-
INTRODUCTIONAcute infective conjunctivitis is a commonproblem in
the primary care setting,accounting for up to 1% of GP
consultationsin the UK.1,2 Standard treatment for acuteinfective
conjunctivitis has traditionally beenwith topical antibiotics.3
There was littleevidence from primary care on which tobase
treatment decisions until 2005, whenthree trials based on primary
carepopulations were published.46 These trialsconfirmed a high rate
of resolution inuntreated cases and a limited effect ofantibiotics
within the primary care setting.Subsequently, clinical guidelines
have beenupdated to limit the use of antibiotics.7 Inaddition, the
differentiation between a viraland bacterial cause is difficult on
clinicalgrounds, and it is generally impractical torequest and
await microbiology resultsbefore initiating treatment.8Since 2005,
GPs have responded to
evidence by reducing prescribing rates foracute infective
conjunctivitis, but over-the-counter availability of
chloramphenicol intheUKhas resulted in a 48% increase in theuse of
topical chloramphenicol.9 Reliableidentification of subgroups that
will benefitfrom antibiotics is important for guidingprescribing
practice in both primary careand pharmacies. Previous studies have
notbeen large enough for reliable subgroup
analysis. Individual patient data meta-analysis has been shown
to be an efficientmethod for subgroup analysis when only alimited
number of trials are available.10This study conducted a
meta-analysis
using individual patient data, with the aim ofassessing the
overall benefit of antibioticsas well as the benefit in different
subgroupsof patients with acute infective conjunctivitisin a
primary care setting.
METHODSelection of studiesThe Cochrane Central Register
ofControlled Trials (CENTRAL), Embase,MEDLINE, and PubMed were
searched forrandomised controlled trials up to andincluding April
2010. Methodological filterswere used for identifying
randomisedcontrolled trials (RCTs) in Embase11 andMEDLINE;12 no
other limits or filters wereused. The following search terms
wereused: (keyword conjunctivitis, bacterial) or(acute or infect*
or bacteria*) conjunctiv*)and (keyword anti-bacterial agents)
or(antibiotic*). Trialswereeligible for inclusionif they were
carried out within the primarycare setting and were
randomised,comparing antibiotic with placebo or notreatment.A total
of 332 potentially relevant trials
were identified; 325 of these were excluded
JM Jefferis, MA, BM, BCh, PGDipClinRes, NIHR,doctoral research
fellow in opthalmology,Newcastle University, Newcastle. RPerera,
MSc,DPhil, university lecturer in medical statistics;PWRose, FRCGP,
MD, university lecturer ingeneral practice, Department of Primary
HealthCare, University of Oxford, Oxford. PGlasziou, PhD,FRACGP,
MRCGP, professor of evidence-basedmedicine, Bond University,
Australia. HEveritt,BSc, MRCGP, MSc, PhD, clinical lecturer
ingeneral practice, Community Clinical Sciences(CCS) Division,
Faculty of Medicine, Health andBiological Sciences, Southampton
University,Southampton. H vanWeeert, MD, PhD, professorof general
practice and family medicine, AcademicMedical Centre, University of
Amsterdam;
RPRietveld, MD, PhD, GP, Amsterdam, theNetherlands.
Address for correspondenceRafael Perera, Division of Public
Health andPrimary Care, University of Oxford, Old RoadCampus,
Headington, Oxford, OX3 7LF.
E-mail:[email protected]: 20 January 2011;
Editors response:21 February 2011; final acceptance: 29March
2011.British Journal ofGeneralPracticeThis is the full-length
article (published online30 Aug 2011) of an abridged version
published inprint. Cite this article as: BrJGenPract 2011;
DOI:10.3399/bjgp11X593811.
Acute infective conjunctivitis inprimary care: who needs
antibiotics?An individual patient data meta-analysis
Joanna Jefferis, Rafael Perera, Hazel Everitt, Henk van Weert,
Remco Rietveld,Paul Glasziou and Peter Rose
Research
AbstractBackgroundAcute infective conjunctivitis is a
commonproblem in primary care, traditionally managedwith topical
antibiotics. A number of clinicaltrials have questioned the benefit
of topicalantibiotics for patients with acute
infectiveconjunctivitis.
