Embed Size (px)
DESCRIPTION
Rathod K, Panchal A. Knowledge, attitude and practice of community pharmacists of Gujarat towards adverse drug reactions. IAIM, 2014; 1(1): 18-25.
Citation preview

KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Original Research Article
Knowledge, attitude and practice of community
pharmacists of Gujarat towards adverse drug reactions
Kajal Rathod1 H.R. Manager2Senior Executive,
Abstract
Background: Adverse drug reactions (ADR) are one of the leading causes of mortality and morbidity
in India. Community pharmacists are first to report and also in contact with patients, so assessing
their knowledge, attitude and practice towards adverse drug reactions
Aim: To assess knowledge, attitude and practices of community pharmacists of Gujarat towards
adverse drug reactions (ADR).
Material and methods: Cross-sectional study was conducted at Gujarat during the period of January
2014 to June 2014 among 150 community pharmacists.
questionnaire which included 8 questions related to knowledge, 6 questions related to attitude and
6 questions related to practice towards adverse drug reaction (ADR).
Results: Community pharmacists
adverse drug reactions (ADR).
Conclusion: Our findings suggest
managerial interventions regularly to improve ADR reporting
Key words
Knowledge, Attitude, Practice, Adverse drug reactions, Community pharmacists, Gujarat.
Introduction
At present one can’t ignore
reactions (ADR) as one of the leading causes of
morbidity and mortality [1, 2, 3]
too much health care costs [4, 5, 6].
Received on: 01-08-2014
Revised on: 18-08-2014
Accepted on:25-08-2014
How to cite this article:
practice of community pharmacists of Gujarat towards adverse drug
reactions.
Available online a
*Corresponding Author: Kajal Rathod
Rhythm Info Callers Pvt. Ltd., Gujarat, India.
E mail: [email protected]
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
Knowledge, attitude and practice of community
pharmacists of Gujarat towards adverse drug reactions
Kajal Rathod1*
, Arpit Panchal2
H.R. Manager, Rhythm Info Callers Pvt. Ltd., Surat, Gujarat, India.
Senior Executive, Reliance Industries Ltd., Surat, Gujarat, India
Adverse drug reactions (ADR) are one of the leading causes of mortality and morbidity
in India. Community pharmacists are first to report and also in contact with patients, so assessing
their knowledge, attitude and practice towards adverse drug reactions is very helpful.
To assess knowledge, attitude and practices of community pharmacists of Gujarat towards
sectional study was conducted at Gujarat during the period of January
among 150 community pharmacists. We had interviewed
8 questions related to knowledge, 6 questions related to attitude and
6 questions related to practice towards adverse drug reaction (ADR).
acists had poor knowledge and practice but good attitude towards
Our findings suggested the need for positive, evidence based
regularly to improve ADR reporting.
Knowledge, Attitude, Practice, Adverse drug reactions, Community pharmacists, Gujarat.
At present one can’t ignore adverse drug
reactions (ADR) as one of the leading causes of
morbidity and mortality [1, 2, 3] which leads to
too much health care costs [4, 5, 6]. Each and
every ADR can’t be documented by the
manufacturer via early safety studies
very much essential to mon
marketing of drugs [3, 7]. The catastrophe of
thalidomide adverse reaction has aw
countries to establish Pharmacovigilance (PV)
systems for detecting ADR
World Health Organization (WHO) definition, an
ADR is any noxious, unintended, and undesired
effects of a drug, which occurs at doses used
How to cite this article: Rathod K, Panchal A. Knowledge, attitude and
practice of community pharmacists of Gujarat towards adverse drug
reactions. IAIM, 2014; 1(1): 18-25.
Available online at www.iaimjournal.com
Kajal Rathod,
Gujarat, India.
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 18
Knowledge, attitude and practice of community
pharmacists of Gujarat towards adverse drug reactions
Rhythm Info Callers Pvt. Ltd., Surat, Gujarat, India.
ndia.
Adverse drug reactions (ADR) are one of the leading causes of mortality and morbidity
in India. Community pharmacists are first to report and also in contact with patients, so assessing
is very helpful.
To assess knowledge, attitude and practices of community pharmacists of Gujarat towards
sectional study was conducted at Gujarat during the period of January
We had interviewed them with
8 questions related to knowledge, 6 questions related to attitude and
poor knowledge and practice but good attitude towards
positive, evidence based educational and
Knowledge, Attitude, Practice, Adverse drug reactions, Community pharmacists, Gujarat.
be documented by the
via early safety studies, so it is
to monitor ADR after
[3, 7]. The catastrophe of
thalidomide adverse reaction has awaked many
countries to establish Pharmacovigilance (PV)
ystems for detecting ADR [8]. According to
World Health Organization (WHO) definition, an
any noxious, unintended, and undesired
of a drug, which occurs at doses used in
Knowledge, attitude and
practice of community pharmacists of Gujarat towards adverse drug
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
humans for prophylaxis, diagnosis, or therapy
[9]. Among various methods of detecting ADR,
spontaneous reporting has contributed
drastically in superior levels of
pharmacovigilance in many countries [10, 11].
