Embed Size (px)
DESCRIPTION
dee
Citation preview
Extrapyramidal syndrome(movement disorders)
Dr. Zuraini, Sp.S

2
Definition
Neurologic syndromes in which abnormal movement occur due to a disturbance of fluency and speed of voluntary movement or the presence of unintended extra movements

3
Ektrapyramidal System
• A GROUP STRUCTURAL OF “ Gray matter” wich located in “ hemispher cerebri” and mainly functional was motor activity
• CONSIST OF: Caudate nucleus
Putamen
Globus palidus
1.Basal Ganglia
2.Brain stem
3.Cortek serebri
4
Nucleus caudatus + Putamen
Corpus striatum (neostriatum)
Putamen + Globus palidus (nucleus lenticularis)

5
• Subthalmicus nuclei• Substantia Nigra• Parts of formatio reticularis
• Area 4 S• Area 6• Area 8
• BRAINSTEM
• CORTEKS CEREBRI
6
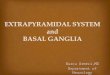
Ekstra Pyramidal Circuit
1. Cortex Striatum Globus pallidus Thalamus Cortex
2. Cortex Striatum Substantia nigra Striatum Cortex
3. Cortex Striatum Substantia nigra Thalamus Cortex
4. Cortex Globus pallidus Sub thalamic nuclei Thalamus Cortex

7
Pathogenesis 〈 1 〉• Results from dysfunction of the extrapyramidal system• Basal ganglion : caudate, putamen, globus pallidus,
subthalamic nucleus, and substantia nigra • motor area of cortex basal ganglion(organizing
movement commands) motor area of cortex # affects the size and speed of movements# selection of components of movements or the sequencing of
multi-step movements

8
Pathogenesis 〈 2 〉
9
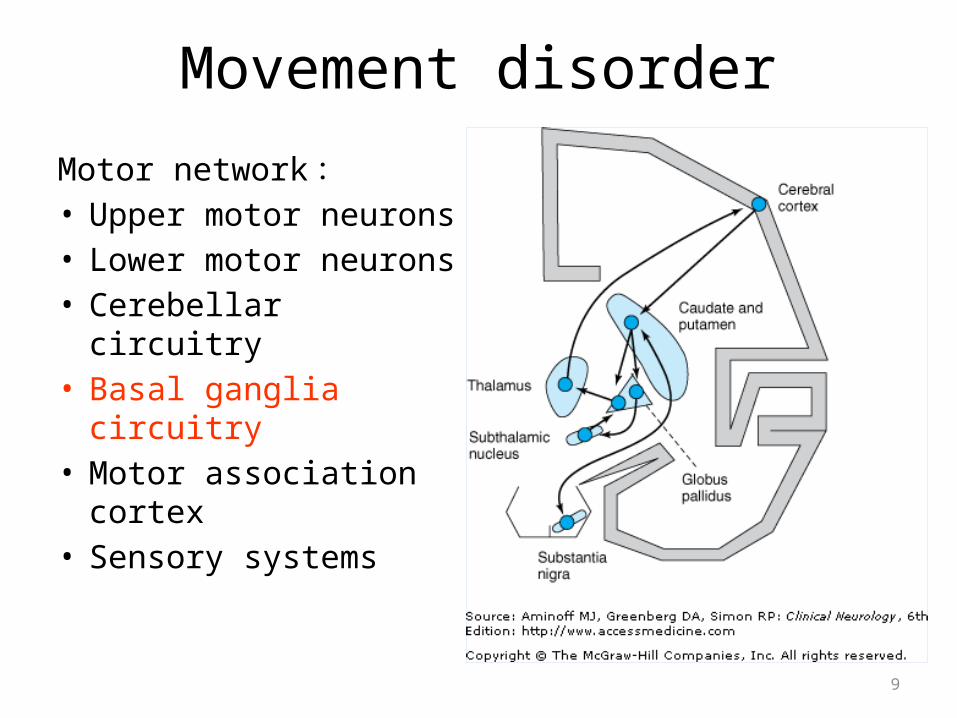
Movement disorder
Motor network :• Upper motor neurons• Lower motor neurons• Cerebellar circuitry• Basal ganglia circuitry• Motor association
cortex• Sensory systems

Thalamus
CortexGlobus pal
Caudatus+put
Subtthalamicusnuclei
PonsSubstantia
nigra
Serebellum
Nigro reticulo spinal tract Piramidal tract
1
3
2
Diagram of ekstrapyramidal circuit
striatum
4
10

