Embed Size (px)
Citation preview
Kenevo® Reimbursement Guide
Information for practitioners and payers
Kenevo Microprocessor Knee Payer Reimbursement Guide
Ottobock | Kenevo Reimbursement Guide | Table of Contents
Table of Contents
1. Executive Summary
2. Recent Guidance for Lower Limb Prosthetics
3. Product Information (Coding, MSRP, FDA Status, Warranty, andPractitioner Training)
4. Features and Benefits
5. Benefits of microprocessor-controlled prosthetic knees to limitedcommunity ambulators: Systematic review
6. Summary: Mobility and Safety with a Microprocessor-Controlled Kneein Moderately Active Amputees
7. Summary: Functional Assessment and Satisfaction of Low MobilityTransfemoral Amputees with Microprocessor Knees
8. Clinical Studies using Microprocessor Knees with K2 Subjects
Kenevo Reimbursement Guide Executive Summary
Kenevo Reimbursement Guide | Executive Summary | Ottobock 1 of 4
Falling is a major issue in patients with transfemoral amputations with a reported annual incidence of more than 50% [1]. On average, individuals who fall with their prosthesis experience 3-4 falls per year [2]. A systematic review found prostheses with microprocessor-controlled knees (MPK) have been demonstrated to improve both psychoemotional and physical aspects of balance and falls. At the time this review was performed, there were only publications of studies with Ottobock MPK in K2 patients [6]. Evidence suggests that use of microprocessor knees (MPKs) can significantly reduce falls by up to 80% in individuals with Medicare functional classification level-2 (MFCL-2) mobility [3, 6, 7, 8]. In addition, a recently published analysis of the RAND Corporation estimated that MPKs may also reduce the risk of fall-related death and sustaining fall-related injuries by up to 79%. In this study, 85% of the evidence analyzed and used as a basis for the authors’ simulation were studies with Ottobock products [2]. Fall-related injuries are costly occurrences. A recent study estimated that medical expenses for treatment related to falls by older adults that did not result in death were close to $50 billion in 2015 [13]. Of that, Medicare funded $37.6 billion, while other payers including private health insurances funded $12 billion. In 2015 there were also 28,486 accidental fall-related deaths that resulted in over $750 million in medical cost [13]. Burns et al. reported that in 2012, hospitalization cost for fall-related injuries was almost $30,000 per occurrence [14]. In individuals with above-knee amputation, MPKs may contribute to containing cost incurring for falls [2].
Since the early 1990s, Medicare adopted MFCLs to rate an amputee’s ability and/or potential to ambulate. Prosthetic knee coverage criteria developed based on these MFCLs, appropriate for the prosthetic devices available at the time have not been modified since. Although MPK technology has progressed to overcome the inverse relationship between stability and function, current coverage criteria restrict advanced technology to younger, healthier, higher-functioning individuals. This is in contrast to other fields of healthcare in which advanced technology serves the oldest, sickest and most restricted patients. As a result of the MFCL restrictions, many transfemoral amputees are unable to benefit from the microprocessor technology covered under their current policy criteria.
A published systematic review of clinical trials [6] investigated whether MFCL-2 amputees might also benefit from using an MPK in safety, performance-based function and mobility and perceived function and satisfaction. Based on a review of 6 publications with 57 subjects with transfemoral amputation (TFA) and MFCL-2 mobility grade [7-12], the study reported that (1) MPK use may significantly reduce uncontrolled falls by up to 80% and significantly improve the
Kenevo Reimbursement Guide Executive Summary
Kenevo Reimbursement Guide | Executive Summary | Ottobock 2 of 4
indicators of fall risk; (2) that walking speed may be increased by 14-25% on level surfaces, by 20% on uneven surfaces and by 30% descending a slope; and (3) that the MPK enabled them to better perform activities of community ambulation actually categorized as part of MFCL-3 mobility grade. This last point is further supported by the fact that 44 to 50 percent of MFCL-2 subjects were able to improve their overall functional level to MFCL-3 when using a C-Leg based on two articles [6, 7, 8]. These results, especially the significant reduction in falls and risk of falling, were recently confirmed in bigger clinical studies with 50 and 30 subjects, respectively [3, 4]. In an observational study with 29 subjects using Kenevo, more than half of the individuals reported significant perceived improvements in activities of community ambulation as well as a significant reduction in additional wheelchair use from 87% to 37% of patients [5]. Finally, in three studies that measured personal preference, 90% of patients preferred the MPK over their previous non-microprocessor knee (NMPK) [5, 7, 8].
The results of the systematic review above suggest it is no longer appropriate to generally withhold MPK technology from MFCL-2 patients [6]. While current research does not justify an MPK fitting for all limited community ambulators, trial fittings could be used to determine whether or not patients with TFA and MFCL-2 mobility grade benefit from MPK use. The following proposal for patient selection and assessment is based on the 2-minute walk test (2MWT):
1) Patients walking up to 95m/305ft/0.8m/s in the 2MWT may qualify for a trial fitting withan MP stance controlled prosthetic knee.
2) Patients walking more than 95m/305ft/0.8m/s in the 2MWT may quality for a trial fittingwith a MP stance and swing controlled C-Leg.
In addition to the sound evidence supporting the use of microprocessor knees for K2 transfemoral amputees, there have been two guidance documents recently released. First, the Veteran’s Administration updated their clinical practice guidelines for the rehabilitation of lower-limb amputees, and determined that microprocessor knees may reduce risk of falls and maximize patient satisfaction in limited and unlimited community ambulators. The guideline recommends microprocessor knees over non-microprocessor knees as the first definitive prosthesis [15]. Their decision was based on two systematic reviews, both of which reported a decrease in stumble and fall frequency with accommodation and use of a microprocessor knee system relative to a non-microprocessor knee system. The studies further support the prescription of microprocessor knees over non-microprocessor knees to improve an individual’s ability to walk faster on level ground, uneven surfaces, and downhill, thus providing the user with an improved sense of security and improved overall satisfaction. [6,16]
Kenevo Reimbursement Guide Executive Summary
Kenevo Reimbursement Guide | Executive Summary | Ottobock 3 of 4
Second, a consensus statement was released by the Lower Limb Prosthetic Workgroup commissioned by the Centers for Medicare and Medicaid Services (CMS). In their statement, the workgroup acknowledged that an amputee functioning at the K2 level may benefit from MPK technology. The workgroup also added significant clarification to the K-Level descriptions, which we ask you to consider adding to your policy [17].
We invite you to thoroughly review the included copy of the full text paper of the systematic review of MPK studies in the limited community ambulator population. We would greatly appreciate the opportunity to present the detailed evidence to you and to discuss a monitored pilot project with beneficiaries of your company with an above-knee amputation and MFCL-2 mobility grade.
References
1. Miller W, Speechley M, Deathe B. The prevalence of risk factors of falling and fear of falling among lower extremity amputees. Arch Phys Med Rehabil 2001;82:1031-1037. View Article
2. Liu H, Chen C, Hanson M, Chaturvedi R, Mattke S, Hillestad R. Economic Value of Advanced Transfemoral Prosthetics. Research Report. RAND Corporation, Santa Monica, CA, 2017. View Article
3. Kaufman KR, Bernhardt KA, Symms K. Functional assessment and satisfaction of transfemoral amputees with mobility (FASTK2): A clinical trial of mixcroprocessor-controlled vs. non-microprocessor-controlled knees. Clin Biomech (Bristol, Avon) 2018 Oct;58:116-122. doi: 10.1016/j.clinbiomech.2018.07.012. Epub 2018 Jul 19.
4. Lansade C, Vicaut E, Paysant J, Ménager D, Cristina MC, Braatz F, Domayer S, Pérennou D, Chiesa G. Mobility and safety with a microprocessor-controlled knee in moderately active amputees: A multi-centric randomized crossover trial. Ann Phys Rehabil Med, 2018 May 14. pii: S1877-0657(18) 30058-7. doi: 10.1016/ j.rehab.2018.04.003. [Epub ahead of print] View Article
5. Mileusnic MP, Hahn A, Reiter S. Effects of a novel microprocessor-controlled knee, Kenevo, on the safety, mobility, and satisfaction of lower-activity patients with transfemoral amputation. J Prosthet Orthot 2017;29(4):198-205.
6. Kannenberg A, Zacharias B, Pröbsting E. Benefits of microprocessor prosthetic knees to limited community ambulators: A systematic review. J Rehabil Res Dev 2014;51(10):1469-1495. View Article
Kenevo Reimbursement Guide Executive Summary
Kenevo Reimbursement Guide | Executive Summary | Ottobock 4 of 4
7. Kahle JT, Highsmith MJ, Hubbard SL. Comparison of Non-microprocessor Knee Mechanism versus C-Leg on Prosthesis Evaluation Questionnaire, Stumbles, Falls, Walking Tests, Stair Descent, and Knee Preference; J Rehabil Res Dev 2008;45(1):1-14. View Article
8. Hafner BJ, Smith DG. Differences in function and safety between Medicare Functional Classification Level-2 and -3 transfemoral amputees and influence of prosthetic knee joint control. J Rehabil Res Dev 2009;46(3):417-434. View Article
9. Theeven P, Hemmen B, Rings F, Meys G, Brink P, Smeets R, Seelen H. Functional added value of microprocessor controlled knee joints in daily life performance of Medicare Functional Classification Level-2 amputees. J Rehabil Med. 2011;43(10):906–15. [PMID:21947182] View Article
10. Theeven PJ, Hemmen B, Geers RP, Smeets RJ, Brink PR, Seelen HA Influence of advanced prosthetic knee joints on perceived performance and everyday life activity of low-functional persons with a transfemoral amputation or knee disarticulation. J Rehabil Med 2012, 44 (5): 454-461. View Article
11. Burnfield JM, Eberly VJ, Gronely JK, Perry J, Yule WJ, Mulroy SJ Impact of stance phase microprocessor-controlled knee prosthesis on ramp negotiation and community walking function in K2 level transfemoral amputees. Prosthet Orthot Int 2012, 36 (1): 95-104. View Article
12. Eberly VJ, Mulroy SJ, Gronley JK, Perry J, Burnfield JM: Impact of a stance phase microprocessor-controlled knee prosthesis on level walking in lower functioning individuals with transfemoral amputation. Prosth Orthot Int 2014; 38(6): 447-455. View Article
13. Florence CS, Bergen G, Atherly A, Burns ER, Stevens JA, Drake C. Medical costs of fatal and nonfatal falls in older adults. J Am Geriatr Soc 2018;66:693-698. View Article
14. Burns ER, Stevens JA, Lee R. The direct costs of fatal and nonfatal falls among older adults – United States. J Safety Res 2016;58:99-103. View Article
15. Veteran’s Administration, Department of Defense. VA/DoD Clinical Practice Guideline for Rehabilitation of Individuals with Lower Limb Amputation. Version 2.0. 2017 (September 2017). Accessed on June 4, 2018. View Guideline
16. Samuelsson KA, Toytari O, Salminen AL, Brandt A. Effects of lower limb prosthesis on activity,participation, and quality of life: A systematic review. Prosthet Orthot Int. Jun 2012;36(2):145-158. View Article
17. CMS.gov. Lower Limb Prosthetic Workgroup Consensus Document. Accessed on 07/05/2018. View Consensus Document
Recent Guidance for LL Prosthetics
Kenevo Reimbursement Guide | Recent Guidance for LL Prosthetics | Ottobock 1 of 4
Centers for Medicare & Medicaid Services (CMS) Lower Limb Prosthetic Workgroup Consensus Document September 2017
A workgroup consisting of members from Centers for Medicare and Medicaid (CMS), National Institute of Health (NIH), Extremity Trauma and Amputation Center of Excellence (EACE), Administration for Community Living, Walter Reed National Military Center, and Department of Veterans Affairs (VA) issued a consensus statement that acknowledged an amputee functioning at the K2 level may benefit from MPK technology, and included the following clarifications of the K-Level descriptions.
“Level 0: Does not have the ability or potential to ambulate or transfer safely with or without assistance and a prosthesis does not enhance their quality of life or mobility.
a. The individual does not have sufficient cognitiveability to safely use a prosthesis with or withoutassistance.
b. The individual requires assistance fromequipment or caregiver in order to transfer anduse of a prosthesis does not improve mobility orindependence with transfers.
c. The individual is wheelchair dependent formobility and use of a prosthesis does notimprove transfer abilities.
d. The individual is bedridden and has no need orcapacity to ambulate or transfer.
Note: If a beneficiary has need of a lower limb prosthesis (LLP) to maintain sitting balance in an appropriately fitted wheelchair, but cannot ambulate or transfer using the prosthetic, the individual may be a candidate for a prosthesis which correlates with K1 activities. Example: A beneficiary with a trans-femoral amputation as well as a spinal cord injury (T4 ASIA B paraplegia) which precludes bi-pedal ambulation or weight bearing during transfers, depends on the resistance of the prosthetic
socket portion to maintain sitting balance. Though this individual may exhibit the functional abilities consistent with K0, s/he may be a candidate for a prosthesis typically provided to a beneficiary with K1 activity abilities.
Level 1: Has the ability or potential to use a prosthesis for transfers or ambulation on level surfaces at fixed cadence, typical of the limited and unlimited household ambulator.
a. The individual has sufficient cognitive ability tosafely use a prosthesis with or without anassistive device and/or theassistance/supervision of one person.
b. The individual is capable of safe but limitedambulation within the home or on a similar flatsurface like a home, with or without an assistivedevice and/or with or without theassistance/supervision of one person.
c. The individual requires the use of a wheelchairfor most activities outside of their residence.
d. The individual is not capable of most of thefunctional activities designated in Level 2.
Level 2: Has the ability or potential for ambulation with the ability to transverse low level environmental barriers such as curbs, stairs or uneven surfaces. This level is typical of the limited community ambulator.
a. The individual can, with or without an assistivedevice (which may include one or two handrails)and/or with or without theassistance/supervision of one person:
1. Perform the Level 1 tasks designated above2. Ambulate on a flat, smooth surface (e.g.,
concrete, asphalt) such as might be foundoutside the home. (e.g., porch, deck, patiogarage, driveway)
3. Negotiate a curb4. Access public or private transportation5. Negotiate 1-2 stairs6. Negotiate a ramp built to ADA
specifications.
Recent Guidance for LL Prosthetics
Kenevo Reimbursement Guide | Recent Guidance for LL Prosthetics | Ottobock 2 of 4
b. The individual may require a wheelchair for distances that are beyond the perimeters of the yard/driveway, apartment building, etc.
c. The individual is only able to increase his/her generally observed speed of walking for short distances or with great effort.
d. The individual is generally not capable of accomplishing most of the tasks at Level 3 (or does so infrequently with great effort).
Level 3: Has the ability or potential for ambulation with variable cadence, typical of the community ambulator who has the ability to transverse most environmental barriers and may have vocational, therapeutic, or exercise activity that demands prosthetic utilization beyond simple locomotion. a. With or without an assistive device (which may
include one or two hand rails), the individual is independently capable (i.e. requires no personal assistance or supervision) of performing the Level 2 tasks above and can:
1. Walk on terrain that varies in texture and level (e.g., grass, gravel, uneven concrete)
2. Negotiate 3-7 consecutive stairs 3. Walk up/down ramps built to ADA
specifications 4. Open and close doors 5. Ambulate through a crowded area (e.g.,
grocery store, big box store, restaurant) 6. Cross a controlled intersection within
his/her community within the time limit provided (varies by location)
7. Access public or private transportation 8. Perform dual ambulation tasks (e.g. carry
an item or meaningfully converse while ambulating)
b. The individual does not perform the activities of Level 4.
Note: If the beneficiary can accomplish the physical tasks described by the K3 level, but requires personal assistance or supervision due to cognitive, sensory or communicative disability, then the
individual is a candidate for a prosthesis which correlates with K3 usage. Example: In addition to the lower limb amputation, if the beneficiary has also experienced a TBI and is capable of performing the above K3 activities, but frequently needs supervision and assistance for safety purposes and redirection of attention, then s/he is a candidate for a prosthesis which correlates with K3 usage. Level 4: Has the ability or potential for prosthetic ambulation that exceeds the basic ambulation skills, exhibiting high impact, stress or energy levels typical of the prosthetic demands of the child, active adult, or athlete. With or without an assistive device (which may include one or two hand rails), this individual is independently capable (i.e. requires no personal assistance or supervision) of performing high impact domestic, vocational or recreational activities such as: a. Running b. Repetitive stair climbing c. Climbing of steep hills d. Being a caregiver for another individual e. Home maintenance (e.g. repairs, cleaning) Note: If the beneficiary can accomplish the physical tasks described by the K4 level, but requires personal assistance or supervision due to cognitive, sensory or communicative disability, then the individual is a candidate for a prosthesis which correlates with K4 usage. Example: The beneficiary exhibits a significant visual impairment in addition to a lower limb amputation. Though s/he demonstrates no other significant co-morbidities, and performs physically at a very high level (e.g., running, climbing stairs), he sometimes requires supervision for safety. S/he is a candidate for a prosthesis which correlates with K4 usage. The Workgroup also suggests that exceptions be considered if additional documentation is included
Recent Guidance for LL Prosthetics
Kenevo Reimbursement Guide | Recent Guidance for LL Prosthetics | Ottobock 3 of 4
which justifies a medical need for componentry in an individual who does not necessarily “fit” the K Level descriptions (e.g., bilateral amputees cannot be strictly held to the K level system). Please note: Not all traits listed for K levels must be realized by the patient in order to receive a K level assignment, but generally, documentation should demonstrate that equivalent activities can be achieved by the prosthetic user.”
Reference CMS.gov. Lower Limb Prosthetic Workgroup Consensus Document. Accessed on 07/05/2018 at: https://www.cms.gov/Center/Special-Topic/Medicare-Coverage-Center.html?redirect=/center/coverage.asp .
Department of Veterans Affairs Department of Defense VA/DoD clinical practice guideline for rehabilitation of individuals with lower limb amputation. Version 2. Sept 2017:39Accessed athttps://www.healthquality.va.gov/guidelines/Rehab/amp/VADoDLLACPG092817.pdf
“C. Pre-Prosthetic Phase. Recommendation [#15] We suggest offering microprocessor knee units over non-microprocessor knee units for ambulation to reduce risk of falls and maximize patient satisfaction.”
Discussion According to two fair quality SRs, microprocessor knees may reduce risk of falls and maximize patient satisfaction in limited and unlimited community ambulators.[93,94] Both reviews reported a decrease in stumble and fall frequency with accommodation and use of a microprocessor knee system relative to a non-microprocessor knee system.[93,94] The studies further support the prescription of microprocessor knees over non-microprocessor knees to improve an individual’s ability to walk faster on level ground, uneven surfaces, and downhill, thus providing the user with an improved sense of security and improved overall satisfaction.[93,94] The Work Group considered that the benefits to the patients, particularly decreasing risk of falling, far outweigh potential harms. The patient focus group participants also expressed a desire to have access to prosthetic devices that fit well and maximize their safety and function, so patient values and preferences were another important consideration when assessing the strength of the recommendation.
Falling is a major issue in patients with transfemoral amputations. Increased number of falls, fear of falling, as well as deterioration in balance, coordination, and endurance, resulting in activity avoidance, decreased independence and mobility have all been reported in this population.[93]
Recent Guidance for LL Prosthetics
Kenevo Reimbursement Guide | Recent Guidance for LL Prosthetics | Ottobock 4 of 4
Therefore, the prescription of microprocessor knees is supported for ambulatory individuals with complex medical conditions affecting balance, as well as for the geriatric population. These populations benefit from microprocessor knees, which have been demonstrated to decrease stumbles and prevent falls by an SR included in our evidence review[93] and two SRs that were excluded because they were superseded by a more recent and comprehensive SR.[95,96] There is insufficient evidence to support using one type of microprocessor knee over another, but the provider should consider the many characteristics of each type of knee when making a selection. Most importantly, the potential impact on the patient’s functional level should be considered as there are a variety of microprocessor knee options available. Some knees may be best suited for the limited community ambulator[93] while others are more appropriate for the highly active patient.[72,97,98] Another consideration when choosing the right microprocessor knee for an individual is the mechanism of charging the knee; some have removable batteries, others have a port for a plug, while others have inductive charging systems. Still another consideration would be the default mode of the device when the power source is depleted. Some knees default to a locked knee while others default to free swing.” (Page 39) References: 72 Highsmith MJ, Kahle JT, Miro RM, et al. Prosthetic interventions for people with transtibial amputation: Systematic review and meta-analysis of high-quality prospective literature and systematic reviews. J Rehabil Res Dev. 2016;53(2):157-184. 93 Kannenberg A, Zacharias B, Probsting E. Benefits of microprocessor-controlled prosthetic knees to limited community ambulators: Systematic review. J Rehabil Res Dev. 2014;51(10):1469-1496.
94 Samuelsson KA, Toytari O, Salminen AL, Brandt A. Effects of lower limb prosthesis on activity, participation, and quality of life: A systematic review. Prosthet Orthot Int. Jun 2012;36(2):145-158. 95 Highsmith MJ, Kahle JT, Bongiorni DR, Sutton BS, Groer S, Kaufman KR. Safety, energy efficiency, and cost efficacy of the C-Leg for transfemoral amputees: A review of the literature. Prosthet Orthot Int. Dec 2010;34(4):362-377. 96 Sawers AB, Hafner BJ. Outcomes associated with the use of microprocessor-controlled prosthetic knees among individuals with unilateral transfemoral limb loss: A systematic review. J Rehabil ResDev. 2013;50(3):273-314. 97 Hafner BJ, Willingham LL, Buell NC, Allyn KJ, Smith DG. Evaluation of function, performance, and preference as transfemoral amputees transition from mechanical to microprocessor control of the prosthetic knee. Arch Phys Med Rehabil. Feb 2007;88(2):207-217. 98 Kahle JT, Highsmith MJ, Hubbard SL. Comparison of nonmicroprocessor knee mechanism versus C-Leg on Prosthesis Evaluation Questionnaire, stumbles, falls, walking tests, stair descent, and knee preference. J Rehabil Res Dev. 2008;45(1):1-14.
