importanceof which of the following aspects?a. intensityb. durationc. consistencyd. variety
7. The SDMS Web site (http://www.sdms.org) Workzone linkprovides exercises designed for all of the followingsonographers excepta. studentb. youngc. experiencedd. injured
8. According to the author, sonographer ergonomic injurydirectly impacts patient care bya. requiring hospitals to invest in ergonomic improvementsb. removing experienced sonographers from the workforcec. increasing “wait times” for sonography examinationsd. reducing the number of portable examinations
9. Which of the following strategies may reduce back injury?a. performing every examination standingb. asking the patient to move closer to the sonographerc. holding the elbow of the scanning arm away from the bodyd. sharing a monitor with the patient
10. When injury occurs, it is important toa. read about ergonomic injuryb. continue to work as usualc. start an exercise programd. report the injury to your employer
JDMS 17:321-322 November/December 2001 321
SDMS-JDMSCME Test
Answer Form
Sonographers and OccupationalOveruse Syndrome: Cause,Effect, and Solutions
Volume 17, Number 6November/December 2001
1.0 SDMS CME Credit
Category: Other
SDMS File #: 0001-01367
_________________________Program Director Signature
Fee:SDMS Member $10.00 USNonmember $25.00 US
NOTE: Tests postmarked afterOctober 31, 2004 will not beaccepted. Allow 4-6 weeks forprocessing. A score of 70% orbetter must be achieved in orderto receive SDMS CME credit.This answer form will bereturned to you and will be yourproof of earning SDMS CMEcredit.
Return your completedanswer form along with theprocessing fee and stampedself-addressed envelope to:
Society of DiagnosticMedical Sonography
P.O. Box 200971Dallas, TX 75320-0971 USA
Instructions1) Each question has only one correct answer. Answer all of the questions.
2) The nonrefundable processing fee for SDMS members is $10.00;$25.00 for nonmembers. This fee can be paid by check or internationalmoney order (U.S. funds drawn on a U.S. bank only).CASH PAYMENTS ARE NOT ACCEPTED.
3) Please note: any SDMS member can take advantage of the JDMS CMEtest at no cost by accessing the test online at http://www.sdms.org/jdms/cme.asp. This free JDMS CME test is an SDMS membership benefitrestricted to only SDMS members. (Access to the online CME test willbe through the applicant’s SDMS membership number.)
4) An ungraded test will be returned for any of the following reasons: testreceived after the expiration date, incorrect processing fee, or missingstamped, self-addressed envelope. If you are unable to provide a self-addressed, stamped envelope, please include an additional $.50 forU.S., Canada, and Mexico; include an additional $1.00 for all othercountries.
Type or Print
Name
Mailing Address
City State/Province/Country Zip+4/Postal Code
Daytime Telephone Email Address
REQUIRED (for CME tracing purposes)
SDMS Members:SDMS Member # Expiration Date
Nonmembers: ORARDMS/CCI # Social Security #
A B C D E
1) � � � � �
2) � � � � �
3) � � � � �
4) � � � � �
5) � � � � �
6) � � � � �
7) � � � � �
8) � � � � �
9) � � � � �
10) � � � � �
Office Use Only
Check #:_________________
Amount: $________________

JDMS 17:323-328 November/December 2001 323
JDMS 17:323-328 November/December 2001
JDMS 17:323-328 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
CARPAL TUNNEL AND MEDIAN NERVE / Wilkinson et al
Ultrasound of theCarpal Tunnel andMedian Nerve:A Reproducibility Study
MAUREEN WILKINSON, DCR(R), DMU, AMS*
KAREN GRIMMER, PHD†
NICOLA MASSY-WESTROPP, BAPPSC(OT)†
The authors describe a protocol for measuring thecarpal tunnel and median nerve in a reproduciblemanner using ultrasound, as well as the variabilityof ultrasound measurements of the median nerve inthe carpal tunnel on repeated testing. Measurementsof the median nerve in the wrist and carpal tunneland measurements of the carpal tunnel were takenon 23 wrists using high-resolution ultrasoundfollowing a specified protocol. These measurementswere repeated a short time later to enable the initialmeasurements to be tested for reproducibility andstability. The same person obtained all measure-ments for the purposes of this study; thus, the resultsrepresent findings in an intraobserver variabilitystudy. Good correlation between the test and retestmeasurements was demonstrated, with r2 valuesbetween 0.72 and 0.98. Paired t test demonstrated nosignificant difference between the test and retestmeasurements. The study shows that repeatedultrasound measurements of the cross-sectionalareas of the carpal tunnel, median nerve at theproximal edge of the carpal tunnel, distal to thecarpal tunnel and at the level of the proximal wristcrease can all be satisfactorily reproduced when astrict ultrasound protocol is adhered to.
Key words: carpal tunnel, median nerve, measure-ments, stability, reproducibility
The carpal tunnel is defined by four bonyprominences. It is defined distally by the hook of thehamate medially and the tubercle of trapeziumlaterally. Proximally, it is defined by the pisiformmedially and the tubercle of the scaphoid laterally. Theflexor retinaculum (transverse carpal ligament)connects these four areas and forms a fibrous sheath,which contains the carpal tunnel. The distal volarflexion crease (distal wrist crease) marks the proximaledge of the flexor retinaculum, the proximal end of thescaphoid, and the pisiform. The pisiform is easilypalpable at the wrist crease and becomes a landmarkfor scanning the carpal tunnel.1 Posteriorly, carpalbones define the floor of the carpal tunnel.
From the *School of Medical Radiation and the †Centre for AlliedHealth Research, University of South Australia.
Reprint requests: Maureen Wilkinson, School of Medical Radiation,University of South Australia, City East Campus, North Terrace, Adelaide,South Australia 5000. E-mail: [email protected].

