Embed Size (px)
Citation preview

Image: Jaimie Duplass, iStockphoto
Key points
• Initial empirical therapy for severe community-acquired pneumonia should be an intravenous -lactam and an oral macrolide.
• Empyema should always be considered early on if there is a poor response to intravenous antibiotics. Children with empyema should be managed at a tertiary paediatric centre.
• Primary lung abscesses are rare; in their management, patience is key.
• The incidence of necrotising pneumonia is increasing. Pneumatocoeles and bronchopulmonary fistulae are recognised sequelae and the clinical course may be very prolonged.
• In cases where there is slow resolution, persistent atelectasis or recurrent severe pneumonia, additional investigations are indicated to try and identify an underlying cause.

Complicated pneumonia inchildren
Educational aims[ To understand the pathogenesis of complicated community-acquired pneumonia
in children
[ To gain an understanding into the management of common complications ofcommunity-acquired pneumonia in children
SummaryCommunity-acquired pneumonia is a common paediatric infection and, evenwith the introduction of pneumococcal and Haemophilus vaccinations, mostchildren will experience at least one episode before adult life. Most cases are self-limiting but a small number of children will develop sequelae and requirehospitalisation. This review focuses on the presentation and management ofcomplications of community-acquired pneumonia in children.
Paediatric community-acquired pneumonia(CAP) is defined as ‘‘the presence of signsand symptoms of pneumonia in a previouslyhealthy child due to an infection which hasbeen acquired outside hospital’’ [1]. Twoprospective population-based studies esti-mate that incidence of CAP is 32.8–33.8 casesper 10 000 children under the age of 5 yearsor 14.4–14.7 cases per 10 000 children underthe age of 16 years in northern Europe [2, 3];the majority of these patients will be mana-ged effectively by primary care, though the
threshold for referral and admission tohospital in those less than 6 months of ageshould be lower [4]. Hospitalisation rates forCAP in children range from 9.5% to 42% [5–7]and the median time to resolution of symp-toms in children with oxygen saturations of.85% at the time of admission is 9 days,regardless of whether treatment is with oralamoxicillin or intravenous benzylpenicillin [8].A recent British Thoracic Society (BTS) guide-line [1] states that severe CAP, as defined bythe clinical parameters summarised in table 1,
Statement of InterestNone declared.
HERMES syllabuslink: B.3.3
Paediatric HERMESsyllabus link: E.1, E.2
Breathe | March 2013 | Volume 9 | No 3 211DOI: 10.1183/20734735.043012
Rishi Pabary,
Ian M. Balfour-Lynn
Dept of PaediatricRespiratory Medicine,Royal Brompton Hospital,London, UK
Royal Brompton Hospital,Sydney Street, London,SW3 6NP, UK

is more likely to be complex and requirehospitalisation. The focus of this review is oncomplicated pneumonia, which develops onlyin a small proportion of immunocompetentchildren who have no other underlying diag-nosis, such as chronic suppurative lungdisease; for management of simple CAP inchildren, we advise the reader to refer to theBTS guideline [1].
While most paediatric CAP will be man-aged in primary or secondary care, complica-tions may necessitate referral to a tertiarycentre. The overall complication rate in arecent BTS Paediatric Pneumonia Audit was7.1% from 2200 cases in 77 hospitals, withempyema in 4.4% and lung abscess in 0.9%of children [9].
Persistent pneumonia
Streptococcus pneumoniae is the most com-mon bacterial cause of CAP in children [10, 11]and significant clinical improvement isexpected in the first 24–48 h after startingempirical treatment with a b-lactam [12].Failure to respond may indicate that thecausative organism is not sensitive to initialtherapy; Staphylococcus aureus, and in parti-cular the toxin-producing Panton-Valentineleukocidin (PVL) strain [13], or atypicalorganisms, such as Mycoplasma pneumoniaeor Fusobacterium necrophorum [14], may causesevere or persistent symptoms. Equally,monotherapy with macrolides may also leadto treatment failure due to emergence ofresistant strains of S. pneumoniae [15, 16] and
therefore first-line treatment of severe CAP inour centre is always with both a b-lactam(usually intravenous co-amoxiclav) and amacrolide (usually oral azithromycin); it hasbeen demonstrated that this regimen reducesmortality in adults hospitalised patients withCAP [17].
The BTS states that oxygen saturation,92% in air in older children is a cardinalsign of severe CAP [1]; only a small number ofthese children will develop respiratory failureor septic shock and require mechanicalventilation on a paediatric intensive care unit(PICU) and, even then, survival in previouslyhealthy children is excellent in developedcountries. Mortality figures in England andWales (UK) in 2011 estimate that only 0.01% ofdeaths in children aged o14 years wereattributable to pneumonia. The total numberof deaths caused by pneumonia across all agegroups in 2011 was 25 696 [18], reflecting thefact that there are co-existing morbidities inthe adult population, while most cases inchildren are secondary to infection in apreviously healthy lung. However, as illu-strated in table 2, even in developed countries,one child per week dies from pneumonia.
Systemic complications
Severe sepsis
Severe sepsis is defined as a systemicinflammatory response in the presence ofinfection with end-organ dysfunction [19].Septic shock occurs when there is cardiovas-cular dysfunction, which usually necessitates
TABLE 1 Signs of severe CAP in children
Infants Older children
Temperature uC .38.5 .38.5
Respiratory rate breaths?min-1 .70 .50
Respiratory distress Moderate–severe recessionNasal flaring
CyanosisGrunting
Intermittent apnoea
Unable to complete sentencesNasal flaring
CyanosisGrunting
Feeding Unable to feed Signs of dehydration
Capillary refill time seconds .2 .2
Information from [1].
CAP in children
Breathe | March 2013 | Volume 9 | No 3212

admission to a PICU for intravenous inotropicsupport [20]. The incidence of this in childrenpresenting with CAP is unclear but from ourexperience, even in children who present withempyema or necrotising pneumonia, it is verylow. A large adult study suggests that severesepsis is a common feature in CAP (48% ofhospitalised patients) with 4.5% of patientsdeveloping septic shock [21].
