Embed Size (px)
Citation preview

PEOPLE CARING FOR PEOPLE
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
Issue # 5
EBOS HealthcareAged Care Division
Free call: 1800 269 534 Free fax: 1800 810 257
Email: [email protected]
June 2013
Save the environment, sign up to receive this newsletter via email. Visit: www.eboshealthcare.com.au
Dietary Strategies for DysphagiaPage 17
NEW!Unifine® Pentip® Plus, Page 12 Vernacare Pulp Bedpan & Support Page 20
Medihoney® Buzz builds for honey treatmentsPage 6
Wound Care Case StudiesPage 8,10
EBOS NEWS & CONFERENCESPage 4,16
Incontinence & the Ageing SkinPage 14

2 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
To the FIFTH EDITION of Carelines!
Our lead feature this issue is on the Medihoney® range of dressings with Leptospermum honey - for challenging and stalled wounds and burns. We have included a very interesting case study as well as the results of the research just released by the University of Technology in Sydney on the wound healing properties of manuka honey.
To complete our feature on wound care we are also presenting a case study on Smith & Nephew’s Allevyn Life.
In this edition we also talk about palliative care, dysphagia, hand hygiene compliance and other relevant topics. Make sure you take the time to read everything!
In the new product section we are presenting, among others, a couple of great product innovations that can help reduce the risk of infections and save nursing time in Aged Care environment: Unifine® Pentips® Plus (pen-needles with inbuilt remover) from Owen Mumford and a new fully disposable Bedpan and Support from Vernacare.
We hope you will find Carelines full of interesting information; as usual we would love to receive your feedback on the content of this issue and on what
you would like to see in the next one.
A couple of reminders on how to get in touch with us:
• The latest issue of Carelines is available on our corporate website www.eboshealthcare.com.au
• If you want to send us comments or suggestions on what you would like to see next in Carelines just email us at [email protected]
• Our online ordering system www.ebosonline.com.au contains over 10,000 products across all the product categories you need for your Facility. Make sure you visit the website, browse the product range and register to order online. It’s quick and easy!
Cheers,
The Aged Care Team
@ EBOS Healthcare
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
National Account ManagerDebbie Greenaway0400 424 [email protected]
National Equipment Co-ordinatorDe’Ann Keevers0417 497 [email protected]
Key Account Manager NSWElizabeth Conridge 0419 612 [email protected]
Key Account Manager VICCarolyn Knight 0411 542 [email protected]
Key Account Manager SAJanet Pitts 0416 130 [email protected]
Key Account Manager QLDLarissa Mueller0417 524 [email protected]
Key Account Manager QLDLiz Wiggins0414 486 [email protected]
Key Account Manager TASPattie Reptik 0419 377 [email protected]
Key Account Manager WACherie Baxter 0405 502 [email protected]
Our Aged Care Team
page 3Contribute to your CPD with Carelines,In the spotlight,EBOS warehouse expansion
page 4A warm welcome
page 5 EBOS Aged Care Division
page 6Medihoney® Wound & Burn Dressings
page 12Unifine® Pentips® Plus
page 14Tena - Incontinence and the ageing skin
page 16 Conference News
page 17 Dietary strategies for management of Dysphagia
page 19Pallative care - Time to talk about it
page 21New Vernacare bedpan and support
page 22Hand hygiene compliance: It’s time for a change

2 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 3
VV
Larissa Mueller is our Key Account Manager in the Brisbane Area and has been with our Aged Care Team for the last 18 months; prior to that she spent many years working with other medical suppliers in the area, gaining a wealth of hands-on experience in the QLD Aged Care industry.
What do you like most of working in the Aged Care industry? I like helping achieve best practice policies and drive results. That’s what I try and do every day with my customers, by providing product and industry knowledge and by keeping them up to date with the latest product news. I love my Job!
What is one of your favorite quotes ? It doesn’t cost anything to smile.
What chore do you absolutely hate doing? The ironing, but it has to be done!
If you won the lottery what is the first thing you would do? Pay off some debt for my closest friends and family. Then buy a ticket to travel the world!
What do you miss most about being a kid? Playing and dreaming.
Have you ever broken any bones, if so how? I broke my ribs and cracked my collarbone while wakeboarding.
Have you ever lived in another country? I was born in Germany and migrated to Australia at the age of five. I went back to live in Germany for 4 years when I was in my twenties.
Name one thing not many people know about you? I love to sing!
Whats your favorite song of all time? Euphoria by Loreen.
What is your computer screen wallpaper at the moment? The ocean with a magnificent sunset.
Who inspires you? My mum, she is the most positive and happy person I know. She has so much wisdom and love for everyone.
If you could invite anyone at your dinner party who would it be? Ricky Martin he is an amazing soul and there is a lot of kindness about him. I wish he was available!
If you could choose anyone, who would you pick as your mentor? My grandma (dad’s mum) she was strong, successful, sporty and fun. I have a history of inspirational women in my family!
If you could witness any event past, present or future, what would it be? See peace on this earth for our children.
What would you name the autobiography of your life? Living happy and healthy.
EBOS WAREHOUSE EXPANSIONIt is official, EBOS Healthcare now has its own warehouse in Perth. The new operation is located in Canning Vale and our Western Australian team has just finished fitting out the new warehouse with racking, shelving, office furniture and everything else required to get our warehouse and office complete. The Perth warehouse is now fully operational and ready to fulfill all of our Western Australian customers requirements.
Greg Cowlishaw, National Operations Manager for EBOS, says: “We had a very tight timeline with a great deal to do, but it was definitely worth the effort. This is another important step in EBOS consolidating and building towards our now complete national presence. It is great to see the investment in the business for Perth, but also in our Sydney warehouse where we are well under way with a large warehouse upgrade, in Brisbane where we have begun more work to create more space and efficiency, and in Melbourne, where we will see the biggest change and investment to any of our current warehouses since I started at EBOS back in 1996.
I am confident that our national expansion and significant capital investment and upgrades will place EBOS in the best position possible to take our customer service and order delivery to a whole new level”.
CARELINES ISSUE #4
Contribute to your Continuing Professional Development (CPD) with CarelinesThe CPD Registration Standard for Nurses and Midwives sets out a minimum requirement of 20 hours of continuing nursing professional development per year for nurses on the nurses’ register.One hour of active learning will equal one hour of CPD, and the CPD must be relevant to the nurse’s context of practice. You can read Carelines as self-directed CPD, as a tool to maintain, improve and broaden your knowledge, expertise and competence as a nurse working in Aged Care.For more information on self-directed CPD, the CPD cycle and how to document your CPD see the Nursing and Midwifery Board of Australia – ‘Continuing professional development registration standard.’

4 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Liz Wiggins - Key Account Manager QLD Welcome to Liz Wiggins who has just joined our Aged Care Sales team. Liz is from Brisbane and will work with Larissa Mueller in the Queensland Aged Care market, concentrating her efforts and expertise on the area North of Brisbane.
Liz has a great deal of experience in both Hospital & Aged care gained during her previous roles within the Healthcare market in Australia.
Welcome to the EBOS team Liz!
Liz Wiggins, Key Account Manager, QLD Aged Care Division.Welcome back De’Ann Keevers
De’Ann has over twenty years’ experience in the Healthcare Industry, eighteen of which have been working with EBOS - or selling EBOS Healthcare products.
De’Ann started with Tasmanian Medical Supplies where she specialised in Aged Care. She was instrumental in the promotion of the EBOS Macerator System into the Tasmanian aged care market and soon proved herself as an expert in this area.
Later on De’Ann moved to Queensland as the Territory Business Manager for Invacare and spent five years in the role. This allowed her to continue to support the aged care market. She built extremely good business relationships and gained considerable experience with the diverse aged care product range.
During the past two years in Queensland De’Ann worked
as “Business Development Manager for Novis Healthcare and this was the catalyst for her passion for Pressure Care, which she lovingly refers to as “her baby”.
With the addition of two beautiful grandsons into her family, De’Ann has just re-located back to Tasmania and re-joined EBOS Healthcare.
She is extremely happy to be back with EBOS in the new role of “National Equipment Co-ordinator”. This is a perfect fit with her speciality in supporting our Aged Care Sales Team using “Solution focused, team oriented leadership”.
De’Ann is dedicated to ensuring our customers receive unsurpassed service at all times. Her main goal is to help EBOS Healthcare consolidate their position as “One Stop Shop” for all medical consumables and equipment for the aged care market.
De’Ann Keevers, National Equipment Co-ordinator Aged Care Division.
A warm welcome ...
4 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 5
CARELINES ISSUE #5
EBOS – A FRESH, INNOVATIVE PARTNER WITH THE PEOPLE, ORGANISATIONAL STRENGTH, PRODUCTS, SYSTEMS AND COVERAGE TO HELP YOU DELIVER SUPERIOR VALUE TO YOUR RESIDENTS
With the continued expansion of the general aged care sector, aged care providers are faced with the challenge of improving quality of service to residents at an economic scale.
EBOS provides a consistently high standard of service, support and a streamlined ordering process as a single supply partner for your medical consumable and equipment needs.
We have a dedicated Product Catalogue for our Aged Care division, where our customers can easily find all the product categories they need every day for their facilities.
Our customers can then review and order these products online through our fast and easy online ordering system at www.ebosonline.com.au. A simple and efficient way to do all your purchases.
We deliver economies of scale and measurable continuous improvement without compromising best practice.
EBOS is Australasia’s largest and most
experienced provider of medical supplies and equipment across the general healthcare market. We are proud to be ‘in-tune’ with the needs of our customers and are committed to providing the most responsive and professional service levels. With a commitment to sourcing sustainable products and providing first class supply chain solutions, EBOS is an outstanding supply partner for aged care facilities.
EBOS Aged Care delivers a comprehensive support package at facility, procurement and management level. We believe we:
• are capable of demonstrating an efficient track record with a national supply chain solution
• have proven management systems and consistent service standards
• are prepared to develop innovative support platforms that complement your culture and strengths
• offer a competitive price without compromising service or support levels
Most importantly, our people bring a commitment to customers, fresh ideas, integrity and determination that provide the best possible service and supply chain solution.
EBOS Aged Care DivisionPEOPLE CARING FOR PEOPLE
AGED CARE DIVISIONPeople car ing fo r peop le
We can meet all your product and service requirements
across all of the following categories:
One Supplier One Place
Infection Prevention
Wound Care
Medical Consumables
Incontinence
Rehab EquipmentNutrition

