-
Kardio & Metabolic Update
Kardiovaskuläres Risiko bei DiabetikernKathrin Hauser
FMH Endokrinologie, Diabetologie
12.12.2019
-
AgendaTeil 1 – DM: die Prognose verbessern
• Zahlen und Entwicklung Schweiz
• Einzelne Risikofaktoren und ihre Relevanz
• We could do better – we must do better!
• Teil 2 – Moderne Therapie: auf Herz und Niere geprüft
• ESC-Guidelines
• … und die Evidenz dazu
-
Teil 1
Die Prognose verbessern
-
Situation Schweiz – Personen mit Diabetes
-
Situation Schweiz – Personen mit zu hohem Cholesterin
-
Situation Schweiz – Personen mit Hypertonie
-
Übergewicht / Adipositas Kanton Thurgau
-
• Kohorte Schweden ~6 Jahre
• 270’000 Patienten mit DM2 vs 1’350’000
Kontrollen
• 5 kvRF: HbA1c, Albuminurie, LDL, Nikotin, BD
➢Risikofaktoren im Ziel: Effekt auf Tod und
Myokardinfarkt
Rawshani A et al, N Engl J Med 2018; Aug 16
-
… die Prognose verbessern!
-
… die Prognose verbessern!
-
Die Situation heute…
-
Multifaktorielle Behandlung bei DM
American Diabetes Association. Stark Casagrande S, et al.
Diabetes Care 2013;36:2271–2279.
-
we must do better!
• Blutdruck ~130/80mmHg
• Statin (the lower the better!)
• HbA1c
-
we must do better!
• Blutdruck ~130/80mmHg
• Statin (the lower the better!)
• HbA1c
-
Teil 2
ESC-Guidelines 2019:
moderne Therapie des DM2Auf Herz und Niere geprüft
-
SGED – Empfehlungen 2016Empfehlungen 2020: coming soon
-
ESC-/EASD-Guidelines 2019Diabetes-Therapie
1. Metformin
2. + GLP1- oder SGLT2-Hemmer
3. + SGLT2- oder GLP1-Hemmer (very high risk)
4. + …
-
ESC-/EASD-Guidelines 2019Cholesterin
-
ESC-/EASD-Guidelines 2019Cholesterin
-
ESC-/EASD-Guidelines 2019Cholesterin
-
ESC-/EASD-Guidelines 2019Blutdruck
-
ESC-/EASD-Guidelines 2019Blutdruck
-
Fallbeispiel 1
62-jähriger Patient
• DM2 seit 8 Jahren
• aHT seit 8 Jahren, EF 62%
• St.n. Non-STEMI 2018
• cvRF: DM, aHT, Dyslipidämie, Adipositas (BMI 32)
Medikation:
• Janumet 50/1000 1-0-1
• Gliclazid MR 60 1-0-0
• Pravastatin 40mg 1-0-0
• ASS 100 1-0-0
• Exforge HCT 1-0-0
Labor:
• HbA1c 7.2%
• LDL 2.6mmol/l
• eGFR 65ml/min
• ACR 2.4mg/mmol
-
Fallbeispiel 1
62-jähriger Patient
• DM2 seit 8 Jahren
• aHT seit 8 Jahren
• St.n. Non-STEMI 2018
• cvRF: DM, aHT, Dyslipidämie, Adipositas (BMI 32)
Medikation:
• Janumet 50/1000 1-0-1
• Gliclazid MR 60 1-0-0
• Pravastatin 40mg 1-0-0
• ASS 100 1-0-0
• Exforge HCT 1-0-0
Labor:
• HbA1c 7.2%
• LDL 2.6mmol/l
• eGFR 65ml/min
• ACR 2.4mg/mmol
-
Fallbeispiel 1
□ Therapie unverändert weiter
□ Pravastatin abends
□ Rosuvastatin 20mg statt Pravastatin
