Embed Size (px)
Citation preview

Acta Med Scand 207: 483488, 1980
Knowledge of Diabetes Mellitus, Diets and Nutrition in Diabetic Patients
Sven-Gunnar Karlander, Inger Alinder and Kjell Hellstrom
From the Deportment of Medicine, St . Erik's Hospitcil, Stockholm. Siiqeden
ABSTRACT. A multiple choice questionnaire was used to test the level of knowledge about diabetes mellitus and diet-nutrition in diabetic patients (n=317), non-diabetic patients (n=70), nursing per- sonnel ( n =53) and third-year medical students ( n =43). The results concerning diabetes were better than those for diet-nutrition. A score of 380% in diet-nutrition was considered necessary for proper management of the diet at home. This level was reached by 84 % of the students, 26 % of the nursing personnel, 29 % of the insulin-treated diabetics ( n = 178), 9 % of the tablet-treated diabetics (n = 124) and 4 % of the non-diabetic patients. It was concluded that the piecemeal instruction system used to teach the diabetic patients is inefficient and should be re- placed by a formal educational program integrated into the patient care system. The level of knowledge among nursing personnel needs to be improved.
Key w.ords: diabetes mellitus, multiple choice test, knowl- edge of disease, knowledge of nutrition. Acta Med Scand 207: 483, 1980.
Education of the patient is of vital importance for the proper control of diabetes mellitus (DM), as the patient shares the responsibility for management of the disease. T h e teaching technique varies from sys- tematic programs t o piecemeal instruction by physicians, nurses and dieticians. Surprisingly little interest has been devoted to evaluating the long- term effect of such education. T h e aim of the cur- rent study was t o explore how much Swedish dia- betic patients treated in an out-patient department know about DM, diets and nutrition.
current study is part of an evaluation of clinical results at our Diabetic Out-Patient Department. All patients visiting the Diabetic Out-Patient Department during Jan.-April 1977 were invited to participate in the study. Out of 376 patients. 39 in general very old patients (mean age about 75 years) either refused or were incapable of under- standing the questions even when read by a nurse. Another 20 patients who visited the department for the first time were excluded as being uninstructed. Of the 317 participating patients, 15 were prescribed a dietary regi- men (group D), 124 a dietary regimen + hypoglycemic tablets (group T) and 178 a dietary regimen + insulin (group I). The mean age was about 10 years higher in group T (66k1.0 years) than in the other groups. The mean duration of DM was 2.4.8.6 and 14.6 years in groups D, T and I, respectively (Table I). For comparison, the study also included 70 non-diabetic patients (group ND) attending the Out-Patient Department (mean age 57 years), 53 members of the nursing staff (nurses and nurses' assistants) and 43 third-year medical students educated in DM. The nursing personnel and the students were tested anonymously.
The questionnaire
All subjects were tested with the aid of a multiple choice questionnaire (Appendix). Questions 1 4 put to all sub- jects, covered basic concepts about DM. Questions 11-13 and TI-T2, dealing with therapy, were given to groups I and T, respectively. These questions were also put to the students and the nursing personnel but not to ND patients. All participants were given questions 5-18, designed to test knowledge about diet and nutrition. Scores concern- ing DM as a disease (questions 1 4 , 11-13. TI-T2), diets and nutrition (questions 5-18) were summarized sepa- rately.
Laborurory investigations
All laboratory investigations are described in the adjacent paper (6).
SUBJECTS A N D METHODS Purticipunrs. Diabetes care at St. Erik's Hospital, Stock- holm, has been presented in an adjacent paper (6). The
Abbreviations: DM = diabetes mellitus, group D = diet- treated patients, group T = tablet-treated patients, group I = insulin-treated patients, group ND = non-diabetic patients.
484 S.-G. Krrrlrrnder et (11 .
Table I . B a s d dritcr on the pcrtients pcirticiprrting in t l lP sr1td.V
Duration No. of No. of Age of DM
Group females males (y . ) ( Y . ) ~~~ ~~~~
D 6 9 53.9f3.9 2.4k0.6 T 77 47 66.0k 1 .O 8.6k0.5 I 102 76 55.5k1.3 14.6k0.7 ND 33 37 57.0f2.1 -
Sra1istic.s Data are presented as mean f S.E.M. A X2-test was used for statistical analysis of scores dealing with diets and nutrition. Because of the repetition of the X2-test, the level of significance was set atp<O.Ol. Correlations were calcu- lated using the Spearman correlation coefficient.
