Embed Size (px)
Citation preview
Vol. XVII No. 3 JOURNAL OF VASCULAR NURSING PAGE 53
Use of lumbar cerebrospinal fluid drainage in thoracoabdominal aortic aneurysm repairs Susan A. Bethel, MS, RN, CNRN
Thoracoabdominal aortic aneurysm repairs present many challenges,
and the complication of paraplegia remains a concern for both the sur-
geon and the nurse caring for the patient in the postoperative period.
Paraplegia can occur secondary to spinal cord ischemia from prolonged
aortic clamping during the repair of the descending thoracic aorta.
Paraplegia is a devastating complication for the patient and family.
Multiple adjunct techniques have been instituted to prevent reduced
spinal cord peifusion during and after the operation, including the use
of shunts and cardiopulmonary bypass, femoral artery-femoral vein
bypass, left atrial-femoral artery bypass, and selective revasculariza-
tion of the dominant intercostal artery. Other methods, such as
somatosensory evoked potential monitoring during the operation and
regional spinal hypothermia techniques, have not reduced the incidence
of paraplegia. ImpJvved outcomes have been seen with the use of meth-
ods to reduce cerebrospinal fluid (CSF) pressure. One such method is
the use of external CSF drainage during the operation, followed by use
of a lumbar drain system for as long as 72 hours after the operation.
This system setup uses a transducer to monitor CSF pressure and a drip
chamber to drain CSF to maintain a normal pressure. This article
describes thoracoabdominal aneurysms, surgical techniques to repair
the aneurysm, and the use of external CSF drainage and related nurs-
ing care measures. (J Vasc Nurs 1999;17:53-8)
The surgical treatment of the descending thoracic aorta and thoracoabdominal aneurysms involves the vasculature of mul- tiple organs, with the potential for major complications and high operative risk. The devastating complication of paraple- gia, resulting from spinal cord ischemia secondary to aortic clamping during surgery, continues to be reported ranging from 6% to 40%. Multiple adjunct methods have been studied and used to prevent paraplegia, including intercostal artery reim- plantation, assisted circulation with anatomic shunts, cardio- vascular pump bypass, somatosensory evoked potential moni- toring, and, recently, the use of external cerebrospinal fluid drainage (CSFD). CSFD started during the operation and con- tinued after the operation has been shown to improve neuro- logic outcome and prevent the effects of spinal cord ischemia.
ETIOLOGY OF T H O R A C O A B D O M I N A L ANEURYSMS The intrathoracic aorta may have a localized enlargement
of all layers of the aortic wall. This enlargement can extend
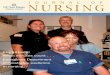
Figure 1. Type H thoracoabdominal aortic aneurysm with multicuff implantation technique for repair. From Moore W. Vascular surger); 4th ed. Philadelphia: WB Saunders; 1993. p. 394. Reprinted with permis- sion of WB Saunders.
from the ascending aorta to the diaphragm and into the abdomen, resulting in a thoracoabdominal aneurysm as shown in Figure 1. This aneurysm continues to dilate and expand and eventually leads to progressive enlargement and rupture. The estimated incidence of thoracic aortic aneurysms is 5.9 cases per 100,000 persons per year. ] Several factors have been cited as etiologies for thoracic aneurysms, including arteriosclero- sis, syphilis, bacterial infections, congenital anomalies, trau- ma, and Marfan 's syndrome. 2 Thoracoabdominal aortic aneurysms (TAA) have been classified into types to better define the extent of the aneurysm. A type I aneurysm extends from below the left subclavian to above the celiac axis. A type II aneurysm extends from below the left subclavian and includes the infrarenal abdominal aorta to the level of the aor- tic bifurcation. A type III aneurysm extends from the sixth intercostal space, tapering to just above the infrarenal abdom- inal aorta to the iliac bifurcation. A type IV aneurysm extends from the twelfth intercostal space, tapering to above the iliac bifurcation. Sail 3 includes a classification as type V aneurysm, which extends from the sixth intercostal space, tapering to just above the renal arteries.
PAGE 54 JOURNAL OF VASCULAR NURSING SEPTEMBER 1999
Anterior Spinal A
Posterolateral S Radicular A. (Adomkiewicz)
Intercostal or Lumber A.)
Infrarenal Radi (From Lumbar A.)
t lA.
