Embed Size (px)
DESCRIPTION
Justus-Liebig-University of Giessen. Dpt. of Neurology. Stroke Management in Germany. Dr. Jens Allendoerfer Dpt. of Neurology University Hospital of Gießen (Head: Prof. Dr. M. Kaps). Bloodletting. Justus-Liebig-University of Giessen. Dpt. of Neurology. built in 1890. Since 1995 - PowerPoint PPT Presentation
Citation preview
Justus-Liebig-University of Giessen Dpt. of Neurology
Stroke Management
in Germany
Dr. Jens AllendoerferDpt. of Neurology
University Hospital of Gießen(Head: Prof. Dr. M. Kaps)
Bloodletting
Justus-Liebig-University of Giessen Dpt. of Neurology
built in 1890
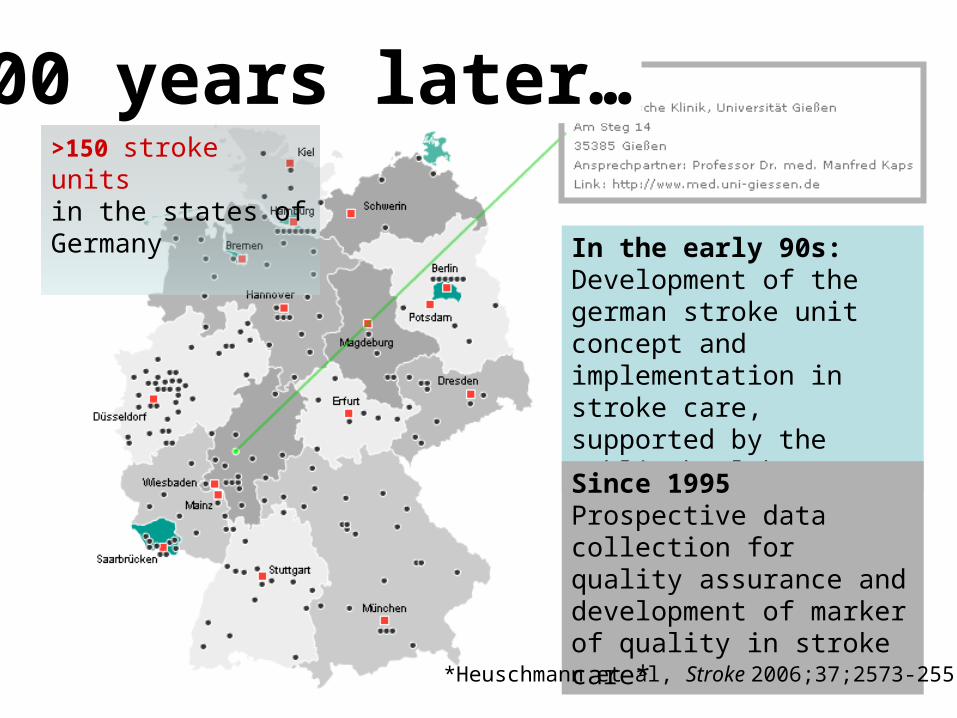
In the early 90s:Development of the german stroke unit concept and implementation in stroke care, supported by the public health system
100 years later…>150 stroke unitsin the states of Germany
Since 1995Prospective data collection for quality assurance anddevelopment of marker of quality in stroke care*
*Heuschmann et al, Stroke 2006;37;2573-2551
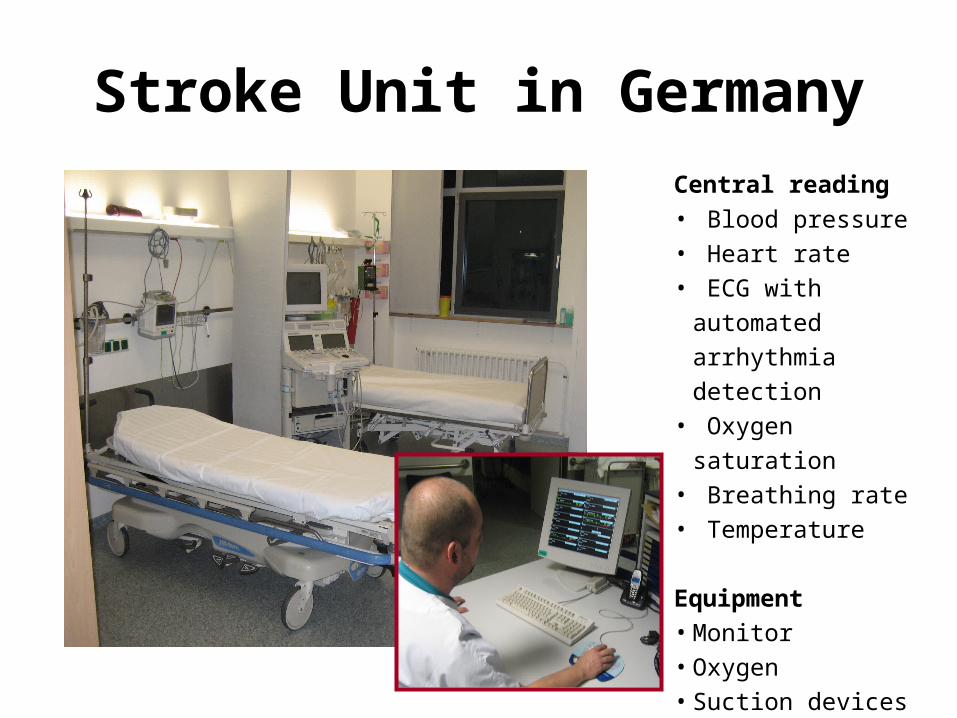
Stroke Unit in GermanyCentral reading
• Blood pressure• Heart rate• ECG with automated
arrhythmia detection• Oxygen saturation• Breathing rate• Temperature