6 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
[Effective on a variety of etiologies]
helping to make wound
management easier
MEDIHONEY® on left, plain alginate on right WK #3 after initiation of MEDIHONEY®
Steven J. Kavros, DPM: Case #1 of 3 presented at 2008 SAWC
Patient history of Crohn’s disease
Two wounds were both managed with systemic steroids, light compression to reduce edema and either plain alginate, or MEDIHONEY® alginate
MEDIHONEY
®
initiated
By WK #2, the wound managed with MEDIHONEY® was reduced by 62%
By WK #3, the wound managed with MEDIHONEY® healed, and the other wound is switched to MEDIHONEY® (heals at WK #4)
Peripheral neuropathy, ESRD, and CCL I
Dense fibrin tissue, slough and limited granulation tissue upon initial presentation
MEDIHONEY
®
initiated
Dressing changes every other day
Wound volume reduced by 25% by WK #4, and by 85% by WK #8. Complete healing by WK #16
Pyoderma
Gangrenosum
Recalcitrant
Diabetic Foot Ulcer
Catherine T. Milne, APRN, MSN, CWOCN: Case #3 of 3 presented at 2008 SAWC & WOCN
Non-healing diabetic foot ulcer WK #8 after initiation of MEDIHONEY®
Medihoney_brochure_9.21.09.indd 5 12/5/11 3:16:28 PMMEDIHONEY®
Antibacterial Honey Wound and burn dressingsMedihoney® is the leading global brand of medical honey-based wound and burn care made from a speific honey, Leptospermum scoparium or Manuka honey, derived from a tea tree bush indigenous to New Zealand. Active Leptospermum Honey is the only species of honey shown in randomized controlled studies to help wounds - that have stalled under first-line treatment - to progress towards healing.
The most common usages of Medihoney® dressing are debridement of wounds and jump-starting the healing of stalled wounds including:
New National Distributor of Medihoney®
Product Range Guide
MEDIHONEY® MEDICAL HONEY
MEDIHONEY® WOUND GEL
MEDIHONEY® TULLE
MEDIHONEY® GEL SHEET
MEDIHONEY® APINATE
MEDIHONEY® HCS
Percentage of Medihoney
100% 80% 100% 80% 95% 63%
Absorbency
Nil. Allows fluid to pass through open weave into secondary absorbent dressing
Minimal to moderate
Moderate to heavy
Minimal to moderate
Ideally suited to/benefits
• Cavity or sinus wounds
• Internal applications
• Ophthalmic use
• Wound debrider for sloughy or necrotic tissue. Very cost effective compared to hydrogels because of long open shelf life
• Wound debrider for sloughy or necrotic tissue. Very cost effective compared to hydrogels because of long open shelf life.
• General wounds. A better formulation for general wound care than Medical Honey because it does not ‘run’. Exit sites
• Skin grafts
• Whole limbs. Can be unfolded to 30cm x 10cm size for applying to a limb. (Add extra Medical Honey if unfolded).
• Conforming around toes/fingers
• Superficial or partial thickness wounds
• People report less stinging with Gel Sheet than other honey dressings. Good for painful wounds
• Leg ulcers
• Pressure ulcers
• Fungating wounds
• Very wet cavity wounds
• Minor burns
• Post Op wounds
• Large grazes
• Superficial/ partial thickness wounds
Open shelf life
Once open, use within 4 months
Once open, use within 4 months
Single use only Single use only Single use only Single use only
• Arterial leg ulcers
• Diabetic foot ulcers
• Donor sites
• Leg ulcers of mixed etiology
• Oncologic wounds
• Pressure ulcers
• Traumatic and surgical wounds
• Venous stasis leg ulcers
• 1st and 2nd degree burns

6 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 7
CARELINES ISSUE #5
Buzz builds for honey treatmentsClaire Thompson UTS news room , Sydney Morning Herald - 21st March 2013
New research proves manuka honey really does help restore
bodily ills.
Researchers are racing against the clock to find a viable alternative to traditional antibiotics, as bacteria continues to build resistance against new drugs at a frightening rate.
The field of chronic wound management illustrates the growing crisis. As antibiotic resistance becomes increasingly widespread, effective treatments for stubborn and slow-healing sores are becoming harder to find.
Enter manuka honey, a natural product derived from the Leptospermum scoparium plant that has unique healing properties. New research from the ithree institute at the University of Technology, Sydney (UTS) shows manuka is the most effective type of honey for the treatment of these chronic wounds.
UTS Professor Elizabeth Harry, who led the study in collaboration with Comvita, a New Zealand-based supplier of medicinal honey, says the research suggests nature may hold the answers to a range of ailments.
The research team looked at two ingredients of honey known to inhibit bacterial growth: methylglyoxal (MGO), which is present at high concentrations in manuka honey, and hydrogen peroxide, which is present in many honeys at varying concentrations, including manuka.
“Honey is naturally inhospitable to bacteria as it contains a complex mixture of antibiotic-like chemicals,” Professor Harry says.
“It’s an excellent example of how years of evolution in making honey can provide an effective, long-term medical solution,” she says. “Bacteria now have a finely honed ability to build resistance to traditional antibiotics, but are unable to do the same with honey.”
The manuka honeys were the most effective at inhibiting growth of all four types of bacteria the researchers tested, she says.
“Interestingly, the MGO level alone can’t explain the variation in the effects we saw,” she says. “The key to the effectiveness of honey is its chemical complexity – it contains several chemicals that inhibit bacterial growth, not just MGO.”
However, the potential benefits of alternative therapies such as manuka honey continue to be ignored by many medical practitioners for a number of reasons, including a lack of funding for clinical trials of such therapies.
“Many clinicians are wary of complementary treatments because of a lack of evidence supporting their use, and because it flies in the face of their clinical training,” says Dr David Johnson, director of Metro South and Ipswich Nephrology & Transplant Services (MINTS) and the medical director of Queensland Renal Transplant Service.
“There’s a negative bias among a lot of clinicians. It’s probably because it’s outside of what they’re generally used to – it’s not within the usual conventional realm of medical thinking.”
Dr Johnson uses Medihoney products to treat device-related infections – those linked to the use of medical equipment. He made the switch from traditional antibiotic treatments after conducting a trial to gauge the efficacy of Medihoney on his kidney dialysis patients’ catheter wounds. The trial showed the honey treatment was effective, affordable and well tolerated by the patients.
“Most importantly, it wasn’t associated with promotion of resistant bacterial strains,” he says.
While Dr Johnson hasn’t embraced complementary medicines entirely, he says there are valid reasons for clinicians to remain open to the possibilities of natural products such as manuka honey, olive leaf extract, fish oil and Cordyceps sinensis, a fungus believed to protect the kidneys.
“There are biologically plausible mechanisms for why they might be beneficial, so I think it’s worth exploring those things,” he says. “What I’d like to see is more trials being done in the area to confirm their safety and efficacy.”
Professor Harry agrees, saying natural therapies have a lot to offer but have needed better science behind them to get clinicians on board.
“It’s time to be open to alternative treatments that have had the stamp of approval by official regulatory bodies,” she says.
Meanwhile, time to find an alternative for traditional antibiotics is rapidly running out.
“Antibiotic resistance is a bit like climate change – we can turn our eyes away from it, but at the end of the day it’s there,” Professor Harry says.
“What we need to do is decide to take action, and decide to be more open-minded about what’s possible.”
This story written and produced by the University of Technology, Sydney, for The Sydney Morning Herald. Author Claire Thompson.
Research Articles:
The Effect of New Zealand Kanuka, Manuka and Clover Honeys on Bacterial Growth Dynamics and Cellular Morphology Varies According to the Species
Lu J, Carter DA, Turnbull L, Rosendale D, Hedderley D, et al. (2013) The Effect of New Zealand Kanuka, Manuka and Clover Honeys on Bacterial Growth Dynamics and Cellular Morphology Varies According to the Species. PLoS ONE 8(2): e55898. doi:10.1371/journal.pone.0055898
Synergism between Medihoney and Rifampicin against Methicillin-Resistant Staphylococcus aureus (MRSA)
Müller P, Alber DG, Turnbull L, Schlothauer RC, Carter DA, et al. (2013) Synergism between Medihoney and Rifampicin against Methicillin-Resistant Staphylococcus aureus (MRSA). PLoS ONE 8(2): e57679. doi:10.1371/journal.pone.0057679