Kenevo Reimbursement Guide Product Information
Kenevo Reimbursement Guide | Product Information | Ottobock 1 of 1
Kenevo Coding1 (U.S. only) The Healthcare Common Procedure Coding System (HCPCS) for prosthetics is an add-on code system. Rather than issuing new HCPCS Level II national codes to describe the various microprocessor knees that came to market, the Alpha-Numeric HCPCS Panel instead issued add-on codes to upgrade the mechanical (non-microprocessor) knee codes.
The following codes apply to Kenevo: L5828 Hydraulic Swing and Stance Phase
Knee (base mechanical knee code) L5845 Stance flexion feature L5848 Stance extension damping feature L5858 Microprocessor control feature, stance
phase, includes sensors L5850 Knee extension assist feature L59992 Inertial Motion Unit Control feature for
intuitive standing and walking backwards.
Kenevo Replacement Battery and Charger: L7367 Lithium Ion Battery, Replacement L7368 Lithium Ion Battery Charger,
Replacement
2019 Manufacturer Suggested Retail Price (MSRP)3 (U.S. only) MSRP for the Inertial Motion Unit code (L5999) is $5000.
FDA Status Under FDA’s regulations, the Kenevo Microprocessor-Controlled Prosthetic Knee is a Class I device, exempt from the premarket notification [510(k)] requirements. The Kenevo prosthetic knee has met all applicable control requirements which include Establishment Registration (21CFR 807), Medical Device Listing (21 CFR part 807), Quality System Regulation (21CFR part820), Labeling (21CFR part 801), and Medical Device Reporting (21 CFR Part 803). The Kenevo prosthetic knee is listed under JOINT, KNEE, EXTERNAL LIMB COMPONENT; Listing Number is E253231 and Manufacturer Registration Number is 3005190268.
Health Canada Compliance This device meets the requirements of the Medical Device Regulations (SOR/98-282). It has been classified as a class I medical device according to the classification criteria outlined in schedule 1 of the Medical Device Regulations.
Warranty Kenevo comes with a three-year manufacturer warranty (extendable to six years) which includes a complimentary condition-based service inspection within the 3-year term. During the warranty period, repair costs are covered except for those associated with damages resulting from improper use.
Who Can Provide a Kenevo? The Kenevo is prescribed by a physician and may only be provided by a qualified Prosthetist who has received specific product training. Ottobock employs a team of orthotists and prosthetists to educate practitioners on fabricating and fitting our products. This includes in-person and online training, webinars, and technical bulletins. We also provide Cooperative Care Services for the more challenging fittings, which includes on-site assistance with the fitting in conjunction with product qualification training for the practitioner.
1 The product/device “Supplier” (defined as an O&P practitioner, O&P patient care facility, or DME supplier) assumes full responsibility for accurate billing of Ottobock products. It is the Supplier’s responsibility to determine medical necessity; ensure coverage criteria is met; and submit appropriate HCPCS codes, modifiers, and charges for services/products delivered. It is also recommended that Supplier’s contact insurance payer(s) for coding and coverage guidance prior to submitting claims. Ottobock Coding Suggestions and Reimbursement Guides are based on reasonable judgment and are not recommended to replace the Supplier’s judgment. These recommendations may be subject to revision based on additional information or alpha-numeric system changes. 2 It is not recommended to bill L5999 to Medicare for Microprocessor Knees. 3 The manufacturer’s suggested retail pricing (MSRP) is a suggested retail price only. Ottobock has provided the suggested MSRP in the event that third-party and/or federal healthcare payers request it for reimbursement purposes. The practitioner and/or patient care facility is neither obligated nor required to charge the MSRP when submitting billing claims for third-party reimbursement for the product (s).
Kenevo Features and Benefits
Kenevo Reimbursement Guide | Features and Benefits | Ottobock 1 of 3
Microprocessor Stance Control Kenevo´s main microprocessor gathers sensoric information at a rate of 100 times per second. It processes this information following programmed instructions to adjust the valve positions via servo motors in real time. The valve positions define the hydraulic fluid resistance of the two independent valves (extension and flexion valves) and therefore the resistances of the knee against flexion and extension separately and variably.
Kenevo is a default stance knee, which means that it always has high stance flexion resistance to support the body weight until stance is disengaged. Its microprocessor stance control monitors each step to reliably detect the safest moment to release swing. This ensures safe body weight support even for the highly variable gait patterns of patients with low mobility and walking aid use. In addition, the microprocessor stance control provides Stumble Recovery Plus and supported sit-to-stand and stand-to-sit functions.
Stumble Recovery Plus Kenevo delivers unmatched safety for your K2 patients through the implementation of Stumble Recovery Plus. After heel rise, as soon as the shank starts the extension movement during the swing phase, Kenevo activates high flexion resistance that is even higher than that adjusted for control of the regular stance phase. This stumble recovery allows the patient to fully load the prosthesis in case of a trip and represents the highest level of safety that is technically possible. Benefits include:
Reduced risk of falling: if the user trips, it iseasier to regain his or her balance
The increased safety can increase the user'sconfidence in the prosthesis
Taking steps backward is possible withconsistently high level of safety
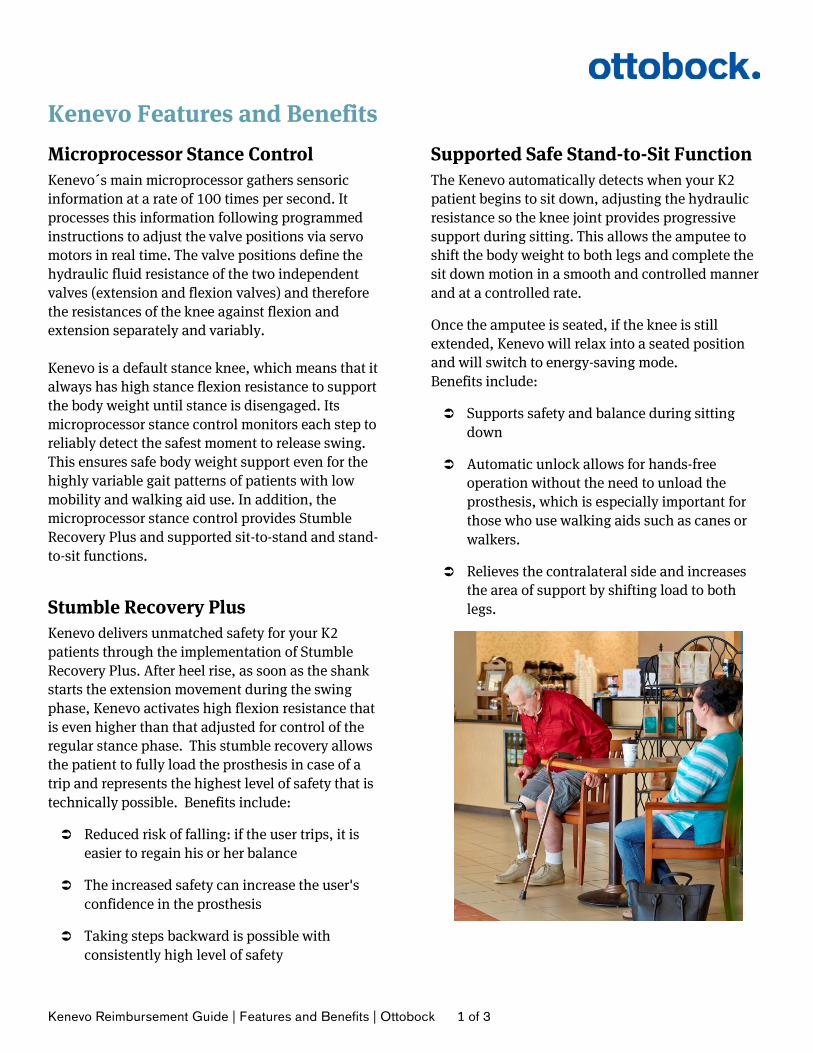
Supported Safe Stand-to-Sit Function The Kenevo automatically detects when your K2 patient begins to sit down, adjusting the hydraulic resistance so the knee joint provides progressive support during sitting. This allows the amputee to shift the body weight to both legs and complete the sit down motion in a smooth and controlled manner and at a controlled rate.
Once the amputee is seated, if the knee is still extended, Kenevo will relax into a seated position and will switch to energy-saving mode. Benefits include:
Supports safety and balance during sittingdown
Automatic unlock allows for hands-freeoperation without the need to unload theprosthesis, which is especially important forthose who use walking aids such as canes orwalkers.
Relieves the contralateral side and increasesthe area of support by shifting load to bothlegs.
Kenevo Features and Benefits
Kenevo Reimbursement Guide | Features and Benefits | Ottobock 2 of 3
Supported Safe Sit-to-Stand Function The Kenevo also automatically detects when the patient begins to stand up.
If the patient pauses during the standing-up motion, the knee will not collapse as long as the patient has made it at least half way (prosthesis has reached at least 45° flexion), which allows the patient to rest on the prosthesis and reposition their weight to the sound limb if standing up in a single motion is too tiring.
The knee switches automatically to Supported Stand-to-sit function if the patient tends to fall backward.
Inertial Motion Unit (IMU) Control Backward Walking This patented microprocessor control technology provides safety and stability when your K2 patient is forced to step backwards (such as when opening a door). Many microprocessor knees do not accommodate backward stepping, which may cause the knee to collapse if a backward step is taken.
Intuitive Standing Maintaining safety and balance while standing is critical for K2 patients. Kenevo allows the patient to intuitively stand on a flexed and stable knee when on level, uneven, or inclined surfaces (e.g. ramps and hills).
Contrast this to traditional K2 prosthetic knees, which require the user to extend the hip to stabilize the knee or cognitively ensure that their center of mass stays ahead of their knee axis to prevent unexpected buckling of the prosthetic knee.
Unlike mechanical knees, Kenevo offers clinicians a range of programmable stance stability options that can be customized to support each patient’s individual capabilities.
Hydraulic Swing and Stance Hydraulic Stance Control Hydraulic stance control provides resistance against knee flexion to support the body weight of the patient and prevent knee collapse. Knee flexion during weight-bearing is damped and controlled, mimicking the eccentric contraction of the quadriceps muscle during gait, to provide for shock absorption during level walking to minimize hip and low-back stress. It also enables step-over-step slope and stair descent and uneven terrain ambulation, allowing patients to “ride” the knee when descending stairs and slopes.
Hydraulic Swing Control The hydraulic swing phase control of Kenevo accommodates walking speeds of up to 3 km/h (1.9 mph). It also provides for terminal swing extension damping that prevents a hard terminal impact that would be hard to control for the patient by decelerating the prosthetic shank prior to heel strike. This mimics the eccentric contraction of the anatomical hamstrings and gluteus maximus muscle. Full extension is then reached smoothly in preparation for heel strike.
Kenevo Features and Benefits
Kenevo Reimbursement Guide | Features and Benefits | Ottobock 3 of 3
Hydraulic Stance Extension Damping After the knee is flexed during stance phase (stance flexion), it needs to extend again to advance the body forward through mid-stance. This feature provides a smooth extension of knee. Without this function, the patient would feel a pronounced “snap back” or “jerk” at the knee, and would also present with an unnaturally looking gait pattern. Energy is conserved by having this feature, as the patient will not have to attempt to control this motion with his residual limb muscles.
Knee Extension Assist The knee extension assist is used in promoting knee extension at the beginning of swing phase extension. This function allows the user to walk more efficiently at variable cadence since the spring extension assist mechanically limits the knee flexion at the end range and begins to bring the knee into extension for a more symmetrical gait at faster walking speeds. It also ensures the knee comes to full extension for the beginning of stance phase for a more secure loading condition during level walking but in particular when descending stairs where full extension facilitates the positioning of the foot on the edge of a stair.
JRRDJRRD Volume 51, Number 10, 2014
Pages 1469–1496
Benefits of microprocessor-controlled prosthetic knees to limited community ambulators: Systematic review
Andreas Kannenberg, MD, PhD;1* Britta Zacharias, Dipl-Ing (FH), CPO;2 Eva Pröbsting, Dipl-Ing (FH), CPO2
1Medical Affairs, Otto Bock HealthCare LP, Austin, TX; 2Clinical Research and Services, Otto Bock HealthCare GmbH, Duderstadt, Germany
Abstract—The benefits of microprocessor-controlled pros-thetic knees (MPKs) have been well established in community ambulators (Medicare Functional Classification Level [MFCL]-3) with a transfemoral amputation (TFA). A system-atic review of the literature was performed to analyze whether limited community ambulators (MFCL-2) may also benefit from using an MPK in safety, performance-based function and mobility, and perceived function and satisfaction. We searched 10 scientific databases for clinical trials with MPKs and identi-fied six publications with 57 subjects with TFA and MFCL-2 mobility grade. Using the criteria of a Cochrane Review on prosthetic components, we rated methodological quality mod-erate in four publications and low in two publications. MPK use may significantly reduce uncontrolled falls by up to 80% as well as significantly improve indicators of fall risk. Perfor-mance-based outcome measures suggest that persons with MFCL-2 mobility grade may be able to walk about 14% to 25% faster on level ground, be around 20% quicker on uneven surfaces, and descend a slope almost 30% faster when using an MPK. The results of this systematic review suggest that trial fittings may be used to determine whether or not individuals with TFA and MFCL-2 mobility grade benefit from MPK use. Criteria for patient selection and assessment of trial fitting suc-cess or failure are proposed.
Key words: community ambulator, limited community ambu-lator, Medicare Functional Classification Level-2, micropro-cessor-controlled knees, mobility, MPK, non-microprocessor-controlled prosthetic knees, perceived function, performance-based function and mobility, safety, transfemoral amputation.
INTRODUCTION
Absence or amputation of a lower limb may be the life-altering consequence of congenital deficiency, trauma, malignancy, peripheral vascular disease, diabetic neuropathy, and other conditions. The risk of leg amputa-tion increases with age for all etiologies; however, vascu-lar disease accounts for up to 82 percent of lower-limb amputations [1]. A more proximal amputation results in greater physical and functional impairment to the indi-vidual, including a decreased likelihood of regaining household or community ambulation and an increased
Abbreviations: 2MWT = 2-min walk test, ABC = Activity-specific Balance Confidence Scale, ADL = activity of daily living, AMP = Amputee Mobility Predictor, GRF = ground reaction force, ICR = instantaneous center of rotation, LCI = Locomotor Capabilities Index, MDC = minimal detectable change, MFCL = Medicare Functional Classification Level, MP = microprocessor, MPK = microprocessor-controlled pros-thetic knee, NMPK = non-microprocessor-controlled prosthetic knee, PEQ = Prosthesis Evaluation Questionnaire, RCT = ran-domized controlled trial, TFA = transfemoral amputation, TUG =Timed “Up and Go” test.*Address all correspondence to Andreas Kannenberg, MD,PhD; Otto Bock HealthCare LP, Riata Business Park,Building 8, Suite 250, 12365-B Riata Trace Pkwy, Austin,TX 78727; 763-489-5105; fax: 763-519-6153. Email: [email protected]://dx.doi.org/10.1682/JRRD.2014.05.0118
1469
1470
JRRD, Volume 51, Number 10, 2014
risk of falling in subjects with above-knee as compared with below-knee amputation [2–13]. According to a con-solidation of recent epidemiological studies, the popula-tion of people with above-knee limb loss living in the United States may be as large as 400,000 [14–15].
Adequate selection of prosthetic components is one of the key processes to achieving the best possible reha-bilitation outcomes. In subjects with transfemoral ampu-tation (TFA), the prosthetic knee is a very important component tasked with restoring knee biomechanics while at the same time providing maximum stability and safety [16–19]. In the early 1990s, Medicare adopted the Medicare Functional Classification Levels (MFCLs), which are used to rate the person with amputation’s abil-ity and/or potential ability to ambulate. Shortly thereafter, based on the prosthetic knees available at that time, Medicare developed coverage criteria (indications/limita-tions and/or medical necessity) for prosthetic knees that were adapted to the MFCL. Medicare’s prosthetic knee coverage criterion has not been modified since its incep-tion and remains in effect today (Table 1) [20]. Addition-ally, the MFCL and coverage criteria have also been adopted by many third-party payors [21]. Fluid stance
control mechanisms available at that time were correctly considered too difficult to be safely operated by lower-functioning individuals, and the remaining traditional stance control mechanisms offered similar levels of inherent stability and support of function [16,22]. As a result, the coverage criteria for prosthetic knees were based on the ability and/or potential ability of subjects to vary cadence and walking speed as the decisive criterion for the selection of an appropriate swing control technol-ogy. As a consequence of these criteria, fluid control prosthetic knee mechanisms, regardless of their use for stance or swing control, have been reserved for usually younger persons with amputation of the higher MFCL-3 and MFCL-4 mobility grade.
In the past 15 yr, prosthetic technology has pro-gressed to microprocessor (MP)-controlled fluid stance as well as stance and swing control mechanisms to over-come the inverse relationship between stability and sup-port of function inherent in non-MP-controlled prosthetic knees (NMPKs). Clinical research, mainly conducted in the unlimited community ambulator (MFCL-3) popula-tion with low to moderate
K-Level Description Medicare Reimbursed ProsthesisK0 Nonambulatory: “Does not have the ability or potential
to ambulate or transfer safely with or without assis-tance and a prosthesis does not enhance quality of life or mobility.”
None
K1 Household Ambulator: “Has the ability or potential to use a prosthesis for transfers or ambulation on level surfaces at fixed cadence.”
Constant Friction Knee
K2 Limited Community Ambulator: “Has the ability or potential for ambulation with the ability to traverse low-level environmental barriers such as curbs, stairs, or uneven surfaces.”
Constant Friction Knee
K3 Unlimited Community Ambulator: “Has the ability or potential for ambulation with variable cadence. Typi-cal of the community ambulator who has the ability to traverse most environmental barriers and may have vocational, therapeutic, or exercise activity that demands prosthetic utilization beyond simple locomo-tion.”
Fluid Control Knee, Non-MP or MP-Controlled Knee
K4 Very Active: “Has the ability or potential for prosthetic ambulation that exceeds the basic ambulation skills, exhibiting high impact, stress, or energy levels, typical of the prosthetic demands of the child, active adult, or athlete.”
Fluid Control Knee, Non-MP or MP-Controlled Knee
methodological quality, has
Table 1. Definition of Medical Function Classification Level (or K-levels) and Medicare Guidelines for Covered Prostheses by K-level of mobility [20].
MP = microprocessor.

1471
KANNENBERG et al. Benefits of MPKs to limited community ambulators
demonstrated improved safety and superior function of MP-controlled prosthetic knees (MPKs) [23] in level walking [24–30], walking on uneven terrain [24–26,31–32], walking on slopes [21,26,33–34], walking on stairs [25,31,35], and stumble recovery [24–25], resulting in significantly reduced numbers of stumbles and falls and improved balance than with NMPKs [24–26,31,34,36].
With current coverage criteria restricting the provi-sion of advanced prosthetic technology to usually younger, healthier, higher-functioning individuals, lower-limb prosthetics finds itself on a different pathway than other fields of healthcare. Typically, most advanced healthcare technologies serve the oldest, sickest, and most restricted patients, as reflected by the fact that 80 percent of lifetime healthcare expenditures are incurred in the second half of life [37] with a substantial share of these accruing in the last year before death [38–40]. Today, the majority of patients undergoing a TFA are over the age of 65 yr [1,41–43] and do not reach the level of unlimited community ambulation [13] using the pros-thetic knees covered under current Medicare criteria, which are simple in technology, limited in function, and often developed decades ago. These findings raise the question whether limited community ambulators (MFCL-2) may also benefit more from using MPKs than from NMPKs as has been demonstrated in unlimited community ambulators (MFCL-3). We therefore con-ducted a systematic review of randomized and nonran-domized clinical trials comparing the effects of NMPK and MPK interventions in limited community ambulators (MFCL-2) with a unilateral TFA in three clinically mean-ingful areas.
First, falling is a major issue in this population [8,44–45], and recurrent falls and fear of falling are associated with functional limitations and deterioration in balance, coordination, and endurance, resulting in activity avoid-ance and decreased independence and mobility [46–50]. Falling and its detrimental consequences pose serious clinical challenges for persons with amputation, espe-cially elderly, lower-functioning individuals who often experience various comorbidities and physical decon-ditioning [44–45]. Therefore, the evaluation of perfor-mance-based and self-reported outcome measures would help assess the effect of MPK use on the safety of ambu-lation with the prosthesis.
Second, the goal of rehabilitation is to enable patients to resume a lifestyle as independent as possible. There-fore, the analysis of performance-based function and
mobility to appraise the person with amputation’s ability to perform household activities of daily living (ADLs) and activities required for community ambulation (e.g., walking on uneven terrain, slopes, and stairs) would allow for drawing conclusions on the effects of MPK use on function and overall mobility as indicators or prereq-uisites for an independent lifestyle and participation.
Third, the perception of function and satisfaction plays an important role on the behavior of patients, such as taking on or avoiding ADLs [9,46–47,51–54]. Thus, the evaluation of self-reported measures to assess per-ceived safety, function, and satisfaction with prosthesis use may allow for judging whether MPK use may create the basis for behavioral changes such as a more self-dependent lifestyle and an increase in general ambulation activity.
The specific outcome measures representing each clinical area of interest were defined a priori and are described in detail in the “Inclusion Criteria” section.
