Embed Size (px)
Citation preview

KEY POINTS IN FEEDING
THE OBESE PATIENTS
DR AHMAD SHALTUT OTHMAN
HOSP SULTANAH BAHIYAH
ALOR SETAR, KEDAH

Introduction
• Obesity is the presence of excess body fat
• Obesity is associated with an increased risk of ‘all-cause mortality’
• Obesity misleads physician into assuming the patients is well nourished
• Excess weight does not buy the patient more “NBM” time

Obesity Classification
WHO 1998

Body Composition CT imaging of the psoas muscle at the L3 level

Obesity in Malaysia
Ismail, M. N., Chee, S. S., Nawawi, H., Yusoff, K., Lim, T. O., & James, W. P. T. (2002). Obesity in Malaysia. Obesity Reviews, 3(3), 203-208.
• 20.7% were overweight and 5.8% obese
• 0.3% BMI values of > 40.0 kg m(-2)
WHO 2014

Challenges and consequences of obesity in the ICU
Curr Gastroenterol Rep (2016) 18:45

Obesity is frequently associated with co-morbid diseases, altered body
composition & altered metabolic processes
Key points 1

Medical comorbidities
• Linked with multiple co-morbidities
• Altered body composition and metabolic response are significant in the obese

Altered body composition
Dympna Gallagher et al. JPEN J Parenter Enteral Nutr. 2011 September ; 35(5 Suppl): 21S–28S.

Metabolic Derangements
• Increased resting metabolic rate
• Unusual response due to :
- Insulin resistance : decrease insulin level and sensitivity
- Obesity is a ‘pro-inflammatory’ state : lower threshold with exaggerated response to infection
- Altered body composition

Metabolic Derangements
• Effects
- Impaired glucose tolerance
- exacerbates stress induced hyperglycemia
- Increased fatty acid mobilization
- high FFA plasma levels and hyperlipidemia
- Accelerated protein degradation
- depletion of lean body mass

Not all critically ill obese patients are the same
Key Points 2
Obese Patients Exhibit Wide and Unpredictable Variability in Energy Expenditure

Not all critically ill obese patients are the same : the influence of prior co-morbidities
0 1 2 3 4 5
0
5
10
15
20
25
30
Perc
en
t
Number of co-morbidities
Prospective observational study of 183
critically ill patients had a BMI ≥ 30 Raham ISRN Obesity 2012

Not all critically ill obese patients are the same :
the influence of prior co-morbidities
Raham ISRN Obesity 2012
0-1 co-morbidity
(n=38)
2 or more co-
morbidities
(n=145)
p values
Discharged alive from ICU by day 28 36 (94.7%) 112 (77.2%) 0.02
Maximum SOFA score 7.5[5.0 to 11.0] 9.0[6.0 to 13.0] 0.04
Delta SOFA score 1.5[0.0 to 3.0] 2.0[1.0 to 5.0] 0.07
Number of days on MV 2.0[1.0 to 5.0] 4.0[2.0 to 7.0] 0.09
Number of days in ICU 3.0[3.0 to 11.0] 6.0[3.0 to 10.0] 0.04
ICU free days in the first 28 days 24.5[17.0 to 25.0] 20.0[3.0 to
24.0] 0.003
Mortality at Day 14 2 (5.3%) 24 (16.6%) 0.08
Mortality at Day 28 2 (5.3%) 30 (20.7%) 0.03

ICU obese patients are not all created equal… so the impact of nutrition therapy are not to be the same across all patients

Hospitalized Obese Patients Exhibit Wide and Unpredictable Variability in
Energy Expenditure
Feurer ID et al. Ann Surg. 1983;197:17-21

Difficulty in determining caloric
requirement for critically ill obese patients
Key Points 3
Have to rely on weight-based predictive equations to calculate energy and protein requirements

Lack of a validated bedside measure to determine lean body mass in the critically ill
makes accurate protein dosing difficult
Indirect Calorimetry is the gold standard

Clinical challenge
• ‘One size does not fit all’
• Difficulty in calculating nutritional goals
• To achieve net protein anabolism
• To avoid worsening of complications of obesity
- hyperglycemia
• To avoid complications of overfeeding / underfeeding
• To avoid further fat weight gain
• Poor feed tolerance due to poor gastric emptying