□ Austausch von Janumet durch GLP1-Analogon und Metformin
□ Austausch von Janumet durch GLP1-Analogon und Metformin,
Weglassen von Gliclazid
□ Austausch von Gliclazid durch SGLT2-Hemmer
-
Fallbeispiel 1
□ Therapie unverändert weiter
□ Pravastatin abends
□ Rosuvastatin 20mg statt Pravastatin
□ Austausch von Janumet durch GLP1-Analogon und Metformin
□ Austausch von Janumet durch GLP1-Analogon undMetformin,
Weglassen von Gliclazid
□ Austausch von Gliclazid durch SGLT2-Hemmer
-
Publizierte cv Outcome-Studien DM2-MedikamenteStand 01/19
Hazard Ratios vs. Placebo und 95% Konfidenzintervalle
-
Publizierte cv Outcome-Studien DM2-MedikamenteStand 01/19
Hazard Ratios vs. Placebo und 95% Konfidenzintervalle
-
GLP1-Analoga - cvRF
HbA1c
kg
BD
HbA1c
kg
BD
-
GLP1-Analoga - cvRF
HbA1c
kg
BD
HbA1c
kg
BD
-
GLP1-Analoga – cv Outcome
Sustain 6
3297 Patienten mit DM2
• HbA1c ≥7.0%
• Mit 0-2 OAD, ± Basal- oderMischinsulin
• ≥ 50 Jahre mit CVD (KHK, CVI, PAVK, NYHA II–III), oder CKD
Stadium ≥ 3
• oder Alter ≥60 Jahre mit ≥ 1 cvRF
Leader
9340 Patienten mit DM2
• HbA1c ≥7.0%
• Mit/ohne OAD, ± Basal- oderMischinsulin
• ≥50 Jahre mit CVD oder CKD
• oder Alter ≥60 Jahre mit ≥ 1 cvRF
Marso SP et al. N Engl J Med 2016;375:1834–44 Marso SP et al. N
Engl J Med 2016; 375:311-322
-
GLP1-Analoga – cv Outcome
Sustain 6
• Alter 65 Jahre, DM-Dauer 14 Jahre
• HbA1c 8.7%
• Gewicht 92 kg
• BD 135/77mmHg
• LDL 2.1mmol/l
• Männeranteil: 60%
Leader
• Alter 64 Jahre, DM-Dauer 13 Jahre
• HbA1c 8.7%
• Gewicht 92 kg (BMI 32kg/m2 )
• BD 135/77 mmHg
• LDL ???
• Männeranteil: 64%
Marso SP et al. N Engl J Med 2016;375:1834–44 Marso SP et al. N
Engl J Med 2016; 375:311-322
-
0
1
2
3
4
5
6
7
8
9
10
0 10 20 30 40 50 60 70 80 90 100 110
Sub
ject
s w
ith
an
eve
nt
(%)
Kaplan–Meier plot for first event adjudication
committee-confirmed MACE (CV death, non-fatal MI and non-fatal
stroke) using ‘in-trial’ data from subjects in the full analysis
set
HR: 0.74 [95% CI: 0.58;0.95]Events: 108 semaglutide; 146
placebop
-
nicht tödlicher MI/CVI, cv Tod
0
1
2
3
4
5
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Week
Patients
with e
vent
(%) CV death
HR: 0.98 (95% CI: 0.65;1.48)
p=0.92
0
1
2
3
4
5
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Patients
with e
vent
(%)
Non-fatal MI
Week
HR: 0.74 (95% CI: 0.51;1.08)
p=0.12
Semaglutide
Placebo
0
1
2
3
4
5
0 8 16 24 32 40 48 56 64 72 80 88 96 104
Week
Non-fatal stroke
Patients
with e
vent
(%)
HR: 0.61 (95% CI: 0.38;0.99)
p=0.04
Marso SP et al. N Engl J Med 2016;375:1834–44
-
