Embed Size (px)
DESCRIPTION
stemi
Citation preview
BY :Juliet C G Umbas (C11108204)
SUPERVISOR :Prof. Dr. dr. Peter Kabo, Ph.D, Sp.FK, Sp.JP, FIHA
Case Report
• MR number : 607725• Name : Mr. E• Gender : Male• Age : 57 years old• Date administered : 27th April 2013
Chief complaint: Chest pain
• It was felt ± 12 hours ago before admitted to the hospital. The location
was at the center of the chest and penetrated to the back, and radiated to
the neck, jaw, and left arm. The pain was described as ‘squeezed’.
Duration of chest pain attack was around 20 minutes, triggered by
activity, and did not relieved by rest. During the attack, patient feel
shortness of breath, sweating and nausea. Vomit (-), epigastric pain (-),
cough (-), fever (-), PND (-), DOE (-)
Defecation and urination were normal
• History of hypertension (+) since 5 years ago but doesn’t
take medication regularly
• History of smoking (+) since 20 years ago (around 1 pack
per day)
• History of diabetes mellitus (-)
• History of dyslipidemia (-)
• Family history of CAD (-)

Modifiable :- Hypertension (+)- Obesity (+)- Smoking (+)
Non - Modifiable :- Male- Age >45 yo

• General status
Moderate illness/overweight/conscious
• Vital sign– Blood Pressure : 170/100 mmHg– Pulse : 86 x/min– Respiratory Rate : 22 x/min– Body Temperature : 36.50 C
Regional statusHead Examination
- Eyes : anemic -/-, icterus -/-- Lip : cyanosis (-)- Neck: lymphadenopathy (-), JVP R - 1 cmH2O
Chest Examination- Inspection : symmetric R=L, normochest- Palpation : mass (-), tenderness (-), VF R=L- Percussion : sonor- Auscultation : breath sound : vesicular
additional sound : ronchi -/-, wheezing -/-

Regional statusCardiac Examination
- Inspection : Ictus cordis wasn’t visible- Palpation : Ictus cordis wasn’t palpable- Percussion : normal heart size
-Upper border : left 2nd ICS-Lower border : left 5th ICS -Right border : right parasternalis line-Left border : left medioclavicular line