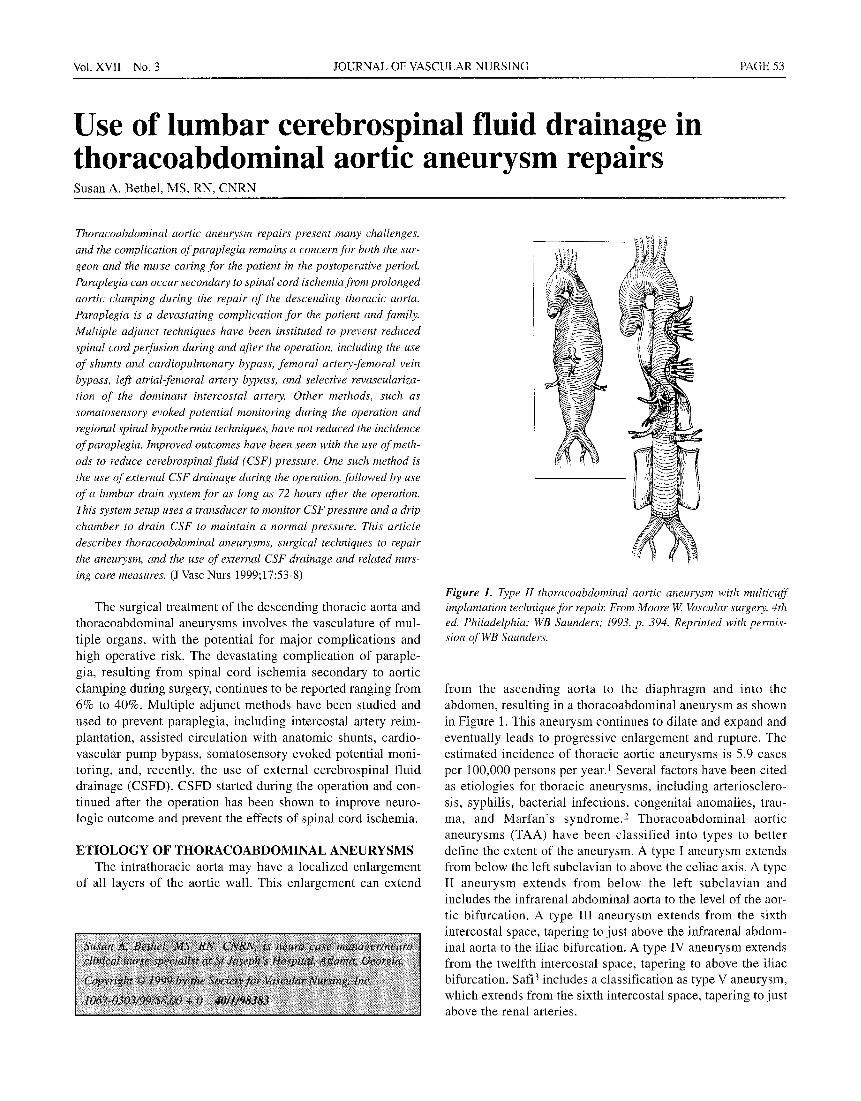
Figure 2. Diagram of the spinal cord blood supply in the lumbosacral segment showing the great radicular artery: Artery of Adamkiewicz supplying the anterior spinal artery. From Szilagyi DE, Hageman JH, Smith RF, Elliott JP. Spinal cord damage in surgery of the abdominal aorta. Surgery 1978;83:38-56. Reprinted with per- mission of Mosby, Inc.