METHODS
Search StrategyThe systematic search of publications was conducted
on October 28 and 29, 2013, using the scientific literature databases Medline, EMBASE, and PsychInfo (all three accessed via DIMDI [German Institute for Medical Doc-umentation and Information]); DARE; Cirrie; CINAHL; Cochrane Library; OTseeker; PEDro; and RECAL Leg-acy. The databases were searched with terms related to MPKs and individuals with a unilateral TFA and MFCL-2 mobility grade. The search terms were combined into a title, abstract, and key word search phrase using Boolean operators, resulting in the following syntax: 1. Unilateral. 2. Femoral. 3. Transfemoral. 4. Above?knee. 5. Through?knee. 6. Knee?disarticulation. 7. Or/2–6. 8. Amput*. 9. Prosth*.10. Or/8–9.11. Microprocessor.12. MP*.
1472
JRRD, Volume 51, Number 10, 2014
13. Or/11–12.14. Knee.15. And/1,7,10,13,14.
The literature search was not extended to study types or specific outcome measures but limited to English- and German-language publications with no limit on the date of publication. In addition, the references of the analyzed full-text publications were searched for additional perti-nent published studies.
ScreeningThe titles and abstracts of the publications found
were independently screened by two authors (A.K. and B.Z.) with regard to inclusion and exclusion criteria to classify them as relevant, not relevant, or possibly rele-vant. Full articles were reviewed for all publications clas-sified as relevant or possibly relevant. Disagreements on references of possible relevance were settled by third author (E.P.) review, and joint discussion of full-text arti-cles occurred among all three authors for final agreement on the classification of relevance of the article.
Inclusion CriteriaInclusion criteria included—
1. Randomized or nonrandomized comparative study that includes a prosthetic knee intervention with compari-son of results of an MPK with those of one or more NMPKs.
2. Study that reports results of individuals with a unilat-eral TFA or knee disarticulation classified as MFCL-2 mobility grade either as the target study group, as a subgroup analysis, or as raw data that permits a post hoc analysis of the MFCL-2 subgroup of the study sample.
3. Study that uses and reports quantifiable results of objective and/or self-reported outcome measures in the areas of safety, function and mobility, and perceived function and satisfaction with the prosthesis. The included studies were explicitly screened for, but not limited to, the following outcome measures as vali-dated representatives for the areas of clinical interest of this review:
a. Safety: Outcomes measures validated for assessing the risk of falling in individuals with lower-limb amputation, such as the self-reported number of stumbles and falls within a defined period of time [55–56], Timed “Up and Go” test (TUG) [57–61], Four Square Step Test [62], Berg Balance Scale
[63–64], obstacle avoidance test [65], Activity-specific Balance Confidence Scale (ABC) [6,66–68], Locomotor Capabilities Index (LCI) advanced score [62], and Prosthesis Evaluation Questionnaire (PEQ) Addendum [34].
b. Performance-based function and mobility: MFCL classification if determined with all prosthetic inter-ventions and validated outcome measures that objectively assess the physical abilities of subjects with lower-limb amputation, such as the Amputee Mobility Predictor (AMP) with and without pros-thesis [69], timed walk tests on level ground [70–71] and uneven terrain [31], the Assessment of Daily Activity Performance in Transfemoral Amputees test for assessing performance in ADLs [72], divided attention tests while walking [34], performance and gait characteristics in slope and stair negotiation such as the Hill and Stair Assess-ment Indices [34], motion analysis [24,35,73–74], or the Montreal Rehabilitation Performance Profile [31,75].
c. Perceived function and satisfaction: Validated self-reported outcome measures such as the PEQ [76–77], Orthotic and Prosthetic Users’ Survey [78], LCI [79–80], Amputee Activity Score [81], Func-tional Measure for Amputees [82–83], Houghton Scale [82,84–85], Prosthetic Profile of the Amputee [82], Orthotics and Prosthetics National Outcomes Tool [82,86], Special Interest Group in Amputation Medicine score [87], and Trinity Amputation and Prosthesis Experience Scales [88–89].
Exclusion CriteriaExclusion criteria included—
1. Studies with implantable knee joints (total knee arthro-plasty or replacement).
2. Studies with patients with a bilateral amputation or an amputation level higher than transfemoral or lower than knee disarticulation.
3. Studies that only report opinions or judgments of the authors but no data that allow for an independent reappraisal.
4. Duplicate article.
Assessment of Methodological QualityAfter screening and sorting articles for pertinence to
the subject of this review, methodological quality and risk of bias were separately assessed by two authors
1473
KANNENBERG et al. Benefits of MPKs to limited community ambulators
(A.K. and B.Z. or E.P.) using the checklist of a Cochrane Systematic Review on prosthetic ankle-foot mechanisms published by Hofstad et al. [90]. It is based on two exist-ing scales for methodological quality assessment of ran-domized controlled trials (RCTs) of van Tulder et al. [91] and Verhagen et al. [92] but was adapted to also evaluate internal and external validity as well as the risk of bias of nonrandomized studies as recommended by Downs and Black [93], Reisch et al. [94], and Zaza et al. [95]. We are not aware of any RCTs in prosthetic research, which is confirmed by the results of a recent systematic review of the entire prosthetic literature [96]. We therefore believe that the scale of Hofstad et al. [90], accepted by the Cochrane Collaboration, is an appropriate tool to assess the methodological quality of clinical trials in prosthetics. The Hofstad checklist comprises 13 criteria for method-ological quality that are all scored using one out of three possible levels: no = 0, yes = 1, or not applicable.
Criteria for Methodological Quality
Selection of PatientsA1. Adequate description of inclusion and exclusion
criteria (with a minimum of three of the following descriptors: age, amputation level, etiology, level of activity, time since amputation, residual limb condition, comorbidities, and sex)?
A2. Homogeneity of the study groups (at least for age, etiology and level of the amputation, and mobility grade)?
A3. Prognostic comparability of the study sample (e.g., for etiology and level of amputation, age, sex, condi-tion of the residual limb, comorbidities, etc.; prognostic comparability is given by definition in within-subject stud-ies with every patient acting as his or her own control)?
A4. Randomization (randomized order of interven-tion: 1 point, randomization of patients to intervention and control groups [RCT]: 2 points)?
InterventionB5. Description of experimental intervention (can the
study be repeated)?B6. Control of cointerventions?B7. Blinding of patients and/or assessors?B8. Timing of measurement (adequate adaptation)?B9. Appropriateness of outcome measures to answer
the research question of the study?
Statistical ValidityC10. Attrition rate not exceeding 20 percent?C11. Adequate sample size (sample size calculation
and power analysis)?C12. Intention-to-treat analysis?C13. Data presentation (point estimates and mea-
sures of variability)?The rules for scoring the individual criteria were
reported in detail by Hofstad et al. [90] and have been strictly followed for this review.
Rating of Methodological Quality According to Hofstad et al. [90]
A grade (high quality). Minimum of 11 points in total, with at least 6 points in the patient selection (A) and intervention (B) criteria with valid scores in blinding (B7) and accommodation (B8).
B grade (moderate quality). Minimum of 6 points in total, with at least 6 points in the patient selection (A) and intervention (B) criteria with a valid score in accom-modation (B8).
C grade (low quality). Minimum of 6 points in total, with at least 6 points in the patient selection (A) and intervention (B) criteria with invalid scores in blinding (B7) and accommodation (B8).
Studies with a total score of less than 6 points were considered to have insufficient quality to be included in this systematic review.
Data ExtractionData extraction from each study included was con-
ducted independently by two reviewers (A.K. and B.Z. or E.P.) using a standardized, self-developed data extraction form that covered the design of the study; inclusion and exclusion criteria, number, age, and sex of the patients; the level and etiology of the amputation; type and sever-ity of comorbidities; control and study intervention; con-current therapies and other potential confounders; follow-up times; outcome measures and their results for every study group; raw data of individual patients, if reported; and the results of statistical comparisons between the study groups (p-values, confidence intervals, etc.). The outcome measures were grouped according to the predefined areas of safety, performance-based func-tion and mobility, and perceived function and satisfaction as described in detail in the “Inclusion Criteria” section.
Because the variability of patient characteristics withinthe MFCL-2 mobility grade is broad, an attempt was
1474
JRRD, Volume 51, Number 10, 2014
made to stratify the subjects based on two well-validated objective measures of the overall physical capabilities, the AMP [69] and the walking speed in timed walk tests [70–71,97] on the NMPK, because such stratification might possibly allow for relating differing results to dif-ferent levels of physical capabilities and thus help guide appropriate component selection.
Post Hoc Analyses, Data Pooling, and Meta-AnalysesRaw data of all subjects allowing for a post hoc sta-
tistical analysis of the MFCL-2 subgroup was reported by one study included in this review [31]. In another study, individual results of the AMP were reported but not sta-tistically analyzed for the different functional level sub-groups [21]. Due to the low patient numbers of n = 9 [31] and n = 8 [21], the post hoc statistical analyses were con-ducted using the Wilcoxon signed rank test with a power of 80 percent in WinSTAT for Excel (Microsoft Corpora-tion; Redmond, Washington). Differences between inter-ventions with a p < 0.05 were considered statistically significant.
Due to inhomogeneity in study designs, patient num-bers, acclimation times, and outcome measures assessed, data pooling and meta-analyses were not suitable.
RESULTS
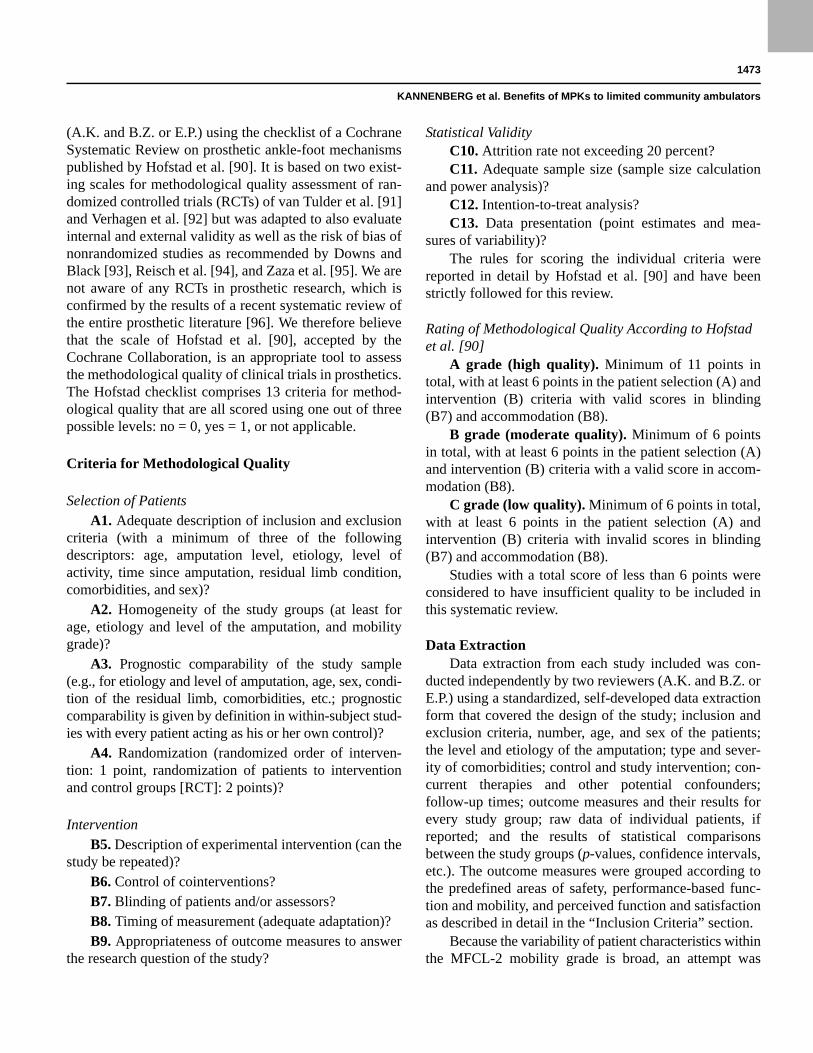
Literature SearchThe literature search found 986 citations in all data-
bases used. A total of 412 duplicates were identified and eliminated. Based on a review of the article titles, 501 publications were excluded as not pertinent. Then, the abstracts of the remaining 73 articles were analyzed to classify 46 as not pertinent, leaving 27 publications for full-text review, after which a further 20 publications were excluded as not pertinent (Figure). No additional pertinent citations were found in the references of the full-text articles. Thus, the literature search ultimately revealed seven publications on five clinical trials with subjects with a unilateral TFA and MFCL-2 mobility grade. Two clinical trials resulting in four publications exclusively studied individuals with MFCL-2 mobility grade [98–101], two studies reported subgroup analyses of MFCL-2 subjects [21,102], and one study reported individual raw data that permitted a post hoc analysis of the MFCL-2 subgroup [31]. Three studies investigated the effects of the MP stance and swing controlled C-Leg
[21,31,102], one study investigated the MP stance con-trolled C-Leg Compact [100–101], and one study investi-gated both the C-Leg and C-Leg
Figure.Flowchart of literature search and analysis.
Compact in randomized order [98–99].
Assessment of Methodological QualityAs expected, we have not been able to identify an
RCT with MPKs in individuals with a unilateral TFA and MFCL-2 mobility grade. The German-language publicationof Wetz et al. had to be excluded from further analysis
1475
KANNENBERG et al. Benefits of MPKs to limited community ambulators
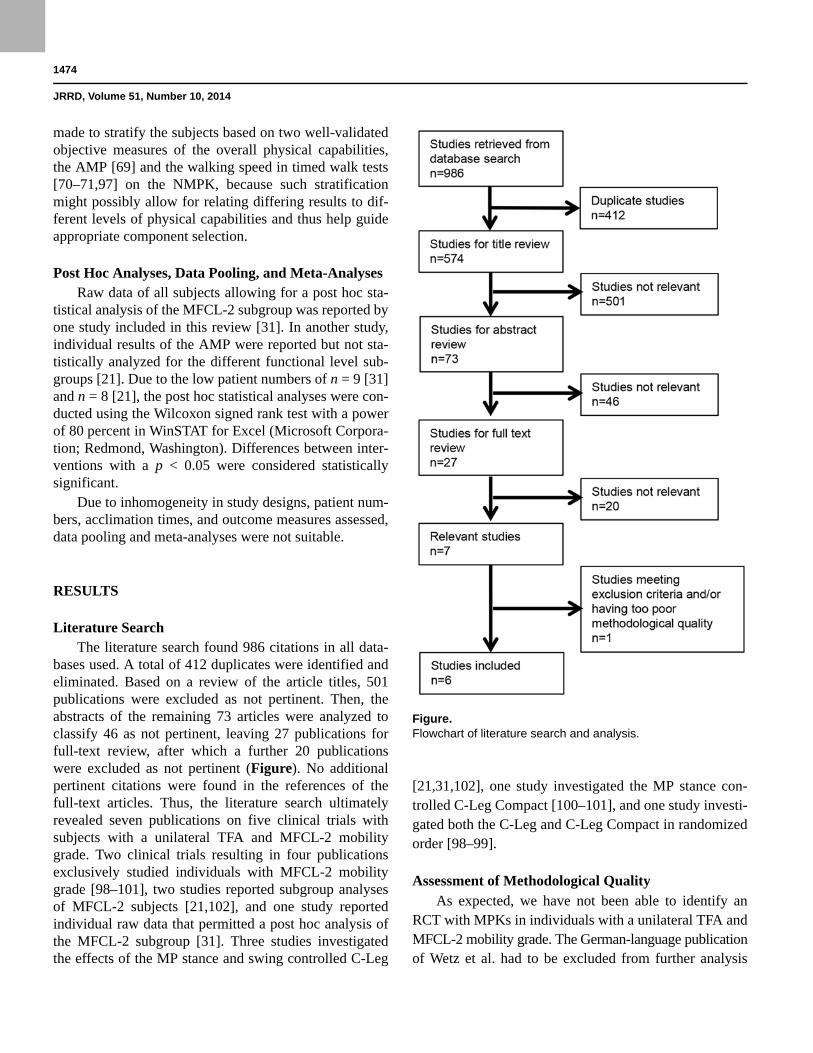
because it met predefined exclusion criterion number 3 [102]. This article only reported qualitative judgments of the authors on the benefits of individual subjects from using an MPK as compared with their existing NMPK after a 1 d trial fitting that did not allow for an indepen-dent reappraisal of the results. Nevertheless, it was included in the assessment of methodological quality, where it was found to not attain the minimum score to be included in further analyses. For the other six relevant publications identified in the literature search, method-ological quality was rated B (moderate) in four articles and C (low) in two articles (Table 2).
Moreover, a methodological uncertainty of all studies was the determination of the MFCL of the individuals. In all studies, only the everyday clinical practice of subjec-tive judgment of the prosthetist and/or physical therapist was used to assign the subjects to a certain MFCL. No study used a reproducible method such as the AMP [69] or the walking speed in timed walk tests [69,97] to sup-port this determination. One study assessed the AMP but did not use it to determine the mobility grade [21]. The individual AMP values ranged from 34 to 41, with most values exceeding 36, the currently recommended upper cutoff for MFCL-2. However, in the original publication of Gailey et al., the mean and standard deviation of AMP values across the MFCL-2 patient sample was 34.65 ± 6.49, with a range of 19 to 41 [69]. The other studies assessed the fastest possible walking speed in timed walk tests [31,98–99] or during motion analysis [100–101]. Because a walking distance of up to 150 m in the 2-min walk test (2MWT) (equals a walking velocity of up to4.5 km/h or 1.25 m/s) is still indicative of limitations of
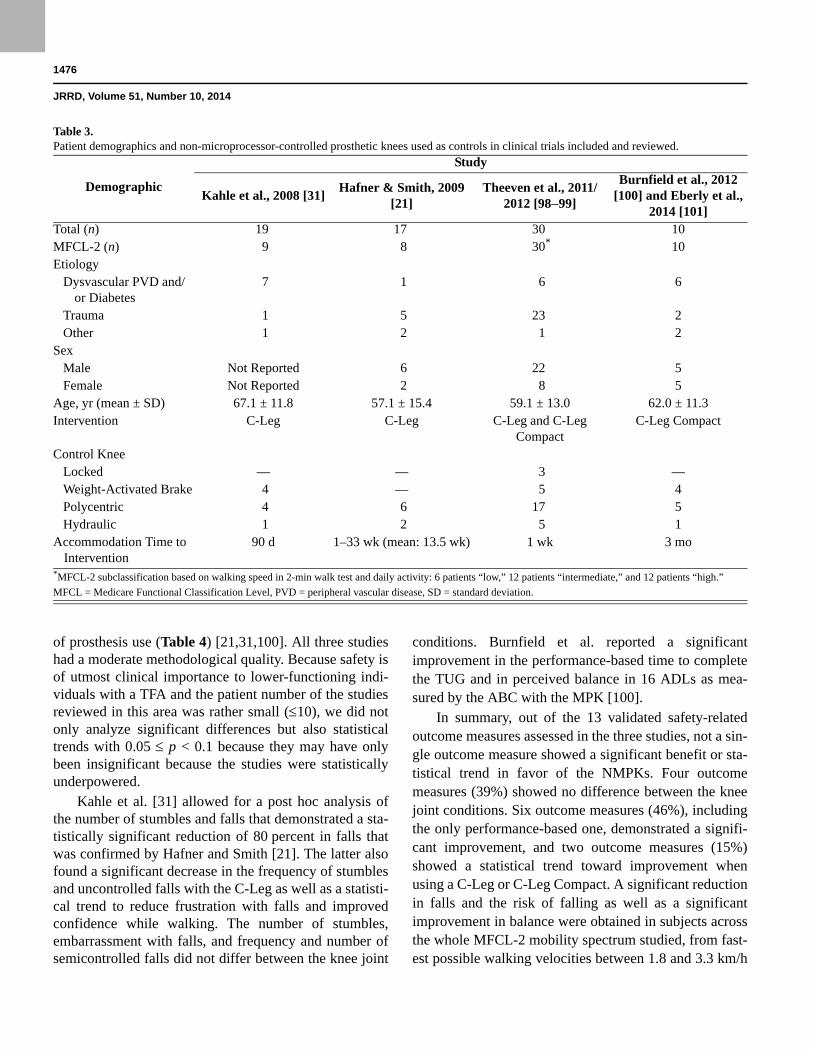
the overall walking capabilities [97], the assignment of the patients studied to the MFCL-2 mobility grade appears justified. Table 3 describes the demographics of the 57 subjects included in the six studies as well as the NMPKs used at the time of enrollment and as controls.
Stratification of Subjects With Medicare Functional Classification Level-2 Mobility Grade
Because only one of the four studies (six publica-tions) reviewed had assessed the AMP, this measure could not be used for a stratification of subjects. One study used the walking speed in the 2MWT as one com-ponent for the stratification of the subjects into low, inter-mediate, and high subgroups [98–99]. The other component, daily activity, had not been assessed in the other studies, but the walking distance or speed in the 2MWT has been shown to correlate well with daily activ-ity [97]. For this reason, the fastest possible walking speed with the NMPK was used to relate the results of three publications [31,100–101] to those of the study that had stratified its sample [98–99] as the best possible approximation. Based on the heterogeneity of the walk-ing speed ranges in the study samples, no a priori sub-groups across all studies and outcomes could be created. However, the relationship between the fastest possible walking speed on the NMPK and the results in the differ-ent outcome categories when using an MPK allow for interesting conclusions.
Safety OutcomesThree studies with a total of 27 limited community
ambulators reported
Study A1 A2 A3 A4 B5 B6 B7 B8 B9 C10 C11 C12 C13Total: A + B
CriteriaTotal: C Criteria
Total: A + B + C Criteria
Overall Grade
outcome measures related to safety
Table 2.Quality rating of five studies according to criteria of Cochrane review of Hofstad et al. [90].
