Embed Size (px)
Citation preview

1
Keratoconus – New Discoveries,
New Controversies
Jan Bergmanson, OD, PhD, PhD h.c., DSc Texas Eye Research and Technology Center University of Houston College of Optometry
Full Financial Disclosure
No Personal Financial Interest in any of the products mentioned in this presentation.
TERTC has received grants from the following
companies over the last 12 months:
Alcon AMO
Bausch & Lomb CooperVision
Contamac TruForm
Funding Ø Internal Funding Ø NEI Core Grant P30 EY007551
TERTC Keratoconus (Kc)Team
Ø Jessica Mathew, OD, PhD Ø John Goosey, MD Ø Rune Brautaset, PhD Ø Maria Nilsson, PhD Ø William Miller, OD, PhD Ø Norman Leach, OD, MS Ø Jan Bergmanson, OD, PhD
Making the Diagnosis
Ø Patient history and symptoms l Gradual development of reduced and/or
distorted vision l Monocular or binocular diplopia or polyopia
• Reported as ghost images or shadows l Mild to severe photophobia or glare l Headaches, asthenopia, and itching associated
with vigorous eye rubbing
Making the Diagnosis
Ø One eye is generally more advanced than the other l Unilateral Kc (?)
• CLEK study (2,379 eyes, 1,579 pts): 13% • Other studies: 3.5 – 20% • (Zadnik, Barr et al. Cornea. 1996)

2
Making the Diagnosis
Ø Objective Clinical Signs l Marked changes in
refraction l Keratometry and/or
keratoscopy mire irregularities
Making the Diagnosis
Ø Objective Clinical Signs l Corneal topography inferior steepening
• 5 - 7 % refractive surgery candidates have subclinical keratoconus
Making the Diagnosis
Ø Objective Clinical Signs l Ophthalmoscopic fundus reflex
Making the Diagnosis
Ø Objective Clinical Signs l Munson's sign
Making the Diagnosis
Biomicroscopy Ø Vogt’s striae
• May disappear with digital pressure
Making the Diagnosis
Ø Fleischer's ring (50 - 90 %)

3
Making the Diagnosis
Ø Apical thinning
Making the Diagnosis
Ø Corneal scarring Ø Try to grade density
Making the Diagnosis
Ø Ruptures in posterior limiting lamina (and endothelium)
Corneal Hydrops
Controversy 1: Ø Is the pathology of Kc restricted to the confines
of the Fleischer Ring? OR
Ø Is it a pancorneal pathology?
Why do we need to know? If peripheral cornea is involved in Kc – Ø Clinical management may need to be modified. Ø Surgical approach – may need to be re-assessed. Ø Our counsel to the Kc Pt should reflect this consideration.
So far… Have we been over-concerned with the cone, ignoring the rest
of the cornea?

4
George Waring: (on corneal dystrophies)
Post-transplant recurrence is
explained by existance of disease in peripheral host
cornea (1998)
Presence of Kc in peripheral cornea could explain post-transplant
recurrence
Past reports of Kc recurrence: Ø Abelson, Collin, Gillette, Dohlman. BJO. 1980. (16 yrs –
1 case) Ø Nirankari et al. BJO. 1983. (22 yrs – 1 case) Ø Bechrakis et al. Cornea. 1994. (10 & 19 yrs - 2 cases ) Ø Patel et al. BJO. 2009. (avg: 20 yrs – 25 cases)
TERTC Research Undertaking:
Clinical in vivo measurements and histopathological research can establish
the presence or the absence of the disease in the peripheral cornea.
Phase I: Histopathology of Kc
Ø Mathew JH, Goosey JD, Bergmanson JPG. Quantified Histopathology of the Keratoconic Cornea. Optometry and Vision Science. 88(8):988-997, 2011.
Pathology of Epithelium in Kc
Ø Epithelial thickness variations l Central cone
• Avg=42.2µm (13.5 – 91.6µm) l Peripheral button
• Avg=54.5µm (29.8 – 90.9µm)
Ø Not always explained by the number of layers of cells
Ø Not always correlated to the absence of ALL
Normal KC KC
~ 0.225µm
Pathology of Epithelium Central Cone & Peripheral Cornea • Abnormal BM synthesis • Pathological cytoplasm/shape • Variable thickness • Independent of stromal events