-Auscultation : Regular sound of I/II heart sound, murmur (-)
Abdominal Examination - Inspection : flat and following breath movement- Auscultation : peristaltic sound (+) , normal- Palpation : liver and spleen unpalpable- Percussion : tympani, ascites (-)
Extremities - No limb oedema
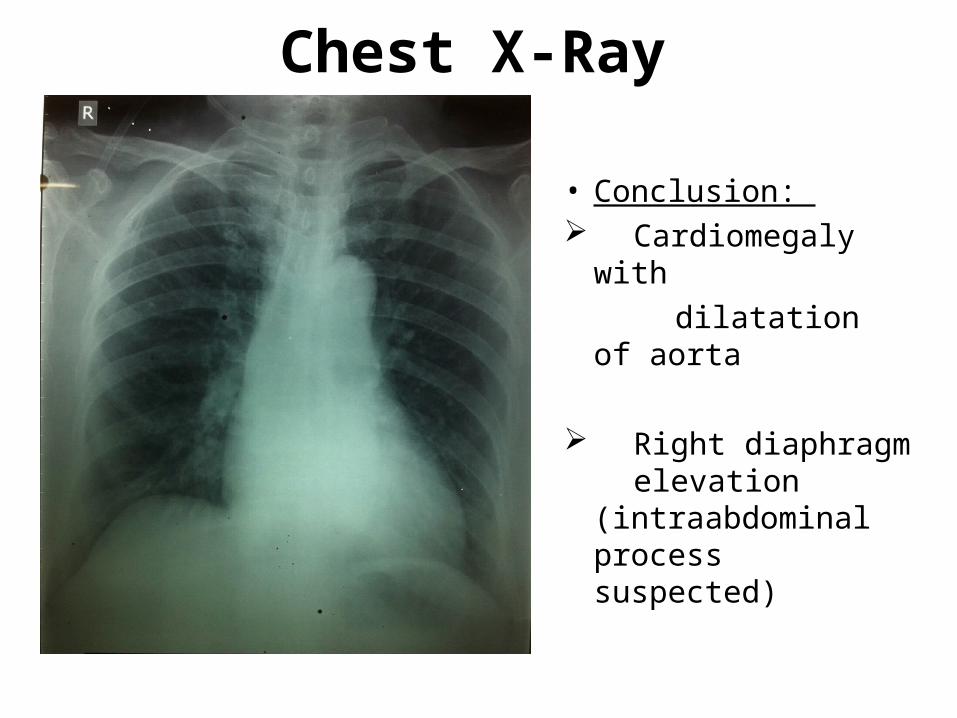
Chest X-Ray
• Conclusion: Cardiomegaly
with dilatation of aorta
Right diaphragm elevation
(intraabdominal process suspected)
Gambar x-ray
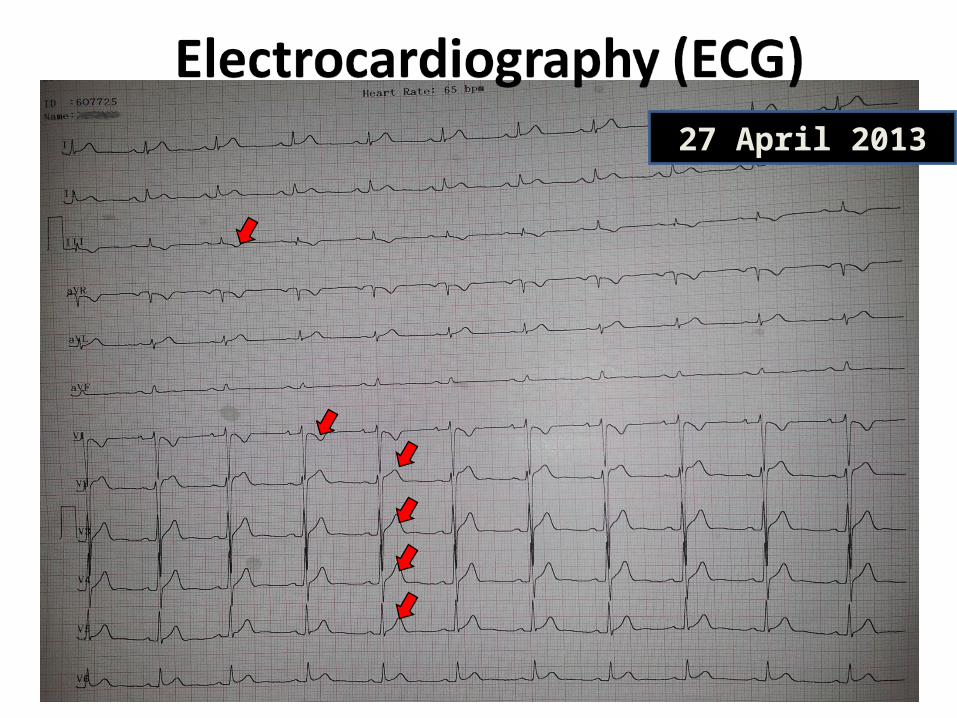
27 April 2013
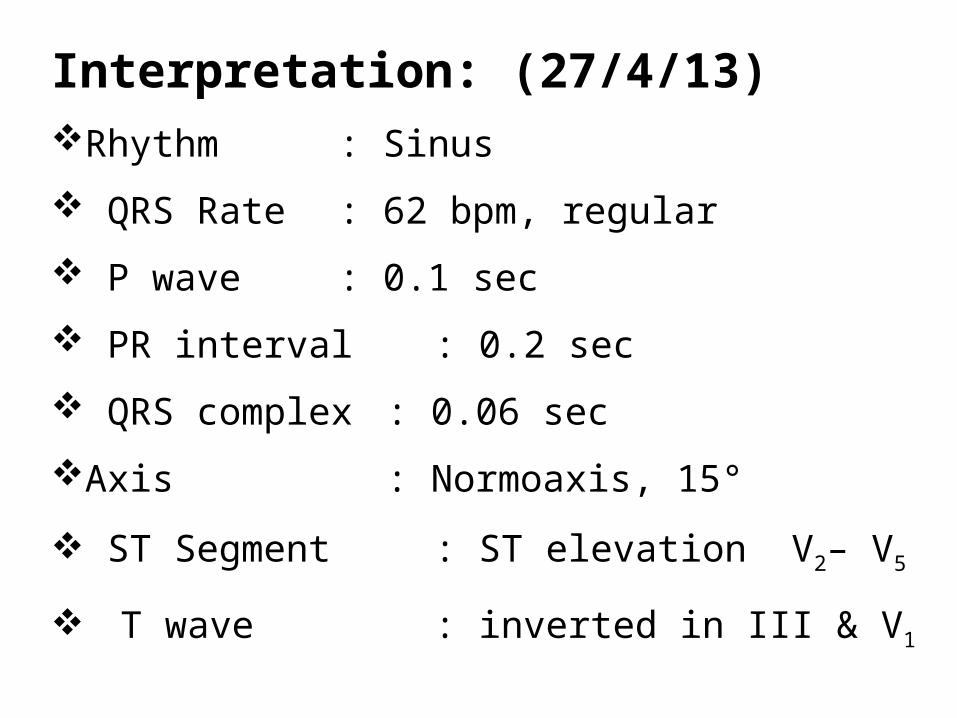
Interpretation: (27/4/13)Rhythm : Sinus
QRS Rate : 62 bpm, regular
P wave : 0.1 sec
PR interval : 0.2 sec
QRS complex : 0.06 sec
Axis : Normoaxis, 15°
ST Segment : ST elevation V2– V5
T wave : inverted in III & V1
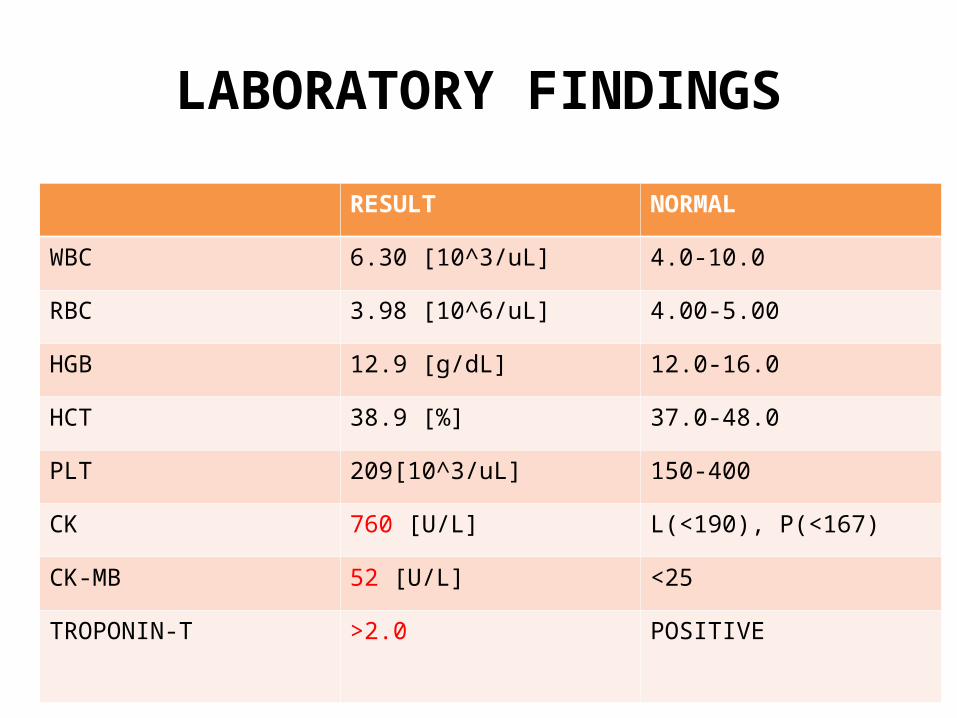
LABORATORY FINDINGS
RESULT NORMAL
WBC 6.30 [10^3/uL] 4.0-10.0
RBC 3.98 [10^6/uL] 4.00-5.00
HGB 12.9 [g/dL] 12.0-16.0
