Embed Size (px)
Citation preview

January 2015 1
Kent Joint Strategic Needs Assessment (Kent JSNA)
Kent ‘Dementia’ JSNA Chapter Summary Update ‘2014/15’
Contact: [email protected] Website: www.kpho.org.uk

January 2015 2
Kent Dementia JSNA Chapter Update 2014 Introduction Dementia is a triad of problems: memory loss, decline in some other aspect of cognition, and difficulties with activities of daily living. More formally, it is a syndrome (that is, a distinct pattern of symptoms and signs) that can be caused by many brain disorders, most of which progress gradually over several years. The symptoms of dementia occur in three groups:
1. Cognitive dysfunction, resulting in problems with memory, language, attention, thinking, orientation, calculation, and problem-solving.
2. Psychiatric and behavioural problems, such as changes in personality, emotional control, social behaviour, depression, agitation, hallucinations, and delusions.
3. Difficulties with activities of daily living, such as driving, shopping, eating, and dressing.
Dementia mainly affects older people, although there is a growing awareness of cases starting before the age of 65. After 65, the likelihood of developing dementia roughly doubles every five years. Early-onset (or young-onset) dementia, by convention, is dementia that develops before 65 years of age. The most common causes of dementia include:
• Alzheimer's disease (about 50%). • Vascular dementia (about 25%). • Dementia with Lewy bodies (DLB) (about 15%). • Frontotemporal dementia (less than 5%).
Source: NICE Clinical Knowledge Summaries
http://cks.nice.org.uk/dementia#!topicsummary Key Issues and Gaps
The expected number of elderly people >65 yrs and over with a limiting long term illness is expected to increase from 120,000 in 2012 to 145,000 in 2020. Of these, the expected number of elderly people with dementia is expected to increase from just under 20,000 in 2012 to just under 25,000 people in 2020.
Based on 2013 estimates, the observed prevalence of dementia (number of dementia patients on QOF registers) is approximately 44% of the expected prevalence across Kent or 9,221 which is an improvement from 37% based on estimates made in 2011.
Who’s at Risk and Why?

January 2015 3
Table 1: The consensus estimates of the population prevalence (%) of late-onset dementia
Previous estimates Current estimates
(Dementia UK 2007) (Dementia UK 2014)
Age (years) Female Male Total Female Male Total
60-64 (0.1)* (0.2)* (0.2)* 0.9 0.9 0.9
65-69 1.0 1.5 1.3 1.8 1.5 1.7
70-74 2.4 3.1 2.9 3.0 3.1 3.0
75-79 6.5 5.1 5.9 6.6 5.3 6.0
80-84 13.3 10.2 12.2 11.7 10.3 11.1
85-89 22.2 16.7 20.3 20.2 15.1 18.3
90-94 29.6 27.5 28.6 33.0 22.6 29.9
95+ 34.4 30.0 32.5 44.2 28.8 41.1
* In the Dementia UK 2007 report, the prevalence of dementia among those aged 60-64 was estimated as part of the young-onset dementia consensus In 2013-14 a Direct Enhanced Service (DES), Facilitating Timely Diagnosis and Support, was introduced for primary care with the aim of encouraging practices to identify patients at clinical risk of dementia, offer an assessment to detect for possible signs of dementia in those at risk, offer a referral for diagnosis where dementia is suspected and support the health and wellbeing of carers of patients diagnosed with dementia. ‘At-risk’ patients were defined as:
Patients aged 60 or over with cardiovascular disease, stroke, peripheral vascular disease or diabetes
Patients aged 40 or over with Down’s syndrome
Other patients aged 50 or over with learning disabilities
Patients with long-term neurological conditions which have a known neurodegenerative element, for example Parkinson’s disease.
In October 2014, NHS England (NHSE) published a second DES, Dementia Identification Scheme. In addition to identifying and referring those individuals at high risk of dementia, this enhanced service also requires practices to work with nursing and care homes to identify patients in their care who may have symptoms of dementia and offer a dementia assessment. It also encourages GPs to make the diagnosis, where they believe they have the skills and competencies to do so. This complements the Facilitating Timely Diagnosis and Support DES, but will expire on 31 March 2015. Early onset Dementia is much rarer in people under 65 as it is estimated that only 2.2 per cent of people who have dementia have young onset dementia. In Kent there are approximately 400 people currently estimated to have young onset dementia. However, according to the Alzheimer Society’s 2007 report ‘Dementia UK: Full