5
Pathology of ALL in KC (eponymous name is Bowman’s layer)
Thinned or Lost over large areas
Pathology of ALL
Ø Central cone l PKP
• 72% was affected • 20% was completely missing
l LKP • 36% was affected • 0% was completely missing
Ø Peripheral button l PKP
• 19% was affected • 5% was completely missing
l LKP • 11% was affected • 0% was completely missing
Pathology of ALL
Ø “Breaks, interruptions, fragmentations, dehiscences, ruptures” of ALL
• Duke-Elder, 1961 • Grayson’s, 1997 • Krachmer, 1997 • Liebowitz & Waring, 1998 • Kauffman, et al., 1998 • Eagle, 1999 • Krachmer & Palay, 2006
Ø No one suggested extreme areas of loss
Ø No one suggested periphery to be involved!
Epithelial Adhesion Apparatus
Ø Hemidesmosomes Ø Basement membrane
(type IV collagen) Ø Type I collagen fibers Ø Type VII collagen fibers Ø Anchoring plaques Ø Fibronectin Ø Laminin
Phase II: Clinically measurements of the in vivo
Kc cornea.
Accepted for publication Cornea, 2012
Demographics of Subjects
Kc Patients Controls
# of subjects 26 26
# of eyes 48 52
Age (mean + SD) 38.7 + 13.2 36.9 + 13.8
Male/Female 13/13 11/15
Spherical equiv (D) -8.5 (+7.18) -2.9 (+3.68)
Visual Acuity (logMar) 0.33 (+0.31) 0.01 (+0.14)

6
Kc grading and distribution of clinical findings
Eye Sim´s K-Value CLEK
Cyl (D) Axis (º) Max K (D) Min K (D) Category 1/2/3
OD -5.27 129.25 52.58 47.28 2/7/14
OS -4.77 60.65 51.18 49.80 4/12/9
Prominant nerve fibres Fleischer´s ring Vogt´s
striae Munson´s sign Anterior corneal scarring
Posterior corneal scarring
OD 20 7 23 3 5 9
OS 19 8 24 0 4 12
Scanning Slit Elevation Topography – Orbscan
Average Range (mm) Kc Controls Diff P
0-3 458.38 (±65.4)
546.1 (±46.0)
87.72 <0.0001
3-5 564.66 (±50.6)
620.36 (±31.0)
55.70 <0.0001
Doughty & Zaman 2000 • Central Av: 535 um • Range: 474-596 um • Periph: 700 um
Optical Coherence Tomography (OCT) – Visante
Visante (OCT) Provided 4 Corneal Thickness Measurements
Ø Centrally Ø 2-5 mm peripherally Ø 5-7 mm peripherally Ø 7-10 mm peripherally
Corneal Thickness (um) in Central and Peripheral Cornea in Kc and Control
Range (mm) Kc Patients Controls p-value Change in Thickness
0-2 470.6 537.0 <0.001 66.4
2-5 501.7 558.5 <0.001 56.8
5-7 548.1 595.5 <0.001 47.4
7-10 605.5 647.4 0.0006 41.9
Kc cornea is thinner also in periphery
In-Vivo Clinical & Histopathological Research
has now Demonstrated Ø Kc appears to involve the entire cornea. Ø Disease manifestation is less pronounced in
the periphery.

7
Controversy 2:
Can Kc recur or was your pt unlucky and had someone else’s
Kc transplanted?
Keratoconus Recurrence We can explain this now!
But, how does this happen? Ø Presence of disease in host cornea
l In periphery l Incomplete cone removal
Ø Presence of disease in donor cornea
Keratoconus Recurrence Case Example
Ø Music Professor & Professional Jazz Musician: l Hx of Kc OU l Bilateral PKP 22 yrs
ago (3 mos apart, 2 donors), Las Vegas
Musician’s Odds in Las Vegas
Ø Given Kc incidence of 1 in 2000 l What is the chance that he would get unlucky with
both eyes? l 1 in 4000000 l YES, One chance in 4 million!
You would not bet in Las Vegas on those odds!
Musician’s Odds in Las Vegas
Ø Most likely, his recurrent Kc came from his own (host) corneas
Ø BCVA 20/25 OD, OS Ø Currently not a candidate for re-graft
Ø Topo pic
Explanation of Kc Recurrence
Ø The disease is pan-corneal. Ø Typical keratoplasty will not eliminate all of
the diseased tissue. Ø Although it is theoretically possible to
transplant a cornea with subclinical Kc, it is a highly unlikely scenario because corneas are screened.