Equipment• Monitor• Oxygen• Suction devices
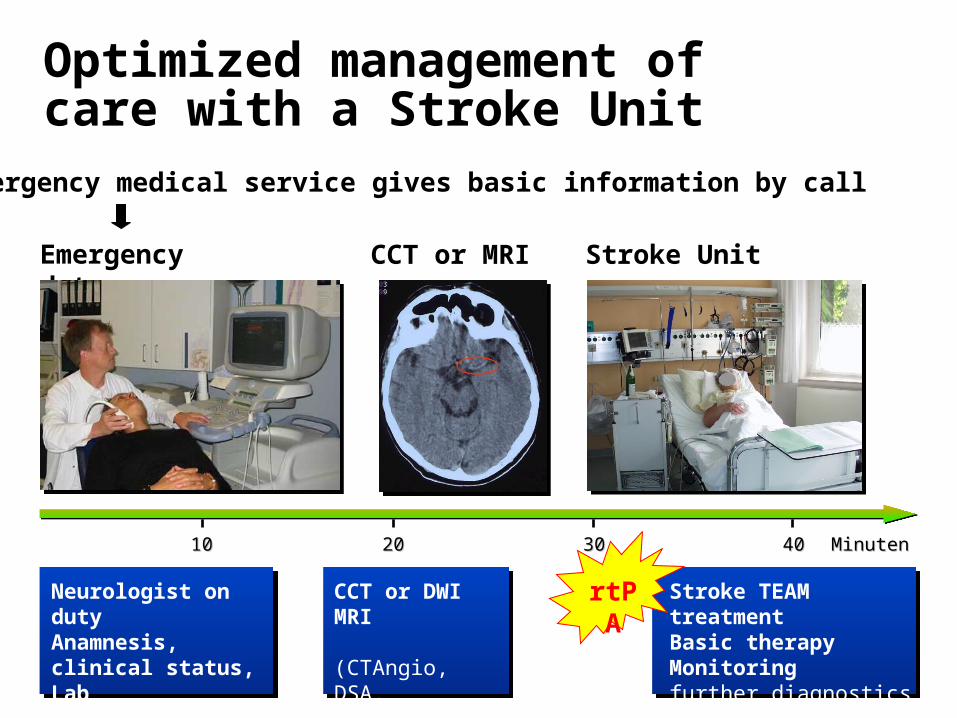
Optimized management of care with a Stroke Unit
MinutenMinuten1010 2020 3030 4040
Neurologist on dutyAnamnesis, clinical status, Lab(EKG, Ultrasound)
CCT or DWI MRI
(CTAngio, DSA,Xray)
Stroke TEAM treatmentBasic therapyMonitoringfurther diagnostics
rtPA
Emergency medical service gives basic information by call
Emergency dpt. CCT or MRI Stroke Unit
Advantages of a Stroke Unit
Admission as early as possible
Organisation of emergency medical service
Specialized staff
Fast diagnosis
Modern treatment strategies
Short hospital stay
Early physio- and speechtherapy
Early Rehabilitation
Admission• demographic data• Time of stroke, of admission• clinical scales like NIHSS & mRS before admission• dependency statusHospital inpatient stay• diagnostic procedures• medical treatment & additional procedures• complications• duration of symptoms• Stroke classification according to TOAST • Findings of MRI and CT scan
End of inpatient treatment• secondary prophylaxis (antiplatelets, statins…)• diagnosis according to ICD-10• clinical scales like NIHSS, mRS, Barthel Index• rehabilitation status (discharge or appointment for rehab.)