Lancet Diabetes Endocrinol 2019;7:776-785
-
Lancet Diabetes Endocrinol 2019;7:776-785
3-Punkte MACE
cv Tod
cv Outcome
-
cv Outcome
Myokardinfarkt
Stroke
Lancet Diabetes Endocrinol 2019;7:776-785
-
Herzinsuffizienz, Niereninsuffizienz
Lancet Diabetes Endocrinol 2019;7:776-785
Hosp. für Herzinsuffizienz
Composite Niere
Verschlechterung GFR
-
Fallbeispiel 1
Optimale Therapie
✓ Rosuvastatin (plus Ezetimibe) statt Pravastatin
✓ GLP1-Analogon + Metformin
-
Fallbeispiel 2
78-jährige Patientin
• DM2 seit 12 Jahren
• Chron. Niereninsuffizienz Stadium 3a
• Hypertensive Herzkrankheit, EF 43%• Rezid. Hosp. wegen
kardialer Dekompensation
• cvRF: DM, aHT, Dyslipidämie, Albuminurie, Übergewicht (BMI
29)
Medikation:
• Jentadueto 2.5/1000 1-0-1
• Co-Valsartan 160/25 1-0-0
• Torasemid 10mg 1-0-0
• Atorvastatin 40mg 1-0-0
• Amlodipin 5mg 0-0-1
Labor:
• HbA1c 6.9%
• LDL 2.4mmol/l
• eGFR 48ml/min
• ACR 4.2mg/mmol
-
Fallbeispiel 2
78-jährige Patientin
• DM2 seit 12 Jahren
• Chron. Niereninsuffizienz Stadium 3a
• Hypertensive Herzkrankheit, EF 43%• Rezid. Hosp. wegen
kardialer Dekompensation
• cvRF: DM, aHT, Dyslipidämie, Albuminurie, Übergewicht (BMI
29)
Medikation:
• Jentadueto 2.5/1000 1-0-1
• Co-Valsartan 160/25 1-0-0
• Torasemid 10mg 1-0-0
• Atorvastatin 40mg 1-0-0
• Amlodipin 5mg 0-0-1
Labor:
• HbA1c 6.9%
• LDL 2.4mmol/l
• eGFR 48ml/min
• ACR 4.2mg/mmol
-
Fallbeispiel 2
□ Therapie unverändert weiter
□ Sistieren / Dosisreduktion von Metformin
□ Austausch von Jentadueto durch Metformin und GLP1-Analogon
□ Austausch von Jentadueto durch Metformin und SGLT2-Hemmer
-
Fallbeispiel 2
□ Therapie unverändert weiter
□ Sistieren / Dosisreduktion von Metformin
□ Austausch von Jentadueto durch Metformin und GLP1-Analogon
□ Austausch von Jentadueto durch Metformin und SGLT2-Hemmer
-
Publizierte cv Outcome-Studien DM2-MedikamenteStand 01/19
Hazard Ratios vs. Placebo und 95% Konfidenzintervalle
-
SGLT2-Hemmer - cvRF
HbA1c
kg
BD
Qiu, R., Balis, D., Capuano, G. et al. Diabetes Ther (2016) 7:
659-678
-
EMPA REG – cv Outcome
7020 Pat. mit DM2 & cv Erkrankung
Placebo vs. Empa 10mg vs. Empa 25mg
• HbA1c 7.1-9.0% mit stabiler DM-Tx
• BMI 10a
• HbA1c 8.0%
• BMI 30.5 kg/m2
• BD 135/76mmHg
• LDL 2.2mmol/l
• Albuminurie 40%
• Männeranteil: 72%
N Engl J Med 2015;373:2117-28.
-
EMPA REG – cv Outcome
N Engl J Med 2015;373:2117-28.
3-Punkte MACE
-
EMPA REG – cv Outcome
N Engl J Med 2015;373:2117-28.
-
EMPA REG – cv Outcome
N Engl J Med 2015;373:2117-28.
-
EMPA REG – cv Outcome
N Engl J Med 2015;373:2117-28.