Acute respiratory distress syndrome
The recent Berlin Consensus defines acuterespiratory distress syndrome (ARDS) as severehypoxaemia refractory to supplemental oxygentherapy that usually occurs within 72 h of anacute inflammatory lung injury that increasesvascular permeability and decreases lungcompliance [22]. ARDS can be categorised asmild, moderate or severe and bilateral radio-graphic opacities are typically present.Pneumonia and septic shock can both leadto ARDS and these children will typicallyrequire conventional mechanical or high-fre-quency oscillation ventilation, both of whichcan accentuate the systemic inflammatoryresponse by the mechanisms summarised infigure 1 [23]. Published mortality rates fromARDS vary from 10% to 90% [24, 25] with mostdeaths secondary to the underlying cause ofacute lung injury (sepsis, trauma or burns)rather than primary respiratory failure; ourexperience is that this is an extremely rareoccurrence secondary to CAP.
Syndrome of inappropriate antidiuretichormone secretion
The syndrome of inappropriate antidiuretichormone secretion is characterised by excessive
release of antidiuretic hormone from the poster-ior pituitary gland leading to dilutional hypona-traemia. It occurs in around one-third ofchildren hospitalised with CAP [26], the mechan-ism for which remains unclear, and is asso-ciated with higher inflammatory markers [27]and poorer outcomes [26]. Severe hyponatrae-mia can cause confusion or seizures and for thisreason fluid restriction (between 50% and 66%of maintenance) is recommended in childrenwith CAP and hyponatraemia who are haemo-dynamically stable and not dehydrated [28].
Haemolytic uraemic syndrome
Haemolytic uraemic syndrome (HUS) is oneof the main causes of acute renal failure in thepaediatric population [29] and has beendescribed following invasive S. pneumoniaeinfection. These cases of ‘‘atypical’’ HUS havea much higher morbidity and mortality thanthose due to typical organisms such asenterotoxigenic Escherichia coli O157 [30, 31].HUS should always be suspected early incases of CAP associated with anaemia, throm-bocytopenia and renal dysfunction (anuria) as75% of these cases are likely to require dialysis[30] and early intervention may be associatedwith better outcome [32].
TABLE 2 Mortality in children aged ,14years for England and Wales (UK), 2011
Age years
,1 1–4 5–14
Total deaths 3154 516 547
Respiratorycauses
77 55 49
Pneumonia 25 19 5
Data are presented as n and are from [18].
Pneumonia
Pulmonary inflammation
Mechanical ventilation
Decreased integrity of the alveolar–capillary membrane
Increased circulating bacteria and pro-inflammatory cytokines
Increased systemic inflammatory response
Sepsis and/or multiple organ dysfunction
Surfactant rupture andinactivation
Translocation of bacteria and pro-inflammatory cytokines
Increased pulmonary oedemaand lymphatic drainage
Ventilator-induced lung injury
Microvascular injury
Figure 1Proposed mechanism of exacerbation of the systemic inflammatory response secondaryto mechanical ventilation. Reproduced and modified from [23] with permission from thepublisher.
CAP in children
Breathe | March 2013 | Volume 9 | No 3 213

Disseminated intravascular coagulation
Disseminated intravascular coagulation (DIC)is a consumptive coagulopathy that canpresent secondary to infection with S. pneu-moniae [33] or M. pneumoniae [34]. Like HUS,thrombocytopenia and anaemia are presentbut renal dysfunction is secondary to acutetubular necrosis rather than the thromboticmicroangiopathy of the renal vasculature, thatis seen in HUS [30]. Activated partial throm-boplastin time and prothrombin time areprolonged in DIC while fibrinogen is reduced;these are all essentially within normal limitsin HUS.
Secondary thrombocytosis
The importance of platelets in the host immuneresponse is increasingly recognised [35] and ithas been demonstrated in adults that secondarythrombocytosis, which has until recently beenconsidered a normal inflammatory responseto infections, is associated with respiratorycomplications of CAP (pleural effusion andempyema) and poorer outcomes [36]. Plateletcounts may therefore be of prognostic value inpaediatric CAP, though there is no role forantiplatelet treatment [1].
Pulmonary complications
Treatment failure may be due to antibioticresistance (or atypical organisms such asMycobacterium tuberculosis being only partiallysensitive to empirical therapy) or becauseCAP is the first presentation of an underlyingcondition such as cystic fibrosis, immunode-ficiency or congenital thoracic malformation(CTM). However, it is more usually becausepulmonary complications to the initial infec-tion have developed; these can be dividedinto 1) those that are due to the accumulationof fluid, 2) those that are due to accumulationof air or 3) atelectasis.
Parapneumonic effusion/empyema
Injury to the lung parenchyma due to infec-tion can lead to increased capillary perme-ability and accumulation of fluid in the pleuralspace, which happens in three distinct stages.In the early stages of infection, fluid is serousand sterile (exudative stage) but over time,typically 1–2 weeks, there is an influx of whiteblood cells and bacteria (fibropurulent stage),
leading to pus formation (empyema). Over2–4 weeks after the primary infection, fibrin isdeposited on the pleural surfaces and thefluid collection becomes organised, leading to aloculated empyema composed of separatepockets of viscous fluid. Around 0.7% ofchildren hospitalised with CAP will developempyema [37] and, in cases where a causativeorganism is isolated (in around 37.7–58.5% ofcases [38] with standard microbiological techni-ques), S. pneumoniae (primarily serotype 1)accounts for 68% [39]. The incidence of child-hood empyema was increasing prior to theintroduction of the heptavalent pneumococcalconjugate vaccine (PCV-7) into the standardchildhood immunisation schedule in 2006 [40,41]. Although it has been reported that incidencedecreased 22% between 2006 and 2008 [42],and those due to serotypes covered by PCV-7declined completely from 48% of cases, the UK-ESPE study reports that there was an increase indisease caused by other serotypes [39]. Ofparticular concern is an increased UK preva-lence of disease caused by serotype 19a [43],which has been associated with a greaterlikelihood of PICU admission and mortality[43–45], and serotype 3, which is able to resistphagocytosis [46, 47] and has been associatedwith increased incidence of bronchopulmonaryfistula [48]. Although both these serotypes arecovered by the new PCV-13 vaccination, itremains to be seen whether other serotypes willsubsequently become more prevalent (the so-called replacement phenomenon) and whateffect this will have on ongoing complicationrates of CAP.