Sanctions in case of incomplete documentation
• Data were compared with ICD data of the health insurance• If the rate of QA documentation is below 80% a reduction of
payment follows• These mechanisms provides a nearly complete
documentation of stroke patients
Scientific evaluation
A data core set of all QA documentations in the different states of germany is given to the ADSR (German Stroke Register Study Group) for further evaluation
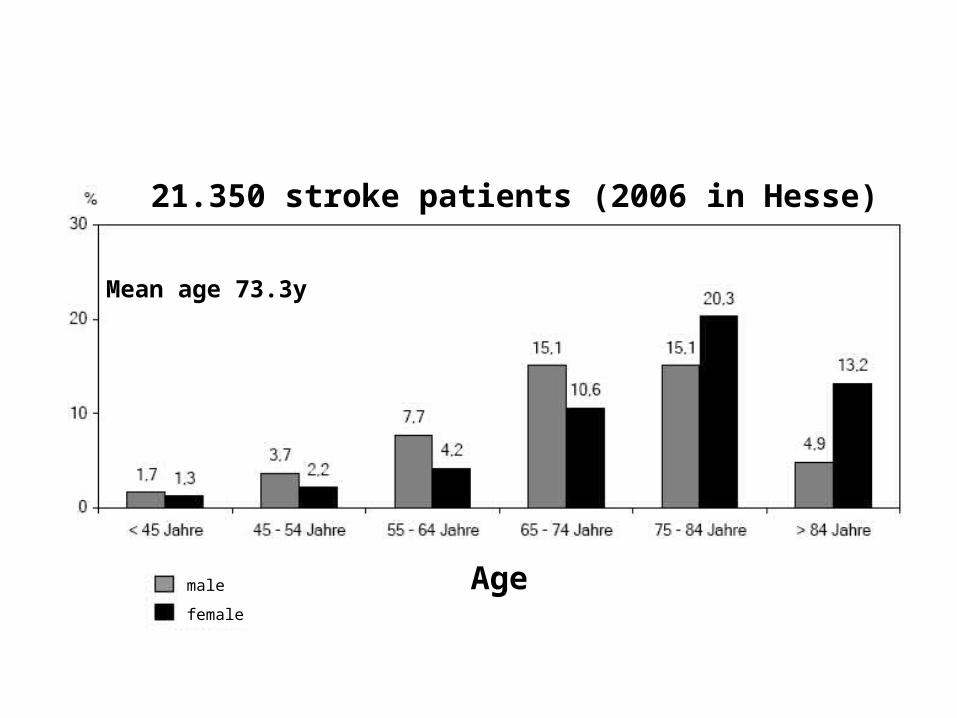
21.350 stroke patients (2006 in Hesse)
male
female
Mean age 73.3y
Age
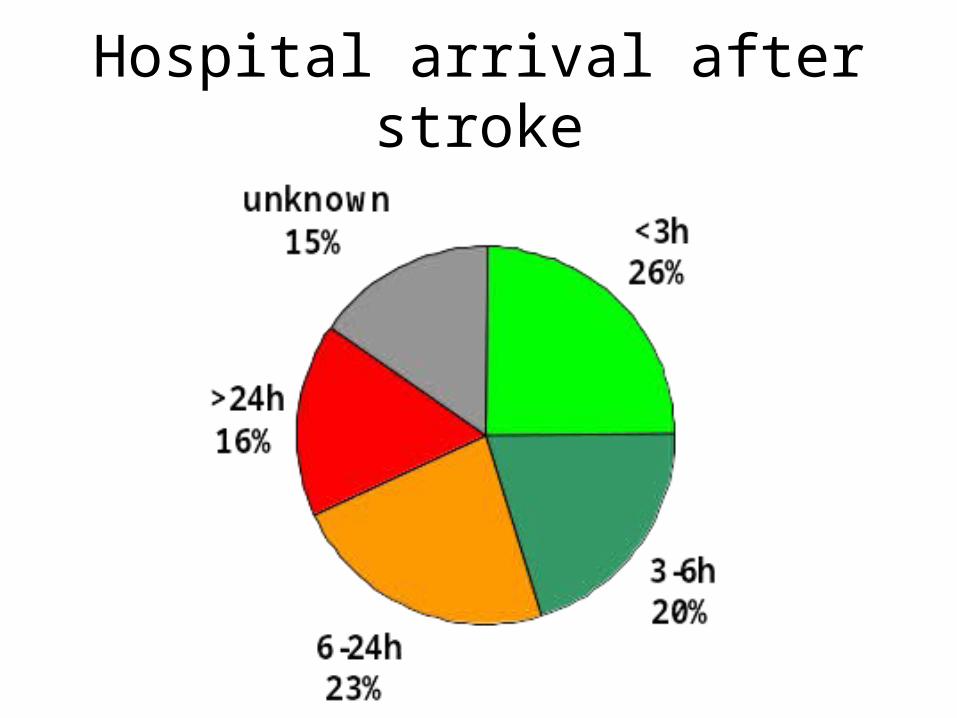
Hospital arrival after stroke
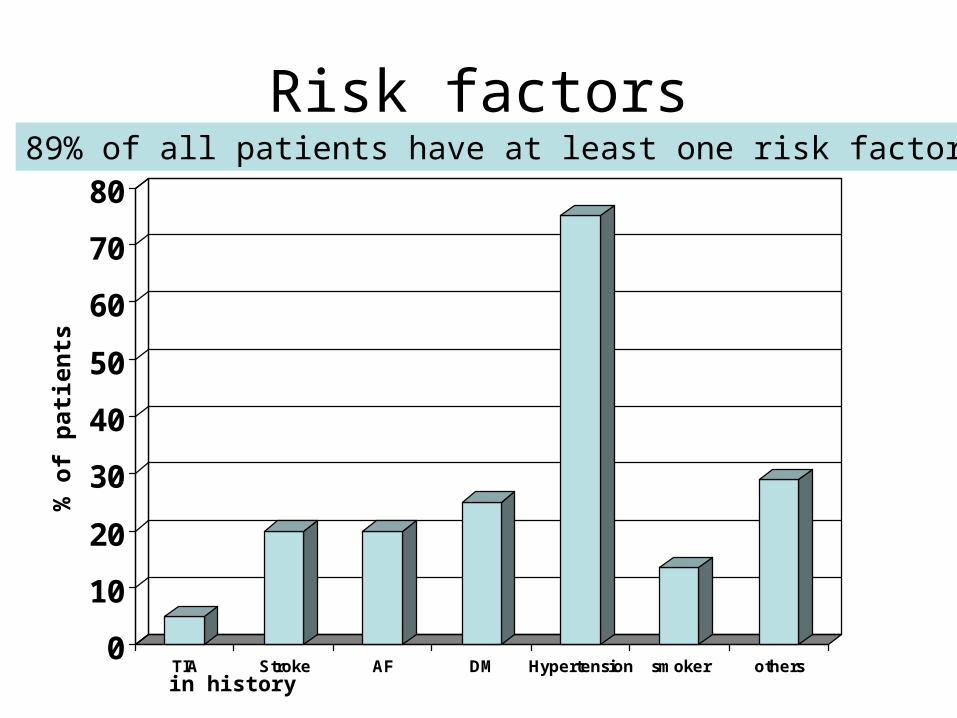
Risk factors