HCT 38.9 [%] 37.0-48.0
PLT 209[10^3/uL] 150-400
CK 760 [U/L] L(<190), P(<167)
CK-MB 52 [U/L] <25
TROPONIN-T >2.0 POSITIVE

LABORATORY FINDINGS
RESULT NORMAL
GDS 88 140
UREUM 48 10-50
CREATININE 0.8 L(<1.3), P(<1,1)
SGOT 29 <38
SGPT 37 <41
NATRIUM 143 136-145
KALIUM 4.9 3.5-5.1
CHLORIDE 110 97-111

Working Diagnosis
STEMI Anterior Wall Onset > 12 Hours KILLIP I
HT Grade II JNC 7
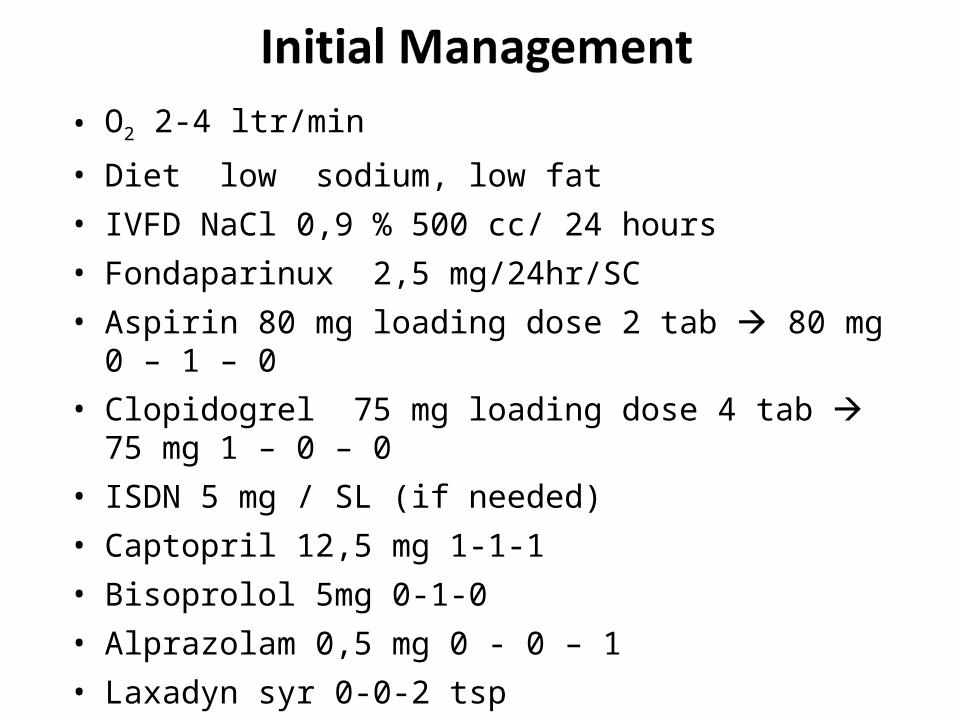
• O2 2-4 ltr/min
• Diet low sodium, low fat• IVFD NaCl 0,9 % 500 cc/ 24 hours• Fondaparinux 2,5 mg/24hr/SC• Aspirin 80 mg loading dose 2 tab 80 mg 0 – 1 – 0• Clopidogrel 75 mg loading dose 4 tab 75 mg 1 – 0 – 0• ISDN 5 mg / SL (if needed)• Captopril 12,5 mg 1-1-1• Bisoprolol 5mg 0-1-0• Alprazolam 0,5 mg 0 - 0 – 1• Laxadyn syr 0-0-2 tsp

PLANNING
• ECG serial• Echocardiography


• Myocardial infarction (MI) is the rapid development of
myocardial necrosis caused by an imbalance between
the oxygen supply and demand of the myocardium.
