Embed Size (px)
Citation preview
Ketamine
• Facilitator: Barbara Bischoff, BSN, RN
Case Study• A 51 year old woman presents to ED with right shoulder pain
11/25/14• Stage 4 Breast Cancer• Carcinoma of breast/Cellulitis• History of left side Mastectomy• Port to left side of chest wall• Pt weight 70 kilograms
Case Study (continued)Initial Medications
• Duragesic Patch 100 mcg/hr (Fentynal) 1 patch Q72 hr• Hydrocodone (APAP) 5 mg/325 mg (Norco) 1 tab PO Q6 hr
PRN•Morphine Sulfate (MS Contin) 60 mg tab PO Q12 hr•Miralax 17 gm 1 time daily PO• Ondansetron (Zophran) 8 mg tab PO Q6 hr
Case Study (continued)
•WBC 7.7 ( 3.9–10.7 x 103 cells/μL)• RBC 3.99 (4.2–5.9 x
106 cells/μL)• H & H 12.2/36.6 (12–16
g/dL/36–47%)• INR 2.6 (2.0–3.0)
• Na 139 (136–145 mEq/L)• K 3.9 (3.5–5 mEq/L)• Cl 104 (98–106 mEq/L)• BUN 7 (10-20 mg/dl)• Creatinine 0.5 (0.7–1.3
mg/dL)
Lab Results on Admission
Case Study (continued)•Patient on Maria Hall 11/25/15-12/2/15•Patient placed in Palliative Care•Patient transferred from Maria Hall to ICU @1300
12/2/15•Continuous monitoring•Pain management with ketamine drip •Ketamine bolus 10 mg with doctor at bedside•Ketamine drip initiated Ketamine 12 mg/Dilaudid 10
mg/hr
Ketamine• Pain Management• Mechanism of Action• Clinical Effects• Therapeutic Administration• Use as an analgesic in palliative care
(FDA, 2014; Micromedex, 2015)
Ketamine•NMDA glutamate receptor antagonist•Binds to opioid mu and sigma receptors•Acts on cerebral cortex and limbic system•Release of endogenous catecholamine•Reduces polysynaptic spinal reflexes •Anesthetic agent used as analgesic to manage complex
pain(Micromedex, 2014, NHS, 2013)
GOPIXPIC. (n.d.).
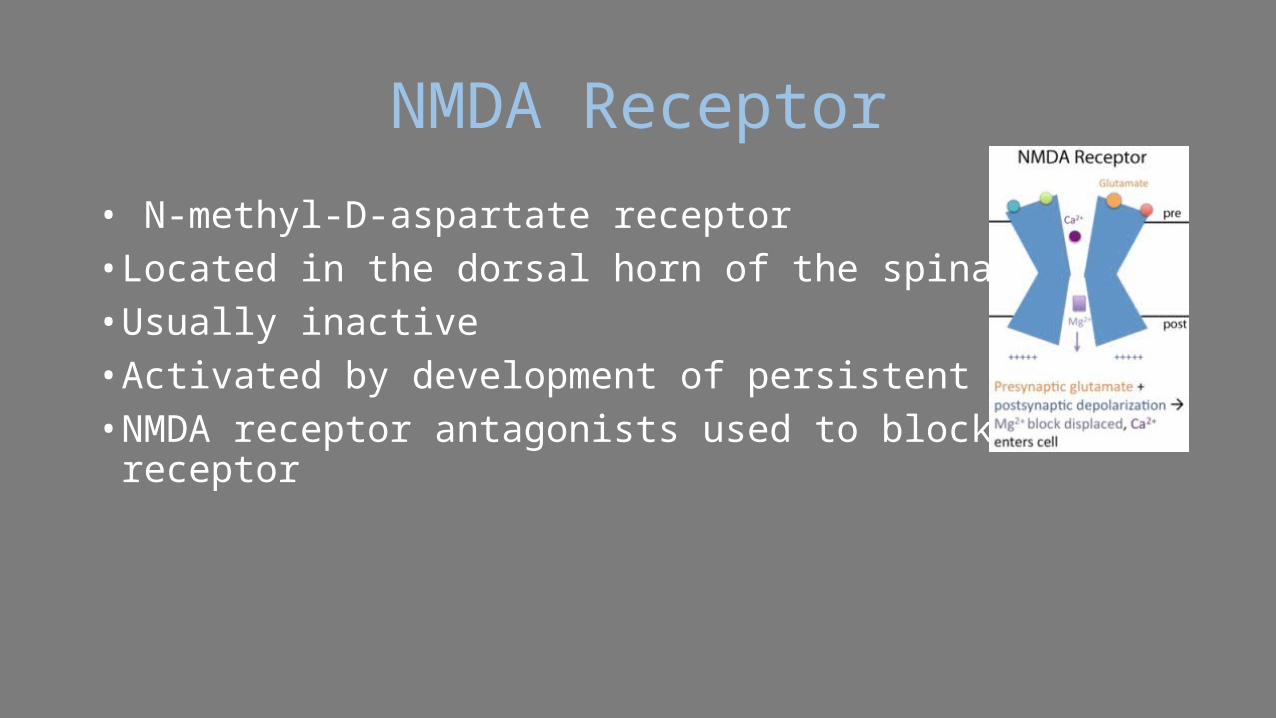
NMDA Receptor• N-methyl-D-aspartate receptor• Located in the dorsal horn of the spinal cord• Usually inactive• Activated by development of persistent pain• NMDA receptor antagonists used to block this receptor
Problem Description• Increasing number of opioid tolerant patients.•High Tolerance•Usual multimodal regimen:•Opioids•Non-opioids•NSAIDs•Gabapentanoids•Muscle Relaxers
• May not manage pain.(Colfer, Wolo & Viscusi, 2013).
Goals of Acute Pain Management in Opioid Tolerant Patients
• Identify at-risk population•Prevent withdrawal symptoms/complications• Effective analgesic treatment in acute pain• Treatment of psychological disorders•Rehabilitation to maintenance therapy
(Bourne, 2010)
Opioid-tolerant patients in practice
• Three main groups of opioid-tolerant patients :•Patients with cancer pain•Patients with chronic non-cancer pain•Patients with current addiction to opioid drugs•Patients on a maintenance drug program
(ANZCA, 2010)
Opioids Alone •Compromise patient safety•Cause side effects•Nausea•Vomiting•Dependence•Respiratory Depression
(Colfer, Wolo & Viscusi, 2013)

