Embed Size (px)
Citation preview

ACTA 0 P H T H A L M 0 L O G I CA 70 (1992) 26-32
Juvenile cataract with autosomal recessive inheritance
A study from the Aland Islands, Finland
Henrik Forsius’, Bjorn Arentz-Grastvedt* and Aldur W. Erik.ss~n’*~
Population Genetics Unit, Folkhalsan Institute of Genetics’, Helsinki, Finland, Central Hospital of Aland2, Mariehamn and
Institute of Human Genetics3. Free University Amsterdam, The Netherlands
Abstract. Juvenile (including congenital and infantile) cataract occurs commonly as part of a more generalized or systematic condition, or as a component of a syn- drome. Isolatedjuvenile cataract is a relatively rare disor- der and the mode of inheritance is often autosomal dominant. Autosomal recessive transmission of isolated juvenile cataract is rare. The present paper is a report of 15 cases of juvenile cataract on the &and Islands (Fin- land) with about 23 000 inhabitants. Twelve belong to 7 sibships of two different pedigrees and 3 cases are spo- radic, of which we have found no genealogical connec- tions in the last 6-10 generations to the two cataracta pedigrees. One of the sporadic cases presented an oper- ated cleft palate and a chromosomal anomaly. In another sporadic case the mother probably had been infected with rubella during early gestation. In the third sporadic case the cataract was combined with partial aniridia, but he has served genealogical connections to one of the cataract pedigrees. Consanguinity between the parents was detected in 5 of the 7 sibships, in some even on vari- ous ancestral levels. Apart from the cataracts, all patients were healthy, with normal intellect, behavior, hearing, growth and development. They were neurologically in- tact and there were no ocular lesions apart from cataract. In the handic familial cases the cataracts appear to be an autosomal recessive trait. A family branch originating from southwestern Sweden and south Norway showed transmission of the cataract in three successive gener- ations. The possibility of quasidominant inheritance is discussed against the background that autosomal re- cessive juvenile catarakt may not be so rare as the small number of recorded cases would suggest. The incidence in Scandinavia seems to be among the highest ever noted. At least this is true for h a n d (about 1/2000) and south Norway.
26
Key words: &and Islanders - autosomal recessive juvenile (congenital and infantile) cataract - isolate.
Both dominant and recessive autosomal inherit- ance of juvenile (including congenital and infan- tile) cataract, not combined with other anomalies has been described. In addition, rare cases of re- cessive X-chromosomal inheritance have been re- ported. Autosomal dominant inheritance, seen in many different forms of juvenile cataract, is no doubt the most common form. The fact that many sporadic cases of autosomal inheritance have been encountered in studies performed in schools for the blind or on similar long series of children, seems to indicate that a recessive mode of inherit- ance is not very rare (Fraser & Friedmann 1967; Merin et al. 1972; Tsukahara et al. 1985; Phillips et al. 1987).
Studies on single families showingjuvenile (con- genital or infantile) cataract with autosomal re- cessive inheritance and no other anomalies are shown in Table 1.