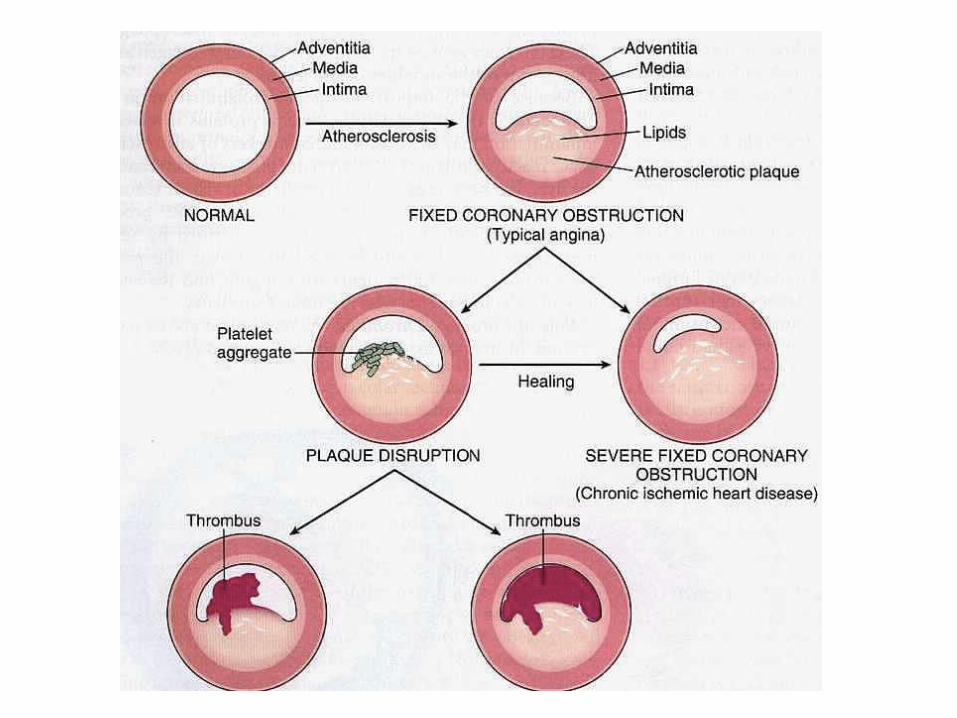
• This usually results from plaque rupture with thrombus
formation in a coronary vessels
• Myocardial infarction (MI) is the rapid development of
myocardial necrosis caused by an imbalance between
the oxygen supply and demand of the myocardium.
• This usually results from plaque rupture with thrombus
formation in a coronary vessels
DEFINITIONDEFINITION
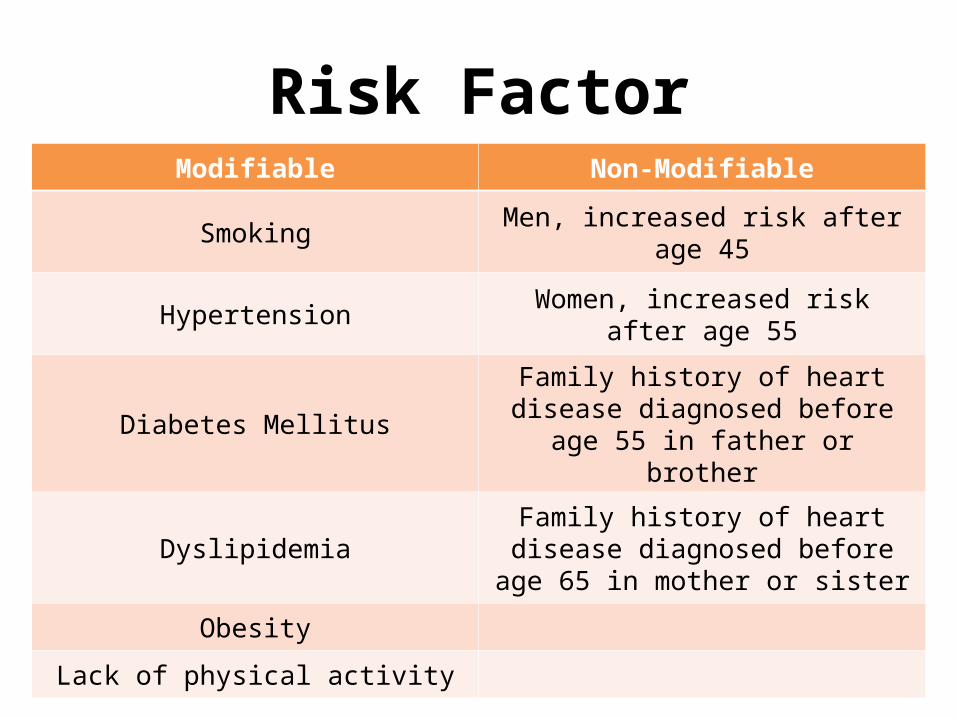
Risk FactorModifiable Non-Modifiable
Smoking Men, increased risk after age 45
Hypertension Women, increased risk after age 55