RESULTS
Knoii-ledge uhoirt DM (yitestions l 4 * 11-13, TI-72) Except for groups T and ND, the percentage cor- rect answers averaged more than 80 in all groups (Table 11). The best results were recorded for the students (93.9+1.1%), 93% of whom scored 380%. This level was also reached by 64% of the nursing personnel, 66% of group D, 52% of group T, 75 9% of group I and 19% of group ND patients. The percentage correct answers was approximately the same for all questions. However, more than 50% of the patients in group T did not know the basal effects of sulphonylurea treatment.
Knoi\ ’ ldge rrborit diets rind nrttrition (ywstions 5-18)
The percentage correct answers in all groups tended to be lower than for the questions about DM. The students’ score averaged 90% and that of the nursing personnel 74%. This result does not differ from that of group I. The non-diabetic pa- tients scored 50%. which is below the scores of groups D and T (Table 11). Reasonably good scores ( 2 8 0 %) were observed for only 29 % of the patients in group I. The corresponding figures for group T (9%) and group ND (4%) were very similar. The level of knowledge among the nursing personnel was inadequate, as 21 % scored less than 60%. The 80% level was reached by only 26%, compared to 84% of the students.
In general, the results for individual questions
varied uniformly among the groups of subject5 (Ta- ble Ill). I t is remarkable that less than 50% of the diabetic patients and only 74% of the nursing per- sonnel identified the very simple definition of car- bohydrates in question 5. Similar poor results were obtained for question 7, in which the participants had to give a good reason w h y diabetics are recom- mended to keep to a low-fat diet. Only about 40% of the diabetic patients and 51 % of the nursing personnel knew that fat gives rise to more energy than protein and carbohydrates. The results also show that even insulin-treated patients had poor knowledge about such an essential nutrient as milk (question 14) and how to plan an adequate breakfast (question 17). It is still more surprising that this also applies to about 50% of the nursing personnel. The best scores were obtained for questions 13, 15 and 18. Here the patients had to choose between var- ious alternatives for a snack (no. 13), to know that juice, beer and lemonade contain sugar (no. 15) and that the Swedish term “light milk’’ stands for milk with a lower fat content than standard milk (no. 18).
Correlations
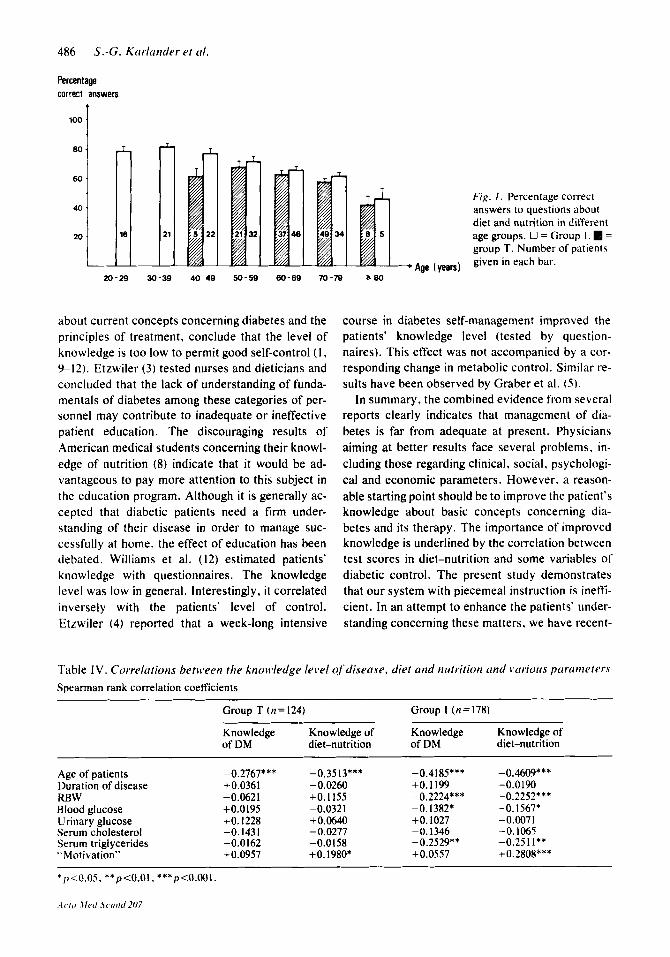
Increasing age in groups T and 1 was associated with a slight but significant decline in knowledge concerning both DM and diet-nutrition (Fig. I and Table IV). The level of knowledge about these sub- jects was much the same in both sexes. I t showed no correlation with the duration of the patients’ DM, the number of visits to the Out-Patient De- partment or whether they had been treated at the Day-care Unit. However, “motivated” patients- those claiming that they planned their meals with the aid of dietary prescription lists, tested their urine for sugar and ketones and exercised regular- ly-reached better scores in diet-nutrition than the others (Table IV). Among the insulin-dependent pa- tients, significant inverse correlations were found between test scores and relative body weight and blood glucose and serum triglyceride concentra- tions.
