Embed Size (px)
Citation preview

KEEPING UP WITH THE CLINICAL ADVANCES: DEPRESSION

Learning Objective
• Describe the molecular targets of novel agents, including adjunctive treatments, currently being investigated

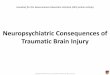
50% of Patients Respond to MonoaminergicAntidepressants
Deficiency in monoamines
Increase monoamine levels with an antidepressant

50% of Patients DO NOT Respond to Monoaminergic Antidepressants
Adequate monoamines
Increase monoamine levels with an antidepressant
Downstream dysfunction in glutamatergic neurotransmission or
neuroplasticity
Pharmacological modulation of downstream dysfunction in glutamatergic
neurotransmission or neuroplasticity

Duration of antidepressant treatment (days)0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28
Monoamine levels
Depressive symptoms
Changes in neuroplasticityand glutamatergicneurotransmission
Beyond Monoamines: The NeuroplasticityHypothesis of Depression

Beyond Monoamines: The Neuroplasticity Hypothesis of Depression
• The depressed brain shows signs of inadequate neuroplasticityand excessive glutamate
• Acting on monoaminergic systems, currently available antidepressants may lead to downstream improvement in neuroplasticity and glutamatergic neurotransmission
• Directly targeting glutamatergic neurotransmission or neuroplasticity may:
• Lead to faster treatment response (e.g., ketamine, rapastinel, SAGE-547, SAGE-217)
• Improve response and remission ratesRacagni G, Popoli M. Dialogues Clin Neurosci 2008;10(4):385-400; Crupi R, Marino A, Cuzzocrea S. Curr Med Chem 2011;18(28):4284-98; Sanacora G, Treccani G, Popoli M. Neuropharmacology 2012;62(1):63-77; Vidal R, Pilar-Cuellar F, dos Anjos S et al. Curr Pharm Design 2011;17(5):521-33; Banasr M, Dwyer JM, Duman RS.
Curr Opinion Cell Biol 2011;23(6):730-7; Duman RS, Aghajanian GK. Science 2012;338(6103):68-72.

Neuroplasticity: Monoamine Signaling and Brain-Derived Neurotrophic Factor Release
CREB
synaptogenesis
neuroplasticity
cell survival
neurogenesis
BDNF: brain-derived neurotrophic factor
CREB: cAMP response element-binding protein
CaMK: calcium/calmodulin-dependent protein kinasePKA: protein kinase A
monoamine
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013.

Genes turned on
Increased neuroplasticity and reduced glutamatergic neurotransmission
Decreased release of glutamate
Increased proteins involved in neuroplasticity
Activation of cAMP response element binding protein (CREB)
Racagni G, Popoli M. Dialogues Clin Neurosci 2008;10(4):385-400;Barbon A et al. Neurochem Int 2011;59(6):896-905.
Downregulation of NMDA receptors
Increased expression of AMPA receptor subunits
Downstream Improvement in Neuroplasticity and Glutamatergic Neurotransmission
DA 5HT NEMonoamine regulation
PKCRSKCaMK
GSK-3Wnt/FrzcAMP
MAPKSignaling cascades

The Three G's Glutamate, GABA, and Glycine

Impaired Neuroplasticity Due to Imbalanced GABA and Glutamate signaling
• Abnormalities in glutamatergic neurotransmission via the N-methyl-D-aspartate receptor (NMDA-R) have a key role in the pathophysiology of depression
Hashimoto K et al. Transl Psychiatry. 2016;6:e744.
NMDA-R

Dysfunction of Glutamate Signaling
• Glutamate is an excitatory neurotransmitter involved in many functions, including synaptic plasticity, learning, and memory
• Studies have shown regional changes in glutamate receptors, as well as elevated levels of glutamate in the brains of patients with MDD
• Normal glutamatergic activity is thought to be involved in maintaining normal neuroplasticity
• Under conditions of stress or depression, glutamate signaling is impaired, leading to a reduction of neuroplasticity
Hashimoto K et al. Transl Psychiatry. 2016;6:e744; Inoshita M et al. Neuropsychiatr Dis Treat. 2018;14:945-953; Sanacora G et al. Neuropharmacology. 2012;62(1):63-77.

