Embed Size (px)
Citation preview

Show Me the Value of
Health Information Exchange (HIE)
Karen E. Edison, M.D.Chair, Department of DermatologyDirector, Center for Health Policy
University of Missouri Health System

Evolution ?
Natural Selection never saw this coming!

Objectives
Understand the federal HITECH Act and how it impacts Missouri
Recognize the role of the Missouri Health Information Organization (HIO) in facilitating the electronic exchange of health information
Identify ways to impact the development of the statewide health information organization

The Health Information Technology for Economic & Clinical Health Act (HITECH Act)
HITECH Act 2009 ($20B) part of the American Recovery and Reinvestment Act (ARRA)
▪ “The Stimulus Bill - $787B”
Goal: Improve the health of Americans and the performance
of their health care system by encouraging health care providers to leverage health IT tools to achieve quality and efficiency goals
▪ David Blumenthal, “Launching HITECH”, New England Journal of Medicine, December 30, 2009

History repeats itself!
• In 1901, there were 2,000,000 phone users in the US
• Cumulative public and private investment was $500M, or $13B in 2009 dollars (about $6500 per user)
• Networks were operated by:
AT&T: ~1.3m
Independent networks: ~700k
• Number of independent networks: 2,811

HITECH Act: Federal Legislative Intent & Goals
Establish HIT and HIE as the cornerstone and primary tool driving health care reform
Adopt and deploy certified EHRs
Develop infrastructure to exchange health information safely, securely and efficiently
Level the playing field for all states to finance and expand states’ roles in EHR adoption and HIE development

What did HITECH fund?
Incentives for providers to adopt – Medicare & Medicaid
Grants to States – Health Information Exchange (Missouri HIO)
Regional Extension Centers to help providers (Missouri HIT Assistance Center)
Workforce development – HIT expertise Research and Development

What the HITECH Act Means for Missouri
Program National Missouri
Statewide HIE56 awards
(states & SDEs) Department of Social Services – $13.8 M
Regional Extension Center 60 awards University of Missouri – $6.8 M
Workforce 45 awards
Full Employment Council (KC) – $5 M Crowder College (Neosho) – $3.6 M Marysville University (St. Louis) – $4.7 M
Health Center Networks 45 awards St. Louis Integrated Health Network – $1 M Missouri Primary Care Association – $1 M
Medicaid NA MO HealthNet – $1.7 M
Broadband NA To Private Organizations – $275 M
Total Funding to Date - More Than $300 M8

Missouri State Goals
1. Improve the quality of medical decision-making and the coordination of care
2. Provide accountability in safeguarding the privacy and security of medical information
3. Reduce preventable medical errors and avoid duplication of treatment
4. Improve the public health
5. Enhance the affordability and value of health care
6. Empower Missourians to take a more active role in their own health care
10
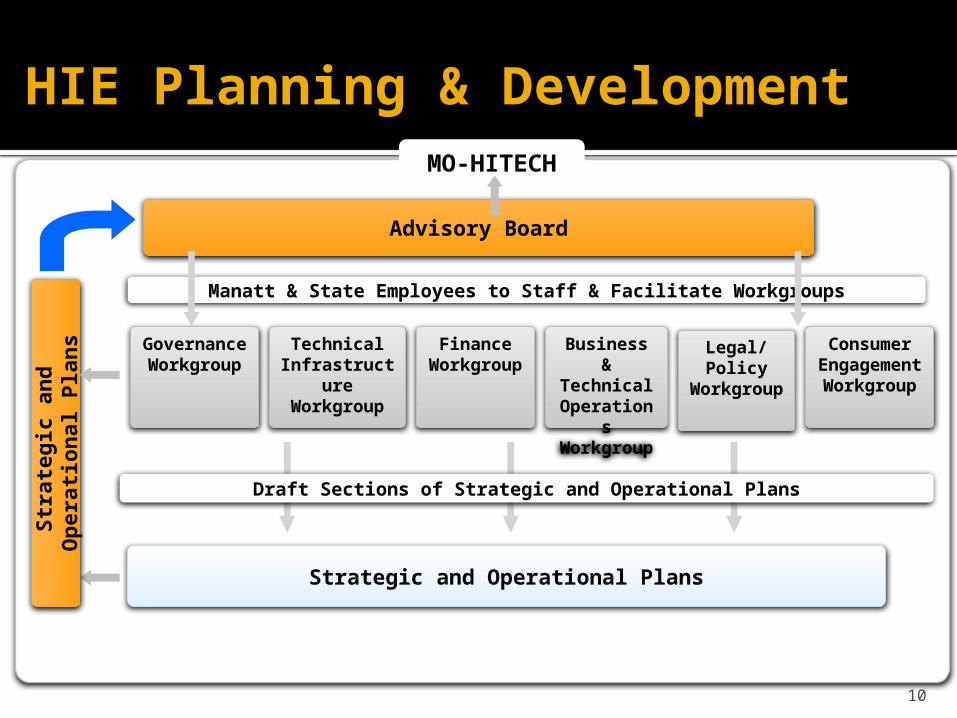
MO-HITECH
Advisory Board
Governance
Workgroup
Technical Infrastruct
ure Workgroup
Finance Workgrou
p
Business &
Technical Operation
s Workgrou
p
Consumer Engageme
nt Workgrou
p
Legal/ Policy
Workgroup
Manatt & State Employees to Staff & Facilitate Workgroups
Strategic and Operational Plans
Draft Sections of Strategic and Operational Plans
Str
ate
gic
an
d
Op
era
tion
al P
lan
sHIE Planning & Development