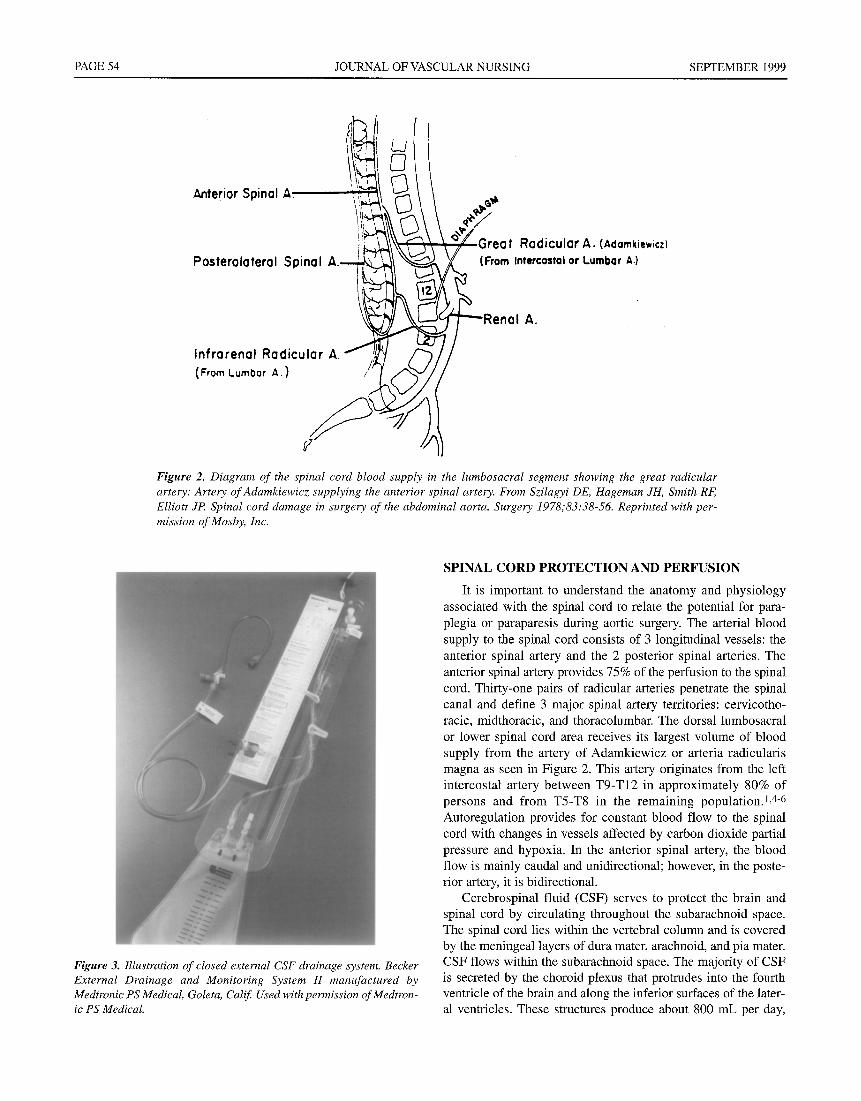
Figure 3. Illustration of closed external CSF drainage system. Becker External Drainage and Monitoring System H manufactured by Medtronic PS Medical, Goleta, Calif. Used with permission of Medtron- ic PS Medical.
SPINAL CORD PROTECTION AND PERFUSION
It is important to understand the anatomy and physiology associated with the spinal cord to relate the potential for para- plegia or paraparesis during aortic surgery. The arterial blood supply to the spinal cord consists of 3 longitudinal vessels: the anterior spinal artery and the 2 posterior spinal arteries. The anterior spinal artery provides 75% of the perfusion to the spinal cord. Thirty-one pairs of radicular arteries penetrate the spinal canal and define 3 major spinal artery territories: cervicotho- racic, midthoracic, and thoracolumbar. The dorsal lumbosacral or lower spinal cord area receives its largest volume of blood supply from the artery of Adamkiewicz or arteria radicularis magna as seen in Figure 2. This artery originates from the left intercostal artery between T9-T12 in approximately 80% of persons and from T5-T8 in the remaining population.], 4-6 Autoregulation provides for constant blood flow to the spinal cord with changes in vessels affected by carbon dioxide partial pressure and hypoxia. In the anterior spinal artery, the blood flow is mainly caudal and unidirectional; however, in the poste- rior artery, it is bidirectional.
Cerebrospinal fluid (CSF) serves to protect the brain and spinal cord by circulating throughout the subarachnoid space. The spinal cord lies within the vertebral column and is covered by the meningeal layers of dura mater, arachnoid, and pia mater. CSF flows within the subarachnoid space. The majority of CSF is secreted by the choroid plexus that protrudes into the fourth ventricle of the brain and along the inferior surfaces of the later- al ventricles. These structures produce about 800 mL per day,
Vol. XVII No. 3 JOURNAL OF VASCULAR NURSING PAGE 55
and the pressure of the CSF system is normally about 10 mm Hg. CSF is reabsorbed by the arachnoid granulations, which are pro- jections from the subarachnoid space, and flows back into the venous sinuses of the brain.