Diabetes MellitusFamily history of heart disease
diagnosed before age 55 in father or brother
DyslipidemiaFamily history of heart disease
diagnosed before age 65 in mother or sister
Obesity
Lack of physical activity
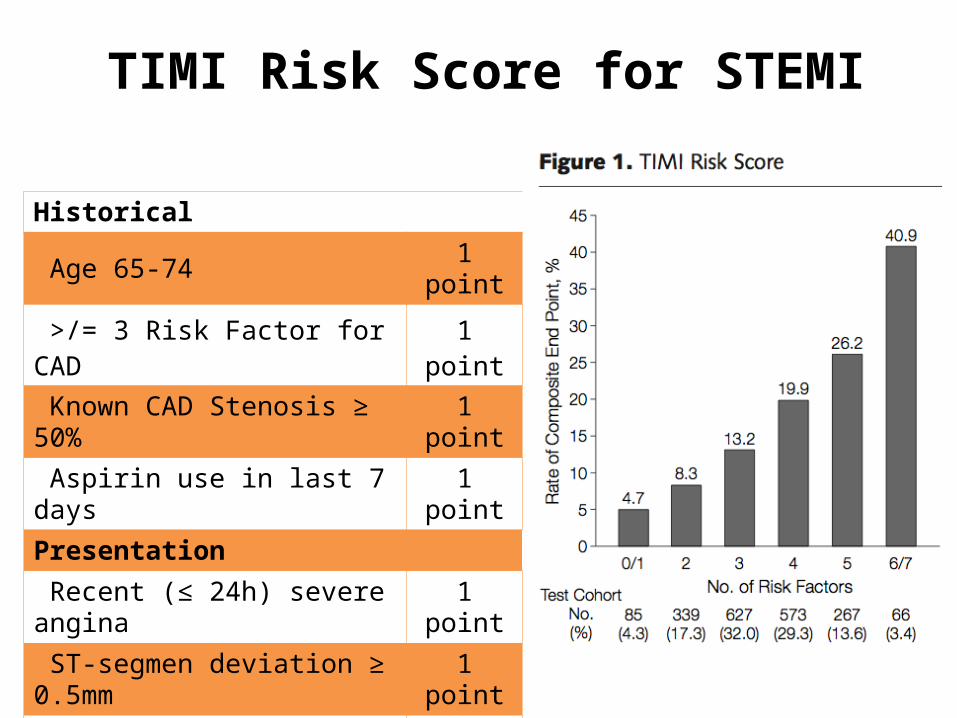
TIMI Risk Score for STEMI
Historical
Age 65-74 1 point
>/= 3 Risk Factor for CAD 1 point
Known CAD Stenosis ≥ 50% 1 point
Aspirin use in last 7 days 1 point
Presentation
Recent (≤ 24h) severe angina 1 point
ST-segmen deviation ≥ 0.5mm 1 point
Elevated serum cardiac markers 1 point
Risk Score = Total (0-7)