Finding Success with Active Leptospermum HoneyAaron Wodash RN, WCCAugustana Care Center, Minneapolis, Minnesota
Case Study
The goal of achieving wound closure is often challenging with complicated patients suffering with multiple co-morbidities. Even when choosing advanced wound care dressings and therapies often times thousands of dollars are spent without progress.
This series describes patients suffering with wounds that were stalled in their progression toward healing despite receiving negative pressure wound therapy (NPWT).
NPWT was initially chosen because of the large size wounds and significant amounts of exudate. However, they were still not showing improvement.
A change in the plan of care was necessary and it was decided to try Active Leptospermum Honey (ALH)* dressings for their known mechanism to jump-start the wound healing process. ALH dressings are known to have a low pH important to alter the environment of the wound bed and believed to be one of the mechanisms responsible for faster wound healing1. ALH has also been shown to have significant debridement properties2 and in our facility has often been used in lieu of more costly enzymatic debriding agents.
The patients in this series had many challenging issues and medical complications including malnourishment, contractures, and the inability to communicate. Patient #1 presented with three stage IV pressure ulcers being treated with NPWT in combination with an enzymatic debriding agent 3x/week for a period of three months but was not showing expected progress. ALH Gel was first initiated in combination with NPWT and the remaining area of slough in the wound was quickly debrided after one week and the wound then began to reduce in size. The NPWT was able to be discontinued and ALH was continued in combination with a Super Absorbent dressing** being changed twice weekly. The rapid progress after months of little progress was considered remarkable.
Patient #2 presented with a full thickness surgical wound also not demonstrating improvement with NPWT. It was decided to discontinue the NPWT and trial ALH after seeing the rapid response in patient #1. This wound also rapidly began to reduce in size and showed significant improvement with the use of ALH.
ALH has shown to be a cost-effective alternative to other costly wound treatment techniques. This data demonstrates situations of wounds not benefiting from NPWT but showing benefits within one week after the introduction of ALH. ALH is now considered at our facility earlier in the wound healing process rather than waiting until after other methods have failed or waiting until the wound has stalled.
Introduction
Methods
Conclusion
Patient 1
A 79 yo female patient was living at home with family receiving home health nursing services and she developed multiple stage IV pressure ulcers. Home health service stopped seeing patient because she required more care than they could provide. Pt was hospitalized for wound infection, UTI, bacteremia, dehydration, and severe protein-calorie malnutrition. Patient underwent incision and drainage with NPWT placement at the hospital and was admitted to our facility for LTC. Past medical history
Date Length Width Depth Area (cm2)
Volume (cm2)
% Area Reduction
% Volume Reduction
2/29/12 4.0 2.0 4.0 6.28 25.13Initial
MeasurementInitial
Measurement
3/7/12 2.9 2.5 3.2 5.69 18.22 9.4% 27.5%
3/14/12 2.7 1.8 3.2 3.82 12.21 39.3% 51.4%
3/21/12 2.6 1.9 2.1 3.88 8.15 38.3% 67.6%
3/28/12 1.8 1.3 1.8 1.84 3.31 70.8% 86.8%
4/3/12 1.5 2.0 1.8 2.36 4.24 62.5% 83.1%
4/11/12 1.2 1.3 1.0 1.23 1.23 80.5% 95.1%
Patient 2
Patient was an 81 year old female with multiple medical problems including: CVA, HTN, CAD, DM, hyperlipidemia, and fall with displaced R femoral neck fracture, s/pR hip hemiarthroplasty on 9/15/11. Pt was hospitalized for post surgical infection requiring explantation on 10/10/11 and then underwent incision and drainage with NPWT placement on 10/27/11. NPWT continued until 2/29/12 when the medical team changed the plan of care.to a plain calcium alginate dressing and foam cover, due to the wound being stalled. Biofilm was suspected in this chronic wound and little progress was seen with the plain calcium alginate. On 3/4/12 ALH Calcium Alginate dressing was started with a Super Absorbent dressing as a secondary dressing and the wound again began to progress. On 3/19/12, an NP changed the plan of care to wet to dry dressings daily. Again the wound failed to progress and ALH was reinstated on 4/7/12 via an order from ortho. The wound continued to improve with this plan of care.
Left IT
2/14/12 5/23/12
References
1. Gethin G, Cowman S. (2008) The impact of Manuka honey dressings on the surface pH of chronic wounds. Int Wound J. ; 5:185-194.
2. Gethin G. (2007) Leptospermum scoparium Honey vs. Hydrogel to deslough venous ulcers: A randomised controlled trial. EWMA
*MEDIHONEY® Active Leptospermum Honey Dressing, Derma Sciences, Inc., Princeton, New Jersey. *XTRASORB® Super Absorbent Dressing, Derma Sciences, Inc., Princeton, New Jersey.
After Failures with Negative Pressure WoundsAaron Wodash RN, WCCAugustana Care Center, Minneapolis, Minnesota
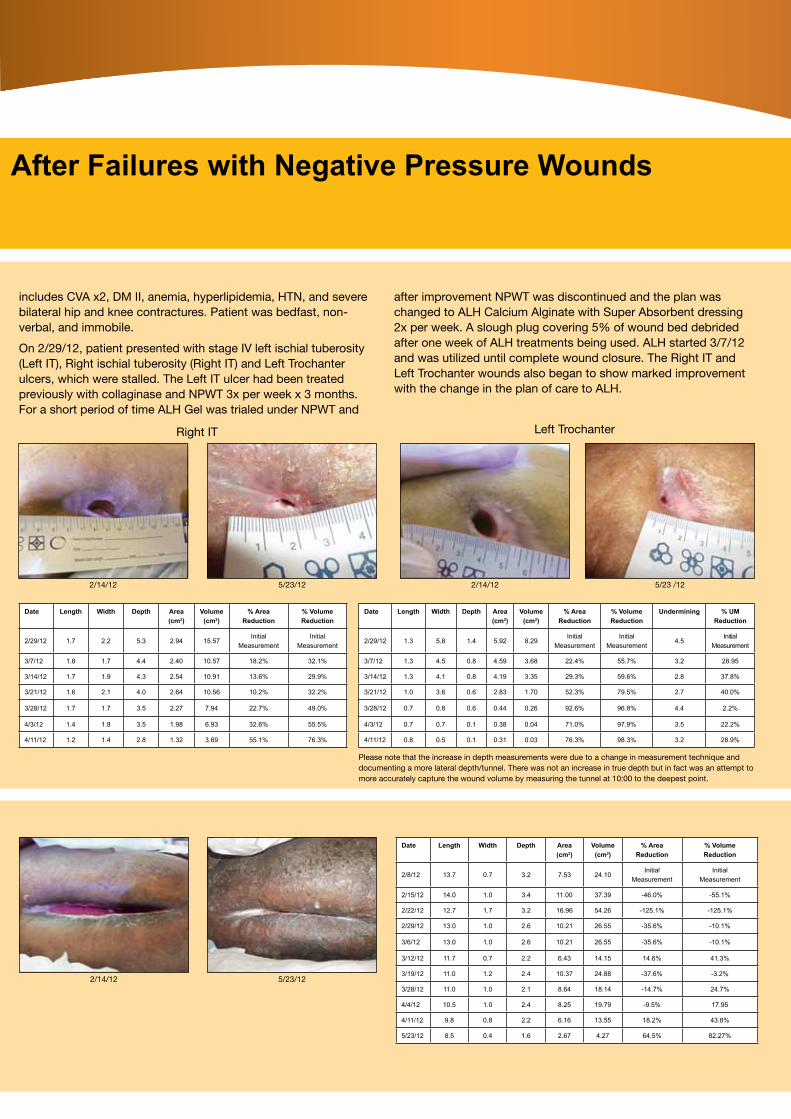
includes CVA x2, DM II, anemia, hyperlipidemia, HTN, and severe bilateral hip and knee contractures. Patient was bedfast, non-verbal, and immobile.
On 2/29/12, patient presented with stage IV left ischial tuberosity (Left IT), Right ischial tuberosity (Right IT) and Left Trochanter ulcers, which were stalled. The Left IT ulcer had been treated previously with collaginase and NPWT 3x per week x 3 months. For a short period of time ALH Gel was trialed under NPWT and
after improvement NPWT was discontinued and the plan was changed to ALH Calcium Alginate with Super Absorbent dressing 2x per week. A slough plug covering 5% of wound bed debrided after one week of ALH treatments being used. ALH started 3/7/12 and was utilized until complete wound closure. The Right IT and Left Trochanter wounds also began to show marked improvement with the change in the plan of care to ALH.
Date Length Width Depth Area (cm2)
Volume (cm2)
% Area Reduction
% Volume Reduction
2/29/12 1.7 2.2 5.3 2.94 15.57Initial
MeasurementInitial
Measurement
3/7/12 1.8 1.7 4.4 2.40 10.57 18.2% 32.1%
3/14/12 1.7 1.9 4.3 2.54 10.91 13.6% 29.9%
3/21/12 1.6 2.1 4.0 2.64 10.56 10.2% 32.2%
3/28/12 1.7 1.7 3.5 2.27 7.94 22.7% 49.0%
4/3/12 1.4 1.8 3.5 1.98 6.93 32.6% 55.5%
4/11/12 1.2 1.4 2.8 1.32 3.69 55.1% 76.3%
Date Length Width Depth Area (cm2)
Volume (cm2)
% Area Reduction
% Volume Reduction
Undermining % UM Reduction
2/29/12 1.3 5.8 1.4 5.92 8.29Initial
MeasurementInitial
Measurement4.5
Initial Measurement
3/7/12 1.3 4.5 0.8 4.59 3.68 22.4% 55.7% 3.2 28.95
3/14/12 1.3 4.1 0.8 4.19 3.35 29.3% 59.6% 2.8 37.8%
3/21/12 1.0 3.6 0.6 2.83 1.70 52.3% 79.5% 2.7 40.0%
3/28/12 0.7 0.8 0.6 0.44 0.26 92.6% 96.8% 4.4 2.2%
4/3/12 0.7 0.7 0.1 0.38 0.04 71.0% 97.9% 3.5 22.2%
4/11/12 0.8 0.5 0.1 0.31 0.03 76.3% 98.3% 3.2 28.9%
Date Length Width Depth Area (cm2)
Volume (cm2)
% Area Reduction
% Volume Reduction
2/8/12 13.7 0.7 3.2 7.53 24.10Initial
MeasurementInitial
Measurement
2/15/12 14.0 1.0 3.4 11.00 37.39 -46.0% -55.1%
2/22/12 12.7 1.7 3.2 16.96 54.26 -125.1% -125.1%
2/29/12 13.0 1.0 2.6 10.21 26.55 -35.6% -10.1%
3/6/12 13.0 1.0 2.6 10.21 26.55 -35.6% -10.1%
3/12/12 11.7 0.7 2.2 6.43 14.15 14.6% 41.3%
3/19/12 11.0 1.2 2.4 10.37 24.88 -37.6% -3.2%
3/28/12 11.0 1.0 2.1 8.64 18.14 -14.7% 24.7%
4/4/12 10.5 1.0 2.4 8.25 19.79 -9.5% 17.95
4/11/12 9.8 0.8 2.2 6.16 13.55 18.2% 43.8%
5/23/12 8.5 0.4 1.6 2.67 4.27 64.5% 82.27%
Right IT Left Trochanter
2/14/12 5/23/12 2/14/12 5/23 /12
Please note that the increase in depth measurements were due to a change in measurement technique and documenting a more lateral depth/tunnel. There was not an increase in true depth but in fact was an attempt to more accurately capture the wound volume by measuring the tunnel at 10:00 to the deepest point.
2/14/12 5/23/12