AimTo determine the benefit of antibiotics for thetreatment of
acute infective conjunctivitis inprimary care and which subgroups
benefitmost.
DesignAn individual patient data meta-analysis.
MethodRelevant trials were identified and individualpatient data
gathered for meta-analysis andsubgroup analysis.
ResultsThree eligible trials were identified. Individualpatient
data were available from all primarycare trials and data were
available for analysisin 622 patients. Eighty per cent (246/308)
ofpatients who received antibiotics and 74%(233/314) of controls
were cured at day 7. Therewas a significant benefit of antibiotics
versuscontrol for cure at seven days in all casescombined (risk
difference 0.08, 95% confidenceinterval (CI) = 0.01 to 0.14).
Subgroups thatshowed a significant benefit from antibioticswere
patients with purulent discharge (riskdifference 0.09, 95% CI =
0.01 to 0.17) andpatients with mild severity of red eye
(riskdifference 0.10, 95% CI = 0.02 to 0.18), while thetype of
control used (placebo drops versusnothing) showed a statistically
significantinteraction (P = 0.03).
ConclusionAcute conjunctivitis seen in primary care can
bethought of as a self-limiting condition, withmost patients
getting better regardless ofantibiotic therapy. Patients with
purulentdischarge or a mild severity of red eye may havea small
benefit from antibiotics. Prescribingpractices need to be updated,
taking intoaccount these results.
Keywordsantibacterial agents; conjunctivitis; familypractice;
meta-analysis.
e542 British Journal ofGeneral Practice, September 2011
-
on review of titles and abstracts by twoindependent assessors;
seven wereretrieved for full text review, and whereclarification
was needed the authors werecontacted; three of these articles met
theinclusion criteria. Authors of individual trialswere contacted
and asked for their rawdata. The following data were
requestedfromeach trial investigator: outcomeonday7, culture
results, age, symptom diaries orGP records, presence of purulent
discharge,and severity of red eye.
OutcomemeasuresThe main outcome measure was cure atday 7.
Bacterial culture positivity atpresentation was used as a
secondaryoutcome measure to identify features thatpredicted
positive bacterial growth. Thereason for usingpositive bacterial
growth asa secondary outcomemeasure is that it hasbeen previously
shown that there is astronger treatment effect in patients with
apositive bacterial culture,4 and this is moreuseful in a clinical
setting where bacterialculture is rarely undertaken. Cure at day
7was defined as no remaining symptomsrecorded in patient diaries at
day 7 for trialsusing diaries, otherwise according to GPrecord on
day 7 stating complete resolutionof conjunctivitis.For trials using
diaries, patients with
missingdata at day 7were countedas curedat day 7 if their last
diary record showedthem as cured (equivalent to last valuecarried
forward). Analysis of diaries showedthat relapse rates after cure
were very low(
-
using the command xtlogit, with trial as theindexing variable to
account for differenceswithin trials. To explore the
potentialpredictors of a positive culture, diagnosticsummary
measures were calculated(sensitivity, specificity, positive
likelihoodratio, negative likelihood ratio, and the oddsratio [OR]
of the likelihood ratios) from thesimple frequency data (not
accounting fortrial differences). An adjusted OR wascalculated to
take account of trialdifferences, using a fixed-effect
conditionallogistic regression model similar to the oneused to
assess the effect interaction, but inthis case with a positive
culture as thedependent variable (outcome).
RESULTSThe search yielded three RCTs conductedin the primary
care setting.46 The data ofall three were available. The
studycharacteristics are shown in Table 1.For the trial by Rietveld
et al,4 data were
available for 163 of the 181 patients initiallyrandomised. For
the trial byRoseet al,5 datawere available for 317 of the 326
patientsinitially randomised. The aim of this meta-analysis was to
compare antibiotic therapyto placebo or no antibiotic therapy,
andtherefore the delayed antibiotic arm of thestudy by Everitt et
al (n = 109) was excludedfrom the meta-analysis.6 From theremaining
198 patients in the trial by Everittet al, data were available for
142. This givesa total number of 622 patients included inthis
meta-analysis.Combining data from all three trials, 80%
(246/308) of patients who receivedantibiotics and 74% (233/314)
of controlswere cured at day 7. The risk differencebetween
antibiotic and control groups was0.08 (95%CI = 0.01 to 0.14),
giving a numberneeded to treat of 13.Table 2 shows the effect of
antibiotics on
the number of patients cured at day 7 fordifferent subgroups.