-
SGLT2-Hemmer cv Outcome-Studien
Zelniker T. et al;Lancet 2019; 393: 31–39
-
Zelniker T. et al;Lancet 2019; 393: 31–39
mit ASCVD
Multiple RF
3-Punkte MACE
-
Zelniker T. et al;Lancet 2019; 393: 31–39
mit ASCVD
Multiple RF
Hosp. wegen HF und cv Tod
-
Zelniker T. et al;Lancet 2019; 393: 31–39
mit bekannter HF
ohne bekannte HF
Hosp. wegen HF und cv Tod
-
SGTL2-Hemmer und die Niere
Lancet Diabetes Endocrinol 2019; 7: 845–54
-
Fallbeispiel 2
□ Therapie unverändert weiter
□ Sistieren / Dosisreduktion von Metformin
□ Austausch von Jentadueto durch Metformin und GLP1-Analogon
□ Austausch von Jentadueto durch Metformin und SGLT2-Hemmer
-
Also was nun wann?!?
Zelniker TA et al. Online ahead of print. Circulation. 2019.
-
Fragen soweit?
-
SGLT2 Inhibitoren in der Prävention von Herzinsuffizienz bei
Diabetikern und nicht-
Diabetikern
-
DAPA-HF: Studien-Design
-
© AstraZeneca 2019
Dapagliflozin bei Patienten mit chronischer HFrEF mit oder ohne
T2D1-4
63
CV = cardiovascular; eGFR = estimated glomerular filtration
rate; ESRD = end stage renal disease; HbA1c = glycated hemoglobin;
HF = heart failure; HFrEF = heart failure with reduced ejection
fraction; hHF = hospitalization for heart failure; KCCQ = Kansas
City Cardiomyopathy Questionnaire; LVEF = left ventricular ejection
fraction; NT-proBNP = N-terminal pro B-type natriuretic peptide;
NYHA = New York Heart Association; SoC = standard of care; T2D =
type 2 diabetes.1. McMurray JJV et al. Article and supplementary
appendix. Eur J Heart Fail. 2019;21:665-675. 2. McMurray JJV et al.
N Engl J Med. 2019. https://doi.org/10.1056/NEJMoa1911303. Accessed
September 19, 2019. 3. Study NCT03036124. ClinicalTrials.gov
website. Accessed August 19, 2019. 4. McMurray JJV et al. Eur J
Heart Fail. 2019;doi: 10.1002/ejhf.1548. Accessed July 16,
2019.
Target primary endpoint events:
8441
Median follow-up: 18.2 months2
Completion: July 20193
Placebo + standard of care
Dapagliflozin 10 mg + standard of care
1:1 D
ou
ble
-blin
d
4744 patients
• ≥18 years of age
• With or without T2D
• Diagnosis of symptomatic HFrEF (NYHA class II-IV) for ≥ 2
months
• LVEF ≤40% within last 12 months
• Elevated NT-proBNP
• eGFR ≥30 ml/min/1.73 m2
• Stable SoC HFrEF treatment
Visit 1
(enrollment)
Day -14
Visit 2 (randomization)
Day 0Visit 6, etc.
Every 120 days
Visit 5
Day 120
Visit 3
Day 14Visit 4
Day 60
Secondary Endpoints
• Time to first occurrence of either of the components of the
composite: CV death or hHF
• Total number of (first and recurrent) hHF and CV death• Change
from baseline measured at 8 months in the total symptom score of
the
KCCQ• Time to first occurrence of any of the components of the
composite: ≥50%
sustained decline in eGFR or reaching ESRD or renal death• Time
to death from any cause
Primary Endpoint
• Time to first occurrence of any of the
components of the composite: CV death or
hHF or an urgent HF visit
-
© AstraZeneca 2019
Einschluss und AusschlusskriterienKey Inclusion Criteria Key
Exclusion Criteria
64
aThis does not apply to diuretics; diuretic dosing may be
titrated to symptoms, signs, weight and other information and may
thus vary. Each patient should, however, be treated with a diuretic
regimen aimed at achieving optimal fluid/volume status for that
individual; bCKD-EPI formula.ACEI = angiotensin-converting enzyme
inhibitor; ARB = angiotensin-receptor blocker; CABG = coronary
artery bypass grafting; CKD-EPI = Chronic Kidney
Disease-Epidemiology Collaboration; eGFR = estimated glomerular
filtration rate; HF = heart failure; HFrEF = heart failure with
reduced ejection fraction; hHF = hospitalization for heart failure;
LVEF = left ventricular ejection fraction; MRA =
mineralocorticoid-receptor antagonist; NT-proBNP = N-terminal pro
B-type natriuretic peptide; NYHA = New York Heart Association; PCI
= percutaneous coronary intervention; SBP = systolic blood
pressure; T1D = type 1 diabetes;T2D = type 2 diabetes.1. McMurray
JJV et al. Article and supplementary appendix. Eur J Heart Fail.