None reporting or under reporting of ADR is a
key barrier for the evolution of
pharmacovigilance programs [12].
association between ADR
knowledge, attitude and practice (KAP) of
community pharmacists had been documented
by various studies [3, 13, 14, 15, 16,
improvement in the KAP of
pharmacists is important for pharmacovigilance
program in any country [18,
pharmacists (CP) are usually
contacted by patients in most ADR and they are
very important source of ADR
the present study, we had selected
pharmacists as the study population and the
objective of the study was to determine the
knowledge, attitude and practice of ADR.
Material and method
Cross-sectional study was conducted at Gujarat
during the period of January 2014 to June 2014.
The study population was 15
pharmacists. Selection of the study population
was random but we had include
who gave voluntary informed written consent
well structured validated and self administered
questionnaire was used to assess the
knowledge, attitude and practice
questionnaire was pretested and verified for
errors. [21, 22, 23] Questionnaire included 8
questions related to knowledge, 6 questions
related to attitude and 6 questions related to
practice towards adverse drug reaction (ADR).
We had interviewed community pharmacists
and collected the data. After that every
community pharmacist had been
20 minutes to fill the questionnaire
they were analyzed.
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
humans for prophylaxis, diagnosis, or therapy
[9]. Among various methods of detecting ADR,
spontaneous reporting has contributed
drastically in superior levels of
ance in many countries [10, 11].
None reporting or under reporting of ADR is a
key barrier for the evolution of
pharmacovigilance programs [12]. Strong
reporting and
itude and practice (KAP) of
d been documented
by various studies [3, 13, 14, 15, 16, 17]. So
the KAP of community
pharmacovigilance
19]. Community
usually first to be
most ADR and they are
reporting [2]. In
we had selected community
as the study population and the
objective of the study was to determine the
knowledge, attitude and practice of ADR.
sectional study was conducted at Gujarat
during the period of January 2014 to June 2014.
The study population was 150 community
. Selection of the study population
included only those
formed written consent. A
well structured validated and self administered
questionnaire was used to assess the
knowledge, attitude and practice [20]. The
as pretested and verified for
Questionnaire included 8
elated to knowledge, 6 questions
related to attitude and 6 questions related to
practice towards adverse drug reaction (ADR).
We had interviewed community pharmacists
and collected the data. After that every
been given time of
inutes to fill the questionnaire and later
Results
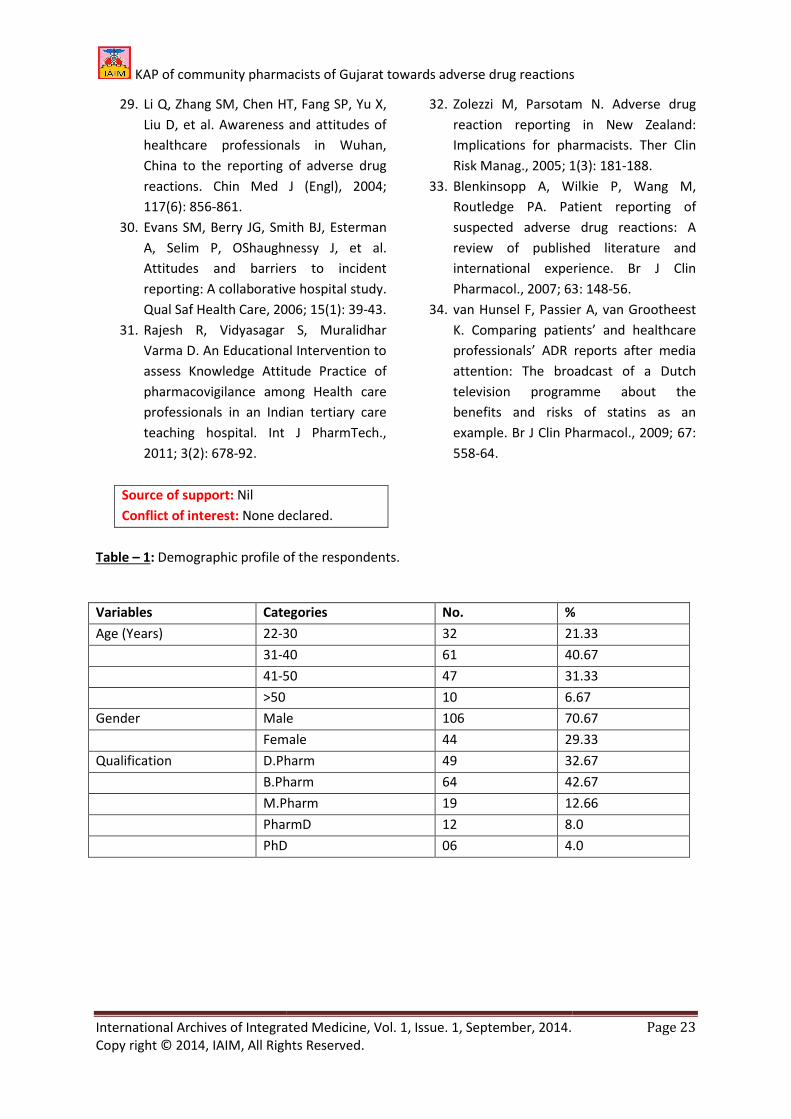
Out study population included 70.67% male
29.33% of female community pharmacists. Of all
the community pharmacists answering the
questionnaire, 32.67% were D.Pharm, 42.67%
were B.Pharm, 12.66% were M.Pharm, 8.0%
were PharmD and 4% were PhD. The highest
number of community pharmacists (40.67%)
was between age group of 31
Table -1.