Systematic studies on a large number of spo- radic cases or on sibships with many affected mem- bers have only been reported by Saebo (1949), who has described 12 families in Telemark, a rural dis- trict in south Norway. Apart from families shown- ing other anomalies, Saebo described two families with total congenital cataract, one family with pos- terior and anterior capsular cataract and two families with nuclear cataract. All parents of those
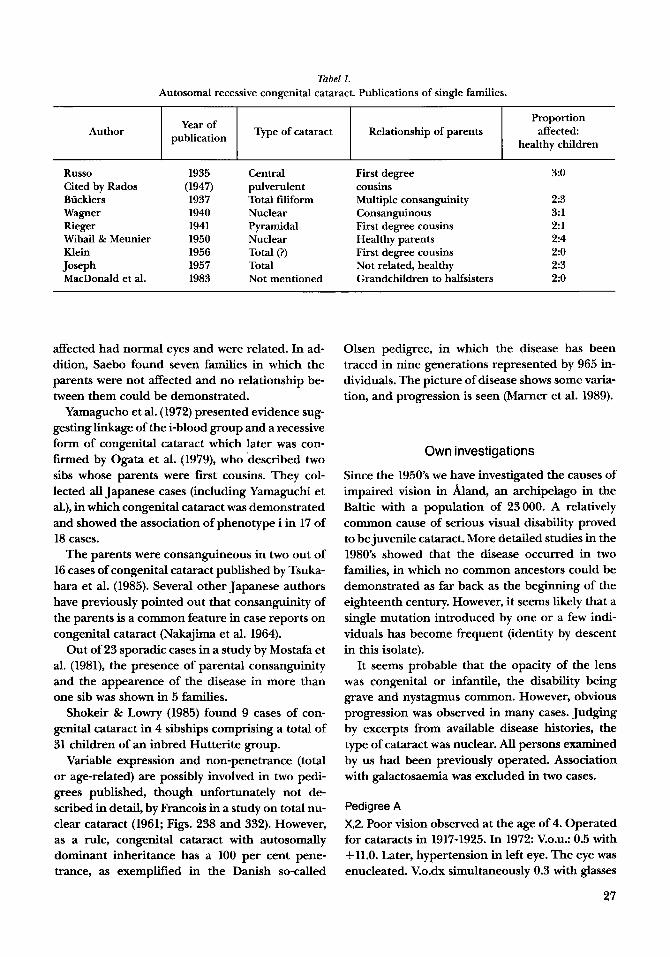
Tabel 1. Autosomal recessive congenital cataract. Publications of single families.
Author Proportion
affected healthy children
Year of publication Type of cataract Relationship of parents Author
Russo Cited by Rados Bucklers Wagner Rieger Wibail & Meunier Klein Joseph MacDonald et al.
Proportion
healthy children I Year Of I Typeofcataract Relationship of parents affected publication
1935 (1947) 1937 1940 1941 1950 1956 1957 1983
Central pulverulent Total filiform Nuclear Pyramidal Nuclear Total (?) Total Not mentioned
First degree cousins Multiple consanguinity Consanguinous First degree cousins Healthy parents First degree cousins Not related, healthy Grandchildren to halfsisters
3:O
2:3 3:l 2:l 2:4 2:o 2:3 2:o
affected had normal eyes and were related. In ad- dition, Saebo found seven families in which the parents were not affected and no relationship be- tween them could be demonstrated.
Yamagucho et al. (1972) presented evidence sug- gesting linkage of the i-blood group and a recessive form of congenital cataract which later was con- firmed by Ogata et al. (1979), who described two sibs whose parents were first cousins. They col- lected al l Japanese cases (including Yamaguchi et al.), in which congenital cataract was demonstrated and showed the association of phenotype i in 17 of 18 cases.
The parents were consanguineous in two out of 16 cases of congenital cataract published by Tsuka- hara et al. (1985). Several other Japanese authors have previously pointed out that consanguinity of the parents is a common feature in case reports on congenital cataract (Nakajima et al. 1964).
Out of 23 sporadic cases in a study by Mostafa et al. (1981), the presence of parental consanguinity and the appearence of the disease in more than one sib was shown in 5 families.
Shokeir & Lowry (1985) found 9 cases of con- genital cataract in 4 sibships comprising a total of 31 children of an inbred Hutterite group.
Variable expression and non-penetrance (total or age-related) are possibly involved in two pedi- grees published, though unfortunately not de- scribed in detail, by Francois in a study on total nu- clear cataract (1961; Figs. 238 and 332). However, as a rule, congenital cataract with autosomally dominant inheritance has a 100 per cent pene- trance, as exemplified in the Danish so-called
Olsen pedigree, in which the disease has been traced in nine generations represented by 965 in- dividuals. The picture of disease shows some varia- tion, and progression is seen (Marner et al. 1989).
Own investigations
Since the 1950's we have investigated the causes of impaired vision in &and, an archipelago in the Baltic with a population of 23000. A relatively common cause of serious visual disability proved to be juvenile cataract. More detailed studies in the 1980's showed that the disease occurred in two families, in which no common ancestors could be demonstrated as far back as the beginning of the eighteenth century. However, it seems likely that a single mutation introduced by one or a few indi- viduals has become frequent (identity by descent in this isolate).