Directly targeting glutamatergic
neurotransmission or neuroplasticity may lead to faster treatment response
and may improve response and
remission rates
Ketamine
NMDA receptorCa2+
Bunney BG, Bunney WE. Int J Neuropsychopharmacol 2012;15:695-713.
Ketamine Directly Targets Glutamate Neurotransmission

Ketamine
• Ketamine (anesthetic)
• Blocks NMDA receptors, evokes glutamate release
• Induces schizophrenia-like symptoms in normal volunteers and exacerbates them in patients
• Short-term, low-dose intravenous ketamine does not induce full range of psychotic symptoms in experimental setting

Ketamine Increases Synaptic Plasticity
AMPARs
Increased synaptic plasticity
mTOR
Bunney BG, Bunney WE. Int J Neuropsychopharmacol 2012;15:695-713.
mammalian Target Of Rapamycin: a critical
intracellular protein that mediates neuroplasticity and
neurotrophic processes

glu
AMPAreceptor
NMDAreceptorblocked byketamine
ERK, AKT
mTOR
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013.
Ketamine’s Antidepressant Effects May Also Be Due to Activation of AMPA Receptors, not the Blocking of NMDA Receptors

Attenuation of Antidepressant Effects of Ketamine by Opioid Receptor Antagonism
Williams NR et al. Am J Psychiatry. 2018; Epub ahead of print.
Recent study showed that ketamine may work to treat depression, at least in part, by activating opioid receptors
Ketamine Placebo
Reduction in symptoms of depression
Naltrexone(opioid-blocking drug)Ketamine
Almost no effect on symptoms of
depression

• Underlying antidepressant mechanism for ketamine may be due to the metabolite (2R,6R)-HNK acting through activation of AMPA receptors, instead of blocking NMDA receptors
• More effective at reducing depression-like symptoms, even though the (S)-form is about 3–4 times more potent at blocking NMDA receptors
• Lacks the negative side effects and potential for abuse that ketamine has
• Future research aims to test the effectiveness of (2R,6R)-HNK for the treatment of depression in humans.
Utility of (2R,6R)-Hydroxynorketamine viaDirect AMPA Activation
Abdallah CG et al. Depress Anxiety 2016; 33: 689-697; Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013; Zanos P et al.
Nature 2016; 533: 481-486; Zhao X et al. Br J Clin Pharmacol. 2012;74(2):304-14.
(2R,6R)-Hydroxynorketamine (HNK)—a metabolite of ketamine

Antidepressant Effect of Ketamine Within Hours in Patients With Treatment-Resistant Depression
* indicates P<.05; †, P<.01; ‡, P<.001
21-It
em H
DR
S Sc
ore
15
25
0
5
10
30
20
-60min
40min
90min
110min
230min
Day 1
Day 2
Day 3
Day 7
Ketamine
*
*
†‡
‡ ‡
Placebo
Zarate CA Jr et al. Arch Gen Psychiatry 2006;63:856-64.
HDRS: Hamilton Depression Rating Scale
Dose of intravenous ketamine consistently decreases
symptoms of depression in patients with treatment-resistant depression in a
rapid (within hours), robust(across many symptoms of depression), and relatively sustained (typically 7-14
days) manner

Rapid Antidepressant Effect of Ketamine in 18 Patients With Treatment-Resistant Depression
29% were considered to be in remission,with an HDRS score of 7 or below (data not shown)
40min
90min
110min
230min
Day 1
Day 2
Day 3
Day 7
Prop
ortio
n W
ith 5
0% C
hang
e in
Sc
ore
From
Bas
elin
e (H
DR
S)
0.8
0
0.2
0.6
KetaminePlacebo
0.4
1.0
HDRS: Hamilton Depression Rating Scale
Zarate CA Jr et al. Arch Gen Psychiatry 2006;63:856-64.