Missouri has elected to be an “Opt In” state

Missouri’s Action Plan and Deliverables
12
6 Coordinated Planning Tracks
Establish governance and decision-making process
Develop privacy and security plan
Develop technology plan
Develop financing plan
Develop EHR adoption plan
Develop consumer engagement plan
3 Key Deliverables State HIE Plan
Strategic Operational
State Medicaid Plan Regional Extension
Center EHR adoption plan
Health IT is the enabler, not the result

There will be no health information exchange without involving the physicians……

What is the Value of Health Information (HI) Exchange?

Benefits for Providers
• Quick access to patient records from inpatient and remote locations for more coordinated, efficient care
• Enhanced decision support, clinical alerts, reminders, and medical information
• Performance-improving tools, real-time quality reporting
• Legible, complete documentation that facilitates accurate coding and billing
• Interfaces with labs, registries, other EHRs and HIEs
• Safer, more reliable prescribing 15

Benefits for Patients
• Reduced need to fill out the same forms at each office visit
• Reliable point-of-care information and reminders notifying providers of important health interventions
• Convenience of e-prescriptions electronically sent to the pharmacy
• Patient portals for online interaction with providers
• Electronic referrals allow for easier access to follow-up care with specialists

Providers Report Positive Influence of EHRs on their Practices
17DesRoches, C., et al, “Electronic Health Records in Ambulatory Care - A National Survey of Physicians” New England Journal of Medicine, 2008;359:50-60. (http://www.nejm.org/doi/pdf/10.1056/NEJMsa0802005)
, DesRoches, C., et al, “Electronic Health Records in Ambulatory Care - A National Survey of Physicians” New England Journal of Medicine, 2008;359:50-60 C., et al, “Electronic Health Records in Ambulatory Care - A National Survey of Physicians” New England Journal of Medicine, 2008;359:50-60. (http://www.nejm.org/doi/pdf/10.1056/NEJMsa0802005)

What is the new Missouri Health Information Organization (HIO) doing?

Missouri HIO
A public-private, collaborative process to inform the strategic approach to Missouri’s health information exchange infrastructure, with a particular focus on: Consumer engagement Privacy and security and compliance with state and
federal law Sustainable financing Transparent governance Technical infrastructure to support statewide HIE Business and technical operations to support
widespread HIT adoption and use
19

Provide leadership for a statewide health information exchange strategy that will lead to improvements in health care quality, affordability, and outcomes for all Missourians
Mission
To leave no physician behind!

Missouri HIO Board John Bluford, President and CEO, Truman Medical Center Kim Day, Senior VP, Regional Markets, Sisters of Mercy Health
System Margaret Donnelly, Director, Missouri Dept. of Health & Senior
Services (ex-officio, voting) Karen Edison, M.D., Co-PI, Missouri HIT Assistance Center (ex-
officio, non-voting) Laura Fitzmaurice, M.D., Chief Medical Information Office,
Children’s Mercy Hospital Craig Glover, Chief Information Officer, Grace Hill Health Centers Tracy Godfrey, M.D., Family Physician, Family Health Center of
Joplin* Melissa Johnsen, Private Citizen and Former Business Executive

