Embed Size (px)
Citation preview

Review Article
Fracture Resistance of Teeth Restored with Post-retainedRestorations: An OverviewMahmoud Khaled AL-Omiri, BDS, PhD, FDS RCS,* Ahmad Abdelaziz Mahmoud, BDS, PhD,*
Mohammad Ramadan Rayyan, BDS, MDSc,†
and Osama Abu-Hammad, BDS, MSc, PhD*
Abstract
Introduction: Posts have been used efficiently to retainrestorations for badly destructed teeth. This articlecritically analyzes the concerned topics related to thefracture resistance of teeth restored with dowel-retained restorations. Methods: A systematic reviewof PubMed/MEDLINE, Cochrane, and Scopus databaseswas completed (from 1960 to 2010). Single or combinedkey words were used to obtain the most possiblecomprehensive list of articles. Checking the referencesof the relevant obtained sources completed the reviewalong with a manual search to locate related articleson the topic. In vivo and ex vivo (laboratory,computer-based finite element, and photoelastic stressanalysis studies) investigations related to the topicwere included. Results: Many factors have beenproposed to influence the fracture resistance of post-restored teeth. Recognizing the significance of thesefactors on the fracture resistance of teeth would aid inchoosing the suitable treatment modality for every indi-vidual case. Fracture resistance was improved if toothstructure loss was limited, a ferrule was obtained,a post with similar physical properties to natural dentinewas used, and adhesive techniques for post luting andcoronal restoration were used. Adhesively luted resin/fiber posts with composite cores appear to be the bestcurrently available option in terms of tooth fractureand biomechanical behaviour. Conclusions: Mostguidelines were based mainly on ex vivo studies andto a lesser extent on limited in vivo studies. The lackof long-term controlled randomized clinical studieswas the main hindrance to reaching a conclusive andundisputable opinion regarding endodontic posts interms of tooth fracture and biomechanical behaviour.(J Endod 2010;36:1439–1449)Key WordsEndodontic post, failure modes, fracture resistance,review
From the *Department of Prosthodontics, University of Jordan,Address requests for reprints to Dr Mahmoud AL-Omiri, BDS, Ph
11942, Jordan. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.005
JOE — Volume 36, Number 9, September 2010
Endodontically treated teeth were claimed to be weaker and more prone to fracturethan vital teeth (1). Fennis et al (2) investigated 46,000 insurance claims and re-
ported a higher incidence of tooth fracture among endodontically treated teeth. Theloss of water and collagen cross-linking might underlie the brittleness and weaknessof enododontically treated teeth (3, 4). On the other hand, some studies reportedthat tooth substance of endodontically treated teeth had comparable biomechanicaland physical properties to vital teeth (5–7).
The loss of structural integrity is the main reason behind the vulnerability ofendodontically treated teeth and their reduced resistance to fracture (5, 8). Mostendodontically treated teeth suffer massive reduction in their structural stabilitybecause of the great loss of coronal dental structure caused by caries, fractures, andaccess preparations.
Tang et al (9) summarized the risks that increased the potential of tooth fractureafter endodontic treatment. The risks included loss of tooth structure, stresses attrib-uted to endodontic and restorative procedures, access cavity preparation, instrumen-tation and irrigation of the root canal, obturation of the root canal, post canalpreparation, post selection, coronal restoration, and inappropriate selection of toothabutments for prostheses.
Vertical root fractures of endodontically treated teeth prepared to receiveendodontic posts were more frequent in the teeth of older patients and when dentinethickness was reduced (10). In their review, Dietschi et al (11) concluded that changesin tooth biomechanical behavior, tissue composition, and moisture after the loss oftooth vitality and proper endodontic treatment were limited and negligible. However,they found that teeth became weaker as they lost more coronal tissue because of cariesor restorative procedures.
Another possible reason behind their inferior resistance to fracture is the reducedproprioception of endodontically treated teeth (12). Consequently, they will be sub-jected to more harmful forces without a protective reflex. Because of their inherentweakness, endodontically treated teeth need to be restored in a manner that wouldprovide protection for the remaining tooth structure but would also allow the restora-tion of esthetic and functional demands (13).
The restoration of endodontically treated teeth should aim at increasing tooth frac-ture resistance especially in cases with extensive tooth destruction (13). Someresearchers recommended the use of posts for support and reinforcement of remainingtooth structure. This claim was supported by the ability of posts to distribute stress ina favorable way that would improve the fracture resistance of restored teeth (14–19).Salameh et al (17, 20) showed that endodontically treated teeth restored with fiberposts and ceramic crowns were more resistant to fracture and had less catastrophicfracture patterns than the ones restored with ceramic crowns and no posts. Inanother study, Salameh et al (21) used porcelain fused to metal, Empress II (Ivoclar
Amman, Jordan; and †Riyadh Colleges of Dentistry and Pharmacy, Riyadh, Saudi Arabia.D, FDS RCS, Department of Prosthodontics, Faculty of Dentistry, The University of Jordan, Amman
Fracture Resistance of Teeth Restored with Post-retained Restorations 1439

Review Article
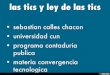
Vivadent, Schaan, Liechtenstein), SR Adoro (Ivoclar Vivadent, NoblePark North, Victoria, Australia), and Cercon (Dentsply Ceramco,York, PA) crowns to restore endodontically treated maxillary incisorsand reported similar conclusions as described previously regardlessthe type of used crown. Also, Cagidiaco et al (18) and Ferrari et al(19) showed that the placement of fibre posts did improve the survivalrate of endodontically treated premolars.Furthermore, Nam et al (22) found that the fracture resistance ofendodontically treated premolars with one to four remaining coronalwalls was significantly increased when they were restored with fiberposts. Moreover, teeth showed better stress distribution and fracturepatterns when restored with fiber posts. However, fracture resistanceof teeth with no remaining coronal walls was not improved when fiberposts were used. Figure 1A through D presents some fracture modesthat associate metal, glass fiber, and carbon fiber posts.
When compared with no post treatment, Nothdurft et al (23) re-ported better fracture resistance of premolars with class II cavity prep-arations after they were restored with zirconia, fiber, or titanium posts.They concluded that posts in premolars with class II cavities wouldimprove tooth resistance to the extra-axial forces. In another study, Noth-durft et al (24) reported no difference in fracture resistance of premo-lars with class II cavities restored with crowns alone or crowns and posts(titanium, zirconium dioxide, glass fiber, and quartz fiber posts). Fromthese two studies, it can be concluded that the use of crowns mightcancel the effect of posts on fracture resistance of restored teeth.
On the other hand, many studies challenged the use of posts forsupport and reinforcement of remaining tooth structure and evenconsidered post placement as a risk factor that weakened the remainingtooth structure and predisposed tooth fracture. These studies showedthat restoring endodontically treated teeth using cast metal, prefabri-cated metal, or fiber posts had negative effects on teeth fracture resis-tance (25–30). Unlike other modes of failure, root fracture of postrestored teeth is the most catastrophic and almost always results inextraction of the involved tooth (27, 28). A higher incidence ofvertical root fractures was reported among teeth restored withtitanium, zirconia, and prefabricated/cast metal endodontic posts (26,28, 31, 32). This was greatly attributed to stress concentration withinthe radicular dentine during post placement and, consequently, thealtered pattern of stress distribution upon loading (32–34).
Fokkinga et al (35) reported that the presence or absence ofmetal/fiber posts did not affect the fracture resistance and failure modesof endodontically treated premolar teeth with resin composite crownsand no retained coronal tooth structure. Therefore, they suggested thatposts are not necessary for the restoration of such teeth. Also, Moham-madi et al (36) found no difference in fracture resistance of premolarsrestored with direct resin composite in the presence or absence of fiberpost and cusp coverage.
Furthermore, Soares et al (29) found that the loss of dentinalstructures and the presence of fibre posts caused more stress concen-tration in tooth and restoration and decreased the fracture resistance ofteeth. However, they found that fiber posts were associated with lesscatastrophic fracture modes when there was an extensive loss of toothtissues.
An in vitro study by Pilo et al (30) showed that endodontic therapyfor upper bifurcated premolars caused loss of more dentine at bifurca-tion area of both roots in comparison to outer areas. Furthermore, thepreparation of post canals undermined root strength because it left lessthan the recommended 1-mm dentine thickness around the post canal.Buccal roots were more affected by this pitfall. Therefore, they recom-mended limiting the use of posts in upper bifurcated first premolars,and when necessary the posts should be used in lingual roots ratherthan the buccal ones.
1440 Khaled AL-Omiri et al. http://endo
The literature is full of controversial conclusions regarding thebest post to use for the restoration of endodontically treated teeth.This article critically analyzes the concerned topics and controversyrelated to the fracture resistance of teeth restored with dowel-retained restorations.
MethodsA systematic review of PubMed/MEDLINE (from 1960 to 2010),
Cochrane, and Scopus databases (to 2010) was completed. Single orcombined key words (fracture resistance, endodontic post and core,fiber posts, adhesive luting, and endodontically treated teeth) wereused to obtain the most possible comprehensive list of articles. Check-ing the references of the relevant obtained sources completed the reviewalong with a manual search to locate the most relevant articles on thetopic. In vivo and ex vivo (laboratory, computer-based finite element,and photoelastic stress analysis studies) investigations related to thetopic were included in this review. Because the number of long-termrandomized controlled clinical trials (RCTs) was limited in this field,retrospective, prospective, descriptive, review, and RCT studies wereincluded. Studies describing post and core systems to restore endodon-tically treated teeth and their mechanical and physical properties wereincluded. Also, articles investigated fiber posts, ceramic posts, castposts, and prefabricated metal posts, and different core systems wereincluded. Furthermore, articles studied failure modes and fractureresistance of teeth restored with different post and core systems wereincluded.
ResultsMethods Used to Assess Stress Distribution and FractureResistance of Post-Restored Teeth
Few RCT studies have investigated the fracture resistance of teethrestored with post and core restorations. This might be attributed to thedifficulties encountered in controlling related factors clinically such asforce magnitude and direction, teeth geometry, and remaining toothstructure (13). In vitro studies, on the other hand, are easier to controland conduct, but their recommendations should be interpreted withcaution because of their limitations and conflicting results.
It is impossible to accurately simulate intraoral conditions byin vitro studies (13). However, attempts were made to investigate frac-ture resistance of endodontically treated teeth restored with posts andcores experimentally (37). Three methods have been frequently usedfor this purpose including laboratory experiments, photoelastic anal-ysis, and finite element analysis (13, 37).
Although most mechanical laboratory studies were aimed at inves-tigating the failure loads and modes of restored teeth, photoelastic andfinite element analysis studies were used to investigate stresses withinrestored teeth upon loading and the effect of post placement on stressvalues and distribution (13).
Laboratory ExperimentsMany mechanical studies were conducted to investigate the effect
of post placement and related factors on the fracture resistance ofendodontically treated teeth (38-43). Extracted teeth, especiallyincisors and premolars, were used in these studies. Static loading ata constant angle was applied to restored teeth in some studies (41,44). However, actual masticatory forces are multidirectional andrepeatedly applied on larger areas (13). In order to mimic such condi-tions, cyclic loading was also applied in some studies (42, 43, 45).Hayashi et al (46) applied simultaneous static and cyclic loading torestored teeth in both horizontal and vertical directions and reportedthat teeth restored with fiber posts and composite cores were more
JOE — Volume 36, Number 9, September 2010dontic.ws

Figure 1. A catastrophic coronal dentine-core-root vertical fracture. (A) A catastrophic horizontal root fracture–associated prefabricated metal post. (B) A favor-able core fracture-associated fiber post. (C) A catastrophic core and root fracture–associated carbon fiber post. (D) A prepared post canal for a glass fiber post.(E) Note the oval shape of the root canal cross-section and the rounded cross-section of the post canal. There was no need for further preparation of the canal toimprove post fitting.
Review Article
resistant to fracture than those restored with metallic posts (46). Also,Hu et al (47) applied static and cyclic loading to teeth restored with castmetal posts, resin composite posts, and carbon fiber posts and foundthat teeth restored with carbon fiber posts were resistant to moreload cycles, whereas cast metal posts required the highest fractureloads. However, resin composite posts were associated with favorableroot fractures, whereas all cast metal posts and carbon fiber postswere associated with unfavorable root fractures (47).
Strain gauges were used to calculate stresses within examined teethmodels. However, this method may need complex mathematical calcu-lation and is limited by the number of gauges that can be placed on the
JOE — Volume 36, Number 9, September 2010
model (48). Experimental studies in general have many limitations. Thestrength of dentine varies according to age, pulpal condition beforeextraction, and the storing media, which may affect the fracture patterns(13). Resins and stones are commonly used for mounting teeth duringtesting (49–51). They set by the exothermic reaction, which may affectthe dental structures (52). Moreover, despite researchers’ attempts toreproduce the resiliency of periodontal ligament and bone, they couldnot provide the correct actual resiliency of these structures. Someexperimental studies applied forces directly on the post head or thecore, which is commonly not the case clinically (49, 50, 53). Thismay produce misleading and contradictory results. Naumann et al
Fracture Resistance of Teeth Restored with Post-retained Restorations 1441

Review Article
(54) highlighted the lack of standardization of test parameters appliedfor in vitro studies of fracture resistance of teeth restored withendodontic posts. They found that 95% of studies used static loading,and only 15% of the studies used thermocycling and mechanical loadingto test fracture resistance of teeth restored with endodontic posts.Furthermore, different studies used different teeth, and 57% of thestudies used upper incisors only. Also, most studies used specimenswithout crowning. Therefore, the different test parameters and stan-dards might be the reason behind the controversy surrounding the issueof fracture resistance of teeth restored with endodontic posts.Photoelastic Stress AnalysisPhotoelastic models were used to study the effect of post place-
ment and related factors on the patterns of stress distribution withinendodontically treated teeth (55–57). Photoelasticity is the propertyof transparent materials to exhibit colorful patterns known as‘‘fringes’’ when stressed under polarized light (55). A transparentdouble-refraction plastic sheet is used to fabricate specimens fortwo-dimensional photoelastic stress analysis (57). Stress concentrationareas can be identified according to the sequence of color bands of thefringes. Three-dimensional photoelastic models are less frequently usedbecause of the difficulty of their construction and their high cost (55).
Photoelastic methods provide visual evidence of stress patternswithin tested models. However, the properties of photoelastic materialsare different from those of tooth structure, and the modeling of objectsmade of more than one material is technically difficult (13).
Finite Element MethodThe finite element method (FEM) has been frequently used for
stress analysis in many aspects of dentistry. Many studies used theFEM to investigate the effect of post placement and related parameterson the stress picture within dowel-restored teeth (34, 58–65).
Models are simulated using a computer and subdivided into a finitenumber of smaller divisions termed elements. Material properties,boundary conditions, and loads are then assigned for the elements.Stress analysis is then performed by solving differential equations ofelements to quantify stresses generated within these elements.
FEM offers the advantages of easy simulation of nonhomogenousmodels and easy changing of parameters like material properties andloading conditions (58). However, material properties, loading condi-tions, and boundaries simulated do not represent the absolute clinicalsituation that constitutes a limitation for the application of this method(13).
Stress Distribution Within Post-Restored Teeth and ItsRelation to Fracture Resistance
Viscoelastic properties of a tooth structure affect stress distribu-tion within the tooth. If viscoelastic properties are undermined, thetooth will be mechanically compromised in terms of stress distribution,values, and concentration. Root canal treatment and post and corerestorations are examples of conditions in which tooth viscoelasticityis reduced and this might be the reason why teeth are more liable tofracture (66). Post insertion alters the pattern of stress distributionwithin root dentine (37). Different posts affect the stress picture inpost-restored teeth differently, which will be discussed in the followingsections. Upon loading, teeth restored without post insertion showa concentration of stresses at the circumference of the tooth withuniform stress distribution within the root canal (67). Post insertionresults in a nonuniform distribution of dentinal stresses within theroot (68). Upon functional loading, critical stress concentration areasare produced at the post-dentine interface that precipitates microcracks
1442 Khaled AL-Omiri et al. http://endo
within the root. These microcracks grow and propagate to cause fatiguefailure and unrestorable root fractures (32, 63). The coronal third ofthe root has been reported as the main site of stress concentration(69, 70).
The inner dentine of the root is usually less mineralized andpossesses more water content than the outer dentine (71). Therefore,the inner dentine has a higher potential for plastic deformation andcrack formation. Using experimental and clinical investigations, Kishenet al (72) examined fractured post and core restored teeth using laserscanning confocal microscopy and scanning electron microscopy andobserved numerous microcracks within the inner dentine materialadjacent to the endodontic post. They also used FEMs of dentine torelate crack formation and root fractures to tensile stresses generatedwithin dentine. High strains were generated within the inner dentinesubstance upon tensile loading. They, among other researchers,concluded that crack formation and fracture progression in post-restored teeth were initiated from the inner region of dentine (72–74). Thickness of the inner dentine and factors related to the post-dentine interface seem to play a major role in stress distribution andfracture resistance of endodontically treated teeth. Therefore, theremoval of inner dentine during post placement should be minimizedas much as possible to maintain adequate fracture resistance ofdowel-restored teeth (72).
Factors That Affect the Fracture Resistance of Post-Restored Teeth
Many factors influence the fracture resistance of post-restoredteeth. Some factors are directly related to the post-core system includingpost length, post diameter, post design, post material, post fitting, corematerial, ferrule effect, and luting cement (13). Other factors arerelated to the restored tooth and include cuspal coverage, remainingcoronal tooth structure, loading conditions, and alveolar bone support(13, 15). The effect of these factors on the fracture resistance of dowel-restored teeth will be discussed in details throughout the followingsections.
Post LengthStress analysis studies showed better stress distribution within
dentine when longer metal, fiber, or zirconia posts were used (65,75). Similarly, increased fracture resistance was associated withincreased post length (15, 76). Longer posts provide greater rigidityand less root bending than short posts (13). An endodontic post shouldextend beyond the level of alveolar bone to provide better root support(77).
Davy et al (75) reported a decrease in cervical stresses when thepost length was increased up to two thirds of the root length. However,increasing the post length beyond two thirds of the root may cause stressconcentration at apical area of the root meanwhile provide no addi-tional support for the cervical region (78). Burns et al (79) reportedminimal effects of the post length on stress distribution within dentine.Other studies supported this finding and found no effect of the postlength on fracture resistance of restored teeth (45, 80, 81). Giovaniet al (82) found no effect of post length on the fracture resistance ofteeth restored with metal cast post and core. However, they showedsignificantly higher fracture resistance for teeth restored with longerglass fiber posts (10-mm long) when compared with shorter ones(6-mm long). On the other hand, Cecchin et al (83) found that longerfiber posts (12- or 8-mm long) were associated with higher fractureresistance of teeth when compared with shorter ones (4-mm long).However, they concluded that too much preparation to get the longestpost space was not essential for better fracture resistance of post-
JOE — Volume 36, Number 9, September 2010dontic.ws

Review Article
restored teeth. In their study, posts that were just above half of rootlength (8-mm long) were enough to improve the root fracture resis-tance and were similar to posts that were two thirds of the root length(12-mm long). Adhesive fixation of the post and ferrule incorporationmight decrease the effect of post length on the fracture resistance ofdowel-restored teeth (45, 81, 84).In conclusion, the optimum post length depends on several factorsincluding root length, crown height, level of bone support, and tech-nique of cementation. Adhesive cements, ferrule effect, and full coronalrestoration may reduce the effect of post length on the tooth fractureresistance (77, 84).
Post DiameterA smaller post diameter is recommended to retain more dentine
during preparation of post channel, which enhances the fracture resis-tance of dowel-restored teeth (39, 85). The ability of a tooth to resistfracture is directly related to the amount of remaining dentinearound the post (39, 86). Increased radicular dentinal stresses wereobserved when a post diameter was increased (58, 87). The largerthe post diameter the less the fracture resistance of a dowel-restoredtooth (39).
Recommendations regarding the adequate amount of radiculardentine around a post vary among researchers. One third of the rootwidth was recommended as the higher limit for the post diameter(52). Some researchers suggested the preservation of 1 mm of sounddentine around the post channel (25). Halle et al (88) recommendedthe preservation of more radicular dentine and suggested that 1.75 mmretained dentine around the post was sufficient to resist fracture of thetooth. In order to reduce failures and fractures, Mou et al (89) recom-mended that the optimum post to root diameter ratio should be approx-imately 1:4.
Post DesignTapered metal posts cause greater cervical stress concentration
than parallel-sided posts (75, 90). This was attributed to the wedgingeffect introduced by tapered posts. Apical stresses, on the otherhand, tend to be higher when parallel-sided posts are used (91).This was attributed to the sharp angles and reduced tooth structureat the apical area. A higher incidence of root fracture was reportedwhen tapered posts were used (50).
Threaded metal posts were associated with stress concentration atthe dentine-thread interface. Such areas can predispose crack forma-tion and jeopardize the fracture resistance of dowel-restored teeth(92). Decreasing the number of threads and increasing the spacesbetween them produces less harmful stresses (93). Prethreading thepost cavity and slight counter rotation of the post after engagementmay also reduce the harmful stresses produced by threads (48). Thereare no clinically available threaded fiber posts. However, Uddanwadikeret al (94) proposed a finite model of threaded fiber post and foundincreased stress concentration because of this post, which reducedthe fracture resistance.
Among various post designs, tapered threaded metal posts werereported as the most hazardous to the fracture resistance of dowel-restored teeth. Likewise, parallel serrated posts were the most favorablein this regard (14). Silva et al (95) compared four different metal poststo glass fiber posts and found better stress distribution within the teethrestored with glass fiber post. Furthermore, they found more stressconcentration at the coronary portion of metal posts. They concludedthat post material was more important for stress distribution than theexternal characteristics of the post. On the other hand, Signore et al(96) found that the survival rate of parallel-sided glass fiber posts
JOE — Volume 36, Number 9, September 2010
was more than that recorded for tapered ones over up to 8 years of func-tion.
Post MaterialThe mechanical properties of materials used for post construction
as well as their biocompatibility may influence the fracture resistance ofrestored teeth. Posts with higher modulus of elasticity like metals areassociated with higher failure loads (52, 97–103). However, theytend to cause catastrophic and irreparable root fractures when theyfail (97, 98, 100, 101, 104–106). Being more rigid than the tooth,high modulus elasticity posts produce stress concentration at criticalareas of the root and cause more fractures (58, 63). Unlike rigidposts, posts with a similar modulus of elasticity to dentine (eg, fiberposts) can distribute stresses more evenly along the post-dentine inter-face and cause less root fractures (56, 58, 63, 107).
Materials with a low modulus of elasticity bend more under loadand tend to fail before causing root fracture (108–110). Thisconstitutes a protective mechanism for the tooth structure. Manystudies showed high clinical survival and success rates for teethrestored with fiber posts (111–113). The vast majority of failureswere attributed to causes other than catastrophic tooth fracture.Cagidiaco et al (110) concluded that fiber posts outperform metal postsin treatment of root canal treated teeth. However, in a randomizedcontrolled clinical pilot study; Naumann et al (114) compared the clin-ical performance of titanium and fiber posts for 2 years and reportedsimilar successful clinical outcomes for both treatments.
Many studies showed better fracture resistance of teeth restoredwith fiber-reinforced resin posts (which had a similar rigidity todentine) when compared with metal or zirconia posts (which hada much higher modulus of elasticity than dentine) (45, 82, 98, 106,115–117). Cast posts and cores were frequently associated with deepcatastrophic root fractures (27, 28, 97, 118).
Nevertheless, Newman et al (119) and Toksavul et al (120) re-ported that less fracture resistance and more catastrophic root fractureswere associated with glass fiber posts when compared to zirconiumposts. Stockton and Williams (121) suggested that fiber post flexibilitymight cause stress redirection toward the post-tooth interface and thusincrease the failure rate. Furthermore, some studies reported no signif-icant difference in fracture resistance of restored teeth when fiber-reinforced resin or metal posts were used (118, 122, 123).Moreover, Fokkinga et al (123) found similar fracture patterns andbehaviors of premolars restored with metal crowns when either metalor fiber posts were used. Also, Nothdurft et al (23) reported no differ-ence in fracture modes and patterns when either titanium, quartz fiber,glass fiber, or zirconium dioxide posts were used to restore premolarswith class II cavity. Furthermore, Toman et al (124) found that teethrestored with resin cemented silica-coated titanium posts andcomposite cores had higher fracture resistance than teeth restoredwith resin-cemented zirconia or glass fiber posts (with or without silicacoating) and composite cores.
Corrosion resistance of post material may influence the fractureresistance of restored teeth. Metal posts were found to corrode overtime(125). It was proposed that corrosion products could migrate throughthe dentinal tubules and build up intratubular pressure, which predis-posed root fractures (13). Titanium posts have high corrosion resis-tance when compared with other metal alloys. Brass alloys, on theother hand, have very low corrosion resistance (13).
The storage of fiber posts in saline water reduces their fracturestrength and causes voids between the resin matrix and fibers (126).However, this does not occur if fiber posts are stored at in a conditionin mineral oil or in human teeth in saline water. This finding might
Fracture Resistance of Teeth Restored with Post-retained Restorations 1443

Review Article
explain some of the controversy found in the literature because differentstorage conditions used in different studies might affect fiber post frac-ture strength differently and thus affect the results.Post FittingGoracci et al (127) concluded that sliding friction was the main
factor that affected resistance to dislocation of resin-bonded fiber posts.Also, the use of dentine adhesive did not improve dislocation resistancewhen compared with the use of resin cement without dentine adhesive.The presence of interfacial gaps and the incomplete removal of smearlayer might be the reason for these findings.
Poorly fitted posts might create levers within the root canal,making the tooth more liable to fracture (128). Close adaptation ofposts to the canal walls was found to increase the fracture resistanceof restored teeth significantly (50). Santos et al (129) showed that lack-ing effective bonding between the root and posts with different elasticmodulus was associated with a higher risk of vertical root fracture inupper premolars. Schmitter et al (81) concluded that when fiberpost-restored teeth were crowned, centrally positioned fiber-reinforced posts did not contribute to load transfer as long as thebond between the tooth and composite core was intact and resin cementwas used to bond the fiber post.
Buttel et al (76) found that the fracture resistance of teeth restoredwith fiber posts and composite crowns without ferrules was not affectedby post fit within the root canal. Therefore, excessive post canal prep-aration to achieve optimal circumferential post fit is unjustifiablebecause it will not increase fracture resistance of teeth. Figure 1E pres-ents adequate post canal preparation when the cross-section of the rootis oval.
Core MaterialLess stiff cores are expected to deform under occlusal loads and
thus reduce the stress concentration within the dentine (108).Composite resins were reported to fracture under loads lower thanthose necessary to fracture the tooth (130). This is considered asa protective mechanism for tooth structure. Cast metal posts and coreswere associated with more root fractures than prefabricated posts andamalgam or composite cores (131). However, crown placement withadequate ferrule can mask the effect of core build ups on the fractureresistance of restored teeth (132–135). This was attributed to the factthat a crown restoration could favourably distribute stresses andredirect them toward the root (90,134).
Coating zirconia posts with tribochemical silica coating and silani-zation increases their fracture resistance and the bond strength tocomposite resin (136). When compared with no airborne particle abra-sion of the post surface, better long time bond strength to compositecores was recorded when zirconia posts were abraded using airborneparticle abrasion and received primer and silane coupling agent to theirsurface (137).
Fiber post surface can be treated by silane coupling agents orbonding agents to improve their bond to composite resins (138). Betterbond strength was recorded when silane coupling agents were used.Treatment of the fiber post surface with hydrogen peroxide before sila-nization increases the bond strength to composite cores more thanusing silane coupling agent alone (139). This might be caused by thedissolution of epoxy resin matrix of the post, which enhances bettersurface characteristics.
Monticelli et al (140) concluded that surface conditioningenhanced fiber post bonding properties. Also, the bond strength of pre-treated fiber posts to composite cores was satisfactory. However, ther-mocycling reduces the bond strength between fiber posts and
1444 Khaled AL-Omiri et al.
composite cores regardless of the pretreatment of the post surface(141).
Radovic et al (142) found that sandblasting increased the micro-tensile bond strength between composite cores and fiber posts. Further-more, they reported no benefit from further chairside treatment (ie,application of silane or bonding agent) of the sandblasted post surfacebecause this was associated with a reduction rather than an improve-ment of bond strength. The use of fiber posts improved the flexuralproperties of core composite resin regardless of the fiber directionin the fiber post (143).
When the post surface was treated with bonding agents before theaddition of the composite core, Artopoulou et al (144) recorded lessadhesive failures between fiber posts and composite cores than thatbetween composite cores and a titanium or stainless steel post.However, the lack of pretreatment of the post surface was associatedwith better retention between metal posts and composite cores thanbetween fiber posts and composite cores.
Core materials on titanium posts had better resistance to torsionalforces when the post surface is treated with chemical surface condi-tioning techniques such as silica coating (145). The bond betweencore material and the fiber post is chemical, and this increases theretention of cores when fiber posts are used. For stability, a reliablebond between the core material and the post should be generated.Schmitter et al (81) concluded that centrally positioned fiber-reinforced posts did not contribute to load transfer as long as thebond between the tooth and composite core was intact.
Ferrule EffectThe ferrule concept was proposed by Rosen (146) in 1961. He
recommended the use of a metal collar extension beyond the gingivalmargin of the core to encircle the tooth. The ferrule effect in associationwith post and core treatment was investigated by many researchers (47,147-150). Most of the previous studies were performed in vitro andgenerally have accepted that ferrules incorporated within cores orfinal crowns might increase the fracture resistance of restored teethby reinforcing their external surfaces to resist stresses accompaniedby functional lever forces. Ferrules also help to maintain the integrityof cement seal around the restoration (151).
Opinions vary regarding the optimum height and design ofadequate ferrule. However, most researchers recommendeda minimum 1- to 2-mm of ferrule height of almost parallel dentine wallsat the whole circumference of the tooth (47, 152). The higher theferrule the greater the fracture resistance (151). A uniform height ofthe ferrule at the whole tooth circumference was recommendedbecause it was found more effective in supporting the tooth thana nonuniform height (150). Al-Omiri and Al-Wahadni (99) reportedthat retaining coronal dentine did increase the fracture resistance ofteeth. However, they found that increasing the amount of retaineddentine more than 2 mm did not improve the tooth fracture resistanceany further. Schmitter et al (81) concluded that increased ferrule heightand resin bonding of the crown resulted in higher fracture loads ofteeth. They recommended the use of resin-bonding agents with crownsthat had a small ferrule height. Also, Dorriz et al (153) recommendedthe use of ferrule or bonding with an opaque porcelain layer (if castmetal post was used) to improve the fracture resistance of grosslydestroyed teeth.
Despite the large number of studies that supported the use offerrules, some researchers questioned the benefit of ferrules becausethey did not provide additional support for restored teeth (50, 104,135, 154, 155). Saupe et al (104) and Al-Hazaimeh and Gutteridge(154) concluded that the use of resin cements in their studies might
JOE — Volume 36, Number 9, September 2010

Review Article
have cancelled the effect of ferrule on the fracture resistance of restoredteeth. These findings were also supported by Mezzomo et al (155) whoreported no significant difference in fracture resistance of nonferruledspecimens restored with resin-cemented posts and ferruled ones. Whenzinc phosphate cement was used, ferruled specimens showed signifi-cantly higher fracture resistance than nonferruled ones. Moreover,Ng et al (156) reported a higher incidence of root fracture among teethrestored with bonded posts and cores when ferrules were incorporated.Also, Naumann et al (157) found that incomplete ferrules (that does notencircle 360� of the tooth) were associated with better tooth fractureresistance when compared with ferrules that totally encircle the tooth.They concluded that tooth structure preservation is more important forthe fracture resistance of post-treated teeth. The findings of these studiesunderlie that the incorporation of ferrules in conjunction with resin-cemented posts for the sake of tooth reinforcement might constitutean unjustifiable insult to the remaining tooth structure.The invasion of the biological width during tooth preparationshould be avoided (5). This creates a dilemma in cases in which noadequate height of tooth structure is remained above the crestal bonefor the incorporation of a ferrule. Surgical crown lengthening andorthodontic extrusion of the tooth may help in the establishment ofadequate ferrules in such cases (151). Besides patient discomfort, extracost and time are required for such procedures. Moreover, surgicalcrown lengthening is accompanied by the reduction of the effectiveroot length, which affects the crown:root ratio negatively. Gegauff(158) investigated the effect of crown lengthening for ferrule purposeson the failure loads of simulated analog teeth restored with post- andcore-retained crowns impeded within simulated periodontal ligamentand alveolar bone. He reported significantly lower failure loads of teeththat received crown lengthening and ferrules. The reduction of support-ing tissues combined with the altered crown:root ratio seemed toweaken the restored teeth even with the incorporation of ferrules.
The literature lacks retrospective and prospective clinical studiesthat investigated the ferrule effect. Torbjorner et al (27) reviewedrecords of 72 failed metal posts and observed more post fractures incases in which a ferrule was not incorporated. However, Cagidiaco etal (18) and Ferrari et al (19) found no role for ferrule effect on thesurvival of premolar teeth restored with fiber posts and compositecores. This could be caused by the effect of resin cements used forthe cementation of fiber posts and the close similarity between thevalues of the elastic modulus of fiber posts/resin cements and the elasticmodulus of dentine and thus obtain favorable stress distribution. Crowncoverage might also explain these results because it directs the load totooth finish line and bypasses the post-core assembly and thus directsstress towards the outer surface of the tooth and prevent tooth fracture.
More controlled clinical follow-ups are required to reach soundconclusions regarding the ferrule effect and its proposed benefits.Nevertheless, the available literature favors the incorporation of a ferrulefor final restorations. However, this should be in balance with theremaining tooth structure and crown:root ratio (11, 151).
Luting CementThe luting cement provides a buffer zone between the post and the
dentine, which might affect stress distribution upon loading (1). Brittleconventional cements like zinc phosphate may disintegrate upon func-tional loading and cause levers that concentrate stresses at the apicalroot portion and cause root fracture (159). Using adhesive cementsallows even stress distribution over the entire bonded surfaces. Conse-quently, a post can absorb functional stresses and then direct themtoward the long axis of root and thus make them more favourable(118). Spazzin et al (107) found that cements with a higher elastic
JOE — Volume 36, Number 9, September 2010
modulus caused higher stress concentration within the cement layer.Also, cement thickness did not affect stress distribution within thepost, dentine, or cement layer.
Previous studies concluded that resin-based cements couldincrease the fracture resistance of dowel-restored teeth (49, 104,154, 155, 160). Teeth restored with posts luted with resin cementswere found more resistant to fracture than teeth restored with postsluted with zinc phosphate or glass ionomer cements (49, 155, 161).According to these studies, the favorable behaviour of fiber-reinforced resin posts might be related to the resin cements frequentlyused to lute them rather than to the post material itself.
In order to obtain favorable stress distribution, the monoblocktype of restoration was recommended for the restoration of pulplessteeth (162). This treatment involves restoring the tooth with post,core, and crown using biomechanically homogenous bonded materialsand adhesive techniques. However, it proved difficult to predict orachieve this because it is difficult to clean the smear layer from theroot, to remove the water droplets and moisture from the root, andto use post and cement materials that do not shrink and have moduliof elasticity that match the dentine (163). The technique of cementationmight also affect the fracture resistance of restored teeth (13). Residueswithin a post space, bubbles within the cement layer, and excessiveseating pressure can cause stress concentration within the root andpredispose fracture (13).
Dietschi et al (164) recommended the use of specific combina-tions of adhesives and cements to overcome the problems of ovoid canalshape and dentine moisture that might reduce the efficacy of adhesionbetween the tooth and the post. Also, Kivanc and Gorgul (117)concluded that self-etching adhesives were better to use than etchand rinse adhesives for luting endodontic posts. An increased ferruleheight and resin bonding of a crown resulted in higher fracture loadsof post-restored teeth (81). Finally, Hammad et al (165) concludedthat the obturation of roots with resin-based obturation materialsincreased the resistance of teeth to vertical root fracture.
Coronal CoverageCrowning endodontically treated posterior teeth and badly
damaged anterior teeth increases their resistance to fracture, whereascrowning endodontically treated anterior teeth with intact coronalstructure does not improve their fracture resistance (13, 166, 167).Artificial crowns alter the distribution and transmission of stressesinto a post-root complex (90, 134, 168). Providing a crown withadequate ferrule has more influence on the fracture resistance ofdowel-restored teeth than factors related to post and core materialsand designs (134, 169). D’Arcangelo et al (170, 171) suggested theuse of fiber posts when veneer restorations were used to restoreendodontically treated teeth because they found that fiber postsincreased the fracture resistance of endodontically treated teethprepared for or restored with composite or porcelain veneers.
Remaining Coronal Tooth StructureSome studies suggested that fracture resistance of post-restored
teeth would be reduced if more coronal dental structures were lost(13, 73, 172, 173). In a retrospective long-term clinical study, Ferrariet al (112) concluded that the mechanical failure of teeth restored withfiber posts was related to the remaining coronal tissues. Similar resultswere reported in a follow-up clinical trial by Cagidiaco et al (110).
Nam et al (22) found that the fracture resistance of endodonticallytreated premolars with one to four remaining coronal walls was signif-icantly increased when they were restored with fiber posts. Moreover,teeth showed better stress distribution and fracture patterns when
Fracture Resistance of Teeth Restored with Post-retained Restorations 1445

Review Article
restored with fiber posts. However, fracture resistance of teeth with noremaining coronal walls was not improved when fiber posts were used.However, the relation between remaining coronal dentine and fractureresistance has been questioned by other researchers especially whencoronal coverage was provided because this might mask the effect ofthe retained tooth structure (104, 154, 174).Loading ConditionsThe magnitude and direction of functional loads play a major role
in stress concentration within dowel-restored teeth. Higher occlusalforces, like in cases of parafunctional habits, were associated withhigher failure rates of such teeth (175–177). Horizontal loads causea significantly higher stress concentration within dentine than loadsmore parallel to the long axis of the tooth (64, 90, 91, 148, 168,178–181). The effect of load direction on maximum stressesgenerated within restored teeth was found to be more significant thanthe effect of post design and dimensions (64, 90). Because of theirinclination, anterior teeth are most likely subjected to morehorizontally directed loads (13, 177). Post insertion would magnifystresses produced within dentine upon such loads (64). This is thereason behind the conception that the preservation of the coronal toothstructure of endodontically treated anterior teeth is more effective fortooth support than post insertion (13).
Meira et al (182) found that the effect of the elastic modulus ofa post on concentration, magnitude, and direction of dentinal stresswas dependent on load direction. They showed that when high-modulus posts were modeled, horizontal loads caused more stresson the apical area of roots and such a load suggested a vertical root frac-ture. On the other hand, they found that forces at 45� and 90� causedmore stress on the cervical area when low-modulus posts weremodeled; such loads suggested debonding of the post.
Alveolar Bone SupportA lower fracture resistance was reported among roots of peri-
odontally compromised teeth reconstructed with posts and cores(183). Naumann et al (184) concluded that the reduction of the levelof bone support would reduce the fracture resistance of fiber postsrestored teeth.
Alveolar bone level is considered a critical factor for stressconcentration and tooth fracture (185). Finite element studies reportedmassive increase in dentinal stresses as the alveolar bone level wasdiminished (91, 180). The loss of alveolar support will lower thelevel of the mechanical fulcrum, which in turn will jeopardize thefracture resistance of post restored teeth (158, 186).
In order to obtain adequate fracture resistance, at least 1:1crown:root ratio should be ensured and the post should extend beyondthe level of alveolar bone (77). Surgical crown lengthening can reducethe crown:root ratio and predispose tooth fracture. Gegauff (158) re-ported significantly lower failure loads of teeth that had crown length-ening even with the presence of a ferrule.
ConclusionsThe fracture resistance of post-restored teeth has been investigated
thoroughly in the literature. Previously, the argument was in favor of re-inforcing the teeth by endodontic posts. Nowadays, there is a generalagreement among researchers that posts per se do not offer reinforce-ment for restored teeth; on the contrary, their insertion involves proce-dures that usually sacrifice tooth structure and reduce the fractureresistance of teeth. Unrepairable root fractures have been frequently re-ported as the most catastrophic mode of failure that was associated withpost placement, especially when rigid posts were used.
1446 Khaled AL-Omiri et al.
The last 2 decades have witnessed a shift toward studying the effectof different post and core systems on the fracture resistance of dowel-restored teeth. Variety of available posts and introduction of newnon-metal post systems have greatly contributed to the large numberof available studies that handled this topic. Recently, a new shift occursagain in favour of using such posts as they are believed to even improvethe fracture resistance of endodontically treated teeth when comparedwith no post treatment. However, this new tendency lacks enoughevidence from long term randomized controlled clinical studies to setthis trend as the standard of future treatment of endodontically treatedteeth.
In order to avoid weakening of teeth by post placement, many postfeatures were thoroughly investigated. Because of the lack of long-termcontrolled clinical trials and the contradictory results of in vitrostudies, the optimum post features are not yet clearly determined.
It is important to keep in mind that the restoration of teeth usingposts does involve a system that consists of post, core material, andluting cement. The overlying crown and functional occlusal loads areadded to this system because they all influence the success of the wholetreatment. Therefore, it is less realistic to test fracture resistance of post-restored teeth without including the effect of coronal coverage, thedirection and magnitudes of masticatory forces, and the cyclic natureof functional loads. Failing to consider all this might be the reasonbehind the contradiction regarding the best post core luting agent touse in order to reduce tooth fracture or even strengthen the endodon-tically treated tooth.
The treatment of endodontically treated teeth using posts might bemore successful if tooth structure loss is limited, a ferrule is obtained,a post with similar physical properties to natural dentine is used, andadhesive techniques for post luting and coronal restoration are used.Therefore, when the advantages and disadvantages of different lutingagent-post-core systems and materials are considered, the adhesivelyluted resin/fiber posts with composite cores appear to be the bestoffered luting agent-post-core system currently available in terms oftooth fracture and biomechanical behaviour.
It is essential to keep in mind that these guidelines are basedmainly on ex vivo studies and to a lesser extent on limited in vivostudies. A lack of long-term controlled randomized clinical studies isthe main hindrance to reaching a conclusive and undisputable opinionregarding endodontic posts in terms of tooth fracture and biomechan-ical behavior.
AcknowledgmentThe authors thank Mrs AbdelAziz for all her help during the
preparation of this manuscript.
References1. Schwartz RS, Robbins JW. Post placement and restoration of endodontically
treated teeth: a literature review. J Endod 2004;30:289–301.2. Fennis WM, Kuijs RH, Kreulen CM, et al. A survey of cusp fractures in a population
of general dental practices. Int J Prosthodont 2002;15:559–63.3. Helfer AR, Melnick S, Schilder H. Determination of moisture content of vital and
pulpless teeth. Oral Surg Oral Med Oral Pathol 1972;34:661–70.4. Rivera EM, Yamauchi M. Site comparisons of dentine collagen cross-links from
extracted human teeth. Arch Oral Biol 1993;38:541–6.5. Peroz I, Blankenstein F, Lange K, et al. Restoring endodontically treated teeth with
posts and cores: a review. Quintessence Int 2005;36:737–46.6. Huang TJ, Schilder H, Nathanson D. Effects of moisture content and endodontic
treatment on some mechanical properties of human dentin. J Endod 1991;18:209–15.
7. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod1992;18:332–5.
8. Reeh ES. Reduction in tooth stiffness as a result of endodontic restorative proce-dures. J Endod 1989;15:512–6.
JOE — Volume 36, Number 9, September 2010

Review Article
9. Tang W, Wu Y, Smales RJ. Identifying and reducing risks for potential fractures inendodontically treated teeth. J Endod 2010;36:609–17.10. Mireku AS, Romberg E, Fouad AF, et al. Vertical fracture of root filled teeth
restored with posts: the effects of patient age and dentine thickness. Int Endod J2010;43:218–25.
11. Dietschi D, Duc O, Krejci I, et al. Biomechanical considerations for the restorationof endodontically treated teeth: a systematic review of the literature—Part 1.Composition and micro- and macrostructure alterations. Quintessence Int2007;38:733–43.
12. Randow K, Glantz P. On cantilever loading of vital and non-vital teeth. Acta OdontolScand 1986;44:271–7.
13. Fernandes A, Dessai G. Factors affecting the fracture resistance of post-core recon-structed teeth: a review. Int J Prosthod 2001;14:355–63.
14. Standlee JP, Caputo AA, Holcomb JP. The dentatus screw: comparative stress anal-ysis with endodontic dowels designs. J Oral Rehabil 1982;9:23–33.
15. Sokol DJ. Effective use of core and post concepts. J Prosthet Dent 1984;52:231–4.16. Silverstein WH. The reinforcement of endodontically treated teeth. Dent Clin North
Am 1964;14:372–81.17. Salameh Z, Ounsi HF, Aboushelib MN, et al. Fracture resistance and failure patterns
of endodontically treated mandibular molars with and without glass fiber post incombination with a zirconia-ceramic crown. J Dent 2008;36:513–9.
18. Cagidiaco MC, Garcıa-Godoy F, Vichi A, et al. Placement of fiber prefabricated orcustom made posts affects the 3-year survival of endodontically treated premolars.Am J Dent 2008;21:179–84.
19. Ferrari M, Cagidiaco MC, Grandini S, et al. Post placement affects survival ofendodontically treated premolars. J Dent Res 2007;86:729–34.
20. Salameh Z, Sorrentino R, Ounsi HF, et al. Effect of different all-ceramic crownsystem on fracture resistance and failure pattern of endodontically treated maxil-lary premolars restored with and without glass fiber posts. J Endod 2007;33:848–51.
21. Salameh Z, Sorrentino R, Ounsi HF, et al. The effect of different full-coveragecrown systems on fracture resistance and failure pattern of endodontically treatedmaxillary incisors restored with and without glass fiber posts. J Endod 2008;34:842–6.
22. Nam SH, Chang HS, Min KS, et al. Effect of the number of residual walls on fractureresistances, failure patterns, and photoelasticity of simulated premolars restoredwith or without fiber-reinforced composite posts. J Endod 2010;36:297–301.
23. Nothdurft FP, Seidel E, Gebhart F, et al. The fracture behavior of premolar teethwith class II cavities restored by both direct composite restorations andendodontic post systems. J Dent 2008;36:444–9.
24. Nothdurft FP, Seidel E, Gebhart F, et al. Influence of endodontic posts on the frac-ture behavior of crowned premolars with Class II cavities. J Dent 2008;36:287–93.
25. Sorensen JA, Martinoff JT. Intra-coronal reinforcement and coronal coverage:a study of endodontically treated teeth. J Prosthet Dent 1984;51:780–4.
26. Fuss Z, Lustig J, Katz A, et al. An evaluation of endodontically treated vertical rootfractured teeth: impact of operative procedures. J Endod 2001;27:46–8.
27. Torbjorner A, Karlsson S, Odman PA. Survival rate and failure characteristics fortwo post designs. J Prosthet Dent 1995;73:439–44.
28. Ferrari M, Vichi A, Garcıa-Godoy F. Clinical evaluation of fiber-reinforced epoxyresin posts and cast post and cores. Am J Dent 2000;13:15B–8.
29. Soares CJ, Soares PV, de Freitas Santos-Filho PC, et al. The influence of cavitydesign and glass fiber posts on biomechanical behavior of endodontically treatedpremolars. J Endod 2008;34:1015–9.
30. Pilo R, Shapenco E, Lewinstein I. Residual dentin thickness in bifurcated maxillaryfirst premolars after root canal and post space preparation with parallel-sideddrills. J Prosthet Dent 2008;99:267–73.
31. Butz F, Lennon A, Heydecke G, et al. Survival rate and fracture strength of endodon-tically treated maxillary incisors with moderate defects restored with different postand core systems, an in-vitro study. Int J Prosthodont 2001;14:58–64.
32. Lertchirakarn V, Palamara JE, Messer HH. Patterns of vertical root fracture: factorsaffecting stress distribution in the root canal. J Endod 2003;29:523–8.
33. Peters MC, Poort HW, Farah JW, et al. Stress analysis of a tooth restored with a postand core. J Dent Res 1983;62:760–3.
34. Toparli M. Stress analysis in a post-restored tooth utilizing the finite elementmethod. J Oral Rehabil 2003;30:470–6.
35. Fokkinga WA, Le Bell AM, Kreulen CM, et al. Ex vivo fracture resistance of directresin composite complete crowns with and without posts on maxillary premolars.Int Endod J 2005;38:230–7.
36. Mohammadi N, Kahnamoii MA, Yeganeh PK, et al. Effect of fiber post and cuspcoverage on fracture resistance of endodontically treated maxillary premolarsdirectly restored with composite resin. J Endod 2009;35:1428–32.
37. Torbjorner A, Fransson B. A literature review on the prosthetic treatment of struc-turally compromised teeth. Int J Prosthodont 2004;17:369–76.
38. Sidoli GE, King PA, Setchell DJ. An in vitro evaluation of a carbon fibre-based postand core system. J Prosthet Dent 1997;78:5–9.
JOE — Volume 36, Number 9, September 2010
39. Tjan AH, Whang SB. Resistance to root fracture of dowel channels with variousthicknesses of buccal dentin walls. J Prosthet Dent 1985;53:496–500.
40. Costa LC, Pegoraro LF, Bonfante G. Influence of different metal restorationsbonded with resin of fracture resistance of endodontically treated maxillarypremolars. J Prosthet Dent 1997;77:365–9.
41. Drummond JL, Bapna MS. Static and cyclic loading of fibre-reinforced dental resin.Dent Mater 2003;19:226–31.
42. Cohen BI, Pagnillo MK, Newman I, et al. Pilot study of the cyclic fatigue character-istics of five endodontic posts with four core materials. J Oral Rehabil 2000;27:83–92.
43. Mannocci F, Ferrari M, Watson TF. Microleakage of endodontically treated teethrestored with fibre posts and composite cores after cyclic loading: a confocalmicroscopic study. J Prosthet Dent 2001;85:284–91.
44. Martinez-Gonzalez A, Amigo-Borras V, Fons-Font A, et al. Response of three typesof cast posts and cores to static loading. Quintessence Int 2001;32:552–60.
45. Isidor F, Brondum K, Ravnholt G. The influence of post length and crown ferrulelength on the resistance to cyclic loading of bovine teeth with prefabricated tita-nium posts. Int J Prosthodont 1999;12:78–82.
46. Hayashi M, Sugeta A, Takahashi Y, et al. Static and fatigue fracture resistances ofpulpless teeth restored with post-cores. Dent Mater 2008;24:1178–86.
47. Hu S, Osada T, Shimizu T, et al. Resistance to cyclic fatigue and fracture of struc-turally compromised root restored with different post and core restorations. DentMater J 2005;24:225–31.
48. Ross RS, Nicholls JI, Harrington GW. A comparison of strains generated duringplacement of five endodontic posts. J Endod 1991;17:450–6.
49. Mendoza D, Eakle W, Kahl E, et al. Root reinforcement with a resin bonded pre-formed post. J Prosthet Dent 1997;78:10–4.
50. Sorensen JA, Engelman MJ. Effect of post adaptation on fracture resistance ofendodontically treated teeth. J Prosthet Dent 1990;64:419–24.
51. King P, Setchell D. An in vitro evaluation of a prototype CFRC prefabricated postdeveloped for the restoration of pulpless teeth. J Oral Rehabil 1990;17:599–609.
52. Sirimai S, Riis DN, Morgano SM. An in vitro study of the fracture resistance and theincidence of vertical root fracture of pulpless teeth restored with six post-and-coresystems. J Prosthet Dent 1999;81:262–9.
53. Eskitascioglu G, Belli S, Kalkan M. Evaluation of two post core systems using twodifferent methods: fracture strength test and a finite elemental stress analysis.J Endod 2002;28:629–33.
54. Naumann M, Metzdorf G, Fokkinga W, et al. Influence of test parameters on in vitrofracture resistance of post-endodontic restorations: a structured review. J OralRehabil 2009;36:299–312.
55. Loney W. Three-dimensional photoelastic stress analysis of the ferrule effect in castpost and core. J Prosthet Dent 1990;63:506–12.
56. Assif D, Oren E, Marshak BL, et al. Photoelastic analysis of stress transfer byendodontically treated teeth to the supporting structure using different restorativetechniques. J Prosthet Dent 1989;61:535–43.
57. Cohen BI, Pagnillo M, Musikant BL, et al. Comparison of the retentive and photoe-lastic properties of two prefabricated endodontic post systems. J Oral Rehabil1999;26:488–94.
58. Albuquerque Rde C, Polleto LT, Fontana RH, et al. Stress analysis of an uppercentral incisor restored with different posts. J Oral Rehabil 2003;30:936–43.
59. Pegoretti A, Fambri L, Zappini G, et al. Finite element analysis of a glass fibre re-inforced composite endodontic post. Biomaterials 2002;23:2667–82.
60. Pierrisnard L, Bohin F, Renault P, et al. Corono-radicular reconstruction of pulp-less teeth: a mechanical study using finite element analysis. J Prosthet Dent 2002;88:442–8.
61. Ho MH, Lee SY, Chen HH, et al. Three-dimensional finite element analysis of theeffects of posts on stress distribution in dentin. J Prosthet Dent 1994;72:367–72.
62. Lewgoy HR, Youssef MN, Matson MR, et al. Finite elements study of the Flexi Postand Flexi Flange post systems in a maxillary central incisor. Pesqui Odontol Bras2003;17:132–6.
63. Lanza A, Aversa R, Rengo S, et al. 3D FEA of cemented steel, glass and carbon postsin a maxillary incisor. Dent Mater 2005;21:709–15.
64. Yang HS, Lang LA, Molina A, et al. The effects of dowel design and load direction ondowel-and-core restorations. J Prosthet Dent 2001;85:558–67.
65. Asmussen E, Peutzfeldt A, Sahafi A. Finite element analysis of stresses in endodon-tically treated, dowel-restored teeth. J Prosthet Dent 2005;94:321–9.
66. Khani MM, Tafazzoli-Shadpour M, Aghajani F, et al. Mechanical vulnerability oflower second premolar utilising visco-elastic dynamic stress analysis. ComputMethods Biomech Biomed Engin 2009;12:553–61.
67. Guzy GE, Nicholls JI. In vitro comparison of intact endodontically treated teeth withand without endo-post reinforcement. J Prosthet Dent 1979;42:39–44.
68. Cailleteau JG, Rieger MR, Akin JE. A comparison of intracanal stresses in a post-restored tooth utilizing the finite element method. J Endod 1992;18:540–4.
69. Holmes DC, Diaz-Arnold AM, Leary JM. Influence of post dimension on stressdistribution in dentin. J Prosthet Dent 1996;75:140–7.
Fracture Resistance of Teeth Restored with Post-retained Restorations 1447

Review Article
70. Darendeliler S, Darendeliler H, Kinoglu T. Analysis of a central maxillary incisor byusing a three-dimensional finite element method. J Oral Rehabil 1992;19:371–83.71. Kishen A, Ramamurty U, Asundi A. Experimental studies on the nature of property
gradients in the human dentine. J Biomed Mater Res 2000;51:650–9.72. Kishen A, Kumar GV, Chen NN. Stress-strain response in human dentine: rethinking
fracture predilection in postcore restored teeth. Dent Traumatol 2004;20:90–100.73. Fan P, Nicholls JI, Kois JC. Load fatigue of five restoration modalities in structurally
compromised premolars. Int J Prosthodont 1995;8:213–20.74. Thorsteinsson TS, Yaman P, Craig RG. Stress analyses of four prefabricated posts.
J Prosthet Dent 1992;67:30–3.75. Davy DT, Dilley GL, Krejci RF. Determination of stress patterns in root-filled teeth
incorporating various dowel designs. J Dent Res 1981;60:1301–10.76. Buttel L, Krastl G, Lorch H, et al. Influence of post fit and post length on fracture
resistance. Int Endod J 2009;42:47–53.77. Leary JM, Aquilino SA, Svare CW. An evaluation of post length within the elastic
limits of dentine. J Prosthet Dent 1987;57:277–81.78. Hunter AJ, Feiglin B, Williams JF. Effects of post placement on endodontically
treated teeth. J Prosthet Dent 1989;62:166–72.79. Burns DA, Krause WR, Douglas HB, et al. Stress distribution surrounding
endodontic posts. J Prosthet Dent 1990;64:412–8.80. Lambjerg-Hansen H, Asmussen E. Mechanical properties of endodontic posts.
J Oral Rehabil 1997;24:882–7.81. Schmitter M, Rammelsberg P, Lenz J, et al. Teeth restored using fiber-reinforced
posts: in vitro fracture tests and finite element analysis. Acta Biomater 2010;6:3747–54.
82. Giovani AR, Vansan LP, de Sousa Neto MD, et al. In vitro fracture resistance ofglass-fiber and cast metal posts with different lengths. J Prosthet Dent 2009;101:183–8.
83. Cecchin D, Farina AP, Guerreiro CA, et al. Fracture resistance of roots prostheti-cally restored with intra-radicular posts of different lengths. J Oral Rehabil 2010;37:116–22.
84. Nissan J, Dmitry Y, Assif D. The use of reinforced composite resin cement ascompensation for reduced post length. J Prosthet Dent 2001;86:304–8.
85. Sorensen JA, Engelman MJ. Effect of post adaptation on fracture resistance ofendodontically treated teeth. J Prosthet Dent 1990;64:419–24.
86. Assif D, Gorfil C. Biomechanical considerations in restoring endodontically treatedteeth. J Prosthet Dent 1994;71:565–7.
87. Mattison GD. Photoelastic stress analysis of cast-gold endodontic posts. J ProsthetDent 1982;48:407–11.
88. Halle E, Nicholls J, Hassel V. An in vitro comparison of hollow post and core anda custom hollow post and core. J Endod 1984;10:96–100.
89. Mou YB, Chen YM, Smales RJ, et al. Optimum post and tooth root diameters fora cast post-core system. Am J Dent 2009;22:311–4.
90. McAndrew R, Jacobsen PH. The relationship between crown and post design onroot stress—a finite element study. Eur J Prosthodont Restor Dent 2002;10:9–13.
91. Reinhardt RA, Krejci RF, Pao YC, et al. Dentin stresses in post reconstructed teethwith diminishing bone support. J Dent Res 1983;62:1002–8.
92. Mentink AG, Creugers NH, Hoppenbrouwers PM, et al. Qualitative assessment ofstress distribution during insertion of endodontic posts in photoelastic material.J Dent 1998;26:125–31.
93. Deutsch AS, Musikant BL, Cavallari J. Retentive properties of a new post and coresystem. J Prosthet Dent 1985;53:12–4.
94. Uddanwadiker RV, Padole PM, Arya H. Effect of variation of root post in differentlayers of tooth: linear vs nonlinear finite element stress analysis. J Biosci Bioeng2007;104:363–70.
95. Silva NR, Castro CG, Santos-Filho PC, et al. Influence of different post design andcomposition on stress distribution in maxillary central incisor: finite element anal-ysis. Indian J Dent Res 2009;20:153–8.
96. Signore A, Benedicenti S, Kaitsas V, et al. Long-term survival of endodonticallytreated, maxillary anterior teeth restored with either tapered or parallel-sidedglass-fiber posts and full-ceramic crown coverage. J Dent 2009;37:115–21.
97. Martinez-Insua A, da Silva L, Rilo B, et al. Comparison of the fracture resistances ofpulpless teeth restored with a cast post and core or carbon-fibre post witha composite core. J Prosthet Dent 1998;80:527–32.
98. Fokkinga WA, Kreulen CM, Vallittu PK, et al. A structured analysis of in vitro failureloads and failure modes of fiber, metal, and ceramic post-and-core systems. Int JProsthodont 2004;17:476–82.
99. Al-Omiri MK, Al-Wahadni AM. An ex vivo study of the effects of retained coronaldentine on the strength of teeth restored with composite core and different postand core systems. Int Endod J 2006;39:890–9.
100. Bonfante G, Kaizer OB, Pegoraro LF, et al. Fracture strength of teeth with flared rootcanals restored with glass fibre posts. Int Dent J 2007;57:153–60.
101. Al-Wahadni AM, Hamdan S, Al-Omiri M, et al. Fracture resistance of teeth restoredwith different post systems: in vitro study. Oral Surg Oral Med Oral Pathol Oral Ra-diol Endod 2008;106:e77–83.
1448 Khaled AL-Omiri et al.
102. Ozcan M, Valandro LF. Fracture strength of endodontically-treated teeth restoredwith post and cores and composite cores only. Oper Dent 2009;34:429–36.
103. McLaren JD, McLaren CI, Yaman P, et al. Dennison JD, McDonald NJ. The effect ofpost type and length on the fracture resistance of endodontically treated teeth.J Prosthet Dent 2009;101:174–82.
104. Saupe WA, Gluskin AH, Radke RA Jr. A comparative study of fracture resistancebetween morphologic dowel and cores and a resin-reinforced dowel system inthe intraradicular restoration of structurally compromised roots. QuintessenceInt 1996;27:483–91.
105. Akkayan B, Caniklioglu B. Resistance to fracture of crowned teeth restored withdifferent post systems. Eur J Prosthodont Rest Dent 1998;6:13–8.
106. Hajizadeh H, Namazikhah MS, Moghaddas MJ, et al. Effect of posts on the fractureresistance of load-cycled endodontically-treated premolars restored with directcomposite resin. J Contemp Dent Pract 2009;10:10–7.
107. Spazzin AO, Galafassi D, de Meira-Junior AD, et al. Influence of post and resincement on stress distribution of maxillary central incisors restored with directresin composite. Oper Dent 2009;34:223–9.
108. Caputo AA, Standlee JP. Biomechamics in Clinical Dentistry. Chicago: QuintessencePublishing Co; 1987:185–203.
109. Bitter K, Kielbassa AM. Post-endodontic restorations with adhesively luted fiber-reinforced composite post systems: a review. Am J Dent 2007;20:353–60.
110. Cagidiaco MC, Goracci C, Garcia-Godoy F, et al. Clinical studies of fiber posts:a literature review. Int J Prosthodont 2008;21:328–36.
111. Grandini S, Goracci C, Tay FR, et al. Clinical evaluation of the use of fiber posts anddirect resin restorations for endodontically treated teeth. Int J Prosthodont 2005;18:399–404.
112. Ferrari M, Cagidiaco MC, Goracci C, et al. Long-term retrospective study of the clin-ical performance of fiber posts. Am J Dent 2007;20:287–91.
113. Piovesan EM, Demarco FF, Cenci MS, et al. Survival rates of endodontically treatedteeth restored with fiber-reinforced custom posts and cores: a 97-month study. IntJ Prosthodont 2007;20:633–9.
114. Naumann M, Sterzenbac G, Alexandra F, et al. Randomized controlled clinical pilottrial of titanium vs. glass fiber prefabricated posts: preliminary results after up to 3years. Int J Prosthodont 2007;20:499–503.
115. Akkayan B, Gulmez T. Resistance to fracture of endodontically treated teethrestored with different post systems. J Prosthet Dent 2002;87:431–7.
116. Hayashi M, Takahashi Y, Imazato S, et al. Fracture resistance of pulpless teethrestored with post-cores and crowns. Dent Mater 2006;22:477–85.
117. Kivanc BH, Gorgul G. Fracture resistance of teeth restored with different postsystems using new-generation adhesives. J Contemp Dent Pract 2008;9:33–40.
118. Cormier CJ, Burns DR, Moon P. In vitro comparison of the fracture resistance andfailure mode of fibre, ceramic, and conventional post systems at various stages ofrestoration. J Prosthodont 2001;10:26–36.
119. Newman MP, Yaman P, Dennison J, et al. Fracture resistance of endodonticallytreated teeth restored with composite posts. J Prosthet Dent 2003;89:360–7.
120. Toksavul S, Toman M, Uyulgan B, et al. Effect of luting agents and reconstructiontechniques on the fracture resistance of pre-fabricated post systems. J Oral Rehabil2005;32:433–40.
121. Stockton LW, Williams PT. Retention and shear bond strength of two post systems.Oper Dent 1999;24:210–6.
122. Hu YH, Pang LC, Hsu CC, et al. Fracture resistance of endodontically treated ante-rior teeth restored with four post-and-core systems. Quintessence Int 2003;34:349–53.
123. Fokkinga WA, Kreulen CM, Le Bell-Ronnlof AM, et al. In vitro fracture behavior ofmaxillary premolars with metal crowns and several post-and-core systems. Eur JOral Sci 2006;114:250–6.
124. Toman M, Toksavul S, Sarikanat M, et al. Fracture resistance of endodonticallytreated teeth: effect of tooth coloured post material and surface conditioning.Eur J Prosthodont Restor Dent 2010;18:23–30.
125. Pameijer CH, Glantz P, Mobasherat MA. On clinical corrosion of pins. Swed Dent J1983;7:161–7.
126. Vano M, Carvalho C, Sedda M, et al. The influence of storage condition and dura-tion on the resistance to fracture of different fiber post systems. Am J Dent 2009;22:366–70.
127. Goracci C, Fabianelli A, Sadek FT, et al. The contribution of friction to the dislo-cation resistance of bonded fiber posts. J Endod 2005;31:608–12.
128. Turner CH. Post retained crown failure: a survey. Dent Update 1982;9:193–202.
129. Santos AF, Tanaka CB, Lima RG, et al. Vertical root fracture in upper premolarswith endodontic posts: finite element analysis. J Endod 2009;35:117–20.
130. Bex RT, Parker MW, Judkins JT, et al. Effect of dentinal bonded resin post-corepreparations on resistance to vertical root fracture. J Prosthet Dent 1992;67:768–72.
131. Chan RW, Bryant RW. Post-core foundations for endodontically treated posteriorteeth. J Prosthet Dent 1982;48:401–6.
JOE — Volume 36, Number 9, September 2010

Review Article
132. Assif D, Bitenski A, Pilo R, et al. Effect of post design on resistance to fracture ofendodontically treated teeth with complete crowns. J Prosthet Dent 1993;69:36–40.133. Gelfand M, Goldman M, Sunderman EJ. Effect of complete veneer crowns on the
compressive strength of endodontically treated posterior teeth. J Prosthet Dent1984;52:635–8.
134. Pilo R, Cardash HS, Levin E, et al. Effect of core stiffness on the in vitro fracture ofcrowned, endodontically treated teeth. J Prothet Dent 2002;88:302–6.
135. Sorensen JA, Engelman MJ. Ferrule design and fracture resistance of endodonti-cally treated teeth. J Prosthet Dent 1990;63:529–36.
136. Xible AA, de Jesus Tavarez RR, de Araujo Cdos R, et al. Effect of silica coating andsilanization on flexural and composite-resin bond strengths of zirconia posts: An invitro study. J Prosthet Dent 2006;95:224–9.
137. Akgungor G, Sen D, Aydin M. Influence of different surface treatments on the short-term bond strength and durability between a zirconia post and a composite resincore material. J Prosthet Dent 2008;99:388–99.
138. Aksornmuang J, Nakajima M, Foxton RM, et al. Regional bond strengths of a dual-cure resin core material to translucent quartz fiber post. Am J Dent 2006;19:51–5.
139. Yenisey M, Kulunk S. Effects of chemical surface treatments of quartz and glassfiber posts on the retention of a composite resin. J Prosthet Dent 2008;99:38–45.
140. Monticelli F, Osorio R, Sadek FT, et al. Surface treatments for improving bondstrength to prefabricated fiber posts: a literature review. Oper Dent 2008;33:346–55.
141. Bitter K, Neumann K, Kielbassa AM. Effects of pretreatment and thermocycling onbond strength of resin core materials to various fiber-reinforced composite posts.J Adhes Dent 2008;10:481–9.
142. Radovic I, Monticelli F, Goracci C, et al. The effect of sandblasting on adhesion ofa dual-cured resin composite to methacrylic fiber posts: microtensile bondstrength and SEM evaluation. J Dent 2007;35:496–502.
143. Hattori M, Takemoto S, Yoshinari M, et al. Durability of fiber-post and resin corebuild-up systems. Dent Mater J 2010;29(2):224–8.
144. Artopoulou II, O’Keefe KL, Powers JM. Effect of core diameter and surface treat-ment on the retention of resin composite cores to prefabricated endodontic posts.J Prosthodont 2006;15:172–9.
145. Akisxli I, Ozcan M, Nergiz I. Effect of surface conditioning techniques on the resis-tance of resin composite core materials on titanium posts. Quintessence Int 2003;34:766–71.
146. Rosen H. Operative procedure in mutilated endodontically treated teeth. J ProsthetDent 1961;11:973–86.
147. Barkhordar RA, Radke R, Abbasi J. Effect of metal collars on resistance ofendodontically treated teeth to root fracture. J Prosthet Dent 1989;61:676–8.
148. Loney RW, Moulding MB, Ritsco RG. The effect of load angulation on fracture resis-tance of teeth restored with cast posts and cores and crowns. Int J Prosthodont1995;8:247–51.
149. Akkayan B. An in vitro study evaluating the effect of ferrule length on fracture resis-tance of endodontically treated teeth restored with fibre reinforced and zirconiadowel systems. J Prosthet Dent 2004;92:155–62.
150. Tan PL, Aquilino SA, Gratton DG, et al. In vitro fracture resistance of endodonticallytreated central incisors with varying ferrule heights and configurations. J ProsthetDent 2005;93:331–6.
151. Stankiewicz NR, Wilson PR. The ferrule effect: a literature review. Int Endod J 2002;35:575–81.
152. Libman WJ, Nicholls JI. Load fatigue of teeth restored with cast posts and cores andcomplete crowns. Int J Prosthodont 1995;8:155–61.
153. Dorriz H, Alikhasi M, Mirfazaelian A, et al. Effect of ferrule and bonding on thecompressive fracture resistance of post and core restorations. J Contemp DentPract 2009;10:1–8.
154. Al-Hazaimeh N, Gutteridge DL. An in vitro study into the effect of the ferrule prep-aration on the fracture resistance of crowned teeth incorporating prefabricatedpost and composite core restorations. Int Endod J 2001;34:40–6.
155. Mezzomo E, Massa F, Libera SD. Fracture resistance of teeth restored with twodifferent post-and-core designs cemented with two different cements: an in vitrostudy. Part I. Quintessence Int 2003;34:301–6.
156. Ng CC, al-Bayat MI, Dumbrigue HB, et al. Effect of no ferrule on failure of teethrestored with bonded posts and cores. Gen Dent 2004;52:143–6.
157. Naumann M, Preuss A, Rosentritt M. Effect of incomplete crown ferrules on loadcapacity of endodontically treated maxillary incisors restored with fiber posts,composite build-ups, and all-ceramic crowns: an in vitro evaluation after chewingsimulation. Acta Odontol Scand 2006;64:31–6.
JOE — Volume 36, Number 9, September 2010
158. Gegauff AG. Effect of crown lengthening and ferrule placement on static load failureof cemented cast post-cores and crowns. J Prosthet Dent 2000;84:169–79.
159. Mitchell CA. Selection of materials for post cementation. Dent Update 2000;27:350–4.
160. Junge T, Nicholls JI, Phillips KM, et al. Load fatigue of compromised teeth:a comparison of three luting cements. Int J Prosthodont 1998;11:558–64.
161. Naumann M, Sterzenbach G, Rosentritt M, et al. Is adhesive cementation ofendodontic posts necessary? J Endod 2008;34:1006–10.
162. Dallari A, Rovatti L. Six years of in vitro/in vivo experience with Composipost.Compend Contin Educ Dent 1996;17:S57–63.
163. Tay FR, Pashley DH. Monoblocks in root canals: a hypothetical or a tangible goal.J Endod 2007;33:391–8.
164. Dietschi D, Duc O, Krejci I, et al. Biomechanical considerations for the restorationof endodontically treated teeth: a systematic review of the literature, Part II (Eval-uation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int 2008;39:117–29.
165. Hammad M, Qualtrough A, Silikas N. Effect of new obturating materials on verticalroot fracture resistance of endodontically treated teeth. J Endod 2007;33:732–6.
166. Vire DE. Failure of endodontically treated teeth: classification and evaluation.J Endod 1991;17:338–42.
167. Aquilino SA, Caplan DJ. Relationship between crown placement and the survival ofendodontically treated teeth. J Prosthet Dent 2002;87:256–63.
168. Joshi S, Mukherjee A, Kheur M, et al. Mechanical performance of endodonticallytreated teeth. Finite Elem Anal Des 2001;37:587–601.
169. Heydecke G, Butz F, Strub JR. Fracture strength and survival rate of endodonticallytreated maxillary incisors with approximal cavities after restoration with differentpost and core systems: an in-vitro study. J Dent 2001;29:427–33.
170. D’Arcangelo C, De Angelis F, Vadini M, et al. In vitro fracture resistance and deflec-tion of pulpless teeth restored with fiber posts and prepared for veneers. J Endod2008;34:838–41.
171. D’Arcangelo C, De Angelis F, Vadini M, D’Amario M, Caputi S. Fracture resistanceand deflection of pulpless anterior teeth restored with composite or porcelainveneers. J Endod 2010;36(1):153–6.
172. Al-Wahadni A, Gutteridge DL. An in vitro investigation into the effects of retainedcoronal dentine on the strength of a tooth restored with a cemented post andpartial core restoration. Int Endod J 2002;35:913–8.
173. Sorrentino R, Monticelli F, Goracci C, et al. Effect of post-retained composite resto-rations and amount of coronal residual structure on the fracture resistance ofendodontically-treated teeth. Am J Dent 2007;20:269–74.
174. Patel A, Gutteridge DL. An in vitro investigation of cast post and partial core design.J Dent 1996;24:281–7.
175. Bergman B, Lundquist P, Sjogren U, et al. Restorative and endodontic results aftertreatment with cast posts and cores. J Prosthet Dent 1989;61:10–5.
176. Bender IB, Freedland JB. Adult root fracture. J Am Dent Assoc 1983;107:413–9.177. Mehta SB, Millar BJ. A comparison of the survival of fibre posts cemented with two
different composite resin systems. Br Dent J 2008;205:E23.178. Yaman SD, Karacaer O, Sahin M. Stress distribution of post-core applications in
maxillary central incisors. J Biomater Appl 2004;18:163–77.179. Abu-Hammad O, Dar-Odeh N. Factors affecting the stress picture in a molar tooth
restored with an endodontic post retained filling. Part 1: the stress picture with thesystem under various loading conditions. Cairo Dent J 2004;20:121–4.
180. Pao YC, Reinhardt RA, Krejci RF. Root stresses with tapered end post design in peri-odontally compromised teeth. J Prosthet Dent 1987;57:281–6.
181. Kalachev YS. Analysis of stresses in hard dental tissues generated by clinical appli-cation of retentive root canal posts. Folia Med (Plovdiv) 2004;46:42–6.
182. Meira JB, Esposito CO, Quitero MF, et al. Elastic modulus of posts and the risk ofroot fracture. Dent Traumatol 2009;25:394–8.
183. Nyman S, Lindhe J. A longitudinal study of combined periodontal and prosthetictreatment of patients with advanced periodontal disease. J Periodontol 1979;50:163–9.
184. Naumann M, Rosentritt M, Preuss A, et al. The effect of alveolar bone loss on theload capability of restored endodontically treated teeth: a comparative in vitrostudy. J Dent 2006;34:790–5.
185. Hunter AJ, Flood AM. The restoration of endodontically treated teeth. Part 2. Posts.Aust Dent J 1989;34:5–12.
186. Chen XM, Wu XH, Niu L, et al. Effects of the loss of alveolar bone on the areas ofperiodontal ligament, mechanical fulcrum and fracture resistance of root and post-core system. Sichuan Da Xue Xue Bao Yi Xue Ban 2005;36:853–7.
Fracture Resistance of Teeth Restored with Post-retained Restorations 1449

CONSORT Randomized Clinical Trial
The Effect of Premedication with Ibuprofen andIndomethacin on the Success of Inferior Alveolar Nerve Blockfor Teeth with Irreversible PulpitisMasoud Parirokh, DDS, MSc,* Rezvan Ashouri, DMD,
†Ali Reza Rekabi, DMD,
†
Nouzar Nakhaee, MD,‡
Abbas Pardakhti, PhD,§
Sara Askarifard, DMD, MS,*
and Paul V. Abbott, DDS, PhDk
Abstract
Introduction: Achieving pulp anesthesia with irrevers-ible pulpitis is difficult. This study evaluated whethernonsteroidal anti-inflammatory drugs assist local anes-thesia. Methods: In a randomized double-blinded clin-ical trial, 150 patients (50 per group) with irreversiblepulpitis were given placebo, 600 mg ibuprofen, or75mg indomethacin 1 hour before local anesthesia.Each patient recorded their pain score on a visual analogscale before taking the medication, 15 minutes afteranesthesia in response to a cold test, during accesscavity preparation and during root canal instrumenta-tion. No or mild pain at any stage was considereda success. Data were analyzed by the chi-square andanalysis of variance tests. Results: Overall success ratesfor placebo, ibuprofen, and indomethacin were 32%,78%, and 62%, respectively (p < 0.001). Ibuprofenand indomethacin were significantly better than placebo(p < 0.01). There was no difference between ibuprofenand indomethacin (p = 0.24). Conclusions: Premedica-tion with ibuprofen and indomethacin significantlyincreased the success rates of inferior alveolar nerveblock anesthesia for teeth with irreversible pulpitis.(J Endod 2010;36:1450–1454)Key WordsAnesthesia, ibuprofen, indomethacin, inferior alveolarnerve block, irreversible pulpitis, nonsteroidal anti-inflammatory drugs, placebo
From the *Oral and Dental Research Center, †EndodonticDepartment, ‡Neuroscience Research Center, and§Pharmaceutics Research Center, Kerman University of MedicalSciences, Kerman, Iran; and kSchool of Dentistry, University ofWestern Australia, Perth, Australia.
Supported by the Neuroscience Research Center, KermanUniversity of Medical Sciences.
Address requests for reprints to Dr Masoud Parirokh, Oraland Dental Research Center, Kerman University of MedicalSciences, Kerman, Iran.0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.007
1450 Parirokh et al.
Pain control particularly during the early phases of endodontic treatment is of para-mount importance and makes both the dentist and the patient confident and
comfortable for the remainder of the treatment (1). The inferior alveolar nerve block(IANB) is the conventional method for anesthetizing mandibular molar teeth (2, 3).Research has shown that gaining anesthesia in mandibular molars with irreversiblepulpitis is much more difficult in comparison to the teeth with normal healthy pulps(4–6). Some investigations have been performed to overcome pulp pain thatremains despite having had an IANB injection (2, 3, 7–14). Numerous investigationshave been performed to increase the success rate of anesthesia during dental, andparticularly endodontic, procedures such as the use of various anesthetic techniquesand solutions as well as pretreatment with analgesics (7–25).
The concept of using preoperative analgesic drugs to increase the effectiveness ofIANB is based on reports of their beneficial effects on reducing postoperative pain (23).Previous investigations using analgesics before administering IANB have reported con-flicting results (10, 23–25). For example, Modaresi et al (23) reported significantimprovements in the success rate of IANB in teeth with inflamed pulps after the useof analgesics, and Ianiro et al (10) reported higher success rates although they werenot significantly different. In contrast, two separate studies reported no significantdifference in IANB success rates when the patients were premedicated with analgesics(24, 25). Several reasons could explain these promising but not completely differentresults such as an insufficient number of subjects (10) and a lack of similarity ofmethods and clinical conditions (23). The aim of this study was to compare two typesof nonsteroidal anti-inflammatory (NSAID) medication (ibuprofen and indomethacin)with a placebo regarding their effects on the success rates of IANB for endodontic treat-ment of mandibular molar teeth with irreversible pulpitis.
Materials and MethodsThis study was approved by the Ethics Committee of Kerman University of Medical
Sciences in Iran (no. KA/ 88-05 and Iranian Registry of Clinical Trials ID no.138803192016N1). The calculation of sample size was based on a medium effectsize of 0.5, an a error of 0.05, and power at 0.8. The sample size was calculatedwith PASS software version 6.0 (NCSS, Kaysville, UT). Based on sample size calculations,up to 50 patients were required in each group.
The following inclusion and exclusion criteria were used for this study. The exclu-sion criteria were the presence of systemic disorders, a sensitivity to lidocaine with1:80,000 epinephrine, a sensitivity to NSAIDs, nasal polyp, a history of gastrointestinalulcers, the presence of widening of the periodontal ligament space, the presence ofa periapical radiolucency, lactation, pregnancy, using any type of analgesic medicationin the preceding 12 hours before the treatment, having a tooth not suitable for resto-ration, and having a full crown.
Inclusion criteria included healthy patients having a first or second mandibularmolar tooth with irreversible pulpitis and normal periapical radiographic appearance.The clinical diagnosis of irreversible pulpitis was confirmed by a response to an electricpulp test (The Element Diagnostic Unit; SybronEndo, Glendora, CA) and a prolonged
JOE — Volume 36, Number 9, September 2010

CONSORT Randomized Clinical Trial
exaggerated response (10 seconds) with moderate to severe pain toa cold test (Roeko Endo-Frost; Roeko, Langenau, Germany) after thesize 2 cotton pellet was removed.One hundred fifty patients were eligible to participate in thisprospective, randomized double-blind study. All patients were adultsover 18 years of age, and they were treated in the postgraduate clinicof the Endodontic Department of Kerman Dental School in Iran fromSeptember 2009 to February 2010. Informed consent of all subjectswho participated in this study was obtained after the nature of the proce-dure and the possible discomforts and risks had been fully explained.All patients who agreed to participate in the study were randomlydivided into three groups of 50 patients each. In order to randomizethe patients, the numbers of patients in each group were written onpaper, and each one was kept in a sealed opaque envelope. Each patientwas asked to choose one of the envelopes and based on the number wasassigned to one of the groups. A pharmacist (AP) was responsible forpreparing the capsules and encoding them to ensure that neither theclinicians nor the patients were aware of the placebo or NSAIDs medi-cation being taken.
All patients were given a capsule of the same color and size 1 hourbefore starting the treatment. The capsules contained either a placebo oflactose powder (placebo group), 600 mg ibuprofen (ibuprofen group)(Hakim Pharmaceutical Co, Tehran, Iran), or 75mg indomethacin(indomethacin group) (Hakim Pharmaceutical Co). Before takingthe capsules, the patients were asked to rate their pain using a Heft-Parker visual analog pain scale (VAS) after the cold test. The VAS scoreswere divided into four categories. No pain corresponded to 0 mm, mildpain was defined as being >0 mm and $54 mm, moderate pain wasdefined as being >54 mm and <114 mm, and severe pain was definedas being $114 mm.
A side-loading cartridge syringe (Dena Instruments; ForgemanInstruments Co, Sialkot, Pakistan) was used to administer the injec-tions. The syringe was equipped with a blood aspiration device anda thumb ring. A 27-G 38-mm needle (Carpule; Heraeus KulzerGmbH, Hanau, Germany) was fitted to the syringe. A blood aspirationtest was performed before the IANB was administered. In all patients,after needle insertion and based on a standard IANB method (26),when bone contact was established, the needle was withdrawn 1 to 2mm and aspiration was performed. If the aspiration was negative forblood, then the anesthetic solution (2% lidocaine with 1/80000epinephrine; Darupakhsh, Tehran, Iran) was injected. One cartridge(1.8 mL) was used in each patient. Fifteen minutes after administeringanesthesia, each patient was asked about any signs of soft-tissue anes-thesia. If the patient did not report profound lip numbness, then theIANB was considered to be a failure, and the patient was excludedfrom the study. In IANB successful patients, the teeth were again testedwith the same cold pulp sensibility test, and the patients were asked torate their pain using the Heft-Parker VAS. Then, the teeth were isolatedwith a rubber dam, and endodontic access cavity preparation wascommenced. Access cavity preparation was only started in patientswho reported lip numbness after administration of the anesthetic.
TABLE 1. Comparison of Baseline Variables between Groups
Characteristic Group 1 (n = 50) Gro
Age 25.9 (�6.0)Sex (%)
Male 22 (44.0)Female 28 (56.0)
Before-anesthesiapain score
106.3 (�24.9) 1
*Significant difference between groups 1 and 3.
JOE — Volume 36, Number 9, September 2010
The patients were instructed to rate any pain experienced duringeach step of access cavity preparation. This was recorded as pain withindentin, when entering the pulp chamber, or when a file was inserted intothe root canals. No or mild pain (faint, weak, and mild pain) were clas-sified as success, whereas moderate and severe pain were classified asthe failure of anesthesia. If a patient reported sensitivity to the cold testbefore starting the access cavity preparation or at any time during subse-quent treatment, another method of anesthesia was then used in orderto be able to continue with the treatment. All patients were monitoredfor 48 hours after the procedure. Chi-square and ANOVA tests wereused to compare qualitative and quantitative data between the threegroups. Because there were differences in VAS scores before medica-tion among the three groups, a repeated-measure ANCOVA was usedto compare variations in VAS scores. The comparisons were consideredsignificant if p < 0.05.
ResultsNone of the patients reported any side effects for up to 48 hours
after the procedures. Table 1 shows the distribution of the baselinecharacteristics of the participants in the present study. The youngestand the oldest participants were 18 and 64 years old, respectively. Nosignificant differences were found between sex or age among thepatients in the three groups (p > 0.05). The only significant differencewas the degree of preoperative pain before using medications (Table 1)with the patients in the indomethacin group showing significantly higherpain scores when they initially presented for treatment (p < 0.03).
The average pain score 1 hour after the medication was takenbased on the Heft-Parker VAS were not significantly different amongthe three groups (p = 0.540) (Fig. 1). However, after adjusting forbaseline VAS scores, there was a significant difference in the amountof pain relief between patients who were given placebo and thosewho took either indometacin or ibuprofen (p < 0.001). All patients re-ported lip numbness, which was assumed to be a sign of IANB success.
The overall success rates for the placebo, ibuprofen, and indo-methacin groups were 32%, 78%, and 62%, respectively (p < 0.001)(Table 2). The ibuprofen and indomethacin groups showed signifi-cantly higher success rates compared with the placebo group (p <0.01). There was no significant difference between ibuprofen and indo-methacin (p = 0.24).
Overall, 64 of the 150 patients failed to show complete success ofanesthesia throughout the present study (placebo group = 34,ibuprofen group = 11, and indomethacin group = 19). Thirty of thesepatients showed sensitivity to the cold pulp test 15 minutes after anes-thesia. Distribution of the failure and success of anesthesia duringdifferent stages of the endodontic procedures is shown in Figure 2for all groups.
DiscussionThe results of the present study have shown that premedication
with two types of NSAIDs (ibuprofen and indomethacin) significantly
up 2 (n = 50) Group 3 (n = 50) p value
26.2 (�9.5) 26.2 (�5.7) 0.962
26 (52.0) 23 (46.0) 0.70624 (48.0) 27 (54.0)
14.4 (�27.0) 120.2 (�26.5) 0.030*
Ibuprofen vs Indomethacin for Inferior Alveolar Nerve Block 1451

TABLE 2. Comparison of Success Rates between the Three Groups
End result
Group Success (%) Failure (%) p value*
1 16 (32) 34 (68) 0.001†
2 39 (78) 11 (22)3 31 (62) 19 (38)
*Chi-square test.†There was a significant difference between groups 1 and 2 and between groups 1 and 3 (p < 0.01)
using pair-wise comparisons with the Bonferroni correction.
Figure 1. Severity of pain scores at different stages: before and 1 hour aftermedication and 15 minutes after the administration of local anesthesia. Thisshows a higher pain rating before starting treatment in the indomethacin group(sample size in each group = 50).
CONSORT Randomized Clinical Trial
increased the success rate of IANB anesthesia for mandibular molarteeth with irreversible pulpitis. The demographic characteristics ofthe patients, such as sex and age, were not significantly different inall three groups (Table 1). Therefore, these factors did not influencethe results. In contrast, the premedication pain scores were significantlyhigher in the indomethacin group than in the other groups (p < 0.05).No significant difference in pain score among the three groups beforeanesthesia confirms the potential of indomethacin as an effectiveadjunctive analgesic for pain during endodontic treatment of teethwith irreversible pulpitis.
Figure 2. Frequency distribution of the stages of failure and success among the thrpain after anesthesia and during access preparation (sample size in each group =
1452 Parirokh et al.
In the present study, of the 120 patients who had no response tothe cold pulp test 15 minutes after anesthesia, 34 reported pain duringaccess cavity preparation or during instrumentation of the root canals.Similar findings have been reported in previous studies, which confirmsthat no response to a cold test is not a guarantee that complete pulpanesthesia has been achieved and that no pain will be felt during rootcanal treatment (5, 10, 15).
Previous studies that have assessed the effectiveness of anesthesiaafter premedication have used either an electric pulp test or a VAS (10,23–25) to rate pain. In the present study, the Heft-Parker VAS was usedto assess patient pain before and after local anesthetic injection. Most ofthe previous investigations on the efficacy of anesthetic techniques andsolutions have used the same method of evaluation (9, 12, 13, 24, 25,27, 28).
In the present study, 2% lidocaine with 1:80000 epinephrine wasused because this is a common anesthetic solution in dental practiceplus most of the previous investigations have used the same solution.The latter allows comparison between studies of the effects of differenttechniques and/or medications on pulp anesthesia (2, 4, 7, 9, 10, 12,13, 18, 22, 23).
Significantly higher amounts of prostaglandins in inflamed pulpscompared with normal pulps have been reported (29). Prostaglandinscan affect tetrodotoxin-resistant receptors and decrease nerveresponses to anesthetic agents (30, 31). Previous investigations havedescribed the anti-inflammatory effects of ibuprofen and indomethacin
ee groups (placebo, ibuprofen, and indomethacin) based on patients reported50).
JOE — Volume 36, Number 9, September 2010

CONSORT Randomized Clinical Trial
(32, 33). Several subtypes of sodium channels play important roles inmediating inflammatory pain, such as Nan 1.7, Nan 1.8, and Nan 1.9(34). Gould et al (33) in their animal study showed that prostaglandinsplay an important role in sodium channel augmentation during inflam-mation and that pretreatment with ibuprofen prevented up-regulation ofNan1.7 and Nan1.8 sodium channels. In particular, the effects of Nan1.7were greater.Ibuprofen has been used in previous investigations for pretreat-ment or posttreatment analgesia (10, 23). Seymour and Ward (35)evaluated various doses of ibuprofen (200 mg, 400 mg, and 600 mg)for the management of postoperative dental pain, and they reporteda trend of higher pain relief in patients who had taken 600-mg doses.
Indomethacin has not been commonly used or recommended inendodontic therapy. However, it has strong anti-inflammatory effects,and, therefore, it was used as one of the analgesics in the present study.Indomethacin is an NSAID that is used for the management of moderateto severe muscular and joint pain (36). However, indomethacin hasseveral side effects that should be considered before prescribing thismedication (36). Shrestha et al (37), in a randomized clinical trial, re-ported that both indomethacin and ketorolac provided similar pain re-lief for patients with gouty arthritis. Ketorolac has been successfully usedto manage endodontic pain (38, 39), and, therefore, it could beextrapolated that indomethacin may have similar effects forendodontic pain. In the present study, only one single dose ofindomethacin was prescribed in order to minimize the possibility ofany side effects for the patients. In addition, the patients weremonitored for 48 hours, and there were no reports of any sideeffects. This may either show a reasonable case selection or thata single dose of either medication is unlikely to cause significantproblems for the patients. Despite the previously mentioned efficacyof indomethacin, ibuprofen may be a better choice because it notonly showed significant effects on the success rate of anesthesia, butit also has fewer side effects than indomethacin.
Several other investigations have evaluated the efficacy of premed-ication on IANB success rates for teeth with irreversible pulpitis (10,23–25). Modaresi et al (23) reported significantly lower sensitivity toelectric pulp tests after premedication with either 400 mg ibuprofenor a combination of 600 mg acetaminophen with 40 mg codeinecompared with the placebo group. In other studies, the root canal treat-ment was commenced, and the patients’ responses during treatmentwere evaluated, which is more similar to clinical situations (10, 24,25). Hence, in the present study, endodontic treatment wasperformed, and the patients’ pain experiences during treatment wereevaluated in addition to using a cold pulp sensibility test.
Ianiro et al (10) studied 40 patients with irreversible pulpitis, andthey reported a trend toward greater success with an IANB afterpretreatment with analgesic drugs although they could not show a signif-icant difference between the placebo and analgesic groups. In contrast,in the present study of 150 patients, both types of NSAIDs showed signif-icantly higher success rates compared with the placebo group. Thedifference in statistical significance between these two studies is likelyto be a result of the difference in the number of patients, and this empha-sizes the need to include as many subjects as possible in such studies.
In contrast to the previously mentioned studies, two other investi-gations have reported no significant differences between ketorolac, 400mg ibuprofen, and 800 mg ibuprofen for patients with irreversible pul-pitis (24, 25). The differences between the inclusion criteria for thevarious studies may be a further reason for conflicting results. In thecurrent study, as well as the study by Ianiro et al (10), only patientswith irreversible pulpitis confirmed by a prolonged pain in responseto a cold pulp test were selected for treatment. In contrast, in boththe Aggarwal et al (24) and Oleson et al. (25) studies, patients were
JOE — Volume 36, Number 9, September 2010
selected on the basis of having spontaneous pain, and they had beenreferred to an emergency clinic for endodontic treatment.
The degree and duration of pulp inflammation when a patient pres-ents for treatment may be another factor contributing to conflictingresults regarding the efficacy of the pretreatment use of analgesics(10, 23–25). In an animal study, Modaresi et al (40) showed that in-flamed dental pulp is resistant to local analgesic. Based on the resultsof the present study and previous investigations (10, 23-25), it can behypothesized that premedication with an analgesic in emergencypatients is not effective because the previously released prostaglandinshave already resulted in the formation of TTx-resistant receptors, and,therefore, the analgesic has no significant adjunctive effect on traditionalanesthetic techniques such as an IANB. In contrast, the use of premed-ication in patients who have had prolonged pain to cold without spon-taneous pain may improve the effectiveness of IANB anesthesia.
In the current investigation, the overall success rates for theplacebo, ibuprofen, and indomethacin groups were 32%, 78%, and62%, respectively. These figures are similar to the study by Ianiro etal (10) who reported 46.2%, 71.4%, and 76.9% success rates forplacebo, acetaminophen, and a combination of acetaminophen withibuprofen, respectively. The current study suggests that combinationsof analgesics are not required and that the use of only one anti-inflammatory drug is just as effective as when combined with acetamin-ophen.
Although more effective anesthesia was obtained when an NSAIDanalgesic was prescribed before treatment, neither drug providedcomplete anesthesia during endodontic treatment of teeth with irrevers-ible pulpitis. Therefore, dentists should also be prepared to use othersupplementary anesthetic techniques to overcome patient’s discomfortwhenever encountered pain in treating teeth with irreversible pulpitis(16, 21). In conclusion, the results of the present study support theuse of NSAID premedication before administering local anesthesia inpatients with irreversible pulpitis if there is no spontaneous painreported by the patient.
References1. Walton RE, Reader A, Nusstein JM. Local anesthesia. In: Torabinejad M, Walton RE,
eds. Endodontics, Principles and Practice. 4th ed. St Louis, MO: Saunders Elsevier;2008:129–47.
2. McLean C, Reader A, Beck M, et al. An evaluation of 4% prilocaine and 3% mepi-vacaine compared with 2% lidocaine (1:100,000 epinephrine) for inferior alveolarnerve block. J Endod 1993;19:146–50.
3. Yared GM, Dagher FB. Evaluation of lidocaine in human inferior alveolar nerveblock. J Endod 1997;23:575–8.
4. Tortamano IP, Siviero M, Costa CG, et al. A comparison of the anesthetic efficacy ofarticaine and lidocaine in patients with irreversible pulpitis. J Endod 2009;35:165–8.
5. Reisman D, Reader A, Nist R, et al. Anesthetic efficacy of the supplemental intraoss-eous injection of 3% mepivacaine in irreversible pulpitis. Oral Surg Oral Med OralPathol Oral Radiol Endod 1997;84:676–82.
6. Hargreaves KM, Keiser K. Local anesthetic failure in endodontics: mechanisms andmanagement (a review). Endod Topics 2002;1:26–39.
7. Robertson D, Nusstein J, Reader A, et al. The anesthetic efficacy of articaine inbuccal infiltration of mandibular posterior teeth. J Am Dent Assoc 2007;138:1104–12.
8. Haase A, Reader A, Nusstein J, et al. Comparing anesthetic efficacy of articaine versuslidocaine as a supplemental buccal infiltration of the mandibular first molar after aninferior alveolar nerve block. J Am Dent Assoc 2008;139:1228–35.
9. Bigby J, Reader A, Nusstein J, et al. Anesthetic efficacy of lidocaine/meperidine forinferior alveolar nerve blocks in patients with irreversible pulpitis. J Endod 2007;33:7–10.
10. Ianiro SR, Jeansonne BG, McNeal SF, et al. The effect of preoperative acetaminophenor a combination of acetaminophen and Ibuprofen on the success of inferior alve-olar nerve block for teeth with irreversible pulpitis. J Endod 2007;33:11–4.
11. Corbett IP, Kanaa MD, Whitworth JM, et al. Articaine infiltration for anesthesia ofmandibular first molars. J Endod 2008;34:514–8.
Ibuprofen vs Indomethacin for Inferior Alveolar Nerve Block 1453

CONSORT Randomized Clinical Trial
12. Mikesell P, Nusstein J, Reader A, et al. A comparison of articaine and lidocaine forinferior alveolar nerve blocks. J Endod 2005;31:265–70.13. Claffey E, Reader A, Nusstein J, et al. Anesthetic efficacy of articaine for inferior
alveolar nerve blocks in patients with irreversible pulpitis. J Endod 2004;30:568–71.
14. Reitz J, Reader A, Nist R, et al. Anesthetic efficacy of the intraosseous injection of0.9mL of 2% lidocaine (1:100,000 epinephrine) to augment an inferior alveolarnerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:516–23.
15. Reader A, Nusstein, Hargreaves KM. Local anesthesia in endodontics. In: Cohen S,Hargreaves KM, eds. Pathways of the Pulp. 9th ed. St Louis, MO: Mosby Elsevier;2006:691–723.
16. Kanaa MD, Whitworth JM, Corbett IP, et al. Articaine buccal infiltration enhances theeffectiveness of lidocaine inferior alveolar nerve block. Int Endod J 2009;42:238–46.
17. Kanaa MD, Whitworth JM, Corbett IP, et al. Articaine and lidocaine mandibularbuccal infiltration anesthesia: a prospective randomized double-blind cross-overstudy. J Endod 2006;32:296–8.
18. Foster W, Drum M, Reader A, et al. Anesthetic efficacy of buccal and lingual infiltra-tions of lidocaine following an inferior alveolar nerve block in mandibular posteriorteeth. Anesth Prog 2007;54:163–9.
19. Jung IY, Kim JH, Kim ES, et al. An evaluation of buccal infiltrations and inferior alve-olar nerve blocks in pulpal anesthesia for mandibular first molars. J Endod 2008;34:11–3.
20. Meechan JG, Kanaa MD, Corbett IP, et al. Pulpal anaesthesia for mandibular perma-nent first molar teeth: a double-blind randomized cross-over trial comparing buccaland buccal plus lingual infiltration injections in volunteers. Int Endod J 2006;39:764–9.
21. Matthews R, Drum M, Reader A, et al. Articaine for supplemental buccal mandibularinfiltration anesthesia in patients with irreversible pulpitis when the inferior alveolarnerve block fails. J Endod 2009;35:343–6.
22. Rosenberg PA, Amin KG, Zibari Y, et al. Comparison of 4% articaine with 1:100,000epinephrine and 2% lidocaine with 1:100,000 epinephrine when used as a supple-mental anesthetic. J Endod 2007;33:403–5.
23. Modaresi J, Dianat O, Mozayeni MA. The efficacy comparison of ibuprofen,acetaminophen-codeine, and placebo premedication therapy on the depth of anes-thesia during treatment of inflamed teeth. Oral Surg Oral Med Oral Pathol Oral Ra-diol Endod 2006;102:399–403.
24. Aggarwal V, Singla M, Kabi K. Comparative evaluation of effect of preoperative oralmedication of ibuprofen and ketorolac on anesthetic efficacy of inferior alveolarnerve block with lidocaine in patients with irreversible pulpitis: a prospective,double-blind, randomized clinical trial. J Endod 2010;36:375–8.
1454 Parirokh et al.
25. Oleson M, Drum M, Reader A, et al. Effect of preoperative ibuprofen on the successof the inferior alveolar nerve block in patients with irreversible pulpitis. J Endod2010;36:379–82.
26. Malamed SF. Handbook of Local Anesthesia. 5th ed. St Louis, MO: Mosby; 2004.227–54.
27. McCartney M, Reader A, Beck M. Injection pain of the inferior alveolar nerve blockin patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2007;104:571–5.
28. Parirokh M, Satvati A, Sharifi R, et al. Efficacy of combining a buccal infiltration withan inferior alveolar nerve block for mandibular molars with irreversible pulpitis.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:468–73.
29. Nakanishi T, Matsuo T, Ebisu S. Quantitative analysis of immunoglobulins andinflammatory factors in human pulpal blood from exposed pulps. J Endod 1995;21:131–6.
30. Hargreaves KM, Karl Keiser, Byrne BE. Analgesics in endodontics. In: Cohen S,Hargreaves KM, eds. Pathways of the Pulp. 9th ed. St Louis, MO: Mosby; 2006:668.
31. Henry MA, Hargreaves KM. Peripheral mechanisms of odontogenic pain. Dent ClinNorth Am 2007;51:19–44.
32. Wassef M, Pelage JP, Velzenberger E, et al. Anti-inflammatory effect of ibuprofen-loaded embolization beads in sheep uterus. J Biomed Mater Res B Appl Biomater2008;86:63–73.
33. Gould HJ 3rd, England JD, Soignier RD, et al. Ibuprofen blocks changes in Nav 1.7and 1.8 sodium channels associated with complete Freund’s adjuvant-inducedinflammation in rat. Pain 2004;5:270–80.
34. Gibbs JL, Hargreaves KM. Mechanisms of odontogenic and non-odontogenic pain.In: Ingle JI, Backland LK, Baumgartner JG, eds. Endodontics. 6th ed. Hamilton, On-tario, Canada: BC Decker Inc; 2008:376–91.
35. Seymour R, Ward P. Evaluation of different doses of soluble ibuprofen and ibuprofentablets in postoperative dental pain. Br J Oral Maxillofac Surg 1996;34:110–4.
36. Indomethacin web page. National Center for Biotechnology Information website.Available at: http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=meds&log$=drug_bottom_one&part=a681027. Accessed February 15, 2010.
37. Shrestha M, Morgan D, Moreden J, et al. Randomized double-blind comparison ofthe analgesic efficacy of intramuscular ketorolac and oral indomethacin in the treat-ment of acute gouty arthritis. Ann Emerg Med 1995;26:682–6.
38. Rogers MJ, Johnson BR, Remeikis NA, et al. Comparison of effect of intracanal use ofketorolac trimethamine and dexamethasone with oral ibuprofen on post treatmentendodontic pain. J Endod 1999;25:381–4.
39. Battrum D, Gutmann J. Efficacy of ketorolac in the management of pain associatedwith root canal treatment. J Can Dent Assoc 1996;62:36–42.
40. Modaresi J, Dianat O, Soluti A. Effect of pulp inflammation on nerve impulse qualitywith or without anesthesia. J Endod 2008;34:438–41.
JOE — Volume 36, Number 9, September 2010

Clinical Research
Diagnosis of Vertical Root Fractures in EndodonticallyTreated Teeth Based on Clinical and Radiographic Indices: ASystematic ReviewIgor Tsesis, DMD,* Eyal Rosen, DMD,* Aviad Tamse, DMD,* Silvio Taschieri, MD, DDS,
†
and Anda Kfir, DMD*
Abstract
Introduction: The diagnosis of vertical root fracture(VRF) is at times complicated for lack of specific signs,symptoms, and/or radiographic features. The purposeof this study was to systematically search and evaluatethe literature regarding the diagnostic accuracy of clin-ical signs and symptoms and radiographic indices forthe diagnosis of VRF in endodontically treated teethby means of a systematic review. Methods: An exhaus-tive literature search combined with strict inclusion andexclusion criteria was undertaken to identify clinicalstudies that assessed the diagnosis of VRF. Results:There is no substantial evidence regarding the accuracyof the clinical and radiographic indices for the diagnosisof VRF in endodontically treated teeth. Conclusions:Evidence-based data concerning the diagnostic accuracyand clinical effectiveness of clinical and radiographicdental evaluation for the diagnosis of VRF in endodon-tically treated teeth are lacking. The need forevidence-based research efforts to elucidate thecurrently unknown situation is of utmost significance.(J Endod 2010;36:1455–1458)Key WordsDiagnosis, systematic review, vertical root fracture
From the *Department of Endodontology, Maurice and Ga-briela Goldschleger School of Dental Medicine, Tel Aviv Univer-sity, Tel Aviv, Israel; and †IRCCS Istituto Ortopedico Galeazzi,Department of Odontology, University of Milan, Milan, Italy.
Address requests for reprints to Dr Igor Tsesis, Departmentof Endodontology, Maurice and Gabriela Goldschleger Schoolof Dental Medicine, Tel Aviv University, Tel Aviv, Israel.E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.003
JOE — Volume 36, Number 9, September 2010
Vertical root fracture (VRF) in endodontically treated teeth is one of the most frus-trating complications of root canal therapy, which results in the tooth or root extrac-
tion (1–4). The VRF is a longitudinally oriented fracture of the root that originates fromits apical end and propagates coronally (5) and is defined as one of the crack types (5).The incidence of vertically fractured teeth has not been described in the literature.However, the prevalence was reported to range from 11%–20% of VRFs in extractedendodontically treated teeth (6, 7).
VRF is usually diagnosed years after all endodontic and prosthetic procedures havebeen completed (8). The final diagnosis of VRF is at times complicated for lack ofspecific signs, symptoms, and/or radiographic features and because several etiologicfactors might be involved. Thus, the differential diagnosis from other pathologic entitiesmight be difficult (3, 8–14).
Evidence-based dentistry is an approach to oral healthcare that integrates the bestavailable clinical evidence to support a practitioner’s clinical expertise for each patient’streatment needs and preferences (15–17). It is based on the process of systematicallyfinding, apprising, and using research findings as the basis for clinical decision-making.Systematic reviews constitute the basis for practicing evidence-based dentistry (15, 17,18). The application of evidence-based dentistry in diagnosis should result in a reduc-tion of errors in the clinical decision-making process (15–18). Thus, evidence-basedreview of the available literature regarding the clinical and radiographic features ofendodontically treated vertically root fractured teeth is of utmost importance (2, 4).
The aim of this study was to systematically search and evaluate the literature regardingthe diagnostic accuracy of clinical signs and symptoms and radiographic indices for thediagnosis of VRF in endodontically treated teeth by means of a systematic review.
Materials and MethodsCriteria for Considering Studies for This Review
This systematic review included clinical studies that assessed the diagnosis of VRFconsistent with the following definition: complete or incomplete fracture initiated fromthe root at any level (5). Case reports, reviews, in vitro studies, and studies of teeth withvital pulps were not included in the review.
The studies had to include patients with confirmed VRFs (target condition) inendodontically treated teeth. Studies with at least one of the following reference stan-dards for VRF confirmation were included (reference standard defined as the best avail-able method for establishing the presence or absence of the target condition (19)). TheVRFs were confirmed during surgical flap procedure, the VRFs were confirmed aftertooth extraction, or the VRFs were identified radiographically as clearly discernableseparation of segments of fractured roots.
The studies had to include detailed data regarding the clinical signs and symptomsand the radiographic findings of the evaluated teeth. Table 1 summarizes the criteria forinclusion of studies in the systematic review.
Search Methods for Identification of StudiesThe following electronic databases were searched. MEDLINE database was
searched by using Evidents web-based search engine (http://medinformatics.uthscsa.
Diagnosis of VRFs in Endodontically Treated Teeth 1455