There were 8 questions for assessment of
knowledge of community pharmacists about
ADR. Among 150 respondents,
aware of terminology ADR. Only 95
the community pharmacists were aware of
national pharmacovigilance centre and
programs. Total 90 (60%) of community
pharmacists were telling all herbal products
were free from ADR. Similarly 79
community pharmacists knew about location of
nearest pharmacovigilance centre. Total 101
(67.33%) respondents believed that ADR should
be reported only when they were
endanger to life as per Table
There were 6 questions related to the attitude
of community pharmacists towards ADR.
Though the respondents had poor knowledge,
they had good attitude towards ADR. Nearly
more than two third of community pharmacists
(80.67%) agreed that they should be involved
ADR reporting process. Total 119 (79.33%)
respondents felt that reporting ADR is part of
professionalism of pharmacists as per
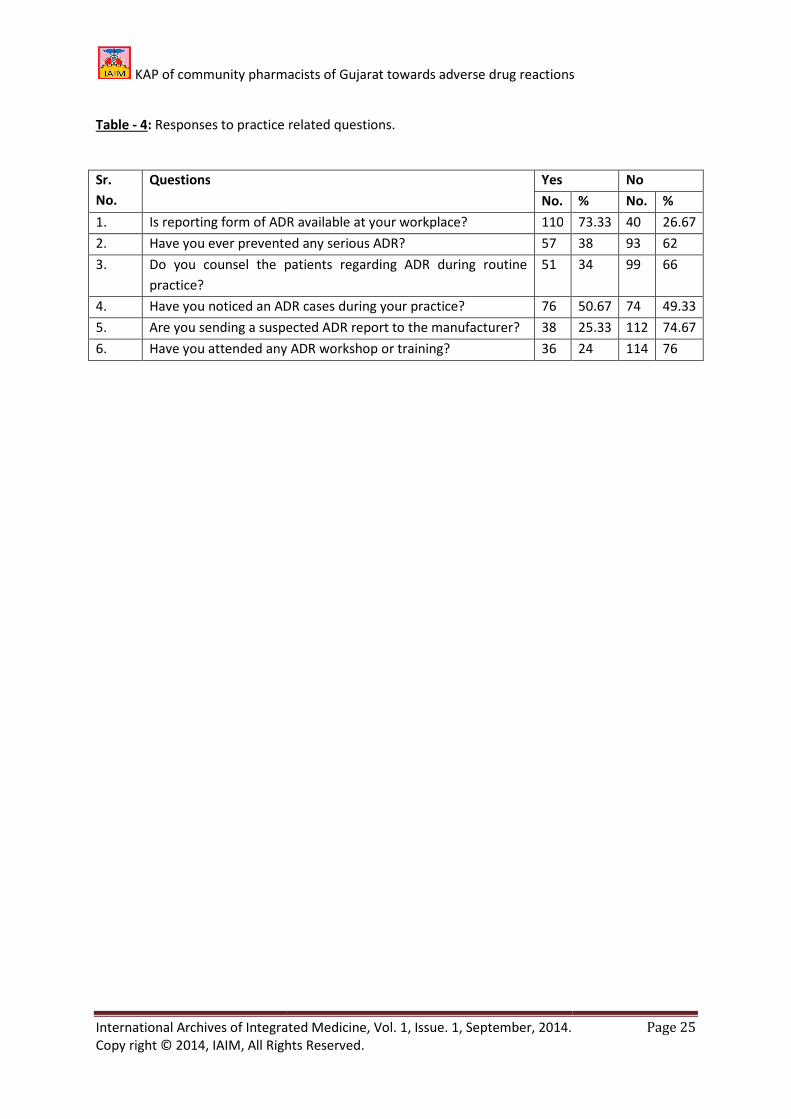
There were 6 questions related to practice of
community pharmacists towards ADR. As
compared to good attitude of th
they had poor practice. Only
community pharmacists had prevented any
serious ADR during their practice. Total 38
(25.33%) had sent suspected ADR report to the
manufacturer. Similarly only 51 (34%) of
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 19
population included 70.67% male and
29.33% of female community pharmacists. Of all
the community pharmacists answering the
questionnaire, 32.67% were D.Pharm, 42.67%
B.Pharm, 12.66% were M.Pharm, 8.0%
were PharmD and 4% were PhD. The highest
number of community pharmacists (40.67%)
was between age group of 31-40 years as per
There were 8 questions for assessment of
knowledge of community pharmacists about
R. Among 150 respondents, 98 (65.33%) were
aware of terminology ADR. Only 95 (63.33%) of
the community pharmacists were aware of
national pharmacovigilance centre and
programs. Total 90 (60%) of community
pharmacists were telling all herbal products
ree from ADR. Similarly 79 (52.67%) of
community pharmacists knew about location of
nearest pharmacovigilance centre. Total 101
(67.33%) respondents believed that ADR should
be reported only when they were grave and
Table – 2.