Pleural effusion or empyema should beconsidered if a child does not respond to48 h treatment with intravenous antibiotics
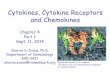
Figure 2Left-sided pleural effusion.
CAP in children
Breathe | March 2013 | Volume 9 | No 3214

[49]. They are diagnosed on the basis ofclinical signs, such as decreased air entry anddullness to percussion over the affected area[50], and may be confirmed by plain chestradiograph (fig. 2), although can be difficultto distinguish from consolidation alone.Thoracic ultrasound is essential to determinethe extent and nature of fluid collections(fig. 3) although there is debate as to whetherthis is useful in predicting outcome [51, 52].Differentiation of solid and cystic areas in thepleural cavity is poor with ultrasound and, ifthere is any doubt about the diagnosis (forexample, the onset of symptoms was insi-dious and inflammatory markers are onlymoderately elevated, raising the possibility ofmalignancy), computed tomography (CT)should be performed prior to making anyfurther decisions on management [53].Although CT should not be undertakenroutinely [1, 37], its utility in certain situationsis illustrated in figure 4, which shows bilateralempyema but also Burkitt’s lymphoma thatwas not evident on ultrasound.
In general, effusions ,2 cm in depth caninitially be managed conservatively, as drai-nage is technically difficult and resolutionmay occur with intravenous antibiotics alone.
For larger effusions or if there is significantrespiratory distress, oxygen requirement ormediastinal shift, patients should be referredto a tertiary paediatric respiratory centre forassessment with or without insertion of achest drain [49]. In our centre, chest drainageis performed using soft pigtail catheters(French gauge 6–10) (fig. 5) inserted undergeneral anaesthesia with ultrasound gui-dance; this approach is felt to reduce patienttrauma and permit early mobilisation as thesmall drains are minimally intrusive. Rapiddrainage by thoracocentesis is not recom-mended due to the risk of re-expansionpulmonary oedema [54, 55] and drains shouldbe clamped for 1 h if o10 mL?kg-1 of fluiddrains from a chest tube in any 60-min period[49]. Serial thoracocentesis of small aliquotsof fluid is not indicated in children as thiseither increases trauma if done under localanaesthesia or requires repeated general
a)
b)
Figure 3Thoracic ultrasound scans showing loculated pocketsof fluid.
a)
b)
Figure 4CT image showing bilateral empyema in associationwith Burkitt’s lymphoma. Red arrows point to areas oflymphoma.
CAP in children
Breathe | March 2013 | Volume 9 | No 3 215

anaesthesia. In cases where drainage is slow,due to the fluid being thick or loculated,twice-daily intrapleural fibrinolytics such asurokinase have been shown to reduce dura-tion of hospital stay [52], incidence of residualpleural thickening [56] and allow resolution ofempyema without surgical intervention in upto 93% of cases [52]. Although in one smallstudy, the failure rate was reported at almost70% [57], in our experience, in 180 childrenwith empyema who required chest drainsbetween 2002 and 2007, of whom 80%received intrapleural urokinase, ,3% wenton to have a surgical procedure. Chest tubesare removed when f50 mL per day is drainingand the integrity of the drain is confirmed;chest radiographs should be repeated 3–4 hafter drain removal to ensure that re-accumu-lation or pneumothorax has not occurred.
Adult studies of fibrinolytics in empyemaare less convincing, probably due to underlyingcomorbidities and a higher incidence of non-infective causes. Around 33% of adults even-tually require surgical intervention [58] andmortality rates are significantly higher [59, 60].The First Multicenter Intrapleural Sepsis Trial(MIST1) found that intrapleural streptokinasedid not reduce mortality, surgical rates or dura-tion of hospital stay [58]. A subsequent trial ofintrapleural tissue plasminogen activator (tPA)and recombinant human DNase (rhDNase)demonstrated significant improvements inpleural opacities on chest radiography andreduction in both the surgical referral rate andduration of hospital stay in adult patientsrandomised to receive both treatments, withno difference seen with either treatment aloneor double-placebo [61]. As yet, there have beenno studies in children investigating combinationtherapy; the presumed mechanism of action ofintrapleural rhDNase is that it breaks downextracellular DNA in the pleural space, thus
reducing fluid viscosity and enhancing drainage,which is equally valid in the paediatric popula-tion and, therefore, merits further investigation.
Primary surgical management of child-hood empyema is usually via a mini-thora-cotomy or video-assisted thoracoscopic surgery(VATS). Both approaches remove pus and fluidfrom the pleural space and reduce the need foropen drainage and decortication [62, 63], andare associated with reduced morbidity com-pared to open thoracotomy [63, 64]. However,children who undergo surgery still require achest drain post-operatively and there is debateas to whether there is any reduction in hospitalstay [65–67] compared with nonsurgical man-agement. Two prospective randomised studiescomparing VATS with chest drains plus intra-pleural fibrinolytics found no difference intreatment failure rate [66, 68] and, althoughVATS failure rates in a subsequent studyundertaken in a different centre were signifi-cantly better (7%) [69], the additional expense[68, 70] and limited availability [69] of VATSsuggest that it should currently be consideredas a second-line treatment option.
Following successful drainage, low-gradefever may persist but is not a contraindicationto discharge provided that the trend isdownwards and there is clinical improve-ment, which can be confirmed by repeatinginflammatory marker tests. Children aredischarged home on oral antibiotics (usually2–4 weeks of co-amoxiclav with or withoutan additional agent on the basis of clinical/microbiological findings) with outpatientfollow-up and repeat chest radiography after6–8 weeks. Radiological findings generallynormalise over time and parents should beadvised that there should be no long-termsequelae in previously healthy children butto seek urgent medical attention for furtherinvestigation if there is any recurrence of
a) b) c)
Figure 5a) Small-bore pigtail catheter. b) Insertion of chest drain using aseptic Seldinger technique. c) Post-procedureradiograph with drain in situ. This patient had rapid drainage of fluid following drain insertion and developedARDS, most likely due to re-expansion pulmonary oedema.
CAP in children
Breathe | March 2013 | Volume 9 | No 3216

symptoms. For more detailed recommenda-tions on the management of pleural infectionin children, refer to the BTS guideline [49].
