Embed Size (px)
Citation preview

JournalofNeurosurgicalAnesthesiologyYearinReview
MartinSmithEditor-in-Chief
@JNeurosurgAnes
@ProfmartinJNA
https://journals.lww.com/jnsa/

Outline
• Journalupdates- newinitiatives
• Year-in-Review- journal clubstyle- presentationsby3authors
DrAmieHoefnagelDrPhillip VlisidesDrArnoleyAbcejo

• clinicalandlaboratoryinvestigations
• reviewarticles
• journalclub
• correspondence– researchletters:earlydatafrompilot/feasibility studies– correspondence totheeditor:commentaryonstudies published inJNA– correspondence toJNAreaders:clinicalobservations describing new
knowledge/clarify controversialissues – mustbenovelanddidactic
• invitededitorials– commentary:onco-published manuscripts– focus:shortstate-of–the-artreview
JournalofNeurosurgicalAnesthesiology publishesarticlesonallaspectsofneuroscienceinanesthesiologyandcriticalcare

• clinicalandlaboratoryinvestigations
• reviewarticles
• journalclub
• correspondence– researchletters:earlydatafrompilot/feasibility studies– correspondence totheeditor:commentaryonstudies published inJNA– correspondence toJNAreaders:clinicalobservations describing new
knowledge/clarify controversialissues – mustbenovelanddidactic
• invitededitorials– commentary:onco-published manuscripts– focus:shortstate-of–the-artreview
JournalofNeurosurgicalAnesthesiology publishesarticlesonallaspectsofneuroscienceinanesthesiologyandcriticalcare

• clinicalandlaboratoryinvestigations
• reviewarticles
• journalclub
• correspondence– researchletters:earlydatafrompilot/feasibility studies– correspondence totheeditor:commentaryonstudies published inJNA– correspondence toJNAreaders:clinicalobservations describing new
knowledge/clarify controversialissues – mustbenovelanddidactic
• invitededitorials– commentary:onco-published manuscripts– focus:shortstate-of–the-artreview
JournalofNeurosurgicalAnesthesiology publishesarticlesonallaspectsofneuroscienceinanesthesiologyandcriticalcare

• 5articlesperissue• freetoread
Editor’schoice

• accessible inacollection viaalinkonthehomepage• freetoreadinperpetuity
SNACCclinicalguidelines andconsensusstatements

Colorfigurescannowbeincludedinonlineversionofthemanuscriptatnocharge.
Colorfigures

SNACCTraineeEngagementCommitteewillproducepodcastsdiscussingJNAarticles
Podcasts

• notanexhaustivelist– topicalissues– breadthofthejournal– onesthatIliked
YearinReview

Journal of Neurosurgical Anesthesiology 2019; 31(1): 7-17
• cognitiveaidsandevidence-basedchecklistsarefrequentlyutilizedincomplexsituations
• notsimplyinstructionstocompleteatask- ensurethatallcontingenciesrelatedtothe
emergencyareconsideredandaccountedfor- taskathandiscompletedfully, despitepossible
distractions
• 11evidence-basedcriticaleventcognitiveaidsforneuroanaesthesiaemergencies

Standarddesignprocessfacilitatessampling
Journal of Neurosurgical Anesthesiology 2019; 31(1): 7-17

Quickreferenceguideforcliniciansfacinganeuroanesthesiaemergency
Journal of Neurosurgical Anesthesiology 2019; 31(1): 7-17

• ShobanaRajan• AdrianaMartin• VibhaMahendra• AmandaKnutson• JamieUejima• GuyKositratna
• MarkWeller• HuiYan• SanchitAhuja• CarylBailey• JohnBebawy
Journal of Neurosurgical Anesthesiology 2019; 31(1): 7-17

Journal of Neurosurgical Anesthesiology 2019; 31(3): 337-341
• ACGMEcompetency-basedassessments(milestones)forresidenteducationnotspecifictoneuroanesthesiology- interpretationnotstraightforward
• 12neuroanesthesiology-specificmilestonesin5majorACGMEdomainsarerecommended- patientcare(7milestones)- medicalknowledge(2milestones)- practice-basedlearningandimprovement(1milestone)- interpersonalandcommunication skills (2milestones)
• eachmilestonedescribedindetail,withclearoutlineofexpectationsatvariouslevelsoftraining

ExampleofamilestonePatientcare7:technicalskills: useandinterpretationofmonitoringandequipment
Journal of Neurosurgical Anesthesiology 2019; 31(3): 337-341
SNACCNeuroanesthesiologymilestonesprovideaframeworkforreviewingresidentperformance.Thetaskforcerecommendsthatthetargetshouldbetoaccomplishlevel4orhighermilestonesbytheendofresidencytraining.