Sandra H. Johnson, J.D., Interim Dean and Professor Emerita of
Law and Health Care* Ethics, Saint Louis University School of Law Herb Kuhn, President and CEO, Missouri Hospital Association Ronald Levy, Director, Missouri Dept. Social Services (ex-officio,
voting)* Ian McCaslin, M.D., Director, MO HealthNet Division (ex-officio,
non-voting) Steve Roling, President and CEO, Healthcare Foundation of
Greater Kansas City* Andrea Routh, Executive Director, Missouri Health Advocacy
Alliance Steve Walli, President and CEO, United HealthCare David Weiss, Senior VP and CIO, BJC Healthcare* Karl Wilson, President and CEO, Crider Health Center
*Officers of the Board

Governance
17 member public-private Board meets the first Wednesday of every month - incorporated on July 13, 2010
Executive search is underway for the Missouri HIO President & CEO
24

Activities
Two Workgroups meet monthly to tackle critical issues and make recommendations to the Board
Technology & Operations Workgroup ▪ Co-Chairs: Melissa Johnsen, Private Citizen &▪ Mitzi Cardenas, Truman Medical Center
Legal & Policy Workgroup ▪ Co-Chairs: Karl Wilson, Crider Health Center &▪ Jerry Sill, Missouri Hospital Association

HIO Board
Consumer Advisory Council is in its formative stages and is anticipated to begin meeting in late 2010 Chair: Andrea Routh, MO Health Advocacy Alliance
Finance and Sustainability Committee Chair: David Weiss, BJC
RFP for technical services partner was released yesterday

Technical Implementation – Phased Rollout Approach
Phase 1 (by June 2011) Implement foundational technologies that will support
robust, sustainable HIE across the state
Phase 2 (by October 2012) Expands technologies to meet key use cases that
support meaningful use requirements & robust HIE
Future Implementation (2013 – ongoing) Will be based on adding technologies to support use
cases that will further promote sustainability and meet market demands

Use Case – Patient Care Summary Exchange
2010 Workflow 2011 Workflow
28
2. Provider refers patient for a specialist consult
3. Provider may send referral and patient care summary to specialist (via fax, via patient)
4. Specialist receives referral and patient care summary information
Missouri HIO
•Provider Directory
•Secure Messaging
1. Patient visits primary care provider; provider needs to refer patient to a specialist
4. Specialist sees patient
1. Patient visits primary care provider; provider needs to refer patient to a specialist
2. Providers uses EHR to access provider directory and identify specialist of choice
3. Provider sends referral and patient care summary to specialist; specialist receives email alert
4. Specialist sees patient

29
Use Case – Retrieval of Patient Information (2012)
Missouri Statewide Health Information Exchange Network
RHIO
Hospital System
Hospital Clinic Labs
FQHC Lab RHC
1. New patient visits primary care provider; provider wants to learn about patient’s medical history
2. Provider uses EHR to initiate search for patient health information
Master Patient Index & Record Locator Service
3. Provider’s EHR system looks up patient using the Statewide HIO’s master patient index (MPI), validates patient consent
5. Statewide HIE Network documents access to Network in audit log
4. Statewide HIO uses its record locator service (RLS) to locate and retrieve information on identified patient from connected Qualified Organizations RHIO
FQHC Lab RHC
- Patient information
6. Aggregated patient health information is returned to provider and information is incorporated into the provider’s EHR
Hospital

Request for Proposals – Technical Services Partner for Statewide Health Information Exchange
Solicits proposals from interested and qualified parties to partner with the Missouri HIO in designing, implementing, and operating Missouri’s statewide HIE platform
Key Milestones* Date – subject to change
Notice to community 11/5/2010
RFP released to vendors 11/12/2010
Letter of intent submitted (required for consideration)
11/19/2010
Vendor Q&A call 11/23/2010
Written proposals submitted 12/10/2010 (11:59 pm CDT)
Finalists announced Early January 2011
Finalist selection Early February 2011

MHIO: 2010 Action Plan
Complete executive search for MHIO President
Obtain ONC approval for strategic and operational plans releasing implementation funding
Develop and release request for proposal (RFP) for technical services
Finalize statewide privacy and security guidance
Coordinate and align with Medicaid Health IT Plan and the Missouri HIT Assistance Center
Develop finance and sustainability model
Initiate communications plan and outreach to consumers and providers