The median nerve is not uniform in its shape as ittravels into, through, and out of the carpal tunnel,superficial to the flexor tendons, deep to the flexorretinaculum. This fact is important when planning theplacement of the transducer so that reproducibility canoccur. In normal patients, the nerve may flatten in thecarpal tunnel before it divides into sensory and motorbranches distal to the carpal tunnel.1
The nerve may slide between tensed flexortendons,2 which may distort the shape of the nerve. Itfollows, therefore, that patient positioning andwhether the patient is moving or holding a positionwill actively affect normal excursion of the nerve.Recognizing this nonuniformity is important whenplanning the placement of the transducer so thatreproducibility can occur.
According to Jeng et al,3 practical tools in activesurveillance programs are needed to detect carpaltunnel syndrome (CTS) with high sensitivity andspecificity. Such tools could be used to reveal potentialCTS cases before symptoms become established andto monitor the results of surgical, medical, orergonomic interventions for more established cases.
Ultrasound is a noninvasive, repeatable, inexpen-sive, and highly sensitive mode of examination of softtissue, and has been demonstrated to provide usefuland reliable information on soft tissue. The carpaltunnel and its contents can be visualized in an efficientand cost-effective manner.4
Several authors have discussed the use ofultrasound in examining the carpal tunnel.1,5-9 Duncanet al9 demonstrated that ultrasound measurements ofthe cross-sectional area of the median nerve in theproximal carpal tunnel are sensitive and specific forcarpal tunnel syndrome, suggesting that ultrasoundmay be useful in the diagnosis of carpal tunnelsyndrome. They also suggested that standardization ofthe sonographic technique was necessary before ultra-sound could become an accepted procedure. Lee et al10
found a high degree of correlation betweenelectromyography and ultrasound measurements ofthe median nerve and recommended the use of ultra-sound as the first step in diagnostic testing afterphysical examination.
Despite the evidence of sensitivity and specificitysupporting the use of ultrasound, no studies appear tohave tested or demonstrated the reproducibility ofmeasurements in repeated examinations. To test theusefulness of ultrasound in the diagnosis of early
carpal tunnel syndrome in later studies, a set protocolwith demonstrable reproducibility of measurements isrequired.
Method
PARTICIPANTS
A convenience sample of 12 volunteers fromcolleagues and students participated in the study.Volunteers had no prior history of injury to the wrist,or known carpal tunnel problems. Ethics approval wassought and granted by our institution.
POSITIONING
The sonographer sat at a comfortable height anddistance from the participant facing the ultrasoundmachine, so that the controls and participants’ wristswere accessed with ease. Participants were positionedin the same manner at each ultrasound examination foreach structure. Participants were seated next to theultrasound machine facing the sonographer.
The arm for examination was supported on a gurneyat a height midway between the elbow and shoulder,with the forearm supinated and the wrist/hand held inslight dorsiflexion. Participants were verballyinstructed to allow their fingers to relax completely;thus, the fingers were semiflexed.
Previous pilot studies have indicated the need forstrict adherence to protocol, so participants were askedto place both feet flat on the floor and look at a fixedobject. A second tester observed each participant toensure that this standard positioning was maintained ateach examination. It is thought that this lessened theeffects of the gliding tendencies of the nerve.
MEASUREMENTS
Cross-Sectional Area of Median Nerve atProximal Carpal Tunnel (Level of Pisiform)
The proximal carpal tunnel was imaged with thetransducer placed midway between the pisiform andthe tubercle of the scaphoid at the level of the distalwrist crease. This is usually the point of maximumswelling in patients with carpal tunnel syndrome.9 Thetransducer was positioned perpendicular to the mediannerve, that is, angled slightly toward the head, theamount of angulation depending on the path of themedian nerve as it goes through the carpal tunnel, to
324 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
CARPAL TUNNEL AND MEDIAN NERVE / Wilkinson et al 325
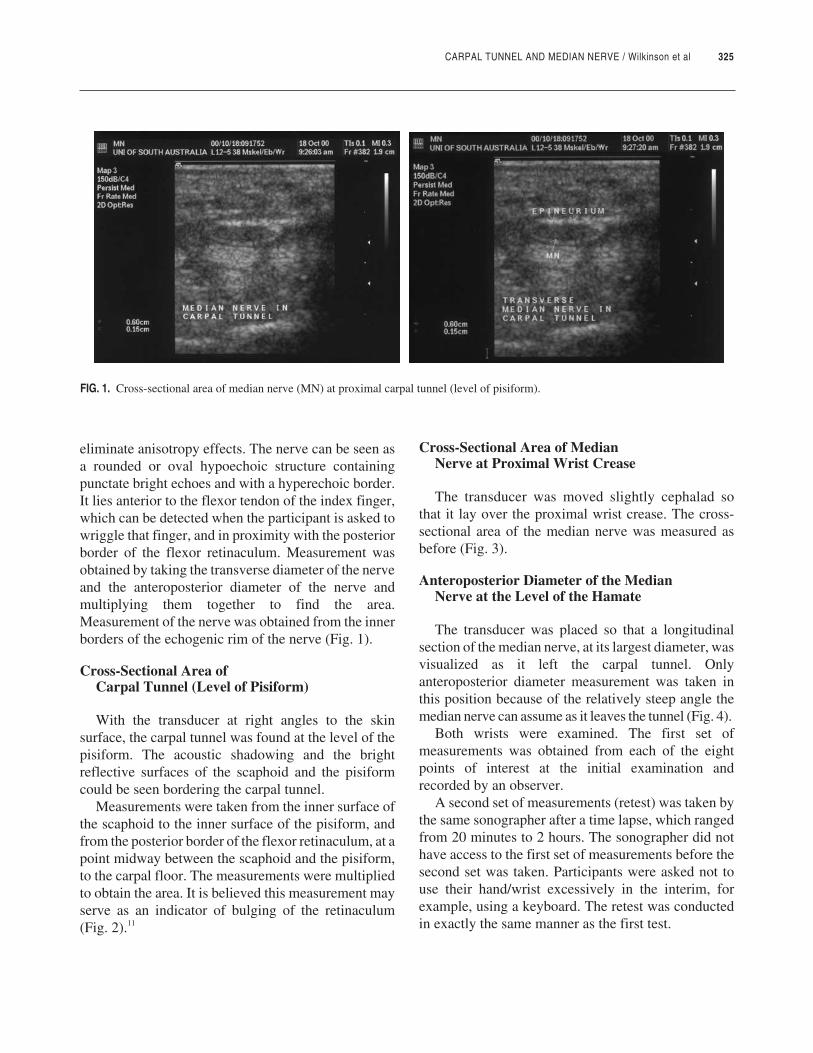
eliminate anisotropy effects. The nerve can be seen asa rounded or oval hypoechoic structure containingpunctate bright echoes and with a hyperechoic border.It lies anterior to the flexor tendon of the index finger,which can be detected when the participant is asked towriggle that finger, and in proximity with the posteriorborder of the flexor retinaculum. Measurement wasobtained by taking the transverse diameter of the nerveand the anteroposterior diameter of the nerve andmultiplying them together to find the area.Measurement of the nerve was obtained from the innerborders of the echogenic rim of the nerve (Fig. 1).
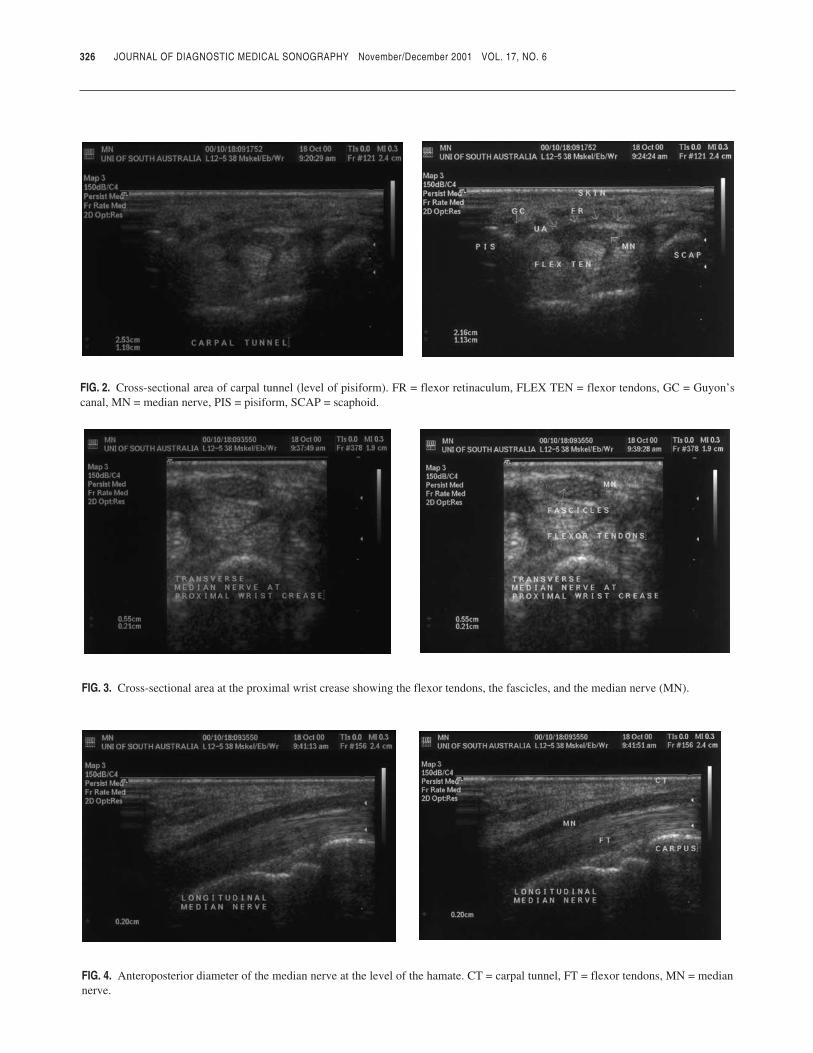
Cross-Sectional Area ofCarpal Tunnel (Level of Pisiform)
With the transducer at right angles to the skinsurface, the carpal tunnel was found at the level of thepisiform. The acoustic shadowing and the brightreflective surfaces of the scaphoid and the pisiformcould be seen bordering the carpal tunnel.
Measurements were taken from the inner surface ofthe scaphoid to the inner surface of the pisiform, andfrom the posterior border of the flexor retinaculum, at apoint midway between the scaphoid and the pisiform,to the carpal floor. The measurements were multipliedto obtain the area. It is believed this measurement mayserve as an indicator of bulging of the retinaculum(Fig. 2).11
Cross-Sectional Area of MedianNerve at Proximal Wrist Crease
The transducer was moved slightly cephalad sothat it lay over the proximal wrist crease. The cross-sectional area of the median nerve was measured asbefore (Fig. 3).
Anteroposterior Diameter of the MedianNerve at the Level of the Hamate
The transducer was placed so that a longitudinalsection of the median nerve, at its largest diameter, wasvisualized as it left the carpal tunnel. Onlyanteroposterior diameter measurement was taken inthis position because of the relatively steep angle themedian nerve can assume as it leaves the tunnel (Fig. 4).
Both wrists were examined. The first set ofmeasurements was obtained from each of the eightpoints of interest at the initial examination andrecorded by an observer.
A second set of measurements (retest) was taken bythe same sonographer after a time lapse, which rangedfrom 20 minutes to 2 hours. The sonographer did nothave access to the first set of measurements before thesecond set was taken. Participants were asked not touse their hand/wrist excessively in the interim, forexample, using a keyboard. The retest was conductedin exactly the same manner as the first test.
FIG. 1. Cross-sectional area of median nerve (MN) at proximal carpal tunnel (level of pisiform).
326 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 2. Cross-sectional area of carpal tunnel (level of pisiform). FR = flexor retinaculum, FLEX TEN = flexor tendons, GC = Guyon’scanal, MN = median nerve, PIS = pisiform, SCAP = scaphoid.
FIG. 3. Cross-sectional area at the proximal wrist crease showing the flexor tendons, the fascicles, and the median nerve (MN).
FIG. 4. Anteroposterior diameter of the median nerve at the level of the hamate. CT = carpal tunnel, FT = flexor tendons, MN = mediannerve.
CARPAL TUNNEL AND MEDIAN NERVE / Wilkinson et al 327
STATISTICAL ANALYSIS
The data were entered into Microsoft Excel version7 for analysis. The measurements of the median nervecross-sectional area at the level of the proximal wristcrease and at the level of the pisiform and the cross-sectional area of the carpal tunnel at the pisiform levelwere collated and divided into right and left wrists.Anteroposterior measurements of the median nervedistal to the carpal tunnel were collated. Averages ofthe right and left initial and retest measurements andstandard deviations were calculated. Pearson r and r2
correlations were calculated to test the stability of testand retest measures. Paired t tests were performed tocompare the measurements of test 1 with those of test2. A significance level of P < .05 was set. The sametests were performed on the combined right and leftmedian nerves distal to the carpal tunnel. Ninety-fivepercent confidence intervals were calculated about themean. These are robust measures of variability andfacilitate comparison between means.
Results
Twenty-four wrists were examined on 10 femaleand 2 male participants. One wrist was excluded from
the study because a previous injury to the wrist madevisualization of the median nerve difficult.
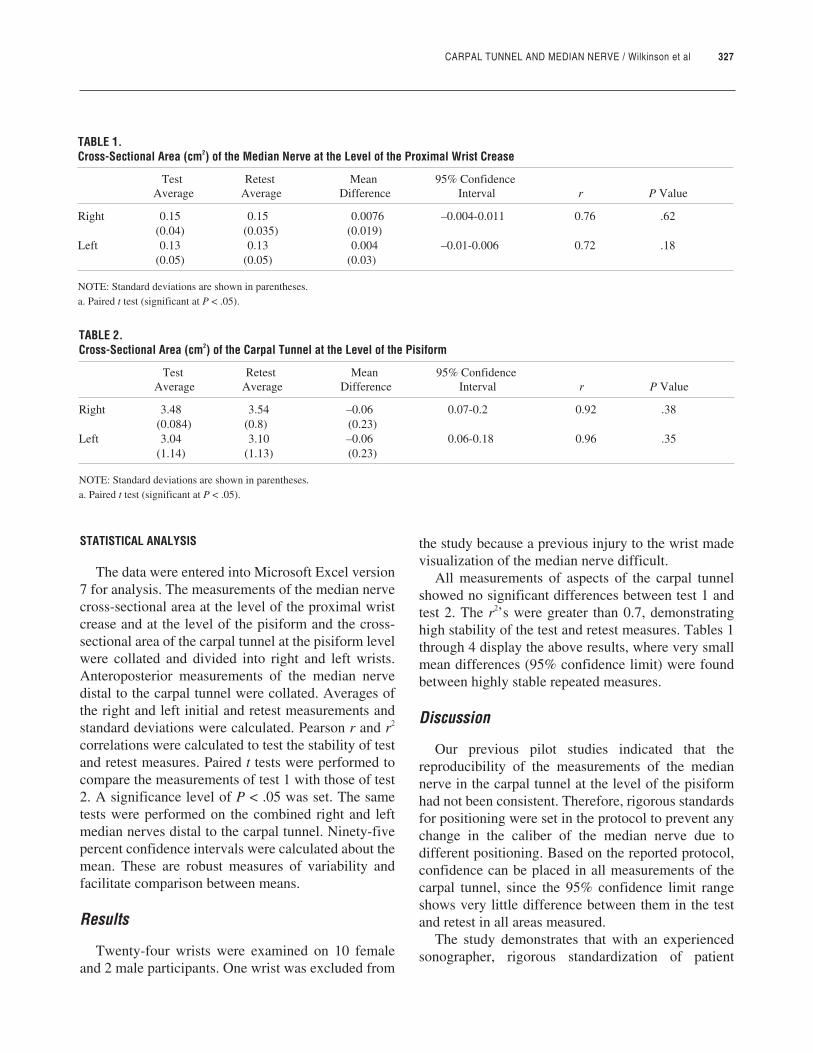
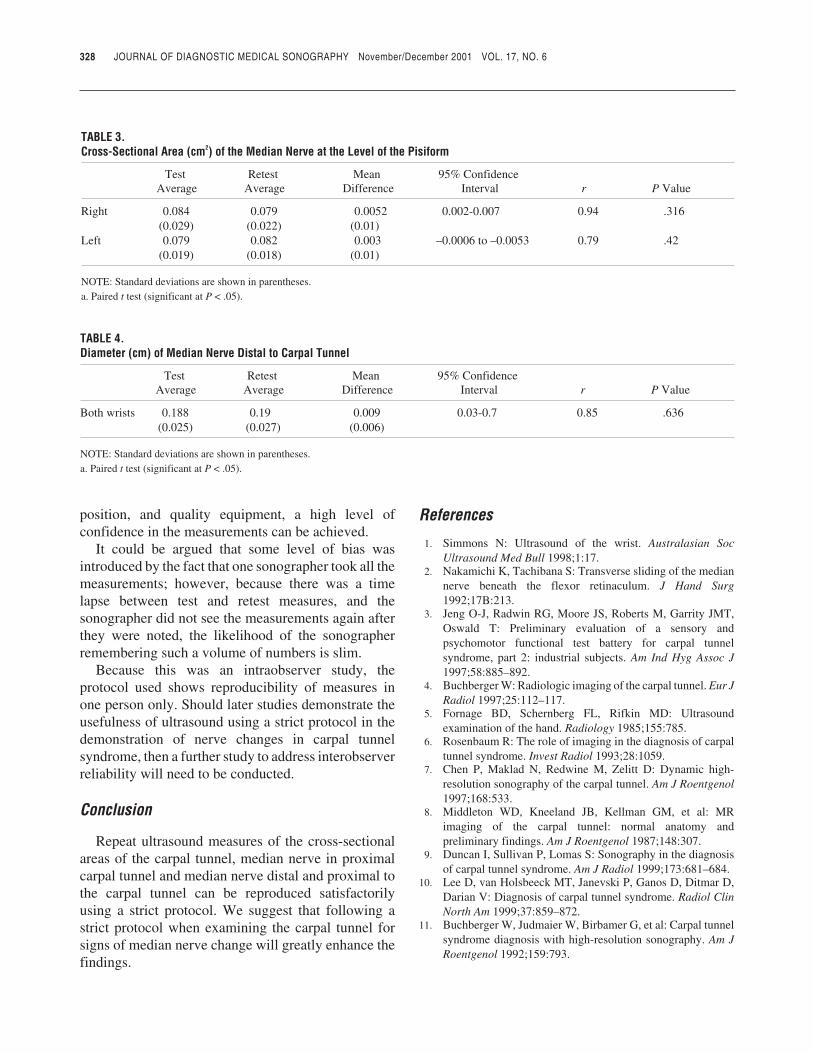
All measurements of aspects of the carpal tunnelshowed no significant differences between test 1 andtest 2. The r2’s were greater than 0.7, demonstratinghigh stability of the test and retest measures. Tables 1through 4 display the above results, where very smallmean differences (95% confidence limit) were foundbetween highly stable repeated measures.
Discussion
Our previous pilot studies indicated that thereproducibility of the measurements of the mediannerve in the carpal tunnel at the level of the pisiformhad not been consistent. Therefore, rigorous standardsfor positioning were set in the protocol to prevent anychange in the caliber of the median nerve due todifferent positioning. Based on the reported protocol,confidence can be placed in all measurements of thecarpal tunnel, since the 95% confidence limit rangeshows very little difference between them in the testand retest in all areas measured.
The study demonstrates that with an experiencedsonographer, rigorous standardization of patient
TABLE 1.Cross-Sectional Area (cm2) of the Median Nerve at the Level of the Proximal Wrist Crease
Test Retest Mean 95% ConfidenceAverage Average Difference Interval r P Valuea
Right 0.15 0.15 0.0076 –0.004-0.011 0.76 .62(0.04) (0.035) (0.019)
Left 0.13 0.13 0.004 –0.01-0.006 0.72 .18(0.05) (0.05) (0.03)
NOTE: Standard deviations are shown in parentheses.a. Paired t test (significant at P < .05).
TABLE 2.Cross-Sectional Area (cm2) of the Carpal Tunnel at the Level of the Pisiform
Test Retest Mean 95% ConfidenceAverage Average Difference Interval r P Valuea
Right 3.48 3.54 –0.06 0.07-0.2 0.92 .38(0.084) (0.8) (0.23)
Left 3.04 3.10 –0.06 0.06-0.18 0.96 .35(1.14) (1.13) (0.23)
NOTE: Standard deviations are shown in parentheses.a. Paired t test (significant at P < .05).
position, and quality equipment, a high level ofconfidence in the measurements can be achieved.
It could be argued that some level of bias wasintroduced by the fact that one sonographer took all themeasurements; however, because there was a timelapse between test and retest measures, and thesonographer did not see the measurements again afterthey were noted, the likelihood of the sonographerremembering such a volume of numbers is slim.
Because this was an intraobserver study, theprotocol used shows reproducibility of measures inone person only. Should later studies demonstrate theusefulness of ultrasound using a strict protocol in thedemonstration of nerve changes in carpal tunnelsyndrome, then a further study to address interobserverreliability will need to be conducted.
Conclusion
Repeat ultrasound measures of the cross-sectionalareas of the carpal tunnel, median nerve in proximalcarpal tunnel and median nerve distal and proximal tothe carpal tunnel can be reproduced satisfactorilyusing a strict protocol. We suggest that following astrict protocol when examining the carpal tunnel forsigns of median nerve change will greatly enhance thefindings.
References
1. Simmons N: Ultrasound of the wrist. Australasian SocUltrasound Med Bull 1998;1:17.
2. Nakamichi K, Tachibana S: Transverse sliding of the mediannerve beneath the flexor retinaculum. J Hand Surg1992;17B:213.
3. Jeng O-J, Radwin RG, Moore JS, Roberts M, Garrity JMT,Oswald T: Preliminary evaluation of a sensory andpsychomotor functional test battery for carpal tunnelsyndrome, part 2: industrial subjects. Am Ind Hyg Assoc J1997;58:885–892.
4. Buchberger W: Radiologic imaging of the carpal tunnel. Eur JRadiol 1997;25:112–117.
5. Fornage BD, Schernberg FL, Rifkin MD: Ultrasoundexamination of the hand. Radiology 1985;155:785.
6. Rosenbaum R: The role of imaging in the diagnosis of carpaltunnel syndrome. Invest Radiol 1993;28:1059.
7. Chen P, Maklad N, Redwine M, Zelitt D: Dynamic high-resolution sonography of the carpal tunnel. Am J Roentgenol1997;168:533.
8. Middleton WD, Kneeland JB, Kellman GM, et al: MRimaging of the carpal tunnel: normal anatomy andpreliminary findings. Am J Roentgenol 1987;148:307.
9. Duncan I, Sullivan P, Lomas S: Sonography in the diagnosisof carpal tunnel syndrome. Am J Radiol 1999;173:681–684.
10. Lee D, van Holsbeeck MT, Janevski P, Ganos D, Ditmar D,Darian V: Diagnosis of carpal tunnel syndrome. Radiol ClinNorth Am 1999;37:859–872.
11. Buchberger W, Judmaier W, Birbamer G, et al: Carpal tunnelsyndrome diagnosis with high-resolution sonography. Am JRoentgenol 1992;159:793.
328 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
TABLE 3.Cross-Sectional Area (cm2) of the Median Nerve at the Level of the Pisiform
Test Retest Mean 95% ConfidenceAverage Average Difference Interval r P Valueaa
Right 0.084 0.079 0.0052 0.002-0.007 0.94 .316(0.029) (0.022) (0.01)
Left 0.079 0.082 0.003 –0.0006 to –0.0053 0.79 .42(0.019) (0.018) (0.01)
NOTE: Standard deviations are shown in parentheses.a. Paired t test (significant at P < .05).
TABLE 4.Diameter (cm) of Median Nerve Distal to Carpal Tunnel
Test Retest Mean 95% ConfidenceAverage Average Difference Interval r P Valuea
Both wrists 0.188 0.19 0.009 0.03-0.7 0.85 .636(0.025) (0.027) (0.006)
NOTE: Standard deviations are shown in parentheses.a. Paired t test (significant at P < .05).
JDMS 17:329-330 November/December 2001
SDMS-JDMS CME TEST
Article: Ultrasound of the Carpal Tunnel and Median Nerve: AReproducibility Study
Authors: Maureen Wilkinson, Karen Grimmer, and Nicola Massy-Westropp
Category: Other
Objectives: After reading the article, the sonographer will be ableto
1. Describe the results of the study and aspects of the scientificmethods used.
2. Specify the landmarks that form the boundaries of the carpaltunnel and the structures that lie superficial and deep to thenerve.
3. Specify the location of a carpal tunnel landmark on the surfaceof the wrist.
4. Describe the course of the median nerve through the carpaltunnel.
5. Specify the location of maximum swelling in patients withcarpal tunnel syndrome.
6. Describe the measurement protocol used in this study.7. Specify reasons that measurements of the cross-sectional
diameter of the median nerve may vary.
1. This study demonstrates that measurements of the carpaltunnel and median nerve area. reproducible by different sonographersb. reproducible by the same sonographerc. independent of protocold. independent of measurement location
2. The portion of the bony prominences forming the carpal tunnelthat is palpable at the wrist crease is thea. hamateb. trapeziumc. pisiformd. scaphoid
3. Measurements of the cross-sectional area of the median nervevary as the result of all of the following excepta. flattening within the tunnelb. nonuniformity in shapec. movement of the flexor tendonsd. sonographer pressure on the transducer
4. The flexor retinaculum forms a fibrous sheath that covers the_________ portion of the carpal tunnela. superficialb. posteriorc. proximald. distal
5. To position the transducer perpendicular to the median nerve,the transducer is angleda. toward the patient’s fingersb. medial from the patient’s armc. lateral from the patient’s armd. toward the patient’s head
6. Measurements of the median nerve were obtained froma. the outer border to the inner borderb. the outer bordersc. the inner border to the outer borderd. the inner borders
7. A strict protocol was adhered to that included all of thefollowing excepta. patients in standard positionb. fingers semiflexed and relaxedc. observer verificationd. multiple sonographers
8. Maximum swelling in patients with carpal tunnel is usuallya. at the distal carpal tunnel (level of the hamate)b. at the proximal carpal tunnel (level of the pisiform)c. midway between the pisiform and the tubercle of the
trapeziumd. at the level of the proximal wrist crease
9. The subjects in this study werea. at high risk for carpal tunnel syndromeb. a selected samplec. a random sampled. a nonrandomized sample
10. The median nerve may assume a relatively steep angle as itleaves the carpal tunnela. proximallyb. distallyc. anteriorlyd. posteriorly
JDMS 17:329-330 November/December 2001 329
SDMS-JDMSCME Test
Answer Form
Ultrasound of the Carpal Tunneland Median Nerve: AReproducibility Study
Volume 17, Number 6November/December 2001
1.0 SDMS CME Credit
Category: Other
SDMS File #: 0001-01509
_________________________Program Director Signature
Fee:SDMS Member $10.00 USNonmember $25.00 US
NOTE: Tests postmarked afterOctober 31, 2004 will not beaccepted. Allow 4-6 weeks forprocessing. A score of 70% orbetter must be achieved in orderto receive SDMS CME credit.This answer form will bereturned to you and will be yourproof of earning SDMS CMEcredit.
Return your completedanswer form along with theprocessing fee and stampedself-addressed envelope to:
Society of DiagnosticMedical Sonography
P.O. Box 200971Dallas, TX 75320-0971 USA
Instructions1) Each question has only one correct answer. Answer all of the questions.
2) The nonrefundable processing fee for SDMS members is $10.00;$25.00 for nonmembers. This fee can be paid by check or internationalmoney order (U.S. funds drawn on a U.S. bank only).CASH PAYMENTS ARE NOT ACCEPTED.
3) Please note: any SDMS member can take advantage of the JDMS CMEtest at no cost by accessing the test online at http://www.sdms.org/jdms/cme.asp. This free JDMS CME test is an SDMS membership benefitrestricted to only SDMS members. (Access to the online CME test willbe through the applicant’s SDMS membership number.)
4) An ungraded test will be returned for any of the following reasons: testreceived after the expiration date, incorrect processing fee, or missingstamped, self-addressed envelope. If you are unable to provide a self-addressed, stamped envelope, please include an additional $.50 forU.S., Canada, and Mexico; include an additional $1.00 for all othercountries.
Type or Print
Name
Mailing Address
City State/Province/Country Zip+4/Postal Code
Daytime Telephone Email Address
REQUIRED (for CME tracing purposes)
SDMS Members:SDMS Member # Expiration Date
Nonmembers: ORARDMS/CCI # Social Security #
A B C D E
1) � � � � �
2) � � � � �
3) � � � � �
4) � � � � �
5) � � � � �
6) � � � � �
7) � � � � �
8) � � � � �
9) � � � � �
10) � � � � �
Office Use Only
Check #:_________________
Amount: $________________
JDMS 17:331-338 November/December 2001 331
DMS 17:331-338 November/December 2001
JDMS 17:331-338 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
CALCIFIC DISORDERS OF THE SHOULDER / Stieler
The Use ofSonography inthe Detection ofBony and CalcificDisorders ofthe ShoulderMARK A. STIELER, MS
Sonography is commonly used for the evaluation ofshoulder symptoms. This report describes some ofthe bony and/or calcific changes that may bevisualized in the ultrasound examination of theshoulder and may not have been detected by othermodalities. Sonography is able to accurately predictthe diameter of the acromioclavicular joint as wellas determine the presence or absence of osteo-arthritis at this joint. The os acromiale is amenableto ultrasonic detection also. Sonography appears tobe more sensitive in the detection of rotator cuffcalcification than the standard shoulder x-ray seriesand has the additional advantage of preciselocalization of the tendon of origin of thecalcification. Sonography is able to reliably detectfractures around the greater tuberosity, and the Hill-Sachs lesion may also be seen. Changes ofirregularity, cyst formation, and sclerosis around thegreater tuberosity may occur in association with theimpingement syndrome. These changes lead toirregularity of the greater tuberosity. Sonographycan detect these changes and, to some degree, gradetheir severity.
Key words: shoulder, ultrasound, sonography,shoulder ultrasound, musculoskeletal ultrasound,calcific tendinitis
The painful shoulder is one of the most commonmusculoskeletal disorders.1 Traditionally, the painfulshoulder has initially been evaluated by plain-film x-ray, followed by specialized techniques such asarthrography, contrast computed tomography (CT),and magnetic resonance imaging (MRI).2 Sonographyis a commonly used application in the evaluation ofshoulder symptoms, and its benefits are wellrecognized, particularly in the assessment of rotatorcuff lesions.3 The diagnostic benefits of the techniqueare augmented by its noninvasive nature and theabsence of ionizing radiation. Additionally,sonography is generally well tolerated by patients andis much less expensive than MRI or CT.
From the Centre for Health and Medical Physics, QueenslandUniversity of Technology, Queensland, Australia.
Reprint requests: Mark A. Stieler, 19 Kingston Drive, Flinders View,Queensland, Australia 4305. E-mail: [email protected].
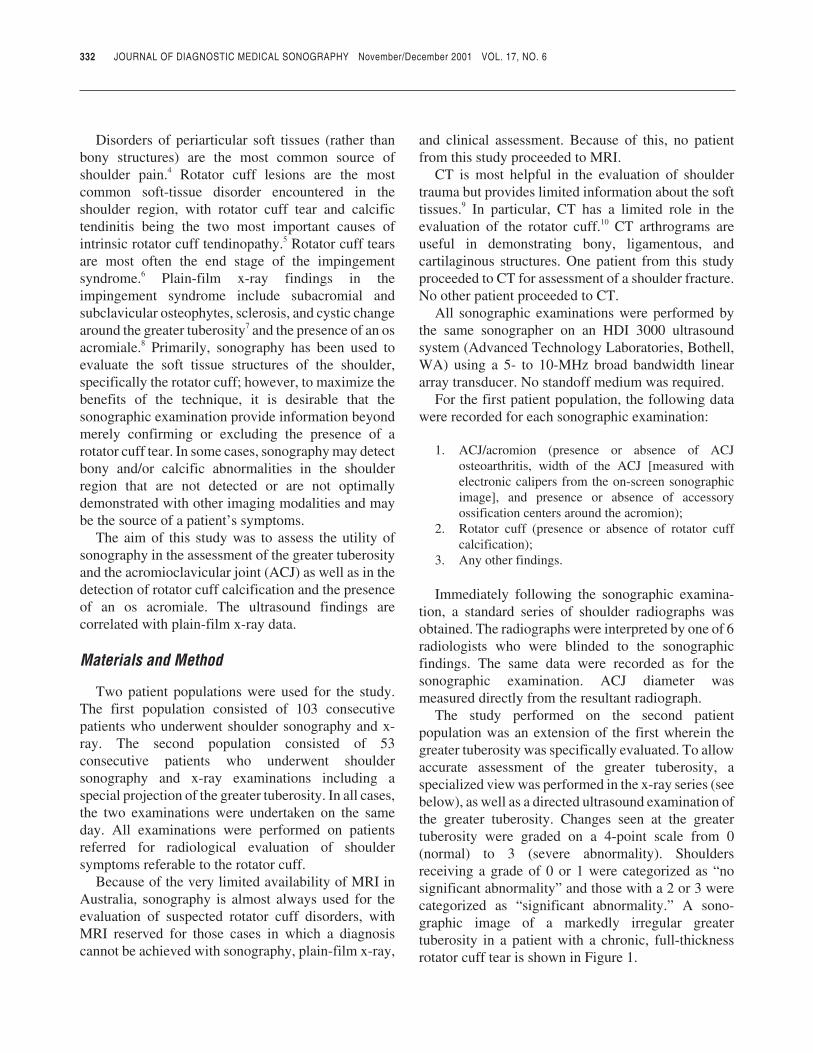
Disorders of periarticular soft tissues (rather thanbony structures) are the most common source ofshoulder pain.4 Rotator cuff lesions are the mostcommon soft-tissue disorder encountered in theshoulder region, with rotator cuff tear and calcifictendinitis being the two most important causes ofintrinsic rotator cuff tendinopathy.5 Rotator cuff tearsare most often the end stage of the impingementsyndrome.6 Plain-film x-ray findings in theimpingement syndrome include subacromial andsubclavicular osteophytes, sclerosis, and cystic changearound the greater tuberosity7 and the presence of an osacromiale.8 Primarily, sonography has been used toevaluate the soft tissue structures of the shoulder,specifically the rotator cuff; however, to maximize thebenefits of the technique, it is desirable that thesonographic examination provide information beyondmerely confirming or excluding the presence of arotator cuff tear. In some cases, sonography may detectbony and/or calcific abnormalities in the shoulderregion that are not detected or are not optimallydemonstrated with other imaging modalities and maybe the source of a patient’s symptoms.
The aim of this study was to assess the utility ofsonography in the assessment of the greater tuberosityand the acromioclavicular joint (ACJ) as well as in thedetection of rotator cuff calcification and the presenceof an os acromiale. The ultrasound findings arecorrelated with plain-film x-ray data.
Materials and Method
Two patient populations were used for the study.The first population consisted of 103 consecutivepatients who underwent shoulder sonography and x-ray. The second population consisted of 53consecutive patients who underwent shouldersonography and x-ray examinations including aspecial projection of the greater tuberosity. In all cases,the two examinations were undertaken on the sameday. All examinations were performed on patientsreferred for radiological evaluation of shouldersymptoms referable to the rotator cuff.
Because of the very limited availability of MRI inAustralia, sonography is almost always used for theevaluation of suspected rotator cuff disorders, withMRI reserved for those cases in which a diagnosiscannot be achieved with sonography, plain-film x-ray,
and clinical assessment. Because of this, no patientfrom this study proceeded to MRI.
CT is most helpful in the evaluation of shouldertrauma but provides limited information about the softtissues.9 In particular, CT has a limited role in theevaluation of the rotator cuff.10 CT arthrograms areuseful in demonstrating bony, ligamentous, andcartilaginous structures. One patient from this studyproceeded to CT for assessment of a shoulder fracture.No other patient proceeded to CT.
All sonographic examinations were performed bythe same sonographer on an HDI 3000 ultrasoundsystem (Advanced Technology Laboratories, Bothell,WA) using a 5- to 10-MHz broad bandwidth lineararray transducer. No standoff medium was required.
For the first patient population, the following datawere recorded for each sonographic examination:
1. ACJ/acromion (presence or absence of ACJosteoarthritis, width of the ACJ [measured withelectronic calipers from the on-screen sonographicimage], and presence or absence of accessoryossification centers around the acromion);
2. Rotator cuff (presence or absence of rotator cuffcalcification);
3. Any other findings.
Immediately following the sonographic examina-tion, a standard series of shoulder radiographs wasobtained. The radiographs were interpreted by one of 6radiologists who were blinded to the sonographicfindings. The same data were recorded as for thesonographic examination. ACJ diameter wasmeasured directly from the resultant radiograph.
The study performed on the second patientpopulation was an extension of the first wherein thegreater tuberosity was specifically evaluated. To allowaccurate assessment of the greater tuberosity, aspecialized view was performed in the x-ray series (seebelow), as well as a directed ultrasound examination ofthe greater tuberosity. Changes seen at the greatertuberosity were graded on a 4-point scale from 0(normal) to 3 (severe abnormality). Shouldersreceiving a grade of 0 or 1 were categorized as “nosignificant abnormality” and those with a 2 or 3 werecategorized as “significant abnormality.” A sono-graphic image of a markedly irregular greatertuberosity in a patient with a chronic, full-thicknessrotator cuff tear is shown in Figure 1.
332 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
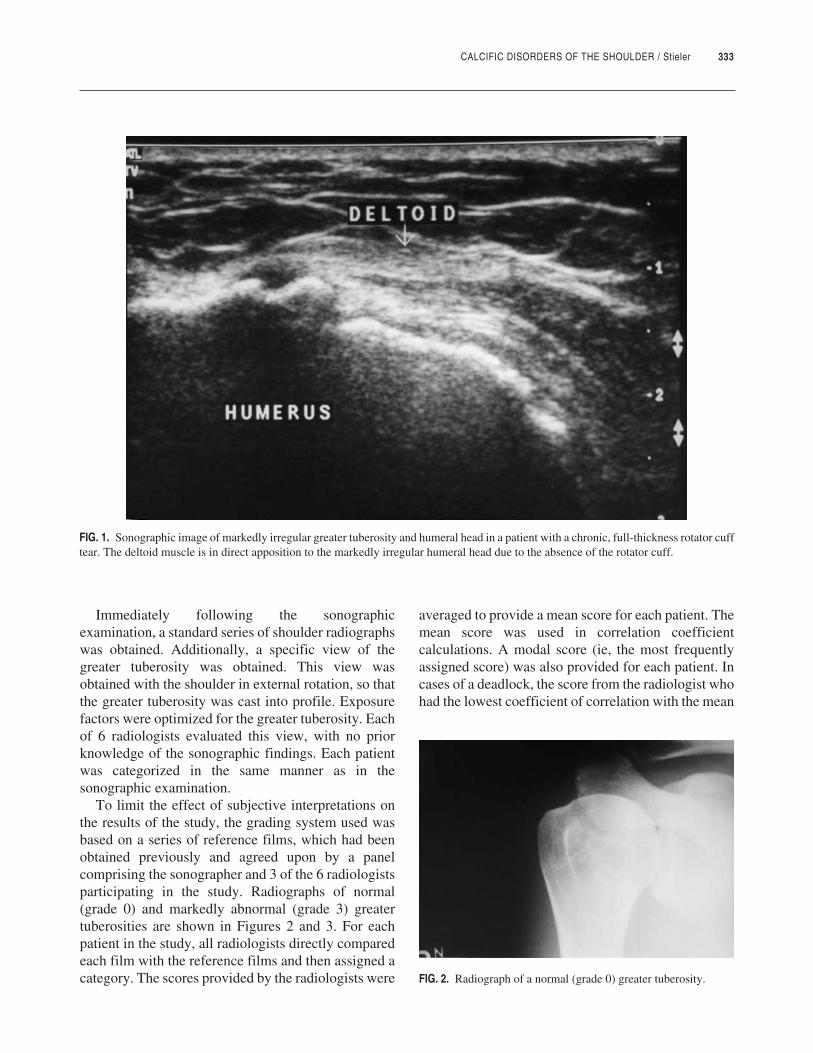
CALCIFIC DISORDERS OF THE SHOULDER / Stieler 333
Immediately following the sonographicexamination, a standard series of shoulder radiographswas obtained. Additionally, a specific view of thegreater tuberosity was obtained. This view wasobtained with the shoulder in external rotation, so thatthe greater tuberosity was cast into profile. Exposurefactors were optimized for the greater tuberosity. Eachof 6 radiologists evaluated this view, with no priorknowledge of the sonographic findings. Each patientwas categorized in the same manner as in thesonographic examination.
To limit the effect of subjective interpretations onthe results of the study, the grading system used wasbased on a series of reference films, which had beenobtained previously and agreed upon by a panelcomprising the sonographer and 3 of the 6 radiologistsparticipating in the study. Radiographs of normal(grade 0) and markedly abnormal (grade 3) greatertuberosities are shown in Figures 2 and 3. For eachpatient in the study, all radiologists directly comparedeach film with the reference films and then assigned acategory. The scores provided by the radiologists were
averaged to provide a mean score for each patient. Themean score was used in correlation coefficientcalculations. A modal score (ie, the most frequentlyassigned score) was also provided for each patient. Incases of a deadlock, the score from the radiologist whohad the lowest coefficient of correlation with the mean
FIG. 1. Sonographic image of markedly irregular greater tuberosity and humeral head in a patient with a chronic, full-thickness rotator cufftear. The deltoid muscle is in direct apposition to the markedly irregular humeral head due to the absence of the rotator cuff.
FIG. 2. Radiograph of a normal (grade 0) greater tuberosity.
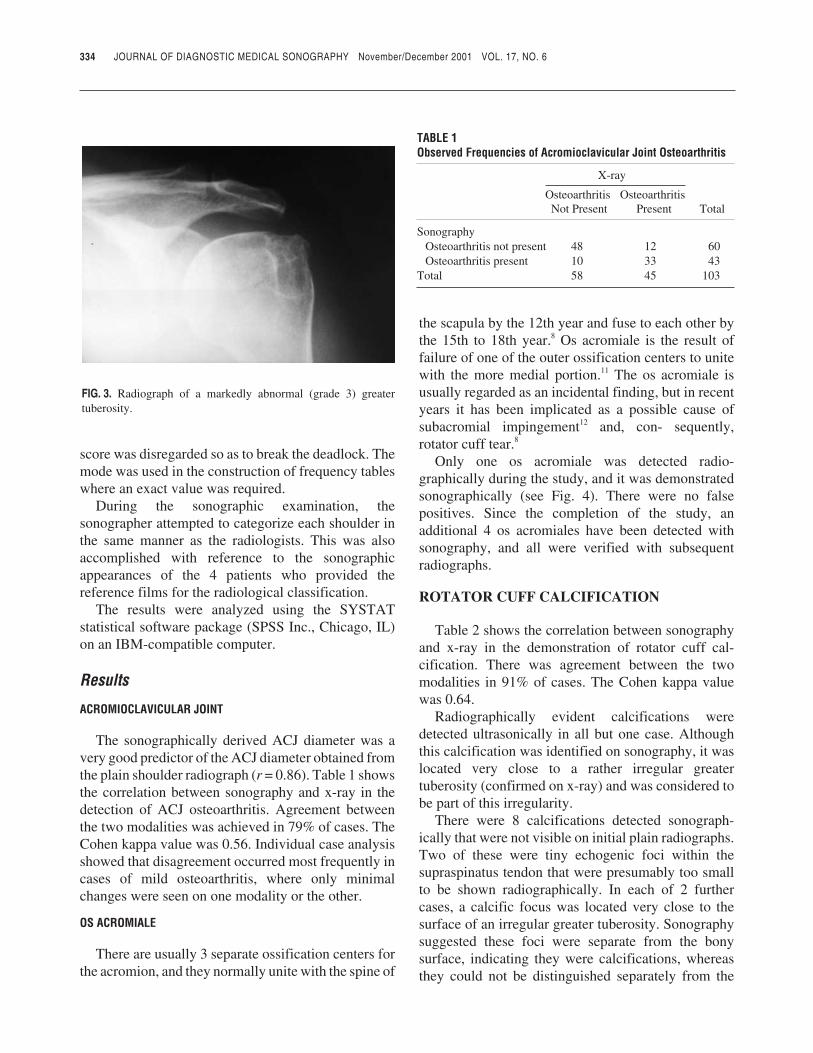
score was disregarded so as to break the deadlock. Themode was used in the construction of frequency tableswhere an exact value was required.
During the sonographic examination, thesonographer attempted to categorize each shoulder inthe same manner as the radiologists. This was alsoaccomplished with reference to the sonographicappearances of the 4 patients who provided thereference films for the radiological classification.
The results were analyzed using the SYSTATstatistical software package (SPSS Inc., Chicago, IL)on an IBM-compatible computer.
Results
ACROMIOCLAVICULAR JOINT
The sonographically derived ACJ diameter was avery good predictor of the ACJ diameter obtained fromthe plain shoulder radiograph (r = 0.86). Table 1 showsthe correlation between sonography and x-ray in thedetection of ACJ osteoarthritis. Agreement betweenthe two modalities was achieved in 79% of cases. TheCohen kappa value was 0.56. Individual case analysisshowed that disagreement occurred most frequently incases of mild osteoarthritis, where only minimalchanges were seen on one modality or the other.
OS ACROMIALE
There are usually 3 separate ossification centers forthe acromion, and they normally unite with the spine of
the scapula by the 12th year and fuse to each other bythe 15th to 18th year.8 Os acromiale is the result offailure of one of the outer ossification centers to unitewith the more medial portion.11 The os acromiale isusually regarded as an incidental finding, but in recentyears it has been implicated as a possible cause ofsubacromial impingement12 and, con- sequently,rotator cuff tear.8
Only one os acromiale was detected radio-graphically during the study, and it was demonstratedsonographically (see Fig. 4). There were no falsepositives. Since the completion of the study, anadditional 4 os acromiales have been detected withsonography, and all were verified with subsequentradiographs.
ROTATOR CUFF CALCIFICATION
Table 2 shows the correlation between sonographyand x-ray in the demonstration of rotator cuff cal-cification. There was agreement between the twomodalities in 91% of cases. The Cohen kappa valuewas 0.64.
Radiographically evident calcifications weredetected ultrasonically in all but one case. Althoughthis calcification was identified on sonography, it waslocated very close to a rather irregular greatertuberosity (confirmed on x-ray) and was considered tobe part of this irregularity.
There were 8 calcifications detected sonograph-ically that were not visible on initial plain radiographs.Two of these were tiny echogenic foci within thesupraspinatus tendon that were presumably too smallto be shown radiographically. In each of 2 furthercases, a calcific focus was located very close to thesurface of an irregular greater tuberosity. Sonographysuggested these foci were separate from the bonysurface, indicating they were calcifications, whereasthey could not be distinguished separately from the
334 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 3. Radiograph of a markedly abnormal (grade 3) greatertuberosity.
TABLE 1Observed Frequencies of Acromioclavicular Joint Osteoarthritis
X-ray
Osteoarthritis OsteoarthritisNot Present Present Total
SonographyOsteoarthritis not present 48 12 60Osteoarthritis present 10 33 43
Total 58 45 103
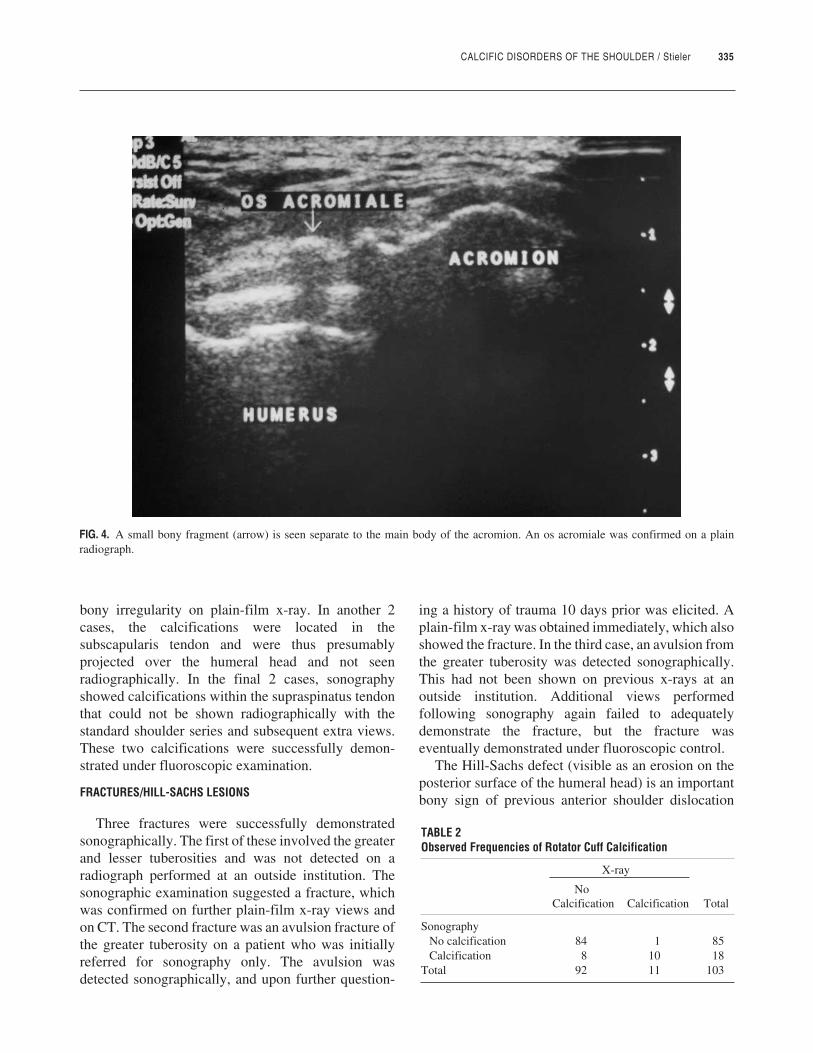
CALCIFIC DISORDERS OF THE SHOULDER / Stieler 335
bony irregularity on plain-film x-ray. In another 2cases, the calcifications were located in thesubscapularis tendon and were thus presumablyprojected over the humeral head and not seenradiographically. In the final 2 cases, sonographyshowed calcifications within the supraspinatus tendonthat could not be shown radiographically with thestandard shoulder series and subsequent extra views.These two calcifications were successfully demon-strated under fluoroscopic examination.
FRACTURES/HILL-SACHS LESIONS
Three fractures were successfully demonstratedsonographically. The first of these involved the greaterand lesser tuberosities and was not detected on aradiograph performed at an outside institution. Thesonographic examination suggested a fracture, whichwas confirmed on further plain-film x-ray views andon CT. The second fracture was an avulsion fracture ofthe greater tuberosity on a patient who was initiallyreferred for sonography only. The avulsion wasdetected sonographically, and upon further question-
ing a history of trauma 10 days prior was elicited. Aplain-film x-ray was obtained immediately, which alsoshowed the fracture. In the third case, an avulsion fromthe greater tuberosity was detected sonographically.This had not been shown on previous x-rays at anoutside institution. Additional views performedfollowing sonography again failed to adequatelydemonstrate the fracture, but the fracture waseventually demonstrated under fluoroscopic control.
The Hill-Sachs defect (visible as an erosion on theposterior surface of the humeral head) is an importantbony sign of previous anterior shoulder dislocation
FIG. 4. A small bony fragment (arrow) is seen separate to the main body of the acromion. An os acromiale was confirmed on a plainradiograph.
TABLE 2Observed Frequencies of Rotator Cuff Calcification
X-ray
NoCalcification Calcification Total
SonographyNo calcification 84 1 85Calcification 8 10 18
Total 92 11 103

