Embed Size (px)
Citation preview


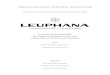
0 5 10 15 20 25 30 35
HCV Japan
HCV West
ICH
HBV end
HBV West
Alkohol
PBC
NASH
%
Kumulative 5-Jahresinzidenz bei Zirrhose
HCC?

HCC - Risiko
►HCV/HBV und HBV/HDV 2 – 6x►Hepatitis und Alkohol 2 – 4x gegenüber
Abstinenz
►Reduktion der HBV-Replikation►Reduktion der HCV-Replikation
Senkung des Risikos:

HCC und HCV
► Alter bei Dx wichtig► Alter bei Infektion wichtig► Männlich wichtig► Schwere der Lebererk wichtig► Phorphyrie wichtig► Eisen ?► Verfettung/DM wahrscheinlich► Genotyp ?► HCV load ?► HBV Koinfekt wichtig► Alkohol wichtig► Rauchen ?► Interferon ?


Häufigkeiten der Neoplasien
►80% duktales Pankreas-Karzinom►<10% periampulläres Karzinom►<10% Neuroendokrine Tumoren►<10% andere, z. B. zystische Neoplasien

Zystische Läsionen
►Häufig Zufallsbefunde – asymptomatisch
►Meist Pseudozysten►Inflammatorische od. infizierte Zysten, Abszess►Congenital: Selten►Echte zystische Neoplasien►Zystische Degeneration von soliden Neoplasien►Parapankreatische Läsionen

Zystische Neubildungen
Brugge et al. NEJM 2004, 351: 1281-26 Muzinöses Zystadenom Dietrich
IPMN

Intraductaler papillärer mucinöser Tumor (Neoplasie) IPMT
Pat. 60-70 Jahre, 32-39% der Läsionen, Prognose gut, wenn noch kein invasives Karzinom
Schmitz-Winnental et al. Curr Gastroenterol Reports 2003

Tumormarker im Zysteninhalt
Brugge et al. NEJM 2004, 351: 1281-26

Zusammenfassung
►Pankreas-Ca, periampulläres Ca, ►Zysten:
►Pseudozysten, zystische Neoplasien►Bildgebung:
►Sonographie (KM), EUS + FNA + Tx, ERCP + Tx, CT, MRT (one stop shop), SRS, FDG-PET, Laparoskopie
►Labor: Tumormarker►CA 19-9, CEA, Chromogranin A►Zysten: Amylase, CA 19-9, CEA, CA 72-4

Oberer Gastrointestinaltrakt► Ösophaguskrazinom: OP; Folgezustände► Magenkarzinom: OP; Folgezustände
Leber/Pankreas/Galle/NET► Pankreas: OP: Folgezustände
Unterer Gastrointestinaltrakt► Kolon-/Rektumkarzinom: Versorgungsqualität
Chirurgie

Pankreaskarzinom
Skizze (modifiziert) aus: Roder JD et al (2001) Maligne Tumoren des Pankreas und der periampullären Region. In: Siewert JR et al (Hrsg.) Praxis der Viszeralchirurgie - Onkologische Chirugie. Springer Berlin S. 502
VMS AORTA
Kaput65 %
Korpus15 %
Kauda10 %
Multifokal ca. 10 %
Periampulläres Caselten
Tumoren des exokrinen Pankreas
Maligne► Duktales Pankreas-Ca 85 %► Nichtduktales Pankreas-Ca 15 %
► ~ 13.000 Neuerkr./J. in D
Benigne ► Serös cystische Neoplasie (SCN)► Muzinös cystische Neoplasie (MCN)► Intraduktal papillär-muzinöse
Neoplasie (IPMN)

Pankreaskarzinom
Duktales Pankreaskarzinom
► > 70 % LK-Metastasen bei Diagnosestellung
► Bei Diagnosestellung nur < 30 % potentiell kurativ resektabel
► Prognose durch R0-Resektabilität bestimmt
► 5-J-ÜL-Rate < 5 % (alle Stadien)
► Trotz multimodalen Therapie-Optionen besteht nur bei vollständiger Tumorresektion eine gewisse Chance auf Heilung
Bildquelle: Becker HD et al (Hrsg) Chirurgische Onkologie. Thieme Stuttgart (2002) S. 356 u. Reißfelder C et al (2008) All. & Visz. Chir. 229 -48

Pankreaskarzinom Operationen 1
Papillen- und Pankreaskop-Ca:
1) Diener M (2007) A Systematic Review and Meta-analysis of Pylorus-preserving Versus Classical Pancreaticoduodenectomy for Surgical Treatment of Periampullary and Pancreatic Carcinoma. Ann Surg 245, 187-200
Bildquelle: Allg. & Visz. Chir. 6 (2008), 431 – 52 u. 4 (2008) 281 - 96
► Partielle Duodenopankreatektomie (Kausch-Whipple)
► Pyloruserhaltende partielle Duodenopankreatektomie (Traverso)
Onkologisch vergleichbar, Funktion besser aber: Magenentleerungsstörung 1)

Pankreaskarzinom Operationen 2
Pankreascorpus-/schwanz-Ca
► Pankreaslinksresektion (i. d. R. mit Splenektomie)
► (Minimal-invasive Operationstechnik)Bildquelle: Allg. & Visz. Chir. 6 (2008), 431 – 52 u. 4 (2008) 281 - 96