DISCUSSION
The selection of patients for this study has been discussed in our adjacent paper (6). We have reasons to believe that the results portray the level of knowledge among diabetic patients in a fairly large Stockholm area. The questions offered in the test deal with simple problems of the type which
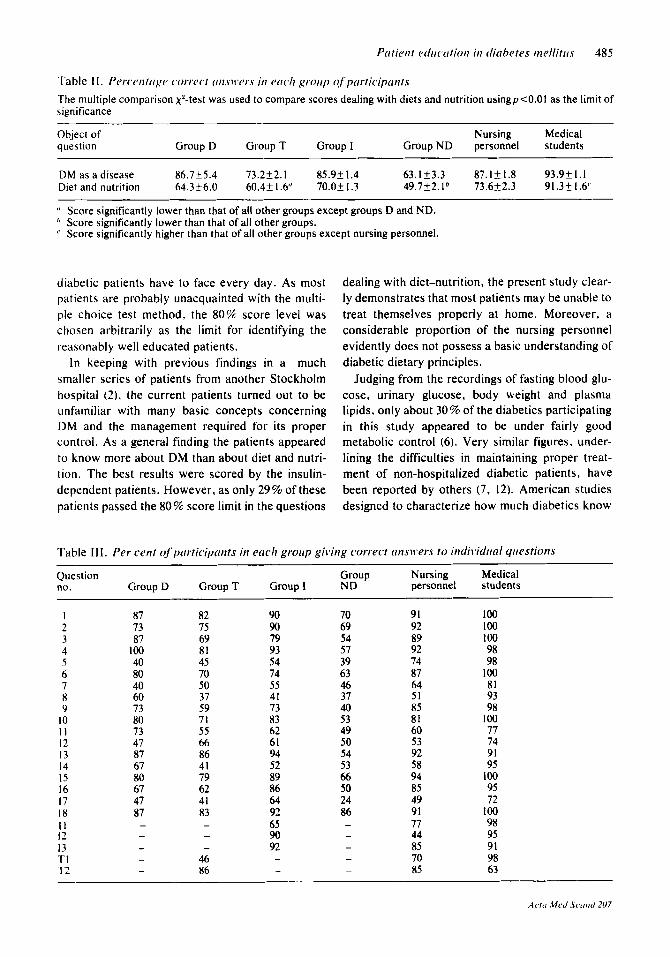
Table I I . Pcr i~~nt r igr c o r r ~ c t wisuws in e r i c Y r groitp c!f'prirticiptrrit.~
The multiple comparison Xz-test was used to compare scores dealing with diets and nutrition usingp<0.01 as the limit of significance
Object of Nursing Medical question Group D Group T Group I Group ND personnel students
DM as a disease 86.7k5.4 73.252.1 85.9f1.4 63.1k3.3 87.121.8 93.9t1.1 Diet and nutrition 64.3t6.0 60.4t I .6' 70.05 I .3 49.7f2.1" 73.6k2.3 91.3f1.6"
(' Score significantly lower than that of all other groups except groups D and ND. ', Score significantly lower than that of all other groups.
Score significantly higher than that of all other groups except nursing personnel.
diabetic patients have to face every day. As most patients are probably unacquainted with the multi- ple choice test method, the 80% score level was chosen arbitrarily as the limit for identifying the reasonably well educated patients.
In keeping with previous findings in a much smaller series of patients from another Stockholm hospital (2). the current patients turned out to be unfamiliar with many basic concepts concerning DM and the management required for its proper control. As a general finding the patients appeared to know more about DM than about diet and nutri- tion. The best results were scored by the insulin- dependent patients. However, as only 29% of these patients passed the 80% score limit in the questions
dealing with diet-nutrition, the present study clear- ly demonstrates that most patients may be unable to treat themselves properly at home. Moreover, a considerable proportion of the nursing personnel evidently does not possess a basic understanding of diabetic dietary principles.