and instability.13 Two Hill-Sachs defects weredemonstrated sonographically. One of these wasshown radiographically, and the other could not beshown despite numerous extra views.
GREATER TUBEROSITY
When the changes involving the greater tuberositywere categorized as either significant or notsignificant, there was a correlation coefficient of 0.70between sonography and the mean score of the 6radiologists. Table 3 shows the case-by-case analysisfor sonography versus the modal score. There wasdisagreement in 5 of 53 cases. When the changesinvolving the greater tuberosity were graded on the 4-point scale, the correlation between sonography andthe mean score of the 6 radiologists was 0.62. Table 4shows the case-by-case analysis for sonography versusthe modal score. There was disagreement in 29 of the53 cases; however, in only 1 case did the disagreementspan more than one category. Additionally, a majorityof cases of disagreement occurred when sonographyshowed mild changes whereas no changes wereobserved radiographically.
Discussion
Sonography is of proven value in the assessment ofthe soft-tissue structures of the shoulder, particularlythe rotator cuff tear.14,15 Some studies have alsoassessed the utility of ultrasound in assessing certaindisorders of bony structures in the shoulder region,including fractures of the greater tuberosity16 andirregularity of the greater tuberosity in patients withrotator cuff tear.17
This study has shown sonography to be of value inthe assessment of certain areas traditionally evaluatedby plain radiographs. In the assessment of the ACJ,sonography proved to be a reliable predictor of ACJwidth. Additionally, sonography was able to predictthe presence of osteoarthritis involving the ACJ,particularly cases with more than mild amounts ofosteoarthritis. This is important in the context of theimpingement syndrome, where ACJ osteoarthritis isrecognized as a causative factor.18 Similarly, the osacromiale has been implicated as a precipitating factorfor impingement.8 Sonography proved capable ofdemonstrating an os acromiale in this study, althoughonly 1 case was encountered in a population of 103.Subsequent experience has confirmed the usefulnessof sonography in the diagnosis of this variant. It isnoted, however, that although the os acromiale may bean etiological factor in the impingement syndrome, itis not common, with an incidence of less than 1% inthis study.
Rotator cuff calcification is considered by someauthors to be related to the impingement process,19
whereas others believe it to be an entirely separatepathologic process.20 Possible triggering mechanismsinclude tissue hypoxia21 and genetic susceptibility.22
Whatever the initial causative mechanism, calcificdeposits of sufficient size may themselves impinge onthe acromion.20 Whether or not it is related to theimpingement process, calcific tendinitis is animportant differential diagnosis, and as such it isimportant to document its presence in individualssuspected of having impingement tendinitis.
In the current study, sonography detected allcalcifications detected radiographically except forone. In this one case, the sonographic study suggested
336 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
TABLE 3Frequency Table Comparing Sonography-Graded GreaterTuberosity Changes With Radiologists’ Modal Score: ChangesGraded as Significant or Not Significant
Radiologists (Mode)
NoSignificant SignificantAbnormality Abnormality Total
SonographyNo significant abnormality 43 3 46Significant abnormality 2 5 7
Total 45 8 53
TABLE 4Frequency Table Comparing Sonography-Graded GreaterTuberosity Changes With Radiologists’ Modal Score: ChangesGraded on a 4-Point Scale
X-ray Grade
0 1 2 3 Total
Sonography grade0 15 4 0 0 191 18 6 3 0 272 1 1 2 2 63 0 0 0 1 1
Total 34 11 5 3 53

CALCIFIC DISORDERS OF THE SHOULDER / Stieler 337
the “calcification” was actually bony irregularitywhereas the radiologist interpreting the plain-film x-rays thought the calcification was discrete from thisirregularity. There were a total of 8 calcificationsdetected on sonography that were not visible on thestandard shoulder x-ray series. It appeared that thesecalcifications were not seen radiographically for anumber of reasons, most commonly thesuperimposition of the calcifications on adjacent bonystructures. Very small calcifications were also missedradiographically. These findings suggest sonographyis more sensitive than plain radiography in thedetection of rotator cuff calcifications. Additionally,sonography is able to precisely localize the tendonwithin which the calcification is contained, which canonly be inferred from plain-film x-rays.
The small number of fractures (3) that were detectedduring the course of the study precludes definitivecomment; however, the fact that 3 of 3 fractures in theregion of the greater tuberosity were successfullydemonstrated suggests that sonography has value inthis area. These findings are in accordance with thoseof another study with a larger population of greatertuberosity fractures.16 Similarly, although only 2 Hill-Sachs defects were encountered in the current study, itwould appear that sonography is of value in thedetection of these lesions.
Calcifications, fractures, and Hill-Sachs defectsshare a common trait in that their demonstration onplain radiographs relies on a view tangential to theabnormality, with even a few degrees of errorrendering the lesion undetectable due tosuperimposition on adjacent bony structures. By itsnature, sonography is not constrained by thesedifficulties, often allowing easier detection of theseabnormalities.
Changes around the greater tuberosity arefrequently seen in association with the impingementsyndrome,23 and the ability to demonstrate thesechanges sonographically would add to the diagnosticvalue of this technique. The main changes that wereobserved radiographically around the greatertuberosity in the study were sclerosis, bonyirregularity, and cyst formation. Although sonographyis unable to detect sclerosis, it was uncommon forsclerosis to be an isolated finding, with most cases ofsignificant degeneration showing bony irregularityand, often, cyst formation in association with the
sclerotic change. Sonography is capable ofdemonstrating this bony irregularity. In the study,sonography was quite effective in detecting thosegreater tuberosities with significant degenerativechange, with disagreement in less than 10% of caseswhen compared with the averaged results of the panelof 6 radiologists. Analysis of agreement betweenindividual radiologists showed that the correlationcoefficients ranged between 0.48 and 1.0, illustratingthat there is still a large element of subjectivityinvolved in an assessment such as this, even whenrelatively objective criteria are developed forinterpretation.
Sonography fared slightly less well when thechanges were graded into 4 categories, with exactagreement occurring in less than half of the cases;however, in only one case was the sonographic grademore than one category outside of the radiologists’modal score.
Although the plain radiograph was adopted as thegold standard in this study, there were a number ofcases in which sonography clearly showed irregularityin spite of a normal radiograph. As is the case with theother conditions already considered in this report(calcifications, fractures, etc.), changes around thegreater tuberosity may be undetected radiographicallyif they are not shown in profile. Intuitively, this wouldbe more of a problem in the milder degrees of greatertuberosity degeneration and may at least partiallyaccount for the 18 cases in which sonography showedmild changes whereas the radiologists reported thegreater tuberosity to be normal.
There are a number of potential limitations of thisstudy. Magnification effects were not taken intoaccount for the measurement of ACJ diameter from theplain radiographs; however, these values were usedonly for the calculation of correlation and not for anabsolute measurement.
Only one sonographer interpreted the sonographicresults. Further studies will be necessary to assessinterobserver variability and factors such as sonog-rapher experience level, equipment level, and so on.
Not all sonographically documented calcificationswere verified by other methods. Calcifications thatwere visualized on sonography but not on radiographswere included in the study if they exhibited typicalsonographic characteristics of calcific foci and if thereason for their nonvisualization radiographically

338 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
could be explained based on their anatomical locationand physical characteristics (ie, size, echodensity).Similarly, the Hill-Sachs lesion, which was visible onsonography but not on radiographs, was includedbased on the typical ultrasonic appearances of a well-defined indentation within the surface of the humeralhead posterolaterally.
In conclusion, this study has shown that sonographyhas the ability to detect certain bony and calcificchanges around the shoulder that have traditionallybeen the province of plain radiography. Although theplain shoulder radiograph will not become superfluousin the foreseeable future, this information will enhancethe value of sonography as a diagnostic test and willoccasionally allow sonographers to detect lesions that,for technical reasons, may not have been visible oninitial radiographs.
References
1. Brown MA, Corrigan AB: Common shoulder problems andtheir management. Modern Med Aust 1991;34(7):90–95.
2. Stiles RG, Otte MT: Imaging of the shoulder. Radiology1993;188:603–613.
3. Collins RA, Gristina AG, Carter RE, Webb LX, Voytek A:Ultrasonography of the shoulder: static and dynamic imaging.Orthop Clin North Am 1987;18:351–360.
4. Wolf WB: Shoulder tendinoses. Clin Sports Med 1992;11:871–890.
5. Uhthoff HK, Sarkkar K: An algorithm for shoulder paincaused by soft-tissue disorders. Clin Orthop 1990;254:121–127.
6. Neer CS: Impingement lesions. Clin Orthop 1983;173:70–77.7. Williamson MP, Chandnani VP, Baird DE, et al: Shoulder
impingement syndrome: diagnostic accuracy of magneticresonance imaging and radiographic signs. AustralasianRadiol 1994;38:265–271.
8. Mudge MK, Wood VE, Frykman GK: Rotator cuff tearsassociated with os acromiale. J Bone Joint Surg Am1984;66:427–429.
9. King LJ, Healy JC: Imaging of the painful shoulder. ManualTher 1999;4:11.
10. Hodler J: Diagnosis of shoulder impingement syndrome.Radiologe 1996;36:944.
11. Hutchinson MR, Veenstra MA: Arthroscopic decompressionof shoulder impingement secondary to os acromiale.Arthroscopy 1993;9:28.
12. Swain RA, Wilson FD, Harsha DM: The os acromiale:another cause of impingement. Med Sci Sports Exerc1996;28:1459.
13. Ito H, Takayama A, Shirai Y: Radiographic evaluation of theHill-Sachs lesion in patients with recurrent anterior shoulderinstability. J Shoulder Elbow Surg 2000;9:495–497.
14. Middleton WD, Teefey SA, Yamaguchi K: Sonography of theshoulder. Semin Musculoskeletal Radiol 1998;2:211–222.
15. Roberts CS, Walker JA II, Seligson D: Diagnostic capabilitiesof shoulder ultrasonography in the detection of complete andpartial rotator cuff tears. Am J Orthop 2001;30:159–162.
16. Patten RM, Mack LA, Wang KY, Lingel J: Nondisplacedfractures of the greater tuberosity of the humerus:sonographic detection. Radiology 1992;182:201–204.
17. Wohlwend JR, van Holsbeeck M, Craig J, et al: Theassociation between irregular greater tuberosities and rotatorcuff tears: a sonographic study. Am J Radiol 1998;171:229.
18. Bigliani LU, Nicholson GP, Flatow EL: Arthroscopicresection of the distal clavicle. Orthop Clin North Am1993;24:133–141.
19. Brukner P: Shoulder pain, part II: rotator cuff tendinitis. AustFam Physician 1996;25:1743–1745.
20. Butters KP, Rockwood CA Jr: Office evaluation andmanagement of the shoulder impingement syndrome. OrthopClin North Am 1988;19:755–765.
21. Codman EA: The Shoulder. Boston, MA, Thomas Todd,1934.
22. Uhthoff HK, Sarkar D: Calcifying Tendinitis in the ShoulderRegion. Philadelphia, PA, WB Saunders, 1990.
23. Hardy DC, Vogler JB, White RH: The shoulder impingementsyndrome: prevalence of radiographic findings andcorrelation with response to therapy. Am J Radiol1986;147:557–561.
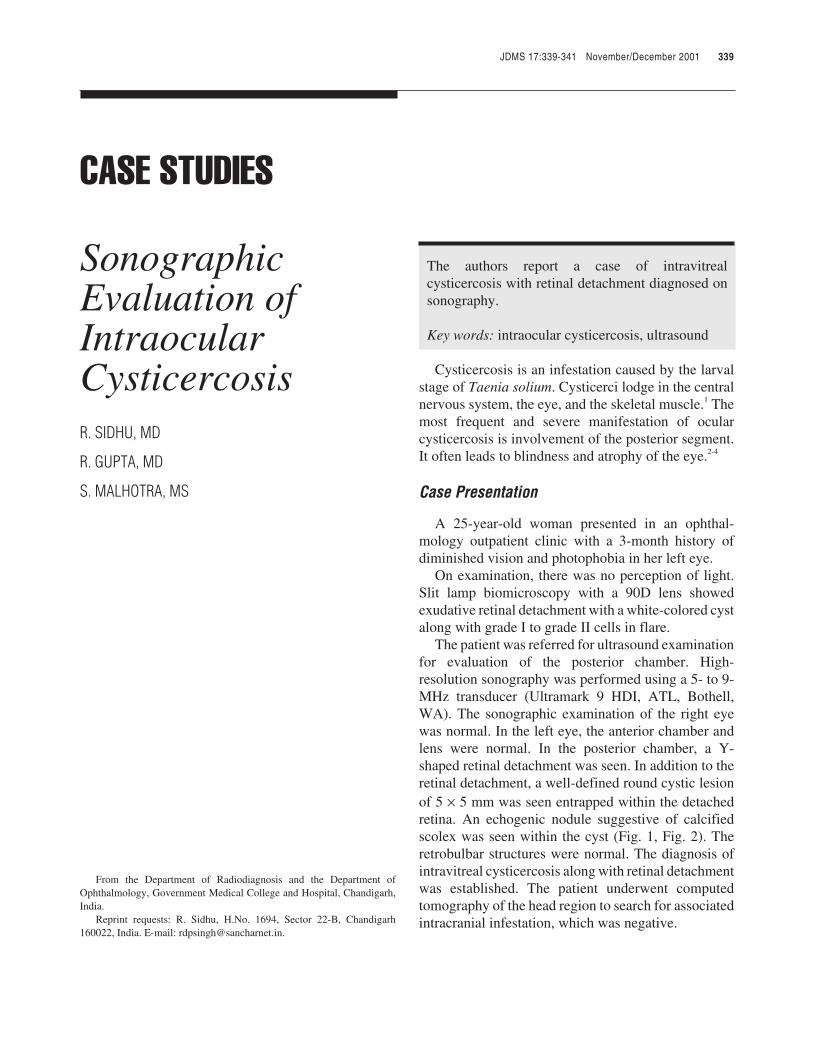
JDMS 17:339-341 November/December 2001 339
JDMS 17:339-341 November/December 2001
JDMS 17:339-341 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
INTRAOCULAR CYSTICERCOSIS / Sidhu et al
CASE STUDIES
SonographicEvaluation ofIntraocularCysticercosisR. SIDHU, MD
R. GUPTA, MD
S. MALHOTRA, MS
The authors report a case of intravitrealcysticercosis with retinal detachment diagnosed onsonography.
Key words: intraocular cysticercosis, ultrasound
Cysticercosis is an infestation caused by the larvalstage of Taenia solium. Cysticerci lodge in the centralnervous system, the eye, and the skeletal muscle.1 Themost frequent and severe manifestation of ocularcysticercosis is involvement of the posterior segment.It often leads to blindness and atrophy of the eye.2-4
Case Presentation
A 25-year-old woman presented in an ophthal-mology outpatient clinic with a 3-month history ofdiminished vision and photophobia in her left eye.
On examination, there was no perception of light.Slit lamp biomicroscopy with a 90D lens showedexudative retinal detachment with a white-colored cystalong with grade I to grade II cells in flare.
The patient was referred for ultrasound examinationfor evaluation of the posterior chamber. High-resolution sonography was performed using a 5- to 9-MHz transducer (Ultramark 9 HDI, ATL, Bothell,WA). The sonographic examination of the right eyewas normal. In the left eye, the anterior chamber andlens were normal. In the posterior chamber, a Y-shaped retinal detachment was seen. In addition to theretinal detachment, a well-defined round cystic lesionof 5 × 5 mm was seen entrapped within the detachedretina. An echogenic nodule suggestive of calcifiedscolex was seen within the cyst (Fig. 1, Fig. 2). Theretrobulbar structures were normal. The diagnosis ofintravitreal cysticercosis along with retinal detachmentwas established. The patient underwent computedtomography of the head region to search for associatedintracranial infestation, which was negative.
From the Department of Radiodiagnosis and the Department ofOphthalmology, Government Medical College and Hospital, Chandigarh,India.
Reprint requests: R. Sidhu, H.No. 1694, Sector 22-B, Chandigarh160022, India. E-mail: [email protected].
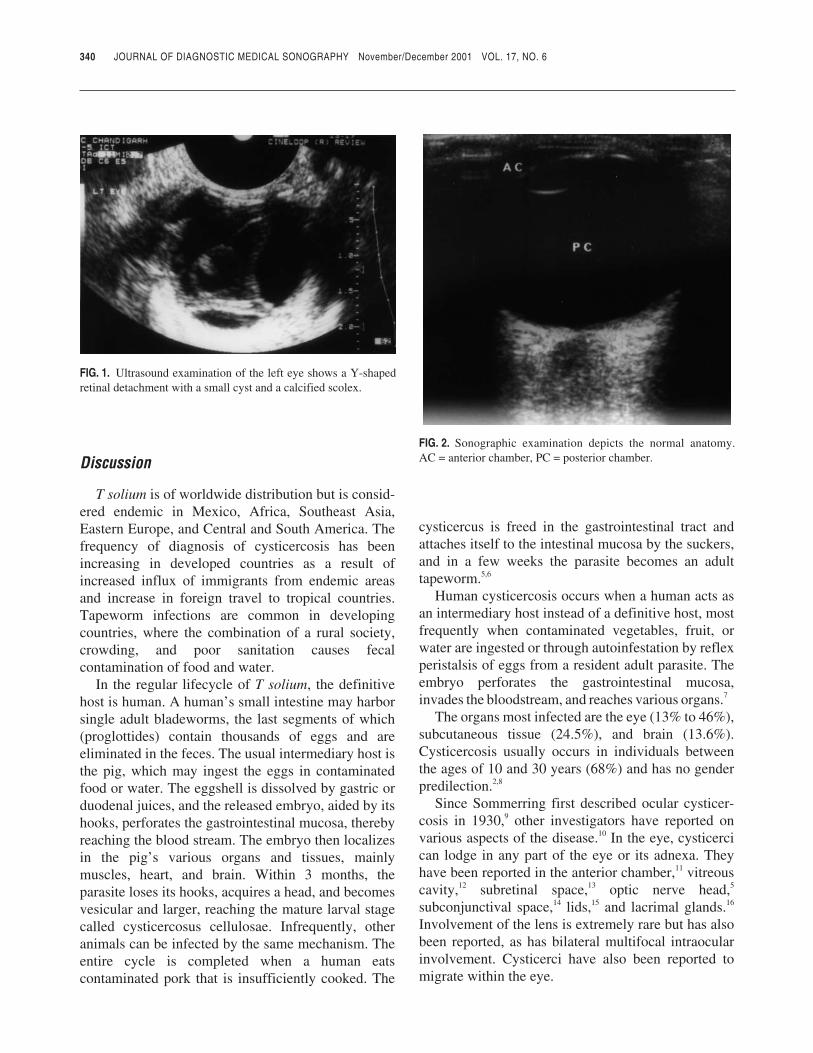
Discussion
T solium is of worldwide distribution but is consid-ered endemic in Mexico, Africa, Southeast Asia,Eastern Europe, and Central and South America. Thefrequency of diagnosis of cysticercosis has beenincreasing in developed countries as a result ofincreased influx of immigrants from endemic areasand increase in foreign travel to tropical countries.Tapeworm infections are common in developingcountries, where the combination of a rural society,crowding, and poor sanitation causes fecalcontamination of food and water.
In the regular lifecycle of T solium, the definitivehost is human. A human’s small intestine may harborsingle adult bladeworms, the last segments of which(proglottides) contain thousands of eggs and areeliminated in the feces. The usual intermediary host isthe pig, which may ingest the eggs in contaminatedfood or water. The eggshell is dissolved by gastric orduodenal juices, and the released embryo, aided by itshooks, perforates the gastrointestinal mucosa, therebyreaching the blood stream. The embryo then localizesin the pig’s various organs and tissues, mainlymuscles, heart, and brain. Within 3 months, theparasite loses its hooks, acquires a head, and becomesvesicular and larger, reaching the mature larval stagecalled cysticercosus cellulosae. Infrequently, otheranimals can be infected by the same mechanism. Theentire cycle is completed when a human eatscontaminated pork that is insufficiently cooked. The
cysticercus is freed in the gastrointestinal tract andattaches itself to the intestinal mucosa by the suckers,and in a few weeks the parasite becomes an adulttapeworm.5,6
Human cysticercosis occurs when a human acts asan intermediary host instead of a definitive host, mostfrequently when contaminated vegetables, fruit, orwater are ingested or through autoinfestation by reflexperistalsis of eggs from a resident adult parasite. Theembryo perforates the gastrointestinal mucosa,invades the bloodstream, and reaches various organs.7
The organs most infected are the eye (13% to 46%),subcutaneous tissue (24.5%), and brain (13.6%).Cysticercosis usually occurs in individuals betweenthe ages of 10 and 30 years (68%) and has no genderpredilection.2,8
Since Sommerring first described ocular cysticer-cosis in 1930,9 other investigators have reported onvarious aspects of the disease.10 In the eye, cysticercican lodge in any part of the eye or its adnexa. Theyhave been reported in the anterior chamber,11 vitreouscavity,12 subretinal space,13 optic nerve head,5
subconjunctival space,14 lids,15 and lacrimal glands.16
Involvement of the lens is extremely rare but has alsobeen reported, as has bilateral multifocal intraocularinvolvement. Cysticerci have also been reported tomigrate within the eye.
340 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 1. Ultrasound examination of the left eye shows a Y-shapedretinal detachment with a small cyst and a calcified scolex.
FIG. 2. Sonographic examination depicts the normal anatomy.AC = anterior chamber, PC = posterior chamber.