Whenever circulation to the spinal cord is compromised by reduction in blood flow, spinal cord infarction results. Spinal cord ischemia can occur during the aortic cross clamp period of thoracoabdominal aneurysm surgical repair. In animal models, the maximum ischemic time for the spinal cord is 8 minutes. 7 Sustained hypotension in the lower body can lower spinal cord perfusion, and a rise in CSF pressure further impairs spinal cord circulation. The pathways in the spinal cord are tightly arranged, and small infarctions can produce signs and symptoms. The clin- ical signs will depend on the vascular territory involved and may
include paraparesis, tetraparesis, paraplegia, or loss of bowel or bladder sphincter control.
SURGICAL REPAIR OF THORACOABDOMINAL AORTIC ANEURYSMS
Lain and Aram were successful in surgically treating tho- racic aneurysms in 1951 with a clear transparent plastic tube in an aortic homograft. Etheredge et al performed the first thora- coabdominal aneurysmectomy with a homograft, temporary aorto-aortic shunt, and reimplantation of the celiac and superi- or mesenteric artery into the graft. 5 Crawford changed the sur- gical techniques in the 1980s by leaving the posterior wall of the aneurysm and implantation of the celiac, superior mesen- teric artery, and renal arteries into a prosthetic graft. Surgical
PAGE 56 JOURNAL OF VASCULAR NURSING SEPTEMBER 1999
repair of this aneurysm requires an incision in the fourth or fifth intercostal space for a type I or II aneurysm or at the level of seventh to ninth interspace for a type III aneurysm. The length of time for aortic clamping during resection contributes to the risk for spinal cord ischemia. The risk has been shown to increase with cross clamp times exceeding 30 minutes) Pro- longed aortic clamping results in sustained hypotension and lower spinal cord perfusion. Selective spinal angiography before surgery to identify the patency of a critical intercostal or lumbar artery can help to identify if it arises from the aneurys- real wall and will increase the risk of postoperative paralysis, s To reduce the incidence of spinal cord ischemia, the intercostal arteries, if patent and supplying the spinal cord circulation, are reimplanted between T8 and L1 level. The addition of left atri- al to left femoral bypass or distal aortic perfusion during the surgical procedure is also used to augment spinal cord perfu- sion. Other intraoperative adjunctive techniques have been used, including the use of hypothermia and somatosensory or motor-evoked potential monitoring. 6-8
Studies have reported 5-year survival rates of 7% to 19% for untreated thoracoabdominal aneurysms. Survival after repair has been reported as a 5-year survival rate of as high as 59% percent. Several complications can occur with extensive operative repair, such as myocardial infarction, renal failure, pulmonary insuffi- ciency, and stroke. The devastating complication of paraplegia remains a major complication, with rates ranging from 6% to 40%.6,9,10
EXTERNAL CSF DRAINAGE The current knowledge of spinal cord ischemia associated
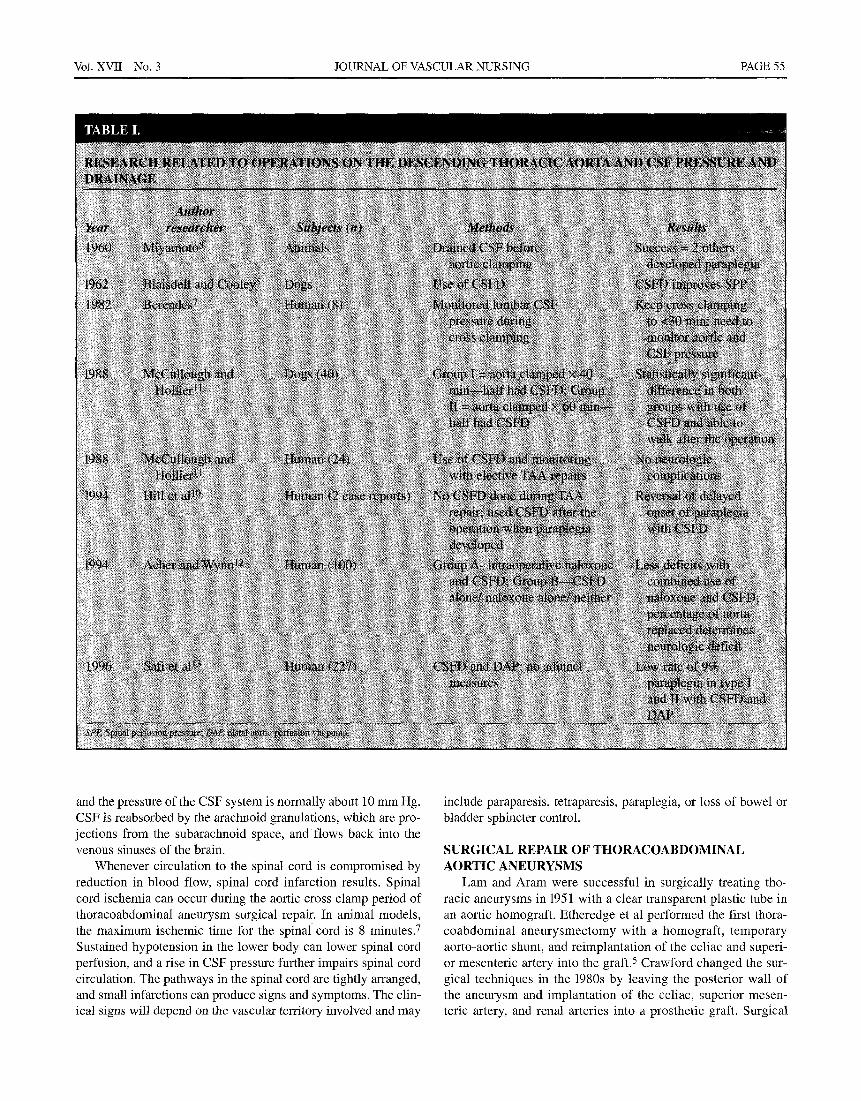