It seems probable that the opacity of the lens was congenital or infantile, the disability being grave and nystagmus common. However, obvious progression was observed in many cases. Judging by excerpts from available disease histories, the type of cataract was nuclear. All persons examined by us had been previously operated. Association with galactosaemia was excluded in two cases.
Pedigree A X,2. Poor vision observed at the age of 4. Operated for cataracts in 1917-1925. In 1972: V.O.U.: 0.5 with +11.0. Later, hypertension in left eye. The eye was enucleated. V.o.dx simultaneously 0.3 with glasses
27
Cat
arac
ta A
land
, A
I 111
.o m
ale.
fem
ale
inve
stig
ated
b
y an
op
hth
alm
olo
gis
t
0 ju
ven
ileca
tara
ct
XI
XI1
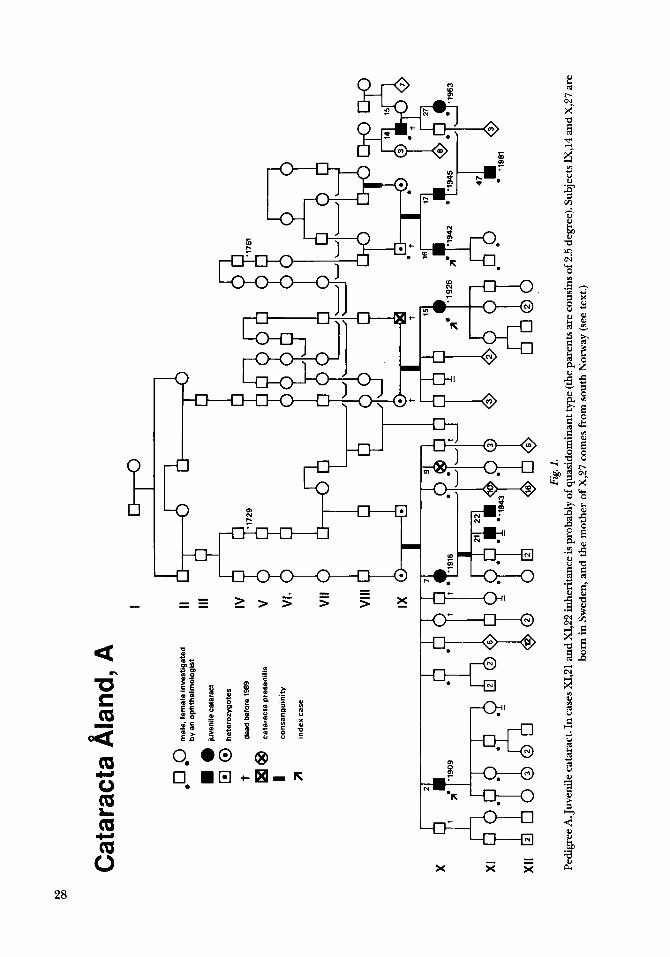
Fig
I. P
edig
ree A
. Juv
enile
cata
ract
. In
case
s XI,2
1 an
d X
I,22
inhe
rita
nce i
s pro
babl
y of
qua
sido
min
ant t
ype (
the p
aren
ts ar
e co
usin
s of 2
.5 d
egre
e). S
ubje
cts I
XJ4
and
X,2
7 ar
e bo
rn in S
wed
en, a
nd th
e m
othe
r of
X,2
7 co
mes
from
sou
th N
orw
ay (
see
text
.)