• promising preclinicaltherapeuticstrategieslargelyfailedtotranslateintoimprovedoutcomesinRCTs
• observational studies
• datascience
• ‘alive’inonecountry‘dead’ inanother
• only outstandingissue inthetransatlanticdivide inthedeterminationofbraindeath
GiventhecostandlogisticburdensofconductingRCTS,…….prioritizewhichresearchmethodsareimportantfor
answeringthemyriadofresearchquestionsinsevereTBI.
Perceived divide between whole brain and brainstem death more to do with emotive concepts rather than hard neurobiological facts - represents a failure to accept the centrality of the brainstem in defining life or death.

Journal of Neurosurgical Anesthesiology 2019; 31(2): 212-217

Journal of Neurosurgical Anesthesiology 2019; 31(2): 212-217

Journal of Neurosurgical Anesthesiology 2019; 31(2): 212-217
Delirium:26% (Training) vs. 17% (Control);P=0.507
HospitalLOS:6.8d (Training)vs.6.4d (Control);P=0.696

Journal of Neurosurgical Anesthesiology 2019; 31(2): 212-217
Declined Participation

Journal of Neurosurgical Anesthesiology 2019; 31(2): 212-217
Non-Adherence
Withdrawals
Training: 5/30 (17%)
Control: 0/31 (0%)
P=0.024

Journal of Neurosurgical Anesthesiology 2019; 31(2): 212-217
Conclusions
• OptimizeStudyDesign
• ConsiderEffectSize
• InterimAnalysis,StoppageRules

• impossibletoidentifyasingleunderlyingcauseforpostoperativedelirium- pharmacologicaltreatmenteitherempirical(e.g.antibiotics) orsymptomoriented(e.g.anti-
psychotics)- primarypreventionusingmulti-component non-pharmacological strategiesasmarterapproach
• cognitivereserveintheperioperativesetting- surgery/anaesthesiaarethedamaging‘hit- postoperativedelirium themanifestationof
cognitiveimpairment
Cancognitivereservebeincreasedbybraintrainingand,inturn,preventperioperativeneurocognitive
disorders suchasdelirium?
Journal of Neurosurgical Anesthesiology 2019; 31(2): 174-177

Journal of Neurosurgical Anesthesiology 2019; May 22, Epub: doi: 10.1097/ANA.0000000000000609
• multipledisparatefactorscontributetoICPelevation- interpretationnotstraightforward
• evidencefordistinctconceptualsubsetsofintracranialhypertensionwithsupportivedatafrompublishedliteratureandinvasiveandnon-invasiveneuromonitoringdata
• 3majorpathophysiologicalsubsets- increasedcerebralbloodvolume- masses andedema- hydrocephalus

Reductioninbloodpressureproducesvasodilationwithincreasedcerebralbloodvolumeontheuninjuredsidewithacorresponding increaseinICP.
Dysautoregulationontheinjured sideandintactautoregulationonthecontralateral(uninjured) side
TheinjuryandassociatededemaincreaseICPsomewhatwithassociateddecrementinintracranialcompliance.
Increaseinbloodpressurecausesvasoconstrictionontheuninjuredside,butdysregulatedhyperemiaandincreasedcerebralbloodvolumeontheinjuredside.
SimilarelevationsinICPareproducedbydistinctly differentphysiological conditions
Journal of Neurosurgical Anesthesiology 2019; May 22, Epub: doi: 10.1097/ANA.0000000000000609

• narrativereviewoftheevidencefortheperioperativemanagementofDOACsinintracranialneurosurgery
• increaseduseofdirectactinganticoagulants- predictablepharmacokinetics- fewerdruginteractions- lowerrisk ofbleeding
• limitedevidencebase- currentguidelines extrapolatedfrompharmacologicaldataandclinicalstudies thatexcluded
neurosurgicalpatients
Journal of Neurosurgical Anesthesiology 2019; Jul 12 Epub: doi: 10.1097/ANA.0000000000000629

DOACsinelectiveintracranialsurgery
• timingofDOACinterruption
• bridgingtherapyandthrombosisrisk
• restartinganticoagulation
Journal of Neurosurgical Anesthesiology 2019; Jul 12 Epub: doi: 10.1097/ANA.0000000000000629