with thoracoabdominal aortic aneurysm repair has evolved from animal research and clinical experience as outlined in Table 1. This table outlines several studies in which CSF pressure was measured and drained during thoracoabdominal aneurysm oper- ations.
Studies have shown that distal aortic pressure decreases markedly during cross clamping and thus causes a decrease in spinal artery pressure and a rise in CSF pressure of 30% to 100%
Vol. XVII No. 3 JOURNAL OF VASCULAR NURSING PAGE 57
higher than baseline values.ll Clinical research during the 1990s used sequential clamping of the aorta and reimplantation of patent intercostal arteries. The use of CSF drainage was initiated before aortic clamping and continued after the operation for as long as 72 hours. CSF pressure was monitored to maintain pres- sure at <10 mm Hg, with intermittent drainage as needed. Researchers concluded that drainage of CSF during the opera- tion and as long as 3 days after the operation can lower the inci- dence of neurologic complications. Sail 3 reported the paraplegia rate decreased to 9%.
Reduction of CSF pressure by lumbar spinal drainage can help to maintain a sufficient perfusion gradient between the local spinal arterial and venous pressures and serves to maintain some cord blood flow.1 External drainage can also permit a longer safe period to allow reinclusion of vital arteries into a thoracoabdom- inal prosthetic graft.
L U M B A R DRAINAGE SETUP During the operative preparation and after intubation and
anesthesia induction, the anesthesiologist inserts a spinal needle into the subarachnoid space at the L4-5 intervertebral space. The lumbar drainage catheter is advanced through the needle to approximately the T12-L1 space. The needle is withdrawn, and the lumbar catheter is left in place. The catheter is secured to the skin and covered with a sterile occlusive dressing. During the operation, the anesthesiologist may use the catheter to manually withdraw CSE An external CSF drainage system must be set up
with sterile technique and filled with sterile isotonic preservative free saline before connecting to the lumbar catheter. An example of this system is seen in the photograph in Figure 3. A nonflush transducer is attached to the system and connected to the bedside monitor with the stopcock open to the transducer and patient line to obtain a waveform and pressure value. The transducer must be attached at the zero reference level of the system and then zeroed to atmospheric pressure when connected to the bedside monitor. The transducer at the zero reference line must be aligned to an anatomic level of the patient before monitoring of CSF pressure. The zero reference level for the system is usually the spinal cord level or the site of the catheter. The surgeon should verify the spe- cific anatomic patient level for zeroing to be used if different. The CSF drip chamber with its reference level must be moved up to the pressure level of 10 mm Hg or as ordered by the physician. Most systems have premarked levels in either millimeters of mer- cury or centimeters of water for setting the correct drip chamber level. The surgeon will order the CSF pressure (either millimeters of mercury or centimeters of water) to be maintained. When CSF pressure exceeds the ordered level, the cerebrospinal spinal fluid is drained into the drip chamber and measured.