INTRAOCULAR CYSTICERCOSIS / Sidhu et al 341
In the posterior segment, access of the parasites ispresumably through the posterior ciliary arteries, andthey have been found near the posterior pole in thesubretinal space, often in the macular area. From thislocation, however, they usually pass through a rent inthe retina into the vitreous.
A rhegmatogenous retinal detachment may developor the perforation may be sealed by an inflammatoryreaction, which leaves a chorioretinal scar. In rarecases, the parasite may pass from the vitreous, throughthe pupil, into the anterior chamber. Infestation of theocular adnexa is probably through the anterior ciliaryarteries.13,16
In 1992, Cardenas et al17 performed a study in 30patients with intraocular cysticercosis and observed a63% incidence of vitreous cavity involvement ascompared to 37% of subretinal involvement. No cystwas observed in the anterior segment. Retinaldetachment was seen in 6* cases (63%).
When the media are clear, the cysticercus is easilyseen by direct ophthalmoscopy or biomicroscopy.However, in the presence of opaque media, ultra-sonography may be valuable in detecting the cyst.When the cyst is subretinal, it shows a curvilinear echocorresponding to the cyst wall. Often, the scolex isseen as a round density connected to this curvilinearecho. A V- or Y-shaped echogenic structure represent-ing the detached retina overlies the cyst. When theparasite is intravitreous, sonography shows acurvilinear cystic structure floating freely in thevitreous cavity. The intravitreous inflammatoryreaction around the cyst may cause low to mediumechoes in the vitreous cavity suggestive of turbidmaterial. An important aspect of the sonography studyis the possibility of observing the parasite’s movementin the vitreous chamber. Ultrasound imaging isvaluable for demonstration and localization of thecyst.18**
Computed tomography (CT), if properlyperformed, can detect intraocular cysticercosis inaddition to intracranial cysticerci. CT may showpinhead areas of increased attenuation. At times,however, it may be difficult to appreciate the cyst insome patients due to the very low density differencebetween the cyst fluid and vitreous fluid. Ultrasoundimaging is especially useful in such cases.
In conclusion, ultrasound is the investigation ofchoice for evaluation of intraocular cysticercosis
because vitreous fluid acts as good acoustic media todetect subtle difference of density between the cystwall and vitreous fluid. This added advantage ofsonography being noninvasive, nonionizing, andeasily available makes it an useful diagnostic tool ininvestigation of intraocular cysticercosis.
References
1. Schenone H, Villaroel F, Rojas A, et al: Epidemiology ofhuman cysticercosis in Latin America, in Flisser, WK,Laclette JP, et al (eds): Cysticercosis: Present State ofKnowledge and Perspectives. New York, Academic Press,1982, pp 25–38.
2. Malik SRK, Gupta AK, Chaudhary S: Ocular cysticercosis.Am J Ophthalmol 1968;66:1169.
3. Lech JR: Ocular cysticercosis. Am J Ophthalmol1949;32:523.
4. Balakrishnan E: Bilateral intraocular cysticerci. Br JOphthalmol 1961;45:150.
5. Wood TR, Binder PS: Intravitreal and intracameralcysticercosis. Ann Ophthalmol 1979;11:1033.
6. Perry HD, Font RL: Cysticercosis of the eyelid. ArchOphthalmol 1978;96:1125.
7. Hutton WL, Vaiser A, Snyder WB: Pars plana vitrectomy forremoval of intravitreous cysticercus. Am J Ophthalmol1976;81:571.
8. Topilow HW, Yimoyines DJ, Freeman HM, Young GAM,Addison R: Bilateral multifocal cysticercosis.Ophthalmology 1981;88:1166.
9. Elder SD. System of Ophthalmology Diseases of the UvealTract. St Louis, MO, CV Mosby, 1996.
10. Gemolotto G: Contribute alla terapia chirurgica delcisticercoendoculare. Arch Ottalmol 1955;59:365.
11. Kapoor S, Kapoor MS: Ocular cysticercosis. J PediatrOphthalmol Strabismus 1978;15:17–172.
12. Mandell LA, Ralph ED: Essentials of Infectious Diseases:Serology and Skin Testing. Boston, MA, Blackwell ScientificPublications, 1985.
13. Bartholomew RS: Subretinal cysticercosis. Am J Ophthalmol1975;79:67–673.
14. Sen DK: Acute suppurative dacryadenitis caused by acysticercus cellulose. J Pediatr Ophthalmol Strabismus1982;19:100–102.
15. Jampol LM, Caldwell JBH, Albert DM: Cysticercuscellulosae in the eyelid. Arch Ophthalmol 1973;89:318–332.
16. Segal P, Mrzyglod S, Smolarz, Dudarewicz J: Subretinalcysticercosis in the macular region. Am J Ophthalmol1964;57:655–664.
17. Cardenas F, Plancarte A, Meza A, Dalma A, Flisser, WK:Taenia solium ocular cysticercosis: findings in 30 cases. AnnOphthalmol 1992;24:25–28.
18. Moragrega E: Ultrasonic diagnosis of intraocular cysticercus,in Hillman JS, Le May MM (eds): Ophthalmic Ultra-sonography. W Junk Publishers, 1984, pp 91–196.
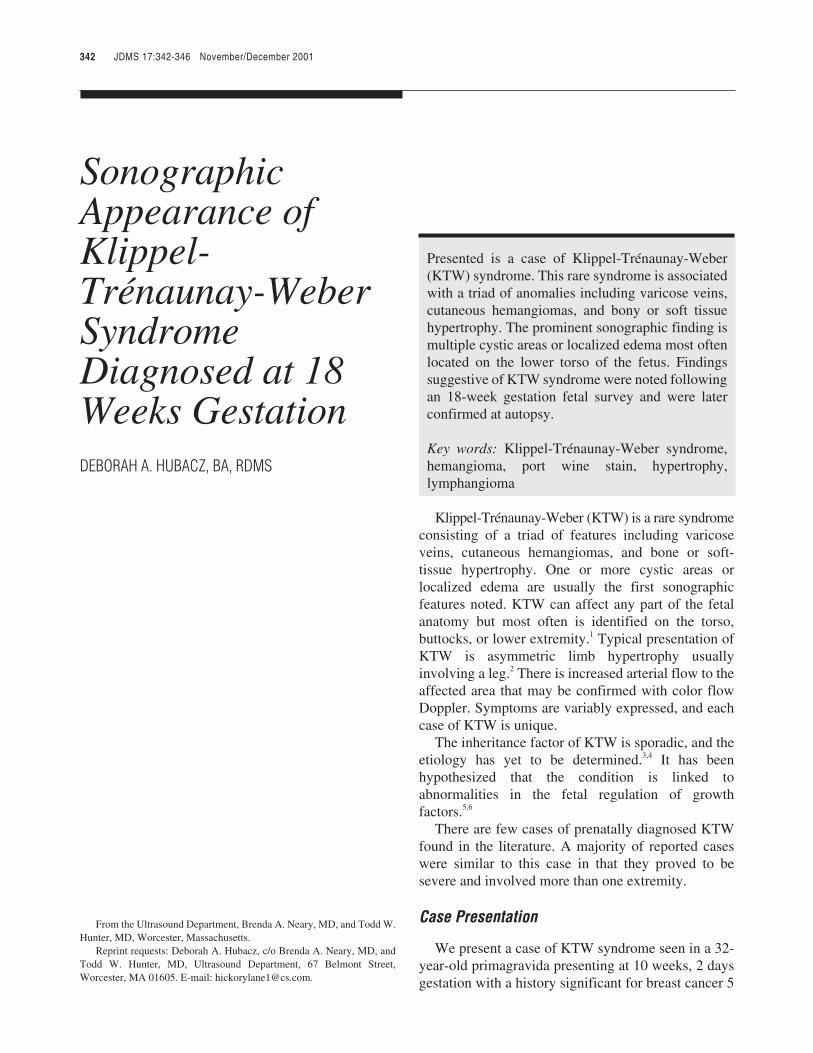
JDMS 17:342-346 November/December 2001
JDMS 17:342-346 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
KLIPPEL-TRÉNAUNAY-WEBER SYNDROME / Hubacz
SonographicAppearance ofKlippel-Trénaunay-WeberSyndromeDiagnosed at 18Weeks GestationDEBORAH A. HUBACZ, BA, RDMS
Presented is a case of Klippel-Trénaunay-Weber(KTW) syndrome. This rare syndrome is associatedwith a triad of anomalies including varicose veins,cutaneous hemangiomas, and bony or soft tissuehypertrophy. The prominent sonographic finding ismultiple cystic areas or localized edema most oftenlocated on the lower torso of the fetus. Findingssuggestive of KTW syndrome were noted followingan 18-week gestation fetal survey and were laterconfirmed at autopsy.
Key words: Klippel-Trénaunay-Weber syndrome,hemangioma, port wine stain, hypertrophy,lymphangioma
Klippel-Trénaunay-Weber (KTW) is a rare syndromeconsisting of a triad of features including varicoseveins, cutaneous hemangiomas, and bone or soft-tissue hypertrophy. One or more cystic areas orlocalized edema are usually the first sonographicfeatures noted. KTW can affect any part of the fetalanatomy but most often is identified on the torso,buttocks, or lower extremity.1 Typical presentation ofKTW is asymmetric limb hypertrophy usuallyinvolving a leg.2 There is increased arterial flow to theaffected area that may be confirmed with color flowDoppler. Symptoms are variably expressed, and eachcase of KTW is unique.
The inheritance factor of KTW is sporadic, and theetiology has yet to be determined.3,4 It has beenhypothesized that the condition is linked toabnormalities in the fetal regulation of growthfactors.5,6
There are few cases of prenatally diagnosed KTWfound in the literature. A majority of reported caseswere similar to this case in that they proved to besevere and involved more than one extremity.
Case Presentation
We present a case of KTW syndrome seen in a 32-year-old primagravida presenting at 10 weeks, 2 daysgestation with a history significant for breast cancer 5
342 JDMS 17:342-346 November/December 2001
From the Ultrasound Department, Brenda A. Neary, MD, and Todd W.Hunter, MD, Worcester, Massachusetts.
Reprint requests: Deborah A. Hubacz, c/o Brenda A. Neary, MD, andTodd W. Hunter, MD, Ultrasound Department, 67 Belmont Street,Worcester, MA 01605. E-mail: [email protected].
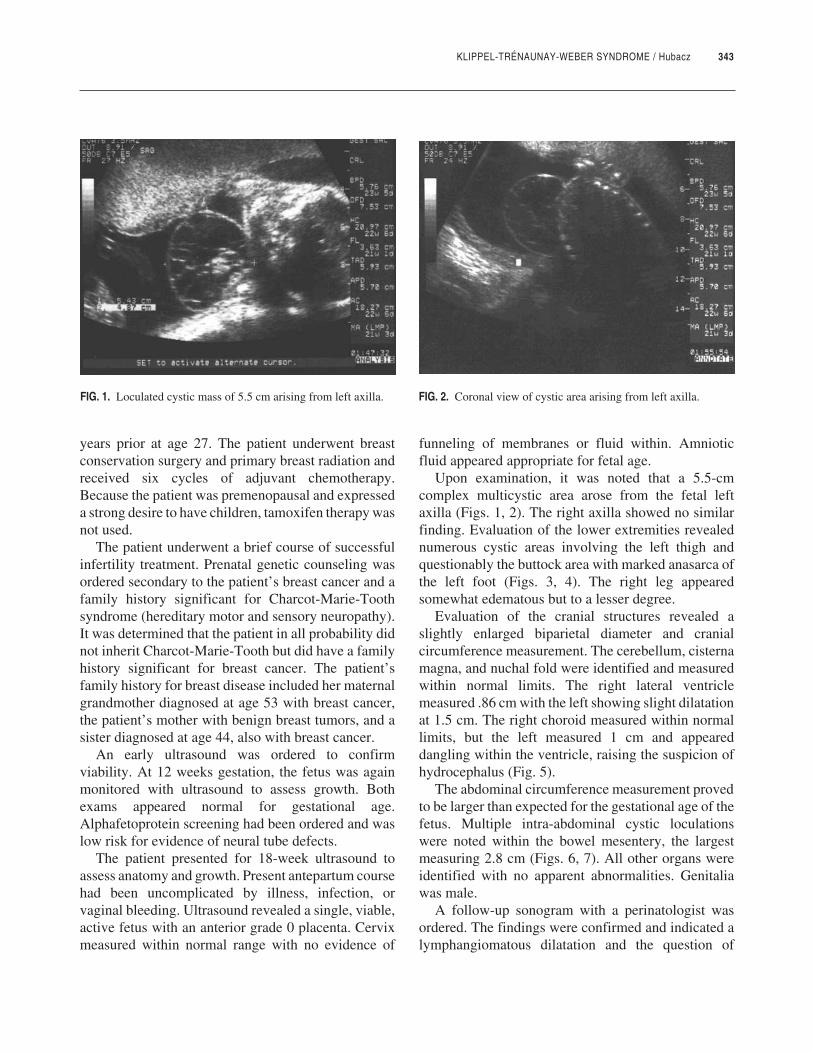
KLIPPEL-TRÉNAUNAY-WEBER SYNDROME / Hubacz 343
years prior at age 27. The patient underwent breastconservation surgery and primary breast radiation andreceived six cycles of adjuvant chemotherapy.Because the patient was premenopausal and expresseda strong desire to have children, tamoxifen therapy wasnot used.
The patient underwent a brief course of successfulinfertility treatment. Prenatal genetic counseling wasordered secondary to the patient’s breast cancer and afamily history significant for Charcot-Marie-Toothsyndrome (hereditary motor and sensory neuropathy).It was determined that the patient in all probability didnot inherit Charcot-Marie-Tooth but did have a familyhistory significant for breast cancer. The patient’sfamily history for breast disease included her maternalgrandmother diagnosed at age 53 with breast cancer,the patient’s mother with benign breast tumors, and asister diagnosed at age 44, also with breast cancer.
An early ultrasound was ordered to confirmviability. At 12 weeks gestation, the fetus was againmonitored with ultrasound to assess growth. Bothexams appeared normal for gestational age.Alphafetoprotein screening had been ordered and waslow risk for evidence of neural tube defects.
The patient presented for 18-week ultrasound toassess anatomy and growth. Present antepartum coursehad been uncomplicated by illness, infection, orvaginal bleeding. Ultrasound revealed a single, viable,active fetus with an anterior grade 0 placenta. Cervixmeasured within normal range with no evidence of
funneling of membranes or fluid within. Amnioticfluid appeared appropriate for fetal age.
Upon examination, it was noted that a 5.5-cmcomplex multicystic area arose from the fetal leftaxilla (Figs. 1, 2). The right axilla showed no similarfinding. Evaluation of the lower extremities revealednumerous cystic areas involving the left thigh andquestionably the buttock area with marked anasarca ofthe left foot (Figs. 3, 4). The right leg appearedsomewhat edematous but to a lesser degree.
Evaluation of the cranial structures revealed aslightly enlarged biparietal diameter and cranialcircumference measurement. The cerebellum, cisternamagna, and nuchal fold were identified and measuredwithin normal limits. The right lateral ventriclemeasured .86 cm with the left showing slight dilatationat 1.5 cm. The right choroid measured within normallimits, but the left measured 1 cm and appeareddangling within the ventricle, raising the suspicion ofhydrocephalus (Fig. 5).
The abdominal circumference measurement provedto be larger than expected for the gestational age of thefetus. Multiple intra-abdominal cystic loculationswere noted within the bowel mesentery, the largestmeasuring 2.8 cm (Figs. 6, 7). All other organs wereidentified with no apparent abnormalities. Genitaliawas male.
A follow-up sonogram with a perinatologist wasordered. The findings were confirmed and indicated alymphangiomatous dilatation and the question of
FIG. 1. Loculated cystic mass of 5.5 cm arising from left axilla. FIG. 2. Coronal view of cystic area arising from left axilla.
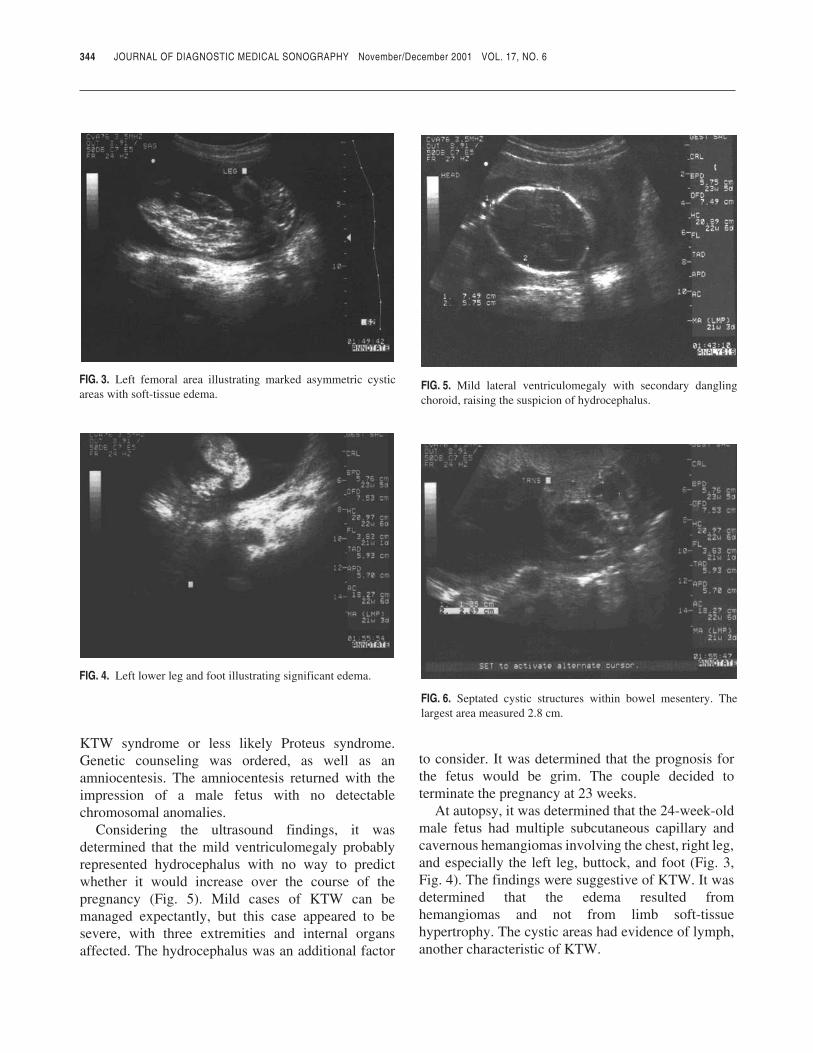
KTW syndrome or less likely Proteus syndrome.Genetic counseling was ordered, as well as anamniocentesis. The amniocentesis returned with theimpression of a male fetus with no detectablechromosomal anomalies.
Considering the ultrasound findings, it wasdetermined that the mild ventriculomegaly probablyrepresented hydrocephalus with no way to predictwhether it would increase over the course of thepregnancy (Fig. 5). Mild cases of KTW can bemanaged expectantly, but this case appeared to besevere, with three extremities and internal organsaffected. The hydrocephalus was an additional factor
to consider. It was determined that the prognosis forthe fetus would be grim. The couple decided toterminate the pregnancy at 23 weeks.
At autopsy, it was determined that the 24-week-oldmale fetus had multiple subcutaneous capillary andcavernous hemangiomas involving the chest, right leg,and especially the left leg, buttock, and foot (Fig. 3,Fig. 4). The findings were suggestive of KTW. It wasdetermined that the edema resulted fromhemangiomas and not from limb soft-tissuehypertrophy. The cystic areas had evidence of lymph,another characteristic of KTW.
344 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 3. Left femoral area illustrating marked asymmetric cysticareas with soft-tissue edema.
FIG. 4. Left lower leg and foot illustrating significant edema.
FIG. 5. Mild lateral ventriculomegaly with secondary danglingchoroid, raising the suspicion of hydrocephalus.
FIG. 6. Septated cystic structures within bowel mesentery. Thelargest area measured 2.8 cm.
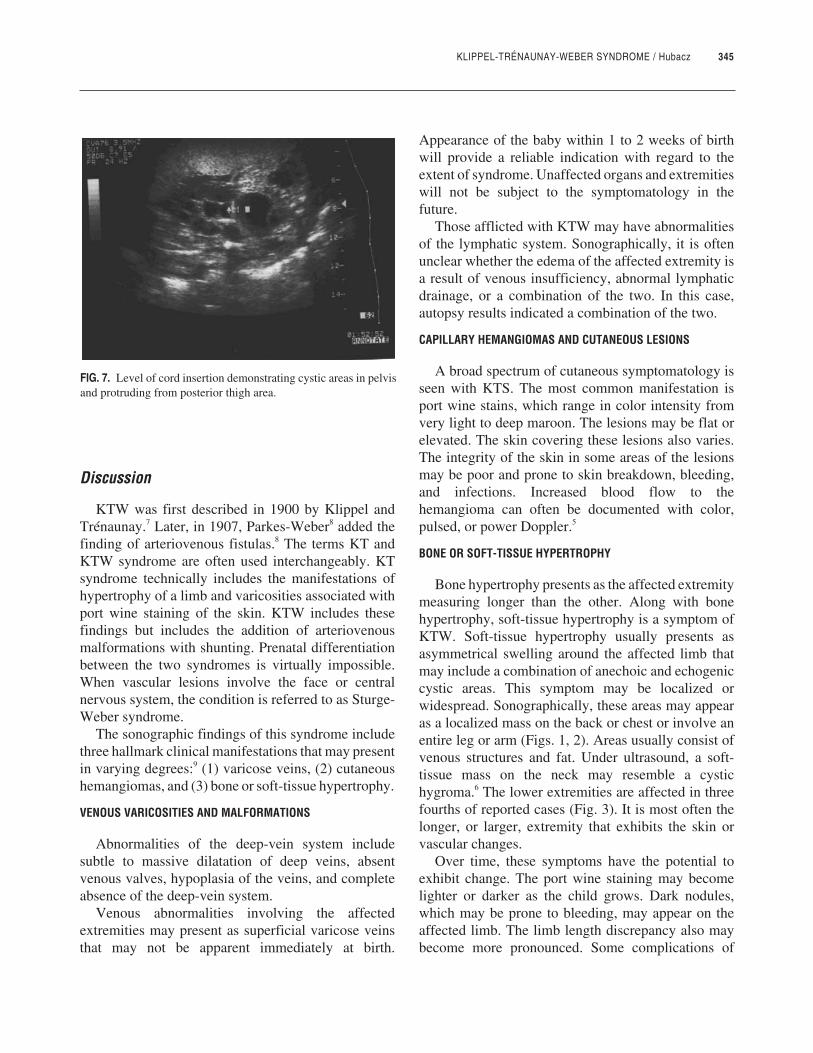
KLIPPEL-TRÉNAUNAY-WEBER SYNDROME / Hubacz 345
Discussion
KTW was first described in 1900 by Klippel andTrénaunay.7 Later, in 1907, Parkes-Weber8 added thefinding of arteriovenous fistulas.8 The terms KT andKTW syndrome are often used interchangeably. KTsyndrome technically includes the manifestations ofhypertrophy of a limb and varicosities associated withport wine staining of the skin. KTW includes thesefindings but includes the addition of arteriovenousmalformations with shunting. Prenatal differentiationbetween the two syndromes is virtually impossible.When vascular lesions involve the face or centralnervous system, the condition is referred to as Sturge-Weber syndrome.
The sonographic findings of this syndrome includethree hallmark clinical manifestations that may presentin varying degrees:9 (1) varicose veins, (2) cutaneoushemangiomas, and (3) bone or soft-tissue hypertrophy.
VENOUS VARICOSITIES AND MALFORMATIONS
Abnormalities of the deep-vein system includesubtle to massive dilatation of deep veins, absentvenous valves, hypoplasia of the veins, and completeabsence of the deep-vein system.
Venous abnormalities involving the affectedextremities may present as superficial varicose veinsthat may not be apparent immediately at birth.
Appearance of the baby within 1 to 2 weeks of birthwill provide a reliable indication with regard to theextent of syndrome. Unaffected organs and extremitieswill not be subject to the symptomatology in thefuture.
Those afflicted with KTW may have abnormalitiesof the lymphatic system. Sonographically, it is oftenunclear whether the edema of the affected extremity isa result of venous insufficiency, abnormal lymphaticdrainage, or a combination of the two. In this case,autopsy results indicated a combination of the two.
CAPILLARY HEMANGIOMAS AND CUTANEOUS LESIONS
A broad spectrum of cutaneous symptomatology isseen with KTS. The most common manifestation isport wine stains, which range in color intensity fromvery light to deep maroon. The lesions may be flat orelevated. The skin covering these lesions also varies.The integrity of the skin in some areas of the lesionsmay be poor and prone to skin breakdown, bleeding,and infections. Increased blood flow to thehemangioma can often be documented with color,pulsed, or power Doppler.5
BONE OR SOFT-TISSUE HYPERTROPHY
Bone hypertrophy presents as the affected extremitymeasuring longer than the other. Along with bonehypertrophy, soft-tissue hypertrophy is a symptom ofKTW. Soft-tissue hypertrophy usually presents asasymmetrical swelling around the affected limb thatmay include a combination of anechoic and echogeniccystic areas. This symptom may be localized orwidespread. Sonographically, these areas may appearas a localized mass on the back or chest or involve anentire leg or arm (Figs. 1, 2). Areas usually consist ofvenous structures and fat. Under ultrasound, a soft-tissue mass on the neck may resemble a cystichygroma.6 The lower extremities are affected in threefourths of reported cases (Fig. 3). It is most often thelonger, or larger, extremity that exhibits the skin orvascular changes.
Over time, these symptoms have the potential toexhibit change. The port wine staining may becomelighter or darker as the child grows. Dark nodules,which may be prone to bleeding, may appear on theaffected limb. The limb length discrepancy also maybecome more pronounced. Some complications of
FIG. 7. Level of cord insertion demonstrating cystic areas in pelvisand protruding from posterior thigh area.

346 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
more severe cases may include arteriovenous fistulawith arterial insufficiency and secondary heart disease,as well as persistent hemorrhage. Cardiomegaly wasreported in a prenatal diagnosis of KTW.10
Each case of KTW has its own combination andvarying degree of symptomatology. There is amale:female ratio of 1:1 associated with KTW.5 Theearliest prenatal diagnosis was made at 14 weeks.3
The sonographic findings in this condition maymimic other syndromes and anomalies. Carefulobservation should be made to rule out largeabdominal wall defects and to confirm whether theedema is localized or presenting overall. Ultrasoundmay reveal other limb findings associated with KTWincluding syndactyly, clinodactyly, polydactyly, or asplit-hand deformity.11
Differential diagnosis would include amniotic bandsyndrome. Amniotic band syndrome usually manifestswith localized limb enlargement but not a substantialincrease in arterial flow to the area. Proteus syndromeis another differential diagnosis to consider. Thissyndrome also manifests with songraphic findings ofbone overgrowth and cystic areas involving the limbsand internal organs. Unlike KTW, these areas are nothemangiomas or a vein abnormality but truly cysticareas with lymph fluid often found within. There willbe no flow seen with color Doppler. Proteus syndromeoften presents with the additional finding ofmacrocephaly.
There is no known cure for KTW syndrome.Conservative symptom treatment may be used inmilder cases. Treatment ranges from compression torelieve the effects of edema and to protecthemangiomas from trauma and bleeding to lasertherapy to reduce or eliminate port wine stains.Superficial varicose veins may be removed if the deep-venous structures are unaffected and able tocompensate. Surgery in early teen years to correctbone length differences is considered if the lengthdiscrepancy is more than 2 cm. Surgery to reduceexcessive tissue may be required. Rarely, amputationof the limb is considered.
Conclusion
Prognosis depends on the type and extent ofinvolvement. Some small vascular anomalies areamenable to surgical correction.12 If the vascularmalformations extend from a limb to the trunk, theprognosis is more dismal in that this scenarioprecludes resection.5
Because the extent of the condition may range frommild to severe, the use of ultrasound to accuratelydocument the affected areas is helpful in the diagnosisand management of each individual case.
References
1. Warhit J, Goldman M, Sachs L, Weiss L, Pek H: Klippel-Trenaunay-Weber syndrome-appearance in utero. J ClinUltrasound Med 1983;2:515–518.
2. Yankowitz J, Slagel D, Williamson R: Prenatal diagnosis ofKlippel-Trenaunay-Weber syndrome by ultrasound. PrenatDiagn 1994;14:745–749.
3. Benacerraf B: Ultrasound Evaluation of Fetal Syndromes.Philadelphia, PA, Churchill Livingstone, 1998, p 277.
4. Hatjis C, Philip A, Anderson G, Mann L: The in uteroultrasonographic appearance of Klippel-Trenaunay-Webersyndrome. Am J Obstet Gynecol 1981;139:972–974.
5. Sanders R: Structural Fetal Abnormalities—The TotalPicture. St Louis, MO, CV Mosby, 1996, pp 17–19, 39–40.
6. Yancy M, Lasley D, Richards D: An unusual neck mass in afetus with Klippel-Trenaunay-Weber syndrome. J UltrasoundMed 1993;12:779–782.
7. Klippel M, Trénaunay P: Du naevus variqueux osteohyper-tophiique. Arch Gen Med 1900;185:641–652.
8. Parkes-Weber F: Angioma formation in connection withhypertrophy of limbs and hemi-hypertrophy. Br J Dermatol1907;19:231.
9. Meholic A, Freimanis A, Stueka J, Lo Piccolo M:Sonographic in utero diagnosis of Klippel-Trenaunay-Webersyndrome. J Ultrasound Med 1991;10:111–114.
10. Drose J, Thickman D, Wiggins J, Haverkamp A: Fetalechocardiographic findings in the Klippel-Trenaunay-Webersyndrome. J Ultrasound Med 1991;10:525–527.
11. Meizner I, Rosenak D, Nadjari M, Maor E: Sonographicdiagnosis of Klippel-Trenaunay-Weber syndrome presentinga sacrococcygeal mass at 14-15 weeks gestation. JUltrasound Med 1994;13:901–904.
12. Shalev E, Romano S, Nseir T, Zuckerman H: Klippel-Trenaunay syndrome—ultrasonic prenatal diagnosis. J ClinUltrasound 1988;16:268–270.
JDMS 17:347-349 November/December 2001 347
JDMS 17:347-349 November/December 2001
JDMS 17:347-349 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
CAROTID ANOMALY AND HOLT-ORAM SYNDROME / Forgosh, Poore
Carotid Anomalyin a Patient WithHolt-OramSyndromeLES B. FORGOSH, MD, FACC, FACP
RHONDA POORE, RDMS, RDCS
The authors present a case of a young mandiagnosed with Holt-Oram syndrome. He was foundto have an additional anomaly, separate ostia for theentire right carotid system, which has not beenassociated with Holt-Oram syndrome in the past.
Key words: separate ostia, hand-heart syndrome,carotid artery, carotid bruit
Case Presentation
The patient is a young man with a past history ofHolt-Oram syndrome (hand-heart syndrome) whopresented for a routine well–young-adult visit. He hashad chromosomal analysis and is a 46 XY malekaryotype. At a few weeks of life, he had a pulmonarybanding on his pulmonary artery secondary to aventricular septal defect. He had this defect completelyrepaired at the age of 11 months. His family history isnegative for other congenital heart diseases, and hissocial history is remarkable for normal developmentand education.
Physical examination revealed a well-developed,well-nourished man with an asymmetric-appearingupper face. Blood pressure was 122/60 mmHg in theleft arm and 126/64 mmHg in the right arm. Pulse was64 bpm, weight was 200 lb, and height was 67 in. Hisright hand is, in fact, smaller than his left hand (theright hand is 13.6 cm in length, and the left hand is 15.6cm in length). The right thumb is hypoplastic andfinger-like, and the patient has hypoplasia of the thenarand hypothenar regions of the right hand. He hasbilateral syndactyly of the second and third toes, withfeet that are broad. Neurological exam is nonfocal.Cardiac exam reveals a regular rate and rhythm, S1,S2, without any obvious S3 or S4. There is a I-II/VIsystolic ejection murmur loudest at the left uppersternal border second intercostal space. There are noobvious heaves or lifts. He does appear to havebilateral carotid bruits on auscultation, but otherwisethe carotids are strong. There is no jugular venousdistention. His face, as mentioned above, is rather
From St. Paul Cardiology, St. Paul, Minnesota.Reprint requests: Les B. Forgosh, 17 West Exchange Street, Suite 750,
St. Paul, MN 55102.

broad and has a mild anti-Mongoloid slant to the eyes.There is hypertelorism, a prominent chin, and a lowposterior hairline.
Echocardiogram showed normal chamber sizeswith normal left and right ventricular wall motionwithout any obvious color flow abnormalities orintrachamber communication.
A carotid ultrasound was obtained, given thepatient’s bruits, which showed an anomalous origin ofthe right internal and right external carotid arteriesdirectly from the right innominate artery. The leftcommon carotid arose from the aorta, and the leftvertebral arose from the left subclavian (Figs. 1, 2 3).
Discussion
Our patient had been seen by genetic specialists andwas diagnosed with Holt-Oram syndrome. He met thecriteria proposed by Zhang et al,1 that is, an inheriteddisorder with a cardiac defect (in his case theventricular septal defect) and upper extremity skeletalabnormalities.
Our patient presented with one slightly differentfinding, that being the lack of a common carotid arteryon the right side. He was noted to have no rightcommon carotid artery arising from his innominatevessel on the right side. In place of this, he had separateostia for the internal and external carotid systems.There have been reports of other vascular abnor-malities of the intracerebral circulation in patients withHolt-Oram syndrome. In reviewing the past andpresent literature on Holt-Oram syndrome, we havenot come across any reference to abnormalitiesinvolving the extracranial carotid circulation.1-10
Koutlas et al2 described a patient who developed anintracerebral hemorrhage due to intracerebral vascularabnormalities. Their patient had no extracranialabnormalities. Our patient, on the other hand, did haveextracranial abnormalities, namely, the separate ostiaof the external and internal carotid arteries off the rightsubclavian. Whether these could possibly cause patho-logical consequences in this patient’s future isunknown. In addition, the presence of the bruit in ourpatient may be due to the transmission of the cardiacmurmur, not to the turbulence within the anomaly. Butat least identifying this anatomical variance at his agewould help with future disease surveillance.
In addition to a screening echocardiogram for apatient suspected of having Holt-Oram syndrome, we
348 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 1. Longitudinal image demonstrating the right internal carotidartery (white arrow), right external carotid artery (gray arrow),branching off the right subclavian artery (black arrow).
FIG. 2. Longitudinal image demonstrating the blood flow throughthe right internal carotid artery (white arrow), right external carotidartery (gray arrow), and the right subclavian artery (black arrow).
FIG. 3. Pulsed and color Doppler image confirming a right externalcarotid artery arising from the right subclavian artery.