11
THE MAIN FUNGTION OF EPS ASCOCIATED WITH
• Ascociative movement• Regulation of posture• Autonomic integration

12
EKSTRAPYRAMIDAL SISTEM DISTURBANCES
• Ektrapyramidal syndroma = Basal Ganglia syndroma
1.Primary functional deficit negative symptom
2.Secundary efect/ “release pheno mena positive symptom

13
EPS SYNDROMA
• Negative symptom
1. Bradikinesia 2. Disturbances posture
• Positive symptom
1.Involuntary movement tremor, athetosis, ballismus, chorea, dystonia
2. Rigiditas

14
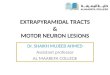
Types of hyperkinetic movement disorders
The differential diagnosis of chorea
Practical Neurology 2007;7;360-373
Slow,distal
dancelike

15
TREMOR A Rythmic Movement 3 to 5/Sec, resting, mainly in fingers, arms and chin

16
Chorea:Arrythmic movement of a forcible, rapid, jerky type, affecting the fingers, hand, and entire limb,or some other part of the body.
Chorea may be limited to one of the body (hemichorea). When the movements involve the proximal limb muscles and are unusualy violent and flinging Hemiballismus

17
Athetosis :Generally denotes abnormal movements that are slow, sinuous, irregular both in arm and fingers

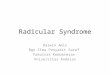
18
Dystonia:An abnormal contorted posture, classically in one or other of the extremes of athetoid movement, with a predilection for muscles of the trunk and limb girdle or a hand or a foot. Dystonia posture also occure without an accompanying athetosis.

19
Clinicopathologic correlation of Extrapyramidal
Symptom Location of lesion
Unilateral plastic rigidity with static tremor contralat subs nigra
Unilateral hemiballismus and hemichorea contralat subthal nucleus
of luysial
Chronic chorea of huntington type caudatus nuc & putamen
Athetosis and dystonia contralateral striatum
Cerebellar incord,”Intention tremor” and homolat cerebel hemisfher
Hypotonia or midle and inf cerebellar
peduncles

20
Drug-induced EPS
• EPS secondary to pharmacologic agents are the most common.
• The risk of developing a drug-induced EPS begins at the onset of treatment with an offending agent.
• Acutely: within hours or a few days• Subacutely: over several weeks• Late or delayed onset: six months or longer after
exposure(tardive) • short-term therapy of minimal therapeutic dosages
should be the strategy employed
21
Five classes of drugs are known to affect central dopaminergic systems
• Central stimulants : act as indirect dopamine agonist ex. Amphetamine
• Levodopa : a precursor of dopamine• Direct dopamine agonist : ex. Bromocriptine• Presynaptic dopamine antagonists : ex. Reserpine• Antagonize or block central dopamine receptors : neuroleptics, metoclopramide 〈 primperam 〉

22
Manifestation
• Acute dystonia• Parkinsonism• Akathisia• Tardive dyskinesia

23
Acute dystonia
Definition long-lasting contraction or spasm of musculature
generally less common than most other extrapyramidal symptomsyoung age and male sex predominantThe pathophysiological mechanism is presently unknown Diagnosis: The most common muscle groups affected are the eyes, jaw, tongue, and neck
trismus, blepharospasm, oculogyric crisis, torticollis, opisthotonus, laryngeal spasm 〈 most dangerous 〉
Treatment anticholinergic drug. Ex. Benztropine, diphenhydramine

24
ParkinsonismPathophysiology: blockade of postsynaptic dopamine(D2) receptors in the corpus striatumDiagnosis 〈 three cardinal symptoms 〉
TremorMuscle rigidityBradikinesia

25
Treatment• Lower dose of agent• Switching to a low potency agent• Anticholinergic drugs

26
Akathisia
Definition a sense of motor restlessness in which the patient feels a
constant need to move about.The most common type of EPSPathophysiology: unknownDiagnosis
• tend to have subjective complaints of ‘inner restlessness’ most often in legs
• They feel that they must move, and this manifests as frequent changes in posture, crossing and uncrossing of the legs…..
• Often associated with severe dysphoria, anxiety, and irritability

27
Treatment•Lower dose of agent•Switching to a low potency agent•Anticholinergic drugs•beta-adrenergic blockers•benzodiazepine

28
Tardive dyskinesia Definition
a syndrome of abnormal movements following at least six months and often many years of drug therapy
Pathophysiologydenervation-hypersensitivity phenomenonIt appears with prolonged receptor blockade, the receptors rebound, becoming supersensitized
DiagnosisCharacterized by involuntary movement of the lips, tongue, jaw, and extremities