Cataracta hand, B
I
II
111
IV
V
VI
VII
Vlll
IX
X
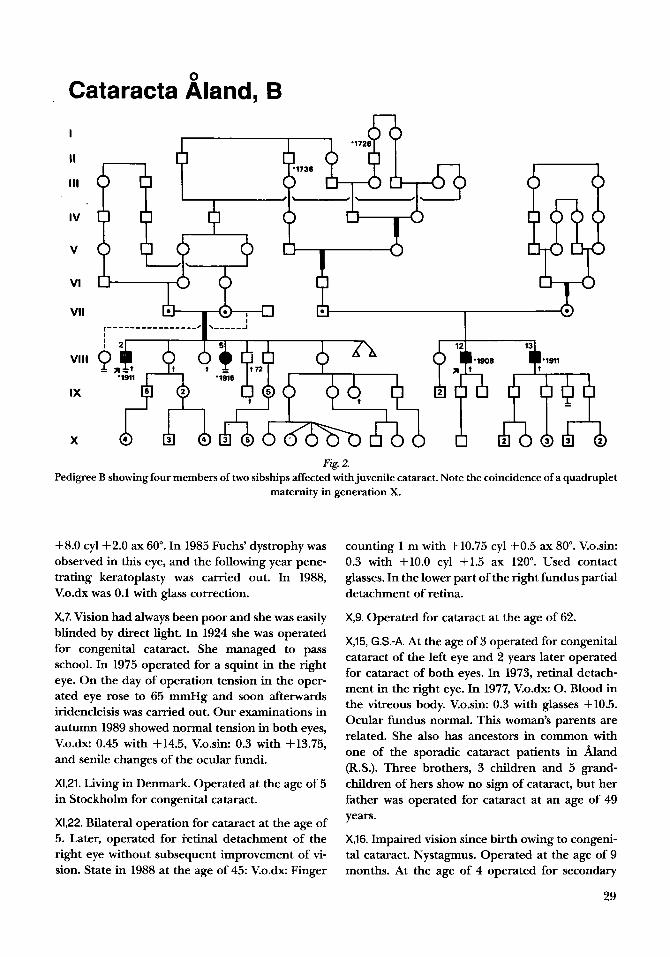
Fig. 2. Pedigree B showing four members of two sibships affected with juvenile cataract. Note the coincidence of a quadruplet
maternity in generation X.
+8.0 cyl+2.0 ax 60". In 1985 Fuchs' dystrophy was observed in this eye, and the following year pene- trating keratoplasty was carried out. In 1988, V.o.dx was 0.1 with glass correction.
X,7. Vision had always been poor and she was easily blinded by direct light. In 1924 she was operated for congenital cataract. She managed to pass school. In 1975 operated for a squint in the right eye. On the day of operation tension in the oper- ated eye rose to 65 mmHg and soon afterwards iridencleisis was carried out. Our examinations in autumn 1989 showed normal tension in both eyes, V.o.dx: 0.45 with +14.5, V.o.sin. 0.3 with +13.75, and senile changes of the ocular fundi.
X1,21. Living in Denmark. Operated at the age of 5 in Stockholm for congenital cataract.
X1,22. Bilateral operation for cataract at the age of 5. Later, operated for i-etinal detachment of the right eye without subsequent improvement of vi- sion. State in 1988 at the age of 45: V.o.dx Finger
counting 1 m with f10.75 cyl +0.5 ax 80". V.o.sin: 0.3 with +10.0 cyl +1.5 ax 120". Used contact glasses. In the lower part of the right fundus partial detachment of retina.
X,9. Operated for cataract at the age of 62.
X,15, G.S.-A. At the age of 3 operated for congenital cataract of the left eye and 2 years later operated for cataract of both eyes. In 1973, retinal detach- ment in the right eye. In 1977, V.o.dx: 0. Blood in the vitreous body. V.o.sin: 0.3 with glasses +10.5. Ocular fundus normal. This woman's parents are related. She also has ancestors in common with one of the sporadic cataract patients in &and (R.S.). Three brothers, 3 children and 5 grand- children of hers show no sign of cataract, but her father was operated for cataract at an age of 49 years.
X,16. Impaired vision since birth owing to congeni- tal cataract. Nystagmus. Operated at the age of 9 months. At the age of 4 operated for secondary
29

cataract of the left eye. Received +10.0 glasses. Fundi normal. State in 1988: V.o.dx: 0.2 with glass correction +9.0. V.o.sin: 0.3 with glass correction +10.5. Secondary glaucoma of the right eye. Ten- sion under control with miotics.
X,17. Poor vision since birth. In 1946 dense white opacities were observed posteriorly in the lenses. Discission carried out on both eyes. Received glasses +13.0. Normal fundi.