0
10
20
30
40
50
60
70
80
TIA Stroke AF DM Hypertension smoker others
89% of all patients have at least one risk factor
% o
f p
atie
nts
in history
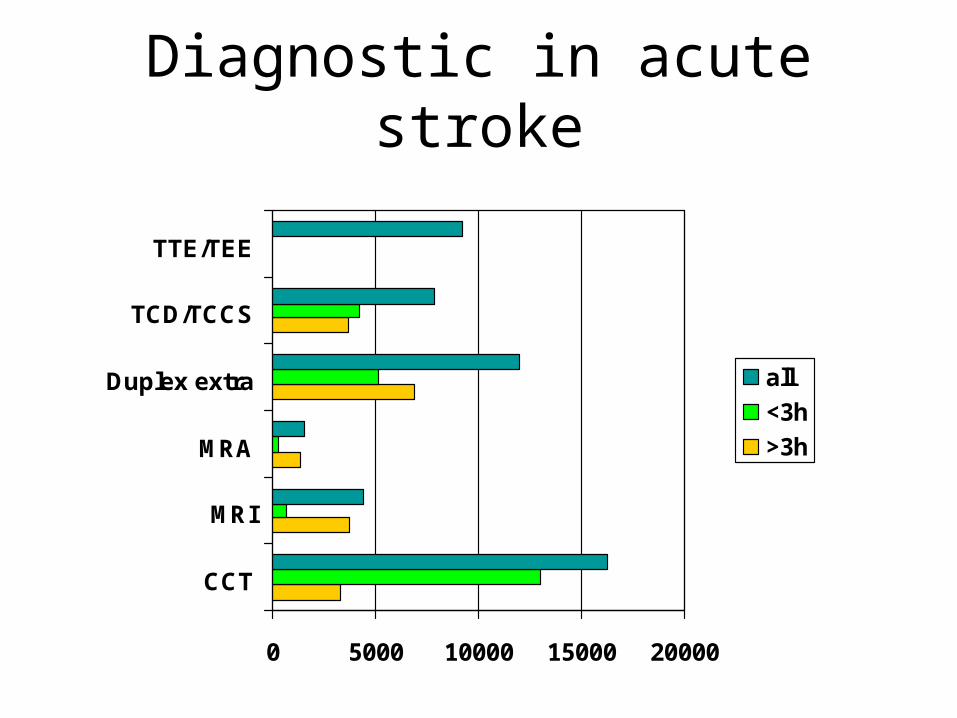
Diagnostic in acute stroke
0 5000 10000 15000 20000
CCT
MRI
MRA
Duplex extra
TCD/TCCS
TTE/TEE
all
<3h
>3h
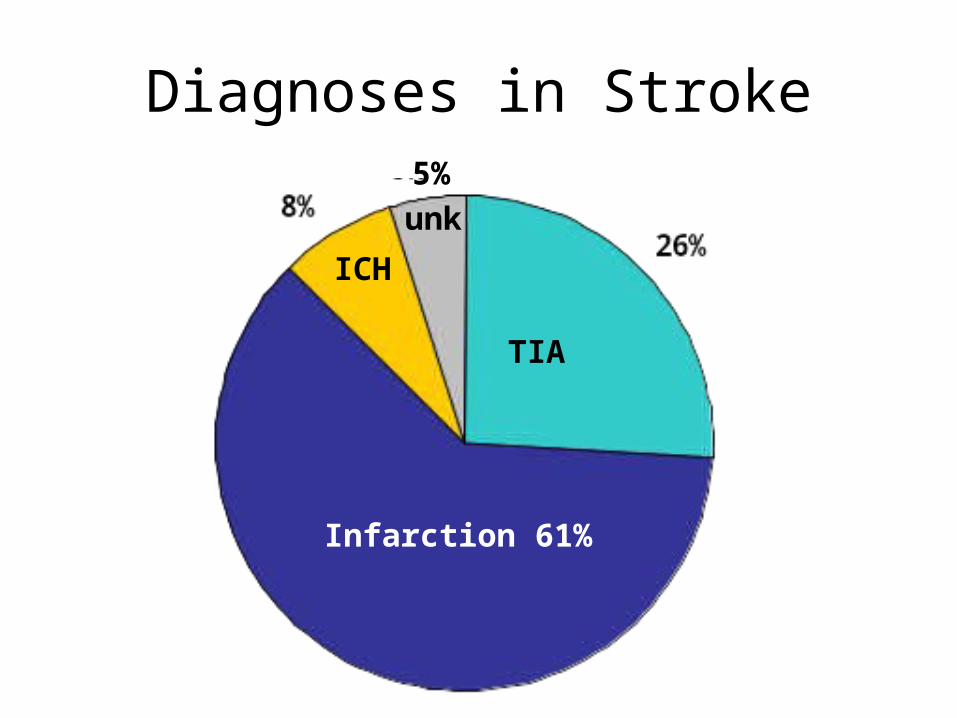
