Embed Size (px)
Citation preview

BritishJournal ofOphthalmoloV, 1990,74,458-461
Oral fluorescein angiography: reassessment of itsrelative safety and evaluation of optimum conditionswith use of capsules
A P Watson, E S Rosen
AbstractInjection of fluorescein intravenously forfundal angiography is associated with a highincidence of minor adverse effects (21%) but avery low incidence of serious (life threatening)reactions (0.05%). A serious reaction may occurwithout warning in a patient with no history ofatopy. There are no reports of oral fluoresceincausing a serious reaction, and minor adverseeffects are uncommon. A study was under-taken to determine optimum conditions fororal fluorescein angiography. Capsules provedmore convenient than a solution for ingestionof fluorescein. A dose of 25 mg/kg body weightproduced good quality angiograms in 75% ofthe patients. The best pictures were obtainedby photographing the fundus after 40 and 60minutes.
Fluorescein fundal angiography (FFA) hasbecome progressively established as a valuableclinical investigation since the technique wasdescribed in detail in 1961.' When fluoresceinis given intravenously reactions can occur.Giving the fluorescein orally makes the risk ofa serious reaction minimal and greatly reducesthe incidence of minor reactions. Previousauthors have already reported that goodquality angiograms can be produced with oralfluorescein,>4 though high intensity earlypasses do not occur.The aims of this study were to evaluate the
use of oral fluorescein in capsule form, todetermine if there is a dose which will reliablygive good quality angiograms, and to discoverthe best time to photograph the fundus afterthe capsules have been taken.
Southport DistrictGeneral Hospital,SouthportA P Watson
Manchester Royal EyeHospital, Oxford Road,ManchesterE S RosenCorrespondence to:A P Watson, FRCS, DistrictGeneral Hospital, Southport,Merseyside PR8 6NJ.Accepted for publication15 February 1990
Materials and methodsAfter the approval of the ethical committee 20healthy volunteers were recruited from the staffof Manchester Royal Eye Hospital and wereasked to give written consent. The subjects wereasked to fast for six hours before being given atest dose of 10 mg of fluorescein in liquid formand being weighed. If over the next half hourthey experienced no symptoms such as faintness,warmth, or itching suggestive of an allergicreaction, they were then given a larger dose incapsule form.* The patients were randomlyassigned to one of five groups, to be given 1, 1-5,*Capsules of sodium fluorescein 500 mg were formulated andprepared by Jill Bumphrey, MPS, at the Leicestershire HealthAuthority District Pharmacy, Leicester Royal Infirmary,Leicester. The raw material specification was fluorescein sodiumBP, NWRHA specification, supplied by Societe Chimique PointetGorard. The pharmacy can supply the capsules at a cost ofapproximately £10 per 100.
2, or 2 5 g of fluorescein. One pupil was dilatedwith tropicamide 1%, plus phenylephrine 10% ifnecessary.
Fundal photographs were taken with either aCanon CF-60U or Kowa Pro I fundus camera20, 30, 40 and 60 minutes after the capsules hadbeen swallowed. The film used was Ilford FP4rated to 800 ASA. The films were developed inKodak D76 for 30 minutes at 20C.