TABLE 1. Criteria for Inclusion of Studies in the Systematic Review
1. Clinical studies that assessed the diagnosis of VRF.2. VRF definition corresponded with the description of
complete or incomplete fracture initiated from the root atany level.
3. Only endodontically treated teeth were included.4. VRF confirmation method was in accordance with the
defined reference standards.5. Detailed data were included regarding the clinical signs and
symptoms and radiographic findings of the evaluated teeth.
VRF, vertical root fractures.
Clinical Research
edu/EviDents/), by using the key words ‘‘vertical root fracture OR ‘‘longi-tudinal root fracture’’, and applying Entrez PubMed limits to ‘‘humans’’and ‘‘English’’. MeSH received the following: (vertical[All Fields] AND(‘‘plant roots’’[MeSH Terms] OR (‘‘plant’’[All Fields] AND ‘‘roots’’[AllFields]) OR ‘‘plant roots’’[All Fields] OR ‘‘root’’[All Fields]) AND(‘‘fractures, bone’’[MeSH Terms] OR (‘‘fractures’’[All Fields] AND‘‘bone’’[All Fields]) OR ‘‘bone fractures’’[All Fields] OR ‘‘fracture’’[AllFields])) OR (longitudinal[All Fields] AND (‘‘plant roots’’[MeSHTerms] OR (‘‘plant’’[All Fields] AND ‘‘roots’’[All Fields]) OR ‘‘plantroots’’[All Fields] OR ‘‘root’’[All Fields]) AND (‘‘fractures, bone’’[-MeSH Terms] OR (‘‘fractures’’[All Fields] AND ‘‘bone’’[All Fields])OR ‘‘bone fractures’’[All Fields] OR ‘‘fracture’’[All Fields])) NOT(‘‘animals’’[MeSH:noexp] NOT ‘‘humans’’[MeSH Terms]) AND (‘‘hu-mans’’[MeSH Terms] AND English[lang]). Scopus search (www.scopus.com) was searched by using the key words ‘‘vertical root frac-ture’’ OR ‘‘longitudinal root fracture’’, by using these filters: articles,limited to dentistry, English language. Query received the following:TITLE-ABS-KEY(‘‘vertical root fracture’’ OR ‘‘longitudinal root frac-ture’’) AND (LIMIT-TO(DOCTYPE, ‘‘ar’’)) AND (LIMIT-TO(SUBJAREA,‘‘DENT’’) OR LIMIT-TO(SUBJAREA, ‘‘MULT’’)) AND (LIMIT-TO(LAN-GUAGE, ‘‘English’’)). Embase database (http://www.embase.com) wassearched by using the key words ‘‘vertical root fracture’’ OR ‘‘longitudinalroot fracture’’, with these limits: humans, English, article, Embase only.MeSH received the following: (’vertical root fracture’ OR ’longitudinalroot fracture’) AND [article]/lim AND [humans]/lim AND [english]/lim AND [embase]/lim.
Related articles, literature reviews that appeared in the MEDLINEsearch engine, and textbook chapters were evaluated, and their refer-ence lists were manually checked.
Data Collection and AnalysisSelection of Studies. The articles were initially evaluated for rele-vance, on the basis of their titles and abstracts, by 3 observers indepen-dently (I.T., A.T., E.R.). Possibly relevant studies were submitted to a fulltext evaluation. The full texts of the studies were obtained and reviewedfor suitability. Cases of disagreement were discussed together untilagreement was achieved. Eventually, the identified suitable articleswere subjected to data extraction, assessment of the methodologicalquality, and data analysis.
Data Extraction. Data were to be extracted by 3 observers indepen-dently. Cases of disagreement were to be subject to joint evaluation bythe observers until an agreement was achieved.
For each study the following methodological parameters were tobe recorded: authors and date of publication; study’s purpose; samplesize; demographic details of the subjects including criteria for inclusion;study design; reference standard type; evaluation methods including thepresence of multiple evaluators, calibration of evaluators, randomiza-tion, and evaluators’ blinding; homogeneity of the subjects; statisticalanalysis type and quality; and funding source.
1456 Tsesis et al.
The following index tests, defined as tests performed to reduce theuncertainty about the presence of the target condition (19, 20), were tobe recorded: tenderness to percussion and/or palpation, presence ofa sinus tract, pain, swelling, presence of periradicular radiolucency,presence of an osseous defect/periodontal pocket, gender and age ofthe patient, tooth type, coronal restoration type, and presence of post.
Methodological Quality Assessment and Data Synthesisand Analysis. On the basis of the study methodological parameters,an assessment of the methodological quality of the included studies wasplanned to be undertaken following the recommendations of the guesteditorial on evidence-based dentistry published by the Journal ofEndodontics in 2009 (15) and the recommendations of ‘‘The CochraneHandbook for Systematic Reviews of Diagnostic Test Accuracy’’ (20).
The diagnostic accuracy was planned to be calculated bycomparing the results of the index tests with the outcomes of the refer-ence standards (16, 19, 21).
ResultsThe search in MEDLINE database by using Evidents web-based
search engine covered all articles published in dental journals inEnglish from 1971–January 2010 and resulted in 197 articles, of which19 were eligible for inclusion (3, 10, 14, 22–37) on the basis of theirtitles and abstracts. The other 178 articles were rejected; 62 were foundto be irrelevant to the topic of the present study, 14 were review articles,52 were case reports, and 50 were ex vivo studies.
The search with Scopus database resulted in 117 articles, of which5 articles (1, 6, 8, 38, 39) were not identified in the MEDLINE databasesearch and were found to be eligible for inclusion on the basis of theirtitles and abstracts.
The search with Embase database yielded no additional articles.The manual search in the related articles and the reference lists of
literature reviews and textbook chapters resulted in 3 additional articlesthat were not previously identified in the electronic search and that wereeligible for inclusion on the basis of their titles and abstracts (40–42).
Full Text EvaluationThe combined search through the electronic databases and the
manual search resulted in a total of 27 studies (1, 3, 6, 8, 10, 14,22–42), which were subjected to a suitability test in accordance withthe criteria for considering studies for this review (Table 1). Six articleswere found to be case reports, reviews, in vitro studies, or were foundirrelevant to the topic of the present study. One article was not compat-ible with the VRF definition. In 5 articles non-endodontically treatedteeth were included (and data could not be separated from endodon-tically treated teeth). In 7 articles the VRF was not confirmed accordingto the reference standards, and 14 articles provided no detailed data onclinical signs and symptoms and radiographic findings of the evaluatedteeth. Eventually, none of the articles submitted to full text evaluationfulfilled the inclusion criteria (Table 2).
As a result, data extraction, methodological quality assessment,and data analysis could not be carried out. Thus, it was not possibleto find substantial evidence regarding the diagnostic accuracy of theindex tests for the diagnosis of VRF in endodontically treated teeth.
DiscussionNumerous studies dealing with the diagnosis of VRF and the clin-
ical and radiographic characteristics of the vertically root fracturedteeth have been published (2, 3, 7–11, 14, 28, 29, 31, 34, 35, 39,42–44). However, their study design, VRF definition, VRFconfirmation methods, and evaluated clinical and radiographic datahave been extremely variable, which resulted in publication of
JOE — Volume 36, Number 9, September 2010

TABLE 2. Excluded Studies and the Reasons for Exclusion
StudyReason forexclusion*
Takeuchi et al, 2009 (33) 3, 4Zadik et al, 2008 (37) 4Miyamoto et al, 2007 (30) 1Cohen et al, 2006 (25) 3Chambrone et al, 2006 (22) 1Tamse et al, 2006 (34) 5Cornelini R et al 2005 (26) 1Fox et al, 2004 (27) 1Llena-Puy et al, 2001 (28) 4Lustig et al, 2000 (29) 5Tamse et al, 1999 (3) 5Tamse et al, 1999 (14) 5Chan et al, 1999 (24) 3, 4, 5Youssefzadeh et al, 1999 (36) 5Chan et al, 1998 (23) 1Nicopoulou-Karayianni et al, 1997 (32) 3, 4Testori et al, 1993 (35) 4Morfis et al, 1990 (31) 4Meister et al, 1980 (10) 5Kawamura-Hagiya et al, 2008 (38) 5Fuss et al, 2001 (8) 5Fuss et al, 1999 (6) 5Walton et al, 1984 (1) 5Pitts et al, 1983 (39) 1Rud et al 1970, (40) 2, 5Abou-Rass M et al, 1983 (41) 3, 5Gher et al, 1987 (42) 5
*Based on incompatibleness to the inclusion criteria of the systematic review (Table 1): (1) case
reports, reviews, in vitro studies, and studies irrelevant to the topic of the current study; (2) incom-
patible with the VRF definition; (3) non-endodontically treated teeth are included; (4) lack of VRF
confirmation according to the reference standards; (5) no detailed data regarding the clinical signs
and symptoms and radiographic findings of the evaluated teeth.
Clinical Research
inconsistent and confusing results (2, 4, 5, 9, 10, 25, 40). The aim of thepresent study was to systematically search and evaluate the availableliterature concerning the diagnostic accuracy of clinical andradiographic indices for the diagnosis of VRF in endodonticallytreated teeth by the means of a systematic review.
Systematic reviews use a systematic approach and explicit method-ology to review and synthesize research evidence, aimed to minimizebias, and explicitly address the issues of the completeness of the iden-tified evidence, assess the quality of the included studies and the studies’combinability (15–18, 21, 45, 46). This systematic process requiresa comprehensive literature search to identify as much of the relevantliterature as possible (17, 18, 21, 47). It is recommended thata combined search of several electronic databases, together withother methods to retrieve studies (such as hand-searching of referencelists of relevant articles and book chapters), will be conducted (16–18,21, 45, 47). In the present study a combined comprehensive literaturesearch of several electronic databases and hand-search of related arti-cles, literature reviews, and textbook chapters was conducted. On thebasis of the study titles and abstracts, 27 possibly relevant articleswere identified. To overcome heterogeneity of information, strict inclu-sion and exclusion criteria were applied to the identified studies.Furthermore, it is crucial that the studies that are compatible with theinclusion criteria of the systematic review will be also subjected to meth-odological quality assessment to determine the strength of evidence(15). In the present study no article was in compliance with the criteriafor entering the systematic review; thus methodological quality assess-ment was not carried out.
The ability to assess the diagnostic accuracy and clinical usefulnessof clinical and radiographic parameters for the diagnosis of a target
JOE — Volume 36, Number 9, September 2010
condition depends on the availability of a valid reference standard.The appropriate reference standard should be carefully chosen andhas to be based on a technique different from that of the tests being eval-uated (16). The right selection of a reference standard is of paramountsignificance. In the present review, 3 types of reference standards wereselected as acceptable for confirmation of the VRF (the target condi-tion): confirmation during surgical flap procedure, confirmation aftertooth extraction, and radiographic identification being a clearlydiscernable separation of segments of fractured root.
In the current systematic review only endodontically treated teethwere included, because it is expected that in vital teeth the signs andsymptoms would be different and reflect pulp inflammation withoutperiradicular changes (5, 24, 48, 49).
While considering the usefulness of a diagnostic evaluation, therelative value of possible health states resulting from the diagnosisand subsequent therapy should be taken into consideration (16).When VRF diagnosis is made, a quick decision to extract the tooth orroot is necessary. The reason is that the inflammation in the supportingtissues would otherwise lead to periodontal breakdown followed by thedevelopment of a deep osseous defect (1) and resorption of the bonefacing the root fracture. Immediate treatment might prevent this unnec-essary bone loss that might lead to complicated restoration of the areaof extraction, if an implant should be considered the treatment ofchoice (2).
A diagnostic process is based on the combination of the patient’ssubjective complaints and objective clinical and radiographic evalua-tion (50). The clinician is supposed to correlate the subjective andobjective findings and formulate a diagnosis (50). In the case of VRFdiagnosis, there is no known single pathognomonic sign, symptom,or radiographic feature to make the diagnosis easy and definitive(29). In 2006 in their article on demographic analysis of VRFs, Cohenet al (25) stated that one of the main reasons for the difficult diagnosis ofVRF is the fact that the final diagnosis is based on constellation of severalsigns and symptoms rather than a single pathognomonic one. There-fore, the present review mandated the inclusion of detailed dataregarding both clinical and radiographic evaluations (index tests) ofthe diagnosed teeth.
The most common signs and symptoms of VRF described in theliterature are deep osseous defects especially on the buccal aspect ofthe susceptible teeth and roots, and highly located sinus tract (3, 10,35). The deep osseous defect (deep probing), especially on thebuccal aspect of the more susceptible teeth and roots (maxillary andmandibular premolars and mesial roots of the mandibular molars),were found in retrospective case series publications in highpercentages and with statistical significance: Meister et al (10), 93%;Tamse (13), 64%; Testori et al (35), 78%; and Tamse et al (3),67%. The sinus tract in the gingiva, especially when it is coronallylocated closer to the gingival margin (as opposed to the sinus tract infailing endodontic cases), is also a typical sign for the diagnosis ofVRF. This type of sinus tract was found by Tamse et al (3) in 35%and by Testori et al (35) in 42% of the VRF teeth.
The most frequent radiographic features of VRF are the ‘‘halo’’appearance, which is a combined periapical and perilateral radiolu-cency in one or both sides of the root, lateral periodontal radiolucencyalong the side of the root, or angular radiolucency from the crestal boneterminating along the root side (14, 32, 35). In mandibular molars,radiolucency in the furcation area can often be observed, coupledwith the types of radiolucencies described above (34).
In the present systematic review no articles passed the inclusioncriteria. That means that unfortunately, evidence-based data concerningthe diagnostic accuracy and clinical effectiveness of the daily used clin-ical and radiographic dental evaluation for the diagnosis of VRF in
Diagnosis of VRFs in Endodontically Treated Teeth 1457

Clinical Research
endodontically treated teeth are lacking. Thus, the need for a cautiousrigorous clinical approach for the diagnosis and follow-up of suspectedVRFs and the need for evidence-based research efforts to elucidate thecurrently unknown are of utmost significance.ConclusionsThe evidence-based data regarding the diagnostic accuracy and
usefulness of the commonly used clinical and radiographic evaluationmethods for the diagnosis of VRF in endodontically treated teeth arelacking. That makes the determination of a fractured root often notdistinctly objective and more of a prediction rather than a definitivediagnosis, as previously stated (25). In case a VRF is suspected, theclinician should be aware of the current conflict between the significantclinical importance of a quick and correct diagnosis and the lack ofevidence-based data supporting the usefulness of common clinicaland radiographic evaluation methods. Future evidence-based researchregarding the diagnosis of VRF is needed and might possibly shed lighton this clinical challenge.
References1. Walton RE, Michelich RJ, Smith GN. The histopathogenesis of vertical root fractures.
J Endod 1984;10:48–56.2. Tamse A. Vertical root fractures in endodontically treated teeth: diagnostic signs and
clinical management. Endodontic Topics 2006;13:84–94.3. Tamse A, Fuss Z, Lustig J, Kaplavi J. An evaluation of endodontically treated vertically
fractured teeth. J Endod 1999;25:506–8.4. Tamse A. Vertical root fractures of endodontically treated teeth. In: Ingle JI,
Bakland LK, Baumgartner JC, eds. Ingle’s endodontics. 6th ed. Hamilton, Ontario,Canada: BC Decker Inc; 2008:676–89.
5. Colleagues for excellence. Cracking the cracked tooth code: detection and treatmentof various longitudinal tooth fractures. Chicago: American Association of Endodon-tics; 2008.
6. Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted endodon-tically treated teeth. Int Endod J 1999;32:283–6.
7. Coppens CRM, DeMoor RJG. Prevalence of vertical root fractures in extractedendodontically treated teeth. Int Endod J 2003;36:926.
8. Fuss Z, Lustig J, Katz A, Tamse A. An evaluation of endodontically treated vertical rootfractured teeth: impact of operative procedures. J Endod 2001;27:46–8.
9. Cohen S, Blanco L, Berman L. Vertical root fractures: clinical and radiographic diag-nosis. J Am Dent Assoc 2003;134:434–41.
10. Meister F Jr, Lommel TJ, Gerstein H. Diagnosis and possible causes of vertical rootfractures. Oral Surg Oral Med Oral Pathol 1980;49:243–53.
11. Moule AJ, Kahler B. Diagnosis and management of teeth with vertical root fractures.Aust Dent J 1999;44:75–87.
12. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod1992;18:332–5.
13. Tamse A. Iatrogenic vertical root fractures in endodontically treated teeth. EndodDent Traumatol 1988;4:190–6.
14. Tamse A, Fuss Z, Lustig J, Ganor Y, Kaffe I. Radiographic features of vertically frac-tured, endodontically treated maxillary premolars. Oral Surg Oral Med Oral PatholOral Radiol Endod 1999;88:348–52.
15. Gutmann JL. Evidence-based/guest editorial. J Endod 2009;35:1093.16. Mileman PA, van den Hout WB. Evidence-based diagnosis and clinical decision
making. Dentomaxillofac Radiol 2009;38:1–10.17. Rosenberg W, Donald A. Evidence based medicine: an approach to clinical
problem-solving. BMJ 1995;310:1122–6.18. Sutherland SE, Matthews DC. Conducting systematic reviews and creating clinical
practice guidelines in dentistry: lessons learned. J Am Dent Assoc 2004;135:747–53.19. Bossuyt PM, Leeflang MM. Chapter 6: developing criteria for including studies. Co-
chrane handbook for systematic reviews of diagnostic test accuracy: the CochraneCollaboration; 2008.
20. Reitsma JB, Rutjes AWS, Whiting P, Vlassov VV, Leeflang MMG, Deeks JJ. Chapter 9:assessing methodological quality. In: Deeks JJ, Bossuyt PM, Gatsonis C, eds. Co-chrane handbook for systematic reviews of diagnostic test accuracy: the CochraneCollaboration; 2009.
1458 Tsesis et al.
21. Whiting P, Westwood M, Burke M, Sterne J, Glanville J. Systematic reviews of testaccuracy should search a range of databases to identify primary studies. J ClinEpidemiol 2008;61:357–64.
22. Chambrone LA, Chambrone L. Tooth loss in well-maintained patients with chronicperiodontitis during long-term supportive therapy in Brazil. J Clin Periodontol 2006;33:759–64.
23. Chan CP, Jeng JH, Chang SH, Chen CC, Lin CJ, Lin CP. Cutaneous sinus tracts of dentalorigin: clinical review of 37 cases. J Formos Med Assoc 1998;97:633–7.
24. Chan CP, Lin CP, Tseng SC, Jeng JH. Vertical root fracture in endodontically versusnonendodontically treated teeth: a survey of 315 cases in Chinese patients. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1999;87:504–7.
25. Cohen S, Berman LH, Blanco L, Bakland L, Kim JS. A demographic analysis ofvertical root fractures. J Endod 2006;32:1160–3.
26. Cornelini R, Cangini F, Covani U, Wilson TG Jr. Immediate restoration of implantsplaced into fresh extraction sockets for single-tooth replacement: a prospective clin-ical study. Int J Periodontics Restorative Dent 2005;25:439–47.
27. Fox K, Wood DJ, Youngson CC. A clinical report of 85 fractured metallic post-retained crowns. Int Endod J 2004;37:561–73.
28. Llena-Puy MC, Forner-Navarro L, Barbero-Navarro I. Vertical root fracture inendodontically treated teeth: a review of 25 cases. Oral Surg Oral Med Oral PatholOral Radiol Endod 2001;92:553–5.
29. Lustig JP, Tamse A, Fuss Z. Pattern of bone resorption in vertically fractured,endodontically treated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2000;90:224–7.
30. Miyamoto T, Morgano SM, Kumagai T, Jones JA, Nunn ME. Treatment history of teethin relation to the longevity of the teeth and their restorations: outcomes of teethtreated and maintained for 15 years. J Prosthet Dent 2007;97:150–6.
31. Morfis AS. Vertical root fractures. Oral Surg Oral Med Oral Pathol 1990;69:631–5.
32. Nicopoulou-Karayianni K, Bragger U, Lang NP. Patterns of periodontal destructionassociated with incomplete root fractures. Dentomaxillofac Radiol 1997;26:321–6.
33. Takeuchi N, Yamamoto T, Tomofuji T, Murakami C. A retrospective study on theprognosis of teeth with root fracture in patients during the maintenance phase ofperiodontal therapy. Dent Traumatol 2009;25:332–7.
34. Tamse A, Kaffe I, Lustig J, Ganor Y, Fuss Z. Radiographic features of vertically frac-tured endodontically treated mesial roots of mandibular molars. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2006;101:797–802.
35. Testori T, Badino M, Castagnola M. Vertical root fractures in endodontically treatedteeth: a clinical survey of 36 cases. J Endod 1993;19:87–91.
36. Youssefzadeh S, Gahleitner A, Dorffner R, Bernhart T, Kainberger FM. Dental verticalroot fractures: value of CT in detection. Radiology 1999;210:545–9.
37. Zadik Y, Sandler V, Bechor R, Salehrabi R. Analysis of factors related to extraction ofendodontically treated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2008;106:e31–5.
38. Kawamura-Hagiya Y, Yoshioka T, Suda H. Logistic regression equation to screen forvertical root fractures using periapical radiographs. Dentomaxillofac Radiol 2008;37:28–33.
39. Pitts DL, Natkin E. Diagnosis and treatment of vertical root fractures. J Endod 1983;9:338–46.
40. Rud J, Omnell KA. Root fractures due to corrosion: diagnostic aspects. Scand J DentRes 1970;78:397–403.
41. Abou-Rass M. Crack lines: the precursors of tooth fractures—their diagnosis andtreatment. Quintessence Int Dent Dig 1983;14:437–47.
42. Gher ME Jr, Dunlap RM, Anderson MH, Kuhl LV. Clinical survey of fractured teeth.J Am Dent Assoc 1987;114:174–7.
43. Dang DA, Walton RE. Vertical root fracture and root distortion: effect of spreaderdesign. J Endod 1989;15:294–301.
44. Kishen A. Mechanisms and risk factors for fracture predilection in endodonticallytreated teeth. Endodontic Topics 2006;13:57–83.
45. Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in system-atic reviews of complex evidence: audit of primary sources. BMJ 2005;331:1064–5.
46. Suebnukarn S, Ngamboonsirisingh S, Rattanabanlang A. A systematic evaluation ofthe quality of meta-analyses in endodontics. J Endod 2010;36:602–8.
47. Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical re-treatment and endodontic surgery: a systematic review. J Endod 2009;35:930–7.
48. Cameron CE. Cracked-tooth syndrome. J Am Dent Assoc 1964;68:405–11.49. Cameron CE. The cracked tooth syndrome: additional findings. J Am Dent Assoc
1976;93:971–5.50. Berman LH, Hartwell GR. Diagnosis. In: Cohen S, Hargreaves KM, eds. Pathways of
the pulp. 9th ed. St Louis, MO: Mosby; 2006:2–39.
JOE — Volume 36, Number 9, September 2010

Clinical Research
Prospective, Randomized Single-blind Study of theAnesthetic Efficacy of 1.8 and 3.6 Milliliters of 2% Lidocainewith 1:50,000 Epinephrine for Inferior Alveolar Nerve BlockMaji Wali, BDS, MS, Melissa Drum, DDS, MS, Al Reader, DDS, MS, and John Nusstein, DDS, MS
Abstract
Introduction: The purpose of this prospective, random-ized study was to compare the degree of pulpal anes-thesia obtained in vital, asymptomatic teeth by using1.8 mL and 3.6 mL of 2% lidocaine with 1:50,000epinephrine compared with 1.8 mL of 2% lidocainewith 1:100,000 epinephrine for inferior alveolar nerve(IAN) block. Methods: Thirty adult subjects randomlyreceived IAN blocks of 1.8 mL and 3.6 mL of 2% lido-caine with 1:50,000 epinephrine and 1.8 mL of 2% lido-caine with 1:100,000 epinephrine at 3 separateappointments in a crossover design. An electric pulptester was used to test for anesthesia in 3-minute cyclesfor 60 minutes of the first molars, first premolars, andlateral incisors. Anesthesia was considered successfulwhen 2 consecutive 80 readings were obtained within15 minutes, and the 80 reading was continuously sus-tained through the 60th minute. Results: By using 1.8mL of 2% lidocaine with 1:50,000 epinephrine, success-ful pulpal anesthesia ranged from 33%–50%, and whenusing 3.6 mL of 2% lidocaine with 1:50,000 epinephrine,success ranged from 40%–60%. When using 1.8 mL of2% lidocaine with 1:100,000 epinephrine, successranged from 40%–60%, with no significant differenceamong the 3 anesthetic formulations. Conclusion:Increasing the epinephrine concentration to 1:50,000epinephrine or increasing the volume to 3.6 mL of 2%lidocaine with 1:50,000 epinephrine did not result inmore successful pulpal anesthesia when comparedwith 1.8 mL of 2% lidocaine with 1:100,000 epinephrineby using the IAN block. (J Endod 2010;36:1459–1462)Key WordsEpinephrine concentrations, inferior alveolar nerveblock, lidocaine, local anesthesia
From the Division of Endodontics, The Ohio State Univer-sity, Columbus, Ohio.
Maji Wali is currently in Baghdad, Iraq.Address requests for reprints to Dr Melissa Drum, Division
of Endodontics, College of Dentistry, The Ohio State University,305 West 12th Ave, Columbus, OH 43210.E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.012
JOE — Volume 36, Number 9, September 2010
The inferior alveolar nerve (IAN) block does not always result in successful pulpalanesthesia (1–6). Failure rates of 10%–39% have been reported in experimental
studies (1). Therefore, it would be advantageous to improve the success rate of theIAN block.
The effect of epinephrine concentration on the success of an IAN block has beenstudied. Bou Dagher et al (7) evaluated 1.8 mL of 2% lidocaine with 3 concentrations ofepinephrine, 1:50,000, 1:80,000, and 1:100,000, in IAN blocks. They found no signif-icant differences between the 3 formulations for anesthetic success or failure by usinga pulp tester to evaluate pulpal anesthesia. Likewise, Yared and Bou Dagher (8) eval-uated 3.6 mL of 2% lidocaine with 3 concentrations of epinephrine, 1:50,000,1:80,000, and 1:100,000, in IAN blocks by using the same methodology as Bou Dagheret al. They also found no significant differences between the 3 formulations for anes-thetic success or failure by using a pulp tester to evaluate pulpal anesthesia. However,Yared and Bou Dagher retrospectively compared the results of the 3.6 mL volume withthe 1.8 mL volume by using the data from Bou Dagher et al and found statistically highersuccess rates with the 3.6 mL volume. The efficacy of 1:50,000 epinephrine in a 2%lidocaine formulation and an increased volume of a 2% lidocaine formulation with1:50,000 epinephrine in providing pulpal anesthesia when administered in an IANblock needs further investigation to ensure its appropriate clinical use.
The purpose of this prospective, randomized single-blind study was to comparethe degree of pulpal anesthesia obtained in vital, asymptomatic teeth by using 1.8 mLand 3.6 mL of 2% lidocaine with 1:50,000 epinephrine compared with 1.8 mL of2% lidocaine with 1:100,000 epinephrine for the IAN block.
Materials and MethodsThirty adult subjects participated in this study. The subjects were in good health
and were not taking any medications that would alter their perception of pain. Exclusioncriteria were as follows: younger than 18 years; older than 65 years; allergies to localanesthetics or sulfites; pregnancy; history of significant medical conditions; taking anymedications that might affect anesthetic assessment (nonsteroidal anti-inflammatorydrugs, opioids, antidepressants, alcohol); active sites of pathosis in area of injection;and inability to give informed consent. The Ohio State University Human Subjects ReviewCommittee approved both the protocol and informed consent document, and writteninformed consent was obtained from each subject.
The subjects randomly received each of 3 solutions in an IAN block at 3 separateappointments, spaced at least 1 week apart, in a crossover design. The 3 solutions were1.8 mL of 2% lidocaine with 1:100,000 epinephrine, 1.8 mL of 2% lidocaine with1:50,000 epinephrine, and 3.6 mL of 2% lidocaine with 1:50,000 epinephrine. Withthe crossover design, there were 90 total injections administered, and each subjectserved as his or her own control. Fifteen sets of 3 IAN block injections were adminis-tered on the right side, and 15 sets of 3 IAN block injections were administered on theleft side. The same side randomly chosen for the first injection was used again for thesecond and third injections. The test teeth chosen for the experiment were the mandib-ular first molar, first premolar, and lateral incisor. The contralateral mandibular caninewas used as the unanesthetized control to ensure that the electric pulp tester was oper-ating properly and that the subject was responding appropriately during each
Anesthetic Efficacy of Lidocaine with Epinephrine for IAN Block 1459

TABLE 1. Percentages and Numbers of Subjects who Experienced Anesthetic Success
Anesthetic formulation
1.8 mL of 2% lidocaine with1:50,000 epinephrine
3.6 mL of 2% lidocaine with1:50,000 epinephrine
1.8 mL of 2% lidocaine with1:100,000 epinephrine
Anesthetic success*First molar 33% (10/30) 40% (12/30) 43% (13/30)First premolar 50% (15/30) 60% (18/30) 60% (18/30)Lateral incisor 37% (11/30) 47% (14/30) 40% (12/30)
n = 30.
*There were no significant differences among the 3 anesthetic formulations.
Clinical Research
experimental portion of the study. Clinical examinations indicated thatall teeth were free of caries, large restorations, and periodontal disease;none had histories of trauma or sensitivity.
Before the experiment, the 3 solutions were randomly assigned 4-digit numbers from a random number table. Each subject was randomlyassigned to the right or left side for the set of injections. The order of theanesthetic solutions was also randomly assigned to determine whichsolutions were to be administered at each appointment. Only therandom numbers were recorded on the data collection and postinjec-tion survey sheets to help blind the experiment.
Five-milliliter Luer-Lok sterile syringes (Becton, Dickinson andCo, Rutherford, NJ) were loaded with 1.8 mL of 2% lidocaine with1:100,000 epinephrine (Xylocaine; Astra Pharmaceutical Products,Inc, Worchester, MA), 1.8 mL of 2% lidocaine with 1:50,000 epineph-rine (Xylocaine), or 3.6 mL of 2% lidocaine with 1:50,000 epinephrine(Xylocaine) under sterile conditions. All anesthetic cartridges werechecked to ensure that the anesthetic solution had not expired. An opa-que tape was placed on each syringe, and the corresponding 4-digitcode number was written on the tape.
At the beginning of each appointment and before any injectionswere given, the experimental teeth and control contralateral caninewere tested 3 times with the pulp tester (Kerr, Analytic TechnologyCorp, Redmond, WA) to record baseline vitality. After the tooth to betested was isolated with cotton rolls and dried with gauze, toothpastewas applied to the probe tip, which was then placed midway betweenthe gingival margin and the occlusal or incisal edge of the tooth. Thecurrent rate was set at 25 seconds to increase from no output (0) tothe maximum output (80). The number associated with the initial
001
57
05
00005:1htiweniacodiL%2Lm81
52Per
cen
tage
of
80 R
ead
ings
1.8 Lm %2 eniacodiL htiw 05:1 , 000enirhpenipe
000,05:1htiweniacodiL%2Lm6.3enirhpenipe
0
000,001:1htiweniacodil%2Lm8.1enirhpenipe
559434731352913171
)setuniM(emiT
Figure 1. Incidence of first molar anesthesia as determined by lack ofresponse to electrical pulp testing at the maximum setting (percentage of80/80s), at each postinjection time interval, for the 3 solutions.
1460 Wali et al.
sensation was recorded. Trained research personnel performed all pre-injection and postinjection tests.
All subjects received a conventional IAN block as described by Jor-gensen and Hayden (9). The needle used for all injections was a 27-gauge 11⁄2 -inch needle (Becton, Dickinson and Company, FranklinLakes, NJ). Once the target site was reached, each anesthetic formula-tion was deposited during a period of 2 minutes. All injections weregiven by the senior author (M.W.).
At 1 minute after each block was given, the first molar was pulptested. At 2 minutes, the first premolar and lateral incisor were tested.At 3 minutes, the contralateral canine was pulp tested, and the subjectwas asked if his/her lip was numb. This cycle of testing was repeatedevery 3 minutes for 60 minutes. At every third cycle the control tooth,the contralateral canine, was tested by a pulp tester without batteriesto test the reliability of the subject. If profound lip numbness was notrecorded within 20 minutes, the block was considered unsuccessful,and the subject was reappointed. All testing was stopped at 60 minutesafter injection.
No response from the subject at the maximum output (80 reading)of the pulp tester was used as the criterion for pulpal anesthesia. Anes-thesia was considered successful when 2 consecutive 80 readings wereobtained within 15 minutes, and the 80 reading was continuously sus-tained through the 60th minute. For most restorative procedures, wewould want the patient numb within 15 minutes and to remain numbthrough the 60th minute.
Data were analyzed statistically. All subjects used for data analysishad profound lip anesthesia. Comparisons of the 3 anesthetic formula-tions for anesthetic success, onset of lip and pulpal anesthesia, were
001
57
05000,05:1 htiw eniacodiL %2 Lm 8.1
ihi
52
Per
cent
age
of 8
0 R
eadi
ngs
pe i pen hri en000,05:1 htiw eniacodiL %2 Lm 6.3
enirhpenipe000,001:1htiweniacodil%2Lm8.1
0
8.1 Lm %2 eniacodil htiw 000,001:1enirhpenipe
559434731352913171
)setuniM( emiT
Figure 2. Incidence of first premolar anesthesia as determined by lack ofresponse to electrical pulp testing at the maximum setting (percentage of80/80s), at each postinjection time interval, for the 3 solutions.
JOE — Volume 36, Number 9, September 2010

Figure 3. Incidence of lateral incisor anesthesia as determined by lack ofresponse to electrical pulp testing at the maximum setting (percentage of80/80s), at each postinjection time interval, for the 3 solutions.
Clinical Research
analyzed nonparametrically by using exact McNemar tests that wereadjusted by using the step-down Bonferroni method of Holm. Witha nondirectional alpha risk of 0.05 and assuming a success rate of40% and a change proportion of 80%, a sample size of 30 subjectswas required to demonstrate a difference in anesthetic success of�30 percentage points with a power of 0.80. Comparisons wereconsidered significant at P <.05.
ResultsThirty adult subjects, 8 women and 22 men, aged 22–44 years with
an average age of 28 years, participated.One hundred percent of the subjects used for data analysis had
profound lip anesthesia. Anesthetic success is presented in Table 1.The success rate for the 1.8 mL of 2% lidocaine with 1:50,000epinephrine formulation was 33% for the first molar, 50% for the firstpremolar, and 37% for the lateral incisor. For the 3.6 mL of 2% lido-caine with 1:50,000 epinephrine formulation, success rates were 40%for the first molar, 60% for the first premolar, and 47% for the lateralincisor. The 1.8 mL of 2% lidocaine with 1:100,000 epinephrinesuccess rates were 43% for the first molar, 60% for the first premolar,and 40% for the lateral incisor. There were no significant differencesamong the 3 anesthetic formulations. Figs. 1 through 3 show theincidence of pulpal anesthesia (80 readings) for the 3 anestheticformulations.
Onset times of lip and pulpal anesthesia are shown in Table 2. Foronset of lip anesthesia, there was a significant difference when 1.8 mL of2% lidocaine with 1:50,000 epinephrine was compared with the other 2
TABLE 2. Mean Onset Times (minutes) of Subjective Lip Anesthesia and Pulpal An
1.8 mL of 2% lidocaine with1:50,000 epinephrine
Onset of lip numbness (min)* 5.9 � 0.5Onset of pulpal anesthesia (min)†
First molar 15.9 � 3.4First premolar 15.5 � 2.7Lateral incisor 14.0 � 2.3
*There was a significant difference when 1.8 mL of 2% lidocaine with 1:50,000 epinephrine was compar†Subjects were excluded from the data analysis if they did not achieve 2 consecutive 80 readings at any ti
JOE — Volume 36, Number 9, September 2010
formulations. For pulpal anesthesia, there were no significant differ-ences among the 3 anesthetic formulations.
DiscussionWe based our use of the electric pulp test reading of 80, signaling
maximum output, as a criterion for pulpal anesthesia on the studies ofDreven et al (10) and Certosimo and Archer (11). These studiesshowed that no patient response to an 80 reading ensured pulpal anes-thesia in vital asymptomatic teeth. In addition, Certosimo and Archerdemonstrated that electric pulp test readings less than 80 resulted inpain during operative procedures in asymptomatic teeth. Therefore,using the electric pulp tester before beginning dental procedures onasymptomatic vital teeth will provide the clinician a reliable indicatorof pulpal anesthesia. Because all subjects felt profound lip numbnessbut pulp testing revealed that subjects did not always have pulpal anes-thesia (80 readings), asking the patient if the lip is numb only indicatessoft tissue anesthesia but does not guarantee successful pulpal anes-thesia.
Regarding epinephrine concentrations, Bou Dagher et al (7) re-corded success rates for 1.8 mL of 2% lidocaine with 1:50,000 epineph-rine of 50% for the first molar, 53% for the first premolar, and 47% forthe lateral incisor. In the current study, success rates were lower for thefirst molar (33%) and lateral incisor (37%) but similar in the firstpremolar (50%). Differences between studies might be due to popula-tion differences. When 1.8 mL of 2% lidocaine with 1:50,000 epineph-rine was compared with 1.8 mL of 2% lidocaine with 1:100,000epinephrine, no differences were found (Table 1). Bou Dagher foundsimilar results.
Regarding the increased volume, Yared and Bou Dagher (8) re-corded success rates for 3.6 mL of 2% lidocaine with 1:50,000 epineph-rine of 77% for the first molar, 80% for the first premolar, and 70% forthe lateral incisor. In the current study, success rates were lower for thefirst molar (40%), lateral incisor (60%), and first premolar (47%).When Yared and Bou Dagher retrospectively compared the results ofthe 3.6 mL volume with the 1.8 mL volume by using different subjectpopulations, they found statistically higher success rates with the 3.6mL volume. In the current study, we found no significant differencebetween the 1.8 mL and 3.6 mL volumes for 2% lidocaine with1:50,000 epinephrine. Therefore, we could not confirm the results ofYared and Bou Dagher.
Generally, 1.8 mL of 2% lidocaine with 1:100,000 epinephrine hadsimilar rates of anesthetic success as other studies of the IAN block (1).Nusstein et al (1) found success rates of 53% for the first molar, 61% forthe first premolar, and 35% for the lateral incisor. These are similar tothe success rates of 43% for the first molar, 60% for the first premolar,and 40% for the lateral incisor in the current study (Table 1). The re-corded success rates of Yared and Bou Dagher (8) for 3.6 mL of 2%lidocaine with 1:100,000 epinephrine were 77% for the first molar,
esthesia
Anesthetic formulation
3.6 mL of 2% lidocaine with1:50,000 epinephrine
1.8 mL of 2% lidocaine with1:100,000 epinephrine
4.7 � 0.5 4.4 � 0.4
11.1 � 2.7 13.3 � 2.710.5 � 2.7 12.5 � 2.511.9 � 3.0 11.6 � 2.8
ed with the other 2 formulations.
me during the 60 minutes. n = 24, first molar; n = 26, first premolar; n = 18, lateral incisor.
Anesthetic Efficacy of Lidocaine with Epinephrine for IAN Block 1461

Clinical Research
80% for the first premolar, and 67% for the lateral incisor. Nusstein et alrecorded success rates for 3.6 mL of 2% lidocaine with 1:100,000epinephrine of 44% for the first molar, 67% for the first premolar,and 32% for the lateral incisor. Therefore, the higher success ratesof Yared and Bou Dagher with the increased volume of 2% lidocainewith 1:100,000 epinephrine were not confirmed by Nusstein et al.None of the 2% lidocaine formulations provided complete pulpal anes-thesia for the mandibular teeth (Table 1; Figs. 1–3). This could presentmeaningful clinical problems because the teeth might not be numb forprocedures requiring complete pulpal anesthesia. Practitioners shouldconsider supplemental techniques such as intraosseous injections (12–16), periodontal ligament injections (17), or a buccal infiltration ofa cartridge of 4% articaine with 1:100,000 epinephrine for the firstmolar (18) when a conventional IAN block fails to provide pulpal anes-thesia for a particular asymptomatic tooth. Because we studied a youngadult population, the results of this study might not apply to children orthe elderly.Onset of pulpal anesthesia varied from 14–15.9 minutes for the1.8 mL of 2% lidocaine with 1:50,000 epinephrine formulation, from10.5–11.9 minutes for the 3.6 mL of 2% lidocaine with 1:50,000epinephrine formulation, and from 11.6–13.3 minutes for the 1.8mL of 2% lidocaine with 1:100,000 epinephrine formulation, with nosignificant differences between the 3 anesthetic formulations. There-fore, increasing the epinephrine concentration to 1:50,000 epinephrineor increasing the volume to 3.6 mL of 2% lidocaine with 1:50,000epinephrine did not increase the onset time of pulpal anesthesiawhen compared with 1.8 mL of 2% lidocaine with 1:100,000 epineph-rine. Other studies that used 1.8 mL of 2% lidocaine with 1:100,000epinephrine for IAN blocks have reported onset of pulpal anesthesiaranged from 8.4–13.2 minutes (19), 8.8–12.3 minutes (20), 10.8–17.2 minutes (21), and 8.2–13 minutes (22) for the first molar, firstpremolar, and lateral incisor. The values for onset are similar to theresults of the current study. Pulp testing the tooth with an electricpulp tester or cold refrigerant in asymptomatic patients will give theclinician a reliable indicator of onset of pulpal anesthesia (10, 11, 23).
Onset of lip anesthesia ranged from 4.4–5.9 minutes, with a signif-icant difference between the 1.8 mL of 2% lidocaine with 1:50,000epinephrine formulation when compared with the other 2 formulations(Table 2). However, the difference of a little more than 1 minute wouldhave little clinical significance. Other studies that used 2% lidocainewith 1:100,000 epinephrine for IAN blocks have reported onset of lipanesthesia of 5.0 minutes (21), 6.1 minutes (20), 8.8 minutes (19),and 4.7 minutes (22). The values are somewhat higher when comparedwith the results of the current study (4.4 minutes), and variationsbetween studies are probably related to differences in populations.However, the time of onset of lip numbness might not indicate the onsetof pulpal anesthesia (Table 1).
We concluded that increasing the epinephrine concentration to1:50,000 epinephrine in a 2% lidocaine solution or increasing thevolume to 3.6 mL of 2% lidocaine with 1:50,000 epinephrine didnot result in more successful pulpal anesthesia when comparedwith 1.8 mL of 2% lidocaine with 1:100,000 epinephrine by usingthe IAN block.
1462 Wali et al.
References1. Nusstein J, Reader A, Beck M. Anesthetic efficacy of different volumes of lidocaine
with epinephrine for inferior alveolar nerve blocks. Gen Dent 2002;50:372–5.2. Hannan L, Reader A, Nist R, Beck M, Meyers WJ. The use of ultrasound for guiding
needle placement for inferior alveolar nerve blocks. Oral Surg Oral Med Oral PatholOral Radiol Endod 1999;87:658–65.
3. Goldberg S, Reader A, Drum M, Nusstein J, Beck M. Comparison of the anestheticefficacy of the conventional inferior alveolar, Gow-Gates, and Vazirani-Akinosi tech-niques. J Endod 2008;34:1306–11.
4. Foster W, Drum M, Reader A, Beck M. Anesthetic efficacy of buccal and lingual infil-trations of lidocaine following an inferior alveolar nerve block in mandibular poste-rior teeth. Anesth Prog 2007;54:163–9.
5. Steinkruger G, Nusstein J, Reader A, Beck M, Weaver J. The significance of needlebevel orientation in achieving a successful inferior alveolar nerve block. J Am DentAssoc 2006;137:1685–91.
6. Mikesell P, Nusstein J, Reader A, Beck M, Weaver J. A comparison of articaine andlidocaine for inferior alveolar nerve blocks. J Endod 2005;31:265–70.
7. Bou Dagher F, Yared GM, Machtou P. An evaluation of 2% lidocaine with differentconcentrations of epinephrine for inferior alveolar nerve block. J Endod 1997;23:178–80.
8. Yared GM, Bou Dagher F. Evaluation of lidocaine in human inferior alveolar nerveblock. J Endod 1997;23:575–8.
9. Jorgensen NB, Hayden J Jr. Premedication, local and general anesthesia in dentistry.2nd ed. Philadelphia, PA: Lea & Febiger; 1967.
10. Dreven L, Reader A, Beck M, Meyers W, Weaver J. An evaluation of the electric pulptester as a measure of analgesia in human vital teeth. J Endod 1987;13:233–8.
11. Certosimo A, Archer R. A clinical evaluation of the electric pulp tester as an indicatorof local anesthesia. Oper Dent 1996;21:25–30.
12. Reisman D, Reader A, Nist R, Beck M, Weaver J. Anesthetic efficacy of the supple-mental intraosseous injection of 3% mepivacaine in irreversible pulpitis. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1997;84:676–82.
13. Nusstein J, Reader A, Nist R, Beck M, Meyers WJ. Anesthetic efficacy of the supple-mental intraosseous injection of 2% lidocaine with 1:100,000 epinephrine in irre-versible pulpitis. J Endod 1998;24:487–91.
14. Parente SA, Anderson RW, Herman WW, Kimbrough WF, Weller RN. Anesthetic effi-cacy of the supplemental intraosseous injection for teeth with irreversible pulpitis.J Endod 1998;24:826–8.
15. Nusstein J, Kennedy S, Reader A, Beck M, Weaver J. Anesthetic efficacy of the supple-mental X-tip intraosseous injection in patients with irreversible pulpitis. J Endod2003;29:724–8.
16. Bigby J, Reader A, Nusstein J, Beck M, Weaver J. Articaine for supplemental intra-osseous anesthesia in patients with irreversible pulpitis. J Endod 2006;32:1044–7.
17. Cohen HP, Cha BY, Spangberg LSW. Endodontic anesthesia in mandibular molars:a clinical study. J Endod 1993;19:370–3.
18. Haase A, Reader A, Nusstein J, Beck M, Drum M. Comparing anesthetic efficacy ofarticaine versus lidocaine as a supplemental buccal infiltration of the mandibularfirst molar after an inferior alveolar nerve block. J Am Dent Assoc 2008;139:1228–35.
19. Vreeland D, Reader A, Beck M, Meyers W, Weaver J. An evaluation of volumes andconcentrations of lidocaine in human inferior alveolar nerve block. J Endod 1989;15:6–12.
20. Hinkley SA, Reader A, Beck M, Meyers WJ. An evaluation of 4% prilocaine with1:200,000 epinephrine and 2% mepivacaine with 1:20,000 levonordefrin comparedwith 2% lidocaine with 100,000 epinephrine for inferior alveolar nerve block.Anesth Prog 1991;38:84–9.
21. McLean C, Reader A, Beck M, Meyers WJ. An evaluation of 4% prilocaine and 3%mepivacaine compared with 2% lidocaine (1:100,000 epinephrine) for inferioralveolar nerve block. J Endod 1993;3:146–50.
22. Chaney MA, Kerby R, Reader A, Beck FM, Meyers WJ, Weaver J. An evaluation oflidocaine hydrocarbonate compared with lidocaine hydrochloride for inferior alve-olar nerve block. Anesth Prog 1991;38:212–6.
23. Hsiao-Wu GW, Susarla SM, White RR. Use of the cold test as a measure of pulpalanesthesia during endodontic therapy: a randomized, blinded, placebo-controlledclinical trial. J Endod 2007;33:406–10.
JOE — Volume 36, Number 9, September 2010

Clinical Research
Photodynamic Therapy Associated with ConventionalEndodontic Treatment in Patients with Antibiotic-resistantMicroflora: A Preliminary ReportAguinaldo S. Garcez, PhD,* Silvia C. Nunez, PhD,
†Michael R. Hamblim, PhD,
‡§k
Hideo Suzuki,* and Martha S. Ribeiro, PhD¶
Abstract
Introduction: This study reports the antimicrobialeffect of photodynamic therapy (PDT) combined withendodontic treatment in patients with necrotic pulp in-fected with microflora resistant to a previous antibiotictherapy. Methods: Thirty anterior teeth from 21patients with periapical lesions that had been treatedwith conventional endodontic treatment and antibiotictherapy were selected. Microbiological samples weretaken (1) after accessing the root canal, (2) afterendodontic therapy, and (3) after PDT. Results: Allthe patients had at least 1 microorganism resistant toantibiotics. PDT used polyethylenimine chlorin(e6) asa photosensitizer and a diode laser as a light source(P = 40 mW, t = 4minutes, E = 9.6 J). Endodontictherapy alone produced a significant reduction innumbers of microbial species but only 3 teeth werefree of bacteria, whereas the combination of endodontictherapy with PDT eliminated all drug-resistant speciesand all teeth were bacteria-free. Conclusions: Theuse of PDT added to conventional endodontic treatmentleads to a further major reduction of microbial load. PDTis an efficient treatment to kill multi-drug resistantmicroorganisms. (J Endod 2010;36:1463–1466)Key WordsAntibiotic resistant bacteria, endodontic re-treatment,laser, photodynamic therapy
From the *Centro de Pesquisa e Pos-Graduacao Sao Leo-poldo Mandic, Campinas, SP, Brazil; †CETAO, Sao Paulo, SP,Brazil; ‡Wellman Center for Photomedicine, MassachusettsGeneral Hospital, Boston, Massachusetts; §Department ofDermatology, Harvard Medical School, Boston, Massachusetts;kHarvard MIT Division of Health Science and Technology, Cam-bridge, Massachusetts; and ¶Center of Lasers and Applications,IPEN-CNEN/SP, Sao Paulo, SP, Brazil.
Address requests for reprints to Dr Aguinaldo Silva Garcez,Sao Leopoldo Mandic University, Campinas, SP, Brazil. E-mailaddress: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.001
JOE — Volume 36, Number 9, September 2010
In the case of endodontic treatment failure, retreatment, surgical treatment, or extrac-tion usually is carried out with the use of antibiotics and antiseptics as adjunctive ther-
apies, but the long-term use of these agents can be rendered ineffective by resistancedeveloping in the target organism (1). Currently, there is an emergence of bacteriawith multiple resistances, and there is a need for alternative antimicrobial approaches(2–6).
The combination of conventional endodontic therapy and photodynamic therapy(PDT) has been shown as an effective approach in reducing bacterial load in in vitroand in vivo models (7–11).
This study investigated the combination of PDT with endodontic treatment inpatients with necrotic pulp harboring microflora resistant to a previous antibiotictherapy.
Materials and MethodsThirty teeth from 21 patients with periapical lesions who had been previously
treated with endodontic treatment associated with antibiotic were selected. Thepatients were in good health and between the ages of 17 and 52 years. All the teethpresented sights and symptoms of periapical periodontitis and apical bone lesiondetected by radiography, and some patients had pain by vertical percussion and/orlocal edema, all requiring root canal retreatment on teeth with closed apices. Thesame practitioner carried out this study in a private dental office in Sao Paulo, Brazil.The protocol was approved by the Institutional Review Board of the Sao Paulo Univer-sity, and all procedures were conducted according to the principles of the Declarationof Helsinki.
Endodontic TreatmentThirty root canals from anterior teeth were re-treated and received endodontic
treatment followed by PDT. Microbiological samples were taken after accessing theroot canal, after endodontic therapy, and after PDT. The first microbiological sampleconfirmed that all the patients had at least 1 microorganism resistant to antibiotic medi-cation.
A periapical radiograph was taken for each case to determine the presence ofapical lesion, the canal morphology, and its length.
The access to the pulp chamber was gained after installation of a rubber dam, andthen the surrounding area received prophylactic asepsis and was irrigated with 5 mL ofchlorhexidine solution at 2% to ensure that the crown of the tooth had minimal micro-bial load (8).
Once the canal was accessed, a Hedstrom file #15 (Maillefer Instruments SA, Bal-laigues, Switzerland) was inserted inside the canal to remove the gutta-percha and rootcanal sealer obturation; then the root canal was irrigated with 1 mL of sterile saline solu-tion. The canal was dried with 3 sterile paper points (Dentsply Latin America, Petrop-olis, Brazil) and left inside the root canal for 1 minute each. All 3 paper points werecombined for microbiological analysis. This procedure was the first microbiologicalsampling representing the initial contamination. The paper points were deposited ina fresh sterile bottle with sterile nutrient broth.
Antimicrobial Effect of PDT Combined with Endodontic Treatment 1463

Figure 1. Means and standard deviations of multi-drug resistant bacteriainside root canal in each step of the treatment.
Figure 2. Bacteria species per patient in each step of the treatment.
Clinical Research
The canals were prepared with manual instrumentation by K files(Maillefer Instruments SA) by using a standard crown-down techniqueworking to 1 mm short of the working length (file #45 was the averageapical preparation diameter). Ten milliliters of sodium hypochlorite at2.5% and hydrogen peroxide at 3% was alternated between each instru-mentation by using an endodontic needle (27-gauge). At the end of theprocedure the root canals were irrigated with 5 mL of 17% ethylenedia-minetetraacetic acid followed by irrigation with 5 mL of phosphate-buffered saline (PBS) solution to remove the smear layer (12).
The canal was irrigated with 5 mL of sterile saline solution to re-move the antimicrobial agent and dried with another 3 paper points byusing the same methodology cited above (second microbiologicalsample).
PhotosensitizerThe photosensitizer used was a conjugate between polyethyleni-
mine (PEI) and chlorin(e6), which has been previously described indetail (13). The photosensitizer was used in a PBS solution at 60mmol/L.
Light SourceThe illumination was performed with a disposable 200-mm diam-
eter fiber-coupled diode laser (MMOptics, Sao Paulo, Brazil). The laserdelivered 660 nm light at a total power of 40 mW out of the fiber. Thefiber was placed in the apical portion of the root canal at a point whereresistance to the fiber was just felt (usually 1 mm from the apex), andspiral movements, from apical to cervical, were manually performed toensure even diffusion of the light inside the canal lumen (14, 15).
After the endodontic procedure, the canal was irrigated with 0.5mL of the photosensitizer and left inside the root canal for 2 minutesas an incubation time. The root canal was then irradiated for 240seconds (total energy, 9.6 J), and the fiber was changed betweeneach patient. The root canal was again irrigated with 10 mL of sterilesaline solution to remove the photosensitizer and dried as before (thirdmicrobiological sample).
A calcium hydroxide paste (Ultradent Products, South Jordan, UT)was placed into the canals; cotton was placed in the pulp chamber, andthe teeth were dressed with temporary restorative material (IRM; Dents-ply Latin America).
One week later, a second session of each therapy was performedwithout microbiological sampling. Thereafter, root canal was sealed byusing conventional techniques with Sealer 26 (Dentsply Petropolis),and the tooth was restored with a composite resin Z250 (3M, Sumare,Brazil). This 1-week interappointment dressing approach was used byGarcez et al (8). Briefly, the pH in the environment is increased; conse-quently, the live-time of reactive oxygen species increases, and thephotodynamic effect is improved at the second session.
Microbiological AnalysesThe samples were sent in a sterile bottle with fresh sterile nutrient
broth (Viability Medium Goteborg Agar III) to a private microbiologicalfacility for identification and to antibiogram analyses. The bacterialspecies were identified on the basis of Gram stain, aerotolerance, colonymorphology, esculin hydrolysis, nitrate reduction, indole production,(alpha)-glycosidase and N-benzoyl-DL-arginine-2-naphthylamide(BANA) hydrolysis, oxidase and catalase activities. The antibiogramtested 17 different antibiotics by using the Kirby-Bauer method (16).
ResultsThe first samples showed that all teeth harbored at least 1 resistant
microorganism, indicating unsuccessful previous treatment and/or
1464 Garcez et al.
antibiotic therapy. The number of multi-drug resistant bacterial speciesdid vary widely between individual teeth, with a mean value of 2.16species per root canal sample (range, 4–1). This was probably dueto differences in the geometry of the root canal systems and initialcontamination. The mean values of the number of species for eachstep are given in Fig. 1.
Among the initial samples, 33% were gram-negative, and 67%were gram-positive bacteria; moreover, 57% were facultative anaer-obes, and 43% were obligate anaerobes.
After the endodontic therapy the infectious burden was reduced to0.8 species per root canal (range, 2–0). After PDT, microorganismgrowth was not detected on any of the samples from any of the rootcanals. Ten of the root canals treated had 100% bacterial eliminationafter endodontic treatment, whereas all 30 teeth showed total absenceof microorganisms after the combination.
The multi-drug resistant bacteria found in the initial samples were,in order of prevalence, Enterococcus sp, Prevotella sp, Actinomycessp, Peptostreptococcus sp, Streptococcus sp, Fusobacterium sp, Por-phyromonas sp, Enterobacter sp, and Propionibacterium sp. Afterthe endodontic therapy, the species found were Enterococcus sp, Acti-nomyces sp, Peptostreptococcus sp, Fusobacterium sp, and Porphyr-omonas sp. All teeth were completely free of bacteria after the 2combination therapies. Fig. 2 shows the number of bacterial speciesthat grew in each sample from each stage of the therapy.
JOE — Volume 36, Number 9, September 2010

Figure 3. Number of species resistant to each type of antibiotic.
Clinical Research
The antibiogram showed bacteria resistant to ampicillin, penicillinG, vancomycin cephalosporin, clindamycin, chloramphenicol, erythro-mycin, and tetracycline. Fig. 3 shows the number of species that wereresistant to each antibiotic.
DiscussionPrevious studies from our group (7, 8) and from other groups (9,
17, 18) showed that a combination of conventional endodontic therapyfollowed by antimicrobial PDT was effective in reducing bacterial load inex vivo root canals (for planktonic and biofilm endodonticmicroorganisms) and in patients. In both studies we used the samephotosensitizer, a conjugate between PEI and chlorin(e6) (PEI-ce6)that has been designed to have a broad-spectrum antimicrobial effectunder illumination (19).
This study shows for the first time, in vivo, the susceptibility ofdrug-resistant bacteria in root canal infections to PDT. The literaturereports that endodontic therapy will have a 94% success rate whena negative microbiological culture is obtained from the root canal atthe time of obturation. On the other hand, when obturation is per-formed and the cultures are positive, the success rate is reduced to68%; in the case of a periapical lesion, the failure of healing is morelikely when the canal is obturated in the presence of persistent infection(20, 21). Treatment procedures to eliminate the infection include rootcanal debridement and mechanical shaping or smoothing (22), irriga-tion with a disinfectant agent, the application of an interappointmentdressing, and sealing of the root canal (23). In case of infection, theuse of antibiotics and antiseptics is an alternative approach, but thelong-term use of antimicrobial agents, however, can be rendered inef-fective by resistance developing in the target organisms (24–26). Ourresults confirm that the long-term use of antibiotics can lead to devel-opment of resistance in microorganisms.
Endodontic treatment alone had an effect in reducing the numberof multi-drug resistant species in root canals and produced a totalbacterial elimination in 10 of 30 teeth, but the addition of PDT produceda reduction in bacterial burden leading to total elimination in all teeth.
Previous studies compared photodynamic antimicrobial therapyof multi-drug resistant bacteria with wild-type strains. Maisch et al(27) found identical killing of methicillin-resistant Staphylococcusaureus (MRSA) and native strain. Wainwright et al (28) showed thatPDT killed MRSA somewhat less efficiently than the native strain; alsoEmbleton et al (29) used a phage delivery system to carry out PDTwith the photosensitizer Sn-ce6 and again found that MRSA was suscep-tible. Tang et al (30) showed that PDT with a polylysine-chlorin(e6)
JOE — Volume 36, Number 9, September 2010
killed multi-drug resistant and native Escherichia coli strains equallyand killed MRSA better than the sensitive strain.
Our results showed that the combination of endodontic therapyand PDT killed all 9 multi-drug resistant bacterial species found inroot canal infections. Therefore, PDT not only kills multi-drug resistantbacteria in vitro but is also effective in eliminating species resistant todiverse antibiotics in patients.
The samples showed that the multi-drug resistant bacteria foundconsisted of facultative and obligate anaerobic species. However, it iswell-known that aerobic microorganisms can deal better with reactiveoxygen species, and the greater susceptibility of anaerobes to the reac-tive oxygen species produced during PDT could explain the 100%reduction of multi-drug resistant bacteria after the combinationtherapy.
Furthermore, the majority of the species found were gram-positive, and the literature has shown that PDT is more efficient in killingthese microorganisms (6, 7, 13, 17). Nevertheless, the photosensitizerused in this study (PEI-ce6) has also a high efficacy in killing gram-negative species compared with alternative photosensitizers such astoluidine blue (31). In fact, despite several attempts to induce resis-tance, the use of PDT to kill bacteria has not resulted in the generationof any PDT resistance among treated species, suggesting that bacteria donot find it easy to develop defenses against the reactive oxygen speciesgenerated during PDT (32).
In addition, the literature has showed that it is safe to use PDTagainst microorganisms near normal cells, for example, cells fromapical region. George and Kishen (33) showed that cytotoxicity wassignificantly less in PDT compared with conventional antimicrobial irri-gation. In an in vitro experiment, Enterococcus faecalis were killed ata faster rate than normal fibroblasts. PDT produced 97.7% bacterialkilling and only 30% fibroblast dysfunction. Also Xu et al (34) suggestedthat there is a safe therapeutic window whereby PDT can inactivateendodontic pathogens without affecting host cell viability.
ConclusionsOur results suggest that the use of PDT as an adjuvant to conven-
tional endodontic treatment leads to a significant further reduction ofbacterial load and is effective against multi-drug resistant bacteria.PDT offers an efficient means of destroying multi-drug resistant bacteriaremaining inside the root canal system after using conventionalendodontic chemomechanical therapy.
AcknowledgmentsThe authors deny any conflicts of interest.
References1. Siqueira JF Jr. Endodontic infections: concepts, paradigms, and perspectives. Oral
Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:281–93.2. Yoshikawa TT. Antimicrobial resistance and aging: beginning of the end of the anti-
biotic era? J Am Geriatr Soc 2002;50:s226–9.3. Hancock RE, Bell A. Antibiotic uptake into gram-negative bacteria. Eur J Clin Micro-
biol Infect Dis 1988;7:713–20.4. Livermore DM. Antibiotic resistance in staphylococci. Int J Antimicrob Agents 2001;
16:3–10.5. Agarwal R, Athar M, Urban SA, Bickers DR, Mukhtar H. Involvement of singlet
oxygen in chloroaluminum phthalocyanine tetrasulfonate-mediated photoenhance-ment of lipid peroxidation in rat epidermal microsomes. Cancer Lett 1991;56:125–9.
6. Phoenix DA, Sayed Z, Hussain S, Harris F, Wainwright M. The phototoxicity of phe-nothiazinium derivates against Escherichia coli and Staphylococcus aureus. FEMSImmun Med Microbiol 2003;39:17–22.
7. Garcez AS, Ribeiro MS, Tegos GP, Nunez SC, Jorge AO, Hamblin MR. Antimicrobialphotodynamic therapy combined with conventional endodontic treatment to elim-inate root canal biofilm infection. Lasers Surg Med 2007;39:59–66.
Antimicrobial Effect of PDT Combined with Endodontic Treatment 1465

Clinical Research
8. Garcez AS, Nunez SC, Hamblin MR, Ribeiro MS. Antimicrobial effects of photody-namic therapy on patients with necrotic pulps and periapical lesion. J Endod2008;34:138–42.
9. George S, Kishen A. Influence of photosensitizer solvent on the mechanisms of pho-toactivated killing of Enterococcus faecalis. Photochem Photobiol 2008;84:734–40.
10. Bergmans L, Moisiadis P, Huybrechts B, Van Meerbeek B, Quirynen M,Lambrechts P. Effect of photo-activated disinfection on endodontic pathogens exvivo. Int Endod J 2008;41:227–39.
11. Bonsor SJ, Nichol R, Reid TM, Pearson GJ. An alternative regimen for root canaldisinfection. Br Dent J 2006;201:101–5.
12. Haapasalo M, Orstavik D. In vitro infection and disinfection of dentinal tubules.J Dent Res 1987;66:1375–9.
13. Tegos GP, Anbe M, Yang C, et al. Protease-stable polycationic photosensitizer conju-gates between polyethyleneimine and chlorin(e6) for broad-spectrum antimicrobialphotoinactivation. Antimicrob Agents Chemother 2006;50:1402–10.
14. Gutknecht N, van Gogswaardt D, Conrads G, Apel C, Schubert C, Lampert F. Diodelaser radiation and its bactericidal effect in root canal wall dentin. J Clin Laser MedSurg 2000;18:57–60.
15. Silva Garcez A, Nunez SC, Lage-Marques JL, Jorge AO, Ribeiro MS. Efficiency ofNaOCl and laser-assisted photosensitization on the reduction of Enterococcus fae-calis in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:e93–8.
16. Bauer AW, Kirby WM, Sherris JC, Turck M. Antibiotic susceptibility testing by a stan-dardized single disk method. Am J Clin Pathol 1966;45:493–6.
17. Fimple JL, Fontana CR, Foschi F, et al. Photodynamic treatment of endodontic poly-microbial infection in vitro. J Endod 2008;34:728–34.
18. Soukos NS, Chen PS, Morris JT, et al. Photodynamic therapy for endodontic disin-fection. J Endod 2006;32:979–84.
19. Tegos GP, Anbe M, Yang C, et al. Protease-stable polycationic photosensitizer conju-gates between polyethyleneimine and chlorin(e6) for broad-spectrum antimicrobialphotoinactivation. Antimicrob Agents Chemother 2006;50:1402–10.
20. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of rootfilling on the outcome of endodontic treatment of teeth with apical periodontitis. IntEndod J 1997;30:297–306. Erratum in: Int Endod J 1998;31:148.
21. Nair PN, Sjogren U, Krey G, Kahnberg KE, Sundqvist G. Intraradicular bacteria andfungi in root-filled, asymptomatic human teeth with therapy-resistant periapical
1466 Garcez et al.
lesions: a long-term light and electron microscopic follow-up study. J Endod1990;16:580–8.
22. Bahcall JK, Barss JT. Understanding and evaluating the endodontic file. Gen Dent2000;48:690–2.
23. Sedgley C. Root canal irrigation: a historical perspective. J Hist Dent 2004;52:61–5.24. Reynaud AF, Geijersstam AH, Ellington MJ, Warner M, Woodford N, Haapasalo M.
Antimicrobial susceptibility and molecular analysis of Enterococcus faecalis origi-nating from endodontic infections in Finland and Lithuania. Oral Microbiol Immu-nol 2006;21:164–8.
25. Pinheiro ET, Gomes BP, Drucker DB, Zaia AA, Ferraz CC, Souza-Filho FJ. Antimicro-bial susceptibility of Enterococcus faecalis isolated from canals of root filled teethwith periapical lesions. Int Endod J 2004;37:756–63.
26. Figdor D. Microbial aetiology of endodontic treatment failure and pathogenic prop-erties of selected species. Aust Endod J 2004;30:11–4.
27. Maisch T, Bosl C, Szeimies RM, Lehn N, Abels C. Photodynamic effects of novel XFporphyrin derivatives on prokaryotic and eukaryotic cells. Antimicrob Agents Che-mother 2005;49:1542–52.
28. Wainwright M, Phoenix DA, Laycock SL, Wareing DR, Wright PA. Photobactericidalactivity of phenothiazinium dyes against methicillin-resistant strains of Staphylo-coccus aureus. FEMS Microbiol Lett 1998;160:177–81.
29. Embleton ML, Nair SP, Heywood W, Menon DC, Cookson BD, Wilson M. Develop-ment of a novel targeting system for lethal photosensitization of antibiotic-resistantstrains of Staphylococcus aureus. Antimicrob Agents Chemother 2005;49:3690–6.
30. Tang HM, Hamblin MR, Yow CM. A comparative in vitro photoinactivation study ofclinical isolates of multidrug-resistant pathogens. J Infect Chemother 2007;13:87–91.
31. Demidova TN, Hamblin MR. Effect of cell-photosensitizer binding and cell density onmicrobial photoinactivation. Antimicrob Agents Chemother 2005;49:2329–35.
32. Lauro FM, Pretto P, Covolo L, Jori G, Bertoloni G. Photoinactivation of bacterialstrains involved in periodontal diseases sensitized by porphycene-polylysine conju-gates. Photochem Photobiol Sci 2002;1:468–70.
33. George S, Kishen A. Advanced noninvasive light-activated disinfection: assessment ofcytotoxicity on fibroblast versus antimicrobial activity against Enterococcus faecalis.J Endod 2007;33:599–602.
34. Xu Y, Young MJ, Battaglino RA, et al. Endodontic antimicrobial photodynamictherapy: safety assessment in mammalian cell cultures. J Endod 2009;35:1567–72.
JOE — Volume 36, Number 9, September 2010

Clinical Research
Antigenic Activity of Bacterial Endodontic Contents fromPrimary Root Canal Infection with Periapical Lesions againstMacrophage in the Release of Interleukin-1b and TumorNecrosis Factor a
Frederico C. Martinho, DDS, MSc,* Wanderson Miguel Maia Chiesa, DDS, MSc,*
Fabio R.M. Leite, DDS, MSc, PhD,† Joni A. Cirelli, DDS, MSc, PhD,‡
and Brenda P.F.A. Gomes, DDS, MSc, PhD*
Abstract
Introduction: Periradicular tissue chronic stimulation byendotoxin may cause apical periodontitis. This studyinvestigated the microbial profile and the levels of endo-toxin found in primary root canal infection with apical pe-riodontitis, determined their antigenicity againstmacrophages through the levels of interleukin (IL)-1band tumor necrosis factor a (TNF-a), and evaluated theirrelationship with clinical and radiographic findings.Methods: Samples were taken from 21 root canalswith primary endodontic infection and apical periodonti-tis with paper points. PCR technique (16S rDNA) wasused for the detection of the target bacteria. LimulusAmebocyte Lysate (LAL) was used to measure endotoxin.The amounts of IL-1ß/ TNF-alpha in macrophages super-natants were measured by enzyme-linked immunosor-bent assay – Duoset-kit (ELISA). Results: Prevotellanigrescens (13/21), Porphyromonas endodonta-lis (6/21), and Treponema socranskii (6/21) were themost frequently detected gram-negative bacterialspecies. The presence of the sinus tract (2/21) wasrelated to the detection of Filifactor alocis (p <0.05), whereas a tooth with a radiolucent area $2 mmwas related to the detection of Treponema denti-cola. A correlation was found between the number of
From the *Department of Restorative Dentistry, EndodonticDivision, Piracicaba Dental School, State University of Campi-nas, Campinas, Brazil; †Department of Semiology and Clinics,Periodontic Division, Dental School, Federal University ofPelotas, Pelotas, Brazil; and ‡Department of Diagnosis andOral Surgery, Periodontic Division, Araraquara Dental School,State University of Sao Paulo, Sao Paulo, Brazil.
Supported by the Brazilian agencies FAPESP (07/58518-4,08/58299-3, 08/ 57954-8, and 08/57551-0) and CNPq(3470820/2006-3, 471631/2008-6, and 302575/2009-0).
Address requests for reprints to Dr Brenda P.F.A. Gomes,Piracicaba Dental School, State University of Campinas-UNICAMP, Department of Restorative Dentistry, EndodonticDivision, Av Limeira 901, Bairro Areiao, Piracicaba, Sao Paulo,Brazil CEP 13414-903. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.012
JOE — Volume 36, Number 9, September 2010
gram-negative bacteria and the levels of IL-1b/TNF-a (p < 0.05). Increased levels ofendotoxin were followed by TNF-a release (p < 0.05). Higher levels of IL-1b (p <0.05) and endotoxin contents were related to the larger size of the radiolucent area.Conclusion: The antigenicity of the endodontic contents is not only related to theamount of endotoxin found in the root canal but also to the number of different speciesof gram-negative bacteria involved in the infection. Moreover, a larger size ($2 mm) ofthe radiolucent area was related to IL-1b and endotoxin. (J Endod 2010;36:1467–1474)
Key WordsAntigenicity, bacteria, endodontic, endotoxin, macrophages
Primary endodontic infection is a polymicrobial infection caused predominantly bygram-negative anaerobic bacteria (1) that present lipopolysaccharide (LPS) on
the outer layers of their cell walls. LPS is released during disintegration, multiplication,or bacterial death (2) and is capable of penetrating into the periradicular tissues (3),acting as endotoxin in the host organism (4) and leading to periradicular inflammationand bone destruction (5). The lipid A is the bioactive component of LPS responsible forthe majority of the immunoresponse (3).
The accumulation of bacteria components in an infected area, particularly endo-toxins (including lipoteichoic acid, peptidoglycan, lipopolysaccharide, and others),can stimulate the release of proinflammatory cytokines by different cell lines throughTLR2 and -4 activation (5–7). The inflammatory tissue present in periradicularlesions is populated predominantly by macrophage (8, 9), which is the majorsource of interleukin-1b (IL-1b) (10), and almost the exclusive producer of tumornecrosis factor a (TNF-a) (11) in the presence of bacteria or LPS.
Clinical investigations of primary endodontic infection have elucidated the strongcorrelation between oral bacteria LPS and the presence of apical periodontitis (6, 12-15). Moreover, higher contents of endotoxins in root canals have been associated withspontaneous pain (6, 12, 16) and clinical signs/symptoms such as pain on palpation,tenderness to percussion, and exudation (6, 12, 14, 16).
Previous in vitro investigations (5–7) have shown that oral bacterial LPS extractedfrom bacteria commonly found in root canal infection induces a potent inflammatoryresponse against different cell line cultures. IL-1b and TNF-a have been detected inperiapical tissues (3, 9, 17–19) and root canal exudates (20–23) from primaryroot canal infection in the presence apical periodontitis. Higher contents of IL-1bhave been detected in teeth with clinical signs/symptoms (3, 23) and larger size ofradiolucent area corresponding to bone resorption (21, 22). However, studiescorrelating all these aspects have not yet been provided in the literature. Therefore,the aim of this clinical study was to investigate the microbial profile and the levels ofendotoxin found in primary root canal infection with apical periodontitis and todetermine their antigenicity against macrophages through the levels of IL-1b/TNF-a,evaluating their relationship with clinical and radiographic findings.
Antigenic Activity of Bacteria from Primary Root Canal Infection with Periapical Lesions 1467

Clinical Research
Material and MethodsPatient Selection
Twenty-one patients who attended the Piracicaba Dental School,Piracicaba, SP, Brazil, in need of endodontic treatment were includedin this research. The age of the patients ranged from 13 to 73 years.Samples were collected from 21 root canals with pulp necrosis andshowing radiographic evidence of apical periodontitis. The selectedteeth showed absence of periodontal pockets more than 4 mm. Thefollowing clinical/radiographic features were found: pain on palpation(9/21), tenderness to percussion (8/21), exudation (12/21), andradiolucent area $2 mm (11/21) and <2 mm (10/21). None of thepatients reported spontaneous pain.
A detailed dental history was obtained from each patient. Patientswho had received antibiotic treatment during the last 3 months or whohad any general disease were excluded. The Human VolunteersResearch and Ethics Committee of the Piracicaba Dental Schoolapproved the protocol describing specimen collection for this investi-gation, and previously all patients signed an informed consent docu-ment.
Sampling ProceduresAll materials used in this study were heat sterilized at 200�C for 4
hours to become apyrogenic. The method followed for the disinfectionof the operative field had been described previously (14, 15). Briefly,the teeth were isolated with a rubber dam. The crown and thesurrounding structures were disinfected with 30% H2O2 for 30seconds followed by 2.5% NaOCl for an additional 30 seconds.Subsequently, 5% sodium thiosulphate was used to inactivate theirrigant. The sterility of the of the external surfaces of the crown waschecked by taking a swab sample from the crown surface andstreaking it on blood agar plates that were incubated aerobically andanaerobically.
A two-stage access cavity preparation was made without the use ofwater spray but under manual irrigation with sterile/apyrogenic salinesolution and by using sterile/apyrogenic high-speed diamond bur. Thefirst stage was performed to promote a major removal of contaminants.In the second stage, before entering the pulp chamber, the access cavitywas disinfected following the protocol described earlier. The sterility ofthe internal surface of the access cavity was checked as previouslydescribed, and all procedures were performed aseptically. A new sterileand apyrogenic bur was used, accomplished by irrigation with sterileapyrogenic water to access the canal. The endotoxin sample was takenintroducing sterile pyrogen-free paper points (size 15; Dentsply-Maillefer, Ballaigues, Switzerland) into the full length of the canal(determined radiographically) and retained in position during 60seconds. Immediately, the paper point was placed in a pyrogen-freeglass and frozen at �80�C for future Limulus amebocyte lysate assay(LAL) and cell culture stimulation. The procedure was repeated withfive sterile paper points. The paper points were pooled in a steriletube containing 1 mL of VMGA (Viability Medium Goteborg Agar) IIItransport medium and immediately processed for DNA extraction forthe detection of target bacteria by molecular method (16S ribosomalDNA).
Bacterial Detection (PCR 16S rDNA)Reference bacteria strains used in this study were purchased from
the American Type Culture Collection (ATCC) and are listed as follows:Dialister pneumosintes (ATCC 33048), Prevotella intermedia (ATCC25611), Prevotella nigrescens (ATCC 33099), Aggregatibacter acti-nomycetemcomitans (ATCC 43718), Porphyromonas gingivalis(ATCC 33277), Filifactor alocis (ATCC 35896), Tannerella forsythia
1468 Martinho et al.
(ATCC 43037), Prevotella tannerae (ATCC 51259), Treponema den-ticola (ATCC 35405), Porphyromonas endodontalis (ATCC 35406),Treponema socranskii (35536), and Parvimonas micra (ATCC33270). Bacterial selection criteria were performed based on themost commonly found species in primarily root canal infection.
DNA Extraction. Microbial DNA from endodontic samples as well asfrom ATCC bacteria were extracted and purified with the QIAamp DNAMini Kit (Qiagen, Hilden, Germany) according to the manufacturer’sinstructions. The DNA concentration (absorbance at 260 nm) wasdetermined using a spectrophotometer (Nanodrop 2000; ThermoScientific, Wilmington, DE).
PCR Assay. The PCR reaction was performed in a thermocyler (My-Cycler; Bio-Rad, Hercules, CA) thermocycler in a total volume of 25 mLcontaining 2.5 mL of 10X Taq buffer (1�) (MBI Fermentas, Mundol-sheim, France), 0.5 mL of dNTP mix (25 mmol/L of each deoxyribonu-cleoside triphosphate–dATP, dCTP, dGTP, and dTTP) (MBI Fermentas,Hanover, MD), 1.25 mL of 25 mmol/L MgCl2, 0.25 mL of forward andreversal universal primers (0.2 mmol/L) (Invitrogen, Eugene, OR),1.5 mL of sample DNA (1 mg/50 mL), 1.5 mL of Taq DNA polymerase(1 U) (MBI Fermentas), and 17.25 mL of nuclease-free water. Theprimer sequences and PCR cycling parameters were previously opti-mized (13-15) and listed in Table 1.
Determination of Endotoxin Concentration(Turbidimetric Test and LAL Assay)
The turbidimetric test (BioWhitaker, Inc, Walkersville, MD) wasused to measure endotoxin concentrations in the root canals usingthe LAL technique. First, as a parameter for the calculation of the amountof endotoxins in root canal samples, a standard curve was plotted usingendotoxins supplied in the kit with a known concentration (100 EU/mL)and its dilutions with the following final concentrations (ie, 0.01, 0.10,1, and 10 EU/mL) following the manufacturer’s instructions.
Test Procedure. All reactions were accomplished in duplicate tovalidate the test. A 96-well microplate (Corning Costar, Cambridge,MA) was used in a heating block at 37�C and maintained at this temper-ature throughout the assay. First, the endotoxin samplings were sus-pended in 1 mL of LAL water supplied on the kit and agitated invortex for 60 seconds and serial diluted to the 10�1. Immediately,100 mL of the blank followed the standard endotoxin solutions inconcentrations (ie, 0.01, 0.10, 1, and 10 EU/mL), and 100 mL of thesamples were added in duplicate in the 96-well microplate. The testprocedure was performed following the manufacturer’s instructions.The absorbencies of endotoxin were measured individually using anenzyme-linked immunosorbent assay plate reader (Ultramark, Bio-Rad Laboratories, Inc) at 340 nm.
Calculation of Endotoxin Concentrations. Because the meanabsorbance value of the standards was directly proportional to theconcentration of endotoxins present, the endotoxin concentrationwas determined from the standard curve.
Cell Culture and Cytokine ExpressionMacrophages (RAW 264.7) were cultured in 100-mm culture
plates in Dulbecco’s modified Eagle minimal essential medium supple-mented (DMEM) with 100 IU/mL of penicillin, 100 mg/mL of strepto-mycin, and 10% heat-inactivated fetal bovine serum and maintainedin a humidified atmosphere at 37�C and 5% CO2 until 90% confluence.Unless noted otherwise, all tissue culture reagents were obtained fromInvitrogen (Carlsbad, CA). Macrophages were released from 100-mmplates with 0.25% trypsin and counted in a Newbauer chamber; a totalof 104 macrophages were grown for 48 hours in each well of six-well
JOE — Volume 36, Number 9, September 2010

TABLE 1. PCR Primer Pairs and Cycling Parameters Used for Detection of Bacteria Species in Primary Root Canal Infection with Apical Periodontitis
Target bacteria Primer pairs (5’- 3’)Amplicon
size Cycles
Universal (16s rDNA) Forward: TCC TAC GGG AGG CAG CAG T Initial denaturation at 95�C for10 min and 40 cycles of 95�C for10 s, 60�C for 10 s, and a finalextension step at 72�C for 25 s
Reverse: GGA CTA CCA GGG TAT CTA ATC CTG TT 466 bp
Dialister pneumosintes Forward: TTC TAA GCA TCG CAT GGT GC Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 55�C for 1 min, 72�C for 2 min,and a final step 72�C for 2 min
Reverse: GAT TTC GCT TCT CTT TGT TG 1105 bp
Prevotella intermedia Forward: TTT GTT GGG GAG TAA AGC GGG 575 bp Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 58�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: TCA ACA TCT CTG TAT CCT GCG T
Prevotella nigrescens Forward: ATG AAA CAA AGG TTT TCC GGT AAG Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 58�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: CCC ACG TCT CTG TGG GCT GCG A 804 bp
Aggregatibacteractinomycetemcomitans
Forward: AAA CCC ATC TCT GAG TTC TTC TTC Initial denaturation at 94�C for30 s and 36 cycles of: 95�C for
30 s, 55�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: ATG CCA ACT TGA CGT TAA AT 557 bp
Porphyromonas gingivalis Forward: AGG CAG CTT GCC ATA CTG CG 404 bp Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 60�C for 1 min, 72�C for 2 min,and a final step 72�C for 2 min
Reverse: ACT GTT AGC AAC TAC CGA TGT
Filifactor alocis Forward: CAG GTG GTT TAA CAA GTT AGT GG Initial denaturation at 95�C for2 min and 26 cycles of 95�C for
30 s, 58�C for 1 min, 72�C for 1 min,and a final step 72�C for 2 min
Reverse: CTA AGT TGT CCT TAG CTG TCT CG 594 bp
Tannerella forsythia Forward: GCG TAT GTA ACC TGC CCG CA Initial denaturation at 95�C for lmin and 36 cycles of 95�C for 30 s,
60�C for 1 min, 72�C for 1 min,and a final step 72�C for 2 min
Reverse: TGC TTC AGT GTC AGT TAT ACC T 641 bp
Prevotella tannerae Forward: CTT AGC TTG CTA AGT ATG CCG 550 bp Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 55�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: CAG CTG ACT TAT ACT CCC G
Treponema denticola Forward: TAA TAC CGA ATG TGC TCA TTT ACA T Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 60�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: TCA AAG AAG CAT TCC CTC TTC TTC TTA 316 bp
Porphyromonasendodontalis
Forward: GCT GCA GCT CAA CTG TAG TC Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 58�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: CCG CTT CAT GTC ACC ATG TC 672 bp
Treponema socranskii Forward: GAT CAC TGTATA CGG AAG GTA GAC A 288 bp Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 56�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: TAC ACT TAT TCC TCG GAC AG
Parvimonas micra Forward: AGA GTT TGA TCC TGG CTC AG Initial denaturation at 95�C for2 min and 36 cycles of 94�C for
30 s, 60�C for 1 min, 72�C for 2 min,and a final step 72�C for 10 min
Reverse: ATA TCA TGC GAT TCT GTG GTC TC 207 bp
Clinical Research
plates, deinduced by incubation for 8 hours in culture medium(DMEM) containing 0.3% fetal bovine serum, and stimulated with 60mL of root canal contents during 24 hours in order to quantify the totalamount of protein released in the culture media, IL-1b, and TNF-a protein. The supernatants were collected and stored at �80�C untilprotein evaluation.
IL-1b and TNF-a Messenger RNA ExpressionThe macrophage cell viability was tested in the present study by its
capacity to express IL-1b and TNF-a messenger RNA after 24 hours ofroot canal contents stimulation. A total of 104 macrophages were grownfor 48 hours in each well of six-well plates, deinduced by incubation for
JOE — Volume 36, Number 9, September 2010 Antigenic Act
8 hours in culture medium (DMEM) containing 0.3% fetal bovineserum, and stimulated with 60 uL of primary infection contents for24 hours for IL-1b and TNF-a messenger RNA expression. Total RNAwas isolated from cells using Trizol (Invitrogen, Carlsbad, CA) accord-ing to the manufacturer’s instructions. The quantity and purity of totalRNA were determined on a Biomate 3 spectrophotometer (Thermo-Spectronic, Rochester, NY). Complementary DNA was synthesized byreverse transcription of 500 ng of total RNA using 2.5 mmol/L Oligo(dT)12-18 primers and 1.25 U/mL Moloney murine leukemia virusreverse transcriptase in the presence of 3 mmol/L MgCl2, 2 mmol/LdNTPs, and 0.8 U/mL RNAse inhibitor according to the manufacturer’sprotocol (Improm II; Promega, Madison, WI, USA). The PCR reactionwas performed in a MyCycler (Bio-Rad) thermocycler using 2 mL of the
ivity of Bacteria from Primary Root Canal Infection with Periapical Lesions 1469

Clinical Research
reverse transcription reaction product on a 20-uL total volume PCRreaction mix (GoTaq Flexi, Promega) in the presence of 100 pmol/mLof each gene’s primers (50 pmol/mL of sense and antisense primers)for IL-1b, TNF-a, and GAPDH genes yielding products of 494, 451,and 418 bp, respectively. The primer pair used for IL-1b (accessionno.: NM031512) was sense 5’-GACCTGTTCTTTGAGGCTGA-3’, antisense5’-CGTTGCTTGTCTCTCCTTGT-3’; TNF-alpha (accession no.:NM012675) sense 5’-GGAGAACAGCAACTCCAGAA-3’, and antisense5’-TCTTTGAGATCCATGCCATT-3’ and for GAPDH (accession no.:BC083065) sense 5’-CACCATGGAGAAGGCCGGGG-3’, and antisense5’-GACGGACACATTGGGGTAG- 3’. The optimized cycling conditionsused for TNF-a and IL-1b were initial denaturation at 95�C for 2minutes and 35 cycles of 95�C for 1 minute, 58�C for 1 minute,72�C for 2 minutes, and a final extension step at 72�C for 7 minutesin the presence of 1.5 mmol/L MgCl2. For GAPDH, conditions wereas follows: initial denaturation at 95�C for 2 minutes and 25 cycles of95�C for 1 minute, 52�C for 1 minute, 72�C for 1 minute, and a finalextension step at 72�C for 10 minutes in the presence of 1.5 mmol/LMgCl2. PCR products were resolved by electrophoresis on 1.5%(w/v) agarose gels containing ethidium bromide (0.5 mg/mL). Theamplified DNA bands were analyzed densitometrically after digitalimaging capture (Image Quant 100; GE Healthcare, Sunnyvale, CA)using ImageJ 1.32j software (National Institute of Health, http://rsb.info.nih.gov/ij/; Bethesda, MD). The density of the bands correspondingto TNF-a and IL-1b messenger RNA in each sample was normalized to thequantity of the housekeeping gene GAPDH and expressed as fold changeover unstimulated control.Measurements of Total Protein Levels Released to theCulture Media
The total amount of protein released in the culture media followingroot canal contents stimulation was measured by the Coomassie (Brad-ford) Protein Assay kit (Rockford, IL). As a parameter for calculation ofthe amount of protein released to the culture media, a standard curvewas plotted using bovine serum albumin standard supplied in the kitwith a known concentration (2.0 mg/mL) with a series bovine serumalbumin concentration (ie, 0, 25, 125, 250, 500, 750, 1,000, 1,500,and 2,000 mg/mL). The protein assay was performed following themanufacturer’s instructions.
Calculation of Protein ConcentrationThe protein standard and sample solutions were measured indi-
vidually using an enzyme-linked immunosorbent assay plate reader (Ul-tramark) at 595 nm. Because this absorbance value was directlyproportional to the concentration of protein, the protein concentrationfrom the samples solutions was determined from the standard curve.
Measurements of IL-1b and TNF-a LevelsThe amounts of IL-1b and TNF-a released to the culture media
following root canal contents stimulation of macrophages weremeasured by enzyme-linked immunosorbent assay (Duoset kit; R&D,Minneapolis, MN). A medium of unstimulated macrophage culturewas used as a negative control. Briefly, standard, control, or samplesolution was added to the enzyme-linked immunosorbent assay wellplate, which had been precoated with specific monoclonal capture anti-body. After shaking gently for 3 hours at room temperature, polyclonalanti–TNF-a and IL-1b antibody, conjugated with horseradish peroxi-dase, was added to the solution, respectively, and incubated for 1hour at room temperature. A substrate solution containing hydrogenperoxidase and chromogen was added and allowed to react for 20minutes. The levels of cytokines were assessed by a micro–enzyme-
1470 Martinho et al.
linked immunosorbent assay reader at 450 nm and normalized withan abundance of standard solution. Each densitometric value wasexpressed as mean� standard deviation and was obtained from threeindependent experiments.
Statistical AnalysisThe data collected for each case (clinical features and the bacteria
isolated) were typed onto a spreadsheet and statistically analyzed usingSPSS for Windows (SPSS, Inc., Chicago, IL). The Pearson chi-square testor the one-sided Fisher exact test, as appropriate, was chosen to test thenull hypothesis that there was no relationship between bacteria speciessuch as endodontic clinical signs/symptoms and the presence ofa specific group of bacteria in the root canal samples. The Pearson coef-ficient was used to correlate the amount of LPS, IL-1b, and TNF-a levelswith the size of the radiolucent area and the number of gram-negativebacteria present in root canals with apical periodontitis. The correlationbetween the presence of clinical/radiographic findings with the medianlevels of LPS, IL-1b, and TNF-a was analyzed using the Student t test orthe Mann-Whitney U test; p < 0.05 was considered statistically significant.
ResultsBacterial Detection (16 rDNA)
Bacterial DNA was detected in all root canal samples (21/21). Themaximum of five species was detected in the root canal samples. At least1 gram-negative species was detected in 18 of 21 root canals (Table 2).Prevotella nigrescens (13/21), Porphyromonas endodontalis (6/21), and Treponema socranskii (6/21) were the three most frequentlytarget gram-negative bacterial species detected. A combination of two ormore gram-negative target species was detected in 8 of 21 root canals(Table 2). The Parvimonas micra positive samples (6/21) were asso-ciated in 100% with at least one gram-negative target bacterial species.Positive associations were found between P. endodontalis and Trepo-nema denticola (p = 0.003, Odds Ratio = 2.000, Confidence Bound =0.899-4.452) and P. micra and Filifactor alocis (p = 0.008, OR =1.667, CB = 0.815-3.409) in primary root canal infection. Teeth withsinus tract (2/21) were related to the presence of F. alocis (p =0.040, OR = 18.000, CB = 0.585-553.586). A radiolucent area $2mm was associated with the presence of T. denticola (p = 0.012,OR = 10.000, CB = 2.685-37.239). A correlation between the numberof different gram-negative bacterial species and the levels of IL-1b (p <0.05, Pearson r = 0.124) (Fig. 1A) and TNF-a (p < 0.05, Pearson r =0.173) (Fig. 1B) was found.
Determination of Endotoxin Concentration(Turbidimetric Test and LAL Assay)
The LAL assay (turbidimetric test) indicated that endotoxin waspresent in 100% of the root canals samples (21/21). The median valueof endotoxin contents was 7,490 pg/mL in root canals with periradicu-lar lesions. A higher median value of endotoxin contents was detected inteeth with the presence of a radiolucent area $2 mm (9,190 pg/mL;range, 257-212,000 pg/mL) than in teeth with a radiolucent area <2mm (3,480 pg/mL; range, 27-289,000 pg/mL). Teeth with exudationpresented higher median levels of endotoxins (9,190 pg/mL; range,355-289,000 pg/mL) than teeth with no exudation (2,620 pg/mL;range, 27-112,000 pg/mL). The median value of endotoxins in the pres-ence of pain on palpation was 5,580 pg/mL (range, 27-269,000 pg/mL), and in its absence it was 35.200 pg/mL (range, 59-289,000 pg/mL). Moreover, in the presence of tenderness to percussion, themedian value was 3,480 pg/mL (range, 27-289,000 pg/mL), and inthe absence of tenderness to percussion, it was 9190 pg/mL (range,59-232,000 pg/mL). Table 3 shows the median concentration of
JOE — Volume 36, Number 9, September 2010

TABLE2.
PCR
Det
ectio
nof
Bac
teri
aSp
ecie
sin
21R
oot
Cana
lsw
ithPr
imar
yR
oot
Cana
lIn
fect
ion
and
Apic
alPe
riod
ontit
is
Targ
etb
acte
ria
ATC
CS1
S2S3
S4S5
S6S7
S8S9
S10
S11
S12
S13
S14
S15
S16
S17
S18
S19
S20
S21
Un
ivers
al(1
6rD
NA
)+
++
++
++
++
++
++
++
++
++
++
Dia
list
er
pn
eu
mo
sin
tes
++
Pre
vote
lla
inte
rmed
ia+
+Pre
vote
lla
nig
resc
en
s+
++
++
++
++
++
++
+A
gg
reg
ati
bact
er
act
ino
myc
ete
com
itan
s+
Po
rph
yro
mo
nas
gin
giv
ali
s+
Fili
fact
or
alo
cis
++
+Ta
nn
ere
lla
fors
yth
ia+
Pre
vote
lla
tan
nera
e+
Trep
on
em
ad
en
tico
la+
++
+Po
rph
yro
mo
nas
en
do
do
nta
lis
++
++
++
+
Trep
on
em
aso
cran
skii
++
++
++
+Parv
imo
nas
mic
ra+
++
++
+
S,sa
mpl
es;
+,
posi
tive
dete
ctio
n.
Clinical Research
JOE — Volume 36, Number 9, September 2010 Antig
enic Acendotoxin according to the clinical findings and the size of the radiolu-cent area. A correlation was found between endotoxin contents and thelevels of TNF-a released in the culture media (p < 0.05, Pearson r =0.740) (Fig. 1C).
Cell Culture and Cytokine ExpressionIL-1b and TNF-a Messenger RNA Expression. The macro-phage cell viability after 24 hours of root canal contents stimulationwas confirmed in the present study tested by its capacity to expressIL-1b and TNF-a messenger RNA.
Measurements of IL-1b and TNF-a Levels. IL-1b and TNF-a were detected in all culture media after stimulation with root canalcontents. The median level of IL-1b (24.835 pg/mL) was present inalmost 90-fold higher than TNF-a (0.2830 pg/mL). A higher medianlevel of IL-1b was detected when one of the following clinical symp-toms/radiographic findings was present: pain on palpation (25.528pg/mL), tenderness to percussion (25.528 pg/mL), or size of the radio-lucent area $2 mm (25.291 pg/mL) was present (Table 3). A higherlevel of TNF-a was found in teeth with exudation (0.2870 pg/mL) thanin its absence (0.2340 pg/mL). A correlation between the levels of IL-1breleased on the culture media and the size of radiolucent area was foundin this study (p < 0.05, Pearson r = 0.028) (Fig. 1D). The medianconcentration of endotoxin, IL-1b, and TNF-a according to clinicalfindings and the size of radiolucent area is shown in Table 3.
DiscussionData obtained in the present study revealed that a wide variety of
gram-negative bacterial species do play a role in primary root canalinfection with apical periodontitis, detecting at least 1 of 11 gram-negative target bacterial species in 18 of 21 root canals investigated,with a predominance of P. nigrescens, P. endodontalis, and T. socra-nskii.
The high frequency of P. nigrescens in primary endodontic infec-tion with apical periodontitis seems to be related to its LPS potential incausing bone resorption (24). The almost exclusive presence of P. en-dodontalis in endodontic infections suggests a specific association withbone resorption and activation of macrophages cells (5, 25). Moreover,P. endodontalis LPS has been detected in a very high percentage insevere endodontic infection (26).
The combination of two or more gram-negative bacterial speciesfound in 8 of 21 root canals investigated indicates that different bacterialLPS with different toxicity structure (lipid A) (27) can be involved in theroot canal infection, enhancing or even inhibiting each other’s antige-nicity activity over periradicular tissues. For instance, P. endodontalisseems to enhance the Fusobacterium nucleatum LPS toxicity (5),whereas Porphyromonas (27) and Bacteroides fragilis (28) arelimited in the presence of Escherichia coli LPS.
The association of Parvimonas micra (gram-positive bacteria)with at least 1 gram-negative target bacteria (eg, F. alocis) found inthe present study turns endodontic contents even more complex andimmunogenic to the immune system. Peptidoglycan (PGN), which ispresent in a significant amount in the gram-positive bacterial cells, playsa synergistic effect on LPS antigenic activity when they activate TLR-2 and-4, respectively (29). In this case, more macrophages differentiate intoosteoclast-like cells through the Receptor Activator for Nuclear Factor kB Ligand (RANKL):Osteoprotegerin (OPG) ratio increase (29). Yosh-ioka et al (30) reported that LPS can bind to P. micra cells conferringto this gram-positive bacteria the capacity to induce a strong TNF-a response in macrophage-like cells. Such critical finding stressesthe importance of considering gram-positive non-LPS components
tivity of Bacteria from Primary Root Canal Infection with Periapical Lesions 1471

Figure 1. The correlation between the number of gram-negative species, endotoxins, and the size of the radiolucent area (mm) and the levels of cytokines. (A) Thecorrelation between the number of gram-negative bacteria (n) and the levels of IL-1b detected in the macrophage supernatant (pg/mL). (B) The correlationbetween the number of gram-negative bacteria (n) and the levels of TNF-a detected in the macrophage supernatant (pg/mL). (C) The correlation between theendotoxin concentration (pg/mL) and the levels of TNF-a detected in the macrophage supernatant (pg/mL). (D) The correlation between the size of the radio-graphic area (mm) and the levels of IL-1b in the macrophage supernatant (pg/mL).
Clinical Research
when interpreting findings on the expression of proinflammatory cyto-kines.
Previous in vitro investigations have attempted to extract LPS inorder to determine the antigenic activity of the endodontic contents(5–7). However, the clinical significance of these investigations isunclear considering the complexity of the antigens involved inendodontic infection described earlier. Moreover, in vitro models,using bacterial growth culture media, fail in reproducing the infectionenvironment, particularly regarding the hemin concentration in theinfection site (31). Hemin concentration (in the hemoglobin form)varies considerably depending on the inflammatory response and bloodvessels integrity, and it might modulate the lipid A structure in the LPSmolecule, which is responsible for the majority of IL-1 induction (27).
To address these points, the present study stimulated macrophagecells with material individually isolated from 21 infected root canalspresenting primary endodontic infection and apical periodontitis,concomitantly investigating the microbiota and the endotoxin contentof each infected root canal. The analysis revealed that the increase inthe number of gram-negative bacteria was significantly followed by anincrease in the IL-1b and TNF-a levels. These findings suggest thatthe presence of clinical signs/symptoms such as bone destructioninvolved in apical periodontitis evoked by the immune system inresponse to LPS is not only associated with the amount of endotoxinelucidated by previous clinical investigations (12, 14–15) but alsowith the presence of a different number and heterogeneity of gram-negative bacteria, which acting synergistically can lead to a strongerimmune response in periapical tissues.
1472 Martinho et al.
P. nigrescens contains a very potent LPS molecule for prosta-glandin E2 stimulation (24) in inflamed pulp tissue (32) and in acutelyinflamed periapical tissue (17). Additionally, IL-1b and TNF-a releasedfrom macrophages supernatants treated with infectious materialderived from teeth with exudation are potent stimuli for prostaglandinE2 release (33). Our results agree with Ataoglu et al (22) who reportedno association between teeth with exudates and higher levels of IL-1band are inconsistent with Kuo et al (23). Furthermore, higher signifi-cantly levels of endotoxin were found in root canal exudation in thiscurrent study corroborating with previous clinical investigations(6, 12, 16).
Even though higher levels of endotoxins were expected particu-larly in pain on palpation and tenderness to percussion, it was not foundin the present study. These particular data might be explained by thecharacteristics of the samples investigated in which a greater numberof cases in the absence of these clinical features were found, contrib-uting to such findings.
Teeth with a larger size of periradicular lesions ($2 mm) wererelated to the detection of T. denticola in the root canal positively asso-ciated with P. endodontalis exhibiting a potent biological activity in cellculture (5) and with chronic bone resorption (29). Higher levels ofendotoxin were found in those teeth, which is in agreement with Scheinand Schilder (16) who reported that the endotoxin contents of teethwith radiolucent area were five times greater than in teeth withoutsuch area.
The larger size of periradicular lesions ($2 mm) was also corre-lated with higher levels of IL-1b in accordance to Tani-Ishii et al (34).
JOE — Volume 36, Number 9, September 2010