CAROTID ANOMALY AND HOLT-ORAM SYNDROME / Forgosh, Poore 349
suggest adding extracranial carotid ultrasound if acarotid bruit is auscultated. Ultrasound of the carotidanatomy is a relatively inexpensive, comfortable, andnoninvasive procedure that can help in themanagement of these patients.3 However, we realizethat this abnormality may not be due to Holt-Oramsyndrome. Early diagnosis and identification of suchextracranial abnormalities could prevent or assist inthe diagnosis of cerebrovascular pathology.
References
1. Zhang KZ, Sun QB, Cheng TO: Holt-Oram syndrome inChina: a collective review of 18 cases. Am Heart J1985;11:572–577.
2. Koutlas ED, Papageorgiou AA, Athyros VG: Holt-Oramsyndrome with malformations of renal and cerebral arteries.Acta Cardiol 1976;51:373–376.
3. Health Care Financing Administration: The WisconsinPhysicians Services Medicare Carrier Fee Schedule. 2001.
4. Tongsong T, Chanprapaph P: Prenatal sonographic diagnosisof Holt-Oram syndrome. J Clin Ultrasound 2000;28:98–100.
5. Ogur G, Gul D, Lenk MK, Imirzalioglu N, Alpay F, Ogur E:Variable clinical expression of Holt-Oram syndrome in threegenerations. Turk J Pediatr 1998;40:613–618.
6. Bennhagen RG, Menahem S: Holt-Oram syndrome inmultiple ventricular septal defects: an association suggestinga possible genetic marker? Cardiol Young 1998;8:128–130.
7. Bohm M: Holt-Oram syndrome. Circulation 1998;98:2636–2637.
8. Schwartz J, Leibovitz A, Berti B, Baumel Y, Habot B: Holt-Oram syndrome in an elderly patient—a case history.Angiology 1992;43:706–708.
9. Filho JDF, Pereira W, Leiria TL, et al: Holt-Oram syndromerevisited: two patients in the same family. Arq Bras Cardiol1999;73:429–434.
10. Basson CT, Cowley GS, Solomon SD, et al: The clinical andgenetic spectrum of the Holt Oram syndrome (hand-heartsyndrome). N Engl J Med 1994;330:885–891.
JDMS 17:350-353 November/December 2001
JDMS 17:350-353 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
CERVICAL ECTOPIC PREGNANCY / Mauk, Forcier
UltrasoundEvaluationand ClinicalManagementof PersistentGestational Sac ina Cervical EctopicPregnancyVICKI L. MAUK, RDMS
GARY L. FORCIER, MD
Early diagnosis with vaginal ultrasound is critical tothe conservative management of cervical ectopicpregnancy. Ultrasound findings of a persistent gesta-tional sac within the endocervical canal duringmedical treatments, when accompanied by a con-tinued decline in HCG levels, does not necessarilysignal a failure of the medical treatment.
Key words: cervical ectopic pregnancy, metho-trexate, potassium chloride, endovaginal
Cervical ectopic pregnancy (CEP) is the rarest formof ectopic gestation. The incidence of cervical ectopicpregnancy is estimated to be 1 in every 2400 live birthsin the United States.1 Early diagnosis with vaginalultrasound is critical to the conservative managementof CEP and in preserving future reproductive capacity.Catastrophic consequences can occur at the time of adilatation and curettage (D&C) in an unsuspectedCEP. Massive hemorrhage historically results in ratesof hysterectomy as high as 50%. Medical therapy withmethotrexate alone or in combination with intrafetalinjection of potassium chloride (KCl) is rapidlybecoming the treatment of choice in CEP.
This is the first report of sonographic findings andclinical management of a persistent gestational sac inthe successful medical management of CEP.
Case Presentation
A woman in her early 30s gravida 2 para 0 with a 6-week history of amenorrhea presented to theemergency room with bright red vaginal bleeding andacute onset of lower abdominal pain. Her history wassignificant for a cone biopsy more than a decade agoand for treatment of chlamydial cervicitis. Initialquantitative human chorionic gonadotropin (hCG) was2269 mIU/mL. An endovaginal ultrasound demon-strated a small fluid collection in the cervical canalsuspected of being an impending spontaneousabortion. Three days after initial ultrasound, the hCGlevel rose to 5144 mIU/mL and a transabdominal andendovaginal evaluation was performed. A Siemens
350 JDMS 17:350-353 November/December 2001
From Personal Women’s Healthcare, Elk Grove, Illinois.Reprint requests: Vicki L. Mauk, 810 Biesterfield Road, Suite 106, Elk
Grove, IL 60007. Fax: 847-981-5580. E-mail: [email protected].
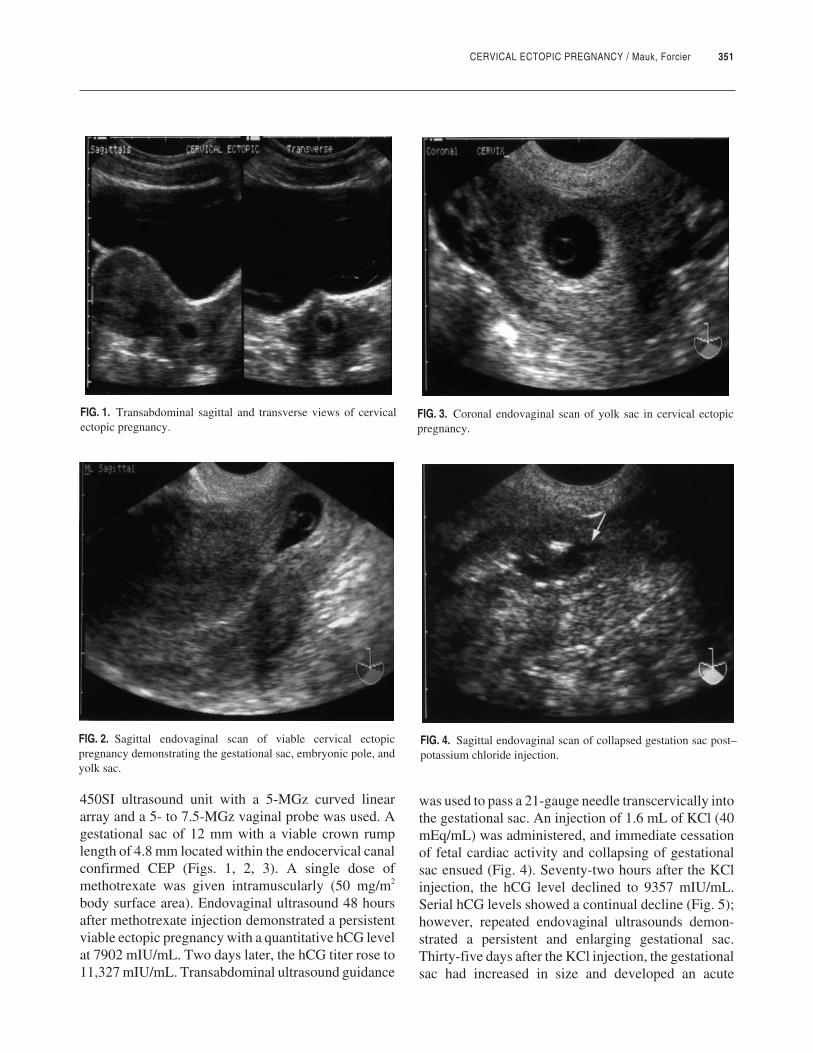
CERVICAL ECTOPIC PREGNANCY / Mauk, Forcier 351
450SI ultrasound unit with a 5-MGz curved lineararray and a 5- to 7.5-MGz vaginal probe was used. Agestational sac of 12 mm with a viable crown rumplength of 4.8 mm located within the endocervical canalconfirmed CEP (Figs. 1, 2, 3). A single dose ofmethotrexate was given intramuscularly (50 mg/m2
body surface area). Endovaginal ultrasound 48 hoursafter methotrexate injection demonstrated a persistentviable ectopic pregnancy with a quantitative hCG levelat 7902 mIU/mL. Two days later, the hCG titer rose to11,327 mIU/mL. Transabdominal ultrasound guidance
was used to pass a 21-gauge needle transcervically intothe gestational sac. An injection of 1.6 mL of KCl (40mEq/mL) was administered, and immediate cessationof fetal cardiac activity and collapsing of gestationalsac ensued (Fig. 4). Seventy-two hours after the KClinjection, the hCG level declined to 9357 mIU/mL.Serial hCG levels showed a continual decline (Fig. 5);however, repeated endovaginal ultrasounds demon-strated a persistent and enlarging gestational sac.Thirty-five days after the KCl injection, the gestationalsac had increased in size and developed an acute
FIG. 1. Transabdominal sagittal and transverse views of cervicalectopic pregnancy.
FIG. 2. Sagittal endovaginal scan of viable cervical ectopicpregnancy demonstrating the gestational sac, embryonic pole, andyolk sac.
FIG. 3. Coronal endovaginal scan of yolk sac in cervical ectopicpregnancy.
FIG. 4. Sagittal endovaginal scan of collapsed gestation sac post–potassium chloride injection.
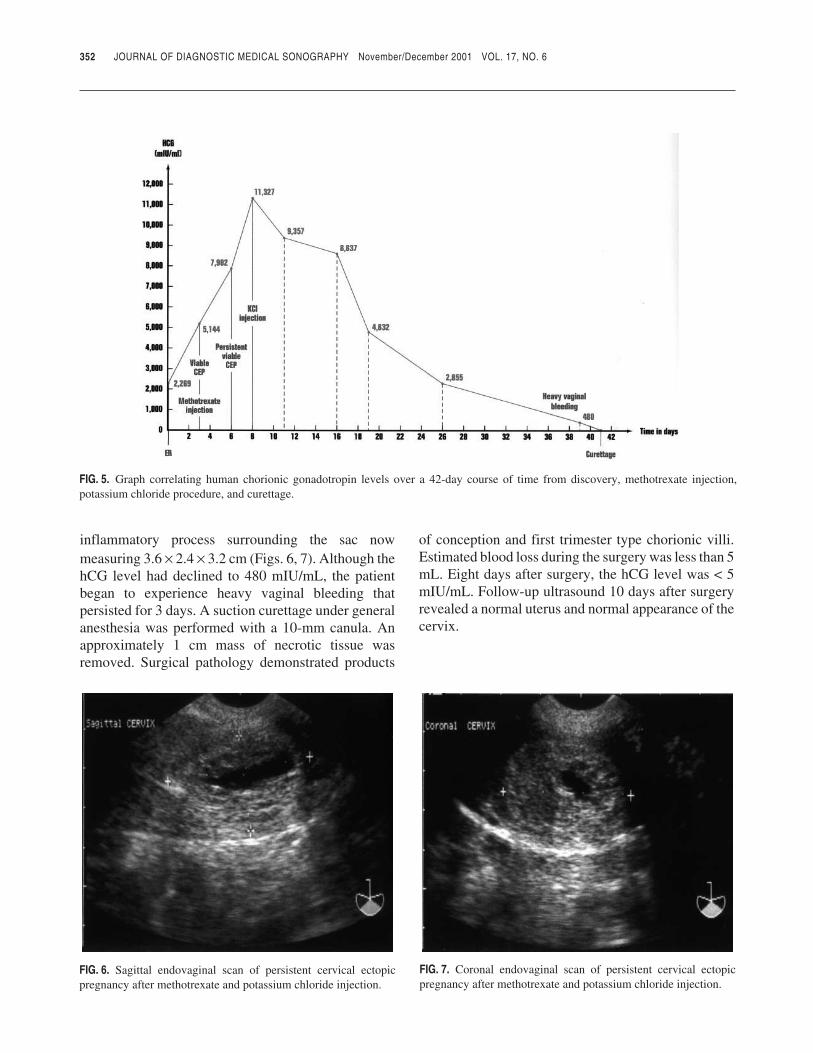
inflammatory process surrounding the sac nowmeasuring 3.6 × 2.4 × 3.2 cm (Figs. 6, 7). Although thehCG level had declined to 480 mIU/mL, the patientbegan to experience heavy vaginal bleeding thatpersisted for 3 days. A suction curettage under generalanesthesia was performed with a 10-mm canula. Anapproximately 1 cm mass of necrotic tissue wasremoved. Surgical pathology demonstrated products
of conception and first trimester type chorionic villi.Estimated blood loss during the surgery was less than 5mL. Eight days after surgery, the hCG level was < 5mIU/mL. Follow-up ultrasound 10 days after surgeryrevealed a normal uterus and normal appearance of thecervix.
352 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 5. Graph correlating human chorionic gonadotropin levels over a 42-day course of time from discovery, methotrexate injection,potassium chloride procedure, and curettage.
FIG. 6. Sagittal endovaginal scan of persistent cervical ectopicpregnancy after methotrexate and potassium chloride injection.
FIG. 7. Coronal endovaginal scan of persistent cervical ectopicpregnancy after methotrexate and potassium chloride injection.

CERVICAL ECTOPIC PREGNANCY / Mauk, Forcier 353
Discussion
Recent conservative medical management treat-ments that have been reported for use in CEP aremethotrexate alone or in combination with KClinjection directly into the gestational sac, cervicalcerclage,2,3 surgical ligation of the cervical branch ofthe uterine arteries4-6 followed by use of a large Foleycatheter to tamponade intracervical bleeding after D&C.2,6-8 Bilateral hypogastric artery ligation9andpercutaneous hypogastric artery emobolization10-12
have also been used to prevent or treat catastrophichemorrhage. In a review of CEP, Ushakov et al13
outlined five necessary conditions for the conservativemedical management of CEP:
1. A reliable diagnosis of CEP.2. A hemodynamically stable patient.3. Menstrual age of < 10 weeks for viable CEP.4. Absence of active renal or hepatic disease.5. Absence of thrombocytopenia or leukopenia.
Conditions 1 and 3 require careful and accuratesonographic evaluation of the patient.
Despite current literature on the success of single-dose methotrexate and KCl injections, the viable CEPencountered in this report was complicated by thepersistent and enlarging gestational sac with heavyvaginal bleeding in spite of declining hCG levels.Ushakov et al13 reported that to achieve successfuleradication of the aberrant trophoblast tissue, con-comitant use of a minor surgical procedure may benecessary under some circumstances.
This report demonstrates that in spite of a persistentand enlarging gestational sac in CEP, methotrexateand KCl therapy was successful. Careful monitoring offalling hCG levels to < 500 mIU/mL provided for an
uncomplicated D&C, preserving the patient’sreproductive capacity.
References
1. Parente JT, Ou CS, Levy J, Legatt E: Cervical pregnancyanalysis: a review and report of five cases. Obstet Gynecol1983;62:79–82.
2. Bachus KE, Stone D, Suh B, et al: Conservative managementof cervical pregnancy with subsequent fertility. Am J ObstetGynecol 1990;162:450–451.
3. Wharton KR, Gore B: Cervical pregnancy managed byplacement of a Shirodkar cerclage before evacuation: a casereport. J Reprod Med 1988;33:227–229.
4. Bayati J, Garcia JE, Dorsey JH, et al: Combined intrauterineand cervical pregnancy from in vitro fertilization and embryotransfer. Fertil Sterility 1998;51:725–727.
5. Bernstein D, Holzinger M, Ovadia J, et al: Conservativetreatment of cervical pregnancy. Obstet Gynecol 1998;58:741–742.
6. Ratten GJ: Cervical pregnancy treated by ligation of thedescending branch of the uterine arteries: case report. Br JObstet Gynaecol 1983;90:367–371.
7. Reginald PW, Reid JE, Paintin DB: Control of bleeding incervical pregnancy: two case reports. Br J Obstet Gynaecol1985;92:1199–1200.
8. Kuppuswani N, Vindekilde J, Sethi CM, et al: Diagnosis andtreatment of cervical pregnancy. Obstet Gynecol1983;61:651–653.
9. Nelson RM: Bilateral internal iliac artery ligation in cervicalpregnancy: conservation of reproductive function. Am JObstet Gynecol 1979;134:145–149.
10. Frates MC, Benson CB, Doubilet PM, et al: Cervical ectopicpregnancy: results of conservative treatment. Radiology1994;191:773–775.
11. Cosin JA, Bean M, Grow D, et al: The use of methotrexateand arterial embolization to avoid surgery in a case of cervicalpregnancy. Fertil Sterility 1997;67S1169–S1171.
12. Lobel SM, Meyerovitz MF, Benson CC, et al: Preoperativeangiographic uterine artery embolization in the managementof cervical pregnancy. Obstet Gynecol 1990;76:938–941.
13. Ushakov FB, Elchalal U, Aceman PJ, et al: Cervicalpregnancy: past and future. Obstet Gynecol Survey1996;52:45–59.
JDMS 17:354-357 November/December 2001
JDMS 17:354-357 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
HYPOCHONDROGENESIS / Pantaleo et al
Hypochondrogenesis:A Rare LethalSkeletal DysplasiaJEAN M. PANTALEO, RT, RDMS*
MARVEEN CRAIG, RDMS†
DONALD M. EHMAN, MD*
A case of achondrogenesis/hypochondrogenesistype II was reported in the fetus of a 24-year-oldwoman. The sonographic diagnosis was made at 16and 18 weeks gestation, when shortened long bonesand a narrow, hypomineralized spine was observed.Targeted scans at a tertiary high-risk centerconfirmed the diagnosis. The patient chose toterminate the pregnancy due to the lethal nature ofthis condition. This case demonstrates the value ofroutine scanning in the early detection of variousfetal abnormalities, including those seen in skeletaldysplasia.
Key words: skeletal dysplasia, achondrogenesis,hypochondrogenesis, dwarfing condition
Skeletal dysplasia occurs with the abnormaldevelopment of the cartilaginous and osseous tissues,resulting in bones that appear shortened, thinned, ordeformed, or that fall more than two standarddeviations below normal.1-4 Evidence of skeletaldysplasia requires a detailed anatomic scan. Skeletaldysplasia, sometimes referred to as a dwarfingcondition, is usually suspected because of familyhistory or a short femur measurement. As a group,lethal skeletal dysplasias are rare. Affected fetusesmay exhibit normal long-bone growth patterns until 21to 26 weeks and are not always detected prenatally byultrasound imaging. A sporadic occurrence of thesetypes of dwarfism may be missed if the patient’s onlyultrasound examination occurs before 26 weeks.1
Case Presentation
A patient in her mid 20s (gravida 3, para 1, TAB 1)was referred for pregnancy at approximately 8 weeksgestation. A single intrauterine pregnancy withpositive embryonic cardiac motion and a crown-rumplength at approximately 8.9 weeks gestation wasfound. A repeat study approximately 2 months latershowed fetal head and abdominal growth consistentwith the patient’s menstrual age. The femur andhumerus appeared shortened, measuring approx-
354 JDMS 17:354-357 November/December 2001
From *Donald M. Ehman, MD, Inc., Brawley, California; and †Tucson,Arizona.
Reprint requests: Jean M. Pantaleo, c/o Donald M. Ehman, MD, Inc.,197 W. Legion Road, #300, Brawley, CA 92227. E-mail: [email protected].
The authors are grateful to Lola Schnittker for photographic assistance.
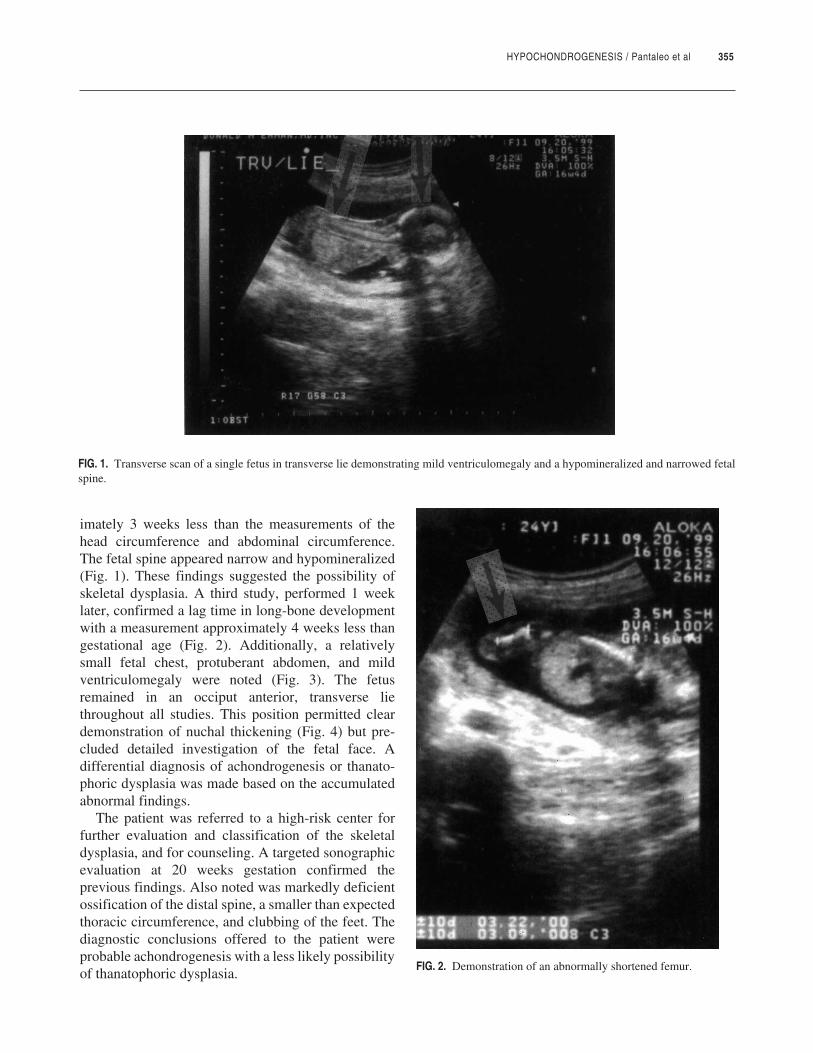
HYPOCHONDROGENESIS / Pantaleo et al 355
imately 3 weeks less than the measurements of thehead circumference and abdominal circumference.The fetal spine appeared narrow and hypomineralized(Fig. 1). These findings suggested the possibility ofskeletal dysplasia. A third study, performed 1 weeklater, confirmed a lag time in long-bone developmentwith a measurement approximately 4 weeks less thangestational age (Fig. 2). Additionally, a relativelysmall fetal chest, protuberant abdomen, and mildventriculomegaly were noted (Fig. 3). The fetusremained in an occiput anterior, transverse liethroughout all studies. This position permitted cleardemonstration of nuchal thickening (Fig. 4) but pre-cluded detailed investigation of the fetal face. Adifferential diagnosis of achondrogenesis or thanato-phoric dysplasia was made based on the accumulatedabnormal findings.
The patient was referred to a high-risk center forfurther evaluation and classification of the skeletaldysplasia, and for counseling. A targeted sonographicevaluation at 20 weeks gestation confirmed theprevious findings. Also noted was markedly deficientossification of the distal spine, a smaller than expectedthoracic circumference, and clubbing of the feet. Thediagnostic conclusions offered to the patient wereprobable achondrogenesis with a less likely possibilityof thanatophoric dysplasia.
FIG. 1. Transverse scan of a single fetus in transverse lie demonstrating mild ventriculomegaly and a hypomineralized and narrowed fetalspine.
FIG. 2. Demonstration of an abnormally shortened femur.
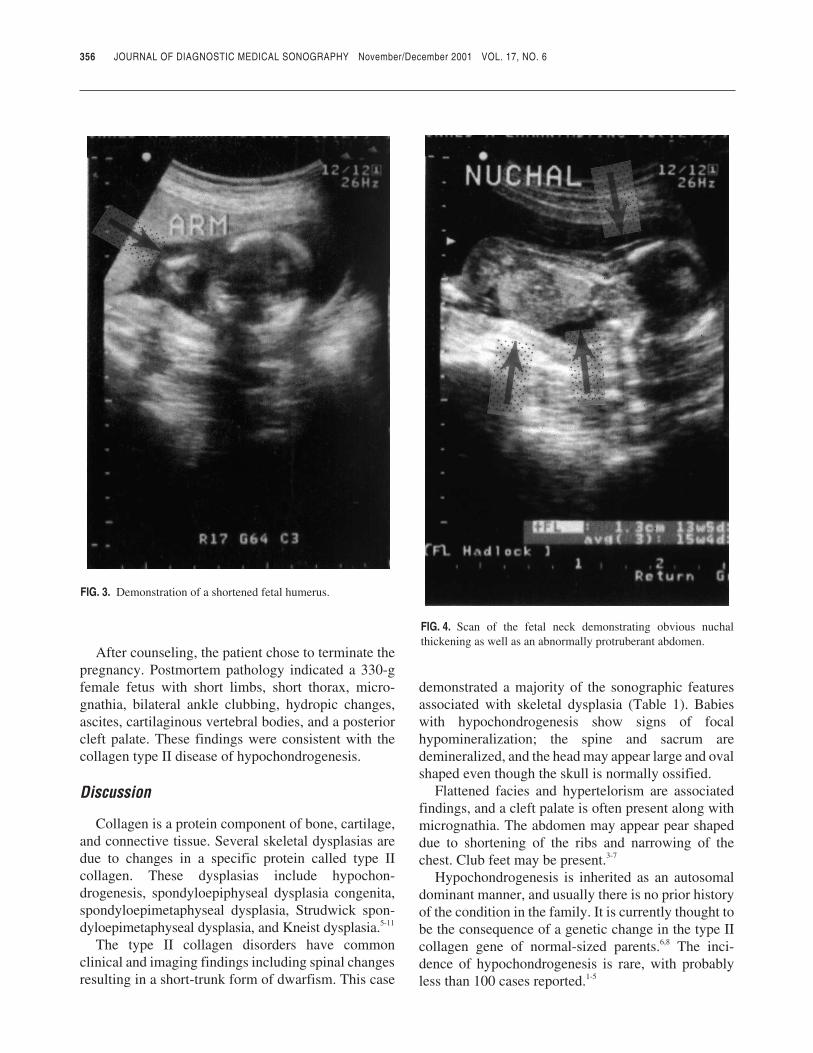
After counseling, the patient chose to terminate thepregnancy. Postmortem pathology indicated a 330-gfemale fetus with short limbs, short thorax, micro-gnathia, bilateral ankle clubbing, hydropic changes,ascites, cartilaginous vertebral bodies, and a posteriorcleft palate. These findings were consistent with thecollagen type II disease of hypochondrogenesis.
Discussion
Collagen is a protein component of bone, cartilage,and connective tissue. Several skeletal dysplasias aredue to changes in a specific protein called type IIcollagen. These dysplasias include hypochon-drogenesis, spondyloepiphyseal dysplasia congenita,spondyloepimetaphyseal dysplasia, Strudwick spon-dyloepimetaphyseal dysplasia, and Kneist dysplasia.5-11
The type II collagen disorders have commonclinical and imaging findings including spinal changesresulting in a short-trunk form of dwarfism. This case
demonstrated a majority of the sonographic featuresassociated with skeletal dysplasia (Table 1). Babieswith hypochondrogenesis show signs of focalhypomineralization; the spine and sacrum aredemineralized, and the head may appear large and ovalshaped even though the skull is normally ossified.
Flattened facies and hypertelorism are associatedfindings, and a cleft palate is often present along withmicrognathia. The abdomen may appear pear shapeddue to shortening of the ribs and narrowing of thechest. Club feet may be present.3-7
Hypochondrogenesis is inherited as an autosomaldominant manner, and usually there is no prior historyof the condition in the family. It is currently thought tobe the consequence of a genetic change in the type IIcollagen gene of normal-sized parents.6,8 The inci-dence of hypochondrogenesis is rare, with probablyless than 100 cases reported.1-5
356 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 3. Demonstration of a shortened fetal humerus.
FIG. 4. Scan of the fetal neck demonstrating obvious nuchalthickening as well as an abnormally protruberant abdomen.