You can influence this process

Resources


35
Putting the “Meaning” in Meaningful UseDr. Karen Edison, M.D.

Meaningful Use

Objectives
Identify “eligible providers” for receiving meaningful use incentive payments and understand the differences between the Medicare and Medicaid incentive programs
Identify the core and menu sets of the meaningful use criteria for eligible providers and identify the timeline for the incentive programs
Recognize the role of the Missouri Health Information Technology Assistance Center (MO HIT AC) in providing assistance to primary care providers in achieving meaningful use

Eligibility
Eligible Providers

39
Eligibility Overview
Medicare Fee-For-Service (FFS) Eligible Professionals (EPs) Eligible Hospitals and Critical Access Hospitals (CAHs)
Medicare Advantage (MA) MA EPs MA-affiliated eligible hospitals
Medicaid EPs Eligible Hospitals (EH)
EPs must choose either the Medicare or Medicaid Incentive (can change once)

40
Medicare Eligible Providers (FFS)
MEDICARE Eligible Professionals (EPs) Doctor of Medicine or Osteopathy Doctor of Dental Surgery or Dental Medicine Doctor of Podiatric Medicine Doctor of Optometry Chiropractor
MEDICARE Eligible Hospitals (EHs) Acute Care Hospitals Critical Access Hospitals (CAHs)

Medicare Advantage Eligible Provider
MA Eligible Professional – Must Furnish, on average, at least 20 hours/week of patient
care services and be employed by the qualifying MA organization; OR
Be employed by, or be a partner of an entity that through contract with the qualifying MA organization furnishes at least 80% of the entity’s Medicare patient care services to enrollees
Hospitals – paid under the Medicare FFS incentive program

Medicaid Eligible Providers
MEDICAID Eligible Professionals: Physicians Nurse Practitioners (NPs) Certified Nurse-Midwives (CNMs) Dentists Physician Assistants (PAs) working in an FQHC or
RHC led by a PA
MEDICAID Eligible Hospitals Acute Care Hospitals (including CAHs) Children’s Hospitals

43
Medicaid Patient Volume Thresholds
Physicians, Dentists, Certified Nurse Midwives, Physician Assistants, Nurse Practitioners 30% Medicaid Patients
Acute Care Hospitals 10% Medicaid Patients
Medicaid EP practicing in an FQHC or RHC 30% “needy individual” patient volume threshold

Medicaid Patient Volume - Pediatricians
Pediatricians 20% Medicaid Patients
▪ Pediatricians with 20% Medicaid patient volume eligible for reduced incentive, totaling $42,502
▪ Pediatricians with 30% Medicaid patient volume are eligible for the full incentive amount - $63,750

Journey towards ‘Meaningful Use’

What is “Meaningful Use?”
Use of a certified EHR in a meaningful manner;
Use of certified EHR technology for electronic exchange of health information to improve quality of health care; and
Use of certified EHR technology to submit clinical quality measures (CQM) and other such measures selected by the Secretary
46

Staged Approach
STAGE 1: Data Capture Focus is on electronic capture of health information in a
structured format
STAGE 2: Data Aggregation Quality improvement at the point of care and electronic
exchange of information Target: 2013
STAGE 3: Data Use to Impact Outcomes Improvements in quality, safety and efficiency; clinical
decision support; & patient self-management tools Target: 2015

48
Meaningful Use Stages
Data Capture and SharingImproved Outcomes
Stage 1 Stage 2 Stage 3

Overview
* For Stage 2, CMS may also consider applying the criteria more broadly to both the inpatient and outpatient hospital settings. CMS expects to propose Stage 2
criteria by the end of 2011.* CMS expects to propose Stage 3 criteria by the end of 2013.

50
POLICY PRIORITIES FOR MEANINGFUL USE

51
Improve quality, safety, efficiency, and reduce health disparities
Access to comprehensive patient health data for patient’s health care team
Use of evidence-based order sets and CPOE
Clinical decision support at the point of care
Generate lists of patients who need care and use the list to reach out to patients

52
Engage patients and families
Provide patients and their families with timely access to data, knowledge, and tools to make informed decisions and to manage their health

53
Improve Care Coordination
Exchange meaningful clinical information among the members of a patient’s professional health care team

Improve population and public health
Submit immunization, syndromic surveillance and reportable disease data to public health agencies

Ensure privacy and security protection for personal health information
Protect confidential information through operating policies, procedures, and technology
Provide transparency of data sharing to patient