Wetz et al., 2005 [102]
0 1 1 0 0 1 0 0 1 1 0 0 0 4 1 5 None
Kahle et al., 2008 [31]
1 0 1 0 1 1 0 1 1 1 0 0 1 6 2 8 B
Hafner & Smith, 2009 [21]
1 1 1 0 1 1 0 1 1 1 0 0 1 7 2 9 B
Theeven et al., 2011 [98]
1 1 1 1 1 1 0 0 1 0 1 0 1 7 2 9 C
Burnfield et al., 2012 [100]
1 0 1 0 1 1 0 1 1 1 0 0 1 6 2 8 B
Theeven et al., 2012 [99]
1 1 1 1 1 1 0 0 1 0 1 0 1 7 2 9 C
Eberly et al., 2014 [101]
1 1 1 0 1 1 0 1 1 1 0 0 1 7 2 9 B
1476
JRRD, Volume 51, Number 10, 2014
Demographic
Study
Kahle et al., 2008 [31]Hafner & Smith, 2009
[21]Theeven et al., 2011/
2012 [98–99]
Burnfield et al., 2012 [100] and Eberly et al.,
2014 [101]Total (n) 19 17 30 10MFCL-2 (n) 9 8 30* 10Etiology Dysvascular PVD and/
or Diabetes7 1 6 6
Trauma 1 5 23 2 Other 1 2 1 2Sex Male Not Reported 6 22 5 Female Not Reported 2 8 5Age, yr (mean ± SD) 67.1 ± 11.8 57.1 ± 15.4 59.1 ± 13.0 62.0 ± 11.3Intervention C-Leg C-Leg C-Leg and C-Leg
CompactC-Leg Compact
Control Knee Locked — — 3 — Weight-Activated Brake 4 — 5 4 Polycentric 4 6 17 5 Hydraulic 1 2 5 1Accommodation Time to
Intervention90 d 1–33 wk (mean: 13.5 wk) 1 wk 3 mo
MFCL = Medicare Functional Classification Level, PVD = peripheral vascular disease, SD = standard deviation.
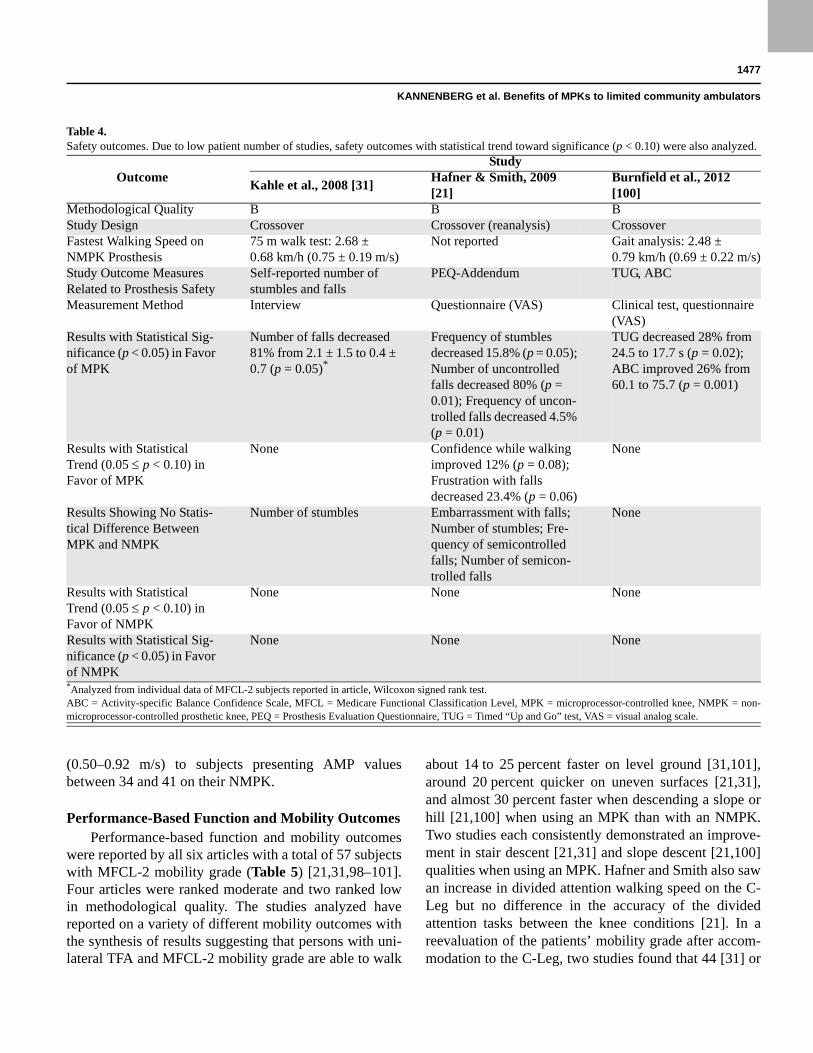
of prosthesis use (Table 4) [21,31,100]. All three studies had a moderate methodological quality. Because safety is of utmost clinical importance to lower-functioning indi-viduals with a TFA and the patient number of the studies reviewed in this area was rather small (10), we did not only analyze significant differences but also statistical trends with 0.05 p < 0.1 because they may have only been insignificant because the studies were statistically underpowered.
Kahle et al. [31] allowed for a post hoc analysis of the number of stumbles and falls that demonstrated a sta-tistically significant reduction of 80 percent in falls that was confirmed by Hafner and Smith [21]. The latter also found a significant decrease in the frequency of stumbles and uncontrolled falls with the C-Leg as well as a statisti-cal trend to reduce frustration with falls and improved confidence while walking. The number of stumbles, embarrassment with falls, and frequency and number of semicontrolled falls did not differ between the knee joint
conditions. Burnfield et al. reported a significant improvement in the performance-based time to complete the TUG and in perceived balance in 16 ADLs as mea-sured by the ABC with the MPK [100].
In summary, out of the 13 validated safety-related outcome measures assessed in the three studies, not a sin-gle outcome measure showed a significant benefit or sta-tistical trend in favor of the NMPKs. Four outcome measures (39%) showed no difference between the knee joint conditions. Six outcome measures (46%), including the only performance-based one, demonstrated a signifi-cant improvement, and two outcome measures (15%) showed a statistical trend toward improvement when using a C-Leg or C-Leg Compact. A significant reduction in falls and the risk of falling as well as a significant improvement in balance were obtained in subjects across the whole MFCL-2 mobility spectrum studied, from fast-est possible walking velocities between 1.8 and 3.3 km/h
Table 3.Patient demographics and non-microprocessor-controlled prosthetic knees used as controls in clinical trials included and reviewed.
*MFCL-2 subclassification based on walking speed in 2-min walk test and daily activity: 6 patients “low,” 12 patients “intermediate,” and 12 patients “high.”
1477
KANNENBERG et al. Benefits of MPKs to limited community ambulators
OutcomeStudy
Kahle et al., 2008 [31]Hafner & Smith, 2009 [21]
Burnfield et al., 2012 [100]
Methodological Quality B B BStudy Design Crossover Crossover (reanalysis) CrossoverFastest Walking Speed on NMPK Prosthesis
75 m walk test: 2.68 ± 0.68 km/h (0.75 ± 0.19 m/s)
Not reported Gait analysis: 2.48 ± 0.79 km/h (0.69 ± 0.22 m/s)
Study Outcome Measures Related to Prosthesis Safety
Self-reported number of stumbles and falls
PEQ-Addendum TUG, ABC
Measurement Method Interview Questionnaire (VAS) Clinical test, questionnaire (VAS)
Results with Statistical Sig-nificance (p < 0.05) in Favor of MPK
Number of falls decreased 81% from 2.1 ± 1.5 to 0.4 ± 0.7 (p = 0.05)*
Frequency of stumbles decreased 15.8% (p = 0.05); Number of uncontrolled falls decreased 80% (p = 0.01); Frequency of uncon-trolled falls decreased 4.5% (p = 0.01)
TUG decreased 28% from 24.5 to 17.7 s (p = 0.02); ABC improved 26% from 60.1 to 75.7 (p = 0.001)
Results with Statistical Trend (0.05 p < 0.10) in Favor of MPK
None Confidence while walking improved 12% (p = 0.08); Frustration with falls decreased 23.4% (p = 0.06)
None
Results Showing No Statis-tical Difference Between MPK and NMPK
Number of stumbles Embarrassment with falls; Number of stumbles; Fre-quency of semicontrolled falls; Number of semicon-trolled falls
None
Results with Statistical Trend (0.05 p < 0.10) in Favor of NMPK
None None None
Results with Statistical Sig-nificance (p < 0.05) in Favor of NMPK
None None None
(0.50–0.92 m/s) to subjects presenting AMP values between 34 and 41 on their NMPK.
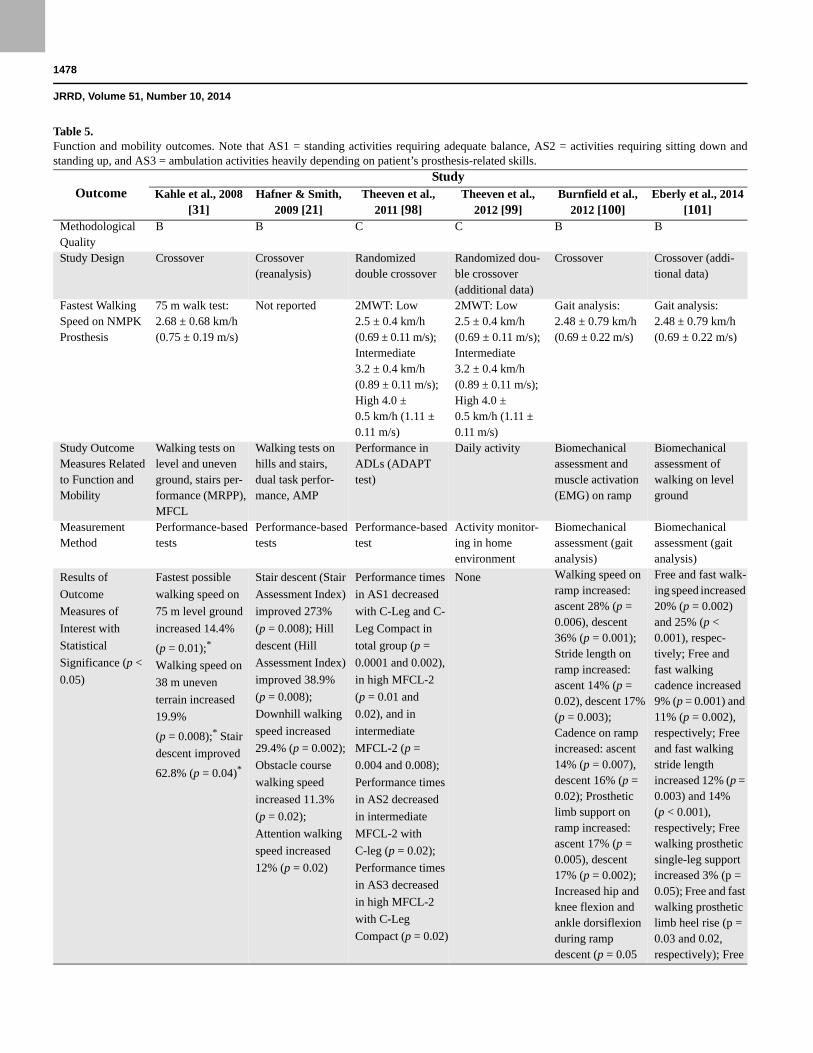
Performance-Based Function and Mobility OutcomesPerformance-based function and mobility outcomes
were reported by all six articles with a total of 57 subjects with MFCL-2 mobility grade (Table 5) [21,31,98–101]. Four articles were ranked moderate and two ranked low in methodological quality. The studies analyzed have reported on a variety of different mobility outcomes with the synthesis of results suggesting that persons with uni-lateral TFA and MFCL-2 mobility grade are able to walk
about 14 to 25 percent faster on level ground [31,101], around 20 percent quicker on uneven surfaces [21,31], and almost 30 percent faster when descending a slope or hill [21,100] when using an MPK than with an NMPK. Two studies each consistently demonstrated an improve-ment in stair descent [21,31] and slope descent [21,100] qualities when using an MPK. Hafner and Smith also saw an increase in divided attention walking speed on the C-Leg but no difference in the accuracy of the divided attention tasks between the knee conditions [21]. In a reevaluation of the patients’ mobility grade after accom-modation to the C-Leg, two studies found that 44 [31] or
Table 4.Safety outcomes. Due to low patient number of studies, safety outcomes with statistical trend toward significance (p < 0.10) were also analyzed.
*Analyzed from individual data of MFCL-2 subjects reported in article, Wilcoxon signed rank test.ABC = Activity-specific Balance Confidence Scale, MFCL = Medicare Functional Classification Level, MPK = microprocessor-controlled knee, NMPK = non-microprocessor-controlled prosthetic knee, PEQ = Prosthesis Evaluation Questionnaire, TUG = Timed “Up and Go” test, VAS = visual analog scale.
1478
JRRD, Volume 51, Number 10, 2014
Table 5. Function and mobility outcomes. Note that AS1 = standing activities requiring adequate balance, AS2 = activities requiring sitting down and standing up, and AS3 = ambulation activities heavily depending on patient’s prosthesis-related skills.
OutcomeStudy
Kahle et al., 2008 [31]
Hafner & Smith, 2009 [21]
Theeven et al., 2011 [98]
Theeven et al., 2012 [99]
Burnfield et al., 2012 [100]
Eberly et al., 2014 [101]
Methodological Quality
B B C C B B
Study Design Crossover Crossover (reanalysis)
Randomized double crossover
Randomized dou-ble crossover (additional data)
Crossover Crossover (addi-tional data)
Fastest Walking Speed on NMPK Prosthesis
75 m walk test: 2.68 ± 0.68 km/h (0.75 ± 0.19 m/s)
Not reported 2MWT: Low 2.5 ± 0.4 km/h (0.69 ± 0.11 m/s); Intermediate 3.2 ± 0.4 km/h (0.89 ± 0.11 m/s); High 4.0 ± 0.5 km/h (1.11 ± 0.11 m/s)
2MWT: Low 2.5 ± 0.4 km/h (0.69 ± 0.11 m/s); Intermediate 3.2 ± 0.4 km/h (0.89 ± 0.11 m/s); High 4.0 ± 0.5 km/h (1.11 ± 0.11 m/s)
Gait analysis: 2.48 ± 0.79 km/h (0.69 ± 0.22 m/s)
Gait analysis: 2.48 ± 0.79 km/h (0.69 ± 0.22 m/s)
Study Outcome Measures Related to Function and Mobility
Walking tests on level and uneven ground, stairs per-formance (MRPP), MFCL
Walking tests on hills and stairs, dual task perfor-mance, AMP
Performance in ADLs (ADAPT test)
Daily activity Biomechanical assessment and muscle activation (EMG) on ramp
Biomechanical assessment of walking on level ground
Measurement Method
Performance-based tests
Performance-based tests
Performance-based test
Activity monitor-ing in home environment
Biomechanical assessment (gait analysis)
Biomechanical assessment (gait analysis)
Results of Outcome Measures of Interest with Statistical Significance (p < 0.05)
Fastest possible walking speed on 75 m level ground increased 14.4%
(p = 0.01);* Walking speed on 38 m uneven terrain increased 19.9%
(p = 0.008);* Stair descent improved
62.8% (p = 0.04)*
Stair descent (Stair Assessment Index) improved 273% (p = 0.008); Hill descent (Hill Assessment Index) improved 38.9% (p = 0.008); Downhill walking speed increased 29.4% (p = 0.002); Obstacle course walking speed increased 11.3% (p = 0.02); Attention walking speed increased 12% (p = 0.02)
Performance times in AS1 decreased with C-Leg and C-Leg Compact in total group (p = 0.0001 and 0.002), in high MFCL-2 (p = 0.01 and 0.02), and in intermediate MFCL-2 (p = 0.004 and 0.008); Performance times in AS2 decreased in intermediate MFCL-2 with C-leg (p = 0.02);Performance timesin AS3 decreasedin high MFCL-2with C-LegCompact (p = 0.02)
None Walking speed on ramp increased: ascent 28% (p = 0.006), descent 36% (p = 0.001); Stride length on ramp increased: ascent 14% (p = 0.02), descent 17% (p = 0.003); Cadence on ramp increased: ascent 14% (p = 0.007), descent 16% (p = 0.02); Prosthetic limb support on ramp increased: ascent 17% (p = 0.005), descent 17% (p = 0.002); Increased hip and knee flexion and ankle dorsiflexion during ramp descent (p = 0.05
Free and fast walk-ing speed increased 20% (p = 0.002) and 25% (p < 0.001), respec-tively; Free and fast walking cadence increased 9% (p = 0.001) and 11% (p = 0.002), respectively; Free and fast walking stride length increased 12% (p = 0.003) and 14% (p < 0.001), respectively; Free walking prosthetic single-leg support increased 3% (p = 0.05); Free and fast walking prosthetic limb heel rise (p = 0.03 and 0.02, respectively); Free
1479
KANNENBERG et al. Benefits of MPKs to limited community ambulators
OutcomeStudy
Kahle et al., 2008 [31]
Hafner & Smith, 2009 [21]
Theeven et al., 2011 [98]
Theeven et al., 2012 [99]
Burnfield et al., 2012 [100]
Eberly et al., 2014 [101]
each); Earlier prosthetic limb heel-off during ramp descent: 21% (p = 0.01)
and fast walking peak hip and thigh extension angles during stance (p = 0.005 each); Free and fast walking peak ankle stance moment (p = 0.001 and 0.008, respectively); Fast walking peak knee loading moment (p = 0.05); Free and fast walking peak knee terminal stance moment (p = 0.04 and 0.03, respectively); Fast walking peak hip stance moment (p = 0.02); Fast walking preswing ankle power generation (p = 0.04); Fast walking peak hip loading response generation (p = 0.05); Free and fast walking intact limb tibialis anterior muscle activity (p = 0.002 and 0.003, respectively) and prosthetic limb gluteus maximus activity (p = 0.02 and 0.02, respectively)
Results Showing No Statistical Difference Between MPK and NMPK
Self-selected walking speed on 75 m level
ground;* Fastest possible walking speed on 6 m level
ground*
AMP;* Accuracy of divided attention task while walking
Performance time in AS1 activities in low MFCL-2 with both MPKs; Performance time in AS2 activities in total group and all subgroups with
Up-time per day; Active time per day; Activity (counts and bouts) per day in total, high, and low subgroup with either MPK and in
Prosthetic limb stance duration in percent of GC during ascent and descent; Prosthetic limb heel-off in percent of GC during ascent;
Fast walking prosthetic limb single-leg support; Free and fast walking peak knee and ankle angles; Free walking peak hip stance moment;
Table 5. (cont)Function and mobility outcomes. Note that AS1 = standing activities requiring adequate balance, AS2 = activities requiring sitting down and standing up, and AS3 = ambulation activities heavily depending on patient’s prosthesis-related skills.