January 2015 4
Report’ the prevalence of early onset dementia could be up to three times higher as it is often missed or undiagnosed. Dementia and learning disability People with Down’s Syndrome have an increased risk of developing Alzheimer’s disease. Three per cent of people with Down’s syndrome in their 30s have dementia, rising to 40 percent in their 50s. By the age of 60 people with Down’s Syndrome have a 55 percent chance of developing dementia compared to a five per cent chance within the general population. The actual numbers are small but with more people with Down’s Syndrome now reaching older age there will be increasing numbers of people with Down’s Syndrome and dementia, who will require specialist assessment and support. The prevalence of dementia in people with other forms of learning disability is also higher than in the general population. Some studies (Cooper 1997, Lund 1985, Moss and Patel 1993) suggest that the following percentages of people with learning disabilities not due to Down’s Syndrome have dementia: 50 years and over: 13 per cent 65 years and over: 22 per cent. This is about four times higher than in the general population. Black and minority ethnic (BME) population Currently prevalence rates for dementia in people from black, Asian and minority ethnic communities in the UK have not been identified. Six per cent of people from black, Asian and minority ethnic communities with dementia experience early onset dementia compared with only 2.2 per cent for the population as a whole, reflecting the younger age profile of these communities. Evidence shows that certain communities such as those from South Asia, African and Caribbean backgrounds have higher incidence and prevalence of cardiovascular disease, which will make them more prone to vascular dementia. There is likely to be significant growth in the number of people with dementia living in black, Asian and minority ethnic communities as the current, relatively young population ages. The Level of Need in the Population Approximately 20,813 people aged over 65 are estimated to have dementia in Kent based on 2013-14 estimates. By 2017 it is predicted that this figure will increase to 21,991. Diagnosis rates for dementia in Kent are around 44%. One of the key objectives within the Kent and Medway strategic plan is to increase these rates to 60%. However, CCGs are coming under increasing pressure from NHSE to increase rates to 67% by March 2015, in line with the commitment given in the Prime Minister’s

January 2015 5
Dementia Challenge and their progress towards this target is being measured on a monthly basis. Tables 1 and 2 show the current situation in terms of the prevalence of dementia and how many patients are on the QOF registers. The estimated growth has then been calculated to 2015 showing the increase in numbers of people with dementia depending on diagnosis rates. Figures have been described by Local Authority and CCG respectively. The tables show that by 2015, assuming a 60% diagnosis rate, 14,455 people will be diagnosed with dementia across Kent and Medway. This means that in two years an additional 6,189 people will need to be assessed as they enter the dementia pathway as people who are newly diagnosed. Table 2: Estimates of prevalence of dementia aged 30+, at varying levels of ascertainment, 2013-14 projected to 2017
Local authorities
2017 - Showing expected numbers at different levels of ascertainment
2013-14
Estimated prevalence
At 2013-14 QOF level
Ascertainment levels
Local authority Estimated prevalence
QOF register
Percentage ascertained
50% 60% 70% 80% 90%
Ashford 1,578
686
43.5
1,775
772
888
1,065
1,243
1,420
1,598
Canterbury 2,346
1,162
49.5
2,526
1,251
1,263
1,516
1,768
2,021
2,274
Dartford 1,092
773
70.8
1,167
827
584
700
817
934
1,051
Dover 1,777
723
40.7
1,877
764
938
1,126
1,314
1,501
1,689
Gravesham 1,247
447
35.9
1,306
468
653
784
914
1,045
1,175
Maidstone 2,076
1,146
55.2
2,200
1,214
1,100
1,320
1,540
1,760
1,980
Sevenoaks 1,711
670
39.1
1,810
709
905
1,086
1,267
1,448
1,629
Shepway 1,838
668
36.3
1,904
692
952
1,143
1,333
1,523
1,714
Swale 1,696
772
45.5
1,778
809
889
1,067
1,244
1,422
1,600
Thanet 2,298
868
37.8
2,330
880
1,165
1,398
1,631
1,864
2,097
Tonbridge & Malling 1,551
628
40.5
1,648
667
824
989
1,154
1,319
1,483
Tunbridge Wells 1,604
678
42.3
1,669
706
835
1,001
1,168
1,335
1,502
Total Kent 20,813
9,221
44.3
21,991
9,743
10,996
13,195
15,394
17,593
19,792
Source: POPPI, PANSI, ONS, QOF, KPHO