Chronic Wounds/Chronic Pain•A wound that fails to heal within 3 months.•Social, psychological, physical and economic cost •Consequences:•Severe impairment of quality of life•Restriction of daily activity•Emotional distress• Lengthy treatment• High treatment expense
(Frykberg, 2011; Werdin et al., 2009; Ruttermann et al.,2013)
Position Statement Pain Management
•American Society for Pain Management Nursing•Nurses must advocate for optimal •Pain management• Symptom relief
•A meta-analysis•52 studies• Spanning 40 years • Found 64% of advanced cancer patients have pain
(Reynolds, Drew & Dunwoody, 2013, Colfer, Wolo & Viscusi, 2013)
Policy Statement•Oral or IV Ketamine will be initiated upon order from a
physician via CPOE.• First 24 hours or TBD by MD•Administered by nurses in critical care• Follow standing order set
(NHS, 2013; Zittel, 2011)

Signs and Symptoms of OpioidWithdrawal
• Sweating
• Restlessness
• Papillary dilation
• Irritability
• Tachycardia
• Nausea
• Hypertension
• Abdominal cramps
• Vomiting
• Hyperalgesia
• Diarrhea
• Myalgia
• Yawning
• Dysphoria
• Fever/chills
• Insomnia
• Rhinorrhea
• Anxiety
• Lacrimation
• Craving for opioids
• Pilorection
(Adapted from Collett, 1998; Bourne, 2010)
Process•Patient specific order• Infusions prepared by pharmacy• Infuse through dedicated line via most proximal port•Use portless IV tubing •No bolus without anesthesia provider
(Zittel, 2011; DRE, 2015)

Low-dose KetamineDefined
• Bolus < 2 mg/kg intramuscular administration• Bolus < 1 mg/kg intravenous administration• Continuous IV is < or = 20 microg/kg per min
(Schmidt, Sandler & Katz, 1999)
Administration• Initial ketamine concurrent with opioid.•Monitor for sedation or confusion• If drowsy notify MD•Ketamine side effects (patient not drowsy):•Hallucinations or dysphoria
•Administer as ordered by MD:• Haloperidol•Midazolam
(NHS, 2013)
Administration ProcessDosing By Pharmacy
•Prepare new syringe every 24 hours.•Dilute ketamine with sodium chloride 0.9%.•Check: Syringe is not cloudy•Protect it from light.•Check: Stability and compatibility.•Rotate SC infusion site daily.
(NHS., 2013)

Monitor•Vital signs •Alertness •Orientation• Evidence of: •Nystagmus •Bad dreams •Unpleasant hallucinations.
(Zittel, 2011)
Report•Heart rate > 100 beats per minute • Systolic B/P < 90 mmHg•Respiratory < 10 breaths per minute•Oxygen saturation of < 93%• Emergence reaction symptoms:•Bad dream•Hallucinations•Nystagmus
(Zittel, 2011)