Pericardial effusion
Accumulation of fluid between the heart andthe pericardial sac, or pericardial effusion, israre in childhood but may co-exist withparapneumonic effusion, particularly left-sidedcases, simply due to the proximity of thepleura and pericardium [71, 72]. Most of theseassociated pericardial effusions improve withtreatment of the underlying infection buturgent echocardiography should be consid-ered in cases of haemodynamic compromiseas pericardiocentesis may be required [73].
Lung abscess
Lung abscesses are thick-walled cavities(o2 cm) containing purulent material thatare the result of acute destruction of the lungparenchyma following inflammation, necrosisand cavitation [74]. They are rare and mainlyseen in children with respiratory co-morbid-ities [75, 76] or neurodevelopmental abnorm-alities who are at increased risk of recurrentaspiration [77] but may be primary, occurringas sequelae of CAP. With the advent ofinterventional radiology, causative organismsin lung abscess can be isolated in around two-thirds of cases [78], with Gram-positive cocci(S. pneumoniae, S. aureus and Streptococcuspyogenes) and, rarely, M. pneumoniae [79]associated with primary forms, and Gram-negative anaerobes more likely in abscessessecondary to other underlying conditions.
Symptoms of primary lung abscess inchildren include fever, cough, dyspnoea andchest pain; there may be localised reductionin air entry and crackles on auscultations ofthe chest as well as dullness to percussion,and, hence, there is overlap with the pre-sentation of uncomplicated CAP, althoughthe evolution of lung abscesses is often moreinsidious [77]. Chest radiography may show athick-walled cavity with an air–fluid level butmisses the diagnosis in around 20% of cases[80] and may not distinguish an abscess fromunderlying congenital thoracic abnormalitiesor consolidation alone; thus, contrast-enhanced CT is the investigation of choice,particularly as it can help to guide percuta-neous diagnostic aspiration with or withoutdrainage [77, 80]. Although ultrasound has a
role in differentiating loculated empyema andlung abscess, it is most useful as a tool formonitoring the response to treatment with noassociated exposure to radiation.
The mainstay of treatment of primary lungabscess has traditionally been intravenouspenicillin for 2–3 weeks followed by a further4–8 weeks of oral antibiotics [81]; our centreoccasionally adds clindamycin to provideadditional cover for S. aureus or metronidazolefor anaerobic cover, and resolution in mostchildren will occur with medical managementalone [82]. The course of disease may beprolonged and fungal infections such asaspergilloma should be considered if there isa poor response to antibiotics. Surgical inter-vention has, in the past, been associated withsignificant morbidity [77, 83] and was recom-mended as an intervention only if prolongedmedical therapy was unsuccessful [84] or ifthere was respiratory compromise, such asmediastinal shift, necessitating mechanicalventilation. However, two recent reports sug-gest that insertion of a pigtail catheter at thetime of presentation and initial CT-guidedpercutaneous aspiration [77] or thoracoscopicdrainage [85] can significantly reduce durationof hospital stay and antibiotic therapy, but thishas yet to be confirmed by larger studies. It isestimated that 90% of children with primarylung abscess will respond to medical manage-ment and make a full recovery althoughempyema, pneumothorax and bronchopul-monary fistulae (defined as an abnormalconnection between the pleural space andbronchial tree) are recognised sequelae [74].Outpatient follow-up should be arranged andconsideration given to the possibility that thelung abscess was a primary presentation of anundiagnosed CTM that became secondarilyinfected. An example of a right upper lobe lungabscess, which are typically seen followingaspiration, and its evolution over time isshown in figure 6.
Necrotising pneumonia
An increasingly recognised sequela of pae-diatric CAP is necrotising or cavitary pneu-monia, which was first described in 1994 [86,87] and has recently been shown to compli-cate up to 20% of childhood empyema [88]. Itis characterised by necrosis and liquefactionof lung parenchyma, which is thought to besecondary to ischaemia caused by thrombosisof intrapulmonary vessels and can culminate
CAP in children
Breathe | March 2013 | Volume 9 | No 3 217

in pulmonary gangrene [89] of single ormultiple lobes [74, 90]. Historically, theprimary causative pathogen was thought tobe S. aureus [91] but S. pneumoniae, particularlyserotypes 1, 3 9V and 14 [88, 89], is now thepredominant cause, although M. pneumoniae[92], methicillin-resistant S. aureus and PVLstrains of S. aureus [93] have also beenimplicated. Diagnosis is usually made on CT,as plain chest radiographs will not accuratelydemonstrate the typical disruption of normalparenchymal architecture where multiple air-or fluid-filled cavities replace the normal lung
tissue [90]. Air-filled cavities (pneumato-coeles) are common in necrotising pneumo-nia as one-way passage of air into theperipheral airways occurs following necrosisof bronchioles and alveoli [74]; if they arisetowards the periphery of the parenchyma,pneumatocoeles may lead to pneumothorax.Where necrosis occurs adjacent to the pleura,a bronchopleural fistula may form, resulting inpneumothorax or pyopneumothorax.
Necrotising pneumonia is usually accom-panied by severe sepsis and prolonged coursesof intravenous antibiotics are necessary. Chest
b) c)a)
Figure 6Right upper lobe lung abscess on a) plain chest radiography and b) CT. c) Good resolution in follow-upradiograph after 6 weeks of antibiotic therapy.
a) b) c) d)
e) f) g) h)
i) j) k) l)
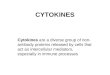
Figure 7Prolonged course of necrotising pneumonia caused by Streptococcus pneumoniae. a) Chest radiography (CXR), day 1; b) CXR, day 4; c) CXR,day 8; d) CXR, day 17; e) CT, day 22; f) CXR, day 27; g) CXR, day 99; h) CT, day 116; i) CT, day 144; j) CXR, day 144; k) CXR, day 178; l) CXR,day 298.