January 2015 6
Table 3: Estimates of prevalence of dementia aged 30+, at varying levels of ascertainment, 2013-14 projected to 2017
Clinical commissioning groups
2017 - Showing expected numbers at different levels of ascertainment
2013-14
Estimated prevalence
At 2013-14 QOF
level
Ascertainment levels
CCG Estimated prevalence
QOF register
Percentage ascertained
50% 60% 70% 80% 90%
NHS Ashford
1,613 710
44.0
1,740
766
870
1,044
1,218
1,392
1,566
NHS Canterbury & Coastal
2,984 1,427
47.8
3,140
1,502
1,570
1,884
2,198
2,512
2,826
NHS DGS
3,103 1,409
45.4
3,220
1,462
1,610
1,932
2,254
2,576
2,898
NHS South Kent Coast
3,256 1,294
39.7
3,456
1,373
1,728
2,074
2,419
2,765
3,111
NHS Swale
1,388 580
41.8
1,494
625
747
897
1,046
1,196
1,345
NHS Thanet
2,213 868
39.2
2,295
900
1,148
1,377
1,607
1,836
2,066
NHS West Kent
6,256 2,933
46.9
6,646
3,116
3,323
3,987
4,652
5,317
5,981
Total Kent 20,813
9,221
44.3
21,991
9,743
10,996
13,195
15,394
17,593
19,792
Source: POPPI, PANSI, ONS, QOF, KPHO
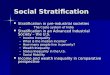
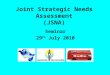
Figures 1 to 4 are the latest graphs depicting change in emergency admission rates for dementia across the seven CCGs in Kent. In comparison with earlier analysis, a decrease or stabilisation in rates appear to show in most CCGs except in Canterbury. Current intermediate care services face challenges in responding effectively to the needs of people with dementia, resulting in higher risk of hospitalisation as demonstrated in the graphs. Once admitted their length of stay is considerably longer. For example, the 2011 utilization review / bed day audit across the seven acute hospital sites in Kent & Medway showed that, in up to 50% of admissions that were audited, no substantive acute care had taken place at the time audit, and that up to 40% of those admissions were waiting for residential care placement. Most of the admissions audited were emergency and were complex frail elderly. People with dementia are also more likely to be admitted to long term care after an acute hospital admission and not given the opportunity to return home with support. People with dementia in general hospitals have worse outcomes in terms of length of stay, mortality and institutionalisation

January 2015 7
Figure 1
Figure 2

January 2015 8
Figure 3
Figure 4:

January 2015 9
Figure 5:
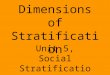
Over the last year Public Health carried out an epidemiological study, using a locally developed King’s Fund based risk stratification tool developed by the Kent & Medway Health Informatics Service, giving commissioners a unique whole system baseline profile of population utilization of health and social care services. Results showed a pareto distribution between need and impact, which varied across different services, particularly hospital and adult social care. For example the top 0.5% (Band 1) of the Kent & Medway risk stratified population with the highest risk scores for rehospitalisation generated up to 20% of the total unscheduled care spend for the whole population, during the year of ‘crisis’. This proportion rises to more than 40% in the context of total spend dementia related emergency admissions for the whole population as shown in Figure 4. This has substantively contributed to the necessary evidence base and strategic planning of the local health and social care integration programme to improve and optimise patient care, and the cornerstone for Kent CCGs’ transformational plans over the next three to five years. Details of the methodology and analysis are available at http://www.kpho.org.uk/joint-strategic-needs-assessments/Integration-JSNA-Chapter. The same approach has been used to explore the prevalence of dementia in the population and the impact on services, relative to the wider burden of multi morbidity as well as other important programme areas for older people’s health such as falls and fracture prevention and end of life care. Figure 5 shows the proportion of people with multiple morbidities by named long term condition for Band 1. It shows that