29
Lipsmacking, facial and lingual masticatory movements, trunk rocking and restless foot movementsReduced by voluntary movements of the affected areasIncreased by voluntary movements of unaffected areasIncreased with emotional arousalAbsent when the individual is asleep

30
TreatmentThe best treatment is preventiongradual reductionLow dose of benzodiazepineDopamine antagonistDopamine depleting agents

31
Movement Disorders
• Parkinson’s Disease - Hypokinetic– Defined as a syndrome consisting of variable
combination of tremor, rigidity, bradykinesia, and characteristic disturbance of gait and posture
– Onset: mid-late life; mean age is 57 yrs
32
– Epidemiology: • Affects all ethnicities• has equal M/F distribution• occurs 1-2 per 1,000 people in general
population• occurs 1 per 100 people that are over 65 yrs• 4th most common disease in the elderly

33
– Cause: unknown– Pathophysiology:
1. Loss of dopaminergic cells in the substantia nigra • Dopamine’s normal function
2. Over excitation of the caudate & putamen3. Over excitation of the corticospinal tracts4. Decrease in thalamic excitation of the motor cortex

34
– Four Hallmark Signs• Resting Tremor (Pill-Rolling)• Rigidity• Bradykinesia• Flexed Posture with shuffling gait
(Festinating)
35
Movement Disorders
• Huntington’s Disease – Hyperkinetic– A neurodegenerative disorder which
predominately has behavioral, cognitive, or movement disorders signs
– Onset: Usually begins during adult life– Epidemiology:• 5-10 per 100,000 in the US• 50% chance to pass on the disorder• Anticipation• Paternal Descent

36
– Cause: Autosomal Dominant Disorder– Pathophysiology:• Mutation on chromosome 4• Uncertainty?

37
• Pathological Changes– Atrophy & neuronal
degeneration of cortex– Hallmark: caudate atrophy

38
– Examination:• Physical Findings– Initial Findings» Gradual onset» Slowed saccadic movements 1st sign» In 85% chorea is predominate movement
disorder

39
– Adult Onset» Prominent chorea» Bradykinesia» Postural reflex compromise
– Terminal Phase» Dysarthria, dysphagia, & respiratory
difficulties– General» Cognitive impairment» Depression» Psychiatric disorders

40
Movement Disorders
• Restless Legs Syndrome – Hyperkinetic– Common movement disorder– Diagnostic Criteria
– Desire to move limbs which is associated with unpleasant sensations
– Restlessness– Worsening of symptoms @ rest w/ temporary
relief w/ movement– Worsening of symptoms @ night

41
– Common Descriptions• Always unpleasant, but not necessarily painful• Need to move• Crawling• Tingling• Itching• Restless

42
CEREBELLUM
• Located in posterior fossa behind pons/med oblongata
• Consists of vermis on medial part and 2 hemispher, with 3 anatomical component
1.Flocculonodularis lob = archicerebellum2.Anterior lob = paleocerebelum3.Posterior lob = neocerebellum

43
Archicerebellum receive afferents fibre from vestibuer system maintain of equilibrium
Paleocerebellum receive aferents fibre from spinocerebellaris tract gait maintenance
Neocerebellum receive aferents fibre and send eferents fibre from/to motor cortek/vestibuler nuclei, basal ganglia and pons maintain postural tonus and modulation motor skill.

44
Pedunculus serebelliTree pairs, located on top and around forth ventricle, make the cerebellum attach to brain stem. Contain of tracts to and from brain stem
Pedunculus cerebelli inferior contain the fibre from med spin, low part of brain stem, nuclei/ vestibuler nerve

45
Pedunculus cerebelli medialis(fibre from pontin nuclei contra lateral)
Pedunculus cerebelli superior
(eferents fibre thalamus / med spinalis )

46
CEREBELLUM FUNCTION
• Regulation and control of muscle tone• Coordination of movement, mainly skill
movement • Control posture and gait

47
CEREBELLUM DYSFUNGTION
• Reduction muscle tone, mainly in acute lesion• Disturb of coordination voluntary movement
ataxia• Disturb of equilibrium and gait• Tremor that derives from ataxia and hipotonia

48
Because the efferent cerebellar pathwayTo the cerebral hemispheres are crossed
And the corticospinal system is againCrossed, a unilateral lesion of the Cerebellum causes an ipsilateral
Disorder of movement

49
• Hipotonia – Decreased of muscle resisten on palpation or
fasive movement (abnormality of activity gamma and alfa motor neuron)
• Disorders of coordination Ataxia– dismetria
– disdiadokinesia
– intention tremor
– Disarthria
– Dyssynergy

50
Dopamine Serotonin GABA Cholinergic
THANK YOU !