1480
JRRD, Volume 51, Number 10, 2014
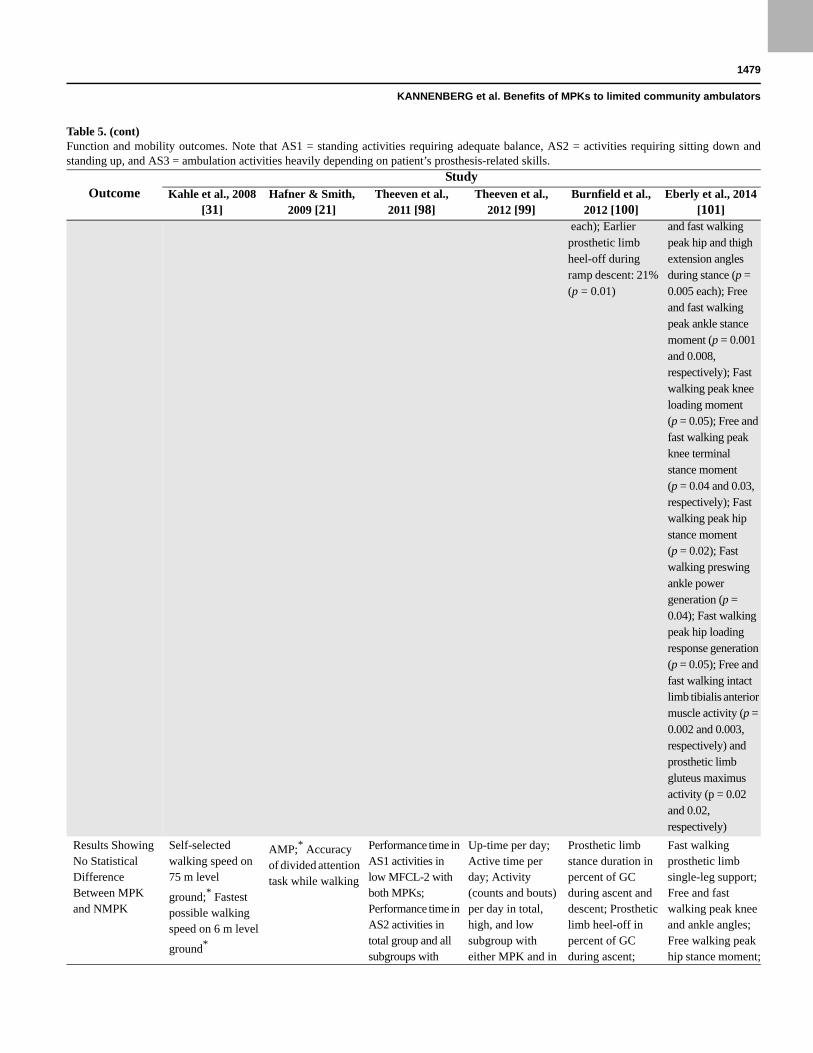
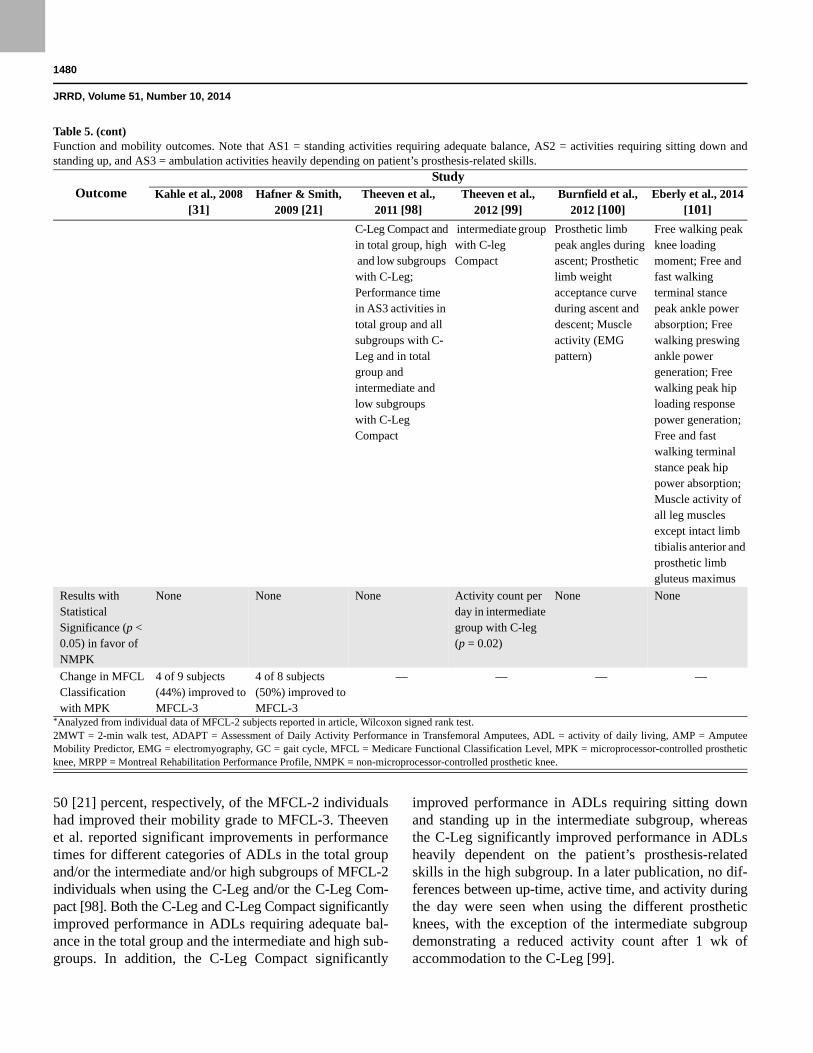
50 [21] percent, respectively, of the MFCL-2 individuals had improved their mobility grade to MFCL-3. Theeven et al. reported significant improvements in performance times for different categories of ADLs in the total group and/or the intermediate and/or high subgroups of MFCL-2individuals when using the C-Leg and/or the C-Leg Com-pact [98]. Both the C-Leg and C-Leg Compact significantlyimproved performance in ADLs requiring adequate bal-ance in the total group and the intermediate and high sub-groups. In addition, the C-Leg Compact significantly
improved performance in ADLs requiring sitting down and standing up in the intermediate subgroup, whereas the C-Leg significantly improved performance in ADLs heavily dependent on the patient’s prosthesis-related skills in the high subgroup. In a later publication, no dif-ferences between up-time, active time, and activity duringthe day were seen when using the different prosthetic knees, with the exception of the intermediate subgroup demonstrating a reduced activity count after 1 wk of accommodation to the C-Leg [99].
OutcomeStudy
Kahle et al., 2008 [31]
Hafner & Smith, 2009 [21]
Theeven et al., 2011 [98]
Theeven et al., 2012 [99]
Burnfield et al., 2012 [100]
Eberly et al., 2014 [101]
C-Leg Compact andin total group, high and low subgroups with C-Leg; Performance time in AS3 activities in total group and all subgroups with C-Leg and in total group and intermediate and low subgroups with C-Leg Compact
intermediate group with C-leg Compact
Prosthetic limb peak angles during ascent; Prosthetic limb weight acceptance curve during ascent and descent; Muscle activity (EMG pattern)
Free walking peak knee loading moment; Free and fast walking terminal stance peak ankle power absorption; Free walking preswing ankle power generation; Free walking peak hip loading response power generation; Free and fast walking terminal stance peak hip power absorption; Muscle activity of all leg muscles except intact limb tibialis anterior and prosthetic limb gluteus maximus
Results with Statistical Significance (p < 0.05) in favor of NMPK
None None None Activity count per day in intermediate group with C-leg (p = 0.02)
None None
Change in MFCL Classification with MPK
4 of 9 subjects (44%) improved to MFCL-3
4 of 8 subjects (50%) improved to MFCL-3
— — — —
*Analyzed from individual data of MFCL-2 subjects reported in article, Wilcoxon signed rank test.2MWT = 2-min walk test, ADAPT = Assessment of Daily Activity Performance in Transfemoral Amputees, ADL = activity of daily living, AMP = Amputee Mobility Predictor, EMG = electromyography, GC = gait cycle, MFCL = Medicare Functional Classification Level, MPK = microprocessor-controlled prosthetic knee, MRPP = Montreal Rehabilitation Performance Profile, NMPK = non-microprocessor-controlled prosthetic knee.
Table 5. (cont)Function and mobility outcomes. Note that AS1 = standing activities requiring adequate balance, AS2 = activities requiring sitting down and standing up, and AS3 = ambulation activities heavily depending on patient’s prosthesis-related skills.

1481
KANNENBERG et al. Benefits of MPKs to limited community ambulators
In summary, out of a total of 51 performance-based outcome measures and 40 biomechanical gait parameters that are related to function and mobility subjected tostatistical analysis, only the activity count per day in the intermediate subgroup of Theeven et al. showed a signif-icant effect in favor of the NMPK as compared with the C-Leg [99]. In 23 outcome measures (45%) and 22 bio-mechanical gait parameters (55%), no differences werefound between the prosthetic knee conditions. For 28 out-come measures (55%) and 18 biomechanical gait param-eters (45%), a significant improvement was demonstratedwhen using an MPK, enabling patients to better and/orfaster execute indoor ADLs as well as activities of com-munity ambulation typical for MFCL-3 mobility gradesuch as medium-distance level, uneven terrain, slope, andhill walking as well as stair negotiation. However, aninteresting relationship between the fastest possiblewalking speed on the NMPK and these improvementswas seen. Improvements in abilities necessary for com-munity ambulation were demonstrated in individualsacross all subgroups of the MFCL-2 mobility graderange, represented by slow to medium maximum walkingvelocities between 1.8 and 3.3 km/h (0.50–0.92 m/s) andhigh AMP values between 34 and 41. In contrast,improvements in indoor ADLs were only seen in individ-uals walking with medium to high maximum velocitiesbetween 2.8 and 4.5 km/h (0.78–1.25 m/s).
Perceived Function, Satisfaction, and Prosthesis Preference
Results on perceived function and satisfaction were reported by five articles with a total of 57 subjects with MFCL-2 mobility grade (Table 6) [21,31,98–100]. Three of these articles [21,31,100] had a moderate methodolog-ical quality and two [98–99] had a low methodological quality. Hafner and Smith reported a significant improve-ment of the perceived ability for multitasking while walking with the C-Leg [21]. Burnfield et al. found a significant improvement in the PEQ Mobility scale, but not in the Houghton Scale, when using the C-Leg Com-pact [100]. Theeven et al. found a significant reduction in perceived difficulty to perform ADLs requiring sitting down and standing up and those heavily dependent on the patient’s prosthesis-related skills in the total MFCL-2 study group with the C-Leg but not in the subgroups and not when using the C-Leg Compact [98]. In a later article, the same research group reported significant improvements in self-reported ambulation, utility,
residual-limb health, and satisfaction with walking in the total group and/or certain subgroups of the same MFCL-2 sample when using the C-Leg and/or C-Leg Compact [99]. Satisfaction with the prosthesis improved signifi-cantly in the total group with the C-Leg (Table 6).
In summary, out of the 96 self-reported outcome measures not a single one demonstrated superiority of the NMPKs. For the majority of 74 perceived outcome mea-sures (77%), no significant differences were found between the prosthetic knee interventions. Use of an MPK resulted in significant improvements in 22 self-reported outcome measures (23%). These were mainly demonstrated for subjects walking at medium to higher velocities between 2.8 and 4.5 km/h (0.78–1.25 m/s).
In their earlier article, Theeven et al. reported that 70 percent of the MFCL-2 individuals subjectively pre-ferred the C-Leg, 23 percent preferred the C-Leg Com-pact, and only 7 percent preferred their previous NMPK [98]. These results are consistent with the findings of Kahle et al., who found that 90 percent of the MFCL-2 subjects in their study preferred the C-Leg [31].
In addition, it is noteworthy that neither study reported any adverse events in association with the use of the C-Leg or C-Leg Compact.
DISCUSSION
We conducted a systematic review of the literature in order to analyze whether or not individuals with a unilateralTFA and MFCL-2 mobility grade may benefit from using MPKs, as has been demonstrated for higher-functioning MFCL-3 individuals [21,23–36]. We were able to iden-tify four studies with six articles that had investigated the effects of MPK use in subjects with a unilateral TFA and MFCL-2 mobility grade and sufficient methodological quality. The moderate to low methodological quality found for the studies complies with the findings of earlier systematic reviews of MPK intervention studies [23,36,96]. Consider, however, that there are serious challenges to prosthetic research, such as limited patient numbers and limited access of research institutions to patients, great functional and prognostic heterogeneity of patients, and practical impossibility of blinding, that result in a comparatively limited methodological quality of prosthetic studies in general [96,103]. Nevertheless, the quality of many clinical studies with MP-controlled components is the highest in the field of prosthetics.
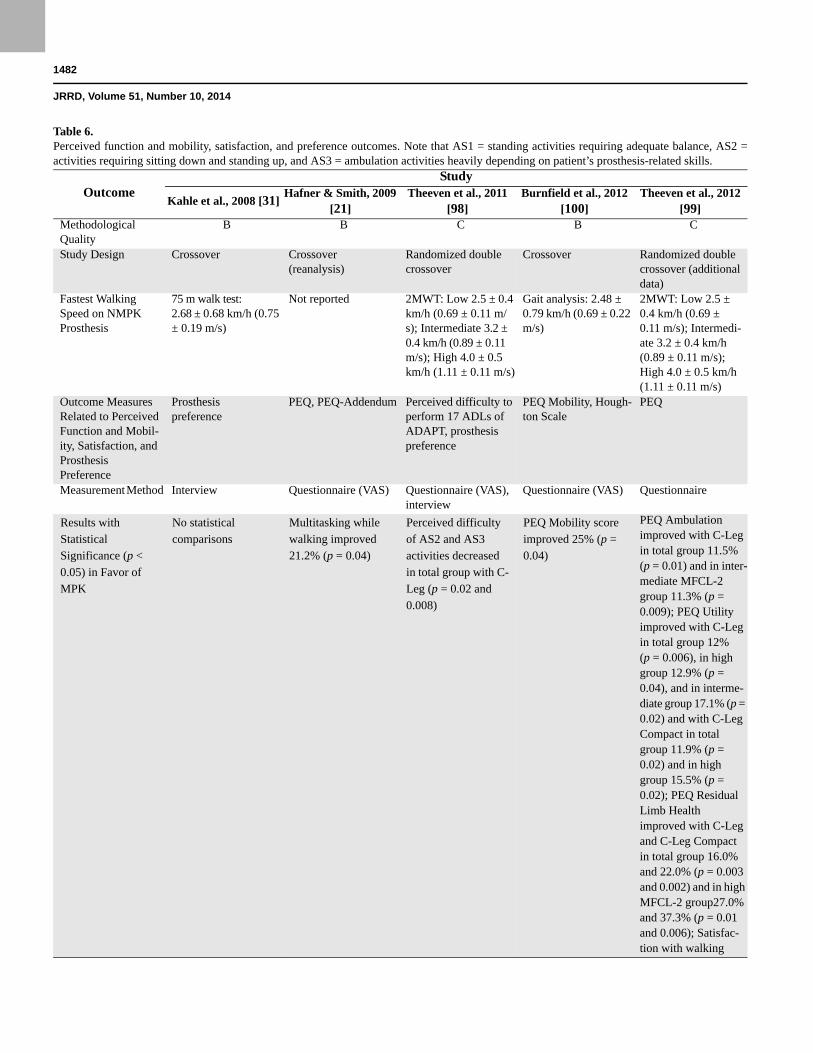
1482
JRRD, Volume 51, Number 10, 2014
Table 6. Perceived function and mobility, satisfaction, and preference outcomes. Note that AS1 = standing activities requiring adequate balance, AS2 = activities requiring sitting down and standing up, and AS3 = ambulation activities heavily depending on patient’s prosthesis-related skills.
OutcomeStudy
Kahle et al., 2008 [31]Hafner & Smith, 2009
[21]Theeven et al., 2011
[98]Burnfield et al., 2012
[100]Theeven et al., 2012
[99]Methodological Quality
B B C B C
Study Design Crossover Crossover (reanalysis)
Randomized double crossover
Crossover Randomized double crossover (additional data)
Fastest Walking Speed on NMPK Prosthesis
75 m walk test: 2.68 ± 0.68 km/h (0.75 ± 0.19 m/s)
Not reported 2MWT: Low 2.5 ± 0.4 km/h (0.69 ± 0.11 m/s); Intermediate 3.2 ± 0.4 km/h (0.89 ± 0.11 m/s); High 4.0 ± 0.5 km/h (1.11 ± 0.11 m/s)
Gait analysis: 2.48 ± 0.79 km/h (0.69 ± 0.22 m/s)
2MWT: Low 2.5 ± 0.4 km/h (0.69 ± 0.11 m/s); Intermedi-ate 3.2 ± 0.4 km/h (0.89 ± 0.11 m/s); High 4.0 ± 0.5 km/h (1.11 ± 0.11 m/s)
Outcome Measures Related to Perceived Function and Mobil-ity, Satisfaction, and Prosthesis Preference
Prosthesis preference
PEQ, PEQ-Addendum Perceived difficulty to perform 17 ADLs of ADAPT, prosthesis preference
PEQ Mobility, Hough-ton Scale
PEQ
Measurement Method Interview Questionnaire (VAS) Questionnaire (VAS), interview
Questionnaire (VAS) Questionnaire
Results with Statistical Significance (p < 0.05) in Favor of MPK
No statistical comparisons
Multitasking while walking improved 21.2% (p = 0.04)
Perceived difficulty of AS2 and AS3 activities decreased in total group with C-Leg (p = 0.02 and 0.008)
PEQ Mobility score improved 25% (p = 0.04)
PEQ Ambulation improved with C-Leg in total group 11.5% (p = 0.01) and in inter-mediate MFCL-2 group 11.3% (p = 0.009); PEQ Utility improved with C-Leg in total group 12% (p = 0.006), in high group 12.9% (p = 0.04), and in interme-diate group 17.1% (p = 0.02) and with C-Leg Compact in total group 11.9% (p = 0.02) and in high group 15.5% (p = 0.02); PEQ Residual Limb Health improved with C-Leg and C-Leg Compact in total group 16.0% and 22.0% (p = 0.003 and 0.002) and in high MFCL-2 group27.0% and 37.3% (p = 0.01 and 0.006); Satisfac-tion with walking
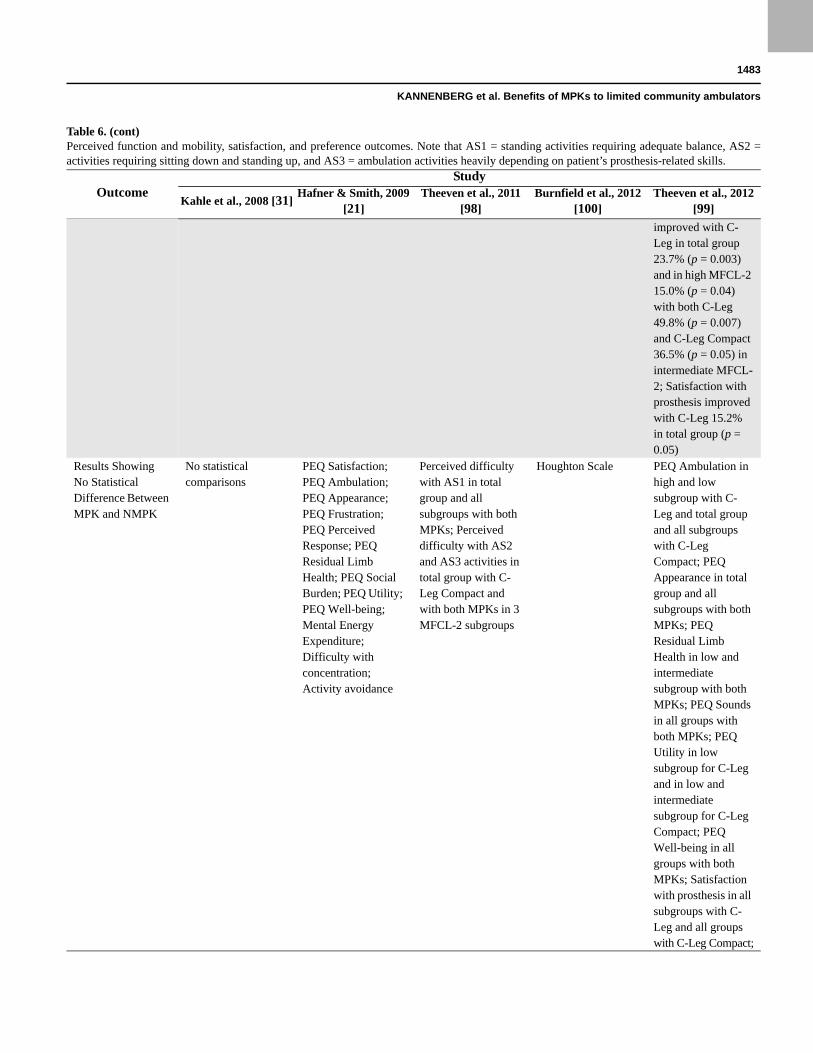
1483
KANNENBERG et al. Benefits of MPKs to limited community ambulators
OutcomeStudy
Kahle et al., 2008 [31]Hafner & Smith, 2009
[21]Theeven et al., 2011
[98]Burnfield et al., 2012
[100]Theeven et al., 2012
[99]
improved with C-Leg in total group 23.7% (p = 0.003) and in high MFCL-2 15.0% (p = 0.04) with both C-Leg 49.8% (p = 0.007) and C-Leg Compact 36.5% (p = 0.05) in intermediate MFCL-2; Satisfaction with prosthesis improved with C-Leg 15.2% in total group (p = 0.05)
Results Showing No Statistical Difference Between MPK and NMPK
No statistical comparisons
PEQ Satisfaction; PEQ Ambulation; PEQ Appearance; PEQ Frustration; PEQ Perceived Response; PEQ Residual Limb Health; PEQ Social Burden; PEQ Utility; PEQ Well-being; Mental Energy Expenditure; Difficulty with concentration; Activity avoidance
Perceived difficulty with AS1 in total group and all subgroups with both MPKs; Perceived difficulty with AS2 and AS3 activities in total group with C-Leg Compact and with both MPKs in 3 MFCL-2 subgroups
Houghton Scale PEQ Ambulation in high and low subgroup with C-Leg and total group and all subgroups with C-Leg Compact; PEQ Appearance in total group and all subgroups with both MPKs; PEQ Residual Limb Health in low and intermediate subgroup with both MPKs; PEQ Sounds in all groups with both MPKs; PEQ Utility in low subgroup for C-Leg and in low and intermediate subgroup for C-Leg Compact; PEQ Well-being in all groups with both MPKs; Satisfaction with prosthesis in all subgroups with C-Leg and all groups with C-Leg Compact;
Table 6. (cont)Perceived function and mobility, satisfaction, and preference outcomes. Note that AS1 = standing activities requiring adequate balance, AS2 = activities requiring sitting down and standing up, and AS3 = ambulation activities heavily depending on patient’s prosthesis-related skills.

1484
JRRD, Volume 51, Number 10, 2014
SafetyObjective and perceived safety is the foundation of
proficient prosthesis use and improvement in function and mobility [8,44–50,104]. The two studies that investi-gated the MP stance and swing controlled C-Leg demon-strated a significant reduction in the self-reported number and frequency of uncontrolled falls than with the use of the NMPKs [21,31]. The only study that investigated the MP stance controlled C-Leg Compact found a significant reduction in the completion time of the performance-based TUG [57–61] that was almost twice as large as the minimal detectable change (MDC) as reported by Resnik and Borgia [105]. The TUG even fell below the cutoff value of 19 s as reported by Dite et al. to indicate a risk of multiple falls in people with transtibial amputation [62]. This finding was accompanied by a significant improve-ment in self-reported balance as measured by the ABC exceeding the validated score of 67, indicating a low risk of falling [6–7,66]. In summary, the best validated perfor-mance-based safety outcome measure and those self-reported measures indicating the most dangerous adverse events of prosthesis use consistently demonstrated a sig-nificant gain in safety when using an MPK. In contrast, the measures that found no difference between the pros-
thetic knees are all indicators of events that are certainly unpleasant, such as stumbles and semicontrolled falls, but involve considerably lesser risks of serious conse-quences. Two of the studies found improvements in safetyin subjects capable of walking between 1.8 and 3.3 km/h on their NMPK prosthesis [31,100]. The third article did not report walking speeds, but the AMP values suggest thatthe patients belonged to the medium- to high-functioning segment of the MFCL-2 population [21]. Thus, it can be concluded that the two hydraulic MPKs studied may improve the safety of prosthesis use in individuals with a unilateral TFA and MFCL-2 mobility grade to the same extent as they do in subjects with a higher mobility grade level [23,36].