TABLE3.
The
Med
ian
Conc
entr
atio
nof
Endo
toxi
n,IL
-1ß
,an
dTN
F-a
inpg
/mL
Acco
rdin
gto
the
Clin
ical
Find
ings
and
Size
ofth
eR
adio
luce
ntAr
ea
Tota
lA
mo
un
tPai
no
np
alp
atio
nTe
nd
ernes
sto
per
cuss
ion
Exud
atio
nSi
zeo
fra
dio
luce
nt
area
n=
21
Pre
sen
tn
=9
Ab
sen
tn
=1
2P
rese
nt
n=
8A
bse
nt
n=
13
Pre
sen
tn
=1
2A
bse
nt
n=
9$
2m
mn
=1
1<
2m
mn
=1
0
En
do
toxi
n(p
g/
mL)
7,4
90
5,5
80
35,2
00
3,4
80
9,1
90
9,1
90
2,6
20
9,1
90
3,4
80
IL-1
ß(p
g/m
L)24.8
35
25.5
28
24.8
35
25.5
28
24.8
35
24.8
35
25.2
91
25.2
91*
15.0
07*
TN
F-a
(pg
/mL)
0.2
830
0.2
605
0.3
150
0.2
340
0.2
870
0.2
870
0.2
340
0.2
575
0.2
870
*Sta
tistic
ally
sign
ifica
ntdi
ffere
nce
(p<
0.05
).
Clinical Research
JOE — Volume 36, Number 9, September 2010 Antigenic Ac
This finding might be related to the PGN present in gram-positive and-negative bacteria, which inhibits the differentiation of monocytes/macrophages into mature cells. Besides this inhibition, PGN promotescytokine production by undifferentiated precursors (29), consequentlyincreasing localized osteolysis particularly at sites with larger number ofmacrophages (35).
More studies that analyze the mechanisms involved in the produc-tion of cytokines and bone resorption are important for the develop-ment of new therapies. The interference in toll-like receptors andinterleukin-1 receptor downstream signaling pathways should beconsidered to control the development and progression of endodonticlesions. In the future, the use of the RNA interference can reduce thedifferentiation of macrophages into osteoclasts; the induction of cyto-solic phospholipase-A (cPLA) and beta-defensin2; and, consequently,the release of TNF-a, IL-1b, and IL-6 (36–38). Another strategy is thesuperexpression of specific regulator proteins such as SOCS3,interferon-gamma, and interleukin-10 through local delivery of DNAvectors (39).
Overall, the present study suggested that the antigenicity of theendodontic contents against macrophages (IL-a and IL-1b release)is not only associated with the amount of endotoxin but also with thenumber of gram-negative bacteria involved in the infection. Furtherinvestigations should be performed in order to assess the effect of anti-microbial agents over different lipid A structures isolated from speciescommonly found in endodontic infections and their mechanism ofaction in different cell types.
AcknowledgmentsThe authors thank Ana Regina de Oliveira Polay, Fernanda
Barrichello Tosello, Thais Mageste Duque, Geovania CaldasAlmeida, and Juliana Melo da Silva for technical support. We arealso thankful to Cambrex for the Kinetic-QCL equipment.
References1. Fabricius L, Dahlen G, Holm SE, et al. Influence of combinations of oral bacteria on
periapical tissues of monkeys. Scand J Dent Res 1982;90:200–6.2. Nair PNR. Pathogenesis of apical periodontitis and the causes of endodontic failures.
Crit Rev Oral Biol Med 2004;15:348–81.3. Lim GC, Torabinejad M, Kettering J, et al. Interleukin 1 b in symptomatic and asymp-
tomatic human perirradicular lesions. J Endod 1994;20:225–7.4. Rietschel ET, Brade H. Bacterial endotoxins. Sci Am 1992;267:54–61.5. Hong CY, Lin SK, Kok SH, et al. The role of lipopolysaccharide in infectious bone
resorption of periapical lesion. J Oral Pathol Med 2004;33:162–9.6. Horiba N, Maekawa Y, Abe Y, et al. Cytotoxicity against various cell lines of lipopoly-
saccharides purified from bacteroides, fusobacterium, and veillonella isolated frominfected root canals. J Endod 1989;15:530–4.
7. Hosoya S, Matsushima K. Stimulation of interleukin-1 beta production of humandental pulp cells by Porphyromonas endodontalis lipopolysaccharide. J Endod1997;23:39–42.
8. Matsuo T, Ebisu S, Shimabukuro Y, et al. Quantitative analysis of immunocompetentcells in human periapical lesions: correlations with clinical findings of the involvedteeth. J Endod 1992;18:497–500.
9. Artese L, Piattelli A, Quaranta M, et al. Immunoreactivity for interleukin 1-beta andtumor necrosis factor-alpha and ultrastructural features of monocytes/macrophagesin periapical granulomas. J Endod 1991;17:483–7.
10. Stashenko P, Dewhirst FE, Rooney ML, et al. Interleukin-1 beta is a potent inhibitorof bone formation in vitro. J Bone Miner Res 1987;2:559–65.
11. Beutler B, Cerami A. Cachectin and tumour necrosis factor as two sides of the samebiological coin. Nature 1986;320:584–8.
12. Jacinto RC, Gomes BPFA, Shah HN, et al. Quantification of endotoxins in necrotic rootcanals from symptomatic and asymptomatic teeth. J Med Microbiol 2005;54:777–83.
13. Vianna ME, Hortz HP, Conrads G, et al. Effect of root canal procedures on endo-toxins and endodontic pathogens. Oral Microbiol Immunol 2007;22:1–8.
14. Martinho FC, Gomes BP. Quantification of endotoxins and cultivable bacteria in rootcanal infection before and after chemomechanical preparation with 2.5% sodiumhypochlorite. J Endod 2008;34:268–72.
tivity of Bacteria from Primary Root Canal Infection with Periapical Lesions 1473

Clinical Research
15. Gomes BP, Martinho FC, Vianna ME. Comparison of 2.5% sodium hypochlorite and2% chlorhexidine gel on oral bacterial lipopolysaccharide reduction from primarilyinfected root canals. J Endod 2009;35:1350–3.
16. Schein B, Schilder H. Endotoxin content in endodontically involved teeth. J Endod1975;1:19–21.
17. McNicholas S, Torabinejad M, Blankenship J, et al. The concentration of prosta-glandin E2 in human periradicular lesions. J Endod 1991;17:97–100.
18. Shimauchi H, Takayama S, Miki Y, et al. The change of periapical exudate prosta-glandin E2 levels during root canal treatment. J Endod 1997;23:755–8.
19. Barkhordar RA, Hussain MZ, Hayashi C. Detection of interleukin-1 beta in humanperiapical lesions. Oral Surg Oral Med Oral Pathol 1992;73:334–6.
20. Safavi KE, Rossomando EF. Tumor necrosis factor identified in periapical tissueexudates of teeth with apical periodontitis. J Endod 1991;17:12–4.
21. Matsuo T, Ebisu S, Nakanishi T, et al. Interleukin-1 alpha and interleukin-1 betaperiapical exudates of infected root canals: correlations with the clinical findingsof the involved teeth. J Endod 1994;20:432–5.
22. Ataoglu T, Ungor M, Serpek B, et al. Interleukin-1beta and tumour necrosis factor-alpha levels in periapical exudates. Int Endod J 2002;35:181–5.
23. Kuo ML, Lamster IB, Hasselgren G. Host mediators in endodontic exudates. I. Indi-cators of inflammation and humoral immunity. J Endod 1998;24:598–603.
24. Chung YH, Chang EJ, Kim SJ, et al. Lipopolysaccharide from Prevotella nigrescensstimulates osteoclastogenesis in cocultures of bone marrow mononuclear cells andprimary osteoblasts. J Periodontal Res 2006;41:288–96.
25. van Winkelhoff AJ, van Steenbergen TJ, de Graaff J. Porphyromonas (Bacteroides)endodontalis: its role in endodontal infections. J Endod 1992;18:431–4.
26. Hanazawa S, Sagiya T, Kitami H, et al. Monoclonal antibody against Porphyromonas(Bacteroides) endodontalis lipopolysaccharide and application of the antibody fordirect identification of the species. J Clin Microbiol 1991;29:2550–3.
27. Dixon DR, Darveau RP. Lipopolysaccharide heterogeneity: innate host responses tobacterial modification of lipid a structure. J Dent Res 2005;84:584–95.
28. Magnuson DK, Weintraub A, Pohlman TH, et al. Human endothelial cell adhesive-ness for neutrophils, induced by Escherichia coli lipopolysaccharide in vitro, is in-hibited by Bacteroides fragilis lipopolysaccharide. J Immunol 1989;143:3025–30.
1474 Martinho et al.
29. Jiang J, Zuo J, Hurst IR, et al. The synergistic effect of peptidoglycan and lipopoly-saccaride on osteoclast formation. Oral Surg Oral Med Oral Pathol Oral Radiol En-dod 2003;96:738–43.
30. Yoshioka M, Grenier D, Mayrand D. Binding of Actinobacillus actinomycetemco-mitans lipopolysaccharides to Peptostreptococcus micros stimulates tumornecrosis factor alpha production by macrophage-like cells. Oral Microbiol Immu-nol 2005;20:118–21.
31. Al-Qutub MN, Braham PH, Karimi-Naser LM, et al. Hemin-dependent modulation ofthe lipid A structure of Porphyromonas gingivalis lypopolysacaccharide. Infect Im-mun 2006;74:4474–85.
32. Cohen JS, Reader A, Fertel R, et al. A radioimmunoassay determination of theconcentrations of prostaglandins E2 and F2 alpha in painful and asymptomatichuman dental pulps. J Endod 1985;11:330–5.
33. Richards D, Rutherford RB. The effects of interleukin 1 on collagenolytic activity andprostaglandin-E secretion by human periodontal-ligament and gingival fibroblast.Arch Oral Biol 1988;33:237–43.
34. Tani-Ishii N, Wang CY, Stashenko P. Immunolocalization of bone-resorptive cyto-kines in rat pulp and periapical lesions following surgical pulp exposure. Oral Mi-crobiol Immunol 1995;10:213–9.
35. Gowen M, Wood DD, Ihrie EJ, et al. An interleukin 1 like factor stimulates boneresorption in vitro. Nature 1983;306:378–80.
36. Fahid FS, Jiang J, Zhu Q, et al. Application of small interfering RNA for inhibition oflipopolysaccharide-induced osteoclast formation and cytokine stimulation. J Endod2008;34:563–9.
37. Fukushima A, Kajiya H, Izumi T, et al. Pro-inflammatory cytokines inducesuppressor of cytokine signaling-3 in human periodontal ligament cells. J Endod2010;36:1004–8.
38. Kim YS, Min KS, Lee HD, et al. Effect of cytosolic phospholipase A(2) on proinflam-matory cytokine-induced bone resorptive genes including receptor activator ofnuclear factor kappa B ligand in human dental pulp cells. J Endod 2010;36:636–41.
39. Kim YS, Min KS, Lee SI, et al. Effect of proinflammatory cytokines on the expressionand regulation of human beta-defensin 2 in human dental pulp cells. J Endod 2010;36:64–9.
JOE — Volume 36, Number 9, September 2010

Clinical Research
Molecular Fingerprinting Reveals the Presence of UniqueCommunities Associated with Paired Samples of Root Canalsand Acute Apical AbscessesFrancisco Montagner, DDS, MSc, PhD,* Brenda P.F.A. Gomes, DDS, MSc, PhD,*
and Purnima S. Kumar, DDS, PhD†
Abstract
Introduction: Acute primary endodontic infections arepolymicrobial infections that affect both the root canal(RC) system and apical tissues. It is known that thesecommunities cannot be detected by conventionalculturing methods. The aim of this study was to examinethe profile of microbial communities in necrotic RCs andacute apical abscesses (AAAs) using an open-endedmolecular approach to compare the diversity andcomposition of the microbiota of these two communi-ties. Methods: Paired samples of RC and PA exudateswere collected from 20 subjects and analyzed byterminal restriction fragment length polymorphism (t-RFLP). The number of peaks, the peak areas, and thecommunity diversity were compared between RCs andPAs. The similarity of the microbial profile of each pairof RCs and PAs was assessed by computing the numberof shared peaks and the Bray-Curtis Similarity Index.Results: A total of 103 and 75.5 unique fragments (t-RFs) were detected in RC and PA samples, respectively.RCs and PAs were not different in the number of speciesor in the community diversity; however, very few specieswere shared between RC and PA samples. No single t-RFfragment was detected in all samples, and the majoritywas detected in only one sample. Low diversity ofspecies was observed in the RCs of smokers. Subjectswith previous pain showed fewer species and greatercommunity diversity. Conclusion: The microbial profilesof the RC and PA communities are distinct and divergedbetween all subjects, suggesting that acute endodonticinfections are microbiologically heterogeneous. (J Endod2010;36:1475–1479)Key WordsAcute endodontic infections, acute apical abscess,community, terminal restriction fragment length poly-morphism
From the *Endodontic Division, Piracicaba Dental School, StateDentistry, The Ohio State University, Columbus, OH, USA
Supported by a seed grant from the College of Dentistry, The Oh56425-1, 2008/06162-4; 2008/57551-0) and CNPq (305437/2006-2
Address requests for reprints to Dr Brenda P.F.A. Gomes, PiracPiracicaba, Sao Paulo, Brasil CEP 13414-903. E-mail address: bpgom0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.004
JOE — Volume 36, Number 9, September 2010 Un
Acute apical abscesses (AAAs) are one of the most frequently treated conditions inendodontic emergency procedures (1). Clinically, they are characterized by spon-
taneous pain, tenderness to percussion, and pain on palpation (2). The presence ofsoft-tissue swelling indicates diffusion through bone and may result in life-threatening conditions if immediate treatment is not provided (3).
Evidence indicates that the acute primary endodontic diseases are polymicrobialinfections, predominantly involving strictly anaerobic, gram-negative cocci, and gram-negative rods, along with facultative streptococci (4, 5). At least 40% of the speciesremain as-yet-cultivated (6).
Several methods have been used to characterize microbial communities associ-ated with endodontic infections. In the recent years, the advent of detection methodsbased on DNA fingerprints within the 16S ribosomal RNA (rRNA) gene has revealedan unexpected diversity of microbial species (7). Data collected from cultivation-based and culture-independent molecular studies have shown that 486 unique bacteria,one archaeal, and 9 fungal taxa are associated with pulpal and periradicular infections(8). The diversity of acute endodontic infections has been assessed by direct DNA-DNAhybridization (9) and polymerase chain reaction (PCR)-based techniques (eg, reverse-capture checkerboard hybridization [10], denaturing gradient gel electrophoresis[11], terminal restriction fragment length polymorphism [12], and 16S cloning andsequencing [13–15]).
Terminal restriction fragment length polymorphism (t-RFLP) is an open-endedmolecular approach that provides information on the structure and profile of microbialcommunities (16). This technique is based on PCR amplification of a unique region ofthe genome with fluorescent-labeled broad-range primers followed by a restrictionenzyme digestion that generates different fragment lengths, each fragment representinga unique species (17). It has been used as a rapid, high-throughput tool to analyzecomplex microbial communities with several as-yet-uncultivable members becausechanges in microbial community structure can be monitored by the presence, absence,and quantity of specific fragments or peaks (16, 18, 19).
Even though many studies have investigated the microbial community in root canalinfection (4) and in acute periapical abscess (5), none of them has studied their simi-larity in the same patient. Therefore, the aim of this study was to examine the profile ofmicrobial communities in necrotic root canals (RCs) and acute apical abscesses (AAAs)from the same patient using t-RFLP of the 16S rRNA gene to compare the diversity andcomposition of the microbiota of these two communities.
University of Campinas, Piracicaba, Sao Paulo, Brazil; and †Division of Periodontology, College of
io State University to Dr Purnima Kumar and the Brazilian Agencies FAPESP (2007/58518-4, 2008/, 470820/2006-3, 471631/2008-6; 302575/2009-0).icaba Dental School, University of Campinas, Endodontic Division, Av Limeira 901, Bairro Areiao,
ique Communities Associated with Paired Samples of Root Canals and Acute Apical Abscesses 1475

Figure 1. The number of species in 20 pairs of RC and AAA samples. Pairs ofsamples are connected by matching lines.
Figure 2. The diversity index in RC and AAA samples. Pairs of samples areconnected by matching lines.
Clinical Research
Materials and MethodsPatient Selection and Clinical Features
The present study was approved by the Ethics Committee inResearch of Piracicaba Dental School (State University of Campinas, Pi-racicaba, Sao Paulo, Brazil), and informed consent was obtained fromall subjects. Twenty patients presenting to the emergency clinic withpulp necrosis, determined by the vitality tests; acute apical abscesses(2); and soft-tissue swelling participated in the study. Subjects withsystemic disease and those who had used antibiotics in the last 3 monthswere excluded from the study. The impossibility of tooth isolation, thepresence of dental caries or coronal destruction that allowed thecommunication between the root canal and the oral cavity, previousendodontic manipulation, poor access to the apical region for sampling(as determined by previous radiographic examination), or the presenceof marginal periodontitis were also exclusion factors. Demographic andclinical information was collected.
Sample Collection From RCsAll clinical procedures were performed under local anesthesia with
2% lidocaine and epinephrine (1:100,000) as described previously byGomes et al (20). Briefly, all dental caries and restorations wereremoved without pulp exposure. The tooth was individually isolatedfrom the oral cavity with a previously disinfected rubber dam. Disinfec-tion of the rubber dam and tooth was performed using 30% hydrogenperoxide and then 2.5% sodium hypochlorite. The solution was inacti-vated with 5% sodium thiosulfate in order to avoid interference with thesampling procedure. The pulp chambers were exposed using sterile dia-mond burs under manual irrigation with sterile saline. Root canals wereclassified as wet or dry based on the presence of exudate. Samples werecollected by inserting sterile paper points to the radiographic workinglength. All samples were immediately transferred to 1 mL of ViabilityMedium Goteborg Agar III transport medium. In multirooted teeth,the largest canal or the one with periapical radiolucency was chosen.
Sample Collection From AAAsAAA samples were collected following sampling from RCs. After
disinfection with 2% chlorhexidine gel, samples were taken intraorallythrough intact mucosa by aspiration with a sterile and disposable 5-mLplastic syringe with a 21-G needle before surgical drainage as describedby Rocas et al (5) and Riggio et al (15). Exudates were classified asbloody or purulent. One hundred microliters of the exudate was imme-diately placed into a test tube containing 900 mL of Viability MediumGoteborg Agar III. All samples were frozen at �20�C until analysis.
DNA IsolationThree hundred fifty microliters of the transport medium was used
to isolate DNA with a Qiagen DNA MiniAmp Kit (Qiagen, Valencia, CA)using the tissue protocol according to the manufacturer’s instruction.The DNA was eluted in 100 mL of TrisHCl + EDTA.
t-RFLP Analysist-RFPL analysis was performed as described previously by Fullmer
et al (19). Bacterial 16S rRNA genes were amplified by polymerasechain reaction (PCR) with fluorescent-labeled broad-range bacterialprimers A18 (5’-TTTGATCCTGGCTCAG-HEX-3’) and 317 (5’-FAM-AAG-GAGGTGATCCAGGC-3’) (Applied Biosystems, Foster City, CA). PCR wasperformed by adding 4 mL of community DNA to a reaction mixture(50-mL final volume), containing 20 nmol of each primer, 40 nmolof deoxynucleotide triphosphates, and 1U of Taq polymerase. Thecycling conditions used were 22 cycles of denaturation at 94�C for 1
1476 Montagner et al.
minute, annealing at 42�C for 2 minutes, and elongation at 72�C for3 minutes followed by a final 10-minute elongation at 72�C. The ampli-cons were purified with the use of a Qiaquick Kit (Qiagen).
A 10-mL aliquot of purified PCR product was digested with 20 U ofeither HhaI or MspI enzymes in a total volume of 20 mL at 37�C for 3hours. Ten microliters of the restriction digestion product was purifiedby AMPure beads (Agencourt Bioscience Corporation, Beverly, MA) ac-cording to the manufacturer’s protocol. Five microliters of the purifiedproduct was denatured with 10 mL of deionized formamide and mixedwith 0.2 mL of GeneScan 1200 LIZ size standard (Applied Biosystems,Foster City, CA). Fragment lengths were determined on an Applied Bio-systems 3730 DNA Analyzer in GeneScan mode. The number of peaksand the height and area of each peak were determined with GeneMap-per 4.0 Software (Applied Biosystems, Foster City, CA). All reactionswere replicated.
JOE — Volume 36, Number 9, September 2010

Figure 3. The distribution of number of species and diversity index in RC and AAA samples, considering smoking status, previous pain, and RC or AAA exudatesduring sampling. A and B represent RC samples, whereas C and D are AAA samples (*p < 0.05).
Clinical Research
Data AnalysisFragments with a peak height less than 50 fluorescence units were
excluded from analysis. Peak areas were standardized by converting theraw values to a proportion of the total area, as previously described(21). Peaks representing less than 1% of the total area were assigneda value of zero, and the percentages of the remaining peaks were recal-culated. Peak areas and the number of peaks generated by each enzymewere averaged for the two fluorophores. The mean number of peaksand the peak areas were used to compute the Shannon-Wiener DiversityIndex. The similarity of the microbial profile of each pair of RCs andAAAs was assessed by computing the number of shared peaks andthe Bray-Curtis Similarity Index. EstimateS 8.2.0 (University of Connect-icut, Storrs, CT) was used to perform the analysis. The Bray-Curtis Simi-larity Index is a quantitative comparative measure that uses the numberof shared species and the levels of each species in both communities.This index is weighted for levels of rare and abundant species, whicha simple percentage similarity will not achieve.
Statistical analysis was performed with JMP (SAS Institute Inc.,Cary, NC). The Wilcoxon matched pair signed rank test was used tocompare total peaks and community diversity between pairs of RCand PA samples. The Wilcoxon matched pair signed rank test wasused to compare shared species and the Bray-Curtis index to comparesamples from RCs and PAs.
ResultsThe mean age of the subjects was 30.5 years (range, 19-54 years).
Seventy-five percent of the subjects were female, and 25% were currentsmokers. All subjects reported a history of spontaneous pain; however,no other systemic signs (eg, pyrexia, malaise, and chills) were
JOE — Volume 36, Number 9, September 2010 Unique Communities
observed. Nine of 20 subjects reported the presence of pain in theinvolved tooth followed by spontaneous remission of the symptomsbefore the dental visit and were categorized as ‘‘previous pain.’’ RCsof 9 incisors, 2 canines, 4 premolars, and 5 molars were sampled. Teethwere caries free (3/20), had caries (7/20), or had restorations (10/20). Gingivitis was associated with 9 of 20 teeth. Seventy percent ofthe teeth had mobility because of the presence of AAA. Radiographicexamination showed widening of the apical periodontal ligament space(6/20) or apical radiolucency (14/20). During sampling, 13 teeth pre-sented wet root canals, and 7 were dry; 11 of these showed purulentexudate, and two teeth had bloody exudate. Nine teeth had bloodyexudate in the AAA.
The number of unique terminal-restriction fragments (t-RFs), rep-resenting the number of individual species, differed between the twofluorescent labels. One hundred eleven FAM-labeled fragments and95 HEX-labeled fragments were generated in RC samples, whereas 84and 67 fragments were generated in AAA samples. These differenceswere not statistically different (Wilcoxon matched pair signed ranktest, p > 0.05). No unique t-RF was ubiquitously found in all samples.One HEX-labeled fragment of 274 bp was detected in 17 of 20 RCsamples and 18 of 20 AAA samples. The majority of the t-RFs was presentin only one sample (RC = 49.7%, AAA = 34.4%).
The number of unique species in each pair of RCs and AAAs isshown in Figure 1. Paired samples are connected by lines. The meannumber of t-RFs was 13.55 (�6.49 standard deviation) in RC and12.68 (�7.79 standard deviation) in AAA samples. There was no statis-tically significant difference between the samples (Wilcoxon matchedpair signed rank test, p = 0.7017).
The diversity of the bacterial communities in RCs and AAAs isshown in Figure 2. Paired samples are connected by lines. The mean
Associated with Paired Samples of Root Canals and Acute Apical Abscesses 1477

Figure 4. The mean number of shared species and the Bray-Curtis Commu-nity Similarity Index in paired samples (*p < 0.05).
Clinical Research
diversity index was 2.647 (�0.506) in the RC sample and 2.650(�0.675) in the AAA sample. There was no statistically significantdifference between the two environments (Wilcoxon matched pairsigned rank test, p = 0.9841).
Figure 3 shows the distribution of number of species and theShannon-Wiener Diversity Index in RCs and AAAs by clinical presenta-tion. RC samples are shown in Figure 3A and B, whereas acute apicalabscess samples are shown in Figure 3C and D. A greater number ofspecies was observed in root canal samples from patients who reportedprevious pain (p = 0.0156). However, these subjects showed lowspecies diversity (p = 0.0190).
The distribution of species shared by each pair of RCs and AAAsand the Bray-Curtis Community Similarity Index between each pair ofRC and AAA communities is shown in Figure 4. Current smokers showedmore similar community profiles in RC and AAA samples than neversmokers (p = 0.048).
DiscussionAlthough it is known that RCs and AAAs are polymicrobial infec-
tions with several uncultivated organisms, there is little evidence onthe microbial profile of RCs and AAA infections in paired samples. Usingan open-ended molecular approach allowed comparisons to be madeof these largely uncultivated microbiomes.
t-RFLP is an open-ended molecular technique that enumeratescultivable, difficult-to-grow and as-yet-uncultivated bacterial taxa, al-lowing comparisons to be made of complex polymicrobial communi-
1478 Montagner et al.
ties. It has been used to examine the microbial diversity in rootcanals with symptomatic/asymptomatic primary infections (6, 12,22). This technique is based on the size and fluorescence of theterminal fragment that is generated after digestion with a restrictionenzyme (16). Each unique species is represented by a different frag-ment length. The same species might have different fragment profilesdepending on the primer set and also on the restriction enzyme thatdigested the PCR product (23). Schutte et al (18) described thatboth in silico or in vitro analysis can predict the fragment length asso-ciated with a specific microbial species. These data were not presentedin the study because individual species profiles have not been deter-mined yet for the A18 and 317 amplicons when digested by MspI orHhaI. Furthermore, the aim of this study was to depict the profile ofmicrobial communities in acute endodontic infections in pairedsamples of RCs and AAAs from the same patient, presenting their diver-sity, without attempting to the description of the individual speciescomposing the consortia.
RCs harbored an average of 103 t-RFs. This is in agreement withprevious reports using t-RFLP analysis to examine root canals of symp-tomatic teeth (6, 12). However, the number of t-RFs from AAAs in thepresent study was significantly greater than that previously reportedusing 16S rRNA sequencing (15, 24). In the present study, several t-RFs were detected once or twice in each sample, indicating that thesespecies are of low abundance. Therefore, it is possible that thesespecies would have been below the detection threshold of 16Scloning and sequencing.
The distribution of species appears to be unique for RC and AAAsamples in each subject because no single t-RF fragment was detected inall samples, and the majority was detected in only one sample. This isconsistent with previous studies on acute endodontic infections that re-vealed different bacterial profiles among samples (11-14), with thegreat majority of the taxa detected in only one sample. The datasuggested that different microbial communities may form theetiologic basis of a single disease (12, 25). Further studies must beundertaken to determine the levels of individual species in RC andperiradicular infections and their relative importance in the balanceof each community.
It has been shown that different species may have similar fragmentlengths, which could underestimate the number of closely relatedspecies (18). The use of two fluorescent primers and more than onerestriction enzyme can reduce these limitations (25). In the presentstudy, the PCR product was digested with HhaI and MspI enzymes,and two fluorophores were used for each enzyme (19). The datawere averaged over the two fluorophores in an effort to limit the under-estimation of community diversity. More fragments were generated bydigestion with MspI when compared with HhaI. Because averagingdata from HhaI and MspI resulted in an underestimation of the numberof species and the community diversity, only results from MspI digestionwere used in statistical analysis.
The mean number of species and the diversity index were notdifferent between the RC and AAA samples; however, very few specieswere shared between RC and AAA samples. This suggests that thesetwo communities are compositionally different. One reason might bethe limitations in the current sampling methods, especially for RC.The sampling procedures for RCs are restricted to bacteria in the plank-tonic state suspended in the main RC or attached to the dentin walls.Alves et al (26) suggested a protocol in which a DNA was extractedfrom root powder samples. However, this method can only be appliedto extracted teeth. It is known that low-abundant members inside dentintubules or RC irregularities may contribute to the community balance(27). However, they might be found at higher counts at the apicaltissues, favoring their detection by molecular methods. Selective
JOE — Volume 36, Number 9, September 2010

Clinical Research
pressures related to nutrition may also influence the microbial compo-sition of both sites (28). Furthermore, although bacteria colonizingroot canals are protected, bacteria invading the periradicular tissuesare under direct influence of host defense mechanisms (6, 8, 10).Our results indicate that the presence of different microbialcommunities in paired RC and AAA infections that may participate inthe same disease.Previous studies observed different microbial communities insamples from different geographic locations (5) and in samples fromresected root ends and apical chronic periodontitis (29). It has alsobeen shown that there is a variation in the species distribution in thecoronal and apical thirds of the root canal in the same patient (26).However, none of them have investigated the effect of local factorsover microbial species distribution in endodontics.
Smoking is considered an important risk factor for endodonticdisease. Krall et al (30) showed in a longitudinal analysis that smokerswere 1.7 times more likely to have RC treatment than nonsmokers. Inthe present study, low species diversity was observed in RC of smokers.The oral environment and supragingival dental plaque are the mainsources of bacteria in root canal infections (31). It has been shownthat the microbiological composition of the subgingival microflora insmokers is different from that of nonsmokers (32), with higher levelsof Parvimonas micra, Fusobacterium nucleatum, Campylobacterrectus, Porphyromonas gingivalis, Actinobacillus actinomycetem-comitans and Bacteroides forsythus (32, 33). It is possible thatsmoking exerts a similar effect by enriching pathogens in the RCenvironment. Smoking can decrease important leukocyte functionssuch as chemotaxis and phagocytosis (34) that could favor pulp andperiradicular tissue colonization. Further large-scale studies examiningthe microbial flora in RCs of smokers and nonsmokers are warranted.
Subjects with previous pain showed fewer species and greatercommunity diversity. Because the Shannon-Wiener Diversity Index isa measure of both number of species as well as the abundance ofeach species, the data suggest that subjects with previous pain hadgreater numbers of certain species. This is in agreement with previousreport by Gomes et al (35), indicating that asymptomatic RC infectionsin patients with previous pain harbored a more complex microbiota,with facultative and strict anaerobes.
In summary, the microbial profiles of the RC and AAA communitiesare distinct, except in smokers. Both communities exhibit the samenumber of species and similar diversity; however, subjects withprevious pain showed greater diversity in the RC system but not theAAA. The microbial profiles of the two communities diverged betweenall subjects, suggesting that acute endodontic infections are microbio-logically heterogeneous.
References1. Boykin MJ, Gilbert GH, Tilashalski KR, et al. Incidence of endodontic treatment:
a 48-month prospective study. J Endod 2003;29:806–9.2. Walton RE, Torabinejad M. Principles and Practice of Endodontics. 3rd ed. Phila-
delphia: Saunders; 2002.3. Flynn TR, Shanti RM, Levi MH, et al. Severe odontogenic infections, part 1: prospec-
tive report. J Oral Maxillofac Surg 2006;64:1093–103.4. De Sousa EL, Ferraz CC, Gomes BP, et al. Bacteriological study of root canals asso-
ciated with periapical abscesses. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2003;96:332–9.
5. Rocas IN, Baumgartner JC, Xia T, et al. Prevalence of selected bacterial namedspecies and uncultivated phylotypes in endodontic abscesses from two geographiclocations. J Endod 2006;32:1135–8.
6. Sakamoto M, Rocas IN, Siqueira JF Jr, et al. Molecular analysis of bacteria in asymp-tomatic and symptomatic endodontic infections. Oral Microbiol Immunol 2006;21:112–22.
JOE — Volume 36, Number 9, September 2010 Unique Communities
7. Siqueira JF Jr, Rocas IN. Exploiting molecular methods to explore endodontic infec-tions: part 1—current molecular technologies for microbiological diagnosis.J Endod 2005;31:411–23.
8. Siqueira JF Jr, Rocas IN. Diversity of endodontic microbiota revisited. J Dent Res2009;88:969–81.
9. Siqueira JF Jr, Rocas IN, Souto R, et al. Microbiological evaluation of acute perira-dicular abscesses by DNA-DNA hybridization. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2001;92:451–7.
10. Siqueira JF Jr, Rocas IN. The microbiota of acute apical abscesses. J Dent Res 2009;88:61–5.
11. Machado de Oliveira JC, Siqueira JF Jr, Rocas IN, et al. Bacterial community profilesof endodontic abscesses from Brazil and USA subjects as compared by denaturinggradient gel electrophoresis analysis. Oral Microbiol Immunol 2007;22:14–8.
12. Saito D, Marsh TL, de Souza Cannavan F, et al. Assessment of intraradicular bacterialcomposition by terminal restriction fragment length polymorphism analysis. OralMicrobiol Immunol 2009;24:369–76.
13. Munson MA, Pitt-Ford T, Chong B, et al. Molecular and cultural analysis of themicroflora associated with endodontic infections. J Dent Res 2002;81:761–6.
14. Jacinto RC, Gomes BP, Desai M, et al. Bacterial examintaion of endodontic infectionsby clonal analysis in concert with denaturing high-performance liquid chromatog-raphy. Oral Microbiol Immunol 2007;22:403–10.
15. Riggio MP, Aga H, Murray CA, et al. Identification of bacteria associated withspreading odontogenic infections by 16S rRNA gene sequencing. Oral Sur OralMed Oral Pathol Oral Radiol Endod 2007;103:610–7.
16. Marsh TL. Terminal restriction fragment length polymorphism (t-RFLP): anemerging method for characterizing diversity among homologous populations ofamplification products. Curr Opin Microbiol 1999;2:323–7.
17. Osborn AM, Moore ERB, Timmis KN. An evaluation of terminal-restriction fragmentlength polymorphism (t-RFLP) analysis for the study of microbial community struc-ture and dynamics. Environ Microbiol 2000;2:39–50.
18. Schutte UME, Abdo Z, Bent SJ, et al. Advances in the use of terminal restriction frag-ment length polymorphism (t-RFLP) analysis of 16S rRNA genes to characterizemicrobial communities. Appl Microbiol Biotechnol 2008;80:365–80.
19. Fullmer SC, Preshaw PM, Heasman PA, et al. Smoking cessation alters subgingivalmicrobial recolonization. J Dent Res 2009;88:524–8.
20. Gomes BP, Pinheiro ET, Gade-Neto CR, et al. Microbiological examination of in-fected dental root canals. Oral Microbiol Immunol 2004;19:71–6.
21. Rees GN, Baldwin SK, Watson GO, et al. Ordination and significance testing of micro-bial community composition derived from terminal restriction fragment length poly-morphisms: application of multivariate statistics. Antonie Van Leeuwenhoek 2004;86:339–47.
22. Hommez GMG, Verhelst R, Vaneechoutte M, et al. Terminal restriction fragmentlength polymorphism analysis of the microflora in necrotic teeth of patients irradi-ated in the head and neck region. J Endod 2008;34:1048–51.
23. Avaniss-Aghajani E, Jones K, Holtzman A, et al. Molecular technique for rapid iden-tification of mycobacteria. J Clin Microbiol 1996;34:98–102.
24. Dymock D, Weightman AJ, Scully C, et al. Molecular analysis of microflora associ-ated with dentoalveolar abcesses. J Clin Microbiol 1996;34:537–42.
25. Siqueira JF Jr, Rocas IN, Debelian GJ, et al. Profiling root canal bacterial commu-nities associated with chronic apical periodontitis from Brazilian and Norwegiansubjects. J Endod 2008;34:1457–61.
26. Alves FR, Siqueira JF Jr, Carmo FL, et al. Bacterial community profiling of cryogen-ically ground samples from the apical and coronal root segments of teeth with apicalperiodontitis. J Endod 2009;35:486–92.
27. Siqueira JF Jr, Rocas IN. Community as the unit of pathogenicity: an emergingconcept as to the microbial pathogenesis of apical periodontitis. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2009;107:870–8.
28. Grenier D, Mayrand D. Nutritional relationships between oral bacteria. Infect Im-mun 1986;53:616–20.
29. Subramanian K, Mickel AK. Molecular analysis of persistent periradicular lesionsand root ends reveals a diverse microbial profile. J Endod 2009;35:950–7.
30. Krall EA, Abreu Sosa C, Garcia C, et al. Cigarette smoking increases the risk of rootcanal treatment. J Dent Res 2006;85:313–7.
31. Okayama H, Nagata E, Ito HO, et al. Experimental abscess formation caused byhuman dental plaque. Microbiol Immunol 2005;49:399–405.
32. Van Winkelhoff AJ, Bosch-Tijhof CJ, Winkel EG, et al. Smoking affects the subgingivalmicroflora in periodontitis. J Periodontol 2001;72:666–71.
33. Zambon JJ, Grossi SG, Machtei EE, et al. Cigarette smoking increases the risk forsubgingival infection with periodontal pathogens. J Periodontol 1996;67:1050–4.
34. Sasagawa S, Suzuki K, Sakatani T, et al. Effect of nicotine on the functions of humanpolymorphonuclear leukocytes in vitro. J Leukoc Biol 1985;37:493–502.
35. Gomes BP, Lilley JD, Drucker DB. Associations of endodontic symptoms and signswith particular combinations of specific bacteria. Int Endod J 1996;29:69–75.
Associated with Paired Samples of Root Canals and Acute Apical Abscesses 1479

Clinical Research
A Cone-Beam Computed Tomography Study of MaxillaryFirst Permanent Molar Root and Canal Morphologyin a Chinese PopulationQing-hua Zheng, DDS,* Yao Wang, DDS,* Xue-dong Zhou, DDS, PhD,
†Qian Wang, DDS,*
Guang-ning Zheng, DDS,‡
and Ding-ming Huang, DDS, PhD†
Abstract
Aim: This study evaluated root and canal morphology ofpermanent maxillary first molars in a Chinese populationusing cone-beam computed tomography scanning.Methodology: The sample included 775 cone-beamcomputed tomography images of maxillary first molars;627 of the subjects had unilateral qualifying molars and74 had bilateral qualifying molars. The following obser-vations were made: (1) frequency of root and canalnumbers, (2) frequency of additional canals in the me-siobuccal root by sex, age, and tooth position, and (3)unilateral and bilateral occurrence of additional canalsin the mesiobuccal root. Results: Fused roots werepresent in 2.71% of unilateral qualifying molars.Multiple canals were present in the following frequen-cies: two canals in 0.31%, three canals in 47.21%,four canals in 50.40%, five canals in 1.75%, and sixcanals in 0.31% of teeth. Additional canals were de-tected in 52.24% of mesiobuccal roots, 1.12% of disto-buccal roots, and 1.76% of palatal roots. Patients aged20 to 30 years showed a higher prevalence of additionalmesiobuccal root canals. This prevalence did not differwith sex and tooth position. Most (71.11%) of the addi-tional mesiobuccal root canals in subjects with bilateralqualifying molars were symmetric. Conclusion: Cone-beam computed tomography scanning is an effectivemethod for studying external and internal dentalmorphology. The root and canal configurations of maxillaryfirst molars in this Chinese population were consistent withpreviously reported data. More attention should be givento the detection of additional canals in patients between20 and 30 years of age. These data may facilitate success-ful endodontic treatment. (J Endod 2010;36:1480–1484)Key WordsCanal morphology, cone-beam computed tomography,maxillary first molar, root morphology
From the *State Key Laboratory of Oral Diseases, Sichuan UniverWest China College of Stomatology, Sichuan University, Chengdu, C
Address requests for reprints to Dr. Ding-ming Huang, Departm610041, China. E-mail address: [email protected]; and Dr.chuan Province 610041, China. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.018
1480 Zheng et al.
Successful endodontic treatment depends on the adequate cleaning, shaping, andfilling of the root canal system. A thorough knowledge of root canal morphology
is essential to achieve this goal (1). The inability to detect, debride, and obturate allextant canals is a major cause of endodontic failure (2).
Maxillary first molars have the most complex root and canal morphology of themaxillary dentition (3), and many studies have attempted to assess their anatomic char-acteristics. It is now generally accepted that the most common form of maxillary firstmolar has three roots and four canals (4). Most reported incidences of a second canal(MB2) in the mesiobuccal root (MBR) exceed 50% (5–7). These teeth also exhibitsome anatomic variation. Sert and Bayirli (8) assessed 200 extracted maxillary firstmolars by clearing and reported that 9.5% of the distobuccal roots (DBRs) hadmore than two canals. Kottoor et al (9) reported one case in which the maxillary firstmolar exhibited three roots and seven canals (three in the MBR, two in the DBR, and twoin the palatal root [PR]).
The internal anatomy of dental roots and canals has been assessed by clearing(6,10,11), in vitro endodontic access with radiography and instruments (12), radio-graphic examination (4), sectioning (13), in vitro macroscopic examination (14), andin vivo root canal therapy (RCT) with magnification (15). Cone-beam computedtomography (CBCT) scanning was introduced in the field of endodontics in 1990(16). This noninvasive three-dimensional (3D) imaging technique has manyendodontic applications, including morphologic analyses. It uses a cone-shapedbeam of radiation to acquire data in a single 360� rotation, which reveals the internalarchitecture of an object. Compared with conventional CT imaging, CBCT allowsincreased accuracy, higher resolution, and scan time and dose reductions (17). Tachi-bana and Matsumoto (16) reviewed the many potential endodontic applications ofCBCT, including the analysis of canal morphology. Baratto et al (18) used threemethods (ex vivo, clinical, and CBCT) to assess the internal morphology of maxillaryfirst molars and concluded that CBCT was effective for the initial identification of suchmorphology. Trevor et al (19) found CBCT to be a reliable method for the detection ofthe MB2 canal when compared with the gold standard of physical sectioning of the spec-imen. CBCT can also provide personal data such as sex, age, and tooth position, whichmay have important implications in the preoperative evaluation of canal morphology fornonsurgical RCT (8, 20). The certain identification of tooth position can also preventthe recruitment of inappropriate tooth samples in studies using extracted teeth, thusensuring the accuracy of the research.
The aim of this study was to evaluate root and canal morphology of permanentmaxillary first molars in a Chinese population using CBCT. The prevalence of additional
sity, Chengdu, China; and Departments of †Conservative Dentistry and Endodontics and ‡Radiology,hina.ent of Conservative Dentistry, 14# 3rd Section, Renmin South Road, Chengdu, Sichuan ProvinceGuang-ning Zheng, Department of Radiology, 14# 3rd Section, Renmin South Road, Chengdu, Si-
JOE — Volume 36, Number 9, September 2010

TABLE 1. Frequency Distribution of Root Morphology in Maxillary First Molars
Root morphology Maxillary first molar (n = 627) (%)
All roots separate 610 (97.29)MBR fused with DBR 10 (1.59)MBR fused with PR 1 (0.16)DBR fused with PR 3 (0.48)All roots fused 3 (0.48)
Clinical Research
canals in the MBR was also evaluated by sex, age, tooth position, andunilateral or bilateral occurrence.
Materials and MethodsWe screened CBCT images from 2,575 subjects that had been ob-
tained in the medical imaging center of West China Hospital of Stoma-tology, Chengdu, between June 2009 and March 2010. The 3DAccuitomo CBCT machine (MCT-1[EX-2F], J. Morita ManufacturingCorp, Kyoto, Japan) used for tooth identification provided a grayscaleimage of 14 bits and had a voxel size of 0.125 mm. All images useda 1-mm slice thickness. Subjects with fully erupted permanent maxillaryfirst molars were selected. Qualified maxillary molars had fully formedapices and lacked root canal fillings, posts, and crown restorations.CBCT images of 775 maxillary molars from 701 patients of Chinesedescent were identified in the database; 74 of these patients had bilateralqualifying molars. Bilateral molar data were only used to analyze thedistribution of unilateral and bilateral occurrence of additional canalsin the MBR.
Axial, coronal, and sagittal two-dimensional section images weredisplayed on a monitor and inspected by two endodontists using OneData Viewer software (J. Morita Manufacturing Corp). An intraexaminercalibration based on the anatomic diagnosis of CBCT images had beenpreviously performed to assess data reliability. The two endodontists,who were assisted by a radiologist with endodontic experience, exam-ined 20 previously selected CBCT images of morphologically diversemaxillary first molars (three, four, and five root canals). They evaluatedthe images twice, with a 1-week interval between the assessments. Thereliability data were analyzed with a kappa test.
After intra-examiner calibration, the two endodontists separatelyevaluated the images in the study sample. Disagreement in the interpre-tation of images was first addressed in a discussion between the twoendodontists. If consensus could not be reached, a radiologist withendodontic experience helped to make the decision. The frequencyof root and canal numbers; the incidence of additional canals in theMBR; and correlations with sex, age, tooth position; and bilateral andunilateral appearance were determined and assessed by the chi-square test.
ResultsKappa test values for intraexaminer variability were greater than
0.76. The 627 patients with unilateral qualifying maxillary first molarswere between 10 and 86 years of age, with a mean age of 30.2 years. Thefrequency distribution of maxillary first molar root morphology is
TABLE 2. Frequency of Root Canal Numbers in 627 Maxillary First Molars
1 2 3No. of teeth and
frequency (%)0 2 (0.31) 296 (47.2
JOE — Volume 36, Number 9, September 2010 Maxillary F
shown in Table 1. Most (97.29%) molars had three separate roots,whereas all roots were fused in 0.48% of teeth.
Table 2 shows the frequency of the root canal numbers in the 627unilateral qualifying molars. The most frequent pattern in this samplewas four canals (50.40%) followed by three canals (47.21%). Teethwith two, five, and six canals comprised 2.37% of the sample.
The frequencies of root canal and apical foramen numbers indifferent roots are shown in Table 3. Most teeth had one foramen perroot (MBR = 87.98%, DBR = 99.04%, and PR = 98.88%). One toothpresented with only two canals in the DBR and PR. Another tooth ex-hibited six canals, with two in each root (MBR, DBR, and PR). The teethwith five canals had two canals in the MBR and an additional canal ineither the DBR or PR (Figs. 1 and 2).
Because the canals in teeth with all roots fused cannot be classifiedas mesial, buccal, and palatal, the following analysis of canal configura-tions in different roots (MBR, DBR, and PR) excludes these three teeth(n = 624). Single canals were the most frequent configuration in DBRsand PRs. Additional canals were detected in 52.24% of MBRs, 1.12% ofDBRs, and 1.76% of PRs.
Table 4 shows the distribution of additional canals in the MBR ofmaxillary first molars by sex, age, and tooth position. The incidence ofadditional canals in the MBR was 54.27% for men and 50.00% forwomen. Multiple MBR canals were found in 54.13% of left maxillaryfirst molars and 49.8% of right molars. No statistical differences wereobserved in these data. The MBR of teeth in patients between 20 and30 years of age showed a significantly higher prevalence of additionalcanals than those of the other age groups (p < 0.05). The lowestfrequency (40%) of additional canals was found in the group of patientswho were more than 60 years of age. There were no statistical differ-ences among groups other than the 20- to 30-year group.
The distribution of unilateral and bilateral occurrence of addi-tional MBR canals among subjects with bilateral permanent maxillaryfirst molars is shown in Table 5. Of 775 subjects examined, 74 subjectsshowed bilateral permanent maxillary first molars (Fig. 2). The bilateraloccurrence among patients with additional root canals in the MBR was71.11%, which was much higher than the unilateral occurrence(28.89%). The frequency of bilateral distribution did not differ withsex and tooth position (Table 6).
DiscussionPrior knowledge of root and canal anatomy facilitates the accurate
detection of all root canals in a tooth during endodontic treatment. Manystudies of the root and canal morphology of the maxillary first molarhave been conducted because this tooth presents complex morphologythat often increases the difficulty of treatment (5, 6). However, most ofthese studies have either completely destroyed the tooth duringexamination or have gained only two-dimensional anatomic informa-tion. Moreover, few studies have incorporated information such asethnic background, age, and sex of the study population, which mayhave important clinical implications for treatment. The recent use ofCBCT has made it possible to conduct a nondestructive 3D global anal-ysis of the external and internal morphology of the root and canalsystem. The 3D Accuitomo CBCT machine used in this study offershigh resolution and is well suited for endodontic applications (16).
No. of canals
4 5 61) 315 (50.40) 11 (1.75) 2 (0.31)
irst Permanent Molar Root and Canal Morphology in a Chinese Population 1481

TABLE 3. Frequency of Root Canal and Apical Foramen Numbers in Different Roots
No. of canals and frequency (%) No. of foramina and frequency (%)
1 2 3 1 2 3
MBR (n = 624) 297 (47.59) 324 (51.92) 3 (0.48) 556 (89.10) 68 (10.90) 0DBR (n = 624) 617 (98.88) 7 (1.12) 0 622 (99.68) 2 (0.32) 0PR (n = 624) 613 (98.24) 11 (1.76) 0 617 (98.88) 7 (1.12) 0
Clinical Research
This study found that 2.71% of maxillary first molars amongpatients of Chinese descent had fused roots. The MBR had a higherfrequency of fusion than other roots. This result was consistent withfindings in Ugandan (21) and, to a lesser extent, Irish (22) populations.However, previous studies of Burmese (23) and Thai (5) populationsfound three separate roots in all maxillary first molars. These differ-ences highlight the influence of ethnic background on maxillary molarroot morphology.
Frequencies of additional canals in the MBR have been reported bymany studies (5, 8, 24). The high frequency (52.40%) of additionalMBR canals in this study is largely consistent with findings fromclearing studies of Asian populations from Thailand (65.0%) andJapan (58.0%) (5, 24). Our result was lower than that of a Turkish
Figure 1. A case of unilateral permanent maxillary first molar with a second canal inby using One Data Viewer software. (A) Coronal view with the mesiobuccal rootmaxillary first molar with MB2), and (D) scanning details.
1482 Zheng et al.
population (93.5%) (8). Our results contrasted with those of a recentstudy of a Chinese population from the Guanzhong area, which useda new modified root canal staining technique (25) and found that33.3% of the MBRs had additional canals. This variation may be causedby the differences in sample sizes, methods, and/or regional popula-tional diversity. The present study found that 79.20% of the additionalcanals in MBR exhibited a single foramen. This result agreed with that ofVertucci (26) who reported that 82% of the additional MBR canalsfused into a single apical foramen.
Variations in additional canals in the DBR and PR have been lessfrequently observed. Our study found additional canals in 1.12% ofDBRs and 1.17% of PRs. These results were similar to these (2.50%
mesiobuccal root (MB2) as viewed in the coronal, sagittal, and axial directionexhibiting 2 canals, (B) sagittal view, (C) axial view (the arrow indicates the
JOE — Volume 36, Number 9, September 2010

Figure 2. Cases of maxillary first molar with root and canal variation in axial section; the black arrows indicate the examined tooth. (A) Two canals and fusedroots, (B) five canals, (C) six canals, and (D) bilateral occurrence of MB2.
TABLE 4. Numbers and Frequency of Additional Root Canals in the MBR of the Maxillary First Molars by Sex, Age, and Tooth Position
Sex Tooth position Age (y)
Male Female Left Right 10�20 20�30 30�40 40�50 50�60 >60
n = 328 n = 296 n = 351 n = 273 n = 225 n = 123 n = 84 n = 102 n = 50 n = 40
No. of teeth 178 148 190 136 113 84 43 43 22 16Frequency (%) 54.27 50.00 4.13 49.82 50.22 68.29* 51.19 42.16 44.00 40.00
*p < 0.05.
TABLE 5. Distribution of Unilateral and Bilateral Occurrence Among 45Patients With Additional Root Canals in the MBR
Number ofpatients
Frequency(%)
MBR with more than onecanal (unilateral, left)
5 11.11
(unilateral, right) 8 17.78(bilateral) 32 71.11Total 45 100
Clinical Research
JOE — Volume 36, Number 9, September 2010 Maxillary F
and 1.20%) reported by al Shlabi et al (22) in a study that used theclearing method.
Sert and Bayirli (8) conducted a clearing study of human perma-nent teeth from Turkish patients and concluded that sex was an impor-tant factor to consider in the preoperative evaluation of canalmorphology for nonsurgical RCT. In contrast, the incidence of addi-tional MBR canals in our sample did not differ by the sex of the patient.This is in concordance with the results of a previous study reported byNeaverth et al (27). We also found that the number of MBR canals wasnot affected by tooth position, which is in agreement with the latter study.
irst Permanent Molar Root and Canal Morphology in a Chinese Population 1483

TABLE 6. Distribution of Unilateral and Bilateral Occurrence of Additional Root Canals in the MBR Among 74 Patients With Bilateral Permanent Maxillary FirstMolars
MBR with additional canal MBR with one canal
Unilateral Bilateral
Left Right Total
n % n % n % n % n
No. of patientsMale 1 3.22 2 6.45 17 54.84 11 35.48 31Female 4 9.30 6 13.95 20 46.51 13 30.23 43Total 5 6.76 8 10.81 37 50.00 24 32.43 74No. of teeth 5 3.38 8 5.41 74 50.00 61 41.22 148
Clinical Research
Hess (28) has reported that a broad canal may diverge into twocanals as a patient grows older because of the apposition of dentinbetween the canal walls at the narrowest points. After 40 years of age,the canal morphology appeared to again become less complicatedbecause of calcification of the canal ramifications. Our study foundsignificantly more additional MBR canals among patients between 20and 30 years of age (68.29%, p < .05). This result was similar tothat of Neaverth et al (27) who found a higher frequency of two MBRcanals in the maxillary first molars of patients between 20 and 40 yearsof age. In our study, less than half of the MBR was found to have addi-tional canals in patients older than 40 years.
Additional MBR canals were symmetrically distributed in 71.11%of our Chinese population. If a patient has a known MB2 in one maxil-lary first molar, the dentist should be aware of the likelihood that anMB2 is present in the opposite molar. We found no differences in bilat-eral occurrence by sex or tooth position. The incidence of additionalcanals in subjects with bilateral maxillary first molars (58.78%) washigher than that of subjects with unilateral maxillary first molars(52.40%). This may partly be caused by the sample size and the highincidence of bilateral distribution of the additional canals, whichaugments the result.
ConclusionsWithin the limitations of this study, it can be concluded that more
than half of maxillary first molars have four canals and three roots in theChinese population. Most of the additional canals were located in theMBR and had one foramen. The incidence of additional MBR canalsdid not differ with sex or tooth position and was usually bilateral.More additional canals were detected by CBCT in patients between 20and 30 years of age. These values may help dentists to locate additionalcanals in the maxillary first molar and thereby achieve better outcomesfor the endodontic treatment of these teeth.
References1. Baisden MK, Kulild JC, Weller RN. Root canal configuration of the mandibular first
premolar. J Endod 1992;18:505–8.2. Vertucci FJ. Root canal morphology and its relationship to endodontic procedure.
Endodontic Topics 2005;10:3–29.3. Vertucci FJ, Haddix JE, Britto LR. Tooth morphology and access cavity preparation.
In: Cohen S, Hargreaves KM, eds. Pathways of the Pulp. 9th ed. St. Louis: MosbyElsevier; 2006:203.
4. Walton R, Torabinejad M. Principles and practice of endodontics. 2nd ed. Philadel-phia: WB Saunders Co; 1996.
5. Alavi AM, Opasanon A, Ng YL, et al. Root and canal morphology of Thai maxillarymolars. Int Endod J 2002;35:478–85.
1484 Zheng et al.
6. Pineda F, Kutler Y. Mesiodistal and buccolingual roentgenographic investigation of7275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101–10.
7. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral MedOral Pathol 1984;58:589–99.
8. Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular andmaxillary permanent teeth by gender in the Turkish population. J Endod 2004;30:391–8.
9. Kottoor J, Velmurugan N, Sudha R, et al. Maxillary first molar with seven root canalsdiagnosed with cone-beam computed tomography scanning: a case report. J Endod2010;36:915–21.
10. Gulabivala K, Aung TH, Alavi A, et al. Root canal morphology of Burmese mandibularmolars. Int Endod J 2001;33:359–70.
11. Omer OE, Al Shalabi RM, Jennings M, et al. A comparison between clearing andradiographic techniques in the study of the root-canal anatomy of maxillary firstand second molars. Int Endod J 2004;37:291–6.
12. Kulild JC, Peters DD. Incidence and configuration of canal systems in themesiobuc-cal root of maxillary first and second molars. J Endod 1990;16:311–7.
13. Seidberg BH, Altman M, Guttuso J, et al. Frequency of two mesiobuccal root canalsin maxillary permanent first molars. J Am Dent Assoc 1973;87:852–6.
14. Pecora JD, Woelfel JB. Sousa Neto MD. Morphologic study of themaxillarymolars.1.External anatomy. Braz Dent J 1991;2:45–50.
15. Buhrley LJ, Barrows MJ, BeGole EA, et al. Effect of magnification on locating the MB2canal in maxillary molars. J Endod 2002;28:324–7.
16. Tachibana H, Matsumoto K. Applicability of x-ray computerized tomography inendodontics. Endod Dent Traumatol 1990;6:16–20.
17. Scarfe WC. Imaging of maxillofacial trauma: evolutions and emerging. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2005;100:S75–96.
18. Baratto Filho F, Zaitter S, Haragushiku GA, et al. Analysis of the internal anatomy ofmaxillary first molars by using different methods. J Endod 2009;35:337–42.
19. Trevor CB, Nathan G, Charles CL, et al. Efficacy of cone-beam computed tomographyas a modality to accurately identify the presence of second mesiobuccal canal inmaxillary first and second molars: a pilot study. J Endod 2010;36:867–70.
20. Fogel HM, Peikoff MD, Christie WH. Canal configuration in the mesiobuccal root ofthe maxillary first molar: a clinical study. J Endod 1994;20:135–7.
21. Rwenyonyi CM, Kutesa AM, Muwazi LM, et al. Root and canal morphology of maxil-lary first and second permanent molars teeth in a Ugandan population. Int Endod J2007;40:679–83.
22. al Shalabi RM, Omer OE, Glennon J, et al. Root canal anatomy of maxillary first andsecond permanent molars. Int Endod J 2000;33:405–14.
23. Ng YL, Aung TH, Alavi A, et al. Root and canal morphology of Burmese maxillarymolars. Int Endod J 2001;34:620–30.
24. Degerness RA, Bowles WR. Dimension, anatomy and morphology of the mesiobuc-cal root canal system in maxillary molars. J Endod 2010;36:985–9.
25. Weng XL, Yu SB, Zhao SL, et al. Root canal morphology of permanent maxillary teethin the Han nationality in Chinese Guanzhong area: a new modified root canal stain-ing technique. J Endod 2009;35:651–6.
26. Vertucci FJ. Root canal morphology of the human permanent teeth. Oral Surg OralMed Oral Pathol 1984;58:589–99.
27. Neaverth EJ, Kolter LM, Kaltenbach RF. Clinical investigation (in vivo) of endodon-tically treated maxillary first molars. J Endod 1987;13:506–12.
28. Hess W. The Anatomy of the Root Canals of the Teeth of Permanent Dentition. Lon-don: John Bale, Sons & Danielsson Ltd; 1925.
JOE — Volume 36, Number 9, September 2010

Clinical Research
Prevalence and Activity of Epstein-Barr Virus andHuman Cytomegalovirus in Symptomaticand Asymptomatic Apical Periodontitis LesionsKatinka Hernadi, MD,* Anita Szalmas, MSc,* Richard Mogyorosi, MD,
†Levente Czompa, MD,
†
Gyorgy Veress, PhD,* Eszter Csoma, PhD,* Ildiko Marton, MD, PhD, DSci,†
and Jozsef Konya, MD, PhD*
Abstract
Introduction: Apical periodontitis is a polymicrobialinflammation with a dominant flora of opportunisticGram-negative bacteria; however, a pathogenic role ofhuman herpesviruses such as Epstein-Barr virus (EBV)and human cytomegalovirus (HCMV) has been implicatedrecently. The aims of this study were to determine the prev-alence, activity, and disease association of EBV and HCMVin apical periodontitis in an Eastern Hungarian population.Methods: Forty samples with apical periodontitis (17symptomatic and 23 asymptomatic) and 40 healthy pulpcontrols were collected. EBV and HCMV prevalenceswere measured by polymerase chain reaction (PCR) detec-tion of the viral DNA and viral activity was tested byreverse-transcription PCR amplification of viral messengerRNA. Results: EBV DNA and EBNA-2 messenger RNAwere found in apical periodontitis lesions at significantly(p < 0.0001) higher frequencies (72.5% and 50%, respec-tively) than in controls (both 2.5%). The occurrence ofHCMV infection was rare in both apical lesions (10%)and controls (0%). The presence of EBV DNA in apicallesions was associated significantly with large ($5 mm)lesion size (p = 0.02) but not with symtoms (p = 0.30).Symptomatic manifestation was significantly associatedwith the co-occurrence (odds ratio [OR], 8.80; 95% confi-dence interval [CI], 1.69-45.76) but not the sole occur-rences of EBNA-2 messenger RNA (OR, 2.29; 95% CI,0.48-11.06) and large lesion size (OR, 4.02; 95% CI,0.81-19.89). Conclusion: EBV infection is a frequentevent in apical periodontitis, whereas the involvementof HCMV still remains to be elucidated. This study showedthat symptomatic manifestation was likely to occur ifa large-sized apical periodontitis lesion is aggravatedwith active EBV infection. (J Endod 2010;36:1485–1489)Key WordsApical periodontitis, Epstein-Barr virus type III virallatency, herpesviruses, human cytomegalovirus, poly-merase chain reaction
From the *Department of Medical Microbiology and †Faculty ofAddress requests for reprints to Dr J Konya, PO Box 17 Debrece
0099-2399/$0 - see front matterCopyright ª 2010 American Association of Endodontists.
doi:10.1016/j.joen.2010.06.008
JOE — Volume 36, Number 9, September 2010
Herpesviruses are supposed to be involved in several oral diseases in immunocompetenthosts, including mucosal inflammations, irreversible pulpitis, and apical and marginal
periodontitis (1–3). Apical periodontitis is essentially a polymicrobial inflammationcaused by opportunistic endodontic bacteria, but other microbes, such as Epstein-Barrvirus (EBV) and human cytomegalovirus (HCMV), can play a pathogenic role (1, 4–7).
Like other herpesviruses, these microbes are capable of persisting in a lifelonglatency after primary infection: EBV initially infects oronasopharyngeal epithelial cellsin a lytic form, and then infects B lymphocytes establishing type I latency, which doesnot influence host cell functions (8–10). HCMV establishes latent infection inCD34+ bone marrow myeloid progenitor cells, dendritic cell (DC) precursors, andmonocytes. For both EBV and HCMV, typical sites of reactivation are the salivaryglands and the mucosal surfaces (8, 11).
During periapical inflammation, there is an influx of leukocytes, of which themononuclear cells may carry latent herpesviruses. The local environment may allowherpesviral activation from the inactive latent phase. In the EBV-infected B lymphocytes,either a phenotype change called type III latency or lytic reactivation can occur. Severalstudies tested the activity of EBV infection by detecting EBNA-2 messenger RNA, which isexpressed only in type III latency. In this latency stage, tumor necrosis factor a (TNF-a)is produced by infected B cells, which is a major mediator of inflammation and tissuedestruction. In these studies, EBNA-2 expression was indeed associated with symptom-atic periods of apical periodontitis (1, 4, 5, 12).
Regarding HCMV, the differentiation of infected monocytes into tissue macro-phages or the maturation of infected DCs is followed by the reactivation of latent infec-tion (11). The released infectious virions are capable of infecting further macrophages,T lymphocytes, endothelial cells, and connective tissue cells (13, 14). The aims of thisstudy were to determine the prevalence and activity of EBV and HCMV by the detection ofviral DNA and messenger RNA in apical periodontitis samples and to analyze theassociation with clinical symptoms.
Material and MethodsForty apical periodontitis samples and 40 impacted third molars used as healthy
pulp controls were collected from patients seeking dental care at the Department of Oraland Maxillofacial Surgery, Faculty of Dentistry, University of Debrecen. The Local EthicalCommittee approved the study (approval number: 2885-2008). Patients were anony-mously coded for identification, and they filled out informed consents. Patients withapical periodontitis also filled out questionnaires, which contained questions aboutgeneral diseases, medications, history of the involved tooth, and related symptoms.
Dentistry, Medical and Health Science Center, University of Debrecen, Debrecen, Hungary.n 4012 Hungary. E-mail address: [email protected]
EBV and HCMV in Apical Periodontitis Lesions 1485

Clinical Research
The inclusion criteria for patients were as follows: individuals ingood health (American Society of Anesthesia I or II) with no severesystemic disease requiring surgical apicoectomy because of the failureof conventional root canal therapy. Patients with either poor generalstatus or systemic diseases or periodontally involved teeth (probingdepth >4 mm) were excluded.
Teeth with apical periodontitis were classified into symptomaticand asymptomatic groups. Symptomatic lesions were characterizedby acute pain, discomfort on biting, sensitivity by percussion, or palpa-tion at the apical region of mucosa. The asymptomatic lesions did nothave any clinical symptoms with the exception of periapical radiolucentarea on radiographs. Based on the radiographic size of the lesion,samples were divided into two subgroups: more or equal to 5 mm($5 mm) and less than 5 mm (<5 mm) diameter of lesions.
Before administrating local anesthetics for apicoectomy, patientsrinsed their mouth with 0.2% chlorhexidine mouthwash for 1 minute,and the teeth, gingiva, and mucosa of the sample area were washedwith 0.2% chlorhexidine. Using a sterile no. 15 blade, gingival inci-sions were extended one or two teeth mesially or distally from thestudied tooth followed by a vertical releasing incision. A full-thickness mucoperiosteal flap was then reflected, and the periapicallesion was exposed with a sterile round barr using sterile saline ascoolant. A sterile curette was used to obtain the periapical sample,which was put into sterile Eppendorf tube with RNAlater RNA stabi-lization reagent (Applied Biosystems, Foster City, CA) and then wasimmediately frozen to �70�C.
All control teeth were matured impacted third molars, with nosigns of caries, cracking, or pulpal inflammation. Before adminis-trating local anesthetics, patients rinsed their mouth with 0.2%chlorhexidine mouthwash for 1 minute and the teeth, gingiva, andmucosa of the sample area were washed with 0.2% chlorhexidine.Using a sterile no. 15 blade, an alveolar reach incision and gingivalincisions were extended one or two teeth mesially from the involved
TABLE 1. Primer Sequences and PCR Conditions
Target Primer sequence Size o
EBV-DNA:BamH1-WP-f 5’ GAGACCGAAGTGAAGGCCCT 3’P-r 5’ GGTGCCTTCTTAGGAGCTGT 3’N-f 5’ GCCAGAGGTAAGTGGACTTTAAT 3’N-r 5’ GAGGGGACCCTGAGACGGGT 3’
EBV-mRNA:EBNA-2P-f 5’ TCCACCACACCCAGGCAC 3’P-r 5’ TGGAGAGGTCAGGTTACTTAC 3’N-f 5’ ACACACACCCACCCGTCTCA 3’N-r 5’ TTGCTGGACGAGGACCCTT 3’
HCMV-DNA:pp65P-f 5’ TCACCTGCATCTTGGTTGCG 3’P-r 5’ TGCCGCTCAAGATGCTGAAC 3’N-f 5’ GGAAACACGAACGCTGACGT 3’N-r 5’ TGCCGCTCAAGATGCTGAAC 3’
HCMV-mRNA:pp65P-f 5’ ACGCGCTGCCGCTCAAGAT 3’P-r 5’ TGTAGTAGACGTCGGGCTCTTT 3’N-f 5’ CGCTGCCGCTCAAGATGCTGAA 3’N-r 5’ ATCTGCTTGCCCGACGCGTGAA 3’
Where reference is not shown, the primers were designed by the authors.
P-f, primary-forward primer; P-r, primary-reverse primer; N-f, nested-forward primer; N-r, nested reverse
1486 Hernadi et al.
tooth followed by a vertical releasing incision. A full-thicknessmucoperiosteal flap was then reflected, and the impacted third molarwas exposed with a sterile round barr using sterile saline as coolant.Each removed tooth was put in a Falcon tube with sterile saline andwas immediately frozen to�70�C. To avoid sample to sample contam-ination in the laboratory, each extracted tooth were packed separatelyinto sterile plastic bag, and it was fractured inside the bag andthereafter pulp tissues were removed.
Homogenized tissue samples were divided into two portions: onefor RNA and the other for DNA isolation. DNA was isolated by High PureViral Nucleic Acid Kit (Roche, Switzerland) according to the manufac-turer’s instructions. The total RNA was extracted with TRI Reagent(Sigma, St Louis, MO) according to the manufacturer’s protocol. Theextracted RNA was turned to complementary DNA (cDNA) by usingthe High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems)with random hexamers. The effectiveness of DNA and RNA isolationwere controlled with polymerase chain reaction (PCR) and reverse-transcription PCR detection of human b-globin and h36B4 house-keeping genes, respectively. Five microliters of DNA or cDNA was ampli-fied in 20 mL final volume using 1 U Red Taq Polymerase (Sigma, StLouis, MO) according to the manufacturer’s instructions. Nested PCRamplification was performed with a 1-mL aliquot of the primary reac-tion. The primers and PCR conditions are shown in Table 1 (15–17).
The significance of differences were analyzed using Yates cor-rected chi-square statistics. If an expected cell value was less thanfive in a contingency table, the Fisher exact test was used. For multivar-iate analysis, logistic regression statistics were used.
ResultsA total of 40 apical periodontitis samples were collected from 36
patients (age, 18-80 years; mean age, 49 years) and 40 healthy pulp
PCR conditions
f amplicon (reference) Temperature profile cycles
171 bp (15) 94�C 58�C 72�C 30�30 s 30 s 90 s
97 bp (15) 94�C 60�C 72�C 35�30 s 30 s 90 s
205 bp (16) 94�C 54�C 72�C 30�30 s 30 s 90 s
120 bp 94�C 63�C 72�C 35�30 s 30 s 90 s
309 bp (17) 94�C 64�C 72�C 30�30 s 30 s 90 s
220 bp (17) 94�C 65�C 72�C 35�30 s 30 s 90 s
195 bp (16) 94�C 60�C 72�C 30�30 s 30 s 90 s
124 bp 94�C 70�C 72�C 35�30 s 30 s 90 s
primer; mRNA, messenger RNA.
JOE — Volume 36, Number 9, September 2010

TABLE 2. Prevalence (DNA) and Activity (mRNA) of EBV and HCMV in Symptomatic, Asymptomatic, Larger ($5 mm)-, and Smaller (<5 mm)-Sized ApicalPeriodontitis Lesions
EBV n (%) HCMV n (%) EBV+ HCMV n (%)
DNA mRNA DNA mRNA DNA
Apical periodontitis (n = 40) 29* (72.5) 20* (50) 4 (10) 0 (0) 3 (7.5)Symptomatic (n = 17) 14* (82) 12* (71) 1 (6) 0 (0) 1 (6)Asymptomatic (n = 23) 15* (65) 8† (35) 3 (13) 0 (0) 2 (9)Lesion size $5 mm (n = 21) 19* (91) 16* (76) 3 (14) 0 (0) 2 (10)Lesion size <5 mm (n = 19) 10* (53) 4‡ (21) 1 (5) 0 (0) 1 (5)Healthy controls (n = 40) 1 (2.5) 1 (2.5) 0 (0) 0 (0) 0 (0)
Using healthy controls as the reference group, statistical tests revealed *p < 0.0001, †p < 0.001 and ‡p < 0.05. The nonlabeled frequencies are not significantly different from those of the healthy controls
Clinical Research
control samples from 25 patients (age, 17-29 years; mean age, 23years).
EBV DNA was detected in apical periodontitis lesions at a signifi-cantly higher frequency than in healthy pulp controls (72.5% vs2.5%, p < 0.0001). The local activation of EBV infection as detectedby EBNA-2 messenger RNA expression was significantly more frequentin apical periodontitis lesions (50% vs 2.5%, p < 0.0001). Sampleswith apical periodontitis were classified into subgroups according tosymptoms and the size of radiographic bone destruction, respectively(Table 2.). Both markers of EBV infection had significantly higherfrequencies in each subgroup compared with healthy controls.Table 2 also shows that EBV DNA and EBNA-2 messenger RNA weredetected more frequently in large lesions compared with small lesionsand in symtomatic lesions compared with asymptomatic ones. BothEBV DNA (p = 0.02) and EBNA-2 messenger RNA (p = 0.002)were significantly associated with a large lesion size.
TABLE 3. Determinants of Symptomatic Periapical Periodontitis
Independentvariable Lesions n Symptomatic n (%)
Lesion size<5 mm 19 4 (21)$5 mm 21 13 (62)
EBV DNANo 11 3 (27)Yes 29 14 (48)
EBNA mRNANo 20 5 (28)Yes 20 12 (60)
Variables Combined
size mRNA
<5 mm No 15 3 (20)
<5 mm Yes9 3 (33)
$5 mm No
$5 mm Yes 16 11 (69)
NA, not applicable.
Adjusted to )EBNA messenger RNA and †lesion size.‡95% confidence interval and the corresponding p value of the calculated OR unless §p for trend calcula
JOE — Volume 36, Number 9, September 2010
Lesion size itself can also be an important clinical determinant ofsymptomatic manifestation. Therefore, we assessed the disease associ-ation of EBV infectious markers together with that of lesion size inlogistic regression statistics allowing both univariate and multivariateanalysis (Table 3). Based on the crude odds ratios and confidenceintervals, large lesion size and EBNA-2-messenger RNA but not EBV-DNA appeared to be significant determinants for symptomatic apical pe-riodontitis in the univariate analysis. However, the adjusted odds ratiosand confidence intervals of the multivariate analysis indicated that thestrength of association has been reduced to a tendency level (p =0.08) for lesion size, and the association between EBNA messengerRNA and symptomatic manifestation has been eliminated (Table 3).Because EBNA messenger RNA and lesion size mutually weakenedeach other’s effect, we hypothesized that the disease association couldbe determined rather by complementary than separated effects of theinvestigated parameters. Therefore, the involved parameters were
Odds ratio(95% confidence interval)‡
Adjusted odds ratio(95% confidence interval)‡
1.0 (ref) 1.0 (ref)6.09 (1.49-24,99) 4.02 (0.81-19.89)*
p = 0.01 p = 0.08
1.0 (ref) 1.0 (ref)2.49 (0.55-11.30) 1.11 (0.19-6.18)†
p = 0.24 p = 0.90
1.0 (ref) 1.0 (ref)4.50 (1.17-17.37) 2.29 (0.48-11.06)†
p = 0.03 p = 0.30
1.0 (ref) NA
1.99 (0.31-13.06) NA
8.80 (1.69-45.76) NAp = 0.027§
ted.
EBV and HCMV in Apical Periodontitis Lesions 1487

Clinical Research
combined, and the odds ratios for symptomatic manifestation werecalculated separately in subgroups with none, any, and both of thehypothesized disease determinants (Table 3). Indeed, the co-occurrence of large lesion size and EBNA-2 messenger RNA was stronglyassociated (odds ratio, 8.80) with symptomatic manifestation. Neitherthe age nor the sex of the patients, tooth localization (left-right or upper-lower), or type of teeth (incissors, canines, or premolars) influencedthe lesion size, the symptoms, or the incidence of EBV DNA andEBNA-2 messenger RNA, respectively (data not shown).Only four apical periodontitis lesions (10%) carried HCMV DNA,and, although HCMV was not found in healthy pulp controls, the differ-ence was not significant in either the whole group of lesions (p = 0.12)or the subgroups. We could not detect HCMV messenger RNA in path-ological or healthy samples (Table 2).
DiscussionIn apical periodontitis, the active participation of EBV was shown
previously by EBNA-2 messenger RNA expression and immunohisto-chemical detection of EBV latent membrane proteins (6, 18). Bothmarkers indicate that a remarkable proportion of inflammatedperiapical lesions harbors EBV infected lymphocytes in type IIIlatency stage. In this study, not only the activity of EBV infection wasanalyzed on the basis of EBNA-2 messenger RNA detection but alsothe occurrence of EBV DNA was measured to detect the prevalence ofthe virus regradless of the infectious stage. Our EBNA-2 messengerRNA results revealed viral activity at a similar level to other studies(1, 4, 5, 12). This study showed that approximately two thirds of theEBV DNA–positive periapical lesions had EBNA-2 messenger RNAexpression, the remaining one third carried EBV in infectious stagesother than type III latency. Most studies on EBV infection in apical pe-riodontitis included the symptomatic manifestation as the only clinicalparameter in the analysis, and they also revealed the associationbetween symptoms and EBNA-2 messenger RNA expression (1, 4, 5,12). The studies by Sabieti et al (1, 4) analyzed the lesion size, andthe pairwise analysis revealed that both symptomatic manifestationand large lesion size were associated with EBNA-2 messenger RNAexpression. In this study, we pointed out that symptomatic manifestationand a large lesion size tend to coexist, and, therefore, their associationwith EBV infection was evaluated in a multivariate statistical analysis. Ac-cording to the results of the multivariate analysis, we hypothesizeda complementary effect of a large lesion size and EBNA-2 expressionupon symptomatic manifestation. Subgrouping of the lesions accordingto this hypothesis allowed us to prove that large-sized apical periodon-titis lesions aggravated with EBV infection at type III latency stage willmost likely be symptomatic. On the other hand, the sole occurrenceof either determinant has little if any effect on symptomatic stage.Another study showed that the lytic stage as detected by the expressionof a viral tegument protein also occured frequently in apical periodon-titis and tended to correlate with lesion size but not with symptomaticmanifestation (16).
From methodologic points, we minimized the contamination ofsamples with high EBV containing compartments such as saliva or peri-odontal pocket flora. The surgical technique itself is performed in a wayto avoid saliva contamination from the oral cavity just to prevent post-operative wound infection. Furthermore, saliva is deprived of live repli-cating cells capable of hosting EBV infection in type III latency.Periodontally involved teeth were excluded from the study to avoida major source of external EBV contamination (19). Because thesame gingival incision technique was applied during operation, contam-ination by gingival sulcus should have affected equally the diseased andthe contol group of samples.
1488 Hernadi et al.
Based on the results by Sunde et al (13), we expected a low viralload in the samples analyzed in this study. Therefore, we applied nestedPCR to increase the specificity and sensitivity of the virus detection, andthe cycle number in the primary PCR was limited to 30 to reduce the riskof in-procedure cross-contamination (20).
With regard to the underlying mechanisms, EBV-infected Blymphocytes in type III latency stage are known to produce TNF-a,transforming growth factor b, and interleukin-10 (21). TNF-a hasthe ability to increase bone resorption and can induce powerful hyper-algesia (22, 23). Ttransforming growth factor b is able to impairantiviral host defenses through the repression of lymphocyteproliferation, cytotoxic T-cell functions, toll-like receptor signaling,and so on. Interleukin-10 is able to inhibit macrophage activationand the antigen-presenting functions (24).
A further aim of this study was to provide data obtained on healthytissue samples. We detected only a negligible occurrence of EBV DNAand EBNA-2 messenger RNA in healthy pulp tissues. Based on theseresults and the similar results of a recent study (16), the most probablesource of EBV infection in apical periodontitis is the immigrating B-lymphocyte population.
The literature on the prevalence of HCMV shows two peaks ofdistribution. Several studies found the frequencies of HCMV messengerRNA to be between 40% and 100% in apical periodontitis lesions (1, 4,5, 12, 17). Our data are more consistent with the findings of otherstudies, which found HCMV occurrence between 0% and 15.9% inapical periodontitis (13, 16, 18). Because these investigationsuniformly tested the pp65 matrix protein coding sequences on HCMVDNA or messenge RNA, the observed biological diversity is probablybecause of the recent alteration of HCMV epidemiology at certaingeographic regions.
Periapical flareups may develop as a result of complex immuneresponses against the herpesviral-bacterial coinfection (5, 18). Thecumulative effects of herpesviruses, endopathogenic bacteria, andproinflammatory immune mechanisms may be manifested inincreased resorption of the periapical alveolar bone and in clinicalsymptoms, such as acute pain, discomfort on biting, and sensitivity topalpation at the apical region of mucosa.
In conclusion, EBV infection is a frequent event in apical perio-dontitis, whereas the involvement of HCMV still remains to be eluci-dated. If EBV infection is present, the infected cells havea remarkable chance to be at type III latency stage, which, in turn, leadsto the production of inflammatory cytokines. This study showed thatsymptomatic manifestation was likely to occur if EBV infection at typeIII latency aggravates a large-sized apical periodontitis lesion.
References1. Sabeti M, Valles Y, Nowzari H, et al. Cytomegalovirus and Epstein-Barr virus DNA
transcription in endodontic symptomatic lesions. Oral Microbiol Immunol 2003;18:104–8.
2. Saygun I, Yapar M, Ozdemir A, et al. Human cytomegalovirus and Epstein-Barr virustype 1 in periodontal abscesses. Oral Microbiol Immunol 2004;19:83–7.
3. Slots J, Contreras A. Herpesviruses: a unifying causative factor in periodontitis? OralMicrobiol Immunol 2000;15:277–80.
4. Sabeti M, Slots J. Herpesviral-bacterial coinfection in periapical pathosis. J Endod2004;30:69–72.
5. Sabeti M, Simon JH, Slots J. Cytomegalovirus and Epstein-Barr virus are associatedwith symptomatic periapical pathosis. Oral Microbiol Immunol 2003;18:327–8.
6. Slots J, Sabeti M, Simon JH. Herpesviruses in periapical pathosis: an etiopathogenicrelationship? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:327–31.
7. Sabeti M, Simon JH, Nowzari H, et al. Cytomegalovirus and Epstein-Barr virus activeinfection in periapical lesions of teeth with intact crowns. J Endod 2003;29:321–3.
8. Slots J, Saygun I, Sabeti M, et al. Epstein-Barr virus in oral diseases. J PeriodontalRes 2006;41:235–44.
JOE — Volume 36, Number 9, September 2010

Clinical Research
9. Kenney S, Theodore E. Woodward Award: development of novel, EBV-targeted ther-apies for EBV-positive tumors. Trans Am Clin Climatol Assoc 2006;117:55–73.discussion 73–4.
10. Bollard CM, Cooper LJ, Heslop HE. Immunotherapy targeting EBV-expressing lym-phoproliferative diseases. Best Pract Res Clin Haematol 2008;21:405–20.
11. Sinclair J, Sissons P. Latency and reactivation of human cytomegalovirus. J Gen Virol2006;87:1763–79.
12. Slots J, Nowzari H, Sabeti M. Cytomegalovirus infection in symptomatic periapicalpathosis. Int Endod J 2004;37:519–24.
13. Sunde PT, Olsen I, Enersen M, et al. Human cytomegalovirus and Epstein-Barr virusin apical and marginal periodontitis: a role in pathology? J Med Virol 2008;80:1007–11.
14. Chen V, Chen Y, Li H, et al. Herpesviruses in abscesses and cellulitis of endodonticorigin. J Endod 2009;35:182–8.
15. Kis A, Feher E, Gall T, et al. Epstein-Barr virus prevalence in oral squamous cellcancer and in potentially malignant oral disorders in an eastern Hungarian popu-lation. Eur J Oral Sci 2009;117:536–40.
16. Li H, Chen V, Chen Y, et al. Herpesviruses in endodontic pathoses: association of Epstein-Barr virus with irreversible pulpitis and apical periodontitis. J Endod 2009;35:23–9.
JOE — Volume 36, Number 9, September 2010
17. Yazdi KA, Sabeti M, Jabalameli F, et al. Relationship between human cytomegalovirustranscription and symptomatic apical periodontitis in Iran. Oral Microbiol Immunol2008;23:510–4.
18. Saboia-Dantas CJ, Coutrin de Toledo LF, Sampaio-Filho HR, et al. Herpesviruses inasymptomatic apical periodontitis lesions: an immunohistochemical approach. OralMicrobiol Immunol 2007;22:320–5.
19. Sahin S, Saygun I, Kubar A, et al. Periodontitis lesions are the main source of salivarycytomegalovirus. Oral Microbiol Immunol 2009;24:340–2.
20. Olmos A, Esteban O, Bertolini E, et al. Nested rt-PCR in a single closed tube. MethodsMol Biol 2003;226:151–60.
21. Rochford R, Cannon MJ, Sabbe RE, et al. Common and idiosyncratic patterns of cyto-kine gene expression by Epstein-Barr virus transformed human B cell lines. ViralImmunol 1997;10:183–95.
22. Rittner HL, Machelska H, Stein C. Leukocytes in the regulation of pain and analgesia.J Leukoc Biol 2005;78:1215–22.
23. Kawashima N, Stashenko P. Expression of bone-resorptive and regulatory cytokinesin murine periapical inflammation. Arch Oral Biol 1999;44:55–66.
24. Hahn CL, Liewehr FR. Innate immune responses of the dental pulp to caries. J Endod2007;33:643–51.
EBV and HCMV in Apical Periodontitis Lesions 1489

Clinical Research
Long-term Survival of Indirect Pulp Treatment Performedin Primary and Permanent Teeth with ClinicallyDiagnosed Deep Carious LesionsRene Gruythuysen, DDS, PhD, Guus van Strijp, DDS, PhD, and Min-Kai Wu, MSD, PhD
Abstract
Introduction: This retrospective study examined clini-cally and radiographically the 3-year survival of teethtreated with indirect pulp treatment (IPT) performedbetween 2000 and 2004. Methods: Sixty-six uncooper-ative children (4-18 years old) with at least one toothwith clinically diagnosed deep caries were included.Radiographically, the lesion depth was greater thantwo thirds of the dentin thickness. Incomplete excava-tion was performed leaving infected carious dentin atthe center of the cavity. After placement of a layer ofresin-modified glass ionomer as liner, the teeth wererestored. A 3-year survival analysis (Kaplan-Meier)was performed. Failure was defined as the presence ofeither a clinical symptom (pain, swelling, or fistula) orradiologic abnormality at recall. In total, 86 of 125(69%) treated primary molars and 34 of 45 (76%)treated permanent teeth were available for both clinicaland radiographic evaluation. Results: The survival ratewas 96% for primary molars (mean survival time, 146weeks) and 93% for permanent teeth (mean survivaltime, 178 weeks). Conclusion: This study showsthat IPT performed in primary and permanent teeth ofyoung patients may result in a high 3-year survivalrate. (J Endod 2010;36:1490–1493)Key WordsCaries detector, caries management, deep caries, indi-rect pulp capping, indirect pulp therapy, indirect pulptreatment, infected dentin, resin-modified glass ion-omer, ultraconservative caries treatment
From the Department of Cariology Endodontology Pedo-dontology Oral Microbiology, Academic Centre for DentistryAmsterdam, The Netherlands.
Address requests for reprints to Dr Rene Gruythuysen,Department of Cariology Endodontology Pedodontology OralMicrobiology, Academic Centre for Dentistry Amsterdam(ACTA). Gustav Mahlerlaan 3004, 1081 LA Amsterdam, TheNetherlands. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.006
1490 Gruythuysen et al.
The discussion of how much carious dentin must be removed in order to arrest thecarious process exists already more than 150 years (1). With reference to the
outcome of the histologic studies of Reeves and Stanley (2), infected dentine shouldbe completely removed in order to arrest the carious process. However, it has been re-ported that carious progression was arrested for at least 10 years when bonded, andsealed composite restorations were placed directly over frank cavitated lesions extend-ing into the dentin (3). Therefore, complete dentine carious removal may not bea prerequisite to arrest carious progression (4, 5). A randomized clinical trial withthe ‘‘Hall technique,’’ in which there is no carious excavation, showed that caries isa disease that will arrest in the right circumstances (6). Taking into account the bene-ficial outcome in five clinical studies (7), indirect pulp treatment (IPT) is recommendedas an appropriate procedure for treating primary teeth with deep carious lesions andasymptomatic pulp inflammation provided that the restoration seals the cavity properly.In summary, the traditional concept of complete carious removal has been challenged.
With IPT, carious dentin near the pulp is preserved to avoid pulp exposure and iscovered with a biocompatible material (8). Pulpal inflammation is inevitable once thedentin is affected. The remaining dentin thickness after carious excavation is a keydeterminant regarding the state of the pulp (9, 10). There is poor correlation,however, between the histologic findings and the clinical diagnosis of pulpal injury.Subjacent to deep carious lesions, the pulp presents chronic inflammatory exudates,including lymphocytes, macrophages, and plasma cells (11), indicating that pulpitishas been developed even in absence of unprovoked pain. On the other hand, formany years, the importance of inflammation in maintaining pulpal health has beenunderestimated. Inflammation was considered an undesirable side effect, frequentlyleading to pulp necrosis. In view of recent results, the inflammatory process shouldbe re-examined to understand its potentially beneficial effect on pulp regeneration(12). Despite extensive pulpal inflammation because of deep caries, a conservativeapproach can still generate a favorable prognosis for pulpal repair.
When pulp exposure has occurred during complete excavation in primary oryoung permanent teeth, (partial) pulpotomy is a treatment option for teeth diagnosedwith reversible pulpitis (7, 13). In case of symptoms referring to irreversible pulpitis,such as unprovoked pain, vital pulp techniques are associated with poor clinicaloutcomes. In those cases, vital pulpectomy is usually needed to save the tooth.Because of the difficulties in cleaning and filling morphologically complex root canalsystems, the placement of a root canal filling does not always prevent coronalbacterial contamination (14, 15). As a result, in some cases, periapical lesions mayemerge. In previous outcome studies and systematic reviews, the average successrate for root canal therapy performed in teeth with vital pulps is rather high (16–18). In Toronto studies, a success rate of 93% was recorded (17). Interestingly,many outcome studies reported both periapical index scores 1 and 2 as ‘‘healed’’ or‘‘successful’’ (17, 19) despite score 2 representing mild periapical inflammation(20). When score 2 would not be considered ‘‘successful,’’ the success rate for vitalteeth would drop to 70% (21). In animal studies (22–24), posttreatment apicalperiodontitis was present in a high percentage of teeth up to 12 months afterperforming vital pulpectomy.
Recent studies showed IPT-treated teeth remaining symptomless and free of radio-logic abnormalities for years (5, 7). The pulp maintains its healing potential and
JOE — Volume 36, Number 9, September 2010

Clinical Research
defence capacity against advancing carious lesions (25) and acts as thebest barrier against bacterial invasion (26). In addition, performance ofIPT is simpler, more patient friendly, and cheaper than a root canaltreatment.This retrospective study evaluated treatment success of deepcarious lesions in primary and permanent teeth. The purpose was toinvestigate the 3-year survival rate of functional (clinical and radiolog-ical successful) primary and permanent teeth treated with IPT.
Materials and MethodsStudy records were selected from a patient pool visiting the faculty
clinic of the Department of Cariology Endodontology Pedodontology ofAcademic Centre for Dentistry Amsterdam. Sixty-six children (40 boysand 26 girls, 4-18 years old) with at least one tooth with clinically diag-nosed deep caries were referred to one operator between 2000 and2004. IPT was performed in teeth that met the following criteria:
1. Restorable permanent and posterior primary teeth without a historyof spontaneous, persistent pain or sensitivity to palpation/percus-sion and/or presence of other clinical signs of inflammation(abscess, sinus tract, and abnormal mobility).
2. Radiographically, the absence of signs of periapical or furcationpathology and/or of pathological resorption. However, in 30% ofthe children, no appropriate preoperative radiograph could bemade because of limited cooperation.
3. Teeth at risk of pulp exposure when complete removal of cariousdentine would be performed.
In total, 125 primary molars and 45 permanent teeth (9 frontteeth, 8 premolars, and 28 molars) were treated with IPT. In primarymolars and permanent teeth, 79.1% and 41.2%, respectively, of therestorations comprised more than one surface. Patients’ cooperationdid not influence the indication for IPT. All patients with deep cariouslesions were treated consecutively. Pulpotomy was only performedwhen a vital pulp was exposed during the excavation procedure (esti-mated 5% of all deep carious lesions). Subsequently, the tooth wasexcluded from the study. In one primary tooth, pulp exposure led tothe diagnosis ‘‘pulp necrosis,’’ also resulting in exclusion from thestudy. Referring to the age of the children, about 20% to 30% of thepermanent teeth treated with IPT were immature at the start of treat-ment.
The criteria for radiographic evaluation were (1) the presence ofan appropriate posttreatment radiograph and (2) the lesion depth wasmore than two thirds of the dentin thickness assessed on a preoperativeradiograph or the restoration depth was greater than two thirds of thedentin thickness assessed on postoperative radiograph. Eighty-six(68.8%) of 125 primary molars and 34 (75.6%) of 45 permanent teethmet these criteria and were available for both clinical and radiologicevaluation.
In primary as well as permanent teeth, IPT was performed simi-larly. After administering local anesthesia and placing a rubber dam,the dentin-enamel junction was completely excavated. The biomassnear the pulp was removed with caution. In one in vivo study, specifictactile information was given about the carious removal procedure;excavation in deep cavities (with excavator) of primary molars wasstopped when the remaining dentin showed increased resistance tomanual instrumentation, coming out in scales or chips (27). The treat-ment protocol in the present study included also the use of a prophybrush to achieve this level of excavation. In order to remove the biomass(Fig. 1A) from the infected dentin, a spoon excavator (#153/154; AshLustra, Dentsply, Addlestone, UK) was used and/or a prophy brush(Screw type black brushes, Crescent, Dentsply Rinn, Elgin, IL; 2000
JOE — Volume 36, Number 9, September 2010 Indire
rpm) with fluoride toothpaste. The Caries Detector (Kuraray Co, Tokyo,Japan) applied in accordance with the manufacturer’s instructions wasused only to check the proper excavation of the dentin-enamel junction.Infected dentin, showing intact parts and dark red staining after appli-cation of the Caries Detector (Fig. 1B), was retained and covered bya layer of resin-modified glass ionomer (RMGI) liner (Vitrebond; 3MESPE, St. Paul, MN).
All permanent teeth were restored with adhesive filling materials(Z100 or Ketac-Molar, 3M ESPE). Nine primary teeth were restoredwith a preformed metal crown (Stainless Steel Crowns, 3M ESPE) ce-mented with glass ionomer (Ketac-Cem, 3M ESPE). All other primaryteeth were restored with adhesive filling materials (Dyract, DentsplyCaulk, York, PA, and Ketac-Molar, 3M ESPE).
Survival was defined as teeth without clinical or radiologic signs orsymptoms. The recall interval was 3 to 6 months depending on the levelof dental hygiene. At recalls, the clinical performance of the teeth wasexamined by percussion and palpation along with the presence of signsof inflammation (pain, abscess, sinus tract, and abnormal mobility).Treatment was considered radiologically successful when (1) thecontours width and structure of the periodontal margin were normaland (2) no signs of pathological tooth resorption were present. Pulpsensitivity tests could not be performed in many of the very young chil-dren, and test outcomes were not reliable in the anxious (older) chil-dren.
Radiographic treatment outcomes and chart notes for each toothwere independently reviewed by two calibrated investigators. Whenopinions differed, discussion was followed by consensus agreement.In case of doubt, the treatment was regarded as a failure. The Cohenkappa coefficient was used to assess the inter- and intraobserver agree-ment of the radiographic assessments.
Kaplan-Meier survival analyses were performed on the censoreddata of both primary and permanent teeth. Statistical analyses were per-formed using SPSS for Windows, version 12.0.1 (SPSS Inc, Chicago, IL).
ResultsThe assessment of the radiographs revealed an inter- and intraexa-
miner agreement of 0.72 and 0.80 (Cohen kappa), respectively. The 3-year survival analyses of IPT treatment, assessed radiographically,showed a survival rate of 96% for primary molars (2 failures; mean[standard deviation] survival time, 145.6 weeks [2.4 weeks]) and93% for permanent teeth (Fig. 2A-D) (1 failure; mean [standard devi-ation] survival time, 178.1 weeks [8.5 weeks]). Failures in primaryteeth were caused by intraradicular bone resorption. The permanenttooth failed because of apical bone resorption.
During the evaluation period, no clinical symptoms were observedin primary molars as well as permanent teeth referring to inflammationof the pulp. The approximal enamel wall of one primary and one perma-nent molar restored with a class I RMGI restoration fractured after 16months and 12 months, respectively. Repair of the restorations did notinfluence the survival of the teeth.
DiscussionThis study contributes to the debate among cariologists and endo-
dontologists whether IPT is a valuable approach to pulp preservation inteeth with deep carious lesions (28). The conservative child-friendlyIPT approach limits the discomfort for uncooperative children byreduced treatment time.
In the present study, deep carious lesions were defined as lesionscomprising more than two thirds of the dentin thickness. Pulp exposurecould be expected if direct complete excavation were pursued. Eitherpre- or postoperative radiographs were used to assure the lesion depth.
ct Pulp Treatment in Teeth with Clinically Diagnosed Deep Carious Lesions 1491

Figure 1. (A) A second mandibular primary molar after excavation of the dentin-enamel junction (DEJ). The biomass is still present in the center of the cavity. (B)The same tooth after removing the biomass with a prophy brush and fluoride toothpaste only. The Caries Detector was used for inspection of the DEJ. After drying thecavity, the RMGI liner was applied, and the cavity was restored with a compomer.
Clinical Research
Because no pulpal excavation was performed, lesion depth could alsobe assessed by postoperative radiographs.
As reported by Leksell et al (29) and Kassa et al (30), up to 50% ofdeep carious lesions may actually have severe pulp involvement. There-fore, it seems reasonable to assume that many teeth in the present studysuffered severe pulp involvement. Ninety-three percent of IPT-treatedpermanent teeth and 96% of primary molars remained neverthelesssymptomless and free of intraradicular/periapical radiolucency forup to 3 years. Future clinical investigations, using sophisticated diag-nostic tools (19), may provide more detailed information about theoutcomes of vital pulp techniques.
Pulpal necrosis can develop without clinical symptoms (11, 31). Alow incidence of pulpal necrosis after IPT was reported (5) for 1 (3%)of 32 IPT-treated teeth. In this study, using radiographic criteria, morethan 90% of the treated teeth remained free of apical radiolucency. Asreported in the present study and in other investigations (5, 7), clinicaloutcomes achieved by IPT, as treatment for asymptomatic pulpalinflammation, were not inferior to those of pulpectomy treatment(15, 21, 19). Recently, it has been questioned (19) whether the tradi-
Figure 2. (A) The first mandibular permanent tooth before IPT in a 6.5-year-old giIPT. (D) The first mandibular permanent tooth completely matured 5 years after I
1492 Gruythuysen et al.
tional strategy for treating deep caries (complete excavation resulting inpulp exposure and vital pulpectomy) still provides the best solution.Furthermore, in some cases with deep caries, without any pretreatmentsymptoms, spontaneous or persistent pain can develop after completeexcavation. A recent cohort study supports this view, reporting a greaterincidence of adverse events in deep cavities and pulpally exposed teeththan in teeth with moderately deep or shallow cavities (odds ratio =7.8) (9). Therefore, performing IPT may avoid or delay root canalinfection and thus root canal treatments.
An adequate sealing of the remaining infected dentine is of theutmost importance in the investigated treatment strategy (IPT) fordeep carious lesions. It has been shown that carious dentin beneatha restoration contains a decreasing number of viable bacteria overtime and ‘‘dries out’’ (5, 32), which is a parameter for lesion arrest(1, 5). In addition, a shift toward a less cariogenic microflora wasobserved (33). In another study (34), a more microorganisms weredetected in teeth submitted to partial carious removal compared withthe complete carious removal group. However, after sealing the cavity,the level of bacterial colonization was similar in the two groups (35).
rl. (B) The same (immature) tooth 1 week after IPT. (C) Almost 2.5 years afterPT (2 years after finishing the clinical evaluation).
JOE — Volume 36, Number 9, September 2010

Clinical Research
Underneath the restoration, a number of microorganisms may survivebut not in sufficient quantity to advance the disease or they are no longercarious active. Sealing of carious dentin arrested the carious process indeep carious lesions, promoted deposition of tertiary dentin, andinduced mineral gain in the radiolucent zone (36).Studies on stepwise excavation advocate removal of carious tissueafter the reaction of the pulpodentin complex after the first excavationstep (36, 37). This study supports the conclusion of Maltz et al (5) thatthe indication for reopening the cavity to remove remaining cariousdentin lacks biological support.
Calcium hydroxide is traditionally the material of choice in deepcarious treatment because of its alkaline biocompatible propertiesand the induction of pulpodentin remineralization. However, in a studyinvestigating the pulpodentin complex response to a RMGI liner appliedin deep cavities, this material was found to be biocompatible compa-rable to calcium hydroxide (38). This was confirmed in a 4-yearfollow-up study (39). Teeth were treated with an IPT techniquecombined with either a calcium hydroxide or RMGI liner. No significantdifference in success rate (89% and 93%, respectively) was found.Additionally and in contrast to calcium hydroxide, RMGI prevents mi-croleakage (40).
Since starting to perform IPT 10 years ago, we apply this approachin every patient (anxious or not) who presents with one or more deepcavities in vital primary or permanent teeth that meet the criteriadescribed in this study. Our 10-year experience with incomplete cariousexcavation confirms the results of the present study.
ConclusionsThe results of this retrospective study on the survival rate of
primary and permanent teeth after performing IPT are promising. Anestimated 96% of primary molars and 93% of permanent teeth survived3 years without showing adverse clinical symptoms or pathologicalsigns on traditional radiographs. Although studies with high-qualityresearch design are necessary to confirm the previously mentionedresults, the traditional strategy of complete carious removal to managedeep carious lesions in primary and permanent teeth with asymptomaticpulpitis may be questioned.
References1. Kidd EA. How ‘clean’ must a cavity be before restoration? Caries Res 2004;38:
305–13.2. Reeves R, Stanley HR. The relationship of bacterial penetration and pulpal pathosis
in carious teeth. Oral Surg Oral Med Oral Pathol 1966;22:59–65.3. Mertz-Fairhurst EJ, Curtis JW Jr, Ergle JW, et al. Ultraconservative and cariostatic
sealed restorations: results at year 10. J Am Dent Assoc 1998;129:55–66.4. Ricketts DN, Kidd EA, Innes N, et al. Complete or ultraconservative removal of de-
cayed tissue in unfilled teeth. Cochrane Database Syst Rev 2006;3:CD003808.5. Maltz M, Oliveira EF, Fontanella V, et al. Deep caries lesions after incomplete dentine
caries removal: 40-month follow-up study. Caries Res 2007;41:493–6.6. Innes NP, Evans DJ, Stirrups DR. The Hall technique; a randomized controlled clin-
ical trial of a novel method of managing carious primary molars in general dentalpractice: acceptability of the technique and outcomes at 23 months. BMC OralHealth 2007;7:18.
7. Fuks AB. Vital pulp therapy with new materials for primary teeth: new directions andtreatment perspectives. J Endod 2008;34:S18–24.
8. American Academy on Pediatric Dentistry Clinical Affairs Committee-Pulp Therapysubcommittee; American Academy on Pediatric Dentistry Council on Clinical Affairs.Guideline on pulp therapy for primary andyoung permanent teeth. Pediatr Dent2008-2009;30(7 suppl):170–174.
9. Whitworth JM, Myers PM, Smith J, et al. Endodontic complications after plasticrestorations in general practice. Int Endod J 2005;38:409–16.
10. Murray PE, Smith AJ, Garcia-Godoy F, et al. Comparison of operative procedure vari-ables on pulpal viability in an ex vivo model. Int Endod J 2008;41:389–400.
JOE — Volume 36, Number 9, September 2010 Indire
11. Bjørndal L, Mjor IA. Pulp-dentin biology in restorative dentistry. Part 4: dentalcaries—characteristics of lesions and pulpal reactions. Quintessence Int 2001;32:717–36.
12. Goldberg M, Farges JC, Lacerda-Pinheiro S, et al. Inflammatory and immunologicalaspects of dental pulp repair. Pharmacol Res 2008;58:137–47.
13. Barrieshi-Nusair KM, Qudeimat MA. A prospective clinical study of mineral trioxideaggregate for partial pulpotomy in cariously exposed permanent teeth. J Endod2006;32:731–5.
14. Moller AJ. Microbiological examination of root canals and periapical tissues ofhuman teeth. Methodological studies. Odontol Tidskr 1966;74(suppl):1–380.
15. Molander A, Reit C, Dahlen G, et al. Microbiological status of root-filled teeth withapical periodontitis. Int Endod J 1998;31:1–7.
16. Sjogren U, Hagglund B, Sundqvist G, et al. Factors affecting the long-term results ofendodontic treatment. J Endod 1990;16:498–504.
17. Marquis VL, Dao T, Farzaneh M, et al. Treatment outcome in endodontics: the Tor-onto Study. Phase III: initial treatment. J Endod 2006;32:299–306.
18. Ng YL, Mann V, Rahbaran S, et al. Outcome of primary root canal treatment: system-atic review of the literature—part 2. Influence of clinical factors. Int Endod J 2008;41:6–31.
19. Wu MK, Shemesh H, Wesselink PR. Limitations of previously published systematicreviews evaluating the outcome of endodontic treatment. Int Endod J 2009;42:656–66.
20. Orstavik D, Kerekes K, Eriksen HM. Clinical performance of three endodonticsealers. Endod Dent Traumatol 1987;3:178–86.
21. Ørstavik D, Qvist V, Stoltze K. A multivariate analysis of the outcome of endodontictreatment. Eur J Oral Sci 2004;112:224–30.
22. Holland GR. Periapical innervation of the ferret canine one year after pulpectomy.J Dent Res 1992;71:470–4.
23. Katebzadeh N, Hupp J, Trope M. Histological periapical repair after obturation ofinfected root canals in dogs. J Endod 1999;25:364–8.
24. Garcia de Paula-Silva FW, Hassan B, Bezerra da Silva LA, et al. Outcome of root canaltreatment in dogs determined by periapical radiography and cone-beam computedtomography scans. J Endod 2009;35:723–6.
25. Simsxek S, Duruturk L. A flow cytometric analysis of the biodefensive response ofdeciduous tooth pulp to carious stimuli during physiological root resorption.Arch Oral Biol 2005;50:461–8.
26. Ricucci D, Langeland K. Apical limit of root canal instrumentation and obturation,part 2. A histological study. Int Endod J 1998;31:394–409.
27. Massara ML, Alves JB, Brandao PR. Atraumatic restorative treatment: clinical, ultra-structural and chemical analysis. Caries Res 2002;36:430–6.
28. Seale NS, Glickman GN. Contemporary perspectives on vital pulp therapy: views fromthe endodontists and pediatric dentists. J Endod 2008;34(7 suppl):S57–61.
29. Leksell E, Ridell K, Cvek M, et al. Pulp exposure after stepwise versus direct completeexcavation of deep carious lesions in young posterior permanent teeth. Endod DentTraumatol 1996;12:192–6.
30. Kassa D, Day P, High A, et al. Histological comparison of pulpal inflammation inprimary teeth with occlusal or proximal caries. Int J Paediatr Dent 2009;19:26–33.
31. Bergenholtz G, Nyman S. Endodontic complications following periodontal and pros-thetic treatment of patients with advanced periodontal disease. J Periodontol 1984;55:63–8.
32. Bjørndal L, Larsen T. Changes in the cultivable flora in deep carious lesionsfollowing a stepwise excavation procedure. Caries Res 2000;34:502–8.
33. Paddick JS, Brailsford SR, Kidd EA, et al. Phenotypic and genotypic selection of mi-crobiota surviving under dental restorations. Appl Environ Microbiol 2005;71:2467–72.
34. Lula EC, Monteiro-Neto V, Alves CM, et al. Microbiological analysis after complete orpartial removal of carious dentin in primary teeth: arandomized clinical trial. CariesRes 2009;43:354–8.
35. Alves LS, Fontanella V, Damo AC, et al. Qualitative and quantitative radiographicassessment of sealed carious dentin: a 10-year prospective study. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2010;109:135–41.
36. Magnusson BO, Sundell SO. Stepwise excavation of deep carious lesions in primarymolars. J Int Assoc Dent Child 1977;8:36–40.
37. Bjørndal L, Larsen T, Thylstrup A. A clinical and microbiological study of deepcarious lesions during stepwise excavation using long treatment intervals. CariesRes 1997;31:411–7.
38. Costa CA, Giro EM, do Nascimento AB, et al. Short-term evaluation of the pulpo-dentin complex response to a resin-modified glass-ionomer cement and a bondingagent applied in deep cavities. Dent Mater 2003;19:739–46.
39. Marchi JJ, de Araujo FB, Froner AM, et al. Indirect pulp capping in the primarydentition: a 4 year follow-up study. J Clin Pediatr Dent 2006;31:68–71.
40. Pereira CL, Cenci MS, Demarco FF. Sealing ability of MTA, Super EBA, Vitremer andamalgam as root-end filling materials. Braz Oral Res 2004;18:317–21.
ct Pulp Treatment in Teeth with Clinically Diagnosed Deep Carious Lesions 1493