January 2015 10
people with only dementia is as low as 5%, while the remaining 95% of persons with dementia have at least one other chronic condition. Broadly speaking, the prevalence of dementia in Band 1 is as high as 15% shown in Figure 6. This trend reduces to less than 1% in Band 4, the remaining 80% of the population having the lowest risk scores. Further work is still required to understand the full distribution of Kent & Medway population of dementia sufferers which number more than 21,000, shown in Tables 1 and 2, across the different risk bands and their differential impact on service utilisation. Figure 6:
Figure 7: Risk Band
Patients – with Dementia
All Patients
Proportion of dementia patients
1 1343 8840 15.2% 2 5111 97244 5.3% 3 2138 247694 0.9% 4 163 1414141 0.0%
Grand Total 8755 1767919 0.5%

January 2015 11
Table 4: CCG name
Risk Band
Patients Spells 09/10
Total Cost 09/10
Spells 10/11
Total Cost 10/11
Spells 11/12
Total Cost 11/12
Total Spells 09/10 to 11/12
Total Cost 09/10 to 11/12
Kent and
Medway
1 1341 767 £1,940,118 2995 £8,750,786 1760 £4,889,146 5522 £15,580,050
2 5103 2827 £7,974,434 3993 £12,279,431 5808 £17,032,495 12628 £37,286,360
3 2132 142 £239,200 138 £238,801 3955 £12,351,721 4235 £12,829,722
4 163 5 £2,766 3 £628 325 £974,843 333 £978,237
Kent and
Medway Total
8739 3741 £10,156,518 7129 £21,269,646 11848 £35,248,205 22718 £66,674,369
Understanding costs of dementia on social care Using the risk stratified population cohort from 04.04.2011, an estimate of the number of people with dementia in each of the risk band has been derived by linking the patient list to inpatient data for 2009/10 to 2011/12. Patients were classified as having dementia if it was recorded in the diagnosis fields of the SUS dataset. Adult social care dataset of the same period was linked to explore associated activity and costs. Table 4 shows that of the out of the 2159 social care clients found in risk band 1 there were 620 patients with dementia representing a prevalence of almost 30% of this group. Table 4 Estimated number of patients with dementia by risk stratification
Risk Band
Social Care Clients
Proportion of total clients in band
Patients with Dementia
Proportion of clients
Proportion of those in risk band
1 2159 9% 620 17% 29% 2 10195 42% 2044 56% 20% 3 7575 31% 889 24% 12% 4 4391 18% 86 2% 2% Total 24320 100% 3639 100% 15%
Table 6 shows social care costs for these, indicating that clients in Band 4 have the highest per capita cost mainly due to relatively much higher expenditure for permanent residential and nursing. A case note audit carried out by social care on a random sample of Band 4 clients suggests most of them had long term care needs such as sensory impairment, mental health problems and learning disabilities which probably explains the need for more long term residential and nursing care.

January 2015 12
Table 6: Social care costs per patient by risk band
Risk Band
Patients with Dementia in the different risk bands
Social Care costs (2009/10-2011/12)
Costs per patient per year
1 620 £14,540,589 £7,817
2 2044 £54,816,740 £8,939
3 889 £18,906,239 £7,088
4 86 £2,642,020 £10,240
Current Services in Relation to Need To download a PDF version of the Dementia pathway please click on this link. Projected Service Use and Outcomes in Three-Five Years and Five-10 Years Figure 8:

January 2015 13
Figure 9:
Figure 10

January 2015 14
Figure 11:
Evidence of What Works Department of Health Department of Health (2009) Living well with dementia: a national dementia strategy. Available at: https://www.gov.uk/government/publications/living-well-with-dementia-a-national-dementia-strategy This strategy provides a strategic framework within which local services can:
a deliver quality improvements to dementia services and address health inequalities relating to dementia;
b provide advice and guidance and support for health and social care commissioners and providers in the planning, development and monitoring of services
c provide a guide to the content of high-quality services for dementia Department of Health (2012) Dementia Challenge. Available at: http://dementiachallenge.dh.gov.uk/ The Prime Minister’s Dementia Challenge launched in March 2012. It sets out plans to go further and faster in improving dementia care, focusing on raising diagnosis rates and improving the skills and awareness needed to support people with dementia - and their carers. It also has details of plans to improve dementia research. Department of Health (2012) The Prime Minister’s Challenge on Dementia: delivering major improvements in dementia care and research by 2015: Annual