The effect of using no
Table 1. Characteristics of principal trialsEveritt et al, 20066
Rietveld et al, 20054 Rose et al, 20055
Setting UK The Netherlands UKPrimary care Primary care Primary
care
Participants 307 adults and children 181 adults 326 children
aged 6 months to 12 yearsStudy design Open, factorial, randomised
Double-blind, randomised Double-blind, randomised
control trial placebo-controlled trial placebo-controlled
trialIntervention Immediate chloramphenicol eye Fusidic acid gel
versus placebo Chloramphenicol 0.5% versus placebo
drops versus delayed chloramphenicoleye drops versus no eye
drops
Determination of cure at day 7 Patient assessed cure as recorded
in GP assessed at day 7 Parent assessed cure as recorded ina daily
diary a daily diary
e544 British Journal ofGeneral Practice, September 2011
Table 2. Subgroup analysis for the outcome cured at day
7Antibiotic group, Control group,a P-value for
Numbers n/N n/N RD (95% CI) NNT RR (95% CI) interactionb
All cases 622 246/308 223/314 0.08 (0.01 to 0.14) 13 1.11 (1.02
to 1.21)Type of control 622Placebo 480 185/235 181/245 0.03 (0.04
to 0.11) 34 1.05 (0.95 to 1.15)Non-placebo 142 61/73 42/69 0.23
(0.08 to 037) 5 1.40 (1.13 to 1.73) 0.03Culture result 547Negative
255 92/127 89/128 0.02 (0.09 to 0.12) 50 1.02 (0.88 to
1.19)Positive 292 119/141 113/151 0.08 (0.01 to 0.17) 13 1.11 (0.99
to 1.24) 0.33Discharge 619Non-purulent 266 94/126 93/140 0.08 (0.03
to 0.19) 13 1.12 (0.96 to 1.31)Purulent 353 151/181 127/172 0.09
(0.01 to 0.17) 12 1.12 (1.00 to 1.25) 0.72Severity 599Mild redness
365 158/186 134/179 0.10 (0.02 to 0.18) 10 1.13 (1.02 to
1.25)Moderate or severe redness 234 77/110 77/124 0.06 (0.06 to
0.18) 17 1.10 (0.91 to 1.33) 0.40Age, years 384
-
placebo in the control group is compared tothe placebo control.
The subgroups thatsignificantly benefited from antibiotics
werethose with a purulent discharge and thosewith a mild severity
of red eye. The type ofcontrol used (placeboor nodrops)
showedastatistically significant interaction. The trialthat used no
placebo showed a significanteffect of antibiotics compared to
control(risk difference [RD] = 023, 95% CI = 0.08 to0.37), while
the combination of the two trialsthat used a placebo showed a
non-
significant effect of antibiotics compared tocontrol (RD = 003,
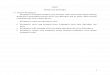
95% CI = 004 to 011).Figure 1 shows the RDs between antibioticand
no antibiotic group for cure at day 7 foreach subgroup. The level
of heterogeneityacross the trials is indicated in Figure 1 by
I2.Sensitivity analyses based on the
assumptions that all missing data were forpatients who were (a)
cured or (b) not curedshowed a reduction of effect in the
no-placebo group (Everitt et al trial only) whenmissing data were
treated as not cured (RD
British Journal ofGeneral Practice, September 2011 e545
Table 3. Predictors of a positive cultureOdds ratio
Culture Culture Sensitivity, Specificity, Unadjusted,
Adjusteda
positive, n/N negative, n/N % % LR+ LR LR+/LR (95% CI)Purulent
discharge 233/311 110/281 75 61 1.91 0.41 4.6 1.7
(1.08 to 2.58)Severity (moderate+) 100/295 131/277 34 53 0.72
1.25 0.6 1.4
(0.89 to 2.12)Age
-
= 0.14; 95% CI = 0 to 0.28). This is moreconsistent with the
null hypothesis than inthe primary analysis. The rest of the
resultswere robust to the choice of imputed valuesfor the missing
data.Table 3 shows the predictors of a positive
culture result at presentation. Specificityand sensitivity are
shown, as are the positiveandnegative likelihood ratios.