Clinical Research
Frequency of Nonodontogenic Pain after EndodonticTherapy: A Systematic Review and Meta-AnalysisDonald R. Nixdorf, DDS, MS,*† Estephan J. Moana-Filho, DDS, MS,‡ Alan S. Law, DDS, PhD,§
Lisa A. McGuire, MLIS,k
James S. Hodges, PhD,¶
and Mike T. John, DDS, MPH, PhD**
Abstract
Introduction: Little is known about ill-defined pain thatpersists after endodontic procedures, including an esti-mate of the problem’s magnitude. We conducteda systematic review of prospective studies that reportedthe frequency of nonodontogenic pain in patients whohad undergone endodontic procedures. Methods: Non-odontogenic pain was defined as dentoalveolar painpresent for 6 months or more after endodontic treatmentwithout evidence of dental pathology. Endodontic proce-dures reviewed were nonsurgical root canal treatment,retreatment, and surgical root canal treatment. Studieswere searched in four databases electronically, comple-mented by hand searching. A summary estimate of non-odontogenic tooth pain frequency was derived usingrandom-effects meta-analysis. Results: Of 770 articlesretrieved and reviewed, 10 met inclusion criteria, andnine had data on both odontogenic and nonodontogeniccauses of pain. A total of 3,343 teeth were enrolledwithin the included studies and 1,125 had follow-upinformation regarding pain status. We identified 48teeth with nonodontogenic pain and estimated a 3.4%(95% confidence interval, 1.4%-5.5%) frequency ofoccurrence. In nine articles containing data regardingboth odontogenic and nonodontogenic causes of toothpain, 56% (44/78) of all cases were thought to havea nonodontogenic cause. Conclusions: Nonodonto-genic pain is not an uncommon outcome after root canaltherapy and may represent half of all cases of persistenttooth pain. These findings have implications for the diag-nosis and treatment of painful teeth that were previouslyroot canal treated because therapy directed at the toothin question would not be expected to resolve nonodon-togenic pain. (J Endod 2010;36:1494–1498)Key WordsDentoalveolar, pain, root canal therapy, systematicreview, tooth
From the *Division of TMD & Orofacial Pain, School of Dentistry, UMinnesota, Minneapolis, MN; ‡Center for Neurosensory Disorders, SSpecialists, Lake Elmo, MN; kBio-Medical Library, University of MinneMinneapolis, MN; and **Division of Epidemiology & Community He
Supported by National Institutes of Health grants: K12-RR02324Address requests for reprints to Dr Donald Nixdorf, University of
[email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.020
1494 Nixdorf et al.
Tooth pain, meaning pain of known pulpal or periradicular etiology, is not the onlyreason for pain perceived in the dentoalveolar regions (1). Nonodontogenic causes
comprise varying etiologies, such as referred myofascial pain (2), headache (3),neuropathic disorders (4), and pain stemming from various pathological conditions(5). Quantifying the frequency of nonodontogenic pain after root canal therapy isimportant for dentists and patients, so patients can make educated decisions byknowing the risks and benefits associated with treatment. Determining the extent ofthis problem is the first step toward the long-term goal of reducing diagnostic errorsthat often lead to irreversible dental procedures in an attempt to alleviate the pain, suchas root canal retreatments, surgical root canal treatments, and tooth extractions (6).
Several studies have investigated the component diagnoses, listed earlier, thatcomprise this group of nonodontogenic pain cases referred to tertiary care centers(5, 7, 8). Even though such pain is thought to be ‘‘rare’’ (9), the magnitude of thisproblem is not known to a degree that would allow for development of appropriatepublic health policy. Important subtypes of this pain are not quantified either, especiallythose pains thought to be neuropathic in nature. For patients and dentists alike, theyrepresent a considerable challenge because they are known to respond less than favor-ably to treatment (10). Given the current situation (ie, multiple diagnoses comprisingthis group of nonodontogenic pain that have widely differing treatment needs), it isimportant to quantify this problem to inform clinicians so they can use this informationin their daily practice. Therefore, we sought to estimate the frequency of nonodonto-genic dentoalveolar pain present at 6 months or greater after root canal therapy by per-forming a meta-analysis, which is a robust method of synthesizing publishedinformation (11).
Materials and MethodsInclusion Criteria
Eligible for inclusion in this review were endodontic procedure articles publishedin any language before June 5, 2009, that reported on postoperative tooth pain after atleast a 6-month follow-up. Qualifying endodontic procedures included initial root canaltreatment or retreatment, surgical or nonsurgical, but not pulpotomy, partial pulpec-tomy, or pulp capping. The unit of observation considered was a human permanenttooth in vivo; primary teeth were excluded. The study outcome was the presence ofdentoalveolar pain that explicitly did not have an odontogenic etiology, such asa cracked tooth, missed canal, or periapical pathosis. Pain could be spontaneous orprovoked by biting, palpation, or percussion.
niversity of Minnesota, Minneapolis, MN; †Department of Neurology, Medical School, University ofchool of Dentistry, University of North Carolina, Chapel Hill, NC, USA; §Private Practice, The Dentalsota, Minneapolis, MN; ¶Division of Biostatistics, School of Public Health, University of Minnesota,alth, School of Public Health, University of Minnesota, Minneapolis, MN.7, U01-DE016746 and U01-DE016747 (DR Nixdorf).Minnesota, 6-320 Moos Tower, 515 Delaware Street SE, Minneapolis, MN 55455. E-mail address:
JOE — Volume 36, Number 9, September 2010

Clinical Research
Another inclusion criterion for studies was that they reportedbaseline data of the population from which the follow-up sample wasdrawn. This requirement, allowing the frequency of occurrence to becalculated, limited study inclusion to case series, cohort, and clinicaltrial studies and excluded cross-sectional and case-control studies. Arti-cles reporting randomized trials were included as a special type ofprospective cohort study; however, the treatment arms were collapsedfor our analysis. Unpublished research and studies reported only inabstract form were not considered.
Information Sources and Search StrategyWe conducted an initial search in MEDLINE via the PubMed inter-
face, covering the period from 1949 to June 5, 2009, and using thesearch terms specified in Figure 1. This search was then adapted foruse and run in the Cochrane Library, TRIP database, and GoogleScholar. We also hand searched the references of prominent articles,literature reviews, and textbook chapters (source list available uponrequest). Our intent was to be broad in scope to ensure the inclusionof as much relevant existing data as reasonably possible. The trainingand reliability assessment of article selection, data abstraction of studyvariables, and the assessment of reported study quality have been previ-ously reported (12).
Statistical MethodsWe used random-effects meta-analysis (13) to determine
a summary estimate of nonodontogenic pain frequency. In a sensitivityanalysis, we examined whether the deletion of a single study substan-tially changed the meta-analysis summary estimate. To explore factorsinfluencing the estimate, we performed a meta-regression to investigatedifferences between studies with the following characteristics: (1)surgical versus nonsurgical treatment, (2) a follow-up rate of recallless than 50% versus greater than or equal to 50%, (3) follow-up at6 to 12 months versus more than 12 months, (4) initial treatment versusretreatment, and (5) above-median quality reporting score versusbelow-median score according to the STROBE criteria (12, 14). Wealso estimated the proportion of nonodontogenic tooth pain amongthe subset of cases that had information on both ‘‘all-cause’’ andnonodontogenic pain. All analyses were performed using the STATAsoftware package (Stata Statistical Software: Release 10.1; StataCorpLP, College Station, TX: StataCorp LP) and the user-written metan andmetareg commands.
Figure 1. A flowchart of the systematic review process.
JOE — Volume 36, Number 9, September 2010
ResultsStudy Identification and Characteristics
We identified 770 articles (495 by electronic searching of data-bases and 275 by hand searching); the oldest was published in 1921.Twenty-eight were published in a language other than English (7French; 6 Chinese; 5 Japanese; 2 each in Italian, Russian, and Spanish;and 1 each in Croatian, Danish, German, and Greek). Screening of titlesand abstracts resulted in 306 articles being excluded. After full-textreview, another 464 articles were excluded, so 10 articles wereincluded in the meta-analysis (Fig. 1). All 10 articles were publishedin English, and 6 of them were identified by hand searching.
The 10 included studies varied in the types of endodontictreatments provided, numbers of teeth treated (6-276), duration offollow-up (1-6 years), and the percentage of teeth followed up(20%-100%) (Table 1). From 3,343 teeth enrolled in the 10 studies,1,125 teeth were followed up for at least 6 months. Among them, 48teeth (4.3%) in seven studies were reported to have pain without anidentifiable odontogenic source. In these studies, teeth were deter-mined to have tooth-related disease when the tooth was presentand ‘‘not properly restored,’’ ‘‘fractured,’’ periapical radiolucencypresent (15, 16), sinus tract present (17), ‘‘root fracture associatedwith severe bone loss’’ (18), and ‘‘failure of coronal restoration’’(19) could be identified with the root canal–treated teeth. Variationin the quality of reporting (STROBE criteria) was observed (inter-quartile range = 8.5-20.5, range = 5-20.5), with a median reportingquality score of 19.8 (possible scores ranging from 0 to 22). Further-more, 9 studies contained details on both ‘‘all-cause’’ pain and non-odontogenic pain, making it possible to calculate the proportion ofsuch pain outcomes.
Summary Estimate of Nonodontogenic Pain FrequencyThe meta-analytic summary estimate of nonodontogenic pain
frequency was 3.4% (95% confidence interval, 1.4%-5.5%, Fig. 2).‘‘Moderate’’ heterogeneity (ie, inconsistency) (20) among study esti-mates was observed (I2 = 65%, p = 0.002). When each study was elim-inated in turn from the analysis and the meta-analysis was run with thenine remaining studies, the summary estimates ranged from 2.1% to4.2%. Thus, individual studies did not unduly influence the summaryestimate even though one study identified 21 of the 48 cases (44%)of nonodontogenic pain.
Exploration of Study HeterogeneityIn meta-regression analyses (Table 2), follow-up duration was
the factor that differentiated pain frequency the most; the three studieswith a follow-up of 6 to 12 months had a frequency of persistent non-odontogenic pain higher by 4.5 percentage points than in the sevenstudies with a follow-up greater than 12 months. The study reportingquality affected pain frequency the least; the five above-medianSTROBE criteria studies had a frequency of persistent nonodontogenicpain higher by 1.5 percentage points than in the five below-medianstudies. However, even when differences were substantial in magni-tude, all were statistically nonsignificant because of small numbersof studies.
Proportion of ‘‘All-Cause’’ Pain That Is NonodontogenicNine studies had data for ‘‘all-cause’’ tooth pain, as previously re-
ported (12), as well as for nonodontogenic pain, thus allowing an esti-mation of the proportion of such pain outcomes in each studypopulation. In these 9 studies, 44 nonodontogenic pain cases (56%)of the 78 ‘‘all-cause’’ pain cases were identified.
Frequency of Nonodontogenic Pain after Endodontic Therapy 1495

TABLE1.
Char
acte
rist
ics
ofth
e10
stud
ies
incl
uded
inth
em
eta-
anal
ysis
Au
tho
rs,
Yea
rEn
do
do
nti
cP
roce
du
reTe
eth
Enro
lled
Foll
ow
-up
,n
(%)
No
no
do
nto
gen
icTo
oth
Pai
nM
ult
iple
Pro
ced
ure
sFo
llo
w-u
p(y
)ST
RO
BE
Rat
ing
Liu
an
dSi
dh
u,1995
Init
ialN
SRC
T6
6(1
00)
00
1-3
.55
Dan
inet
al,
1999*
Peri
ap
icalSu
rgery
10
10
(100)
00
1-1
10.7
von
Arx
an
dK
urt
,1999
Peri
ap
icalSu
rgery
50
43
(86)
17
1-1
8Fa
rzan
eh
et
al,
2004a
*R
etr
eatm
en
tN
SRC
T523
103
(20)
079
4-6
20.5
Farz
an
eh
et
al,
2004b
*In
itia
lN
SRC
T442
122
(28)
371
4-6
20.5
Po
lyca
rpo
uet
al,
2005
Co
mb
ined
Treatm
en
ts400
†175
(44)
21
0†
1-1
20
Marq
uis
et
al,
2006*
Init
ialN
SRC
T532
131
(25)
764
4-6
19.5
de
Ch
evi
gn
yet
al,
2008a*
Init
ialN
SRC
T582
137
(24)
671
4-6
20.5
de
Ch
evi
gn
yet
al,
2008b
*R
etr
eatm
en
tN
SRC
T477
122
(26)
694
4-6
20.5
Sau
nd
ers
et
al,
2008
Peri
ap
icalSu
rgery
321
276
(86)
40
6-6
8.5
Ag
gre
gate
valu
es:
3,3
43
1,1
25
(37)
48
386
1-6
19.8
NSR
CT,
nons
urgi
cal
root
cana
lth
erap
y.
*Ref
eren
cefo
und
byha
ndse
arch
ing.
†As
sum
edth
atea
chpa
tient
cont
ribu
ted
only
one
toot
hbe
caus
eno
tex
plic
itly
stat
ed.
Figure 2. Random effects meta-analysis of the frequency of nonodontogenictooth pain in 10 studies.
Clinical Research
1496 Nixdorf et al.
DiscussionThis systematic review identified 10 prospective studies (3,343
enrolled teeth) and estimated the frequency of nonodontogenic painat 6 months or more after root canal treatment to be 3.4% (95% confi-dence interval, 1.4%-5.5%). At this rate, with more than 16.4 millionroot canal treatments performed annually in the United States (21),each year over half a million endodontic patients would be at risk fornonodontogenic pain.
Nonodontogenic dentolalveolar pain is often difficult to diagnose(5, 8) because it is poorly understood (22). Even defining and catego-rizing such persistent pain is challenging, but conceptually nonodonto-genic pain in the dentoalveolar region can arise from four potentialprocesses: (1) referred musculoskeletal pain disorder, (2) neuro-pathic pain disorder, (3) headache disorders presenting in the dentoal-veolar region, and (4) a pathological process outside the immediatedentoalveolar region that refers pain to that area, such as sinus disease,salivary gland disorders, brain tumors, angina, throat cancer, andcraniofacial vascular disorders (1).
In theory, our nonodontogenic pain frequency estimate is an esti-mate of the incidence of this condition. In practice, because the condi-tion is challenging to diagnose, misclassification at baseline by failing toidentify a nonodontogenic reason for pain results in the inclusion ofsuch cases in the reported studies. Misclassified neuropathic pain casesat baseline would be expected to continue to be painful after endodontictreatment (9) or become more recalcitrant (23), whereas nonodonto-genic cases of referred pain from distant tissues, such as musculoskel-etal, pathological, and headache disorders, would likely not beadequately addressed with endodontic treatment. The amount ofmisclassification is not known because to our knowledge such researchresults have not been reported. Furthermore, because patients under-going endodontic treatment commonly exhibit preexisting dentoalveo-lar pain of inflammatory origin (24), this study cannot differentiatebetween patients whose nonodontogenic pain arose from preexistingpathosis and patients whose pain arose from the procedure. Therefore,our estimate represents a mixture of truly incident and remissive casesas well as maintenance of the condition in patients misclassified at base-line. For this reason, we call this estimate a frequency of occurrence,which quantifies the burden of nonodontogenic pain, a conditionwith many clinical challenges.
JOE — Volume 36, Number 9, September 2010

TABLE 2. The assessment of study heterogeneity by meta-regression
Comparison of SubgroupsCoefficient
(Standard Error) p Value
Surgical treatment vsnonsurgical treatment
�2.7% (2.7) 0.36
$50% follow-up rate vs<50% follow-up rate
�2.8% (2.7) 0.34
>12 months vs 6-12 monthsfollow-up duration
�4.5% (2.6) 0.13
Retreatment vs initialtreatment*
�2.3% (2.1) 0.35
Above-median vs below-median reported studyquality (STROBE criteria)
1.5% (2.6) 0.57
*Four studies with missing data.
Clinical Research
The meta-analytic approach allows aggregation of data to producea robust estimate (11) but has known limitations based on the quality ofthe studies included (25, 26). Therefore, we restricted our meta-analysis to prospective studies, which are thought to produce moreaccurate results in general (27) and to endodontic outcome studiesin particular (12). Seven of the 10 studies identified were publishedin the last decade, suggesting an increased interest in reportingpatient-oriented outcomes and more design rigor in recent endodonticstudies. Only one study assessed nonodontogenic pain as its primaryoutcome. This study found a frequency of occurrence of 12% (21/175) (15), a number substantially higher than our meta-analysissummary, which may therefore suggest that our meta-analytic summaryestimate is low.
In exploratory analyses, studies with a shorter follow-up (6-12months) had a greater frequency of persistent nonodontogenic painthan those with a longer follow-up, which is an important finding(28) and may suggest that such persistent pain improves with time. Areduced frequency of persistent postprocedural pain over time hasbeen observed by other studies investigating nondental surgical modelsof human pain, such as cesarean sections (29), and has been suggestedto occur with orofacial pains (23) but has not been explored in relationto endodontic procedures.
A methodologic problem of our review was that the reporting unitwas the tooth, whereas the outcome of persistent dentoalveolar pain isa patient-based measure. Teeth within the same individual do not repre-sent statistically independent observations because they share the sameenvironment, so confidence intervals for our point estimates should belarger than presented. However, we believe that this is not likely a majorproblem because even though 6 studies reported multiple observationsper patient, the difference between the number of patients and the totalnumber of teeth was low (12%; 386/3,343). Another important issue inthis review was the large proportion of patients that were not followed(67%; 2,218/3,343), which allows ample opportunity for missing casesof nonodontogenic pain. This is potentially troubling becauseendodontic patients have been found not to inform their endodontistwhen persistent pain is present (30). This is not supported by ourmeta-regression, which found that studies with less than 50% follow-up rates had higher pain frequencies than those with greater than orequal to 50% follow-up rates. This finding, although not statisticallysignificant, is contrary to the common view. Caution needs to be usedwhen interpreting such results because these assessments are explor-atory and do not take into account that of the 6 studies having greaterthan 50% follow-up rate, four had the lowest STROBE scores, and theabove-median STROBE criteria studies had higher frequenciescompared with the below-median half.
Our meta-analysis provides some insight about the proportion ofpersistent pain after endodontic procedures that is nonodontogenic in
JOE — Volume 36, Number 9, September 2010
nature. Combining the present study’s finding with our previous studythat estimated the frequency of ‘‘all-cause’’ tooth pain to be 5.3%(12), nonodontogenic cases may account for 64% (3.4/5.3) of theseteeth with pain. When comparing the proportion of patients exhibitingnonodontogenic pain among those determined to have all-cause pain inthe 9 studies with available data, the proportion was 56% (44/78).When we use the best single study to assess this proportion (ie, the studythat used nonodontogenic pain as its primary outcome [15]), this frac-tion was 57% (21/37). This suggests that at least half of all persistenttooth pain is of nonodontogenic nature, so these cases would best bemanaged without further endodontic therapy. This is contrary to currentopinion (31-34) and practice (9) in dentistry, which advocates retreat-ment. Regardless of the recommended approach to treat pain afterendodontic care, the large proportion of nonodontogenic pain hassubstantial implications for diagnoses and further treatment of thesepain conditions.
In conclusion, 3.4% of patients experienced persistent pain ofnonodontogenic origin after root canal therapy, a number that likelyrepresents about half of all persistent ‘‘tooth’’ pain. Therefore, theoutcome of nonodontogenic tooth pain is not as rare as commonlyassumed. Given that nonodontogenic pain has diverse etiologies andsuccessful treatment is often difficult, further research is needed to diag-nose nonodontogenic pain subtypes, quantify the burden on the indi-vidual experiencing it, provide adequate treatment, and assess long-term outcomes. Also needed is research that differentiates cases of non-odontogenic pain from those of a local etiology because tooth-basedpathology is amenable to endodontic retreatment and nonodontogenicpain would be best treated if recognized.
AcknowledgmentsThe authors thank Estelle Arnaud-Battandier, David Bereiter,
Dino Bilankov, Zheng Chang, Wenjung Kang, Sergey Khasabov,Thomas List, Keiichiro Okamoto, Akimasa Tashiro, and Ana Vellyfor translating articles.
References1. Mattscheck D, Law AS, Nixdorf DR. Diagnosis of non-odonogentic toothache. In:
Hargreaves KM, Cohen S, eds. Cohen’s pathways of the pulp. 10th ed. St. Louis,MO: Mosby Inc; 2011:49–70.
2. Wright EF. Referred craniofacial pain patterns in patients with temporomandibulardisorder. JAMA 2000;131:1307–15.
3. Alonso AA, Nixdorf DR. Case series of four different headache types presenting astooth pain. J Endod 2006;32:1110–3.
4. Baad-Hansen L. Atypical odontalgia—pathophysiology and clinical management.J Oral Rehabil 2008;35:1–11.
5. Israel HA, Ward JD, Horrell B, et al. Oral and maxillofacial surgery in patients withchronic orofacial pain. J Oral Maxillofac Surg 2003;61:662–7.
6. Linn J, Trantor I, Teo N, et al. The differential diagnosis of toothache from otherorofacial pains in clinical practice. Aust Dent J 2007;52:S100–4.
7. Fricton JR. Critical commentary 1—a unified concept of idiopathic pain: Clinicalfeatures. J Orofac Pain 1999;13:185–9.
8. de Siqueira SRDT, Nobrega JCM, Valle LBS, et al. Idiopathic trigeminal neuralgia:clinical aspects and dental procedures. Oral Surg Oral Med Oral Path Oral Rad En-dod 2004;98:311–5.
9. Oshima K, Ishii T, Ogura Y, et al. Clinical investigation of patients who developneuropathic tooth pain after endodontic procedures. J Endod 2009;35:958–61.
10. Lewis MAO, Sankar V, De Laat A, et al. Management of neuropathic orofacial pain.Oral Surg Oral Med Oral Path Oral Rad and Endod 2007;103(suppl 1). S32.e1,S32.e24.
11. Borenstein M, Hedges LV, Higgins JPT, et al. Introduction to meta-analysis. Padstow,UK: John Wiley & Sons, Ltd; 2009.
12. Nixdorf DR, Moana-Filho EJ, Law AS, et al. Frequency of persistent tooth pain afterroot canal therapy: a systematic review and meta-analysis. J Endod 2010;36:224–30.
13. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88.
Frequency of Nonodontogenic Pain after Endodontic Therapy 1497

Clinical Research
14. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting ofobservational studies in epidemiology (STROBE): explanation and elaboration.Ann Intern Med 2007;147:W163–94.
15. Polycarpou N, Ng YL, Canavan D, et al. Prevalence of persistent pain after endodontictreatment and factors affecting its occurrence in cases with complete radiographichealing. Int Endod J 2005;38:169–78.
16. de Chevigny C, Dao TT, Basrani BR, et al. Treatment outcomes in endodontics: theToronto study—phases 3 and 4: orthograde retreatment. J Endod 2008;34:131–7.
17. Farzaneh M, Abitbol S, Lawrence HP, et al. Treatment outcome in endodontics—theToronto study. Phase II: initial treatment. J Endod 2004;30:302–9.
18. Marquis VL, Dao T, Farzaneh M, et al. Treatment outcome in endodontics: the Tor-onto study. Phase III: initial treatment. J Endod 2006;32:299–306.
19. Sanders A, Slade GD, Lim S, et al. Impact of oral disease on quality of life in the USand Australian populations. Community Dent Oral Epidemiol 2009;37:171–81.
20. Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses.BMJ 2003;327:557–60.
21. American Dental Association. Survey of dental services rendered and distribution ofdentists in the United States by region and state, 1999. Chicago, IL: American DentalAssociation; 2002.
22. Quail G. Atypical facial pain—a diagnostic challenge. Aust Fam Physician 2005;34:641–5.23. Allerbring M, Haegerstam G. Chronic idiopathic orofacial pain. A long-term follow-
up study. Acta Odontol Scand 2004;62:66–9.24. Fouad A, Levin L. Pupal reactions to caries and dental procedures. In:
Hargreaves KM, Cohen S, eds. Cohen’s Pathways of the Pulp. 10th ed. St. Louis,MO: Mosby, Inc; 2011:504–28.
1498 Nixdorf et al.
25. Moles DR, Needleman IG, Niederman R, et al. Introduction to cumulative meta-analysis in dentistry: lessons learned from undertaking a cumulative meta-analysis in periodontology. J Dent Res 2005;84:345–9.
26. Spangberg LSW. Systematic reviews in endodontics—examples of GIGO? Oral SurgOral Med Oral Path Oral Rad Endod 2007;103:723–4.
27. Cummings SR, Newman TB, Hulley SB. Designing a cohort study. In: Cummings SR,Newman TB, Hulley SB, eds. Designing Clinical Research. 3rd ed. Philadelphia, PA:Lippincott, Williams & Wilkins; 2007:97–107.
28. Savitz DA. Integration of evidence across studies. In: Interpreting EpidemiologicalEvidence: Strategies for Study Design and Analysis. New York, NY: Oxford UniversityPress; 2003:261–83.
29. Nikolajsen L, Sorensen HC, Jensen TS, et al. Chronic pain following Caesareansection. Acta Anaesthesiol Scand 2004;48:111–6.
30. Lobb WK, Zakariasen KL, McGrath PJ. Endodontic treatment outcomes: do patientsperceive problems? J Am Dent Assoc 1996;127:597–600.
31. Abbott PV. Factors associated with continuing pain in endodontics. Aust Dent J 1994;39:157–61.
32. Cohn SA. Clinical update—the teeth and the maxillary sinus: the mutual impact ofclinical procedures, disease conditions and their treatment implications. Part 1. Thedifferential diagnosis of tooth sinus pain—the dentist’s view. Aust Endod J 1999;25:29–31.
33. Boucher Y, Sobel M, Sauveur G. Persistent pain related to root canal filling andapical fenestration: a case report. J Endod 2000;26:242–4.
34. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review.J Endod 2006;32:601–23.
JOE — Volume 36, Number 9, September 2010

Basic Research—Biology
Regulation of the Stromal Cell–derived Factor-1a–CXCR4Axis in Human Dental Pulp CellsQi-mei Gong, MS, Jing-jing Quan, MS, Hong-wei Jiang, PhD, and Jun-qi Ling, PhD
Abstract
Introduction: Although the presence of the stromalcell–derived factor (SDF)-1a–CXCR4 axis has been re-ported in dental pulp tissue, little has been known aboutthe underlying regulation of this axis in dental pulp stemcells (DPSCs). The purpose of this study was to investi-gate whether inflammation or hypoxia can regulatethis axis in cultured human dental pulp cells (DPCs).Methods: Primary cultures of DPCs were stimulatedby various concentrations of lipopolysaccharide (LPS)for 48 hours, and the production of SDF-1a or CXCR4was assessed through the enzyme-linked immunosor-bent assay and Western blotting, respectively. Addition-ally, DPCs were incubated in a hypoxic condition (1%O2) for 24 hours, and the cell proliferation ability was de-tected by methylthiazol tetrazolum assay. Quantitativereverse-transcription polymerase chain reaction (RT-PCR) was used to observe messenger RNA level changesof hypoxia inducible factor-1a(HIF-a), SDF-1a, andCXCR4. The effects of hypoxia on cell migration abilitywere further confirmed by transmigration assay.Results: All concentrations of LPS inhibited SDF-1aproduction except that 1 mg/mL LPS increased theexpression of CXCR4. Hypoxia promoted the prolifera-tion of DPCs in a 24-hour culture period. QuantitativeRT-PCR showed that messenger RNA levels of HIF-a and CXCR4 increased, whereas SDF-1a decreased inhypoxic DPCs. Transmigration assay indicated thathypoxia increased the migration ability of DPCs.Conclusions: These results suggested that inflamma-tion and hypoxia might play an important role in regu-lating the SDF-1a-CXCR4 axis, which further recruitsDPSCs to participate in reparative dentinogenesis. (J En-dod 2010;36:1499–1503)
Key WordsCXC chemokine receptor 4, dental pulp cells, hypoxia-induced factor-1a, pulp regulation, stromal cell–derivedfactor-1a
From the Department of Operative Dentistry and Endodontics, GUniversity, Guangzhou, Guangdong, China.
Qi-mei Gong and Jing-jing Quan contributed equally to this studSupported by the Specialized Research Fund for the Doctoral PrAddress requests for reprints to Dr Jun-qi Ling, Department of O
University, Guangzhou 510055, PR China. E-mail address: lingjq@m0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.011
JOE — Volume 36, Number 9, September 2010
Dental pulp tissue has the ability to regenerate dentin in response to tooth injuriescaused by trauma or infection. This regeneration process is also known as repar-
ative dentinogenesis, and its typical pathological feature is the formation of tertiarydentin, which results from the recruitment and proliferation of dental pulp stem cells(DPSCs) (1). After damage of the tooth, these progenitor cells will be activated tomigrate to the injury sites and differentiate into odontoblast-like cells, which synthesizeand excrete an extracellular matrix to form the reparative dentin. Until now, many typesof signal molecules have been shown to be involved in this complex process.
Stromal cell–derived factor 1a (SDF-1a), a member of the chemokine family,with its receptor, CXC chemokine receptor 4 (CXCR4), forms the SDF-1a/CXCR4axis. The primary role of this axis is to mobilize CD34+ hematopoietic stem cells tothe bone marrow (2). It has also been reported to promote the migration and differ-entiation of tissue-committed stem cells (TCSCs) to injury sites under some pathologicalconditions, such as diabetes, liver cirrhosis, or myocardial infarction (3–5). Ourprevious study found that in inflamed dental pulp positive staining of this axis couldbe detected in endothelial cells of the microblood vessels, which were surroundedby a large number of pulp cells (6). Another study also showed that CXCR4-positivedental pulp cells (DPCs) were localized in the perivascular area (7). Because CXCR4has been reported as a new surface stem cell marker (8), these studies suggestedthat the SDF-1a/CXCR4 axis plays an important role in recruiting DPSCs from thestem cell niche to the injury sites. However, the detailed regulation mechanisms ofthis axis in DPSCs are currently unknown. This information is needed to further inves-tigate the contribution of DPSCs to the secretion of SDF-1a and the expression of CXCR4and analyze the factors that can influence this axis in DPSCs.
DPCs isolated from mammalian dental pulp are found to be a heterogeneous pop-ulation of DPSCs and other progenitors, which possess mesenchymal stem cells likequalities similar to bone marrow mesenchymal cells (BMSCs) (9, 10). In order tofurther look through the regulation of the SDF-1a/CXCR4 axis in DPSCs, weestablished two injury models of inflammation and hypoxia by using cultured humanDPCs to find whether these injuries could affect the activity of this axis in DPCs. Wehypothesize that by mimicking the stress environment of dental pulp in vitro, theproliferation and migration ability of DPCs may be changed. Meanwhile, theexpression levels of SDF-1a and CXCR4 may also be affected.
Materials and MethodsDPCs Culture
Healthy teeth were collected from the extracted premolars or third molars fororthodontic reasons of patients (age, 13-25 years) in the Department of Oral and Maxil-lofacial Surgery, the Affiliated Stomatology Hospital of Sun Yat-sen University, Guangzhou,
uanghua School and Hospital of Stomatology & Institute of Stomatological Research, Sun Yat-sen
y.ogram of Higher Education of China (grant no. 20070558205).perative Dentistry and Endodontics, Guanghua School and Hospital of Stomatology, Sun Yat-senail.sysu.edu.cn.
Regulation of SDF-1a-CXCR4 in HDPCs 1499

Basic Research—Biology
China. Informed consent was obtained from each patient, and researchprotocols were approved by the Ethics Committee of the university. DPCswere isolated as previously reported (10). DPCs were cultured in alpha-modified Eagle medium (a�MEM; Gibco, Grand Island, NY) supple-mented with 100 U/mL penicillin, 100 mg/mL streptomycin (Sigma,St. Louis, MO), and 10% fetal bovine serum (FBS, Gibco). Cultureswere maintained at 37�C in an incubator (5% CO2/20% O2).Enzyme-Linked Immunosorbent AssayAfter being stimulated with different concentrations (0.1, 1, and 10
mg/mL) of Escherichia coli (E. coli 055:B5) lipopolysaccharide (LPS,Sigma) for 48 hours, supernatant of DPCs was collected, and the SDF-1a production was measured in triplicate using an enzyme-linkedimmunosorbent assay (ELISA) kits (R&D Systems, Minneapolis, MN)following the manufacturer’s instructions.
Western BlottingDPCs were treated with LPS (0.1, 1, and 10 mg/mL) for 48 hours
and then harvested in radioimmunoprecipitation lysis buffer (10 mmol/LTris-HCL, 1 mmol/L EDTA, 1% sodium dodecyl sulfate, 1% NonidetP-40, 1:100 proteinase inhibitor cocktail, 50 mmol/L b-glycerophos-phate, and 50 mmol/L sodium fluoride). Western blotting was per-formed as described (11). Proteins were detected with polyclonalantibodies against human CXCR4 (fusin (H-118):sc-9046, 1:200,Santa Cruz, CA) and monoclonal antibodies against human b-actin(1:5,000; Cell Signaling, Beverly, MA).
Cell Proliferation AssayThe hypoxic condition was achieved by reducing the oxygen
concentration to 1% in a chamber by using a gas mixture (5% CO2
and balanced N2). DPCs were plated at a concentration of 5 � 103/well in 96-well plates and incubated for 6, 12, 18, and 24 hours, respec-tively, in normoxia (20% O2) or hypoxia (1% O2). The cell proliferationability was evaluated by using methylthiazol tetrazolium (MTT, Sigma)assay as described before (7).
Quantitative RT-PCRAfter incubation for 6, 18, and 24 hours, respectively, in normoxia
or hypoxia, the total RNA was extracted by using Trizol (Invitrogen,Carlsbad, CA). Quantifications of HIF1-a, SDF-1a, CXCR4, and b-actinmessenger RNA (mRNA) were performed based on the reportedmethods (6). Data of these targeted genes were normalized to theinternal control b-actin to obtain DCt. The final quantities of gene ofinterest relative to normoxic samples were reported by 2-DDCt method(12). The details of primers used were listed in Table 1.
Transmigration AssayTranswell inserts (5-mm pore, Corning, New York) were used in
this assay. After being cultured for 18 hours under normoxia or
TABLE 1. Primer Sequences Used in Quantitative RT-PCR
Gene Prime
HIF-1a Forward: 5’-AAGGTATTGReverse: 5’-CAGCACCAA
SDF-1a Forward: 5’-CCCGTCAGCReverse: 5’-CGTTGGCTCT
CXCR4 Forward: 5’-GACCGCTTCReverse: 5’-GCCAACCATG
b-actin Forward: 5’-GCATGGGTCReverse: 5’-TCGTCCCAGT
1500 Gong et al.
hypoxia, 300 mL DPCs (3 � 105 cells/mL) were seeded in the upperchamber, and 600 mL of serum-free medium with or without 100 ng/mL rhSDF-1a (R&D) was placed in the lower chamber. The chamberswere incubated for 10 hours. Then, nonmigrating cells were scraped offfrom the top, and migrating cells were stained with Hoechst 33342(Sigma, St. Louis, MO) and observed by using a fluorescence micros-copy. Five fields under a 400-fold magnification were randomlyselected, and immunoreactive cells were counted.
Statistical AnalysisData analysis was performed using SAS 8.1 (SAS, Raleigh, NC).
A paired Student t test was used to compare two means. One-wayanalysis of variance was applied to compare two or more means fol-lowed by the Student-Newman-Keuls test. Differences in which p wasless than 0.05 were considered to be statistically significant.
ResultsLPS Inhibited SDF-1a Expression
The ELISA assay showed that nonstimulated DPCs secreted SDF-1aconstitutively. After being stimulated with various concentrations of LPS(0.1, 1, and 10 mg/mL) for 48 hours, SDF-1a production of DPCssignificantly reduced (p < 0.05) in comparison with the control group(Fig. 1).
LPS Increased CXCR4 ProductionIn our preliminary study, we used the method of immunofluores-
cence to show that CXCR4 staining was mostly found in the cytoplasm ofcultured DPCs (data were not shown). In order to detect protein levelchanges before and after LPS stimulation, Western blotting was per-formed, and the analysis showed that 1 mg/mL LPS increased the expres-sion of CXCR4 in DPCs after 48 hours of treatment (p < 0.05); the othertwo concentrations had no similar effect (Fig. 2).
Hypoxia Promoted DPCs ProliferationAfter being cultured for 6, 12, 18, or 24 hours either in normoxia
or hypoxia, the MTT assay was used to determine whether hypoxia hadan effect on cell proliferation. MTT results showed an increased opticaldensity value in all hypoxic groups during the 24-hour cultivationperiod (p < 0.05), indicating that DPCs proliferated at a faster ratein hypoxic culture condition (Fig. 3).
Hypoxia Affected the mRNA Levels of HIF-1a, SDF-1a, andCXCR4
To investigate the effect of hypoxia on expression of these candi-date genes, DPCs were exposed to normoxia or hypoxia for differentperiods (6, 18, and 24 hours). Quantitative RT-PCR was then performedto analyze HIF-1a, SDF-1a, and CXCR4 mRNA expression levels in DPCsunder different culture conditions. Compared with normoxic DPCs,
rs Length
CACTGCACAGGC-3’ 99bpGCAGGTCATAGG-3’CTGAGCTACAG-3’ 64bpGGCAACATG-3’TACCCCAATGA-3’ 63bpATGTGCTGAA-3’
AGAAGGATTCCT-3’ 106bpTGGTGACGAT-3’
JOE — Volume 36, Number 9, September 2010

Figure 1. ELISA analysis of SDF-1a levels in DPCs. Normal DPCs expressedSDF-1a constitutively. After being stimulated with LPS, SDF-1a productionsignificantly reduced. Data were shown as means� standard deviation of threeindependent experiments. *p < 0.05 as compared with the control group. Figure 3. The effects of hypoxia on DPCs proliferation. An increased optical
density value was observed at each time point during the 24-hour cultureperiod. Data were shown as means� standard deviation of three independentexperiments. *p < 0.05 as compared with the normoxic group.
Basic Research—Biology
hypoxic DPCs expressed high levels of HIF-1a and CXCR4 but low levelsof SDF-1a in the 6-, 18-, and 24-hour groups, respectively (Fig. 4).
Hypoxia Enhanced SDF-1a–Dependent Cell MigrationThe transmigration assay was performed to determine the effect of
hypoxia on DPCs migration ability. Compared with normoxic DPCs,hypoxic DPCs displayed more migratory properties. Because 100 ng/mL rhSDF-1a has been proven to have a maximum ability to migrateDPCs in vitro (7), we added this concentration of rhSDF-1a in thelower chamber to further observe effects of hypoxia. If hypoxia isable to increase CXCR4 amount in DPCs, more cells would cross micro-pores of the transwell inserts and migrate to the other side. Our resultsfound that in the presence of rhSDF-1a, more hypoxic DPCs crossed the5-mm micropores (p < 0.05) in comparison with the normoxic group(Fig. 5).
DiscussionDental pulp is frequently inflamed because of bacterial infection of
dental caries. One of the histological features in inflamed dental pulp isthe adhesion and migration of various leukocytes. In our previousresearch, we showed that SDF-1 and its receptor CXCR4 were mainlyidentified in inflammatory cells, indicating this axis had been involvedin dental pulp infection. However, the regulation of this axis in DPCs
Figure 2. Western blotting results of CXCR4 production in DPCs; 1 mg/mLLPS increased the expression of CXCR4 in DPCs after 48 hours of treatment;the other two concentrations did not affect CXCR4 production. Data wereshown as means � standard deviation of three independent experiments.*p < 0.05 as compared with the control group.
JOE — Volume 36, Number 9, September 2010
under inflammatory stimulation in vitro was less reported. In thepresent study, we used different concentrations of LPS to stimulateDPCs, and we found that the secretion of SDF-1a was largely sup-pressed, whereas 1 mg/mL LPS increased the production of CXCR4. Itis surprising that the SDF-1a amount decreased because in the previousstudy expression of SDF-1 mRNA in inflamed dental pulp was signifi-cantly increased. Additionally, our results seem contrary to otherresearchers’ work (eg, Hosokawa et al found (13) that 10 mg/mLLPS significantly enhanced the production of SDF-1 in human gingivalfibroblasts). Another group also showed that heat-killed Enterococcusfaecalis was able to increase SDF-1 production in human dental pulpfibroblasts (14). The expression of SDF-1 has been reported to becomplexly regulated. It is known that LPS of gram-negative bacterialcells could induce synthesis of proinflammatory cytokines, such asinterleukin (IL)-1 or tumor necrosis factor a (TNF-a) (15). Fedyket al (16) showed a novel down-regulation of SDF-1 in response toinflammation of human gingival fibroblasts, which were probablyaffected by monocyte-derived IL-1a and TNF-a (16). A recent reportshowed that LPS from Porphyromonas gingivalis could alter thebalance of cytokines, which led to a decreased SDF-1 production inhuman gingival and periodontal ligament fibroblasts (17). Taking theseinto account, we speculated that SDF-1a expression changes in DPCsmight be caused either directly by LPS or indirectly by inflammatorycytokines. On one hand, LPS may escape from the immune response
Figure 4. The expression levels of the mRNAs encoding HIF-1a, SDF-1a, andCXCR4 in hypoxic DPCs relative to normoxic DPCs as determined by quantita-tive RT-PCR. The HIF-1a and CXCR4 expression level increased, but SDF-1aexpression decreased in the 24-hour culture period. Data were shown asmeans � standard deviation of three independent experiments.
Regulation of SDF-1a-CXCR4 in HDPCs 1501

Figure 5. Transmigration assay showed hypoxia improved DPCs’s migrationability, and hypoxic DPCs displayed increased responsiveness to 100 ng/mLrhSDF-1a. Data were shown as means� standard deviation of three indepen-dent experiments. *p < 0.05 as compared with the normoxia group; **p <0.05 as compared with the group of normoxia plus rhSDF-1a.
Basic Research—Biology
to inhibit SDF-1a production. On the other hand, these inflammatorycytokines such as IL-1 and/or TNF-a may contribute to the suppressionof SDF-1a production during the disease process. The results of CXCR4production agree with Takabayashi et al’s report (18), which stated that100 ng/mL LPS increased the mRNA expression of CXCR4 in human oralcarcinoma cells in a 24-hour period. Petty et al also found that, duringthe development of LPS-induced pneumonitis in mice, a significantincrease in CXCR4 was found on circulating neutrophils (19). Recentfindings show that CXCR4 is not only involved in LPS binding but alsoresponsible for triggering signals in response to LPS (20).
The oxygen concentration of human organisms varies between thetissues; in the eyes, it varies from 1% to 5% and in the bone marrowfrom 0% to 4% (21). In some pathological processes such as cerebralischemia, the oxygen tension in the brain can be even lower (22).Dental pulp is in the center of a tooth and has limited or no collateralcirculation except from the small root apical end. This structure makesdental pulp susceptible to injury in which inflammation can increase theinternal pressure and lead to hypoxia. Normally, cell culture is per-formed at an atmospheric oxygen concentration (20% O2). However,many studies on stem cells indicated that the hypoxic condition canamplify progenitor cell numbers (23). The effect of hypoxia on DPCs,especially in the human species, is less reported. Sakdee et al (24)showed that 3% O2 significantly promoted the proliferation of humanDPCs from day 3 to 14. Consistent with Sakdee’s results, we foundthat DPCs proliferated at a faster rate in 1% O2. It might be explainedthat hypoxia reduces oxidative damage to DNA (21). Additionally,limited energy only allows the expression of highly evolutionaryconserved signals, which control the self-renewal abilities of stem cells.Recently, Wang et al (25) found that simulated ischemia (serum depri-vation and hypoxia) increased side population stem cells of the dentalpulp. Furthermore, these stressful conditions also promoted the expres-sion of OCT4, which plays an important role in maintaining the self-renewal capacity and pluripotency of these dental pulp stem cells (25).
Hypoxia can induce the expression of hypoxia inducible factor(HIF), which consists of an a (HIF-a) and a b (HIF-b, or ARNT)subunit. Under normoxia, HIF-a is translated but rapidly degraded.When oxygen levels decrease, the stabilized HIF-a proteins candimerize HIF-b in the nucleus and then bind to a core sequence of(A/G CGTG) in hypoxia-response elements of target genes (26).Hypoxia-response elements have been found in nearly 200 genes, whichare related to metabolism, angiogenesis, or cell differentiation. In ourstudy, real-time PCR showed that the HIF1-a mRNA level increased in
1502 Gong et al.
the 24-hour culture period, indicating that hypoxia promoted theexpression of HIF1-a in DPCs.
As a transcriptional factor, HIF can regulate both ligands andreceptors of the SDF-1a-CXCR4 axis. Ceradini et al (27) reportedthat the 5’ flanking region of the human SDF-1 gene had two potentialHIF-1 binding sites. A putative HIF-1 binding site was also shown in theCXCR4 promoter by Schioppa’s group (28). To the best of our knowl-edge, this is the first study showing the regulation of the SDFa-1-CXCR4in hypoxic DPCs. Unexpectedly, we found that in the 24 hours the mRNAlevel of SDF-1a reduced, which was inconsistent with Ceradini’s report.The mechanisms leading to this down-regulation are currentlyunknown because many transcriptional pathways have been involvedin hypoxic or ischemic responses (29). Gross et al (30) found thatthe SDF-1 mRNA level of inner ear cells decreased after 5 hours ofhypoxic culture, and they suggested that the down-regulation of SDF-1 might generate signals to regulate the migration of local precursorcells. A recent report also detected a decreased pattern of SDF-1mRNA expression in the rat hippocampus after transient globalischemia. They mentioned that a short period of hypoxia (1 day) mightbe sufficient to provoke neuronal death but insufficient for SDF-1 geneinduction (31). Because the hypoxic condition used in our study isa transient period of 24 hours, it is possible that this time interval wouldnot be efficient for HIF to act as a promoter to increase SDF-1a produc-tion. Nevertheless, whether SDF-1a has a protein level stabilization orother posttranslational mechanism needs to be investigated further.The increase in the level of CXCR4 mRNA suggests that HIF-1a mightbind to the promoter of CXCR4 and regulate its transcription. This isconsistent with the transmigration assay results of our study. Whenusing the concentration of 100 ng/mL rhSDF-1a, hypoxic DPCsmigrated efficiently through the transwell inserts, indicating that hypoxiamight increase the distribution of CXCR4. We also found that without therhSDF-1a, hypoxia also improved DPCs’ migration ability.
The SDFa-1-CXCR4 axis has been reported in DPSCs research. Forexample, CXCR4 has been used as a stem cell marker in side populationcells sorting from porcine dental pulp (32). Furthermore, an in vivoexperiment found that transplanted DPSCs could induce endogenousaxon guidance via SDFa-1-CXCR4 signaling interactions (33). Becausethe expression of this axis has also been found in leukocytes, lymphocytes,and dendritic cells (34), it indicates that communication betweendifferent cell types in dental pulp may be particularly crucial in the homingof DPSCs. Considering the fact that the recruitment of CXCR4-positivestem/progenitor cells to a SDF-1 gradient may be regulated by severalmolecules related to inflammation or hypoxia (27, 35), the down-regulation of SDF-1a in two stress models of our study indicate that DPSCsmay follow the gradient signal to efficiently mobilize to the injury sites.
To sum up, our present study suggests that both inflammation andhypoxia might regulate the SDF-1a-CXCR4 axis in DPCs. Further studieswill focus on the specific signal pathways and in vivo animal models ofdental pulp injury. All these studies will deeply look through the wholemechanism of SDF-1a-CXCR4 axis in pulp regeneration, which mightgive some clues to the regenerative endodontic therapies.
AcknowledgmentsWe would like to thank Siyu Cao for critical review of this
article.
References1. Goldberg M, Farges JC, Lacerda-Pinheiro S, et al. Inflammatory and immunological
aspects of dental pulp repair. Pharmacol Res 2008;58:137–47.2. Wang J, Loberg R, Taichman RS. The pivotal role of CXCL12 (SDF-1)/CXCR4 axis in
bone metastasis. Cancer Metastasis Rev 2006;25:573–87.
JOE — Volume 36, Number 9, September 2010

Basic Research—Biology
3. Yano T, Liu Z, Donovan J, et al. Stromal cell derived factor-1 (SDF-1)/CXCL12 atten-uates diabetes in mice and promotes pancreatic beta-cell survival by activation of theprosurvival kinase Akt. Diabetes 2007;56:2946–57.
4. Asano Y, Iimuro Y, Son G, et al. Hepatocyte growth factor promotes remodeling ofmurine liver fibrosis, accelerating recruitment of bone marrow-derived cells intothe liver. Hepatol Res 2007;37:1080–94.
5. Saxena A, Fish JE, White MD, et al. Stromal cell-derived factor-1alpha is cardiopro-tective after myocardial infarction. Circulation 2008;117:2224–31.
6. Jiang HW, Ling JQ, Gong QM. The expression of stromal cell-derived factor 1 (SDF-1) in inflamed human dental pulp. J Endod 2008;34:1351–4.
7. Jiang L, Zhu YQ, Du R, et al. The expression and role of stromal cell-derived factor-1alpha-CXCR4 axis in human dental pulp. J Endod 2008;34:939–44.
8. Miller RJ, Banisadr G, Bhattacharyya BJ. CXCR4 signaling in the regulation of stemcell migration and development. J Neuroimmunol 2008;198:31–8.
9. Liu L, Ling J, Wei X, et al. Stem cell regulatory gene expression in human adult dentalpulp and periodontal ligament cells undergoing odontogenic/osteogenic differenti-ation. J Endod 2009;35:1368–76.
10. Huang GT, Gronthos S, Shi S. Mesenchymal stem cells derived from dental tissues vs.those from other sources: their biology and role in regenerative medicine. J DentRes 2009;88:792–806.
11. Jiang HW, Zhang W, Ren BP, et al. Expression of toll like receptor 4 in normalhuman odontoblasts and dental pulp tissue. J Endod 2006;32:747–51.
12. Mani SA, Guo W, Liao MJ, et al. The epithelial-mesenchymal transition generatescells with properties of stem cells. Cell 2008;133:704–15.
13. Hosokawa Y, Hosokawa I, Ozaki K, et al. CXCL12 and CXCR4 expression by humangingival fibroblasts in periodontal disease. Clin Exp Immunol 2005;141:467–74.
14. Sipert CR, Moraes IG, Bernardinelli N, et al. Heat-killed Enterococcus faecalis altersnitric oxide and CXCL12 production but not CXCL8 and CCL3 production by culturedhuman dental pulp fibroblasts. J Endod 2010;36:91–4.
15. Hahn CL, Liewehr FR. Relationships between caries bacteria, host responses, andclinical signs and symptoms of pulpitis. J Endod 2007;33:213–9.
16. Fedyk ER, Jones D, Critchley HO, et al. Expression of stromal-derived factor-1 isdecreased by IL-1 and TNF and in dermal wound healing. J Immunol 2001;166:5749–54.
17. Morandini AC, Sipert CR, Gasparoto TH, et al. Differential production of macrophageinflammatory protein-1alpha, stromal-derived factor-1, and IL-6 by human culturedperiodontal ligament and gingival fibroblasts challenged with lipopolysaccharidefrom P. gingivalis. J Periodontol 2010;81:310–7.
18. Takabayashi T, Takahashi N, Okamoto M, et al. Lipopolysaccharides increase theamount of CXCR4, and modulate the morphology and invasive activity of oral cancercells in a CXCL12-dependent manner. Oral Oncol 2009;45:968–73.
JOE — Volume 36, Number 9, September 2010
19. Petty JM, Sueblinvong V, Lenox CC, et al. Pulmonary stromal-derived factor-1expression and effect on neutrophil recruitment during acute lung injury.J Immunol 2007;178:8148–57.
20. Triantafilou M, Lepper PM, Briault CD, et al. Chemokine receptor 4 (CXCR4) ispart of the lipopolysaccharide "sensing apparatus. Eur J Immunol 2008;38:192–203.
21. Ivanovic Z. Hypoxia or in situ normoxia: The stem cell paradigm. J Cell Physiol 2009;219:271–5.
22. Erecinska M, Silver IA. Tissue oxygen tension and brain sensitivity to hypoxia. RespirPhysiol 2001;128:263–76.
23. Keith B, Simon MC. Hypoxia-inducible factors, stem cells, and cancer. Cell 2007;129:465–72.
24. Sakdee JB, White RR, Pagonis TC, et al. Hypoxia-amplified proliferation of humandental pulp cells. J Endod 2009;35:818–23.
25. Wang J, Wei X, Ling J, et al. Side population increase after simulated transientischemia in human dental pulp cell. J Endod 2010;36:453–8.
26. Weidemann A, Johnson RS. Biology of HIF-1alpha. Cell Death Differ 2008;15:621–7.
27. Ceradini DJ, Kulkarni AR, Callaghan MJ, et al. Progenitor cell trafficking is regu-lated by hypoxic gradients through HIF-1 induction of SDF-1. Nat Med 2004;10:858–64.
28. Schioppa T, Uranchimeg B, Saccani A, et al. Regulation of the chemokine receptorCXCR4 by hypoxia. J Exp Med 2003;198:1391–402.
29. Safronova O, Morita I. Transcriptome remodeling in hypoxic inflammation. J DentRes 2010;89:430–44.
30. Gross J, Moller R, Amarjargal N, et al. Expression of erythropoietin and angiogenicgrowth factors following inner ear injury of newborn rats. Prague Med Rep 2009;110:310–31.
31. Riek-Burchardt M, Kolodziej A, Henrich-Noack P, et al. Differential regulation ofCXCL12 and PACAP mRNA expression after focal and global ischemia. Neurophar-macology 2010;58:199–207.
32. Iohara K, Zheng L, Wake H, et al. A novel stem cell source for vasculogenesis inischemia: subfraction of side population cells from dental pulp. Stem Cells 2008;26:2408–18.
33. Arthur A, Shi S, Zannettino AC, et al. Implanted adult human dental pulp stem cellsinduce endogenous axon guidance. Stem Cells 2009;27:2229–37.
34. Farges JC, Keller JF, Carrouel F, et al. Odontoblasts in the dental pulp immuneresponse. J Exp Zool B Mol Dev Evol 2009;312B:425–36.
35. Kucia M, Reca R, Miekus K, et al. Trafficking of normal stem cells and metastasis ofcancer stem cells involve similar mechanisms: pivotal role of the SDF-1-CXCR4 axis.Stem Cells 2005;23:879–94.
Regulation of SDF-1a-CXCR4 in HDPCs 1503

Basic Research—Biology
Inherent Differential Propensity of Dental Pulp Stem CellsDerived from Human Deciduous and Permanent TeethVijayendran Govindasamy, PhD,* Aimi Naim Abdullah, BSc,† Veronica Sainik Ronald, BSc,†
Sabri Musa, BDS, MSc,†
Zeti Adura Che Ab. Aziz, BDS, MSc,‡
Rosnah Binti Zain, BDS, MS,§
Satish Totey, PhD,* Ramesh R. Bhonde, PhD,* and Noor Hayaty Abu Kasim, PhD‡
Abstract
Introduction: Lately, several new stem cell sources andtheir effective isolation have been reported that claim tohave potential for therapeutic applications. However, itis not yet clear which type of stem cell sources are mostpotent and best for targeted therapy. Lack of under-standing of nature of these cells and their lineage-specific propensity might hinder their full potential.Therefore, understanding the gene expression profilethat indicates their lineage-specific proclivity is funda-mental to the development of successful cell-based ther-apies. Methods: We compared proliferation rate, geneexpression profile, and lineage-specific propensity ofstem cells derived from human deciduous (SCD) andpermanent teeth (DPSCs) over 5 passages. Results:The proliferation rate of SCD was higher (cell number,25 � 106 cells/mL; percent colony-forming units[CFUs], 151.67 � 10.5; percent cells in S/G2 phase,12.4 � 1.48) than that of DPSCs (cell number, 21 �106 cells/mL; percent CFUs, 133 � 17.62; percent cellsin S/G2 phase, 10.4 � 1.18). It was observed that foldexpression of several pluripotent markers such asOCT4, SOX2, NANOG, and REX1 were higher (>2) inSCD as compared with DPSCs. However, DPSCs showedhigher expression of neuroectodermal markers PAX6,GBX2, and nestin (fold expression >100). Similarly,higher neurosphere formation and neuronal markerexpression (NF, GFAP) were found in the differentiatedDPSCs into neuron-like cells as compared with SCD.Conclusions: This study thus demonstrates that bothSCD and DPSCs exhibit specific gene expression profile,with clear-cut inclination of DPSCs toward neuronallineage. (J Endod 2010;36:1504–1515)Key WordsDeciduous teeth, dental pulp stem cells, inherentpropensity, permanent teeth
From the *Stempeutics Research Malaysia Sdn Bhd, Kuala Lumpvative Dentistry, and §Department of Oral Pathology, Oral MedicinUniversity of Malaya, Kuala Lumpur, Malaysia.
Address requests for reprints to Noor Hayaty Abu Kasim, BDS, PLumpur, Malaysia. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.006
1504 Govindasamy et al.
The therapeutic potential of stem cells derived from human dental pulp since itsdiscovery (1) in regenerative medicine has been extensively studied at several
preclinical (2) and clinical levels (3). The dental pulp tissue (DPT) appears to bean excellent source for stem cells because it can be obtained from the deciduousdentition requiring extraction as part of a planned serial extraction for managementof occlusion and is originated from migrating neural crest cells during early devel-opment of embryos (4). The DPT can be isolated from various age groups and teeth;for example, cells isolated from dental tissue of human impacted tooth germ areknown as tooth germ progenitor cells (TGPCs) (5); stem cells from human exfoliateddeciduous teeth are known as SHED (6), and stem cells can also be isolated fromhuman permanent teeth (impacted molar) (DPSCs) (7) or from apical papilla(SCAP) (8).
Our present work is specifically focused on stem cells from extracted deciduous(SCD) and permanent teeth (DPSCs). Past studies showed that both these groups ofcells are able to differentiate into osteogenic, chondrogenic, adipogenic, and myogeniccells in culture (9, 10). Moreover, recent studies have shown that both SHED andpermanent teeth are able to break germ layer commitment and differentiate intocells expressing neurons (11) and hepatocytes (12). Furthermore, this group of cellshas been reported to have potential for use in cell-based therapy for neurodegenerativeand cardiac diseases (13, 14).
It has been established that gene expression and growth factor profile reflect thesource of tissue from which the stem cells have been obtained. This indicates that stemcell heterogeneity is biologically relevant. We have demonstrated previously that geneexpression profile, growth pattern, and propensity of human embryonic stem cells,bone marrow–derived mesenchymal stromal cells, and umbilical cord are different,and hence mesenchymal stem cells derived from various tissue sources are differentfrom each other and indicate their propensity toward a specific lineage (15, 16).Therefore, it is logical that different tissue sources might generate stem cell productsproducing different cytokines and growth factors that might be more suited forspecific clinical applications. Similarly, we hypothesized that gene expression varieswithin various sources of the same group such as in the case of stem cells of dentalorigin, which determines the development pathway of these cells.
Although during the past few years the interest in dental stem cells has risen mark-edly and several reports on characterization and differentiation of dental stem cells fromdifferent sources and age groups have been published (17), the gene expressionprofile–dependent propensity toward lineage specificity remains poorly understood.Therefore, we undertook this present study comparing proliferation rate, gene
ur, Malaysia; and †Department of Children‘s Dentistry and Orthodontics, ‡Department of Conser-e & Periodontology/Oral Cancer Research and Coordinating Centre(OCRCC), Faculty of Dentistry,
hD, Department of Conservative Dentistry, Faculty of Dentistry, University of Malaya, 50603 Kuala
JOE — Volume 36, Number 9, September 2010

Basic Research—Biology
expression profile, and their lineage propensity of SCD and DPSCs tobetter understand their inherent therapeutic potential for specific clin-ical indications.Materials and MethodsIsolation and Culture of SCD and DPSCs
Sound intact human third molars from adults (24–35 years ofage) and deciduous teeth (5–8 years of age) were collected withinformed consent from patients undergoing extraction at the Depart-ment of Children Dentistry and Orthodontics and Department of Oraland Maxillofacial Surgery, University of Malaya, respectively, underapproved guidelines set by the Medical Ethics Committee, Faculty ofDentistry, University of Malaya (Medical Ethics Clearance Number DFCD0907/0042(L). Root surfaces were cleaned with povidone-iodine(Sigma Aldrich, St Louis, MO), and the pulps were extirpated within2 hours after extraction and processed. The pulp tissue was mincedinto small fragments before digestion in a solution of 3 mg/mL collage-nase type I (Gibco, Grand Island, NY) for 40 minutes at 37�C. Afterneutralization with 10% of fetal bovine serum (FBS) (Hyclone; ThermoFisher Scientific Inc, Waltham, MA), the cells were centrifuged and wereseeded in culture flasks with culture medium containing a-MEM (Invi-trogen, Carlsbad, CA), 0.5% 10,000 mg/mL penicillin/streptomycin (In-vitrogen); 1% 1 � Glutamax (Invitrogen) and 10% FBS, withhumidified atmosphere of 95% of air and 5% of CO2 at 37�C. Non-adherent cells were removed 48 hours after initial plating. The mediumwas replaced every 3 days. When primary culture became subconfluent,after 10–14 days, cells were collected by trypsinization and processedfor subsequent passages. All the experiments were done with pool of 5dental pulp tissues. Therefore, 3 different pooled samples were used in3 replicates. Human bone marrow samples were taken after writtenconsent by using guidelines approved by the Ministry of Health,Malaysia. Bone marrow–derived mesenchymal stem cells (BM-MSCs)cultures were established from 3 donors (age range, 18–25 years)as previously described (18).
TABLE 1. List of Primers Used in this Study
Gene symbol / name Forward
18s RNA CGGCTACCATCCAAGGAAREX1 GCGTACGCAAATTAAAGTCCAGAOCT 3/4 (POU5F1) CGACCATCTGCCGCTTTGAGSOX2 CCCCCGGCGGCAATAGCANANOG CCTCCTCCATGGATCTGCTTATTCAOsteocalcin CATGAGAGCCCTCACAOsterix GCAGCTAGAAGGGAGTGGTGABCG2 GTTTATCCGTGGTGTGTCTGGAFP AGAACCTGTCACAAGCTGTGPAX6 ATGAACAGTCAGCCAATGGGGATA2 AGCCGGCACCTGTTGTGCAAb-III Tubulin AACAGCACGGCCATCCAGGMSX1 CCTTCCCTTTAACCCTCACACNF ACGCCTGAGGAATGGTTCACGBMP 4 GTCCTGCTAGGAGGCGCGAGhTERT AGCTATGCCCGGACCTCCATNestin CAGCGTTGGAACAGAGGTTGGHNF-3 Beta GACAAGTGAGAGAGCAAGTGHAND 1 TGCCTGAGAAAGAGAACCAGGFAP CGATCAACTCACCGCCAACAKRT1-5 CACAGTCTGCTGAGGTTGGANUUR1 CGGACAGCAGTCCTCCATTAAGGTTH TCATCACCTGGTCACCAAGTTKRT-8 TGAGGTCAAGGCACAGTACGTGF 1 GCCCGCTTCTCTTACAGTGTGATT
JOE — Volume 36, Number 9, September 2010 Inherent Pr
Colony-forming UnitsThe number of colony-forming units (CFUs) was determined by
plating 100 cells in 35-mm dish. After 14 days in culture, the cellswere fixed in 100% methanol for 20 minutes and stained by 3% crystalviolet stain. Colonies more than 2 mm in diameter were counted. TheCFU equals the total number of colonies divided by the initial numberof cells multiplied by 100%.
Growth KineticsThe proliferation rate was determined by plating 5000 cells/cm2
from SCD and DPSCs per T25 cm2 culture flask (BD Pharmingen,San Diego, CA). Three replicates were performed for each passageand time point. Cells were detached by trypsinization after reaching con-fluency of 90%. Cells were counted and assessed for viability by meansof trypan blue dye exclusion before the next passage. Cells were re-plated for subsequent passages, and total of 5 passages were studiedin this experiment. Growth kinetics was analyzed by calculating popu-lation doubling (PD) time. The PD time was obtained by the formula:TD = tplg2/(lgNH – lgNI), where NI is the inoculum cell number, NHis the cell harvest number, and t is the time of the culture (in hours).
Cell Cycle AnalysisCells were seeded at 5000 cells/cm2 on a 35-mm tissue culture
dish (BD Pharmingen) and cultured until reaching a confluence of90%. The cells were detached, fixed, and permeabilized in 70% ethanolovernight in the dark at 4�C. DNA was stained with propidium iodide/RNase staining buffer (BD Pharmingen) in a volume of 500 mL (con-taining 1 � 106 cells) for 15 minutes at room temperature and thenwashed in DPBS (Invitrogen). DNA content was analyzed on GuavaTechnologies (Millipore, Billerica, MA) flow cytometer by using Cyto-soft, Version 5.2, Guava Technologies software.
Flow Cytometric AnalysisThe immunophenotyping was done by using flow cytometry at
passage 5. On reaching 90% confluency, the cells were harvested
Reverse Base pairs
GCTGGAATTACCGCGGCT 186CAGCATCCTAAACAGCTCGCAGAAT 282
CCCCCTGTCCCCCATTCCTA 572TCGGCGCCGGGGAGATACAT 447TCGGCGCCGGGGAGATACAT 259
AGAGCGACACCCTAGAC 314GCAGGCAGGTGAATTCTTCC 358CTGAGCTATAGAGGCCTGGG 651GACAGCAAGCTGAGGATGTC 675CACACCAGGGGAAATGAGTC 625TGACTTCTCCTGCATGCACT 243
CTTGGGGCCCTGGGCCTCCGA 242CCGATTTCTCTGCGCTTTTC 284
GCCTCAATGGTTTCC 555GTTCTCCAGATGTTCTTCG 338
GCCTGCAGCAGGAGGATCTT 184TGGCACAGGTGTCTCAAGGGTAG 388
ACAGTAGTGGAAACCGGAG 234AGGATGAACAAACAC 254
GTGGCTTCATCTGCTTCCTGTC 158GAGCTGCTCCATCTGTAGGG 155
CTGAAATCGGCAGTACTGACAGCG 711GGTCGCCGTGCCTGTACT 124
TGATGTTCCGGTTCATCTCA 160AGTACGTGCAGACGGTGGTAGTTT 497
opensity Lineage-specific Potential of Various Sources of Dental Stem Cells 1505

Figure 1. Morphology, CFUs, DNA content, and growth kinetics of SCD and DP-MSC. (A, B) Phase contrast microscope; original magnification, �10 of SCD andDPSCs, respectively, at passage 5; (C, D) CFUs of SCD and DPSCs, respectively, at passage 5; (E) long-term growth curves of SCD and DPSCs; (F) PD time of SCD andDPSCs at passages 1; and (G, H) assessment of DNA content in SCD and DPSCs, respectively, at passage 5. In all experiments, the results represent average of 5culture replicates with SD, and a representative photomicrograph was given for each experiment. SD, standard deviation. Scale bar, 100 mmol/L. (This figure isavailable in color online at www.aae.org/joe/.)
Basic Research—Biology
with 0.05% trypsin (Invitrogen) and resuspended in phosphate-buffered saline (PBS) at a cell density of 1.5 � 106 cells/mL. Twohundred microliters of the cell suspension (1 � 105 cells) was incu-bated with the labeled antibodies in the dark for 1 hour at 37�C. Thefollowing antibodies were used to mark the cell surface epitopes:CD90-phycoerythrin (PE), CD44-PE, CD73-PE, CD166-PE and CD34-PE, CD45-fluoroisothiocyanate (FITC), and HLA-DR-FITC (all fromBD Pharmingen). All analyses were standardized against negativecontrol cells incubated with isotype-specific immunoglobulin (Ig)G1-PE and IgG1-FITC (BD Pharmingen). At least 10,000 events wereacquired on Guava Technologies flow cytometer, and the results wereanalyzed by using Cytosoft, Version 5.2, Guava Technologies.
Differentiation of DPSCsThe cultures were initiated at a density of 1000 cells/cm2 in 6-well
plates and were grown to confluence and subjected to differentiationinto adipogenic, chondrogenic, and osteogenic lineages as per themethod described earlier (18).
1506 Govindasamy et al.
Adipogenic lineage was stimulated by inducing the cells with10% FBS, 200 mmol/L indomethacin, 0.5 mmol/L 3-isobutyl-1-me-thyxanthine (IBMX), 10 mg/mL insulin, and 1 mmol/L dexamethasone(all reagents from Sigma Aldrich). Lipid droplets were visualized bystaining with oil red O staining (Sigma Aldrich). The percent ofadipocytes was estimated by counting 500 total cells in multiplefields.
For chondrogenesis differentiation, briefly cells were cultured inmedia supplemented with ITS+1 (Sigma Aldrich), 50 mmol/L L-ascor-bic acid-2 phosphates (Sigma Aldrich), 55 mmol/L sodium pyruvate(Invitrogen), 25 mmol/L L-proline (Sigma Aldrich), and 10 ng/mL oftransforming growth factor-beta (TGF-b) (Sigma Aldrich). Assessmentof proteoglycan accumulation was visualized by alcian blue staining(Sigma Adrich).
The osteogenic differentiation was stimulated in a 3-week culturein media supplemented with 10% FBS, 10�7 mol/L dexamethasone, 10mmol/L b-glycerol phosphate (Fluka, Buchs, Switzerland), and 100mmol/L of L-ascorbic acid-2 phosphates. Assessment of calcium
JOE — Volume 36, Number 9, September 2010

TABLE 2. Phenotype Characterization, Colony-forming Ability, DNA Contentand Differentiation Potential of SCD and DPSCs Cultured at Passage 5
Parameters SCD DPSCs
Phenotypiccharacterization (%)*CD34 0 0CD44 94.21 � 2.9 95.83 � 1.8CD45 0 0CD73 99.88 � 3.1 99.45 �4.1CD90 93.71 � 0.9 99.49 � 0.8CD166 98.11 � 0.8† 79.85 � 6.8HLA-DR 0 0
Colonies (CFU)(% cells seeded)‡
151.67 � 10.5† 133 � 17.62
Cell cycleanalysis§
% of G1/G0 phase 87.6 � 1.48 89.6 � 1.18% of S/G2 phase 12.4 � 1.48† 10.4 � 1.18
In vitro adipogenicdifferentiationk
58 � 8† 45 � 6
In vitro osteogenicdifferentiation¶
59 � 5 64 � 8
SCD, stem cells derived from human deciduous teeth; DPSCs, stem cells derived from human perma-
nent teeth.
*Fluorescence-activated cell sorter analysis (FACS) of SCD and DPSCs: The result shows the average
value of % positive cells � standard deviation to the total number of cells analyzed (n $ 5).†P < .05.‡Percent SCD and DPSCs colonies grown at passage 5. Data are expressed as average value of % of
colonies � standard deviation.§Percent DNA content in SCD and DPSCs observed in G1/GO and S/G2 phase at passage 5.kPercent neutral oil droplet formation stained with red O cells out of 500 total cell counted.¶Percent mineralized area.
Basic Research—Biology
accumulation was visualized by von Kossa staining. Percentage ofcalcium accumulation was analyzed by using Image ProPlus software(Media Cybernetics, San Diego, CA). Osteogenic differentiation is pre-sented as percent of the mineralized area in the total culture area. Quan-titative amplifications of osteogenic markers (osteocalcin and osterix)were carried out in duplicate by using SYBR green master mix (AppliedBiosystems, Foster City, CA). Polymerase chain reactions were run on anABI 7900HT RT-PCR system (Applied Biosystems), and SDS v2.1 soft-ware was used to analyze the results. All measurements were normalizedby 18s rRNA. The sense and antisense primers used for each gene areshown in Table 1.
Human Taqman Low Density ArrayHuman Taqman Low Density Array (TLDA) (Applied Biosystems)
containing a well-defined set of validated gene expression markers tocharacterize embryonic stem cell identity was used for analyzing theexpression of a focused panel of pluripotent and stem cell markers.The 384 wells of each TLDA card were preloaded with fluorogenicprobes and primers (Applied Bioystems). The pooled cDNAs wereloaded on the microfluidic cards for thermal cycling on an ABI PRISM7900HT Sequence Detection System (Applied Biosystems). Expressionvalues for target genes were normalized to the expression of 18srRNA. Transcriptional analysis was performed for BM-MSCs (earlypassage), SCD and DPSCs (both early and late passages). For dataanalysis, the ABI PRISM 7900HT sequence detection system software(SDS) calculated the levels of target (SCD and DPSCs) gene expres-sion in samples relative to the level of expression in the calibrator(BM-MSCs) with comparative CT method (DDCT). For estimationof the fold change by TLDA when the initial transcript levels wereundetectable, the initial cycle threshold (CT) value was assigned tobe 39, which would lead to a possible underestimation of the actualfold change.
JOE — Volume 36, Number 9, September 2010 Inherent Pr
Reverse Transcription Polymerase Chain Reaction andReal-time Reverse Transcription Polymerase ChainReaction
Total RNA was extracted by using Trizol (Invitrogen) according tothe manufacturer’s instructions. The RNA was reverse-transcribed intocDNA by using Superscript II reverse transcriptase (Invitrogen) accord-ing to the manufacturer’s instructions. cDNA amplification was per-formed in a thermocycler by using Taq polymerase supplied with KClbuffer and 1.5 mmol/L MgCl2 (Invitrogen) at 94�C/1 min, 58�C/30sec, 72�C/1 min. Polymerase chain reaction (PCR) products wereresolved on 1.5% agarose (Invitrogen) gel run in 1� Tris borate–ethyl-enediaminetetraacetic acid buffer. The primer sequences are tabulatedin Table 1.
For the real-time PCR, the amplification reaction was performed byusing Taqman Universal Master Mix and Assay-on-Demand Taqmanprimer/probe sets (Applied Biosystems) according to manufacturer’sprotocol using the ABI 7900HT RT-PCR system (Applied Biosystems).The assays for OCT 4, SOX 2, NANOG, and DNMT1 wereHs00742896_s1 (130 base pairs [bp]), Hs02387400_g1 (122 bp),Hs02387400_g1 (109 bp), and Hs00945900_g1 (100 bp). Eukaryotic18S rRNA (assay ID Hs99999901_s1 [188 bp]) was used as an internalcontrol in all assays. The relative quantification of gene expression wasassessed by DDCT method. All PCRs were performed in duplicates. Theexpressions of some primers in the semiquantitative reverse transcrip-tion (RT)-PCR analysis were quantified in duplicate by using SYBRgreen master mix. PCR reactions were run on an ABI 7900HT RT-PCR system, and SDS v2.1 software was used to analyze the results.All measurements were normalized by 18s rRNA.
Neurogenic DifferentiationFor neuronal differentiation, SCD and DPSCs were cultured at the
rate of 10,000 cells/mL in a non-coated 35-mm dish containing Neuro-basal-A medium (Invitrogen) supplemented with B-27 supplement (In-vitrogen), penicillin-streptomycin, L-glutamine, epidermal growthfactor (EGF), and basic fibroblast growth factor (bFGF) (all from Invi-trogen) for 15 days. Neurosphere-like bodies generated after 15 dayswere then counted. Briefly, a fixed area (10 mm2) of the center ofeach well was converted into a digital image with a digital still camera(DSC-S70; Sony, Tokyo, Japan), and the number of neurosphereswith a diameter of more than 60 mm was counted with a Scion ImageBeta 4.02 (Scion Corporation, Frederick, MD).
Neurospheres that were generated after 15 days of incubation weretriturated by using poliSCD glass pipettes, and single-cell suspensionwas obtained and seeded on gelatin-coated 35-mm dishes in neurodif-ferentiation medium one (Neurobasal A) containing 1 mg/mL laminin(Invitrogen), 5 mg/mL fibronectin (Nitta Gelatin, Osaka, Japan), 2mmol/L L-glutamine, 10 mg/mL N2 supplement (Invitrogen), 20 ng/mL bFGF, and 40 ng/mL EGF. The medium was changed to neurodiffer-entiation medium 2 (Neurobasal A) containing 1 mg/mL laminin, 5 mg/mL fibronectin, 2 mmol/L L-glutamine, 10 mg/mL N2 supplement, 20ng/mL neurotrophin-3 (Peprotech, Rocky Hill, NJ) after 24 hours ofcultivation. The medium was changed every 3 days. Immunocytochem-ical analysis was performed 21 days after cultivation. The cells werefixed for 30 minutes in cold 4% paraformaldehyde in PBS, treatedwith 0.1% Triton-X for optimal penetration of cell membrane, and incu-bated at room temperature in a blocking solution (0.5% bovine serumalbumin; Sigma Aldrich) for 30 minutes. The primary antibodies usedwere goat anti-human-OCT4 (1:400; ABCAM Inc, San Francisco, CA),mouse anti-human-GFAP (1:400; Chemicon, Temecula, CA), andmouse anti-human-b-III tubulin (1:400; Chemicon). Secondary anti-bodies used were FITC-conjugated rabbit anti-goat IgG (1:700;
opensity Lineage-specific Potential of Various Sources of Dental Stem Cells 1507

Figure 2. Immunophenotype analysis of SCD and DPSCs at passage 5. Cells were tested against human antigens CD34, CD44, CD45, CD73, CD90, CD166, and HLA-DR. 7-Amino-actinomycin D (7-AAD) was used to check the viability of the cells. SD, standard deviation; CD, cluster of differentiations. Scale bar, 100 mmol/L. (Thisfigure is available in color online at www.aae.org/joe/.)
Basic Research—Biology
Chemicon) and rhodamine-conjugated anti-mouse IgG (1:500; Chem-icon). Slides were counterstained with 4’, 6’-diamidino-2-phenylindoledihydrochloride (DAPI; Chemicon) for 5 minutes. Fluorescent imageswere captured by using a Nikon Eclipse 90i microscope (Nikon, Tokyo,Japan) and Image-Pro Express software (Media Cybernetics, Inc, SilverSpring, MD).
Karyotype AnalysisCultures were treated with colcemid 2 hours before harvest,
detached by trysinization, and treated with 0.5 mol/L hypotonic solution(KCl/water) before fixing with Conroy’s solution (3:1 methanol/glacialacetic acid). The spreads were treated with 0.005% trypsin, stained withGiemsa (Sigma Aldrich), and 20–30 separate metaphase spreads wereexamined for each culture.
Data and Statistical AnalysisThe descriptive statistical analyses were performed by using the
software SPSS for Windows (Version 11.0; SPSS Predictive Analytics,Chicago, IL). The data were analyzed by using two-way analysis of vari-ance (ANOVA). The significance level was set at P = .05. Tukey post hocmultiple comparison tests were carried out to determine the differencesbetween groups. To visualize the differences between SCD and DPSCs,we applied a novel approach based on principle component analysis(PCA) (Plymouth Routines In Multivariate Ecological Research version
1508 Govindasamy et al.
6 [PRIMER 6] software [http://www.zen87707.zen.co.uk/primer-e])on our pluripotent array results. PCA is a mathematical algorithmthat describes the data on the basis of their dissimilarity, so that a greaterdistance corresponds with a greater dissimilarity. The main aim of thistechnique is to reduce the dimensionality and to display the nature of thevariation present in the data. This is achieved by creating new variables,the’’ principle components’’ that are linear combinations of the obser-vations (19). The first principle component explains as much of thevariation as possible with a single statistic. The second principal compo-nent, which is uncorrelated with the first, accounts for as much aspossible of the remaining variation, and so on. If there are P variables,then it is possible to calculate P different principle components, but thefirst few will normally account for most of the variation, and these mighttherefore be used to describe the data without undue loss of information(20).
ResultsIsolation and Characterization of SCD and DPSCs
Morphologic characteristics of SCD and DPSCs displayed indistin-guishable fibroblastic morphology resembling that of BM-MSCs(Fig. 1A, B). The colony-forming properties of SCD and DPSCs wereassessed. The CFUs were higher in SCD as compared with those ofDPSCs (P < .05) (Table 2). The number and size of colonies weremore in SCD than in DPSCs, indicating that SCD has higher
JOE — Volume 36, Number 9, September 2010

Figure 3. In vitro mesoderm differential potentiality of SCD and DPSCs. Osteogenesis was confirmed by mineralized matrix deposition stained with von Kossastaining at day 21 in SCD (A) and DPSCs (B) followed by confirmation of osteogenesis at mRNA level; mRNA expression of osterix and osteocalcin by RT-PCRby using SYBR green reagent, and values were normalized to 18sRNA. Adipogenesis was detected by neutral oil droplet formation stained with oil red O at day21 in SCD (C) and DPSCs (D). Chondrogenesis was detected by the presence of proteoglycans stained with alcian blue at day 21 in SCD (E) and DPSCs (F).All experiments were conducted at passage 5. Results represent average of 5 culture replicates. (This figure is available in color online at www.aae.org/joe/.)
Basic Research—Biology
proliferation rate than DPSCs (Fig. 1C, D). This result reflected thegrowth kinetics of the cells. After the end of passage 5, overall cellyield was significantly higher in SCD (25� 106 cells) in T25 cm2 flaskas compared with DPSCs (21 � 106 cells) (Fig. 1E) (P < .05). Thetime required for PD varied between approximately 27 hours (P1) and29 hours (P5) for SCD, whereas approximately 28 (P1) and 29 hours(P5) were observed in DPSCs (Fig. 1F). We further analyzed cell cycleanalysis of SCD and DPSCs at passage 5. Flow cytometry analysis re-vealed that the percentage of proliferation rate was higher in SCD (S+ G2 + M = 12.4� 1.48) (P < .05) with approximately 85% of cellsin phase G1/GO, as compared with that of DPSCs (S + G2 + M = 10.4
JOE — Volume 36, Number 9, September 2010 Inherent Pr
� 1.18) with approximately 90% of the cells in phase G1/GO (Table 2;Fig. 1G, H).
Cell Surface Antigen Profile of SCD and DPSCsImmunophenotyping of stem cells derived from SCD or DPSCs
showed that the cells were negative for hematopoietic markers (21)CD34 and CD45 and HLA-DR, whereas more than 90% of cells werepositive for mesenchymal stem cell markers (22) CD44, CD73,CD90, and CD166. Cells from SCD expressed higher percentage ofCD166 (98.11 � 0.8) (P < .05) than cells derived from DPSCs(79.85 � 6.8) (Table 2; Fig. 2).
opensity Lineage-specific Potential of Various Sources of Dental Stem Cells 1509

Figure 4. Karyotyping analysis of SCD and DPSCs. (A) Karyotype expanded in SCD and DPSCs at passage 5 revealed chromosomal stability. Results are represen-tative of 3 experiments.
Basic Research—Biology
Differentiation of SCD and DPSCs Into Classic LineagesOsteogenic differentiation was confirmed in both SCD and DPSCs
by the deposition of a silver-stained mineralized matrix (Fig. 3A, B).Percent mineralization was 59 � 5 for SCD and 64 � 8 for DPSCs,respectively (Table 2). The mRNA expression of 2 osteoblast markers,osteocalcin and osterix (22, 23), was found to be higher in SCD ascompared with DPSCs. Observations from the real-time PCR analyseswere in line with the results from the staining assays. Adipogenic differ-entiation was confirmed in both SCD and DPSCs by the accumulation ofneutral lipid vacuoles (Fig. 3C, D). After adipogenic induction, 58%�8% of SCD and 45%� 6% of DPSCs possessed cells with an adipogenicphenotype (Table 2). Thus, a higher number of SCD (P < .05) than thatof DPSCs featured an adipogenic differentiation capacity. Chondrogenicdifferentiation was confirmed by the formation of spheres in the micro-mass culture and the secretion of cartilage-specific proteoglycans stain-able. Both SCD and DPSCs demonstrated a cartilage-like phenotype withchondrocyte-like lacunae (Fig. 3E, F).
Cytogenetic Stability of SCD and DPSCsBoth SCD and DPSCs showed normal karyotypes at passage 5. A
representative ideogram is illustrated in Fig. 4.
Pluripotent Gene Array Analysis between SCD and DPSCsPluripotent marker profiles of SCD and DPSCs were compared
with BM-MSCs as a calibrator to evaluate the stability of the gene expres-sion profile over the course of culture. Forty-one genes were up-regulated, whereas 12 genes were down-regulated in either SCD orDPSCs as compared with BM-MSCs (Fig. 5A–C). On the whole, thepluripotent was highly maintained in SCD as compared with DPSCsand BM-MSCs. The expression profiles (ratio [DPSCs were kept at1]) of some of the pluripotent markers (16, 23) between DPSCs andSCD at passage 5 were as follows: POU5F1 (OCT3/4) (18.54); TDGF1(17.98); SOX2 (10.14); GABR3 (21.73); GAL (32.4); IFTM1(28.40); and LIN28 (9.72). We also found that SCD expressed some
1510 Govindasamy et al.
of the endoderm and mesoderm markers such as GATA6, GATA4,SOX17, CDH5, FLT1, and DES (22, 23) as compared with DPSCs.Interestingly, DPSCs expressed higher neuron/ectoderm markers(24). The expression profiles (ratio [SCD was kept at 1]) at passage5 were as follows: nestin (10.08); GBX2 (1.14); PAX6 (1.50); andTH (2.09). PCA (Fig. 5D), on the basis of up-regulated genes, showed98.7% of all the variance between the experimental groups (SCD andDPSCs at passages 1 and 5) could be described by using the first(#PC1) and second principle (#PC2) component analysis. The remain-ing principle component (#PC3) had minor contributions to the totalgene expression variance and produced no significant shifts betweenthe experimental groups.
Confirmation of Pluripotent Array AnalysisThe expression of OCT4, SOX2, and NANOG was significantly up-
regulated (P < .05) in SCD as compared with DPSCs (Fig. 6A, B). Onthe contrary, the expression of some of the neuron markers (25)(PAX6, NUUR1, nestin, b-III tubulin) was up-regulated in DPSCscompared with in SCD. These results were consistent with the pluripo-tent array results (Fig. 6A, C).
Neuronal Differentiation in SCD and DPSCsAs shown in Fig. 7A, B, both SCD and DPSCs are capable of forming
3 distinct neurospheres. The neurospheres counted at day 15 revealedthat DPSCs had a significantly increased number of neurites ascompared with SCD. The total neurospheres counted per 10 mm2
between SCD and DPSCs were as follows: 30� 7 and 39� 9, respec-tively, (P < .001) in the range of neurosphere sizes from 60–80 mmol/L; 29 � 1 and 25 � 5, respectively, in the range of neurosphere sizesfrom 81–100 mmol/L; and 9 � 1 and 12 � 2, respectively, in neuro-sphere sizes greater than 100 mmol/L (Fig. 7C). Once attached in coateddish at day 16, these neurospheres spontaneously show outgrowth anddendrite-like structure by day 5 (Fig. 7D–I). Real-time PCR showeda higher expression of neuronal markers (23) (bIII-tubulin, NF,
JOE — Volume 36, Number 9, September 2010

Figure 5. Expression profile of pluripotent/stem cells and lineage markers of SCD and DPSCs at passages 1 and 5. Expression levels of set of pluripotent/lineagemarker genes. Gene levels were normalized against 18s, and mRNA from BM-MSCs was used as calibrator. (A) The genes were represented in the heat map (lowexpression in black and high expression in red); (B) percentage of up-regulated genes in SCD or DPSCs as compared with BM-MSCs; (C) percentage of down-regulated genes in SCD or DPSCs as compared with BM-MSCs; (D) PCA of pluripotent/stem cells and lineage markers of SCD and DPSCs. Cells were plotted accord-ing to their coordinates on PC1 and PC2. (This figure is available in color online at www.aae.org/joe/.)
Basic Research—Biology
GFAP; P < .05; P < .001) with the down-regulation of OCT4 in neuronalcells differentiated from DPSCs, as compared with neuronal cells differ-entiated from SCD (Fig. 7J). This was also established at protein level(Fig. 7K–N).
DiscussionThe aim of this study was to characterize and to assess the propen-
sity toward specific lineage of SCD and DPSCs. The growth kineticsresults revealed that SCD possessed higher proliferation rate thanDPSCs. Our results are concurrent with previous reports on thecomparison between SCD and DPSCs (26). The use of SCD and DPSCsis easy for several reasons. The first and foremost reason is the ease ofisolation, noninvasive collection with less or no ethical issues comparedwith BM-MSCs (26).
We further demonstrated that both SCD and DPSCs were able todifferentiate into osteoblasts, adipocytes, and chondrocytes, thus qual-ifying the minimum requirement of MSCs (27). However, quantification
JOE — Volume 36, Number 9, September 2010 Inherent P
results of osteogenic and adipogenic indicated that SCD exhibited betterdifferentiation capability than DPSCs. SCD was regarded as a novel pop-ulation of stem cells that is capable of differentiating into various celltypes (at both in vitro and in vivo) into osteoblasts, odontoblasts,adipocytes, chondrocytes, and even hepatocytes (12, 28–30). On theother hand, DPSCs were considered to be more appropriatecandidates for dental tissue regeneration (31) and neurodegenerativediseases (32). Nonetheless, most of the stem cells might differentiatein vitro into the desirable cells through well-defined transcriptionalcascade, which can be initiated experimentally with xenobiotics suchas IBMX, dexamethasone, and insulin (33–35).
In the current study we have investigated the inherent propensity ofthe stem cells to differentiate into their natural destiny on the basis oftheir origin. We found that SCD highly expressed many pluripotentmarkers as compared with DPSCs. Similar findings have been reportedpreviously by our group (16) by using Wharton’s jelly mesenchymalstem cells (WJ-MSCs), whereby higher expression of pluripotentmarkers was found in WJ-MSCs as compared with BM-MSCs. Hence,
ropensity Lineage-specific Potential of Various Sources of Dental Stem Cells 1511

Figure 6. Expression profile of pluripotent and lineage-specific stem cell markers of SCD and DPSCs. (A) Semiquantitative RT-PCR of selected pluripotent/stemcells and lineage markers. (B) Relative levels of selected pluripotent/stem cells and lineage markers were performed by Taqman-based assay qRT-PCR. (C) Relativelevels of selected pluripotent/stem cells and lineage markers were performed by SYBR green–based qRT-PCR. The lower the CT value, the more copies are present inthe specific sample. Values are presented after normalized to 18s RNA level. The average of 2 replicates is displayed.
Basic Research—Biology
these data support the notion that SCD is more primitive or pluripotentpopulation of cells similar to WJ-MSCs. One of the striking features ofthis study is the overexpression of many transcription factors such asPOU5F1 (also known as OCT3/4), SOX2, NANOG, and LIN28 that areresponsible for the maintenance of pluripotency in early embryosand embryonic stem cells (36, 37). The abundant persistence ofthese markers leading to stemness status was very recently shownwhere limbal progenitor cells could be induced to pluripotent stemcells with the characteristics of embryonic stem cells under differentculture conditions and without induction of exogenous transcriptionfactors (38). Given that cells from the same organ or tissue will sharesome commonalities in gene expression and share the same microen-vironmental niche (39), we hypothesize that the generation ofectoderm-specific cell type would be highly efficient as comparedwith BM-MSCs, because DPSCs are of neural crest origin (4). On thebasis of our results, we predicted that SCD could also be forced toform desired cell type under the influence of appropriate microenviron-ment. PCA performed on the dataset by using the regulated genesshowed that SCD and DPSCs exhibited a distinct expression pattern.
1512 Govindasamy et al.
Van de Waterbeemd et al (40) used this PCA method to study the optimalharvest point in bacterial vaccine production, and Liu et al (41)described the detection of endogenous signaling activation pathwaysby an oncogenic stimulus. Here we show yet another novel facet ofPCA method to distinguish between gene expression pattern of SCDand DPSCs.
Dental cells are neural crest derived (4), and because neural creststem cells can differentiate into neural cells in vivo (42, 43), dentalpulp stem cells are likely to have a greater potential for neuraldifferentiation than any other stem cells. However, our data revealeddifferential admixture of lineage proclivity between DPSCs and SCD,although both came from the same origin. The ectoderm lineagecommitment of DPSCs was reflected by their ability to express higherneuronal mRNA in undifferentiated state. To test whether thevariation of neuronal mRNA found in undifferentiated DPSCs and SCDwill reflect their end point differentiation, we detouredundifferentiated DPSCs and SCD cells into neuronal cells andcharacterized them. A generally accepted experiment for thepresence of neuronal cells is the induction of neurospheres (44–46)
JOE — Volume 36, Number 9, September 2010

Figure 7. Schematic overview of the generation of neurospheres in SCD and DPSCs and gene expression profile of selected neuron markers. (A, B) Formation ofneurosphere in non-coated dish for 15 days under neuron media in SCD and DPSCs, respectively; (C) the neurospheres formed under neuron-condition media atday 15. The number of neurosphere was divided with small (61–80 mmol/L), medium (81–100 mmol/L), and large diameters (>100 mmol/L). (D, E) Neuro-spheres were transferred into a coated dish at day 16 and were migrated radially out of the sphere in SCD and DPSCs, respectively. (F, G) After 2 days of maturation,cells had morphologic features typical of neuron in SCD and DPSCs, respectively. (H, I) After 5 days of maturation, dendrite-like outgrowth from SCD and DPSCs,respectively, showing complex neuronal processess (arrow and insert); (J) gene expression profile of OCT4, nestin, b-III tubulin, GFAP, and NF at day 20 in SCDand DPSCs. (K–N) Specific co-immunocytochemical staining of neurospheres indicated the presence of b-III tubulin and GFAP at day 20 in SCD and DPSCs, respec-tively. In both co-immunocytochemical pictures, nuclei were stained with DAPI (blue) and OCT4 (green); )P < .05, ))P < .01, and )))P < .001. (This figureis available in color online at www.aae.org/joe/.)
Basic Research—Biology
JOE — Volume 36, Number 9, September 2010 Inherent Propensity Lineage-specific Potential of Various Sources of Dental Stem Cells 1513

Basic Research—Biology
in which cells aggregate to floating spheres. We found higherneurospheres in DPSCs as compared with SCD. One of the probablereasons could be the tremendous fold expression of nestin that wasfound in DPSCs as compared with SCD. Nestin, the marker forneuroepithelial stem cells (47, 48), seems to be essential for theinduction of neurospheres (49). Wislet-Genedebien et al (50) gener-ated neurospheres only from rat BM-MSCs after induction of nestinexpression by supplementation with N2 and B27. This abundant expres-sion of nestin could potentially enable DPSCs to differentiate more effi-ciently than SCD into neural cells and/or act neuroprotective aftertransplantation. Whether DPSCs indeed possess the ability to differen-tiate into neuronal committed cells is currently under investigation.We are aware that the expression of 1 or 2 markers like GFAP, NF, orbIII-tubulin is not sufficient proof for neuronal functionality. Neverthe-less, our finding is a step forward in evaluating higher propensity ofDPSCs toward neuronal lineage as compared with SCD, which is noveland unexpected.In conclusion, our study showed that gene variations occurredwithin the different sources of the same stem cells, and these variationsdetermine their lineage propensity toward a specific destination. Fromthis study we infer that SCD retained their plasticity over the passages,whereas DPSCs lost their plasticity and were shown to be morecommitted toward neuronal lineage. Our results clearly demonstratedthat both SCD and DPSCs could act as useful candidates for regenerativemedicine in various diseases, emphasizing the usage of DPSCs forneurologic diseases.
AcknowledgmentsThis work was funded by University Malaya Research Grant
(UMRG/RG073/09HTM) under Stempeutics Research Malaysia SdnBhd and University Malaya joint research collaboration. We are grate-ful to Ms Saratha Thevi Thrichelvam, Stempeutics Research MalaysiaSdn. Bhd, Kuala Lumpur, Malaysia for her assistance in FACS, karyo-typing, cell cycle data analysis and Ms Srinda Nathan from AnalisaResources for helping with TLDA pluripotent microarray.
References1. Gronthos S, Mankani M, Brahim J, et al. Postnatal human dental pulp stem cells
(DPSCs) in vitro and in vivo. Proc Natl Acad Sci U S A 2000;97:13625–30.2. Ikeda E, Yagi K, Kojima M, et al. Multipotent cells from the human third molar: feasi-
bility of cell-based therapy for liver disease. Differentiation 2008;76:495–505.3. D‘Aquino R, De Rosa Alfredo, Lanza V. Human mandible bone defect repair by the
grafting of dental pulp stem/progenitor cells and collagen sponge biocomplexes.Eur Cell Mater 2009;18:75–83.
4. Lumsden AG. Spatial organization of the epithelium and the role of neural crest cellsin the initation of the mammalian tooth germ. Development 1988;103:155–69.
5. Seo BM, Miura M, Gronthos S, et al. Investigation of multipotent postnatal stem cellsfrom human periodontal ligament. Lancet 2004;364:149–55.
6. Sonoyama W, Liu Y, Fang D, et al. Mesenchymal stem cell-mediated functional toothregeneration in swine. PLoS ONE 2006;1:e79.
7. Gronthos S, Brahim J, Li W, et al. Stem cell properties of human dental pulp stemcells. J Dent Res 2002;81:531–5.
8. Laino G, Carinci F, Graziano A, et al. In vitro bone production using stem cellsderived from human dental pulp. J Craniofac Surg 2006;17:511–5.
9. Iohara K, Zheng L, Ito M, et al. Side population cells isolated from porcine dentalpulp tissue with self-renewal and multipotency for dentinogenesis, chondrogenesis,adipogenesis, and neurogenesis. Stem Cells 2006;24:2493–503.
10. Zhang W, Walboomers XF, Van Kuppevelt TH, et al. In vivo evaluation of humandental pulp stem cells differentiated towards multiple lineages. J Tissues EngRegen Med 2008;2:117–25.
11. Takeyasu M, Nozaki T, Daito M. Differentiations of dental pulp stem cells into neurallineage. Pediatric Den J 2006;16:154–62.
12. Ishkitiev N, Yaegaki K, Calenic B, et al. Deciduous and permanent dental pulpmesenchymal cells acquire hepatic morphologic and functional features in vitro.J Endod 2010;36:469–74.
1514 Govindasamy et al.
13. Arthur A, Rychkov G, Shi S, et al. Adult human dental pulp stem cells differentiatetoward functionally active neurons under appropriate environmental cues. StemCells 2008;26:1787–95.
14. Gandia C, Arminan A, Garcia-Verdugo JM, et al. Human dental pulp stem cellsimprove left ventricular function, induce angiogenesis and reduce infarct size inrats with acute myocardial infarction. Stem Cells 2008;26:638–45.
15. Pal R, Totey S, Mamidi MK, et al. Propensity of human embryonic stem cell linesduring early stage of lineage specification controls their terminal differentiationinto mature cell types. Exp Biol Med 2009;234:1230–43.
16. Nekanti U, Rao VB, Bahirvani AG, et al. Long-term expansion and pluripotent markerarray analysis of Wharton’s Jelly-derived mesenchymal stem cells. Stem Cells Dev2010;19:117–30.
17. Lindroos B, Maenpaa K, Ylikomi T, et al. Characterization of human dental stemcells and buccal mucosa fibroblasts. Biochem Biophys Res Commun 2008;368:329–35.
18. Pal R, Hanwate M, Jan M, et al. Phenotypic and functional comparison of culturecondition for upscaling of bone marrow derived mesenchymal stem cells.J Tissue Eng Regen Med 2009;3:163–74.
19. Afifi AA, Azen SP. Statistical analysis: a computer oriented approach. 2nd ed. NewYork: Academic Press; 1979.
20. Jollifte IT. Principle component analysis. 2nd ed. Aberdeen, UK: Springer Series inStatistics; 2002.
21. Nakamura S, Yamada Y, Baba S, et al. Culture medium study of human mesenchymalstem cells for pratical use of tissue engineering and regenerative medicine. J Bio-Medical Materials and Engineering 2008;18:129–36.
22. Karaoz E, Dogan BN, Aksov A, et al. Isolation and in vitro characterization of dentalpulp stem cells from natal teeth. Histochem Cell Biol 2010;133:95–112.
23. Morsceck C, Vollner F, Saugspier M, et al. Comparison of human dental follicle cells(DFCs) and stem cells from human exfoliated deciduous teeth (SCD) after neuraldifferentiation in vitro [published online ahead of print July 10, 2009]. Clin OralInvest doi:10.1007/s00784-009-0310-4.
24. Vescovi AL, Reynolds BA, Fraser DD, et al. bFGF regulates the proliferative fate ofunipotent (neuronal) and bipotent (neuronal/astroglial) EFG-generated CNSprogenitor cells. Neuron 1993;11:951–66.
25. Vollner F, Ernst W, Driemel O, et al. A two-step strategy for neuronal differentiationin vitro of human dental follicle cells. Differentiation 2009;77:433–41.
26. Nakamura S, Yamada Y, Katagiri W, et al. Stem cell proliferation pathways compar-ison between human exfoliated deciduous teeth and dental pulp stem cells by geneexpression profile from promising dental pulp. J Endod 2009;35:1536–42.
27. Dominici M, Blanc KL, Mueller I, et al. Minimal criteria for defining multipotentmesenchymal stromal cells: the international society for cellular therapy positionstatement. Cytotherapy 2006;8:315–7.
28. Koyama N, Okubo Y, Nakao, et al. Evaluation of pluripotency in human dental pulpcells. J Oral Maxillofac Surg 2009;67:501–6.
29. Kerkis I, Kerkis A, Dozortsev, et al. Isolation and characterization of a population ofimmature dental pulp stem cells expressing Oct-4 and other embryonic stem cellmarkers. Cells Tissues Organs 2006;184:105–16.
30. Miura M, Gronthos S, Zhao M, et al. SCD: stem cells from human exfoliated decid-uous teeth. Proc Natl Acad Sci U S A 2003;100:5807–12.
31. Batouli S, Miura M, Brahim J, et al. Comparison of stem-cell-mediated osteogenesisand dentinogenesis. J Dent Res 2003;82:976–81.
32. Sasaki R, Aoki S, Yamato M, et al. Neurosphere generation from dental pulp of anadult rat incisor. Eur J Neurosci 2008;27:538–48.
33. Owen M, Friedenstein AJ. Stromal stem cells: marrow-derived osteogenic precur-sors. Ciba Found Symp 1988;136:42–60.
34. Toma C, Pittenger MF, Cahill KS, et al. Human mesenchymal stem cells differentiateto a cardiomycte phenotype in the adult murine heart. Circulation 2002;105:93–8.
35. Dennis JE, Merriam A, Awadallah A, et al. A quadripotential mesenchymal progen-itor cell isolated from the marrow of an adult mouse. J Bone Miner Res 1999;14:700–9.
36. Niwa H. How is pluripotency determined and maintained? Development 2007;134:635–46.
37. Pesce M, Anastassiadis K, Scholer HR. Oct-4: lessons of totipotency from embryonicstem cells. Cells Tissues Organs 1999;165:144–52.
38. Balasubramanian S, Babai N, Chaundhuri A, et al. Non cell-autonomous reprogram-ming of adult ocular progenitors: generation of pluripotent stem cells without exog-enous transcription factors. Stem Cells 2009;12:3053–62.
39. Ma D, Ma Z, Zhang X, et al. Effect of age and extrinsic microenvironment on theproliferation and osteogenic differentiation of rat dental pulp stem cell in vitro.J Endod 2009;35:1546–53.
40. Van de Waterbeemd B, Streefland M, Peenings J, et al. Gene-expression-basedquality indicates optimal harvest point in Bordetella pertussis cultivation for vaccineproduction. Biotechnol Bioeng 2009;103:900–8.
41. Liu Z, Wang M, Alvarez JV, et al. Singular value decomposition-based regression acti-vation of endogenous signaling pathways in vivo. Genome Biol 2008;9:R180.
JOE — Volume 36, Number 9, September 2010

Basic Research—Biology
42. Lasky JL, Wu H. Notch signaling, brain development and human disease. Pediatr Res2005;57:104R–9.43. Pardal R, Ortega-Saenz P, Duran R, et al. Glial-like stem cells sustain physiologic
neurogenesis in the adult mammalian carotid body. Cells 2007;131:364–77.44. Cattaneo E, McKay R. Proliferation and differentiation of neuronal stem cells regu-
lated by nerve growth factor. Nature 1990;347:762–5.45. Reynolds BA, Weiss S. Generation of neurons and astrocytes from isolated cells of
the adult mammalian central nervous system. Science 1992;255:1707–10.46. Stroch A, Paul G, Csete M, et al. Long term proliferation and dopaminergic differ-
entiation of human mesencephalic neural precursor cells. Exp Neurol 2001;170:317–25.
JOE — Volume 36, Number 9, September 2010 Inherent P
47. Dahlstrand J, Lardelli M, Lendahl U. Nestin mRNA expression correlates with thecentral nervous system progenitor cell state in many, but not all, regions of devel-oping central nervous system. Brain Res Dev 1995;84:109–29.
48. Lendahl U, Zimmerman LB, McKay RD. CNS stem cells express a new class of inter-mediate filament protein. Cells 1990;60:585–95.
49. Tropepe V, Hitoshi S, Sirard C, et al. Direct neural fate specification from embryonicstem cells: a primitive mammalian neural stem cell stage acquired through a defaultmechanism. Neuron 2001;30:65–78.
50. Wislet-Gendebien S, Leprince P, Moonen G, et al. Regulation of neural markers nes-tin and GFAP expression by cultivated bone marrow stromal cells. J Cell Sci 2003;116:3295–302.
ropensity Lineage-specific Potential of Various Sources of Dental Stem Cells 1515