Nutrition assessment
• Nutritional risk screening -include biomarkers of metabolic syndrome, determination of level of inflammation
• Evaluation of comorbid conditions -identify preexisting /emerging comorbidities
• Functionality of GI tract
• Risk of aspiration


Estimating Energy Requirements
• Main components of energy expenditure
- Basal metabolic rate (BMR)
- Diet induced thermogenesis
- Level of activity
- Alterations to all above during
illness / disease

Estimating BMR
Why is it difficult in the obese?
As weight is gained, both fat mass (FM) and fat free mass (FFM) are gained
• Not in a linear fashion
• As the body gets fatter, more FM is gained than FFM
• FFM is more metabolically active than FM
• Variable presence of chronic comorbidities
Dickerson 2005


Challenges in estimating energy requirements
• assessment and calculation of energy and protein requirements is ‘one of the most problematic and controversial aspects of nutrition support’
• lack of a validated bedside measure to determine ‘lean body mass’ makes accurate protein dosing difficult
• rely on weight-based predictive equations for calculation

• The disproportionate ratio of FM compared to FFM increases the risk of overfeeding energy when using weight-based predictive equations to calculate REE

How accurate are resting energy expenditure (REE) prediction equations in obese trauma and burn patients?
Stucky CC1, Moncure M, Hise M, Gossage CM, Northrop D.
OBJECTIVES: • The first objective was to compare REE calculated by prediction equations to the measured REE in
obese trauma and burn patients. Our hypothesis was that an equation using fat-free mass would give a more accurate prediction. The second objective was to consider the effect of a commonly used injury factor on the predicted REE.
METHODS: • A retrospective chart review was performed on 28 patients. REE was measured using indirect
calorimetry and compared with the Harris-Benedict and Cunningham equations, and an equation using type II diabetes as a factor. Statistical analyses used were paired t test, +/-95% confidence interval, and the Bland-Altman method.
RESULTS: • Measured average REE in trauma and burn patients was 21.37 +/- 5.26 and 21.81 +/- 3.35 kcal/kg/d, respectively.
Harris-Benedict underpredicted REE in trauma and burn patients to the least extent, while the Cunningham equation underpredicted REE in both populations to the greatest extent. Using an injury factor of 1.2, Cunningham continued to underestimate REE in both populations, while the Harris-Benedict and Diabetic equations overpredicted REE in both populations.
CONCLUSIONS:
• The measured average REE is significantly less than current guidelines. This finding suggests that a hypocaloric regimen is worth considering for ICU patients. Also, if an injury factor of 1.2 is incorporated in certain equations, patients may be given too many calories. (highly unreliable)
JPEN J Parenter Enteral Nutr. 2008 Jul-Aug;32(4):420-6

Determining energy requirements
• No predictive equations of the literature used in this study had the same values of REE as compared to those of indirect calorimetry

• Measure (IC) vs Predicted value
• The accuracy was very low for all predictive equations used,

J Parent Ent Nutr 2013;37:342

ASPEN
Curr Opin Crit Care 2012, 18:174–177

Impact of BMI on estimating energy expenditure
Error:
- Overfeeding in low BMI grp
- Underfeeding in high BMI grp

Weight based predictive equations are less accurate
• Underestimate the REE of obese individuals when IBW is used
• Overestimate energy expenditure when ABW is used

Indirect Calorimetry
• Gold standard
• Measures O₂ uptake and CO₂ released
• Energy expenditure can be calculated
• Costly
• Need trained personnel
• Takes time to complete
• Methodological complications

Key Points 4
Provide early and aggressive
nutritional support
Do not be misled by the well nourished adipose tissue

Nutrition
critically
ill obese
Early
& Aggressive
Minimize
complications
Minimize protein
catabolism
Optimize
Protein
intake

Aim of Nutrition Support in Critically Obese
• Prevent overfeeding
• Minimize metabolic complications
• Maintain lean body mass
• Support immune function
• Support wound healing
• Avoid fluid overload

Ongoing debate
• Optimal route of delivery
• Target dose
• Macronutrient components (proportion of protein and non-protein calories)

Start EN early within 24-48 hrs of admission to ICU
Caloric Debt Adequacy of EN
Caloric debt associated with Longer ICU stay
Days on mechanical ventilation Complications Mortality
Rubinson CCM 2004; Villet Clin Nutr 2005; Dvir Clin Nutr 2006; Petros Clin Nutr 2006