Thepredictivevalues of combined factors are also shown.
DISCUSSIONSummaryThe individual patient data meta-analysis
ofantibiotic use for acute conjunctivitis inprimary care shows that
there is a smalloverall significant effect of antibiotics
versuscontrol,with anumberneeded to treat of 13.However, most
patients recovered by day 7whether they received antibiotics or
not.Taking only the two trials that used aplacebo control, there
was no overallsignificant effect of antibiotics versuscontrol.
Patient subgroups identified asgaining a benefit from antibiotic
were thosewith purulent discharge andmild severity ofred eye.
Predictors of bacterial culturepositivity at presentation were
purulentdischarge and age less than 5 years.It was found that
patients with a mild
severity of red eye were more likely tobenefit from antibiotics
compared to thosewith a moderate or severe red eye. Thiscould be
because viral and allergic causesof conjunctivitis, as well as
alternativediagnoses such as episcleritis, may give amore
dramatically red eye.17 It may also bethat in patients with only
mild red eye, thediagnosis of acute conjunctivitis hingesmoreon
thepresenceofmorespecific signsand symptoms, such as purulent
discharge.Previous studies have described purulent
discharge as an indicator of a bacterialcause,1518 with the
presumption that thiswould help clinicians decide which
patientswould benefit from antibiotics. In this study,purulent
discharge did predict benefit fromantibiotics, and also predicted a
positivebacterial culture. However, bacterial culturepositivity was
not an indicator of benefitfrom antibiotics in this study. This
mayreflect the inaccuracy of cultures,particularly in the primary
care settingwhere transport times may confound theresults. It may
also be due to an insufficientsample size. However, in either case,
theeffect is likely to be small and the findingsdemonstrate that
even when the cause ofconjunctivitis is bacterial, most patients
willget better without the use of antibiotics.As well as cure rate
at day 7, which was
the main outcome measure in this study, it
is also important to know whetherantibiotics may shorten the
duration ofsymptoms. To address this, survivalanalyses were carried
out on the twodatasets using patient diaries. Results
wereconsistent with those reported in thismeta-analysis, with no
difference in recovery timefor the trial by Rose et al,5 but a
cleardifference in the trial by Everitt et al,6 whichused no
placebo.
Strengths and limitationsA key strength of this study is that
using theindividual patient data from three
trialsyielded622patients, giving thestudygreaterpower thananyof the
individual studies, andenabling subgroup analysis. There was alow
level of heterogeneity across thestudies, allowing the data to be
combined.However, there are also some limitations.The quality of
the three studies includedwas variable. All three studies detailed
theirrandomisation techniques. The trials byRose et al5 and
Rietveld et al4 were blindedand used adequate masking. In the Rose
etal trial,5 nine of the 326 patients were lostwith respect to
7-day follow-up. In theRietveld et al trial,4 18 of the 181
patientswere lost to follow-up. In the Everitt et altrial,6
therewere no data on cure at day 7 for56 of the 198 patients. It
should also benoted that a large number of patients (30%)in the
control arm of the Everitt et al trialwent on to receive
antibiotics.Two of the studies included in this meta-
analysis used a placebo in the control arm,while one did not.
Figure 1 shows asignificant effect of antibiotics versuscontrol in
the trial using no placebo, but notin the two trials using a
placebo. Thishighlights the need for using a placebo inrandomised
controlled drug trials, but alsosuggests that there could be a
hygiene orirrigation effect of putting non-antibioticdrops into the
eye. This is an interestingfinding and would be an area for
furtherresearch. Although a lack of evidenceprohibits clear
guidelines here, cleaning theeyes is a cheap and simple procedure
andcould be part of management advice givenby GPs.All the studies
here were carried out in
primary care populations. This thereforelimits the implications
of this study tounselected primary care populations.