Diagnoses in Stroke
Infarction 61%
TIA
ICH
5%
unk
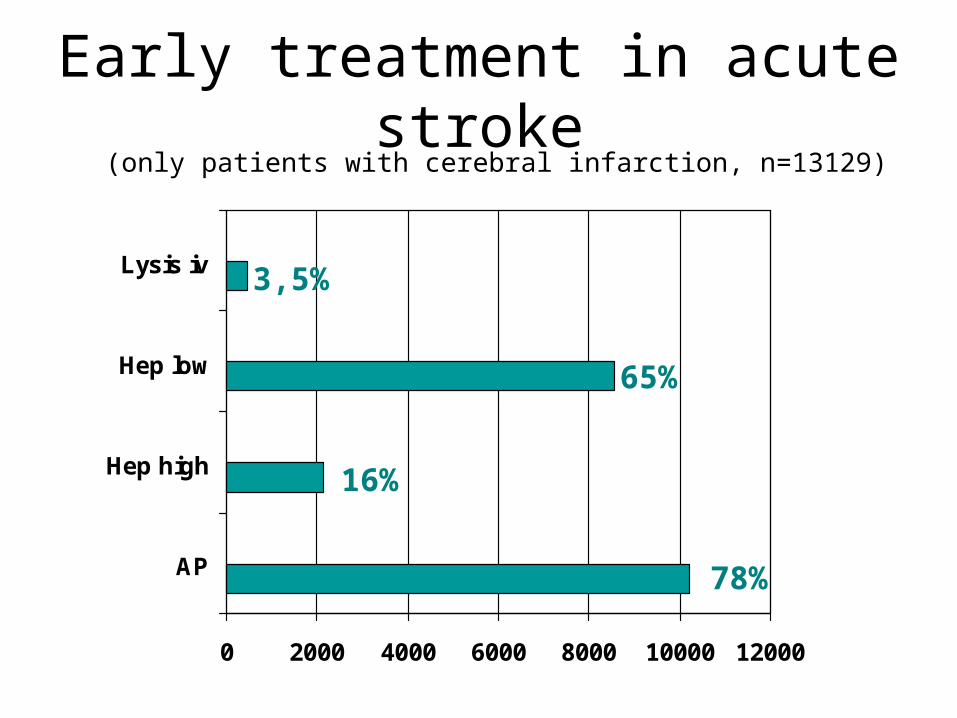
Early treatment in acute stroke
0 2000 4000 6000 8000 10000 12000
AP
Hep high
Hep low
Lysis iv
(only patients with cerebral infarction, n=13129)
78%
16%
65%
3,5%
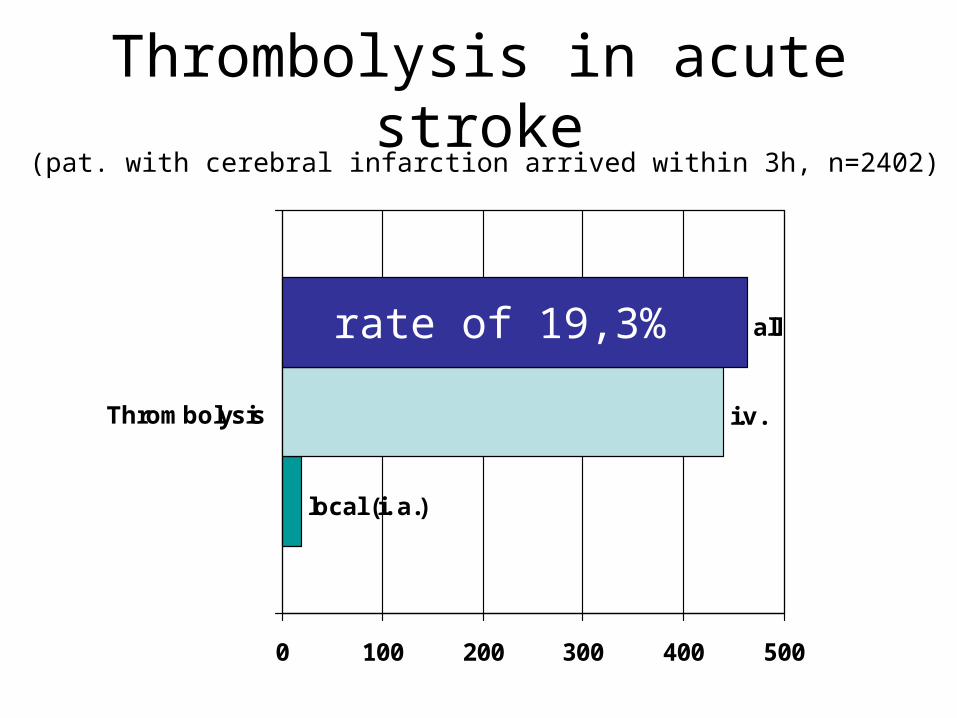
Thrombolysis in acute stroke
local (i. a.)