CAP in children
Breathe | March 2013 | Volume 9 | No 3218

drains may need to be in situ for many weeksdue to persistent air leaks from bronchopul-monary fistulae; in order to minimise the riskof obstruction, our centre recommends largerand stiffer drains than for empyema, assignificant volumes of air can accumulaterapidly following blockage, with subsequentlung collapse. Fibrinolytics are not used asthey may impair healing of pleural holes. Long-term outcome with conservative managementis good, with a mortality rate of 5.5% [87, 94],although one series reported that 66% ofchildren required thoracotomy for decortica-tion, bronchopulmonary fistula repair or par-tial pneumonectomy [94]. Healing of thefistula may be promoted by excising theparietal pleura, which encourages adherenceof the lung to the chest wall. In our opinion,patience is paramount and the more invasivesurgical option of muscle flap thoracoplastyshould only be used as a last resort as it istechnically difficult and, because grafts perma-nently reduce vital capacity, associated withsignificant morbidity post-operatively [95].Figure 7 shows serial radiographs from a childwith necrotising pneumonia due to pneumo-coccal infection; the course is prolonged andpneumatocoeles are prominent.
Atelectasis
Acute atelectasis is defined as collapse ofpart or all of one lung. It was historicallyconsidered to be due to alveolar deflation butevidence is now emerging that it is due toaccumulation of alveolar fluid [74]. It canoccur secondary to mucus plugging in CAP,suggesting that chest physiotherapy may be
useful, although there is little evidence tosupport this [96] and a Cochrane Review iscurrently being undertaken. Flexible broncho-scopy, both as a diagnostic and therapeuticintervention, has been shown to be beneficialin atelectasis associated with infections inchildren [97].
Further investigations and follow-up
In our centre, we recommend that all patientswith complicated CAP be followed up asoutpatients until there is complete resolutionon chest radiography. If there is chronicatelectasis on the chest radiograph, othercauses such as airway compression by lymphnodes (as seen in tuberculosis and malig-nancy) or an inhaled foreign body should beconsidered.
Flexible bronchoscopy may reveal luminalblockage, compression or narrowing (bronch-omalacia), and should be considered incomplicated CAP where there is a prolongedcourse. Furthermore, any child who has morethan one episode of complex CAP confirmedby radiography should be fully investigated toseek an underlying cause; first-line investiga-tions that are undertaken in our centre andsummarised in table 3.
The final point to consider is that respira-tory infections do not always reflect a primaryunderlying pulmonary pathology. A child withrecurrent CAP was recently referred to ourcentre for respiratory investigations, which wereall entirely unremarkable. Echocardiographysubsequently revealed an atrial septal defectand the patient had full resolution of symptomsfollowing surgical closure.
TABLE 3 Possible underlying causes for recurrent pneumonia and first-line investigations
Cause Investigation
Aspiration (silent) Video fluoroscopy
Gastro-oesophageal reflux disease pH/impedance study with or without milk scan
Bronchiectasis High-resolution chest CT with or without contrast
Immunodeficiency Immunoglobulins and vaccine responses
Cystic fibrosis Sweat test and genetic analysis
Primary ciliary dyskinesia Nasal nitric oxide ¡ ciliary brushings
Congenital heart disease Echocardiogram
CAP in children
Breathe | March 2013 | Volume 9 | No 3 219

References
1. Harris M, Clark J, Coote N, et al. British ThoracicSociety guidelines for the management of commu-nity acquired pneumonia in children: update 2011.Thorax 2011; 66: Suppl. 2, ii1–ii23.
2. Senstad AC, Suren P, Brauteset L, et al. Community-acquired pneumonia (CAP) in children in Oslo,Norway. Acta Paediatr 2009; 98: 332–336.
3. Clark JE, Hammal D, Hampton F, et al. Epidemiologyof community-acquired pneumonia in children seenin hospital. Epidemiol Infect 2007; 135: 262–269.
4. Jadavji T, Law B, Lebel MH, et al. A practical guide forthe diagnosis and treatment of pediatric pneumonia.CMAJ 1997; 156: S703–S711.
5. Bunuel Alvarez JC, Vila Pablos C, TresserrasGonzalez E, et al. Estudio descriptivo de la neumoniaadquirida en la comunidad en la edad pediatrica.Una perspectiva desde atencion primaria. [Adescriptive study of community-acquired pneumoniain childhood. A primary care perspective]. AtenPrimaria 1999; 23: 397–402.
6. Jokinen C, Heiskanen L, Juvonen H, et al. Incidenceof community-acquired pneumonia in the populationof four municipalities in eastern Finland. Am JEpidemiol 1993; 137: 977–988.
7. MacIntyre CR, McIntyre PB, Cagney M. Community-based estimates of incidence and risk factors forchildhood pneumonia in Western Sydney. EpidemiolInfect 2003; 131: 1091–1096.
8. Atkinson M, Lakhanpaul M, Smyth A, et al.Comparison of oral amoxicillin and intravenousbenzyl penicillin for community acquired pneumoniain children (PIVOT trial): a multicentre pragmaticrandomised controlled equivalence trial. Thorax2007; 62: 1102–1106.
9. Thomson A. British Thoracic Society PaediatricPneumonia Audit 2010/11. Report2011. www.brit-thoracic.org.uk/audit.aspx Date last updated: January22, 2013.
10. Heiskanen-Kosma T, Korppi M, Jokinen C, et al.Etiology of childhood pneumonia: serologic results ofa prospective, population-based study. Pediatr InfectDis J 1998; 17: 986–991.
11. Michelow IC, Olsen K, Lozano J, et al. Epidemiologyand clinical characteristics of community-acquiredpneumonia in hospitalized children. Pediatrics 2004;113: 701–707.
12. Toikka P, Virkki R, Mertsola J, et al. Bacteremicpneumococcal pneumonia in children. Clin Infect Dis1999; 29: 568–572.
13. Woodhead M. Community-acquired pneumonia inEurope: causative pathogens and resistance pat-terns. Eur Respir J 2002; 20: Suppl. 36, 20s–27s.
14. Dykhuizen RS, Olson ES, Clive S, et al.Necrobacillosis (Lemmiere’s syndrome): a rare causeof necrotizing pneumonia. Eur Respir J 1994; 7:2246–2248.
15. Sutcliffe J, Tait-Kamradt A, Wondrack L. Streptococcuspneumoniae and Streptococcus pyogenes resistant tomacrolides but sensitive to clindamycin: a commonresistance pattern mediated by an efflux system.Antimicrob Agents Chemother 1996; 40: 1817–1824.