The significant gain in safety can be explained by the difference in technology between the MP default stance control and the non-MP default swing control knees that are usually prescribed for MFCL-2 subjects, namely weight-activated “safety” brake knees and 4-bar or multi-axial polycentric knees. In brake knees, stance control and stability is activated by the combination of full knee extension and weight loading. In polycentric knees, stance stability is achieved by projection of the instanta-neous center of rotation (ICR) behind the vector of the
OutcomeStudy
Kahle et al., 2008 [31]Hafner & Smith, 2009
[21]Theeven et al., 2011
[98]Burnfield et al., 2012
[100]Theeven et al., 2012
[99]
Satisfaction with walking in low subgroup with C-Leg and in all groups with C-Leg Compact
Results with Statistical Significance (p < 0.05) in Favor of NMPK
No statistical comparisons
None None None None
Prosthesis Preference
8 subjects (90%) preferred C-Leg
— 21 subjects (70%) preferred C-Leg, 7 subjects (23%) preferred C-Leg Compact
— —
2MWT = 2-min walk test, ADAPT = Assessment of Daily Activity Performance in Transfemoral Amputees, ADL = activity of daily living, AMP = Amputee Mobility Predictor, EMG = electromyography, GC = gait cycle, MFCL = Medicare Functional Classification Level, MPK = microprocessor-controlled prosthetic knee, NMPK = non-microprocessor-controlled prosthetic knee, PEQ = Prosthesis Evaluation Questionnaire, VAS = visual analog scale.
Table 6. (cont)Perceived function and mobility, satisfaction, and preference outcomes. Note that AS1 = standing activities requiring adequate balance, AS2 = activities requiring sitting down and standing up, and AS3 = ambulation activities heavily depending on patient’s prosthesis-related skills.

1485
KANNENBERG et al. Benefits of MPKs to limited community ambulators
vertical ground reaction force (GRF) at full knee exten-sion. If not fully extended at heel strike, both brake and polycentric knees may fail to provide knee stability due to lever moments exceeding the braking capacity (brake knees) or shift of the ICR close to or even in front of the GRF (polycentric knees) resulting in a knee flexion moment that immediately voids knee stability. Full knee extension at loading response can be achieved by walk-ing straight on level ground with more or less fixed velocity, cadence, and stride length as is postulated for MFCL-2 individuals. However, many ADLs and commu-nity ambulation require locomotion in confined spaces with turns, stepping in different directions, variation of step length, negotiation of barriers and obstacles, and movements of the upper body that may change the posi-tion of the center of mass and the resulting GRF, which may prevent the prosthetic knee from reaching full exten-sion [25]. Designed as default swing knees, brake and polycentric knees will inevitably collapse when loaded in such situations [16–22,106–108], thus exposing the patient to a substantial risk of falling. The very limited safety of weight-activated brake knees has been demon-strated in a clinical trial with elderly persons with a dys-vascular above-knee amputation [104]. Although accommodated to the brake knee, the patients preferred a locked knee for safety reasons [104].
In contrast, the default setting of the two MPKs stud-ied is to control stance stability unless they are explicitly switched into swing control. But even when in the swing mode, the two MPKs provide high flexion resistance for stumble recovery during the swing extension movement that is able to prevent knee collapse even if the prosthesis is fully loaded [27,35]. Unlike in the typical MFCL-2 knee joints, turns, changes in walking direction, move-ments of the upper body, stepping onto obstacles, walk-ing on ramps, walking on stairs, and even stumbles do not affect the stance safety of the C-Leg or C-Leg Com-pact [24–25,27,35].
With the safety limitations described previously, the prosthetic knees typically prescribed for MFCL-2 indi-viduals may even contribute to activity avoidance, increased dependency, and limited community ambula-tion. Because the C-Leg and C-Leg Compact have been demonstrated to reduce uncontrolled falls, to lower the risk of falling, and to improve balance, they may create a safe foundation for increasing community ambulation and independence in individuals with a TFA and MFCL-2mobility grade.
Performance-Based Function and MobilityAll six articles consistently reported that, when using
an MPK, limited community ambulators may signifi-cantly improve their abilities to perform activities of community ambulation such as negotiating uneven ter-rain and environmental obstacles [21,31], ramps [100], hills [21], and stairs [21,31] and multitasking while walk-ing [21]. The higher-functioning MFCL-2 subgroups may also improve the ability to perform many indoor ADLs [98]. The reduction in the activity count seen in the intermediate subgroup of Theeven et al. [99] when using an MPK might possibly be explained by the increase in stride length as demonstrated in one of the other articles [101], resulting simply in fewer steps required to ambulate the same distance. The significant improvements in 55 percent of all performance-based outcome measures assessed indicate that the two hydrau-lic MPKs studied may enable limited community ambu-lators to perform activities that, by definition, are typical for unlimited community ambulators with MFCL-3 mobility grade. This is further supported by the fact that two articles found that 44 to 50 percent of MFCL-2 sub-jects were able to improve their overall functional level to MFCL-3 when using a C-Leg [21,31]. However, these findings must be interpreted with caution, because the definition of the MFCL is very general and grants much room for subjective interpretation by the assessor, espe-cially when speculating about the functional “potential” of the patient (Table 1). To date, no approved tests exist to objectify the assignment of a patient to a certain func-tional level. The AMP has been proposed to address this issue, but the currently recommended cutoff values to distinguish the functional levels have not yet been vali-dated [69]. Nevertheless, one or more performance-based tests to objectify the functional classification or even a com-pletely new, validated, and unambiguously quantifiable functional classification of patients that ideally may also be used as outcome measures would represent substantial progress away from the current ambiguous classification. Based on the fastest possible walking speed on the NMPK, the studies reviewed have demonstrated a huge patient variability within the MFCL-2 mobility grade. Performance-based tests might therefore also help indi-cate clinically meaningful improvements within a func-tional classification level that are inevitably missed today.
Across the studies, there was an interesting relation-ship between the maximum walking speed on the NMPKs

1486
JRRD, Volume 51, Number 10, 2014
as a validated indicator of the overall walking capabilities [97] and the improvements in activities of community ambulation on the one hand and in indoor ADLs on the other. While improvements in activities of community ambulation have been demonstrated across the entire MFCL-2 mobility range [21,31,100–101], improvements in performance in indoor ADLs have only been shown for higher-functioning individuals within the MFCL-2 mobility spectrum, capable of walking at fast velocities of about 2.8 to 4.5 km/h [98]. This discrepancy may be explained by the difference in accommodation time between the trials, which was 3 mo on average in the studies that investigated community ambulation and only as short as 1 wk in the study of indoor ADLs. It could well be that lower-functioning individuals need more time and training to adapt to a prosthetic intervention than higher-functioning subjects and that the results of the latter might have further improved with longer accommodation [27,34,109]. Comparing the statistical and individual results in the various subgroups, Theeven et al. stressed the importance of an individual patient assessment because some individuals of the high sub-group did not improve their performance on either MPK whereas some subjects of the low subgroup did [98].
As for safety of prosthesis use, the improvement in performance-based function and mobility outcomes can be explained by the differences in technology between the prosthetic knees. Many ADLs in the house and activi-ties of community ambulation such as sitting down and walking on slopes, on stairs, on uneven terrain, and over obstacles are physiologically performed by nondisabled subjects with knee flexion during weight-bearing. In sub-jects with a TFA, this control must be provided by the prosthetic knee. The knee mechanisms typically fitted in limited community ambulators have in common that they do not allow for knee flexion during weight-bearing (yielding). Therefore, consider that the assignment of an individual to the MFCL-2 mobility grade and the com-monly consequent selection of prosthetic componentry may technically restrict the achievable mobility of a part of this population. Knee flexion during weight-bearing (yielding) is only permitted by hydraulic stance control knees [16–19,22,106–108]. Based on technical consider-ations [16–19,22,106–108] and one older study [110], MFCL-2 subjects are hardly able to safely control the switching mechanisms of hydraulic NMPKs. Meanwhile, sensor input and MP control have overcome the physical challenges to safely use hydraulic knees. As the results of
the studies reviewed have consistently shown, the hydraulic default stance MPKs C-Leg and C-Leg Com-pact may enable individuals with a TFA and MFCL-2 mobility grade to execute activities of community ambu-lation, as well as indoor ADLs, better and faster while increasing safety of prosthesis use at the same time. These findings are consistent with those for individuals with MFCL-3 mobility grade [23].
In addition, those individuals who are capable of walking at a faster velocity of more than 2.9 km/h (0.8 m/s)on their NMPK tend to benefit more from the C-Leg than from the C-Leg Compact [98]. This might be explained by the fact that patients who walk faster are also more likely to walk with a broader range of walking speeds, thuspossibly taking advantage of the additional MP hydraulic swing control of the C-Leg rather than of the conventionalhydraulic swing control of the C-Leg Compact.
Perceived Function and SatisfactionSomewhat unexpectedly, the improvements in per-
ceived function and mobility as assessed by self-reported outcome measures for use of an MPK lag behind the per-formance-based improvements. Only 22 percent of the self-reported outcome measures related to function, mobil-ity, and satisfaction showed a significant improvement as a result of MPK use, mainly in the higher-functioning subset of the MFCL-2 mobility range for indoor ADLs. Note, however, that the perceived difficulty to perform the ADLs investigated in Theeven et al. was relatively low across all subgroups, even when using a NMPK, leaving not much room for further improvement [98]. For the lower-functioning, slower-walking subset of the MFCL-2 mobility range, only Burnfield et al. reported a significant increase in the PEQ Mobility scale [100], but the reported increase was twice as big as the MDC as reported by Resnik and Borgia [105]. This means that MFCL-2 individuals, especially at the lower end of the studied mobility spectrum, experience greater improve-ments in objective performance by MPK use than they subjectively acknowledge. In contrast, the two studies that asked the subjects for their personal prosthesis pref-erence found that 90 percent of patients preferred the MPK over their previous NMPK [31,98]. The explana-tion for this discrepancy between the limited perceived functional improvements and the clear prosthetic knee preference may be found in the far better improvement of perceived safety of prosthesis use with either MPK as discussed previously.

1487
KANNENBERG et al. Benefits of MPKs to limited community ambulators
Recommendation for PracticeThe results of this systematic review suggest that the
use of MP hydraulic stance only or MP stance and swing control prosthetic knees may improve safety, function, and mobility of limited community ambulators with uni-lateral TFA. In light of these findings, it no longer appears appropriate to generally withhold this advanced prosthetic technology from MFCL-2 individuals. On the other hand, the current state of the research does not jus-tify fit of an MPK in all limited community ambulators. But even high-quality clinical research with RCTs only allows for conclusions on the basis of means and aver-ages of the studied population but not on an individual patient [111]. Several European healthcare systems, e.g., in Germany, Austria, the Netherlands, Italy, and France, have addressed the issue of individual decision-making in prosthetics by allowing trial fittings to study whether an individual patient benefits from an MPK intervention, as supported by the findings of Theeven et al. [98]. Many factors contribute to the success or failure of prosthetic interventions, including the actual everyday mobility needs, the basic physical capabilities, and the personal objectives and motivation of the patient [112]. Based on the clinical studies analyzed in the present systematic review, the following suggestions for preliminary quali-fying and decision-making criteria can be made:
1. Patients who walk less than 60 m (195 ft) on theirNMPK in the 2MWT, which equals an average walk-ing speed of less than 1.8 km/h (1.1 mph), have notyet been studied with MPK interventions. That doesnot necessarily mean that these patients disqualify foran MPK trial fitting, but no research-based sugges-tions or recommendations for this patient group canbe given.
2. Patients who are capable of walking between 60 and95 m (195 to 310 ft) in the 2MWT on their NMPK,which equals an average walking speed between 1.8and 2.9 km/h (1.1–1.8 mph) may benefit from usingan MPK for safety and to improve the abilitiesrequired for community ambulation. Their walkingspeed and ability to vary walking velocity suggeststhat MP swing control may not necessarily berequired; therefore, a trial fitting with the MP stancecontrolled C-Leg Compact may be considered.
3. Patients who are able to walk more than 95 m (310 ft)in the 2MWT on their NMPK, which equals a walkingspeed of faster than 2.9 km/h (1.8 mph) may benefitfrom using an MPK for safety, community ambula-
tion, and indoor ADLs. Their higher walking speed is likely to result in a higher ability to vary walking velocities and may therefore justify a trial fitting with the MP stance and swing controlled C-Leg. After appropriate training and accommodation, the
patient should demonstrate an improvement in the dis-tance walked in the 2MWT as a validated outcome mea-sure for the overall walking capabilities and mobility [104,113]. The MDC in subjects with a lower-limb amputation has been reported to be between 17 m (56 ft) [104] and 34.3 m (113 ft) [105], but the latter value hasbeen established for mixed groups of higher-functioningsubjects with transtibial amputation and TFA. In elderly,nonamputated, prefrail, and frail subjects; patients withstroke; and patients with hip fracture, improvements inshort-distance (3–10 m) walking speed of 0.1 m/s areconsidered clinically meaningful [114–119] and correlatewith the risk of falling [120], frailty [121], and even sur-vival [122–123]. We therefore believe that a minimumimprovement in average walking speed in the 2MWT of0.1 m/s, which would result in an increase in the distancewalked of at least 12 m (40 ft), may also be consideredclinically meaningful and justify the use of an MPK inindividuals with a TFA and MFCL-2 mobility grade. Inaddition, an improvement in the TUG exceeding theMDC of 3.6 s [105], preferably under the cutoff value of19 s that indicates a risk of multiple falls in subjects withtranstibial amputation, may be considered a clinically rel-evant improvement in prosthesis safety [62]. Likewise,an improvement of perceived balance on the ABC [6–7,66] indicates improved confidence in prosthesis use.An MDC for the ABC score in subjects with an amputationhas not yet been established, but an improvement overthe cutoff value of 67 for a low risk of falling may beconsidered clinically relevant.
In everyday practice, the AMP is increasingly used to objectify the determination of the functional level of an individual with a lower-limb amputation [69]. Unfortu-nately, none of the studies reviewed used the AMP, nei-ther to determine the functional level nor as an outcome measure. However, based on the published research on the AMP [69,105], an improvement of the score that exceeds the MDC of 3.4 points [105] may also be consid-ered clinically meaningful. Further research with more patients and improved methodological quality is war-ranted to corroborate and refine or revise these prelimi-nary suggestions.

1488
JRRD, Volume 51, Number 10, 2014
LimitationsThis systematic review has several limitations.
Although the literature search strategy and the medical databases searched were quite comprehensive, it is possi-ble that not all existing clinical studies and publications on the effects of MPK use in the limited community ambulator population have been identified. Also, the restriction on English- and German-language publica-tions may have resulted in missing important studies on this subject published in other languages. Moreover, a publication bias toward favorable results of the use of the MPKs cannot fully be excluded.
The relatively low total patient number of 57 limited community ambulators and especially the low number of individuals with a dysvascular amputation is a limitation of this systematic review. There is some evidence, how-ever, that many of these individuals may belong to the very low-functioning segment of the MFCL-2 mobility spectrum that has not yet been studied with MPK inter-ventions [104]. The challenges to prosthetic research in this population became obvious in Theeven et al. in that only 40 percent of patients who met the inclusion criteria agreed to participate and almost all of the dropouts had been subjects with a dysvascular amputation [98–99]. Nevertheless, future research will have to address the specific conditions and needs of that population.
Also, grouping study results according to the fastest possible walking speed and basing the recommendations for preliminary qualifying and decision-making criteria for trial fittings has limitations. Only one study [98–99] used the 2MWT to determine walking speed. One study [31] used the 75 m fastest possible walking speed on level ground test that, when analyzing the completion times, comes close to the 2MWT; one study [100–101] only reported the walking speed measured during motion capture in the gait laboratory; and one study did not report any walking speed at all [21]. Hafner and Smith, however, reported individual AMP values that indicated that the patients belonged to the intermediate- and high-functioning MFCL-2 mobility segment [21]. It seems likely that some of the patients in the motion analysis study may not be able to maintain the walking speed measured in the gait laboratory as the average walking velocity in the 2MWT [100–101]. We therefore believe that patients who walk less than 60 m (195 ft) in the 2MWT should not generally be excluded from MPK trial fittings. However, in light of the consistent results of this systematic review, it seems appropriate to make MPK
trial fittings available to the higher-functioning subset of limited community ambulators first. This approach also complies with the current paradigm that a certain basic physical fitness is required to likely benefit from using an MPK.
CONCLUSIONS
The results of this systematic review of clinical trials on interventions with MPKs in individuals with a unilat-eral TFA and MFCL-2 mobility grade suggest that these subjects may significantly reduce the number of falls and their risk of falling, improve their balance, and better per-form activities of community ambulation that are actually categorized as part of the MFCL-3 mobility grade. Because these results have been derived from studies with low to moderate methodological quality in a yet lim-ited number of patients, trial fittings with different types of MPKs (MP stance only or MP stance and swing con-trol) may be considered to evaluate whether an individual benefits from using an MPK compared with NMPKs usu-ally prescribed for MFCL-2 individuals. Criteria for appraising success or failure of the trial fitting based on the 2MWT, AMP, TUG, and ABC have been suggested. Given the challenges to objectify the current general and ambiguous definitions of the MFCLs, an evidence-based and unambiguously quantifiable functional classification or one or more validated outcome measures to corrobo-rate the classification would help better define patient groups to be subjected to clinical research and sharpen coverage and reimbursement criteria.
ACKNOWLEDGMENTS
Author Contributions:
Drafting of manuscript: A. Kannenberg, B. Zacharias, E. Pröbsting.Financial Disclosures: All authors are employees of Otto Bock HealthCare LP (Austin, Texas) or Otto Bock HealthCare GmbH (Dud-erstadt, Germany), the manufacturers of the two MPKs subject to all studies reviewed. The company did not influence the design and exe-cution of the study nor the interpretation of the study results.Funding/Support: Otto Bock HealthCare allowed the authors to work on the article during their regular working hours and use the company’s office equipment (computers, Internet access, etc.).
1489
KANNENBERG et al. Benefits of MPKs to limited community ambulators
REFERENCES
1. Dillingham TR, Pezzin LE, MacKenzie EJ. Limb amputa-tion and limb deficiency: Epidemiology and recent trendsin the United States. South Med J. 2002;95(8):875–83.[PMID:12190225]
2. Davies B, Datta D. Mobility outcome following unilaterallower limb amputation. Prosthet Orthot Int. 2003;27(3):186–90. [PMID:14727699]http://dx.doi.org/10.1080/03093640308726681
3. Robbins CB, Vreeman DJ, Sothmann MS, Wilson SL,Oldridge NB. A review of the long-term health outcomesassociated with war-related amputation. Mil Med. 2009;174(6):588–92. [PMID:19585770]http://dx.doi.org/10.7205/MILMED-D-00-0608
4. Norvell DC, Czerniecki JM, Reiber GE, Maynard C, Pec-oraro JA, Weiss NS. The prevalence of knee pain andsymptomatic knee osteoarthritis among veteran traumaticamputees and nonamputees. Arch Phys Med Rehabil.2005;86(3):487–93. [PMID:15759233]http://dx.doi.org/10.1016/j.apmr.2004.04.034
5. Buckley JG, O’Driscoll D, Bennett SJ. Postural sway andactive balance performance in highly active lower-limbamputees. Am J Phys Med Rehabil. 2002;81(1):13–20.[PMID:11807327]http://dx.doi.org/10.1097/00002060-200201000-00004
6. Miller WC, Deathe AB, Speechley M. Psychometricproperties of the Activities-specific Balance ConfidenceScale among individuals with a lower-limb amputation.Arch Phys Med Rehabil. 2003;84(5):656–61.[PMID:12736877]http://dx.doi.org/10.1016/S0003-9993(02)04807-4
7. Miller WC, Deathe AB. A prospective study examiningbalance confidence among individuals with lower limbamputation. Disabil Rehabil. 2004;26(14–15):875–81.[PMID:15497916]http://dx.doi.org/10.1080/09638280410001708887
8. Miller WC, Speechley M, Deathe B. The prevalence andrisk factors of falling and fear of falling among lowerextremity amputees. Arch Phys Med Rehabil. 2001;82(8):1031–37. [PMID:11494181]http://dx.doi.org/10.1053/apmr.2001.24295
9. Miller WC, Deathe AB, Speechley M, Koval J. The influ-ence of falling, fear of falling, and balance confidence onprosthetic mobility and social activity among individualswith a lower extremity amputation. Arch Phys Med Reha-bil. 2001;82(9):1238–44. [PMID:11552197]http://dx.doi.org/10.1053/apmr.2001.25079
10. Hof AL, van Bockel RM, Schoppen T, Postema K. Con-trol of lateral balance in walking. Experimental findingsin normal subjects and above-knee amputees. Gait Pos-ture. 2007;25(2):250–58. [PMID:16740390]http://dx.doi.org/10.1016/j.gaitpost.2006.04.013
11. Stepien JM, Cavenett S, Taylor L, Crotty M. Activity lev-els among lower-limb amputees: Self-report versus stepactivity monitor. Arch Phys Med Rehabil. 2007;88(7):896–900. [PMID:17601471]http://dx.doi.org/10.1016/j.apmr.2007.03.016
12. Genin JJ, Bastien GJ, Franck B, Detrembleur C, WillemsPA. Effect of speed on the energy cost of walking in uni-lateral traumatic lower limb amputees. Eur J ApplPhysiol. 2008;103(6):655–63. [PMID:18478251]http://dx.doi.org/10.1007/s00421-008-0764-0
13. van Velzen JM, van Bennekom CA, Polomski W, Sloot-man JR, van der Woude LH, Houdijk H. Physical capacityand walking ability after lower limb amputation: A sys-tematic review. Clin Rehabil. 2006;20(11):999–1016.[PMID:17065543]http://dx.doi.org/10.1177/0269215506070700
14. Ziegler-Graham K, MacKenzie EJ, Ephraim PL, TravisonTG, Brookmeyer R. Estimating the prevalence of limbloss in the United States: 2005 to 2050. Arch Phys MedRehabil. 2008;89(3):422–29. [PMID:18295618]http://dx.doi.org/10.1016/j.apmr.2007.11.005
15. National Limb Loss Information Center [Internet]. Ampu-tation statistics by cause: Limb loss in the United States.Knoxville (TN): Amputee Coalition of America; 2008[cited 2013 Nov 11]. Available from: http://www.amputee-coalition.org/fact_sheets/amp_stats_cause.pdf
16. Michael JW. Modern prosthetic knee mechanisms. ClinOrthop Relat Res. 1999;361(361):39–47.[PMID:10212594]http://dx.doi.org/10.1097/00003086-199904000-00006
17. Huang ME, Levy CE, Webster JB. Acquired limb defi-ciencies. 3. Prosthetic components, prescriptions, andindications. Arch Phys Med Rehabil. 2001;82(3 Suppl 1):S17–24. [PMID:11239332]http://dx.doi.org/10.1016/S0003-9993(01)80032-0
18. Jamieson SC, Davies AJ. Prosthetics. In: Brammers CM,Spires SC, editors. Manual for clinical problems in physicalmedicine and rehabilitation. Philadelphia (PA): Hanley &Belfus; 2001. p. 409–20.