Basic Research—Biology
Comparison of Tetraacetylethylendiamine + SodiumPerborate and Sodium Hypochlorite Cytotoxicityon L929 FibroblastsGabriella Simbula, PhD,* Claudia Dettori, DDS,
†Tania Camboni, PhD,*
and Elisabetta Cotti, DDS, MS†
Abstract
Introduction: Tetraacetylethylenediamine in associa-tion with sodium perborate (TAED+P) can be suggestedfor its use as an endodontic disinfectant because of itsantimicrobial activity against different bacterial specieswhen used at low concentrations. The purpose of thisstudy was to measure the cytotoxicity of TAED+P onL929 fibroblasts and to compare it with that of sodiumhypochlorite (NaOCl). Methods: L929 fibroblasts weregrown in Dulbecco Modified Eagle Medium containing10% fetal calf serum (FCS) at 37�C and 5% CO2. Atconfluence, cells were split, plated in a 96-well plate,and incubated for 24 hours to allow attachment. Thetwo disinfectants TAED+P and NaOCl were tested atvarious concentrations. The neutral red uptake and the3-(4,5-dimethylthiazol-2-yl)-2,5 diphenyl tetrazoliumbromide assays were used to evaluate the cell viability.The 50% inhibitory dose values for both disinfectantswere calculated and statistically analyzed. The effectof both disinfectants on fibroblast viability was alsodetermined in the presence of various concentrationsof FCS. One-way analysis of variance with post hoc anal-ysis using Tukey multiple comparison test was used forparametric data. Results: Both disinfectants induceda dose-related loss of cell viability; TAED+P resultedless cytotoxic than NaOCl in all the examined experi-mental conditions. Conclusions: These data supportthe possible use of TAED+P as an endodontic irrigant.Further studies are required to analyze its antibacterialactivity against endodontic pathogens. (J Endod2010;36:1516–1520)Key WordsCytotoxicity, endodontic irrigation, sodium perborate,tetraacetylethylenediamine
From the * Department of Toxicology, Oncology and Mole-cular Pathology Unit, University of Cagliari, Cagliari, Italy; and†Department of Conservative Dentistry and EndodonticsUniversity of Cagliari, Cagliari, Italy.
Address requests for reprints to Dr Elisabetta Cotti, viaRoma #149, Cagliari, 09124, Italy. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.010
1516 Simbula et al.
It is well recognized that a variety of anaerobic and facultative aerobic bacterial speciesrepresent the main etiologic agent of pulp necrosis and apical periodontitis (1). The
growth of microbial species in the endodontic environment form dense bacterial bio-films (1–4) that may be associated with refractory periapical periodontitis (5, 6)because it offers an increased resistance to antimicrobial agents (7, 8).
The primary aim for the prevention and treatment of apical periodontitis consistson the eradication of microorganisms from the endodontic system. Because mechanicalinstrumentation of the root canal alone is not sufficient to reduce endodontic infectionand to promote healing, copious irrigation with antibacterial products in combinationwith the endodontic instrumentation and the application of antimicrobial medicationsbetween two successive appointments is necessary to achieve a considerable reductionin bacterial counts (1, 9).
The ideal endodontic irrigating solution should have a broad antibacterial spec-trum, dissolve necrotic tissue debris, and prevent the formation of smear layer or re-move it when it is formed (9). Furthermore, it should be biocompatible with livehost tissues (9). Sodium hypoclorite (NaOCl), at different concentrations, representsthe most commonly used endodontic irrigating solution because of its broad spectrumof antimicrobial activity and its properties to dissolve necrotic tissues (8, 9). Becauseirrigation with NaOCl is still not predictably effective, recent studies have focused onsearching for an alternative solution (9, 10, 11).
Tetraacetylethylenediamine in association with sodium perborate (TAED+P) canbe suggested for its use as an endodontic disinfectant because of its antimicrobialactivity against different bacterial species when used at low concentrations (12). Sprattet al (12) investigated in vitro the decontamination efficacy of a TAED+P 3% solution(pH = 8), which is equivalent to 0.26% peracetic acid, against waterborne species ofa biofilm model. The contaminating oral species tested were Streptococcus oralis,Enterococcus faecalis, and Staphylococcus aureus. The authors concluded thatTAED+P provided effective control on the dental unit water line biofilms (12). Becauseof its capacity to release oxygen, TAED+P has also been tested as a bleaching activatorand compared with sodium–perborate–hydrogen peroxide and sodium perborate–distilled water mixtures. The data obtained showed that TAED+P may increase the effec-tiveness of the bleaching process in virtue to its ability to accelerate oxygen release fromsodium perborate–distilled water mixtures (13). On these bases, the aim of this study isto test the cytotoxicity TAED+P on L929 fibroblasts and to compare it with that of NaOCl,which is still the ‘‘gold standard’’ for endodontic irrigation (9) despite its possibleadverse effects (14).
Materials and MethodsChemicals
TAED+P (Perasafe; Antec International, Sufolk, UK) and 5% NaOCl (Niclor; Ogna,Muggio, Milano, Italy) were tested. Neutral red and (3-[4,5-dimethylthiazol-2-yl]-2,5diphenyl tetrazolium bromide) methyl-thiazolyl-diphenil-tetrazolium bromide (MTT)(Sigma Chemical Company, St Louis, MO) were used for the cytotoxicity tests.
JOE — Volume 36, Number 9, September 2010

*120
140
100
120
140
**** ***
4 hours2 hours
40
60
80
100
% V
iabi
lity
vs C
ontro
l%
Via
bilit
y vs
Con
trol
% V
iabi
lity
vs C
ontro
l%
Via
bilit
y vs
Con
trol
NaOCl
TAED+P
**** 40
60
80
NaOCl
TAED+P
*
0
20
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
Dose (%)
0
20
Dose (%)
100
120
140
****** 100
120
140
****** **
24 hours6 hours
20
40
60
80
NaOCl
TAED+P 20
40
60
80
NaOCl
TAED+P0
Dose (%)
0
Dose (%)
Figure 1. The effect of increasing concentrations of NaOCl and TAED+P on L929 cell viability determined by MTT assay. Results are the means � standard devi-ation from three separate experiments. Significantly different from control cells for *p < 0.05, **p < 0.01, and ***p < 0.001.
100
120
140
100
120
140
***
4 hours2 hours
20
40
60
80
% V
iabi
lity
vs C
ontro
l%
Via
bilit
y vs
Con
trol
% V
iabi
lity
vs C
ontro
l%
Via
bilit
y vs
Con
trol
NaOCl
TAED+P
***
20
40
60
80
NaOCl
TAED+P
***
0
20
Dose (%)
0
20
100
120
140
***100
120
140
*** *** *** ***
24 hours6 hours
20
40
60
80
NaOCl
TAED+P
****
20
40
60
80
NaOCl
TAED+P
****
0
20
0
20
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
Dose (%)
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
Dose (%)
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
Dose (%)
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
Figure 2. The effect of increasing concentrations of NaOCl and TAED+P on L929 cell viability determined by NRU assay. Results are the means � standard devi-ation from three separate experiments. Significantly different from control cells for *p < 0.05, **p < 0.01, and ***p < 0.001.
Basic Research—Biology
JOE — Volume 36, Number 9, September 2010 Comparison of TAED+P and NaOCl Cytotoxicity on L929 Fibroblasts 1517

Basic Research—Biology
Cell Line CultureThe L929 fibroblast cell line was supplied by Interlab Cell Line
Collection (Servizio Biotecnologie, IST, Genova, Italy). L929 cellswere maintained in Dulbecco medium (DMEM; Invitrogen Srl, Milan,Italy) supplemented with 2 mmol/L L-Glutamine (Invitrogen), 100IU/mL to 100 mg/mL of penicillin-streptomycin (Invitrogen), and10% fetal calf serum (FCS) (Hyclone Laboratories Inc, Logan, UT) ina humidified atmosphere of 5% CO2/95%O2 at 37�C. At confluence,cells were washed with Hanks’ balanced salt solution (Invitrogen),treated with 0.05% trypsin/0.5 mmol/L EDTA, and collected in culturemedia. Cell suspension was counted by microscope with a Neubauerchamber and seeded in 96-well microtrite plates at a concentrationof 1� 104 cells/well. Each experiment was conducted using six culturesfor each group; 2% TAED+P and 5% NaOCl were dissolved in distilledwater and added to the culture medium to the final concentrations spec-ified in the text in the presence or in the absence of FCS. The cytotoxicityof the two disinfectants was evaluated after a 2-, 4-, 6-, and 24-hourincubation period.
Cell ViabilityThe cytotoxity of the test materials was examined at doses ranging
from 0.0025% to 0.5%. Cell viability was determined by the neutral reduptake (NRU) and MTT assays. Determination of the viability of theadherent cells by NRU assay was performed according to Borefreundand Puerner (15). The percentage of cell viability at each dose wascalculated by comparing the absorbance of each dose with the control(untreated cells). For the MTT assay, 200 mL of 1:10 diluted MTT stock(5 mg/mL of MTT in Hanks’ balanced salt solution) was added to eachculture. A cell-free blank was included for each experiment. After incu-
120
60
80
100
0% FCS
2% FCS
NaOCl 24h
0
20
40 5% FCS
10% FCS
% V
iabi
lity
vs C
ontro
l
100%
50%
75%
***
*** ***
0%
25%
Perc
enta
ge In
hibi
tion
(ID%
)
Dose (%)
0
0.002
50.0
05
0.007
5
0.012
5
Dose (%)
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
Figure 3. (A) The dose-related inhibition of cell proliferation by TAED+P comparehours. (B) The effect of increasing concentrations of TAED+P or NaOCl on L929 celcells for *p < 0.05, **p < 0.01, and ***p < 0.001. (This figure is available in co
1518 Simbula et al.
bation for 4 hours, 200 mL of destaining solution (isopropanol–10%NP40-0.4N HCl) was added to each well. The absorbance ofeach well was determined using the Packard Spectra Count microplatereader (Packard Instrument Co, Downers Grove, IL) at the wavelengthof 570 nm with the background subtraction at 690 nm. To make datacomparable between NaOCl and TAED+P, the percentage of cell viabilityat each tested dose was calculated by comparing the absorbance of eachdose with the control (untreated cells).
Statistical AnalysisInstant software Prism 5 (GraphPad Software, San Diego, CA) was
used to analyze the data. One-way analysis of variance with the post hocanalysis using the Tukey multiple comparison test was used for para-metric data. A p value of <0.05 was considered statistically significant.
ResultsThe effect of NaOCl and TAED+P solutions at concentrations
ranging from 0.0025% to 0.5% on cell viability was assessed by NRUand MTT assays. The viability of untreated cells remained unchangedall throughout the experimental period.
Both disinfectants NaOCl and TAED+P induced a dose-relatedinhibitory effect on the cell viability of L929 fibroblasts (Figs. 1 and2). Supporting the known cytotoxic action of NaOCl on cultured fibro-blasts, the earliest toxic effect was detected by MTT assay already 2 hoursafter treatment in the presence of NaOCl concentrations $0.025%,where a 60% of cell loss was observed. Moreover, a progressivedecrease in cell viability was observed at 4, 6, and 24 hours with allthe NaOCl tested concentrations except for the 0.0025% dose, whichdid not affect cell viability as compared with viability of the untreated
120 TAED+P 24h
60
80
100
0% FCS
2% FCS
0
20
40 5% FCS
10% FCS
% V
iabi
lity
vs C
ontro
l
NaOCl
TAED+P
ID
***
50
0.025 0.0
5 0.5
Dose (%)
0
0.002
50.0
05
0.007
5
0.012
50.0
25 0.05 0.5
d with NaOCl at concentrations 0.0025% up to 0.5% using the MTT assay at 24l viability in the presence or absence of FCS. Significantly different from controllor online at www.aae.org/joe/.)
JOE — Volume 36, Number 9, September 2010

Basic Research—Biology
cells. Similar results were obtained with the NRU method (Fig. 2) even ifthe effect observed at early time points (2, 4, and 6 hours) was lessdramatic because of the reduced sensitivity of NRU assay comparedwith MTT in detecting viability of the cells. Data obtained by testingthe effect of various concentrations of TAED+P on cell viability showedthat this disinfectant is less toxic than NaOCl at concentrations #0.025at each examined time point; the difference in the activity of the twodisinfectant was more pronounced at 24 hours. From examinationwith the optic microscope (data not shown), it appeared that TAED+Ptreatment with doses ranging from 0.0025% to 0.025% induced lesschanges in the morphology of fibroblasts compared with NaOCl ateach time point evaluated.Figure 3A presents the 50% inhibition dose values for both disin-fectants. The 50% inhibition dose of NaOCl and TAED+P was estimatedat 50 mg/mL (0.005%) and at 350 mg/mL (0.035%), respectively. Anal-ysis of the statistical data showed that TAED+P is less cytotoxic thanNaOCl.
Because the MTT assay was shown to be more sensitive than theNRU assay in detecting variation in cell viability, the following experi-ments were performed by MTT assay. The presence of different FCSconcentrations, ranging from 0% to 10%, may mimic what happensin vivo in the presence of tissue damage. Therefore, we determinedthe effect on fibroblasts viability of both disinfectants also in the pres-ence of increasing FCS concentrations.
200*
30 min.
100
150NaOCl**
***
***
0
50% V
iabi
lity
vs C
ontro
l
TAED+P
Dose (%)
100
150
200
NaOCl
*** *** ****** ***
30 min.+24hours
0
50% V
iailit
y vs
Con
trol
TAED+P
00.0
025
0.005
0.007
5
0.012
50.0
25 0.05 0.5 1
Dose (%)
00.0
025
0.005
0.007
5
0.012
50.0
250.0
5 0.5 1
Figure 4. The effect of increasing concentrations of TAED+P and NaOCl onL929 cell viability after 30 minutes of pretreatment and 24-hour release deter-mined by MTT assay. Results are the means � standard deviation from threeseparate experiments. Significantly different from control cells for *p < 0.05,**p < 0.01, and ***p < 0.001.
JOE — Volume 36, Number 9, September 2010
As indicated in Figure 3B, the presence or absence of FCS did notinterfere with the efficacy of NaOCl and TAED+P at any of the testedconcentrations. Finally, we treated fibroblasts with increasing concen-trations of both TAED+P and NaOCl for 30 minutes, and then themedium was replaced with fresh medium without disinfectants to eval-uate the recovery of the cells 24 hours after the treatment.
Data obtained showed that although after 30 minutes the viabilityof cells treated with NaOCl and TAED+P were comparable at each testedconcentration, after 24 hours the cells treated with TAED+P (and notthe cells treated with NaOCl) appeared to be able to recover viabilityat low doses up to 0.025% (Fig. 4).
DiscussionIn order to reduce the number of microorganisms from
endodontic infection and to increase the chances for successful treat-ment and prevention of apical periodontitis, complete instrumentationof the root canal system should be accomplished in conjunction with theuse of an antibacterial irrigating solution (1, 9). During endodontictreatment, the irrigants can come in contact with the periradiculartissues, and in some instance they can create complications such astissue damage and subsequent degrees of discomfort to the patientwith possible interferences with the healing process (14). Therefore,it is important to select an irrigant with therapeutic benefits that couldbe weighed against its potential cytotoxic effects and to use a dilutedconcentration of the irrigant that still exhibits adequate antibacterialproperties. The purpose of our investigation was to test the cytotoxicityof TAED+P compared with that of NaOCl on L929 fibroblasts using theNRU and MTT assays.
The MTT method was shown to be more sensitive than the NRUassay in its ability to reveal cell loss (Figs. 1 and 2) in accordancewith previous studies (16). Our results regarding the cytotoxicity ofNaOCl are in agreement with those obtained by other researchers(17, 18) and support the suggestion to use this product at the lowestpossible concentration that is still effective (1%) (9).
In this study, TAED+P exhibited a cytotoxicity that was lower thanthat of NaOCl at concentrations #0.025 at each examined time point.Furthermore, only the fibroblasts treated with increasing concentra-tions of TAED+P for 30 minutes and then maintained in fresh mediumfor 24 hours were able to recover viability (Fig. 4). Finally, we didnot observe any interference of different calf serum (FCS) concentra-tions with the cytotoxic effect of both disinfectants, indicatinga stability of these compounds even in the presence of simulatedtissue damage.
In conclusion, both TAED+P and NaOCl induce a dose-related lossof cell viability, and from our results it appears that TAED+P is less cyto-toxic than NaOCl. These data support the possible use of TAED+P as anirrigating solution if the microbiological studies in progress confirm itsantibacterial activity against endodontic pathogens.
References1. Baumgartner JC, Siqueira JF, Sedgeley CM, et al. Microbiology of endodontic
disease. In: Ingle JI, Bakland LK, Baumgartner JC, eds. Ingle’s Endodontics. 6thed. Hamilton, Ontario: BC Decker Inc; 2008:221–308.
2. Spratt DA, Pratten J, Wilson M, et al. An in vitro evaluation of the antimicrobial effi-cacy on biofilms of root canal isolates. Int Endod J 2001;37:300–7.
3. Debicka P, Lipski M, Buckowska-Ralinska J, et al. Biofilm formation on root canal-review. Ann Acad Med Stetin 2008;54:152–6.
4. Leonardo MR, Rossi MA, Silva LAB, et al. EM evaluation of bacterial biofilm andmicroorganisms on the external root surface of human teeth. J Endod 2002;28:815–8.
5. Noguchi N, Noiri Y, Narimatsu M, et al. Identification and localization of extraradic-ular biofilm-forming bacteria associated with refractory endodontic pathogens.Appl Environ Microbiol 2005;71:8738–43.
Comparison of TAED+P and NaOCl Cytotoxicity on L929 Fibroblasts 1519

Basic Research—Biology
6. Chavez de Paz LE. Redefining the persistent infection in root canals: possible role ofbiofilm communities. J Endod 2007;33:652–62.7. Estrela C, Sydney BG, Figueiredo JAP, et al. A model system to study antimicrobial
strategies in endodontic biofilms. J Appl Oral Sci 2009;17:87–91.8. Estrela C, Sydney BG, Figueiredo JAP, et al. Antibacterial efficacy of intracanal medi-
caments on bacterial biofilm. J Appl Oral Sci 2009;17:1–7.9. Zehnder M. Root canal irrigants. J Endod 2006;32:389–98.
10. Giardino L, Ambu E, Savoldi E, et al. Comparative evaluation of antimicrobial efficacyof sodium hypochlorite and tetraclean against Enterococcus faecalis biofilm.J Endod 2007;33:852–5.
11. Torabinejad M, Shabahang S, Aprecio RM, et al. The antimicrobial effect of MTAD:an in vitro investigation. J Endod 2003;29:400–3.
12. Spratt DA, Latif J, Montebugnoli LL, et al. In vitro modeling of dental water linecontamination and decontamination. FEMS Microbiol Lett 2004;235:363–7.
1520 Simbula et al.
13. Celik EU, Turkun M, Yapar GD. Oxygen release of tetra acetyl ethylene diamine(TAED) and sodium perborate combination. Int Endod J 2008;41:571–6.
14. Hulsmann M. R}odig T, Nordmayer S. Complications during root canal irrigation. En-dod Topics 2009;16:27–63.
15. Borefreund E, Puerner JA. Cytotoxicity of metals, metal-metal and metal-chelatorcombinations assayed in vitro. Toxicology 1986;39:121–34.
16. Hidalgo E, Bartolome R, Barroso C, et al. Silver nitrate: antimicrobial activity relatedto cytotoxicity in human culture fibroblasts. Skin Pharmacol Appl Skin Physiol 1998;11:140–51.
17. Hildago E, Bartolome R, Dominguez C. Cytotoxicity mechanisms of sodium hypo-chlorite in cultured human dermal fibroblasts and its bactericidal effectiveness.Chem Biol Interact 2002;139:265–82.
18. Zhang W, Torabinejad M, Li Y. Evaluation of cytotoxicity of MTAD using the MTT-Tetrazolium method. J Endod 2003;29:654–7.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
Effects of Different Curing Units and Luting Agentson Push-out Bond Strength of Translucent PostsYahya Orcun Zorba, PhD,* Ali Erdemir, PhD,† Ali Turkyilmaz,† and Ayce Unverdi Eldeniz, PhD‡
Abstract
Introduction: The aim of this study was to evaluate theeffects of different curing units and 2 luting cements onthe push-out bond strength of a translucent fiber post.Methods: Thirty maxillary incisor roots were endodon-tically treated. Post spaces were prepared, and thesmear layers were removed. Posts (FRC Postec Plus)were luted with either a self-etch cement (Panavia F2.0) or a self-adhesive cement (Maxcem). Luting agentswere then light-activated with a quartz-tungsten-halogen, a blue light–emitting diode, or a plasma-arccuring unit. Roots/cemented posts were transversallysectioned from coronal to apical. Push-out tests wereperformed, and data were analyzed by using three-way analysis of variance and Tukey tests. Results:Push-out bond strengths were significantly affected bythe type of luting agent (P < .05) and root region (P <.05). The type of light source used in curing did not affectpush-out bond strengths (P > .05). Conclusions: Self-adhesive resin cement provided higher bond strengththan the self-etch cement when smear layer wasremoved before the post cementation. The push-outbond strength in the apical portion of the root wassignificantly lower than in the coronal region. The useof different curing units in the photoirradiation ofdual-cured resin cement did not affect the retention ofthe fiber post as a result of the limited light transmissioncapability of this post. (J Endod 2010;36:1521–1525)Key WordsCuring units, luting agents, push out bond strength
From the *Department of Restorative Dentistry andEndodontics, Faculty of Dentistry, Erciyes University, Kayseri,Turkey; †Department of Endodontics, Faculty of Dentistry,Kirikkale University, Kirikkale, Turkey; and ‡Department ofEndodontics, Faculty of Dentistry, Selcuk University, Konya,Turkey.
Address requests for reprints to Dr Yahya Orcun Zorba,Department of Restorative Dentistry and Endodontics, Facultyof Dentistry, Erciyes University, 38039, Melikgazi, Kayseri,Turkey. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.04.026
JOE — Volume 36, Number 9, September 2010
Fiber posts, in combination with resin cements, have been widely used to restoreendodontically treated teeth (1). The resin cements can be categorized according
to adhesion technique as etch-and-rinse, self-etch, or self-adhesive. Although all 3classes of cements have been investigated, the correct clinical choice among them isnot always clear (2).
In terms of polymerization, resin cements can be self-curing, light-curing, or dual-curing. Self-curing cement is difficult to manipulate and place because of its limitedworking time. Light-curing resin is not recommended for fiber-post cementationbecause of inadequate depth of cure in the apical portion of the root, even when trans-lucent posts are used (3). Dual-curing cement sets mainly through radical polymeriza-tion that is initiated by either light exposure or self-cures. Although dual-cured resincements have been recommended for the cementation of fiber posts, some dual-cured cements might not reach to an adequate degree of conversion in the absenceof light (4); therefore, light-curing is recommended (5). Adequate curing is consideredto be especially important in the apical portion of the root canal (6).
Various types of curing units are routinely available for the light activation ofcomposite resins, including quartz tungsten halogen (QTH), light-emitting diodes(LED), plasma arcs (PAC), and lasers (7). However, limited data are available aboutthe effects of different light sources on post bond strength.
The purpose of this in vitro study was to evaluate the effects of different light-curing techniques and adhesives on the retention of fiber posts in different root regions.The null hypothesis is that the push-out strength of root canal fiber posts is not signif-icantly affected by curing technique, type of adhesive system, or root region.
Materials and MethodsThirty extracted human maxillary incisor teeth with straight root canals were used
in this study. Crowns were removed to obtain a root height of 17 mm. A working lengthof 1 mm above the radiographic apex was established. The root canals were instru-mented by using stainless steel K-files (#08-10-15; Dentsply Maillefer, Ballaigues,Switzerland), Mtwo rotary nickel-titanium instruments (#10-15-20-25; Sweden & Mar-tina, Due Carrare, Padova, Italy), and .06 taper profiles (#30-35-40; Dentsply Maillefer)mounted in a 16:1 gear-reduction handpiece driven by an electric motor (X-Smart;Dentsply DeTrey GmbH, Konstanz, Germany). Instrumentation was performed undera loupe (Heine, Herrsching, Germany) at 2.5� magnification. The root canals wereirrigated with 2.5% sodium hypochlorite after each instrument. The root canals weredried with paper points and obturated with gutta-percha cones and AH Plus sealer(Dentsply) by using a lateral condensation technique with a finger spreader (ManiInc, Tochigi, Japan).
Immediately after obturation, the post spaces were prepared by removing 10 mmof gutta-percha by using a #2 Peeso reamer (Mani Inc., Tochigi-Ken, Japan), retainingat least 5 mm of root filling at the apical level (8). The canal walls were enlarged by usingFRC Postec Plus low-speed post drill (#1; Ivoclar-Vivadent, Schaan, Liechtenstein), andthe smear layer was removed by using ultrasonic agitation (ART P1; Bonart Co, Taiwan),with a #15 hand-file and 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) followedby 5 mL of 5.25% NaOCl as an irrigant. Final irrigation was accomplished with 10 mL ofdistilled water. The root canals were dried by using paper points.
Before cementation, posts (FRC Postec Plus) were cleaned with 95% ethanol, anda single layer of silane coupling agent (Monobond-S; Ivoclar-Vivadent) was applied to
Effects of Curing and Luting Agents on Push-out Bond Strength 1521

TABLE1.
Effe
ctof
Lutin
gSy
stem
s,Cu
ring
Tech
niqu
e,an
dR
oot
Reg
ion
onPo
stR
eten
tion
Lig
ht
sou
rce
Fail
ure
mo
de
(%)
Luti
ng
syst
emR
oo
tre
gio
nQ
THLE
DP
AC
QTH
(PA
/LA
/C/M
)LE
D(P
A/L
A/C
/M)
PA
C(P
A/L
A/C
/M)
Maxc
em
)C
oro
nal
16.1
2�
1.9
0a
15.2
7�
1.9
6a
16.0
3�
1.8
5a
40/1
3.3
/26.7
/20
33.3
/13.3
/20/3
3.3
33.3
/20/2
6.7
/20
Ap
ical
8.3
5�
1.8
2c
7.2
9�
1.9
9c,
d7.0
5�
1.1
4c,
d33.3
/26.7
/6.7
/33.3
33.3
/33.3
/6.7
/26.7
40/2
6.7
/6.7
/26.7
Pan
avi
aF
2.0
†C
oro
nal
11.4
8�
1.9
9b
12.2
8�
2.4
5b
11.5
5�
2.3
4b
40/1
3.3
/20/2
6.7
33.3
/13.3
/26.7
/26.7
33.3
/13.3
/26.7
/26.7
Ap
ical
6.6
6�
2.0
4c,
d4.4
1�
2.1
8c,
d6.5
7�
1.6
9c,
d33.3
/26.7
/6.7
/33.3
26.7
/33.3
/6.7
/33.3
33.3
/26.7
/6.7
/33.3
Valu
esar
em
ean�
stan
dard
devi
atio
nin
MPa
.Sy
mbo
lsre
pres
ent
diffe
renc
esam
ong
lutin
gsy
stem
s(P
<.0
5).
Low
erca
sele
tters
repr
esen
tsi
gnifi
cant
diffe
renc
esam
ong
root
regi
ons
(P<
.05)
.N
osi
gnifi
cant
diffe
renc
esw
ere
foun
dam
ong
failu
rem
odes
.
C,co
hesi
vew
ithin
post
syst
em;
LA,
adhe
sive
betw
een
lutin
gm
ater
ial
and
dent
in;
LED
,lig
ht-e
mitt
ing
diod
e;M
,m
ixed
adhe
sive
/coh
esiv
e(c
ombi
natio
nof
any
2of
PA/L
A/C)
;PA
,ad
hesi
vebe
twee
npo
stan
dre
sin
cem
ent;
PAC,
plas
ma
arc;
QTH
,qu
artz
tung
sten
halo
gen.
Basic Research—Technology
the post surface. Roots were randomly divided into 2 experimentalgroups according to luting material, and each group was further dividedinto 3 subgroups (n = 5) according to the curing unit used, as follows:(1) Panavia F 2.0 (Kuraray Dental, Tokyo, Japan) + QTH (Blue Swan;Dentanet, Istanbul, Turkey); (2) Panavia F 2.0 + LED (Blue Swan; Den-tanet); (3) Panavia F 2.0 + PAC (Remecure; Remedent, Deurle,Belgium); (4) Maxcem (KerrHawe, Bioggio, Switzerland) + QTH;(5) Maxcem + LED; (6) Maxcem + PAC.The luting systems were applied according to the manufacturers’instructions. The specimens were polymerized with the tip of the lightunit in direct contact with the coronal end of the post. Exposure timeswere 90 seconds with the QTH and LED units and 12 seconds with thePAC unit. After polymerization, specimens were stored for 24 hours at37C� in light-proof boxes.
Push-out TestPosts/cemented roots were sectioned perpendicularly to their long
axes into series of 1-mm slices by using a low-speed diamond saw(Micracut; Metkon, Bursa, Turkey) under a water coolant. Six sliceswere obtained from each root, 3 representing the coronal region and3 representing the apical region of the post space.
Push-out bond strengths were carried out by securing each slice tothe metal support of a universal testing machine (Model 500; Testomet-ric, Rochdale, Lancashire, UK), with the apical aspect facing a cylindricalplunger of 0.65-mm diameter. Loading was performed at a crossheadspeed of 0.5 mm/min until bond failure occurred. Push-out strength(MPa) was calculated by dividing the load at debonding (N) by thearea (mm2) (9, 10). In total, push-out tests were conducted on 30 sli-ces for each experimental subgroup (15 coronal, 15 apical).
After bond-strength testing, failure type was determined byanalyzing each sample under a stereomicroscope (Olympus SZ 6045TR Zoomstereomicroscope; Olympus Optical Co, Tokyo, Japan) at40� magnification. Type of failure was classified into 4 categories asfollows: (1) adhesive failure between post and luting material; (2)adhesive failure between dentin and luting material; (3) cohesive failureof the post system; (4) mixed failure (a combination of 2 of the above).
Statistical AnalysisStatistical analysis was performed by using SPSS, Version 11.0
(SPSS, Chicago, IL), with a significance level set at P <.05. Three-wayanalysis of variance and Tukey post hoc tests were used to analyzepush-out bond strength, and c2 test was used to analyze failure modes.
Scanning Electron Microscope AnalysisA scanning electron microscope (SEM) (JSM-5600; JEOL Ltd, To-
kyo, Japan) evaluation of the post space was also performed after smearlayer removal and the primer application of Panavia. Each root was cutin a mesiodistal direction with a low-speed diamond saw for these eval-uations. Also, 2 specimens tested in push-out mode were processed forobservation under the SEM, with the aim of assessing the site of bondfailure from each subgroup. The root sections were split along the buc-colingual axis with a hammer and chisel. Exposed root canals weregold-sputtered (Polaron Range SC7620; Quorum Technology, New-haven, UK), and SEM photomicrographs at�100 and�1500 originalmagnification were taken of the canal walls at 1-mm and 8-mm levels.
ResultsTable 1 shows the push-out bond strengths and distribution of fail-
ures for each of the experimental groups. Push-out bond strength wasfound to vary significantly according to type of luting system and rootregion (P < .05); however, curing unit used had no effect on push-
1522 Zorba et al. JOE — Volume 36, Number 9, September 2010

Figure 1. Morphologic aspects of intraradicular coronal dentin at different magnifications (A, with smear layer; B, without smear layer; C, after primer of Panavia F2.0 was applied; D, after push-out test in specimens luted with Panavia F 2.0; E, after push-out test in specimens luted with Maxcem; F, mixed-type failure).
Basic Research—Technology
out bond strength of the tested post at either the coronal or apical level(P > .05). The bond strength of the self-adhesive (Maxcem) was higherthan that of the self-etch resin cement (Panavia F) (P < .05). Apicalpush-out bond strength was significantly lower than coronal push-outbond strength for all groups (P < .05). The c2 test revealed no signif-icant difference in failure modes among the groups tested (P > .05).
SEM analysis revealed more open dentin tubules in the coronalregion than in the apical region. Short resin tags were observed inthe open tubules with both cements tested. However, Maxcem showedmore resin tags than Panavia F in both coronal and apical regions afterpush-out test. Figs. 1 and 2 show the morphologic changes happened inintraradicular dentin of coronal and apical root sections, respectively,before and after the smear layer removal, Panavia F’s primer, and afterthe testing.
DiscussionThe FRC Postec post used in the present study has elasticity similar to
dentin and is translucent, radiopaque, and designed to be tapered forbetter preservation of tooth structure (11, 12). In the present studya Peeso reamer was used to remove the coronal part of root filling andthe reamer of this post system (FRC Postec Plus reamer) was used toprepare the canal dentin according to the manufacturer’s suggestionsto achieve optimal matching between the post and root canal walls.
JOE — Volume 36, Number 9, September 2010
In the endodontic literature, there is no consensus on the timeinterval between the endodontic treatment and the post space prep-aration. Posts can be inserted immediately after completion of theroot canal filling or at a later time after full setting of the sealer.Some previous studies reported that immediate post space prepara-tion was less time-consuming procedure and preferable as a result ofits demonstrated less apical leakage (13). Therefore, post spaceswere immediately prepared after the root fillings in this study, aswe routinely apply this method in our clinics, although there isrecently mentioned detrimental effect of unset epoxy resin sealerto fiber post retention (14).
The thin slice (1-mm) push-out strength test is considered to bea valid method for evaluating fiber post adhesion to root canal walls(15). It has been reported to be more reliable than the microtensilemethod for measuring the adhesion of fiber posts (16). This methodis easy and allows fabrication of several specimens from 1 root aswell as testing regional differences between root sections (15).
In push-out tests, to ensure that the shear force is concentrated onthe adhesive interface is important. If this force is not completelycentralized, friction with part of the dentin wall can be increased, modi-fying the result (17). The risk of friction is higher when discs of greaterthickness and with cylindrical versus conical posts were evaluated (18,19). The tapered post used in the present study has a constant anglealong its length, and friction is minimized by directing the axial force
Effects of Curing and Luting Agents on Push-out Bond Strength 1523

Figure 2. Morphologic aspects of intraradicular apical dentin at different magnifications (A, with smear layer; B, without smear layer; C, after primer of Panavia F2.0 was applied; D, after push-out test in specimens luted with Panavia F 2.0; E, after push-out test in specimens luted with Maxcem; F, mixed-type failure).
Basic Research—Technology
from the smallest to the largest diameter, concentrating the push-outforce at the adhesive interface.
Hypothesis studied in the present study was partially accepted aspush-out bond strength of tested fiber post and was found to vary ac-cording to the type of adhesive system used and region of the root,but it was not affected when different curing units were used.
When both self-etch and self-adhesive luting systems were tested tolute fiber posts to root dentin, better bond strength values were obtainedwith self-adhesive resin cement. This result is in accordance with thefindings of Radovic et al (20) and Bitter et al (21). This could be attrib-utable to the removal of the smear layer before the cementation of thepost to dentin with alternative irrigation of 17% EDTA and 5.25% NaOCl.Self-adhesive cements contain multifunctional phosphoric acid methac-rylates that are claimed to react with the hydroxyapatite of the hardtissue. To ensure a correct infiltration pattern, these cements shouldbe able to etch the substrate in short time and require optimal wettingproperties to achieve a fast interaction with dentin (22). It has been re-ported that when smear layer is present, despite their initial acidic pH,self-adhesive cements did not produce any evidence of dentin deminer-alization and/or hybridization (23, 24). Therefore, the presence of thesmear layer has been recognized as the ‘‘weak’’ link in bonding of self-adhesive cements. Phosphoric acid etching before self-adhesive cementapplication has been shown to be detrimental to effective dentin
1524 Zorba et al.
bonding (25), and usage of a milder acidic agent has been proposed(24). Most likely, use of EDTA (26) together with NaOCl effectivelyremoved the superficial loosely bound fraction of the smear layerand enhanced the adhesion of self-adhesive cement in the present study(Fig. 1). Distilled water irrigation before post cementation probablyeliminated the negative effect of NaOCl on the adhesive bonding todentin (27).
Both adhesive cements tested demonstrated measurable adhesionto root dentin, with the highest values for the coronal region and lowestfor the apical region in accordance with the previous reports (28, 29).The explanation for this result could be attributed to different factorssuch as regional differences in the quantity, volume, and orientationof the tubules toward the apical portion of the root canal, apicalsclerosis, the high cavity configuration factor (28), the difficulty in visu-alization and access to the apical part, restrictions in the flow and distri-bution of the material in this region that make more bubbles and voidswithin the cement (30), and thick smear layer formation during the postspace preparation (Figs. 1A and 2A) that could not be modified by theadhesive cement or removed by EDTA/NaOCl irrigation (Figs. 1B and2B) for optimum bonding.
The mechanical properties of dual-cure adhesives were also foundto be affected by different curing strategies (31) because these cementshave been shown to reach inadequate degree of conversion in the
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
absence of light. However, within the post space, high attenuation oflight passing through the canal might jeopardize bonding quality, espe-cially in the apical region. To circumvent this problem, previous studieshave recommended using high-intensity light-curing units to increasethe curing efficiency of adhesive resins especially in deep cavities(32). Therefore, 3 different curing units, QTH, LED, and PAC, wereused to start the polymerization of dual-cure resin cements in thepresent study. However, no significant difference was found in bondstrength values, although high-intensity light-curing units were alsoevaluated. This result could be explained by reduced effectiveness ofthese light sources as a result of light scattering within the resin cement,shadowing produced by both the tooth structure and the post, andlimited light transmission capability of translucent FRC Postec Pluspost used in the present study (33–36).Evaluation of the failure modes in the present study demonstratedno cohesive failure inside the root canal dentin, which indicates thatbond strengths to root canal dentin were weaker compared with theshear bond strength of the dentin itself (21). Both Maxcem and PanaviaF cements demonstrated more adhesive failures between post/resincement and between cement/dentin when specimens from apical regionwere evaluated and compared with the coronal region. Cohesive andmixed-type failure modes were detected more in specimens obtainedfrom coronal root region with both cements. Therefore, the bondstrength between post/cement and cement/dentin could be consideredas the limiting factor of the measured bond strength values.
ConclusionWithin the limits of this in vitro study, self-adhesive cement, Max-
cem, demonstrated better bonding to dentin than self-etch cement,Panavia F, when smear layer was removed before post cementationwith EDTA/NaOCl. The use of different curing units for the photoirradia-tion of dual-cured resin cement had no effect on the retention of FRCPostec post because of the limited light transmission capability of thispost. Push-out bond strength was significantly lower in the apical thirdthan in the coronal region, regardless of the type of cement or curingtechnique used.
AcknowledgmentsThis study was supported by a grant-in-aid (2007-17) from
the Kırıkkale University Scientific Project Research Foundation,Turkey. This study was also partially supported by a grant givenby Selcuk University, Scientific Research Project CoordinationCenter and conducted in the Research Laboratories of Faculty ofDentistry.
References1. Zhang L, Huang L, Xiong Y, Fang M, Chen JH, Ferrari M. Effect of post-space treat-
ment on retention of fiber posts in different root regions using two self-etchingsystems. Eur J Oral Sci 2008;116:280–6.
2. Rosenstiel SF, Land MF, Crispin BJ. Dental luting agents: a review of the current liter-ature. J Prosthet Dent 1998;80:280–301.
3. Roberts HW, Leonard DL, Vandewalle KS, Cohen ME, Charlton DG. The effect ofa translucent post on resin composite depth of cure. Dent Mater 2004;20:617–22.
4. Kumbuloglu O, Lassila LV, User A, Vallittu PK. A study of the physical and chemicalproperties of four resin composite luting cements. Int J Prosthodont 2004;17:357–63.
5. Radovic I, Corciolani G, Magni E, et al. Light transmission through fiber post: theeffect on adhesion, elastic modulus and hardness of dual-cure resin cement.Dent Mater 2009;25:837–44.
6. Goracci C, Grandini S, Bossu M, Bertelli E, Ferrari M. Laboratory assessment of theretentive potential of adhesive posts: a review. J Dent 2007;35:827–35.
7. Zorba YO, Bayındır YZ, Turgut H, Yildiz M. Quality of curing in relation to differentlight sources by measuring hardness, degree of conversion and depth of cure. MatRes Innov 2009;13:464–7.
JOE — Volume 36, Number 9, September 2010
8. Abramovitz I, Tagger M, Tamse A, Metzger Z. The effect of immediate vs. delayedpost space preparation on the apical seal of a root canal filling: a study in anincreased-sensitivity pressure-driven system. J Endod 2000;26:435–9.
9. Hashem AA, Ghoneim AG, Lutfy RA, Fouda MY. The effect of different irrigatingsolutions on bond strength of two root canal-filling systems. J Endod 2009;35:537–40.
10. Babb BR, Loushine RJ, Bryan TE, et al. Bonding of self-adhesive (self-etching) rootcanal sealers to radicular dentin. J Endod 2009;35:578–82.
11. Demiryurek EO, Kulunk S, Yuksel G, Sarac D, Bulucu B. Effects of three sealers onbond strength of a fiber post. J Endod 2010;36:497–501.
12. Baldissara P, Zicari F, Valandro LF, et al. Effect of root canal treatments on quartzfiber posts bonding to root dentin. J Endod 2006;32:985–8.
13. Solano F, Hartwell G, Appelstein C. Comparison of apical leakage between imme-diate versus delayed post space preparation using AH Plus sealer. J Endod 2005;31:752–4.
14. Vano M, Cury AH, Goracci C, et al. Retention of fiber posts cemented at different timeintervals in canals obturated using an epoxy resin sealer. J Dent 2008;36:801–7.
15. Goracci C, Grandini S, Bossu M, Bertelli E, Ferrari M. Laboratory assessment of theretentive potential of adhesive posts: a review. J Dent 2007;35:827–35.
16. Goracci C, Tavares AU, Fabianelli A, et al. The adhesion between microtensile andpush out bond strength measurements. Eur J Oral Sci 2004;112:353–61.
17. de Durao Mauricio PJ, Gonzalez-Lopez S, Aguilar-Mendoza JA, Felix S, Gonzalez-Rodrıguez MP. Comparison of regional bond strength in root thirds among fiber-reinforced posts luted with different cements. J Biomed Mater Res B Appl Biomater.2007;83:364–72.
18. Patierno JM, Rueggeberg FA, Anderson RW, Weller RN, Pashley D. Push-out strengthand SEM evaluation of resin composite bonded internal cervical dentin. Endod DentTraumatol 1996;12:227–36.
19. Wakefield C, Draughn R, Sneed W, Davis T. Shear bond strengths of six bondingsystems using the push-out method of in vitro testing. Oper Dent 1998;23:69–76.
20. Radovic I, Mazzitelli C, Chieffi N, Ferrari M. Evaluation of the adhesion of fiber postscemented using different adhesive approaches. Eur J Oral Sci 2008;116:557–63.
21. Bitter K, Meyer-Lueckel H, Priehn K, Kanjuparambil JP, Neumann K, Kielbassa AM.Effects of luting agent and thermocycling on bond strengths to root canal dentine. IntEndod J 2006;39:809–18.
22. Moszner N, Salz U, Zimmermann J. Chemical aspects of self-etching enamel-dentinadhesives: a systematic review. Dent Mater 2005;21:895–910.
23. Yang B, Ludwig K, Adelung R, Kern M. Micro-tensile bond strength of three lutingresins to human regional dentin. Dent Mater 2006;22:45–56.
24. Monticelli F, Osorio R, Mazzitelli C, Ferrari M, Toledano M. Limited decalcification/diffusion of self-adhesive cements into dentin. J Dent Res 2008;87:974–9.
25. De Munck J, Vargas M, Van Landuyt K, Hikita K, Lambrechts P, Van Meerbeek B.Bonding of an auto-adhesive luting material to enamel and dentin. Dent Mater2004;20:963–71.
26. Gu XH, Mao CY, Kern M. Effect of different irrigation on smear layer removal afterpost space preparation. J Endod 2009;35:583–6.
27. Dimitrouli M, Gunay H, Geurtsen W, Luhrs AK. Push-out strength of fiber posts de-pending on the type of root canal filling and resin cement. Clin Oral Investig 2010[Epub ahead of print].
28. Onay EO, Korkmaz Y, Kiremitci A. Effect of adhesive system type and root region onthe push-out bond strength of glass-fibre posts to radicular dentin. Int End J 2010;43:259–68.
29. de Durao Mauricio PJ, Gonzalez-Lopez S, Aguilar-Mendoza JA, Felix S, Gonzalez-Rodrıguez MP. Comparison of regional bond strength in root thirds among fiber-reinforced posts luted with different cements. J Biomed Mater Res B Appl Biomater2007;83:364–72.
30. Bolhuis P, de Gee A, Feilzer A. The influence of fatigue loading on the quality of thecement layer and retention strength of carbon fiber post-resin composite core resto-rations. Oper Dent 2005;30:220–7.
31. Tanoue N, Koishi Y, Atsuta M, Matsumura H. Properties of dual-curable lutingcomposites polymerized with single and dual curing modes. J Oral Rehabil 2003;30:1015–21.
32. Santos GC, El-Mowafy O, Rubo JH, Santos MJ. Hardening of dual-cure resin cementsand a resin composite restorative cured with QTH and LED curing units. J Can DentAssoc 2004;70:323–8.
33. Musanje L, Darvell BW. Curing light attenuation in filled-resin restorative materials.Dent Mater 2006;22:804–17.
34. Faria e Silva AL, Arias VG, Soares LE, Martin AA, Martins LR. Influence of fiber posttranslucency on the degree of conversion of a dual-cured resin cement. J Endod2007;33:303–5.
35. Kim YK, Kim SK, Kim KH, Kwon TY. Degree of conversion of dual-cured resin cementlight-cured through three fibre posts within human root canals: an ex vivo study. IntEndod J 2009;42:667–74.
36. Goracci C, Corciolani G, Vichi A, Ferrari M. Light-transmitting ability of marketedfiber posts. J Dent Res 2008;87:1122–6.
Effects of Curing and Luting Agents on Push-out Bond Strength 1525

Basic Research—Technology
An In Vitro Evaluation of Performance of Two ElectronicRoot Canal Length Measurement Devices duringRetreatment of Different Obturating MaterialsVivek Aggarwal, MDS,*
‡Mamta Singla, MDS,
†and Debipada Kabi, MDS*
Abstract
Introduction: The purpose of this in vitro evaluationwas to study the accuracy of Root ZX and ProPex systemduring retreatment of canals obturated with different obtu-rating materials (gutta-percha + zinc oxide–eugenol sealer,gutta-percha + AH plus sealer, and Resilon + Epiphanysealer). Methods: Sixty human mandibular premolar rootswere instrumented with Rotary ProTaper until size F4under copious irrigation. After instrumentation, actualworking length was directly measured by using #15 Flex-oFile. Electronic working length was taken with the helpof Root ZX and ProPex. Teeth were divided into 3 groupsand obturated by using lateral condensation of gutta-percha + zinc oxide–eugenol sealer (group I), gutta-percha + AH plus sealer (group II), and Resilon + Epiphanysealer (group III). After 7 days, the obturating materialswere removed by using Gates-Glidden burs and K-files.A new electronic working length was taken. Original andpost-treatment electronic working lengths were comparedwith actual working length. Accuracy of both electronicroot canal length measurement devices was calculatedfor tolerance limits of �0.5 mm and �1.0 mm. Accuracywas compared by using c2 tests, and difference betweenactual working length and original and post-treatmentelectronic working lengths was compared by using Studentt test. Results: The accuracy of electronic root canallength measurement devices before root canal obturationwas 83.3% and 93.3% for Root ZX and ProPex, respec-tively, for a tolerance limit of �0.5 mm and 100% fora tolerance limit of �1.0 mm. There was no statisticallysignificant effect of different obturating materials testedin this study on the accuracy of Root ZX and ProPex fortolerance limits of �0.5 mm and �1.0 mm. Studentt test revealed insignificant differences between themean of actual working length and original and post-treatment electronic working lengths. Conclusions:Root ZX and ProPex can be a useful adjunct witha high accuracy rate during root canal preparation andretreatment. (J Endod 2010;36:1526–1530)From the *Department of Dental Surgery, Safdarjung Hospital, NeTechnology, Modinagar, India; and ‡Vivek Aggarwal is presently AsMilia Islamia, New Delhi, India.
Address requests for reprints to Dr Vivek Aggarwal, Departmentcom.0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.04.016
1526 Aggarwal et al.
Key WordsElectronic root canal length measurement devices, endodontic retreatment, endodonticworking length, root canal obturation
The endodontic literature has established the role of bacteria and their by-products ininitiation and progression of periapical pathosis (1–3). Once infected, root canal
space harbors a plethora of bacteria, which grow mostly in sessile biofilms,aggregates, co-aggregates, and planktonic cells (3–5). Reduction in bacterial countis accomplished by a triad of mechanical shaping, cleaning (with various irrigatingsolutions), and disinfection with intracanal medicaments (6, 7). The endodontictherapy does not always provide a desirable healing outcome. Presence of clinicalsigns and symptoms, along with radiographic evidence of periapical bonedestruction, indicates the need for retreatment (7–9).
The most common cause of retreatment is the incomplete debridement of the rootcanal space along with defective root canal space obturation (10–12). Therefore, theaim of retreatment is similar to the primary treatment, ie, thorough debridement of theroot canal space and to shape it, so as to receive an obturation that provides a seal in all3 dimensions (13, 14). For this purpose, orthograde nonsurgical retreatment isconsidered as the first line of treatment (13, 14). The extent of thechemomechanical debridement should be within the root canal and should extendup to minor apical constriction (15). Minor apical constriction is a histologic entityand is generally present 0.5–1.0 mm short of the radiographic apex (15, 16). It isvery important to accurately determine the length of the root canal to limit theinstrumentation and root canal obturation within the confines of canal space. Forthis purpose, electronic root canal length measurement devices are used as anadjunct to the well-established radiographic techniques (17).
The electronic root canal length measurement devices have gained popularityworldwide. They have been classified in the literature as generations of apex locators,but the generations do not provide the details of actual working mechanism of thesedevices (17). Root ZX (J Morita Corp, Tokyo, Japan) is one of the most commonlyused electronic root canal length measurement devices This device uses 2 differentalternating currents with different frequencies. It calculates the ratio of impedancesof 2 different frequencies. At the apical terminus, there is a sharp change in the imped-ance, and Root ZX recognizes it as the apex (17). Recently some multi-frequency elec-tronic root canal length measurement devices have been introduced to overcome someof the drawbacks of Root ZX. However, they work on a principle similar to impedancethat is based on electronic root canal length measurement devices (17). Various factorsaffect the impedance of the root canal walls including the smear layer and size of the
w Delhi, India; †Department of Conservative Dentistry & Endodontics, Institute of Dental Sciences &sistant Professor, Department of Conservative Dentistry & Endodontics, Faculty of Dentistry, Jamia
of Dental Surgery, Safdarjung Hospital, New Delhi, India. E-mail address: drvivekaggarwal@gmail.
JOE — Volume 36, Number 9, September 2010

Figure 1. (a) Plastic box; (b) file clip; (c) endodontic file; (d) sample tooth, (e) cold cure resin to stabilize sample; (f) saline-soaked sponge; (g) lip clip; (h)freshly mixed alginate; (i) radiographic film.
TABLE 1. Accuracy (%) of Electronic Root Canal Length Measurement Devicebefore Root Canal Obturation (tolerance limit, �0.5 mm and �1.0 mm)
Root ZX ProPex
TL, ±0.5 mm TL, ±1.0 mm TL, ±0.5 mm TL, ±1.0 mm
83.3% 100% 93.3% 100%
TL, tolerance limit.
Basic Research—Technology
dentinal tubules (18, 19). Recently it has been shown that root canalpreparation and residual root canal filling material also affect the rootcanal impedance (20). Newer obturating materials, which form a hybridlayer with dentin and provide a monoblock effect, can affect the rootimpedance as compared with conventional gutta-percha system (20).
Various studies have evaluated the accuracy of different electronicroot canal length measurement devices and effect of various factors(root canal pre-enlargement, different endodontic solutions, file size,stage of apex formation) (21, 22). Very limited studies have beenperformed to check the accuracy of different electronic root canallength measurement devices during retreatment with variousobturating materials (23). The purpose of this in vitro evaluation wasto study the accuracy of Root ZX and ProPex system during retreatmentof canals obturated with different obturating materials (gutta-percha +zinc oxide–eugenol sealer; gutta-percha + AH plus sealer, and Resilon+ Epiphany sealer).
Methods and MaterialsSixty freshly extracted, caries-free, human permanent mandibular
premolars with radiographically matured apex were collected. The teethwere radiographed buccolingually and mesiodistally to rule out anyaberrant canal morphology and to confirm a single canal. Teeth wereplaced in 5.25% NaOCl for 2 hours. Remaining soft tissue remnantswere removed with the help of a hand scaler. Teeth were stored innormal saline (0.9% NaCl) for a maximum period of 1 month. Teethhaving approximately same width were selected for the study as far aspossible. All the samples were decoronated at the level of cementoena-mel junction with help of diamond disks (Horico H557F220; Pfingst &Company, South Plainfield, NJ) in a straight air motor handpiece toobtain a flat reference point for future working length measurements.
After location of root canal system, the canal was gently irrigatedwith 5.25% NaOCl. A size 15 FlexoFile (Dentsply Maillefer, Tulsa, OK)was inserted into the canal until it was observed at the apical foramen
JOE — Volume 36, Number 9, September 2010
and its tip was tangential to the foramen. The apical tip and the file werevisualized with the help of EyeMag Loupes (EyeMag Smart system; CarlZeiss, Oberkochen, Germany) with a magnification of 2.5�. Thestopper was gently adjusted to correspond to the flat reference surface.The length between the stopper and the tip of the file was measured withthe help of a digital caliper and recorded to the nearest 0.01 mm. Theworking length was measured by subtracting 0.5 mm from this length.This was repeated 3 times, and the average value was recorded as theinitial working length of the root. Canals were instrumented with Pro-Taper rotary (Dentsply Maillefer) instruments in sequence with S1, fol-lowed by Sx, up to coronal two thirds. A sequential apicalinstrumentation was done with S2, F1, F2, F3, and finally F4 files untilworking length. The canals were irrigated between change of each file,alternatively delivering 10 mL of sodium hypochlorite (5.25%) and eth-ylenediaminetetraacetic acid (EDTA) solution (17%) with a 27-gaugeneedle. After root canal preparation, the canal length was again directlymeasured (by visualizing the apex and file), and this length wasrecorded as actual working length (AWL).
Measurement of Working Length with Electronic RootCanal Length Measurement Devices
Root ZX and ProPex (Dentsply Maillefer, Ballaigues, Switzerland)devices were used according to the manufacturer’s recommendations.
Performance of 2 Electronic Root Canal Length Measurement Devices 1527

TABLE 2. Accuracy (%) of Electronic Root Canal Length Measurement Device during Retreatment of Various Root Canal Obturation Materials (tolerance limit,�0.5 mm and �1.0 mm)
Root ZX ProPex
TL, ±0.5 mm TL, ±1.0 mm TL, ±0.5 mm TL, ±1.0 mm
Gutta-percha and zinc oxide–eugenol 70% 90% 90% 90%Gutta-percha and AH plus 80% 100% 90% 100%Resilon 70% 100% 70% 100%
TABLE 3. Mean Difference between AWL andPjAWL�EWL1
nj EWL1
Root ZX ProPex
0.31 mm 0.22 mm
Basic Research—Technology
Teeth were embedded in freshly mixed alginate and placed in a plasticcylinder. The walls of the cylinder were perforated before placement ofalginate. Small amount of cold cure resin was applied to firmly hold theroot in place in the cylinder. The cylinder was placed in plastic box filledwith saline-soaked sponge. A slot was prepared between the box andsponge to hold and standardize the x-ray film (Fig. 1). The canalswere irrigated with 5 mL of 5.25% NaOCl, and excess solution wasremoved with absorbent paper points. The labial clip was firmly securedto the plastic box, with part of it embedded in the saline-soaked sponge.The file clip was attached to #15 FlexoFile. For using Root ZX, the filewas inserted until the apex reading was reached. The file was withdrawnto flashing bar between 1 and apex on display. For using ProPex, the filewas advanced until foramen was reached, as indicated by red signal, andthen withdrawn to 0.0 signal. The reading was noted as electronicworking length 1 (REWL1 for Root ZX and PEWL1 for ProPex).
The samples were divided into 6 groups on the basis of type ofobturation and different electronic root canal length measurementdevices used during retreatment. Groups I and IV were obturated byusing gutta-percha and zinc oxide–eugenol, groups II and V were ob-turated by using gutta-percha and AH plus sealer, and groups III andVI were obturated by using Resilon and Epiphany sealer. The canalswere irrigated with 5 mL of NaOCl and dried with absorbent paperpoints. Groups I and IV were obturated by using lateral compactionof gutta-percha and zinc oxide–eugenol sealer. Groups II and V wereobturated by using lateral compaction of gutta-percha and AH plussealer. In groups III and VI, Epiphany self-etching primer was appliedin the canals with the help of a suitable micro brush, and excess wasremoved with the help of absorbent paper points. Epiphany sealerwas mixed according to manufacturer’s recommendations and placedin the canal with the help of Resilon master point. The selected masterpoint was coated with sealer and gently seated at the working length.Lateral compaction was performed by using digital spreader(NTD11T; Brasseler, Lemgo, Germany). Accessory medium-fine Re-silon points coated with sealer were laterally compacted into the canaluntil they could not be introduced more than 3 mm into the root canal.The excess material was seared off and compacted with a plugger(Premier Dental Products, Plymouth Meeting, PA) 1 mm below thecanal opening. The coronal surface was light-cured for 40 seconds. Apostoperative radiograph was obtained. The canal entrances in all thegroups were sealed with Cavit-G (3M ESPE, Seefeld, Germany). Thespecimens were stored at 100% humidity at 37�C for 7 days.
After 7 days, the temporary restoration was removed. Before initi-ating retreatment, a tentative working length was obtained with the helpof radiograph. The coronal and middle thirds of root canal obturationwere removed by using Gates-Glidden burs along with alternate irriga-tion with sodium hypochlorite (5.25%) and EDTA solution (17%). Thesamples were then again placed in plastic cylinder with freshly mixedalginate. After setting of alginate, the remaining apical third of theroot canal obturation was removed by using size 25, 30, and 35 K-filesuntil working length 1 mm short of radiographic length was achieved.The canals were again rinsed with NaOCl and dried with absorbentpaper points. A size 25 FlexoFile was taken, and root canal length
1528 Aggarwal et al.
was measured by using the electronic root canal length measurementdevices as described previously. Root ZX was used in groups I, II,and III, and ProPex was used in groups IV, V, and VI. If an apex readingwas not achieved, the file was advanced more apically. The reading wasnoted as EWL 2 (REWL2 for Root ZX and PEWL2 for ProPex). A newradiograph was obtained to determine the extent of root canal fillingpresent in the root.
The AWL was compared with original and post-treatment EWL.Differences were calculated (AWL – EWL1, AWL – EWL2), and tolerancelimits of�0.5 mm and�1.0 mm were taken. A negative difference indi-cated that EWL was larger and file tip had crossed the foramen. A posi-tive difference indicated that tip was short of foramen. The performanceof electronic root canal length measurement devices was evaluated interms of percentages of acceptable measurements (tolerance limit of�0.5 mm and �1.0 mm). The percentages were compared by usingc2 tests. Also the mean of difference between AWL and original andpost-treatment EWLs was calculated and compared by using Studentt test.
ResultsIn 2 samples, canals were blocked with obturating material
(1 each of zinc oxide–eugenol and Resilon & Epiphany). Two freshsamples were prepared and replaced the original blocked samples,keeping the final sample size of 60. The accuracy of electronic rootcanal length measurement devices before root canal obturation was83.3% and 93.3% for Root ZX and ProPex, respectively, when tolerancelimit of�0.5 mm was taken (Table 1). The electronic root canal lengthmeasurement devices gave 100% accurate readings for a tolerance limitof �1.0 mm. The accuracy of 2 electronic root canal length measure-ment devices after retreatment of various root canal obturating mate-rials is depicted in Table 2. There was no statistically significant effectof different obturating materials tested in this study on the accuracyof Root ZX and ProPex for tolerance limits of �0.5 mm and �1.0mm (c2 test, P > .05). Mean differences between AWL and originaland post-treatment EWLs were calculated (Tables 3 and 4). Therewas no statistically significant difference between all the groups.
DiscussionThe aim of the endodontic treatment/retreatment is to shape,
clean, and fill the root canal system until the minor apical foramenor the cementodentinal junction (15, 16, 24). Electronic root canallength measurement devices are a useful help to a clinician to locatethe root canal length. Recent electronic root canal lengthmeasurement devices provide certain advantages over the 2-dimensional x-rays: no radiation exposure, convenient to use, and
JOE — Volume 36, Number 9, September 2010

TABLE 4. Mean Difference between AWL and EWL2PjAWL�EWL2
nj during Retreatment of Various Root Canal Obturation Materials
Root ZX ProPex
Gutta-percha and zinc oxide–eugenol 0.42 mm 0.37 mmGutta-percha and AH plus 0.36 mm 0.29 mmResilon 0.43 mm 0.39 mm
Basic Research—Technology
a high accuracy rate (17). The electronic root canal length measure-ment devices work on the basis of impedance and capacitance of theroot canal system. As the apical constriction is reached, there is a drasticchange in the impedance and capacitance (17). The recent electronicroot canal length measurement devices recognize this change as a ratioor difference of impedance between the 2 or more sine wave frequen-cies (17). It has been shown that root canal contents can have an influ-ence on the accuracy of electronic root canal length measurementdevices (25, 26), although the recent electronic root canal lengthmeasurement devices give a predictable success rate even in thepresence of irrigating solution and/or pus (27, 28). Al-Bulushi et al(20) showed that root canal preparation and root canal obturationaffected the impedance of the root canal system, which might also affectthe reading of electronic root canal length measurement devices duringretreatment. The present study evaluated the influence of different rootcanal obturating materials on the accuracy of 2 electronic root canallength measurement devices.
It has been shown in the literature that the distance between theapical constriction and the apex ranges from 0.5–1.0 mm (15). There-fore in the present study, the AWL was recorded by subtracting 0.5 mmfrom the measurement obtained when file appeared at the foramen. Themethodology used during EWL determination was modified from Alveset al (23) and Kaufman et al (28). The inner cylinder was filled with
Figure 2. Radiograph showing extrusion of root canal obturating material.
JOE — Volume 36, Number 9, September 2010
freshly mixed alginate. Cold cure resin was used to stabilize the samples.The outer plastic box was filled with 0.9% NaCl–soaked sponge toobtain a conductive contact between the lip clip and the file clip–K-file. During EWL determination, the file was advanced to penetratethe apex and get a warning signal and then retract the file to get a consis-tent 0.5 (Root ZX) and 0.0 (ProPex) signal (28).
During retreatment, 2 samples were blocked by root canal obturat-ing materials. This might be due to the fact that no solvent was usedduring the retreatment. Kaufman et al (28) have stated that gutta-percha solvents like xylol can give shorter results with electronic rootcanal length measurement devices and thus lead to incomplete debride-ment. The working length was electronically obtained before and afterroot canal obturation (EWL1 and EWL2). The success of both electronicroot canal length measurement devices was obtained for tolerance limitsof �0.5 mm and�1.0 mm. The apical zone can have a wide range ofshapes, and the distance between the apical constriction and the apexranges from 0.5–1.0 mm (15, 16). Various authors have taken anerror range of �0.5 mm to assess the accuracy of the electronic rootcanal length measurement devices (29–31), whereas some haverelaxed the limit to �1.0 mm (32, 33). Root ZX and ProPex gave83.3% and 93.3% success rates, respectively, for a tolerance limit of�0.5 mm. These values were comparable with results conducted oncanals with/without root canal instrumentation (21–23, 25–28, 30).
Difference between AWL and EWL was obtained, and accuracy ofelectronic root canal length measurement devices was taken on toler-ance limits of �0.5 mm and �1.0 mm. Negative values indicatedthat EWL was larger than AWL, and the file had crossed the apicalconstriction. Post-treatment EWLs showed a trend toward longer valuesthan the AWL. In 2 of the samples, files exceeded the tolerance limit of1.0 mm beyond the apex (1 each of Root ZX and ProPex) during retreat-ment of gutta-percha and zinc oxide–eugenol sealer. Radiographicexamination revealed that the obturating material was pushed out ofthe apex, and the file had to penetrate into the obturating material totouch the conductive alginate and give an apex reading (Fig. 2). If thesereadings were eliminated, both the electronic root canal lengthmeasurement devices gave100% success rate for a tolerance limit of�1.0 mm during retreatment.
Root ZX calculates the ratio of impedance values at 2 frequencies(8 KHz and 0.4 KHz) (17). Root ZX has a built-in processor that relatesthe value of ratio with the position of file. The value of ratio is indepen-dent of the canal contents. ProPex is multi-frequency–based electronicroot canal length measurement device. It differs from Root ZX in termsof number of sine wave frequencies used. Also the calculation of theimpedance is based on the energy of the signal in contrast to amplitudeof the signal, which is used by Root ZX (30). Both of the electronic rootcanal length measurement devices work independently of the canalcontents (17, 30). The results of the present study showed that therewas no statistically significant influence of different obturatingmaterials on the accuracy of both electronic root canal lengthmeasurement devices. Also there was no difference between Root ZXand ProPex during retreatment.
The mean difference between the AWL and EWL before obturationwas�0.31 mm for Root ZX and�0.22 mm for ProPex. During retreat-ment, the mean difference between the AWL and post-treatment EWL
Performance of 2 Electronic Root Canal Length Measurement Devices 1529

Basic Research—Technology
remained less than�0.5 mm, irrespective of the obturating material orthe electronic root canal length measurement devices used. The resultsare comparable with those of Alves et al (23) and Goldberg et al (26).In the present study, it was found that the 2 tested electronic rootcanal length measurement devices (Root ZX and ProPex) gave accept-able readings in determination of root canal length in single-rootedteeth after root canal preparation and during retreatment. But it shouldnot be concluded that electronic root canal length measurement devicescould replace radiographs. Electronic root canal length measurementdevices should be used with caution during retreatment, because thereare chances of overinstrumentation if the obturating material isextruded beyond the apex. Nevertheless, the electronic root canal lengthmeasurement devices can be a useful adjunct with a high accuracy rateduring retreatment.
References1. Block RM, Bushell A, Rodrigues H, Langeland K. A histopathologic, histobacterio-
logic, and radiographic study of periapical endodontic surgical specimens. OralSurg Oral Med Oral Pathol 1976;42:656–78.
2. Abou-Rass M, Bogen G. Microorganisms in closed periapical lesions. Int Endod J1998;31:39–47.
3. Baumgartner JC, Falkler WA. Bacteria in the apical 5 mm of infected root canals.J Endod 1991;17:380–3.
4. Chugal NM, Clive JM, Spangberg LS. Endodontic infection: some biologic and treat-ment factors associated with outcome. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2003;96:81–90.
5. Seltzer S, Soltanoff W, Sinai I, Smith J. Biologic aspects of endodontics: part IV—periapical tissue reactions to root filled teeth whose canals had been instrumentedshort of their apices. Oral Surg Oral Med Oral Pathol 1969;28:724–38.
6. Paque F, Musch U, Hulsmann M. Comparison of root canal preparation using RaCeand ProTaper rotary Ni-Ti instruments. Int Endod J 2005;8:8–16.
7. Barbizam JVB, Fariniuk LF, Marchesan MA, Pecora JD, Sousa-Neto MD. Effectivenessof manual and rotary instrumentation techniques for cleaning flattened root canals.J Endod 2002;28:365–6.
8. Abou-Rass M. Evaluation and clinical management of previous endodontic therapy.J Pros Dent 1982;47:528–34.
9. De Cleen M, Schuurs A, Wesselin KP, Wu M. Periapical status and prevalence ofendodontic treatment in an adult Dutch population. Int Endod J 1993;26:112–9.
10. Friedman S, Stabholz A, Tamse A. Endodontic retreatment: case selection and tech-nique—part 3: retreatment techniques. J Endod 1990;16:543–9.
11. Saunders W, Saunders E, Sadiq J, Cruickshank E. Technical standard of root canaltreatment in an adult Scottish sub-population. Br Dent J 1997;10:382–6.
12. Weiger R, Hitzler S, Hermle G, Lost C. Periapical status, quality of root canal fillingsand estimated endodontic treatment need in an urban German population. EndodDent Traumatol 1997;13:69–74.
1530 Aggarwal et al.
13. Taintor J, Ingle J, Fahid A. Retreatment versus further treatment. Clin Prevent Dent1983;5:8–14.
14. Lovdahl P, Gutmann J. Problems in nonsurgical root canal retreatment. In:Gutmann J, Dumsha T, Lovdahl P, eds. Problem solving in endodontics. 3rd ed.St Louis, MO: Mosby; 1993:157–202.
15. Ricucci D. Apical limit of root canal instrumentation and obturation, part 1: litera-ture review. Int Endod J 1998;31:384–93.
16. Ricucci D, Langeland K. Apical limit of root canal instrumentation and obturation,part 2: a histological study. Int Endod J 1998;31:394–409.
17. Nekoofar MH, Ghandi MM, Hayes SJ, Dummer PMH. The fundamental operatingprinciples of electronic root canal length measurement devices. Int Endod J2006;39:595–609.
18. Meredith N, Gulabivala K. Electrical impedance measurements of root canal length.Endod Dent Traumatol 1997;13:126–31.
19. Levinkind M, Vandernoot TJ, Elliott JC. Electrochemical impedance characterisationof human and bovine enamel. J Dent Res 1990;69:1806–11.
20. Al-Bulushi A, Levinkind M, Flanagan M, Ng Y-L, Gulabivala K. Effect of canal prep-aration and residual root filling material on root impedance. Int Endod J 2008;41:892–904.
21. Ibarrola JL, Chapman BL, Howard JH, Knowles KI, Ludlow MO. Effect of preflaringon Root ZX apex locators. J Endod 1999;25:625–6.
22. Ounsi HF, Naaman A. In vitro evaluation of the reliability of the Root ZX electronicapex locator. Int Endod J 1999;32:120–3.
23. Alves AMH, Felippe MCS, Felippe WT, Rocha MJC. Ex vivo evaluation of the capacityof the Tri Auto ZX to locate the apical foramen during root canal retreatment. IntEndod J 2005;38:718–24.
24. Katz A, Tamse A, Kaufman AY. Tooth length determination: a review. Oral Surg OralMed Oral Pathol 1991;72:238–42.
25. Jenkins J, Walker W, Schindler W, Flores C. An in vitro evaluation of the accuracy ofthe root ZX in the presence of various irrigants. J Endod 2001;27:209–11.
26. Goldberg F, De Silvio A, Manfre S, Nastri N. In vitro measurement accuracy of anelectronic apex locator in teeth with simulated apical root resorption. J Endod2002;28:461–3.
27. Haffner C, Folwaczny M, Galler K, Hickel R. Accuracy of electronic apex locators incomparison to actual length: an in vivo study. J Dent 2005;33:619–25.
28. Kaufman AY, Jella S, Yoshpe M. Accuracy of a new apex locator: an in vitro study. IntEndod J 2002;35:186–92.
29. Pagavino G, Pace R, Baccetti TA. A SEM study of in vivo accuracy of the Root ZX elec-tronic apex locator. J Endod 1998;24:438–41.
30. Plotino G, Grande NM, Brigante L, Lesti B, Somma F. Ex vivo accuracy of three elec-tronic apex locators: Root ZX, Elements Diagnostic Unit and Apex Locator and Pro-Pex. Int Endod J 2006;39:408–14.
31. Saito T, Yamashita Y. Electronic determination of root canal length by newly devel-oped measuring device: influences of the diameter of apical foramen, the size of K-file and the root canal irrigants. Dentist Japan (Tokyo) 1990;27:65–72.
32. Fan W, Fan B, Gutmann JL, Bian Z, Fan MW. Evaluation of the accuracy of three elec-tronic apex locators using glass tubules. Int Endod J 2006;39:127–35.
33. Keller ME, Brown CE Jr, Newton CW. A clinical evaluation of the Endocater: an elec-tronic apex locator. J Endod 1991;17:271–4.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
Physicochemical Properties of Methacrylate Resin–basedRoot Canal SealersGabriela Alessandra Marin-Bauza, MS,* Fuad Jacob Abi Rached-Junior, MS,*
Aline Evangelista Souza-Gabriel, PhD,* Manoel Damiao Sousa-Neto, PhD,†
Carlos Eduardo Saraiva Miranda, PhD,* and Yara Teresinha Correa Silva-Sousa, PhD*
Abstract
Introduction: This study assessed in vitro the physico-chemical properties of 2 methacrylate resin-based sealers(Epiphany SE and Hybrid Root SEAL), comparing the resultswith a well-established epoxy resin-based sealer (AH Plus).Methods: Five samples of each material were used foreach test (setting time, flow, radiopacity, dimensionalchange after setting, and solubility) according to AmericanNational Standards Institute/American Dental Association(ANSI/ADA) Specification 57. The samples were assignedto 3 groups: I, AH Plus; II, Epiphany SE; and III, HybridRoot SEAL. The distilled and deionized water used at thesolubility test was submitted to atomic absorption spec-trometry to observe the presence of Ca2+, K+, Ni2+,and Zn2+ ions. In addition, the surface morphology ofthe specimens was analyzed by means of scanning elec-tron microscopy (SEM). Statistical analysis was performedby using one-way analysis of variance and Tukey-Kramertest (P < .05). Results: Flow, radiopacity, and solubility ofall sealers were in accordance with ANSI/ADA. The settingtime of Hybrid Root SEAL did not agree with ANSI/ADA require-ments. The dimensional change of all sealers was greater thanthe values considered acceptable by ANSI/ADA. The spectrom-etry analysis showed significant Ca2+ ions release for AH Plus.In SEM analysis, Hybrid Root SEAL presented spherical mono-mers with inferior size than AH Plus and Epiphany SE. Conclu-sions: It might be concluded that physicochemicalproperties of the tested sealers conformed to ANSI/ADA(2000) standardization, except for the setting time ofHybrid Root SEAL and the dimensional change of allsealers, which did not fulfill the ANSI/ADA requirements.(J Endod 2010;36:1531–1536)Key WordsEpoxy-resin and sealer, methacrylate, physicochemical
From the *School of Dentistry, University of Ribeirao Preto,Ribeirao Preto, Sao Paulo, Brazil; and †School of Dentistry,Department of Restorative Dentistry, University of Sao Paulo,Ribeirao Preto, Sao Paulo, Brazil.
Address requests for reprints to Prof. Yara T. Correa SilvaSousa, Rua Celia de Oliveira Meireles, 350 Bairro JardimCanada, Ribeirao Preto, Sao Paulo, CEP 14024-070, Brazil.E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.002
JOE — Volume 36, Number 9, September 2010
Root canal sealers should present good physicochemical properties and appropriatebiological performance (1). Research accomplished in the endodontic field aims to
obtain a sealer that meets all the ideal criteria to achieve the best prognosis of root canaltherapy (2, 3).
Synthetic resins have been discussed and tested as endodontic core filling mate-rials for many decades. Because of the success of the resin-based sealers, the AH serieswas developed more than 50 years ago (4). AH Plus (Dentsply De Trey Gmbh, Konstanz,Germany), a 2-component paste/paste sealer, is the result of this product developmentand is frequently used in this kind of research because of its well-studied and good phys-icochemical properties (5–8).
A new filling material commercially named as Real Seal (SybronEndo, Orange, CA)or Epiphany (Pentron Clinical Technologies, Wallingford, CT) has been introduced toreplace conventional sealers, with the promise of improving clinical performance (1,9). Epiphany is a dual-cure methacrylate resin-based cement (9, 10). The resinmatrix consists of a mixture of urethane dimethacrylate (UDMA), polyethylene glycoldimethacrylate (PEGDMA), ethoxylated bisphenol A dimethacrylate (EBPADMA),bisphenol A glycidyl dimethacrylate (BisGMA), silane-treated glass barium sulfate,silica, calcium hydroxide, bismuth oxychloride, peroxide, photo initiator, stabilizers,and pigments (7). This system uses a self-etching primer and also comprises Resilon(Resilon Research LLC, Madison, CT), which is a radiopaque thermoplastic syntheticmaterial that contains bioactive glass, bismuth oxychloride, and barium sulfate (11,12). In essence, a monoblock effect is produced, in which the core material(Resilon), sealer (Epiphany), and dentinal tubules become a single solid structure(13, 14).
The second generation of methacrylate sealer replaced the original by the intro-duction of the Epiphany SE Self-Etch Sealer (Pentron Clinical Technologies), a self-etchdual-cure, hydrophilic resin sealer that bonds to both Resilon and dentin, withouta separate priming step (15). According to the manufacturer, the 2 main bases ofthe Epiphany resinous matrix (EBPADMA and BisGMA) were kept the same in thisnew system. Acidic methacrylate resins and 2-hydroxyethyl methacrylate (HEMA)were added to Epiphany SE and were responsible for the self-etching characteristicsof the sealer (16).
Hybrid Root SEAL sealer (Sun Medical, Tokyo, Japan), also commercialized asMetaSEAL (Parkell Inc, Farmington, NY), has been recently introduced as anotheroption for root canal obturation. This methacrylate resin-based sealer also has adhe-sion to the radicular dentin and to solid filling materials (17, 18). This sealer isa self-etch hydrophilic material as a result of the inclusion of the acidic monomer 4-methacryloxyethyl trimellitate anhydride (4-META), which is capable of diffusingthrough the demineralized surface to form the hybrid layer after polymerization (19,20). However, because of the presence of this acid radical in its composition, thecytotoxicity of Hybrid Root SEAL is high in the first week after placement, decreasingover time (21).
The combination of resin-based sealers and adhesive systems has been demon-strated to improve performance regarding the sealing capacity (22), increase thebond strength to dentin (13, 14), and form hybrid layer (23). Therefore, a numberof tests have been developed to assess the physical properties of the endodontic filling
Physicochemical Properties of Methacrylate Resin–based Root Canal Sealers 1531

Basic Research—Technology
materials to ensure workability when used in clinical situations (5). Todate, literature is limited to provide information regarding physicalproperties of Epiphany SE and Hybrid Root SEAL.The purpose of this in vitro study was to assess the setting time,flow, radiopacity, dimensional change after setting, and solubility ofthe 2 methacrylate resin-based sealers (Epiphany SE Self-Etch Sealerand Hybrid Root SEAL) and 1 epoxy-amine resin sealer (AH Plus), ac-cording to American National Standards Institute/American DentalAssociation (ANSI/ADA) (2000) standards. In addition, the externaland internal surface morphology of all sealers was analyzed by usingscanning electron microscopy (SEM).
Materials and MethodsSetting time, flow, radiopacity, solubility, and dimensional change
after setting for AH Plus (group I), Epiphany SE (group II), and HybridRoot SEAL (group III) sealers were measured according to ANSI/ADAstandards for dental root canal sealing materials (24) by one evaluatorblinded to the identification of the materials.
All tested materials were manipulated in accordance to the man-ufacturer’s instructions. AH Plus and Epiphany SE are displayed as 2pastes, and for each tested sample, 15 mm of the sealer was dispensedonto a mixing pad and spatulated for 20 seconds to obtain a homoge-neous mixture. Hybrid Root SEAL is a power/liquid sealer and wasspatulated for 20 seconds onto a mixing pad in the proportion of 1:3.
Because the sealers in groups II and III were dual-curable resins,they were mixed and handled in a darkroom under low wattage red safe-light bulb (15 W). In addition, the specimens in groups II and III werelight-cured (Ultralux; Dabi Atlante, Ribeirao Preto, SP, Brazil) for 40seconds and 20 seconds, respectively.
For physicochemical tests, the arithmetic mean of 5 replicates foreach sealer was recorded and considered as the result of the test.
Setting TimeFive plasters of cast rings with an internal diameter of 10 mm and
a thickness of 2 mm were prepared for each group. The externalborders of the molds were fixed with wax on a glass plate (75 � 25� 1 mm). The molds were filled with the material and transferred toa chamber with 95% relative humidity and a temperature of 37 �C. Inaddition, the specimens in groups II and III were light-cured for 40and 20 seconds, respectively (Ultralux; Dabi Atlante). After 150 � 10seconds from the onset of mixing, a Gilmore-type needle with a massof 100� 0.5 g and a flat end of 2.0� 0.1 mm in diameter was carefullylowered vertically onto the horizontal surface of the testing sample. Theneedle tip was cleaned, and the probing was repeated until indentationsceased to be visible. The time used from the start of mixing to this pointwas recorded. If the results differed by more than �5%, the test wasrepeated.
Flow TestThe amount of 0.5 mL of each sealer tested was placed on a glass
plate (10� 10� 3 mm) by using a graduated disposable 3-mL syringe.At 180� 5 seconds after the onset of mixing, another plate with a massof 20 � 2 g and a load of 100 g were carefully applied on top of thematerial. Ten minutes after mixing the cement, the load was removed,and the major and minor diameters of the compressed discs weremeasured by using a digital calliper with a resolution of 0.01 mm (Mi-tutoyo MTI Corporation, Tokyo, Japan). If both measurements wereconsistent to within 1 mm, the results were recorded. If the majorand minor diameter discs were not uniformly circular or did not matchwithin 1 mm, the test was repeated.
1532 Marin-Bauza et al.
Radiopacity TestFive acrylic plates (2.2 cm� 4.5 cm� 1 mm), containing 4 wells
measuring 1 mm in depth and 5 mm in diameter, were prepared andplaced over a glass plate covered by cellophane sheet. In group I, thefreshly mixed sealer was introduced into the wells by using a syringeto avoid the formation of bubbles. In groups II and III, the respectivematerial applicators were used to fill the wells. Another glass platecovered with cellophane was placed on top until complete setting(chemically or light-cured), and any excess sealer was removed.Each plate was kept in an incubator (37 �C, 95% relative humidity)for a period corresponding to 3 times the setting time. Each well wasfilled with one of the sealers, following a sequence according to thesetting time of the material from the longest to the shortest, so thatthe samples would be ready for radiographic evaluation after the finalsetting of all materials.
Each one of the acrylic plates containing the root filling materialswas positioned, at the time of the radiographic exposure, alongsideanother acrylic plate (1.3 cm � 4.5 cm � 1 mm) containing analuminum step wedge made of 1100 alloy, with the thickness varyingfrom 1–10 mm in uniform steps of 1 mm each (23). This set of acrylicplates was placed in front of this phosphor plate, and a digital radio-graph was taken (Digora system; Soredex Orion Corporation, Helsinki,Finland). Care was taken to place the samples next to the aluminum stepwedge and in the middle of the phosphor plate. Radiographic imageswere obtained by using the Spectro 70x x-ray machine (Dabi Atlante)at 70 kVp and 8 mA. The object-to-focus distance was 30 cm, andthe exposure time was 0.2 seconds. Exposed imaging plates of thetest samples were immediately scanned after exposure (DigoraScanner) and analyzed by using Digora for Windows 5.1 software.
Dimensional Change after SettingFive Teflon molds, prepared for the production of 3.58-mm-high
cylindrical test bodies measuring 3 mm in diameter, were placed ona glass plate wrapped with a fine cellophane sheet. The molds were filledwith a slight excess of freshly mixed sealers, and a microscope slide,also wrapped in cellophane, was pressed onto the upper surface ofthe mold. The assembled group was kept firmly joined with a C-shapedclamp and transferred to an incubator (37 �C, 95% relative humidity)left to stand for a period corresponding to 3 times the setting time. Afterthis period, the flat ends of the molds, containing the samples, weregrinded with 600-grit wet sandpaper. The samples were removedfrom the mold, measured with a digital caliper, stored in a 50-mL vesselcontaining 2.24 mL of distilled and deionized water, and kept in an incu-bator (37 �C, 95% relative humidity) for 30 days. The sample was thenremoved from the container, blotted dry on absorbent paper, andmeasured again for length. The percentage of the dimensional alter-ations was calculated by using the following formula:
L30 � L
L� 100
where L30 is the length of the sample after 30 days of storage, and L isthe initial length of the sample.
SolubilityA 1.5-mm-thick cylindrical Teflon (polytetrafluroethylene; Du-
Pont, HABIA, Knivsta, Sweden) mold measuring 7.75 mm in inner diam-eter was filled with freshly mixed sealers. The mold was supported bya larger glass plate and covered with a cellophane sheet. An imperme-able nylon thread was placed inside the material, and another glassplate, also covered with cellophane film, was positioned on the mold
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
and pressed manually in such a way that the plates touched the entiremold in a uniform manner. The assembly was placed in an incubator(37 �C, 95% relative humidity) and left to stand for a period corre-sponding to 3 times the setting time. As soon as the samples wereremoved from the mold, they were weighed 3 times each in an analyticalbalance (HM-200; A & D Engineering Inc, Bradford, MA), and the meanreading was recorded. The samples were suspended by nylon threadand placed 2-by-2 inside a plastic vessel with a wide opening containing7.5 mL of distilled and deionized water, taking care to avoid any contactbetween them and the inner surface of the container. The containerswere sealed and left for 7 days in an incubator (37 �C, 95% relativehumidity). After this period, the samples were removed from thecontainers, rinsed with distilled and deionized water, blotted dry withabsorbent paper, and placed in a dehumidifier for 24 hours. After-wards, they were weighed again. The weight loss of each sample, ex-pressed as percentage of the original mass (m% = mi – mf), wastaken as the solubility of the sealer.The liquid of the specimen’s immersion was analyzed by atomicabsorption spectrometry (Perkin Elmer Instruments GmbH, Uberlin-gen, Germany) to quantify the levels of Ca2+, K+, Ni2+, and Zn2+ ions.Merck solutions with 1000 mg/L concentration (Merck, Darmstadt,Germany) were used to prepare the standard solution of the differentmetals. Metal analytical curves were obtained from appropriate dilu-tions of each respective stock solution. The concentration intervals ofthe solutions were Ca2+, 0–20 mg/L; K+, 0.2–1 mg/L; Zn2+, 0–1.5mg/L; and Ni2+, 0.3–1.5 mg/L. During the chemical analyses of the solu-tions, the following wavelengths were used: Ca2+, 422.7 nm; K+, 766.5nm; Zn2+, 213.9 nm; and Ni2+, 234.0 nm. This spectrophotometer issupplied with hollow cathode lamps with different light spectra exclu-sively for measuring metallic ions. The obtained solutions were sprayedinto the atomic absorption spectrophotometer for ion quantification.The analyses were made in triplicate for each specimen; arithmeticmean was done and considered as the results of the concentration ofCa2+, K+, Zn2+, and Ni2+, expressed as mg/mL.
Statistical AnalysisFive specimens from each group were tested, and the means were
statistically compared. The Kolmogorov-Smirnov test showed that theresults were consistent with a normal distribution curve. The para-metric statistical analysis was performed (one-way analysis of variance[ANOVA] and post hoc Tukey-Kramer test), and the significance levelwas set as 5% (GraphPad InStat; GraphPad Software Inc, San Diego,CA).
SEM ExaminationFor SEM examination, cylindrical Teflon molds (3� 4 mm) were
filled with freshly mixed sealers. The molds were supported by a glassplate covered with a cellophane sheet and placed in a chamber (37 �C,95% relative humidity) for a period corresponding to 3 times the setting
TABLE 1. ANSI/ADA (2000) Standards, Mean Values, and Standard Deviations of E
Physicochemical properties AH Plus
Setting time (min) 579.00 � 4.95a
Flow (mm) 36.76 � 3.04b
Radiopacity (mm Al) 5.97 � 0.24a
Dimensional change (%) 1.69 � 0.31b
Solubility (%) 0.74 � 0.41a
The same superscripted letters indicate significant statistical difference (comparison between lines, P < .
JOE — Volume 36, Number 9, September 2010 Ph
time. After that, the samples were sectioned with a #15 disposablesurgical scalpel blade, fixed on a metallic stub (10 � 5 mm), andsputter-coated with gold-palladium (Bal-Tec AG, Balzers, Germany)at 20 mA. The internal surface morphology of the samples was qualita-tively assessed by a field emission SEM (JSM 5410; Jeol Technic Co, To-kyo, Japan) at an accelerating voltage of 15 kV at differentmagnifications.
ResultsPhysicochemical Properties
Table 1 shows the mean values and standard deviations of thephysicochemical properties (setting time, flow, radiopacity, dimen-sional change after setting, and solubility) of the tested sealers.
Setting TimeThe ANSI/ADA (2000) requires that the setting time of a sealer
shall be within 10% of that stated by the manufacturers. According tothem, the setting times of AH Plus, Epiphany SE, and Hybrid RootSEAL were 8–10 hours (480–600 minutes), 25 minutes, and 16 hours(960 minutes), respectively. In this study, AH Plus and Epiphany SEwere in agreement with the ANSI/ADA standards, and Hybrid RootSEAL did not conform to the standards. Statistical analysis demonstratedthat the setting time of AH Plus (579.00 � 4.95 minutes) was signifi-cantly longer than that of the other groups. Hybrid Root SEAL (63.40� 2.70 minutes) showed intermediate results, and Epiphany SE(24.40 � 4.39 minutes) exhibited the inferior setting time (one-wayANOVA, post hoc Tukey-Kramer test, P < .05). In summary, AH Plus> Hybrid Root SEAL > Epiphany SE.
Flow TestThe ANSI/ADA (2000) requires that a sealer shall have a diameter
of no less than 20 mm, and all groups of this study conformed to thestandards. Statistical analysis showed that the mean values of HybridRoot SEAL (45.94 � 0.61 mm) were significantly higher than thoseof AH Plus (36.76 � 3.04 mm) and Epiphany SE (34.43 � 2.17mm), which were statistically similar between themselves (one-way AN-OVA, post hoc Tukey-Kramer test, P < .05). In summary, Hybrid RootSEAL > AH Plus = Epiphany SE.
Radiopacity TestAll materials showed radiopacity above the 3 mm of aluminum rec-
ommended by ANSI/ADA Specification 57 (2000). Statistical analysisdemonstrated that AH Plus presented the superior results (5.97 �0.24 mm Al), statistically different from the other groups. EpiphanySE (5.51 � 0.12 mm Al) showed intermediate values, followed byHybrid Root SEAL (4.71� 0.04 mm Al), which showed the inferior ra-diopacity (one-way ANOVA, post hoc Tukey-Kramer test, P < .05). Insummary, AH Plus > Epiphany SE > Hybrid Root SEAL.
ach Experimental Group
Sealers
Epiphany SE Hybrid Root Seal
24.40 � 4.39b 63.40 � 2.70c
34.43 � 2.17b 45.94 � 0.61a
5.51 � 0.12b 4.71 � 0.04c
2.22 � 0.41b 3.45 � 0.34a
0.94 � 0.72a –1.25 � 1.10b
05).
ysicochemical Properties of Methacrylate Resin–based Root Canal Sealers 1533

TABLE 2. Levels of Metallic Ions, Expressed as mg/mL -1, Released in theImmersion Liquid of Samples
Groups
Metallicions AH Plus Epiphany SE
Hybrid RootSEAL
Ca2+ 43.22 � 11.39 7.80 � 3.43 <0.5K+ 0.58 � 0.36 0.32 � 0.26 0.74 � 0.10Ni2+ <0.6 <0.6 <0.6Zn2+ <0.2 0.92 � 0.88 <0.2
Basic Research—Technology
Dimensional Change after SettingANSI/ADA states that the maximum limit is 1% for linear shrinkage
and 0.1% for expansion. The dimensional change of all sealers wasgreater than values considered acceptable by ANSI/ADA. Statistical anal-ysis demonstrated higher dimensional change for Hybrid Root SEAL(3.45% � 0.34%). AH Plus (1.69% � 0.31%) and Epiphany SE(2.22% � 0.41%) presented the lower results and were statistically
Figure 1. Internal portion of sealers after complete setting time. (A, B) AH Plus wand compacted surface. (C, D) Epiphany SE with original magnification of�350 andstructure. (E, F) Hybrid Root SEAL with original magnification of �350 and �3500with AH Plus and Epiphany SE.
1534 Marin-Bauza et al.
similar between themselves (one-way ANOVA, post hoc Tukey-Kramertest, P < .05). In summary, Hybrid Root SEAL > AH Plus = Epiphany SE.
SolubilityA root canal sealer should not exceed 3% by mass when the solu-
bility of the set material is tested (ANSI/ADA 2000). Statistical analysisshowed higher solubility for AH Plus (0.75%� 0.41%) and EpiphanySE (0.94% � 0.72%), which were statistically similar among them-selves. The lower solubility was observed in Hybrid Root SEAL(–1.25% � 1.10%) group. The obtained results showed agreementwith the ANSI/ADA standardization.
Distilled and deionozed water used for the solubilty test wassubmitted to atomic absorption spectrometry analysis in order to checkthe amount of ions released from each sealer. Table 2 shows the ionsreleased to the immersion liquid in each experimental group.
It was verified that AH Plus sealer released significant level ofCa2+ (43.22 � 11.39 mg mL–1) when compared with the othergroups. For K+ ions, the release was higher in Hybrid Root SEAL,
ith original magnification of �350 and �3500, respectively. Note an irregular�3500, respectively. Note the plate-shape monomers compacted in the sealer
, respectively. Observe spherical monomers with inferior size when compared
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
followed by AH Plus and Epiphany SE. Regarding Ni2+, all groups pre-sented concentration inferior of 0.6 mg/L. For Zn2+, the largest valuewas observed for Epiphany SE, whereas AH Plus and Hybrid Root SEALpresented smaller concentrations than the smallest point of the analyt-ical curve.SEMFig. 1 illustrates the internal portion of sealers of each studied
group. Photomicrographs of AH Plus revealed an irregular and com-pacted surface (Fig. 1A, B). Epiphany SE exhibited plate-shape mono-mers distributed in the sealer structure (Fig. 1C, D). Photomicrographsof Hybrid Root SEAL presented spherical monomers with inferior sizewhen compared with the AH Plus and Epiphany SE sealers (Fig. 1E,F). At higher magnification (�3500), polymeric chains of AH Plusand Epiphany SE seemed better compacted and organized than HybridRoot SEAL (Fig. 1E).
DiscussionNew dental materials intending to obtain a better clinical perfor-
mance have been introduced on the market (25). On this concern,methacrylate resin-based root canal filling materials such as Epiphanyand Hybrid Root SEAL were developed. Before the clinical use of thesematerials, it is necessary to perform several standardized tests to checktheir physiochemical and biological properties (5).
In this study, the physiochemical tests were conducted on the basisof Specification 57 of ANSI/ADA (2000), following the modificationsproposed by Carvalho-Junior et al (26), which suggested a reductionof 80% in volume of the test samples dimensions, aiming to contributeto the rational use of endodontic materials without affecting the results.
The setting time is primarily a control test on the stable behavior ofa product and is dependent on the constituent components, theirparticle size, the ambient temperature, and relative humidity (3, 5).According to the ANSI/ADA standards, the setting time of a sealer canvary only 10% in relation to that established by the manufacturer. Inthe present study, only the setting time of the Hybrid Root SEAL didnot conform to ANSI/ADA specifications. AH Plus showed the highestmean values (579.00 minutes), followed by Hybrid Root SEAL (63.40minutes) and Epiphany SE (24.40 minutes). These results agree withthe literature reports that show a setting time between 494 and 817minutes for AH Plus and between 23.10 and 25.03 minutes forEpiphany (7, 15). There is no report regarding the setting time ofHybrid Root SEAL, and the manufacturer informs that this sealerpresents working time of 35 minutes and complete setting after 16hours.
AH Plus showed a setting time almost 9 times greater than HybridRoot SEAL and 24 times greater than Epiphany SE as a result of the slowpolymerization reaction of epoxy resin amines; hence the conversion ofmonomers into polymers occurs gradually (15, 27). Hybrid Root SEALand Epiphany SE are dual-curable resin composites containing a catalystcomponent that accelerates the process (28).
Another relevant aspect of the methodology is the fact that themethacrylate-based sealers were manipulated in a radiographic pro-cessing room to ensure that the sealer was not exposed to light duringthe experiment (10, 12, 15). The photo initiators present in EpiphanySE and Hybrid Root SEAL might start the polymerization process beforetheir insertion into the molds.
ANSI/ADA establishes as 20 mm the acceptable minimum value forthe diameter of the disc formed by the sealer. In this study, the highestflow was presented in Hybrid Root SEAL group (45.94 mm), followed byAH Plus (36.76 mm) and Epiphany SE (34.43 mm); thus, all sealerswere consistent with ANSI/ADA (2000). Previous investigations re-
JOE — Volume 36, Number 9, September 2010 Ph
ported flow values close to those obtained in this study for AH Plusand Epiphany sealers (7, 15). The highest flow obtained with HybridRoot SEAL can be attributed to the presence of 4-META that has onehydrophilic and other hydrophobic radical (19), probably responsiblefor the increase of the sealer viscosity. SEM analysis showed that HybridRoot SEAL is composed of small spherical particles that form a lesscompact and viscous structure than AH Plus and Epiphany SE, whichmight have contributed to the superior flow values achieved with HybridRoot SEAL.
A degree of radiopacity is indispensable for the control of rootfilling placement. Although the standards require only a lower limitto this property, it should be realized that extreme contrast in a materialmight lead to a false impression of a dense and homogenous fill (5).ANSI/ADA establishes that the radiopacity should be greater than orequal to 3 mm of aluminum. Although the radiopacity values of thesealers were statistically different among themselves, all groups werein agreement with ANSI/ADA specification.
The difference in the results can be attributed to the radiopacifyingagents of the studied sealers. AH Plus has calcium tungstate and zirco-nium oxide in its composition (18). Epiphany SE has bismuth oxychlor-ide and barium borosilicate (7, 12), and Hybrid Root SEAL has onlyzirconium oxide in its formula (18). Bismuth oxychloride has higherradiopacifying effect, followed by zirconium oxide, calcium tungstate,and barium borosilicate (29). However, the resulting radiopacitydepends on the chemical interaction among the radiopacifying agents(29). The results of this study can suggest that the zirconium oxide asso-ciated to the calcium tungstate in AH Plus produces superior radiopac-ity. Although Epiphany has bismuth oxychloride and bariumborosilicate in its composition, the synergic effect did not guaranteethe major radiopacity. Hybrid Root SEAL has only one radiopacifyingagent and, therefore, was the least opaque material.
Dimensional change demonstrates, in percentage, the shrinkageor expansion of the material after setting (5). ANSI/ADA states thatthe maximum limit is 1% for linear shrinkage and 0.1% for expansion.The dimensional change of all tested sealers was greater than the valuesconsidered acceptable by ANSI/ADA (AH Plus, 1.69%; Epiphany SE,2.22%; and Hybrid Root SEAL, 3.46%). Previous investigations that eval-uated the dimensional change of different sealers obtained values ragingfrom 0.62%–1.28% for AH Plus (7, 26) and 2.43%–8.07% forEpiphany (7, 15). The results of this physicochemical property canbe explained by water sorption after polymerization, a diffusion-controlled process that occurs mainly in the resin matrix, because ofits polar nature (30). It has been demonstrated that polymerized mate-rials from mixtures of hydrophilic monomers had high water sorption(31). In this study, the presence of hydrophilic radicals in methacrylate-based sealers resulted in higher water sorption and, consequently,higher expansion (32).
ANSI/ADA (2000) establishes that solubility of sealers should notexceed 3% by mass. Solubility results of all groups were within ANSI/ADA recommendations (AH Plus, 0.75%; Epiphany SE, 0.94%; andHybrid Root SEAL, –1.25%). Versiani et al (7) and Donnelly et al(33) found higher solubility values for Epiphany than those obtainedin this research (3.41% and 4.02%, respectively). Resende et al (15)reported only 0.34% of solubility for Epiphany SE. Other authors(15, 26, 33) reported solubility values raging from 0.06%–0.41% forAH Plus. The mass increase presented by Hybrid Root SEAL probablyoccurred as a result of the water absorption, because this sealerpresented the larger dimensional alteration. Atomic absorptionspectrometry analysis was conducted to determine the componentsreleased during the solubility test period. The analysis of theimmersion liquid revealed highest calcium concentrations in theliquid of AH Plus.
ysicochemical Properties of Methacrylate Resin–based Root Canal Sealers 1535