were 6 questions related to the attitude
of community pharmacists towards ADR.
Though the respondents had poor knowledge,
they had good attitude towards ADR. Nearly
more than two third of community pharmacists
(80.67%) agreed that they should be involved in
ADR reporting process. Total 119 (79.33%)
respondents felt that reporting ADR is part of
of pharmacists as per Table – 3.
There were 6 questions related to practice of
community pharmacists towards ADR. As
compared to good attitude of the respondents,
they had poor practice. Only 57 (38%) of
community pharmacists had prevented any
serious ADR during their practice. Total 38
(25.33%) had sent suspected ADR report to the
manufacturer. Similarly only 51 (34%) of

KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
community pharmacists were co
patients regarding ADR as per Table
results showed that community pharmacists
poor knowledge and practice but good attitude
towards ADR.
Discussion
ADR has significant role in morbidity and
mortality of health set up with its associated
monetary penalty [9, 24]. To recognize ADR
causing drugs, many countries have initiated
pharmacovigilance programs in the recent past.
It is advisable for each country to
own pharmacovigilance programs
individual variation in drug response, different
prescription habits, regulatory body for drugs,
drug availability etc. [9].
Under reporting of ADR is one of the serious
problem for various pharamcovigilance
programs which are good enough to i
drug use patterns [25]. It is essential to improve
the knowledge, attitude and practices (KAP) of
the community pharmacists
reporting and Pharmacovigilance
improvement of reporting rate.
better knowledge about drugs and they are also close
to patient in both hospital and society and thus they
can contribute significantly in ADR reporting.
present study suggested that
pharmacists had poor knowledge towards ADR
reporting and pharmacovigilance
is comparable with other previous studies [15,
26, 27].
Present study showed that 82 (54.67%)
community pharmacists don’t know how t
report ADR. Similar observations had been
noted in China [28] where most
poor knowledge on how to report ADR
opposite side, various studies conducted at UK
[29] and Australia [30] showed adequate
knowledge among participants on how to report
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
community pharmacists were counseling the
Table - 4. All these
results showed that community pharmacists had
poor knowledge and practice but good attitude
has significant role in morbidity and
with its associated
To recognize ADR
countries have initiated
pharmacovigilance programs in the recent past.
country to establish their
own pharmacovigilance programs because of
individual variation in drug response, different
prescription habits, regulatory body for drugs,
one of the serious
for various pharamcovigilance
programs which are good enough to improve
essential to improve
ractices (KAP) of
towards ADR
reporting and Pharmacovigilance for better
. Pharmacists have
drugs and they are also close
to patient in both hospital and society and thus they
can contribute significantly in ADR reporting. The
that community
pharmacists had poor knowledge towards ADR
reporting and pharmacovigilance activity, which
previous studies [15,
Present study showed that 82 (54.67%)
t know how to
observations had been
participants had
to report ADR. On the
studies conducted at UK
] showed adequate
knowledge among participants on how to report
ADR. Rajesh, et al. [31] showed that educational
support significantly increased knowledge,
attitude and practice of pharmacovigilance
among health care providers.
suggested need for awareness programs for the
pharmacists about ADR reporting.
Present study showed good
community pharmacist, though the knowledge
was poor. The findings of
consistent with other studies
where pharmacists showed
towards ADR reporting but different from th
study done at New Zealand, where pharmacists
showed negative attitude [32
study, 79.33% of the community pharmacist
were agreed that ADR reporting was a part of
their professionalism. These results were
to study conducted at Saudi Arabia [15] where
the vast majority of p
considered ADR reporting a
professionalism. In the pre
towards ADR was also very poor. Only
of community pharmacists had prevented any
serious ADR during their practice. Total 38
(25.33%) had sent suspected ADR report to the
manufacturer.
Overall poor KAP score
present study which suggested
improve the ADR reporting. For the same
certain steps like improvement
in future to reduce the incidence of
clinical practice and reduction in health care
costs. Promotion of patient self
an important step [33, 34]. Patient self
can play complimentary role to
reporting in developing country such as India. It
was also opined that reporting
should be prioritized. Reporting should be made
easy and convenient by e mail or
telephone, fax etc., which can improve speed
and quality of reports.