DOACsinemergencyintracranialsurgery
• establishtimingoflastDOACdose/checkrenalfunction
• considernatureandurgencyofsurgery
• non-specificapproachestoreversal,e.g.PCC
• specificDOACantidotes
Interdisciplinaryco-operationbetweenneuroanesthesiologist,neurosurgeonandhaematologistessentialforoptimal
patientoutcomes.
Journal of Neurosurgical Anesthesiology 2019; Jul 12 Epub: doi: 10.1097/ANA.0000000000000629

Journal of Neurosurgical Anesthesiology 2018; 31(4) : 413-421
• severeVAEisamajorconcernoftheseatedposition forneurosurgery
• rarely,severeVAEcancauseenoughgasexchangeimpairment,hemodynamiccollapse,orpersistentneurologicdeficitsnecessitatingemergentreturntothesupineposition
• wecharacterizedthesecasesof“extremeVAE,”studiedtheiroutcomes,andstudiedtheirintraoperativecourseandmanagement

Methods
• Retrospectivecaseseriesofseatedneurosurgicalprocedures• (404craniotomies,324DBSimplantations)
• DefinedExtremeVAE asaclinicallydiagnosedVAEthatnecessitatedemergentpositionfromtheseatedtoaflatposition
• 8CasesofExtremeVAEIdentified• 6CraniotomiesforPosteriorFossaTumorresection• 2DBSplacements
• Patientcomorbidities,intraoperativevariables/events/management,hemodynamic/neurologic/dispositionoutcomeswererecorded
Journal of Neurosurgical Anesthesiology 2018; 31(4) : 413-421

Results
TherewerenoextremeVAEcasesinvolvingtortocollisdenervationsorcervicalspineprocedures.
Therewere6extremeVAEduringposteriorfossasurgeries,withatotalincidenceof1.5%.And2extremeVAEduringDBSplacement,0.6% incidence.
Inonepatient(C),careoflife-sustainingmeasureswaswithdrawnduetoinabilitytocontrolbleedingoffriablecerebralvasculature.
Therewere2instancesoftransientST-segmentchangesandventriculararrhythmiainpatientswithairappearingintheaorticroot,andinbothinstancesthisrapidlyresolved.
NonewneurologicaldeficitswereattributedtotheVAEandemergentsupinepositioninginanyofthepatients.
Nonewpostoperativecardiovascularorcardio-electrophysiologicderangementswereattributedanyVAE.
Journal of Neurosurgical Anesthesiology 2018; 31(4) : 413-421

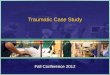
PatientA PatientB PatientG
Δ EtCO2MAP
* Supine
PosteriorFossaCraniotomyinBMI53patient
VAEassociatedwithsevere reductioninEtCO2andMAP.Intra-aorticairnoted.Sustainedectopyandventriculartachycardia.
30-40mLoffrothybloodaspirated(blackline).
Post-op:Unchangedneuroexam.Notropinemia,nohemodynamicinstability.
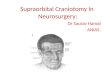
PosteriorFossaCraniotomywithoutCVCline
VAE inleftandrightcardiacchambers.Hyopotension,NewS-Tchanges.
Emergent leftlateral decubituspositioningwithalmostinstantaneousresolutionofhemodynamiccompromise.
DBSplacementinseatedposition
Patientbegan tocoughafterburrholewithsignificantreductioninEtCO2vianasalcannula.Severe chestpaindevelops.
SupinepositionwithgradualresolutionofEtCO2tobaseline.
Results (cont’d)Journal of Neurosurgical Anesthesiology 2018; 31(4) : 413-421

• extremeVAE(severeVAEnecessitatingemergentreturntosupineposition) isarareevent
• centralvenouscatheterizationandaspirationduring VAEplayednodemonstrableroleinpatientoutcomeswithnoappreciableairaspiratedinmajorityofcases
• itappearsthatthehemodynamic andneurologic sequelae,iftreatedrapidly,aretransient andresolveshortlyafterpositionchange
ConclusionsJournal of Neurosurgical Anesthesiology 2018; 31(4) : 413-421

Journal of Neurosurgical Anesthesiology 2019; 31(3): 318-322
• prospectivemulticenterstudy including36physicians(18left- &18right-handed)and7200patients
• patientsrandomizedtohaveLPsperformedbyleft- andrighthandedphysicians- eachphysician performed200LPsduringwhichthelateralityofrecumbentposition wasdecidedaftera
second randomization- successful LPdefinedbyfreeflowofCSFatfirstattempt