Safety and Efficacy of Repeated-Dose Intravenous Ketamine
• Repeated doses (six infusions over the course of several weeks) have shown promise from an efficacy and safety standpoint
• Even when dose is escalated
• No advantage in efficacy in sustaining the initial antidepressant effects for two times verses three times a week intravenous ketamine in patients (n=67)
Aan het rot M et al. Biol Psychiatry. 2010;67(2):139-45; Cusin C et al. Aust N Z J Psychiatry. 2017;51(1):55-64; Singh JB et al. Biol Psychiatry. 2016;80(6):424-31.

Ketamine Formulations• Ketamine intranasal administration 50 mg vs saline placebo (n=27)−Effective, easier to administer1
• Intranasal esketamine (S-enantimer of racemic ketamine)− 0.20 mg/kg and 0.40 mg/kg intravenous esketamine exhibited significant
reductions in MADRS scores compared with placebo (n=30)2
−After a 1-week period, all three intranasal esketamine treatment groups (28 mg, 56 mg, or 84 mg) changes in MADRS total scores were statistically superior to placebo on Day 8 (n=67)3
• Efficacy and safety of intravenous, intramuscular and subcutaneous routes for treating depression with ketamine4
−All three had comparable antidepressant effects; Subcutaneous has fewest adverse effects
Lapidus KA et al. Biol Psychiatry. 2014;76(12):970-6; Singh JB et al. Am J Psychiatry. 2016;173(8):816-26; Daly EJ et al. Presented at the 54th Annual Meeting of the ACNP; Dec.
2015; Hollywood, FL; Loo CK et al. Acta Psychiatr Scand. 2016;134(1):48-56.
MADRS: Montgomery-AsbergDepression Rating Scale

A Consensus Statement on the Use of Ketamine in the Treatment of Mood Disorders
Recommendations from the American Psychiatric Association Council of Research Task Force on Novel Biomarkers and Treatment Recommendations for Clinical Use of Ketamine
Patient Selection • Strongest evidence for major depressive disorder• Less evidence in other mood disorders• Baseline symptom assessment• Antidepressant treatment history• Physical and laboratory • Informed consent including discussion of potential risks and benefits
Clinical Experience and Training
• Currently no recommendations or guidelines• Clinicians should be prepared to manage potential cardiovascular events and behavioral effects of ketamine
Treatment Setting • Setup for monitoring of cardiovascular and respiratory function
Medication Delivery • Most studies use 0.5 mg/kg of IV ketamine delivered over 40 minutes• Dose may need to be adjusted for patients with BMI>30
Follow-up and Assessments • Use rating instruments to assess clinical response and evaluate risk:benefit ratio of continued treatment
Efficacy of Longer-term Repeated Administration
• Studies suggest that repeated dosing may extend the duration of ketamine effects• Ketamine administration 2X/week over 2-3 weeks seems as effective as 3X/week over 2-3 weeks• Taper or discontinue treatment based on an individual patient basis
Safety Measures and Continuation of Treatment
• Risk of cognitive impairment and cystitis are associated with chronic ketamine use• Substance abuse liability• Frequent ketamine administration is not recommended
Future Directions • Major knowledge gaps remain regarding long-term efficacy and safety • Further, large-scale studies are needed • Clinicians providing ketamine treatment are encouraged to participate in coordinated systems of data collection
Sanacora G et al. JAMA Psychiatry. 2017;74(4):399-405.