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 20
Rajesh, et al. [31] showed that educational
support significantly increased knowledge,
attitude and practice of pharmacovigilance
among health care providers. These findings
suggested need for awareness programs for the
pharmacists about ADR reporting.
esent study showed good attitude of the
community pharmacist, though the knowledge
was poor. The findings of our study were
other studies of UK [13, 30],
where pharmacists showed positive attitude
reporting but different from the
study done at New Zealand, where pharmacists
showed negative attitude [32]. In the present
79.33% of the community pharmacists
reporting was a part of
These results were similar
di Arabia [15] where
the vast majority of pharmacists (90%)
reporting as part of their
In the present study, practice
also very poor. Only 57 (38%)
of community pharmacists had prevented any
g their practice. Total 38
(25.33%) had sent suspected ADR report to the
was noted during
present study which suggested there is need to
reporting. For the same,
improvement in ADR reporting
the incidence of ADR in
reduction in health care
romotion of patient self reporting is also
Patient self reporting
complimentary role to increase ADR
developing country such as India. It
was also opined that reporting of serious ADR
should be prioritized. Reporting should be made
easy and convenient by e mail or website,
which can improve speed

KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Patient safety and better community is the
prime goal which can be achieved by active and
voluntary participation of community
pharmacists in the pharmacovigilance
However, pharmacovigilance center
up positive attitude of the pharmacists,
them understand value of reporting in morbidity
and mortality reduction by reporting
updating them regarding pharmacovigilance
news time to time.
Conclusion
We identified the knowledge, attitude and
practice of the community pharmacists
regarding ADR monitoring and
pharmacovigilance. Overall the
attitude and practice scores were low. Our
findings suggested the need for
evidence based educational and managerial
interventions regularly.
Acknowledgement
Authors acknowledge the immense help
received from the scholars whose articles are
cited and included in references
manuscript. The authors are
authors / editors /publishers of all those articles,
journals and books from where the literat
this article has been reviewed and discussed.
References
1. Gallagher RM, Kirkham JJ, Mason JR,
Bird KA, Williamson PR, Nunn AJ, et al.
Development and inter
of the Liverpool adverse drug reaction
causality assessment tool,
2011; 6(12): e28096.
2. Elkalmi RM, Hassali MA, Ibrahim MIM,
Widodo RT, Efan QM, Hadi MA.
Pharmacy students’ knowledge and
perceptions about pharmaco vigilance i
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
and better community is the
which can be achieved by active and
of community
pharmacists in the pharmacovigilance program.
center has to keep
up positive attitude of the pharmacists, make
value of reporting in morbidity
by reporting and by
pharmacovigilance
We identified the knowledge, attitude and
of the community pharmacists
monitoring and
pharmacovigilance. Overall the knowledge,
scores were low. Our
the need for positive,
educational and managerial
acknowledge the immense help
received from the scholars whose articles are
cited and included in references of this
also grateful to
authors / editors /publishers of all those articles,
journals and books from where the literature for
this article has been reviewed and discussed.
Gallagher RM, Kirkham JJ, Mason JR,
Bird KA, Williamson PR, Nunn AJ, et al.
Development and inter-rater reliability
of the Liverpool adverse drug reaction
causality assessment tool, PloS One,
Elkalmi RM, Hassali MA, Ibrahim MIM,
Widodo RT, Efan QM, Hadi MA.
Pharmacy students’ knowledge and
perceptions about pharmaco vigilance in
Malaysian public universities.
Pharm Educ, 2011; 75(5)
3. Kharkar M, Bowalekar S. Kno
attitude and perception/practices (KAP)
of medical practitioners in India towards
adverse drug reaction (ADR) reporting.
Perspect Clin Res, 2012; 3(3)
4. Patel KJ, Kedia MS, Bajpai D, Mehta SS,
Kshirsagar NA, Gogtay NJ. Evaluation of
the prevalence and economic burden of
adverse drug reactions presenting to the
medical emergency department of a
tertiary referral centre: A prospective
study. BMC Clinical Pharmacology, 2007;
7(1): 7-8.
5. Dormann H, Muth-
Criegee-Rieck M, Tegeder
HT, et al. Incidence and costs of adverse
drug reactions during hospitalization.
Drug Saf, 2000; 22(2)
6. Ernst FR, Grizzle AJ. Drug
morbidity and mortality: Updating the
cost-of-illness model.
(Wash), 2001; 41(2):
7. Stricker BH, Psaty BM. Detection,
verification, and quantification of
adverse drug reactions.
329(7456): 44-47.
8. Meyboom RH, Egberts AC, Gribnau FW,
Hekster YA. Pharmacovigilance in
perspective. Drug Saf, 1999; 21(6):
447.
9. World Health Organization. Safety of
Medicines - A guide for detecting and
reporting adverse drug reactions.
Geneva, Switzerland: World Health
Organization, 2002.
10. Waller PC. Making the most of
spontaneous adverse drug reaction
reporting. Basic Clin
2006; 98: 320-323.