XI, 47 (son of X,17). Operated at the age of one year for bilateral cataract. The following year discission of secondary cataract was carried out. On this oc- casion slight oscillating nystagmus was observed. In 1987 refraction was +19.0 in the right eye and + 19.50 cyl - 1.0 in the left. Vision binocularly 0.2. Undulating nystagmus, normal fundi.
X,27 (married to X,17 and mother to XI,47). Cata- ract since birth. At the age of 14 months, an oper- ation for cataract was carried out on both eyes. Somewhat irregular dense cataract was present centrally, peripherally and red reflex but also fine, diffuse opacities in the lens. Nystagmus. Opacities of the lens axially just under the capsule.
IX, 14 (father of X,27). Operation for congenital cataract 1930. His wife is Norwegian and not re- lated to him. His parents are not closely related, but both come from the same region in Halland, Sweden.
Pedigree €3 V111,2. Operated for cataract several times as a child. Used cataract glasses. Vision o.u.: Finger counting 0.5 m with glasses. Has for 10 years attended a school for the blind.
V111,5. Has for 5 years attended a school for the blind. Operated seven times for congenital cata- ract. Before that, totally blind. Status in 1988: V.o.dx: Finger counting 1.5 m with + 14.0 glass cor- rection. V.o.sim Finger counting 10 cm with glass correction + 14.5. Fundi normal. Nystagmus, abun- dant secondary cataract in both eyes.
V111,12. Poor vision at school. Both eyes operated several times in 1921. In 1953 an unsuccessful oper- ation for retinal detachment of the left eye. V.o.dx Finger counting 2 m with +5.0 glasses. V.o.sin: 0. Changes of the fundi typical for malignant myopia with lange white areas where sclera is bare, choroi- dal sclerosis. Occasional pigments peripherally.
30
V111,13. The previous patient’s brother. Cataract was diagnosed in childhood. Operated at the age of 13. Further data lacking.
During our research in hand in 1988 we found, in addition to the above familial cases, three spo- radic cases of juvenile cataract:
1. R.S., male, born in 1965. Partial aniridia with a flat cornea and a wide limbal zone in both eyes. Congenital nystagmus. Central anterior cataract in the right eye. In the left eye in addition an elevated central opacity of the lens. His parents are not closely related but have several ancestral connec- tions with pedigree A. His paternal great grand- father died in 1879 at an age of 44 and was noted as blind. His mother has a translucent iris with ir- regular pupillary border. Obviously, a genetically different anomaly is involved, but it is interesting that Franceschetti and Dieterle (1959) found two cases of central pulverulent cataract and one of anterior fusiform cataract among ten children of a consanguineous marriage.
2. M.L., female born in 1980. Operated for cleft pa- late and central congenital cataract at the Univer- sity Eye Department, Helsinki. The patient has the karyotype 46,XX,t (8;18)(q2;ql). There is a de novo balanced reciprocal translocation because both parents have normal chromosomes. Breakage and reunion have occurred at the bands 8q2 and 18ql in the long arms of chromosome 2 and 18, respec- tively. A de novo translocation where both parents have normal chromosomes is usually not associ- ated whit clinical abnormality. Occasionally (<lo%), however, genes may be damaged at the breakpoints and produce chromosomal imbalance and an abnormal phenotype.
3. D.A., male born in 1981. The mother was in the second to third month of pregnancy when the sib- lings had rubella. Congenital cataract in the right eye, but no other signs of maternal rubella. The pa- tient was operated for cataract and later with epikeratoplasty at the University Eye Department, Helsinki. Vision on the right eye 0.6 with glasses -3.5 cyl +1.25 ax 125”.
Discussion
In our studies on &and we have published separ- ately papers in juvenile cataracts developing as a consequence of other ocular diseases, e.g. autoso-
mal recessive form of tapetoretinal degenerations with varying clinical features, which also have a high frequency in the hand population (Forsius & Eriksson 1964, 1970; Forsius et al. 1980). All patients in the accompanying pedigrees had
bilateral cataracts even though the advent of the cataracts, or at least their detection, was not always synchronous in both eyes. The diagnosis was, as a rule, made during the first years of life, but the many patients - particularly from the older gener- ations - were operated considerably later even if they had had bad eyesight from their infancy.