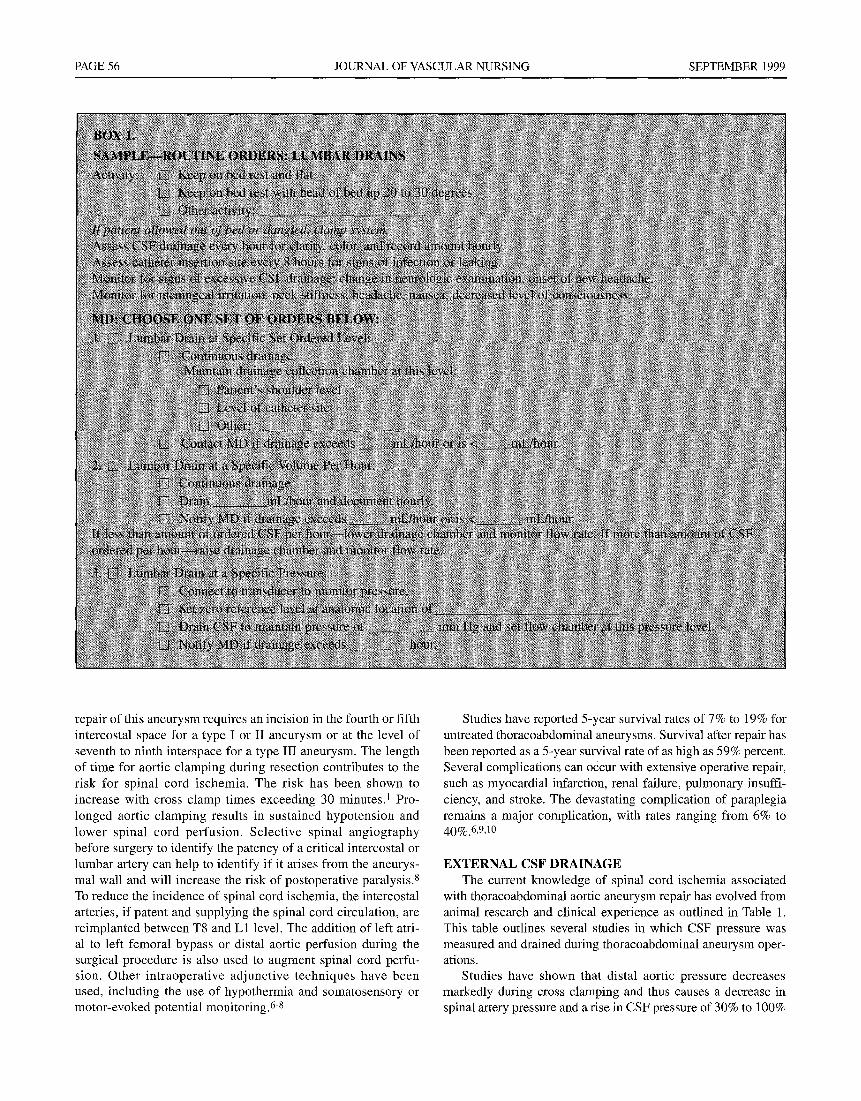
Lumbar drains are indicated for the treatment of various other types of problems. Lumbar drainage can also be used for treat- ment of postoperative or traumatic dural fistulae (cerebrospinal leaks). There are 3 types of lumbar drain management tech- niques: (1) draining at a specific level, (2) draining to a specified volume, and (3) draining at a specified pressure) 4 A sample of

PAGE 58 JOURNAL OF VASCULAR NURSING SEPTEMBER 1999
standing orders, which were developed for all 3 types of drain management, are found in Box 1 and can be used. The purpose of the use of lumbar drains with thoracoabdominal aneurysm repair is to drain to maintain a specified pressure. This type of drainage is shown as option No. 3 on these standing orders.
When draining CSF, the fluid will drain into the drip cham- ber until the preset level of millimeters of mercury is achieved. When the system is set to monitor pressure, no CSF is drained into the drip chamber. When CSF pressure exceeds the specific ordered pressure level, the stopcock is opened to drain the CSF and turned off to monitoring of the pressure.