2019;21:665-675.
• Men and women ≥18 years of age, with or without T2D
• Documented diagnosis of symptomatic HFrEF for ≥2 months (NYHA
class II-IV)
• LVEF ≤40% within the last 12 months
• Elevated NT-proBNP (≥600 pg/mL or ≥400 pg/mL if hHF within 12
months or ≥900 pg/mL if atrial fibrillation/flutter irrespective of
hHF history)
• Optimal pharmacological and device therapy for HF
• Optimal and stablea (≥4 weeks) background standard of care for
HFrEF as per local guidelines including (unless contraindicated or
not tolerated): ACEI, ARB, or sacubitril/valsartan; beta-blocker;
and if appropriate a MRA
• eGFRb ≥30 mL/min/1.73 m2
• Treatment within 8 weeks or intolerance to SGLT2 inhibitor
• T1D
• Symptomatic hypotension or SBP
-
© AstraZeneca 2019
Primärer Endpunkt: CV Tod / hHF / dringliche HF Visite1,2
65
DAPA = dapagliflozin; HF = heart failure; hHF = hospitalization
for heart failure; HR = hazard ratio; NNT = number needed to treat;
RRR = relative risk reduction
1. McMurray JJV et al. N Engl J Med. 2019.
https://doi.org/10.1056/NEJMoa1911303. Accessed September 19, 2019.
2. McMurray J. Presentation at: European Society of Cardiology
Congress. September 1, 2019; Paris, France.
2105931096147819172075216322582371Placebo
2106121146156020022147222123052373DAPA
32
28
24
20
16
12
8
4
0
242115 18129630No. at Risk Months from Randomization
Cu
mu
lati
ve P
erc
en
tag
e (
%)
36
HR 0.74 (0.65, 0.85)
p=0.00001
NNT = 21
DAPA
Placebo
26%
RRR
-
© AstraZeneca 2019
Komponenten des primären Endpunktes1,2
*Defined as unplanned hospitalization for HF or urgent HF visit
requiring intravenous therapy
CV = cardiovascular; DAPA = Dapagliflozin; HF = Heart failure;
HR = Hazard ratio; RRR = relative risk reduction.
1. McMurray JJV et al. N Engl J Med. 2019.
https://doi.org/10.1056/NEJMoa1911303. Accessed September 19, 2019.
2. McMurray J. Presentation at: European Society of Cardiology
Congress. September 1, 2019; Paris, France.
66
2105931096147819172075216322582371Placebo
2106121146156020022147222123052373DAPA
No. at Risk
Months from Randomization
20
15
10
5
0
242115 18129630
Cu
mu
lati
ve
Pe
rce
nta
ge
(%
)
DAPA
PlaceboHR 0.70 (0.59, 0.83)
p=0.00003
30% RRR
13.7%
10.0%
20
15
10
5
0
242115 18129630
Cu
mu
lati
ve
Pe
rce
nta
ge
(%
)
DAPA
Placebo
2346641219163620912230227923302371Placebo
2326711242166421272248229323392373DAPA
No. at Risk
Months from Randomization
HR 0.82 (0.69, 0.98)
p=0.029
18% RRR
11.5%
9.6%
Worsening HF Event* CV Death
-
© AstraZeneca 2019
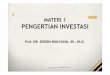
Hospitalisation wegen Herzinsuffizienz (hHF)1,2
6
7
1. McMurray JJV et al. N Engl J Med. 2019.
https://doi.org/10.1056/NEJMoa1911303. Accessed September 19, 2019.