19. Nelson VS, Flood KM, Bryant PR, Huang ME, Pasquina PF,Roberts TL. Limb deficiency and prosthetic management.1. Decision making in prosthetic prescription and man-agement. Arch Phys Med Rehabil. 2006;87(3 Suppl 1):S3–9. [PMID:16500187]http://dx.doi.org/10.1016/j.apmr.2005.11.022
20. Region B medical supplier bulletin. DMEPOS bulletin95–01. 1995 Jan.
21. Hafner BJ, Smith DG. Differences in function and safetybetween Medicare Functional Classification Level-2 and-3 transfemoral amputees and influence of prosthetic kneejoint control. J Rehabil Res Dev. 2009;46(3):417–33.[PMID:19675993]http://dx.doi.org/10.1682/JRRD.2008.01.0007
1490
JRRD, Volume 51, Number 10, 2014
22. Blumentritt S. Biomechanische aspekte zur indikation vonprothesenkniegelenken [Biomechanical aspects of theindications of prosthetic knee joints]. Orthopädie-Technik.2004;55(6):508–24. German.
23. Sawers AB, Hafner BJ. Outcomes associated with the useof microprocessor-controlled prosthetic knees amongindividuals with unilateral transfemoral limb loss: A sys-tematic review. J Rehabil Res Dev. 2013;50(3):273–314.[PMID:23881757]http://dx.doi.org/10.1682/JRRD.2011.10.0187
24. Bellmann M, Schmalz T, Blumentritt S. Comparative bio-mechanical analysis of current microprocessor-controlledprosthetic knee joints. Arch Phys Med Rehabil. 2010;91(4):644–52. [PMID:20382300]http://dx.doi.org/10.1016/j.apmr.2009.12.014
25. Blumentritt S, Schmalz T, Jarasch R. The safety of C-leg:Biomechanical tests. J Prosthet Orthot. 2009;21(1):2–15.http://dx.doi.org/10.1097/JPO.0b013e318192e96a
26. Berry D, Olson MD, Larntz K. Perceived stability, func-tion, and satisfaction among transfemoral amputees usingmicroprocessor and non-microprocessor controlled pros-thetic knees: A multicenter survey. J Prosthet Orthot.2009;21(1):32–42.http://dx.doi.org/10.1097/JPO.0b013e318195b1d1
27. Kaufman KR, Levine JA, Brey RH, Iverson BK,McCrady SK, Padgett DJ, Joyner MJ. Gait and balance oftransfemoral amputees using passive mechanical andmicroprocessor-controlled prosthetic knees. Gait Posture.2007;26(4):489–93. [PMID:17869114]http://dx.doi.org/10.1016/j.gaitpost.2007.07.011
28. Mâaref K, Martinet N, Grumillier C, Ghannouchi S,André JM, Paysant J. Kinematics in the terminal swingphase of unilateral transfemoral amputees: Microproces-sor-controlled versus swing-phase control prostheticknees. Arch Phys Med Rehabil. 2010;91(6):919–25.[PMID:20510984]http://dx.doi.org/10.1016/j.apmr.2010.01.025
29. Segal AD, Orendurff MS, Klute GK, McDowell ML, Pec-oraro JA, Shofer J, Czerniecki JM. Kinematic and kineticcomparisons of transfemoral amputee gait using C-Legand Mauch SNS prosthetic knees. J Rehabil Res Dev.2006;43(7):857–70. [PMID:17436172] |http://dx.doi.org/10.1682/JRRD.2005.09.0147
30. Schmalz T, Blumentritt S, Jarasch R. Energy expenditureand biomechanical characteristics of lower limb amputeegait: The influence of prosthetic alignment and differentprosthetic components. Gait Posture. 2002;16(3):255–63.[PMID:12443950]http://dx.doi.org/10.1016/S0966-6362(02)00008-5
31. Kahle JT, Highsmith MJ, Hubbard SL. Comparison ofnonmicroprocessor knee mechanism versus C-Leg onProsthesis Evaluation Questionnaire, stumbles, falls,walking tests, stair descent, and knee preference. J Reha-
bil Res Dev. 2008;45(1):1–14. [PMID:18566922] http://dx.doi.org/10.1682/JRRD.2007.04.0054
32. Seymour R, Engbretson B, Kott K, Ordway N, Brooks G,Crannell J, Hickernell E, Wheeler K. Comparisonbetween the C-leg microprocessor-controlled prostheticknee and non-microprocessor control prosthetic knees: Apreliminary study of energy expenditure, obstacle courseperformance, and quality of life survey. Prosthet OrthotInt. 2007;31(1):51–61. [PMID:17365885]http://dx.doi.org/10.1080/03093640600982255
33. Highsmith MJ, Kahle JT, Miro RM, Mengelkoch LJ.Ramp descent performance with the C-Leg and interraterreliability of the Hill Assessment Index. Prosthet OrthotInt. 2013;37(5):362–68. [PMID:23327837]http://dx.doi.org/10.1177/0309364612470482
34. Hafner BJ, Willingham LL, Buell NC, Allyn KJ, SmithDG. Evaluation of function, performance, and preferenceas transfemoral amputees transition from mechanical tomicroprocessor control of the prosthetic knee. Arch PhysMed Rehabil. 2007;88(2):207–17. [PMID:17270519]http://dx.doi.org/10.1016/j.apmr.2006.10.030
35. Schmalz T, Blumentritt S, Marx B. Biomechanical analy-sis of stair ambulation in lower limb amputees. Gait Pos-ture. 2007;25(2):267–78. [PMID:16725325]http://dx.doi.org/10.1016/j.gaitpost.2006.04.008
36. Highsmith MJ, Kahle JT, Bongiorni DR, Sutton BS,Groer S, Kaufman KR. Safety, energy efficiency, and costefficacy of the C-Leg for transfemoral amputees: Areview of the literature. Prosthet Orthot Int. 2010;34(4):362–77. [PMID:20969495]http://dx.doi.org/10.3109/03093646.2010.520054
37. Alemayehu B, Warner KE. The lifetime distribution ofhealth care costs. Health Serv Res. 2004;39(3):627–42.[PMID:15149482]http://dx.doi.org/10.1111/j.1475-6773.2004.00248.x
38. Lubitz JD, Riley GF. Trends in Medicare payments in thelast year of life. N Engl J Med. 1993;328(15):1092–96.[PMID:8455667]http://dx.doi.org/10.1056/NEJM199304153281506
39. Hoover DR, Crystal S, Kumar R, Sambamoorthi U, Can-tor JC. Medical expenditures during the last year of life:Findings from the 1992–1996 Medicare current benefi-ciary survey. Health Serv Res. 2002;37(6):1625–42.[PMID:12546289]http://dx.doi.org/10.1111/1475-6773.01113
40. Calfo S, Smith J, Zezza M. Last year of life study. Balti-more (MD): Centers for Medicare & Medicaid Services,Office of the Actuary; 2004 [cited 2013 Oct 28]. Avail-able from: http://www.cms.gov/Research-Statistics-Data-and-Systems/Research/ActuarialStudies/downloads/Last_Year_of_Life.pdf
41. Limbless Statistics [Internet]. National Amputee Statisti-cal Database (NASDAB). Edinburgh (United Kingdom):
1491
KANNENBERG et al. Benefits of MPKs to limited community ambulators
The Amputee Statistical Database for the United King-dom Information Services Division, NHS Scotland; 2009 [cited 2012 Oct 10]. Available from: http://www.limbless-statistics.org/documents/Report2006-07.pdf
42. Buckley CM, O’Farrell A, Canavan RJ, Lynch AD, De LaHarpe DV, Bradley CP, Perry IJ. Trends in the incidenceof lower extremity amputations in people with and with-out diabetes over a five-year period in the Republic of Ire-land. PLoS ONE. 2012;7(7):e41492. [PMID:22859991]http://dx.doi.org/10.1371/journal.pone.0041492
43. Global Lower Extremity Amputation Study Group. Epi-demiology of lower extremity amputation in centres inEurope, North America and East Asia. Br J Surg. 2000;87(3):328–37. [PMID:10718803]http://dx.doi.org/10.1046/j.1365-2168.2000.01344.x
44. Gauthier-Gagnon C, Grisé MC, Potvin D. Enabling fac-tors related to prosthetic use by people with transtibial andtransfemoral amputation. Arch Phys Med Rehabil. 1999;80(6):706–13. [PMID:10378500]http://dx.doi.org/10.1016/S0003-9993(99)90177-6
45. Tinetti ME. Clinical practice. Preventing falls in elderlypersons. N Engl J Med. 2003;348(1):42–49.[PMID:12510042]http://dx.doi.org/10.1056/NEJMcp020719
46. Tinetti ME, Speechley M, Ginter SF. Risk factors for fallsamong elderly persons living in the community. N Engl JMed. 1988;319(26):1701–7. [PMID:3205267]http://dx.doi.org/10.1056/NEJM198812293192604
47. Maki BE, Holliday PJ, Topper AK. Fear of falling andpostural performance in the elderly. J Gerontol. 1991;46(4):M123–31. [PMID:2071833]http://dx.doi.org/10.1093/geronj/46.4.M123
48. Tinetti ME, Mendes de Leon CF, Doucette JT, Baker DI.Fear of falling and fall-related efficacy in relationship tofunctioning among community-living elders. J Gerontol.1994;49(3):M140–47. [PMID:8169336]http://dx.doi.org/10.1093/geronj/49.3.M140
49. Speechley M, Tinetti M. Falls and injuries in frail and vig-orous community elderly persons. J Am Geriatr Soc.1991;39(1):46–52. [PMID:1987256]
50. Nevitt MC. Falls in older persons: Risk factors and preven-tion. In: Berg RL, Cassells JS, Stokes J, editors. The secondfifty years: Promoting health and preventing disability. Wash-ington (DC): National Academy Press; 1990. p. 263–90.
51. Bertera EM, Bertera RL. Fear of falling and activityavoidance in a national sample of older adults in theUnited States. Health Soc Work. 2008;33(1):54–62.[PMID:18326450]http://dx.doi.org/10.1093/hsw/33.1.54
52. Fletcher PC, Hirdes JP. Restriction in activity associatedwith fear of falling among community-based seniors usinghome care services. Age Ageing. 2004;33(3):273–79.
[PMID:15082433] http://dx.doi.org/10.1093/ageing/afh077
53. Delbaere K, Crombez G, Vanderstraeten G, Willems T,Cambier D. Fear-related avoidance of activities, falls andphysical frailty. A prospective community-based cohortstudy. Age Ageing. 2004;33(4):368–73. [PMID:15047574]http://dx.doi.org/10.1093/ageing/afh106
54. Kempen GI, van Haastregt JC, McKee KJ, Delbaere K,Zijlstra GA. Socio-demographic, health-related and psy-chosocial correlates of fear of falling and avoidance ofactivity in community-living older persons who avoidactivity due to fear of falling. BMC Public Health. 2009;9:170–76. [PMID:19490640]http://dx.doi.org/10.1186/1471-2458-9-170
55. Mackenzie L, Byles J, D’Este C. Validation of self-reported fall events in intervention studies. Clin Rehabil.2006;20(4):331–39. [PMID:16719031]http://dx.doi.org/10.1191/0269215506cr947oa
56. Peel N. Validating recall of falls by older people. AccidAnal Prev. 2000;32(3):371–72. [PMID:10776852] http://dx.doi.org/10.1016/S0001-4575(99)00066-4
57. Schoppen T, Boonstra A, Groothoff JW, de VriesJ, Göeken LN, Eisma WH. The Timed “up and go”test: Reliability and validity in persons with unilaterallower limb amputation. Arch Phys Med Rehabil.1999;80(7): 825–28. [PMID:10414769]http://dx.doi.org/10.1016/S0003-9993(99)90234-4
58. Shumway-Cook A, Brauer S, Woollacott M. Predictingthe probability for falls in community-dwelling olderadults using the Timed Up & Go Test. Phys Ther. 2000;80(9):896–903. [PMID:10960937]
59. Bischoff HA, Stähelin HB, Monsch AU, Iversen MD,Weyh A, von Dechend M, Akos R, Conzelmann M, DickW, Theiler R. Identifying a cut-off point for normalmobility: A comparison of the timed ‘up and go’ test incommunity-dwelling and institutionalised elderly women.Age Ageing. 2003;32(3):315–20. [PMID:12720619]http://dx.doi.org/10.1093/ageing/32.3.315
60. Thrane G, Joakimsen RM, Thornquist E. The associationbetween timed up and go test and history of falls: TheTromsø study. BMC Geriatr. 2007;7:1–7.[PMID:17222340]http://dx.doi.org/10.1186/1471-2318-7-1
61. Desai A, Goodman V, Kapadia N, Shay BL, Szturm T.Relationship between dynamic balance measures andfunctional performance in community-dwelling elderlypeople. Phys Ther. 2010;90(5):748–60.[PMID:20223944]http://dx.doi.org/10.2522/ptj.20090100
62. Dite W, Connor HJ, Curtis HC. Clinical identification ofmultiple fall risk early after unilateral transtibial amputa-tion. Arch Phys Med Rehabil. 2007;88(1):109–14.
1492
JRRD, Volume 51, Number 10, 2014
[PMID:17207685] http://dx.doi.org/10.1016/j.apmr.2006.10.015
63. Berg K, Wood-Dauphinee S, Williams JI. The Balance Scale: Reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med. 1995;27(1):27–36. [PMID:7792547]
64. Major MJ, Fatone S, Roth EJ. Validity and reliability of the Berg Balance Scale for community-dwelling persons with lower-limb amputation. Arch Phys Med Rehabil. 2013;94(11):2194–2202. [PMID:23856150]http://dx.doi.org/10.1016/j.apmr.2013.07.002
65. Houdijk H, van Ooijen MW, Kraal JJ, Wiggerts HO, Polomski W, Janssen TW, Roerdink M. Assessing gait adaptability in people with a unilateral amputation on an instrumented treadmill with a projected visual context. Phys Ther. 2012;92(11):1452–60.[PMID:22836005] http://dx.doi.org/10.2522/ptj.20110362
66. Lajoie Y, Gallagher SP. Predicting falls within the elderly community: Comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch Gerontol Geriatr. 2004;38(1):11–26.[PMID:14599700]http://dx.doi.org/10.1016/S0167-4943(03)00082-7
67. Powell LE, Myers AM. The Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci. 1995;50A(1):M28–34. [PMID:7814786]http://dx.doi.org/10.1093/gerona/50A.1.M28
68. Miller WC, Speechley M, Deathe AB. Balance confi-dence among people with lower-limb amputations. Phys Ther. 2002;82(9):856–65. [PMID:12201800]
69. Gailey RS, Roach KE, Applegate EB, Cho B, Cunniffe B, Licht S, Maguire M, Nash MS. The Amputee Mobility Predictor: An instrument to assess determinants of the lower-limb amputee’s ability to ambulate. Arch Phys Med Rehabil. 2002;83(5):613–27. [PMID:11994800]http://dx.doi.org/10.1053/apmr.2002.32309
70. Datta D, Ariyaratnam R, Hilton S. Timed walking test: An all-embracing outcome measure for lower-limb ampu-tees? Clin Rehabil. 1996;10:227–32.http://dx.doi.org/10.1177/026921559601000307
71. Brooks D, Parsons J, Hunter JP, Devlin M, Walker J. The2-minute walk test as a measure of functional improve-ment in persons with lower limb amputation. Arch Phys Med Rehabil. 2001;82(10):1478–83. [PMID:11588757] http://dx.doi.org/10.1053/apmr.2001.25153
72. Theeven P, Hemmen B, Stevens C, Ilmer E, Brink P, Seelen H. Feasibility of a new concept for measuring actual functional performance in daily life of transfemoral amputees. J Rehabil Med. 2010;42(8):744–51.[PMID:20809056]http://dx.doi.org/10.2340/16501977-0591
73. Vrieling AH, van Keeken HG, Schoppen T, Otten E, Hal-bertsma JP, Hof AL, Postema K. Uphill and downhill walking in unilateral lower limb amputees. Gait Posture. 2008;28(2):235–42. [PMID:18242995] http://dx.doi.org/10.1016/j.gaitpost.2007.12.006
74. Fradet L, Alimusaj M, Braatz F, Wolf SI. Biomechanical analysis of ramp ambulation of transtibial amputees with an adaptive ankle foot system. Gait Posture. 2010;32(2): 191–98. [PMID:20457526] http://dx.doi.org/10.1016/j.gaitpost.2010.04.011
75. Pelland L, McKinley P. The Montreal Rehabilitation Per-formance Profile: A task-analysis approach to quantify stair descent performance in children with intellectual dis-ability. Arch Phys Med Rehabil. 2001;82(8):1106–14. [PMID:11494191] http://dx.doi.org/10.1053/apmr.2001.24225
76. Legro MW, Reiber GD, Smith DG, del Aguila M, Larsen J, Boone D. Prosthesis evaluation questionnaire for per-sons with lower limb amputations: Assessing prosthesis-related quality of life. Arch Phys Med Rehabil. 1998;79(8):931–38. [PMID:9710165] http://dx.doi.org/10.1016/S0003-9993(98)90090-9
77. Franchignoni F, Giordano A, Ferriero G, Orlandini D, Amoresano A, Perucca L. Measuring mobility in people with lower limb amputation: Rasch analysis of the mobil-ity section of the prosthesis evaluation questionnaire. J Rehabil Med. 2007;39(2):138–44. [PMID:17351696] http://dx.doi.org/10.2340/16501977-0033
78. Heinemann AW, Bode RK, O’Reilly C. Development and measurement properties of the Orthotics and Prosthetics Users’ Survey (OPUS): A comprehensive set of clinical outcome instruments. Prosthet Orthot Int. 2003;27(3): 191–206. [PMID:14727700] http://dx.doi.org/10.1080/03093640308726682
79. Franchignoni F, Orlandini D, Ferriero G, Moscato TA. Reliability, validity, and responsiveness of the Locomotor Capabilities Index in adults with lower-limb amputation undergoing prosthetic training. Arch Phys Med Rehabil. 2004;85(5):743–48. [PMID:15129398] http://dx.doi.org/10.1016/j.apmr.2003.06.010
80. Franchignoni F, Giordano A, Ferriero G, Muñoz S, Orlan-dini D, Amoresano A. Rasch analysis of the Locomotor Capabilities Index-5 in people with lower limb amputa-tion. Prosthet Orthot Int. 2007;31(4):394–404. [PMID:18050010] http://dx.doi.org/10.1080/03093640701253952
81. Panesar BS, Morrison P, Hunter J. A comparison of three measures of progress in early lower limb amputee rehabil-itation. Clin Rehabil. 2001;15(2):157–71. [PMID:11330761] http://dx.doi.org/10.1191/026921501669259476
1493
KANNENBERG et al. Benefits of MPKs to limited community ambulators
82. Gauthier-Gagnon C, Grise MC. Tools for outcome mea-surement in lower limb amputation. Montreal (Canada):University of Montreal; 2001.