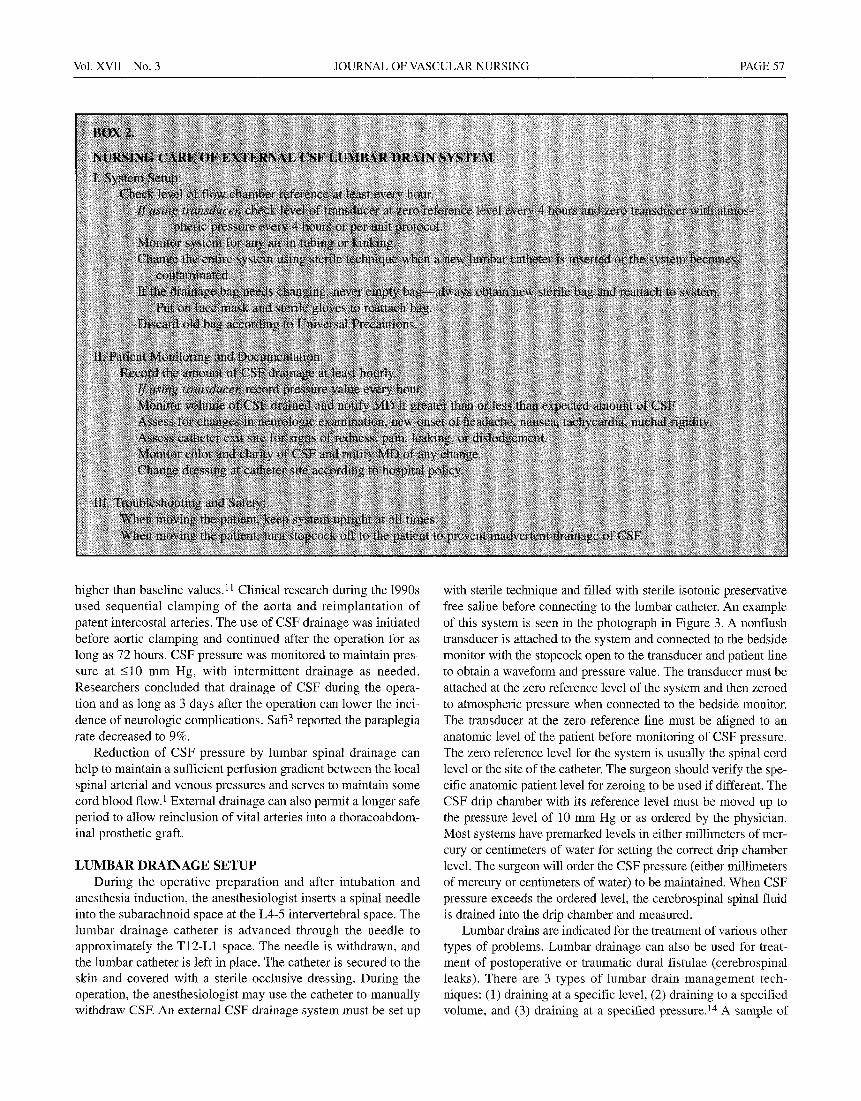
NURSING CARE OF CSF LUMBAR SYSTEM Specific key components of nursing care are outlined in
Box 2. The external CSF drainage system must be maintained as a closed system at all times during the postoperative phase. A comprehensive neurologic assessment should be done at least every hour or per hospital policy. Clarify with the physician spe- cific orders for level of activity and whether head of bed should be elevated. The lumbar catheter and closed CSF drainage system is maintained for a period of 48 to 72 hours after the operation, and the CSF pressure and volume of drainage closely monitored.
A working knowledge of thoracoabdominal aneurysms and the effects of prolonged aortic clamping during surgical repair are important for the nurse in the postoperative phase. Neuro- logic assessment, especially of motor functioning of the lower extremities and bowel and bladder functioning, must be included in the care plan. Other potential complications that need to be considered are myocardial infarction, renal failure, pulmonary insufficiency, and stroke. Aseptic tech- nique becomes essential in the maintenance of the lumbar catheter and the closed external CSF drainage system to pre- vent infection. The nurse must know the normal characteris- tics of CSF, the pressure level to be maintained, and assess for signs of abnormal CSF drainage.