January 2015 15
report of progress. Available at: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/200030/9535-TSO-2900951-PM_Challenge_Dementia_ACCESSIBLE.PDF The progress of the Dementia Challenge is overseen by three groups of ‘champions’. This is their latest progress report. NICE Guidance NICE/Social Care Institute for Excellence (2006) CG42 Dementia: supporting people with dementia and their carers in health and social care Available at: http://www.nice.org.uk/nicemedia/live/10998/30318/30318.pdf Dementia is associated with complex needs and, especially in the later stages, high levels of dependency and morbidity. These care needs often challenge the skills and capacity of carers and services. This guideline makes recommendations for the identification, treatment and care of people with dementia and the support of carers. Settings relevant to these processes include primary and secondary healthcare, and social care. Wherever possible and appropriate, agencies should work in an integrated way to maximise the benefit for people with dementia and their carers. Quick reference guide: http://www.scie.org.uk/publications/misc/dementia/dementia-qrg.pdf NICE (2010) End of life care for people with dementia: commissioning guide: implementing NICE guidance http://www.nice.org.uk/media/0A2/66/CommissioningGuideEoLDementia.pdf This commissioning guide has been developed to help support the local implementation of NICE clinical guidelines to commission integrated end of life care services for people with dementia. The guide makes the case for commissioning end of life care for people with dementia, highlighting key benefits. It specifies service requirements, key components of which are highlighted as: assessment and care planning, coordination of care with ongoing review, and developing personalised high-quality care across a number of settings. It then looks at determining local service levels ensuring co-operation and quality assurance. Links to the clinical guidance are included throughout. The guide is aimed primarily at health and social care professionals responsible for commissioning dementia services and/ or end of life services for people with dementia. It should be read together with related NICE guidance and strategies. NICE (2011) Dementia: care pathway. Available at: http://pathways.nice.org.uk/pathways/dementia This pathway covers supporting people with dementia and their carers in health and social care. Dementia is a progressive and largely irreversible clinical syndrome that is characterised by a widespread impairment of mental function. Although many people with dementia retain positive personality traits and personal attributes, as their condition progresses they can experience some or all of the following: memory loss, language impairment, disorientation, changes in personality, difficulties with activities of daily living, self-neglect, psychiatric symptoms (for example, apathy, depression or psychosis) and out-of-character behaviour (for example, aggression,

January 2015 16
sleep disturbance or disinhibited sexual behaviour, although the latter is not typically the presenting feature of dementia). Dementia is associated with complex needs and, especially in the later stages, high levels of dependency and morbidity. These care needs often challenge the skills and capacity of carers and services. Other Guidance Alzheimers Society (2011) Optimising treatment and care for people with behavioural and psychological symptoms of dementia Available at: http://www.alzheimers.org.uk/site/scripts/download_info.php?downloadID=609 This best practice guide was developed in consultation with an advisory group of leading clinicians specialising in dementia. It is aimed at a wide range of health and social care professionals caring for people with dementia who have behavioural and psychological symptoms to provide evidence-based support, advice and resources. Institute for Research and Innovation in Social Services (2011) Leading for outcomes: dementia Available at: http://www.iriss.org.uk/sites/default/files/iriss_leading_for_outcomes_dementia_final-3.pdf This guide is intended for anyone working with people with dementia, and their carers. It provides evidence-based advice, support and training materials to help them focus on outcomes important to people. It is aimed at team leaders, managers and trainers in social services and related areas and is geared to the Scottish perspective and context. It contains exercises and training materials which leaders can access and adapt as appropriate. User views and User Engagement The views of service users and their carers are sought in a number of ways and each CCG has its own process for seeking views from patients and the public. However, the community events and insight gathering which has been undertaken as part of the development of dementia friendly communities has highlighted a number of themes, such as:
Reluctance of some GPs to refer people to the memory assessment service.
The need for more respite and day services.
Better out of hours support.
Better support post diagnosis.
The need for increased awareness for GPs of dementia and awareness of services, particularly those provided by the voluntary sector.
Unacceptable waits to receive a diagnosis from the memory service.
The lack of appropriate information at the right time.
The need for organisations who deal with the public, such as bus companies, banks and supermarkets, to be more dementia friendly.