11. Vallano A, Cereza G, Pedròs C, Agustí A,
Danés I, Aguilera C,
solutions for spontaneous reporting of
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 21
Malaysian public universities. Am J
Pharm Educ, 2011; 75(5).
Kharkar M, Bowalekar S. Knowledge,
attitude and perception/practices (KAP)
of medical practitioners in India towards
adverse drug reaction (ADR) reporting.
Perspect Clin Res, 2012; 3(3): 90-94.
Patel KJ, Kedia MS, Bajpai D, Mehta SS,
Kshirsagar NA, Gogtay NJ. Evaluation of
lence and economic burden of
adverse drug reactions presenting to the
medical emergency department of a
tertiary referral centre: A prospective
BMC Clinical Pharmacology, 2007;
-Selbach U, Krebs S,
Rieck M, Tegeder I, Schneider
HT, et al. Incidence and costs of adverse
drug reactions during hospitalization.
Drug Saf, 2000; 22(2): 161-168.
Ernst FR, Grizzle AJ. Drug-related
morbidity and mortality: Updating the
illness model. J Am Pharm Assoc
1(2): 192-199.
Stricker BH, Psaty BM. Detection,
verification, and quantification of
adverse drug reactions. Br Med J, 2004;
Meyboom RH, Egberts AC, Gribnau FW,
Hekster YA. Pharmacovigilance in
Drug Saf, 1999; 21(6): 429-
World Health Organization. Safety of
A guide for detecting and
reporting adverse drug reactions.
Geneva, Switzerland: World Health
, 2002.
Waller PC. Making the most of
spontaneous adverse drug reaction
lin Pharmacol Toxicol.,
Vallano A, Cereza G, Pedròs C, Agustí A,
Aguilera C, et al. Obstacles and
solutions for spontaneous reporting of

KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
adverse drug reactions in the hospital.
Br J Clin Pharmacol., 2005; 60: 653
12. Hazell L, Shakir SA. Under
adverse drug reactions.
29(5): 385-396.
13. Sweis D, Wong IC. A survey on factors
that could affect adverse drug reaction
reporting according to hospital
pharmacists in Great Britain.
2000; 23(2): 165-172.
14. Herdeiro MT, Figueiras A, Polnia J,
Gestal-Otero JJ. Physicians’ Attitudes
and Adverse Drug Reaction Reporting.
Drug saf, 2005; 28(9): 825
15. Bawazir SA. Attitude of community
pharmacists in Saudi Arabia towards
adverse drug reaction reporting.
Pharm J, 2006; 14(1): 75
16. Aziz Z, Siang TC, Badarudin NS.
Reporting of adverse drug reactions:
Predictors of under
Malaysia. Pharmacoepidemiol Drug Saf,
2007; 26(2): 223-228.
17. Gavaza P, Brown CM, Lawson KA,
Rascati KL, Wilson JP, Ste
Influence of attitudes on pharmacists'
intention to report serious adverse drug
events to the Food and Drug
Administration. Br J Clin Pharmacol.,
2011; 72(1): 143-152.
18. Van Grootheest AC, Van Puijenbroek EP,
De Jongvan den Berg LTW. Contribution
of pharmacists to the reporting of
adverse drug reactions.
Pharmacoepidemiol Drug Saf, 2002;
11(3): 205-210.
19. Herdeiro MT, Polnia J, Gestal
Figueiras A. Improving the Reporting of
Adverse Drug Reactions.
31(4): 335-344.
20. Rathod GB, Parmar P. Comparison
regarding knowledge, attitude and
practice of blood donation between
health professionals and general
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
adverse drug reactions in the hospital.
2005; 60: 653-658.
Shakir SA. Under-reporting of
adverse drug reactions. Drug Saf, 2006;
Sweis D, Wong IC. A survey on factors
that could affect adverse drug reaction
reporting according to hospital
pharmacists in Great Britain. Drug Saf,
Herdeiro MT, Figueiras A, Polnia J,
Otero JJ. Physicians’ Attitudes
and Adverse Drug Reaction Reporting.
825-833.
Bawazir SA. Attitude of community
pharmacists in Saudi Arabia towards
adverse drug reaction reporting. Saudi
75-83.
Aziz Z, Siang TC, Badarudin NS.
Reporting of adverse drug reactions:
Predictors of under-reporting in
Pharmacoepidemiol Drug Saf,
Gavaza P, Brown CM, Lawson KA,
Rascati KL, Wilson JP, Steinhardt M.
Influence of attitudes on pharmacists'
intention to report serious adverse drug
events to the Food and Drug
Br J Clin Pharmacol.,
Van Grootheest AC, Van Puijenbroek EP,
De Jongvan den Berg LTW. Contribution
of pharmacists to the reporting of
adverse drug reactions.
Pharmacoepidemiol Drug Saf, 2002;
Herdeiro MT, Polnia J, Gestal-Otero JJ,
Figueiras A. Improving the Reporting of
Adverse Drug Reactions. Drug Saf, 2008;
, Parmar P. Comparison
regarding knowledge, attitude and
practice of blood donation between
health professionals and general
population. Int J Cur Res Rev, 2012;
4(21): 114-120.