Key aspects of patient education to be included in the care plan are an explanation of why the lumbar catheter is being used, the importance of adhering to activity limitations, and the safety measures to ensure patency of the drainage system.
SUMMARY The use of a lumbar drainage system for a patient after tho-
racoabdominal aneurysm repair operation can offer an adjunc- tive treatment and preventative measure to avoid neurologic complications. Repair of thoracoabdominal aneurysms has been studied extensively to determine best practice for the prevention of paraplegia. Surgical technique during repair to avoid pro- longed aortic clamping and the maintenance of spinal cord per- fusion pressure has been shown to reduce the effects of spinal cord ischemia. An effective method is to monitor CSF pressure during and after the operation and include the capability to drain CSF to maintain a normal pressure.
A thorough understanding of the dynamics of spinal cord circulation, spinal perfusion pressure, CSF, and the skill of maintaining a closed lumbar drainage system can enhance the nursing care of postoperative TAA patients. The vascular nurse,
with expertise in the care of the thoracic surgery patient, can be instrumental in the prevention and reduction of major com- plications.
REFERENCES 1. Fann J, Miller D. Descending thoracic aortic aneurysms In:
Bane A, Geha A, Laks H, Hammond G, Naunheim K, editors. Glenn's thoracic and cardiovascular surgery. Stan- ford: Appleton & Lange; 1996. p 2255-72.
2. Cohn L. Thoracic aortic aneurysms and aortic dissection. In: Sabiston D, Spencer F, editors. Surgery of the Chest. Philadelphia: WB Saunders; 1990. p. 1182-91.
3. Sail H, Campbell M, Ferreira M, Azizzadeh A, Miller C. Spinal cord protection in descending thoracic and thoracoab- dominal aortic aneurysm repair. Semin Thorac Cardiovasc Surg 1998;10;41-4.
4. Benevente O, Barnett H. Spinal Cord Ischemia. In: Barnett H, Mohr S, Stein B, Yatsu F, editors. Stroke pathophysiology diagnosis and management. New York: Churchill Living- stone; 1998. p. 571-765.
5. Connolly J. Prevention of spinal cord complications in aortic surgery. J Surg 1998;176:92-101.
6. Griepp R, Ergin M, Galla J, Lansman S, Khan N, Quintana C, et al. Looking for the artery of Adamkiewicz: a quest to minimize paraplegia after operations for aneurysms of the descending thoracic and thoracoabdominal aorta. J Thorac Cardiovasc Surg 1996; 112:1202-15.
7. Berendes J, Bredee J, Schipperheyn J, MashourY. Mechanisms of spinal cord injury after cross-clamping of the descending thoracic aorta. Circulation 1982;66(Suppl I):I-112-I-116.
8. Drenger B, Parker S, Frank S, Beattie C. Changes in cere- brospinal fluid pressure and lactate concentrations during thoracoabdominal aortic aneurysm surgery. Anesthesiology 1997;86:41-7.
9. Crawford E, Svensson L, Hess K, Shenaq S, Cosellli J, Sail H, et al. A prospective randomized study of cerebrospinal fluid drainage to prevent paraplegia after high risk surgery on the thoracoabdominal aorta. J Vasc Surg 1991; 13:36-45.
10. Hill A, Kalman R Johnston K, Vosu H. Reversal of delayed- onset paraplegia after thoracic aortic surgery with cere- brospinal fluid drainage 1994;20:315-7.
11. McCullough J, Hollier L, Nugent M. Paraplegia after tho- racic aortic occlusion influence of cerebrospinal fluid drainage. J Vasc Surg 1988;7:153-60.
12. Acher C, Wynn M, Hoch J, Popic P, Archibald J, Turnipseed W. Combined use of cerebral spinal fluid drainage and naloxone reduces the risk of paraplegia in thoracoabdominal aneurysm repair. J Vasc Surg 1994;19:236-48.
13. Sail HJ, Hess KR, Randel M, lliopoulos DC, Baldwin JC, Mootha RK, et al. Cerebrospinal find drainage and distal aortic perfusion: reducing neurologic complications in repair of thoracoabdominal aortic aneurysm types I and 1I. J Vasc Surg 1996;23;223-8.
14. Thompson H. Lumbar drain management; clinical guideline series. Chicago: American Association of Neuroscience Nurses; 1998.