• right-handedphysicianshadhigherLPsuccessratewithpatients inthe leftlateralposition(1595/1800vs.1408/1800;P=0.006)
• left-handedphysicianshadhigherLPsuccessratewithpatientsinrightlateralposition(1424/1800vs.1593/1800;P=0.001)
• patientfactors(age,sex,height,weight)didnotaffectLPsuccessrate
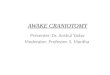
Multivariable analysis of factors affecting success of LP
Physicians handedness andpatientlateralityaffectsthesuccess oflumbar.Right-handedphysicians haveagreaterchanceofperformingsuccessful LPswhenpatientsareintheleftLRP,andviceversa.
Journal of Neurosurgical Anesthesiology 2019; 31(3): 318-322

• singlecentrestudyof126patientshavingendovascularthrombectomy- 116(92%)receivedconscious sedation- guideline recommendsystolicBPbetween140and180mmHg
• systolicBP<140mmHgin30.2%and>180mmHgin14.3%ofpatientsonarrivalinneuroradiologysuite
Journal of Neurosurgical Anesthesiology 2019; 31(3): 299-305

• haemodynamicinstabilitywascommon- 77.8%hadatleastoneepisodeofhypotension (SBP<140mmHg)- 19.1%hadatleastoneepisodeofhypertension (SBP>180mmHg)- mostself-limiting
• haemodynamicinterventionrequiredin38.9%ofpatients- 15.1%forhypotension- 19.8%forhypertension
• hypotension- morecommon inpatientsreceivingsedation(80.2%vs.50%,p=0.043)- poorcontrol(SBP<140mmHgfor>15mindespite intervention)occurredin12.7%ofpatients- lowerbaselineBPassociatedwithahigherriskofintraproceduralhypotension
(OR,0.92;95%CI,0.89-0.96;P<0.001)
Thereisafrequentneedforhaemodynamic interventionduringendovascular thrombectomy,arguingfortheroutinepresenceofanaesthetists
Journal of Neurosurgical Anesthesiology 2019; 31(3): 299-305

• synopsisofinnovativeresearch,recurringthemesandnovelexperimentalfindings- intracranialsurgery- spine surgery- stroke- traumaticbraininjury- subarachnoid haemorrhage- neuromonitoring- anestheticneurotoxicity- perioperativecognitivedysfunction anddelirium
Comprehensivereviewofclinicalandbasicscienceinneuroanaesthesiaandcriticalcare,including162citations.
Journal of Neurosurgical Anesthesiology 2019; 31(2): 178-189

Journal of Neurosurgical Anesthesiology 2019; 31(4): 359-360
• 30,590anesthesiologistsand38,600surgeonsworkingintheUnitedStatesduring2017- 31journals categorizedunderAnesthesiology - medianImpactFactorof2.56- 200journals categorizedunderSurgery- medianImpactFactorof1.81.3
• adjustedfornumberofpractitioners,surgeonshadfivetimesmorejournalsthananesthesiologists,withanImpactFactordilutedby30%
• researchanditspublicationdrivenby- scientificendeavour- ambitionforstatus- answersratherthanquestions

• thereviewprocess- vastlymoreeffectivethanitappearstobe- integrityandcommitmentofreviewers- assessments basedonmanuscriptspresentedtoreviewers
• acceptanceofanabundanceofflawedmanuscripts- cleverrevisions ofpriorversions rejectedbytheirauthors’first-choicejournal- acceptedbyauthors’second, third,etc.choicejournal
Journal of Neurosurgical Anesthesiology 2019; 31(4): 359-360
…..upto90%ofmedicalresearchisseriouslyflawedbecausebiasinfavorofpreferredresults“isunavoidableandpeopleshouldtakethatforgrantedwhenthey…readotherscientists’work.JohnIoannidis

• centralclearinghouseformanuscriptreview- noevaluationofmanuscripts’ quality- trackedhistory, including allpriorversions, allreviewsofallpriorversions, andallprioreditorial
correspondence, foreverysubmission ofeachmanuscript forwardedtointendedjournal
• implications- coveringupdesign inadequacies in‘revisions’ becomesdifficult/impossible- likelyleadtoshrinkageofjournal portfolios- bigpay-offforscience
Imagine the rate of progress that would follow from reversing the ratio of good/bad science from 25/75 to 75/25!
Journal of Neurosurgical Anesthesiology 2019; 31(4): 359-360

547reviewsconductedby177reviewers

@JNeurosurgAnes
https://journals.lww.com/jnsa/
• JNAistheofficialjournalofSNACC– becomeareviewer– submitamanuscript– writeafocuseditorial– citeJNAmanuscriptsinyourwork– socialmedia