Comparison with existing literatureA previous Cochrane Review of
the use ofantibiotics for conjunctivitis also showed ajust
significant benefit of antibioticsoverall.19 However, this review
includedstudies from secondary care as well as
e546 British Journal ofGeneral Practice, September 2011
FundingNo funding was received for this work.
ProvenanceFreely submitted; externally peer reviewed.
Competing interests
All authors have completed the UnifiedCompeting Interest form
atwww.icmje.org/coi_disclosure.pdf (availableon request from the
corresponding author)and declare that they have no conflicts
ofinterests that may be relevant to thesubmitted work.
Discuss this articleContribute and read comments aboutthis
article on the Discussion
Forum:http://www.rcgp.org.uk/bjgp-discuss
-
primary care and included some olderstudies that were not
thought to be of highquality. Three more-recent studies, notcarried
out in primary care, have shown asignificant effect of antibiotics
forconjunctivitis.2022 It is difficult to comparethe present
studies with these three recenttrials in secondary care, as their
focus wasmicrobiological rather than clinical. Allthree trials
confined their analyses toculture-positive patients, and
henceexcluded over half the randomised patients.The spectrum of
illness seen in secondarycare, and the focus onmicrobiological
cure,is likely to account for these differences.The small effect of
antibiotics in acute
conjunctivitis that has been shown here issimilar to that found
in systematic reviewslooking at sore throat and otitis
media.23,24
Recent evidence also suggests that the useof antibiotics for
acute otitis media mayincrease the recurrence rate.25
TheNationalInstitute for Health and Clinical Excellencehas drawn up
guidelines to limit the use ofantibiotics for self-limiting
respiratory tractinfections in primary care.26,27 In light of
thepresent findings, similar guidelines need to
be drawn up for the use of antibiotics inacute infective
conjunctivitis. These resultssupport the recent statement that it
was amistake to make chloramphenicol availableover the counter
because of the low efficacyof the drug in treating
conjunctivitis.28
Implications for practiceThis individual patient data
meta-analysisdemonstrates that topical antibiotics are
oflimitedbenefit in acute infective conjunctivitisand most patients
will get better withoutthem. There is a limited set of patients
whomay benefit from antibiotics, includingpatients with purulent
discharge andpatients with mild severity of red eye.However, even
in these groups the benefit ofantibiotics is limited. Judicious use
ofantibiotics is important to reduce the risks ofantibiotic
resistance in the population.Prescribing practices and
over-the-counterpolicies need to be updated to reflect
thesefindings. Furthermore, patient expectationsof antibiotic use
need to be addressed, asthey are likely to be a strong driving
forcebehind prescribing decisions.
British Journal ofGeneral Practice, September 2011 e547
-
e548 British Journal ofGeneral Practice, September 2011
REFERENCES1. Dart J. Eye disease at a community health centre.
BMJ 1986; 293(6560):
14771480.
2. McDonnell P. How do general practitioners manage eye disease
in thecommunity? Br J Ophthalmol 1988; 72(10): 733736.
3. Everitt H, Little P. How do GPs diagnose andmanage acute
infectiveconjunctivitis? A GP survey. Fam Pract 2002; 19(6):
658660.
4. Rietveld R, Riet G, Bindels P, et al. The treatment of acute
infectiousconjunctivitis with fusidic acid: a randomised controlled
trial. Br J Gen Pract2005; 55(521): 924930.
5. Rose P, Harnden A, Brueggemann A, et al. Chloramphenicol
treatment foracute infective conjunctivitis in children in primary
care: a randomiseddouble-blind placebo-controlled trial. Lancet
2005; 366(9479): 3743.
6. Everitt H, Little P, Smith P. A randomised controlled trial
of managementstrategies for acute infective conjunctivitis in
general practice. BMJ 2006;333(7563): 321324.
7. NICE. Clinical Knowledge Summaries. Clinical summary: acute
infectiveconjunctivitis. London: National Institute for Health and
Clinical
Excellence.http://cks.library.nhs.uk/conjunctivitis_infective/management/quick_answers/scenario_acute_infective_conjunctivitis#-304649
(accessed 3 May 2011).