January 2015 17
Unmet Needs and Service Gaps The current model of service delivery for people with dementia is not joined up or designed to be proactive enough to identify people early in order to provide personalised support and prevent people reaching crisis point. The need for good joint working has been underlined repeatedly in a number of reports, but continues to be a barrier for people with dementia. Consequently too many resources are tied up in expensive acute in patient or care home provision. Timely diagnosis is the key to helping people with dementia, ensuring their families and carers get the support they need to plan for the future and enabling them to make informed choices about how they would like to be cared for. With early intervention, and access to the right services and support, people with dementia can continue to live well for many years. Currently, average diagnosis rates across Kent are 43%. The Prime Minister’s Challenge on Dementia (2012) has set an ambition to achieve a diagnosis rate of 67% by 2015. Forty seven per cent of people with dementia do not feel part of their community. They often experience anxiety and depression and three quarters do not feel society is geared up to deal with dementia (Dementia 2012: A national challenge, Alzheimer’s Society, 2012). Sixty two per cent of people with dementia living alone are lonely and it can sometimes be hard to access services, which only adds to this isolation (Dementia 2013. The hidden voice of loneliness, Alzheimer’s Society, 2013). The drive to keep people in their own homes and avoid admission to residential care has the potential to increase these feelings of loneliness and isolation. People with dementia do not have the same access to intermediate care as people without dementia. This is partly due to the fact that it is often thought that people with dementia cannot benefit from rehabilitation services. They also require input for longer period of time. The National Dementia Strategy Impact Assessment calculated that hospital at home rehabilitation schemes could reduce the average length of stay by almost seven days per patient, at an average cost of £3,780 per care episode (Department of Health, 2009, Impact Assessment of the National Dementia Strategy, v 16). About one third of people with dementia live in residential care, while about two thirds of people who live in care homes are thought to have dementia. Research in 2012/13 by the Care Quality Commission (CQC) found that people with dementia living in a care home are more likely to go into hospital with avoidable conditions (such as urinary infections, dehydration and pressure sores) than similar people without dementia. Once in hospital, people with dementia (not just those admitted from a care home) are more likely to stay there longer, be readmitted and die there. It also found the number of multiple emergency admissions to hospital of people with dementia living in at a care home was 10 per cent higher for those with dementia than similar patients without dementia. Findings from a national survey of bereaved people, of which one fifth of the responses were related to dementia, found that one in 10 responses relating to dementia rated their end of life care in the last three months of life as ‘poor’. Less than half (46 per cent) of bereaved relatives of people with dementia rated the

January 2015 18
overall quality of care received by the deceased person across all settings as outstanding or excellent. (First national VOICES survey of bereaved people: key findings report, July 2012). As indicated above, 2.2% of people will develop dementia before the age of 65. Whilst this is a relatively small number of people, the needs and challenges of this group of people are often different from those individuals who develop dementia in later life. They may still be in employment and may still have dependent children. They tend to very physically fitter which can present problems if they exhibit challenging behaviours, particularly if they are being cared for alongside older, frailer individuals. There are very few services to meet the needs of this group of individuals (or their families), particularly when someone can no longer be cared for at home. Very often, the only alternative is to place them in a care home with people who tend to be much older and have very different needs. Recommendations for Commissioning Kent’s vision for dementia friendly communities is an inclusive community where people living with dementia and their carers are active participants within community life. The aim is to develop a whole system approach to dementia friendly communities, working alongside key organisations and people to establish their roles and responsibilities in making this happen Kent plans to co-produce a Kent wide agreement which will create the conditions to allow dementia friendly communities to thrive. Recommendations for Needs Assessment Work Public Health is currently exploring how to model the impact of increased diagnostic rates for dementia. Using demographics, service provision data and evidence from risk stratification, a framework will be developed to try to understand the patient journey along the pathway and estimate the demand for services as the disease progresses over time and estimated costs for both health and social care. The work will attempt to provide a starting point to test out some of the assumptions that have been made to consolidate the tool. Additional data from other services such as mental health cluster information (PbR) will be used to ensure the use of real costs to calculate mental health/health expenditure. Whilst the integration agenda is key to improving the lives of people with dementia and their carers, the needs of people with dementia also need to be considered as part of other strategies, eg urgent care, intermediate care, end of life. As approximately 90% of people with dementia will have other co-morbidities, dementia needs to considered as part of the long term conditions agenda and not seen as separate to ensure that individuals receive holistic care. All organisations, within both the statutory and non-statutory sectors need to ensure that their staff receive some level of dementia training, so that they are able to manage most people with dementia. Specialist mental health services should only become involved when people’s needs increase and become more challenging.

January 2015 19
Key Contacts Abraham George – Consultant in Public Health [email protected] Linda Caldwell – Senior Associate SECSU [email protected]