Juvenile cataract was observed on hand in 15 individuals of a population of 23000. Three of these cases were sporadic and probably do not have a genetical etiology.
The type of inheritance in the twelve familial cases in Aland could not be definitely established. Since we were able to examine the parents and off- spring of affected individuals and in most cases found that they were consanguineous, autosomal recessive inheritance is probably involved. The penetrance for autosomally dominant cataract being almost 100 per cent, we consider it likely that our two pedigrees show autosomally recessive and not irregular autosomal (dominant) inheritance. There is also an approximative 3:l ratio of normal to affected (when corrected for family size and an essentially complete ascertainment is considered).
However, we found two families with direct ver- tical inheritance. In both of them (Pedigree A) quasidominance is probable. The parents of XI,21 and XI.22 are closely related. In the second family branch the interpretation of the inheritance is more difficult. The father X,17 comes from the Aland Islands but his wife X,27 is born in Halland in southwestern Sweden, where also the affected maternal grandfather (IX,14) of XI,47 was born. M,14 is the only case known in the ascendency of X,27 with poor eye sight in youth, although he had 3 sisters, many cousins and many uncles and aunts on both the paternal and the maternal side with- out visual impairment. Moreover his parents and grandparents and their sibs had normal vision. The parents of X,27 have no common ancestors back to the middle of the 18th century, but both parents and their ancestors come from the same area. Autosomal dominant inheritance with ir- regular or low penetrance of the cataract mutation could explain why no affected subjects were found in any collateral or ancestral lines of IX,14. How-
ever, no convincing evidence of that mode af inhe- ritance of juvenile cataract has so far been re- ported. Francois (1961) published two pedigrees with two cases, where the transmission seems to have skipped one generation (non-penetrance of the cataract). Skipping of juvenile cataract in two or three generations has, however, not been re- ported. Against this background an autosomal re- cessive inheritance seems much more plausible than a dominant de novo mutation in M.14.
The wife of M,14 is born in the parish of Rael- ingen in southern Norway. Her parents and grand- parents and her 8 sibs and their 12 children had no signs of cataract. It is of interest to note that M,15 comes from the same part of south Norway from which Saebo’s patients with autosomal recessive juvenile cataract originated (Saebo 1949). There- fore, it is not quite unlikely that the mother of X,27 is a heterozygote (carrier) of the mutant cataract gene and that the cataract in three successive generations (IX,14, X,27 and XI,47) could be due to a recessive and not a dominant mutation. The similarity in clinical expression of the cataract and the resemblance of the medical histories (anam- nestic information) of the patients in both the &and and Halland families also speak in favour of autosomal recessive inheritance.
We conclude that the cataract in pedigree A with apparent vertical transmission in two and three generations is an autosomal recessive trait with quasidominant (‘pseudodominant’) inherit- ance, even if an autosomal dominant de novo mu- tation starting in M,14 cannot be definitively ex- cluded.
Acknowledgments
These studies were possible thanks to support from the Finnish Society of Sciences and Letters. Mrs. Eva Palm- gren’s suggestions and constructive criticism of the Eng- lish language contributed greatly to the readability of this paper. We are grateful to Mrs. Verna Carlsson and the staff of the Public Record Office of &and for the help with the genealogical studies.
Dedicated to our colleague of many years standing, Professor Johan Fellman, Ph.D., on the occasion of his 60th birthday.
References
Bucklers M (1937): Cataracta filiformis. 2 Augenheilk 91: 338-342.
31
Forsius H R & Eriksson A W (1964): DifFerents aspects ophtalmoscopiques de la dtgenerescence tapeto-reti- nienne chez les habitants d’un archipel. Ophthalmo- logica 147: 40-56.
Forsius H R & Eriksson A W (1970): Tapeto-retinal de- generations with varying clinical features in h a n d Is- landers. J Med Genet 7: 200-212.