Judging from the recordings of fasting blood glu- cose, urinary glucose, body weight and plasma lipids, only about 30% of the diabetics participating in this study appeared to be under fairly good metabolic control ( 6 ) . Very similar figures, under- lining the difficulties in maintaining proper treat- ment of non-hospitalized diabetic patients, have been reported by others (7, 12). American studies designed to characterize how much diabetics know
Table Il l . Per cent qf'ptirticipunts in ericli groirp gii ing correct (insii'ers to indi~Vdrinl yriestionA
Question Group Nursing Medical no. Group D Group T Group I ND personnel students
7 8 9
10 1 1 12 13 14 15 16 17 18 I I 12 13 TI T2
87 73 87
100 40 80 40 60 73 80 73 47 87 67 80 67 47 87 - - - - -
~
82 75 69 81 45 70 50 37 59 71 55 66 86 41 79 62 41 83 - - -
46 86
90 90 79 93 54 74 55 41 73 83 62 61 94 52 89 86 64 92 65 90 92 - -
70 69 54 57 39 63 46 37 40 53 49 50 54 53 66 50 24 86 - - - - -
91 92 89 92 74 87 64 51 85 81 60 53 92 58 94 85 49 91 77 44 85 70 85
100 100 100 98 98
100 81 93 98
100 77 74 91 95
100 95 72
100 98 95 91 98 63
486 S.-G. Ktrrlunder et id.
Percentage correct answers
Fig. I . Percentage correct answers to questions about diet and nutrition in different age groups. 0 = Group I . = group T. Number of patients given in each bar.
--+ Age (years)
about current concepts concerning diabetes and the principles of treatment, conclude that the level of knowledge is too low to permit good self-control (1 , 9-12). Etzwiler (3) tested nurses and dieticians and concluded that the lack of understanding of funda- mentals of diabetes among these categories of per- sonnel may contribute to inadequate or ineffective patient education. The discouraging results of American medical students concerning their knowl- edge of nutrition (8) indicate that it would be ad- vantageous to pay more attention to this subject in the education program. Although it is generally ac- cepted that diabetic patients need a firm under- standing of their disease in order to manage suc- cessfully at home, the effect of education has been debated. Williams et al. (12) estimated patients' knowledge with questionnaires. The knowledge level was low in general. Interestingly, it correlated inversely with the patients' level of control. Etzwiler (4) reported that a week-long intensive
course in diabetes self-management improved the patients' knowledge level (tested by question- naires). This effect was not accompanied by a cor- responding change in metabolic control. Similar re- sults have been observed by Graber et al. ( 5 ) .
In summary, the combined evidence from several reports clearly indicates that management of dia- betes is far from adequate at present. Physicians aiming at better results face several problems, in- cluding those regarding clinical, social, psychologi- cal and economic parameters. However. a reason- able starting point should be to improve the patient's knowledge about basic concepts concerning dia- betes and its therapy. The importance of improved knowledge is underlined by the correlation between test scores in diet-nutrition and some variables of diabetic control. The present study demonstrates that our system with piecemeal instruction is ineffi- cient. In an attempt to enhance the patients' under- standing concerning these matters, we have recent-
Table I V . Correlrrtions betuqeen the knowledge level of'disetrse, diet and nritrition rind \*cirioirs pirrcrmeters Spearman rank correlation coefficients
Group T (n=124)
Knowledge Knowledge of Knowledge Knowledge of of DM diet-nutrition of DM diet-nutrition
Group I ( n = 178)
Age of patients Duration of disease RBW Blood glucose Urinary glucose Serum cholesterol Serum triglycerides "Motivation"
-0.2767*** + 0.036 1 -0.0621 +0.0195 +0.1228 -0.1431 -0.0162 +0.0957
-0.35 l3*** - 0.0260
-0.0321
-0.0277 -0.0158
+O. I I55
+0.0640
+O. 1980*
-0.4185*** +0.1199 -0.2224*** -0.1382*
-0.1346 -0.2529**
+O. 1027
+0.0557
-0.4609*** -0.0190 -0.2252*** -0.1567* -0.0071 -0.1065 -0.25 I I** + 0.2808** *
* 1 ~ 0 . 0 5 . **p<O.Ol, ***p<O.001.
Patient ediicotion in ditrbetes mellitrrs 487
ly started a formal educational program integrated into the patient care system. The results of these efforts will be the subject of future publications.
APPENDIX Tlrr yr/estionnair.t~ I . Which c~ftlre~fblloii~ing alternritii~es is correct? Patients with DM have ( a ) too much sugar in blood and urine, ( b ) too little sugar in blood as the sugar is excreted in the urine. ( c ) no sugar in blood but plenty of sugar in the urine, ( d ) no sugar in blood or urine. Correct answer ( n ) .