Other Glutamatergic ModulatorsFailed to Show Efficacy or No
Longer in Development
1. Mathew SJ et al. Neuropsychopharmacology. 2017; 2. Zarate CA et al. Am J Psychiatry. 2006;163(1):153-5; 3. Smith EG et al. J Clin Psychiatry 2013; 74: 966–973; 4. Sanacora G et al. Neuropsychopharmacology. 2017;42(4):844-853; 5. Preskorn SH et al. J
Clin Psychopharmacol. 2008;28(6):631-7; 6. Heresco-levy U. et al. Int J Neuropsychopharmacol. 2013;16(3):501-6; 7. Liu RJ et al. Neuropsychopharmacology. 2017;42(6):1231-1242; 8. Nagele P et al. Biol Psychiatry. 2015;78(1):10-8.
Agent TargetRiluzole Voltage-gated sodium
channelsDid not out-preform placebo on mean MADRS1.05
Memantine NMDA receptor Trials for depression unsuccessful2,3
Lanicemine NMDA receptor Failed to show superior efficacy4
CP-101,606 NMDA-NR2B subunit Ceased due to association with cardiac conduction abnormalities5
EVT-101 NR2B selective antagonist
Clinical hold issued by the FDA
MK-0657 NMDA-NR2B subunit Weak evidence of efficacy
AZD-6423 NMDA receptor Weak evidence of efficacy
AVP-923 NMDA receptor, Sigma-1 receptor, SERT, NET
Alzheimer, no TRD efficacy
AVP-786 NMDA receptor, Sigma-1 receptor, SERT, NET
Alzheimer, no TRD efficacy
Agent Target
d-Cycloserine NMDA receptor Moderate evidence6
GLYX-13 (rapastinel)
NMDA receptor Currently in Phase III; Moderate evidence7
AXS 05 dextro-methorphan +
bupropion
Currently in Phase III; Moderate evidence
Nitrous oxide NMDA receptor Preliminary evidence of efficacy for MDD8
Still in Development

Rapastinel: An NMDA Receptor Glycine-Site Functional Partial Agonist vs Positive Allosteric Modulator
• Allosteric modulator of both glutamate and glycine at novel binding site
• Functional partial agonist of the glycine site of the NMDA receptor
• In preclinical studies, rapastinel showed robust antidepressant effects with rapid onset and appeared to increase neuroplasticity and enhance synaptic function
Moskal JR et al. Expert Opin Investig Drugs. 2014;23(2):243-54; Preskorn S et al. J PsychiatrPract. 2015;21(2):140-9; Liu RJ et al. Neuropsychopharmacology. 2017;42(6):1231-1242.
NMDA receptor
Glutamate Glycine
Novel binding site

Rapastinel: An NMDA Receptor Glycine-Site Functional Partial Agonist vs Positive Allosteric Modulator
• Produces rapid antidepressant effects−Single Dose Study Phase IIA (n=116): Single IV dose of rapastinel
dose of 1, 5, 10, or 30 mg, or placebo1
• At 1-week post-infusion, 5 and 10 mg of rapastinel showed significant antidepressant response
−Repeated Dose Study Phase IIB (n=116): Weekly infusion of IV rapastinel (at doses of 1, 5, or 10 mg) or placebo, with follow-up on days 3, 7, and 142
• IV rapastinel 5 or 10 mg showed a reduction in HAM-D scores on days 1 through 7, but no effects were observed thereafter
• No ketamine-like side effects• Currently in large phase III trials for MDD
1. Moskal JR et al. Expert Opin Investig Drugs. 2014;23(2):243-54; 2. Preskorn S et al. J Psychiatr Pract. 2015;21(2):140-9; Liu RJ et al. Neuropsychopharmacology. 2017;42(6):1231-1242.

Novel Positive Allosteric Modulators
• SAGE-547 (brexanolone), is a intravenous (IV) formulation of allopregnanolone, a naturally occurring neuroactive steroid that acts as a positive allosteric modulator of GABA-A receptors, including both synaptic and extrasynapticpopulations
• SAGE-217, a novel, oral neuroactive steroid that, like SAGE-547, is a positive allosteric modulator of GABAA receptors, targeting both synaptic and extrasynaptic GABA-A receptors

Extrasynaptic Benzodiazepine-Insensitive GABA-A Receptor
4∝
6∝
𝛽
𝛿𝛽
GABA binding site Neurosteroid
binding site
GABA-A Complex Receptorcontain 𝛿 subunit