Basic Research—Technology
Overall, this laboratory study disclosed that the physicochemicalproperties of the 3 tested sealers (Epiphany SE, Hybrid Root SEAL,and AH Plus) conformed to ANSI/ADA (2000) standardization, exceptfor the setting time of Hybrid Root SEAL and the dimensional changeof all sealers, which did not fulfill the ANSI/ADA requirements. Neverthe-less, it is important to highlight that these new resin-based filling mate-rials have not had the same extensive evaluation that gutta-percha andconventional sealers have had. Further studies with these adhesivematerials after longer periods of storage and under biologic conditionsshould be conducted.
References1. De-Deus G, Di Giorgi K, Fidel S, Fidel RA, Paciornik S. Push-out bond strength of
Resilon/Epiphany and Resilon/Epiphany self-etch to root dentin. J Endod 2009;35:1048–50.
2. Grossman LI. Solubility of root canal cements. J Dent Res 1978;57:927.3. Gambarini G, Romeo U, Tucci E, et al. Cytotoxicity of Epiphany SE endodontic sealer:
a comparative in vitro study. Med Sci Monit 2009;15:PI15–8.4. Schroeder A. The impermeability of root canal filling material and first demonstrations
of new root filling materials. SSO Schweiz Monatsschr Zahnheilkd 1954;64:921–31.5. Ørstavik D. Materials used for root canal obturation: technical, biological and clin-
ical testing. Endodontic Topics 2005;12:25–38.6. Sousa-Neto MD, Coelho FI, Marchesan MA, Alfredo E, Silva-Sousa YTC. Ex vivo study
of the adhesion of an epoxy-based sealer to human dentine submitted to irradiationwith Er: YAG and Nd: YAG. Int Endod J 2005;38:866–70.
7. Versiani MA, Carvalho-Junior JR, Padilha MI, Lacey S, Pascon EA, Sousa-Neto MD. Acomparative study of physicochemical properties of AH Plus and Epiphany rootcanal sealants. Int Endod J 2006;39:464–71.
8. Bouillaguet S, Shaw L, Barthelemy J, Krejci I, Wataha JC. Long-term sealing ability ofPulp Canal Sealer, AH Plus, GuttaFlow and Epiphany. Int Endod J 2008;41:219–26.
9. Shipper G, Ørstavik D, Teixeira FB, Trope M. An evaluation of microbial leakage inroots filled with a thermoplastic synthetic polymer-based root canal filling material(Resilon). J Endod 2004;30:342–7.
10. Mathias-Junior O, Souza-Gabriel AE, Miranda CES, Pecora JD, Silva-Sousa YTC,Sousa-Neto MD. Solubility of Epiphany sealer prepared with resinous solvent.J Endod 2009;35:715–8.
11. Tanomaru-Filho M, Jorge EG, Guerreiro-Tanomaru JM, Goncalves M. Radiopacityevaluation of new root canal filling materials by digitalization of images. J Endod2007;33:249–51.
12. Onay EO, Ungor M, Ozdemir BH. In vivo evaluation of the biocompatibility of a newresin-based obturation system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2007;104:60–6.
13. Teixeira CS, Felippe WT. The effect of application time of EDTA and NaOCl on intra-canal smear layer removal: a SEM analysis. J Endod 2004;38:285–90.
1536 Marin-Bauza et al.
14. Rached-Junior FJA, Souza-Gabriel AE, Alfredo E, Miranda CES, Silva-Sousa YTC,Sousa-Neto MD. Bond strength of Epiphany sealer prepared with resinous solvent.J Endod 2009;35:251–5.
15. Resende LM, Rached-Junior FJA, Versiani MA, et al. A comparative study of physi-cochemical properties of AH Plus, Epiphany, and Epiphany SE root canal sealers.Int Endod J 2009;42:785–93.
16. Pentron. Epiphany� Soft Resin Endodontic Obturation System. Wallingford, CT:Pentron Clinical Technologies, LLC; 2007.
17. Lawson MS, Loushine B, Mai S, et al. Resistance of a 4-META–containing,methacrylate-based sealer to dislocation in root canals. J Endod 2008;34:833–7.
18. Belli S, Ozcan E, Derinbay O, Eldeniz AU. A comparative evaluation of sealing abilityof a new, self-etching, dual-curable sealer: Hybrid Root Seal (MetaSeal). Oral SurgOral Med Oral Pathol Oral Radiol Endod 2008;106:45–52.
19. Chang JC, Hurst TL, Hart DA, Estey AW. 4-META use in dentistry: a literature review.J Prosthet Dent 2002;87:216–24.
20. Van Landuyt K, Snauwaert J, De Munck JD, et al. Systematic review of the chemicalcomposition of contemporary dental adhesives. Biomaterials 2007;28:3757–85.
21. Ames JM, Loushine RJ, Babb BR, et al. Contemporary methacrylate resin-based rootcanal sealers exhibit different degrees of ex vivo cytotoxicity when cured in their self-cured mode. J Endod 2009;35:225–8.
22. Gillespie WT, Loushine RJ, Weller RN, et al. Improving the performance of EndoREZroot canal sealer with a dual-cured two-step self-etch adhesive II: apical and coronalseal. J Endod 2006;32:771–5.
23. Perdigao J, Lopes MM, Gomes G. Interfacial adaptation of adhesive materials to rootcanal dentin. J Endod 2007;33:259–63.
24. ANSI/ADA specification no. 57: endodontic sealing material, 2000.25. Kim YK, Grandini S, Ames JM, et al. Critical review on methacrylate resin-based root
canal sealers. J Endod 2010;36:383–99.26. Carvalho-Junior JR, Correr-Sobrinho L, Correr AB, Sinhoreti MA, Consani S, Sousa-
Neto MD. Solubility and dimensional change after setting of root canal sealers:a proposal for smaller dimensions of test samples. J Endod 2007;33:1110–6.
27. Lin-Gibson S, Landis FA, Drzal PL. Combinatorial investigation of the structure-properties characterization of photopolymerized dimethacrylate networks. Bioma-terials 2006;27:1711–7.
28. Pawinska M, Kierklo A, Marczuk-Kolada G. New technology in endodontics: theResilon-Epiphany system for obturation of root canals. Adv Med Sci 2006;51:154–7.
29. Bortoluzzi EA, Guerreiro-Tanomaru JM, Tanomaru-Filho M, Duarte MA. Radio-graphic effect of different radiopacifiers on a potencial retrograde filling material.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:628–32.
30. Phillips RW, Skinner EW. Skinner’s science of dental materials. Philadelphia: Saun-ders; 1991:624.
31. Braden M, Clarke RL. Water absorption characteristics of dental microfinecomposite filling materials: I—proprietary materials. Biomaterials 1984;5:369–72.
32. Skrtic D, Antonucci JM. Dental composites based on amorphous calcium phosphate:resin composition/physicochemical properties study. J Biomaterials Applications2007;21:375–93.
33. Donnelly A, Sword J, Nishitani Y, et al. Water sorption and solubility of methacrylateresin-based root canal sealers. J Endod 2007;33:990–4.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
Effect of Calcium Phosphate Cements on Growth andOdontoblastic Differentiation in Human Dental Pulp CellsSun-Kyung Lee,* Sang-Kwang Lee, MSD,* Sang-Im Lee, MSD,* Jeong-Hui Park, MSD,†
Jun-Hyeog Jang, PhD,‡
Hae-Won Kim, PhD,†§
and Eun-Cheol Kim, DDS, PhD*
Abstract
Objective: Calcium phosphate cements (CPCs) are aninteresting class of bone substitute materials. However,the biological effects of CPCs have not been well studiedin human dental pulp cells (HDPCs). The purpose of thisstudy was to investigate the effects of CPCs on themechanical properties, growth, and odontoblastic differ-entiation in HDPCs compared with Portland cement (PC)and mineral trioxide aggregate (MTA). Methods: Exper-imental CPCs either containing chitosan (Ch-CPC) orwithout chitosan (CPC) were composed from the a-tri-calcium phosphate powder. Setting time, compressivestrength measurements, cell growth, alkaline phospha-tase (ALP) activity, the levels of messenger RNA fordifferentiation-related genes, and mineralization of theHDPCs on various cements were assessed. Results:The setting time for CPC-Ch was 7.5 minutes, whichwas significantly less than the 8.6 minutes for the CPC.On the seventh day of immersion, the compressivestrength of CPC-CH reached 13.1 MPa, which was higherthan 10.8 MPa of CPC. CPC and Ch-CPC-treated cellsshowed decreased cell proliferation but increased thelevels of ALP activity, enhanced mineralized noduleformation, and upregulated odontoblastic markersmessenger RNA including osteonectin, osteopontin,bone sialoprotein, dentin matrix protein-1, matrix extra-cellular phosphoglycoprotein, and dentin sialophospho-protein (DSPP), compared with untreated control. Theresponse of CPC and CP-CPC were similar to that of PCand MTA. However, the adhesion, growth, and differen-tiation in Ch-CPC–treated cells were similar to that in theCPC. Conclusion: CPC may be useful for pulp-cappingapplications based on its abilities to promote HDPCdifferentiation. (J Endod 2010;36:1537–1542)Key WordsCalcium phosphate cement, chitosan, cytotoxicity,human dental pulp cell, odontoblastic differentiation
From the *Department of Oral and Maxillofacial Pathology andKorea; †Department of Nanobiomedical Science and WCU ResearchSchool of Medicine, Inha University, Incheon, Korea; and §Departm(ITREN), Dankook University, Cheonan, Korea.
Hae-Won Kim and Eun-Cheol Kim contributed equally to this arSupported by a grant from the Korea Healthcare technology R&Address requests for reprints to Dr Eun-Cheol Kim, Department
Iksan, South Korea 570-749. E-mail address: eckwkop@wonkwang0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.04.027
JOE — Volume 36, Number 9, September 2010
Traditionally, different formulations of calcium hydroxide (CH) have been used forconservative pulp therapy (1). However, there are disadvantages associated with
the use of CH, such as the presence of tunnels in the dentin bridge and the lack of adhe-sion and degradation after acid etching (2, 3). Recently, several materials have beenproposed as candidates for direct pulp capping including mineral trioxide aggregate(MTA). MTA induces hard tissue repair of the exposed pulp in experimental animalsand promotes dentin bridge formation (4, 5).
Previously, we reported that the mean thickness of the dentin bridges observed inthe MTA group was statistically greater than that of the CH group (6). In addition, signif-icantly greater immunostaining for dentin sialoprotein (DSP) and heme oxygenase-1(HO-1) was observed in the MTA group than in the CH group (6). Moreover, we showedthat the combination of MTA and an enamel matrix derivative promotes more rapiddifferentiation of human dental pulp cells (HDPCs) than MTA alone (7). In addition,we reported that radiopaque Portland cement (PC) is biocompatible and facilitatesodontoblastic differentiation of HDPCs (8). Although MTA is considered to be superiorto CH, the hard tissue–forming mechanism of MTA is basically similar to that of CH,which is known to cause inflammatory and necrotic changes in the subjacent pulp (9).
An alternative pulp-capping material to CH is self-setting calcium phosphatecement (CPC). CPC is a bioactive material that is available in powder and liquid forms,which, when mixed, primarily form hydroxyapatite (10). Self-setting CPC materials arewidely used for orthopedic and dental applications and have the potential to stimulateosteogenesis (11). The self-setting, moderate compressive strength even in loading sitesand highly biocompatibility properties (12) suggest that CPC is superior to pure CH,which means that this material may have applications in pulp capping to induce repar-ative dentin formation or as a lining material (13).
Chitosan is a candidate material for biomedical applications because of its distinc-tive biological properties, which include good biodegradability, biocompatibility, andosteoconductivity (14). In the study of Xu et al (15), chitosan was incorporated intoCPC, thereby increasing the flexural strength, toughness, and strain to failure of thematerial (15). This CPC-chitosan scaffold was found to be biocompatible and to supportthe adhesion and proliferation of osteoblast cells (16). The addition of chitosanstrengthened the CPC and increased alkaline phosphatase (ALP) activity in bonemarrow stem cells (17). However, it has not been investigated whether HDPCs candifferentiate into odontoblast-like cells when exposed to CPC or chitosan-supplemented CPC (CPC-Ch).
The aim of this study was to evaluate the mechanical and biological effectsincluding setting time, compressive strength, surface morphology, cell adhesion,
Institute of Wonkwang Biomaterials Implant, School of Dentistry, Wonkwang University, Iksan,Center, Dankook University, Cheonan, Korea; ‡Department of Biochemistry, School of Medicine,
ent of Biomaterials Science, School of Dentistry and Institute of Tissue Regeneration Engineering
ticle.D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea (A084458).of Oral and Maxillofacial Pathology, College of Dentistry, Wonkwang University, 344-2 Shinyong,.ac.kr.
Effect of CPCs on HDPCs 1537

Basic Research—Technology
proliferation, and odontoblastic differentiation of CPC and CPC-Ch onHDPCs and to compare the results with MTA and PC.Materials and MethodsPreparation of Experimental Cements
The CPC powder a-tricalcium phosphate (TCP) was produced bythe reaction of CaCO3 and dicalcium phosphate anhydrous at 1,400�Cand followed by ball milling and sieving down to 45 mm. Commercialhydroxyapatite (Alfa Aesar, Ward Hill, MA) powder was added at 2 wt%to enhance the crystallization reaction. As the liquid phase, 5% wtNa2HPO4 with or without 2% chitosan solution (Sigma-Aldrich Chemi-cal Co, St Louis, MO) was prepared. The setting reaction was made withthe powder-to-liquid ratio (mixing ratio of powder with respect toliquid) of 3.0, and the mixture was stored at 37�C in 100% humiditychamber for different periods of time. The setting time of the cementswas measured by means of Gillmore needle test according to AmericanSociety for Testing and Materials C266-99-A standard (18). Phasechange of the cements during soaking in saline solution was character-ized with x-ray diffraction (Shimadzu Co, Kyoto, Japan). Compressivestrength of the samples was measured using a mechanical testingmachine (Instron 3344; Instron Corp, Canton, MA). Five total speci-mens were tested under each condition (as hardened and stored for7 days in humidity chamber) were tested. Morphology of the specimenswas observed by scanning electron microscopy (Hitachi Co, Tokyo,Japan).
Under aseptic conditions, white MTA (ProRoot; Dentsply, Tulsa,OK) and PC (Ssangyong, Seoul, Korea) were mixed according to themanufacturer’s instruction. Each sample (diameter, 6 mm; thickness,2 mm) was allowed to set for 24 hours at 37�C in 100% humidity.
Cell CultureWe used the HDPCs lines immortalized by transfection with the
telomerase catalytic subunit hTERT gene (19). Cells were cultured inDulbecco’s Modified Eagle’s Medium supplemented with 10% fetalbovine serum, 100 U/mL penicillin, and 100 mg/mL streptomycin ina humidified atmosphere of 5% CO2 at 37�C. For mineralization exper-iments, cells were cultured in 50 mg/mL ascorbic acid (AA) and 10mmol/L b-glycerophosphate (bGP)-containing media as describedpreviously (20). The cements were all placed at the bottom of 24-well tissue culture plates, washed twice with phosphate buffer solution,dried under laminar flow for 24 hours at room temperature, and ster-ilized by gamma-radiation with 37.2 Gray before being used to culturecells. HDPCs were seeded at 1 � 105 cells per well on the preparedcements and cultured for up to 14 days.
TABLE 1. Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR) Primers Se
Gene
Osteonectin (ON) Forward: AReverse: C
Osteopontin (OPN) Forward: CReverse: G
Bone sialoprotein (BSP) Forward: TReverse: G
Dentin sialophosphoprotein (DSPP) Forward: CReverse:CT
Dentin-matrix protein-1 (DMP-1) Forward:CReverse:CT
MEPE Forward: AReverse: G
GAPDH Forward:CReverse:A
1538 Lee et al.
Cell Adhesion and ViabilityAt each culturing period (1, 7, and 14 days), the cells were har-
vested, and the cell viability was measured as the mitochondrial nicotin-amide adenine dinucleotide– and nicotinamide adenine dinucleotidephosphate–dependent dehydrogenase activity using a cell proliferationassay kit (CellTiter 96 Aqueous One Solution; Promega, Madison,WI). A colorimetric measurement was performed using a microplatereader at an absorbance of 490 nm. The cell growth morphology wasobserved by scanning electron microscopy at an accelerating voltageof 15 kV after fixing with glutaraldehyde (2.5%), dehydrating witha graded series of ethanol (75%, 90%, 95%, and 100%), and treatingwith hexamethyldisilazane and platinum coating.
ALP ActivityIncubated HDPCs were washed with PBS and then sonicated with
a cell disruptor. ALP activity was measured using p-nitrophenyl phos-phate (3 mmol/L final concentration) as the substrate in 0.7 mol/L2-amino-methyl-1-propanol, pH of 10.3, and 6.7 mmol/L MgCl2. Absor-bance was measured at 410 nm using an enzyme-linked immunosor-bent assay reader (Beckman Coulter, Fullerton, CA).
Alizarin Red StainingCells were cultured in DMEM containing 10% FBS, 50 mg/mL AA,
and 10 mmol/L bGP in the absence or presence of cements for 14 daysfor mineralized nodule assay. The culture medium was replaced withfresh culture medium every 2 days. After 14 days of treatment, thecalcium deposition of HDPCs was studied using 0.1% alizarin red Sstaining solution (Sigma-Aldrich, St. Louis, MO). The samples werefixed with 70% ice-cold ethanol for 1 hour, rinsed twice with PBS,and stained with 40 mmol/L alizarin red solution for 10 minutes underconditions of gentle agitation. The pictures of alizarin red S stainingwere photographed under light microscopy.
Reverse Transcription-Polymerase Chain ReactionThe total RNA of pulp cells was extracted using the Trizol reagent
(Life Technologies, Gaithersburg, MD) according to the manufacturer’sinstruction. Then, 1 mg RNA was reverse-transcribed for first-strandcomplementary DNA (cDNA) synthesis (Gibco BRL, Rockville, MD).The cDNA was amplified in a final volume of 20 mL containing 2.5mmol/L magnesium dichloride, 1.25 U Ex Taq polymerase (Bioneer,Daejeon, Korea) and 1 mmol/L specific primers. Amplification was per-formed for 30 cycles in a DNA thermal cycler. Primer sequences fordifferentiation markers are detailed in Table 1. The PCR productswere resolved on a 1.5% agarose gel and stained with ethidium
quence
Sequence (5’ -3’) Size (bp)
CATGGGTGGACACGGCAACAGCCTAATGTGAA 405CAAGTAAGTCCAACGAAAGGTGATGTCCTCGTCTGTA 347GGAGATGACAGTTCAGAAGTACTGGTGCCGTTTATGC 333AGTGATGAATCTAATGGCGATTTGCTGCTGTCTGAC 488AGGAGCACAGGAAAAGGAGGGTGGTATCTTCCCCCAGGAG 213TGCGAGTTTTCTGTGTGGTTTTCTTCCCCCAGGAG 503GGAGTCAACGGATTTGGTCGTATGCCTTCTCCAGGTGGTGAAGAC 306
JOE — Volume 36, Number 9, September 2010

TABLE 2. Summary of Characteristics of the Experimental Calcium Phosphate Cements Used in This Study (CPC, CPC-Ch, PC and MTA)
CPC CPC-Ch PC MTA
Starting powder a-TCP a-TCP + chitosan Calcium silicates Calcium silicates,bismuth oxide
Setting time (ave. min) 8.6 7.5 468 165Crystalline phase* Hydroxyapatite HydroxyapatiteCompressive strength (MPa) 10.8 � 3.0 13.1 � 2.1 19.5 ˜30.1 40.0†
CPC, calcium phosphate cement; CPC-Ch, CPC with chitosan; PC, Portland cement; and MTA, mineral trioxide aggregate.
*Newly formed after soaking for 7 days in saline.†After 24 h of immersion in water.
Basic Research—Technology
bromide. The intensity of each band after normalization with glyceral-dehyde 3-phosphate dehydrogenase messenger RNA was quantified onthe photographed gels with a densitometer (Quantity One; Bio-Rad,Hercules, CA).
Statistical AnalysisData are presented as mean � standard deviation. Continuous
variables in the present study met the criteria for a normal distributionand were assumed to be parametric. The statistical analysis of the datawas performed by one-way analysis of variance followed by a multiple-comparison Tukey test with the use of an SPSS program (SPSS 12.0;SPSS GmbH, Munich, Germany). Statistical significance was determinedat p < 0.05.
ResultsSetting Time, Compressive Strength, and SurfaceMorphology of the Cements
The characteristics of the experimental cements, CPC and CPC-Ch,are summarized in Table 2. Data on both PC and MTA are also presentedfor comparison (21, 22). Although both experimental CPCs hardened
Figure 1. Scanning electron microscopic morphology of the (A) CPC and (B and
JOE — Volume 36, Number 9, September 2010
within 10 minutes of mixing with basic solvent, in a process driven bythe acid-basic reaction, the PC and MTA have very long setting times,which have been concerned as the major drawback of the PC andMTA (21). The compressive strengths of CPCs were approximately 10to 13 MPa, which were significantly increased up to 20 to 25 MPa afterincubation in water. The PC and MTA have compressive strengths insimilar ranges of CPCs that were also increased when immersed in water.
Figure 1 shows the SEM surface morphologies of the CPC and CPC-Ch specimens after soaking in PBS for 7 days. The surfaces of bothcements showed similar morphologies with numerous ultrafine crystal-lites in a rosette form, which is typical of the apatite crystals observed inCPC.
Effects of Cements on Cell Viability and MorphologyThe levels of cell growth, as measured by the (3-(4,5-dimethyl-
thiazol-2-yl)-5-(3-carboxymethoxyphenyl)-2-(4-sulfophenyl)-2H-tetrazolium, inner salt) assay, are represented in Figure 2A. It wasobserved that all the materials including MTA, PC, CPC, and CPC-Chshowed cytotoxicity against HDPCs when the cells were incubated at24 hours. In contrast, the MTA and PC did not show significant cytotox-icity against HDPCs at 14 days, whereas CPC and CPC-Ch showed
C) chitosan CPC. Results were reproduced in two separate experiments.
Effect of CPCs on HDPCs 1539

% o
f co
ntro
l
0
0 2
0 4
0 6
0 8
0 0 1
0 2 1
h c - C P C C P C C P A T M l o r t n o c
* *
*
* * * *
* *
s t n e m e c
y a d 1 s y a d 7 s y a d 4 1
MTA PC
CPC CPC-ch
Figure 2. The effects of cements on (A) cell viability and (B) adhesion by the MTS method and SEM, respectively. )Statistically significant difference as comparedwith control, p < 0.05. SEM micrographs of the HDPCs grown on the MTA, PC, CPC, and CPC cements for 7 days of culture. Results (n = 5) were reproduced inthree separate experiments.
Basic Research—Technology
cytotoxicity at 1, 7, and 14 days. However, there was no significantdifference in cell viability between CPC and CPC-Ch for 1, 7, and 14 days.
To investigate the influence of the cements on cell spreading, SEMinvestigations of adhesion were performed (Fig. 2B). The HDPCs on allsamples showed an elongated/spindle-shaped morphology. There wereno differences in spreading among the MTA, PC, CPC, and CPC-Chgroups.
1540 Lee et al.
Effects of Cements on the Odontoblastic Differentiationof HDPCs
To investigate the odontoblast-like differentiation of HDPCs treatedwith the cements, we assessed the levels of ALP activity, alizarin redstaining, and messenger RNA expression of differentiation markerssuch as osteonectin (ON), osteopontin (OPN), bone sialoprotein(BSP), dentin matrix protein-1 (DMP-1), matrix extracellular
JOE — Volume 36, Number 9, September 2010

Figure 3. The effects of cements on (A) ALP activity; (B) the formation of calcification nodules; and (c) the expression of ON, OPN, BSP, MEPE, DMP-1 and DSPPmessenger RNA in HDPCs. HDPCs were cultured in DMEM with 0.05 mmol/L AA and 10 mmol/L bGP in the presence of indicated kinds of cements for 14 days. Thecells treated with bGP and AA were used as a negative control. Representative ALP data were the average of five replicates. After 14 days, representative photographsof alizarin red S staining are shown (original magnification,�200). The RT-PCR data represent one of three independent experiments with similar results. (D) Therelative density of cytokine mRNA to GAPDH messenger RNA. Levels of messenger RNA genes were measured by densitometry. The relative level of gene expressionwas normalized against the GAPDH messenger RNA signal, and the control was set as 1.0. Relative density values represent the mean� standard deviation of threeindependent experiments. )Significant difference from control (p < 0.05).
Basic Research—Technology
JOE — Volume 36, Number 9, September 2010 Effect of CPCs on HDPCs 1541

Basic Research—Technology
phosphoglycoprotein (MEPE), and dentin sialophosphoprotein(DSPP) (23). Observation from alizarin red S staining at 14 daysshowed a strong positive calcium deposition in HDPCs exposed of allkind of cements, whereas the stain was not obvious in control cells.As shown in Figure 3A and B, the ALP activity and calcium depositionof the CPC-Ch–treated group was similar to that of the CPC, PC, andMTA group. CPC and CPC-Ch increased the messenger RNA expressionlevels of the odontogenic genes DMP-1, DSPP, MEPE, ON, OPN, and BSPas compared with the control treatment at 1, 7, and 14 days of cultiva-tion. In contrast, no significant differences in the levels of mRNA expres-sion for markers genes were observed between the CPC and CPC-Chgroups (Fig. 3C and D).DiscussionAlthough CPCs are attractive materials for bone reconstruction
(eg, alveolar ridge augmentation and craniofacial recovery) (14), theirutility in the regeneration of dental pulp-dentin complex tissue has notbeen well documented. Bacterial growth inhibition and better mechan-ical properties than CH was observed for hydraulic CPC (24). In addi-tion, newly developed CPC-based root canal sealers were well adaptedto the canal wall and infiltrated into the dentinal tubules (25). As the a-TCP–based CPC used in the present study is cell compatible and stim-ulates osteoblastic differentiation and mineralization (10), it is expectedto facilitate the growth and odontoblastic differentiation of pulp cells.Furthermore, the addition of chitosan to CPC, which is known toenhance mechanical properties (26, 27), is also required to addressthe efficacy in biological roles in dentin regeneration.
Mechanical strength is a critical parameter for biomaterials usedin tooth repair or pulp capping therapy. The compressive strength of theexperimental CPCs was increased from 10.8 MPa to 13.1 MPa by theaddition of chitosan, and this increase is attributed to the strengtheningeffect of the transformed apatite nanocrystallites, which interlock toform a more compact network than that formed by the original a-TCP–based structure.
We tested the experimental CPCs for their effects on HDPC prolif-eration and odontogenesis. We found that CPC and CPC-Ch were cyto-toxic for HDPCs at 1, 7, and 14 days of cultivation. These results aresupported by the data of Khashaba et al (28) who reported that CPCdecreased the proliferation of human gingival fibroblasts and a mousefibroblast cell line. In the CPC setting, TTCP (Ca4[PO4]2O) and dical-cium phosphate anhydrous (CaHPO4) dissolved in the liquid as Ca2+,PO4
3�, and OH� ions, which then reprecipitated to form hydroxyapatite(29). It seems likely that the ionic activities and pH changes thatoccurred during setting were responsible for the observed cytotoxicities(30).
In our study, CPC and CPC-Ch promoted odontoblastic differenti-ation of HDPCs, as evidenced by the formation of mineralized nodules,the induction of ALP activity in the early stage, and the up-regulation ofodontoblastic markers; these results are consistent with other studies inmesenchymal stem cells (17). But chitosan did not enhance adhesion,growth and differentiation of HDPCs on CPC. These contrary results maybe due to different sources of chitosan. In summary, the study reportsfor the first time that CPC facilitates the growth and differentiation ofHDPCs, whereas these effects of CPC were not affected by chitosan.
References1. Pereira JC, Segala AD, Costa CAS. Human pulpal response to direct pulp capping
with an adhesive system. Am J Dent 2000;13:139–47.2. Cox CF, Subay RK, Ostro E, et al. Tunnel defects in dentin bridges: their formation
following direct pulp capping. Oper Dent 1996;21:4–11.
1542 Lee et al.
3. Cox CF, Hafez AA, Akimoto N, et al. Biocompatibility of primer, adhesive and resincomposite systems on non-exposed and exposed pulps of non-human primate teeth.Am J Dent 1998;11:S55–63.
4. Pitt Ford TR, Torabinejad M, Abedi HR, et al. Using mineral trioxide aggregate asa pulp-capping material. J Am Dent Assoc 1996;127:1491–4.
5. Faraco IM Jr, Holland R. Response of the pulp of dogs to capping with mineraltrioxide aggregate or a calcium hydroxide cement. Dent Traumatol 2001;17:163–6.
6. Min KS, Park HJ, Lee SK, et al. Effect of mineral trioxide aggregate on dentin bridgeformation and expression of dentin sialoprotein and heme oxygenase-1 in humandental pulp. J Endod 2008;34:666–70.
7. Min KS, Yang SH, Kim EC. The combined effect of mineral trioxide aggregate andenamel matrix derivative on odontoblastic differentiation in human dental pulpcells. J Endod 2009;35:847–51.
8. Min KS, Lee SI, Lee Y, et al. Effect of radiopaque Portland cement on mineralizationin human dental pulp cells. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2009;108:e82–6.
9. Kuratate M, Yoshiba K, Shigetani Y, et al. Immunohistochemical analysis of nestin,osteopontin, and proliferating cells in the reparative process of exposed dental pulpcapped with mineral trioxide aggregate. J Endod 2008;34:970–4.
10. Dickens-Venz SH, Takagi S, Chow LC, et al. Physical and chemical properties ofresin-reinforced calcium phosphate cements. Dent Mater 1994;10:100–6.
11. Ruhe PQ, Hedberg-Dirk EL, Padron NT, et al. Porous poly (DL-lactic-co-glycolicacid)/calcium phosphate cement composite for reconstruction of bone defects.Tissue Eng 2006;12:789–800.
12. Lye KW, Tideman H, Merkx MA, et al. Bone cements and their potential use ina mandibular endoprosthesis. Tissue Eng Part B Rev 2009;15:485–96.
13. Chaung HM, Hong CH, Chiang CP, et al. Comparison of calcium phosphate cementmixture and pure calcium hydroxide as direct pulp-capping agents. J Formos MedAssoc 1996;95:545–50.
14. Muzzarelli RAA, Biagini G, Bellardini M, et al. Osteoconduction exerted by methyl-pyrolidinone chitosan in dental surgery. Biomaterials 1993;14:39–43.
15. Xu HHK, Quinn JB, Takagi S, et al. Processing and properties of strong and non-rigidcalcium phosphate cement. J Dent Res 2002;81:219–24.
16. Xu HHK, Simon CG Jr. Fast setting calcium phosphate-chitosan scaffold: mechanicalproperties and biocompatibility. Biomaterials 2005;26:1337–48.
17. Moreau JL, Xu HH. Mesenchymal stem cell proliferation and differentiation on aninjectable calcium phosphate-chitosan composite scaffold. Biomaterials 2009;30:2675–82.
18. Am Society for Testing and Materials. Standard test method for time of setting ofhydraulic-cement paste by Gillmore needles. Annual book of ASTM standards.Conshohocken, PA: American Society for Testing and Materials; 2006;ASTMC266–03.
19. Kitagawa M, Ueda H, Iizuka S, et al. Immortalization and characterization of humandental pulp cells with odontoblastic differentiation. Arch Oral Biol 2007;52:727–31.
20. Yasuda Y, Ogawa M, Arakawa T, et al. The effect of mineral trioxide aggregate on themineralization ability of rat dental pulp cells: an in vitro study. J Endod 2008;34:1057–60.
21. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literaturereview-part I: chemical, physical, and antibacterial properties. J Endod 2010;36:400–13.
22. Camilleri J. The physical properties of accelerated Portland cement for endodonticuse. Int Endod J 2008;41:151–7.
23. D’Souza RN, Bachman T, Baumgardner KR, et al. Characterization of cellularresponses involved in reparative dentinogenesis in rat molars. J Dent Res 1995;74:702–9.
24. Kouassi M, Michaılesco P, Lacoste-Armynot A, et al. Antibacterial effect of a hydrauliccalcium phosphate cement for dental applications. J Endod 2003;29:100–3.
25. Yang SE, Baek SH, Lee W, et al. In vitro evaluation of the sealing ability of newlydeveloped calcium phosphate-based root canal sealer. J Endod 2007;33:978–81.
26. Lian Q, Li DC, He JK, et al. Mechanical properties and in-vivo performance ofcalcium phosphate cement-chitosan fibre composite. Proc Inst Mech Eng H2008;222:347–53.
27. Pan Z, Jiang P, Fan Q, et al. Mechanical and biocompatible influences of chitosanfiber and gelatin on calcium phosphate cement. J Biomed Mater Res B ApplBiomater 2007;82:246–52.
28. Khashaba RM, Chutkan NB, Borke JL. Comparative study of biocompatibility of newlydeveloped calcium phosphate-based root canal sealers on fibroblasts derived fromprimary human gingiva and a mouse L929 cell line. Int Endod J 2009;42:711–8.
29. Dagang G, Kewei X, Haoliang S, et al. Physicochemical properties of TTCP/DCPAsystem cement formed in physiological saline solution and its cytotoxicity. J BiomedMater Res A 2006;77:313–23.
30. Matsuya S, Takagi S, Chow LC. Effect of mixing ratio and pH on the reaction betweenCa4(PO4)2O and CaHPO4. J Mater Sci Mater Med 2000;11:305–11.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
Effect of Cement Type, Relining Procedure, and Length ofCementation on Pull-out Bond Strength of Fiber PostsVanessa Cruz Macedo, MD, DDS,* Andre Luis Faria e Silva, PhD, MD, DDS,†
and Luis Roberto Marcondes Martins, PhD, MD, DDS‡
Abstract
Introduction: As opposed to the cementation metalposts, the cementation of fiber posts has several detailsthat can significantly influence the success of post reten-tion. This study evaluated the effect of the reliningprocedure, the cement type, and the luted length ofthe post on fiber posts retention. Methods: Onehundred eighty bovine incisors were selected to assesspost retention; after endodontic treatment, the canalswere flared with diamonds burs. Post holes wereprepared in lengths of 5, 7.5, and 10 mm; the fiber postswere relined with composite resin and luted with RelyXARC, RelyX Unicem, or RelyX Luting 2. All cements aremanufactured by 3M ESPE (St. Paul, MN). Sampleswere subjected to a pull-out bond strength test ina universal testing machine; the results (N) weresubmitted to a three-way analysis of variance and theTukey post hoc test (a = 0.05). Results: The improve-ment of post retention occurred with the increase of thepost length luted into the root canal; the relining proce-dure improved the pull-out bond strength. RelyX Unicemand RelyX ARC showed similar values of retention, bothshowing higher values than RelyX Luting 2. Conclusion:Post length, the relining procedure, and the cement typeare all important factors for improving the retention offiber posts. (J Endod 2010;36:1543–1546)Key WordsBond strength, fiber post, resin cement
From the *Department of Dental Materials and Prosthodon-tics, Sao Jose dos Campos Dental School, Sao Paulo StateUniversity, Sao Jose dos Campos, SP, Brazil; †Department ofDentistry, Federal University of Sergipe, Aracaju, SE, Brazil;and ‡Department of Restorative Dentistry, Piracicaba DentalSchool, University of Campinas, Piracicaba, SP, Brazil.
Address requests for reprints to Andre Luis Faria e Silva,Departamento de Odontologia, Campus da Saude ‘‘Prof JoaoCardoso Nascimento Junior,’’ Rua Claudio Batista S/N, BairroSanatorio, Aracaju/SE, Brazil 49060-100. E-mail address:[email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.04.014
JOE — Volume 36, Number 9, September 2010
Intraradicular posts are commonly used to restore endodontically treated teeth whentheir remaining coronal tissue can no longer provide adequate support and retention
for the restoration (1, 2). For decades, endodontically treated teeth have been restoredusing cast metal posts; despite their high retention and thin resulting cement film, theseconventional posts have a high elastic modulus and can lead to root fractures (3, 4). Onthe other hand, the similar elastic modulus of fiber posts, resin cements, and dentin isconsidered to be advantageous for improving the performance of restorations (5, 6).
In contrast to rigid posts, fiber posts do not need to be inserted to a length equal toor longer than the depth of the clinical crown in order to reduce the chance of rootfracture (7). This is advantageous for short roots or for roots presenting a high degreeof curvature. Once the fiber posts are adhesively luted into the canal, a high in-depthinsertion into the root canal is not necessary to improve retention (8). This is feasiblebecause the bonding of the cement to dentin walls is more effective in the cervical regionthan in the apical region (9, 10).
Despite the cited advantages, the mismatch between the diameters of the postspace and the fiber post remains a clinical problem (11, 12); prefabricated posts donot fit well into elliptical-shaped canals (13) or flared canals that result from cariousextension, trauma, pulpal pathosis, or iatrogenic misadventure (11). In such cases, ifthe post does not fit well, the layer of resin cement might be excessively thick, favoringthe formation of air bubbles and predisposing the post to debonding (14).
One solution for this issue is to reline the fiber post with resin composite (15);customizing the post increases its adaptation to the root walls and reduces the thicknessof the resin cement (14). Improving the contact between the post and the canal wallsmay also reduce the dependence on the bonding for retention (16). It has been shownthat cements with lower bonding potential but other favorable mechanical propertiesmay be useful in luting relined fiber posts (17). Therefore, the aim of this study wasto evaluate the effect of fiber post relining with resin composite, cement type usedfor luting, and post-hole length on the pull-out bond strength of fiber posts luted toroot canals.
Materials and MethodsOne hundred eighty recently extracted bovine incisors with similar root sizes and
lengths were selected for this study. The crowns were removed above the cementum-enamel junction with a low-speed diamond saw in order to obtain a remaining rootheight of 16 mm. For the endodontic treatment, a step-back preparation techniquewas used; to flare the coronal and middle third of the canal, a #2 Gates Glidden drillwas inserted several millimeters into the canal. This was repeated with #3 and #4 drills.Apical preparation was conducted with the final master apical file of size 40; flaring ofthe canal was completed with filing to size 70. All enlargement procedures were fol-lowed by irrigation with 2.5% sodium hypochlorite solution. The prepared root canalswere obturated with gutta-percha cones using the lateral condensation technique andSealer-26 resin sealer (Dentsply Ind Com Ltda, Petropolis, RJ, Brazil). The specimenswere stored in 100% humidity for at least 72 hours to allow for the resin sealer to set.
After the storage period, the coronal gutta-percha was removed with a hot Rheininstrument at 5-, 7.5-, and 10-mm depth. In order to obtain a standardized flared canal,the canals were enlarged using #4138 and 4137 high-speed diamond burs (KG Soren-sen Ind e Com LTDA, Sao Paulo, SP, Brazil) under water irrigation. Three post spacedepths were prepared: 5, 7.5, and 10 mm. In order to facilitate handling, the roots
Pull-out Strength of Fiber Posts 1543

TABLE 1. Description of Cements Used in This Study and the Application Protocols
Cement Classification Application protocol
RelyX ARC Resin cement The canal walls were etched with 35% phosphoric acid for 15 seconds, rinsed for15 seconds, and gently air dried. Excess water was removed from the postspace with absorbent paper points. The Scotchbond Multipurpose PlusActivator (3M ESPE, St Paul, MN) was applied into the root canal with amicrobrush of compatible size and air dried for 5 seconds. Afterwards, theScotchbond Multipurpose Plus Primer (3M ESPE) and also air dried. Thedual-cured resin cement RelyX ARC was mixed and placed over the posts,which was inserted into the root canal with light pressure. The excess ofluting material was removed and light activation was performed for40 seconds.
RelyX Unicem Self-adhesive resin cement The root canal walls were rinsed with water using a syringe and then gently driedwith paper points. The cement capsule was activated for 2 seconds and mixedautomatically in a high-speed triturator for 10 seconds. Afterwards, the resincement was applied into the root canals by means of Elongation Tip (3M ESPE).The post was then seated in the root canal; the excess resin was subsequentlyremoved. The light activation was performed for 40 seconds.
RelyX Luting Resin-modified glass ionomer The root canal walls are cleaned and dried as described for RelyX Unicem. Thecement was mixed for 10 s inserted into the canal with 50 K-file. The post wasinserted into the canal with light pressure and stabilized during 2 min. Then,the excess material was removed.
Basic Research—Technology
were embedded in polystyrene resin blocks. Parallelism between thepost and resin block was obtained using a parallel meter.
The prepared root canals received either relined or nonrelinedfiber posts; a 1.5-mm diameter glass fiber-reinforced epoxy post system(Reforpost; Angelus, Londrina, Brazil) was used. The Adper SingleBond 2 adhesive system (3M ESPE, St Paul, MN) was applied and lightcured over the previously silanized post before the cementation proce-dure. For the relining procedure, the fiber post was treated as previouslydescribed. Afterwards, the canal walls were lubricated with a hydrosol-uble gel; the fiber post was covered with resin composite Filtek Z250(3M ESPE) and inserted into the canal. The resin composite was lightcured for 20 seconds, the relined fiber post was removed, and the resincomposite was light cured again for 20 seconds. Copious rinsingremoved the lubricant gel from the root canal. The cements used forcementation and the details of the luting procedures are described inTable 1.
The specimens were stored in 100% humidity at 37�C for 24 hoursbefore testing. The pull-out test was performed parallel to the long axisof both the post and the tooth at a cross-head speed of 0.5 mm/minusing a universal testing machine (Model 4411; Instron Inc, High Wy-combe, UK). The force required to dislodge each post was then re-corded in newtons. The independent variables tested in this studywere the post relining, the cement type, and the depth of luting. Statis-tical analysis was performed by applying a three-way analysis of variancefollowed by the Tukey post hoc test at a 95% confidence level.
ResultsAnalysis of variance revealed statistically significant differences for
all factors (p < 0.01); however, there was no significant effect for anyinteraction between the factors (p > 0.05). Comparisons using the
TABLE 2. Bond Strength Means (Standard Deviations) for All Cements and Post T
Ceme
Post type RelyX ARC RelyX Un
Non-relined post 245.1 (74.5) 208.4 (83.Relined post 336.7 (91.6) 362.4 (87.Pooled average 290.9 (94.8) A 285.4 (115
For the pooled averages, means followed by distinct letters are significantly different (Tukey test, 95% co
1544 Macedo et al.
Tukey test are shown in Tables 2 and 3. Because statistical significanceswere detected only for the factors observed individually, comparisonswere performed only for the pooled average. Relined posts presentedsignificantly higher pull-out bond strengths than nonrelined posts.Regarding the depth of post cementation, posts that were luted ata 10-mm depth presented the highest values followed by those lutedat a 7.5-mm depth. RelyX ARC and RelyX Unicem showed similar resultsfor retention, both showing significantly higher bond strengthscompared with RelyX Luting 2.
DiscussionWhen restoring root-filled teeth, clinicians are opting for materials
that have an elastic modulus similar to that of dentin, that are capable ofcreating homogenous stress distribution, and that are able to decreasethe incidence of catastrophic root fractures (18, 19). Fiber posts haveelastic moduli similar to that of dentin and have the ability to bond to thissubstrate by the use of adhesive cements. Thus, it has been shown that itis not necessary to increase the depth of fiber post cementation in orderto improve fracture resistance (7). However, the results of the currentstudy show that, irrespective of the type of cement used, increasing thedepth of cementation is beneficial to improve the post retention.
Several studies have shown that the bond strength of resin cementsto root canals is effective in the cervical third but weak in the apical third(11, 20–22). Thus, it is reasonable to assume that the bond to thecervical third of the root canal could be enough to promote properpost retention. Regardless of the low bond strength in the apicalregions, the frictional retention in these areas contributes to thedislocation resistance of the fiber post (23, 24). Frictional retentionis directly proportional to the contact area (the larger the contactsurfaces, the better the retention). This explains the results of this
ypes (N)
nts
icem RelyX Luting 2 Pooled average
8) 101.7 (57.0) 185.1 (94.3) B8) 147.1 (71.0) 282.1 (127.3) A.2) A 124.4 (67.8) B
nfidence level).
JOE — Volume 36, Number 9, September 2010

TABLE 3. Bond Strength Means (Standard Deviations) for All Post Lengths and Post Types (N)
Post length
Post type Cement 5 mm 7.5 mm 10 mmOverall for cement
by post type Pooled average
RelyX ARC 199.9 (72.3) 254.4 (65.1) 281.1 (67.8) 245.1 (74.5) ANon-relined post RelyX Unicem 146.6 (46.5) 213.2 (91.0) 265.8 (65.0) 208.4 (83.8) A 185.1 (94.3) B
RelyX Luting 44.1 (10.8) 110.3 (34.3) 150.8 (52.2) 101.7 (57.0) BRelyX ARC 318.3 (67.6) 300.3 (36.4) 391.5 (126.4) 336.7 (91.6) A
Relined post RelyX Unicem 304.8 (57.9) 387.5 (84.1) 394.9 (94.1) 362.4 (87.8) A 282.1 (127.3) ARelyX Luting 78.0 (23.9) 173.5 (48.0) 189.8 (72.4) 147.1 (71.0) B
Pooled average 181.9 (116.1) C 239.9 (108.6) B 279.0 (122.2) A
For the pooled averages, means followed by distinct letters are significantly different (Tukey test, 95% confidence level).
Basic Research—Technology
study; fiber posts luted deeper provided the highest pull-out bondstrengths.
In addition to the contact area, closer contact between cement typeand dentin is also important in order to improve the frictional retentionof the post. In this study, the relining procedure increased the postretention to the root canal. A higher post-to-root canal adaptationincreases the sustained pressure during cementation (16). The appli-cation of sustained pressure results in better contact between thecement/post assembly and the dentin (25). This results in higher fric-tional retention compared with nonrelined posts and consequently inincreased pull-out bond strengths. Furthermore, a higher sustainedpressure during cementation reduces blister formation in the cement(25); blisters can act as flaw-initiating sites during pull-out testing,interfering with the bond strength. Based on these results, it seemsthat the relining procedure increases the fiber post retention byimproving the contact between the cement and the adhesive ratherthan by reducing the defects observed in thin cement layers.
Regarding the cement, the RelyX Luting 2 presented the lowestvalues of pull-out bond strength. This is a resin-modified glass ionomer,exhibiting lower bond strengths than other evaluated cements (26). Thelow bond strength is probably related to the application over the smearlayer because no acid solution is applied before cementation. Thus, theretention provided by RelyX Luting 2 is more dependent on frictionalretention than on its bonding to dentin. Because the mechanical prop-erties of this cement are poorer compared with the resin cements, it isexpected that this cement will have the lowest retention (27).Conversely, RelyX Unicem is a self-adhesive resin cement and interactsvery superficially with the substrate, resulting in poor bond strength(28). However, it appears that RelyX Unicem has good chemical inter-action with the calcium in hydroxyapatite, improving their mechanicalproperties (29). Furthermore, self-adhesive resin cements appear tohave low shrinkage because of their viscoelastic properties, leadingto better intimate contact of the resin cement with the root canal wallsand higher frictional resistance (30).
RelyX ARC is a conventional dual-cured resin cement that gener-ates higher bond strength to dentin than the other cements evaluated(27). However, its high polymerization shrinkage and the resultingstress could impair the bonding to the root dentin (31). This increasesthe dependency on mechanical properties of cement for improving thepost retention. Despite being a dual-cured material, deeper portions ofcement are inaccessible to light, rendering the material dependent onthe chemical curing. This can reduce the degree of conversion of thecement and consequently affect its mechanical properties. However,the use of a primer that is activated before insertion of the cementmay improve the conversion. The primer contains sodium and sulfinicacid salts that react with the primer’s acidic resin monomers to producefree radicals that would enhance the polymerization reaction of thecement (32, 33). Thus, the approach indicated by the manufacturer
JOE — Volume 36, Number 9, September 2010
of RelyX ARC improves both the mechanical properties of the cementand post retention.
Although fiber post retention seems to be derived predominantlyfrom frictional retention, the luted length of the post is just as importantto improve their retention. Relining the fiber post reduces the thicknessof the cement layer and also improves the frictional retention. Thereduction of resin thickness may also reduce the polymerization stressbecause the stress development increases associated with increasedvolume of the resin cement (34). In conclusion, the use of cementwith proper mechanical properties is essential for adequate postretention.
References1. Fernandes AS, Shetty S, Coutinho I. Factors determining post selection: a literature
review. J Prosthet Dent 2003;90:556–62.2. Soares CJ, Soares PV, de Freitas Santos-Filho PC, et al. The influence of cavity design
and glass fiber posts on biomechanical behavior of endodontically treated premo-lars. J Endod 2008;34:1015–9.
3. Dietschi D, Duc O, Krejci I, et al. Biomechanical considerations for the restorationof endodontically treated teeth: a systematic review of the literature, Part II (Evalu-ation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int 2008;39:117–29.
4. Nakamura T, Ohyama T, Waki T, et al. Stress analysis of endodontically treatedanterior teeth restored with different types of post material. Dent Mater J 2006;25:145–50.
5. Schmitter M, Huy C, Ohlmann B, et al. Fracture resistance of upper and lower inci-sors restored with glass fiber reinforced posts. J Endod 2006;32:328–30.
6. D’Arcangelo C, De Angelis F, Vadini M, et al. In vitro fracture resistance and deflec-tion of pulpless teeth restored with fiber posts and prepared for veneers. J Endod2008;34:838–41.
7. Santos-Filho PC, Castro CG, Silva GR, et al. Effects of post system and length on thestrain and fracture resistance of root filled bovine teeth. Int Endod J 2008;41:493–501.
8. Braga NM, Paulino SM, Alfredo E, et al. Removal resistance of glass-fiber andmetallic cast posts with different lengths. J Oral Sci 2006;48:15–20.
9. Faria e Silva AL, Arias VG, Soares LE, et al. Influence of fiber-post translucency on thedegree of conversion of a dual-cured resin cement. J Endod 2007;33:303–5.
10. Faria e Silva AL, Casselli DS, Ambrosano GM, et al. Effect of the adhesive applicationmode and fiber post translucency on the push-out bond strength to dentin. J Endod2007;33:1078–81.
11. D’Arcangelo C, Cinelli M, De Angelis F, et al. The effect of resin cement film thicknesson the pullout strength of a fiber-reinforced post system. J Prosthet Dent 2007;98:193–8.
12. Teixeira CS, Silva-Sousa YT, Sousa-Neto MD. Bond strength of fiber posts toweakened roots after resin restoration with different light-curing times. J Endod2009;35:1034–9.
13. De-Deus G, Murad C, Paciornik S, et al. The effect of the canal-filled area on thebacterial leakage of oval-shaped canals. Int Endod J 2008;41:183–90.
14. Grandini S, Goracci C, Monticelli F, et al. SEM evaluation of the cement layerthickness after luting two different posts. J Adhes Dent 2005;7:235–40.
15. Grandini S, Sapio S, Simonetti M. Use of anatomic post and core for reconstructingan endodontically treated tooth: a case report. J Adhes Dent 2003;5:243–7.
16. Faria-e-Silva AL, Pedrosa-Filho CF, Menezes MS, et al. Effect of relining on fiber postretention to root canal. J Appl Oral Sci 2009;17:600–4.
Pull-out Strength of Fiber Posts 1545

Basic Research—Technology
17. Naumann M, Sterzenbach G, Rosentritt M, et al. Is adhesive cementation ofendodontic posts necessary? J Endod 2008;34:1006–10.18. Naumann M, Blankenstein F, Dietrich T. Survival of glass fibre reinforced composite
post restorations after 2 years-an observational clinical study. J Dent 2005;33:305–12.19. Bitter K, Noetzel J, Stamm O, et al. Randomized clinical trial comparing the effects of
post placement on failure rate of postendodontic restorations: preliminary results ofa mean period of 32 months. J Endod 2009;35:1477–82.
20. D’Arcangelo C, Zazzeroni S, D’Amario M, et al. Bond strengths of three types of fibre-reinforced post systems in various regions of root canals. Int Endod J 2008;41:322–8.
21. Giachetti L, Grandini S, Calamai P, et al. Translucent fiber post cementation usinglight- and dual-curing adhesive techniques and a self-adhesive material: push-outtest. J Dent 2009;37:638–42.
22. Hayashi M, Okamura K, Wu H, et al. The root canal bonding of chemical-cured total-etch resin cements. J Endod 2008;34:583–6.
23. Goracci C, Fabianelli A, Sadek FT, et al. The contribution of friction to the dislocationresistance of bonded fiber posts. J Endod 2005;31:608–12.
24. Faria-e-Silva AL, Reis AF, Martins LR. The effects of different luting procedures in thepush-out bond strength of fibre posts to the root canal. Braz J Oral Sci 2008;27:1653–6.
25. Chieffi N, Chersoni S, Papacchini F, et al. The effect of application sustained seatingpressure on adhesive luting procedure. Dent Mater 2007;23:159–6.
1546 Macedo et al.
26. Bonfante G, Kaizer OB, Pegoraro LF, et al. Tensile bond strength of glass fiber postsluted with different cements. Braz Oral Res 2007;21:159–64.
27. Amaral M, Santini MF, Wandscher V, et al. An in vitro comparison of differentcementation strategies on the pull-out strength of a glass fiber post. Oper Dent2009;34:443–5.
28. De Munck J, Vargas M, Van Landuyt K, et al. Bonding of an auto-adhesive lutingmaterial to enamel and dentin. Dent Mater 2004;20:963–71.
29. Gerth HU, Dammaschke T, Zuchner H, et al. Chemical analysis and bonding reactionof RelyX Unicem and Bifix composites—a comparative study. Dent Mater 2006;22:934–41.
30. Dauvillier BS, Feilzer AJ, De Gee AJ, et al. Visco-elastic parameters of dental restor-ative materials during setting. J Dent Res 2000;79:818–23.
31. Tay FR, Loushine RJ, Lambrechts P, et al. Geometric factors affecting dentin bondingin root canals: a theoretical modeling approach. J Endod 2005;31:584–9.
32. Arrais CA, Giannini M, Rueggeberg FA. Effect of sodium sulfinate salts on the poly-merization characteristics of dual-cured resin cement systems exposed to attenuatedlight-activation. J Dent 2009;37:219–27.
33. Faria-e-Silva AL, Moraes RR, Ogliari FA, et al. The role of the primer. J Oral Sci 2009;51:255–9.
34. Braga RR, Boaro LC, Kuroe T, et al. Influence of cavity dimensions and their deri-vates (volume and ‘C’ factor) on shrinkage stress development and microleakage ofcomposite restorations. Dent Mater 2006;22:818–23.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
Comparative Evaluation of Modified Canal Staining andClearing Technique, Cone-Beam Computed Tomography,Peripheral Quantitative Computed Tomography, SpiralComputed Tomography, and Plain and ContrastMedium–enhanced Digital Radiography in Studying RootCanal MorphologyPrasanna Neelakantan, MDS, Chandana Subbarao, BDS, and Chandragiri V. Subbarao, MDS
Abstract
Introduction: This study investigated the accuracy ofcone-beam computed tomography (CBCT), peripheralquantitative computed tomography (pQCT), spiralcomputed tomography (SCT), plain (plain digi), andcontrast medium–enhanced digital radiographs(contrast digi) in studying root canal morphology.Methods: The root canal anatomy was analyzed in 95teeth using CBCT, pQCT, SCT, plain digi, and contrastdigi. After flushing out the radiopaque dye, access cavi-ties were sealed, and the teeth were subject to the modi-fied canal staining and clearing technique. The numberof root canals (Vertucci classification and Gulabivala’sadditional classes) was calculated by three calibratedendodontists and two maxillofacial radiologists. Erro-neous or unsuccessful identifications of root canalswere statistically analyzed by one-way analysis of vari-ance (p = 0.05). Results: The modified canal stainingand clearing technique identified an average of 1.8root canals per mandibular central incisor, 2.3 per maxil-lary first premolar, 3.9 per maxillary first molar, 3.8 permaxillary and mandibular second molar, and 4.3 permandibular first molar. CBCT and pQCT were erroneousin 0.29% and 2.05% cases, whereas SCT, contrast digi,and plain digi were unsuccessful in 15.58%, 14.7%, and23.8%, respectively. There was a significant differencebetween all the methods (p < 0.05) in the unsuccessfulidentification of root canals except between CBCT andmodified canal staining and clearing technique wherethere was no significant difference (p > 0.05). Conclu-sions: CBCT and pQCT were as accurate as the modifiedcanal staining and tooth clearing technique in identi-fying root canal systems. (J Endod 2010;36:1547–1551)From the Department of Conservative Dentistry and EndodonticAddress requests for reprints to Dr Neelakantan Prasanna, Plot 1
yahoo.com.0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.008
JOE — Volume 36, Number 9, September 2010
Key WordsCone-beam computed tomography, contrast media, digital radiograph, modified stain-ing and clearing, morphology, peripheral quantitative computed tomography, rootcanal, spiral computed tomography
Successful endodontic therapy stems from thorough canal debridement and effectivefilling of the root canal system, for which knowledge of morphology of the root canals
is a critical prerequisite (1). Internal complexities of the root canal are genetically deter-mined and have definitive importance in anthropology (2). These factors necessitate theidentification of a method that accurately determines the root canal morphology.
There are numerous reports on the root canal morphologies of different popula-tions, which is extremely important for an endodontist as well as general dental prac-titioners. Also of interest to us are the methods that have been used in these studies (3).The methods most commonly used in analyzing the root canal morphology are canalstaining and tooth clearing (4–6), conventional radiographs (7–9), digital andcontrast medium–enhanced radiographic techniques (10, 11), radiographicassessment enhanced with contrast media (12, 13), and more recently computedtomographic techniques (14–16). Canal staining and tooth clearing (CS) isgenerally considered the gold standard in these studies (4, 5, 17). A modification ofthis technique proposed by Weng et al (18) is accurate, allows the appreciation of intri-cate details, and is nondestructive. An ideal technique would be one that is accurate,simple, non-destructive, and, most importantly, feasible in the in vivo scenario. Thegold standard methods CS and the modified method cannot be used in vivo.
The application of computed tomography (CT) scans in endodontics was first re-ported by Tachibana and Matsumoto in 1990 (19). A CT scan uses a fan-shaped beamand multiple exposures around an object to reveal the internal architecture of thisobject, thereby helping the clinician to view morphologic features as well as pathologyfrom different three-dimensional (3D) perspectives. The distinct advantage of a CT scanis that it allows for 3D reconstruction of root canal systems. CT scanning has been sug-gested as the preferential imaging modality in difficult situations demanding localizationand description of root canal systems because of its ability to render 3D information(20–22)
s, Saveetha Dental College and Hospitals, Saveetha University, Chennai, India.500, 16th Main Road, Anna Nagar West, Chennai, Tamil Nadu, India. E-mail address: prasu_endo@
Comparative Evaluation of Various Imaging Techniques in Studying Root Canal Morphology 1547

Figure 1. Classification of canal configurations according to Vertucci.
Basic Research—Technology
Cone-beam computed tomography (CBCT) scanning or digitalvolume tomography (DVT) uses an extraoral imaging scanner toproduce 3D scans of the maxillofacial skeleton at a considerably lowerradiation dose than conventional CT scanning. CBCT scanning hasbeen shown to be more accurate than digital radiographs in deter-mining root canal systems. CBCT scanning has also been usedin vivo in diagnosis and preoperative assessment (20, 23–26).Another computed tomography technique, peripheral quantitativecomputed tomography (pQCT), was originally introduced for bonemineral analysis. The only report on pQCT in studying root canalanatomy showed that this method offers accurate 3D reconstructionof the root canal systems (RCS) and analysis of endodonticprocedures (16). The planar resolution of pQCT is approximately70 � 70 mm, which is lower than mCT. Nevertheless, it might proveto be a nondestructive method of investigation at low cost and shorterscanning times. Spiral CT (SCT) has been used in several cases of diag-nosis of aberrant root canal systems (27–32) as well as in theidentification of the root canal morphology of Indian molars (33).
Despite a plethora of studies and clinical reports showing the canalmorphology of different populations, the most accurate and idealmethod is yet to be ascertained with scientific evidence. The hypothesistested in this study was that there is a difference in the identification ofthe number of root canal systems between the modified canal stainingand clearing technique (gold standard) versus CBCT, pQCT, SCT,contrast medium–enhanced digital radiographs, and plain digital radio-graphs. The aim of this in vitro investigation was to compare the efficacyof the six aforementioned methods in identifying root canal systems.
Materials and MethodsA total of 95 recently extracted teeth (20 mandibular first molars,
20 maxillary first molars, 20 mandibular second molars, 20 maxillarysecond molars, 7 maxillary first premolars, and 8 mandibular centralincisors) with intact roots and mature apices were collected from theOral Surgery Department of the University and stored at 100% humidity.It was ensured that for every tooth type, the number of roots was stan-dardized (mandibular incisors, 1; maxillary first premolars, 2; maxil-lary first and second molars, 3; and mandibular first and secondmolars, 2). The methodology was approved by the Institutional Review
Figure 2. Additional classes of canal configurations according to Gulabivala.
1548 Neelakantan et al.
Board of the university. The teeth were washed under tap water imme-diately after extraction and stored in distilled water with thymol iodidecrystals until the collection was complete. After this, the samples werewashed thoroughly under tap water and immersed in 2.5% sodiumhypochlorite for 30 minutes to remove adherent soft tissue.
CT ScansThe teeth were randomly inserted into foam arches in close contact
to each other to simulate their natural alignment in a dental arch. Anacrylic facing was placed on the facial side to mimic soft tissue on theradiographs. All the teeth were scanned by a CBCT scanner (3DAccui-tomo; J Morita Corporation, Osaka, Japan), a pQCT scanner (ResearchSA+; Stratec Medizin-technik GmbH, Pforzheim, Germany), and a SCTscanner (GE Electricals, Milwaukee, WI) with constant thicknesses of125 m/slice, 250m/slice, and 650m/slice respectively. The teeth wereviewed both cross-sectionally and longitudinally. Volume-renderingand multiplanar volume reconstruction were performed using theAdvantage Windows workstation (GE Systems, Milwaukee, WI).
Digital Radiography with Contrast MediumFollowing the scanning procedure, all the teeth were exposed to
a radiograph using a digital radiography unit (DSX 730; Owandy DentalImaging, France; and Kodak 2100 X ray unit; Kodak Dental Systems, At-lanta, GA). Access cavities were prepared in all the teeth. After gainingentry into the pulp chamber, the pulp tissue was extirpated with a finebarbed broach (Denstply Maillefer, Ballaigues, Switzerland). The teethwere placed in 5% sodium hypochlorite for 30 minutes to dissolve thepulp tissue (10), washed in water, dried, and a water-soluble low-viscosity radiopaque medium (diatrizoate sodium, Hypaque; AmershamHealth Inc, Princeton, NJ) was delivered into the root canals witha monoject syringe with a needle gauge 23 to 27 depending on the teethand root canal size. The teeth were subjected to vacuum for 2 minutes(24 mm Hg), and a reapplication of vacuum was performed after 3minutes. The penetration of the dye into the niches of the root canalsystem was enhanced by ultrasonication for 2 minutes. The teethwere placed in a model simulating the maxillary or mandibular arches,and radiographs were taken in the buccolingual direction using a digitalradiography unit (DSX 730 and Kodak 2100). All radiographs (before
JOE — Volume 36, Number 9, September 2010

TABLE 1. Average Number of Root Canals Identified with the Six Methods
ToothConventionalradiographs CBCT pQCT SCT
Digital radiograph withcontrast medium
Modified canalclearing and staining
Mandibular central incisor (n = 8) 1 1.8 1.8 1.8 1.8 1.8Maxillary first premolar (n = 7) 2 2.3 2.1 2.1 2 2.3Maxillary first molar (n = 20) 3.1 3.8 3.8 3.3 3.2 3.9Maxillary second molar (n = 20) 3.1 3.8 3.7 2.7 3.5 3.8Mandibular first molar (n = 20) 2.8 4.3 4.2 3.4 3.1 4.3Mandibular second molar (n = 20) 2.8 3.8 3.3 2.9 2.7 3.8
CBCT, cone-beam computed tomography; pQCT, peripheral quantitative computed tomography; SCT, spiral computed tomography.
Basic Research—Technology
and after introducing contrast medium) were taken in two horizontalangulations: 0� and 30�.
Modified Canal Staining and Clearing TechniqueThe contrast medium was flushed out with water followed by
5.25% sodium hypochlorite and then rinsed again with water. Theaccess cavities were sealed with light cure composite resin and lightcured for 40 seconds. The modified method of canal staining hasbeen described in detail elsewhere (18). Briefly, after immersion ofthe teeth in India ink, the teeth were placed in a hyperbaric oxygenchamber set to a pressure of 0.6 MPa for 2 hours. The method of decal-cification and rendering the teeth transparent was adopted from Rob-ertson et al (34). After 12 hours of drying, the teeth were decalcifiedin 10% nitric acid for 28 to 30 hours. The acid was changed after 24hours and was stirred every 8 hours. The endpoint of decalcificationwas determined by taking periodic radiographs of five sample teeth.After thorough washing of the decalcified teeth in running tap waterfor 4 hours, the samples were dehydrated in ascending concentrationsof ethanol (70%, 80%, 95%, and 100%) for 1 day, and the sampleswere rendered transparent by immersing in methyl salicylate for 2days. The samples were analyzed using a magnifying lens (3�).
For all the methods, the evaluation was performed by three preca-librated and standardized endodontists and two oral and maxillofacialradiologists. To eliminate any bias, the evaluators were asked to analyzeevery slice (both cross-sectional and longitudinal) as well as the imagesobtained by multiplanar volume reconstruction to quantify the numberof root canals. The number of root canals per tooth identified withmodified canal staining and clearing technique was used as the goldstandard to compare the number of root canals identified with CBCT,pQCT, SCT, contrast medium–enhanced digital radiographs, and digitalradiography. The identification of root canal systems was done accord-ing to Vertucci’s classification (4) and Gulabivala’s additional classes(17) (Figs. 1 and 2). The total number of root canals was calculatedfor each tooth studied. In any canal system with divisions of the canal,the maximum number of divisions was considered as the number ofcanals. For example, type II canal system was considered as two canals,type 1-3-1 as three canals, and type VI as two canals.
The average number of root canals identified per tooth type wascalculated for all the methods. Descriptive statistical analysis was per-
TABLE 2. Correct Identification of the Total Number of Root Canals by All the Me
EvaluatorDigital radiograph
(% correct)CMDR
(% correct) (%
Endodontist 1 80 88Endodontist 2 83 86Endodontist 3 82 89Radiologist 1 80 88Radiologist 2 80 87All 82 84
CMDR, contrast medium–enhanced digital radiography; CBCT, cone-beam computed tomography; pQCT, pe
staining.
JOE — Volume 36, Number 9, September 2010 Comparative Eva
formed by calculating the percentage of root canals found from themodified canal staining and clearing method with those identifiedwith CBCT, pQCT, SCT, contrast medium–enhanced digital radiographs,and digital radiographic images. Interrater agreement was measuredbetween all three endodontist evaluators and two radiologists as wellas between each pair of endodontist evaluators and the radiologists. In-trarater agreement was measured by having all three endodontists andthe two radiologists evaluate one half of the CBCT, pQCT, SCT, contrastmedium–enhanced digital radiographs, and digital radiographicimages at each of two separate sessions. The percentage of unsuccessfulidentifications as compared with the modified canal staining andclearing method (0% unsuccessful) was statistically analyzed by one-way analysis of variance with a p value of 0.05 considered significant.
ResultsThe average number of root canals identified by all the methods is
depicted in Table 1. The percentage of root canals found from the modi-fied canal staining and clearing analysis with those identified with CBCT,pQCT, SCT, contrast medium–enhanced digital radiographs, and digitalradiographic images is given in Table 2. Table 3 presents the percentageof unsuccessful identification of root canals by all the methods analyzedin this study.
Interrater and Intrarater AgreementFor the modified canal staining and clearing method, each pair of
endodontist evaluators agreed with each other 100% of the time. ForCBCT and pQCT, each pair of endodontist evaluators and radiologistsagreed with each other between 98% and 100% of the time, whereasfor SCT they agreed with each other 95% to 98% of the time. For digitalradiography and contrast medium–enhanced digital radiographs, eachpair of endodontists agreed with each other 80% to 83% and 86% to89% of the time. Among all three endodontist evaluators and two radi-ologist evaluators, total agreement was found 100% of the time for themodified canal staining and clearing method, 99% for CBCT and pQCT,98% for SCT, and 82% for digital radiography and 84% for contrastmedium–enhanced digital radiographs.
Intrarater agreement results showed that the endodontist evalua-tors agreed with themselves 100% of the time for the modified canal
thods
CBCTcorrect)
pQCT(% correct)
SCT(% correct)
MCS(% correct)
99 100 98 100100 98 96 10099 98 95 10098 99 98 100
100 99 96 10099 99 98 100
ripheral quantitative computed tomography; SCT, spiral computed tomography; MCS, modified canal
luation of Various Imaging Techniques in Studying Root Canal Morphology 1549

TABLE 3. Unsuccessful Identification of Root Canals in Individual Teeth in Allthe Techniques Compared with the Modified Canal Staining and ClearingTechnique
Method
Missed oneRCS in a
tooth (%)
Missed two ormore RCS
in a tooth (%) Total (%)
Digital radiograph 0 23.8 23.8CMDR 0 14.7 14.7SCT 0.58 15 15.58CBCT 0.29 0 0.29pQCT 0.88 1.17 2.05
CMDR, contrast medium–enhanced digital radiography; CBCT, cone-beam computed tomography;
pQCT, peripheral quantitative computed tomography; SCT, spiral computed tomography; RCS,
root canal staining.
Basic Research—Technology
staining and clearing technique interpretation; 98% for CBCT, pQCT,and SCT; between 78% and 84% for digital radiographs; and 85% to93% for contrast medium–enhanced digital radiograph interpretation.The evaluators failed to identify one or more root canals with digitalradiographs in 23.8% of teeth, contrast medium–enhanced digitalradiographs in 14.8%, SCT in 15.58%, CBCT in 0.29%, and pQCT in2.05% of the teeth. There was a significant difference between all themethods (p < 0.05) in unsuccessful identification of root canals.
DiscussionFailure to identify extra canals is implicated as one of the most
common reasons for the failure of endodontic treatment (1). The anal-ysis of the root canal morphologies of teeth of different populations,ethnicities, and preoperative assessment of root canal systems is ofimportance in this regard. This study compared the efficacy of the sixmethods (modified canal staining and clearing, CBCT, pQCT, SCT,digital radiography, and contrast medium–enhanced digital radiog-raphy) in identifying root canal systems. In the absence of overlyingbone, tissue, and anatomic features, it may not be possible to directlyextrapolate the results of this in vitro investigation to the clinicalscenario.
The canal staining and clearing technique is considered the goldstandard method of studying root canal anatomy. We used the modifiedcanal staining and clearing technique in this study. Although nonde-structive and more accurate than the conventional staining and clearingmethod, the main disadvantage of this method is that it cannot be usedin vivo (18). A method that has the accuracy of the canal staining andclearing technique and yet is clinically feasible is essential in endodonticpractice.
Radiographs taken after the introduction of radiopaque contrastmedia are more useful than plain radiographs in the assessment ofroot canal anatomy (12). Hypaque is a tensioactive, water-solublecontrast medium with a specific gravity similar to sodium hypochlorite.It is an aqueous solution of two iodine salts: sodium iodine and diatri-zoate meglumine. The low surface tension enables its penetration intothe niches of the root canal system (12). This alteration of subjectcontrast induced by variations in transmission of the radiographicbeam between the tooth and the contrast medium definitely improvesthe visibility of canal systems in comparison with conventional radio-graphs. Digital radiographs were used in this study because they aremore accurate than conventional radiographs in analyzing root canalanatomy (10).
Exposing radiographs in two different horizontal angulations (30�
shift and orthoradial position) provide additional information on rootcanal systems but show some amount of inherent distortion, whichmakes radiographic determination of some characteristics difficult.Our study showed that endodontists and radiologists only identified
1550 Neelakantan et al.
86% to 89% of root canals as compared with the modified canal stainingand clearing method. Passive injection of the contrast medium results inthe entrapment of air bubbles, hampering proper visualization of apicalanatomy (10, 12, 35). Despite the injection of contrast media underpressure in our study, it is possible that complete perfusion may notoccur (35). This is probably the reason why this method failed to iden-tify the intricacies of root canal anatomy. The clearing and staining tech-nique has been shown to be more accurate than the radiographictechnique with contrast medium (35). Our results are in agreement.
CT scanning is currently widely used in implantology, maxillofacialreconstruction, and endodontic diagnosis as well as for the assessmentof canal preparation, obturation, and the removal of root fillings (20,23, 27, 28). The main advantages of CT scanning are that it isnondestructive and allows 3D reconstruction and visualization of theexternal and internal anatomy of the teeth.
The results of our study showed that CBCT scanning was as accu-rate as the modified canal staining and clearing technique in identifyingcanal anatomy. CBCT scanning was erroneous only in 0.29% of the teethexamined. The differences between the results obtained by the evalua-tors were not significantly different when endodontists were comparedwith radiologists. However, in some instances of analysis of the CTimages, radiologists were able to interpret the number of root canalsbetter than endodontist evaluators, but this was not true for allendodontist evaluators. Nevertheless, the experience of the radiologistsin the analysis of CT images may be an attributable factor. Theendodontic evaluators and radiologists identified 98% to 100% ofroot canals as compared with modified canal staining and clearingmethod when CBCT and pQCT were used. The slice thickness forCBCT ranges from 80 to 200 m. The slice thickness used in our studywas 125 m. The primary advantages of CBCT are significantly lowereffective radiation dose, short exposure time (2-5 seconds), less expen-sive than conventional CT scanning, and highly accurate. Also, CBCTmeasurements are geometrically accurate because of the fact that theCBCT voxels (3D pixels containing data) are isotropic (20, 26).pQCT, with a slice thickness of 250 m failed to identify 2.05% of RCSas compared with the gold standard. Also, the large pixel size asmentioned earlier is responsible for a low resolution, which maycause errors in the identification of intricate details of the root canalsystem. The advantages of pQCT are that it is economic, scanningtimes are shorter, and it allows mapping of multiple teeth at the sametime (16). Our study showed that SCT did not identify 15.58% of rootcanals. The frequent errors were in differentiating type II canal systemsfrom type III and 1-3-1 systems and in differentiating type IV canalsystems from type 3-2. We attribute this to the slice thickness. The usualthickness of each slice in SCT ranges from 0.65 mm to 1.0 mm (33). Inour study, it was 0.65 mm/slice. It is possible that this slice thicknessdoes not offer sufficient reproducibility along the length of the canal(14). For example, type VI canal system may be misinterpreted asa type IV system if the fusion and subsequent division of the canals iscovered in the same slice. Another main disadvantage of SCT is theincreased radiation dose as compared with CBCT scanning (20).
ConclusionsCBCT and pQCT are as accurate as the gold standard (modified
canal staining and clearing technique) in identifying root canalanatomy. The application of 3D reconstruction based on CBCT andpQCT require further evaluation to validate its clinical application.
References1. Grossman IL, Oliet S, Del Rio E. Endodontic Practice. 11th ed. Philadelphia, PA: Lea
and Fabringer; 1988:145–51.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
2. Sperber GH. The phylogeny and odontogeny of dental morphology. In: Sperber GH,ed. From Apes to Angels. New York, NY: Wiley-Liss; 1990:215–9.3. Cleghorn BM, Christie WH, Dong CC. Root and root canal morphology of the human
permanent maxillary first molar: a literature review. J Endod 2006;32:813–21.4. Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc
1978;97:47–50.5. Alavi AM, Opasanon A, Ng YL, et al. Root and canal morphology of Thai maxillary
molars. Int Endod J 2002;35:478–85.6. Awawdeh L, Abdullah H, Al-Qudah A. Root form and canal morphology of Jordanian
maxillary first premolars. J Endod 2008;34:956–61.7. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of
7275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101–10.8. Weine FS, Hayami S, Hata G, et al. Canal configuration of the mesiobuccal root of the
maxillary first molar of a Japanese sub-population. Int Endod J 1999;32:79–87.9. Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the me-
siobuccal and distal roots of permanent first molars in a Kuwait population—a clin-ical study. Int Endod J 2008;41:755–62.
10. Fan B, Gao Y, FanW, et al. Identification of a C-shaped canal system in mandibularsecond molars. Part II. The effect of bone image superimposition and intraradicularcontrast medium on radiograph interpretation. J Endod 2008;34:160–5.
11. Patel S, Dawood A, Whaites E, et al. New dimensions in endodontic imaging: part 1.Conventional and alternative radiographic systems. Int Endod J 2009;42:447–62.
12. Naoum HJ, Love RM, Chandler NP, et al. Effect of X-ray beam angulation and intra-radicular contrast medium on radiographic interpretation of lower first molar rootcanal anatomy. Int Endod J 2003;36:12–9.
13. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent firstmolar teeth ate various ages. Int Endod J 1993;26:257–67.
14. Plotino G, Grande NM, Pecci R, et al. Three dimensional imaging using micrcom-puted tomography for studying tooth macromorphology. J Am Dent Assoc 2006;137:1555–61.
15. Fan B, Yang J, Gutmann JL, et al. Root canal systems in mandibular first premolars withC-shaped root configurations. Part I: Microcomputer tomography mapping of theradicular groove and associated root canal cross-sections. J Endod 2008;34:1337–41.
16. Sberna MT, Rizzo G, Zacchi E, et al. A preliminary study of the use of peripheralquantitative computed tomography for investigating root canal anatomy. Int EndodJ 2009;42:66–75.
17. Gulabivala K, Aung TH, Alavi A, et al. Root and canal morphology of Burmesemandibular molars. Int Endod J 2001;34:359–70.
18. Weng XL, Yu SB, Zhao SL, et al. Root canal morphology of permanent maxillary teethin the Han nationality in Chinese Guanzhong area: a new modified root canal stain-ing technique. J Endod 2009;35:651–6.
19. Tachibana H, Matsumoto K. Applicability of x-ray computerized tomography inendodontics. Endod Dent Traumatol 1990;6:16–20.
20. Patel S, Horner K. The use of cone beam computed tomography in endodontics. IntEndod J 2009;42:755–6.
JOE — Volume 36, Number 9, September 2010 Comparative Eva
21. La SH, Jung DH, Kim EC, et al. Identification of independent middle mesial canal inmandibular first molar using cone-beam computed tomography imaging. J Endod2010;36:542–5.
22. Bornstein MM, Wolner-Hanssen AB, Sendi P, et al. Comparison of intraoral radiog-raphy and limited cone beam computed tomography for the assessment of root-fractured permanent teeth. Dent Traumatol 2009;25:571–7.
23. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod2007;33:1–6.
24. Peters OA, Laib A, Ruegsegger P, et al. Three-dimensional analysis of root canalgeometry using high-resolution computed tomography. J Dent Res 2000;79:1405–9.
25. Mozzo P, Procacci C, Tacconi A, et al. A new volumetric CT machine for dentalimaging based on the cone-beam technique: preliminary results. Eur Radiol1998;8:1558–64.
26. Matherne RP, Angelopoulos C, Kulilid JC, et al. Use of cone-beam computed tomog-raphy to identify root canal systems in vitro. J Endod 2008;34:87–9.
27. Gopikrishna V, Reuben J, Kandaswamy D. Endodontic management of a maxillaryfirst molar with two palatal roots and a single fused buccal root diagnosed withspiral computed tomography—a case report. Oral Surg Oral Med Oral PatholOral Radiol Endod 2008;105:e74–8.
28. Sachdeva GS, Ballal S, Gopikrishna V, et al. Endodontic management of a mandibularsecond premolar with four roots and four root canals with the aid of spiralcomputed tomography: a case report. J Endod 2008;34:104–7.
29. Aggarwal V, Singla M, Logani A, et al. Endodontic management of a maxillary firstmolar with two palatal canals with the aid of spiral computed tomography: a casereport. J Endod 2009;35:137–9.
30. Chandra SS, Rajasekaran M, Shankar P, et al. Endodontic management of a mandib-ular first molar with three distal canals confirmed with the aid of spiral computer-ized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2009;108:e77–81.
31. Ma L, Chen J, Wang H. Root canal treatment in an unusual maxillary first molardiagnosed with the aid of spiral computerized tomography and in vitro sectioning:a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:e68–73.
32. Rani AK, Metgud S, Yakub SS, et al. Endodontic and esthetic management of maxil-lary lateral incisor fused to a supernumerary tooth associated with a talon cusp byusing spiral computed tomography as a diagnostic aid: a case report. J Endod 2010;36:345–9.
33. Reuben J, Velmurugan N, Kandaswamy D. The evaluation of root canal morphologyof the mandibular first molar in an Indian population using spiral computed tomog-raphy scan: an in vitro study. J Endod 2008;34:212–5.
34. Robertson D, Leeb IJ, McKee M, et al. A clearing technique for the study of root canalsystems. J Endod 1980;6:421–4.
35. Bedford JM, Martin DM, Youngson CC. Assessment of a contrast medium as anadjunct to endodontic radiography. Int Endod J 2004;37:806–13.
luation of Various Imaging Techniques in Studying Root Canal Morphology 1551

Basic Research—Technology
Design Improvement and Failure Reduction of EndodonticFiles through Finite Element Analysis: Application to V-TaperFile DesignsRui He, PhD,* and Jun Ni, PhD
†
Abstract
Introduction: Torsional stiffness and bending flexibilityare essential characteristics as far as the performanceand safety of the endodontic files are concerned. Inade-quacy in addressing these requirements in file designleads to increased risk of file failure. The stiffness andflexibility of the endodontic file are greatly dependenton its geometric design. The aim of this study was toevaluate the influence of geometric features on themechanical performance of endodontic files throughnumerical simulations. Methods: Finite element modelsof V-Taper file were developed, and the mechanicalbehavior of the file under bending and torsional loadswas simulated. The influence of helix angle, taper, andflute length was evaluated through parametric studies.Results: In the helix angle range between 5 and 40degrees, the bending flexibility and torsional stiffnessboth improve with increasing helix angle. The torsionalstiffness increases with increasing taper or decreasingflute length, accompanied by a decrease in bending flex-ibility. Changing the flute length alone does not result ina change in the stress profile in the tip section. Theelastic limit of V-Taper file tip section was estimatedin the form of transverse deflection and angular defor-mation in bending and in torsion, respectively. Conclu-sions: The influence of helix angle, taper, and flute lengthon the bending flexibility and torsional stiffness of V-Taperfiles was quantitatively assessed through parametricstudies with finite element method. The elastic limit ofthe V-Taper file tip section was estimated. A design meth-odology for achieving improved mechanical performanceswas proposed. (J Endod 2010;36:1552–1557)Key WordsBending flexibility, elastic limit, endodontic file design,failure reduction, finite element method, helix angle,taper, torsional stiffness
From *Research and Development, Boston Scientific Corpo-ration, St Paul, Minnesota; and †Department of MechanicalEngineering, University of Michigan, Ann Arbor, Michigan.
Address requests for reprints to Dr Rui He, Boston ScientificCorporation, Research and Development, 4100 Hamline Ave N,St Paul, MN 55112-5798. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.All rights reserved.doi:10.1016/j.joen.2010.06.002
1552 He and Ni
In recent decades nickel-titanium (NiTi) rotary files have gained increasing popularityover stainless steel files in root canal preparation. Mainly due to the superelastic
behavior of its base material of nitinol, NiTi files are more flexible than stainless steelfiles (1, 2) and better preserve the canal anatomy with less canal aberrations such aszips, ledges, apical foramen transportation, or perforations (3–5). Despite theseadvantages, however, fracture of NiTi files remains a concern in clinical practices(6, 7). A recent questionnaire survey revealed that a significant population ofgeneral dental practitioners and endodontists have encountered endodontic filefractures (8).
An endodontic file faces 2 obvious challenges in canal instrumentation. It firstneeds to be strong to facilitate effective cutting of the dentin material for canal shapingpurposes. Adequate torsional strength is necessary to maintain the cutter geometry andedge strength of the file, preventing torsional damage. A file also needs to be flexible inbending to follow the canal anatomy during instrumentation with good centering ability(9), and to minimize the aberrations to the canal. In addition, adequate flexibility helpslower the bending stresses and reduce the risk of flexural fatigue failure (10).
Both torsional stiffness and bending flexibility are essential characteristics for fileperformance and safety concerns. Inadequacy in addressing these performancerequirements in file design leads to increased risk of file failure. Studies suggestedthat flexural failure and torsional failure are the 2 major failure modes for rotaryNiTi files (6, 7, 11–13). Numerous studies also showed that the stiffness andflexibility of endodontic files are greatly dependent on their geometric design,including taper, helix angle, cross-section shape, tip size, and length, etc. (14–20).
The mechanical performance of endodontic files can be evaluated through labtesting or numerical simulation. Numerical simulation is a low cost alternative to labtesting. The numerical simulation method is often more convenient than lab testingwhen it comes to studying ‘‘what-if’’ scenarios. Numerical modeling has been increas-ingly used to study the mechanical behavior of the endodontic file in the past decade.With a boundary integral method, Turpin et al (16) calculated the stresses on files inbending and in torsion and found that the cross-section shape has a marked influenceon the stress profile. With a finite element model, Berutti et al (17) evaluated thebending and torsional behavior of NiTi files and found that a file with concave crosssection is more flexible in bending but less stiff in torsion compared to one with a convexcross section. Xu et al (14) studied the influence of cross-sectional profile on torsionaland flexural behavior of NiTi files and found that the peak torsional stress decreaseswith increasing inner core diameter. Kim et al (21) created full-length models of 3commercial NiTi files and calculated stress distribution and force responses in simu-lated canal shaping and residual stresses after unloading. Necchi et al (22) simulatedthe insertion and withdrawal of a commercial file against a rigid root canal and obtaineda strain map of the file. They also investigated the influence of file material and root canalgeometry on the strain profile. Their work was extended in another study (23) toinclude the effect of several NiTi material variants on the strain profile. Kim et al(24) and Kim et al (25) studied the effect of cross-section shape on the stress profileduring simulated bending, torsion, and canal shaping by using full-length numericalmodel of commercial files.
It should be pointed out that numerical simulation has its own limitations. Forexample, a model that contains only the gross geometry of an endodontic file might
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
not allow for the study of the effects of material imperfection ormanufacturing defects present in physical instruments (26).Material and MethodsIn this work numerical models were developed to study the influ-
ence of geometric features on the mechanical behavior of endodonticfiles. The numerical models discussed throughout the scope of thiswork were constructed using the cross-sectional profile of a V-Taperfile (Guidance Endo, Albuquerque, NM). A non-linear stress-straincurve of nitinol presented in the literature (17) was used in this studyto approximate the mechanical behavior of the base material. This mate-rial model describes the behavior of nitinol in 3 distinct phases,including an initial linear elastic phase, a superelastic plateau phase,and a final strain-hardening phase.
While studying the effect of the helix angle (angle between thetangent of the helical cutting edge and the longitudinal axis of thefile), a set of 8 file models was created. The helix angle was fixed oneach model but increased evenly from 5 to 40 degrees across modelsby increment of 5 degrees. All models have the same length of 1.8mm and the same taper of zero degree. A short length was chosen tolower the computational cost. All models share a common taper to avoidpossible variation in results caused by a change in taper. The diameter ofthe cross section is 0.40 mm, coincident to that of an ISO size 40 tip. Toverify the generality of results from fixed-helix models, a file with varyinghelix angle and zero taper was also included in this study. The helix angleon this file increases from 9 degrees at the tip to 20 degrees at the shankend, matching the measured helix profile of a V-Taper file.
While studying the effect of taper, 2 file models were created, withzero taper on one model and a 0.06 taper on the other. The helix angleon both models increases from 9 degrees at the tip end to 20 degrees atthe shank end. Both models have the same length of 1.8 mm.
While evaluating the impact of flute length, 8 models were created,with file length increasing evenly from 6 to 20 mm across models byincrements of 2 mm. All models have a size 40 tip, a 0.02 taper, andan identical helix profile that increases from the tip to the shank. Thehelix angle at the tip is 10 degrees. The helix angle at the shank varieswith the model length, from 16 degrees on the 6-mm length model to 30degrees on the 20-mm length model.
A cantilever beam boundary condition was applied to all filemodels. The models were constrained on all translational and rotationaldegrees of freedom at the shank end and were loaded at the tip end.
ResultsEffect of the Helix Angle
A bending moment of 0.7 N�mm was applied to the tip end of thefile on 8 models of fixed helix angles. As the helix angle increases from 5degrees to 40 degrees across the models, the simulated tip deflectionincreases continuously from 2.52 to 3.55 mm (Fig. 1a). Similar resultswere observed when a transverse load of 0.4 N was applied to the tip.Interestingly, the tip deflection on the model with helix varying from9–20 degrees (2.66 mm) falls in between those observed on the 5-degree helix model (2.52 mm) and on the 20-degree helix model(2.79 mm). This result suggested that the bending flexibility of thefile increases with increasing helix angle (or decreasing pitch).
Torsional behavior was also simulated on the same set of models.When subjected to a 0.4 N�mm torque, the angular deformation at thetip end decreases continuously with increasing helix angle, from 97degrees on the 5-degree helix model to 36 degrees on the 40-degreehelix model (Fig. 1b). When the same torque was applied to the modelwith helix varying from 9–20 degrees, its angular deformation (94degrees) falls in between those observed on the 5-degree helix model
JOE — Volume 36, Number 9, September 2010 Design Improvement
and on the 20-degree helix model (61 degrees). This result indicatesthat the torsional stiffness of the file increases with increasing helixangle. This correlation between torsional stiffness and the helix anglewas also reported in the finite element studies on twist drills (27, 28).
The stress profiles on the files under bending and torsion werealso simulated. It was found that the helix angle greatly affects thebending stress distribution. Although a minimal stress zone is alwayslocated on the neutral plane, the location of peak stress varies withthe helix angle. To illustrate this point, Fig. 1c, d present the bendingstress profiles on the cross-sectional views of a 15-degree helix modeland a 35-degree helix model, respectively. The peak stress occurs righton the cutting edge on the 15-degree model but shifts to the base of theflute on the 35-degree model. Regardless of helix angle, however, thepeak stress is always located in the plane of bending. These observationsagree with the results reported in other studies (16, 17, 25). Due to thefact that the base is closer to the neutral plane than the edge is, the peakstress on the 35-degree helix is lower than that on the 15-degree helix.No correlation was observed between the peak bending stress and thehelix angle.
In contrast, a correlation was observed between peak stress andhelix angle under torsional deformation. The peak stress on the modelwas found to decrease continuously as the helix angle increases from 5degrees to 25 degrees across models when loaded with a 0.4 N�mmtorque. The peak torsional stress is consistently located at the base ofthe flute regardless of helix angle, an observation also reported in otherstudies (16, 17, 25). Fig. 1e, f show the torsional stress distribution onthe 15-degree and 35-degree helix models, respectively. Because of theconsistency in peak stress location across models, the peak stress valuecorrelates inversely with the torsional stiffness of the file. It is note-worthy that after the helix angle reaches 25 degrees, further increasein helix angle results in only minimal change in peak torsional stress.This is because at or above 25-degree helix angle, the stresses on themodel decrease to the nitinol superelasticity plateau, where a largechange in strain results in only minimal change in stress.
Effect of the TaperThe taper feature obviously adds more material to the file and
makes a stiffer file body, which affects both bending and torsionalbehavior of the file. When subjected to a 0.7 N�mm bending moment,the zero-taper model reported a tip deflection of 2.66 mm, compared toa 1.04-mm tip deflection on the 0.06-taper model. Similarly, when sub-jected to a 0.7 N�mm torque, the tip angular deformation drops from352 degrees on the zero-taper model to 122 degrees on the 0.06-tapermodel. These observations indicate that an increase in taper results inan increase in torsional rigidity but a decrease in bending flexibility.This result is in agreement with the reported testing results of a commer-cial endodontic file (19).
The taper also has a great impact on the stress profile. The taperfeature makes the shank stiffer than the tip and directs the higherstresses to the tip, a result also reported by Kim et al (24). In addition,an increase in taper adds more material to the overall body, leading toan increase in stiffness and decrease in stress. Under 0.7 N�mmloading, the peak stress in bending and in torsion drops by 19% and10% respectively as the taper increases from zero to 0.06.
Effect of the Flute LengthAn increase in the flute length adds slenderness to the file body,
resulting in decreased resistance to deformation. When a 3.0 N�mmbending moment was applied to the tip of a file with a size 40 tip anda 0.02 taper, the tip deflection increases continuously with increasingflute length, from 4.5 mm on the 6-mm-length model to 7.7 mm on
and Failure Reduction of Endodontic Files through Finite Element Analysis 1553

Figure 1. Simulated mechanical behavior of V-Taper endodontic files in bending and torsion. (This figure is available in color online at www.aae.org/joe/.)
Basic Research—Technology
the 20-mm-length model. This indicates that a file of longer flute lengthhas better bending flexibility.
The transverse deflection of the cutting edge along the file lengthwas plotted in Fig. 1g for 3 models of different length. This plot showsthat the deflection peaks at the tip and drops quickly within a few milli-meters of the tip, regardless of the file length. This quick drop of deflec-tion is mainly due to the effect of the taper. Moving toward the fixedshank end, the deflection approaches asymptotically to zero. Interest-ingly, despite the marked difference in their deflection profiles, modelsof different length have an identical stress profile in their common
1554 He and Ni
section as a result of the identical boundary condition on them(Fig. 1h). Fig. 1h also shows that the stress reaches its peak at a veryshort distance from the tip, where the helical cutting edge crosses thebending plane. The stress drops rapidly to the superelasticity stressplateau of nitinol within less than 3 mm from the tip.
The angular deformation and torsional stresses were also exam-ined for models of different length. Similar results were obtained asin the case of bending. Angular deformation increases with increasingflute length, indicating that the torsional stiffness of a file decreases withincreasing flute length.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
DiscussionImpact of Geometric Parameters
The taper feature introduces base material to the file body andincreases the stiffness of the file (15, 19, 20). A larger taper offersstronger resistance to torsional breakage and helps maintain thecutting edge strength and cutting efficacy. Apparently a large tapermakes the rotary file a bigger cutter and helps remove more dentinmaterial from the canal wall, but it also encounters a higher torqueduring preparation (29, 30). On the other hand, the taper makesa stiffer file, leading to higher risk of root canal straightening,abbreviation, or transportation during instrumentation (9, 15). Italso results in higher bending stresses and lower resistance toflexural fatigue failure (30). Therefore, a large taper file is appropriatewhen strong stiffness or high cutting efficacy is needed, such as duringinitial orifice enlargement (31) or while preparing the first half of theworking length using a crown-down technique (4). It can also be usedto address calcified but relatively straight canals. In contrast, a file withsmall taper is suitable for severely curved or S-shaped canals wheregreat flexibility is needed (32, 33). The disadvantage of using a smalltaper file is that it has a relatively poor capability of producinga taper-shaped canal (33).
The stiffness of a file decreases with increasing flute length.Although a longer file has superior bending flexibility, it provides lessresistance to twist deformation. Files of different flute length share anidentical stress profile in their common section, suggesting an equalpropensity for file damage. In a canal treatment, the selection of flutelength is obviously dependent on the canal anatomy and the instrumen-tation protocol. The simulation results showed that severe deformationand plastic stresses are concentrated within 3 mm of the tip regardlessof flute length, suggesting that file damage is most likely to occur in thetip section. This observation agrees with results from other studies (6,19, 34).
To date, studies on the helix angle and its influence on mechanicalstrength of endodontic files are very limited. Low et al (35) acknowl-edged that the spiral flute design adds complexity to the flexuralbehavior and developed a curve-fitting based model to include the effectof flute helix. Our work is probably one of the first studies that examinedthe helix angle in relation to the structural strength of endodontic files indetails. Our study suggested that the helix angle influences the mechan-ical strength of the file in a different way than other geometric param-eters do. As discussed earlier, an increase in bending flexibility is alwaysaccompanied by a decrease in torsional stiffness as the taper or the flutelength of a file changes, or vice versa. Other studies suggested that thegeometric feature of cross-sectional profile influences the mechanicalstrength of the file in a similar way as the taper or length factor does(16, 17). Our study showed that as the helix angle increases, the
Figure 2. Estimated elastic limit of V-Taper file tip section. (This figure is availab
JOE — Volume 36, Number 9, September 2010 Design Improvement
bending stiffness decreases, but the torsional stiffness increases. Inother words, the 2 seemingly competing characteristics of bendingflexibility and torsional stiffness can be simultaneously improved withincreasing helix angle. Files with large helix angle reportedly havelonger flex fatigue life than files with small helix angle (18), whichcan be largely credited to the high flexibility and low bending stressesassociated with large helix angle.
The favorable correlation between helix angle and mechanicalperformances could imply new alternatives for file selection in clinicalpractices. In situations where more flexibility is needed to negotiateseverely curved canals or more stiffness is needed to address highlycalcified canals, or a combination of both cases, endodontists canswitch to files of larger helix angle potentially to solve the problem. Ifthe endodontists have access to a variety of helix angles within thesame file family, it will make this solution even more attractive. Thisis because endodontists thus are able to keep their choice on otherfeatures of the file, such as cross-sectional shape, tip size, taper, length,which could be driven by personal experience or clinical protocols.
Safe Use of Endodontic FilesEmpowered by the superelasticity behavior of nitinol, NiTi
endodontic files can take fairly large deformation and stay in the elasticdeformation domain. However, severe loading will still deform thematerial plastically and expose the file to permanent damage. Theload at which plastic deformation develops is referred to as the elasticlimit of the file. If the load on the file is kept below the elastic limit of thefile during instrumentation, the risk of file failure can be greatly reduced(36).
With numerical simulations the elastic limit of a file can be readilyestimated. The numerical model allows for calculation of the peak stresson a file under specific loading conditions, thus a curve of peak stressversus load can be obtained. The load at the transition point from elasticstresses to plastic stresses on this curve is the elastic limit of the file.
As a simple example, the stress-load curves of a size 25, 0.04 taper,1.8-mm length V-taper tip section under pure bending and pure torsionas a cantilever beam were established (Fig. 2). The peak stress reachesthe yield point of nitinol (�530 MPa) when the file is bent under a 0.6N�mm bending moment, or when the tip deflection reaches 0.8 mm. Inthis case, the elastic limit of the file segment was depicted by either thebending moment or the tip deflection. Similarly, as the file is loaded intorsion, the elastic limit of the file was identified as 0.5 N�mm torque or80-degree twist of the tip. Following this approach, the elastic limit ofa full-length endodontic file under more complex loading conditionscan be determined.
The bending load applied to a file during the instrumentation islargely determined by the morphology of a root canal system (canal
le in color online at www.aae.org/joe/.)
and Failure Reduction of Endodontic Files through Finite Element Analysis 1555

Figure 3. Finite element analysis–assisted endodontic file design for mechan-ical performance. (This figure is available in color online at www.aae.org/joe/.)
Basic Research—Technology
angle, curvature, length, etc), which can be clinically determined, suchas through a preoperative radiographic study (37). The torsional loadduring instrumentation, which is dependent on the canal anatomy andthe cutter geometry of the rotary file, can be mathematically computedwith analytical models such as the one proposed by He (38). The clin-ical load that a file receives during instrumentation is then fully deter-mined. If the clinical load exceeds the elastic limit of the file, the file is atrisk of being damaged. Once such risk is identified, the same processcan be followed to select a file with an elastic limit greater than the clin-ical load. The risk of file damage in a canal treatment is then minimized.
Alternatively, the risk of file damage can be lowered by using thetorque-limiting feature on the handpiece. This feature allows the motorto automatically stop and then reverse the rotation once the preset tor-que is reached, thus protecting the endodontic file against excessivetorsional deformation (39). Setting the torque limit in a way suchthat the torsional load in combination with the expected bendingload is below the elastic limit of the file, the risk of developing file failureis reduced. It is worth noting, though, that the actual torque output oncertain models of torque-control motor was higher than the preset tor-que and the reported torque at fracture for several rotary files (40),which limits the effectiveness of using those motors for preventing filedamage.
It is also noteworthy that some studies suggested that as soon as theNiTi material enters the superelastic plateau where the stress-inducedphase transformation from austenite to martensite begins, the materialis subjected to an accelerated rate of crack propagation in low cyclefatigue (41, 42). To maximize the fatigue life of the endodontic file,the elastic limit should be redefined as the load at which the phasetransformation of NiTi material starts.
Finite Element Analysis–assisted Endodontic File DesignIn previous sections we evaluated the impact of geometric param-
eters on the mechanical behavior of endodontic files with finite elementmodels. We also estimated the elastic limit of the files under differentmodes of deformation. Integrating these 2 pieces of work together,we developed a methodology that provides a means to guide the filedesign process to achieve improved mechanical performances. As illus-trated in Fig. 3, the design process starts by specifying the radial andlongitudinal dimensions of the file. It is followed by parallel efforts todesign the taper, helix, and cross-sectional profile. Once a prototype
1556 He and Ni
design is obtained, it is evaluated against the design requirements ontorsional stiffness and bending flexibility. The design for mechanicalperformances is completed if the requirements on file stiffness and flex-ibility are met.
The core of this design process is to use finite element models toassist evaluating a design against the performance requirements andmaking design changes accordingly. Performance requirements definethe upper limit of load or deformation that is safe to a file, which isessentially the elastic limit of the file. Whether a design survives a specificelastic limit can be readily evaluated with finite element analysis. If detri-mental stresses are reported from the simulation, the design iterationstarts where 1 or more geometric parameters will be optimized. Thework of design optimization could benefit from the knowledge ofmechanical behavior in its relation to the design parameters.
ConclusionsIn this study, the impact of helix angle, taper, and flute length on
mechanical performances of V-Taper endodontic file designs was quan-titatively assessed through parametric studies with numerical simula-tions. Improvements on torsional stiffness and bending flexibilitywere attained through modification of geometric parameters will beoptimized. The elastic limit of the V-Taper file tip section was also esti-mated in both bending and torsion. A design methodology for achievingimproved mechanical performances was proposed.
AcknowledgmentsThe authors deny any conflicts of interest.
References1. Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and
torsional properties of Nitinol root canal files. J Endod 1988;14:346–51.2. Canalda-Sahli C, Brau-Aguade E, Berastegui-Jimeno E. A comparison of bending and
torsional properties of K-files manufactured with different metallic alloys. Int EndodJ 1996;29:185–9.
3. Esposito PT, Cunningham CJ. A comparison of canal preparation with nickel-titanium and stainless steel instruments. J Endod 1995;21:173–6.
4. Schafer E, Lohmann D. Efficiency of rotary nickel-titanium FlexMaster instrumentscompared with stainless steel hand K-Flexofile: part 1—shaping ability in simulatedcurved canals. Int Endod J 2002;35:505–13.
5. Schafer E, Schulz-Bongert U, Tulus G. Comparison of hand stainless steel and nickeltitanium rotary instrumentation: a clinical study. J Endod 2004;30:432–5.
6. Sattapan B, Nervo GJ, Palamara JE, et al. Defects in rotary nickel-titanium files afterclinical use. J Endod 2000;26:161–5.
7. Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-titanium endodontic instruments after clinical use. J Endod 2004;30:722–5.
8. Parashos P, Messer HH. Questionnaire survey on the use of rotary nickel-titaniumendodontic instruments by Australian dentists. Int Endod J 2004;37:249–59.
9. Vaudt J, Bitter K, Neumann K, et al. Ex vivo study on root canal instrumentation oftwo rotary nickel-titanium systems in comparison to stainless steel hand instru-ments. Int Endod J 2009;42:22–33.
10. Pruett JP, Clement DJ, Carnes DL Jr. Cyclic fatigue testing of nickel-titaniumendodontic instruments. J Endod 1997;23:77–85.
11. Barbosa FO, Gomes JA, de Araujo MC. Fractographic analysis of K3 nickel-titaniumrotary instruments submitted to different modes of mechanical loading. J Endod2008;34:994–8.
12. Ugur I, Nihan G. Deformation and fracture of Mtwo rotary nickel-titanium instru-ments after clinical use. J Endod 2009;35:1396–9.
13. Gianluca P, Nicola MG, Massimo C, et al. A review of cyclic fatigue testing of Nickel-Titanium rotary instruments. J Endod 2009;35:1469–76.
14. Xu X, Eng M, Zheng Y, et al. Comparative study of torsional and bending propertiesfor six models of nickel-titanium root canal instruments with different cross-sections. J Endod 2006;32:372–5.
15. Schafer E, Dzepina A, Danesh G. Bending properties of rotary nickel-titanium instru-ments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:757–63.
16. Turpin YL, Chagneau F, Vulcain JM. Impact of two theoretical cross-sections ontorsional and bending stresses of nickel-titanium root canal instrument models.J Endod 2000;26:414–7.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
17. Berutti E, Chiandussi G, Gaviglio I, et al. Comparative analysis of torsional andbending stresses in two mathematical models of nickel-titanium rotary instruments:ProTaper versus ProFile. J Endod 2003;29:15–9.
18. Tripi TR, Bonaccorso A, Condorelli GG. Cyclic fatigue of different nickel-titaniumendodontic rotary instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2006;102:e106–14.
19. Melo MC, Pereira ES, Viana AC, et al. Dimensional characterization and mechanicalbehaviour of K3 rotary instruments. Int Endod J 2008;41:329–38.
20. Camara AS, de Castro Martins R, Viana ACD, et al. Flexibility and torsional strength ofProTaper and ProTaper Universal rotary instruments assessed by mechanical tests.J Endod 2009;35:113–6.
21. Kim HC, Cheung GS, Lee CJ, et al. Comparison of forces generated during root canalshaping and residual stresses of three nickel-titanium rotary files by using a three-dimensional finite-element analysis. J Endod 2008;34:743–7.
22. Necchi S, Taschieri S, Petrini L, et al. Mechanical behaviour of nickel-titanium rotaryendodontic instruments in simulated clinical conditions: a computational study. IntEndod J 2008;41:939–49.
23. Petrini L, Necchi S, Taschieri S, et al. Numerical study on the influence of materialcharacteristics on Ni-Ti endodontic instrument performance. Journal of MaterialsEngineering and Performance 2009;18:631–7.
24. Kim HC, Kim HJ, Lee CJ, et al. Mechanical response of nickel-titanium instrumentswith different cross-sectional designs during shaping of simulated curved canals. IntEndod J 2009;42:593–602.
25. Kim TO, Cheung GS, Lee JM, et al. Stress distribution of three NiTi rotary files underbending and torsional conditions using a mathematic analysis. Int Endod J 2009;42:14–21.
26. Kim HC, Yum J, Hur B, et al. Cyclic fatigue and fracture characteristics of ground andtwisted Nickel-Titanium rotary files. J Endod 2010;36:147–52.
27. Chen W- C. Applying the finite element method to drill design based on drill defor-mations. Finite Elements in Analysis and Design 1997;26:57–81.
28. Selvam SVM, Sujatha C. Twist drill deformation and optimum drill geometry.Computers & Structures 1995;57:903–14.
29. da Silva FM. Kobayashi C, Suda H. Analysis of forces developed during mechanicalpreparation of extracted teeth using RaCe rotary instruments and ProFiles. Int En-dod J 2005;38:17–21.
JOE — Volume 36, Number 9, September 2010 Design Improvement
30. Grande NM, Plotino G, Pecci R, et al. Cyclic fatigue resistance and three-dimensionalanalysis of instruments from two nickel-titanium rotary systems. Int Endod J 2006;39:755–63.
31. Bryant ST, Dummer PM, Pitoni C, et al. Shaping ability of .04 and .06 taper ProFilerotary nickel-titanium instruments in simulated root canals. Int Endod J 1999;32:155–64.
32. Schafer E, Vlassis M. Comparative investigation of two rotary nickel-titaniuminstruments: ProTaper versus RaCe–part 2: cleaning effectiveness and shapingability in severely curved root canals of extracted teeth. Int Endod J 2004;37:239–48.
33. Yang GB, Zhou XD, Zhang H, et al. Shaping ability of progressive versus constanttaper instruments in simulated root canals. Int Endod J 2006;39:791–9.
34. Shen Y, Cheung GS, Peng B, et al. Defects in nickel-titanium instruments after clinicaluse: part 2—fractographic analysis of fractured surface in a cohort study. J Endod2009;35:133–6.
35. Low D, Ho AW, Cheung GS, et al. Mathematical modeling of flexural behavior ofrotary nickel-titanium endodontic instruments. J Endod 2006;32:545–8.
36. Gambarini G. Rationale for the use of low-torque endodontic motors in root canalinstrumentation. Endod Dent Traumatol 2000;16:95–100.
37. Schafer E, Diez C, Hoppe W, et al. Roentgenographic investigation of frequencyand degree of canal curvatures in human permanent teeth. J Endod 2002;28:211–6.
38. He R. Modeling, analysis, and experimental investigation of root canal instrumenta-tion (PhD dissertation). Ann Arbor, MI: University of Michigan; 2007.
39. Yared GM, Kulkarni GK. Failure of ProFile Ni-Ti instruments used by an inexperi-enced operator under access limitations. Int Endod J 2002;35:536–41.
40. Yared G, Kulkarni GK. Accuracy of the DTC torque control motor for nickel-titaniumrotary instruments. Int Endod J 2004;37:399–402.
41. Dauskardt RH, Duerig TW, Ritchie RO. Effects of in situ phase transformation onfatigue-crack propagation in Titanium-Nickel shape-memory alloys. In: Proceedingsof the MRS International Meeting on Advanced Materials, May 31-June 3, 1988, To-kyo, Japan:243–249.
42. McKelvey AL, Ritchie RO. Fatigue-crack propagation in Nitinol, a shape-memory andsuperelastic endovascular stent material. Journal of Biomedical Materials Research1999;47:301–8.
and Failure Reduction of Endodontic Files through Finite Element Analysis 1557