21. Parmar P, Rathod GB. Study of
knowledge, attitude and perception
regarding medico-
general population. Int J Med Pharm Sci,
2013; 3(6): 1-6.
22. Rathod GB, Rathod
A. Study of knowledge,
practice of general
Waghodia towards Diabetes
J Cur Res Rev, 2014;
23. Parmar P, Rathod GB, Rathod S, Goyal R,
Aggarwal S, Parikh A. Study of
knowledge, attitude and practice of
general population of Gandhinagar
towards hypertension.
Microbiol. App. Sci, 2014;
24. Moore N, Lecointre D, Noblet C,
M. Frequency and cost of serious
adverse drug reactions in a department
of general medicine. Br J Clin
Pharmacol., 1998; 45: 301
25. Lee A, Thomas SHL. Adverse drug
reactions. In: Walker R and Edward C.
Clinical pharmacy and Therapeutics. 3
edition, Churchill Livingstone
33-46.
26. Vessal G, Mardani Z, Mollai M.
Knowledge, attitudes, and perceptions
of pharmacists to adverse drug reaction
reporting in Iran.
2009; 31(2): 183-187.
27. Ting KN, Stratton-Powell DM, Anderson
C. Community pharmacists views on
adverse drug reactions reporting in
Malaysia: A pilot study.
Sci., 2010; 32(3): 339
28. Green CF, Mottram DR, Rowe PH,
Pirmohamed M. Attitudes and
knowledge of hospital p
adverse drug reaction reporting.
Pharmacol., 2001; 51(1):
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 22
population. Int J Cur Res Rev, 2012;
Parmar P, Rathod GB. Study of
knowledge, attitude and perception
-legal autopsy in
general population. Int J Med Pharm Sci,
S, Parmar P, Parikh
knowledge, attitude and
general population of
Diabetes mellitus. Int
6(1): 63-68.
Parmar P, Rathod GB, Rathod S, Goyal R,
Aggarwal S, Parikh A. Study of
knowledge, attitude and practice of
general population of Gandhinagar
towards hypertension. Int. J. Curr.
2014; 3(8): 680-685.
Moore N, Lecointre D, Noblet C, Mabille
M. Frequency and cost of serious
adverse drug reactions in a department
of general medicine. Br J Clin
Pharmacol., 1998; 45: 301-308.
Lee A, Thomas SHL. Adverse drug
In: Walker R and Edward C.
Clinical pharmacy and Therapeutics. 3rd
Churchill Livingstone, 2003, p.
G, Mardani Z, Mollai M.
Knowledge, attitudes, and perceptions
of pharmacists to adverse drug reaction
reporting in Iran. Pharm World Sci,
187.
Powell DM, Anderson
C. Community pharmacists views on
adverse drug reactions reporting in
Malaysia: A pilot study. Pharm World
339-342.
Green CF, Mottram DR, Rowe PH,
Pirmohamed M. Attitudes and
knowledge of hospital pharmacists to
adverse drug reaction reporting. Br J Clin
Pharmacol., 2001; 51(1): 81-86.
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
29. Li Q, Zhang SM, Chen HT, Fang SP, Yu X,
Liu D, et al. Awareness and attitudes of
healthcare professionals in Wuhan,
China to the reporting of adverse drug
reactions. Chin Med J (Engl), 2004;
117(6): 856-861.
30. Evans SM, Berry JG, Smith BJ, Esterman
A, Selim P, OShaughnessy J, et al.
Attitudes and barriers to incident
reporting: A collaborative hospital study.
Qual Saf Health Care, 2006; 15(1)
31. Rajesh R, Vidyasagar S, Muralidhar
Varma D. An Educational Intervention to
assess Knowledge Attitude Practice of
pharmacovigilance among Health care
professionals in an Indian tertiary care
teaching hospital. Int J PharmTech.,
2011; 3(2): 678-92.
Source of support: Nil
Conflict of interest: None declared.
Table – 1: Demographic profile of the respondents.
Variables Categ
Age (Years) 22-30
31-40
41-50
>50
Gender Male
Female
Qualification D.Pharm
B.Pharm
M.Pharm
PharmD
PhD
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
Li Q, Zhang SM, Chen HT, Fang SP, Yu X,
Liu D, et al. Awareness and attitudes of
healthcare professionals in Wuhan,
China to the reporting of adverse drug
Chin Med J (Engl), 2004;
Evans SM, Berry JG, Smith BJ, Esterman
A, Selim P, OShaughnessy J, et al.
Attitudes and barriers to incident
reporting: A collaborative hospital study.
Qual Saf Health Care, 2006; 15(1): 39-43.
ar S, Muralidhar
Varma D. An Educational Intervention to
assess Knowledge Attitude Practice of
pharmacovigilance among Health care
professionals in an Indian tertiary care
teaching hospital. Int J PharmTech.,
32. Zolezzi M, Parsotam N. Adve
reaction reporting in New Zealand:
Implications for pharmacists.