2. What is the cairse of DM? ( a ) All organs are normal but the patient eats too much sugar. The pancreas pro- duces ( b ) too much insulin, ( c ) too little insulin. ( d ) The stomach produces too little gastric fluid. Correct answer (c) .
3. What is the reason for the increased prodrrction of [trine in patients ic’ith DM? ( a ) Sweat production is sub- normal. ( h ) The patient excretes sugar in the urine, which forces the kidneys to produce more urine. (c ) The patient is nervous and uses water as a sedative. ( d ) All patients with DM suffer from kidney disease associated with a high production of urine. Correct answer (6). 4. The patient nitlr DM has to test the urine regularly
%t,ith Clinitest to get i~formfrtion about: ( a ) the amount of salts in the urine, ( b ) the amount of sugar in the urine, (c) whether the urine is infected or not, ( d ) whether kidney disease is present or not. Correct answer ( b ) .
5 . What is carbohydrate? ( a ) All kinds of fat. ( b ) All types of nutrients that give rise to energy. (c) A type of nutrients that contain both sugar and fat. ( d ) Sugar and nutrients that can be transformed into sugar in the body. Correct answer ( d ) .
6. Which ofthe following nutrients contains significant a m ~ r r n t s ofprotein? ( a ) Oil, ( b ) syrup, ( c ) apple, ( d ) cod fish. Correct answer ( d ) .
7. Which of the ,following statements is correct:’ ( a ) The patient with DM is recommended to eat plenty of fat. which contains valuable amounts of energy but no sugar. ( b ) I t is unimportant whether the patient eats small or large amounts of fat. ( c ) The patient is recommended to avoid fat-rich diets. ( d ) The patient should eat no fat at all. Correct answer ( c ) .
8. Which of the ,following nutrients gives rise to the Iur.gc.st urnounts of energy? ( a ) Protein, (b ) fat, ( c ) car- bohydrate, ( d ) all these nutrients contain the same amounts of energy. Correct answer (b).
9. A patient with DM is recommended to plan his meals in thefollowing way. ( a ) He is not permitted to eat more than 3 meals per day. ( b ) He has to eat one heavy meal in the morning and one in the evening and only a light meal during the day. ( c ) He ought to have breakfast, lunch and dinner as well as 2-3 light meals in between. ( d ) It is not necessary to plan the meals according to a special system. Correct answer ( c ) .
10. Which of the following nutrients is so poor in energy content that it can be eaten without restriction? ( a ) Sugar- free cakes, ( b ) low-fat milk, (c) carrots, ( d ) cucumber. Correct answer ( d ) .
11. A glass of light beer ( 2 % alcohol) contains the same amounts of sugar as a glass of: ( a ) “sugar-free” lemonade, ( b ) light milk, (c) mineral water, ( d ) orange juice. Correct answer ( b ) .
12. How many dl of orange juice contain the same omortnt of energy as one fruit portion on the prescription l ist? ( a ) 1, ( b ) 2, (c) 3, ( d ) 4. Correct answer ( a ) .
13. Which of the following dishes can be recommended as ( I snuck? ( a ) A hot-dog, ( 6 ) coffee or tea with an unsweetened bun and a small apple, (c ) fruit cream with I dl low-fat milk, ( d ) a cake of sugar-free chocolate (dia- betes type). Correct answer ( b ) .
14. A patient with DM may be permitted to drink up to 4 dl low-fat milk per day. Which of the following statements is correct? ( a ) The patient has to drink the main part in the morning when the stomach is empty. ( b ) I t does not matter when or how the patient drinks these 4 dl milk. ( c ) The patient is permitted to drink only one glass of milk at a time and the recommended interval between each glass is several hours. ( d ) The patient is permitted to drink milk only together with lunch and dinner. Correct answer (c).
IS. Which qf the folloiting statements is correct? A patient with DM is permitted to drink unlimited amounts of ( a ) juice, ( b ) light beer, (c) “Pommac” (a lemonade). ( d ) none of these. Correct answer ( d ) .
16. Which of the following alternatives contains too mirch carbohydrate to be recommendable as a light mealfor a patient with DM? ( a ) A small apple, ( b ) a big banana, (c) a slice of crisp rye-bread with low-fat mar- garine, ( d ) a slice of white bread with low-fat cheese. Correct answer ( b ) .