16. Lonks JR, Garau J, Gomez L, et al. Failure ofmacrolide antibiotic treatment in patients withbacteremia due to erythromycin-resistantStreptococcus pneumoniae. Clin Infect Dis 2002; 35:556–564.
17. Waterer GW, Somes GW, Wunderink RG. Monotherapymay be suboptimal for severe bacteremic pneumo-coccal pneumonia. Arch Int Med 2001; 161: 1837–1842.
18. Office for National Statistics. Mortality Statistics:Deaths registered in England and Wales (Series DR),2011. www.ons.gov.uk/ons/publications/re-reference-tables.html?edition5tcm%3A77-277727
19. Goldstein B, Giroir B, Randolph A. Internationalpediatric sepsis consensus conference: definitionsfor sepsis and organ dysfunction in pediatrics.Pediatr Crit Care Med 2005; 6: 2–8.
20. Waterer GW, Quasney MW, Cantor RM, et al. Septicshock and respiratory failure in community-acquiredpneumonia have different TNF polymorphism asso-ciations. Am J Respir Crit Care Med 2001; 163:1599–1604.
21. Dremsizov T, Clermont G, Kellum JA, et al. Severesepsis in community-acquired pneumonia: whendoes it happen, and do systemic inflammatoryresponse syndrome criteria help predict course?Chest 2006; 129: 968–978.
22. Ranieri VM, Rubenfeld GD, Thompson BT, et al.Acute respiratory distress syndrome: the BerlinDefinition. JAMA 2012; 307: 2526–2533.
23. Beutz MA, Abraham E. Community-acquired pneu-monia and sepsis. Clin Chest Med 2005; 26: 19–28.
24. Artigas A, Bernard GR, Carlet J, et al. The American-European Consensus Conference on ARDS, part 2:Ventilatory, pharmacologic, supportive therapy, studydesign strategies, and issues related to recovery andremodeling. Acute respiratory distress syndrome. AmJ Respir Crit Care Med 1998; 157: 1332–1347.
25. Reynolds HN, McCunn M, Borg U, et al. Acuterespiratory distress syndrome: estimated incidenceand mortality rate in a 5 million-person populationbase. Crit Care 1998; 2: 29–34.
26. Dhawan A, Narang A, Singhi S. Hyponatraemia andthe inappropriate ADH syndrome in pneumonia. AnnTrop Pediatr 1992; 12: 455–462.
27. Nair V, Niederman MS, Masani N, et al.Hyponatremia in community-acquired pneumonia.Am J Nephrol 2007; 27: 184–190.
28. Ellison DH, Berl T. Clinical practice. The syndrome ofinappropriate antidiuresis. N Engl J Med 2007; 356:2064–2072.
29. Moghal NE, Brocklebank JT, Meadow SR. A review ofacute renal failure in children: incidence, etiology andoutcome. Clin Nephrol 1998; 49: 91–95.
30. Brandt J, Wong C, Mihm S, et al. Invasive pneumo-coccal disease and hemolytic uremic syndrome.Pediatrics 2002; 110: 371–376.
31. Waters AM, Kerecuk L, Luk D, et al. Hemolyticuremic syndrome associated with invasive pneumo-coccal disease: the United kingdom experience.J Pediatr 2007; 151: 140–144.
32. Trompeter RS, Schwartz R, Chantler C, et al.Haemolytic-uraemic syndrome: an analysis of prog-nostic features. Arch Dis Child 1983; 58: 101–105.
33. Konda S, Zell D, Milikowski C, et al. Purpurafulminans associated with Streptococcus pneumoniaesepticemia in an asplenic pediatric patient. ActasDermosifiliogr 2012 DOI: 10.1016/j.ad.2012.05.009
34. Nilsson IM, Rausing A, Denneberg T, et al.Intravascular coagulation and acute renal failure in achild with mycoplasma infection. Acta Med Scand1971; 189: 359–365.
35. Mirsaeidi M, Peyrani P, Aliberti S, et al.Thrombocytopenia and thrombocytosis at time ofhospitalization predict mortality in patients withcommunity-acquired pneumonia. Chest 2010; 137:416–420.
EducationalquestionsWhich of the followingstatements is/are true?
1) In severe CAP,
a) Staphylococcus aur-eus is the most commoncausative organism
b) Hypernatraemiacan result due to thesyndrome of inappropri-ate antidiuretic hormonesecretion
c) If acute respiratorydistress syndrome(ARDS) develops, bilat-eral radiological signs areusually present
d) Mortality fromARDS usually occurs dueto primary respiratoryfailure
e) Haemolytic uraemicsyndrome caused byStreptococcus pneumoniaeis associated with highermorbidity and mortalitythan cases that are dueto Escherichia coli
2) In paediatricempyema,
a) there are threepathological stages (exu-dative, fibropurulent andorganisational)
b) incidence of hasfallen since introductionof pneumococcalvaccination
c) S. pneumoniae sero-type 19a is associatedwith bronchopulmonaryfistula
d) computed tomo-graphy is a first-lineinvestigation that is usedto guide thoracocentesis
e) no more than10 mL?kg-1 of fluidshould be drained withinany 60-min period
3) Lung abscesses
a) are more commonin children with neuro-developmentalabnormalities
CAP in children
Breathe | March 2013 | Volume 9 | No 3220

36. Prina E, Ferrer M, Ranzani OT, et al.Thrombocytosis is a marker of poor outcome incommunity-acquired pneumonia. Chest 2012 [Inpress DOI: 10.1378/chest.12-1235].
37. Sonnappa S, Jaffe A. Treatment approaches forempyema in children. Paediatr Respir Rev 2007; 8:164–170.
38. Menzies SM, Rahman NM, Wrightson JM, et al.Blood culture bottle culture of pleural fluid in pleuralinfection. Thorax 2011; 66: 658–662.
39. Thomas MF, Simmister C, Elemraid MA, Clark JE,Rushton SP, Gorton R, Paton JY, Spencer DA. TheUK-ESPE study: paediatric empyema in the UK. ArchDis Child 2012; 97: A20–A21.
40. Rees JH, Spencer DA, Parikh D, et al. Increase inincidence of childhood empyema in West Midlands,UK. Lancet 1997; 349: 402.