Risk Manag., 2005; 1(3)
33. Blenkinsopp A, Wilkie P, Wang M,
Routledge PA. Patient reporting of
suspected adverse drug reactions: A
review of published literature an
international experience. Br J Clin
Pharmacol., 2007; 63: 148
34. van Hunsel F, Passier A, van Grootheest
K. Comparing patients’ and healthcare
professionals’ ADR reports after media
attention: The broadcast of a Dutch
television programme about the
benefits and risks of statins as an
example. Br J Clin Pharmacol., 2009; 67:
558-64.
None declared.
of the respondents.
ategories No. %
30 32 21.33
40 61 40.67
50 47 31.33
10 6.67
Male 106 70.67
Female 44 29.33
D.Pharm 49 32.67
B.Pharm 64 42.67
M.Pharm 19 12.66
PharmD 12 8.0
PhD 06 4.0
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 23
Zolezzi M, Parsotam N. Adverse drug
reaction reporting in New Zealand:
Implications for pharmacists. Ther Clin
Risk Manag., 2005; 1(3): 181-188.
Blenkinsopp A, Wilkie P, Wang M,
Routledge PA. Patient reporting of
suspected adverse drug reactions: A
review of published literature and
international experience. Br J Clin
Pharmacol., 2007; 63: 148-56.
van Hunsel F, Passier A, van Grootheest
K. Comparing patients’ and healthcare
professionals’ ADR reports after media
attention: The broadcast of a Dutch
television programme about the
fits and risks of statins as an
example. Br J Clin Pharmacol., 2009; 67:
%
21.33
40.67
31.33
6.67
70.67
29.33
32.67
42.67
12.66
8.0
4.0

KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Table - 2: Responses to knowledge related questions.
Sr.
No.
Questions
1. Do you know about adverse drug reactions (ADR)
2. Do you consider every drug
harmless?
3. Every herbal product available in the
adverse drug reactions (
4. Do you know how to make report of ADR
4. Do you have any idea regarding National
Pharmacovigilance Centre and programs?
5. Do you know where the nearest Pharmacovigilance
Centre is located?
6. ADR should be reported only when they are grave
endanger to life. – Is it true?
7. Reports of National ADR C
people?
Table – 3: Responses to attitude related questions.
Sr.
No.
Questions
1. Community pharmacist should
2. ADR reporting is part of the professionalism of pharmacist
3. Do you think serious ADR
the relevant authority?
4. ADR reporting should be made compulsory for all
pharmacists?
5. Consulting the physician is important before reporting an ADR?
6. Do you agree that ADR is related to t
or not?
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
Responses to knowledge related questions.
Yes
No. %
about adverse drug reactions (ADR)? 98 65.33
Do you consider every drug obtainable in the shop is 46 30.66
available in the shop may have
adverse drug reactions (ADR)?
90 60
make report of ADR? 68 45.33
have any idea regarding National
entre and programs?
95 63.33
where the nearest Pharmacovigilance 79 52.67
should be reported only when they are grave and
Is it true?
101 67.33
National ADR Centre are available for all 57 38
Responses to attitude related questions.
Yes
No.
Community pharmacist should be involved in ADR reporting? 121
ADR reporting is part of the professionalism of pharmacist? 119
encourage pharmacists to report it to 98
ADR reporting should be made compulsory for all practicing 96
onsulting the physician is important before reporting an ADR? 59
that ADR is related to the drug, before reporting 101
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 24
No
No. %
65.33 52 34.67
30.66 104 69.34
60 40
45.33 82 54.67
63.33 55 36.67
52.67 71 47.33
67.33 49 32.67
93 62
No
% No. %
89.67 29 19.33
79.33 31 20.67
65.33 52 34.67
64 54 36
39.33 91 60.67
67.33 49 32.67
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Table - 4: Responses to practice
Sr.
No.
Questions
1. Is reporting form of ADR
2. Have you ever prevented any serious ADR
3. Do you counsel the patients regarding ADR during
practice?
4. Have you noticed an ADR cases
5. Are you sending a suspected ADR report to the
6. Have you attended any ADR workshop or training?
KAP of community pharmacists of Gujarat towards adverse drug reactions
International Archives of Integrated Medicine, Vol. 1, Issue. 1, September, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
related questions.
Yes
No.
of ADR available at your workplace? 110
ou ever prevented any serious ADR? 57
patients regarding ADR during routine 51
Have you noticed an ADR cases during your practice? 76
g a suspected ADR report to the manufacturer? 38
any ADR workshop or training? 36
KAP of community pharmacists of Gujarat towards adverse drug reactions
Page 25
No
% No. %
73.33 40 26.67
38 93 62
34 99 66
50.67 74 49.33
25.33 112 74.67
24 114 76





