Basic Research—Technology
Tissue Dissolution by Sodium Hypochlorite: Effect ofConcentration, Temperature, Agitation, and SurfactantSonja Stojicic, DDS, MSc,*† Slavoljub Zivkovic, DDS, PhD,† Wei Qian, DDS, PhD,*
Hui Zhang, DDS, PhD,* and Markus Haapasalo, DDS, PhD*
Abstract
Aim: Sodium hypochlorite is the most commonly usedendodontic irrigant because of its antimicrobial andtissue-dissolving activity. The aim of this study was toevaluate and compare the effects of concentration,temperature, and agitation on the tissue-dissolvingability of sodium hypochlorite. In addition, a hypochloriteproduct with added surface active agent was comparedwith conventional hypochlorite solutions. Methods:Three sodium hypochlorite solutions from two differentmanufacturers in concentrations of 1%, 2%, 4%, and5.8% were tested at room temperature, 37�C, and45�C with and without agitation by ultrasonic and sonicenergy and pipetting. Distilled and sterilized tap waterwas used as controls. Pieces of bovine muscle tissue(68 � 3 mg) were placed in 10 mL of each solutionfor five minutes. In selected samples, agitation was per-formed for one, two, or four 15-second periods per eachminute. The tissue specimens were weighed before andafter treatment, and the percentage of weight loss wascalculated. The contact angle on dentin of the threesolutions at concentrations of 1% and 5.8% wasmeasured. Results: Weight loss (dissolution) of thetissue increased almost linearly with the concentrationof sodium hypochlorite. Higher temperatures and agita-tion considerably enhanced the efficacy of sodium hypo-chlorite. The effect of agitation on tissue dissolution wasgreater than that of temperature; continuous agitationresulted in the fastest tissue dissolution. Hypochloritewith added surface active agent had the lowest contactangle on dentin and was most effective in tissue disso-lution in all experimental situations. Conclusions: Opti-mizing the concentration, temperature, flow, and surfacetension can improve the tissue-dissolving effectivenessof hypochlorite even 50-fold. (J Endod 2010;36:1558–1562)From the *Division of Endodontics, Department of Oral Bio-logical & Medical Sciences, Faculty of Dentistry, University ofBritish Columbia, Vancouver, Canada; and †Department forRestorative Dentistry and Endodontics, Faculty of Dentistry,University of Belgrade, Belgrade, Serbia.
Address requests for reprints to Dr Markus Haapasalo, Divi-sion of Endodontics, Oral Biological & Medical Sciences, UBCFaculty of Dentistry, 2199 Wesbrook Mall, Vancouver, BC,Canada V6T 1Z3. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.021
1558 Stojicic et al.
Key WordsAgitation, Chlor-Xtra, sodium hypochlorite, surfactant, temperature, tissue dissolution
Success in endodontic treatment depends to a great extent on chemomechanicaldebridement of the canals. Although instruments remove most of the canal contents
in the main root canal area, irrigation plays an indispensable role in all areas of the rootcanal system, in particular those parts that are inaccessible for instrumentation (1). Themost favorable features of irrigants are their flushing action, tissue-dissolving ability,antimicrobial effect, and low toxicity (2, 3). Sodium hypochlorite is the mostcommonly used endodontic irrigant because of its well-known antimicrobial andtissue-dissolving activity (4–6).
The dissolving capability of sodium hypochlorite relies on its concentration,volume, and contact time of the solution but also on the surface area of the exposedtissue (7). However, high concentrations are potentially toxic for periapical tissue(8–10). Also, changes in mechanical properties such as decreased microhardnessand increased roughness of radicular dentin have been reported after exposure tosodium hypochlorite in concentrations of 2.5% and 5.25% (11).
Possible ways to improve the efficacy of hypochlorite preparations in tissue disso-lution are increasing the pH (12) and the temperature of the solutions, ultrasonic acti-vation, and prolonged working time (13). Although there is a general consensus thatincreased temperature enhances the effectiveness of hypochlorite solutions, thereare only a few published articles about this (14–16). It has been suggested thatpreheating low-concentration solutions improves their tissue-dissolving capacity withno effect on their short-term stability. Also, systemic toxicity is lower compared withthe higher-concentration solutions (at a lower temperature) with the same efficacy(15). The impact of mechanical agitation of the hypochlorite solutions on tissue disso-lution was found to be very important by Moorer and Wesselink (7) who emphasizedthe great impact of violent fluid flow and shearing forces caused by ultrasound on theability of hypochlorite to dissolve tissue. However, the mechanisms involved are notcompletely understood (13). Despite several separate reports of the various ways toimprove the effectiveness of tissue dissolution by sodium hypochlorite, the relativeimportance of temperature, concentration, and agitation remains unclear. In thepresent study, all these factors were examined under controlled conditions to allowcomparison of their role. Finally, a hypochlorite product with an added surface activeagent was compared with conventional products in the different experimental settings.
Materials and MethodsSolutions
Sodium hypochlorite solutions in concentrations of 1%, 2%, 4%, and 5.8% weretested. Stock solution of 6 % sodium hypochlorite (Regular 1; EMD Chemicals Inc,Gibbstown, NJ) and 5.8% sodium hypochlorite (Regular 2; Inter-Med, Inc/Vista DentalProducts, Racine, WI) were obtained from the manufacturers. Two different hypochlo-rite products with 5.8% sodium hypochlorite were included in the experiments: oneconventional solution (Regular 2, Vista-Dental) and one with a surface active agentadded (Chlor-Xtra, Vista-Dental). The amount of available chlorine was obtained bythe manufacturers. The solutions were kept at 4�C following the recommendationsof the manufacturer and brought to room temperature (RT) before use. One percent,
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
2%, 4%, and 5.8% solutions of sodium hypochlorite were prepared bydiluting the stock solution in distilled water. Distilled and sterilized tapwater was used as controls.Dissolution of TissueBovine meat was used as a tissue sample in the experiment. It was
kept frozen at �15�C in 100% humidity. Frozen tissue was cut intopieces of 4� 4� 2 mm using stainless steel blade. Because the surfacearea has a great impact on the tissue dissolution, each sample hada similar size and shape. The samples had an original weight of 68 �3 mg with no significant difference between groups.
The experiments were done at RT and at 37�C and 45�C. A waterbath (Water Bath Digital 10L; Fisher Scientific, Ottawa, Ontario, Canada)was used for the experiments at 37�C and 45�C. The temperature of thesolutions was confirmed using a thermometer (Fisher Scientific).
Three different means of agitation were tested: ultrasonic, sonic,and pipetting. An ultrasonic system (Varios Lux 350; NSK, Kanuma,Japan) with a slender steel tip (E 7) at power setting 4 was used todeliver ultrasonic energy. Sonic vibration at 10,000 cpm was appliedby EndoActivator (Dentsply, Tulsa, OK) using a flexible polymer tipsize 25/04 (medium). The tips (ultrasonic and sonic) were immersedin the hypochlorite solutions into a depth of 10 mm, 5 mm away fromthe tissue specimens, without touching them. A transfer pipette (grad,5.8 mL, Fisher Scientific) was used for mechanical agitation of the hypo-chlorite solutions; the tip of the pipette was at 5 mm distance from thetissue specimen. Agitation was performed 15 seconds per each minuteduring the 5-minute incubation period. The three hypochlorite solu-tions in selected concentrations were tested at RT and at 45�C withand without agitation. In addition, the effect of duration of agitationby pipetting was studied using the 2% and 5.8% solutions of the Regular2 hypochlorite solution (Vista-Dental) at RT as follows: the tissue spec-imens were treated for 5 minutes in the hypochlorite solutions, pipettingwas done as above either for one or two 15-second periods per eachminute, or continuously throughout the 5-minute experiment.
TABLE 1. Tissue Weight Loss (% � Standard Deviation) After 5 Minutes of ExposTemperatures
% of weight loss RT
Distilled water (control) �0.87 � 1.59Sterilized water (control) �2.26 � 1.351%
Regular 1 �3.21 � 1.85Regular 2 �5.52 � 1.38Chlor-Xtra �6.51 � 3.05
2%Regular 1 4.41 � 1.79Regular 2 3.95 � 2.04Chlor-Xtra 7.75 � 2.08†
4%Regular 1 20.52 � 3.00†
Regular 2 18.13 � 2.22†
Chlor-Xtra 28.19 � 3.27†,‡
5.8%Regular 1 29.93 � 2.24†
Regular 2 27.28 � 4.47†
Chlor-Xtra 41.55 � 5.22†,‡
RT, room temperature; regular 1, sodium hypochlorite (EMD Chemicals Inc); regular 2, sodium hypochlori
agent (Inter-Med, Inc./Vista Dental Products).
*p < 0.05.†p < 0.001 versus distilled water.‡p < 0.05.§p < 0.01.kp < 0.001 versus regular 1.
JOE — Volume 36, Number 9, September 2010
The specimens were weighed on an electronic balance (FX-300;A&D Company, Ltd, Tokyo, Japan) before the hypochlorite treatmentsand placed each in 10 mL of preheated hypochlorite solution in sepa-rate beakers in the temperature-controlled water bath. Five parallelsamples per group were included in all experiments. After 5 minutesin the solution, the samples were blotted dry and weighed again. Thepercentage of weight loss was calculated.
Contact Angle MeasurementExtracted human maxillary canine and mandibular premolars
were used to prepare the dentin surfaces for contact angle measure-ments. After cutting off the crown and apical third of the root, each toothwas split in half labiopalatally using a low-speed diamond saw. Each cutsurface was polished using a series of abrasive papers (CarbiMet; Bueh-ler, Lake Bluff, IL) in the following sequence (120/P120, 180/P180,240/P280, 320/P400, 400/P800, and 600/P1200). A 1.5-mL dropletof 1% and 5.8% hypochlorite solutions or distilled water (control)was placed on coronal root dentin using a 2-mL pipette. The contactangle was measured within 30 seconds using a NRL Contact Angle Goni-ometer (Rame-hart, Netcong, NJ). Six parallel measurements were per-formed with each solution on dentin surfaces of both teeth.
Data AnalysisWeight loss was expressed as mean value� standard deviation of
the percentage of the tissue weight loss. Data were analyzed using one-way analysis of variance followed by the Tukey post hoc test for multiplecomparisons (SPSS Inc, Chicago, IL). Statistical significance wasconsidered at p < 0.05.
ResultsTissue weight loss after 5 minutes in different concentrations of
sodium hypochlorite at three different temperatures is shown inTable 1. Weight loss increased with increasing concentrations ofsodium hypochlorite. A significant difference in weight loss wasobserved after exposure to 2% Chlor-Xtra and 4% and 5.8% (p <
ure to Three Sodium Hypochlorite Products at Different Concentrations and
37�C 45�C
1.40 � 2.33 10.91 � 1.712.36 � 1.14 8.26 � 1.86
�0.27 � 2.23 1.16 � 1.92�0.29 � 1.24 1.72 � 1.87
1.19 � 1.26 4.74 � 2.12
10.72 � 2.30† 14.61 � 5.278.25 � 2.30* 14.18 � 3.45
13.07 � 0.80† 21.10 � 2.16*,§
26.63 � 3.13† 36.26 � 2.95†
24.93 � 1.32† 33.61 � 3.58†
37.90 � 5.77†,k 49.17 � 5.20†,k
40.68 � 2.64† 49.10 � 6.52†
38.31 � 3.29† 48.18 � 4.45†
59.05 � 6.20†,k 67.28 � 8.80†,k
te (Inter-Med, Inc./Vista Dental Products); Chlor-Xtra, sodium hypochlorite with added surface active
Tissue Dissolution by NaClO 1559

TABLE2.
Effe
ctof
Thre
eD
iffer
ent
Met
hods
ofAg
itatio
non
Tiss
ueD
isso
lutio
n(%
Tiss
ueW
eigh
tLo
ss�
Stan
dard
Dev
iatio
n)by
the
Thre
eH
ypoc
hlor
itePr
oduc
ts
RT
45� C
No
agit
atio
nU
SEA
PN
oag
itat
ion
US
EAP
Dis
tilled
wate
r�
0.8
7�
1.5
92.3
5�
1.2
61.8
6�
1.3
32.1
8�
1.4
410.9
1�
1.7
110.5
0�
4.3
810.9
0�
3.7
111.9
1�
2.3
9St
eri
lize
dta
pw
ate
r�
2.2
6�
1.3
51.7
8�
1.1
92.6
7�
2.0
81.4
8�
1.0
68.2
6�
1.8
610.0
3�
3.5
58.5
8�
2.0
611.0
4�
1.7
42% R
eg
14.4
1�
1.7
911.7
6�
1.9
5‡
12.7
6�
1.6
3‡
20.5
6�
1.6
7‡
14.6
1�
5.2
729.8
5�
2.8
9‡
29.0
1�
1.0
5‡
37.3
1�
2.2
5‡
Reg
23.9
5�
2.0
411.3
9�
3.9
8†
12.8
3�
2.4
7‡
17.8
0�
0.8
5‡
14.1
8�
3.4
529.1
5�
3.6
6‡
26.0
7�
1.0
6‡
33.9
5�
2.3
7‡
Ch
lor-
Xtr
a7.7
5�
2.0
816.9
6�
3.2
8‡
16.2
5�
0.8
8‡
20.6
5�
1.6
8‡
21.1
0�
2.1
638.3
7�
3.7
2‡
35.1
7�
5.4
7‡
40.9
0�
1.8
0‡
5.8
% Reg
129.9
3�
2.2
436.2
8�
3.8
9*
34.1
9�
3.5
235.9
4�
3.0
2*
49.1
0�
6.5
274.9
9�
7.1
7‡
69.9
6�
4.7
8‡
73.0
0�
4.1
2‡
Reg
227.2
8�
4.4
734.0
0�
3.4
132.7
6�
3.3
839.1
6�
3.6
0‡
48.1
8�
4.4
575.5
1�
7.9
8‡
68.8
2�
7.0
9‡
71.6
8�
5.9
0‡
Ch
lor-
Xtr
a41.5
5�
5.2
248.0
3�
6.4
8§
47.7
6�
6.1
4§
48.9
1�
7.6
2§
67.2
8�
8.8
081.3
8�
2.8
8†
78.2
6�
2.9
8*
87.9
3�
7.1
3‡,§
US,
ultr
asou
nd;
EA,
endo
activ
ator
;P,
pipe
tting
.
*p<
0.05
.†p
<0.
01.
‡p
<0.
001
vers
usno
agita
tion.
§p
<0.
001
vers
usre
gula
r1.
Basic Research—Technology
1560 Stojicic et al.
0.001) of Regular 1 and Regular 2 sodium hypochlorite comparedwith controls at RT. Tissue specimens immersed in 1% sodium hypo-chlorite at RT increased in weight after 5 minutes.
Heating the hypochlorite solutions greatly increased tissue disso-lution; the magnitude of the increase compared with RT varied from30% to 300% depending on the concentration, temperature, andtype of hypochlorite (Table 1). Of the three solutions, the one withadded surface active agent dissolved significantly more tissue thanthe two other solutions in all temperature/concentration groups(Table 1).
The effect of the three different methods of agitation on the tissue-dissolving ability of 2% and 5.8% sodium hypochlorite is shown inTable 2. The tissue weight loss was significantly higher at both testedtemperatures when sodium hypochlorite solutions were agitatedthan without agitation (p < 0.001 for 2% and p < 0.01 for 5.8%sodium hypochlorite, Table 2). Under agitation at RT, tissue weightloss was significantly higher with 5.8% Chlor-Xtra than with both5.8% regular hypochlorite products (Table 2). Agitation experimentswith an increased time of active agitation from 25% to 100% showedcontinuous increase in tissue dissolution as the relative time of agita-tion increased (Table 3). The increase of tissue dissolution from noagitation to 100% agitation (pipette) in Regular 2 hypochlorite at RTwas 12.7-fold with 2% and 2.1-fold with 5.8% solution. Tissue weightloss was significantly higher after simultaneous action of temperatureand agitation than by either one alone (Tables 1-3). Chlor-Xtra (5.8%)had the lowest contact angle of the three hypochlorite solutions. Therewas no significant difference in contact angle between the 1% solutions(p > 0.05) (Table 4).
DiscussionA great number of studies have focused on the tissue-dissolving
ability of sodium hypochlorite. It has been found that the solvent capa-bility of sodium hypochlorite depends on its concentration; time;volume; pH; temperature; agitation; and the type, amount, and surfacearea of the tissue (2, 5, 7, 12). However, great variations among thesefactors contribute to the difficulty of making comparisons betweendifferent studies and the relative importance of each factor (17).The present study evaluated the effect of concentration, temperature,and agitation on sodium hypochlorite ability to dissolve organic mate-rial in a standardized setting. Tissues from a number of differentsources have been used in studies about sodium hypochloritetissue-dissolving ability (6). Porcine muscle tissue (1, 12), rabbitliver (7), rat connective tissue (5), pig palatal mucosa (18), bovinemuscle tissue (2), and bovine pulp (3) have been used to determinedissolution ability of different irrigants. The reasons for using differenttissue instead of dental pulp have been availability and easier standard-ization of the surface area of each specimen (2). Tissue specimensused in the present study were prepared from bovine muscle tissuewith a standardized weight of 68 � 3 mg. The meat specimens werecubical in shape (4� 4� 2 mm) giving an equal surface area. Pilotexperiments had shown that it was difficult to determine the endpointof complete dissolution of the tissue because of a great number ofbubbles (result of saponification reaction); therefore, fixed time wasused instead, and the samples were weighed before and after exposure.Other methods have used different approaches (eg, measuring thechanges in the solutions, such as the amount of available chlorine inthe solution after completed dissolution [7] or the amount of hydrox-yproline in the residual tissue after incubation with the solution [19]).
Previous studies have shown that the tissue-dissolving ability ofsodium hypochlorite solution decreases if it is diluted (2, 5, 16).Results from the present study showed that 5.8% sodium
JOE — Volume 36, Number 9, September 2010

TABLE 3. Effect of Agitation by Pipetting for 0%, 25%, 50%, and 100% of the 5-Minute Exposure Time on Tissue Dissolution (%� Standard Deviation) by 2% and5.8% Regular (Reg 2) Hypochlorite at Room Temperature
Agitation/no. of agitation per each minute
Solutions No agitation 15/45 15/15/15/15 Continuous
2% sodium hypochlorite 2.71 � 1.68 14.51 � 2.07† 24.56 � 2.37† 34.68 � 3.84†
5.8% sodium hypochlorite 29.94 � 2.31 39.11 � 4.44* 50.36 � 2.86† 63.14 � 6.90†
*p < 0.05.†p < 0.001 versus no agitation.
Basic Research—Technology
hypochlorite was the most effective in agreement with the previousstudies. Interestingly, tissue weight loss after 5 minutes in 2% ofsodium hypochlorite solution was equal to controls with distilled andsterilized tap water. It should be emphasized, however, that theweight loss in water did not change after 5 minutes, whereas itcontinued to increase in 2% sodium hypochlorite after the first 5-minute period (results not shown). Tissue specimens immersed in1% solutions increased in weight during the 5-minute exposure. Thiscan probably be explained by hydration of the tissue after the initial-dissolving action of sodium hypochlorite on the meat. Other studieshave also reported a similar effect on tissue by low-concentration hypo-chlorite solutions (5). However, longer exposure times will causeweight loss also with mild hypochlorite solutions.
The present study showed that heating the sodium hypochloritesolution enhanced its ability to dissolve organic material. These resultsare in accordance with other studies (14–16). Kamburis et al (20)found that heated sodium hypochlorite solutions were more effectivein removing organic debris from dentin shavings than unheated solu-tions at the same concentration. It has also been shown that sodiumhypochlorite solutions were stable for a period of 4 hours when heatedto 37�C (21). Sirtes et al (15) found that 1%, 2.62%, and 5.25% solu-tions had an unchanged quantity of available chlorine for 1 hour at 45�Cand 60�C, respectively. Therefore, in the present study, all experimentswere finished in less than 1 hour to exclude the possibility of the loss ofactivity of sodium hypochlorite during experimentation at highertemperatures.
The effect of the surface active agent to hypochlorite was firstshown by Cameron (22) who showed that the addition of the surfacemodifiers enhanced the ability of sodium hypochlorite to dissolveorganic material. Clarkson et al (6) tested the dissolution ability of threedifferent brands of sodium hypochlorite available in Australia and re-ported that the products with surfactants dissolved porcine pulp ina shorter time than regular sodium hypochlorite at the same concentra-tion. The present study not only confirmed these findings but alsoshowed that the advantage over regular products remained also whenthe products were diluted, heated, or agitated. Although not knownin detail, it is possible that the better performance of Chlor-Xtra overregular hypochlorite is based partly on better contact on the surfaceof the tissue as well as faster exchange with fresh solution, both facili-
TABLE 4. Contact Angle (Mean � Standard Deviation) on Dentin of Three Sodium
1%
Distilled water Reg 1 Reg 2 Chlor-Xt
39.33 � 12.35 52.17 � 13.58 44.83 � 12.33 41.42 � 9
*p < 0.05.†p < 0.001 versus distilled water.‡p < 0.01.§p < 0.001 versus 5.8% Reg 1.
JOE — Volume 36, Number 9, September 2010
tated by the surface active agent. The lower contact angle of 5.8% Chlor-Xtra as compared with the two regular hypochlorites supports theassumption of better wetting of the surface of the substrate. Whendiluted to 1%, there was no significant difference in contact anglebetween the products, obviously because of the higher proportion ofthe water.
The importance of agitation on the tissue-dissolving ability ofsodium hypochlorite has been reported, but there are very few studieson the effect of agitation on this (7). Aqueous solution of sodium hypo-chlorite is a dynamic balance of sodium hydroxide and hypochlorousacid. When sodium hypochlorite is in contact with organic material,sodium hydroxide reacts with fatty acids creating soap and glycerol,which is known as saponification reaction. It also reacts with aminoacids creating salt and water (neutralization). In addition, hypochlo-rous acid acts with amino acids creating chloramine and water. Thesereactions, which happen mostly at the surface, lead to liquefaction of theorganic tissue (23). At the same time, molecules of sodium hypochlo-rite involved in the reactions are consumed, resulting in the decline oflocal activity. It is therefore important to supply active hypochlorite tothe area and also remove the remnants of dissolved tissue. In this study,the effect of three different agitation methods on the tissue-dissolvingability of sodium hypochlorite was investigated. It was found that theagitation of the solution improved their dissolving ability; however, therewere no significant differences between the three methods of agitation.
The use of ultrasound energy in root canal preparation and irriga-tion has for a long time been a matter for debate. Although someresearchers have reported great success of ultrasonics in root canalcleaning (24–28), others did not find ultrasound superior comparedwith root canal irrigation using the syringe (29–31). The mechanismof passive ultrasonic action has been attributed to acoustic streaming(microstreaming) and cavitation (13, 32). A sonic action hasa similar mechanism of action to ultrasonic although the pattern ofthe oscillating file is different. However, according to Lumley et al(33), cavitation is limited to the distance of less than 100 mm. All exper-iments in the present study were performed in the beaker with the ultra-sonic/sonic tip immersed in the solutions to a depth of 10 mm, 5 mmaway from the tissue specimen without touching it. Therefore, the possi-bility to evaluate the direct impact of ultrasonic or sonic energy by cavi-tation was excluded. However, acoustic streaming developed by this
Hypochlorite Solutions (1% and 5.8%)
5.8%
ra Reg 1 Reg 2 Chlor-Xtra
.59 71.92 � 12.76† 54.58 � 13.91*,‡ 36.25 � 8.25§
Tissue Dissolution by NaClO 1561

Basic Research—Technology
mechanism creates stirring action and rapid movements of the liquidfurther away from the energy source. This is likely to be the mechanismby which ultrasonic affects cleaning of the peripheral parts in root canalin vivo. Within the limitations of the present study, all three methods ofagitation improved tissue dissolution. In clinical endodontics penetra-tion of irrigants to the most apical canal and to other peripheral areasuch as fins and webs remains a great challenge, and both ultrasonicand sonic agitation may in that environment have advantages whichcould not be demonstrated in the present study design.In conclusion, an increase in concentration and temperature ofsodium hypochlorite greatly increased its efficacy in tissue dissolution.Refreshing the hypochlorite solution at the site of dissolution by agita-tion, preferably continuous, also resulted in a marked increase of hypo-chlorite effect. High temperature and agitation had an additive effect onthe tissue dissolution. The sodium hypochlorite product with addedsurface active agent was the most effective in tissue dissolution at allconcentrations and temperatures.
References1. Hasselgren G, Olsson B, Cvek M. Effects of calcium hydroxide and sodium hypochlo-
rite on the dissolution of necrotic porcine muscle tissue. J Endod 1988;14:125–7.2. Turkun M, Cengiz T. The effects of sodium hypochlorite and calcium hydroxide on
tissue dissolution and root canal cleanliness. Int Endod J 1997;30:335–42.3. Okino LA, Siqueira EL, Santos M, et al. Dissolution of pulp tissue by aqueous solu-
tion of chlorhexidine digluconate and chlorhexidine digluconate gel. Int Endod J2004;37:38–41.
4. Rosenfeld EF, James GA, Burch BS. Vital pulp tissue response to sodium hypochlo-rite. J Endod 1978;4:140–6.
5. Hand RE, Smith ML, Harrison JW. Analysis of the effect of dilution on the necrotictissue dissolution property of sodium hypochlorite. J Endod 1978;4:60–4.
6. Clarkson RM, Moule AJ, Podlich H, et al. Dissolution of porcine incisor pulps insodium hypochlorite solutions of varying compositions and concentrations. AustDent J 2006;51:245–51.
7. Moorer WR, Wesselink PR. Factors promoting the tissue dissolving capability ofsodium hypochlorite. Int Endod J 1982;15:187–96.
8. Mehra P, Clancy C, Wu J. Formation of a facial hematoma during endodontictherapy. J Am Dent Assoc 2000;131:67–71.
9. Gernhardt CR, Eppendorf K, Kozlowski A, et al. Toxicity of concentrated sodiumhypochlorite used as an endodontic irrigant. Int Endod J 2004;37:272–80.
10. Barnhart BD, Chuang A, Lucca JJ, et al. An in vitro evaluation of the cytotoxicity ofvarious endodontic irrigants on human gingival fibroblasts. J Endod 2005;31:613–5.
11. Ari H, Erdemir A, Belli S. Evaluation of the effect of endodontic irrigation solutions onthe microhardness and the roughness of root canal dentin. J Endod 2004;30:792–5.
12. Christensen CE, McNeal SF, Eleazer P. Effect of lowering the pH of sodium hypochlo-rite on dissolving tissue in vitro. J Endod 2008;34:449–52.
1562 Stojicic et al.
13. Zehnder M. Root canal irrigants. J Endod 2006;32:389–98.14. Rossi-Fedele G, De Figueiredo JA. Use of a bottle warmer to increase 4% sodium
hypochlorite tissue dissolution ability on bovine pulp. Aust Endod J 2008;34:39–42.
15. Sirtes G, Waltimo T, Schaetzle M, et al. The effects of temperature on sodium hypo-chlorite short-term stability, pulp dissolution capacity, and antimicrobial efficacy.J Endod 2005;31:669–71.
16. Abou-Rass M, Oglesby SW. The effects of temperature, concentration, and tissue typeon the solvent ability of sodium hypochlorite. J Endod 1981;7:376–7.
17. Beltz RE, Torabinejad M, Pouresmail M. Quantitative analysis of the solubilizingaction of MTAD, sodium hypochlorite, and EDTA on bovine pulp and dentin.J Endod 2003;29:334–7.
18. Naenni N, Thoma K, Zehnder M. Soft tissue dissolution capacity of currently usedand potential endodontic irrigants. J Endod 2004;30:785–7.
19. Koskinen KP, Stenvall H, Uitto VJ. Dissolution of bovine pulp tissue by endodonticsolutions. Scand J Dent Res 1980;88:406–11.
20. Kamburis JJ, Barker TH, Barfield RD, et al. Removal of organic debris from bovinedentin shavings. J Endod 2003;29:559–61.
21. Frais S, Ng YL, Gulabivala K. Some factors affecting the concentration of availablechlorine in commercial sources of sodium hypochlorite. Int Endod J 2001;34:206–15.
22. Cameron JA. The effect of a fluorocarbon surfactant on the surface tension of theendodontic irrigant, sodium hypochlorite. A preliminary report. Aust Dent J1986;31:364–8.
23. Estrela C, Estrela CR, Barbin EL, et al. Mechanism of action of sodium hypochlorite.Braz Dent J 2002;13:113–7.
24. Sabins RA, Johnson JD, Hellstein JW. A comparison of the cleaning efficacy of short-term sonic and ultrasonic passive irrigation after hand instrumentation in molarroot canals. J Endod 2003;29:674–8.
25. Cameron JA. The synergistic relationship between ultrasound and sodium hypochlo-rite: a scanning electron microscope evaluation. J Endod 1987;13:541–5.
26. Ahmad M, Pitt Ford TJ, Crum LA. Ultrasonic debridement of root canals: acousticstreaming and its possible role. J Endod 1987;13:490–9.
27. Ahmad M, Pitt Ford TR, Crum LA. Ultrasonic debridement of root canals: an insightinto the mechanisms involved. J Endod 1987;13:93–101.
28. Weller RN, Brady JM, Bernier WE. Efficacy of ultrasonic cleaning. J Endod 1980;6:740–3.
29. Mayer BE, Peters OA, Barbakow F. Effects of rotary instruments and ultrasonic irri-gation on debris and smear layer scores: a scanning electron microscopic study. IntEndod J 2002;35:582–9.
30. Cymerman JJ, Jerome LA, Moodnik RM. A scanning electron microscope studycomparing the efficacy of hand instrumentation with ultrasonic instrumentationof the root canal. J Endod 1983;9:327–31.
31. Tauber R, Morse DR, Sinai IA, et al. A magnifying lens comparative evaluation ofconventional and ultrasonically energized filing. J Endod 1983;9:269–74.
32. van der Sluis LW, Versluis M, Wu MK, et al. Passive ultrasonic irrigation of the rootcanal: a review of the literature. Int Endod J 2007;40:415–26.
33. Lumley PJ, Walmsley AD, Laird WR. Streaming patterns produced around endosonicfiles. Int Endod J 1991;24:290–7.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
Detection of Dentinal Cracks after Root-end Resection: An ExVivo Study Comparing Microscopy and Endoscopy withScanning Electron MicroscopyThomas von Arx, Prof.Dr.med.dent.,* Renato Kunz, Dr.med.dent.,
†
Adrienne Christina Schneider, Dr.med.dent.,* Walter Burgin, med.ing.,*
and Adrian Lussi, Prof.Dr.med.dent.†
Abstract
Introduction: Dentinal cracks are occasionally observedat the cut root face after root-end resection in apicalsurgery. The objective of this ex vivo study was to eval-uate and compare the efficiency of visual aids to identifyroot-end dentinal cracks. Methods: Twenty-six ex-tracted human molars were decoronated, and the rootcanals were instrumented and filled. The apical 3 mmof the roots were resected, and the cut root faces wereassessed with microscopy at �16 and �24 magnifica-tion and with endoscopy at �8 and �64 magnification(four visual aids). Roots were then duplicated for inspec-tion with scanning electron microscopy. The presence,type, and location of cracks were registered by a blindedobserver, with the scanning electron microcopy servingas the reference. The percentages of correct identifica-tion of dentinal cracks were then statistically comparedamong the four test configurations. Results: Endoscopy�64 showed the highest sensitivity for crack identifica-tion, irrespective of the applied methodology (ie, per rootand per crack). However, higher scores of false-positivecracks (lower specificity) were found with endoscopy�64 than with the other tested visual aids. The correctdetection and location of complete canal cracks(55.3%, 52.6%, 68.4%, and 78.9%) were higher thanthe detection of incomplete canal cracks (42.2%,42.2%, 52.0%, and 64.7%) using the four tested visualaids (microscopy at �16 and �24 magnificationand endoscopy at �8 and �64 magnification, respec-tively). Only one of five intradentin cracks was identifiedwith endoscopy �64. Conclusions: Overall, endoscopy�64 proved the most accurate visual aid for the identi-fication of dentinal cracks after root-end resection inextracted human teeth; however, it also providedthe most false identifications. (J Endod 2010;36:1563–1568)From the Departments of *Oral Surgery and Stomatology and †PSwitzerland.
Address requests for reprints to Dr Thomas von Arx, DepartmentCH-3010 Bern, Switzerland. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.016
JOE — Volume 36, Number 9, September 2010
Key WordsApical surgery, dentinal crack, endoscopy, microscopy, root end
The ideal goal of apical surgery is to create optimum conditions for healing by sealingany path from the root canal to the periradicular tissues (1). Therefore, the identi-
fication and treatment of possible pathways, such as isthmuses, accessory canals, andcracks or microfractures, is of utmost importance to avoid the recurrence of leakagewith subsequent infection. The introduction of microsurgical principles almost 15 yearsago, including microinstruments, well-focused illumination, and magnification, led toa realization of the importance of detecting microscopic findings to improve the healingoutcome of apical surgery (2–4). Working with loupes or with a surgical microscopehas become widely accepted and recommended in conventional and surgicalendodontics. Several authors have suggested that the use of aids to enhance visionmight be decisive in achieving high success rates in apical surgery (3, 5, 6). Thesaying ‘‘you can only treat what you can see,’’ however, is greatly influenced by theclinician’s ability to (1) identify microscopic findings and (2) correctly interpretthese microelements at the cut root face. Hence, the accuracy of identification ofmicroscopic findings will play a decisive role in apical surgery.
Recent experimental studies have evaluated and compared the effectiveness ofdifferent visual aids in identifying microstructures after root-end resection. An experi-mental study showed enhanced accuracy of crack identification in extracted humanteeth with increasing magnification, but the overall accuracy ranging between 39%and 58% was lower than expected (7). Using transillumination of the root end, whetheralone or in combination with a dye, was reported as a more accurate way of diagnosingroot-end dentinal cracks (8). Another experimental study compared endoscopy withscanning electron microscopy for the detection of microelements at the cut root facein extracted human teeth after root-end resection (9). That research showed the correctidentification of isthmuses in all teeth, but cracks were less accurately identified. Theobjective of the present study was to evaluate and compare the accuracy of the micro-scope and the endoscope for the identification of dentinal cracks after root-end resec-tion in extracted human teeth.
Materials and MethodsThe material comprised 26 extracted human molars with closed apices. None of
the teeth presented with a root canal filling (teeth were radiographed mesiobuccally and
reventive, Restorative and Pediatric Dentistry, School of Dental Medicine, University of Bern, Bern,
of Oral Surgery and Stomatology, School of Dental Medicine, University of Bern, Freiburgstrasse 7,ibe.ch.
Detection of Dentinal Cracks After Root-end Resection 1563

Figure 1. A schematic illustration of a cut root face with various cracks. A 12-sector grid was used for location of cracks. The notch was always made at themidbuccal aspect of the cut root face.
Basic Research—Technology
orofacially). After the removal of all periodontal tissues from the rootsurfaces, the teeth were stored in a saturated mineral solution (10)at 37�C.For root canal treatment, the crowns were partially removed (3mm from the occlusal plane), and the pulps were shaped accordingto the ‘‘balanced force technique’’ (11). Canals were irrigated withNaOCl 3%. After drying with paper points, canal obturation was accom-plished with lateral condensation using gutta-percha points and sealer(AH Plus; Dentsply DeTrey, Konstanz, Germany). Access cavities wereclosed with glass ionomer cement (Ketac-Fil; 3M ESPE, Seefeld,Germany). Subsequently, all teeth were stored at 37�C and 100%humidity for a minimum of 4 weeks to allow complete setting of thecanal sealer.
Root-end resection was performed perpendicular to the long axisof the root at a level of 3 mm from the apex using a cylindrical fissurebur under copious irrigation. In addition, a notch was prepared at thejunction of the cut root face and the buccal root surface to standardizethe orientation of the resection plane for the subsequent analysis. Theroots were air dried and stained with 2% methylene blue dye (12). Afterthe methylene blue was rinsed off with water, root surfaces were driedagain. Subsequently, the root-end faces were examined with a surgicalmicroscope (Moller Denta 300; Haag-Streit International, Koeniz,Switzerland) at�16 and�24 magnification and with a rigid endoscope(Hopkins Tele-Otoscope 70o; Karl Storz GmbH, Tuttlingen, Germany) at�8 and�64 magnification, yielding four different test configurations.Video sequences limited to 2 minutes per root were recorded for subse-quent image analysis.
The primary study parameter was the presence (or absence) ofdentinal cracks at the resection plane. A crack was defined as anydark line within the resected dentinal surface that appeared to disruptthe integrity of the dentin, not including artifacts produced by the resec-tion of the root end (8). Three different types of dentinal cracks weredistinguished (13): incomplete canal cracks, complete canal cracks,and intradentin cracks.
After the microscopic and endoscopic visual evaluation, root endswere duplicated for scanning electron microscopy (SEM) analysis bytaking impressions with silicone (Impregum Penta Soft, 3M ESPE).Impressions were poured with resin (Epofix, Struers, Birmensdorf,Switzerland) and sputter coated with gold and palladium (SputterSCD 050; Balzers Union AG, Balzers, Liechtenstein). The SEM was deter-mined as the reference baseline. The SEM examination was performedby a blinded observer, with the time limited to 2 minutes. SEM evalua-tion was done between�50 and�200 magnification (Stereoscan 200;Cambridge Instruments Ltd, Cambridge, United Kingdom).
The following analyses were performed to compare the four testvisual aids with SEM: (i) analysis 1: presence (or absence) and typeof crack, with the root as the unit of evaluation, and (ii) analysis 2:concurrence between test visual aid and SEM, with regard to type andlocation of crack, using a 12-sector grid (Figs. 1-7).
Figure 2. An SEM reference image (�28.9 magnification) of cut root facepresenting with one incomplete canal crack (upper right quadrant) and twocomplete canal cracks (lower quadrants). The notch on the midbuccal aspectis clearly visible. The black holes on the cut root face are caused by entrappedtiny air bubbles during impression taking for making the root replicas.
StatisticsFor comparison of the four methods (microscopy �16, micros-
copy �24, endoscopy �8, and endoscopy �64) with SEM, Cohenkappa values were calculated based on the sector data (14). Forcomparisons among the different methods, the sensitivity and specificity(for definitions, see http://en.wikipedia.org/wiki/Sensitivity_and_specificity) of crack identification were assessed using the root data.Furthermore, the cracks’ percentage values were transformed with anArcsine transformation, and their effect size was compared with Cohen’scritical hc (15).
1564 von Arx et al.
ResultsDuring the evaluation process, three teeth had to be discarded
because root-end inspection was impossible because of artifacts, rootfracture, or irregular root-face cutting. This resulted in 23 teeth witha total of 52 roots to be assessed (52 roots � 12 sectors/root = 624sectors). The evaluation per sectors showed good concurrence betweenall test configurations and SEM, with kappa values of 0.90 (microscopy�16), 0.90 (microscopy �24), 0.87 (endoscopy �8), and 0.84(endoscopy �64).
JOE — Volume 36, Number 9, September 2010

Figure 3. An image of the same cut root face obtained with a microscope(�16 magnification); the two complete canal cracks in the lower quadrantscan be identified, but the incomplete canal crack in the upper right quadrantis barely visible. (This figure is available in color online at www.aae.org/joe/.)
Figure 5. An image of the same cut root face obtained with an endoscope(�8 magnification); all three cracks are clearly visible. (This figure is avail-able in color online at www.aae.org/joe/.)
Basic Research—Technology
Analysis 1SEM showed that 49 of 52 roots presented with a crack at the
resection plane (Table 1). Twenty-eight roots had a complete canalcrack, 44 roots had an incomplete canal crack, and only 5 roots hadan intradentin crack. Endoscopy �64 showed the highest sensitivityof all tested visual aids with regard to crack detection for categoriesall cracks (95.9%), complete canal cracks (92.9%), and incompletecanal cracks (90.9%). The statistical evaluation for sensitivity wassignificantly higher for endoscopy �64 than for both microscopemagnifications (p < 0.05). In contrast, the specificity of endoscopy�64 was lower (all cracks, 33.3%; complete canal cracks, 87.5%;incomplete canal cracks, 75.0%) than the specificity of endoscopy�8, microscopy �16, and microscopy �24 for the same categories,with statistically significant differences between endoscopy �64 and
Figure 4. An image of the same cut root face obtained with a microscope(�24 magnification); all three cracks are visible, but the incomplete canalcrack in the upper right is still difficult to identify. (This figure is availablein color online at www.aae.org/joe/.)
JOE — Volume 36, Number 9, September 2010
both microscope magnifications only for all cracks (p < 0.01). For in-tradentin cracks, no significant differences were found for specificityand sensitivity when the four test configurations were compared.
Analysis 2SEM showed a total of 145 cracks (38 complete canal cracks, 102
incomplete canal cracks, and 5 intradentin cracks) that were seen at thecut root faces of the 52 roots (Table 2). Endoscopy�64 exhibited thehighest percentages of concurrence between tested visual aid and SEMwith regard to the type and location of cracks for all categories (ie, allcracks, 66.9%; complete canal cracks, 78.9%; incomplete canalcracks, 64.7%; and intradentin cracks, 20%). For the category allcracks, endoscopy �64 was significantly better than all other testconfigurations (p < 0.05). For the categories complete canal cracksand incomplete canal cracks, endoscopy �64 was significantly betterthan microscopy �16 and �24 (p < 0.05), but no significant
Figure 6. An image of the same cut root face obtained with an endoscope(�64 magnification): a view of the incomplete canal crack in the upper rightquadrant. (This figure is available in color online at www.aae.org/joe/.)
Detection of Dentinal Cracks After Root-end Resection 1565

Figure 7. An image of the same cut root face obtained with an endoscope(�64 magnification): a view of the two complete canal cracks in the lowerquadrants. (This figure is available in color online at www.aae.org/joe/.)
Mic
rosc
op
e�
24
End
osc
op
e�
8En
do
sco
pe�
64
ctly
ent
Co
rrec
tly
pre
sen
tC
orr
ectl
yab
sen
tC
orr
ectl
yp
rese
nt
Co
rrec
tly
abse
nt
Co
rrec
tly
pre
sen
tC
orr
ectl
yab
sen
t
337
344
247
175.5
b89.8
95.9
ab
c100
d66.7
33.3
cd
220
22
24
23
26
21
71.4
f85.7
92.9
ef
1.7
91.7
95.8
87.5
629
636
540
665.9
h81.8
90.9
gh
5.0
75.0
62.5
75.0
60
45
146
145
020.0
20.0
7.8
95.7
97.8
95.7
Basic Research—Technology
difference was found between endoscopy�64 and endoscopy�8. Forintradentin cracks, no significant differences were found among thefour test configurations.
False-positive cracks were more frequently seen with endoscopy�64 than with the other tested visual aids, with significant differencesfor the category all cracks when comparing endoscopy �64 withmicroscopy �16 and �24 (p < 0.01), for the category incompletecanal cracks when comparing endoscopy �64 with microscopy �16and �24 (p < 0.05), and for the category intradentin crackswhen comparing endoscopy �64 with microscopy �16 (p < 0.05)(Table 3).
TABLE1.
Iden
tifica
tion
ofCr
acks
per
Roo
t(n
=52
)
SEM
(ref
eren
ce)
Mic
rosc
op
e�
16
Cra
ckp
rese
nt
Cra
ckab
sen
tC
orr
ectl
yp
rese
nt
Co
rre
abs
All
crack
s49
337
Sen
siti
vity
(%)
75.5
a
Speci
fici
ty(%
)100
Co
mp
lete
can
alcr
ack
s28
24
19
2Se
nsi
tivi
ty(%
)67.9
e
Speci
fici
ty(%
)9
Inco
mp
lete
can
alcr
ack
s44
830
Sen
siti
vity
(%)
68.2
g
Speci
fici
ty(%
)7
Intr
ad
en
tin
crack
s5
47
04
Sen
siti
vity
(%)
0Sp
eci
fici
ty(%
)9
a,b
,c,d
,e,g
,hSi
gnifi
cant
diffe
renc
es(p
<0.
01).
f Sign
ifica
ntdi
ffere
nces
(p<
0.05
).
DiscussionThe present study evaluated the identification of dentinal cracks
after root-end resection in extracted human molars. Microscopy(�16 and �24 magnification) and endoscopy (�8 and �64magnification) were the visual aids tested, and SEM served as thereference.
A total of 145 cracks were identified with SEM in 52 roots. Themajority (70.3%) of detected cracks were incomplete canal cracks.However, because crack identification was only performed at the resec-tion plane (ie, 3 mm from the apex), it can be speculated that incom-plete canal cracks might be complete canal cracks and vice versa ina different plane (16). It has been shown that instrumentation for ortho-grade root canal preparation can lead to the development of cracks, inparticular in the apical area (17). The clinical significance of dentinalcracks identified during apical surgery has not yet been clarified. Acomplete canal crack might contribute to leakage resulting in the recur-rence of periapical infection and might explain surgical (and nonsur-gical) failures in an unknown number of cases.
Concerns that root-end cavity preparation using sonic- orultrasonic-powered microtips might augment crack formation havebeen refuted in three cadaver studies (18-20) and in one clinicalstudy (21). Reasons for crack development in the present materialincluded the extraction of the tooth and ex vivo treatment (crown resec-tion, endodontic preparation and obturation, and root-end resection)(16, 20, 22, 23). None of the teeth in this study was endodonticallytreated before extraction.
1566 von Arx et al. JOE — Volume 36, Number 9, September 2010

TABLE2.
Iden
tifica
tion
ofCr
acks
byTy
pean
dLo
catio
n(N
=14
5)
SEM
(ref
eren
ce)
Mic
rosc
op
e�
16
Mic
rosc
op
e�
24
End
osc
op
e�
8En
do
sco
pe�
64
Cra
ckp
rese
nt
Typ
ean
dlo
cati
on
corr
ect
Loca
tio
nco
rrec
tb
ut
wro
ng
typ
eC
rack
no
tid
enti
fied
Typ
ean
dlo
cati
on
corr
ect
Loca
tio
nco
rrec
tb
ut
wro
ng
typ
eC
rack
no
tid
enti
fied
Typ
ean
dlo
cati
on
corr
ect
Loca
tio
nco
rrec
tb
ut
wro
ng
typ
eC
rack
no
tid
enti
fied
Typ
ean
dlo
cati
on
corr
ect
Loca
tio
nco
rrec
t,b
ut
wro
ng
typ
eC
rack
no
tid
enti
fied
All
crack
s145
64
12
69
63
16
66
80
16
49
97
19
29
Perc
en
tag
e44.1
a8.3
47.6
d43.5
b11.0
45.5
e55.2
c11.0
33.8
f66.9
a,b
,c13.1
20.0
d,e
,f
Co
mp
lete
can
al
crack
s
38
21
611
20
612
26
48
30
35
Perc
en
tag
e55.3
g15.8
28.9
52.6
h15.8
31.6
i68.4
10.5
21.1
78.9
g,h
7.9
13.2
i
Inco
mp
lete
can
alcr
ack
s102
43
653
43
10
49
53
12
37
66
16
20
Perc
en
tag
e42.2
j5.9
l52.0
m42.2
k9.8
48.0
n52.0
11.8
36.3
o64.7
j,k
15.7
l19.6
m,n
,o
Intr
ad
en
tin
crack
s5
00
50
05
10
41
04
Perc
en
tag
e0
0100
00
100
20.0
080.0
20.0
080.0
a,b
,d,e
,f,h
,j,k
,m,n
,oSi
gnifi
cant
diffe
renc
es(p
<0.
01).
c,g,
I,l Si
gnifi
cant
diffe
renc
es(p
<0.
05).
Basic Research—Technology
JOE — Volume 36, Number 9, September 2010
The main finding of the present study was that endoscopy at�64 magni-fication yielded the highest percentage of correct identification (66.9%)of root-end dentinal cracks compared with the other tested visual aids(44.1%-55.2%). Similar results were recently presented in a study thatassessed the identification of artificially created cracks in extractedhuman permanent incisors after root-end resection (7). That study re-ported the following enhanced accuracies of crack identification withincreasing magnification: 39% accuracy for unaided vision, 45% accu-racy for loupes (�3.3 magnification), 53% accuracy for the micro-scope (�10 magnification), and 58% accuracy for the endoscope(�35 magnification). The difference in accuracy among the four visu-alization techniques was significant (p = 0.0007). However, in contrastto the present study, Slaton et al (7) assessed if a specimen (root-endsurface) was correctly identified as having or not having a crack,without specific determination of the type and location of the crack.
A detailed analysis of the data of the present study with regard tothe identification of a specific type of crack showed that sensitivity wasalways better for complete canal cracks (52.6%-78.9%) than forincomplete canal cracks (42.2%-64.7%) and intradentin cracks(0%-20%). None of the intradentin cracks was detected with micros-copy, and only one intradentin crack (20%) was identified with endos-copy. Similarly, lower sensitivity of crack detection of intradentin cracks(36%) compared with incomplete canal cracks (73%) and completecanal cracks (97%) was reported in a previous experimental studycomparing endoscopy and SEM (9).
In the present study, the misinterpretation of incomplete canalcracks as complete canal cracks was found to range from 5.9% to15.7% and of complete canal cracks as incomplete canal cracksfrom 7.9% to 15.8%. In contrast, a complete canal crack or an incom-plete canal crack was never misinterpreted as an intradentin crack orvice versa. Interestingly, crack misinterpretation differed whencomparing microscopy with endoscopy. Complete canal cracks weremore frequently misinterpreted as incomplete canal cracks withmicroscopy than with endoscopy, whereas the misinterpretation ofincomplete canal cracks as complete canal cracks was higher withendoscopy than with microscopy. In addition, endoscopy �8 and�64 showed more false-positive crack identification (6.9% and12.4%) compared with microscopy �16 and �24 (each 4.8%). Infact, endoscopy �64 yielded relatively high false-positive results forincomplete canal cracks (13.7%) and intradentin cracks (40%).When the endoscope is used at this high magnification, the opticallens and light source are very close to the root-end surface (0.5-1mm), and grooves or surface irregularities caused by the resectionbur may produce a change in light reflection, creating the illusion ofa crack (8).
Slaton et al (7) also described an interesting finding when loadwas applied for artificially creating cracks. They reported that the dentinaround the area of strain became opaque or frosted in appearancebefore a crack developed. The authors speculated that these changeswere caused by the formation of many microscopic cracks that hadnot yet formed a macrocrack. This finding should heighten the clini-cian’s suspicion that a crack may be present. Studies about crack prop-agation have shown microcracking at the crack tip and crack opening(macrocracking) in the so-called ‘‘crack wake’’ (24, 25).
Staining (eg, with methylene blue) may not necessarily enhancethe detection of cracks because the dye cannot flow into craze linesunless there is a break in the surface. Once a crack has propagatedinto a fissure or fracture, these can be stained with dyes. A recent studyevaluated and compared crack identification using transilluminationand various dyes (8). The technique that provided the best discrimina-tion between cracked and noncracked resected roots was methyleneblue plus transillumination. In a clinical situation, however,
Detection of Dentinal Cracks After Root-end Resection 1567

TABLE 3. False-Positive Cracks Identified with Visual Aid but not Present in SEM
Microscope �16 Microscope �24 Endoscope �8 Endoscope �64
No. of additional cracks 7 7 10 18% false-positives (= n/145) 4.8a 4.8b 6.9 12.4ab
No. of additional complete canal cracks 2 1 1 2% false-positives (= n/38) 5.3 2.6 2.6 5.3No. of additional incomplete canal cracks 5 5 8 14% false positive (= n/102) 4.9c 4.9d 7.8 13.7cd
No. of additional intradentin cracks 0 1 1 2% false positive (= n/5) 0e 20.0 20.0 40.0e
a,bSignificant differences (p < 0.01).c,d,eSignificant differences (p < 0.05).
Basic Research—Technology
transillumination may be difficult to apply if the root end is level withthe bone after resection. Wright et al (8) suggested removing a smallamount of buccal bone overlying the root surface or transilluminatingthrough bone.
Whether radicular dentinal cracks can enlarge during functioningand in this way result in future leakage pathways or root fracturesremains to be investigated (20). Whether there is a need for extendingroot-end cavity preparation to include and to obturate canal cracksidentified at the resection level is a topic for future clinical research.
ConclusionsEndoscopy at �64 magnification yielded the highest percentages
of correct identification of root-end dentinal cracks (categories: allcracks, complete canal cracks, and incomplete canal cracks). Withrespect to the correct detection of a specific type of crack, completecanal cracks showed the highest sensitivity of identification with endos-copy at �64 magnification. The correct identification of intradentincracks was low with endoscopy and nonexistent with microscopy. Arelatively high number of false-positive incomplete canal cracks and in-tradentin cracks was registered with endoscopy at �64 magnificationcompared with the other visual aids.
AcknowledgmentThe authors thank Brigitte Megert, Department of Preventive,
Restorative and Pediatric Dentistry, University of Bern, for her helpwith the scanning electron microscopy evaluation.
References1. European Society of Endodontology. Quality guidelines for endodontic treatment:
consensus report of the European Society of Endodontology. Int Endod J 2006;39:921–30.
2. Kim S. Principles of endodontic microsurgery. Dent Clin N Am 1997;41:481–97.3. Rubinstein RA, Kim S. Short-term observation of the results of endodontic surgery
with the use of a surgical operation microscope and Super-EBA as root-end fillingmaterial. J Endod 1999;25:43–8.
4. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review.J Endod 2006;32:601–23.
5. Rubinstein RA, Kim S. Long-term follow-up of cases considered healed one yearafter microsurgery. J Endod 2002;28:378–83.
1568 von Arx et al.
6. Taschieri S, del Fabbro M, Testori T, et al. Endodontic surgery using 2 differentmagnification devices: preliminary results of a randomized controlled study.J Oral Maxillofac Surg 2006;64:235–42.
7. Slaton CC, Loushine RJ, Weller RN, et al. Identification of resected root-end dentinalcracks: a comparative study of visual magnification. J Endod 2003;29:519–22.
8. Wright HM, Loushine RJ, Weller RN, et al. Identification of resected root-enddentinal cracks: a comparative study of transillumination and dyes. J Endod2004;30:712–5.
9. von Arx T, Montagne D, Zwinggi C, et al. Diagnostic accuracy of endoscopy in peri-radicular surgery—a comparison with scanning electron microscopy. Int Endod J2003;36:691–9.
10. Zero DT, Rahbek I, Fu J, et al. Comparison of the iodide permeability test, thesurface microhardness test, and mineral dissolution of bovine enamel followingacid challenge. Caries Res 1990;24:181–8.
11. Roane J, Sabala C, Ducanson M. The ‘‘balanced force’’ concept for instrumentationof curved canals. J Endod 1985;11:203–11.
12. Cambruzzi JV, Marshall FJ, Pappin JB. Methylene blue dye. An aid to endodonticsurgery. Endo Report 1985;11:311–4.
13. Layton CA, Marshall JG, Morgan LA, et al. Evaluation of cracks associated with ultra-sonic root-end preparation. J Endod 1996;22:157–60.
14. Fleiss JL. Statistical methods for rates and proportions. 2nd ed. New York, NY: JohnWiley & Sons; 1981.
15. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York,NY: Psychology Press; 1988.
16. Altshul JH, Marshall G, Morgan LA, et al. Comparison of dentinal crack incidenceand of post removal time resulting from post removal by ultrasonic or mechanicalforce. J Endod 1997;23:683–6.
17. Adorno CG, Yoshioka T, Suda H. The effect of root preparation technique and instru-mentation length on the development of apical root cracks. J Endod 2009;35:389–92.
18. Calzonetti KJ, Iwanowski T, Komorowski R, et al. Ultrasonic root-end cavity prepa-ration assessed by an in situ impression technique. Oral Surg Oral Med Oral PatholOral Radiol Endod 1998;85:210–5.
19. Gray GJ, Hatton JF, Holtzmann DJ, et al. Quality of root-end preparation using ultra-sonic and rotary instrumentation in cadavers. J Endod 2000;26:281–3.
20. De Bruyne MAA, de Moor RJG. SEM analysis of the integrity of resected root apices ofcadaver and extracted teeth after ultrasonic root-end preparation at different inten-sities. Int Endod J 2005;38:310–9.
21. Morgan LA, Marshall JG. A scanning electron microscopic study of in vivo ultrasonicroot-end preparations. J Endod 1999;25:567–70.
22. Dang DA, Walton RE. Vertical root fracture and root distortion: effect of spreaderdesign. J Endod 1989;15:294–301.
23. Onnink PA, Davis RD, Wayman BE. An in-vitro comparison of incomplete root-fractures associated with three obturation techniques. J Endod 1994;20:32–7.
24. Nalla RK, Kinney JH, Ritchie RO. On the fracture of human dentin: is it stress- orstrain-controlled? J Biomed Mater Res 2003;67A:484–95.
25. Kruzic JJ, Nalla RK, Kinney JH, et al. Mechanistic aspects of in-vitro fatigue-crackgrowth in dentin. Biomaterials 2005;26:1195–204.
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
The Quality of Root Canal Preparation and Root CanalObturation in Canals Treated with Rotary versusSelf-adjusting Files: A Three-dimensional Micro-computedTomographic StudyZvi Metzger, DMD,*
†Raviv Zary, DMD,
†Raphaela Cohen, DMD,
†Ehud Teperovich, DMD,
†
and Frank Paque, DMD‡
Abstract
Aim: The study was designed to quantitatively evaluatethe quality of root canal preparation and root canal obtu-ration in canals treated with either rotary or self adjustingfiles, using three-dimensional micro–computed tomo-graphic (CT) analysis. Methodology: Pair-matchedroot canals were instrumented with either rotarynickel-titanium files or self-adjusting files following themanufacturers’ instructions. The area of the canal wallunaffected by the preparation procedure was analyzedusing before and after micro-CT images. Root canalobturation was done using lateral compaction withgutta-percha and AH26 (Dentsply-DeTrey, Konstanz,Germany). Teeth were scanned a third time, and theadaptation of the filling material to the canal wallswas evaluated three-dimensionally by micro-CT analysisand the area of canal wall untouched by the filling wasdetermined. The correlation between these two param-eters within each of the groups was studied using thePearson correlation test. Results: A high percentageof unaffected root canal walls (60% �14%) and areasuntouched by the root canal filling (45% � 15%) werefound in canals treated with rotary files. Both parame-ters were significantly smaller in canals treated withself-adjusting files (17%� 9% and 17%� 11%, respec-tively) (p < 0.01). No correlation was found betweenthese parameters within each of the groups. Conclu-sion: Within the limitations of the present study, theself-adjusting files allowed better cleaning and shapingand better adaptation of the root canal filling than thoseallowed by rotary files. (J Endod 2010;36:1569–1573)Key WordsMicroCT, obturation, root canal filling, SAF, self adjust-ing file
From the *Department of Endodontology, The Goldschleger Sc‡Department of Preventive Dentistry, Peridontology and Cariology,
Dr Ehud Teperovich, Dr Raphaela Cohen, and Dr Raviv Zary are etant to the same company.
Address requests for reprints to Dr Zvi Metzger, School of Dental Mac.il.0099-2399/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.003
JOE — Volume 36, Number 9, September 2010
Root canal obturation is an essential stage of root canal treatment aimed to seal theroot canal in order to prevent future bacterial contamination/recontamination of
the canal space (1). Many obturation methods have been introduced over the years,each attempting to provide a better seal of the root canal (2). All have in commonthe assumption that the root canal is properly cleaned and shaped before the obturationstage. It is assumed by all that if the root canal is not adequately prepared and if tissueremnants and debris are present along the walls, proper sealing may be jeopardized,even with the best root canal filling method (3, 4).
When simple, narrow, straight root canals with round cross-sections are consid-ered, most current rotary nickel-titanium file systems will adequately clean and shapethe canal with favorable results. The case is different in oval, flat, or curved rootcanals.
In flat root canals, rotary file systems often fail to adequately clean and shape thecanal, leaving ‘‘fins’’ that may have not been prepared (2–4). In such a case, even warmgutta-percha obturation methods will fail to adequately seal the root canal (4). Clinicalbuccolingual radiographs will fail to detect such discrepancy.
Micro–computed tomographic (CT) studies by Peters et al (6) have furtherextended the understanding of the limitations of rotary file systems. They clearly showedthat inadequate preparation also often occurs in curved root canals, even if they do nothave a flat cross-section. In upper molars treated with the ProTaper system (Dentsply-Maillefer, Ballaigues, Switzerland), 49% (�29%) of the canal wall was left untouched,even in the larger palatal canals (6). Again, two-dimensional, clinical periapical radio-graphs cannot disclose the discrepancies.
This led to the recent introduction of a new self-adjusting file (SAF), which notonly adapts itself longitudinally to a curved canal, as most rotary nickel-titanium filesdo, but also adapts itself to the cross-section of the canal (5). Rather than machiningeach canal into one with a circular cross-section, it removes an even dentin layerfrom all around the root canal, thus respecting the shape of a given root canal ratherthan imposing a circular cross-section on every canal no matter what its shape (5).Recent micro-CT analysis of root canals prepared with this new file indicated thatthis new technology allows for a higher percent of the root canal surface to beaffected by the procedure (5). The resulting apical size is usually at least equivalentto a #40 file.
hool of Dental Medicine, Tel Aviv University, Tel Aviv; †Redent-Nova Inc, Raanana, Israel; andUniversity of Zurich, Zurich, Switzerland.mployed by ReDent-Nova, manufacturer of the SAF file. Dr Zvi Metzger serves as a scientific consul-
edicine, Tel Aviv University, Ramat Aviv, Tel Aviv 69978, Israel. E-mail address: [email protected].
Root Canal Preparation and Obturation in Canals Treated with Rotary vs Self-adjusting Files 1569

Basic Research—Technology
Following the concept of the previously mentioned micro-CT anal-ysis methods, a new method for quantitative three-dimensional analysisof the adaptation of root canal filling material to the canal walls was de-signed. This new method was applied in the present study to quantita-tively evaluate and compare the results of instrumentation with an SAF tothose obtained with nickel-titanium rotary files.
Materials and MethodsExperimental Design
The study was designed to compare two instrumentation methodsusing two three-dimensional parameters: (1) the quality of root canalcleaning and shaping, as expressed by the root canal wall areaaffected/unaffected by the procedure, and (2) the quality of obturation,as expressed by the percent of the root canal wall area (after prepara-tion) touched/untouched by the root canal filling material.
TeethTeeth were selected from a large random collection of extracted
human teeth that were recently extracted for reasons unrelated to thepresent study and kept in 10% buffered formalin. Both three-dimensional images and two-dimensional cross-sections obtainedusing micro-CT scanning were available for each tooth in this collection.
Ten pairs of roots were selected based on matching root canalmorphology. These 20 roots included two mesial roots of lower molars,two distal roots of lower molars, six premolars, eight incisors, and twocanines. Pair selection was based on visual similarity in shape, size, flat-ness, and curvature of the root canals, as seen in a set of three-dimensional micro-CT images of each of the roots. The two roots ofeach pair were randomly assigned to one of the two treatment groups(rotary files or SAFs).
Root Canal Cleaning and ShapingTwo file systems were used: rotary nickel-titanium files (ProTaper,
Dentsply-Maillefer, Ballaigues, Switzerland) and SAFs (ReDent-NovaLtd, Ra’anana, Israel). Each instrument was applied following its man-ufacturer’s instructions.
Rotary FilesThe rotary files (ProTaper) were operated with a handpiece
attached to a speed- and torque-controlled motor (X-Smart,Dentsply-Maillefer) at 250 rpm. The sequence used was ProTaper S1,S2, F1, F2, and F3 with RC-Prep (Premier, Plymouth Meeting, PA)used as a chelator/lubricant with each file. The canal was irrigatedwith 5 mL 3% NaOCl between the instruments. A final flush with 5 mL17% EDTA was applied, followed by an additional flush with 5 mL3% NaOCl to remove the EDTA, and the canal was dried using paperpoints.
SAFThe SAF (ReDent) was operated for 4 minutes using a GentlePower
Lux 20LP KaVo handpiece, (KaVo, Biberach, Germany) adapted witha RDT3 head (ReDent-Nova, Raanana, Israel) (5). The micromotorrotation speed was set at 5,000 rpm, which resulted in an in-and-outoperation of 5,000 vibrations per minute with an amplitude of 0.4mm. The file was used with a manual in-and-out motion to the workinglength. Continuous irrigation was applied throughout the procedure(5) at 5 mL/min using a special irrigation apparatus (VATEA irrigationdevice, part of the SAF-System, ReDent); 3% NaOCl was used for irriga-tion during the first 3 minutes of the operation, followed by 1 minute of
1570 Metzger et al.
irrigation with 17% EDTA. A final flush with 5 mL 3% NaOCl was used toremove the EDTA, and the canal was dried using paper points.
Micro-CT Evaluation of the Root Canal PreparationBefore preparation and scanning, each experimental tooth was
mounted on scanning electron microscopy carriers (014001-T; Bal-Tec AG, Balzers, Liechtenstein) to allow exact repositioning in thescanning system. Specimens were scanned before and after prepara-tion by using a commercially available micro-CT system (mCT 40;Scanco Medical, Bruttisellen, Switzerland). Teeth were scanned at70 kV and 114 mA with an isotropic resolution of 18 mm. Althoughthe mounting device ensured almost exact repositioning of the spec-imens, superimposition was further calculated with newly developedsoftware (IPL Register 1.01, Scanco Medical), as previously reportedby Paque et al. (7). The final exact superimposition of the teethbefore and after preparation was with a precision better than onevoxel.
Individual root canal models were reconstructed up to the levelof the cementoenamel junction using specially developed software(IPL V5.06B, Scanco Medical). Superimposition of the root canalsbefore and after preparation enabled visualization and quantitativelythree-dimensional evaluation of the amount of un-instrumentedareas (Fig. 1). This parameter was expressed as a percentage ofthe number of static surface voxels of the total number of surfacevoxels.
Root Canal ObturationRoot canal obturation was performed using the lateral compac-
tion technique with gutta-percha and AH26 sealer (Dentsply-DeTrey,Konstanz, Germany). A gutta-percha master cone (DiaDent, Almere,The Netherlands) was fitted with tug-back in each root canal. Sealerwas placed into the canal using a lentulo spiral followed by insertionof the master cone to the predetermined working length. Nickel-titanium finger spreaders (Dentsply-Maillefer) were used to conductthe lateral compaction using XXF/ XF accessory cones (Sure-Endo,Paris, France). When no additional cones could be inserted, thegutta-percha mass was cut off 1 mm apical to the canal orifice usinga heated plugger (Dentsply-Maillefer). The freshly cut surface wasvertically condensed using a cold plugger (Dentsply-Maillefer). Thesealer was then allowed to set for 4 days at 37�C and 100%humidity.
Evaluation of Obturation Quality by Three-DimensionalMicro-CT Analysis
Each tooth was subjected to a third micro-CT scan as detailedearlier. Differences in the radiopacity between the root canal fillingand the root dentin allowed differentiation between the two. For eachroot, the filling material was three-dimensionally reconstructed andsuperimposed with the image of the root canal after cleaning andshaping. Superimposition of root fillings and the prepared root canals(third and second scanning) allowed a three-dimensional analysis ofthe areas of the root canal surface, which were touched/untouchedby the root canal filling.
Statistical MethodsThe area unaffected by instrumentation and the area untouched by
the root canal filling of the two instrumentation groups were comparedwith each other using the Student t test. The one-tailed Pearson corre-lation test was used to study the correlation within each group betweenthe unaffected surface in a given root canal and the area untouched bythe root canal filling in the same canal.
JOE — Volume 36, Number 9, September 2010

Figure 1. Three-dimensionally reconstructed micro-CT images of root canal preparation and obturation. (A) A flat root canal prepared with the SAF file.(B) A flat root canal prepared with a rotary file. (C) A good root canal filling adaptation with 98.1% of the canal wall in contact with the root canal fillingmaterial. (D) A poor root canal filling adaptation with only 68.9% of the root canal wall in contact with the root canal filling material. Note the unin-stumented lingual ‘‘fin’’ in B that was most probably full of debris, which prevented the sealer from flowing into it in D. Red: root canal surface beforetreatment. Blue: root canal surface post-treatment. Yellow: area touched by the root canal filling. Right, in each panel: buccal view, left: distal view.(resolution = 18 mm). (This figure is available in color online at www.aae.org/joe/.)
Basic Research—Technology
ResultsPercent Root Canal Surface Unaffected by Root CanalPreparation
The root canal surface unaffected by root canal preparation wascalculated as a percent of the root canal surface area before preparation(Table 1 and Fig. 1A and B). A wide range of this three-dimensionalparameter was recorded, between 5.3% and 76.6%. The mean unaf-fected area was 16.7% (�8.9%) and 60.2% (�13.6%) in the selfSAF and rotary file groups, respectively (Fig. 2).
JOE — Volume 36, Number 9, September 2010 Root Canal Prep
Percent Root Canal Surface After Preparation Untouchedby the Root Canal Filling Material
The root canal surface untouched by the root canal filling mate-rial was calculated as a percent of the root canal surface area afterroot canal preparation (Table 1 and Fig. 1C and D). A wide range ofthis parameter was recorded, between 1.9% and 75.1%. The meanarea untouched by the root canal filling was 17.0% (�11.0%)and 44.6% (�14.5%) in the SAF and rotary file groups, respectively(Fig. 2).
aration and Obturation in Canals Treated with Rotary vs Self-adjusting Files 1571

TABLE 1. A Three-Dimensional Micro-CT Analysis of the Quality of Cleaning and Shaping and Root Canal Filling Adaptation to the Canal Walls
Pair # Type of canal MethodArea unaffected by rootcanal preparation (%)
Area untouched by rootcanal filling (%)
1 R-S RF 66.7 28.9SAF 14.9 1.9
2 R-S RF 64.4 64.3SAF 7.1 15.8
3 R-S RF 49.4 42.4SAF 20.8 8.5
4 R-C RF 28.0 38.8SAF 33.8 23.5
5 R-C RF 76.6 37.6SAF 5.3 5.8
6 F-S RF 63.0 44.1SAF 21.6 30.5
7 F-S RF 73.0 75.1SAF 5.8 15.1
8 F-S RF 60.9 47.0SAF 20.2 8.0
9 F-S RF 59.3 37.1SAF 21.1 29.4
10 F-C RF 61.1 31.1SAF 15.9 31.2
R-S, round cross-section, straight; R-C, round cross-section, curved; F-S, flat cross-section, straight; F-C, flat cross-section, curved; RF, Rotary files.
Basic Research—Technology
Correlation Between the Area Unchanged by the RootCanal Preparation and the Area Untouched by the RootCanal Filling
No correlation was found within each of the groups between thepercent of the area unaffected by the root canal preparation and thearea untouched by the root canal filling.
DiscussionMany obturation methods are used today, ranging from traditional
lateral compaction to a variety of heat-softened gutta-percha tech-niques. All are aimed at providing a good adaptation of the root canalfilling material to the canal walls, thus ensuring an adequate seal that
0
20
40
60
80
100
Rotary FileSelf Adjusting File
Area Unaffected by C&S Area Untouched by RCF
Perc
ent
Figure 2. Comparison between the quality of the root canal preparation andadaptation of the root canal filling in root canals treated with rotary files orSAFs. The quality of root canal preparation is expressed as a percent of theroot canal surface that was unaffected by the file. Adaptation of the root canalfilling is expressed as a percent of the root canal surface after preparation thatwas untouched by the root canal filling. RCF, root canal filling; C&S, cleaningand shaping.
1572 Metzger et al.
will prevent bacterial contamination/re-contamination of the root canalsystem.
When applied in adequately prepared canals with no tissueremnants and with a clean, prepared dentin surface, this goal may berather easily achieved. The case may be different in root canals thatwere inadequately cleaned and shaped. Tissue and debris remainingin parts of the canal that were unaffected by the procedure may presenta barrier that does not allow for the root canal filling to intimately touchthe root canal wall, thus forming the weakest link in the chain of stepsaimed to properly seal the canal.
This may happen in curved canals in which the files failed to touchsome of the walls (6) but constitutes an even greater problem in the caseof flat or ribbon-shaped canals. In these canals, a rotary nickel-titaniumfile alone may be unable to adequately prepare the canal (Fig. 1B andD). Its action may result in a canal prepared to accommodate a certainthickness of master cone or root canal filling but may allow for buccaland/or lingual ‘‘fins’’ full of tissue remnants and debris to remainuntouched (3, 4). These buccal and/or lingual defects may gounobserved in regular periapical radiographs; the root canal fillingthat is present in the central part of the canal will most likely maskthem. Bacterial retention in or penetration into and through thesedefects may result in endodontic failure in an apparentlyradiographically acceptable case.
Even though the relation between the quality of cleaning andshaping and the potential of the root canal filling to intimately touchthe walls of the prepared root canal is readily understood, it has never,to the best of our knowledge, been established quantitatively for thewhole canal. A study aimed to investigate the correlation between theseparameters calls for a high variety of root canal cleaning and shapingscores that could later be analyzed against root canal filling adaptationto the walls of the same canals.
The roots selected for the present study intentionally includeda random variety of root canal morphologic shapes. This was doneso that a wide spectrum of cleaning and shaping results would beavailable for analysis. These roots ranged from simple straight rootcanals with a round cross-section, which were likely to score highin effective cleaning and shaping using any file system, to curved rootsor those with flat root canals that were likely to result in a higher
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
percent of root canal wall unaffected by rotary nickel-titanium files(5, 6).The present study clearly showed that the two instrumentationsgroups differed from each other. This difference was found in boththe quality of cleaning and shaping, as expressed by the percent ofthe root canal surface affected/unaffected by the procedure, and inthe quality of root canal obturation, as expressed by the percent ofthe canal wall that is/is not in intimate contact with the root canal fillingmaterial. Treatment with the SAF allowed for better results with bothparameters (Fig. 2).
No correlation could be found between the two parameters withineach group. This could result from the relatively small number of spec-imens in each of the groups. Further studies with larger groups may beneeded to establish such correlation.
Lateral compaction was used in the present study because it is themost commonly used obturation method. It may be of interest to test thesame concept with heat-softened gutta-percha obturation methods,which are commonly expected to provide a better adaptation to thecanal walls; nevertheless, this was beyond the scope of the present study.
Micro-CT scanning has been used previously to evaluate the qualityof root canal fillings. Jung et al (7) have shown that the root canal fillingmay be differentiated from the canal wall in a micro-CT scan using digitalroot slices. Former studies of root canal obturation quality commonlyused two-dimensional analysis of either root slices (7–10) or digitalcross-sections generated from micro-CT scans (7). These could atbest serve as a semiquantitative representation of what happens in thecanal at large.
A three-dimensional analysis of micro-CT images, similar to theone used in the present study, was first applied by Zakizadeb et al(11) to evaluate intraorifice barriers. It was also recently applied byHammad et al (12) for the analysis of the volume of voids and gapspresent in root canal fillings.
The present study was, to the best of our knowledge, the first to usea three-dimensional micro-CT analysis to quantitatively measure theadaptation of the root canal filling material to the walls in the wholecanal. As such, it provides far more comprehensive information aboutthe adaptation of the whole root canal filling, which is unaffected by thechoice of the plane in which a given section or digital cross-sectionhappens to be.
JOE — Volume 36, Number 9, September 2010 Root Canal Prep
ConclusionsA micro-CT-based quantitative three-dimensional method for
analysis of root canal filling adaptation to the canal walls was presented.It may serve as a useful tool to study and compare the quality of rootcanal fillings. Within the limitations of the present study, the SAFs al-lowed better cleaning and shaping and better adaptation of the rootcanal filling than those allowed by rotary files.
AcknowledgmentThe contribution of Mr Ofer Shalev to this study is recognized
and highly appreciated.
References1. Ricucci D, Lin LM, Spangberg LSW. Wound healing of apical tissues after root canal
therapy: a long-term clinical, radiographic, and histopathologic observation study.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:609–21.
2. Whitworth J. Methods of filling root canals: principles and practice. Endod Topics2005;12:2–24.
3. Wu M-K, Wesselink PR. A primary observation on the preparation and obturation inoval canals. Int Endod J 2001;34:137–41.
4. De-Deus G, Gurgel-Filho ED, Magalhaes KM, et al. A laboratory analysis of gutta-percha-filled area obtained using Thermafil, System B and lateral condensation.Int Endod J 2006;39:378–83.
5. Metzger Z, Teperovich E, Zary R, et al. Respecting the root canal: a new concept ofa Self Adjusting File (SAF). J Endod 2010;36:679–90.
6. Peters OA, Peters CI, Schonenberger K, et al. ProTaper rotary root canal prepara-tion: effects of root canal anatomy on final shape analyzed by micro CT. Int Endod J2003;36:86–92.
7. Jung M, Lommel D, Klimek J. The imaging of root canal obturation using micro-CT.Int Endod J 2005;38:617–26.
8. Paque F, Laib A, Gautschi H, et al. Hard-tissue debris accumulation analysis by high-resolution computed tomography scans. J Endod 2009;35:1044–7.
9. Ardila CN, Wu M-K, Wesselink PR. Percentage of filled canal area in mandibularmolars after conventional root canal instrumentation and after noninstrumentationtechnique (NIT). Int Endod J 2003;36:591–8.
10. Wu M-K, van der Sluis LWM, Wesselink PR. A preliminary study of the percentage ofthe gutta-percha-filled area in the apical canal filled with vertically compacted warmgutta-percha. Int Endod J 2002;35:527–35.
11. Zakizadeh P, Marshal SJ, Hoover CI, et al. A novel approach in assessment coronalleakage of intraorifice barriers: a saliva leakage and micro-computed tomographyevaluation. J Endod 2008;34:871–5.
12. Hammad M, Qualtrough A, Silikas N. Evaluation of root canal obturation: a three-dimensional in vitro study. J Endod 2009;35:541–4.
aration and Obturation in Canals Treated with Rotary vs Self-adjusting Files 1573

Basic Research—Technology
Subcutaneous Connective Tissue Reaction to MethacrylateResin–based and Zinc Oxide and Eugenol SealersOsvaldo Zmener, DDS,* Cornelis H. Pameijer, DMS, MScD, DSc, PhD,†
Gabriel A. Kokubu, DDS,* and Daniel R. Grana, DVM*
Abstract
Introduction: An evaluation was made of the connec-tive tissue reaction in rats after subcutaneous implanta-tion of methacrylate resin-based sealers (EndoREZ[Ultradent Products, Inc, South Jordan, UT] with a poly-merization accelerator and RealSeal [Sybron DentalSpecialties, Orange, CA]) and Pulp Canal Sealer (SybronDental Specialties), a zinc oxide and eugenol-based sealerused as the control. Methods: Silicone tubes containingthe test materials were implanted in 24 Wistar rats. Solidsilicone rods of the same size served as the negativecontrols. After 10, 30, and 90 days, the animals (n = 8per period) were euthanized and the implants withsurrounding tissues dissected and processed for routinehistological evaluation. A four-category evaluationsystem was used to measure and record the microscopicobservations according to the thickness of a fibrouscapsule, the vascular changes, and the various types ofinflammatory cells. Results: Initially, a severe inflamma-tory reaction was observed of the soft tissues in directcontact with both EndoREZ/Accelerator and Real Seal.The severity decreased over time and was resolved atthe end of the experiment. Pulp Canal Sealer showeda severe tissue reaction for all observation periods. Thenegative controls showed an initial mild to moderateinflammatory reaction. After 30 days, healthy fibrousconnective tissue was observed, which increased overtime. After 10 days, no statistically significant differencesbetween the experimental groups were observed. After90 days, EndoREZ and RealSeal were statistically signif-icantly less toxic than Pulp Canal Sealer (p > 0.05).Conclusions: After 90 days, both methacrylate resin-based sealers were considered biologically acceptablewhen implanted in subcutaneous connective tissues ofthe rat. Pulp Canal Sealer remained toxic for the durationof the study. (J Endod 2010;36:1574–1579)Key WordsBiocompatibility, endodontics, methacrylate-basedsealers, tissue response
From the *School of Dentistry, University of El Salvador, BuenosSupported in part by Ultradent Dental Products Inc.Address requests for reprints to Dr Cornelis H. Pameijer, 10 Hig
0099-2399/$0 - see front matterCopyright ª 2010 American Association of Endodontists.
doi:10.1016/j.joen.2010.06.019
1574 Zmener et al.
The current concept among clinicians is that after complete debridement, total oblit-eration of the root canal space with a biocompatible material constitutes the key
factor for successful endodontic therapy (1). Different materials have been advocatedfor filling root canals; gutta-percha cones complemented with a sealer cement is themost widely used (2). During the last decade, methacrylate resin-based sealers(MRBSs) have gained popularity for root canal obturation (3). Preliminary reportshave shown that two well-established MBRSs (ie, EndoRez [ER; Ultradent Products,Inc, South Jordan, UT] and RealSeal (RS; Sybron Dental Specialties, Orange, CA),formerly Epiphany, are both well tolerated by living tissues (4–7) and have shownpromise for in vivo human clinical trials (8–10). More recently, an ER Accelerator(ACC, Ultradent Products Inc.) has been introduced. The ACC is composed oftriethylene glycol dimethacrylate, tertiary amines, and a proprietary ingredient. Thetechnique the manufacturer recommends is the following. When the master gutta-percha cone has been placed to length, two or three #20 to #25/.02 taper accessorycones dipped in ACC are harpooned in the sealer and pushed into the canal space asfar as possible. The combination of ER and ACC accelerates the polymerization ofthe sealer, thus allowing for an immediate continuation of the coronal restoration. Italso prevents dislodgement of the obturating material when a post space is preparedimmediately after obturation, potentially causing early bacterial leakage (11).
Previous reports (12, 13) have shown that certain components from methacrylateresin-based materials may remain unpolymerized even after setting and can subse-quently be released from the resin matrix. When the sealer is accidentally extrudedthrough the apex or through a lateral canal, which is not an uncommon experiencein endodontics (14), the unpolymerized components may be toxic to the periapicaltissues. Although the biocompatibility of ER and RS has been investigated (4–7), theeffect of ER/ACC in contact with living tissues and compared with RS has not beenreported yet. Therefore, the purpose of this study was to evaluate thebiocompatibility of ER/ACC and RS and to compare them with Pulp Canal Sealer(PCS, Sybron Dental Specialties), a zinc oxide and eugenol-based sealer, when im-planted subcutaneously in connective tissue of rats.
Materials and MethodsThe protocol of this study was approved by the Research Ethics Committee of the
Argentine Dental Association. Autoclaved silicone tubes closed at one end (Raholin SRL,V. Madero, BA, Argentina) and 10-mm long with an internal diameter of 1 mm werefilled flush with freshly prepared ER/ACC, RS, or PCS (positive control). Solid siliconerods (SIRODs) of the same size as the tubes were used as negative controls. ER alonewas not tested because this had been done previously under similar conditions (5). Themethacrylate resin–based sealer samples were prepared in such a way that the
Aires, Argentina; and †University of Connecticut School of Dental Medicine, Farmington, CT, USA.
hwood, Simsbury, CT 06070. E-mail address: [email protected].
JOE — Volume 36, Number 9, September 2010

TABLE 1. Severity of Tissue Reaction to the Test Materials
ER/ACC RS PCS SIROD
Days n NO MI MO SE NO MI MO SE NO MI MO SE NO MI MO SE
10 8 0 0 0 8 0 0 0 8 0 0 0 8 0 6 2 030 8 0 0 8 0 0 0 8 0 0 0 0 8 8 0 0 090 8 7 1 0 0 6 2 0 0 0 0 0 8 8 0 0 0
NO, no reaction; MI, mild reaction; MO, moderate reaction; SE, severe reaction.
Basic Research—Technology
formation of an oxygen-inhibited layer was prevented. The sealerswere prepared under aseptic conditions according to the followingmethod.
In group ER/ACC (n = 8), the experimental design necessitateda slight modification of the manufacturer’s recommendations. ER wasinjected through an automixing tip in a glass syringe measuring25-mm long with a 5-mm internal diameter (De Luca SA, Buenos
Figure 1. (A-F) Representative specimens of ER/ACC, RS, and PCS at the 10-day ocontact (hematoxylin and eosin (H&E), original magnification �40). (A) A highercontact with the sealer (black arrow) and a severe granulomatous tissue reaction wseen (H&E, original magnification�100). (C) RS: a low magnification of tissue/matthe outlined area in C. A thick layer of necrotic tissue in direct contact with the seacontaining many newly formed capillaries (white arrow) can be seen (H&E, originalcontact (H&E, original magnification �40). (F) A higher magnification of the areaa severe granulomatous tissue reaction (H&E, original magnification �150). (Thi
JOE — Volume 36, Number 9, September 2010 Su
Aires, Argentina). Two size #40 gutta-percha cones dipped in ACCwere subsequently inserted in the sealer and left for 3 secondseach after which they were removed. The sealer was then immediatelyinjected into the silicone tubes through a 30-G needle. The procedurewas repeated using a new syringe for each animal.
In group RS (n = 8), the sealer was extruded through an automix-ing tip attached to the two-barrel delivery syringe directly into a plastic
bservation period. (A) ER/ACC: a low-power magnification of tissue/materialmagnification of the outlined area in A. A thin band of necrotic tissue in directith dark material particles and newly formed capillaries (white arrow) can be
erial contact (H&E, original magnification�40). (D) A higher magnification ofler (black arrow) is present. Below it, a severe granulomatous tissue reactionmagnification�100). (E) PCS: low magnification of the area of tissue/materialof tissue/material contact in E showing extruded dark particles surrounded bys figure is available in color online at www.aae.org/joe/.)
bcutaneous Connective Tissue Reaction to Methacrylate Resin–based Sealer 1575

Basic Research—Technology
syringe, which in turn delivered the mixture through a 30-G needle intothe silicone tube.In group PCS (n = 8), the sealer was prepared on a glass slab ac-cording to the manufacturer’s recommendations. The mixture wasloaded in a plastic syringe and injected into the silicone tube thougha 30-G needle.
Excess material was removed from the open end of the tubes witha sterile plastic instrument. After preparation, the samples were imme-diately implanted in the subcutaneous connective tissues of white maleWistar rats weighing approximately 200 g each. The husbandry andmanagement of the animals met the requirements of the ISO 10993–1 (1992) and ISO 10993-2 (1992) standards (15, 16) as well as theInternational Regulatory Requirements for the Care and Use ofLaboratory Animals (17). All surgical procedures were performedunder strict aseptic conditions. After anesthesia through the intraperi-toneal administration of ketamine chloride (14 mg/kg body weight)and acepromazine (10mg/kg body weight), the dorsal skin was shaved
Figure 2. (A-F) A representative sample of ER/ACC, RS, and PCS of the 30-day o(H&E, original magnification �80). (B) A higher magnification of the outlined aretissue concentration (black arrow). Below it is an artifact (ART) within an area oftissue/material contact (H&E, original magnification �40). (D) A higher magnificmaterial particles can be seen in direct contact with the sealer (black arrow). Belowmagnification�150). (E) PCS: a low power of tissue/material contact (H&E, origincles within a severe granulomatous tissue reaction. Note the presence of numerous(This figure is available in color online at www.aae.org/joe/.)
1576 Zmener et al.
and disinfected with 10% iodine-povidone solution (Phoenix SAIC, BA,Argentina). Four approximately 18-mm-long incisions were madethrough the dermis with a scalpel and further prepared by blunt dissec-tion. Subsequently, one sample of each of the four groups was carefullyplaced into the pocket. A distance of at least 20 mm between the sampleswas present to avoid interference of tissue response between two mate-rials. Finally, the wounds were closed with silk sutures, and the animalswere maintained on a regular diet and water ad libitum. Eight animalswere euthanized after 10, 30, and 90 days with an anesthetic overdoseresulting in eight samples per group per time period.
The implants with surrounding tissues were dissected and fixed in10% neutral buffered formalin (pH 7.4). After 48 hours of fixation, thesamples were processed for routine histological evaluation. Paraffinblocks were oriented parallel to the long axis of the tubes and longitu-dinal serial sections of approximately 7-mm thick were cut from themiddle of the implants and stained with hematoxylin and eosin. To eval-uate the tissue response, three sections of the center of each specimen
bservation period. (A) ER/ACC: a low magnification of tissue/material contacta in A. In direct contact with the sealer, there is a dense fibrogranulomatousfat cells (H&E, original magnification �150). (C) RS: a low magnification ofation of the outlined area in C. A thick granulomatous zone containing many
it is a number of wide newly formed capillaries (white arrow) (H&E, originalal magnification�40). (F) A higher magnification of E showing material parti-wide newly formed capillaries (arrows) (H&E, original magnification �150).
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
were analyzed and digitally photographed at different magnificationsunder a light microscope. All sections were analyzed independently,and two trained evaluators who were blind to the study scored the tissuereactions using the following criteria: NO: no reaction, fibrous-capsuleformation, and absence of inflammatory cells; MI: a mild reaction andthe presence of a fibrous-capsule formation with few inflammatorycells; MO: a moderate reaction and fibrous-capsule formation withthe presence of polymorphonuclear leukocytes, lymphocytes, plasmo-cytes, and macrophages; and SE: a severe reaction and the presence oflarge accumulations of polymorphonuclear leukocytes, lymphocytes,plasmocytes, macrophages, foreign-body giant cells, and congestedcapillaries. Before the analysis, both evaluators were calibrated byhaving them analyze a set of 70 similar but unrelated slides displayingvarious types of inflammatory cells to endodontic sealers. In case ofFigure 3. (A-F) A representative sample of ER/ACC, RS, and PCS at the 90-day obsshowing extrusion (ES) of the sealer (H&E, original magnification �40). (B) A higconnective tissue encapsulation free of inflammatory cells is present (black arrow)fication �850). (C) RS: a low magnification of tissue/material contact (H&E, origiNote the presence of a thick fibrous connective tissue capsule (arrow). A few inflamm(H&E, original magnification�850). (E) PCS: an overview of the area of tissue/mategranulomatous tissue slightly invaginated within the lumen of the tube (black arrowa fibrous connective tissue (arrow) that appeared to isolate the inflammatory reacfigure is available in color online at www.aae.org/joe/.)
JOE — Volume 36, Number 9, September 2010 Su
a disagreement between the evaluators, the sample under discussionwas analyzed jointly until a consensus was reached. Data were analyzedby the Wilcoxon signed rank test to determine if there was a statisticallysignificant difference between materials at each observation period. Thetotal effect of time and material upon the tissue reaction was analyzedusing the Kruskal-Wallis and the Dunn test. The significance level wasset at p < 0.05. A sealer was considered to be biologically acceptablewhen tissue reactions were recorded as NO to MI.
ResultsOne animal from the 10-day time period had to be excluded from
the study and was replaced with another undergoing the same implanta-tion procedures. Macroscopic examination showed that wound healing
ervation period. (A) ER/ACC: an overview of the area of tissue/material contacther magnification of A. In contact with the extruded material, a dense fibrous. The white arrow indicates a wide newly formed vessel (H&E, original magni-nal magnification �40). (D) A higher magnification of the outlined area in C.
atory cells can be seen within the capsule as well as in the surrounding tissuesrial contact showing numerous material particles (white arrow) surrounded by) (H&E, original magnification�40). (F) A higher magnification of E showingtion from the surrounding tissues (H&E, original magnification �850).(This
bcutaneous Connective Tissue Reaction to Methacrylate Resin–based Sealer 1577

Figure 4. (A) A representative specimen of SIRODs after the 10-day obser-vation period. In contact with the material (empty space), there is a moderatefibrogranulomatous tissue (black arrow) with inflammatory cells and newlyformed capillaries (H&E, original magnification �100). (B) A representativespecimen of SIRODs after 90 days. In contact with the material (empty space),a thick dense fibrous connective encapsulation (arrow) without inflammatorycells can be seen (H&E, original magnification�850).(This figure is availablein color online at www.aae.org/joe/.)
Basic Research—Technology
was satisfactory at all observation periods. Histological evaluationshowed that the implants were surrounded by fibrous connective tissueof irregular thickness. It could be easily distinguished from the tissuereaction at the site where the tissues were in direct contact with thetest material. The severity of tissue reaction is presented in Table 1.After 10 days, the tissue reaction to ER/ACC, RS, and PCS wasscored severe and was extensively dispersed around the end of the tubes(Figs. 1A-F). The majority of ER/ACC samples with direct tissue contactpresented with an inflammatory reaction with slight invagination intothe lumen of the tubes. Some ER/ACC and RS samples exhibiteda thin necrotic zone in the direct contact area. Each group displayedmany newly formed vessels and randomly dispersed dark particles,which appeared to have been released from the implanted materials.A mild to moderate reaction was observed in SIROD implants.
After 30 days, the intensity of the inflammatory reaction to ER/ACCand RS decreased slightly and was scored as moderate (Fig. 2A-D). Indirect tissue contact, both materials displayed a fibrogranulomatoustissue, which appeared less dispersed and showed a tendency to be sur-rounded by a fibrous tissue containing many inflammatory cells. Incontact with PCS, a persistent severe granulomatous tissue invaginationcontaining many dark particles was observed. This granulomatous reac-tion was surrounded by an incipient layer of fibrous tissue, which wasfree of inflammatory cells (Fig. 2E and F). In contact with SIRODs, therewas a thin fibrous connective tissue containing a few inflammatory cells.
After 90 days, some ER/ACC samples showed extrusion of the mate-rial into the surrounding tissues. In seven samples, a thick dense andmature fibrous tissue capsule (approximately 70- to 90-mm thick) freeof inflammatory cells was present (Fig. 3A and B), whereas only onesample had a mild tissue reaction. The RS samples showed a dense fibrouscapsule (50- to 80-mm thick) without inflammatory cells, whereas twocases were scored as mild with a few inflammatory cells still persistingwithin the capsule (Fig. 3C and D). PCS samples exhibited a severe persis-tent granulomatous tissue reaction containing necrotic areas as well asrandomly distributed inflammatory cells. Particles of the material wereobserved at the end and within the lumen of the tubes in all samples.Higher magnifications showed the granulomatous tissues to be isolatedby a thick fibrous tissue encapsulation. Many newly formed capillariesand a high concentration of acute and chronic inflammatory cells werealso seen (Fig. 3E and F). A thick dense fibrous connective tissue, freeof inflammatory cells, was observed in all SIROD samples (Fig. 4).
The Wilcoxon signed rank test showed no statistically significantdifferences (p > 0.05) between the reaction to ER/ACC, RS, and PCSat the 10-day observation period. After 30 days, no statistical differenceswere found between ER/ACC and RS (p > 0.05), whereas both ER/ACCand RS significantly differed from PCS (p < 0.05). For both periods, ER/ACC, RS, and PCS differed significantly from SIRODs. After 90 days, ER/ACC and RS differed significantly from PCS (p < 0.05) but not from SI-RODs, whereas PCS remained significantly different from SIRODs. Theeffect of time for ER/ACC and RS showed that the 10 and 30 days differedsignificantly (p < 0.05) from the 90-day observation period. However,no significant differences (p > 0.05) were observed for PCS between alltime intervals.
DiscussionThe implantation of endodontic filling materials into subcutaneous
connective tissue of rats is a valid screening method for testing biocom-patibility (18, 19). PCS was used as the positive control because itstoxicity has been previously determined by in vitro (20, 21) and invivo experiments (22, 23). SIRODs were used as the negative controlbecause they have been proven to be biocompatible (5, 6, 24, 25),a finding that was confirmed in this study. The initial inflammatory
1578 Zmener et al.
reaction of SIRODs may be a consequence of the surgical trauma.This subsided rapidly, and after 90 days a well-organized healthy densefibrous tissue free of inflammatory cells was observed. The biocompat-ibility of ER has previously been tested (4–6); however, theincorporation of the ACC changes not only the original chemicalcomposition of ER but also gives the sealer a shorter setting time; anevaluation of the toxicity is therefore essential to determine its safety.
The preparation of ER/ACC and RS samples was performed in sucha way that no oxygen-inhibited layer was formed. Oxygen inhibits free-radical polymerization of resin-based materials yielding an uncuredsurface layer (26, 27), which is of particular concern for MBRSbecause it greatly affects the outcome in toxicity tests. Elution ofuncured chemical components from the oxygen-inhibited layer is oneof the main causes for tissue damage. However, severe reactionswere observed for ER/ACC and RS at the short-term period, revealingthat even after setting they still are an irritant. As has been shown(28), unreacted monomer persists in polymerized methacrylate resins.These unreacted monomers (28) undergo a rapid elution and theleaching of these unbound molecules (29), and other componentscaused the severe inflammatory reactions observed after 10 days. Thesefindings are consistent with those of Costa et al (30, 31) and aresupported by previous experiments of Ferracane and Condon (12)
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
who found that the loss of components from a methacrylate resin-basedmaterial in a water-based medium in vitro is initially rapid and, there-fore, a similar behavior can be expected in vivo. It is significant to notethat the initial severe reaction decreased over time and had beenresolved at the end of the experiment although a few persistent inflam-matory cells still remained adjacent to RS. After the rapid initial loss, thematerial depletes progressively slower over time (12), thus causing lessirritation. Therefore, the setting time is significant with respect to irri-tation. ER/ACC sets in 7 minutes, RS in 25 minutes, and PCS in 260minutes (Zmener and Pameijer, unpublished data, 2009). The fastersetting of ER/ACC could be a contributory factor in reducing the releaseof components, in effect locking in potential irritants (12).The tissue reaction to PCS was severe at all observation periodsand is most likely caused by unreacted eugenol, which is highly toxicto tissues (32). Our findings for PCS are in agreement with otherswho reported that, like other zinc oxide and eugenol-based sealers(33–35), PCS reacted toxic in cell cultures (20, 21, 36) and incontact with living tissues (22, 37–39). However, the results for ER/ACC or RS disagree with those of Scarparo et al (39) who showedintense tissue reactions to ER. Their observations did not extend beyond60 days, however. In the study reported here, a 90-day observationperiod was used. Longer time periods allow more time for elution ofcomponents causing a depletion of chemical components that arepotential irritants. On the other hand, shortening of setting time maycontribute to a lower output of uncured components from ER as shownhere. Within the limitations of this study, it was concluded that ER/ACCand RS exhibited similarly and were both well tolerated by the subcuta-neous connective tissue of rats after 90 days of implantation. PCS,however, remained toxic even after a 90-day observation period.
AcknowledgmentDr. Pameijer is a consultant for Ultradent Products Inc.
References1. Nguyen TN. Obturation of the root canal system. In: Cohen S, Burns RC. Pathways of
the Pulp. 4th ed. St Louis: Mosby; 1987:183–94.2. Taintor JF, Ross PN. Opinions and practices of American Endodontic Diplomates.
Dent J 1978;44:321–5.3. ADA Council of Scientific affairs. Statement on posterior resin-based composites.
ADA Council on Dental Benefit Programs. J Am Dent Assoc 1998;129:1627–8.4. Louw NP, Pameijer CH, Norval G. Histopathological evaluation of a root canal sealer
in subhuman primates. J Dent Res 2001;80:654.5. Zmener O. Tissue response to a new methacrylate-based root canal sealer: preliminary
observations in the subcutaneous connective tissue of rats. J Endod 2004;30:348–51.6. Zmener O, Banegas G, Pameijer CH. Bone tissue response to a methacrylate-based
endodontic sealer: a histological and histometric study. J Endod 2005;31:457–9.7. Sousa CJA, Montes CRM, Pascon EA, et al. Comparison of the intraosseous biocom-
patibility of AH Plus, EndoREZ and Epiphany root canal sealers. J Endod 2006;32:656–62.
8. Zmener O, Pameijer CH. Clinical and radiographic evaluation of a resin-based rootcanal sealer. Am J Dent 2004;17:19–22.
9. Zmener O, Pameijer CH. Clinical and radiographical evaluation of a resin-based rootcanal sealer: a 5-year follow-up. J Endod 2007;33:676–9.
10. Cotton TP, Schindler WG, Schwartz SA, et al. A retrospective study comparing clinicaloutcomes after obturation with Resilon/Epiphany or gutta-percha/Kerr sealer.J Endod 2008;34:789–97.
11. Zmener O, Pameijer CH, Alvarez Serrano S. Effect of immediate and delayed postspace preparation on coronal bacterial microleakage in root canals obturatedwith a methacrylate-based sealer with an without accelerator. An ex vivo study.Am J Dent 2010;23:116–20.
JOE — Volume 36, Number 9, September 2010 Su
12. Ferracane JL, Condon JR. Rate of elution of leachable components from composite.Dent Mat 1990;6:282–7.
13. Ferracane JL. Elution of leachable components from composites. J Oral Rehabil1994;21:441–52.
14. Augsburger RA, Peters DD. Radiographic evaluation of extruded obturation mate-rials. J Endod 1990;16:492–7.
15. ISO 10993-1:1992, Biological Evaluation of Medical Devices—Part 1: Guidance onSelection of Tests. Geneva: ISO; 1992.
16. ISO 10993-2:1992, Biological Evaluation of Medical Devices—Part 2: AnimalWelfare Requirements. Geneva: ISO; 1992.
17. Bayne K. Developing guidelines of the care and use of animals. Ann N Y Acad Sci1998;30:105–10.
18. Olsson B, Sliwkowsky A, Langeland K. Subcutaneous implantation for the biologicalevaluation of endodontic materials. J Endod 1981;7:355–69.
19. FDI. Federation Dentaire Internationale. Recommended standard practices for thebiological evaluation of dental materials. Int Dent J 1980;30:174–6.
20. Zmener O, Cabrini RL. Monocyte-lymphocyte adhesion to three zinc oxide andeugenol-based endodontic cements: an in vitro assay. Acta Odontol Latinoam1986;3:27–32.
21. Pinna L, Brackett MG, Lockwood PE, et al. In vitro cytotoxicity evaluation of a self-adhesive methacrylate resin-based root canal sealer. J Endod 2008;34:1085–8.
22. Pascon EA, Leonardo MR, Safavi K, et al. Tissue reaction to endodontic materials:methods, criteria, assessment and observations. Oral Surg Oral Med Oral Pathol1991;72:222–37.
23. Kolokouris I, Economides N, Beltes P, et al. In vivo comparison of the biocompat-ibility of two root canal sealers implanted into the subcutaneous connective tissue ofrats. J Endod 1998;24:82–5.
24. Zmener O, Guglielmotti B, Cabrini RL. Biocompatibility of two calcium hydroxide-based endodontic sealers: a quantitative study in the subcutaneous connective tissueof the rat. J Endod 1988;14:229–35.
25. Zmener O, Guglielmotti B, Cabrini RL. Tissue response to an experimental calciumhydroxide-based endodontic sealer: a quantitative study in the subcutaneousconnective tissue of the rat. Endod Dent Traumatol 1990;6:66–72.
26. Andrzejewska E, Linden LA, Rabek JF. The role of oxygen in camphorquinone-initialphotopolymerization. Macromol Chem Phys 1998;199:441–9.
27. Versiani MA, Carvalho-Junior JR, Padilha MIAF, et al. A comparative study of phys-icochemical properties of AH Plus and Epiphany root canal sealants. Int Endod J2006;39:464–71.
28. Rueggeberg FA, Margeson DH. The effect of oxygen inhibition on an unfilled/filledcomposite system. J Dent Res 1990;69:1652–8.
29. Rathbun MA, Craig RG, Hanks CT, et al. Cytotoxicity of a BIS-GMA dental compositebefore and after leaching in organic solvents. J Biomed Mater Res 1991;25:443–57.
30. Costa CAS, Hebling J, Teixeira MF. Preliminary study of the biological compatibilityof the dentine adhesives All-bond 2 and Scotchbond MP. Histological evaluation ofsubcutaneous implants in rats. Rev Odontol USP 1997;11:11–8.
31. Costa CAS, Teixeira HM, Lopes Nascimento AB, et al. Biocompatibility of two currentadhesive resins. J Endod 2000;26:512–6.
32. Molnar EJ. Residual eugenol from zinc-oxide-eugenol compounds. J Dent Res 1967;46:645–9.
33. Rodrigues H, Spangberg L, Langeland K. Biologic effects of dental materials. 9.Effect of zinc oxide-eugenol cements on He La cells in vitro. Estomat Cult1975;9:191–4.
34. Zmener O, Cabrini RL. Effects of three calcium hydroxide-based materials on humanblood monocytes and lymphocytes. Endod Dent Traumatol 1987;3:28–32.
35. Zmener O, Goldberg F, Cabrini RL. Effects of two gutta-percha formulations and onezinc oxide-eugenol and Canada balsam mixture on human blood monocytes andlymphocytes. Endod Dent Traumatol 1989;5:73–7.
36. Geurtsen W, Leyhausen G. Biological aspects of root canal filling materials—histo-compatibility, cytotoxicity and mutagenicity. Clin Oral Invest 1997;1:5–11.
37. Tagger M, Tagger E. Subcutaneous reactions to implantation of tubes with AH26 andGrosman’s sealers. Oral Surg Oral Med Oral Pathol 1986;62:434–40.
38. Yesilsoy C, Koren LZ, Morse DR, et al. A comparative tissue toxicity evaluation ofestablished and newer root canal sealers. Oral Surg Oral Med Oral Pathol 1988;65:459–67.
39. Scarparo RK, Grecca FS, Fachin EVF. Analysis of tissue reactions to methacrylateresin-based, epoxy resin-based, and zinc oxide-eugenol endodontic sealers.J Endod 2009;35:229–32.
bcutaneous Connective Tissue Reaction to Methacrylate Resin–based Sealer 1579