2. In House Data, AstraZeneca Pharmaceuticals LP. CSP
D1699C00001.
DAPA 10 mg
Placebo
2125961101148319242082216822642371Placebo
2106131147156320072153222323062373DAPA 10 mg
No. at Risk Months from Randomization
20
15
10
5
0
242115 18129630
Cu
mu
lati
ve
Pe
rce
nta
ge
(%
)
25
30
HR 0.70 (0.59, 0.83)
p
-
© AstraZeneca 2019
Sekundärer Endpunkt: Gesamtmortalität1,2
6
8* Nominal p-value.
DAPA = Dapagliflozin; HR = Hazard ratio.
1. McMurray JJV et al. N Engl J Med. 2019.
https://doi.org/10.1056/NEJMoa1911303. Accessed September 19,
2019.. 2. McMurray J. Presentation at: European Society of
Cardiology Congress. September 1, 2019; Paris, France.
24
20
16
12
8
4
0
242115 18129630
Cu
mu
lati
ve P
erc
en
tag
e (
%)
DAPA
Placebo
2356651221163820922231227923302371Placebo
2336721243166621302251229623422373DAPA
No. at Risk Months from Randomization
HR 0.83 (0.71, 0.97)
p=0.022*
17%
RRR
-
Take Home
• Orale Antidiabetika sind neu Herzmedikamente
• Bei koronarer Herzkrankheit
• Bei Herzinsuffizienz
• … SGLT2-Hemmer auch Nierenmedikamente (Anmerkung der
Diabetologin)
• Weitere Anpassung der Guidelines unterwegs
-
Fragen?
-
Übergewicht und Adipositas in der Schweiz
Quelle: Bundesamt für Gesundheit BAG
Anteil der weiblichen und männlichen Personen mit Übergewicht
oder Adipositas nach Altersgruppe (2012)
15-24 25-49 50-64 65+ 15-24 25-49 50-64 65+
17% 28% 40% 48% 33% 54% 62% 60%
-
Herzinsuffizienz und Diabetes
Rawshani A et al, N Engl J Med 2018; Aug 16
Risiko für ein Ereignis bei Patienten mit DM2 und keinem RF
ausserhalb des
Zielbereichs verglichen mit Patienten ohne DM
0 0.5 1 1.5 2
Death
MI
hHF
Stroke
HR (95% CI)
1.06 (1.00, 1.12)
0.84 (0.75, 0.93)
0.95 (0.84, 1.07)
1.45 (1.34, 1.57)
-
Herzinsuffizienz und Diabetes
16.2%
14.1%
11.5%
5.1%4.2%
% E
reig
nis
als
cv E
rste
reig
nis
PAVK HF (ohne MI) non-fatal MI CVI cv Tod
Kohortenstudie mit ~1.9 Mio DM2-Patienten und Inzidenz von
kardiovaskulären Erkrankungen 1
Eine häufige Kombination 2
DM2-Studien: HF-Prävalenz 10-30%
HF-Studien: DM2-Prävalenz ~30%
1. Shah AD et al. Article and appendix. Lancet Diabetes
Endocrinol. 2015;3:105-113; 2. Seferović PM et al. Eur J Heart
Fail. 2018;20:853-872.
-
Herzinsuffizienz und Diabetes
➢28% der DM2-Patienten hatten nicht diagnostizierteHF
➢Signifikant höhere Inzidenzvon undiagnostizierter HF bei
folgenden Aspekten:
• Zunehmendes Alter
• WeiblichesGeschlecht
• BMI ≥30 kg/m2
• Dyspnoe
• Müdigkeit
• Bekannte aHT
No Heart Failure, 72%
Heart Failure (HFrEF), 5%
Heart Failure (HFpEF), 23%
Boonman-de Winter LJ, et al High prevalence of previously
unknown heart failure and left ventricular dysfunction in patients
with type 2 diabetes. Diabetologia 2012;55:2154–2162