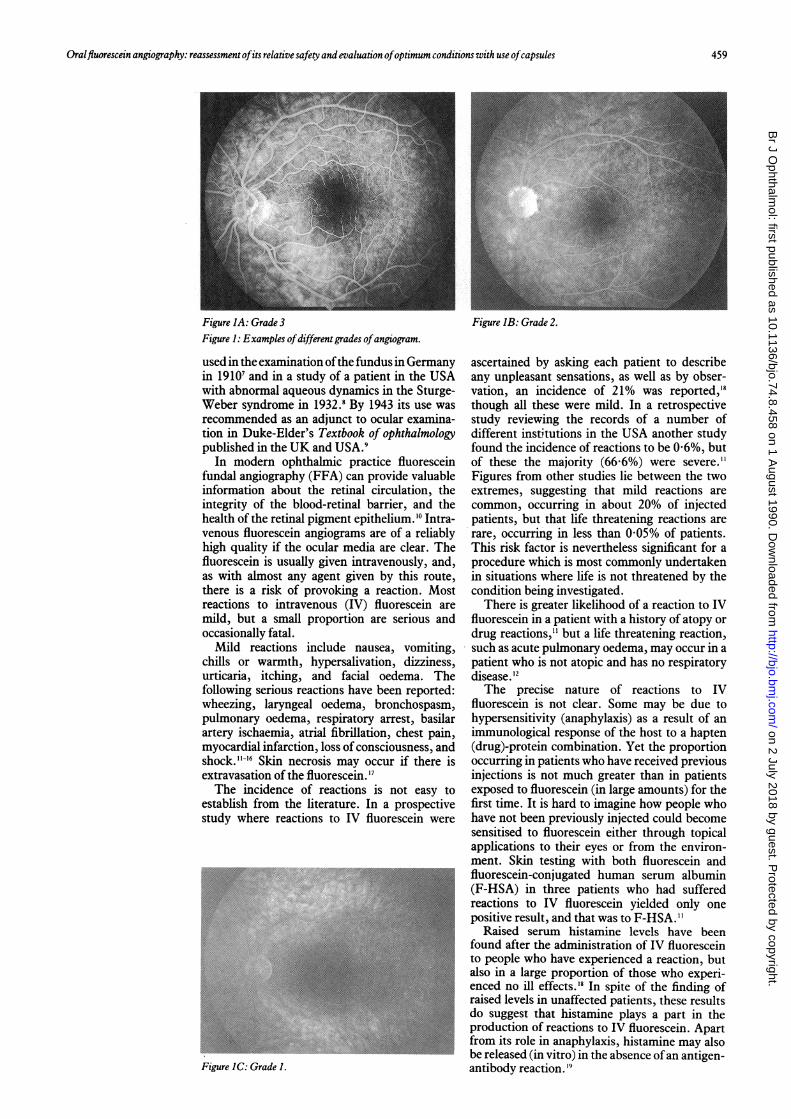
ResultsThe 80 angiograms were graded into fourcategories: 3=strong fluorescence; 2=moderatefluorescence; 1=faint fluorescence; 0=no usefulfluorescence.
Grade 3 angiograms were comparable inquality with those produced by intravenousfluorescein. Grade 2 angiograms were also ofgood quality, and any abnormal leakage wouldbe readily seen. In the grade 1 angiograms thedisc and macula could be distinguished and itwould be possible to recognise any major leakage.However, small amounts of late leakage might bemissed. Grade 0 angiograms did not show anysignificant degree of fluorescence, and fundalfeatures could not be distinguished. Examples ofangiograms from categories 1, 2, and 3 are shownin Figure 1.
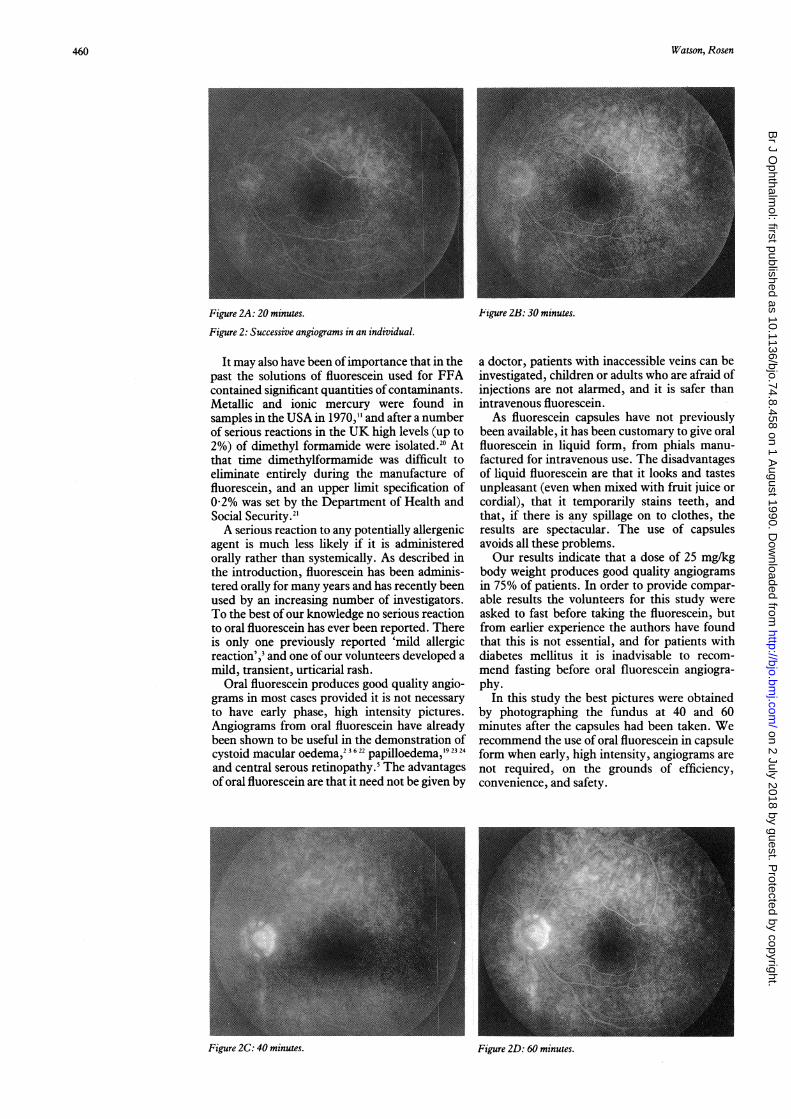
For 15 of the 20 volunteers one or moreangiograms in grade 2 or 3 were produced, and12 of these 15 had one or more grade 3 angio-grams. All except one had been given a dose offluorescein equivalent to at least 25 mg/kg bodyweight. The best quality angiograms wereobtained at 40 or 60 minutes after they had takenthe capsules, though good quality angiogramscould also be obtained at 30 minutes in somecases. An example of progression offluorescencein successive angiograms is shown in Figure 2.For five of the 20 subjects no useful angio-
grams were obtained. In four of these five therewas no visible fluorescence. Although two of thefive had been given fluorescein equivalent to lessthan 15 mg/kg body weight, the other three hadreceived a dose of over 30 mg/kg.None of the subjects experienced any reaction
to the test dose of liquid fluorescein. After takingthe capsules one person developed a mildurticarial rash on the extensor surfaces of herarms and legs. She experienced no other illeffects. She was given chlorpheniramine maleate4 mg by mouth, and the rash resolved over thenext four hours.
DiscussionFluorescein was first synthesised in 1871. It was
458
on 2 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.8.458 on 1 August 1990. D
ownloaded from
Oralfluorescein angiography: reassessment ofits relative safety andevaluation ofoptimum conditions with use ofcapsules
Figure IA: Grade 3Figure 1: Examples ofdifferent grades ofangiogram.
used in the examination ofthe fundus in Germanyin 19107 and in a study of a patient in the USAwith abnormal aqueous dynamics in the Sturge-Weber syndrome in 1932.8 By 1943 its use wasrecommended as an adjunct to ocular examina-tion in Duke-Elder's Textbook of ophthalmologypublished in the UK and USA.9
In modern ophthalmic practice fluoresceinfundal angiography (FFA) can provide valuableinformation about the retinal circulation, theintegrity of the blood-retinal barrier, and thehealth of the retinal pigment epithelium.'0 Intra-venous fluorescein angiograms are of a reliablyhigh quality if the ocular media are clear. Thefluorescein is usually given intravenously, and,as with almost any agent given by this route,there is a risk of provoking a reaction. Mostreactions to intravenous (IV) fluorescein aremild, but a small proportion are serious andoccasionally fatal.Mild reactions include nausea, vomiting,
chills or warmth, hypersalivation, dizziness,urticaria, itching, and facial oedema. Thefollowing serious reactions have been reported:wheezing, laryngeal oedema, bronchospasm,pulmonary oedema, respiratory arrest, basilarartery ischaemia, atrial fibrillation, chest pain,myocardial infarction, loss ofconsciousness, andshock.'11-6 Skin necrosis may occur if there isextravasation of the fluorescein."7The incidence of reactions is not easy to
establish from the literature. In a prospectivestudy where reactions to IV fluorescein were
Figure IC: Grade 1.
Figure IB: Grade 2.
ascertained by asking each patient to describeany unpleasant sensations, as well as by obser-vation, an incidence of 21% was reported,'8though all these were mild. In a retrospectivestudy reviewing the records of a number ofdifferent institutions in the USA another studyfound the incidence of reactions to be 0-6%, butof these the majority (66 6%) were severe."Figures from other studies lie between the twoextremes, suggesting that mild reactions arecommon, occurring in about 20% of injectedpatients, but that life threatening reactions arerare, occurring in less than 0 05% of patients.This risk factor is nevertheless significant for aprocedure which is most commonly undertakenin situations where life is not threatened by thecondition being investigated.There is greater likelihood of a reaction to IV
fluorescein in a patient with a history of atopy ordrug reactions," but a life threatening reaction,such as acute pulmonary oedema, may occur in apatient who is not atopic and has no respiratorydisease. 12The precise nature of reactions to IV
fluorescein is not clear. Some may be due tohypersensitivity (anaphylaxis) as a result of animmunological response of the host to a hapten(drug)-protein combination. Yet the proportionoccurring in patients who have received previousinjections is not much greater than in patientsexposed to fluorescein (in large amounts) for thefirst time. It is hard to imagine how people whohave not been previously injected could becomesensitised to fluorescein either through topicalapplications to their eyes or from the environ-ment. Skin testing with both fluorescein andfluorescein-conjugated human serum albumin(F-HSA) in three patients who had sufferedreactions to IV fluorescein yielded only onepositive result, and that was to F-HSA."
Raised serum histamine levels have beenfound after the administration of IV fluoresceinto people who have experienced a reaction, butalso in a large proportion of those who experi-enced no ill effects.'8 In spite of the finding ofraised levels in unaffected patients, these resultsdo suggest that histamine plays a part in theproduction of reactions to IV fluorescein. Apartfrom its role in anaphylaxis, histamine may alsobe released (in vitro) in the absence ofan antigen-antibody reaction. '9
459
on 2 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.8.458 on 1 August 1990. D
ownloaded from
Watson, Rosen
Figure 2A: 20 minutes.
Figure 2: Successive angiograms in an individual.
It may also have been ofimportance that in thepast the solutions of fluorescein used for FFAcontained significant quantities of contaminants.Metallic and ionic mercury were found insamples in the USA in 1970,"1 and after a numberof serious reactions in the UK high levels (up to2%) of dimethyl formamide were isolated.20 Atthat time dimethylformamide was difficult toeliminate entirely during the manufacture offluorescein, and an upper limit specification of0-2% was set by the Department of Health andSocial Security.2'A serious reaction to any potentially allergenic
agent is much less likely if it is administeredorally rather than systemically. As described inthe introduction, fluorescein has been adminis-tered orally for many years and has recently beenused by an increasing number of investigators.To the best of our knowledge no serious reactionto oral fluorescein has ever been reported. Thereis only one previously reported 'mild allergicreaction',' and one of our volunteers developed amild, transient, urticarial rash.
Oral fluorescein produces good quality angio-grams in most cases provided it is not necessaryto have early phase, high intensity pictures.Angiograms from oral fluorescein have alreadybeen shown to be useful in the demonstration of
2316 22 192324cystoid macular oedema, papilloedema,and central serous retinopathy.5 The advantagesof oral fluorescein are that it need not be given by
Figure 2B: 30 minutes.
a doctor, patients with inaccessible veins can beinvestigated, children or adults who are afraid ofinjections are not alarmed, and it is safer thanintravenous fluorescein.As fluorescein capsules have not previously
been available, it has been customary to give oralfluorescein in liquid form, from phials manu-factured for intravenous use. The disadvantagesof liquid fluorescein are that it looks and tastesunpleasant (even when mixed with fruit juice orcordial), that it temporarily stains teeth, andthat, if there is any spillage on to clothes, theresults are spectacular. The use of capsulesavoids all these problems.Our results indicate that a dose of 25 mg/kg
body weight produces good quality angiogramsin 75% of patients. In order to provide compar-able results the volunteers for this study wereasked to fast before taking the fluorescein, butfrom earlier experience the authors have foundthat this is not essential, and for patients withdiabetes mellitus it is inadvisable to recom-mend fasting before oral fluorescein angiogra-phy.
In this study the best pictures were obtainedby photographing the fundus at 40 and 60minutes after the capsules had been taken. Werecommend the use of oral fluorescein in capsuleform when early, high intensity, angiograms arenot required, on the grounds of efficiency,convenience, and safety.
Figure 2D: 60 minutes.
460
Figure 2C: 40 minutes.
on 2 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.8.458 on 1 August 1990. D
ownloaded from

Oralfluorescein angiography: reassessment ofitsirelative safety and evaluation ofoptimum conditions with use ofcapsules
All the photographs were taken by Richard Hancock (generalmedical photographer) and Adam Prest (medical research pho-tographer), whose skill and commitment enabled this study tocome to a successful conclusion.The authors wish to thank those friends and colleagues at
Manchester Royal Eye Hospital who volunteered to take oralfluorescein for this study, which would not have been possiblewithout their involvement.
1 Novotny HR, Alvis DL. A method of photographingfluorescence in circulating blood in the human retina.Circulation 1%1; 24: 82-6.
2 Kelley JS, Kincaid M. Retinal fluorography using oralfluorescein. Arch Ophthalmol 1979; 97: 2331-2.
3 Kelley JS, Kincaid M, Hoover RE, McBeth C. Retinalfluorograms using oral fluorescein. Ophthalmology 1980; 87:805-11.
4 Oral fluorescein study group. Oral fluorography. J Am OptomAssoc 1985; 56: 784-92.
5 Azad R, Nayak BK, Tewari HK, Khosola PK. Oralfluorescein angiography. Indian J Ophthalmol 1984; 32:415-7.
6 Noble MJ, Cheng H, Jacobs PJ. Oral fluorescein and cystoidmacular oedema: detection in aphakic and pseudophakiceyes. BrJ Ophthalmol 1984; 68: 221-4.
7 Burk A. Die klinische, physiologische und pathologischeBedeutung der Fluoreazenz in augenach Darreichung vonUranin. Klin Monatsbl Augenheilkd 1910; 48: 445-54.
8 Tyson HH. Nevus flammeus of the face and globe associatedwith glaucoma, vascular changes in the iris and a calcifiedvascular growth in the occipital lobe of the brain, with righthomonymous hemianopia. Arch Ophthalmol 1932; 8: 365-71.
9 Duke-Elder S. Textbook ofophthalmology. London: Kimpton,1943:2:1150.
10 Rosen ES. Fluorescence photography of the eye. London:Butterworths, 1%9.
11 Stein MR, Parker CW. Reactions following intravenousfluorescein. AmJr Ophthalmol 1971; 72: 861-8.
12 Hess JB. Pacuraiu RJ. Acute pulmonary edema followingintravenous fluorescein angiography. Am J Ophthalmol1976;82: 567-70.
13 Kirson LE, Wilson ME. Atrial fibrillation associated withintravenous fluorescein. Anesth Analg 1987; 66: 283.
14 Butner RW, McPherson AR. Adverse reactions in intra-venous fluorescein angiography. Ann Ophthalmol 1983; 15:1084-6.
15 Karhunen U, Raitta C, Kala R. Adverse reactions tofluorescein angiography. Acta Ophthalmol (Kbh) 1986; 64:282-6.
16 Yannuzzi LA, Roherer KT, Tindel LG, et al. Fluoresceinangiography complication survey. Ophthalmology 1986; 93:611-7.
17 Elman MJ, Fine SL, Sorenson J, et al. Skin necrosis followingfluorescein extravasation. A survey of the macula society.Retina 1987; 7: 89-93.
18 Arroyave CM, Wolbers R, Ellis PP. Plasma comple-ment and histamine changes after intravenous administra-tion of sodium fluorescein. Am J Ophthalmol 1979; 87:474-9.
19 Eustace P, Travers S, Mooney D. Oral Fluorescein angio-graphy in disc oedema. Bull Soc Belge Ophtalmol 1984; 211:35-41.
20 Jacob JSH, Rosen ES, Young E. Report on the presence of atoxic substance, dimethyl formamide, in sodium fluoresceinused for fluorescein angiography. BrJ7 Ophthalmol 1982; 66:567-8.
21 Buckley H. Fluorescein injection. DHSS communication.Reference no. 2-10/81. 23 June 1982.
22 Morgan KS, Franklin RM. Oral fluorescein angioscopy inaphakic children.J Pediatr Ophthalmol Strabismus 1984; 21:33-6.
23 Ghose S, Nayak BK. Role oforal fluorescein in the diagnosis ofearly papilloedema in children. BrJr Ophthalmol 1987; 71:910-5.
24 Bynke HG. Differentiation of papilloedema from pseudo-papilloedema by fluorescein ophthalmoscopy. Acta Ophthal-mol (Kbh) 1970; 48: 752-8.
461
on 2 July 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.8.458 on 1 August 1990. D
ownloaded from