Basic Research—Technology
Subcutaneous Connective Tissue Reaction to MethacrylateResin–based and Zinc Oxide and Eugenol SealersOsvaldo Zmener, DDS,* Cornelis H. Pameijer, DMS, MScD, DSc, PhD,†
Gabriel A. Kokubu, DDS,* and Daniel R. Grana, DVM*
Abstract
Introduction: An evaluation was made of the connec-tive tissue reaction in rats after subcutaneous implanta-tion of methacrylate resin-based sealers (EndoREZ[Ultradent Products, Inc, South Jordan, UT] with a poly-merization accelerator and RealSeal [Sybron DentalSpecialties, Orange, CA]) and Pulp Canal Sealer (SybronDental Specialties), a zinc oxide and eugenol-based sealerused as the control. Methods: Silicone tubes containingthe test materials were implanted in 24 Wistar rats. Solidsilicone rods of the same size served as the negativecontrols. After 10, 30, and 90 days, the animals (n = 8per period) were euthanized and the implants withsurrounding tissues dissected and processed for routinehistological evaluation. A four-category evaluationsystem was used to measure and record the microscopicobservations according to the thickness of a fibrouscapsule, the vascular changes, and the various types ofinflammatory cells. Results: Initially, a severe inflamma-tory reaction was observed of the soft tissues in directcontact with both EndoREZ/Accelerator and Real Seal.The severity decreased over time and was resolved atthe end of the experiment. Pulp Canal Sealer showeda severe tissue reaction for all observation periods. Thenegative controls showed an initial mild to moderateinflammatory reaction. After 30 days, healthy fibrousconnective tissue was observed, which increased overtime. After 10 days, no statistically significant differencesbetween the experimental groups were observed. After90 days, EndoREZ and RealSeal were statistically signif-icantly less toxic than Pulp Canal Sealer (p > 0.05).Conclusions: After 90 days, both methacrylate resin-based sealers were considered biologically acceptablewhen implanted in subcutaneous connective tissues ofthe rat. Pulp Canal Sealer remained toxic for the durationof the study. (J Endod 2010;36:1574–1579)Key WordsBiocompatibility, endodontics, methacrylate-basedsealers, tissue response
From the *School of Dentistry, University of El Salvador, BuenosSupported in part by Ultradent Dental Products Inc.Address requests for reprints to Dr Cornelis H. Pameijer, 10 Hig
0099-2399/$0 - see front matterCopyright ª 2010 American Association of Endodontists.
doi:10.1016/j.joen.2010.06.019
1574 Zmener et al.
The current concept among clinicians is that after complete debridement, total oblit-eration of the root canal space with a biocompatible material constitutes the key
factor for successful endodontic therapy (1). Different materials have been advocatedfor filling root canals; gutta-percha cones complemented with a sealer cement is themost widely used (2). During the last decade, methacrylate resin-based sealers(MRBSs) have gained popularity for root canal obturation (3). Preliminary reportshave shown that two well-established MBRSs (ie, EndoRez [ER; Ultradent Products,Inc, South Jordan, UT] and RealSeal (RS; Sybron Dental Specialties, Orange, CA),formerly Epiphany, are both well tolerated by living tissues (4–7) and have shownpromise for in vivo human clinical trials (8–10). More recently, an ER Accelerator(ACC, Ultradent Products Inc.) has been introduced. The ACC is composed oftriethylene glycol dimethacrylate, tertiary amines, and a proprietary ingredient. Thetechnique the manufacturer recommends is the following. When the master gutta-percha cone has been placed to length, two or three #20 to #25/.02 taper accessorycones dipped in ACC are harpooned in the sealer and pushed into the canal space asfar as possible. The combination of ER and ACC accelerates the polymerization ofthe sealer, thus allowing for an immediate continuation of the coronal restoration. Italso prevents dislodgement of the obturating material when a post space is preparedimmediately after obturation, potentially causing early bacterial leakage (11).
Previous reports (12, 13) have shown that certain components from methacrylateresin-based materials may remain unpolymerized even after setting and can subse-quently be released from the resin matrix. When the sealer is accidentally extrudedthrough the apex or through a lateral canal, which is not an uncommon experiencein endodontics (14), the unpolymerized components may be toxic to the periapicaltissues. Although the biocompatibility of ER and RS has been investigated (4–7), theeffect of ER/ACC in contact with living tissues and compared with RS has not beenreported yet. Therefore, the purpose of this study was to evaluate thebiocompatibility of ER/ACC and RS and to compare them with Pulp Canal Sealer(PCS, Sybron Dental Specialties), a zinc oxide and eugenol-based sealer, when im-planted subcutaneously in connective tissue of rats.
Materials and MethodsThe protocol of this study was approved by the Research Ethics Committee of the
Argentine Dental Association. Autoclaved silicone tubes closed at one end (Raholin SRL,V. Madero, BA, Argentina) and 10-mm long with an internal diameter of 1 mm werefilled flush with freshly prepared ER/ACC, RS, or PCS (positive control). Solid siliconerods (SIRODs) of the same size as the tubes were used as negative controls. ER alonewas not tested because this had been done previously under similar conditions (5). Themethacrylate resin–based sealer samples were prepared in such a way that the
Aires, Argentina; and †University of Connecticut School of Dental Medicine, Farmington, CT, USA.
hwood, Simsbury, CT 06070. E-mail address: [email protected].
JOE — Volume 36, Number 9, September 2010

TABLE 1. Severity of Tissue Reaction to the Test Materials
ER/ACC RS PCS SIROD
Days n NO MI MO SE NO MI MO SE NO MI MO SE NO MI MO SE
10 8 0 0 0 8 0 0 0 8 0 0 0 8 0 6 2 030 8 0 0 8 0 0 0 8 0 0 0 0 8 8 0 0 090 8 7 1 0 0 6 2 0 0 0 0 0 8 8 0 0 0
NO, no reaction; MI, mild reaction; MO, moderate reaction; SE, severe reaction.
Basic Research—Technology
formation of an oxygen-inhibited layer was prevented. The sealerswere prepared under aseptic conditions according to the followingmethod.
In group ER/ACC (n = 8), the experimental design necessitateda slight modification of the manufacturer’s recommendations. ER wasinjected through an automixing tip in a glass syringe measuring25-mm long with a 5-mm internal diameter (De Luca SA, Buenos
Figure 1. (A-F) Representative specimens of ER/ACC, RS, and PCS at the 10-day ocontact (hematoxylin and eosin (H&E), original magnification �40). (A) A highercontact with the sealer (black arrow) and a severe granulomatous tissue reaction wseen (H&E, original magnification�100). (C) RS: a low magnification of tissue/matthe outlined area in C. A thick layer of necrotic tissue in direct contact with the seacontaining many newly formed capillaries (white arrow) can be seen (H&E, originalcontact (H&E, original magnification �40). (F) A higher magnification of the areaa severe granulomatous tissue reaction (H&E, original magnification �150). (Thi
JOE — Volume 36, Number 9, September 2010 Su
Aires, Argentina). Two size #40 gutta-percha cones dipped in ACCwere subsequently inserted in the sealer and left for 3 secondseach after which they were removed. The sealer was then immediatelyinjected into the silicone tubes through a 30-G needle. The procedurewas repeated using a new syringe for each animal.
In group RS (n = 8), the sealer was extruded through an automix-ing tip attached to the two-barrel delivery syringe directly into a plastic
bservation period. (A) ER/ACC: a low-power magnification of tissue/materialmagnification of the outlined area in A. A thin band of necrotic tissue in directith dark material particles and newly formed capillaries (white arrow) can be
erial contact (H&E, original magnification�40). (D) A higher magnification ofler (black arrow) is present. Below it, a severe granulomatous tissue reactionmagnification�100). (E) PCS: low magnification of the area of tissue/materialof tissue/material contact in E showing extruded dark particles surrounded bys figure is available in color online at www.aae.org/joe/.)
bcutaneous Connective Tissue Reaction to Methacrylate Resin–based Sealer 1575

Basic Research—Technology
syringe, which in turn delivered the mixture through a 30-G needle intothe silicone tube.In group PCS (n = 8), the sealer was prepared on a glass slab ac-cording to the manufacturer’s recommendations. The mixture wasloaded in a plastic syringe and injected into the silicone tube thougha 30-G needle.
Excess material was removed from the open end of the tubes witha sterile plastic instrument. After preparation, the samples were imme-diately implanted in the subcutaneous connective tissues of white maleWistar rats weighing approximately 200 g each. The husbandry andmanagement of the animals met the requirements of the ISO 10993–1 (1992) and ISO 10993-2 (1992) standards (15, 16) as well as theInternational Regulatory Requirements for the Care and Use ofLaboratory Animals (17). All surgical procedures were performedunder strict aseptic conditions. After anesthesia through the intraperi-toneal administration of ketamine chloride (14 mg/kg body weight)and acepromazine (10mg/kg body weight), the dorsal skin was shaved
Figure 2. (A-F) A representative sample of ER/ACC, RS, and PCS of the 30-day o(H&E, original magnification �80). (B) A higher magnification of the outlined aretissue concentration (black arrow). Below it is an artifact (ART) within an area oftissue/material contact (H&E, original magnification �40). (D) A higher magnificmaterial particles can be seen in direct contact with the sealer (black arrow). Belowmagnification�150). (E) PCS: a low power of tissue/material contact (H&E, origincles within a severe granulomatous tissue reaction. Note the presence of numerous(This figure is available in color online at www.aae.org/joe/.)
1576 Zmener et al.
and disinfected with 10% iodine-povidone solution (Phoenix SAIC, BA,Argentina). Four approximately 18-mm-long incisions were madethrough the dermis with a scalpel and further prepared by blunt dissec-tion. Subsequently, one sample of each of the four groups was carefullyplaced into the pocket. A distance of at least 20 mm between the sampleswas present to avoid interference of tissue response between two mate-rials. Finally, the wounds were closed with silk sutures, and the animalswere maintained on a regular diet and water ad libitum. Eight animalswere euthanized after 10, 30, and 90 days with an anesthetic overdoseresulting in eight samples per group per time period.
The implants with surrounding tissues were dissected and fixed in10% neutral buffered formalin (pH 7.4). After 48 hours of fixation, thesamples were processed for routine histological evaluation. Paraffinblocks were oriented parallel to the long axis of the tubes and longitu-dinal serial sections of approximately 7-mm thick were cut from themiddle of the implants and stained with hematoxylin and eosin. To eval-uate the tissue response, three sections of the center of each specimen
bservation period. (A) ER/ACC: a low magnification of tissue/material contacta in A. In direct contact with the sealer, there is a dense fibrogranulomatousfat cells (H&E, original magnification �150). (C) RS: a low magnification ofation of the outlined area in C. A thick granulomatous zone containing many
it is a number of wide newly formed capillaries (white arrow) (H&E, originalal magnification�40). (F) A higher magnification of E showing material parti-wide newly formed capillaries (arrows) (H&E, original magnification �150).
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
were analyzed and digitally photographed at different magnificationsunder a light microscope. All sections were analyzed independently,and two trained evaluators who were blind to the study scored the tissuereactions using the following criteria: NO: no reaction, fibrous-capsuleformation, and absence of inflammatory cells; MI: a mild reaction andthe presence of a fibrous-capsule formation with few inflammatorycells; MO: a moderate reaction and fibrous-capsule formation withthe presence of polymorphonuclear leukocytes, lymphocytes, plasmo-cytes, and macrophages; and SE: a severe reaction and the presence oflarge accumulations of polymorphonuclear leukocytes, lymphocytes,plasmocytes, macrophages, foreign-body giant cells, and congestedcapillaries. Before the analysis, both evaluators were calibrated byhaving them analyze a set of 70 similar but unrelated slides displayingvarious types of inflammatory cells to endodontic sealers. In case ofFigure 3. (A-F) A representative sample of ER/ACC, RS, and PCS at the 90-day obsshowing extrusion (ES) of the sealer (H&E, original magnification �40). (B) A higconnective tissue encapsulation free of inflammatory cells is present (black arrow)fication �850). (C) RS: a low magnification of tissue/material contact (H&E, origiNote the presence of a thick fibrous connective tissue capsule (arrow). A few inflamm(H&E, original magnification�850). (E) PCS: an overview of the area of tissue/mategranulomatous tissue slightly invaginated within the lumen of the tube (black arrowa fibrous connective tissue (arrow) that appeared to isolate the inflammatory reacfigure is available in color online at www.aae.org/joe/.)
JOE — Volume 36, Number 9, September 2010 Su
a disagreement between the evaluators, the sample under discussionwas analyzed jointly until a consensus was reached. Data were analyzedby the Wilcoxon signed rank test to determine if there was a statisticallysignificant difference between materials at each observation period. Thetotal effect of time and material upon the tissue reaction was analyzedusing the Kruskal-Wallis and the Dunn test. The significance level wasset at p < 0.05. A sealer was considered to be biologically acceptablewhen tissue reactions were recorded as NO to MI.
ResultsOne animal from the 10-day time period had to be excluded from
the study and was replaced with another undergoing the same implanta-tion procedures. Macroscopic examination showed that wound healing
ervation period. (A) ER/ACC: an overview of the area of tissue/material contacther magnification of A. In contact with the extruded material, a dense fibrous. The white arrow indicates a wide newly formed vessel (H&E, original magni-nal magnification �40). (D) A higher magnification of the outlined area in C.
atory cells can be seen within the capsule as well as in the surrounding tissuesrial contact showing numerous material particles (white arrow) surrounded by) (H&E, original magnification�40). (F) A higher magnification of E showingtion from the surrounding tissues (H&E, original magnification �850).(This
bcutaneous Connective Tissue Reaction to Methacrylate Resin–based Sealer 1577

Figure 4. (A) A representative specimen of SIRODs after the 10-day obser-vation period. In contact with the material (empty space), there is a moderatefibrogranulomatous tissue (black arrow) with inflammatory cells and newlyformed capillaries (H&E, original magnification �100). (B) A representativespecimen of SIRODs after 90 days. In contact with the material (empty space),a thick dense fibrous connective encapsulation (arrow) without inflammatorycells can be seen (H&E, original magnification�850).(This figure is availablein color online at www.aae.org/joe/.)
Basic Research—Technology
was satisfactory at all observation periods. Histological evaluationshowed that the implants were surrounded by fibrous connective tissueof irregular thickness. It could be easily distinguished from the tissuereaction at the site where the tissues were in direct contact with thetest material. The severity of tissue reaction is presented in Table 1.After 10 days, the tissue reaction to ER/ACC, RS, and PCS wasscored severe and was extensively dispersed around the end of the tubes(Figs. 1A-F). The majority of ER/ACC samples with direct tissue contactpresented with an inflammatory reaction with slight invagination intothe lumen of the tubes. Some ER/ACC and RS samples exhibiteda thin necrotic zone in the direct contact area. Each group displayedmany newly formed vessels and randomly dispersed dark particles,which appeared to have been released from the implanted materials.A mild to moderate reaction was observed in SIROD implants.
After 30 days, the intensity of the inflammatory reaction to ER/ACCand RS decreased slightly and was scored as moderate (Fig. 2A-D). Indirect tissue contact, both materials displayed a fibrogranulomatoustissue, which appeared less dispersed and showed a tendency to be sur-rounded by a fibrous tissue containing many inflammatory cells. Incontact with PCS, a persistent severe granulomatous tissue invaginationcontaining many dark particles was observed. This granulomatous reac-tion was surrounded by an incipient layer of fibrous tissue, which wasfree of inflammatory cells (Fig. 2E and F). In contact with SIRODs, therewas a thin fibrous connective tissue containing a few inflammatory cells.
After 90 days, some ER/ACC samples showed extrusion of the mate-rial into the surrounding tissues. In seven samples, a thick dense andmature fibrous tissue capsule (approximately 70- to 90-mm thick) freeof inflammatory cells was present (Fig. 3A and B), whereas only onesample had a mild tissue reaction. The RS samples showed a dense fibrouscapsule (50- to 80-mm thick) without inflammatory cells, whereas twocases were scored as mild with a few inflammatory cells still persistingwithin the capsule (Fig. 3C and D). PCS samples exhibited a severe persis-tent granulomatous tissue reaction containing necrotic areas as well asrandomly distributed inflammatory cells. Particles of the material wereobserved at the end and within the lumen of the tubes in all samples.Higher magnifications showed the granulomatous tissues to be isolatedby a thick fibrous tissue encapsulation. Many newly formed capillariesand a high concentration of acute and chronic inflammatory cells werealso seen (Fig. 3E and F). A thick dense fibrous connective tissue, freeof inflammatory cells, was observed in all SIROD samples (Fig. 4).
The Wilcoxon signed rank test showed no statistically significantdifferences (p > 0.05) between the reaction to ER/ACC, RS, and PCSat the 10-day observation period. After 30 days, no statistical differenceswere found between ER/ACC and RS (p > 0.05), whereas both ER/ACCand RS significantly differed from PCS (p < 0.05). For both periods, ER/ACC, RS, and PCS differed significantly from SIRODs. After 90 days, ER/ACC and RS differed significantly from PCS (p < 0.05) but not from SI-RODs, whereas PCS remained significantly different from SIRODs. Theeffect of time for ER/ACC and RS showed that the 10 and 30 days differedsignificantly (p < 0.05) from the 90-day observation period. However,no significant differences (p > 0.05) were observed for PCS between alltime intervals.
DiscussionThe implantation of endodontic filling materials into subcutaneous
connective tissue of rats is a valid screening method for testing biocom-patibility (18, 19). PCS was used as the positive control because itstoxicity has been previously determined by in vitro (20, 21) and invivo experiments (22, 23). SIRODs were used as the negative controlbecause they have been proven to be biocompatible (5, 6, 24, 25),a finding that was confirmed in this study. The initial inflammatory
1578 Zmener et al.
reaction of SIRODs may be a consequence of the surgical trauma.This subsided rapidly, and after 90 days a well-organized healthy densefibrous tissue free of inflammatory cells was observed. The biocompat-ibility of ER has previously been tested (4–6); however, theincorporation of the ACC changes not only the original chemicalcomposition of ER but also gives the sealer a shorter setting time; anevaluation of the toxicity is therefore essential to determine its safety.
The preparation of ER/ACC and RS samples was performed in sucha way that no oxygen-inhibited layer was formed. Oxygen inhibits free-radical polymerization of resin-based materials yielding an uncuredsurface layer (26, 27), which is of particular concern for MBRSbecause it greatly affects the outcome in toxicity tests. Elution ofuncured chemical components from the oxygen-inhibited layer is oneof the main causes for tissue damage. However, severe reactionswere observed for ER/ACC and RS at the short-term period, revealingthat even after setting they still are an irritant. As has been shown(28), unreacted monomer persists in polymerized methacrylate resins.These unreacted monomers (28) undergo a rapid elution and theleaching of these unbound molecules (29), and other componentscaused the severe inflammatory reactions observed after 10 days. Thesefindings are consistent with those of Costa et al (30, 31) and aresupported by previous experiments of Ferracane and Condon (12)
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
who found that the loss of components from a methacrylate resin-basedmaterial in a water-based medium in vitro is initially rapid and, there-fore, a similar behavior can be expected in vivo. It is significant to notethat the initial severe reaction decreased over time and had beenresolved at the end of the experiment although a few persistent inflam-matory cells still remained adjacent to RS. After the rapid initial loss, thematerial depletes progressively slower over time (12), thus causing lessirritation. Therefore, the setting time is significant with respect to irri-tation. ER/ACC sets in 7 minutes, RS in 25 minutes, and PCS in 260minutes (Zmener and Pameijer, unpublished data, 2009). The fastersetting of ER/ACC could be a contributory factor in reducing the releaseof components, in effect locking in potential irritants (12).The tissue reaction to PCS was severe at all observation periodsand is most likely caused by unreacted eugenol, which is highly toxicto tissues (32). Our findings for PCS are in agreement with otherswho reported that, like other zinc oxide and eugenol-based sealers(33–35), PCS reacted toxic in cell cultures (20, 21, 36) and incontact with living tissues (22, 37–39). However, the results for ER/ACC or RS disagree with those of Scarparo et al (39) who showedintense tissue reactions to ER. Their observations did not extend beyond60 days, however. In the study reported here, a 90-day observationperiod was used. Longer time periods allow more time for elution ofcomponents causing a depletion of chemical components that arepotential irritants. On the other hand, shortening of setting time maycontribute to a lower output of uncured components from ER as shownhere. Within the limitations of this study, it was concluded that ER/ACCand RS exhibited similarly and were both well tolerated by the subcuta-neous connective tissue of rats after 90 days of implantation. PCS,however, remained toxic even after a 90-day observation period.
AcknowledgmentDr. Pameijer is a consultant for Ultradent Products Inc.
References1. Nguyen TN. Obturation of the root canal system. In: Cohen S, Burns RC. Pathways of
the Pulp. 4th ed. St Louis: Mosby; 1987:183–94.2. Taintor JF, Ross PN. Opinions and practices of American Endodontic Diplomates.
Dent J 1978;44:321–5.3. ADA Council of Scientific affairs. Statement on posterior resin-based composites.
ADA Council on Dental Benefit Programs. J Am Dent Assoc 1998;129:1627–8.4. Louw NP, Pameijer CH, Norval G. Histopathological evaluation of a root canal sealer
in subhuman primates. J Dent Res 2001;80:654.5. Zmener O. Tissue response to a new methacrylate-based root canal sealer: preliminary
observations in the subcutaneous connective tissue of rats. J Endod 2004;30:348–51.6. Zmener O, Banegas G, Pameijer CH. Bone tissue response to a methacrylate-based
endodontic sealer: a histological and histometric study. J Endod 2005;31:457–9.7. Sousa CJA, Montes CRM, Pascon EA, et al. Comparison of the intraosseous biocom-
patibility of AH Plus, EndoREZ and Epiphany root canal sealers. J Endod 2006;32:656–62.
8. Zmener O, Pameijer CH. Clinical and radiographic evaluation of a resin-based rootcanal sealer. Am J Dent 2004;17:19–22.
9. Zmener O, Pameijer CH. Clinical and radiographical evaluation of a resin-based rootcanal sealer: a 5-year follow-up. J Endod 2007;33:676–9.
10. Cotton TP, Schindler WG, Schwartz SA, et al. A retrospective study comparing clinicaloutcomes after obturation with Resilon/Epiphany or gutta-percha/Kerr sealer.J Endod 2008;34:789–97.
11. Zmener O, Pameijer CH, Alvarez Serrano S. Effect of immediate and delayed postspace preparation on coronal bacterial microleakage in root canals obturatedwith a methacrylate-based sealer with an without accelerator. An ex vivo study.Am J Dent 2010;23:116–20.
JOE — Volume 36, Number 9, September 2010 Su
12. Ferracane JL, Condon JR. Rate of elution of leachable components from composite.Dent Mat 1990;6:282–7.
13. Ferracane JL. Elution of leachable components from composites. J Oral Rehabil1994;21:441–52.
14. Augsburger RA, Peters DD. Radiographic evaluation of extruded obturation mate-rials. J Endod 1990;16:492–7.
15. ISO 10993-1:1992, Biological Evaluation of Medical Devices—Part 1: Guidance onSelection of Tests. Geneva: ISO; 1992.
16. ISO 10993-2:1992, Biological Evaluation of Medical Devices—Part 2: AnimalWelfare Requirements. Geneva: ISO; 1992.
17. Bayne K. Developing guidelines of the care and use of animals. Ann N Y Acad Sci1998;30:105–10.
18. Olsson B, Sliwkowsky A, Langeland K. Subcutaneous implantation for the biologicalevaluation of endodontic materials. J Endod 1981;7:355–69.
19. FDI. Federation Dentaire Internationale. Recommended standard practices for thebiological evaluation of dental materials. Int Dent J 1980;30:174–6.
20. Zmener O, Cabrini RL. Monocyte-lymphocyte adhesion to three zinc oxide andeugenol-based endodontic cements: an in vitro assay. Acta Odontol Latinoam1986;3:27–32.
21. Pinna L, Brackett MG, Lockwood PE, et al. In vitro cytotoxicity evaluation of a self-adhesive methacrylate resin-based root canal sealer. J Endod 2008;34:1085–8.
22. Pascon EA, Leonardo MR, Safavi K, et al. Tissue reaction to endodontic materials:methods, criteria, assessment and observations. Oral Surg Oral Med Oral Pathol1991;72:222–37.
23. Kolokouris I, Economides N, Beltes P, et al. In vivo comparison of the biocompat-ibility of two root canal sealers implanted into the subcutaneous connective tissue ofrats. J Endod 1998;24:82–5.
24. Zmener O, Guglielmotti B, Cabrini RL. Biocompatibility of two calcium hydroxide-based endodontic sealers: a quantitative study in the subcutaneous connective tissueof the rat. J Endod 1988;14:229–35.
25. Zmener O, Guglielmotti B, Cabrini RL. Tissue response to an experimental calciumhydroxide-based endodontic sealer: a quantitative study in the subcutaneousconnective tissue of the rat. Endod Dent Traumatol 1990;6:66–72.
26. Andrzejewska E, Linden LA, Rabek JF. The role of oxygen in camphorquinone-initialphotopolymerization. Macromol Chem Phys 1998;199:441–9.
27. Versiani MA, Carvalho-Junior JR, Padilha MIAF, et al. A comparative study of phys-icochemical properties of AH Plus and Epiphany root canal sealants. Int Endod J2006;39:464–71.
28. Rueggeberg FA, Margeson DH. The effect of oxygen inhibition on an unfilled/filledcomposite system. J Dent Res 1990;69:1652–8.
29. Rathbun MA, Craig RG, Hanks CT, et al. Cytotoxicity of a BIS-GMA dental compositebefore and after leaching in organic solvents. J Biomed Mater Res 1991;25:443–57.
30. Costa CAS, Hebling J, Teixeira MF. Preliminary study of the biological compatibilityof the dentine adhesives All-bond 2 and Scotchbond MP. Histological evaluation ofsubcutaneous implants in rats. Rev Odontol USP 1997;11:11–8.
31. Costa CAS, Teixeira HM, Lopes Nascimento AB, et al. Biocompatibility of two currentadhesive resins. J Endod 2000;26:512–6.
32. Molnar EJ. Residual eugenol from zinc-oxide-eugenol compounds. J Dent Res 1967;46:645–9.
33. Rodrigues H, Spangberg L, Langeland K. Biologic effects of dental materials. 9.Effect of zinc oxide-eugenol cements on He La cells in vitro. Estomat Cult1975;9:191–4.
34. Zmener O, Cabrini RL. Effects of three calcium hydroxide-based materials on humanblood monocytes and lymphocytes. Endod Dent Traumatol 1987;3:28–32.
35. Zmener O, Goldberg F, Cabrini RL. Effects of two gutta-percha formulations and onezinc oxide-eugenol and Canada balsam mixture on human blood monocytes andlymphocytes. Endod Dent Traumatol 1989;5:73–7.
36. Geurtsen W, Leyhausen G. Biological aspects of root canal filling materials—histo-compatibility, cytotoxicity and mutagenicity. Clin Oral Invest 1997;1:5–11.
37. Tagger M, Tagger E. Subcutaneous reactions to implantation of tubes with AH26 andGrosman’s sealers. Oral Surg Oral Med Oral Pathol 1986;62:434–40.
38. Yesilsoy C, Koren LZ, Morse DR, et al. A comparative tissue toxicity evaluation ofestablished and newer root canal sealers. Oral Surg Oral Med Oral Pathol 1988;65:459–67.
39. Scarparo RK, Grecca FS, Fachin EVF. Analysis of tissue reactions to methacrylateresin-based, epoxy resin-based, and zinc oxide-eugenol endodontic sealers.J Endod 2009;35:229–32.
bcutaneous Connective Tissue Reaction to Methacrylate Resin–based Sealer 1579

Basic Research—Technology
Efficacy of Ultrasonic versus Laser-activated Irrigation toRemove Artificially Placed Dentin Debris PlugsRoeland J.G. De Moor, DDS, MSc, PhD,* Maarten Meire, DDS, MSc,* Kawe Goharkhay, DMD, MD,‡
Andreas Moritz, DMD, DM, PhD,‡
and Jacques Vanobbergen, DDS, PhD†
Abstract
Introduction: The study assessed the efficacy of laseractivated irrigation (LAI) with Erbium: YttriumAluminum Garnet (Er:YAG) and Erbium Chromium: Yt-trium Scandium Gallium Garnet (Er,Cr:YSGG) wave-lengths as compared with passive ultrasonic irrigation(PUI). Previously proposed irrigation times were usedfor LAI (4� 5 seconds) and the intermittent flush tech-nique (3� 20 seconds). Methods: We used a splitroot model with an artificial root canal wall groove.Roots were prepared to an apical size # 40 with ProFiles0.06 (Dentsply Maillefer, Baillaigues, Switzerland). Fivegroups of 20 straight canine roots were evaluated asfollows: Group 1: hand irrigation for 20 s with 2.5%NaOCl (CI); Group 2: PUI performed once for 20 s withthe #20 Irrisafe (Satelec Acteon group, Merignac,France) (PUI 1); Group 3: PUI for 3x 20 s with the Irrisafe(PUI 2); Group 4: LAI with the Er,Cr:YSGG laser and Z2(200 mm) Endolase tip (Biolase, San Clemente, USA)at 75 mJ for 4x 5 s (LAI 1); Group 5: LAI with the Er:YAGlaser (HoYa Versawave, Cortaboeuf, France) and a 200mm endodontic fiber at 75 mJ for 4x 5 s (LAI 2). Imagesfrom the groove were taken before and after irrigation.The quantity of dentin debris in the groove after theexperimental protocols was evaluated. Results: Statisti-cally significant differences (p < 0.05) were foundbetween CI and all other groups and between PUI 1and the other groups. Conclusion: LAI techniques usingerbium lasers (Er:YAG or Er,Cr:YSGG) for 20 seconds(4� 5 seconds) are as efficient as PUI with the intermit-tent flush technique (3� 20 seconds). (J Endod2010;36:1580–1583)Key WordsIrrigation, laser, root canal, ultrasound
From the Departments of *Operative Dentistry and Endo-dontology and †Community Dentistry and Oral Public Health,Dental School, Ghent University, Ghent University Hospital,Ghent, Belgium; and ‡Department of Conservative Dentistry,Dental School, Bernhard Gottlieb University Clinic of Dentistry,Vienna, Austria.
Address requests for reprints to Dr Roeland J.G. De Moor,Department of Restorative Dentistry and Endodontology, GhentUniversity Hospital, Dental School, De Pintelaan 185, B-9000Gent, Belgium. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.06.007
1580 De Moor et al.
Effective endodontic treatment requires the combination of physical and chemicalagents to eradicate soft-tissue debris, smear layer, and microorganisms because
buildup of debris in the root canal system makes effective cleaning and disinfectionimpossible. The use of lasers at different wavelengths has been proposed to supplementconventional endodontic cleaning procedures (1–4). A considerable limitation,however, is the unidirectional emission of the laser beam, which makes it difficult toaccess the entire root canal wall with the laser. The laser fiber must be movedrepeatedly in a spiraling motion along the root canal walls in order to maximize thearea exposed to the laser beam, but even this is not completely efficient and theentire root canal wall will not be exposed to the laser beam (2, 4). Alternativeapproaches such as side-firing tips have limited use because of their size (4) or requirefurther investigation before clinical application (5, 6).
Laser-activated irrigation (LAI) with an erbium laser has been introduced asa method for activating the irrigant (5–10). The effect is based on cavitation; inwater, activation of the laser at subablative settings may result in the formation oflarge elliptical vapor bubbles, which expand and implode. These vapor bubbles maycause a volumetric expansion of 1,600 times the original volume, which increasespressure and drives fluid out of the canal. When the bubble implodes after 100 to200 microseconds, an underpressure develops and sucks fluid back into the canal,inducing secondary cavitation effects. Therefore, the laser works as a fluid pump.Another technique, passive ultrasonic irrigation (PUI), is also based on the principleof cavitation and acoustic streaming (11). The ultrasonic activation of irrigants there-fore plays a pivotal role in contemporary endodontics (12, 13).
The removal of dentin debris from the root canal using LAI has been investigated inonly two studies (10, 11). Both studies, de Moor et al (10) with an Er,Cr:YSGG laser(2,780 nm) and de Groot et al (11) with an Er:YAG laser (2,940 nm), have shownthat LAI is significantly more effective in removing dentin debris from the apical partof the root canal than PUI or hand irrigation when the irrigant was activated for 20seconds. It remains unknown (1) whether the use of PUI for more than 20 seconds(3� 20 seconds according to van der Sluis et al [14]) is as effective as 20 secondsof LAI , and (2) whether there is a difference between the efficacy of LAI performedwith an Er:YAG laser or Er,Cr:YSGG laser (both erbium lasers, with different wave-lengths, 2,780 nm and 2,940 nm, respectively). Therefore, the aim of the present studywas to evaluate ex vivo the removal of artificially placed dentin debris in standardizedroot canals by (1) active hand irrigation for 20 seconds, (2) PUI with an Er:YAG orEr,Cr:YSGG laser, and (3) LAI for 20 seconds and 3 � 20 seconds.
Material and MethodsSample Selection and Preparation
For the setup of this study, an experimental root canal model described by Lee et al(15) was used (Fig. 1). One hundred maxillary canines with straight roots wereselected. These roots were mounted and prepared as described in de Moor et al(9). After verification of the location of the apical foramen with an ISO size 15 filethrough the apical foramen, the teeth were decapitated at 19 mm of the location ofthe apical foramen with a diamond disc (Horico, Berlin, Germany). The coronal 3mm of the canals were enlarged by a round bur with a diameter of 2.3 mm (Komet,Dusseldorf, Germany, 340.202.001.001.023, American size 8) and simulating the
JOE — Volume 36, Number 9, September 2010

Figure 1. A schematic representation of the specimen preparation. On one half of the instrumented root canal, a groove was cut 2 to 6 mm from the apex. In thecoronal 3 mm, an artificial pulp chamber was prepared over a length of 3 mm (diameter = 2.3 mm). (This figure is available in color online at www.aae.org/joe/.)
Basic Research—Technology
pulp chamber (Fig. 1). The root canals were then instrumented with theProFile system (Dentsply Maillefer, Baillaigues, Switzerland) until size40, taper 0.06 (master apical file) 1 mm short of the apical foramen(working length). The standardization of the root canal outline waschecked; pictures of the canals (3,040 � 2,040 pix) were taken, andthe diameter of 10 randomly chosen models was measured at 2, 6,and 10 mm from the apical end of the canal using image analysis soft-ware (Sigmascan Pro Image Analysis Version 5.0; SPSS Inc., Chicago,IL) (9). After instrumentation, the roots were longitudinally splitthrough the canal. A standard groove 4 mm in length, 0.2 mm in width,and 0.5 mm in depth was cut in one canal wall 2 to 6 mm from the apex;the dimension of the groove is comparable to an apical oval root canal(15). Each groove was filled with dentin debris that had been mixed for5 minutes with 2% NaOCl to simulate a situation in which dentin debrisaccumulates in uninstrumented canal extensions during root canalpreparation. This model was introduced to standardize the root canalanatomy and the amount of dentin debris present in the root canalbefore the irrigation procedure, and it was intended to increase the reli-ability of the evaluation of dentin debris removal. The methodology issensitive, and the data are reproducible (14). So, a total of 100 blockswith root canal–prepared roots and plugged root canal wall grooveswere used for the experiment and randomly divided in five groups of 20.
Irrigation ProtocolsFive irrigation protocols were investigated: conventional irrigation
(CI) with 2.5% sodium hypochlorite (NaOCl), two protocols using PUI,and two protocols using LAI. In group 1 (n = 20), hand irrigation with 4mL 2.5% NaOCl was performed with a 10-mL syringe (Terumo, Leuven,Belgium) and a 27-G endodontic needle (Monoject; Sherwood Medical,St Louis, MO). For 20 seconds, the needle was inserted 1 mm short ofthe working length and moved slowly over a distance of 4 mm up and
JOE — Volume 36, Number 9, September 2010
down in the apical half of the root canal. The flow rate was approxi-mately 0.3 mL/s, and the total irrigant volume was 6 mL. In group 2(n = 20) (PUI 1), a stainless steel noncutting wire (#20) (Irrisafe, Sat-elec Acteongroup) was used driven by an ultrasonic device (SuprassonPmax Newtron; Satelec, Acteongroup, Merignac, France) at powersetting ‘‘blue 4’’ (frequency 30 KHz, displacement amplitude about30 mm according to the manufacturer) for 20 seconds. The tip of theIrrisafe was kept 1 mm from the apical stop. After this procedure,the canal was flushed with 2 mL 2.5% NaOCl with a syringe and a 27-G endodontic needle (Monoject). In group 3 (n = 20) (PUI 2), thesame protocol as in group 2 was performed but with a 3� 20 secondsactivation of the irrigant. The irrigant was flushed out and renewed aftereach activation cycle. In group 4 (n = 20) (LAI 1), the NaOCl was acti-vated by laser irradiation (Er,Cr:YSGG laser; Waterlase Millenium, Biol-ase, San Clemente, CA) using an endodontic fiber (Z2, Endolase Tip,Biolase) with a diameter of 200 mm and 25-mm length, with pulse ener-gies of 75 mJ at 20 Hz. The fiber was kept 5 mm away from the mostapical preparation and then kept stationary for 5 seconds. A markwas put on the fiber with a black marker at 13 mm in order to positionit in the root canal at this depth. This protocol was repeated four times,without removing the tip from the root canal. At the end of this proce-dure, the canal was flushed with 2 mL 2.5% NaOCl using a syringe witha endodontic needle. In group 5 (n = 20) (LAI 2), the same protocol asin group 4 was followed but with an Er:YAG laser (HoYa Versawave, Cor-taboeuf, France) and a 200-mm endodontic fiber at 75 mJ. The irrigantwas also activated for 4� 5 seconds. After irrigation, the canals werecarefully dried with paper points (size 35).
Evaluation of Dentin Debris RemovalAfter unlocking the two halves, the amount of remaining debris in
the artificial grooves was evaluated. Digital images of the groove were
Ultrasonic vs Laser-activated Irrigation 1581

Basic Research—Technology
taken before and after irrigation at 40� magnification. These imageswere scored by two dentists who were unaware of the irrigation tech-niques used. Scores were assigned based on the following system: 0:the groove is empty, 1: less than half of the groove is filled with dentindebris, 2: more than half of the groove is filled with dentin debris, and 3:the groove is completely filled with dentin debris.Statistical AnalysisThe interrater agreement was determined (Cohen kappa), and
data were initially analyzed using explorative data analysis. Chi-squaretests were performed to determine whether the observed frequencies(counts) markedly differ from the frequencies expected by chance. Acorrection for multiple testing was performed using the Holm proce-dure, a variant of the Bonferroni adjustment. It is a step-down proce-dure in that one starts with the most extreme (ie, the smallest)p value and continues with less extreme p values in the successive rejec-tion decisions. Because of this adjustment, the level of significance wasset between a < 0.05 and a < 0.005.
ResultsTable 1 shows the debris scores after irrigation with the five
different techniques. Highly significant differences were found betweenCI and both PUI and LAI protocols (p < 0.001). Statistically significantdifferences were also observed between PUI 1 and both groups of LAI,LAI 1 and LAI 2 (p < 0.001). The Cohen kappa coefficient of interrateragreement was 0.85.
DiscussionThe model chosen for this study on the effectiveness of irrigation in
removing dentin debris in artificial irregularities and extensions allowsthe comparison of the presence of debris before and after irrigation. Inmost studies, the amount of debris is evaluated only after preparationand irrigation. Furthermore, these studies did not report how muchdebris was present before irrigation and are therefore unable to estab-lish the extent of removal using the different irrigation procedures. Inthe present study, the groove cut in the root canal wall is made in orderto simulate uninstrumented extensions in the apical half. Canines wereused because they have wide canals (16, 17), and, hence, the root canbe more easily split in the mesiodistal direction.
The generation of shockwaves by dental lasers inside root canalscan play an important role in smear layer removal (5–10). Similarly,smear layer removal can be achieved when water is activated in rootcanals using erbium lasers (Er,Cr:YSGG or Er:YAG) (6, 9, 10),causing the formation of vapor bubbles that expand and implode (5,
TABLE 1. Dentin Debris Scores After Conventional Irrigation With 2.5% NaOCl, PaLaser–Activated Irrigation
Irrigation technique
Debr
0 1
CI*PUI 1*, † 6 (30) 7 (35)PUI 2*, † 12 (60) 6 (30)LAI 1*, † 15 (75) 5 (25)LAI 2*, † 16 (80) 4 (20)
Debris scores: 0: the groove is empty, 1: less than half of the groove is filled with dentin debris, 2: more th
CI, conventional hand irrigation during 20 seconds with 2.5% NaOCl; PUI 1, PUI during 20 s with the #20 Ir
LAI 1, LAI with the Er,Cr:YSGG laser and Z2 (200 mm) Endolase tip (Biolase, San Clemente, CA) at 75 mJ dur
mm endodontic fiber at 75 mJ during 4� 5 seconds.
*Statistically significant differences between groups: CI-PUI 1, CI-PUI 2, CI-LAI 1, and CI-LAI 2 (p < 0.00†Statistically significant differences between groups: PUI 1-LAI 1 and PUI 1-LAI 2 (p < 0.001).
1582 De Moor et al.
7, 8, 10). This was also shown in the present study. Apparently, thereis no difference in the efficacy of both wavelengths in terms of smearlayer removal at the settings used in this study.
The present study is the first to compare the effects of Er:YAG andEr,Cr:YSGG wavelengths on laser-induced cavitation for smear layerremoval. Both wavelengths have a good absorption in water and sodiumhypochlorite (18). The laser light is used here at subablative settings,which does not damage the root canal wall and hence the formationof ledges is avoided (2, 4). The fiber is also inserted centrally in theroot canal without contact with the root canal wall and keptstationary during emission. Also, no spiral motion is made in theirrigant, which is needed when the laser fiber is used in theconventional way and when the whole root canal wall has to beexposed directly to the laser light. In this respect, the risk of ledgecreation appeared to be greater with Er:YAG than with Er,Cr:YSGG (4,19). Care must be taken, however, when using the laser fibers in theroot canal, as apical extrusion of the irrigant after laser activation hasbeen described at the present power settings (6). A previous study byGeorge et al (6) showed that there was twice as much dye penetrationthrough the apical constriction with the fiber tip at 4 mm than at 5 mm.Therefore, a distance of 5 mm from the apical stop to the fiber tip wasused for the present evaluation. All apical stops were also controlledunder magnification 40� (Pico Opmi, Zeiss) by two dentists and nodamage or widening of the unprepared last 1 mm up (from the apicalstop to the outer surface of the root) was seen. These findings confirmthe findings of our previous study (9).
Another interesting finding is that the intermittent flush technique(PUI 2) was as effective as both LAI protocols (12). Therefore, withinthe confines of the present study (removal of debris from a root canalwall groove), the use of an expensive laser device to obtain comparableresults is not necessary. In the study by de Groot et al (10), however,more efficacy was attributed to LAI with an Er:YAG laser because of theformation of secondary cavitation bubbles. The fluid flow associatedwith such an inertial collapse, combined with acoustic streaming result-ing from the oscillations of smaller bubbles, was thought to explain thecleaning efficacy of LAI. The secondary cavitation bubbles allowed bettercleaning of the root canal wall because they are excited by the bubblecollapse of the consecutive laser pulse. Hence, new research shouldbe focused not only on the removal of debris from the root canal wallbut also on the cleanliness of the entire root canal, especially in the apicalthird, and the debridement of anastomes and isthmuses. In addition, theEr:YAG used at subablative settings is also efficient in removing biofilms,even those with Escherichia faecalis (19). Thus, the combination ofcavitation and direct interaction with the biofilm, with the possibility ofsight firing (6) and overcoming the limitations of a straight forwarded
ssive Ultrasonic Irrigation, Er:YAG Laser–Activated Irrigation, and Er,Cr:YSGG
is scores (%)
N (total)2 3
5 (25) 15 (75) 207(35) 20
2 (10) 202020
an half of the groove is filled with dentin debris, 3: the groove is completely filled with dentin debris.
risafe (Satelec Acteon Group, Merignac, France); PUI 2, PUI during 3� 20 seconds with the Irrisafe;
ing 4� 5 seconds; LAI 2, LAI with the Er:YAG laser (HoYa Versawave, Cortaboeuf, France) and a 200-
1).
JOE — Volume 36, Number 9, September 2010

Basic Research—Technology
laser beam (4), might finally result in an added value for erbium lasers inroot canal treatment when used at subablative settings (20).ConclusionLAI techniques with erbium lasers (Er:YAG or Er,Cr:YSGG) for 20
seconds (4� 5 seconds) are as efficient as passive ultrasonic irrigationwith the intermittent flush technique (3� 20 seconds).
References1. Kimura Y, Wilder-Smith P, Matsumoto K. Lasers in endodontics: a review. Int Endod
J 2000;33:173–85.2. Stabholz A, Sahar-Helft S, Moshonov J. Laser in endodontics. Dent Clin North Am
2004;48:809–32.3. Meire M, De Moor RJG. Lasers in endodontics: laser disinfection, an added value?
Endod Pract Today 2007;1:159–72.4. De Moor RJG, Torbeyns D, Meire M. Lasers in endodontics. Part 2: root canal wall
cleanliness and modification. Endod Pract Today 2009;3:19–33.5. George R, Walsh LJ. Apical extrusion of root canal irrigants when using Er:YAG and
Er, Cr:YSGG lasers with optical fibers: an in vitro dye study. J Endod 2008;34:706–8.6. George R, Meyers IA, Walsh LJ. Laser activation of endodontic irrigants using
improved conical laser fiber tips for removing smear in the apical third of theroot canal. J Endod 2008;34:1524–7.
7. Blanken JW, Verdaasdonk RM. Cavitation as a working mechanism of the Er, Cr:YSGGlaser in endodontics: a visulatisation study. J Oral Laser Applic 2007;7:97–106.
8. Blanken J, Meire M, De Moor RJG, et al. Laser activated irrigation or cavitationcausing laser driven irrigation. Part 1: a visualisation study. Lasers Surg Med2009;41:514–9.
JOE — Volume 36, Number 9, September 2010
9. De Moor RJG, Blanken J, Meire M, et al. Laser activated irrigation or cavitationcausing laser driven irrigation. Part 2: evaluation of the efficacy. Lasers Surg Med2009;41:520–3.
10. de Groot SD, Verhaagen B, Versluis M, et al. Laser-activated irrigation within rootcanals: cleaning efficacy and flow visualization. Int Endod J 2009;42:1077–83.
11. van der Sluis LMW, Wu M-K, Versluis M, et al. Passive ultrasonic irrigation of the rootcanal: a review of the literature. Int Endod J 2007;40:415–26.
12. Plotino G, Pameijer CH, Grande NM, et al. Ultrasonics in endodontics: a review of theliterature. J Endod 2007;33:81–95.
13. Gu LS, Kim JR, Ling J, et al. Review of contemporary irrigant agitation techniques anddevices. J Endod 2009;35:791–804.
14. van der Sluis LMW. Passive ultrasonic irrigation of the root canal [PhD thesis]. ACTA(Academisch Centrum Tandheelkunde Amsterdam), Amsterdam, The Netherlands;2007.
15. Lee SJ, Wu MK, Wesselink PR. The effectiveness of syringe irrigation and ultrasonicsto remove debris from simulated irregularities within prepared root canal walls. IntEndod J 2004;37:672–8.
16. Kerekes K, Tronstad L. Morphometric observations on root canals of human ante-rior teeth. J Endod 1977;3:24–9.
17. Wu M-K, Roris A, Barkis D, et al. Prevalence and extent of long oval canals inthe apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:739–43.
18. De Moor RJG, Delme KIM. Laser-assisted cavity preparation and adhesion toerbium-lased tooth structure: part 1. Laser-assisted cavity preparation. J AdhesDent 2009;11:427–38.
19. Varella CH, Pileggi R. Obturation of root canal system treated by Cr, Er:YSGG laserirradiation. J Endod 2007;33:1091–3.
20. Meire M, De Prijck K, Coenye T, et al. Evaluation of Nd:YAG and Er:YAG irradiationand antibacterial photodynamic therapy on Enterococcus faecalis biofilms on dentindisks. Int Endod J 2009;42:351–9.
Ultrasonic vs Laser-activated Irrigation 1583

Case Report/Clinical Techniques
Cone-Beam Computed Tomographic Evaluation ofSpontaneously Healed Root FractureKaan Orhan, DDS, PhD,* Umut Aksoy, DDS,† and Atakan Kalender, DDS, PhD†
Abstract
Introduction: Dental trauma can lead to injuries inteeth and their supporting structures, which occursmost commonly in young patients and varies inseverity from enamel fractures to avulsions. Root frac-tures are relatively uncommon among dental traumas,mostly affecting the permanent dentition. It has beenreported that root fractures can undergo healing,whereas pulp necrosis can also occur. Methods: Inthis report, we present a case of the utilization ofcone-beam computed tomography (CBCT) in the detec-tion of possible cervical or internal resorption secondaryto a mid-horizontal fracture in a 36-year-old malepatient. The fractured teeth spontaneously healed andwere diagnosed radiographically after 28 years. Initially,conventional radiographs showed fractured fragmentswith radiolucent lines. Because of possible invasivecervical resorption and doubt over internal resorptionin the conventional images, it was decided to examinethe teeth with cone-beam computed tomography withthree-dimensional reconstructions. Results: The imagesclearly showed the displaced fragments of the root frac-ture. Despite the appearance in the conventional radio-graph, no evidence of cervical or internal resorptionwas detected in the teeth other than the healed rootfracture. Conclusion: It was concluded that CBCTimages should be obtained for root fractures, especiallythose in which cervical or internal resorption is sus-pected from routine conventional radiographs. (J Endod2010;36:1584–1587)Key Wordscone-beam computed tomography, diagnosis,endodontic problems, healing, management ofendodontic problems, root fracture
From the Departments of *Oral Diagnosis and Radiologyand †Endodontics, Near East University, Mersin, Turkey.
Address requests for reprints to Dr Kaan Orhan, Near EastUniversity, Faculty of Dentistry, Department of Oral Diagnosisand Radiology, Mersin 10, Turkey. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.04.004
1584 Orhan et al.
Traumatic injuries occur more commonly in young patients and vary in severity fromenamel fractures to avulsions, which are the cause of emergency treatment in dental
practice. Root fractures of permanent teeth can be cited as an example of these kinds ofinjuries. Horizontal root fractures have a relatively low incidence, ranging from 0.5% to7% when compared with other dental impact injuries. They are frequently seen in themiddle third of the root followed by apical and coronal third fractures; the most affectedteeth are the maxillary central incisors of male patients (1–5).
Although root fractures can be generally detected shortly after the injury, they areidentified occasionally at subsequent routine dental examinations (1, 6–8). Thediagnosis of root fractures is accomplished with clinical and radiographicexamination. Clinical examination includes evaluation of the mobility, presenceor absence of tenderness and pain to palpation of the soft tissues, and percussion ofthe teeth and pulp testing. Radiographic examination can establish the diagnosisof root fracture but must be performed carefully. Two or three radiographs taken atvarious angles may be needed because of the angulation of the fracture. If the x-raybeam does not pass directly through the fracture line, it usually cannot be seen onthe radiographs (9–13).
However, in the last decade, with the development of cone-beam computed tomog-raphy systems (CBCT), dentoalveolar imaging can be performed with less radiation andgreater accuracy (14). In recent studies, it was shown that dental CBCT can be recom-mended for the assessment root canal systems (15), apical periodontitis (16), andinflammatory root resorptions (17) and has been shown to be useful in the diagnosisand management of these kinds of dentoalveolar trauma patients (13–16, 18). In thisreport, we aimed to present a case regarding the use of CBCT in the detection of possiblecervical or internal resorption secondary to a spontaneous healed mid-horizontalfracture and to discuss the potential use of CBCT in root fractures.
Case ReportA 36-year-old man was referred to our clinic with the chief complaint of pain in the
mandibular right second molar. A routine periapical radiograph revealed suspicion ofa horizontal root fracture in the maxillary right central incisor (Fig. 1). The patient’smedical history was unremarkable, but the dental history revealed that he had beenhit in his mouth by his friend’s head during a game while he was 8 years old. The patientalso stated that his central incisors had displaced palatinally, and he had replaced themalone by his hand and did not seek any professional dental care at that time. Althoughthe clinical examination showed palatinally displaced teeth and slight discolorations ofthe central incisors, the patient had no complaints except for the pain in the molar tooth.Vitality testing with solid carbon dioxide (CO2 ice) and an electric pulp tester (DigitestParkell, Farmingdale, NY) elicited no response from both the maxillary right and leftcentral incisors. There was no mobility, fistulae, or pain to percussion or palpation.However, in the periapical radiograph, slight radiolucent areas in the fracture linewere seen, which were interpreted to be possible resorption areas in the teeth (Fig. 1).
It was decided to obtain CBCT imaging for further evaluation. CBCT analysis wasperformed in all three dimensions, axial, sagittal, and cross-sectional images, witha 0.4-mm slice thickness (Newtom 3G; Quantitative Radiology SRL, Verona, Italy).The axial images revealed horizontal root fractures of the maxillary right central andleft central incisors. Sagittal and cross-sectional views also showed horizontal root frac-tures in the middle third with pulp obliterations of the teeth. However, there was noevidence of periradicular pathology and no cervical or internal resorption, except
JOE — Volume 36, Number 9, September 2010

Figure 1. (a) A panoramic radiograph and (b) periapical radiograph of the patient showing root fractures. Note the arrows showing radiolucent possible resorp-tion area in the fracture line.
Case Report/Clinical Techniques
for the spontaneously healed root fracture of the incisors (Fig. 2).Three-dimensional reconstructed images also showed the healedfractures in detail (Fig. 3).
DiscussionTraumatic dental injuries are everyday occurrences in children
and adolescents (2, 19, 20). Maxillary central incisors are the mostvulnerable to injury, sustaining approximately 80% of all dentalinjuries, followed by the maxillary lateral and the mandibularincisors (21). The literature indicates that many factors may influencethe type of healing that occurs for root fractures. For root fractures, the
Figure 2. Axial, sagittal, and cross-sectional CBCT images showing a healed root frainternal resorption.
JOE — Volume 36, Number 9, September 2010
length of time between the trauma and the treatment, the stage of rootdevelopment, and any associated signs and symptoms of mobility andpain may influence the type of healing (22).
The healing of root fractures with or without initial treatment is re-ported to occur in up to 80% of cases, whereas pulp necrosis occurredin 20% (23–25). When the fracture line allows communication with theoral cavity, immobilization is difficult, and microbial contamination ofthe pulp with subsequent pulpal necrosis is almost inevitable (4, 7).
Root fractures in the apical and middle thirds usually require noimmediate treatment, but because of the pathological changes that canoccur several years after injuries, long-term follow-up of patients with
cture of the incisors without evidence of periradicular pathology or cervical or
CBCT Evaluation of Spontaneously Healed Root Fracture 1585

Figure 3. A three-dimensional image of root fractures using volumetricrendering software.
Case Report/Clinical Techniques
traumatic injuries is very crucial (4, 26–28). Davidovich et al (3)reported such a trauma case, which resulted in invasive cervicalresorption 13.5 years after the trauma. In that case, early signs ofcervical resorption were missed at 8 years in the follow-up radiographicexaminations.
Because periapical radiographs are two-dimensional images ofthree-dimensional structures, the superimposition of adjacent struc-tures may obscure the visibility of fractures. A three-dimensionalimaging protocol should be used in detecting fractures, especially asan only choice for vertical root fractures (12, 29). Youssefzadeh et al(30) reported an in vivo study that was conducted with medicalcomputed tomography (MDCT) on the detection of vertical root frac-tures and found out that MDCT was far better than conventional periap-ical radiographs. However, the radiation dose, the limited availability,and the increased cost impede its use in dentistry (10, 12, 31).
CBCT produces a cone shaped x-ray beam, and this makes itpossible to capture the image in a single shot, rather than capturingslices separately, as in MDCT. The most important advantage of thisimaging modality is acquiring comparative images with a much lowerradiation dose than MDCT (10–13). In recent studies, it wasconcluded that CBCT scans are more accurate than periapicalradiographs and effective in a safe way to detect both horizontal andvertical root fractures (9, 11, 12, 32). It was also concluded thatcurrently CBCT should be considered when conventionalradiographic techniques fail to provide information for diagnosinghorizontal root fractures (32).
In our case, vitality testing and the electric pulp tester elicited noresponse from both the maxillary right and left central incisors. Therewas no mobility, fistulae, or pain to percussion or palpation. However,in the periapical radiograph, radiolucent areas in the fracture line wereseen, which were interpreted as possible cervical or internal resorptionin the teeth. Therefore, it was decided to perform CBCT so as not to themiss any delayed complications of trauma, like resorptive processesthat may lead to tooth loss.
CBCT images showed no sign of pathology in the teeth in our case.Estrela et al (17) reported in a recent study that inflammatory rootresorption was determined more accurately and at earlier stages byusing CBCT scans than with conventional radiographic images becauseof the three-dimensional view potential. It was also stated that inflamma-tory root resorption might be underestimated when evaluated with onlyperiapical radiographs. We suggest obtaining three-dimensional CBCTimages for the detection of possible cervical or internal resorption incases similar to ours.
1586 Orhan et al.
Although in the present case the initial diagnosis showed that CBCTimages were superior in diagnostic efficacy to conventional radio-graphic images, for follow-up the CBCT images should not necessarilyreplace conventional methods. CBCT studies cause higher radiationexposures (4-20 times greater). From the standpoint of radiationrisk, CBCT appears to have three to seven times the risk of a panoramicexamination depending on the area examined, the degree of collima-tion, and the acquisition software version. Thus, the decision to selectan imaging modality for diagnostic purposes, as in this case, shouldbe based on the diagnostic yield expected and in accordance with theALARA (as low as reasonably achievable) principle (31, 33). Inconclusion, from the radiation protection point of view, thediagnostic information of CBCT must improve the treatment results;without such a benefit, this technique should not be recommended.
References1. Andreasen FM, Andreasen JO. Crown fractures. Textbook and Color atlas of trau-
matic injuries to the teeth. 3rd ed. Copenhagen: Munksgaard; 1994:219–56.2. Gomes AP, de Araujo EA, Goncalves SE, et al. Treatment of traumatized permanent inci-
sors with crown and root fractures: a case report. Dent Traumatol 2001;17:236–9.3. Davidovich E, Heling I, Fuks AB. The fate of a mid-root fracture: a case report. Dent
Traumatol 2005;21:170–3.4. Andreasen FM, Andreasen JO. Root fractures. Textbook and Color atlas of traumatic
injuries to the teeth. 3rd ed. Copenhagen: Munksgaard; 1994:279–313.5. Caliskan MK. Prognosis of large cyst-like periapical lesions following nonsurgical
root canal treatment: a clinical review. Int Endod J 2004;37:408–16.6. Yates JA. Root fractures in permanent teeth: a clinical review. Int Endod J 1992;25:
150–7.7. Trope M, Chivian N, Sigurdsson A, et al. Traumatic injuries. In: Cohen S, Burns RC,
eds. Pathways of the pulp. 8th ed. St. Louis: Mosby; 2002:603–49.8. Tziafas D, Margelos I. Repair of untreated root fracture: a case report. Endod Dent
Traumatol 1993;9:40–3.9. Patel S, Dawood A, Ford TP, et al. The potential applications of cone beam computed
tomography in the management of endodontic problems. Int Endod J 2007;40:818–30.
10. Cotton TP, Geisler TM, Holden DT, et al. Endodontic applications of cone-beamvolumetric tomography. J Endod 2007;33:1121–32.
11. Patel S. New dimensions in endodontic imaging: part 2. Cone beam computedtomography. Int Endod J 2009;42:463–75.
12. Hassan B, Metska ME, Ozok AR, et al. Detection of vertical root fractures inendodontically treated teeth by a cone beam computed tomography scan. J Endod2009;35:719–22.
13. Patel S, Dawood A, Whaites E, et al. New dimensions in endodontic imaging: part 1.Conventional and alternative radiographic systems. Int Endod J 2009;42:447–62.
14. Mozzo P, Procacci C, Tacconi A, et al. A new volumetric CT machine for dentalimaging based on the cone-beam technique: preliminary results. Eur Radiol1998;8:1558–64.
15. Matherne RP, Angelopoulos C, Kulild JC, et al. Use of cone-beam computed tomog-raphy to identify root canal systems in vitro. J Endod 2008;34:87–9.
16. Estrela C, Bueno MR, Leles CR, et al. Accuracy of cone beam computed tomographyand panoramic and periapical radiography for detection of apical periodontitis.J Endod 2008;34:273–9.
17. Estrela C, Bueno MR, De Alencar AH, et al. Method to evaluate inflammatory rootresorption by using cone beam computed tomography. J Endod 2009;35:1491–7.
18. Bornstein MM, Wolner-Hanssen AB, Sendi P, et al. Comparison of intraoralradiography and limited cone beam computed tomography for the assessment ofroot-fractured permanent teeth. Dent Traumatol 2009;25:571–7.
19. de Blanco LP. Treatment of crown fractures with pulp exposure. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1996;82:564–8.
20. Garcia-Godoy F, Pulver F. Treatment of trauma to the primary and young permanentdentitions. Dent Clin North Am 2000;44:597–632.
21. Andreasen FM, Andreasen JO. Crown fractures. Textbook and Color atlas oftraumatic injuries to the teeth. 3rd ed. Copenhagen: Munksgaard; 1994. 257–77.
22. Feely L, Mackie IC, Macfarlane T. An investigation of root-fractured permanentincisor teeth in children. Dent Traumatol 2003;19:52–4.
23. Artvinli LB, Dural S. Spontaneously healed root fracture: report of a case. Dent Trau-matol 2003;19:64–6.
24. Camp JH. Management of sports-related root fractures. Dent Clin North Am 2000;44:95–109.
25. Rintaro T, Kiyotaka M, Minoru K. Conservative treatment for root fracture locatedvery close to gingiva. Dent Traumatol 2005;21:111–4.
JOE — Volume 36, Number 9, September 2010

Case Report/Clinical Techniques
26. Cheung SP, Walker RT. Root fractures:a case of dental non-intervention. Endod DentTraumatol 1988;4:186–8.27. Cohen S, Burns RC. Pathways of the pulp. 6th ed. St. Louis: Mosby; 1994: 452.28. Simon S, Lumley PJ, Cooper PR, et al. Trauma and dentinogenesis: a case report. J
Endod 2010;36:342–4.29. Hassan B, Metska ME, Ozok AR, et al. Comparison of five cone beam computed
tomography systems for the detection of vertical root fractures. J Endod 2010;36:126–9.
30. Youssefzadeh S, Gahleitner A, Dorffner R, et al. Dental vertical root fractures: valueof CT in detection. Radiology 1999;210:545–9.
JOE — Volume 36, Number 9, September 2010
31. Ludlow JB, Davies-Ludlow LE, Brooks SL. Dosimetry of two extraoral direct digitalimaging devices: NewTom cone beam CT and Orthophos Plus DS panoramic unit.Dentomaxillofac Radiol 2003;32:229–34.
32. Kamburoglu K, Ilker Cebeci AR, Grondahl HG. Effectiveness of limited cone-beamcomputed tomography in the detection of horizontal root fracture. Dent Traumatol2009;25:256–61.
33. Angelopoulos C, Thomas SL, Hechler S, et al. Comparison between digital panoramicradiography and cone-beam computed tomography for the identification of themandibular canal as part of presurgical dental implant assessment. J Oral MaxillofacSurg 2008;66:2130–5.
CBCT Evaluation of Spontaneously Healed Root Fracture 1587

Case Report/Clinical Techniques
Cytotoxic Chemotherapy-induced Odontalgia: A DifferentialDiagnosis for Dental PainYehuda Zadik, DMD, MHA,* Vladimir Vainstein, MD,† Ilana Heling, DMD,‡ Tzahi Neuman, MD,§
Scott Drucker, BSc,k
and Sharon Elad, DMD, MSc*
Abstract
Introduction: Peripheral neurotoxicity and neuro-pathic pain are well-known complications of severalanti-cancer chemotherapeutic agents. Such pain mightcause an impairment of the patient’s quality of lifeand is a common limiting factor of anti-cancer chemo-therapy. Neurotoxicity in orofacial structures has beenpreviously described as diffuse jaw pain or numbness.Currently, localized pulpal pain is not listed asa possible complication of cytotoxic therapy. Theaim of this report was to suggest cytotoxic-inducedneurotoxicity as a differential diagnosis for toothacheduring anti-cancer therapy. Methods: We describedthe diagnostic process in a patient suffering from severepulpal pain in apparently intact teeth during cytotoxictherapy. A non-Hodgkin’s lymphoma patient com-plained of 2 episodes of excruciating dental painevoked by mouth breathing, which caused nocturnalawakenings. Results: Both episodes developed imme-diately after administrations of cyclophosphamide aspart of an anti-cancer chemotherapy protocol. Clinicalparameters and radiographic characteristics eliminatedother possible dental and facial etiologies. Pulp extirpa-tion (pulpectomy) resulted in immediate pain relief. Inboth episodes, cytologic evaluation of the extirpatedpulp tissue failed to show inflammation or an infiltra-tion of lymphoma cells. Conclusions: This case pre-sented a circumstantial relation between the clinicalpresentation of dental pain, with associated significantimpairment of the patient’s quality of life, and thetiming of administrations of high-dose cyclophospha-mide. It suggests that chemotherapy-induced toxicitymight manifest as pulpitis-like toothache, which mightpresent a diagnostic challenge for the dental practi-tioner. (J Endod 2010;36:1588–1592)Key WordsCancer, chemotherapy, cyclophosphamide, dental,neuropathy, pain, tooth
From the *Department of Oral Medicine, Hebrew University-Hadsity Medical Center, Jerusalem, Israel; ‡Department of EndodonticsPathology, Hadassah University Medical Center, Jerusalem, Israel; a
Address requests for reprints to Dr Yehuda Zadik, Hebrew UniverIsrael. E-mail address: [email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.004
1588 Zadik et al.
Orofacial pain in oncology patients is quite common, affecting up to 70% of patientswith cancer (1). Non-dental orofacial pain related to malignancy can be attributed
to a variety of etiologies including space-occupying lesion, leukemic infiltration,secondary anemia, chemotherapy or radiotherapy mucositis, acute and chronicgraft-versus-host disease, secondary infection, postsurgery pain, osteoradionecrosis,bisphosphonate-related osteonecrosis of jaws, and nerve damage caused by cytotoxicchemotherapy and/or radiotherapy (2). In general, the vast majority of such pain isdirectly associated with the tumor itself (in 87%–93% of the cases), although muchless frequently it is associated with anti-cancer therapy (17%–21%) or both (1).
Neuropathic pain is induced by a primary lesion or dysfunction of the nervoustissues and might be triggered by local or systemic conditions (such as local injuryor diabetes mellitus, respectively) that affect structures along the neuraxis (3). Approx-imately 50% of pain in cancer patients can be categorized as exclusively or partly neuro-pathic (4). The nerve damage associated with the administration of chemotherapeuticagents might be manifested as purely sensory neuropathy, mixed sensorimotor neurop-athy (with or without the involvement of autonomic nervous system), and/or mentalstatus changes. These effects characteristically result from accumulation of the cytotoxicagent throughout multiple cycles of therapy; symptoms disappeared within days of eachadministration of chemotherapy, but their severity and duration increased over subse-quent cycles (5).
Neuropathic pain induced by chemotherapy is difficult to control with analgesicmedications (4) and is thus a well-recognized clinical problem. In addition to its influ-ence on the patient’s quality of life, many patients are unable to complete their necessarytreatment cycles because of this neuropathy (6, 7). McCarthy and Skillings (8) reportedorofacial complications among chemically treated breast cancer patients. As high as65% of their patients suffered from orofacial neurotoxicity during a 7-week course;of these patients, 86% suffered from orofacial pain.
The aim of our study was to report a case of severe dental pain in 2 teeth occurringon 2 separate episodes in a lymphoma patient and to discuss the diagnosis of pulpalneuropathic pain caused by anti-cancer drugs.
Case ReportA 54-year-old man bedridden with non-Hodgkin’s lymphoma presented with 2
episodes of intense dental pain. He had been diagnosed 6 months earlier with largeB-cell lymphoma primarily involving bone marrow, mediastinum, and the centralnervous system. The lymphoma had manifested as paraparesis, transverse myelitis,and mediastinal lymphadenopahy. An anti-lymphoma protocol of rituximab, cyclophos-
assah School of Dental Medicine, Jerusalem, Israel; †Department of Hematology, Hadassah Univer-, Hebrew University-Hadassah School of Dental Medicine, Jerusalem, Israel; and §Department ofnd kSchool of Dental Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.sity-Hadassah School of Dental Medicine, Department of Oral Medicine, P.O. Box 91120, Jerusalem,
JOE — Volume 36, Number 9, September 2010

Figure 1. Timing of dental pain in relation to anti-lymphoma protocol.
Case Report/Clinical Techniques
phamide, and doxorubicin was administrated to the patient, accompa-nied by intrathecal injections of cytarabine infused through an Ommayacatheter (Fig. 1). Other medications taken by the patient were aspirin,folic acid, lactulose, mesna, leucovorin, methenamine, simvastatin, sul-famethoxazole/trimethoprim, and tamsulosin. Fig. 1 presents the timingof the 2 episodes of dental pain with relation to the chemotherapeutictreatments. The patient’s medical history included hyperlipidemia,nonalcoholic fatty liver, and benign prostatic hyperplasia.
TABLE 1. Description of the 2 Dental Pain Episodes
Episode First episode
Pain timing On the third day of the first administratcyclophosphamide (8/2008).
Symptoms Intense pain (VAS 9).*The pain awakened him from sleep
intensified with drinking cold liquids astimulation.
Oral evaluation Normal mucosal tissue.Second right mandibular molar:
No dental decay, intact pre-existing restadequate contact area with adjacent to
occlusal abrasion, no cervical lesioPeriodontal status: probing depth up to
non-tender.Cold stimuli yielded pain that remained
minutes after removal of stimuluPercussion (vertical/horizontal) and ves
palpation tests yielded intense paiDifferential diagnosis (1) Malignant pulpal infiltrate
(2) Chemotherapy-induced neurotoxManagement Second mandibular right molar:
Pulp tissue was sampled to cytology evaPulpectomy (tetracycline/triamcinol
intracanal dressing).Follow-up Pain resolved immediately.
Cytologic examination did not reveal B ceamputated pulp or inflammatory ce
*Visual analogue scale of 0–10, with ‘‘0’’ as no pain and ‘‘10’’ as the most intense pain.
JOE — Volume 36, Number 9, September 2010
Dental pain was located initially in the right mandibular molarregion and later in the left maxillary molar region. The pain was ratedby the patient as 9 and 10 on a 0–10 pain scale in the first and secondepisodes, respectively (Table 1). During the 2 episodes, pain wasevoked by mouth breathing and by drinking cold beverages. The paincaused nocturnal awakenings. Eating did not evoke pain. There wasno history of dental pain during the year preceding chemotherapy.The patient did not report any other (extraoral) neuropathic pain.
Second episode
ion of On the first day of the second administration ofcyclophosphamide (9/2008).
andnd air
Intense pain (VAS 10).*The pain awakened him from sleep.
oration,oth, non.3 mm,
for 3.5s.tibularn.
No tenderness over the maxillary sinuses.Normal mucosal tissue.
First left maxillary molar:No dental decay, intact pre-existing restoration,
no occlusal abrasion, no cervical lesion.Periodontal status: probing depth up to 3 mm,
non-tender.Cold stimuli yielded intense pain (which subsided
on removal of stimulus).Percussion (vertical/horizontal) and vestibular
palpation tests yielded intense pain.
icity(1) Malignant pulpal infiltrate
(2) Chemotherapy-induced neurotoxicity
luation.one
First maxillary left molar:Pulp tissue was sampled to cytology evaluation.
Pulpectomy (tetracycline/triamcinoloneintracanal dressing).
lls in thells.
Pain resolved immediately.Cytologic examination did not reveal B cells in the
amputated pulp or inflammatory cells.
Cytotoxic Chemotherapy-induced Odontalgia 1589

Figure 2. Periapical radiographs of the affected teeth in the first (a) and second (b) episodes.
Figure 3. Cytology of the extirpated pulp (first episode); normal blood smearwith no sign of malignancy or inflammation. Original magnification, �630.(This figure is available in color online at www.aae.org/joe/.)
Case Report/Clinical Techniques
Examination included clinical (vestibular) palpation and percus-sion, cold tests, periodontal probing, and radiography (Fig. 2; Table 1).No dental caries lesions were observed in the affected teeth. Physicalexamination eliminated other possible etiologies such as caries withpulp involvement, lateral periodontal abscess or perio-endo lesion,cracked tooth, vertical root fracture, and food impaction as well asa mucosal origin for the pain. Pain from the opposing teeth was ruledout as well. Periodontal probing depth up to 3 mm was measuredaround the tooth. Percussion (vertical/horizontal) and vestibularpalpation tests yielded intense pain. Cold stimuli resulted in pain lasting3.5 minutes after removal of the stimuli.
Results of blood tests taken on the day of initial presentation(August 10th) were the following: white blood cell count, 10.7 �109/L (normal limits, 4–10 � 109/L) with 90.2% (9.7 � 109/L)neutrophils; red blood cell count, 3.42 � 1012/L (normal, 4.5–6 �1012/L); hemoglobin level, 9.7 g/dL (normal, 14–18 g/dL); plateletcount, 292.0 � 109/L (normal, 140–400 � 109/L); alanine amino-transferase level, 25 U/L (normal, 6–53 U/L); aspartate aminotrans-ferase level, 20 U/L (normal, 2–60 U/L); fasting glucose level, 4.9mmol/L (normal, 4–6 mmol/L); and blood creatinine level, 49 mmol/L (normal, 58–110 mmol/L). Blood tests taken on September 21stafter his second episode yielded similar results.
During the first episode no definitive diagnosis was reached, buta working diagnosis of direct infiltration of lymphoma cells into thepulp chamber causing local pressure and pain was made. This led tothe assumption that the chemotherapy would reduce the presumedlymphomatous infiltrate and would therefore help resolve the pressureand pain. On the basis of this initial diagnosis and the fact that the painwas not attributed to a known dental pathology, the decision was madeby the patient and practitioners not to perform an irreversible interven-tion for pain relief (ie, pulpectomy), but rather to manage the pain bypowerful analgesics. The patient received oxycodone 30 mg every 4hours (Oxycod syrup; Rafa Pharmaceutics, Jerusalem, Israel) forpain relief and was evaluated daily. Despite the chemotherapy, therewas no improvement in dental pain during a 2-week course. Conse-quently, because of the severity of the symptoms the decision wasmade to take a more radical treatment approach. Under local anesthesia(inferior alveolar nerve block with 3.6 mL of 2% lidocaine with1:100,000 epinephrine), the dental pulp of the affected tooth was extir-pated, and the root canal system was dressed with combined triamcin-olone acetonide (1.0%) and demeclocycline calcium (3.021%) paste(Ledermix paste; Haupt Pharma GmbH, Wolfratshausen, Germany).
1590 Zadik et al.
This treatment resulted in immediate pain relief. It should be mentionedthat despite a regional nerve block, additional intrapulpal anesthesiawas needed as a result of pain during procedure.
Similarly, in the second episode, which happened a month afterthe beginning of the first episode, the pain characteristics were notspecific and resembled those of the first episode (Table 1). Periodontalprobing depth up to 3 mm was measured around the tooth. Percussion(vertical/horizontal) and vestibular palpation tests yielded intense pain.Cold stimuli yielded intense pain; however, the pain receded on removalof the stimulus. The same first line supportive treatment was recommen-ded to the patient by using powerful analgesics. On follow-up 3 dayslater, no symptomatic improvement was reported. It was agreed torepeat the same ultimate dental treatment as in the first episode. Pulpextirpation (after buccal and palatal infiltration of 3.6 mL of 2% lido-caine with 1:100,000 epinephrine) resulted in immediate pain reliefin this episode as well.
In both episodes cytologic evaluation (by T.N.) was performed onpulp content that was collected by 19-gauge needle as well as fromdebris on the endodontic file. No lymphoma, inflammatory process,or infection were seen (Fig. 3). Whole body positron emission tomog-raphy scan after injection of fluorodeoxyglucose (18F), performed
JOE — Volume 36, Number 9, September 2010

Case Report/Clinical Techniques
between the first and second pain episodes, revealed diffuse absorptionin bone marrow and spleen (standard uptake value, 3.8) and anterior-superior part of mediastinum (standard uptake value, 2.6). No involve-ment of the head and neck region was detected.Endodontic treatments and rehabilitation of the extirpated teethwere not completed as a result of the patient’s poor medical condition.Eight months after the second episode the patient died as a result ofdecubitus-induced sepsis.
DiscussionIn the medically competent patient, the differential diagnosis of
acute severe dental pain includes irreversible pulpitis, acute periapicalperiodontitis or lateral periodontal abscess, and the related diagnosis ofperio-endo lesion and vertical root fracture, as well as food impaction(9). All these potential diagnoses were ruled out in the 2 episodes bya comprehensive clinical-radiologic evaluation (10) as describedabove.
Other conditions that might mimic severe dental pain include neu-rovascular orofacial pain, (pre-) trigeminal neuralgia, referred painfrom maxillary sinus, ear, carotid artery, heart pathology, and paincaused by intracranial tumor (11). However, other manifestationsneeded for diagnosis, such as suitable systemic signs, ear, nose, throat,or chest symptoms, were not present. Moreover, in all of these condi-tions, although the pulp is the site of the referred pain, pulp extirpationhas not relieved the pain, thus ruling out these conditions in our patient.Pain caused by central nervous system involvement of lymphoma wasalso ruled out in our patient because the pain was localized and affectedbilateral dentition and because of the timing of pain in relation to thetherapy.
After the exclusion of all the above possible conditions, a diagnosisof infiltration by lymphoma cells into the pulp chamber (12–14)causing local pressure and pain was made. This assumption wasruled out retrospectively by histologic examination of the extirpatedpulp tissue. After a comprehensive search of the literature, thepossibility of neuropathic dental pain caused by chemotherapy wasraised (15, 16).
Neurotoxicity in the orofacial structures has been described asdiffuse jaw pain or numbness. However, localized toothache as a mani-festation of such neurotoxicity has not been extensively studied and isnot listed as a possible orofacial complication of administration of cyto-toxic agents (1, 2, 17, 18). Peripheral neurotoxicity and neuropathicpain including thermal (cold or heat) allodynia and hyperalgesia arewell-known complications of several anti-cancer chemotherapeuticagents (19). Facial (oral) cold sensitivity is the most commonly re-ported form of the acute transient neuropathic symptoms ofoxaliplatin-treated colorectal cancer patients, experienced while eatingand drinking. This sensitivity has previously been described as causing‘‘symptoms of short duration that resolve and do not interfere with func-tion’’ and only rarely was debilitating because patients can adapt toavoid cold stimuli (20). The present patient, however, experiencedspontaneous intense pain that was relieved only by pulpectomy. In theirseries of 34 breast cancer patients treated by chemotherapy, McCarthyand Skillings (8) mentioned that one patient undergoing breast cancerchemotherapy suffered from ‘‘dental sensitivity’’ and stated that ‘‘this canbe a complication of chemotherapy.’’ In an additional series ofvincristine-treated patients, 33% and 28% of the patients sufferedfrom dental pain in their maxillary and mandibular teeth, respectively(21). The characteristics of the presented pain case were similar tothose of the so-called atypical odontalgia, ie, a severe throbbing painlocalized to teeth or supporting tissues with no clinical or radiographicpathologic findings, dental procedures (most commonly endodontic
JOE — Volume 36, Number 9, September 2010
therapy, extraction, or apical surgery) might result in temporary relief,but the pain characteristically returns in days or weeks and mightmigrate after the dental procedure (including midline crossing andinvolving both jaws) (22, 23). This similarity strengthens thediagnosis of neuropathic dental pain in the presented patient becauseatypical odontalgia mostly attributed to nerve deafferentation painresulted from peripheral nerve injury (23).
The anti-cancer agent most likely to have induced the pulpneuropathy of our patient is cyclophosphamide; in the first episode,the pain appeared on the third day of cyclophosphamide administra-tion, and in the second episode the pain appeared on the first day ofadministration of cyclophosphamide (Fig. 1). Moreover, in the firstepisode the other agents (cytarabine, doxorubicin, mesna, and rituxi-mab) were administrated a week before the beginning of the pain,and only cyclophosphamide was administrated in proximity to thetime of pain. Generally, cyclophosphamide and its isomer ifosfamidecan induce central manifestations of encephalopathy and changes inmental status (6) and peripheral sensorimotor and autonomic neurop-athy (24). However, the fact that cyclophosphamide is not a well-knownsensory neuropathy causative is a limitation of this hypothesis. Of the 4remaining agents (cytarabine, doxorubicin, mesna, and rituximab) theonly agent that is known to have neurotoxicity as an adverse effect is cy-tarabine (cytosine arabinoside). This agent was reported to induceseveral central neurologic toxicities such as encephalopathy, seizures,cerebellar dysfunction, aseptic meningitis, intrathecal myelopathy(25). However, it is unlikely that cytarabine is the causative agent inthis case because it was not given during the second pain episode.
This case presents a circumstantial relation between the clinicalpresentation of dental pain and the timing of high-dose cyclophospha-mide administrations. It suggests that cytotoxic therapy-induced neuro-toxicity might manifest as a pulpal-type toothache that can presenta diagnostic challenge for the dental practitioner. As mentioned above,the induction of peripheral neuropathy is a clinical problem because itimpairs quality of life and is a common limiting factor of anti-cancerchemotherapy. Pulpal extirpation, although it irreversibly impairsdental pulp vitality and requires later endodontic treatment and rehabil-itation of the tooth, provided immediate relief for the reported pain.More research is needed, however, for the establishment of this entityof chemotherapy-induced neuropathic dental pain and determinationof its optimal management.
References1. Benoliel R, Epstein J, Eliav E, Jurevic R, Elad S. Orofacial pain in cancer: part I—
mechanisms. J Dent Res 2007;86:491–505.2. Elad S, Epstein J, Klasser G, Sroussi H. Orofacial pain in the medically complex
patient. In: Sharav Y, Benoliel R, eds. Orofacial pain and headache. Edinburgh:Mosby Elsevier; 2008:321–48.
3. Benoliel R, Eliav E. Neuropathic orofacial pain. Oral Maxillofac Surg Clin North Am2008;20:237–54.
4. Clark GT, Saravanan R. Orofacial pain and neurosensory disorders and dysfunctionin cancer patients. Dent Clin N Am 2008;52:183–202.
5. Pasetto LM, D’Andrea MR, Rossi E, Monfardini S. Oxaliplatin-related neurotoxicity:how and why? Crit Rev Oncol Hematol 2006;59:159–68.
6. Sioka C, Kyritsis AP. Central and peripheral nervous system toxicity of commonchemotherapeutic agents. Cancer Chemother Pharmacol 2009;63:761–7.
7. Stengel M, Baron R. Oxaliplatin-induced painful neuropathy: flicker of hope orhopeless pain? Pain 2009;144:225–6.
8. McCarthy GM, Skillings JR. Orofacial complications of chemotherapy for breastcancer. Oral Surg Oral Med Oral Pathol 1992;74:172–8.
9. Rossman L, Hasselgren G, Wolcott J. Diagnosis and management of orofacial dentalpain emergencies. In: Cohen S, Hargreaves K, eds. Pathways of the pulp. 9th ed. StLouis, MO: Mosby Elsevier; 2006:40–58.
10. Bender IB. Pulpal pain diagnosis: a review. J Endod 2000;26:175–9.11. Sharav Y, Benoliel R. Acute orofacial pain. In: Sharav Y, Benoliel R, eds. Orofacial
pain and headache. Edinburgh: Mosby Elsevier; 2008:75–90.
Cytotoxic Chemotherapy-induced Odontalgia 1591

Case Report/Clinical Techniques
12. Biggs JT, SabalaZebra C XII. part I—large-cell lymphoma. J Endod 1992;18:570–1.13. Biggs JT, SabalaZebra C XII. part 2—large-cell lymphoma. J Endod 1992;18:632–4.14. Payne M, al-Damouk JD. Gingival swelling as a manifestation of non-Hodgkin’slymphoma. Br Dent J 1993;175:293–4.15. Peterson DE, Sonis ST. Oral complications of cancer chemotherapy: present status
and future studies. Cancer Treat Rep 1982;66:1251–6.16. Rosenberg SW. Oral complications of cancer chemotherapy: a review of 398
patients. J Oral Med 1986;41:93–7.17. Epstein JB, Elad S, Eliav E, Jurevic R, Benoliel R. Orofacial pain in cancer: part II—
clinical perspectives and management. J Dent Res 2007;86:506–18.18. Fischer DJ, Klasser GD, Epstein JB. Cancer and orofacial pain. Oral Maxillofac Surg
Clin North Am 2008;20:287–301.19. Binder A, Stengel M, Maag R, et al. Pain in oxaliplatin-induced neuropathy: sensitisation
in the peripheral and central nociceptive system. Eur J Cancer 2007;43:2658–63.
1592 Zadik et al.
20. Leonard GD, Wright MA, Quinn MG, et al. Survey of oxaliplatin-associated neurotox-icity using an interview-based questionnaire in patients with metastatic colorectalcancer. BMC Cancer 2005;5:116.
21. McCarthy GM, Skillings JR. Jaw and other orofacial pain in patients receiving vincris-tine for the treatment of cancer. Oral Surg Oral Med Oral Pathol 1992;74:299–304.
22. Benoliel R, Heir GM, Eliav E. Neuropathic orofacial pain. In: Sharav Y, Benoliel R,eds. Orofacial pain and headache. Edinburgh: Mosby Elsevier; 2008:255–94.
23. Blasberg B, Eliav E, Greenberg MS. Orofacial pain. In: Greenberg MS, Glick M,Ship JA, eds. Burket’s oral medicine. 11th ed. Hamilton, Ontario, Canada: BC DeckerInc; 2008:257–88.
24. JOE editorial board. Evidence-based review of clinical studies on pharmacology(non-anesthetic studies). J Endod 2009;35:1123–9.
25. Cavaliere R, Schiff D. Neurologic toxicities of cancer therapies. Curr Neurol NeurosciRep 2006;6:218–26.
JOE — Volume 36, Number 9, September 2010

Case Report/Clinical Techniques
Metastasis of Hepatocellular Carcinoma into the Mandiblewith Radiographic Findings Mimicking a Radicular Cyst: ACase ReportHisako Fujihara, DDS, PhD,*
†Daichi Chikazu, DDS, PhD,
†Hideto Saijo, DDS, PhD,
†
Hideyuki Suenaga, DDS, PhD,†
Yoshiyuki Mori, DDS, PhD,†
Mitsuyoshi Iino, DDS, PhD,†
Yoshiki Hamada, DDS, PhD,* and Tsuyoshi Takato, MD, PhD†
Abstract
Introduction: Hepatocellular carcinoma (HCC) isa common neoplasm worldwide, with more than halfof the tumors associated with regional metastasis.Extrahepatic metastasis is also common, and the mostfrequently affected sites are the lungs, abdominal lymphnodes, diaphragm, and bone. However, HCC metastasisto the mandible is rare, with approximately 50 cases re-ported in the literature. Methods: In this report, wedescribe a case of HCC metastasis to the mandible atthe apex of #18 root in a 62-year-old man. This patienthad already been diagnosed with metastasis to pancre-atic caput lymph node. The radiographic features of themandible resembled radicular cyst and did not showtypical findings of malignancy. Results: Under the firstdiagnosis of radicular cyst, root canal treatment wasinitially performed, and then surgical treatment of theremoval of the cystic lesion and #18 extraction were per-formed. Finally, the lesion was diagnosed as HCC metas-tasis from pathological examination. Consequently, hereceived constitutional chemotherapy in the hepatitisunit and is now in remission. Conclusion: This caseshows the importance of considering the differentialdiagnosis of malignancy. (J Endod 2010;36:1593–1596)Key wordsCarcinoma, diagnosis, hepatocellular carcinoma, metas-tasis to mandible, radicular cyst
From the *Department of Oral and Maxillofacial Surgery,School of Dental Medicine, Tsurumi University, Kanagawa,Japan; and †Department of Oral-maxillofacial Surgery, Dentistryand Orthodontics, The University of Tokyo Hospital, Tokyo,Japan.
Address requests for reprints to Dr Hisako Fujihara, Depart-ment of Oral and Maxillofacial Surgery, School of Dental Medi-cine, Tsurumi University, 2-1-3, Tsurumi, Tsurumi-ku,Yokohama, Kanagawa 230-8501, Japan. E-mail address:[email protected]/$0 - see front matter
Copyright ª 2010 American Association of Endodontists.doi:10.1016/j.joen.2010.05.009
JOE — Volume 36, Number 9, September 2010
Hepatocellular carcinoma (HCC) is the fifth most common cancer. It is estimated that8,500 to 11,500 new cases of HCC occur annually in the United States, with a rela-
tively higher frequency reported in Southeast Asia including Japan (1, 2). Among allHCC patients, more than 25% of patients are reported to have extrahepaticmetastasis, with 10.1% of patients showing bone metastasis (3). The preferred site isthe vertebrae, followed by the ribs, sternum, and pelvis in decreasing order. Themandible is an uncommon site of extrahepatic metastasis of HCC. Here, we reporta rare case of HCC metastasis to the mandible with characteristic radiographic findingsmimicking radicular cyst at the apex of the molar root.
Case ReportA 62-year-old Japanese man was referred to the Department of Oral-maxillofacial
Surgery, Dentistry and Orthodontics, the University of Tokyo Hospital, with a chiefcomplaint of slight swelling and discomfort of the left mandible. The symptomswere noticed 1 month previously. He did not suffer from any paralysis, pain, or dyski-nesia. He had a history of HCC caused by hepatitis C infection from a transfusion ofcoagulation factor VIII blood product for hemophilia A. For the treatment of HCC, hehad undergone transcatheter arterial embolization and radiofrequency ablation whenhe was 57 years old. He later underwent resection of the S8 liver area when he was 61years old.
The clinical examination showed a soft, painless slight swelling in the left mandib-ular angle region, with no trismus or neurologic problems such as mental nerve pares-thesia or facial nerve paralysis. Intraorally, he had healthy dentition with good oralhygiene and a normal mucous membrane. There was slight swelling of the buccalside of the #18 gingiva. An old composite resin restoration was noted on the occlusalaspect of #18. The tooth responded negatively to electric pulp vitality test, and nodiscomfort or pain was noted on percussion. On the mesiobuccal aspect of the tooth,the probing depth measured 4 mm, whereas the mobility of the tooth was within normallimits. On panoramic x-ray examination, a radiolucent, well-defined lesion about 20mm in diameter consistent with the appearance of a radicular cyst was observed atthe apex of #18 (Fig. 1). Root absorption of #18 was unclear. On computed tomo-graphic (CT) images, a smooth circular lesion was also observed in the same region.A slight resorption of the buccal cortical bone was observed on horizontal slices (Fig. 2Aand B). The correlation between the apex of #18 and the circular lesion was not cleareven on the CT images, and, unfortunately, dental x-ray examination was impossiblebecause of his vomiting reflex. There were also small circular radiolucent lesions inthe right mandibular body in the #29 and #30 regions. On CT images, these severalsmall circular lesions were also observed on the relatively lingual side of the mandible.
Laboratory data revealed slight anemia (hemoglobin = 11.2 g/dL) and a decreasedplatelet count (8.9� 104 /mm), but other blood cell counts were within normal limits.Coagulation factors were also within normal limits, and his coagulability was as follows:prothrombin time = 12.5 seconds and 71.7%, international normalized ratio = 1.42,activated partial thromboplastin time = 54.7 seconds, and fibrinogen = 239 units.Hepatic-related factors were as follows: lactate dehydrogenase = 264 IU/L, glutamic
A Case of Metastasis of Hepatocellular Carcinoma into the Mandible 1593

Figure 1. Radiologic findings: pantomography at the first referral. The redarrows indicate a radiolucent circular lesion at the apex of #18. There werealso radiolucent lesions in the body of the right mandible below teeth #29and #30.
Case Report/Clinical Techniques
oxaloacetic transaminase = 87 IU/L, glutamic pyruvic transaminase = 74IU/L, gamma-glutamyl transpeptidase = 66 IU/L, and alpha-fetoprotein(ALP) = 346 IU/L. Tumor markers showed relatively high AFP andAFP-L3 (lectin 3) levels of 158.5 ng/mL and 41.1%, respectively.
At his first visit to our department, HCC metastasis to a caputpancreatic lymph node had already been diagnosed based on positronemission tomography-CT images (Fig. 2C), which was consistent withthe high AFP level. On the PET-CT images, high accumulations were
Figure 2. CT and CT-PET images: (A) sagittal CT image. The red arrow indicates ahorizontal CT image. The red arrow indicates slight bone absorption of the outerindicates pancreatic head lymph node metastasis. This diagnosis had already been mthe right premolar region was suggested to be periodontitis of #28 by clinical sympnancy compared with red spot. This lesion was finally diagnosed as HCC metastasi
1594 Fujihara et al.
also observed at the mandibular level (Fig. 2D). The apex of #18showed accumulation, and stronger accumulation was observed inthe #28 region. The standard uptake value (SUV) of the apex of #18was 4.7, and the SUV of the #28 region was 7.9 or 23.7 with artifact.
On comparison with pantomography, periodontitis and the metal-cast prosthetic of #28 were considered to be the cause of the accumu-lation. The SUV of the caput pancreas lymph node was 8.0 and that of theliver was 5.4. These PET-CT images were consistent with other radio-logic findings.
On the basis of these findings, this lesion was diagnosed as a #18radicular cyst with little possibility of malignant tumor or otherpathology unrelated to the tooth. Because his systemic condition waspoor, planned surgical treatment of #18 was amended to root canaltreatment. To start the root canal treatment, a conventional endodonticaccess opening was made with a rubber dam placement. An accesscavity was prepared, and the root canal was instrumented with stainlesssteel hand files until an apical stop of ISO #40 could be created. Persis-tent seepage of dark red, muddy exudate through the root canal dimin-ished gradually with instrumentation. The root canal was irrigatedfrequently with 1.3% sodium hypochlorite followed by a final rinsewith 5 mL sterile saline. Subsequently, sterilized cotton with iodinewas placed, and the access cavity was temporarily sealed with sterilecotton with Sandarac Vanish (G.C., Tokyo, Japan). At the next visit,the root canal was reentered and irrigated alternately with 1.3% sodiumhypochlorite and sterile saline with a crown-down technique.
lesion with a clear, smooth margin resembling a radicular cyst of #18. (B) Aside of the cortical bone. (C) A PET image of the abdomen. The black arrowade before the first referral. (D) A PET image of the oral region. The red spot intoms. The red arrow points to yellow spot that shows less suggestion of malig-s.
JOE — Volume 36, Number 9, September 2010

Case Report/Clinical Techniques
During root canal treatment for 2 months, the swelling of thebuccal mucosa of #18 decreased. However, it suddenly became prom-inent. Therefore, conservative root canal treatment was thought to beineffective for this cystic lesion, so extraction of #18 was inevitable. Atthat time, his general condition had improved, and surgical removalof the cystic lesion concomitant with extraction of #18 was performedunder general anesthesia with replenishment of coagulation factor VIII(Advate; Baxter, Deerfield, IL). Surprisingly, the cystic lesion wascomposed of soft solid tissue suspected to be a tumorous lesion. Thespecimen was pathologically analyzed with hematoxylin-eosin staining,and immunostained for hepatocytes, glypican-3 (GPC-3), alphafetopro-tein (AFP), and cytokeratin (CAM 5.2). Hematoxylin-eosing stainingshowed the lesion to have an alveolar or trabecular pattern. Eosino-philic granules in abundant cytoplasm, mild nuclear pleomorphism,prominent nucleoli, and numerous mitotic figures were observed inthe thick-walled lesion (Fig. 3A and B). Additional immunohistochem-ical study revealed that the tumor cells were positive for hepatocyte-specific antigen (Fig. 3C), GPC-3 (Fig. 3D), and CAM 5.2 (Fig. 3E)
Figure 3. Histopathological findings of the specimen. (A) Hematoxylin-eosinstaining: the lesion was composed of atypical cells showing an alveolar orfascicular pattern, with eosinophilic granules in the cytoplasm. There arewell-developed trabecular patterns and cells with abundant cytoplasm, mildnuclear pleomorphism, prominent nucleoli, and numerous mitotic figures.The bar indicates 50 mm. (B) A higher magnification of the same section.The bar indicates 10 mm. (C-F) Immunohistochemical reaction was positivefor (C) hepatocyte, (D) GPC-3, and (E) CAM 5.2 and negative for (F) AFP. Barsfrom C to F indicate 50 mm.
JOE — Volume 36, Number 9, September 2010
but negative for AFP (Fig. 3F). Considering these findings, this specimenwas diagnosed as HCC metastasis to the oral region.
Immediately after the diagnosis was made, he was transferred tothe hepatitis unit and underwent systemic chemotherapy with fluoro-uracil (5-FU) and irradiation treatment. Since the completion of thistreatment, he has been in remission for 6 months.
DiscussionHCC is the most common malignant tumor of the liver. The number
of new HCC patients is approximately 500,000 to 1 million per year andis increasing (2). HCC usually undergoes intrahepatic metastasis in theearly stages, and only 25% of HCC patients develop extrahepatic metas-tasis. The preferred sites are the lungs (34%-70%), regional lymph no-des (16%-45%), and bone (6% in vertebrae, ribs, and long bones) (4–9). However, HCC metastasis to the mandible is very rare. Since Dick etal (10) first reported a case of HCC metastasis to the mandible in 1957,approximately 50 cases have been documented in the literature to ourknowledge (11–23). Patients ranged from 25 to 88 years, with a meanage of 63.9 years; 47 were male, and 2 were female. The mandible is themost commonly affected area in the oral and maxillofacial region. Thisage and sex predilection resembles that of primary HCC, whichfrequently occurs in men and takes several years to metastasize to theoral and maxillofacial region. Several pathways of HCC metastasis tothe oral region have been postulated. One of them is hematogenouspathway; the tumor reaches the circulation through invasion ofhepatic arterial and/or portal venous branches. Most oral metastasesare associated with lung metastases, and they possibly occur by thisroute (24). Another possible pathway of metastasis is an anastomoticnetwork of paravertebral veins that bypasses the pulmonary, inferiorcaval and portal venous circulations (25, 26). This pathway may beresponsible for metastasis to the vertebral bodies, which are thepreferred site of bony HCC metastasis. This could be the most likelypathway from HCC without pulmonary metastasis, as observed in ourpatient (27, 28).
On the other hand, the mandibular angle and body have a richblood supply, and blood flow slows down in this area, allowing depo-sition of metastatic cells (29). This is the main reason that the mandibleis the most commonly involved region. Moreover, it could also behypothesized that the pulp in tooth #18 became necrotic with a devel-oping periapical lesion. The increased area of inflammation wouldresult in an increased blood flow with more permeable vessel walls,which may allow deposition of metastatic cells. Although the exactpathway of HCC metastasis to the apex of #18 in our patient is stillunclear, the previously mentioned pathways would be reasonablebecause the apex of #18 is positioned near the mandibular angle andbody.
Radiographically, all reported cases of HCC metastasis to themandible showed findings suspicious of tumor, such as tumor massformation in the bone (10–14, 17–19, 21, 23, 24), osteolytic lesions(14, 16, 20, 22), and ill-defined borders (3, 10, 11, 15). Thepresent case was quite different from these reported patients in that(1) the site of metastasis was the apex of #18 and (2) the margin ofthe lesion was clearly defined in x-rays. Moreover, the SUV of the PETof the apex of #18 was only 4.7 although that of the pancreatic caputlymph node metastasis was 8.0. This result did not suggest malignancyof the #18 apex lesion because the SUV of malignant lesions ranges from7.0 to 9.0. Consequently, this patient was not diagnosed as having meta-static HCC to the mandible, and malignancy was excluded initially. Therelation between the #18 root and the lesion was still obscure; there-fore, the lesion was not clarified as being odontogenic or not. The firstperiod of root canal treatment seemed to be effective because swelling
A Case of Metastasis of Hepatocellular Carcinoma into the Mandible 1595

Case Report/Clinical Techniques
of the buccal mucosa decreased. Fortunately, his general condition hadrecovered when the lesion became prominent again, and extraction of#18 and removal of the lesion were performed. Finally, the pathologicaldiagnosis of HCC metastasis to the mandible was made.There were also several small circular radiolucent lesions in theright mandible body in the #29 and #30 region. On CT images, theywere observed on the lingual side in horizontal slices. Moreover, thepatient had never had objective or subjective symptoms in the rightmandible from the first time of his referral. Before starting the root canaltreatment for #18, these lesions were compared with the findings ofpantomography performed by his general practitioner 5 years beforehis treatment. Similar lesions in the right mandible were also observedin the old pantomograph, and their diameters and positions werealmost identical; these lesions were diagnosed as static bone cysts orother benign lesions. There was no cystic lesion at the apex of #18. Afterthe cystic lesion of #18 was diagnosed as HCC metastasis, we consideredrediagnosing with a pathological examination of the right mandibularlesions because they might possibly have had the same diagnosis.
However, we dared to postpone the pathological examination forseveral reasons: (1) the lesions had been there before the cystic lesionof #18 apex occurred; (2) they were deep below the buccal corticalbone, and biopsy would be more invasive and more difficult to coagu-late than the removal of #18 cystic lesion and extraction; and (3) in thecase that they were malignant, chemotherapy would be effective. Sixmonths after chemoradiotherapy, the lesions of the right mandiblehad not increased and did not cause any symptoms. In fact, the definitivediagnosis of the right mandibular radiolucent lesions was still unclear.
Patients with HCC have a relatively good survival rate, with a 5-yearcumulative survival rate of more than 50% when surgical treatment isperformed (30). However, when there is bone metastasis, the survivalrate decreases sharply; 1-year survival is 15% to 20%, and 2-year survivalis around 4% (31–33). The present patient was still alive and inremission 6 months after the diagnosis of HCC metastasis to themandible after effective chemotherapy in the hepatitis unit of our hospital.
In conclusion, this report describes the unusual features of a caseof oral metastatic HCC in which the lesion was located at the apex ofa root with the appearance of a radicular cyst. This case shows that clini-cians should consider the possibility of malignancy in the differentialdiagnosis, even if a malignant lesion is not suggested by the clinical find-ings, especially in patients with a history of a malignant tumor.
References1. Kuhlman JE, Fishman EK, Leichner PK, et al. Skeletal metastases from hepatoma:
frequency, distribution, and radiographic features. Radiology 1986;160:175–8.2. Anthony PP. Hepatocellular carcinoma: an overview. Histopathology 2001;39:109–18.3. Yoshimura Y, Matsuda S, Naitoh S. Hepatocellular carcinoma metastatic to the
mandibular ramus and condyle: report of a case and review of the literature.J Oral Maxillofac Surg 1997;55:297–306.
4. Natsuizaka M, Omura T, Akaike T, et al. Clinical features of hepatocellular carci-noma with extrahepatic metastases. J Gastroenterol Hepatol 2005;20:1781–7.
5. Cha C, Fong Y, Jarnagin WR, et al. Predictors and patterns of recurrence after resec-tion of hepatocellular carcinoma. J Am Coll Surg 2003;197:753–8.
1596 Fujihara et al.
6. Katyal S, Oliver JH, Peterson MS, et al. Extrahepatic metastases of hepatocellularcarcinoma. Radiology 2000;216:698–703.
7. Tunc B, Filik L, Tezer-Filik I, et al. Brain metastasis of hepatocellular carcinoma:a case report and review of the literature. World J Gastroenterol 2004;10:1688–9.
8. Chang JY, Ka WS, Chao TY, et al. Hepatocellular carcinoma with intra-atrial tumorthrombi. A report of three cases responsive to thalidomide treatment and literaturereview. Oncology 2004;67:320–6.
9. Chang L, Chen YL, Kao MC. Intracranial metastasis of hepatocellular carcinoma:review of 45 cases. Surg Neurol 2004;62:172–7.
10. Dick A, Mead SG, Mensh M, et al. Primary hepatoma with metastasis to the mandible.Am J Surg 1957;94:846–50.
11. Pires FR, Sagarra R, Correa ME, et al. Oral metastasis of a hepatocellular carcinoma.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:359–68.
12. Ramon Ramirez J, Seoane J, Montero J, et al. Isolated gingival metastasis from hepa-tocellular carcinoma mimicking a pyogenic granuloma. J Clin Periodontol 2003;30:926–9.
13. Arai R, Otsuka T, Mori K, et al. Metastasis of hepatocellular carcinoma to the supra-maxillary gingiva and right ventricle. Hepatogastroenterology 2004;51:1159–61.
14. Junquera L, Rodriguez RC, Torre A, et al. Hepatocellular carcinoma metastatic to themandible: a case involving severe hemorrhage. Med Oral 2004;9:345–9.
15. Niedzielska I, Langowska AH, Pajak J, et al. Mandible metastasis of hepatocellularcarcinoma. Wiad Lek 2004;57:392–4.
16. Chen SY, Cheng PW, Tsai CC. Pathology quiz case: mandibular metastasis of hepa-tocellular carcinoma. Arch Otolaryngol Head Neck Surg 2005;131:735–6.
17. Teshigawara K, Kakizaki S, Sohara N, et al. Solitary mandibular metastasis as an initialmanifestation of hepatocellular carcinoma. Acta Med Okayama 2006;60:243–7.
18. Han L, Bhan R, Zak I, et al. Metastatic hepatocellular carcinoma to the mandiblemasquerading as a parotid gland mass: a potential pitfall in the diagnosis by fineneedle aspiration biopsy. Diagn Cytopathol 2007;35:674–6.
19. Huang SF, Wu RC, Chang JT, et al. Intractable bleeding from solitary mandibularmetastasis of hepatocellular carcinoma. World J Gastroenterol 2007;13:4526–8.
20. Kamatani T, Tatemoto Y, Tateishi Y, et al. Isolated metastasis from hepatocellularcarcinoma to the mandibular condyle with no evidence of any other metastases:a case report. Br J Oral Maxillofac Surg 2008;46:499–501.
21. Li R, Walvekar RR, Nalesnik MA, et al. Unresectable hepatocellular carcinoma witha solitary metastasis to the mandible. Am Surg 2008;74:346–9.
22. Piot B, Adam P, Sagan C, et al. Mandibular metastasis of hepatocellular carcinoma.Apropos of 3 cases. Rev Stomatol Chir Maxillofac 1994;95:431–4.
23. Zanirato S, Porta C, Moroni M, et al. Jaw bone metastasis from hepatocellular carci-noma. Ital J Gastroenterol Hepatol 1997;29:478–9.
24. Takinami S, Yahata H, Kanoshima A, et al. Hepatocellular carcinoma metastatic tothe mandible. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:649–54.
25. Batson OV. The vertebral system of veins as a means for cancer dissemination. ProgClin Cancer 1967;3:1–18.
26. Batson OV. The function of the vertebral veins and their role in the spread of metas-tases. 1940. Clin Orthop Relat Res 1995;312:4–9.
27. Hirshberg A, Leibovich P, Buchner A. Metastases to the oral mucosa: analysis of 157cases. J Oral Pathol Med 1993;22:385–90.
28. Hirshberg A, Shnaiderman-Shapiro A, Kaplan I, et al. Metastatic tumours to the oralcavity - pathogenesis and analysis of 673 cases. Oral Oncol 2008;44:743–52.
29. Romanas MM, Cherian R, McGregor DH, et al. Hepatocellular carcinoma diagnosedby fine-needle aspiration of the parotid gland. Diagn Cytopathol 2004;30:401–5.
30. Schwarz RE, Smith DD. Trends in local therapy for hepatocellular carcinoma andsurvival outcomes in the US population. Am J Surg 2008;195:829–36.
31. Seong J, Koom WS, Park HC. Radiotherapy for painful bone metastases from hepa-tocellular carcinoma. Liver Int 2005;25:261–5.
32. Taki Y, Yamaoka Y, Takayasu T, et al. Bone metastases of hepatocellular carcinomaafter liver resection. J Surg Oncol 1992;50:12–8.
33. Kaizu T, Karasawa K, Tanaka Y, et al. Radiotherapy for osseous metastases fromhepatocellular carcinoma: a retrospective study of 57 patients. Am J Gastroenterol1998;93:2167–71.
JOE — Volume 36, Number 9, September 2010