Pankreaskarzinom Folgen nach OP
Pylorus Belegzellen (Intrinsic factor)
Duodenal-Passage
Vagotomie Insulin/ exkr.Sekr.
Whipple + (+) + + +Traverso + + +Linksresektion +Folgen Dumping
(früh/spät)Vit B 12 Pancreocibale
AsynchronieMotilität/ Sekretion
BZ / Verdauung

Pankreaskarzinom Folgen nach OP
Perioperative Letalität < 3 – 5 %
Perioperative Morbidität: 30 %- Pankreasfistel 5 – 12 %- Galleleck 2 – 6 %- Magenentleerungsstörung (Traverso) ≥ 19 %- Diabetes mellitus
Funktionelle Folgen- Exokrine Pankreasinsuffizienz (ADEK-Vit)- Malnutrition/Maldigestion/Appetitlosigkeit- Nahrungsunverträglichkeit (Schmerz/Meteorismus)- Laktoseintoleranz verstärkt- Pancreocibale Asynchronie- ggf. Vitamin B12-Mangel- ggf. Dumpingsyndrom- Gewichtsverlust
Keim V et al (2009) Der pankreasoperierte Patient. Nachsorge, Diagnostik und Therapie. DÄB 106, 789–94

PankreasresektionFolgezustände - Empfehlungen
Delbrück H (2006) Rehabilitationsmaßnahmen in der Onkologie. Hilfen auf dem Weg zurück ins Leben. Im Focus Onkologie 6, 67 - 75
AK Supportive Maßnahmen in der Onkologie (ASO) der Deutschen Krebsgesellschaft (DKG) und der Multinational Association of Supportive Care in Cancer (MASCC) www.onkosupport.de

Test
Test
• 126 Pat mit Karnofsky-Index < 80
oder
• > 10mg Morphin tgl.
oder
• Schmerzscore ≥ 20
• clinical benefit response 23,8% (Gem) vs. 4,8% (5-FU) – p.0022
(Schmerz, Karnofsky-Index, Gewicht)
Burris HA et al, J Clin Oncol 15(6): 2403-13; 1997

Test
Test
Burris HA et al, J Clin Oncol 15(6): 2403-13; 1997

PankreaskarzinomKombination von Gemcitabine mit Erlotinib (Tarceva®)
Prognose abhängig vom rash
Moore MJ et al, J Clin Oncol 25; 1960-5; 2007
16%
9%
43%
mOS 6,24 vs. 5,91 Mo*
CBR 57,5 vs. 49,2%

PankreaskarzinomKombination von Gemcitabine oder Capecitabine mit ErlotinibPrognose abhängig vom rash
Boeck S.H. et al, Proc ASCO: #4011; 2010
mOS 6,9 vs. 6,6 Mo (ns)

Pankreaskarzinom- FolFIrinOx -
Conroy T et al, NEJM 364: 1817-28; 2011
RR 31 vs. 9,4%
PFS 6,4 vs. 3,3 Mo
OS 11,1 vs. 6,8 Mo
28%

Pankreaskarzinom- Radio-Chemotherapie -
Huguet F et al, J Clin Oncol 27; 2269-77; 2009
Huguet F et al, J Clin Oncol 25; 326-31; 2007
Overall survival: (21 Studien – 13PhIII, 6 Ph II, 2 Metaanalysen)
• RadioChemotherapie > best supportive care• RadioChemotherapie = Chemotherapie
Huguet F et al, J Clin Oncol 27; 2269-77; 2009

1-J.-Ü.:
65,3%
vs.
47,5%
Pankreaskarzinom- Radio-Chemotherapie -
Huguet F et al, J Clin Oncol 25; 326-31; 2007

Test
Pankreaskarzinom- Adjuvante Chemotherapie: Prognoseverbesserung -
Neoptolemus JP et al, NEJM 350: 1200-10; 2004Oettle H et al, JAMA 297; 267-77; 2007

Test
Test

CONKO-41st-line chemo +/- enoxaparin
FRAGEM-Studie1st-line chemo +/- dalteparin
VTE (first 3 months)
p<0.01
%
Riess ASCO 2009-2010; Pelzer ECCO-ESMO 2009 Maraveyas ECCO-ESMO 2009
%
0.00
4.00
6.00
8.00
10.00
2.00
Observation Enoxaparin
9.9 %
1.3 %
VTE profile
ControlLMWH
0
10
2025
35
5
RR=0.38p<0.02
RR=0.138p<0.002
RR=0.046p<0.001
RR=0.083p<0.028
AllOverall
<100D ClinicalVTE <100D
LethalVTE <100D
31
1218
9
25
3
15
30
Pankreaskarzinom- Niedermolekulares Heparin -
Prophylaxe mit LMWH begleitend zur Chemotherapie (mindestens 3 Monate) reduziert signifikant die Rate thromboembolischer Ereignisse(kein Einfluß aufs Überleben)

NET
WHO 2010
Update Gastrointestinale Tumoren 2011
Neue Nomenklatur
Neues Organspezifisches Stagingsystem
Neue Grading Klasssifikation

Update Gastrointestinale Tumoren 2011
US und europäische Inzidenz der NET

Update Gastrointestinale Tumoren 2011

Update Gastrointestinale Tumoren 2011

Update Gastrointestinale Tumoren 2011
Grading:im Wesentlichen nach dem Proliferationsindex
•G1:<2 Mitosen/10 HPF und/oder <= 2% