Embed Size (px)
DESCRIPTION
ketokonazol
Citation preview

A double-blind, randomized, placebo-controlled study to assess the efficacy ofketoconazole for reducing the risk ofovarian hyperstimulation syndrome
Mohammad Ebrahim Parsanezhad, M.D.,a Saeed Alborzi, M.D.,a Mahnaz Pakniat, M.D.,a
and Ernst Heinrich Schmidt, M.D.b
Shiraz University of Medical Sciences, Shiraz, Iran, and Evang. Diakonie Teaching Hospital of GottingenUniversity, Bremen, Germany
Objective: To evaluate the role of ketoconazole in prevention of ovarian hyperstimulation syndrome (OHSS)in women with the polycystic ovary syndrome (PCOS) undergoing ovarian stimulation with gonadotropins.
Design: Prospective, randomized, double-blind, placebo-controlled study.
Setting: University hospitals.
Patient(s): One hundred nine women with PCOS who were referred for treatment with gonadotropins.
Intervention(s): Fifty patients were randomly assigned to receive two ampoules of hMG beginning on day2 or 3 of the cycle and ketoconazole (50 mg every 48 hours) starting on the first day of hMG treatment.Fifty-one patients received the same amount of hMG plus one tablet of placebo every 48 hours.
Main Outcome Measure(s): Follicular development, E2 level, and pregnancy rate.
Result(s): The total number of hMG ampoules and duration of treatment to attain ovarian stimulation werehigher among ketoconazole recipients. The serum E2 level and number of patients with dominant follicles onday 9 of the cycle were greater in placebo recipients. Serum E2 level and total number of follicles at the timeof hCG administration did not differ between the two groups. The cancellation rate and OHSS rate weresimilar in the two groups.
Conclusion(s): Ketoconazole does not prevent OHSS in patients with PCOS who are undergoing ovarianstimulation. It may reduce the rate of folliculogenesis and steroidogenesis. (Fertil Steril� 2003;80:1151–5. ©2003 by American Society for Reproductive Medicine.)
Key Words: Polycystic ovary, gonadotropins, hyperstimulation, ketoconazole
Ovarian hyperstimulation syndrome (OHSS)is a relatively common and potentially life-threat-ening complication of ovarian stimulation withgonadotropins (1). In its severe form, the syn-drome is characterized by extreme ovarianmultifollicular enlargement, ascites, hydrotho-rax, hypovolemia, and hemoconcentration (2).
The underlying mechanisms leading toOHSS remain to be elucidated, but excessivequantities of peptides regulating the growthand permeability of blood vessels are likely tobe involved (3). Some authors have suggestedthat augmentation of steroids and peptide pro-duction from the multifollicular hyperstimu-lated ovaries may be responsible for severalfeatures of the OHSS (4).
Vascular endothelial growth factor has beenshown to exert a twofold effect: It serves as apotent promoter of neovasculogenesis and in-creases vascular permeability (5–7).
Early identification of patients at risk andprevention of OHSS is clinically important.Several methods have been recommended forminimizing the probability of OHSS in high-risk patients, including canceling the cycle be-fore administration of hCG or reducing theovulatory hCG dose (8), withholding lutealsupport with hCG (9), cryopreserving all em-bryos for further use in a nonstimulated cycle(10), repeating aspiration of ovarian folliclesand early corpus luteum cysts (11), administer-ing human albumin at the time of hCG injec-
Received December 5,2002; revised andaccepted April 2, 2003.Reprint requests:Mohammad EbrahimParsanezhad, M.D., P.O.Box 71345-1657, Shiraz,Iran (FAX: 98-711-229-6486; E-mail:[email protected]).a Department of Obstetricsand Gynecology, School ofMedicine, Shiraz Universityof Medical Sciences.b Department of Obstetricsand Gynecology, Evang.Diakonie Teaching Hospitalof Gottingen University.
IN VITRO FERTILIZATIONFERTILITY AND STERILITY�VOL. 80, NO. 5, NOVEMBER 2003Copyright ©2003 American Society for Reproductive MedicinePublished by Elsevier Inc.Printed on acid-free paper in U.S.A.
0015-0282/03/$30.00doi:10.1016/S0015-0282(03)01177-4
1151

tion (12), using GnRH analogue to trigger ovulation (13),and performing vaginal aspiration of ascites (14).
Ketoconazole interferes with cytochrome P450 enzymesystems in testis, ovary, adrenal gland, and liver. Steroido-genesis is inhibited by its action on the C17-20 lyase, thecholesterol side-chain cleavage enzyme, and the 17�-hy-droxylase. In gonads, it inhibits aromatase, and adrenocor-tical steroid biosynthesis is inhibited at the 11�-hydroxyla-tion and 18-hydroxylation steps.
The antiandrogenic effect of ketoconazole may be usefulin the management of metastatic prostate carcinoma andhirsutism. Its anticortisolic effect may be useful in the treat-ment of most patients with Cushing’s syndrome (15–17).
Ketoconazole, a broad-spectrum imidazole antimycoticagent, was recently reported to reduce the incidence ofOHSS in women with PCOS undergoing superovulationwith gonadotropins (18). Because this study was not placebocontrolled, however, a placebo effect could not be ruled out.
We performed a double-blind, placebo-controlled studyto assess the role of ketoconazole in prevention of multifol-licular development, excess ovarian steroidogenesis, andmoderate and severe OHSS in patients with PCOS undergo-ing superovulation with gonadotropins.
MATERIALS AND METHODS
The study was performed at Shiraz University of MedicalSciences, Shiraz, Iran. From September 2000 to November2002, we enrolled 637 women with PCOS from our infer-tility division into this prospective, randomized, double-blind, placebo-controlled study.
Patients were interviewed, the study protocol was describedto them, and patients’ charts were carefully reviewed. Patientshad undergone a complete infertility evaluation that includedhormonal assay, hysterosalpingography, postcoital testing, se-men analysis, and endometrial biopsy. Inclusion criteria wereinfertility, an elevated serum LH level, a normal or elevatedFSH level, an LH-to-FSH ratio greater than 2, elevated testos-terone and DHEAS levels, oligomenorrhea or amenorrhea, andat least 10 follicles smaller than 8 mm in diameter in thesubcapsular region around the hyperechogenic central stromaon ultrasonography.
Except for PCOS-related anovulatory infertility, womenwith other infertility factors were excluded. A total of 528patients were excluded (217 women did not fulfill the inclu-sion criteria and 311 women declined to participate). Thus,109 women were randomly allocated after giving informedconsent. The ethics review committee for human research ofthe university approved the study.
Women had been unsuccessfully treated with clomiphenecitrate at daily doses of up to 200 mg for 5 days. All werebeing considered for treatment with hMG. They received
their allocated intervention from the first menstrual cycleafter randomization.
Serum concentrations of liver aminotransferase and bili-rubin were measured by using kinetic and colour anylinmethods, respectively. E2 was assayed by using the Coat-a-Count recombinant immunoassay (Diagnostics Products Co.,Los Angeles, CA) 2 to 3 days after the start of menstrualbleeding or progesterone-induced bleeding between days 1and 3 of menstrual cycle. During this time, transvaginalultrasonography was performed by using a 5-MHz transvag-inal transducer (Medison 600, Korea).
All patients had sonographic characteristics of PCOS.Liver aminotransferase and bilirubin levels were normal inall patients. The serum E2 level was normal for the earlyfollicular phase.
Before receiving the allocated intervention and undergo-ing work-up, all patients were randomized by using a ran-dom table. A pharmacist who did not take part in this studyadministered medication and placebo. Neither the patientsnor the physician and laboratory staff knew the treatmentprotocol.
The ketoconazole administration protocol was similar tothat used as alternate protocol by Gal et al. (18). Fiftypatients received two ampoules of hMG (75 IU of FSH and75 IU of LH per ampoule) (Organon, Oss, The Netherlands)i.m. beginning on day 2 or 3 of the cycle and the minimaldose of ketoconazole (50 mg) starting on the first day ofhMG treatment. Ketoconazole was given at a dose of 50 mgevery 48 hours, and its administration was limited up to thelast day of hMG stimulation. Fifty-one patients received thesame hMG protocol but received one placebo tablet every 48hours.
Ovarian stimulation was monitored by ultrasonographicassessment of total number of growing follicles, mean di-ameter of the follicles, and the full endometrial thickness andmeasurement of E2 every 2 days.
Ovulation was triggered by i.m. injection of 10,000 IU ofhCG (Organon) when the leading follicle reached a diametergreater than 16 mm and the E2 concentration was greaterthan 300 pg/mL for each main follicle (�16 mm in diame-ter). Liver aminotransferase and bilirubin measurement wasrepeated on the last day of ketoconazole and hMG adminis-tration.
Ovarian hyperstimulation syndrome was predicted by us-ing the criteria described by Rabe et al. (19). The syndromewas graded by using established criteria (20). If a patient wasat risk of OHSS, the hCG dose was reduced to 5,000 IU orher cycle was cancelled (i.e., administration of hCG waswithheld). Patients were monitored during the luteal phase 6� 2 days and 12 � 1 days after injection of hCG. They wereasked about symptoms of OHSS (abdominal pain, nausea,vomiting, diarrhea, and weight gain).
1152 Parsanezhad et al. Ketoconazole in prevention of OHSS Vol. 80, No. 5, November 2003
Transvaginal ultrasonography was performed to measureperitoneal fluid, ovarian size, total number of cysts, andmaximum cyst diameter. Blood samples were obtained formeasurement of E2, �-hCG, plasma proteins, and electro-lytes and for a blood count. If any evidence of moderateOHSS was present, the patient was hospitalized for furthermanagement.
Clinical and laboratory variables were compared betweenthe treatment and placebo groups. Statistical analysis wasperformed by using the Student t-test and �2 test. Correla-tions were calculated at a 95% level of confidence. P�.05was considered significant.
RESULTSOne hundred one women completed the study protocol.
Three ketoconazole recipients and five placebo recipientswere lost to follow-up.
Ketoconazole and placebo recipients did not statisticallydiffer in mean (�SD) age (26.3 � 3.1 years vs. 28.33 � 4.0),body mass index (27.12 � 2.1 kg/m2 vs. 28.62 � 4.8 kg/m2),duration of infertility (3.7 � 1.8 years vs. 3.8 � 1.4 years), andpercentage of participants with primary infertility (81.4% vs.75%). Ketoconazole had no side effects with the treatmentprotocol.
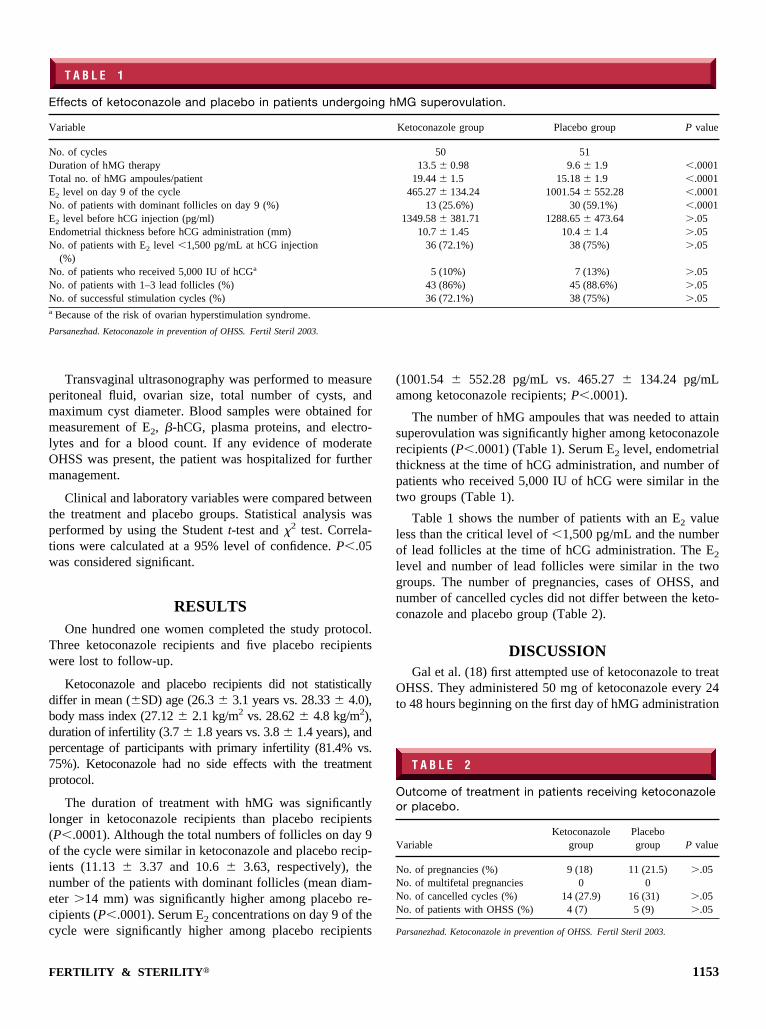
The duration of treatment with hMG was significantlylonger in ketoconazole recipients than placebo recipients(P�.0001). Although the total numbers of follicles on day 9of the cycle were similar in ketoconazole and placebo recip-ients (11.13 � 3.37 and 10.6 � 3.63, respectively), thenumber of the patients with dominant follicles (mean diam-eter �14 mm) was significantly higher among placebo re-cipients (P�.0001). Serum E2 concentrations on day 9 of thecycle were significantly higher among placebo recipients
(1001.54 � 552.28 pg/mL vs. 465.27 � 134.24 pg/mLamong ketoconazole recipients; P�.0001).
The number of hMG ampoules that was needed to attainsuperovulation was significantly higher among ketoconazolerecipients (P�.0001) (Table 1). Serum E2 level, endometrialthickness at the time of hCG administration, and number ofpatients who received 5,000 IU of hCG were similar in thetwo groups (Table 1).
Table 1 shows the number of patients with an E2 valueless than the critical level of �1,500 pg/mL and the numberof lead follicles at the time of hCG administration. The E2
level and number of lead follicles were similar in the twogroups. The number of pregnancies, cases of OHSS, andnumber of cancelled cycles did not differ between the keto-conazole and placebo group (Table 2).
DISCUSSIONGal et al. (18) first attempted use of ketoconazole to treat
OHSS. They administered 50 mg of ketoconazole every 24to 48 hours beginning on the first day of hMG administration
T A B L E 1
Effects of ketoconazole and placebo in patients undergoing hMG superovulation.
Variable Ketoconazole group Placebo group P value
No. of cycles 50 51Duration of hMG therapy 13.5 � 0.98 9.6 � 1.9 �.0001Total no. of hMG ampoules/patient 19.44 � 1.5 15.18 � 1.9 �.0001E2 level on day 9 of the cycle 465.27 � 134.24 1001.54 � 552.28 �.0001No. of patients with dominant follicles on day 9 (%) 13 (25.6%) 30 (59.1%) �.0001E2 level before hCG injection (pg/ml) 1349.58 � 381.71 1288.65 � 473.64 �.05Endometrial thickness before hCG administration (mm) 10.7 � 1.45 10.4 � 1.4 �.05No. of patients with E2 level �1,500 pg/mL at hCG injection
(%)36 (72.1%) 38 (75%) �.05
No. of patients who received 5,000 IU of hCGa 5 (10%) 7 (13%) �.05No. of patients with 1–3 lead follicles (%) 43 (86%) 45 (88.6%) �.05No. of successful stimulation cycles (%) 36 (72.1%) 38 (75%) �.05a Because of the risk of ovarian hyperstimulation syndrome.
Parsanezhad. Ketoconazole in prevention of OHSS. Fertil Steril 2003.
T A B L E 2
Outcome of treatment in patients receiving ketoconazoleor placebo.
VariableKetoconazole
groupPlacebogroup P value
No. of pregnancies (%) 9 (18) 11 (21.5) �.05No. of multifetal pregnancies 0 0No. of cancelled cycles (%) 14 (27.9) 16 (31) �.05No. of patients with OHSS (%) 4 (7) 5 (9) �.05
Parsanezhad. Ketoconazole in prevention of OHSS. Fertil Steril 2003.
FERTILITY & STERILITY� 1153

and reported a significant reduction in OHSS after treatmentwith ketoconazole.
The regimen that we used does not differ from that usedas alternate protocol by Gal et al. (18) in terms of drug,dosage, and follow-up. We found a slow rate of E2 produc-tion during the follicular phase (on day 9 of the cycle) in theketoconazole group compared with placebo recipients. Sim-ilar results were reported when a different dose of ketocon-azole was given (21).
On the 9th day of the cycle, equal numbers of follicleswere growing in the two groups. However, significantlymore placebo recipients had dominant follicles. This findingsuggests that the drug did not affect the total number ofgrowing follicles, but the rate of follicular growth was re-duced. Ketoconazole was expected to prevent multiple fol-licular growth and excess steroidogenesis despite continuinggonadotropin administration to attain acceptable numbers ofdominant follicles, an appropriate serum E2 level, and asuccessful stimulation cycle.
When administration of gonadotropins was continued toreach an acceptable number of dominant follicles to triggerovulation by hCG, some patients developed hyperstimulatedovaries. Zelinski-Wooten et al. (22) and Moudgal et al. (23)also reported a similar finding. They discovered thattrilostane, a 3�-hydroxysteroid dehydrogenase inhibitor, andfadrozole, a nonsteroidal aromatase inhibitor, administeredthroughout the follicular phase to rhesus monkeys undergo-ing ovarian stimulation with human gonadotropins had noeffect on the total number of antral follicles and their distri-bution, the number of retrieved oocytes, and ovulation, de-spite a profound reduction in E2 levels. In contrast, Gal et al.(18) found a substantial reduction in the number of medium-sized follicles and reported a reduction in cancellation ratefrom 37% to 7%.
In our study, the incidence of OHSS in both groups wassimilar to that reported by Gal et al. (18) in their untreatedcycles. We also found no significant difference in the rates ofcycle cancellation and hyperstimulated cycles between ke-toconazole and placebo recipients. The numbers of success-ful stimulation cycles were also similar in the two groups.Our results suggest that during ovulation induction withgonadotropins, ketoconazole may decrease the rate of fol-liculogenesis and steroidogenesis.
The total number of follicles, including small, medium-sized, and leading follicles, and serum E2 levels were similarin the ketoconazole and placebo groups at the time of hCGadministration. These findings may explain why ketocon-azole does not prevent OHSS.
Gal et al. (18) reported that low-dose ketoconazole didnot affect progesterone production. Because progesteronedoes not play a critical role in our results, we did notconsider these values in our analysis.
Zelinski-Wooten et al. (22) reported a reduced fertiliza-tion rate among trilostane-treated monkeys. Similar resultswere reported by Moudgal et al. (23) when aromatase inhib-itor was administered. Although we did not evaluate thefertilization process, the similar pregnancy rate per ovulatorycycle in our two groups may support the idea that low-doseketoconazole does not adversely affect fertilization.
In conclusion, low-dose ketoconazole during stimula-tion cycles with gonadotropins may reduce the rate offolliculogenesis and steroidogenesis. Ketoconazole has nobeneficial effect on the development of multiple follicles,final serum levels of E2 at the time of HCG administra-tion, OHSS development, and cycle cancellation. Furtherstudy to evaluate the effects of various protocols of keto-conazole on vasoactive agents affecting OHSS may behelpful.
References
1. Schenker JG, Ezra Y. Complications of assisted reproductive tech-niques. Fertil Steril 1994;61:411–22.
2. Aboulghar MA, Mansour RT, Serour GI, Elhelw BA, Shaarawy M.Elevated concentrations of angiogenin in serum and ascitic fluid frompatients with severe ovarian hyperstimulation syndrome. Hum Reprod1998;13:2068–71.
3. Pellicer A, Albert C, Mercader A, Musoles F, Remohi J, Simon C. Thepathogenesis of ovarian hyperstimulation syndrome: in vivo studiesinvestigating the role of interleukin-1�, interleukin-6, and vascularendothelial growth factor. Fertil Steril 1999;71:482–9.
4. Neulen J, Yan Z, Raczek S, Wiendel K, Keck C, Weich HA, et al.Human chorionic gonadotropin dependent expression of vascular en-dothelial growth factor/vascular permeability factor in human granulosacells: importance in ovarian hyperstimulation syndrome. J Clin Endo-crinol Metab;80:1967–71.
5. Yan Z, Weich HA, Bernart W, Breckwoldt M, Neulen J. Vascularendothelial growth factor (VEGF) messenger ribonucleic acid (mRNA)expression in luteinized human granulose cells in vitro. J Clin Endo-crinol Metab 1993;77:1723–5.
6. McLure N, Healy DL, Rogers PA, Sullivan J, Beaton L, Haning RV, etal. Vascular endothelial growth factor as capillary permeability agent inovarian hyperstimulation syndrome. Lancet 1994;344:235–6.
7. Shweieki D, Itin A, Neufeld G, Gitay-Goren H, Keshet E. Patterns ofexpression of vascular endothelial growth factor (VEGF) and VEGFreceptors in mice suggest a role in hormonally regulated angiogenesis.J Clin Invest 1993;91:2235–43.
8. Sher G, Salem R, Feinman M, Dodge S, Zouves C, Knutzen V.Elimination the risk of life-endangering complications following over-stimulation with menotropin fertility agents; a report on women under-going in vitro fertilization and embryo transfer. Obstet Gynecol 1993;81:1009–11.
9. Asch RH, Li HP, Balmaceda JP, Weckstein LN, Stone SC. Severeovarian hyperstimulation syndrome in assisted reproductive technol-ogy; definition of high risk groups. Hum Reprod 1991;6:1395–9.
10. Amso N, Ahuja K, Morris N, Shaw RW. The management of predictedovarian hyperstimulation involving gonadotropin releasing hormoneanalog with elective cryopreservation of all pre-embryos. Fertil Steril1990;53:1087–90.
11. Amit A, Yaron Y, Yovel I, Peyser MR, David MP, Botchan A, et al.Repeated aspiration of ovarian follicles and early corpus luteum cysts inan in-vitro fertilization program reduced the risk of hyperstimulationsyndrome in high responders. Hum Reprod 1993;8:1184–6.
12. Asch RH, Ivery G, Goldsman M, Fredrick JL, Stone SC, Balmaceda JP.The use of intravenous albumin in patients at high risk for severeovarian hyperstimulation syndrome. Hum Reprod 1993;8:1015–20.
13. Ron ER. Complications of ovulation induction. Baillieres Clin ObstetGynecol 1993;7:435–53.
14. Aboulghar MA, Mansour RT, Serour GI, Amin YM. Ultrasonicallyguided vaginal aspiration of ascites in the treatment of ovarian hyper-stimulation syndrome. Fertil Steril 1990;53:933–5.
15. Sonino N. The use of ketoconazole as an inhibitor of steroid production.N Engl J Med 1987;317:812–8.
1154 Parsanezhad et al. Ketoconazole in prevention of OHSS Vol. 80, No. 5, November 2003

16. Pepper G, Brenner SH, Gabrilove JL. Ketoconazole use in the treatmentof ovarian hyperandrogenism. Fertil Steril 1990;54:438–44.
17. Isik AZ, Gokmen O, Zeyneloglu HB, Senoz S, Zorlu CG. Low doseketoconazole is an effective and a relatively safe alternative in thetreatment of hirsutism. Aust N Z J Obstet Gynaecol 1996;36:487–9.
18. Gal M, Edlar-Geva T, Margalioth EJ, Barr I, Oryl J, Diamanti Z.Attenuation of ovarian response by low-dose ketoconazole during su-perovulation in patients with polycystic ovary syndrome. Fertil Steril1999;27:26–31.
19. Insler V, Lunenfeld E, Lunenfeld B. Ovarian hyperstimulation syn-drome. In: Rabe T, Diedrich K, Runnebaum B (eds). Manual onassisted reproduction. Berlin: Springer, 1997:154–69.
20. Lunenfeld B, Insler V, Rabau E. Induction de l’ovulation par les
gonadotrophines. In: Oricard R, Ferrin J (eds). L’ovulation. Paris:Masson, 1969:27.
21. Gal M, Orly J, Barr I, Algur N, Boldes R, Diamant YZ. Low doseketoconazole attenuates serum androgen levels in patients with poly-cystic ovary syndrome and inhibits ovarian steroidogenesis in vitro.Fertil Steril 1994;61:823–32.
22. Zelinski-Wooten MB, Hess DL, Wolf DP, Stouffer RL. Steroid reduc-tion during ovarian stimulation impairs oocyte fertilization, but notfolliculogenesis, in rhesus monkeys. Fertil Steril 1994;61:1147–55.
23. Moudgal NR, Shetty G, Selvaraj N, Bhatnagar AS. Use of a specificinhibitor for determining whether there is a role for estrogen in follicle/oocyte maturation, ovulation and preimplantation embryo development.J Reprod Fertil Suppl 1996;50:69–81.
FERTILITY & STERILITY� 1155





