83. Callaghan BG, Sockalingam S, Treweek SP, Condie ME.A post-discharge functional outcome measure for lowerlimb amputees: Test-retest reliability with trans-tibialamputees. Prosthet Orthot Int. 2002;26(2):113–19.[PMID:12227445]http://dx.doi.org/10.1080/03093640208726633
84. Devlin M, Pauley T, Head K, Garfinkel S. HoughtonScale of prosthetic use in people with lower-extremityamputations: Reliability, validity, and responsiveness tochange. Arch Phys Med Rehabil. 2004;85(8):1339–44.[PMID:15295762]http://dx.doi.org/10.1016/j.apmr.2003.09.025
85. Miller WC, Deathe AB, Speechley M. Lower extremityprosthetic mobility: A comparison of 3 self-report scales.Arch Phys Med Rehabil. 2001;82(10):1432–40.[PMID:11588750]http://dx.doi.org/10.1053/apmr.2001.25987
86. Hart DL. Orthotics and Prosthetics National Office Out-comes Tool (OPOT): Initial reliability and validity assess-ment for lower extremity prosthetics. J Prosthet Orthot.1999;11:101–11.http://dx.doi.org/10.1097/00008526-199901140-00007
87. Ryall NH, Eyres SB, Neumann VC, Bhakta BB, TennantA. The SIGAM mobility grades: A new population-specificmeasure for lower limb amputees. Disabil Rehabil. 2003;25(15):833–44. [PMID:12851094]http://dx.doi.org/10.1080/0963828021000056460
88. Gallagher P, Maclachlan M. Development and psycho-metric evaluation of the Trinity Amputation and Prosthe-sis Experience Scales (TAPES). Rehabil Psychol. 2000;45:130–54. http://dx.doi.org/10.1037/0090-5550.45.2.130
89. Gallagher P, Maclachlan M. The Trinity Amputation andProsthesis Experience Scales and quality of life in peoplewith lower-limb amputation. Arch Phys Med Rehabil.2004;85(5):730–36. [PMID:15129396]http://dx.doi.org/10.1016/j.apmr.2003.07.009
90. Hofstad C, Linde H, Limbeek J, Postema K. Prescriptionof prosthetic ankle-foot mechanisms after lower limb ampu-tation. Cochrane Database Syst Rev. 2004;(1):CD003978.[PMID:14974050]http://dx.doi.org/10.1002/14651858.CD003978.pub2
91. van Tulder MW, Assendelft WJ, Koes BW, Bouter LM.Method guidelines for systematic reviews in the CochraneCollaboration Back Review Group for Spinal Disorders.Spine. 1997;22(20):2323–30. [PMID:9355211]http://dx.doi.org/10.1097/00007632-199710150-00001
92. Verhagen AP, de Vet HC, de Bie RA, Kessels AG, BoersM, Bouter LM, Knipschild PG. The Delphi list: A criterialist for quality assessment of randomized clinical trials for
conducting systematic reviews developed by Delphi con-sensus. J Clin Epidemiol. 1998;51(12):1235–41. [PMID:10086815] http://dx.doi.org/10.1016/S0895-4356(98)00131-0
93. Downs SH, Black N. The feasibility of creating a check-list for the assessment of the methodological quality bothof randomised and non-randomised studies of health careinterventions. J Epidemiol Community Health. 1998;52(6):377–84. [PMID:9764259]http://dx.doi.org/10.1136/jech.52.6.377
94. Reisch JS, Tyson JE, Mize SG. Aid to the evaluation oftherapeutic studies. Pediatrics. 1989;84(5):815–27.[PMID:2797977]
95. Zaza S, Carande-Kulis VG, Sleet DA, Sosin DM, ElderRW, Shults RA, Dinh-Zarr TB, Nichols JL, ThompsonRS; Task Force on Community Preventive Services.Methods for conducting systematic reviews of the evi-dence of effectiveness and economic efficiency of inter-ventions to reduce injuries to motor vehicle occupants.Am J Prev Med. 2001;21(4 Suppl):23–30.[PMID:11691559]http://dx.doi.org/10.1016/S0749-3797(01)00379-8
96. Samuelsson KA, Töytäri O, Salminen AL, Brandt A.Effects of lower limb prosthesis on activity, participation,and quality of life: A systematic review. Prosthet OrthotInt. 2012;36(2):145–58. [PMID:22307861]http://dx.doi.org/10.1177/0309364611432794
97. Gremeaux V, Damak S, Troisgros O, Feki A, Laroche D,Perennou D, Benaim C, Casillas JM. Selecting a test forthe clinical assessment of balance and walking capacity atthe definitive fitting state after unilateral amputation: Acomparative study. Prosthet Orthot Int. 2012;36(4):415–22.[PMID:22389424]http://dx.doi.org/10.1177/0309364612437904
98. Theeven P, Hemmen B, Rings F, Meys G, Brink P, SmeetsR, Seelen H. Functional added value of microprocessor-controlled knee joints in daily life performance of Medi-care Functional Classification Level-2 amputees. J Reha-bil Med. 2011;43(10):906–15. [PMID:21947182]
99. Theeven PJ, Hemmen B, Geers RP, Smeets RJ, Brink PR,Seelen HA. Influence of advanced prosthetic knee jointson perceived performance and everyday life activity levelof low-functional persons with a transfemoral amputationor knee disarticulation. J Rehabil Med. 2012;44(5):454–61. [PMID:22549656]http://dx.doi.org/10.2340/16501977-0969
100. Burnfield JM, Eberly VJ, Gronely JK, Perry J, Yule WJ,Mulroy SJ. Impact of stance phase microprocessor-controlled knee prosthesis on ramp negotiation and commu-nity walking function in K2 level transfemoral amputees.Prosthet Orthot Int. 2012;36(1):95–104.
1494
JRRD, Volume 51, Number 10, 2014
[PMID:22223685] http://dx.doi.org/10.1177/0309364611431611
101. Eberly VJ, Mulroy SJ, Gronley JK, Perry J, Yule WJ,Burnfield JM. Impact of a stance phase microprocessor-controlled knee prosthesis on level walking in lower func-tioning individuals with a transfemoral amputation. Pros-thet Orthot Int. 2014;38(6):447–55. [PMID:24135259]http://dx.doi.org/10.1177/0309364613506912
102. Wetz HH, Hafkemeyer U, Drerup B. Einfluss des C-Leg-Kniegelenk-Passteiles der Fa. Otto Bock auf die Versor-gungsqualität Oberschenkelamputierter. Eine klinisch-biomechanische Studie zur Eingrenzung von Indikation-skriterien [The influence of the C–Leg knee shin systemof Otto Bock on the care of above-knee amputees: A clin-ical biomechanical study to define indications]. Ortho-pade. 2005;34(4):298–319. German. [PMID:15812621]http://dx.doi.org/10.1007/s00132-005-0783-z
103. van der Linde H, Hofstad CJ, Geurts AC, Postema K,Geertzen JH, van Limbeek J. A systematic literaturereview of the effect of different prosthetic components onhuman functioning with a lower-limb prosthesis. J Reha-bil Res Dev. 2004;41(4):555–70. [PMID:15558384]http://dx.doi.org/10.1682/JRRD.2003.06.0102
104. Devlin M, Sinclair LB, Colman D, Parsons J, Nizio H,Campbell JE. Patient preference and gait efficiency in ageriatric population with transfemoral amputation using afree-swinging versus a locked prosthetic knee joint. ArchPhys Med Rehabil. 2002;83(2):246–49.[PMID:11833030]http://dx.doi.org/10.1053/apmr.2002.27464
105. Resnik L, Borgia M. Reliability of outcome measures forpeople with lower-limb amputations: Distinguishing truechange from statistical error. Phys Ther. 2011;91(4):555–65.[PMID:21310896]http://dx.doi.org/10.2522/ptj.20100287
106. Seymour R. Prosthetics and orthotics: Lower limb andspinal. Philadelphia (PA): Lippincott Williams & Wilkins;2002.
107. Radcliffe CW. The Knud Jansen Lecture: Above-kneeprosthetics. Prosthet Orthot Int. 1977;1(3):146–60.[PMID:617371]
108. Radcliffe CW. Four-bar linkage prosthetic knee mecha-nisms: Kinematics, alignment and prescription criteria.Prosthet Orthot Int. 1994;18(3):159–73. [PMID:7724349]
109. Highsmith MJ. Microprocessor knees: Considerations foraccommodation and training. J Prosthet Orthot. 2013;25(4S):60–64.http://dx.doi.org/10.1097/JPO.0b013e3182a891b5
110. Isakov E, Susak Z, Becker E. Energy expenditure and car-diac response in above-knee amputees while using pros-theses with open and locked knee mechanisms. Scand JRehabil Med Suppl. 1985;12:108–11. [PMID:3868034]
111. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Rich-ardson WS. Evidence based medicine: What it is and whatit isn’t. BMJ. 1996;312(7023):71–72. [PMID:8555924]http://dx.doi.org/10.1136/bmj.312.7023.71
112. Morgenroth DC. Prescribing physician perspective onmicroprocessor-controlled prosthetic knees. J ProsthetOrthot. 2013;25(4S):53–55.http://dx.doi.org/10.1097/JPO.0b013e3182a88d02
113. Parker K, Kirby RL, Adderson J, Thompson K. Ambula-tion of people with lower-limb amputations: Relationshipbetween capacity and performance measures. Arch PhysMed Rehabil. 2010;91(4):543–49. [PMID:20382285]http://dx.doi.org/10.1016/j.apmr.2009.12.009
114. Perera S, Mody SH, Woodman RC, Studenski SA. Mean-ingful change and responsiveness in common physicalperformance measures in older adults. J Am Geriatr Soc.2006;54(5):743–49. [PMID:16696738]http://dx.doi.org/10.1111/j.1532-5415.2006.00701.x
115. Kwon S, Perera S, Pahor M, Katula JA, King AC, GroesslEJ, Studenski SA. What is a meaningful change in physi-cal performance? Findings from a clinical trial in olderadults (the LIFE-P study). J Nutr Health Aging. 2009;13(6):538–44. [PMID:19536422]http://dx.doi.org/10.1007/s12603-009-0104-z
116. Perry J, Garrett M, Gronley JK, Mulroy SJ. Classificationof walking handicap in the stroke population. Stroke.1995;26(6):982–89. [PMID:7762050]http://dx.doi.org/10.1161/01.STR.26.6.982
117. Alley DE, Hicks GE, Shardell M, Hawkes W, Miller R,Craik RL, Mangione KK, Orwig D, Hochberg M, ResnickB, Magaziner J. Meaningful improvement in gait speed inhip fracture recovery. J Am Geriatr Soc. 2011;59(9):1650–57. [PMID:21883109]http://dx.doi.org/10.1111/j.1532-5415.2011.03560.x
118. Purser JL, Weinberger M, Cohen HJ, Pieper CF, MoreyMC, Li T, Williams GR, Lapuerta P. Walking speed pre-dicts health status and hospital costs for frail elderly maleveterans. J Rehabil Res Dev. 2005;42(4):535–46.[PMID:16320148]http://dx.doi.org/10.1682/JRRD.2004.07.0087
119. Schmid A, Duncan PW, Studenski S, Lai SM, Richards L,Perera S, Wu SS. Improvements in speed-based gait clas-sifications are meaningful. Stroke. 2007;38(7):2096–2100.[PMID:17510461]http://dx.doi.org/10.1161/STROKEAHA.106.475921
120. Viccaro LJ, Perera S, Studenski SA. Is timed up and gobetter than gait speed in predicting health, function, andfalls in older adults? J Am Geriatr Soc. 2011;59(5):887–92. [PMID:21410448]http://dx.doi.org/10.1111/j.1532-5415.2011.03336.x
121. Castell MV, Sánchez M, Julián R, Queipo R, Martín S,Otero Á. Frailty prevalence and slow walking speed in

1495
KANNENBERG et al. Benefits of MPKs to limited community ambulators
persons age 65 and older: Implications for primary care. BMC Fam Pract. 2013;14(1):86. [PMID:23782891] http://dx.doi.org/10.1186/1471-2296-14-86
122. Hardy SE, Perera S, Roumani YF, Chandler JM, Studen-ski SA. Improvement in usual gait speed predicts bettersurvival in older adults. J Am Geriatr Soc. 2007;55(11):1727–34. [PMID:17916121]http://dx.doi.org/10.1111/j.1532-5415.2007.01413.x
123. Studenski S, Perera S, Patel K, Rosano C, Faulkner K,Inzitari M, Brach J, Chandler J, Cawthon P, Connor EB,Nevitt M, Visser M, Kritchevsky S, Badinelli S, Harris T,Newman AB, Cauley J, Ferrucci L, Guralnik J. Gait speedand survival in older adults. JAMA. 2011;305(1):50–58.[PMID:21205966]http://dx.doi.org/10.1001/jama.2010.1923
Submitted for publication May 2, 2014. Accepted in revised form September 30, 2014.
This article and any supplementary material should be cited as follows:Kannenberg A, Zacharias B, Pröbsting E. Benefits of microprocessor-controlled prosthetic knees to limited community ambulators: Systematic review. J Rehabil Res Dev. 2014;51(10):1469–96.http://dx.doi.org/10.1682/JRRD.2014.05.0118
Kenevo | Clinical Research Summary – Lansade (2018) | Ottobock Page 1 of 1
Clinical Research Summary
Mobility and Safety with a Microprocessor-Controlled Knee in Moderately Active Amputees Lansade C, Vicaut E, Paysant J, Ménager D, Cristina MC, Braatz F, Domayer S, Pérennou D, Chiesa G. Mobility and safety with a microprocessor-controlled knee in moderately active amputees: A multi-centric randomized crossover trial. Ann Phys Rehabil Med 2018 May 14. pii: S1877-0657(18)30058-7. doi:10.1016/j.rehab.2018.04.003. [Epub ahead ofprint]
This was a multinational (France, Germany, Austria), multi-center (16 sites), randomized cross-over trial comparing the effects of a microprocessor-controlled prosthetic knee specifically designed for subjects with above-knee amputation and low to moderate mobility (Kenevo®) to those of non-microprocessor knees (NMPK) typically covered and prescribed for subjects with MFCL-2 mobility. Participants were eligible for enrollment if they presented a moderate level of mobility as defined by ICF items d4601 and d4602 (corresponds to MFCL-2 in the U.S.) and a completion time for the Timed-up-and-go test (TUG) of >19 sec, which indicates an increased risk for multiple falls in transtibial amputees (Dite et al., 2007).
Subjects were randomized to either continue to use their NMPK for 30 days and then use the Kenevo MPK for 90 days, or to start using the Kenevo MPK right away for 90 days and then return to their previous NMPK for 30 days.
The primary outcome measure of the study was the TUG completion time, secondary outcome measures chosen were the Locomotor Capabilities Index 5 (LCI-5), the SF-36v2 for quality of life, and the QUEST questionnaire for satisfaction with the prosthesis.
The trial originally enrolled 35 patients, of whom five dropped out or were excluded for medical reasons before the baseline assessment. Eventually, 30 individuals with transfemoral amputation and a mean age of 65.6 ± 10.1 years were available for the intention-to-treat (ITT) analysis. Because of three protocol violations, 27 individuals with a mean age of 64.5 ± 9.7 years were subjected to a per-protocol (PP) analysis.
Results: With the Kenevo MPK, subjects performed the TUG significantly faster [ITT median Q1-Q3: 18.2 sec. (16.2-25.2) versus 21.8 sec. (19.5-28.4), p=.001; PP median Q1-Q3: 17.9 sec. (15.4-22.7) versus 21.4 sec. (19.3-26.6), p=.001)] as compared to the NMPK condition, indicating a reduced risk of falling with the MPK. Perceived mobility as assessed with the LCI-5 improved significantly in both the ITT (p=.006) and the PP analysis (p=.02), as did the SF-36v2 mental component score (p=.01), physical activity score (p=.04), limitations related to physical health score (p=.005), mental health score (p=.009) and vitality score (p=.02) in the ITT analysis, and the mental component score (p=.03), limitations related to physical health score (p=.002), mental health score (p=.007) and vitality score (p=.03) in the PP analysis. Subject satisfaction was also significantly improved with the Kenevo MPK.
Conclusion: In conclusion, this multi-center randomized cross-over trial confirms the results of earlier research suggesting that individuals with transfemoral amputation and MFCL-2 mobility may benefit from using MPKs in terms of improved safety, increased mobility and better quality of life.
Kenevo Reimbursement Guide | Summary FASTK2 Study - Kaufman | Ottobock 1 of 1
Clinical Research Summary
Functional Assessment and Satisfaction of Low Mobility Transfemoral Amputees with Microprocessor Knees Kaufman KR, Bernhardt KA, Symms K. Functional assessment and satisfaction of transfemoral amputees with mobility (FASTK2): A clinical trial of microprocessor-controlled vs. non-microprocessor-controlled knees. Clin Biomech (Bristol, Avon) 2018 Oct;58:116-122. doi: 10.1016/ j.clinbiomech.2018.07.012. Epub 2018 Jul 19.
This study was a prospective non-randomized crossover clinical trial. Each subject was tested using their current non-microprocessor knee (NMPK), fit and tested with a microprocessor knee (MPK) after approximately 3 months of use, and then refit with their NMPK and tested again after 4 weeks, i.e. A-B-A study design.
This study enrolled 50 unilateral transfemoral amputees (TFA) fit in prosthetic clinics in 19 states throughout the United States. Subjects had a mean age of 69±9 years (range 55-83 yr.) and were Medicare Functional Classification Level K2 (n=48) or K3 (n=2). The primary amputation etiologies were peripheral arterial disease (50%), total knee arthroplasty infection (14%), infection (12%), trauma (10%), deep vein thrombosis (8%), cancer (4%), or blood disorder (2%). The subjects received a randomly assigned MPK knee from one of four manufacturers (OttoBock Compact [MP stance control knee], Ossur Rheo 3, Endolite Orion 2, Freedom Innovation Plié 3 [all MP swing and stance control knees]). All prosthesis fittings were performed by the subjects' own certified prosthetist according to the manufacturer's fitting guidelines
with oversite provided by the manufacturer's representative.
Outcome measures were self-reported falls in the month prior to each assessment, patient activity (ActiGraph GT3X) over 4 days, and patient satisfaction as assessed by the Prosthesis Evaluation Questionnaire (PEQ).
Results: Seventeen subjects dropped out before they could be fit with a MPK, leaving 33 datasets for the per-protocol analysis. Use of a MPK resulted in a significant reduction in falls (p=0.01). The median number of falls of 2.0 (IQR 0.0–6.0) at baseline when using a NMPK was reduced to 0.0 when using the MPK (IQR 0.0–3.25) and increased to 3.0 falls (IQR 0–3.0) falls per person per month when reverting back to the NMPK. Notably, when reverting back to the NMPK, patients reported a greater fear of falling and the prosthetists had concerns about patient safety, which resulted in 10 subjects declining to participate in the reconversion to the NMPK.
The subjects spent significantly less time sitting (p=0.01) when using the MPK, and the decrease in amount of time seated was offset by a significant increase in median activity counts (p=0.02). The time spent sitting increased and the time active decreased again when subjects returned to their NMPK. Further, the complexity of the gait as measured by the entropy increased when using the MPK and returned toward the baseline level when reverting back to the NMPK. However, the increase in gait entropy did not attain statistical significance. Patient satisfaction reflected the reduction in falls and improvement in activity. There was a significant improvement in PEQ satisfaction subscales when using the MPK (p≤0.01).
Conclusion: “This clinical trial confirmed that the provision of a MPK to patients with a TFA and low, i.e. K2, mobility will result in improved function inthe free-living environment, a reduction in falls,and, subsequently, improved patient satisfaction.”
Clinical Studies Using Microprocessor Knees with K2 Subjects
Kenevo Reimbursement Guide | K2 Clinical Studies | Ottobock 1 of 1
1. Kaufman KR, Bernhardt KA, Symms K.Functional assessment and satisfaction oftransfemoral amputees with mobility (FASTK2):A clinical trial of microprocessor-controlled vs.non-microprocessor-controlled knees. ClinBiomech (Bristol, Avon) 2018 Oct;58:116-122.doi: 10.1016/ j.clinbiomech.2018.07.012. Epub2018 Jul 19. View Article
2. Lansade C, Vicaut E, Paysant J, Ménager D,Cristina MC, Braatz F, Domayer S, Pérennou D,Chiesa G. Mobility and safety with amicroprocessor-controlled knee in moderatelyactive amputees: A multi-centric randomizedcrossover trial. Ann Phys Rehabil Med, 2018 May14. pii: S1877-0657(18) 30058-7. doi: 10.1016/j.rehab.2018.04.003. [Epub ahead of print]View Article
3. Mileusnic MP, Hahn A, Reiter S. Effects of a novelmicroprocessor-controlled knee, Kenevo, on thesafety, mobility, and satisfaction of lower-activity patients with transfemoral amputation. J Prosthet Orthot, 2017;29(4):198-205.View Article
4. Kannenberg A, Zacharias B, Pröbsting E.Benefits of microprocessor-controlled prostheticknees to limited community ambulators:Systematic review. J. Rehabil. Med. 2014;51(10): 1469-1496. View Article
5. Eberly VJ, Mulroy SJ, Gronley JK, Perry J, YuleWJ, Burnfield JM. Impact of a stance phasemicroprocessor-controlled knee prosthesis onlevel walking in lower functioning individualswith a transfemoral amputation. Prosthet Orthot Int, 2014; 38(6): 447-55 (ISSN: 1746-1553)View Article
6. Theeven P, et al. Influence of AdvancedProsthetic Knee Joints on Perceived Performanceand Everyday Life Activity Level of Low-Functional Persons with a transfemoralAmputation or Knee Disarticulation. J. Rehabil. Med. 2012;44:454-461 View Article
7. Burnfield JM, et.al. Impact of Stance PhaseMicroprocessor-Controlled Knee Prosthesis onRamp Negotiation and Community WalkingFunction in K2 Level Transfemoral Amputees.POI. 2012;36(1):95-104. View Article
8. Theeven P, et al. Functional Added Value ofMicroprocessor-Controlled Prosthetic Knee Jointsin Daily Life Performance of Medicare FunctionalClassification Level-2 Amputees. J. Rehabil. Med. 2011;43:906-915. View Article
9. Hafner BJ. et al. Differences in Function andSafety between Medicare FunctionalClassification Level-2 and -3 TransfemoralAmputees and Influence of Prosthetic Knee JointControl. J. Rehabil. Med. 2009;46(3):417-434.View Article
10. Kahle JT, et al. Comparison of Non-Microprocessor Knee Mechanism versus C-Leg onProsthesis Evaluation Questionnaire, Stumbles,Falls, Walking Tests, Stair Descent, and KneePreference. J. Rehabil. Med. 2008;45(1):1-14.View Article
Contact information: Ottobock US ∙ P 800 328 4058 ∙ F 800 962 2549 Ottobock CA ∙ P 800 328 4058 ∙ F 800 962 2549professionals.ottobockus.com professionals.ottobock.ca.com [email protected]
© 2
019
Otto
Boc
k H
ealth
Car
e LP
● 0
1259



