56
Stage 1 Meaningful Use Objectives
Stage 1 objectives (2011 and 2012) Include a core set of objectives that all EPs must
meet, as well as a menu set of objectives and measures (EP must select 5 from Menu Set).
EPs must report on 20 of 25 Meaningful Use Objectives
Reporting period is 90 days for first year; full year in subsequent years
For some objectives and measures, 80% of a provider’s patients must have a record in the certified EHR

Core ObjectivesStage 1 Meaningful Use CORE Objective Stage 1 Measure
Use CPOE At least one medication order entered for 30% of patients
Implement drug to drug and drug allergy interaction checks
Functionality enabled
E-Prescribing 40% of permissible prescriptions
Record demographics 50%
Maintain an up-to-date problem list 80%
Maintain active medication allergy list 80%
Record and chart changes in vital signs 50%
Record smoking status 50%
Implement one clinical decision support rule 1 rule (tracking compliance with rule not required)

Core ObjectivesStage 1 Meaningful Use CORE Objective Stage 1 Measure
Capability to exchange key clinical information (i.e., problem list, medication list, medication allergies, diagnostic test results) among providers of care and patient authorized entities electronically
1 test of the functionality
Provide patients with an electronic copy of their health information upon request
50% of those who request electronic copy, within 3 business days
Provide clinical summaries for patients for each office visit
50% of all office visits, within 3 business days
Protect electronic health information created or maintained by a certified EHR
Conduct or review a security risk analysis and implement updates as necessary
Report clinical quality measures as specified by the Secretary of HHS
2011 – report via attestation; 2012: report electronically

Menu Set of Objectives and Measures
Stage 1 Meaningful Use Menu Objective
Stage 1 Measure
Implement drug-formulary checks Functionality enabled
Incorporate clinical lab test results into Certified EHR Technology as structured data
40% of those with results in either a positive/negative or numerical format
Generate lists of patients by specific conditions to use for quality improvement and other activities
1 list
Send reminders to patients per patient preference for preventive or follow-up care
20% of patients 65+ or 5 years and younger
Provide patients with timely electronic access to their health information
10% of patients, within 4 business days
Use Certified EHR Technology to identify patient-specific education resources and provide those resources to the patient if appropriate
10%

Menu Set of Objectives and Measures
Stage 1 Meaningful Use Menu Objective
Stage 1 Measure
Perform medication reconciliation 50%
Provide summary of care record for each transition of care or referral
50%
Capability to submit electronic data to immunization registries or Immunization Information Systems and actual submission in accordance with applicable law and practice
1 test
Capability to submit electronic syndromic surveillance data to public health agencies and actual submission in accordance with applicable law and practice
1 test

Reporting Requirements for Quality Measures – 6 total measures
Report Three Core Measures Hypertension: Blood Pressure Measurement Tobacco Use Assessment and Tobacco Cessation Adult Weight Screening
Alternate Core Measures Weight Assessment for children and adolescents Influenza Immunization Childhood Immunization

62
Menu set – Quality Measures
EPs choose three measures from a menu of 38 additional Clinical Quality Measures, which include: Hemoglobin A1C > 9 LDL <100 BP <140/90 Asthma Assessment Colorectal CA screening Others…

Incentives

64
INCENTIVE PAYMENTS

Medicare EP Payment Schedule
Adoption Year 2011 2012 2013 2014 2015 2016 TOTAL PENALTY
2011 $18,000 $12,000 $8,000 $4,000 $2,000 $0 $44,0002012 $18,000 $12,000 $8,000 $4,000 $2,000 $44,0002013 $15,000 $12,000 $8,000 $4,000 $39,0002014 $12,000 $8,000 $4,000 $24,0002015 $0 1%2016 $0 2%
3% 3% 3% 3% 3% 3% 3% 3% 3%
Maximum Payment

66
Medicare Incentive payments
Medicare EPs practicing in Health Professional Shortage Areas (HPSAs) receive a 10% additional incentive payment

Medicaid EP Payment Schedule
Payment Amount for Year: 2011 2012 2013 2014 2015 2016
2011 $21,2502012 $8,500 $21,2502013 $8,500 $8,500 $21,2502014 $8,500 $8,500 $8,500 $21,2502015 $8,500 $8,500 $8,500 $8,500 $21,2502016 $8,500 $8,500 $8,500 $8,500 $8,500 $21,2502017 $8,500 $8,500 $8,500 $8,500 $8,5002018 $8,500 $8,500 $8,500 $8,5002019 $8,500 $8,500 $8,5002020 $8,500 $8,5002021 $8,500
TOTAL Possible Incentive $63,750 $63,750 $63,750 $63,750 $63,750 $63,750
First Year Medicaid EP Qualifies to Receive Payment