HYPOCHONDROGENESIS / Pantaleo et al 357
Early diagnosis of hypochondrogenesis providesthe patient with the option to terminate. Laterdiagnosis is also valuable because it allows the patienttime for counseling and preparation.
Because sonographers are most often the first tovisualize the problem, they must be familiar with thesonographic signs of the anomaly. The importance ofunderstanding the gestational age at which charac-teristics of the disorder may present and the necessityof careful long-bone measurements cannot beoverstated. Each fetal limb should be imaged andmeasured during routine obstetrical sonographicexaminations. Sonographers need to be alert to the factthat true bowing of a limb or artifactual shadowingfrom overlying limbs may give the appearance of ashortened long bone. The presence of abnormalmineralization may result in a reduction in echo-genicity of the bone. The reduced echogenicity maymake long-bone imaging difficult or may give a falseimpression that the long bones are very thin. Cal-culation of the thoracic circumference/abdominalcircumference ratio is equally important to rule out thepresence of an abnormally narrow thorax. The normalthoracic circumference/abdominal circumference ratiois 0.89.1
Sonographers should routinely check for thepresence of other associated abnormalities including
polyhydramnios, polydactyly, club foot, abnormalnuchal thickening, cleft lip or palate, cardiac defects,and the presence of a two-vessel umbilical cord.
In the hands of skilled operators and interpreters,sonography has proven to be the most accurateimaging modality for the early detection of skeletaldysplasias.
References
1. Bader-Armstrong B: Normal and abnormal fetal limbs, inBerman MC, Cohen HL (eds): Diagnostic MedicalSonography: A Guide to Clinical Practice. 2nd ed.Philadelphia, PA, Lippincott-Raven Publishers, 1997, pp345–358.
2. Nolan RL: The fetal musculoskeletal system, in Sauerbrii EE(ed): A Practical Guide to Ultrasound in Obstetrics andGynecology. Philadelphia, PA, Lippincott-Raven Publishers,1998, pp 349–376.
3. Mahoney BS: Ultrasound evaluation of the fetal musculo-skeletal system, in Callen PW (ed): Ultrasonography inObstetrics and Gynecology. 3rd ed. Philadelphia, PA, WBSaunders Company, 1994, pp 264–269.
4. Sanders RC: Structural Fetal Abnormalities: The TotalPicture. St Louis, MO, Mosby-Year Book Inc, 1996, pp 163–165.
5. Jeanty P, Silva S: Achondrogenesis. June 17, 1999. Availableat: http://www.thefetus.net. Accessed February 28, 2001.
6. Wertelecki W: Hypochondrogenesis, WED, SEMD, Kneistsyndrome. March 12, 2000. Available at: http://www.ibisbirthdefects.org. Accessed March 16, 2001.
7. Chen H: Achondrogenesis, in Pediatrics/Genetics andMetabolic Disease. December 10, 2000. Available at: http://www.emedicine.com. Accessed March 16, 2001.
8. Korkko J, Cohn DH, Ala-Kokko L, et al: Widely distributedmutations in the COL2A1 gene produce achondrogenesistype II/hypochondrogenesis. Am J Med Genet 2000;92:95–100.
9. Soothill PW, Vuthiwong C, Rees H: Achondrogenesis type 2diagnosed by transvaginal ultrasound at 12 weeks gestation.Prenat Diagn 1993;13:523–528.
10. Spranger J, Winterpacht A, Zabel B: The type IIcollagenopathies: a spectrum of chondroplasias. Eur JPediatr 1994;153:56–65.
11. Whitley CB, Gorlin RJ: Achondrogenesis: new nosology withevidence of genetic heterogeneity. Radiology1983;148:693–698.
TABLE 1Sonographically Visible Features Strongly Associated WithLethal Skeletal Dysplasia
Abnormal calvariumAbnormal spineShortened long bonesSmall thoraxHypomineralizationMultiple fracturesPolydactylyNonimmune hydropsPolyhydramniosAbnormal posturing or immobility
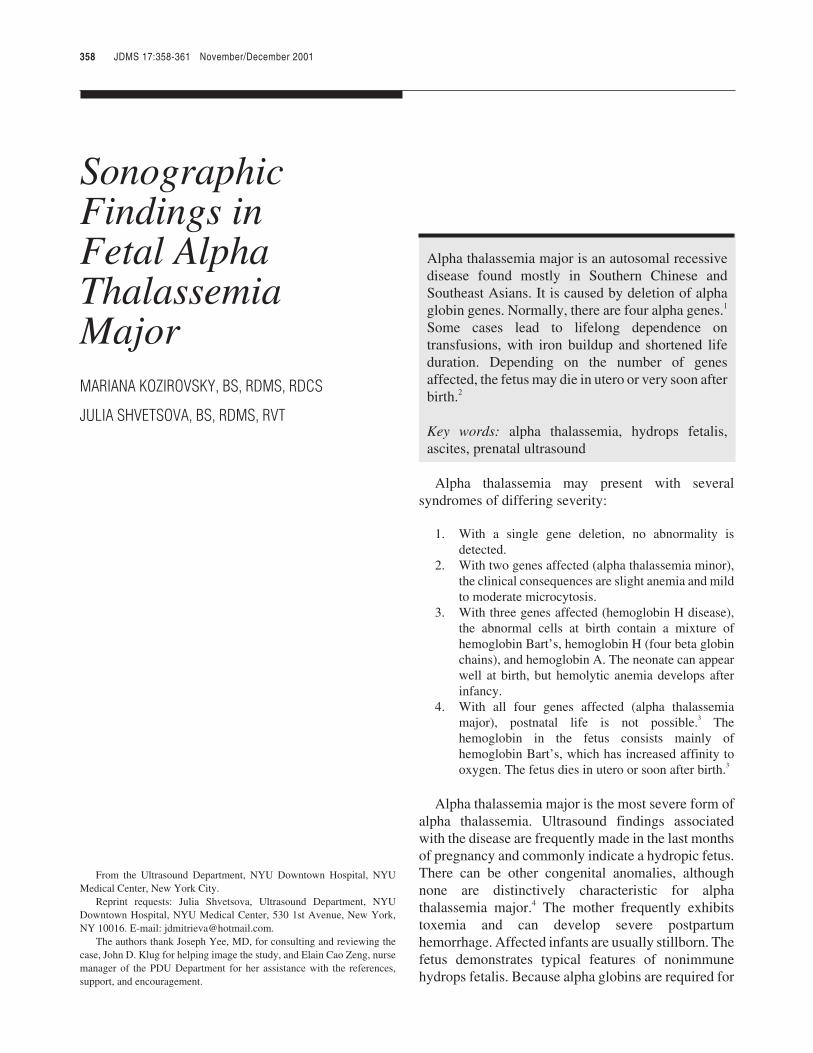
JDMS 17:358-361 November/December 2001
JDMS 17:358-361 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FETAL ALPHA THALASSEMIA MAJOR / Kozirovsky, Shvetsova
SonographicFindings inFetal AlphaThalassemiaMajorMARIANA KOZIROVSKY, BS, RDMS, RDCS
JULIA SHVETSOVA, BS, RDMS, RVT
Alpha thalassemia major is an autosomal recessivedisease found mostly in Southern Chinese andSoutheast Asians. It is caused by deletion of alphaglobin genes. Normally, there are four alpha genes.1
Some cases lead to lifelong dependence ontransfusions, with iron buildup and shortened lifeduration. Depending on the number of genesaffected, the fetus may die in utero or very soon afterbirth.2
Key words: alpha thalassemia, hydrops fetalis,ascites, prenatal ultrasound
Alpha thalassemia may present with severalsyndromes of differing severity:
1. With a single gene deletion, no abnormality isdetected.
2. With two genes affected (alpha thalassemia minor),the clinical consequences are slight anemia and mildto moderate microcytosis.
3. With three genes affected (hemoglobin H disease),the abnormal cells at birth contain a mixture ofhemoglobin Bart’s, hemoglobin H (four beta globinchains), and hemoglobin A. The neonate can appearwell at birth, but hemolytic anemia develops afterinfancy.
4. With all four genes affected (alpha thalassemiamajor), postnatal life is not possible.3 Thehemoglobin in the fetus consists mainly ofhemoglobin Bart’s, which has increased affinity tooxygen. The fetus dies in utero or soon after birth.3
Alpha thalassemia major is the most severe form ofalpha thalassemia. Ultrasound findings associatedwith the disease are frequently made in the last monthsof pregnancy and commonly indicate a hydropic fetus.There can be other congenital anomalies, althoughnone are distinctively characteristic for alphathalassemia major.4 The mother frequently exhibitstoxemia and can develop severe postpartumhemorrhage. Affected infants are usually stillborn. Thefetus demonstrates typical features of nonimmunehydrops fetalis. Because alpha globins are required for
358 JDMS 17:358-361 November/December 2001
From the Ultrasound Department, NYU Downtown Hospital, NYUMedical Center, New York City.
Reprint requests: Julia Shvetsova, Ultrasound Department, NYUDowntown Hospital, NYU Medical Center, 530 1st Avenue, New York,NY 10016. E-mail: [email protected].
The authors thank Joseph Yee, MD, for consulting and reviewing thecase, John D. Klug for helping image the study, and Elain Cao Zeng, nursemanager of the PDU Department for her assistance with the references,support, and encouragement.
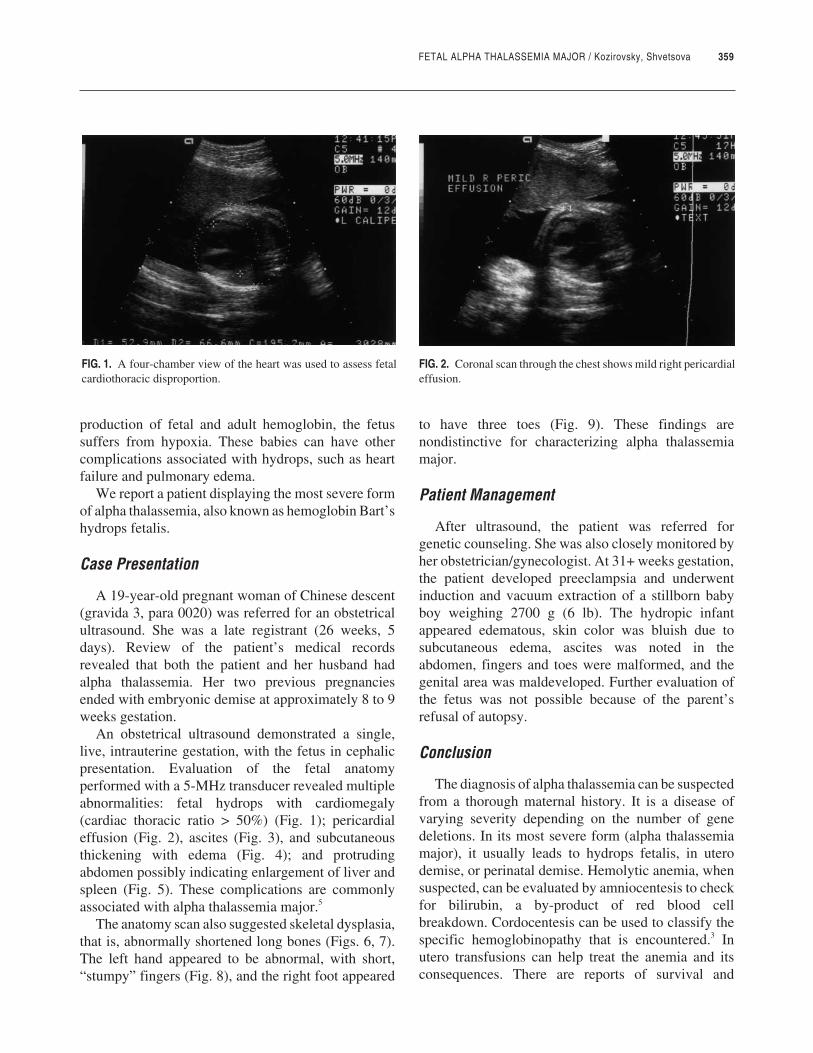
FETAL ALPHA THALASSEMIA MAJOR / Kozirovsky, Shvetsova 359
production of fetal and adult hemoglobin, the fetussuffers from hypoxia. These babies can have othercomplications associated with hydrops, such as heartfailure and pulmonary edema.
We report a patient displaying the most severe formof alpha thalassemia, also known as hemoglobin Bart’shydrops fetalis.
Case Presentation
A 19-year-old pregnant woman of Chinese descent(gravida 3, para 0020) was referred for an obstetricalultrasound. She was a late registrant (26 weeks, 5days). Review of the patient’s medical recordsrevealed that both the patient and her husband hadalpha thalassemia. Her two previous pregnanciesended with embryonic demise at approximately 8 to 9weeks gestation.
An obstetrical ultrasound demonstrated a single,live, intrauterine gestation, with the fetus in cephalicpresentation. Evaluation of the fetal anatomyperformed with a 5-MHz transducer revealed multipleabnormalities: fetal hydrops with cardiomegaly(cardiac thoracic ratio > 50%) (Fig. 1); pericardialeffusion (Fig. 2), ascites (Fig. 3), and subcutaneousthickening with edema (Fig. 4); and protrudingabdomen possibly indicating enlargement of liver andspleen (Fig. 5). These complications are commonlyassociated with alpha thalassemia major.5
The anatomy scan also suggested skeletal dysplasia,that is, abnormally shortened long bones (Figs. 6, 7).The left hand appeared to be abnormal, with short,“stumpy” fingers (Fig. 8), and the right foot appeared
to have three toes (Fig. 9). These findings arenondistinctive for characterizing alpha thalassemiamajor.
Patient Management
After ultrasound, the patient was referred forgenetic counseling. She was also closely monitored byher obstetrician/gynecologist. At 31+ weeks gestation,the patient developed preeclampsia and underwentinduction and vacuum extraction of a stillborn babyboy weighing 2700 g (6 lb). The hydropic infantappeared edematous, skin color was bluish due tosubcutaneous edema, ascites was noted in theabdomen, fingers and toes were malformed, and thegenital area was maldeveloped. Further evaluation ofthe fetus was not possible because of the parent’srefusal of autopsy.
Conclusion
The diagnosis of alpha thalassemia can be suspectedfrom a thorough maternal history. It is a disease ofvarying severity depending on the number of genedeletions. In its most severe form (alpha thalassemiamajor), it usually leads to hydrops fetalis, in uterodemise, or perinatal demise. Hemolytic anemia, whensuspected, can be evaluated by amniocentesis to checkfor bilirubin, a by-product of red blood cellbreakdown. Cordocentesis can be used to classify thespecific hemoglobinopathy that is encountered.3 Inutero transfusions can help treat the anemia and itsconsequences. There are reports of survival and
FIG. 1. A four-chamber view of the heart was used to assess fetalcardiothoracic disproportion.
FIG. 2. Coronal scan through the chest shows mild right pericardialeffusion.
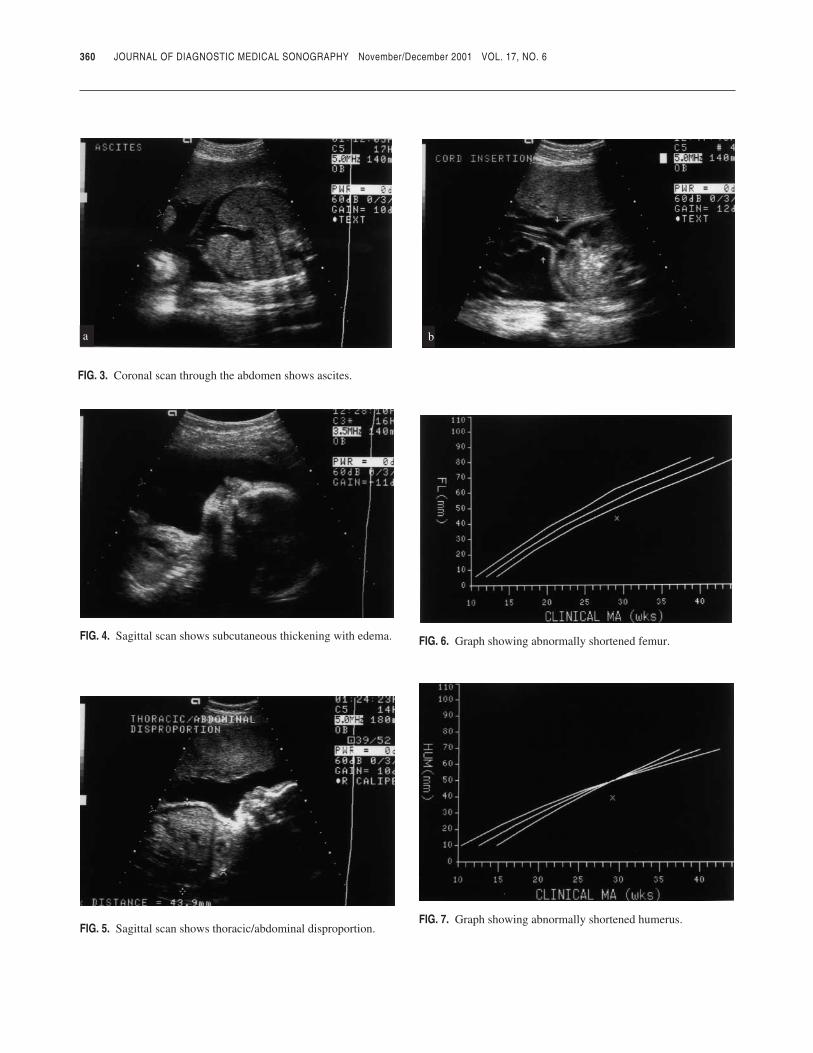
360 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 4. Sagittal scan shows subcutaneous thickening with edema.
FIG. 3. Coronal scan through the abdomen shows ascites.
FIG. 5. Sagittal scan shows thoracic/abdominal disproportion.
FIG. 6. Graph showing abnormally shortened femur.
FIG. 7. Graph showing abnormally shortened humerus.
a b
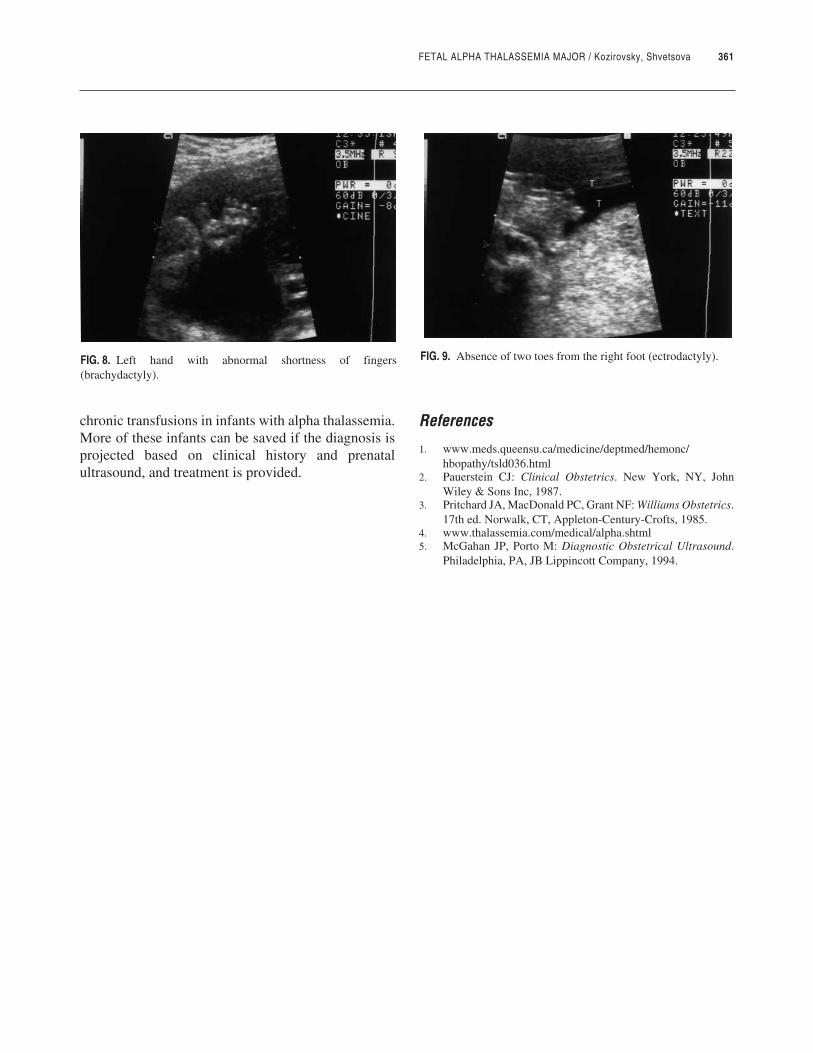
FETAL ALPHA THALASSEMIA MAJOR / Kozirovsky, Shvetsova 361
chronic transfusions in infants with alpha thalassemia.More of these infants can be saved if the diagnosis isprojected based on clinical history and prenatalultrasound, and treatment is provided.
References
1. www.meds.queensu.ca/medicine/deptmed/hemonc/hbopathy/tsld036.html
2. Pauerstein CJ: Clinical Obstetrics. New York, NY, JohnWiley & Sons Inc, 1987.
3. Pritchard JA, MacDonald PC, Grant NF: Williams Obstetrics.17th ed. Norwalk, CT, Appleton-Century-Crofts, 1985.
4. www.thalassemia.com/medical/alpha.shtml5. McGahan JP, Porto M: Diagnostic Obstetrical Ultrasound.
Philadelphia, PA, JB Lippincott Company, 1994.
FIG. 8. Left hand with abnormal shortness of fingers(brachydactyly).
FIG. 9. Absence of two toes from the right foot (ectrodactyly).
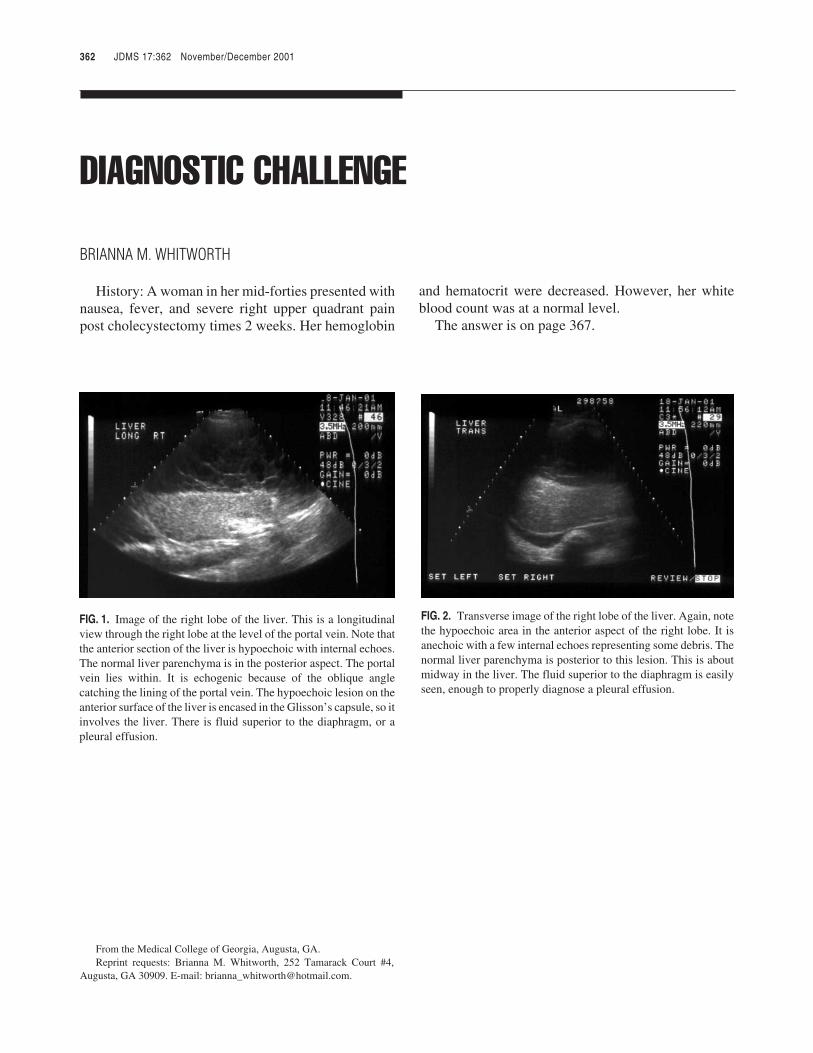
JDMS 17:362 November/December 2001
JDMS 17:362 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
DIAGNOSTIC CHALLENGE / Whitworth
DIAGNOSTIC CHALLENGE
BRIANNA M. WHITWORTH
History: A woman in her mid-forties presented withnausea, fever, and severe right upper quadrant painpost cholecystectomy times 2 weeks. Her hemoglobin
and hematocrit were decreased. However, her whiteblood count was at a normal level.
The answer is on page 367.
362 JDMS 17:362 November/December 2001
From the Medical College of Georgia, Augusta, GA.Reprint requests: Brianna M. Whitworth, 252 Tamarack Court #4,
Augusta, GA 30909. E-mail: [email protected].
FIG. 1. Image of the right lobe of the liver. This is a longitudinalview through the right lobe at the level of the portal vein. Note thatthe anterior section of the liver is hypoechoic with internal echoes.The normal liver parenchyma is in the posterior aspect. The portalvein lies within. It is echogenic because of the oblique anglecatching the lining of the portal vein. The hypoechoic lesion on theanterior surface of the liver is encased in the Glisson’s capsule, so itinvolves the liver. There is fluid superior to the diaphragm, or apleural effusion.
FIG. 2. Transverse image of the right lobe of the liver. Again, notethe hypoechoic area in the anterior aspect of the right lobe. It isanechoic with a few internal echoes representing some debris. Thenormal liver parenchyma is posterior to this lesion. This is aboutmidway in the liver. The fluid superior to the diaphragm is easilyseen, enough to properly diagnose a pleural effusion.