41. Roxburgh CS, Youngson GG, Townend JA, et al.Trends in pneumonia and empyema in Scottishchildren in the past 25 years. Arch Dis Child 2008; 93:316–318.
42. Koshy E, Murray J, Bottle A, et al. Impact of theseven-valent pneumococcal conjugate vaccination(PCV7) programme on childhood hospital admis-sions for bacterial pneumonia and empyema inEngland: national time-trends study, 1997–2008.Thorax 2010; 65: 770–774.
43. Thomas MF, Sheppard CL, Guiver M, et al.Emergence of pneumococcal 19A empyema in UKchildren. Arch Dis Child 2012; 97: 1070–1072.
44. Picazo J, Ruiz-Contreras J, Hernandez B, et al. Clonaland clinical profile of Streptococcus pneumoniaeserotype 19A causing pediatric invasive infections: a2-year (2007–2009) laboratory-based surveillance inMadrid. Vaccine 2011; 29: 1770–1776.
45. Pelton SI, Huot H, Finkelstein JA, et al. Emergence of19A as virulent and multidrug resistant pneumococ-cus in Massachusetts following universal immuni-zation of infants with pneumococcal conjugatevaccine. Pediatr Infect Dis J 2007; 26: 468–472.
46. AlonsoDeVelasco E, Verheul AF, Verhoef J, et al.Streptococcus pneumoniae: virulence factors, patho-genesis, and vaccines. Microbiol Rev 1995; 59:591–603.
47. Neeleman C, Geelen SP, Aerts PC, et al. Resistance toboth complement activation and phagocytosis intype 3 pneumococci is mediated by the binding ofcomplement regulatory protein factor H. InfectImmun 1999; 67: 4517–4524.
48. McKee AJ, Ives A, Balfour-Lynn IM. Increasedincidence of bronchopulmonary fistulas complicatingpediatric pneumonia. Pediatr Pulmonol 2011; 46:717–721.
49. Balfour-Lynn IM, Abrahamson E, Cohen G, et al. BTSguidelines for the management of pleural infection inchildren. Thorax 2005; 60: Suppl. 1, i1–i21.
50. Jaffe A, Balfour-Lynn IM. Management of empyemain children. Pediatr Pulmonol 2005; 40: 148–156.
51. Ramnath RR, Heller RM, Ben-Ami T, et al.Implications of early sonographic evaluation ofparapneumonic effusions in children with pneumo-nia. Pediatrics 1998; 101: 68–71.
52. Thomson AH, Hull J, Kumar MR, et al. Randomisedtrial of intrapleural urokinase in the treatment ofchildhood empyema. Thorax 2002; 57: 343–347.
53. Kearney SE, Davies CW, Davies RJ, et al. Computedtomography and ultrasound in parapneumoniceffusions and empyema. Clin Radiol 2000; 55:542–547.
54. Paksu MS, Paksu S, Akgun M, et al. Bilateralreexpansion pulmonary edema associated withpleural empyema: a case report. Eur J Pediatr 2011;170: 1205–1207.
55. Ozlu O, Kilic A, Cengizlier R. Bilateral re-expansionpulmonary edema in a child: a reminder. ActaAnaesthesiol Scand 2000; 44: 884–885.
56. Singh M, Mathew JL, Chandra S, et al. Randomizedcontrolled trial of intrapleural streptokinase inempyema thoracis in children. Acta Paediatr 2004;93: 1443–1445.
57. Barbato A, Panizzolo C, Monciotti C, et al. Use ofurokinase in childhood pleural empyema. PediatrPulmonol 2003; 35: 50–55.
58. Maskell NA, Davies CW, Nunn AJ, et al. U.K.Controlled trial of intrapleural streptokinase forpleural infection. N Engl J Med 2005; 352:865–874.
59. Farjah F, Symons RG, Krishnadasan B, et al.Management of pleural space infections: apopulation-based analysis. J Thorac Cardiovasc Surg2007; 133: 346–351.
60. Davies CW, Kearney SE, Gleeson FV, et al. Predictorsof outcome and long-term survival in patients withpleural infection. Am J Respir Crit Care Med 1999; 160:1682–1687.
61. Rahman NM, Maskell NA, West A, et al. Intrapleuraluse of tissue plasminogen activator and DNase inpleural infection. N Engl J Med 2011; 365: 518–526.
62. Kern JA, Rodgers BM. Thoracoscopy in the manage-ment of empyema in children. J Pediatr Surg 1993; 28:1128–1132.
63. Kern L, Robert J, Brutsche M. Management ofparapneumonic effusion and empyema: medicalthoracoscopy and surgical approach. Respiration2011; 82: 193–196.
64. Subramaniam R, Joseph VT, Tan GM, et al.Experience with video-assisted thoracoscopic surgeryin the management of complicated pneumonia inchildren. J Pediatr Surg 2001; 36: 316–319.
65. Kurt BA, Winterhalter KM, Connors RH, et al. Therapyof parapneumonic effusions in children: video-assisted thoracoscopic surgery versus conventionalthoracostomy drainage. Pediatrics 2006; 118:e547–e553.
66. St Peter SD, Tsao K, Spilde TL, et al. Thoracoscopicdecortication vs tube thoracostomy with fibrinolysisfor empyema in children: a prospective, randomizedtrial. J Pediatr Surg 2009; 44: 106–111.
67. Gates RL, Hogan M, Weinstein S, et al. Drainage,fibrinolytics, or surgery: a comparison of treatmentoptions in pediatric empyema. J Pediatr Surg 2004;39: 1638–1642.
68. Sonnappa S, Cohen G, Owens CM, et al. Comparisonof urokinase and video-assisted thoracoscopic sur-gery for treatment of childhood empyema. Am JRespir Crit Care Med 2006; 174: 221–227.
69. Bishay M, Short M, Shah K, et al. Efficacy of video-assisted thoracoscopic surgery in managing child-hood empyema: a large single-centre study. J PediatrSurg 2009; 44: 337–342.
70. Cohen E, Weinstein M, Fisman DN. Cost-effective-ness of competing strategies for the treatmentof pediatric empyema. Pediatrics 2008; 121:e1250–e1257.