Medicaid EP Incentives
EPs can receive a total of 6 years of payment (total: $63,750)
the first incentive payment year at $21,250, plus five years at $8,500
EPs can start qualifying for incentives in January 2011. Medicaid incentives run through 2021
EPs may demonstrate MU as late as FY 2016 and still qualify for the maximum total incentive

Medicaid – Adopt/Implement/Upgrade
Medicaid EPs can receive the incentive in their first participation year for adopting, implementing or upgrading an EHR
Adopt: Acquire and Install Implement: Start Using Upgrade: Expand
Must be certified EHR technology

70
Incentive Payments – Key Concepts

Eligibility begins for EPs in any calendar year beginning on or after January 1, 2011
Payment year: The first year an EP receives an incentive payment
For the first payment year, the reporting period is any 90-day period within a payment year in which the physician successfully demonstrates meaningful use of certified EHR technology
In subsequent payment years, the EHR reporting period is the entire payment year – after the first payment year, the physician must successfully demonstrate meaningful use of certified EHR technology for the entire year

Payment - Timing
CMS expects to begin making Medicare incentive payments in May, 2011 EPs will receive a single incentive payment for a
payment year, not periodic installments Estimate is that it will be 15-46 days from successful
MU attestation to making incentive payments
States determine deadlines for Medicaid incentives, but most are expected to be in place by Summer 2011

A bit more detail on Medicare payments… The Medicare incentive payment amounts are a
maximum. An individual provider’s incentive payment is equal to 75% of the total “allowed charges” during the payment year, up to the amounts outlined in the chart
2 milestones required to trigger payment Successfully demonstrating Meaningful Use EP’s allowed charges have reached the qualifying
threshold for maximum incentive payment for the Payment Year ($24,000 for 2011)
EPs who do not meet the maximum threshold during the year will receive their payment the following year

How does a physician get started?
In order to qualify for a meaningful use incentive payment, an EP must have certified EHR technology
Medicare EPs must: Have a National Provider Identifier (NPI) Be enrolled in the CMS Provider Enrollment,
Chain and Ownership System (PECOS)
Registration
All physicians must register via the EHR Incentive Program website: http://cms.gov/EHrIncentivePrograms
EPs must attest that they are meaningful users through a secure mechanism (e.g., claims-based reporting, online portal) for Payment Year 2011

Registration: Medicaid
States will connect to the EHR Incentive Program website to verify provider eligibility and prevent duplicate payments
States will ask for additional information to make timely and accurate payments: Patient Volume Licensure Meaningful Use Certified EHR Technology

Resources
Are you a primary care physician in a small practice? You may be eligible for assistance from the
Missouri HIT Assistance Center The Assistance Center serves primary care
physicians in small (10 or fewer providers) practices with adoption, implementation, and achievement of meaningful use of certified EHR technologies
For more information: www.ehrhelp.missouri.edu

Missouri Health
Information Technology Assistance
Center
Your Answer to All Things EHR

Missouri HIT Assistance Center
Partnership: University of Missouri
▪ Dept of Health Management and Informatics▪ Center for Health Policy ▪ Dept of Family and Community Medicine
Missouri Telehealth Network
Primaris
Missouri Primary Care Association
Kansas City Quality Improvement Consortium
Hospital Industry Data Institute (Critical Access Hospitals)

Missouri HIT Assistance Center - Vision
Assist Missouri's health care providers in using electronic health records to improve the access and quality of health services; to reduce inefficiencies and avoidable costs; and to optimize the health outcomes of Missourians

81
EHR Adoption Challenges
FinancialFinancial
Organization Change
Organization Change
• Expense of system• Uncertainty around ROI• Provider and staff productivity• Uncertainty about financial incentives
• Disruption of workflow and productivity• Privacy and security concerns• Maintaining patient centeredness and satisfaction
• Concerns about technically supporting a system• Lack of necessary computer skills • Finding the right EHR to suit practice needs (“usability”)• Having the right IT staff in place• Possibility of information overload
TechnicalTechnical