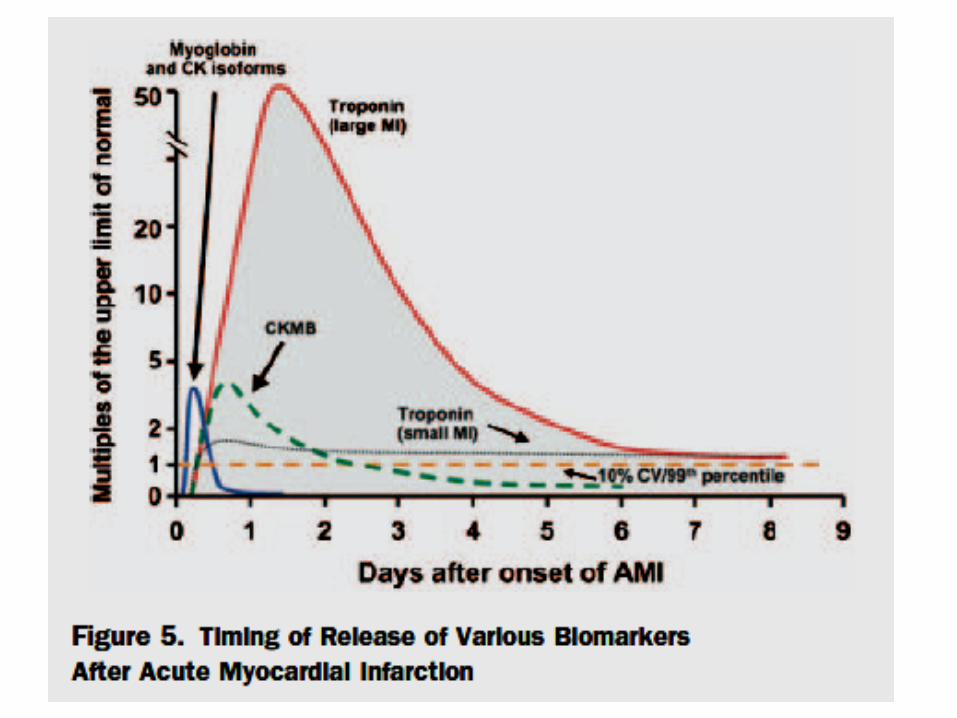
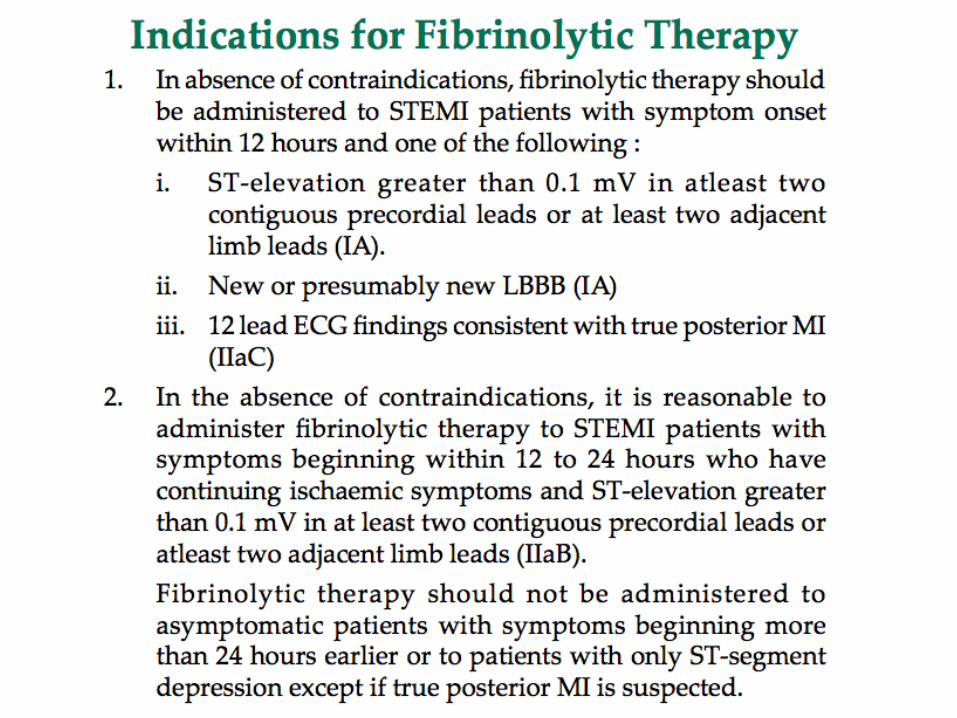
1. Clinical history of ischaemic type chest pain lasting >20 minutes
2. Changes in serial ECG tracings3. Rise and fall of serum cardiac biomarkers
such as Creatinine Kinase-MB fraction and troponin
WHO Diagnostic Criteria

Clinical Features
• Duration : variable, often more than 30 minutes.• Quality : Feels squeezing, pressurelike, tightness,
heaviness, and burning. • Location : Retrosternal, often with radiation to or
isolated discomfort in neck, jaw, shoulders, or arms—frequently on left.
Associated features : Not relieve with rest or nitrat


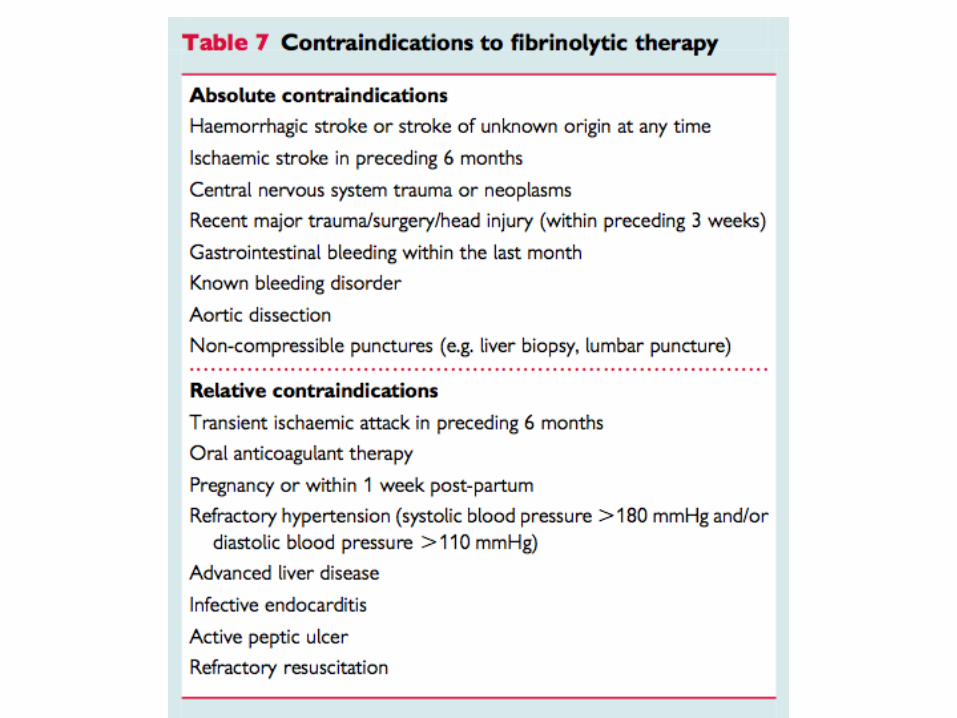
• Fixing the chest pain and fearnesso Bed resto Diet o O2 2-4 lpmo Nitrate sublingual/oral/IVo Antiplatelet : aspirin and clopidogrelo Morfin/petidineo Diazepam 2-5mg/8 hour• Stabilizing the hemodynamic ( blood pressure and pheripheral pulse
control)o β-blockero Calcium chanel blocker (CCB)o ACE-Inhibitor• Reperfusion of the myocardo Thrombolitic
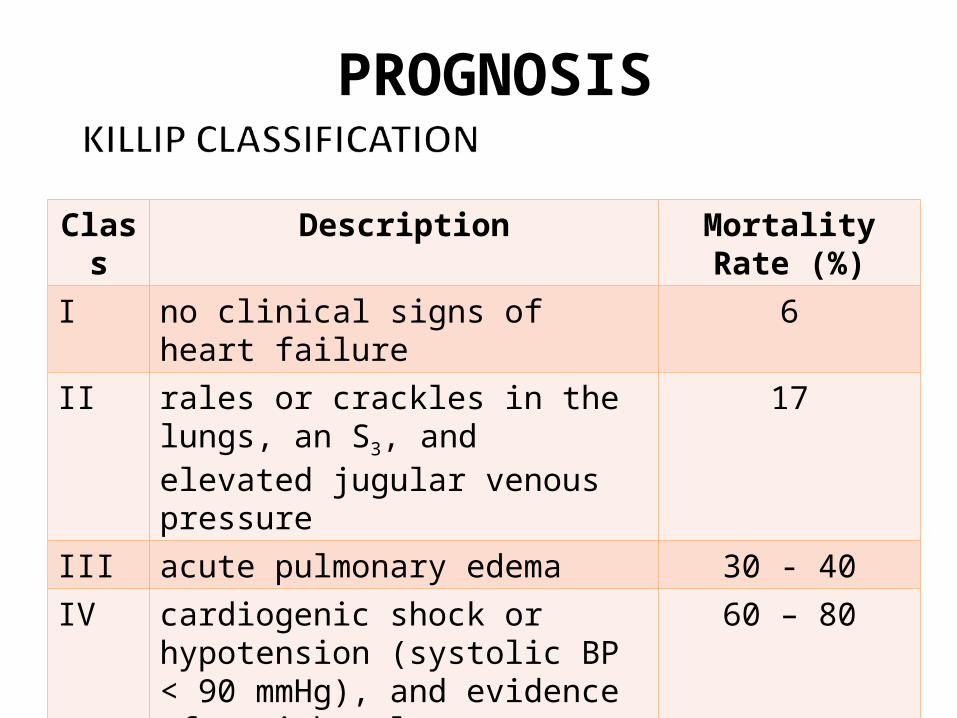
Class Description Mortality Rate (%)
I no clinical signs of heart failure 6II rales or crackles in the lungs, an S3,
and elevated jugular venous pressure17
III acute pulmonary edema 30 - 40IV cardiogenic shock or hypotension
(systolic BP < 90 mmHg), and evidence of peripheral vasoconstriction
60 – 80
PROGNOSIS