17. Which of the following breakjkt meals is most irr- appropriate for a patient ii3ifh DM? Coffee or tea ( a ) + 2 glasses of juice + 2 slices of white bread + unsweetened marmalade, ( b ) + 1 glass juice + 2 slices of white bread with low-fat cheese, ( c )+ l glass light milk+2 slices of white bread with smoked meat, (d )+ 1 glass light milk+ 1 egg + a slice of white bread with brawn. Correct answer (a ) .
18. A patient with DM is recommended to use light milk instead of regular milk since light milk contains ( 0 ) less sugar, ( b ) more protein, ( c ) more calcium, ( d ) less fat. Correct answer (d ) .
11. Acid ( =ketones) in the urine means: ( a ) Urine con- tains blood. (6) Sugar metabolism is poorly controlled. ( c ) Urine contains bacteria. ( d ) Urine is normal. Correct answer ( b ) .
12. Insulin ought lo be injected s i ibc /~ t~rneuf is~~ ut: ( a ) the abdomen, ( b ) the outside of the upper arm. ( c ) the outside of the thigh, ( d ) anywhere. Correct answer ( c ) .
13. When is the most convenient time to inject the morning dose ofinsulin? ( a ) Half an hour before break- fast, ( b ) during breakfast, ( c ) directly after breakfast, ( d ) half an hour after breakfast. Correct answer ( a ) .
TI. The purpose of giving sulfonylrrrea tablets to adrrlt patients with DM is: ( a ) to administer insulin in tablets, ( b ) to administer a compound that stimulates the pancreas to produce more insulin, (c) to eliminate the need for dietary restrictions, ( d ) to administer a compound that reduces the blood level by stimulating a high excretion of sugar in the urine. Correct answer ( b ) .
T2. When is a patient Uith DM recommended to take
488 S.-G. K~iriutides et (11.
his toblets? ( a ) Not later than one hour before breakfast, ( b ) when having breakfast, (c ) half an hour after break- fast, ( d ) one hour after breakfast. Correct answer ( b ) .
REFERENCES 1. Beaser, S. B.: Teaching the diabetic patient. Diabetes
5: 146, 1956. 2. Burman, P. & Hellstrom, K.: Ambulant kostbehand-
ling av diabetiker. Chimar eller realitet? Lakartid- ningen 68: 4379, 1971.
3. Etzwiler, D. D.: Who's teaching the diabetic? Dia- betes 16: 1 1 1 , 1%7.
4. - The Minnesota experience. Presented at the ses- sion on Evaluation of Diabetes Education Programs, 20th Annual Postgraduate Course in Diabetes, Jan. 21, 1973.
5. Graber, A. L., Christman, B. G., Alogna, M. T. & Davidson, J. K.: Evaluation of diabetes patient-edu- cation programs. Diabetes 26: 61, 1977.
6. Karlander. S.-G., hinder , I . & Hellstrom. K.:
Metabolic control of diabetes mellitus during routine management at an out-patient department. Acta Med Scand 207: 475. 1980.
7. Lundbaek, K.: Long term diabetes. The clinical pic- ture in diabetes mellitus of 15-25 years duration with a follow-up of a regional series of cases. Munksgaard, Copenhagen 1953.
8. Phillips, M. G.: The nutrition knowledge of medical students. J Med Educ 46: 86. 1971.
9. Stone, D. B.: A study of the incidence and causes of poor control in patients with diabetes mellitus. Am J Med Sci 241:436. 1961.
10. Watkins, J . D., Williams, T. F., Martin, D. A., Hogan, M. D. & Anderson. E.: A study of diabetic patients at home. Am J Public Health 57: 452. 1967.
1 1 . Williams, T. F., Anderson. E.. Watkins, J . D. & Coyle, V.: Dietary errors made at home by patients with diabetes. J Am Diet Assoc 51: 19, 1967.
12. Williams, T. F., Martin, D. A , , Hogan. M. D., Wat- kins, J. D. & Ellis, E. V.: The clinical picture of diabetic control, studied in four settings. Am J Public Health 57: 441, 1967.







![Super Power of Antioxidant in Oxidative Stress and ... · (diabetic nephropathy), nerves (diabetic neuropathy), eyes (diabetic retinopathy) usually occur [5,6]. Diabetes Mellitus](https://img.pdfslide.net/doc/110x75/5f6fc8d141aef333fb46f152/super-power-of-antioxidant-in-oxidative-stress-and-diabetic-nephropathy-nerves.jpg)





