Ann Pardoe Tissue Viability Nurse, NHS North East London and the City, Chingford Health Centre, 109 York Road, London E4 8LF
Introduction
Type 2 diabetes is a complex metabolic disorder, which is becoming increasingly common in the UK. The condition is associated with a range of serious systemic complications that carry both a considerable human cost, in terms of their impact on the affected individual, and economic cost, due to the financial burden they impose on health care systems. The development of diabetic foot ulceration (DFU) is one of the most common diabetes-related complications, with around 5% of individuals with diabetes developing a foot ulcer in any given year1. The development of a foot ulcer is a critical event and requires careful management if adverse outcomes such as amputation are to be avoided. Even though understanding of diabetic foot disease continues to advance approximately 0.5% of the diabetic population undergo lower limb amputation each year1. The impact the development of a DFU has on an individual’s quality of life can be severe and wide-ranging. For example a frequent requirement of DFU management is that the patient should cease any weight-bearing activity in order to facilitate healing. The resultant loss of mobility often restricts daily activities, leisure and social interactions, and consequently impacts on patient quality of life2. Increased anxiety and depression have been reported, with lack of motivation to self-care and concerns of being a burden on carers. These feelings can be further enhanced due to concerns that the wound may never resolve, fear for the future and a loss of hope that control over their life can ever be regained3. Individuals need to integrate treatment-related procedures, adopt lifestyle changes and coping strategies to overcome the impact their wound is having on their everyday lives. The measurements of wound size, depth, appearance of the wound bed and exudate levels are routinely recorded as part of the wound assessment. Whilst the documentation of such wound characteristics is an essential part of the wound assessment process, equally important are the assessment of patient-centred issues and priorities. In addition to considering wound-related impacts in the assessment process, it is essential that these are then used to inform the management approach taken4. The ability of the Healthcare Professional to interact with the patient in an holistic way through communication about treatments is indicative of a positive therapeutic environment. The success of this relationship can lead patients to feel empowered to discuss treatment
options and concerns, with clinical decision based on what is important to the individual. By adopting a patient-centred approach, patients are able to feel m ore in control of their lives, their self-esteem may improve and active coping strategies can develop5. This can impact positively in improving the ability of patients to self-manage, concord with treatment, lead to improved patient satisfaction with care and achieve better outcomes.
Background
Mrs W is a 63-year-old female with poorly controlled insulin-dependent diabetes, hypercholesterolemia and renal failure. She lives at home alone supported by her daughter who visits on a daily basis. Mrs W has slept in her armchair for the past five years with her legs in a dependant position. Mrs W had recently been admitted to secondary care due to infection of a longstanding DFU to the lateral aspect of her left foot. During admission surgery was performed to debride the devitalized soft tissue and amputate the 5th metatarsal along with the proximal, intermediate and distal phalanges. The post-operative wound was not closed, but left to heal via secondary intention.
Initial assessment
Following discharge from hospital management of Mrs W’s post-amputation wound was initially undertaken by the District Nurse Team who visited on a daily basis. However, soon after discharge Mrs W was referred to the Tissue Viability Service due to concerns over the condition of the wound.
On initial assessment by the Tissue Viability Nurse the wound to the lateral aspect of her left foot measured 10cm x 7cm and 3cm in depth. The wound bed was covered by 70% fibrous slough with a small area of necrotic tissue to the lateral aspect of the wound. The remaining tissue at the wound margins was unhealthy pale pink, with no evidence of granulation or epithelialisation (see Figure 1). The wound was producing copious amounts of exudate which the District Nurse Team found challenging to contain, resulting in leaking into Mrs W’s slippers. The skin had become macerated at the wound margins, and had become ‘boggy’ on the plantar aspect of the foot. The wound was malodourous, which was causing some distress to the patient and her daughter.
Both lower legs were oedematous with an element of lymphoedema due to long-term leg dependency from sitting in her chair (see Figure 2). A vascular assessment was
performed to determine arterial status of the leg; good flow and biphasic sounds were detected in the tibial vessels and an ABPI of 1.2 was calculated. However due to the underlying co-morbidities compression bandage therapy was contraindicated.
Mrs W was found to have a random blood glucose level of 16mmol. Pain was controlled with regular analgesia.
Current treatment
The wound was being dressed daily by the District Nurse with layered AquacelTM followed by PROFORE™ 1 and PROFORE 2 bandages applied from toe to knee.
Wellbeing impacts
Prior to the initial assessment in the clinic the Tissue Viability Nurse had visited Mrs W in her own home with the District Nurse in order to determine if a referral was necessary. On this occasion Mrs W was dressed all in black and was sitting in a darkened room. Throughout the visit Mrs W sat with her eyes closed or looked down at the floor, with no eye contact or spontaneous engagement in conversation, only replying with ‘yes’ or ‘no’
Figure 1: Appearance of the wound on first visit to clinic (9/8/2012)
Figure 2: Lymphoedema of the limb
The information and recommendations in this poster are provided by the author(s) and have not been verified by Smith & Nephew. Smith & Nephew accepts no responsibility for the content of this poster and shall not be responsible for any reliance placed on the content. It may harm a patient’s health or cause you injury to use the products described in this poster otherwise than in accordance with the uses for which they are licensed. Smith & Nephew does not recommend or promote unlicensed use of any of its products. Professional medical advice should be sought for the use of any product named in this poster. ™Trademark of Smith & Nephew TM All trademarks acknowledged © Smith & Nephew November 2012
answers to questions. The District Nurses reported that they found it difficult to engage with Mrs W during their visits and that she had little interest in following advice or asking questions related to the wound’s progress.
Management challenges
• The management and containment of exudate and odour
• Poorly controlled diabetes
• Previous history of non-concordance.
• Engaging Mrs W in her own care
• Addressing issues around Mrs W’s wellbeing
Treatment intervention
The wound-related symptoms of exudate and odour were identified as having a major impact on Mrs W wellbeing. The focus of the treatment intervention was therefore to resolve these symptoms by addressing the bacterial burden within the wound bed which was thought to be the underlying cause. In addition to treating the causative bacterial burden any
management regimen needed to effectively contain the exudate to arrest further tissue maceration and prevent leakage onto clothing.
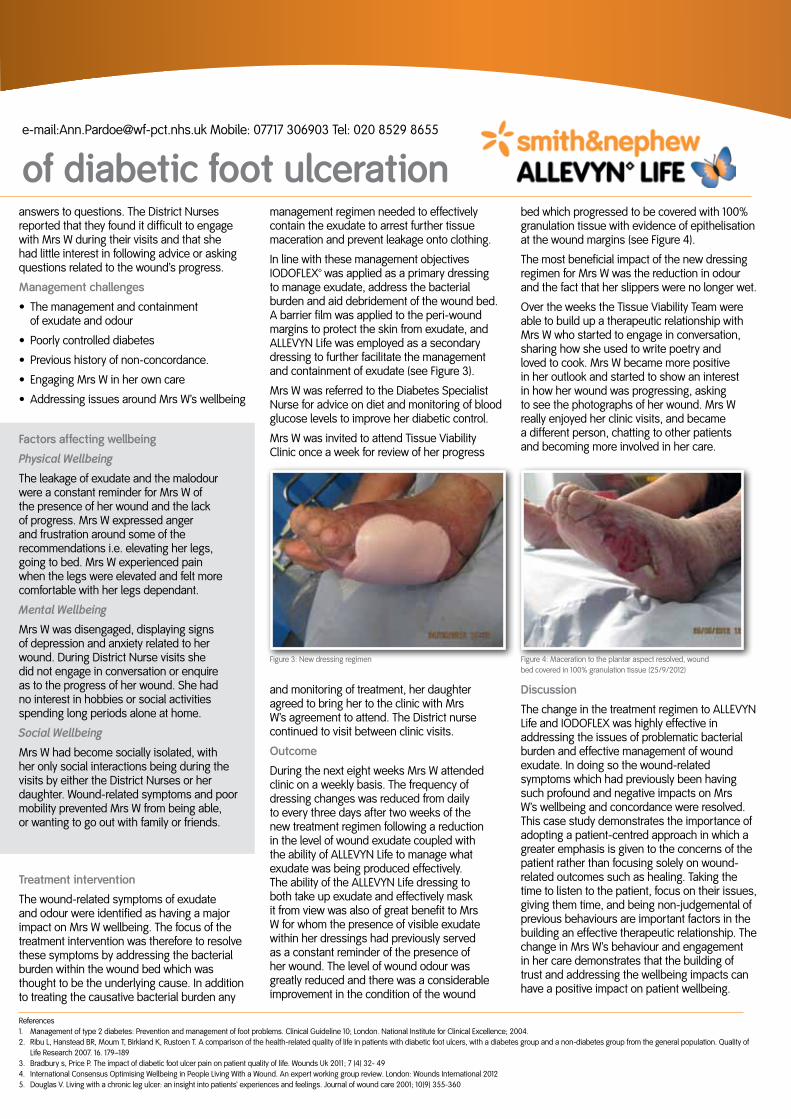
In line with these management objectives IODOFLEX™ was applied as a primary dressing to manage exudate, address the bacterial burden and aid debridement of the wound bed. A barrier film was applied to the peri-wound margins to protect the skin from exudate, and ALLEVYN Life was employed as a secondary dressing to further facilitate the management and containment of exudate (see Figure 3).
Mrs W was referred to the Diabetes Specialist Nurse for advice on diet and monitoring of blood glucose levels to improve her diabetic control.
Mrs W was invited to attend Tissue Viability Clinic once a week for review of her progress
and monitoring of treatment, her daughter agreed to bring her to the clinic with Mrs W’s agreement to attend. The District nurse continued to visit between clinic visits.
Outcome
During the next eight weeks Mrs W attended clinic on a weekly basis. The frequency of dressing changes was reduced from daily to every three days after two weeks of the new treatment regimen following a reduction in the level of wound exudate coupled with the ability of ALLEVYN Life to manage what exudate was being produced effectively. The ability of the ALLEVYN Life dressing to both take up exudate and effectively mask it from view was also of great benefit to Mrs W for whom the presence of visible exudate within her dressings had previously served as a constant reminder of the presence of her wound. The level of wound odour was greatly reduced and there was a considerable improvement in the condition of the wound
bed which progressed to be covered with 100% granulation tissue with evidence of epithelisation at the wound margins (see Figure 4).
The most beneficial impact of the new dressing regimen for Mrs W was the reduction in odour and the fact that her slippers were no longer wet.
Over the weeks the Tissue Viability Team were able to build up a therapeutic relationship with Mrs W who started to engage in conversation, sharing how she used to write poetry and loved to cook. Mrs W became more positive in her outlook and started to show an interest in how her wound was progressing, asking to see the photographs of her wound. Mrs W really enjoyed her clinic visits, and became a different person, chatting to other patients and becoming more involved in her care.
Discussion
The change in the treatment regimen to ALLEVYN Life and IODOFLEX was highly effective in addressing the issues of problematic bacterial burden and effective management of wound exudate. In doing so the wound-related symptoms which had previously been having such profound and negative impacts on Mrs W’s wellbeing and concordance were resolved. This case study demonstrates the importance of adopting a patient-centred approach in which a greater emphasis is given to the concerns of the patient rather than focusing solely on wound-related outcomes such as healing. Taking the time to listen to the patient, focus on their issues, giving them time, and being non-judgemental of previous behaviours are important factors in the building an effective therapeutic relationship. The change in Mrs W’s behaviour and engagement in her care demonstrates that the building of trust and addressing the wellbeing impacts can have a positive impact on patient wellbeing.
e-mail:[email protected] Mobile: 07717 306903 Tel: 020 8529 8655
of diabetic foot ulceration
Figure 3: New dressing regimen Figure 4: Maceration to the plantar aspect resolved, wound bed covered in 100% granulation tissue (25/9/2012)
References1. Management of type 2 diabetes: Prevention and management of foot problems. Clinical Guideline 10; London. National Institute for Clinical Excellence; 2004.2. Ribu L, Hanstead BR, Moum T, Birkland K, Rustoen T. A comparison of the health-related quality of life in patients with diabetic foot ulcers, with a diabetes group and a non-diabetes group from the general population. Quality of
Life Research 2007. 16. 179–1893. Bradbury s, Price P. The impact of diabetic foot ulcer pain on patient quality of life. Wounds Uk 2011; 7 (4) 32- 494. International Consensus Optimising Wellbeing in People Living With a Wound. An expert working group review. London: Wounds International 20125. Douglas V. Living with a chronic leg ulcer: an insight into patients’ experiences and feelings. Journal of wound care 2001; 10(9) 355-360
Factors affecting wellbeing
Physical Wellbeing
The leakage of exudate and the malodour were a constant reminder for Mrs W of the presence of her wound and the lack of progress. Mrs W expressed anger and frustration around some of the recommendations i.e. elevating her legs, going to bed. Mrs W experienced pain when the legs were elevated and felt more comfortable with her legs dependant.
Mental Wellbeing
Mrs W was disengaged, displaying signs of depression and anxiety related to her wound. During District Nurse visits she did not engage in conversation or enquire as to the progress of her wound. She had no interest in hobbies or social activities spending long periods alone at home.
Social Wellbeing
Mrs W had become socially isolated, with her only social interactions being during the visits by either the District Nurses or her daughter. Wound-related symptoms and poor mobility prevented Mrs W from being able, or wanting to go out with family or friends.
12 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Unifine® Pentips® Plus - the world’s first pen needle with built-in remover - can help prevent needlestick injuriesThe Unifine Pentips Plus from specialist UK medical devices manufacturer Owen Mumford allows healthcare staff, as well as adults and children who rely on regular injections, to change their pen needles more easily and safely.
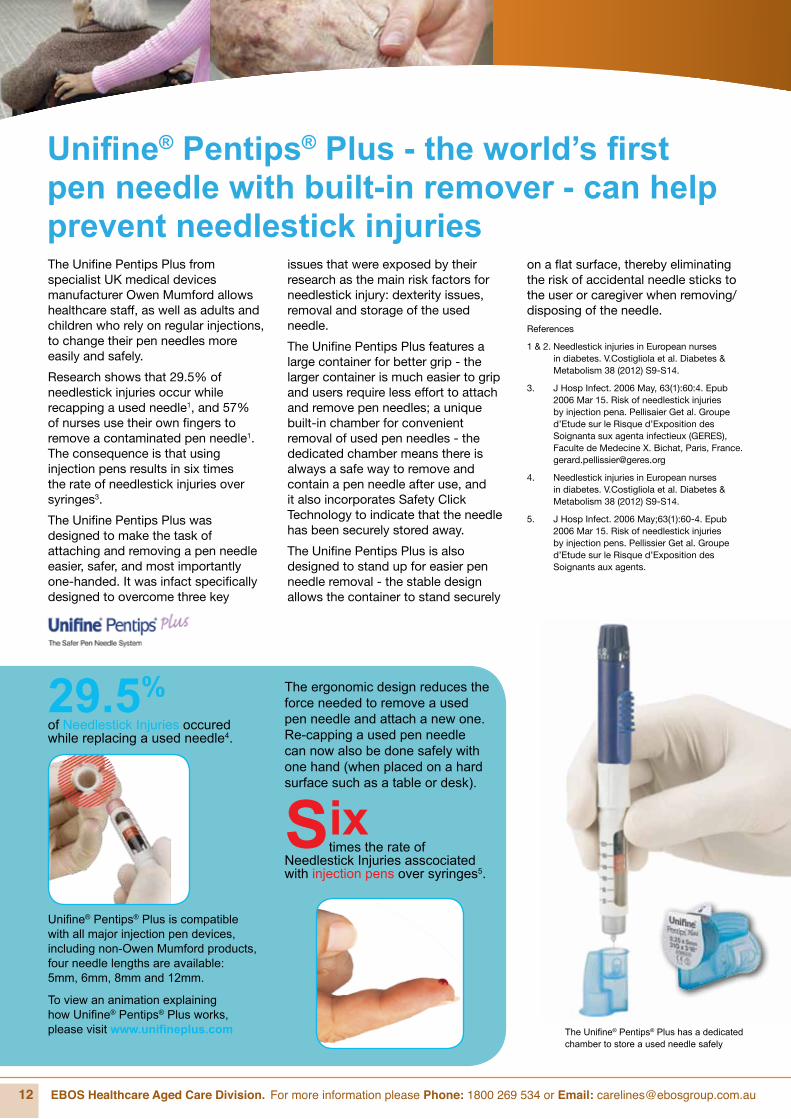
Research shows that 29.5% of needlestick injuries occur while recapping a used needle1, and 57% of nurses use their own fingers to remove a contaminated pen needle1. The consequence is that using injection pens results in six times the rate of needlestick injuries over syringes3.
The Unifine Pentips Plus was designed to make the task of attaching and removing a pen needle easier, safer, and most importantly one-handed. It was infact specifically designed to overcome three key
issues that were exposed by their research as the main risk factors for needlestick injury: dexterity issues, removal and storage of the used needle.
The Unifine Pentips Plus features a large container for better grip - the larger container is much easier to grip and users require less effort to attach and remove pen needles; a unique built-in chamber for convenient removal of used pen needles - the dedicated chamber means there is always a safe way to remove and contain a pen needle after use, and it also incorporates Safety Click Technology to indicate that the needle has been securely stored away.
The Unifine Pentips Plus is also designed to stand up for easier pen needle removal - the stable design allows the container to stand securely
on a flat surface, thereby eliminating the risk of accidental needle sticks to the user or caregiver when removing/ disposing of the needle.References
1 & 2. Needlestick injuries in European nurses in diabetes. V.Costigliola et al. Diabetes & Metabolism 38 (2012) S9-S14.
3. J Hosp Infect. 2006 May, 63(1):60:4. Epub 2006 Mar 15. Risk of needlestick injuries by injection pena. Pellisaier Get al. Groupe d’Etude sur le Risque d’Exposition des Soignanta sux agenta infectieux (GERES), Faculte de Medecine X. Bichat, Paris, France. [email protected]
4. Needlestick injuries in European nurses in diabetes. V.Costigliola et al. Diabetes & Metabolism 38 (2012) S9-S14.
5. J Hosp Infect. 2006 May;63(1):60-4. Epub 2006 Mar 15. Risk of needlestick injuries by injection pens. Pellissier Get al. Groupe d’Etude sur le Risque d’Exposition des Soignants aux agents.
The Unifine® Pentips® Plus has a dedicated chamber to store a used needle safely
Unifine® Pentips® Plus is compatible with all major injection pen devices, including non-Owen Mumford products, four needle lengths are available: 5mm, 6mm, 8mm and 12mm.
To view an animation explaining how Unifine® Pentips® Plus works, please visit www.unifineplus.com
29.5%
of Needlestick Injuries occured while replacing a used needle4.
Six times the rate of
Needlestick Injuries asscociated with injection pens over syringes5.
The ergonomic design reduces the force needed to remove a used pen needle and attach a new one. Re-capping a used pen needle can now also be done safely with one hand (when placed on a hard surface such as a table or desk).

12 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 13
CARELINES ISSUE #5
The Range
Unifine® Pentips® Plus stands upright on a flat surface, allowing a one handed capped process. A Safe Zone is created around the device, keeping the user’s hand away from exposed pen needle.
Why Risk It? One handed capping is safer.

14 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Understanding the effects of incontinence on ageing skin
Infants and the elderly have very frail skin types – especially when exposed to incontinence. As we get older, most skin functions deteriorate and the rate of cell replacement is slower, meaning elderly skin takes longer to heal and is more susceptible to external irritants than younger skin.
How skin changes as we get older
The skin changes in several ways as we age:
• The degenerative process inherent to ageing produces a thinning, drying and sagging of our skin1
• The dermo-epidermal junction flattens out
• Skin injuries increase.
Elderly skin experiences a loss of approximately 50% of dermal thickness by the age of 802 , which means the skin is less resilient. It is also slower to heal and has decreased sensory perception, which could lead to increased skin injury.
The effects of incontinence on elderly skin
In elderly patients requiring continence aids, skin irritations increase in a non-breathable occlusive environment when the skin is exposed to urine, faeces or frequent cleansing for prolonged periods. This is because normal skin pH becomes alkaline when exposed to the ammonia associated with urine or faeces. It’s this process that reduces the skin’s barrier function.
Quality continence aids are designed to quickly draw urine away from the skin whilst still creating a breathable environment to allow the skin to breathe and maintain a healthy pH level. Quality continence aids should be used in conjunction with
preventative skin care products to create a comprehensive continence care plan that helps to maintain skin integrity and comfort.
A common skin issue in patients with incontinence is Incontinence Associated Dermatitis or IAD, the clinical manifestation of moisture-associated skin damage3. Skin humidity and ageing skin are aggravating factors in the development of IAD4. Therefore cleaning with harsh soap may not be the most appropriate component of the patient’s skin care regime. Skin cleansers and gentle body washes that match the patient’s skin pH are a good choice, as harsh soap have a high alkaline level and should be avoided5.
Owing to the fragile nature of elderly skin, and the fact that up to 42% of skin problems are prevalent in long term incontinent patients6, a careful and thorough skin regime in combination with a high quality, breathable continence aid is critical to skin health and quality of life.
That’s why TENA now has a modern skin care range of products specifically designed for use on fragile and sensitive elderly skin. TENA Skin Care includes five products designed for gentle no-rinse care, which not only helps to maintain healthy skin but also saves time, with no need for rinsing and drying. TENA Wash Cream and TENA Wet Wipes are also 3-in-1 skin care products meaning that they cleanse, moisturise and leave a protective layer all in one application.
• TENA Wash Cream: a 3-in-1 no-rinse emulsion, which can be safely left on the skin and in skin folds. It is a gentle cleanser, moisturiser and protective cream all in one.
Recent Community and Aged Care trials of TENA Skin Care saw some amazing results and feedback from participants.
“My client’s skin started improving immediately. The skin regime of lotions has decreased. We are using these products twice per day with fantastic results…this client is now happy to go out into the community with family and friends – what a terrific result!” [Erica]
“…I believe that since the introduction of the TENA Skin Care range, skin issues have resolved and resident skin conditions have improved, particularly in the reduction of excoriations. As Quality Co-ordinator, I highly recommend the use of the TENA Skin Care products.
Staff loved the implementation of the TENA Wet Wipes. They are soft but strong, protect the resident’s skin and effectively clean the area without any skin irritation even with the most sensitive skin.” [Carolyn, Fairview Village]
“I just can’t put it into words – thank you so much. You really made life so much easier, I hope to restart my croquette again, I really have got my confidence back. Thank you again” [Margaret]
14 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 15
CARELINES ISSUE #5
• TENA Wet Wipes: a 3-in-1 pre-moistened large and soft wipe that cleanses, moisturises and leaves a protective layer on even the most delicate skin.
• TENA Soft Wipe: a soft and strong cellulose wipe that is lint free and designed for gentle skin cleansing with TENA Wash Cream. An extra-large wipe with excellent wet and dry strength, it can also be used in the place of a face washer, saving on laundry.
• TENA Skin Lotion: A mild and gentle moisturiser ideal for dry and sensitive skin, helping restore the natural skin moisture balance.
• TENA Barrier Cream: forms a transparent protective barrier over irritated or high-risk skin to protect from external irritants.
The newest addition to TENA’s skin care range is the TENA Shampoo & Shower, available to order from July. It combines a gentle all-over body wash with a mild conditioning shampoo for use on delicate hair and skin in the bath or shower. Not only does it save staff time combining shampoo and body wash into one product, it has also been specifically designed to be extra gentle on elderly skin and hair, leaving it soft and clean.
References
1 Farage M. A, Miller K. W, Berardesca E, Maibach H. Textbook of Aging Skin. Germany: Springer-Velag Berlin Heidelberg; 2010
2 Wagen et al, Promoting Continence: A Clinical and Research Resource. Elsevier Health Sciences 2002: 150
3 Beeckman D et al, Prevention and treatment of incontinence-assocaited dermatitis: literature review, Journal of Advanced Nursing 2009:11423.
4 Runeman, B Skin interaction with absorbent hygiene products. Clinics in Dermatology 2008 26 (1):46
5 nursingcenter.com/prodev/ce_article.asp?tid=1130247 [webpage on the Internet] USA: Advances in Skin & Wound Care: The Journal for Preventing and Healing; 2011. Available from www.nursingcenter.com
6 Runeman, B Skin interaction with absorbent hygiene products. Clinics in Dermatology 2008 26 (1):46

16 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Conference NewsComing up this year:Nurses In Management Aged Care (NIMAC) 3-5 July 2013The NIMAC Conference and Trade Exhibition 2013 brings together nurses working in the aged care industry.
This annual event provides the opportunity for nurses to gather, network and visit the trade exhibition and speak with sponsors who provide relevant information, products and services. The theme for this year’s Conference is ‘Enriching Culture Through Diversity’. The program for 2013 is informative and challenging. It will encourage delegates to develop new visions and strategies for the future.
Leading Age Services Australia (LASA) National Congress 5-7 August 2013The LASA Congress will provide a unique opportunity for members of the aged services industry to extend their knowledge in their respective professional fields. The program will include presentations and panel discussions on a wide range of issues including: leadership, governance, current government policy challenges, innovation, consumer behaviour, business processes, human capital development, technology, integrated housing, entrepreneurship, and much more.
The theme ‘New Frontier: New Focus’ is perfect for the time we are living in. Age
Services are experiencing change never before witnessed and the industry is looking to advance and plan their future to create stability and certainty.
ACSA NATIONAL CONFERENCE 2013, 10 - 13 Nov, MelbourneAged and Community Services Australia (ACSA) 2013 National Conference Theme ‘Facing reform – jumping hurdles and staying in the race’ aims to address the changes currently happening in the industry and offer broad picture solutions to those challenges. Speakers: Ms Ita Buttrose, Professor Ian Maddocks, Dr Colin Milner, Peter Shergold, Dr Adam Fraer, Ms Gill Hicks, Justice Michael Kirby, Mr Jeff Kennett AC and many other international speakers.
HEALTHCARE PTY LTD
Solutions for Dysphagia, Supplements for Nutrition
• Pro
-aid
He
alth
care Quality Assured •
Care & Nutritio
nHealth Care
www.proaidhealthcare.com.au & 1300 897 965.
TM

16 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 17
CARELINES ISSUE #5
Dietary Strategies for Management of DysphagiaDysphagia: Difficulty swallowingNicola Fox, Accredited Practising Dietitian and Clinical Nutritionist BHlthSci (Nutr & Diet) Hons APD
Dysphagia affects many groups of people including Stroke Sufferers, Multiple Sclerosis, Parkinson’s Disease, Motor Neurone Disease, People with Cancer of the throat and/or mouth, People with head and neck injuries, People with Chronic Heartburn, Internal burns associated with poisoning or radiotherapy, medical accidents resulting in tearing of the throat lining.
In Aged Care you will see some Dysphagia sufferers in the above groups but mostly it will be the elderly and those affected by Alzheimer’s Disease or other Dementias, poor dentition, stroke, traumatic brain injury, Parkinsonism, amyotrophic lateral sclerosis, debilitation after cardiac surgery, brain injury or prolonged intubation.
There are many different signs and symptoms associated with Dysphagia. Some examples are - a wet gurgly voice, coughing or choking when eating or drinking, drooling, pocketing of food, difficulty initiating the swallowing process, poor lip closure, poor head control, slurred speech, and excessively long eating time are indicators of swallowing difficulty. If any of these conditions persist, assessment by speech pathologist is warranted, and modifications in food and liquid consistencies may be indicated.
Management of dysphagia may involve consultation with specialists from many disciplines including a Speech Pathologist,
Dietitian, Occupational Therapist or Physiotherapist.
People with Dysphagia need assessment and management to avoid dehydration and malnutrition - if liquids and foods are not being consumed in adequate amounts. For some People, the ability to tolerate food or liquids declines to the point that tube feeding is required to replace oral feedings
Also of concern is aspiration. People with Dysphagia need assistance to reduce the chance of food and drink going down ‘the wrong way’ and ending up in the airways and lungs which can lead to aspiration pneumonia which is associated with increased mortality.
People affected by Dysphagia may require the texture of liquids and foods to be modified with a thickening product in order to help them swallow more safely.
Thin liquids (other than pure water taken alone in small sips) may need to be avoided. Commercial thickeners and thickened fluids are available. Different products and consistencies for thickening food and liquids should be tried until the best tolerated texture for the individual’s swallowing function is found. Most speech pathologists recommend either fluid nectar (apricot juice consistency), soft (honey consistency) or firm (pudding consistency) depending on the client’s abilities and functional recovery.
Thickening products are designed to assist patients with swallowing function by preventing aspiration.
Solid foods need to be pureed or
softened, so they need less chewing and require less propulsive force to clear them through the pharynx.
Food also needs to look appealing to stimulate appetite. For example - puree meat and vegetables separately so they do not look unappetising. Use deep coloured vegetables. Use food moulds to present purred foods in an appealing manner.
Include highly seasoned, flavourful, aromatic foods; add sugar or spices. Serve food at cold temperatures. Try offering small frequent meals and avoid sticky and bulky foods.
Nicola Fox,Accredited Practising Dietician and Clinical Nutritionist.
HEALTHCARE PTY LTD
Solutions for Dysphagia, Supplements for Nutrition
• Pro
-aid
He
alth
care Quality Assured •
Care & Nutritio
nHealth Care
www.proaidhealthcare.com.au & 1300 897 965.
TM
18 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]

www.eboshealthcare.com.au 19
CARELINES ISSUE #5
18 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Pallative Care - Time to talk about it
Palliative Care Australia has released last month the results of their survey on Palliative Care awareness, conducted by Pure Profile on 1,000 Australians to mark ‘Palliative Care Week’ which ran from 19th to 25th May 2013. The initiative aimed to increase awareness about palliative care services, and showed that too many Australians do not talk enough about end of life care with their loved ones and do not know what is offered or how to access palliative care.
The survey shows that half of Australians who recently lost a loved one had not discussed with them their end of life care, that only 15% of those who died had an advanced care plan in place which detailed their wishes, and almost 30% were not catered for in the place of their choice.
Overall, 56 per cent of respondents said their loved one’s wishes were carried out as expected.
Dr Yvonne Luxford (Palliative Care Australia CEO) said: “Unfortunately the survey reveals Australians simply aren’t having conversations about death and dying and are therefore flying blind when it comes to understanding the end of life wishes of their loved ones. Discussion about the type of care we want, and what we want to be cared for are important for every single one of us.
While there is nothing tougher than losing a loved one, talking about and planning for a loved one’s final weeks is a simple act of love everyone can do to reduce the burden on those left behind and help make decision making simpler at a difficult time.”
PCA president Professor Patsy Yates said that while death is not an easy topic for discussion it is essential to alleviate the stress felt by all those who have to make decisions about end of life care without insights into the person’s wishes. Advance care planning can ensure our loved ones’ choices for medical treatment
are recognized so that their beliefs, preferences and values are respected.”
The survey also shows that awareness about accessing palliative care services needs to be raised.
While 45% of respondents’ loved ones received palliative care, another 44% didn’t and the remaining 11% did not know what Palliative care is. Of those receiving palliative care, 83 per cent say it far or somewhat exceeded expectations, but 17 per cent reported they found it difficult to access palliative care services.
There are a wide range of specialist services available to help ensure Australians have quality end of life care, and an extensive amount of information at hand to help people prepare for death and dying.
Visit the Palliative Care Australia website for more information. www.palliativecare.org.au
Gen. Peter Cosgrove, newly appointed chairman of the aged services industry peak body Leading Age Services Australia (LASA), says in an interview on ABC Radio that 83,000 more aged care beds are needed within 9 years to care for the growing elderly population.General Cosgrove launched LASA’s “three million reasons” campaign in Sydney
at the end of May; the name of the campaign comes from the fact that there are 3 million Australians who are over 65 (as per 2011 Census report), and current Aged Care resources are nowhere near the level where the system will be able to cope with the aging population.
It is estimated that the number of people over 65 in this country needing aged care services will be doubling from three million now to over six million in 2050, so it is quite simple - we will have so
many more people to be looked after in Aged Care hence the system needs more funding.
General Cosgrove says ‘the numbers are real and they are sobering: 83,000 beds need to be built in residential aged care in the next nine years at an estimated cost of $17 billion’.
Aged Care Cannot Meet the DemandAs Elderly Population Grows

20 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
For more information:
Join the Evolution
Break the cycle of cross-infection with Vernacare’s new 100% disposable solution for patient toileting ...Vernacare’s new bedpan and disposable pulp support not only helps to reduce the risk of cross infection, but also supports hospitals’ sustainability agendas, providing environmental, financial and nursing time savings.
The products have been developed collaboratively with clinicians across the globe, to provide a 100% disposable solution to patient toileting.
The fully disposable system reduces the risk of cross-infection associated with re-usable plastic products and helps tackle spiralling HAIs costs.
• Intuitive tear-shaped design minimises contact with patient’s skin
• Curved edges allows easier patient positioning
• Ergonomic design reduces pressure on coccyx
• Can be used in all major commode chair brands
• Independent support pillars distribute weight evenly
• Inner ribbed wall provides strength when used in bed
• Can be disposed of in pulp disposal unit
Financial Benefits
� Reduced HCAI costs
� Rationalise multiple products
� Reduced cleaning costs
Environmental Benefits
� Eliminate plastic supports being landfilled
� Reduced energy consumption vs washer disinfectors
� Reduced clinical waste impact
Nursing Benefits
� Nurse time saved
� More time released to care
� Easier to toilet patient
� Increased staff satisfaction
Infection Prevention Benefits
� Fully disposable system
� Lower risk of cross infection
� Increased patient safety
� Easier to clean plastic support
• Free Call 1800 269 534 • Free Fax 1800 810 257 • Email [email protected]

20 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 21
CARELINES ISSUE #5
Vernacare Launch New Disposable Bedpan & SupportAs a leading provider of infection prevention products and solutions, Medical Product manufacturer Vernacare UK are changing how patients are toileted in hospital and aged care environment with the launch of their fully disposable pulp Bedpan and Support.
The innovative system, which makes use of a new disposable pulp bedpan liner and disposable pulp support, is a significant step forward for infection prevention.
The design of current pulp bedpans has not evolved for decades, and has always required the use of a plastic support when used to toilet patients in bed. Vernacare have addressed this challenge through an extensive project to develop the world’s first fully disposable support, helping to minimise the risk of cross infection.
This challenge has resulted in extensive detailed design work and global field-based evaluations, gaining very positive support from clinicians and patients alike.
“The new product combines increased user comfort with functional performance -and we believe that the removal of a plastic support and the switch to Vernacare’s unique fully-disposable system will continue to help in driving down infection rates and support patient safety” said Emma Sheldon, Vernacare Global Marketing Director.
The new system has been developed with patients in mind, as the unique patented design will help improve the patient experience, by providing a more
comfortable and dignified alternative to traditional bedpans.
“The design has been developed collaboratively with customers from across the world, ensuring it addressed the needs of the global healthcare market in terms of functionality and ease of use for both patient and nurse.” added Jane Kent, Vernacare New Product Development Manager. “The disposable nature of the support will provide significant cost savings to facilities by helping to reduce their infection rates, and we have seen similar interventions produce exceptional results, such as the study involving the Vernacare Washbowl, conducted at Salford Royal Hospital for example”.
In February 2007, the Vernacare detergent proof Washbowl was introduced as a part of several interventions at Salford Royal NHS Foundation Trust. The study found that over a 6 month period, cases of Clostridium Difficile infection reduced by 56%*, and have been maintained since that time.
Vernacare’s award winning detergent proof washbowl was recently showcased at the Infection Prevention Society Conference & Exhibition on 1-3 October 2012, alongside the latest products in Vernacare’s new product development pipeline.
The new system of disposable bedpan and bedpan support will also reduce the environmental impact and cost of processing plastic supports and will provide a significant time saving for nurses, which will in turn release more time to spend caring for patients.
For further information, free samples or to arrange a free trial, please contact us at [email protected]
Reference.
Reducing Clostridium Difficile infection in acute care by using an improvement collaborative - Power M, Wigglesworth N et al, Salford Royal NHS Foundation Trust, UK, BMJ 2010; 341: c3359
Bedpan & support

22 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Hand Hygiene Compliance: It’s Time For A Change
For over 70 years, the Deb Group has been providing skin care solutions in the form of hand hygiene products and dispensers, for all types of workplace and public environments, spanning industrial, commercial, automotive, food and healthcare sectors.
Deb’s skin care solution for the healthcare sector has been specifically designed to satisfy all occupational, community and acute healthcare needs; comprising a complementary range of skin care products & support activities to help raise the level of staff compliance, improve skin condition and reduce the risk of cross-infection.
Deb has gained a deep insight into the factors that affect skin care compliance by working with healthcare professionals, to increase levels of hand hygiene, for over 20 years. As such, Deb also offers advice on how to drive improvements and encourage behavioural change amongst colleagues, patients and visitors to prevent the spread of harmful bacteria and viruses.
Maintaining good skin condition is vital to protecting the health of both staff and patients. The Cutan hand hygiene product range encourages best practice to achieve safe and acceptable levels of care through the use of a Hand Hygiene Procedure, which consists of 3 simple stages to achieve maximum hand hygiene compliance: Cleanse, Sanitise and Restore.
Deb also offers a bespoke service where dispensers can be tailored to meet specific requirements, providing choice of colour, logo and message. Customised dispensers are a great way to raise awareness of the hand hygiene facilities available and also to promote an appropriate infection prevention message whilst reflecting the organisation’s corporate style.
There has never been a better time to talk to your EBOS Key Account Manager about improving your hand hygiene provision with the Cutan range.
Buy 2x Cartridges of
Cutan Foam Hand Sanitizer 1L
(code DEB6195EE) and receive a
FREE Dispenser(XXBONUS241)
Cleanse - Apart from cleaning any visible soilings from hands, the physical action of a good hand washing technique will remove high levels of bacteria and viruses present on the skin.
Sanitise - Hand sanitising is an effective way to reduce bacterial counts on visibly clean hands, when access to soap and running water is inconvenient.
Restore - This is the most important step in maintaining good skin condition. As a consequence of frequent hand washing, it is necessary to regularly replenish the natural oils and secretions lost from the skin via the use of a conditioning cream.

22 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 23
CARELINES ISSUE #5
An excellent value for money solution combining some of the best of the premium9 features in an Overlay System.
Prevention is the core strategy of this product, designed and developed to ensure the debilitating effects of Decubitus Ulcers are avoided.
Used in conjunction with an effective pressure injury preventative strategy including diet, exercise and care management, the premium5 is a highly effective pressure care overlay solution.
Easy to place over any existing mattress this lightweight, manoeuvrable and versatile overlay system is especially appropriate for home care and nursing home settings.
Best suited for:
� Home care
� Nursing home
Key SpecificationCode PTAM0030Length (mm)* 2000Width (mm)* 880Depth (mm)* 135Max User Weight 150kg
The premium8 is the economical full mattress replacement system for the high risk user. Ideal for the heavier patient, the system provides an increased cell depth to prevent bottoming out and enhance therapeutic benefits and comfort.
Best suited for:
� Home care
� Nursing home
Key SpecificationCode PTAM0050Length (mm)* 2000Width (mm)* 880Depth (mm)* 230Max User Weight 180kg
The premium9 is a cost effective, professional solution for high to very high risk
patients. The unique heel zone ensures effective alternation of the high risk calcaneus and
malleolus areas of the lower leg. Combined with lateral side bolsters for additional
patient stability, it is ideal for patients at risk of developing pressure related ulceration.
Best suited for:
� Home care
� Nursing home
� Hospital
� ICU/HCU
Key SpecificationCode PTAM0070Length (mm)* 2000Width (mm)* 880Depth (mm)* 280Max User Weight 180kg
* Mattress dimensions.
* Mattress dimensions.
* Mattress dimensions.
Carelines SPECIALReceive a FREE crash mat when you purchase
the premium5, premium8 & premium9 overlay systems Code: 19220009 + 19220010 + 19220011 + XXBONUS240
Valued at $116
Mention Carelines to receive this great offeremail: [email protected]

24 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
We hope you enjoyed this issue!
Visit: www.eboshealthcare.com.au
to receive this newsletter via email
Just click on the subscribe button.
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
Carelines is an EBOS initiative designed to support
the ongoing education and development of our
valued customers and their staff. Each edition
explores a wide range of topics relevant to the
aged care sector such as advanced wound
care, incontinence, infection prevention, nutrition
and oral care. Our objective is to continue
the support of people caring for people.





