8. Rietveld RP, ter Riet G, Bindels PJ, et al. Predicting
bacterial cause ininfectious conjunctivitis: cohort study on
informativeness of combinations ofsigns and symptoms. BMJ 2004;
329(7459): 206210.
9. Davis H, Mant D, Scott C, et al. Topical antibiotic use for
acute infectiveconjunctivitis:relative impact of clinical evidence
and over the counterprescribing. Br J Gen Pract 2009; 59(569):
897900.
10. Koopman L, van der Heijden GJ, Glasziou P, et al. A
systematic review ofanalytical methods used to study subgroups in
(individual patient data) meta-analyses. J Clin Epidemiol 2007;
60(10): 10021009.
11. Wong SS, Wilczynski NL, Haynes RB.Developing optimal search
strategies fordetecting clinically sound treatment studies in
EMBASE. J Med Libr Assoc2006; 94(1): 4147.
12. Higgins PT, Green S. Cochrane handbook for systematic
reviews ofinterventions. http://www.cochrane-handbook.org (accessed
3 May 2011).
13. Gigliotti F, WilliamsW, Hayden F, et al. Etiology of acute
conjunctivitis inchildren. J Paediatr 1981; 98(4): 531536.
14. Weiss A, Brinder J, Nazar-Stewart V. Acute conjunctivitis in
childhood.
J Paediatr 1993; 122(1): 1014.
15. Granet D. Allergic rhinoconjunctivitis and differential
diagnosis of the red eye.Allergy Asthma Proc 2008; 29(6):
565574.
16. BenEzra D. Current practice: diagnosis and treatment in
primary healthcare.Allergy 1995; 50(21 Suppl): 3033; discussion
3438.
17. Weber CM, Eichenbaum JW. Acute red eye. Differentiating
viral conjunctivitisfrom other, less common causes. Postgrad Med
1997; 101(5): 185186,189192, 195196.
18. Jackson WB. Differentiating conjunctivitis of diverse
origins. Surv Ophthalmol1993; 38(Suppl): 91104.
19 Sheikh A, Hurwitz B. Antibiotics versus placebo for acute
bacterialconjunctivitis. Cochrane Database Syst Rev 2006;
(2):CD001211.
20. Karpecki P, DePaolis M, Hunter JA, et al. Besifloxacin
ophthalmic suspension0.6% in patients with bacterial
conjunctivitis: a multicenter, prospective,randomized, double
masked, vehicle-controlled, 5-day efficacy and safetystudy. Clin
Ther 2009; 31(3): 514526.
21. Abelson MB, Heller W, Shapiro AM, et al. Clinical cure of
bacterialconjunctivitis with azithromycin 1%: vehicle-controlled,
double-maskedclinical trial. Am J Ophthalmol 2008; 145(6):
959965.
22. Tepedino ME, Heller WH, Unser DW, et al. Phase III efficacy
and safety studyof besifloxacin ophthalmic suspension 0.6% in the
treatment of bacterialconjunctivitis. Curr Med Res Opin 2009;
25(5): 11591169.
23. Glasziou PP, Del Mar CB, Sanders S, HayemM. Antibiotics for
acute otitismedia in children. Cochrane Database Syst Rev 2004;
(1):CD000219.
24. Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore
throat. CochraneDatabase Syst Rev 2006; (4):CD000023.
25. Bezakova N, Damoiseaux RA, Hoes AW, et al. Recurrence up to
3.5 yearsafter antibiotic treatment of acute otitis media in very
young Dutch children:survey of trial participants. BMJ 2009; 338:
b2525.
26. National Institute for Health and Clinical Excellence.
Prescribing of antibioticsfor self-limiting respiratory tract
infections in adults and children in primarycare. London: National
Institute for Health and Clinical Excellence,
2008.http://www.nice.org.uk/nicemedia/pdf/CG69FullGuideline.pdf
(accessed 3 May2011).
27. Butler C. Commentary: Controversies in NICE guidance on
antibioticprescribing for self limiting respiratory tract
infections in primary care. BMJ2008; 337: a656.
28. Scott G. Over the counter chloramphenicol eye drops. BMJ
2010; 340: c1016.