How are Obese Patients Actually Being Fed?
Total 25-<30 30-<35 35<-40 >=40 P-value
Nutritional Prescription
Mean Energy [Kcal/kg/day] (SD) 24.0 (5.8) 23.8 (3.7) 20.2 (3.4) 17.9 (2.8) 15.0 (4.0) <0.0001
Mean Protein [grams/kg/day] (SD)
1.2 (0.3) 1.2 (0.3) 1.0 (0.2) 0.9 (0.2) 0.8 (0.3) <0.0001
Nutrition Received
Mean Energy [Kcal/kg/day] (SD) 14.0 (7.6) 13.6 (6.7) 11.2 (5.9) 9.8 (5.1) 8.1 (4.4) <0.0001
Mean Protein [grams/kg/day] (SD)
0.6 (0.4) 0.6 (0.3) 0.5 (0.3) 0.4 (0.3) 0.4 (0.3) <0.0001
Received EN protein supplements 173 (6.2%) 50 (6.1%) 28 (7.1%) 17 (10.5%) 22 (12.9%) 0.0002
Average caloric deficit in Severely Obese: 12000kcal/10days
- Delayed initiation and Sub-optimal delivery

Survival of patients according to BMI ( Obesity Paradox ?)

Recommendations for nutrition support in critically ill obese patients

Avoid overfeeding (hypercaloric) / underfeeding (hypocaloric)
Key Points 5

• Risks associated with over-feeding: – Hyperglycemia – Hepatic dysfunction
from fatty infiltration – Respiratory acidosis
from increased CO2 production
– Difficulty weaning from the ventilator in mechanically ventilated patients
• Risks associated with under-feeding: – Depressed
ventilatory drive – Decreased
respiratory muscle function
– Impaired immune function
– Increased infection – Loss of lean body
mass and malnutrition if chronic
Increased morbidity
Crit Care. 2015; 19(1): 35

Ensure acceptable nutritional regime/target Hypocaloric vs eucaloric feeding
Key Points 6

Permissive underfeeding allows for both protein and caloric deficits whereas the intent of hypocaloric, high protein diets is to provide only a calorie deficit while ensuring adequate protein intake.

Hypocaloric High Protein Feeding
• delivery of energy that is reduced from total energy expenditure principally through the reduction in carbohydrate input, while targeting high protein and adequate delivery of other nutrients (provision of energy at 60 -70% of requirements)

Benefits of Hypocaloric High Protein Nutrition
Support for Critically Ill Obese Patients
• Decreased potential for overfeeding
• Positive nutritional outcomes ( provide nutrients without exacerbating metabolic issues)
• Assists with glycemic control
• Fat weight loss
• Positive clinical outcomes

Dickerson RN, Boschert KJ, Kudsk KA, Brown RO. Hypocaloric enteral tube feeding in critically ill obese patients.
Nutrition. 2002;18:241-246

OBJECTIVE: We respectively compared the nutritional and clinical efficacies of eucaloric
and hypocaloric enteral feedings in 40 critically ill, obese patients admitted to the trauma or
surgical intensive care unit.
METHODS: Adult patients, 18 to 69 years old, with weights greater than 125% of ideal
body weight, normal renal and hepatic functions, and who received at least 7 d of enteral tube
feeding were studied. Patients were stratified according to feeding group: eucaloric feeding
(≥20 kcal/kg of adjusted weight per day; n = 12) or hypocaloric feeding (<20 kcal/kg of
adjusted weight per day; n = 28). The goal protein intake for both groups was approximately
2 g/kg of ideal body weight per day. Clinical events and nutrition data were recorded for 4
wk.
RESULTS: Patients were similar according to sex, age, weight, body mass index, Second
Acute Physiology and Chronic Health Evaluation score, Trauma score, and Injury Severity
Score. The hypocaloric feeding group received significantly fewer calories than the eucaloric
group (P ≤ 0.05). The hypocaloric group had a shorter stay in the intensive care unit (18.6 ±
9.9 d versus 28.5 ± 16.1 d, P < 0.03), decreased duration of antibiotic therapy days (16.6 ±
11.7 d versus 27.4 ± 17.3 d, P < 0.03), and a trend toward a decrease in days of mechanical
ventilation (15.9 ± 10.8 d versus 23.7 ± 16.6 d, P = 0.09). There was no statistically
significant difference in nitrogen balance or serum prealbumin response between groups.
CONCLUSION: These data suggest that hypocaloric enteral nutrition support is as least as
effective as eucaloric feeding in critically ill, obese patients.
Dickerson RN, Boschert KJ, Kudsk KA. Hypocaloric enteral tube feeding in critically ill obese patients. Nutrition. 2002; 18:241–246.