JDMS 17:363-366 November/December 2001
JDMS 17:363-366 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FOCUSING ON THE ISSUES / Craig
FOCUSING ON THE ISSUES
A Gathering ofAngelsMARVEEN CRAIG, RDMS
There was no premonition, no bolt from the blue,when sonographer Sandra Karol awoke that Februaryday. It was simply a day off, to be used to indulgeoneself; a day to be enjoyed. All of that was about tochange as she tuned into a program about Project V-Day, dedicated to stopping violence against women byempowering them. Viewers were urged to think abouthow they could use their lives to end the pain andsuffering being endured by women throughout theworld.
Long after the program ended, Sandy couldn’t stopthinking about what she could do to help. She foundherself looking around and taking stock of her life. Shehad everything she needed: a loving family, goodfriends, and a satisfying ultrasound career. All in all, itwas a very comfortable life. But, a question promptedby the television show kept intruding on her thoughts.What could one lone person do? She recalled the earlydays of her career, when she had volunteered to go toAfrica under the auspices of Africare. Even afterpolitical instability and the ensuing violence in theregion forced her to put that dream on hold, she felt aspecial bond with Africa. Random thoughts tumbledthrough her mind well into the night, but by morningshe began putting them down on paper. She listed whatshe, as an individual, might offer to such a project. Shepossessed a knowledge and love of ultrasound, time,energy, and a desire to help. Slowly, a new thoughtbegan to take form, and by midday she had formulateda plan.
When my phone rang that day, I had no idea that Iwas about to become a recruit. The caller was myfriend, Sandy Karol. After we exchanged pleasantries,she asked me what I knew about Project V-Day. “Not awhole lot,” I said. “I know what it stands for. Why?”
“Because, I’m interested in getting involved and I’dlike to run an idea by you. I’ve decided that I want tosend a portable ultrasound unit to Africa. In order tomake that happen, I figure I need to accomplish fourthings: secure an ultrasound unit, find someone whoneeds and will use it, find a sonographer to provide
JDMS 17:363-366 November/December 2001 363

training, and come up with round-trip travel to Africa.What do you think? Is it doable?”
I recall feeling a little skeptical, but not wanting todiscourage her completely, I answered cautiously,“Well, anything is possible . . . but this sounds like amajor undertaking. Are you willing to invest the timeand energy necessary to actually pull it off? Do youhave any resources or even a plan?”
“Yes to the first, no to the second, and, sort of,” shereplied. “I contacted someone at Project V-Day andwas referred to several women’s groups andhumanitarian organizations. They all thought the ideawas terrific, but it just isn’t the sort of thing that theyare equipped to do.”
“That’s not surprising, Sandy. Think of all thebureaucracy that exists in large organizations. Theremust be hundreds of stumbling blocks. If your goal isto get aid to the people who need it, you would bebetter off dealing with them directly. Last year, I wroteabout two sonographers from New York who went toteach in Africa for a month, and I know of anothersonographer who is there right now developing aneducational program. Why not contact them to see ifthey have any ideas or advice?”
The conversation ended after she had taken downthe sonographers’ contact information, and I hadpolitely asked her to keep me informed. I put thematter on my mental back burner, convinced that itwould be some time before I would be hearing fromSandra Karol again.
I couldn’t have been more wrong. Sandy phoned ore-mailed me daily to report on her activities or plans,and to occasionally ask for information or opinionsabout her progress. And, what progress she made! Shebegan her crusade with a campaign of phone calls,faxes, and e-mails. She seemed able to interest andrecruit almost everyone she contacted into a rapidlygrowing network of corporate, professional,sonographer, and lay volunteers. With every call, shereceived encouragement and often referrals tosomeone else who might be able to help her.
Acting on my earlier advice, Sandy contacted AnnPolin in Ghana and heard firsthand about theultrasound program she had developed. Ann gave hermany insights and also mentioned the need to findother sonographers who would be willing to take herplace when her year in Ghana was up. She then spokewith Kathy Velekkakan and Barbara Rosenberg inNew York. Sandy sounded elated when she reported
that they were delighted with the prospect of returningto Africa. With the encouragement of their familiesand employers, the two sonographers had quicklyarranged to spend their vacations delivering theequipment and providing 30 days of instruction.
Incredibly, another problem was solved whenKathy Velekkakan suggested that the MedicalMissionaries of Mary might be good candidates for theequipment. Sandy wasted no time in making thatcontact and learned that the organization maintained60 missions in 14 different countries, Africa amongthem. The nun she spoke with could hardly believe theoffer and assured her that the community would bevery grateful for such a magnificent gift. So it was, thatin less than a week, half of the necessary goals hadbeen achieved.
Karol then turned her attention to finding someonewilling to provide ultrasound equipment. From theoutset, she was convinced that a hand-held ultrasoundunit was essential. On the strength of that conviction,she dubbed the project Hand-Held Africa. Then,always starting at the top of the corporate ladder, sheplaced calls to several manufacturers, including KevinGoodwin, CEO of SonoSite Inc. in Seattle.
To her amazement, her call was put through and shefound herself explaining the nature of her call and herrequest. Goodwin listened patiently as she describedthe special requirements she thought the setting calledfor, describing the rigors of transportation by jeep overdusty, almost nonexistent roads. She stressed the needfor a battery backup because of the unreliability ofpower in the remote areas of the country. Goodwin,undaunted by the parameters she had specified, agreedto consider her request and asked her to send him anoverview of the project.
In her reply, Sandy described how very differentlythe many organizations that constituted the Project V-Day coalition were addressing the problems ofviolence toward women. Whereas one organizationgave Afghanistani women video cameras to film thebrutality to which they are subjected; another givescattle to women or villages as a means of increasingthe status of women and to hopefully avoid spousalbeatings. She later shared that correspondence withme, and I was particularly impressed with her closingargument:
Little and big things move mountains! My project issimply a way of “giving something back” for thescholarship that brought me into ultrasound. I know
364 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6

FOCUSING ON THE ISSUES / Craig 365
and love ultrasound—especially obstetricalsonography and its ability to save the lives of bothmother and child. That’s it. Period.I’ve gathered an angel network to help me find anddeliver a very simple one-to-one donation to severalhard-working nuns in a small village in Tanzania.With your help, they could see 100 patients a week,100 babies a week . . . perhaps as many as 5000women per year!
In mid-April, SonoSite adopted the role of corporate“angel” with its promise of a SonoSite 180 to theHand-Held Africa project.
To overcome the hurdle of transportation, Sandybrainstormed with her growing network. Several ideaswere proposed, such as identifying firms that didbusiness in Africa to see whether they would allow oursonographers to “hitch a ride” on their corporate jets.Another thought was to ask for the donation offrequent flier miles from members of the ultrasoundcommunity. The final suggestion involved identifyingthose airlines that provided regular service to Africaand exploring the possibility that they would bewilling to provide the transportation as a humanitariangesture. As luck would have it, one of Sandy’s closefriends mentioned that British Airways providedregular service to Africa. She placed a call, and withina matter of days John Lampl at the New York office ofBritish Airways agreed to check on the matter. Herrequest was granted and confirmed, with a promise toprovide round-trip tickets from New York to Africawhenever our sonographers wished to travel.
In only 60 days, Sandy Karol had accomplished thegoals necessary to make Hand-Held Africa a reality.From the beginning, everyone who heard about theplan reacted positively. The spread of the news byword of mouth resulted in complete strangerscontacting her to offer advice, opinions, and services.One of Sandy’s friends, a private duty nurse in Florida,discussed the project with a patient. That man,Geoffrey Hurt, contacted Sandy with concerns aboutthe need to frequently recharge the ultrasound unit’slithium batteries using a gas-powered generator. Heproposed the less-expensive alternative of using solarpower instead, and offered his engineering talents ifrequired. Ben Deeley, the SonoSite salesrepresentative for North Carolina, mentioned theproject to a friend who had developed a compressionprogram for use on the Internet. His friend hasvolunteered his services as a consultant to make it
possible to send the African-generated real-timeimages to any interpretive team or sister hospital backin the United States. A number of sonographers whohave heard about the project have contacted Sandy andvolunteered to staff any future projects, wherever theymight be. To date, 27 “angels” have gathered to ensurethat Hand-Held Africa successfully launches inJanuary 2002. And in so doing, they have provided theproof that, indeed, anything is possible.
As I began collecting information for this story, Icontacted Kathy Velekkakan and Barbara Rosenbergto get some impressions about their upcomingadventure. Kathy commented:
We are going to Kabanga Hospital in NorthwesternTanzania, close to Lake Tanganyika,” said Kathy.“We will be working with Dr. Nuru, a Tanzaniandoctor, and an as-yet-unnamed nurse practitioner.This 155-bed hospital serves the Waha tribe, whospeak Kiha and Kiswahili. In addition, because of aninflux of refugees from Burundi and the Congo(formerly Zaire), the Akgoma Hospital has set up aclinic at a United Nations refugee camp. Having asmall, portable ultrasound unit will be very helpful inthis clinic.
I’m so happy to be going back to Africa. When wereturned home after our first trip two years ago, webegan looking for another opportunity to serve. TheMedical Missionaries of Mary is family to me, andhaving the chance to return, this time to one of theirhospitals, is like serving your sister or your mother. Iam currently an associate member of theorganization. . . . Associate members are individualswho have a close commitment to the community, butwho do not take vows.
Twenty-five years ago, as a young woman, Ientered this community hoping to make my vows andstay for a lifetime. Hand-Held Africa represents thefirst time in all of those years that I will have a chanceto fulfill that original call. Now that I’m a wife andmother, I’d like my family to feel our responsibilitytowards the world and our sisters and brothers inplaces where there is so much need.
The other half of the sonographer team, Barbara,had this to say:
I can’t believe that I’m actually going to have theopportunity to travel to Africa again. Our experiencethere last time was truly life changing. We even hopeto be able to see our Kenyan friends, since Tanzania isright next door to Kenya. But I have to keep remindingmyself that those are countries, not states, and the

366 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
distances are very great in Africa, not to mention thelogistics of travel and lodging.
This new adventure will be different from the last,in that the conditions are going to more primitive thanbefore. In Kenya, we were still near city amenitiessuch as automobiles, stores, and an airport. I don’tthink that will be the case where we’re going inTanzania. It is not in an area frequented by tourists, asit is somewhat inaccessible. I’m going into thisventure a little more informed than last time, but thatjust means I’m expecting more surprises, and Iunderstand that I must learn to just go with whatevercomes along.
We plan to take some reference books with us forthe hospital. I really feel that the books will beindispensable, not only for our students but for us too,since I know we will see things in their patients thatwe have never encountered in upstate New York.
I also checked in with Sandra Karol to find out whatshe and her “angels” were going to do with all of theirfree time:
Hand-Held Africa is pretty much in a holding patternuntil January. I don’t know about the rest of my angel
team, but as I look back on what we accomplished,I’m still amazed at how everything came together soquickly.
I recently found out that the Medical Missionariesof Mary have several missions in Brazil. Now that wehave such a large network and have some experienceunder our belts, I’ve been thinking . . . A for Africa, Bfor Brazil. Do you think it’s doable?
During the course of her odyssey, many people haveasked Sandra Karol why she decided to tackle such aproject. She always gives this reply:
My inspiration is Mother Teresa, who was only 4 feet,11 inches tall. She worked in the mud. She neverasked for a dime, but she changed the world, one gooddeed at a time.
Correspondence: Marveen Craig, 11510 NorthCharoleau Drive, Tucson, AZ 85737. E-mail:[email protected].

ANSWER TO DIAGNOSTIC CHALLENGE 367
ANSWER TO DIAGNOSTIC CHALLENGE
Answer to Diagnostic Challenge
Subcapsular hematoma on the anterior surface of the liver
Postoperative complications are rare following a cholecystectomy. However, they do occur occasionally.The complications include common bile duct injury, retained cystic duct stones, hepatic artery injury, andfluid collection due to an abscess or hematoma. A small area of the liver can be punctured, which causes apooling of blood within the capsule of the liver. The patient’s severe pain was due to the pooled blood thatstretched the Glisson’s capsule that surrounds the liver. The hypoechoic area measured 8 × 15 × 22 cm. Thecommon hepatic and common bile ducts measured within normal limits. The surrounding liver parenchymawas of normal echogenicity. This focal lesion may be confused with a biloma, hematoma, or an abscess. Abiloma is a collection of bile outside of the ductal system. It can appear as upper abdominal fluid that hascollected. An abscess is an area of infection and can cause a fluid buildup in an area. An abscess usuallycauses the white blood cell count to increase because of the infection, but this patient had a normal whiteblood cell count. We still cannot rule it out. A hematoma is a pooling of blood in an area that can be septateddue to blood coagulation and the blood settling. Fresh blood appears anechoic and becomes more echogenicas it ages. Hematomas can also appear anechoic with aging.
In this patient, sonography could not provide a definitive diagnosis. The primary method of confirmationof a hematoma is to drain the lesion and examine the material. The patient underwent aspiration of the areaunder computed tomography the following day after the ultrasound. With a guidewire and drainage catheterplacement, the area was drained. A 14-French drain 100 cc of old-blood-appearing fluid was removed with alarge amount of fibrinous material within. The fluid was not sent for lab tests. This material’s appearanceconfirmed that it was a hematoma. If the area had been a biloma, the fluid would have been a greenish color.Had the area been an abscess, the fluid would have had a thick pus appearance. The punctured area healed,the pain was relieved, and the patient had no other complications.

JDMS 17:368 November/December 2001
JDMS 17:368 November/December 2001
LETTER TO THE EDITOR
The case study titled “Pyomyositis: A DifferentialDiagnosis for Venous Thrombosis” (Journal ofDiagnostic Medical Sonography 2001;17:258–262)was interesting from a clinical perspective butcontained some significant technical errors thatescaped the author’s attention. Figure 1, captioned“Doppler signal taken from dorsalis pedis arterydemonstrating normal flow,” is a split-screen imageshowing a center-steered color box and Dopplersample volume placed perpendicular relative to theplane of the dorsalis pedis artery and vein. The spectralwaveform shows what appears to be a low velocity,low resistance arterial waveform that the authorinterpreted as normal flow. I have two concerns withthis presentation.
First, although the ultrasound beam (samplevolume) angle is labeled as 60° to the artery on theimage, the true angle is clearly closer to 90°. Thisextremely steep beam-to-vessel angle produced a verypoor (low) frequency shift that significantly reducedthe system’s sensitivity to (1) detect low-flow statesand (2) display subtle but diagnostically importantvelocity information. The erroneously displayedsample volume angle of 60° adds to the measurementerror, resulting in an artificially low arterial velocity. Ifthe sample volume had truly been adjusted to a 60°angle, the cursor “wings” would have been alignedparallel to the vessel walls. Clearly, this imageconfirms that the angle adjustment cursor is notaligned parallel to the arterial wall.
Second, the arterial waveform is labeled as “normalflow” when, in reality, the waveform does notrepresent a normal dorsalis pedis artery velocitypattern; nor can we determine whether the flow state isnormal. The word flow implies “volume flow.” Bloodflow velocity and volume flow are not the samemeasurement. The relatively high diastolic flowvelocity implied by the spectral display would suggestmore of a hyperemic state, which is abnormal for apedal artery. Unfortunately, the 90° sample volume
angle “desensitized” the frequency shift to the pointwhere one cannot accurately determine whether amore high-resistant, “normal,” reverse flow com-ponent exists. It is logical to assume that the patientcould have vascular hyperemia secondary to theinitially diagnosed hypervascular mass and staphylo-coccus aureus infection. Therefore, a relatively highend-diastolic (low-resistance) velocity would beexpected.
Misplacement and misalignment of the samplevolume relative to the orientation of the blood vessel isthe most common source of diagnostic error invascular sonography. The high precision required toaccurately detect and analyze both normal andcomplex pathological vascular disease states makes itimperative that the sonographic practitionerunderstand the pitfalls of Doppler beam steering andangle-related velocity estimate errors. It is unfortunatethat the angle placement error also escaped theeditorial review process.
Miles M. Cramer, BS, RVT, FSVT
Seattle, Washington
368 JDMS 17:368 November/December 2001
JDMS 17:369-371 November/December 2001
JDMS 17:369-371 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
SUBJECT INDEX
Subject IndexAdrenal pathology, during pregnancy, 104Alpha thalassemia major, sonographic findings in fetal
alpha thalassemia major, 358Aortic insufficiency etiology, echocardiography role and,
59Atrioventricular valves, pseudoreversal of values E and A
points, 34
Bony disorders, use of sonography in the detection of bonyand calcific disorders of the shoulder, 331
Brachial artery occlusion, ultrasound diagnosis of, 217Breast ultrasound, coded harmonics in, 22
Calcific disorders, use of sonography in the detection ofbony and calcific disorders of the shoulder, 331
Carotid anomaly, carotid anomaly in a patient with Holt-Oram Syndrome, 347
Case studiesadrenal pathology during pregnancy, 104antenatal diagnosis of short umbilical cord syndrome,
253atrioventricular valves pseudoreversal of values E and A
points, 34brachial artery occlusion ultrasound diagnosing, 217carotid anomaly in a patient with Holt-Oram Syndrome,
347hepatic hemangioma prenatal diagnosing, 99hydrometrocolpos prenatal diagnosis of, 220hypochondrogenesis: a rare lethal skeletal dysplasis, 354malpositioned pacemaker lead through ultrasound diag-
nosis, 172Monckeberg’s arteriosclerosis of liver and spleen
demonstrated by ultrasound, 225pulmonary sequestration subdiaphragmatic extralobar,
41pyomyositis: a differential diagnosis for venous throm-
bosis, 258self-inflicted orchiectomy, hematoma mimicking rup-
tured testis, 175sonographic appearance of Klippel-Trénaunay-Weber
syndrome diagnosed at 18 weeks gestation, 342sonographic evaluation of intraocular cysticercosis, 339sonographic findings in fetal alpha thalassemia major,
358thoracic-abodominal aortic dissection as incidental renal
hypertension ultrasound finding, 230ultrasound evaluation and clinical management of
persistent gestational sac in a cervical ectopicpregnancy, 350
uterine fibroid embolization, pre and postembolization,167
velamentous cord insertion with vasa previa, 94Circulation pathways, conceptual understanding of, 234Cloaca, prenatal diagnosis of hydrometrocolpos, 220Coded harmonics, breast ultrasounds and, 22Critical thinking, creative sonography projects integrated
with critical thinking, 290Cysticercosis, sonographic evaluation of intraocular
cysticercosis, 339
Diagnostic challenges, 46, 108, 179, 303, 362
Echocardiographers, musculoskeletal pain reducing bystretch exercises, 123
Echocardiographyaortic insufficiency etiology and, 59natural history and, 59pathophysiology and, 59
Ectopic pregnancy, ultrasound evaluation and clinicalmanagement of persistent gestational sac in acervical ectopic pregnancy, 350
Editorial, standards for assurance of minimum entry-levelcompetence for the diagnostic ultrasound profes-sion, 307
Educationconstructivist classroom creativity, 109creative sonography projects integrated with critical
thinking, 290creativity fostering in Allied Health settings, 181fetal cardiac anatomy and circulation pathways concep-
tual understandings, 234Erratum, 122Extensor tenosynovitis, sonographic evaluation of extensor
tenosynovitis, 275Extralobar pulmonary sequestration, 41
Fetalanomalies three-dimensional ultrasound visualization,
88cardiac anatomy conceptual understanding of, 234heart valves pseudoreversal of valves E and A points, 34hepatic hemangioma prenatal diagnosis, 99
sonographic appearance of Klippel-Trénaunay-Weber syndrome diagnosed at 18 weeksgestation, 342
sonographic findings in fetal alpha thalassemia major,358
three-dimensional head sonography, 74
JDMS 17:369-371 November/December 2001 369
Fetal mortality, hydrops fetalis in a documented parvovirusinfection causing fetal mortality, 271
Finger, middle finger’s flexor tendons measurement anddata reproducibility, 211
Gallstones, gallstone ileus, 268Gestational sac, ultrasound evaluation and clinical
management of persistent gestational sac in acervical ectopic pregnancy, 350
Hematoma, mimicking ruptured testis after self-inflictedorchiectomy, 175
Hernia, prenatal ultrasonographic diagnosis on congenitaldiaphragmatic hernia at 11 weeks gestation, 286
Hip dysplasia, infant hip developmental evaluation, 162Holt-Oram Syndrome, carotid anomaly in a patient with
Holt-Oram Syndrome, 347Hydrometrocolpos, prenatal diagnosis of, 220Hypertension, portal hypertension review, 193Hypochondrogensis, a rare lethal skeletal dysplasis, 354
Infants, hip developmental dysplasia evaluation, 162Internet
ARDMS linking with registrants, 250OBGYN.NET and sonography, 120The Fetus.Net, 294
Intraocular cysticercosis, sonographic evaluation of intra-ocular cysticercosis, 339
Intravenous contrast agents, renal pathology evaluating, 29
Klippel-Trénaunay-Weber syndrome, sonographic appearanceof Klippel-Trenaunay-Weber syndrome diagnosedat 18 weeks gestation, 342
Letters to editor, 304, 368Liver, Monckeberg’s arteriosclerosis as ultrasound demon-
stration, 225
Monckeberg’s arteriosclerosis, liver and spleen ultrasounddemonstration, 225
Munchausen Syndrome, hematoma mimicking rupturedtestis after self-inflicted orchiectomy, 175
Musculoskeletal pain, stretch exercises reducing, 123
Natural history, echocardiography’s role, 59Neonatal neurosonography, experiences and benefits, 3
Obstetrics surface rendering, 3-dimensional routine plandeveloping, 16
Occupational overuse syndrome, sonographers andoccupational overuse syndrome: cause, effect, andsolutions, 312
Pacemakers, malpositioned lead through patent foramenovale, 172
Pain, musculoskeletal pain reducing by stretch exercises,123
Patent foramen ovale, pacemaker lead malposition diag-nosis, 172
Pathophysiology, echocardiography’s role, 59Picture archiving and communicating system (PACS),
sonographer’s acceptance of, 80Placenta, a rare case of duplicated placenta and bifurcated
umbilical cord in a Singleton pregnancy, 280Pregnancy
adrenal pathology during, 104a rare case of duplicated placenta and bifurcated
umbilical cord in a Singleton pregnancy, 280clinical management of persistent gestational sac in a
cervical ectopic pregnancy, 350Klippel-Trénaunay-Weber syndrome diagnosed at 18
weeks gestation, 342Prenatal diagnosis
fetal hepatic hemangioma, 99ultrasonographic diagnosis on congenital diaphragmatic
hernia at 11 weeks gestation, 286velamentous cord insertion with vasa previa, 94
Pulmonary sequestration, subdiaphragmatic extralobar, 41Pyomyositis, differential diagnosis for venous thrombosis,
258
Renal hypertension ultrasound, thoracic-abdominal aorticdissection as incidental finding, 230
Renal pathology, evaluations with intravenous contrastagents, 29
SDMS-JDMS CME tests, 329musculoskeletal pain reducing with stretch exercises,
141neonatal neurosonography, 14portal hypertension, 201rotator cuff sonography, 151venous thrombosis diagnosis, 263
Shoulder, use of sonography in the detection of bony andcalcific disorders of the shoulder, 331
Skeletal dysplasis, hypochondrogenesis: a rare lethalskeletal dysplasis, 354
Sonographers, sonographers and occupational overuse syn-drome: cause, effect, and solutions, 312
Sonography issueseditor’s addendum, 190a gathering of angels, 363inspirations, 190mentors praise, 186mentors praising, 241sonographer please, not stenographer, 298sonography abuse, 113sonography’s global village of, 47
Spleen, Monckeberg’s arteriosclerosis as ultrasounddemonstration, 225
Testis, self-inflicted orchiectomy mimicking ruptured testis,175
370 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6