71. Roberts JE, Bezack BJ, Winger DI, et al. Associationbetween parapneumonic effusion and pericardialeffusion in a pediatric cohort. Pediatrics 2008; 122:e1231–e1235.
72. Donnelly LF, Klosterman LA. The yield of CT ofchildren who have complicated pneumonia andnoncontributory chest radiography. AJR Am JRoentgenol 1998; 170: 1627–1631.
73. Dass R, Deka NM, Barman H, et al. Empyemathoracis: analysis of 150 cases from a tertiary carecentre in North East India. Ind J Pediatr 2011; 78:1371–1377.
b) are primarilycaused by Gram-positiveorganisms
c) can be diagnosedon chest radiography in90% of cases
d) Ultrasound scan isthe most useful radiolo-gical test
e) can be a primarypresentation of acongenital thoracicmalformation
4) Necrotisingpneumonia
a) complicates up to20% of childhoodempyema
b) is predominantlycaused by Staphylococcusaureus
c) Pneumatocoeles aresmall pneumothoraces
d) may require surgi-cal intervention in two-thirds of cases
e) Fibrinolytics may beused to aid drainageof necrotic lungparenchyma
5) Further investigations
a) should be underta-ken routinely in all chil-dren who present withempyema
b) Flexible broncho-scopy can be both diag-nostic and therapeutic
c) Exhaled nitric oxideis a screening test forprimary ciliary dyskinesia
d) Video fluoroscopycan demonstrate gastro-oesophageal refluxdisease
e) Congenital heartdisease may predisposeto recurrent pneumoniain infants
CAP in children
Breathe | March 2013 | Volume 9 | No 3 221

74. Kendig EL, Wilmott RW, Kendig and Chernick’sDisorders of the Respiratory Tract in Children. 8thEdn. Philadelphia: Saunders/Elsevier; 2012.
75. Evans DA, Fiedler MA. Lung abscess in a patient withcystic fibrosis: case report and review of theliterature. Pediatr Pulmonol 1996; 21: 337–340.
76. Canny GJ, Marcotte JE, Levison H. Lung abscess incystic fibrosis. Thorax 1986; 41: 221–222.
77. Patradoon-Ho P, Fitzgerald DA. Lung abscess inchildren. Paediatr Respir Rev 2007; 8: 77–84.
78. Chan PC, Huang LM, Wu PS, et al. Clinical manage-ment and outcome of childhood lung abscess: a 16-year experience. J Microbiol Immunol Infect 2005; 38:183–188.
79. Leonardi S, del Giudice MM, Spicuzza L, et al. Lungabscess in a child with Mycoplasma pneumoniaeinfection. Eur J Pediatr 2010; 169: 1413–1315.
80. Hogan MJ, Coley BD. Interventional radiology treat-ment of empyema and lung abscesses. PaediatrRespir Rev 2008; 9: 77–84.
81. Tan TQ, Seilheimer DK, Kaplan SL. Pediatric lungabscess: clinical management and outcome. PediatrInfect Dis J 1995; 14: 51–55.
82. Asher MI, Spier S, Beland M, et al. Primary lungabscess in childhood: the long-term outcome ofconservative management. Am J Dis Child 1982; 136:491–494.
83. Kosloske AM, Ball WS Jr, Butler C, et al. Drainage ofpediatric lung abscess by cough, catheter, orcomplete resection. J Pediatr Surg 1986; 21: 596–600.
84. Tseng YL, Wu MH, Lin MY, et al. Surgery for lungabscess in immunocompetent and immunocompro-mised children. J Pediatr Surg 2001; 36: 470–473.
85. Nagasawa KK, Johnson SM. Thoracoscopic treat-ment of pediatric lung abscesses. J Pediatr Surg 2010;45: 574–578.
86. Kerem E, Bar Ziv Y, Rudenski B, et al. Bacteremicnecrotizing pneumococcal pneumonia in children.Am J Respir Crit Care Med 1994; 149: 242–244.
87. Sawicki GS, Lu FL, Valim C, et al. Necrotisingpneumonia is an increasingly detected complicationof pneumonia in children. Eur Respir J 2008; 31:1285–1291.
88. Ramphul N, Eastham KM, Freeman R, et al.Cavitatory lung disease complicating empyema inchildren. Pediatr Pulmonol 2006; 41: 750–753.
89. Hsieh YC, Hsiao CH, Tsao PN, et al. Necrotizingpneumococcal pneumonia in children: the role ofpulmonary gangrene. Pediatr Pulmonol 2006; 41:623–629.
90. Hodina M, Hanquinet S, Cotting J, et al. Imaging ofcavitary necrosis in complicated childhood pneumo-nia. Eur Radiol 2002; 12: 391–396.
91. Knight GJ, Carman PG. Primary staphylococcalpneumonia in childhood: a review of 69 cases.J Paediatr Child Health 1992; 28: 447–450.
92. Wang RS, Wang SY, Hsieh KS, et al. Necrotizingpneumonitis caused by Mycoplasma pneumoniae inpediatric patients: report of five cases and review ofliterature. Pediatr Infect Dis J 2004; 23: 564–567.
93. Labandeira-Rey M, Couzon F, Boisset S, et al.Staphylococcus aureus Panton-Valentine leukocidincauses necrotizing pneumonia. Science 2007; 315:1130–1133.
94. Hacimustafaoglu M, Celebi S, Sarimehmet H, et al.Necrotizing pneumonia in children. Acta Paediatr2004; 93: 1172–1177.
95. Parikh DH, Crabbe D, Auldist A, et al., eds PediatricThoracic Surgery. London: Springer, 2009.
96. Lukrafka JL, Fuchs SC, Fischer GB, et al. Chestphysiotherapy in paediatric patients hospitalised withcommunity-acquired pneumonia: a randomisedclinical trial. Arch Dis Child 2012; 97: 967–971.
97. Liang Y, Liu XC, Jiang QB. [Role of flexible broncho-scopy in the treatment of infection-associatedatelectasis in children]. Chin J Pediatr 2003; 41:649–651.
Suggestedanswers
1) c and e2) a and e3) a and e4) a and d5) b and e
CAP in children
Breathe | March 2013 | Volume 9 | No 3222