Caloric intake in medical ICU patients: consistency of care with guidelines and relationship to clinical outcomes.
Krishnan JA, Parce PB, Martinez A, Diette GB, Brower RG. Chest. 2003 Jul;124(1):297-305.
Study objectives • To assess the consistency of caloric intake with American College of Chest
Physicians (ACCP) recommendations for critically ill patients and to evaluate the relationship of caloric intake with clinical outcomes.
• The average caloric intake among 187 participants was 50.6% of the ACCP targets
• The following outcomes were assessed: status on hospital discharge (alive vs dead); spontaneous ventilation before ICU discharge (yes vs no); and ICU discharge without developing nosocomial sepsis (yes vs no).
Conclusions • Study participants were underfed relative to ACCP targets (ie,
33 to 65% of ACCP targets; approximately 9 to 18 kcal/kg per day) was associated with better outcomes than higher levels of caloric intake.

Eucaloric (Optimal calories)
• Optimal amount of calories for critically ill patients: depends on how you slice the cake!
CONCLUSIONS:
• The most appropriate available analyses suggest that attempting to meet caloric targets may be associated with improved clinical outcomes in critically ill patients.
Heyland DK1, Cahill N, Day AG. Crit Care Med 2011 Dec;39(12):2619-26
Optimal Nutrition (>80%) Is Better!

0
10
20
30
40
50
60
0 500 1000 1500 2000
AllPatients< 20
20-25
25-30
30-35
35-40
>40Protein/Calories Delivered
Mo
rta
lity
(%
)
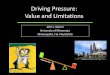
Relationship of Protein/Caloric Intake, 60 day Mortality and BMI
BMI
Increased intakes of energy and protein appear to be associated with improved clinical outcomes in critically ill patients, particularly when BMI is <25 or ≥35 (high risk patient subgroup).

• 113 select ICU patients with sepsis or burns
• On average, receiving 1900 kcal/day and 84 grams of protein


How do we increase nutrition delivery in the Obese Patient?
• Enterally
- High protein
- Protein supplements
• Parenterally
- IV amino acids
- Supplemental PN


The TOP – UP Trial
Stratified by
- site, BMI
- Med vs Surg
RANDOMISED
PN for 7 days
EN alone
Primary outcome 60 days mortality
HIGH RISK
ICU Patients BMI < 25 BMI ≥ 35

Hypothesis
• Increased early energy and protein delivery with EN & PN to underweight (BMI < 25) and obese (BMI ≥ 35) critically ill patients will result in improved survival at 60 days versus standard EN alone

Eligibility criteria
• Inclusion criteria
- Critically ill adult patients (>18 yrs old)
- Expected to require MV > 48 hrs
- Expected ICU dependency ≥ 5 days
- Are on EN or are to be initiated on EN
within 7 days of ICU admission
- Have a BMI of < 25 or ≥ 35 based on pre -
ICU actual or estimated dry weight


Study Intervention
• Both group start EN as per standard care ASAP
• Upon enrollment, study dietitians calculated total volume over 24hrs of either EN or PN required to receive goal calories and proteins
• The PN solution was started at 25mls/hr and increase by 25mls/hr increment every 4 hrs as tolerated (monitoring blood glucose every 4 hrs and electrolytes every 12 hrs) till 100% of goal calories are reached
• As PN rate increased, EN rate decreased (paired feeding)


EN + SPN significantly increased calorie/protein delivery




Conclusion of Top Up Trial
• Topping UP obese critically ill patient feasible
• Possible signals of benefit
- Hand grip strength
- Quality of life

Conclusion
• Need more robust evidence to direct the right feeding strategy for critically ill obese patients
• Tools to optimise energy and protein delivery should be considered and implemented
• No estimation equation accurately estimates requirements in obese individuals - Indirect Calorimetry remains gold standard

Conclusion
• Aggressive use of EN and protein supplements to meet caloric targets are indicated
• Hypocaloric nutrition with protein optimization may be considered for some selected obese ICU patients
• Application with PN and EN regimens are achievable