Two Types of GABA-A Mediated InhibitionGABA neuron
glial cell
Tonic InhibitionPhasic Inhibition
GABA
Benzodiazepine-sensitive GABA-A
receptor
extrasynaptic
Benzodiazepine-insensitive GABA-A
receptorpostsynaptic
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013
neurosteroid
cholesterol
pregnenolone

Allosteric Modulation of ExtrasynapticGABA-A Receptors
4∝
6∝
𝛽𝛿𝛽
GABA binding site Novel PAM
binding sitePositive Allosteric
Modulation (PAM) can increase receptor efficiency
and/or potency
PAM
Increased tonicGABAergic current
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013; Tuem KB, Atey TM. Front Neurol. 2017;8:442.
Extrasynpatic GABA-A contain 𝛿 subunit

SAGE-547: Positive Allosteric Modulator of GABA-A Receptors for PPD
Two Double-Blind, Placebo-Controlled, Phase-III Studies• Women (age 18 – 45) with severe postpartum depression (PPD) for ≤6
months • 3 groups administered a continuous inpatient infusion for 60 hours
• (brexanolone IV 90 g/kg/hour; brexanolone IV 60 g/kg/hour; and placebo)
• Results: Both brexanolone groups experienced a greater mean reduction in HAM-D score compared with placebo after 60 hours
− brexanolone IV 90 g/kg/hour: 17.7 points; P = 0.0252− brexanolone IV 60 g/kg/hour: 19.9 points; P = 0.0013
• Effects observed at 60 hours was maintained at the 30-day follow-up• Brexanolone was well-tolerated overall, and the most common adverse events
were headache, dizziness and somnolence.Meltzer-Brody SE, et al. Poster P5-168. and Meltzer-Brody SE, et al. Poster P5-169.
Presented at: American Psychiatric Association Annual Meeting; May 5-9, 2018; New York.

SAGE-217: Positive Allosteric Modulator of GABA-A Receptors for MDD
• Phase II Clinical Trial: randomized, double blind, placebo controlled clinical trial − 89 subjects with moderate-to-severe major depressive disorder
(MDD); ages 18-65
• Onset of action is within 24 hours after first dose• At the end of 14 days patients receiving 30mg of SAGE-217 had
a 17.6-point reduction from baseline in HAM-D scale vs. 10.7 point on placebo (p<0.0001)
• Most common adverse events were headache, dizziness, nausea, somnolence− AE rates were 53% on SAGE-217 and 46% on placebo
Gunduz-Bruce H et al. Biol. Psychiatry. 2018;83:S108-128.

The Endogenous Opioid System

Identified Phases of Reward Processing
Keren H et al. Am J Psychiatry. 2018; Epub ahead of print.
Reward Phase Associated Symptom Translational Term Example
Experimental Task
Prediction Anticipatory anhedonia
Reward/loss anticipation
Monetary incentive delay task
Decision Impaired decision making Choice Iowa gambling task
Action Low energy Effort expenditure Effort expenditure for rewards task
Experience Consummatoryanhedonia
Reward/loss feedback
Monetary incentive delay task

Neural Aberrations During Reward Processing in Depression
• Meta-analyses of 38 fMRI and 12 EEG studies• fMRI studies revealed significantly reduced striatal activation in
depressed compared with healthy individuals during reward feedback.
• When region-of-interest analyses were included, reduced activation was also observed in reward anticipation, effect stronger in individuals <18
• EEG studies involved mainly the FRN event-related potential• FRN was also significantly reduced in depression, with pronounced
effects in individuals under age 18. In longitudinal studies, reduced striatal activation in fMRI and blunted FRN in EEG were found to precede the onset of depression in adolescents.
Keren H et al. Neuroimage. 2018;178:266-276.
EEG: electroencephalogram; fMRI: functional magnetic resonance imaging; FRN: feedback-related negativity

receptorμ
δreceptor
κreceptor
Endogenous Opioid Receptors
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013; Benarroch EE. Neurology. 2012;79(8):807-14.
Opioid Peptides𝛽-endorphinenkephalindynorphin
Opioid ReceptorsMu (μ) àDelta (δ) à
Kappa (κ) à

Location of Opioid Receptors
Nummenmaa L, Tuominen L. Br J Pharmacol. 2018;175(14):2737-2749.
Location of Mu-Receptors in the Brain Overlap of human emotion circuit

Partial Agonist(e.g. buprenorphine)
Full Agonist(e.g. methadone)
Dose of Opioid
Opioid Effect
Mu opioid receptor
partialagonist
Partial agonist binds to the opioid receptor and causes it to open more frequently than the resting
state but less frequently than with a full agonist
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed. 2013.