SUBJECT INDEX 371
Thoracic-abdominal aortic dissection, from renalhypertension ultrasound, 230
Tibial tendon injury, coded harmonic imaging in theevaluation of posterior tibial tendon injury, 265
Ultrasonographic diagnosis, prenatal ultrasonographicdiagnosis on congenital diaphragmatic hernia at 11weeks gestation, 286
Ultrasound departments, PACS acceptance in, 80Umbilical cord, a rare case of duplicated placenta and
bifurcated umbilical cord in a Singletonpregnancy, 280
Umbilical Cord Syndrome, Antenatal Diagnosis of ShortUmbilical Cord Syndrome, 253
Uterine fibroid embolization, pre- and postembolizationsonographic findings, 167
Vasa previa, prenatal diagnosis of velamentous cordinsertion, 94
Velamentous cord insertion, prenatal diagnosis with vasaprevia, 94
Venous thrombosis, pyomyositis: a differential diagnosisfor venous thrombosis, 258
Women, frail older women’s health, 203World Wide Web. see Internet
JDMS 17:372-373 November/December 2001
JDMS 17:372-373 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
AUTHOR INDEX
Author IndexAndrew, A.: Portal Hypertension: A Review, 193Andrist, L.S., Katz, V.L., Elijah, R., Farmer, R.M.:
Developing a Plan for Routine 3-Dimensional SurfaceRendering in Obstetrics, 16
Andrist, L.S., Katz, V.L., Elijah, R., Farmer, R.M.:Visualization of Fetal Anomalies With Surface 3-Dimensional Ultrasound: A Case Series, 88
Andrist, L.S., Schroedter, W.: Standards for Assurance ofMinimum Entry-Level Competence for the DiagnosticUltrasound Professional, 307
Baier, S.R., Tank, E.S., Watson, P.T.: Persistent Cloaca:Prenatal Diagnosis of Hydrometrocolpos, 220
Bak, D.M., Vest, T., Hodges, S.: SubdiaphragmaticExtralobar Pulmonary Sequestration, 41
Barr, R.G.: see Peterson, C.L.Benson, C.B.: see Smith, A.M.Bieker, T.: see Parks, A.Bierig, S.M., Waggoner, A.D.: Aortic Insufficiency:
Etiology, Pathophysiology, Natural History, and theRole of Echocardiography, 59
Bierig, M.: see Hall, R.
Cervantez, D.M., Roberts, D.L., Hazen, M.J.: HydropsFetalis in a Documented Parvovirus Infection CausingFetal Mortality, 271
Cho, J.Y.: see Kim, M-JChristenssen, W.D.: Stretch Exercises: Reducing the
Musculoskeletal Pain and Discomfort in the Arms andUpper Body of Echocardiographers, 123
Coffin, C.: see Hall, R.Craig, M.: see Pantaleo, J.M.Craig, M.: A Gathering of Angles, 363Craig, M.: In Praise of Mentors: Part One and Two, 186, 241Craig, M.: Sonographer Abuse, 113Craig, M.: Sonographer Please, Not Stenographer, 298Craig, M.: Sonography’s Global Village, 47Cyrethia, M.: see Hale, D.M.
DeLange, M: see Lo, D.Dempsey, R.: Thoracic-Abdominal Aortic Dissection as an
Incidental Finding on a Routine Renal Ultrasound forHypertension, 230
Dobson, J.D.: see Mitchell, C.C.Drose, J.A., Hobbins, J.C., Shaffer, E.M.: Pseudoreversal of
the Atrioventricular Valves E and A Points, 34DuBose, T.J.: OBGYN.net and Sonography, 120DuBose, T.J.: Three-Dimensional Fetal Head, 74Durbin, S.A.: Inspirations, 190
Ehman, D.M.: see Pantaleo, J.M.Elijah, R.: see Andrist, L.S.Evans, K.D.: Farooki, S.: Sonographic Evaluation of
Extensor Tenosynovitis, 275Evans, K.D., Mazzei, L.A., Teaford, M.H.: Removing Some
of the Gray Concerning the Health of Frail OlderWomen, 203
Farmer, R.M.: see Andrist, L.S.Farooki, S.: see Evans, K.D.Forcier, G.L.: see Mauk, V.L.Forgosh, L.B., Poore, R.: Carotid Anomaly in a Patient With
Holt-Oram Syndrome, 347
Grimmer, K.: see Wilkinson, M.Gupta, R.: see Sidhu, R.
Hagen-Ansert, S.: Conceptual Understanding of FetalCardiac Anatomy and Circulation Pathways, 234
Hagen-Ansert, S.: Creative Sonography Projects IntegratedWith Critical Thinking, 290
Hagen-Ansert, S.: Creativity in the ConstructivistClassroom for the Allied Health Student, 109
Hagen-Ansert, S.: Fostering Creativity in the Allied HealthSetting, 181
Hale, D.M., McShane, C.: The Fetus.Net, 294Hall, R., Bierig, M., Coffin, C., Ismail, C., Jones, A.,
Kawamura, D., Persutte, W., Roberts, D., Spitz, J.L.:Ultrasound Practitioner Master’s Degree Curriculum andQuestionnaire Response by the SDMS Membership, 154
Hazen, M.J.: see Cervantez, D.M.Hobbins, J.C.: Drose, J.A.Hodges, S.: see Bak, D.M.Holden, L.B.: Pyomyositis: A Differential Diagnosis for
Venous Thrombosis, 258Holling, A.: Sonography of the Rotator Cuff: An Overview,
144van Holsbeeck, M.: see Leahy, E.Hubacz, D.A.: Sonographic Appearance of Klippel-
Trénaunay-Weber Syndrome Diagnosed at 18 WeeksGestation, 342
Ismail, C.: see Hall, R.
Jakes, C.: Sonographers and Occupational Overuse Syn-drome: Cause, Effect, and Solutions, 312
Jones, A.: see Hall, R.Jones, D.: see Jones, E.D.Jones, E.D., Wallin, S., Jones, D.: Fetal Hepatic Hemangi-
oma: Prenatal Diagnosis, 99
372 JDMS 17:372-373 November/December 2001

AUTHOR INDEX 373
Kabat, M.A.: see Wharton, P.Katz, V.L.: see Andrist, L.S.Kawamura, D.: see Hall, R.Khorasani, R.: see Smith, A.M.Kim, M-J., Cho, J.Y.: Prenatal Ultrasongraphic Diagnosis
of Congenital Diaphragmatic Hernia at 11 WeeksGestation, 286
Kozirovsky, M., Shvetsova, J.: Sonographic Findings inFetal Alpha Thalassemia Major, 358
Leahy, E., van Holsbeeck, M.: Coded Harmonic Imaging inthe Evaluation of Posterior Tibial Tendon Injury, 265
Lo, D., McLeary, M., DeLange, M.: SonographicEvaluation of the Infant Hip for Development Dysplasiaof the Hip, 162
McEvoy, M.: see Reaiche, H.McLeary, M: see Lo, D.Malhotra, S.: see Sidhu, R.Massy-Westropp, N.: see Wilkinson, M.Mauk, V.L., Forcier, G.L.: Ultrasound Evaluation and
Clinical Management of Persistent Gestational Sac in aCervical Ectopic Pregnancy, 350
Mazzei, L.A.: see Evans, K.D.Merton, D.A.: Multiplanar 3-Dimensional Neonatal
Neurosonography: Initial Experiences and PotentialBenefits, 3
Miniard, J.K.: Ultrasound Diagnosis of MalpositionedPacemaker Lead Through a Patent Foramen Ovale, 172
Mitchell, C.C., Yeast, J., Dobson, J.R.: Antenatal Diagnosisof Short Umbilical Cord Syndrome, 253
Moffatt, M.D.: Diagnostic Challenge, 46
O’Brien, J., Sheehan, K.: Prenatal Diagnosis of aVelamentous Cord Insertion Associated With a VasaPrevia, 94
Pantaleo, J.M., Craig, M., Ehman, D.M.: Hypochon-drogenesis: A Rare Lethal Skeletal Dysplasia, 354
Parks, A., Russ, P.D., Bieker, T., Stamm, E.R.:Monckeberg’s Arteriosclerosis of the Liver and SpleenDemonstrated by Ultrasound, 225
Parmeter, B., Rodway, L.: Diagnosis of Brachial ArteryOcclusion, 217
Persutte, W.: see Hall, R.Peterson, C.L., Barr, R.G.: Evaluation of Renal Pathology
With an Intravenous Ultrasound Contrast Agent: CaseStudies, 29
Pitts, C., Williams, C.: Diagnostic challenge, 108Poore, R.: see Forgosh, L.B.
Rapp, C.L., Stravros, A.T.: Coded Harmonics in BreastUltrasound: Does It Make a Difference, 22
Reaiche, H., Williams, M., McEvoy, M.: SonographicMeasurement of Middle Finger Flexor Tendons: NormalMeasurements and Reproducibility of Data, 211
Roberts, D.: see Hall, R.Roberts, D.L.: see Cervantez, D.M.Rodway, L.: see Parmeter, B.Romeyn, A.: see Wharton, P.Russ, P.D.: see Parks, A.Russ, P.D.: Hematoma Mimicking Ruptured Testis After
Self-Inflicted Orchiectomy: A Case of MunchausenSyndrome, 175
Sanghvi, M.: Adrenal Pathology Seen During Pregnancy,104
Schroedter, W.: see Andrist, L.S.Shaffer, E.M.: see Drose, J.A.Sheehan, K.: see O’Brien, J.Shvetsova, J.: see Kozirovsky, M.Sidhu, R., Gupta, R., Malhotra, S.: Sonographic Evaluation
of Intraocular Cysticercosis, 339Simkulet, J.: see Wharton, P.Smith, A.M., Benson, C.B., Sophis, J., Khorasani, R.: Time
Saving and Sonographer Acceptance of PACS in anUltrasound Department, 80
Sophis, J.: see Smith, A.M.Spitz, J.L.: see Hall, R.Stamm, E.R.: see Parks, A.Stieler, M.A.: The Use of Sonography in the Detection of
Bony and Calcific Disorders of the Shoulder, 331Stravros, A.T.: see Rapp, C.L.
Tank, E.S.: see Baier, S.R.Teaford, M.H.: see Evans, K.D.
Vest, T.: see Bak, D.M.Vitale, J., Zambuto, D.: Uterine Fibroid Embolization:
Sonographic Findings Pre- and Postembolization, 167
Waggoner, A.D.: see Bierig, A.M.Walkup, D.W.M.: A Rare Case of Duplicated Placenta and
Bifurcated Umbilical Cord in a Singleton Pregnancy, 280Walkup, D.W.M.: Diagnostic Challenge, 179Wallin, S.: see Jones, E.D.Watson, P.T.: see Baier, S.R.Wharton, P., Kabat, M.A., Simkulet, J., Romeyn, A.:
Gallstone Ileus, 268Whitworth, B.: Diagnostic Challenge, 362Wilkinson, M., Grimmer, K., Massy-Westropp, N.:
Ultrasound of the Carpal Tunnel and Median Nerve: AReproducibility Study, 323
Williams, C.: see Pitts, C.Williams, M.: see Reaiche, H.
Yeast, J.: see Mitchell, C.C.
Zambuto, D.: see Vitale, J.
JDMS 17:374-367 2001 November/December 2001
JDMS 17:374-367 2001 November/December 2001
JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
STAYING E-CONNECTED / Dempsey
STAYING E-CONNECTED
ElectronicSubmission ofJournal ArticlesRICH DEMPSEY, RDMS, RVT
Many medical journals now accept electronicsubmissions of material for publication.1 Recently, theJournal of Diagnostic Medical Sonography (JDMS)has joined this growing list. Each publication has itsguidelines for authors, which need to be obtained andreviewed prior to submission. Size, format, imageresolution, and the requirement for a hard-copyversion vary. This information is readily available onthe home page of the publication. Information withregard to JDMS submission is available through theSociety of Diagnostic Medical Sonographers (SDMS)Web site (http://www.sdms.org). An e-mail to theeditor at [email protected] can be used foradditional questions or to quickly clarify thepublication’s requirements.
JDMS is fortunate to be one of only a few journalswith access to a Web-based submission and reviewprocess. At the peer connect Web site (http://212.58.231.10/jdms), authors may submit on-line,review the progress of their submission, and evenaccess reviewer suggestions and comments.Sonographers can now submit an article at home, attheir convenience, without purchasing blank disks,copying documents, or even making a trip to the postoffice.
On-line submission requires Internet access, as wellas the document, a separate title page, and images indigital format. Once the article is submitted on-line, itwill be given an identification number and convertedto a pdf file on the Web site that will be available forreview. Because the review process must beanonymous, authors are requested not to include theirname on the source manuscript itself.
There are many excuses for failing to submitinteresting case reports to a professional journal.Reluctance to undertake the task of converting asonographic image into a publishable format iscertainly a major factor. In the past, preparation ofultrasound images from film format to publisher-usable prints was both time consuming and expensive.However, recent advances in computer technologyhave lessened the daunting task of image
374 JDMS 17:374-367 2001 November/December 2001
Editor’s Note. Staying e-Connected will provide Web site and softwarereviews and information on the innovative use of digital resources insonography. The format will vary from single reviews to multiple shortdescriptions. Sonographers may contribute to this symposium bysubmitting to the editor descriptive narratives and analyses of digitalresources. Submissions may range from single paragraphs to multiplepages in length. Selection of material for publication is at the discretion ofthe editor and editorial board.
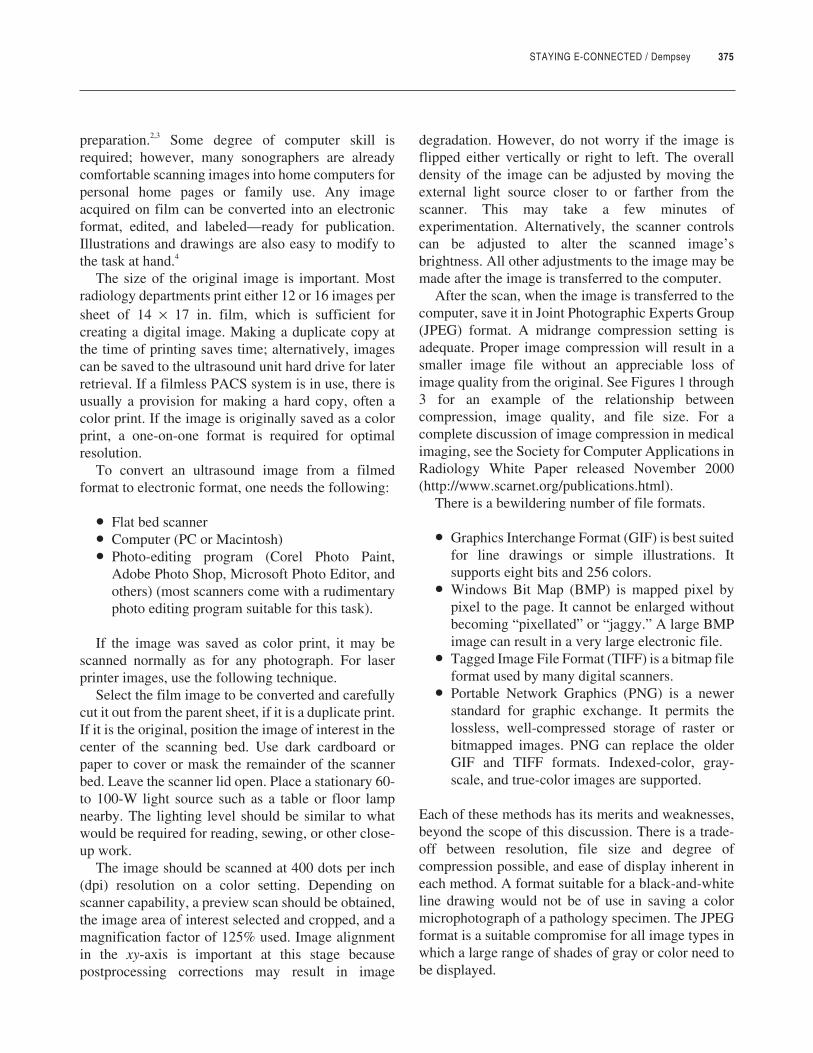
STAYING E-CONNECTED / Dempsey 375
preparation.2,3 Some degree of computer skill isrequired; however, many sonographers are alreadycomfortable scanning images into home computers forpersonal home pages or family use. Any imageacquired on film can be converted into an electronicformat, edited, and labeled—ready for publication.Illustrations and drawings are also easy to modify tothe task at hand.4
The size of the original image is important. Mostradiology departments print either 12 or 16 images persheet of 14 × 17 in. film, which is sufficient forcreating a digital image. Making a duplicate copy atthe time of printing saves time; alternatively, imagescan be saved to the ultrasound unit hard drive for laterretrieval. If a filmless PACS system is in use, there isusually a provision for making a hard copy, often acolor print. If the image is originally saved as a colorprint, a one-on-one format is required for optimalresolution.
To convert an ultrasound image from a filmedformat to electronic format, one needs the following:
• Flat bed scanner• Computer (PC or Macintosh)• Photo-editing program (Corel Photo Paint,
Adobe Photo Shop, Microsoft Photo Editor, andothers) (most scanners come with a rudimentaryphoto editing program suitable for this task).
If the image was saved as color print, it may bescanned normally as for any photograph. For laserprinter images, use the following technique.
Select the film image to be converted and carefullycut it out from the parent sheet, if it is a duplicate print.If it is the original, position the image of interest in thecenter of the scanning bed. Use dark cardboard orpaper to cover or mask the remainder of the scannerbed. Leave the scanner lid open. Place a stationary 60-to 100-W light source such as a table or floor lampnearby. The lighting level should be similar to whatwould be required for reading, sewing, or other close-up work.
The image should be scanned at 400 dots per inch(dpi) resolution on a color setting. Depending onscanner capability, a preview scan should be obtained,the image area of interest selected and cropped, and amagnification factor of 125% used. Image alignmentin the xy-axis is important at this stage becausepostprocessing corrections may result in image
degradation. However, do not worry if the image isflipped either vertically or right to left. The overalldensity of the image can be adjusted by moving theexternal light source closer to or farther from thescanner. This may take a few minutes ofexperimentation. Alternatively, the scanner controlscan be adjusted to alter the scanned image’sbrightness. All other adjustments to the image may bemade after the image is transferred to the computer.
After the scan, when the image is transferred to thecomputer, save it in Joint Photographic Experts Group(JPEG) format. A midrange compression setting isadequate. Proper image compression will result in asmaller image file without an appreciable loss ofimage quality from the original. See Figures 1 through3 for an example of the relationship betweencompression, image quality, and file size. For acomplete discussion of image compression in medicalimaging, see the Society for Computer Applications inRadiology White Paper released November 2000(http://www.scarnet.org/publications.html).
There is a bewildering number of file formats.
• Graphics Interchange Format (GIF) is best suitedfor line drawings or simple illustrations. Itsupports eight bits and 256 colors.
• Windows Bit Map (BMP) is mapped pixel bypixel to the page. It cannot be enlarged withoutbecoming “pixellated” or “jaggy.” A large BMPimage can result in a very large electronic file.
• Tagged Image File Format (TIFF) is a bitmap fileformat used by many digital scanners.
• Portable Network Graphics (PNG) is a newerstandard for graphic exchange. It permits thelossless, well-compressed storage of raster orbitmapped images. PNG can replace the olderGIF and TIFF formats. Indexed-color, gray-scale, and true-color images are supported.
Each of these methods has its merits and weaknesses,beyond the scope of this discussion. There is a trade-off between resolution, file size and degree ofcompression possible, and ease of display inherent ineach method. A format suitable for a black-and-whiteline drawing would not be of use in saving a colormicrophotograph of a pathology specimen. The JPEGformat is a suitable compromise for all image types inwhich a large range of shades of gray or color need tobe displayed.
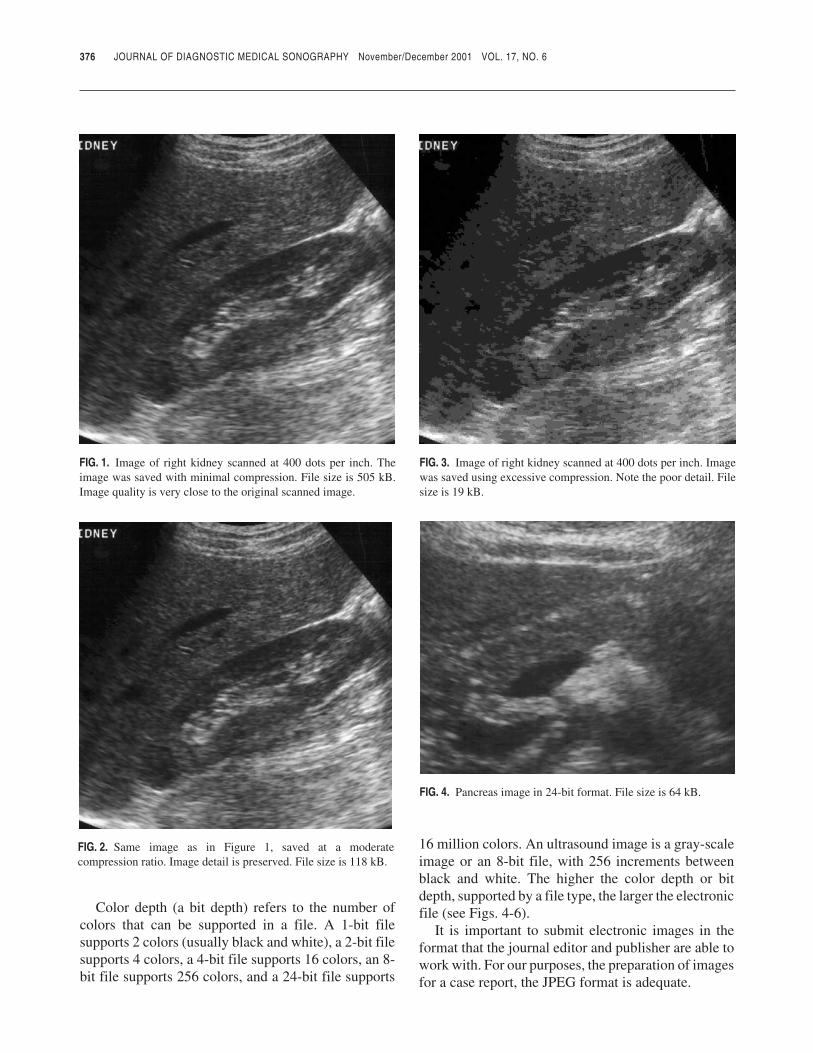
Color depth (a bit depth) refers to the number ofcolors that can be supported in a file. A 1-bit filesupports 2 colors (usually black and white), a 2-bit filesupports 4 colors, a 4-bit file supports 16 colors, an 8-bit file supports 256 colors, and a 24-bit file supports
16 million colors. An ultrasound image is a gray-scaleimage or an 8-bit file, with 256 increments betweenblack and white. The higher the color depth or bitdepth, supported by a file type, the larger the electronicfile (see Figs. 4-6).
It is important to submit electronic images in theformat that the journal editor and publisher are able towork with. For our purposes, the preparation of imagesfor a case report, the JPEG format is adequate.
376 JOURNAL OF DIAGNOSTIC MEDICAL SONOGRAPHY November/December 2001 VOL. 17, NO. 6
FIG. 1. Image of right kidney scanned at 400 dots per inch. Theimage was saved with minimal compression. File size is 505 kB.Image quality is very close to the original scanned image.
FIG. 2. Same image as in Figure 1, saved at a moderatecompression ratio. Image detail is preserved. File size is 118 kB.
FIG. 3. Image of right kidney scanned at 400 dots per inch. Imagewas saved using excessive compression. Note the poor detail. Filesize is 19 kB.
FIG. 4. Pancreas image in 24-bit format. File size is 64 kB.
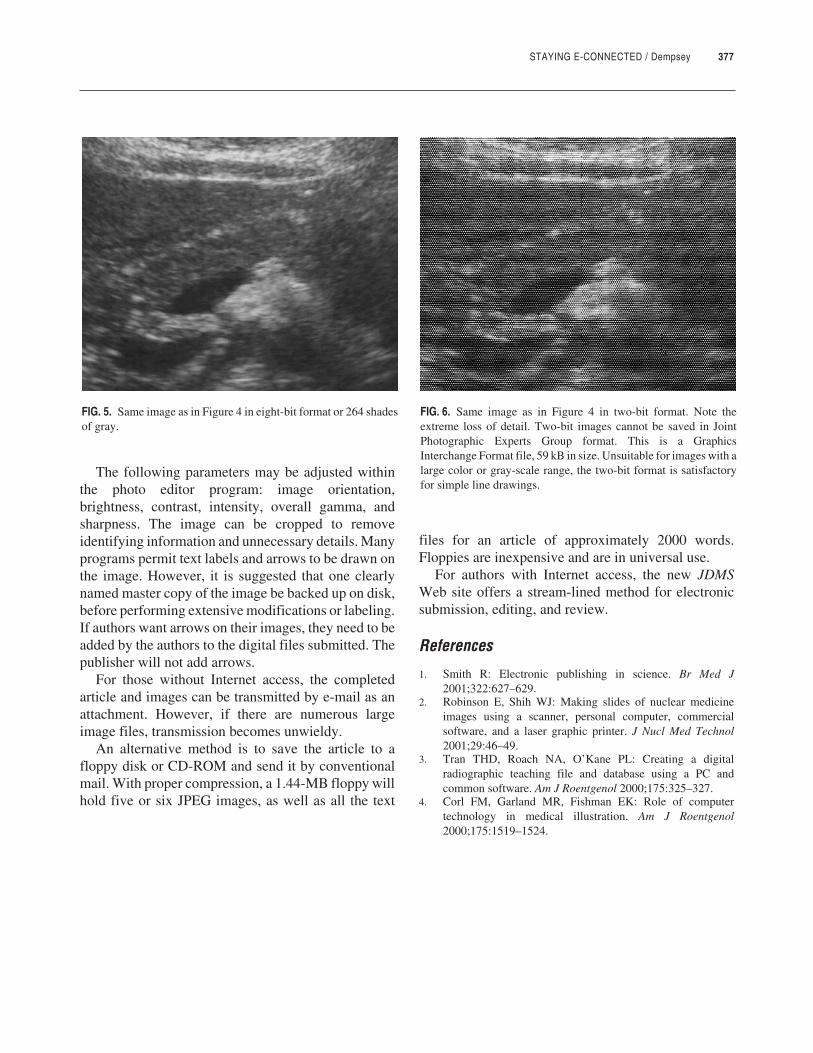
STAYING E-CONNECTED / Dempsey 377
The following parameters may be adjusted withinthe photo editor program: image orientation,brightness, contrast, intensity, overall gamma, andsharpness. The image can be cropped to removeidentifying information and unnecessary details. Manyprograms permit text labels and arrows to be drawn onthe image. However, it is suggested that one clearlynamed master copy of the image be backed up on disk,before performing extensive modifications or labeling.If authors want arrows on their images, they need to beadded by the authors to the digital files submitted. Thepublisher will not add arrows.
For those without Internet access, the completedarticle and images can be transmitted by e-mail as anattachment. However, if there are numerous largeimage files, transmission becomes unwieldy.
An alternative method is to save the article to afloppy disk or CD-ROM and send it by conventionalmail. With proper compression, a 1.44-MB floppy willhold five or six JPEG images, as well as all the text
files for an article of approximately 2000 words.Floppies are inexpensive and are in universal use.
For authors with Internet access, the new JDMSWeb site offers a stream-lined method for electronicsubmission, editing, and review.
References
1. Smith R: Electronic publishing in science. Br Med J2001;322:627–629.
2. Robinson E, Shih WJ: Making slides of nuclear medicineimages using a scanner, personal computer, commercialsoftware, and a laser graphic printer. J Nucl Med Technol2001;29:46–49.
3. Tran THD, Roach NA, O’Kane PL: Creating a digitalradiographic teaching file and database using a PC andcommon software. Am J Roentgenol 2000;175:325–327.
4. Corl FM, Garland MR, Fishman EK: Role of computertechnology in medical illustration. Am J Roentgenol2000;175:1519–1524.
FIG. 5. Same image as in Figure 4 in eight-bit format or 264 shadesof gray.
FIG. 6. Same image as in Figure 4 in two-bit format. Note theextreme loss of detail. Two-bit images cannot be saved in JointPhotographic Experts Group format. This is a GraphicsInterchange Format file, 59 kB in size. Unsuitable for images with alarge color or gray-scale range, the two-bit format is satisfactoryfor simple line drawings.





