82
EHR Implementation Challenges
Require significant support to carry out proper workflow re-design
Result can be piecemeal and less effective use of EHR capabilities and fewer financial and quality benefits Substantial time spent customizing forms and redesigning
workflow More time spent with patients leading to longer workdays
or fewer patients during the initial period Overburdened planning and implementing without
additional technical support

Conflicting messages

Gap in the costs and incentives at an individual physician level
$K
2009 2010 2011 2012 2013 2014 2015
-30
-5
-5 +18
-5 +12
+8+4 +2
-5-10 -5
Physician costMedicare
incentive
Net gap:-$21K
Source: Massachusetts eHealth Collaborative

Positive Financial Returns with Increasing BenefitsNet benefit from using an EMR for a 5 year period was $86,400 per provider
85
Wange, S., et al. (2003) “A Cost-Benefit Analysis of Electronic Medical Records in Primary Care”. The American Journal of Medicine. V.114 , April

“I think of the regional extension centers as a comprehensive support team for small practices. These centers will provide not only technical assistance, but general information when these small practices need help.”
AAFP President-elect Roland Goertz, M.D., M.B.A., testifying before the House Energy and Commerce Committee's Health Subcommittee that solo and small rural practices, in particular, need assistance if they are to adopt health information technology. 86
Missouri HIT Assistance Center

Who will we serve?
PRIORITY: Primary Care Providers, including physicians (Family Practice, Internal Medicine, OB/GYN, Pediatrics) and other health care professionals (NP, PA) with prescribing privileges in the following settings:
Small group practices (10 or fewer providers with prescriptive privileges)
Ambulatory clinics connected with a public or critical access hospital
Community health centers and rural health clinics Other ambulatory settings that predominately serve
uninsured, underinsured, and medically underserved populations
55 Critical Access and Rural Hospitals

Service Area and Demographics
Population - 5,874,327
Primary Care Providers - 5300
Priority PCPs - 2400
Priority PCPs Served - 1167
Total Providers - 17,946
CAH and Rural Hospitals - 55

Who are we and what is our role?
Team of experienced local Health IT professionals with intimate knowledge of the Missouri medical community
Part of a national network of select organizations designated by HHS to assist providers with modernizing their practices with certified EHRs
Direct, rapid and reliable access to a pipeline of key information on health IT and meaningful EHR use
89

Who are we and what is our role?
For providers who do not currently have a certified EHR system We help you choose and implement one in your office
For providers who already have a system We help eligible providers meet the criteria for
incentive payments from Medicare or Medicaid for the meaningful use of certified EHRs

Assistance Center Services
Continuing Education and Training for ALL Providers Vendor Selection and Group Purchasing
Group Purchasing Vendor Selection
EHR Implementation and Project Management Practice Workflow Analysis and Redesign
Practice Readiness Assessment Change Management Workflow Re-Design
Functional Interoperability and HIE Resources for Health Information Exchange Security Risk Analysis
Help Providers Achieve “Meaningful Use”

EHR Vendor Selection
Vetted Vendors : Allscripts
Professional Amazing Charts Cerner e-MDs eClinicalWorks EHS
GE Centricity Greenway McKesson
Practice Partner NextGen Pulse Sage Intergy

The Missouri HIT Assistance Center will work with any vendor (within reason)
We help you with each step toward meaningful use
Practice readiness assessment Workflow analysis for redesign Vendor Selection Implement HR Meaningful Use attestation Meaningful Use incentives

For physicians with EHRs we provide a direct path to meaningful use
Identify barriers Identify solutions Standardize processes Analyze reports Meaningful Use incentives

Our ultimate goal?
To help prevent the demise of the small independent practice, particularly in Missouri’s most underserved communities

Many Thanks for slides I borrowed!
Ron Levy, Director of Missouri Dept. Social Services
Karl Korkendorfer MD, Family & Community Medicine, Univ. of Missouri
Amy Hoyt, Counsel Dept. of Insurance
Benoy Thomas, MHI & MHA Candidate
Mike Fondell, EHR Pathways Kier Walls, Manatt Probably others………..

Additional Resources
Information, tip sheets, & more from CMS: http://www.cms.gov/EHRIncentivePrograms
Info about Missouri’s statewide HIO and MO HealthNet (Medicaid) Incentive Program: http://www.dss.mo.gov/hie
Learn about certification & other ONC programs: http://healthit.hhs.gov

For More Information:
Website: http://ehrhelp.missouri.edu
E-Mail: [email protected]
Phone: 1-877-882-9933





