Opioid Receptor
Main Endogenous
Agonists
Effect on Pain
Effects on Behavior
Mu (μ) 𝛽-Endorphin
Metenkephalin
analgesia (spinal)
• antidepressant-like behavior
• euphoria• reward and physical
dependence• improved mood• respiration• sedation
Mu-opioid receptor agonists may also have antidepressant potential
Mu opioid receptor
agonist

Opioid Receptor
Main Endogenous
Agonists
Effect on Pain
Effects on Behavior
Delta (δ) Enkephalins Analgesia (supraspinal
& spinal analgesia)
• sedation• inhibition of
dopamine release• modulation of mu-
opioid receptors
Delta-opioid receptors may have antidepressant and anti-anxiety actions
agonist
Delta opioid
receptor

Opioid Receptor
Main Endogenous
Agonists
Effect on Pain
Effects on Behavior
Kappa (κ) Dynorphin A Analgesia (spinal)
• worsened mood• diuresis• dysphoria
Kappa neurons may interact to block Mu neurons and thus, kappa agonists worsen
depression and cause dysphoria in animal models
agonist
Kappa opioid
receptor

Kappa opioid
receptor Currently being studied for their potential antidepressant actions
antagonist
Kappa antagonist, especially if combined with a small degree of
mu agonist, will potentiate possible antidepressant effects by a novel non
monoaminergic mechanism

Endogenous Opioid Receptors
• κ-opioid receptor antagonists have antidepressant potential• Likely to be implicated in mood regulation• All 3 opioid receptors modulate BDNF activity and neurogenesis in the hippocampus
Opioid Receptor
Main Endogenous Agonists
Reward Mechanisms
Effect on Pain AgonismEffects on Behavior
Mu (μ) 𝛽-EndorphinMet-enkephalin
Facilitates Analgesia (spinal)
Improved mood, reward anddependence, euphoria,
antidepressant-like behavior, sedation
Delta (δ) Enkephalins Facilitates Analgesia (supraspinal &
spinal analgesia)
Improved mood; antidepressant and antianxiety-like behavior, sedation
Kappa (κ) Dynorphin A Inhibits Analgesia (spinal) Worsened mood; dysphoria, anti-reward, sedation
Benarroch EE. Neurology. 2012;79(8):807-14; Lutz PE, Kieffer BL. Trends Neurosci. 2013;36(3):195-206.

dynorphin
This leads to an increase in dopamine release in nucleus accumbens
Nucleusaccumbens
Ventraltegmentalarea
Mesolimbic dopamine
pathway
𝛽-endorphin
GABA interneuron
In contrast, the activation of kappa (𝜿) receptors located presynaptically in the nucleus accumbens inhibits dopamine
release
VTA
NA
Activation mu (𝝁) receptors located on GABA interneurons
leads to a disinhibition of dopaminergic neurons projecting
the nucleus accumbens
Spanagel R et al. Proc Natl Acad Sci USA. 1992;89(6):2046-50.
Mu and Kappa Systems Appear to Counteract, Especially in the Mesolimbic Dopaminergic System
DA

Buprenorphine
• Partial mu opioid agonist• Kappa antagonist• Currently used in addiction treatment• Open label, positive data in refractory depression• Low Dose Buprenorphine Reduces Suicidal Ideation−Double-blind, placebo-controlled trial 88 patients received either
0.1-0.8 mg/day (mean dose 0.44 mg/day) or placebo for 4 weeks−Very low dosages of buprenorphine were associated with
decreased suicidal ideation in a group of severely suicidal patients without substance abuse
Yovell Y et al. Am J Psychiatry. 2016;173(5):491-8.

ALKS 5461: Buprenorphine & Samidorphan• Combination of buprenorphine
(partial μ-opioid agonist, kappa antagonist) and samidorphan (μ antagonist)
• Samidorphan added to counteract the μ-opioid agonist activity of buprenorphine & reduce its addictive potential
• Kappa antagonism has shown antidepressant activity in animal models
• Possible adjunct to ongoing antidepressant
Fava M et al. Am J Psychiatry. 2016;173(5):499-508.
Study 205• Ph III Double-blind, placebo controlled • 11 week trial in AD non-responders
(n=814)• Doses of buprenorphine/ samidorphan−0.5/0.5 mg−2/2 mg
• Neither dose was statistically superior to placebo on primary endpoint (MADRS at week 5)−Post hoc analysis showed significance
for the 2/2 mg dose at other time points

ALKS 5461: Buprenorphine & Samidorphan
Ehrich E et al. Biol Psychiatry. 2017;81(10):S23.
• Ph III Multicenter, randomized, double-blind, pbo-controlled (n=407)
• Doses of buprenorphine/samidorphan− 1/1 mg− 2/2 mg
• Evidence of antidepressant activity in both groups
• Statistically significant for the 2/2mg group only
Study 207
The most common AEs:− Nausea− Dizziness− Fatigue
2/2mg Superior to Placebo− Improving core symptoms of
depression (MADRS-6, p=0.018)− Overall symptoms of depression
(MADRS-10, p=0.026)
No pattern of AEs indicative of abuse potential

ALKS 5461 as Adjunct in MDD
• Study 208: ongoing long-term phase 3b will evaluate the efficacy, safety, and tolerability of ALKS 5461 as adjunctive treatment in patients with MDD
• Agonist-antagonist opioid modulation represents a novel approach to the treatment of MDD
• May be an alternative to adjunct treatment with antipsychotics
Ehrich E et al. Neuropsychopharmacology. 2015;40(6):1448-55; Fava M et al. Am J Psychiatry. 2016;173(5):499-508.

Other Targets in Depression Treatments
Emerging Somatic Treatments • Deep Transcranial Magnetic Stimulation (DTMS)• Repetitive Transcranial Magnetic Stimulation (rTMS)• Synchronized Transcranial Magnetic Stimulation (sTMS)• Low Field Magnetic Stimulation (LFMS)
Bewernick B et al. F1000Res. 2015;4; Drevets WC et al. Biol Psychiatry. 2013;73(12):1156-63; Navarria A et al. Neurobiol Dis. 2015;82:254-61; Khajavi D et al. J Clin Psychiatry. 2012;73(11):1428-33; Dale E et al. Biochem
Pharmacol. 2015;95(2):81-97; Scarr E et al. Front Cell Neurosci. 2013;7:55; Cohen IV et al. Sci Rep. 2017;7(1):1450; Magid M et al. J Clin Psychiatry. 2014;75(8):837-44; Parsaik AK et al. J Psychiatr Pract. 2016;22(2):99-110.
Glucocorticoid Receptor Antagonists
Agent Clinical Trial PhaseMifepristone IIIMetyrapone IIIOrg-34517 II
Acetylcholine Muscarinic (AChM) Receptor Antagonist
• Scopolamine may exert antidepressant effects by acting on the MTORC1 complex via the mTOR pathway and thereby inducing synaptogenesis
Acetylcholine (Ach) Release Inhibitor and Neuromuscular Blocking Agent
• Onabotulinumtoxin A - yreatment in the glabellar (forehead) region can treat MDD
• Effects of one injection last up to 16 weeks

Summary
• Neurobiological substrates of depression may go beyond monoaminergic circuits
• Glutamatergic targets like ketamine, esketamine, and rapastinel have shown promise in treatment of MDD
• Opioid agents like buprenorphine and ALKS 5461 have shown efficacy in treatment of MDD
• Additional research is needed to validate these targets