i.v.
all
0 100 200 300 400 500
Thrombolysis
(pat. with cerebral infarction arrived within 3h, n=2402)
rate of 19,3%
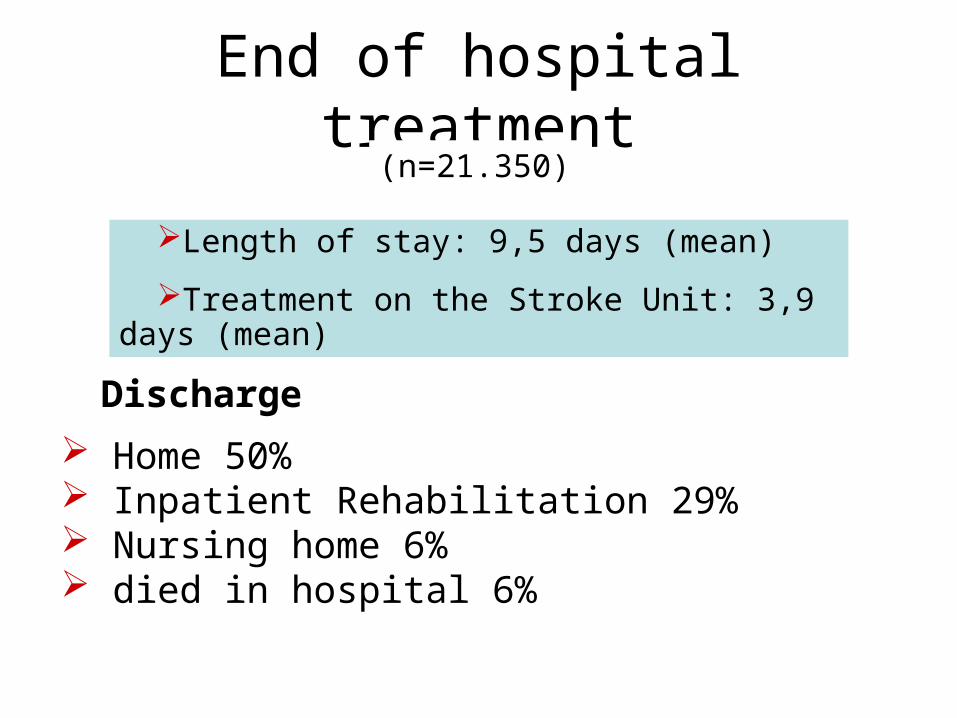
End of hospital treatment
Length of stay: 9,5 days (mean)
Treatment on the Stroke Unit: 3,9 days (mean)
(n=21.350)
Home 50% Inpatient Rehabilitation 29% Nursing home 6% died in hospital 6%
Discharge
Useful data or waste?
1. Jauss M, Allendoerfer J, Stolz E, Schutz HJ, Misselwitz B. Treatment results of stroke patients aged >80 years receiving intravenous rt-PA. Cerebrovasc Dis 2007;24(2-3):305-6.
2. Foerch C, Misselwitz B, Humpich M, Steinmetz H, Neumann-Haefelin T, Sitzer M. Sex disparity in the access of elderly patients to acute stroke care. Stroke 2007;38(7):2123-6.
3. Foerch C, Misselwitz B, Sitzer M, Berger K, Steinmetz H, Neumann-Haefelin T. Difference in recognition of right and left hemispheric stroke. Lancet 2005;366(9483):392-3.
4. Sitzer M, Foerch C, Neumann-Haefelin T, Steinmetz H, Misselwitz B, Kugler C, Back T. Transient ischaemic attack preceding anterior circulation infarction is independently associated with favourable outcome. J Neurol Neurosurg Psychiatry 2004;75(4):659-60.
5. Suenkeler IH, Nowak M, Misselwitz B, Kugler C, Schreiber W, Oertel WH, Back T. Timecourse of health-related quality of life as determined 3, 6 and 12 months after stroke. Relationship to neurological deficit, disability and depression. J Neurol 2002;249(9):1160-7.
And some more papers by the ADSR were supported by the stroke registry of Hesse (Heuschmann et. al….Stroke 2003, JAMA 2004, Arch Int Med 2004, Stroke 2006, )