Onset and Duration•Rapid Onset:• IV within 30 seconds •Half-life:•10-15 min (Alpha phase)• > 2.5 h (Beta phase)
• IM within 3-4 minutes.•Duration: • IV 2 mg/kg lasts 5-10 minutes • IM 9 to 13 mg/kg lasts 12-25 minutes
(SEMAC, Micromedex, 2015)
Common Side Effects•Dizziness• Tachycardia•Altered mental status•Anxiety•Palpitations• Slurred speech•Hallucinations•Nystagmus
•Mydriasis•Muscular hypertonus• Trismus•Psychomotor reactions •Psychomimetic reactions• Emergence delirium•Hypertension•Chest Pain
Converting from IV to Oral Ketamine•Oral ketamine is more potent than IV ketamine •Dose reduction with change•Prescribed in divided doses - four times daily• Titrated in 5-10 mg increments per order• IV infusion may be stopped with the first dose •Or gradually reduced with increase of oral infusion.
(NHS., 2013)
Contraindications•Drug allergy•Use of droxidopa•Pregnancy•Breast-feeding•Head trauma or injury •Bleeding in the brain• Stroke • Increased spinal fluid
pressure
• Increased ocular pressure•Bladder or urinary
problems •Congestive heart failure •High blood pressure •Mental or mood
problems• Thyroid problems.
Pain Management Resource Sites•American Society of Regional Anesthesia and Pain
Management •• http://www.asra.com/ •American Society for Pain Management ••
http://www.aspmn.org/ •American Society of Anesthesiologists ••
http://www.asahq.org/ • Food and Drug Administration
••http://www.fda.gov/Drugs/ •Anesthesia Patient Safety Foundation ••
http://www.apsf.org/• Institute for Safe Medication Practices ••
http://www.ismp.org/
(Colfer, Wolo & Viscusi, 2013).

Thank you for your Time
Questions? Comments?
References• ANZCA (Australian and New Zealand College of Anesthetists, Faculty of Pain Medicine). (2010).
Acute Pain Management: Scientific Evidence (3rd ed.). Melbourne, Victoria, Australia. ANZCA.• Bourne, N. (2010). Acute pain management in the opioid-tolerant patient. Nursing Standard.
25, 12, 35-39.• Chin, M.L. (2014). Multimodal analgesia: Role of non opioid analgesics. American Society of
Regional Anesthesia and Pain. Retrieved from https://www.asra.com/pain-resource/article/35/multimodal-analgesia-role-of-non-opioid-analgesics• Colfer, K., Wolo, E. & Viscusi, E.R. (2013). Acute pain management: Current
trends,technologies, and new agents. Journal of Legal Nurse Consulting, 24(1), 11-19.• Collett, B.J. (1998). Opioid tolerance: the clinical perspective. British Journal of Anaesthesia,
81(1), 58-68.• Dickenson, A. H. (1997). NMDA receptor antagonists: Interactions with opioids. Acta
Anaethesiologica Scandinavica, 41(1), 112-115.
References (Cont)• Drugs.com. (2015). Droxidopa. Retrieved from
http://www.drugs.com/mtm/droxidopa.html• FDA (U. S Food and Drug Administration). (2014). "Off-Label" and investigational use
Of marketed drugs, biologics, and medical devices - information sheet guidance for institutional review boards and clinical investigators. Retrieved from http://www.fda.gov/regulatoryinformation/guidances/ucm126486.htm
• Frykberg, R.G. (2011). The science of advanced wound care: What should you be using in your office? Podiatry Today Supplement: Emerging evidence on advanced wound care for diabetic foot ulcerations. HMP Communications, LLC (HMP), 1-3, 8-15.
• GOPIXPIC. (n.d.). Cerebral cortex. Limbic system. Image retrieved from http://www.gopixpic.com/limbic-system-not/
• Loftus, R.W., Yeager, M.P., Clark, J.A., Brown, J.R., Abdu, W.A., Sengupta, D.K. & Beach, M.L. (2010). Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology, 113(3), 639-646. doi: 10.1097/ALN.0b013e3181e90914.
References (Cont)
• Medtronic. (2014). Common Types of chronic pain. Retrieved from http://www.medtronicneuro.com.au/chronic_pain_commontypes.html
• Micromedex. (2014). Ketamine Hydrochloride. DrugPoint Summery. Retrieved from http://www.micromedexsolutions.com/micromedex2/librarian/PFDefaultActionId/evidence
• NHS. (2013). Ketamine in palliative care. Lothian.• Reynolds, J., Drew, D. & Dunwoody, C. 2013. American Society for Pain
Management Nursing Position Statement: Pain Management at the End of Life.
• Ruttermann M., Maier-Hasselmann, A., Nink-Grebe, B. & Burckhardt, M. (2013). Clinical practice guideline: Local treatment of chronic wounds in patients with peripheral vascular disease, chronic venous insufficiency, and diabetes. Dtsch Arztebl Int; 110(3): 25–31. DOI: 10.3238/arztebl.2013.0025
References (Cont)• Schmid, R.L., Sandler, A.N. & Katz, J. (1999).Use and efficacy of low-dose
ketamine in the management of acute postoperative pain: a review of current techniques and outcomes. Pain, 82(2), 111-125. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10467917• SEMAC (State Emergency Medical Advisory Committee). (n.d.). Ketamine.
Drug Formulary. Retrieved from https://www.health.ny.gov/professionals/ems/pdf/ketamine_formulary• Sigma-Aldrich. (2015). S-(+)-Ketamine hydrochloride. Picture retrieved
from http://www.sigmaaldrich.com/catalog/product/sigma/k1884?lang=en®ion=US• Werdin, F., Tennenhaus, M., Schaller, H.E. & Rennekampff, H.O. (2009).
Evidence-based Management Strategies for Treatment of Chronic Wounds. Open Access Journal of Plastic Surgery, 9(19), 169-179.