8
Ünal et al., Cornea, 2006 (Turkey)
Ø Reported ‘recurrence’ of Kc in corneas of 2 separate individuals who got transplants from the same donor: l One received PKP for FED, the other for
corneal scarring
The disease can travel in both directions!
Recurrent Kc Latency is Long
Average is 15 years
No immediate worry for patient and practitioner –
just regular monitoring…
Take Home Message Recurrence of Kc
Ø Has a long latency period: 1-2 decades Ø Will be first noticed topographically Ø May not require re-graft Ø Most likely will come from host cornea.
New Explanations to Ectasia Controversy 3: Lamellar Splitting vs Slipping

9
Dawson et al. Ophthalmol. 2008;115(12):2181-2191 –
“…believe that interlamellar slippage is
most likely caused by the fracture of collagen type VI bridging filament
networks that frequently join adjacent lamellae together throughout the entire
corneal stroma…”
Dawson et al. Ophthalmol. 2008;115(12):2181-2191 –
“…keratocytes, which reside in the
interlamellar space, may accelerate this first phase of the biomechanical failure
process, particularly if interlamellar shear (e.g., eye rubbing) or fracture results in
keratocyte cellular damage…”
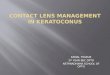
Lamellar Count Results
0
50
100
150
200
250
300
350
400
450
1 2 3 4 5 6 Normal
# of
lam
ella
e
Cornea
Number of Lamellae in Kc Corneas
Total Lamellae
Anterior Lamellae
Posterior Lamellae
Healthy vs. Kc Cornea
Ø Healthy Cornea: 242 (Bergmanson, Horne et al., 2005)
Ø Kc Cornea: 357
Despite anterior stromal lamellar dropout, we counted more lamellae!
Normal Fragmented
0 50
100 150 200 250 300 350 400 450
1 2 3 4 5 6 Normal
# of
lam
ella
e
Cornea
Number of Lamellae in Kc Corneas
Total Lamellae
Anterior Lamellae
Posterior Lamellae
Dawson and colleagues (including Stulting and Edelhauser). Ophthalmol. 2008;115(12):2181-2191.
Corneal Ectasia After Excimer LaserKeratorefractive Surgery: Histopathology,Ultrastructure, and Pathophysiology
Daniel G. Dawson, MD, 1,2 J. Bradley Randleman, MD,1 Hans E. Grossniklaus, MD, 1Terrence P. O’Brien, MD, 2 Sander R. Dubovy, MD,2 Ingo Schmack, MD,1,3 R. Doyle Stulting, MD, PhD,1Henry F. Edelhauser, PhD1
Purpose: To evaluate the histopathology and ultrastructure of corneas developing ectasia after LASIK orphotorefractive keratectomy (PRK).
Design: Retrospective case series.Participants: Thirteen specimens from 12 patients undergoing corneal transplantation for progressive
ectasia after LASIK (12 specimens) or PRK (1 specimen) were obtained for histopathologic and ultrastructuralevaluation.
Methods: All 13 ectatic corneas were submitted in formalin for light microscopy. Nine specimens werebisected, and the second half was placed in 2.5% glutaraldehyde for transmission electron microscopy (TEM).
Main Outcome Measures: Corneal histopathology, ultrastructure, and pathophysiology.Results: Light microscopy of the post-LASIK specimens showed corneal epithelial hypoplasia and occa-
sional foci of epithelial hyperplasia, Bowman’s layer breaks, a normal stromal thickness of the LASIK !ap, anormal thickness of the hypocellular primitive stromal scar, a thinned residual stromal bed (RSB), and larger thannormal artifacteous interlamellar clefts in the RSB of the ectatic region. The post-PRK specimen showed similar"ndings with the addition of a thinned hypercellular "brotic stromal scar. TEM showed thinning of the collagenlamellae and loss o! amellar number in the RSB of post-LASIK ectasia corneas or throughout the entire cornealstromal bed in the post-PRK ectasia cornea, with the posterior aspect of the corneal stroma being most a#ected.
Conclusions: Histopathologic and ultrastructural studies suggest that interlamellar and inter"brillar biome-chanical slippage occurs when the cornea becomes ectatic after LASIK or PRK in the postoperative stress-bearing regions of the corneal stroma. This 2-phase chronic biomechanical failure process is similar to that seenin keratoconus. Composite sciences classify this chronic biomechanical failure process as inter"ber fracture.
Financial Disclosure(s): The authors have no proprietary or commercial interest in any materials discussedin this article. Ophthalmology 2008;115:2181–2191 © 2008 by the American Academy of Ophthalmology.

10
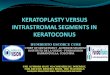
Post Refractive Surgery Ectasia vs Kc
Post PRK Ectasia Dawson et al.
Kc TERTC, Houston, Tx
Kc TERTC, Houston, Tx
Post LASIK Ectasia Dawson et al.
Post Refractive Surgery Ectasia vs Kc
Proposed Ectasia Etiology:
Post-Refractive Sx = Kc
Conclusion
Lamellar fragmentation (predominantly)
+ Anterior stromal tissue loss
(secondarily) =
Corneal ectasia
New Hypothesis: Lamellar Fragmentation Ectasia
1um
Normal Fragmented