Forsius H R, Eriksson A W & Damsten M (1980): Re- cessive tapetoretinal degeneration with varying diag- noses in &and. In: Eriksson A W, Forsius H, Nevan- linna H R, Workman P L & Norio R J (eds.): Population structure and genetic disorders, p 553-558. Acad Press, London.
Franceschetti A & Dieterle P (1959): Cataracte fusiforme congenitale en pagode et ses relations avec la cataracte pulverulente centrale Bulletins et MCmoires de la So- ciete Franqaise d’Ophthalmologie 72: 341-351.
Francois J (1961): Heredity in Ophtalmology, p 356. C.V. Mosby Co., St Louis.
Fraser G R & Friedmann A I (1967): The causes of blind- ness in childhood, p 57-69, 174-179. The Johns Hop- kins Press, Baltimore.
Joseph R (1957): Congenital total cataract - possibly re- cessive. Br J Ophthalmol41: 444-445.
Klein D (1956): Cataracte congenitale familiale: consan- guinite des parents. J Genet Hum 5: 283-284.
MacDonald E B, Douglas R & Harden P A (1983): A Cau- casian family with the i phenotype and congenital cataracts. Vox Sang 44.322-325.
Marner E, Rosenberg T & Eiberg H (1989): Autosomal dominant congenital cataract. Morphology and genetic mapping. Acta Ophthalmol (Copenh) 67: 151- 158.
Merin S, Lapithis A G, Horovitz D, Michaelson I C (1972): Childhood blindness in Cyprus. Am J Ophthalmol 74:
Mostafa M S E, Temtamy S, El-Gamma1 M Y, Abdel Sayed S I, Abdel-Salam M & El-Baroudy R (1981): Genetic studies of congenital cataract. Metab Pediatr Syst Oph- thalmol5: 233-242.
Nakajima A (1964): Population genetic study of blinding diseases in Japan. Proc 2nd Intern Cong Hum Genet, Rome, 1961,3: 1961.
538-542.
Ogata H, Okubo Y & Akabane T (1979): Phenotype i asso- cuated with congenital cataract in Japanese. Transfu- sion 19: 166-168.
Phillips C I, Levy A M, Newton M & Stokoe N L (1987): Blindness in schoolchildren: importance of heredity, congenital cataract, and prematurity. Br J Ophthalmol
Rados A (1947): Central pulverulent (discoid) cataract and its heredity transmission. Arch Ophthalmol 3 8 57-77.
Rieger H (1941): Erbfragen in den Augenheilkunde. Graefes Arch Clin Exp Ophthalmol. 143: 277-299.
Saebo J (1949): An investigation into the mode of heredity of congenital and juvenile cataracts. Br J
Shokeir M H K & Lowry R B (1985): Juvenile cataract in Hutterites. Am J Med Genet 22: 495-500.
Tsukahara S, Sasamoto M, Watanabe I & Phillips C I (1985): Diagnostic survey at Yamanashi school for blind: Importance of heredity. Jpn J Ophthalmol 29:
Wagner H (1940): Recessive vererbter angeborener Star. Klin Monatsbl Augenheilkd 104 337-338.
Wibail R & Meunier A (1950): Cataracte congenitale hereditaire du noyau embryonnaire. Bull SOC Belge Ophthalmol95: 339-345.
Yamaguchi H, Okubo Y & Tanaka M (1972): A note on possible close linkage between the Ii blood locus and a congenital cataract locus. Proc Jpn Acad 48: 625-628.
71: 578-584.
Ophthalmol33: 601-629.
315-321.
Received on April llth, 1991.
Author’s address: Prof. Henrik R. Forsius, MD, Folkhalsan Institute of Genetics, Topeliusgatan 20, SF-00250 Helsingfors, Finland.
32















![Autosomal recessive ichthyosis with limb reduction defect ... · including autosomal dominant, autosomal recessive and X-linked inheritance [1,2]. Associated cutaneous and extracutaneous](https://img.pdfslide.net/doc/110x75/5ec8c9b91adfdf12ab3e663c/autosomal-recessive-ichthyosis-with-limb-reduction-defect-including-autosomal.jpg)













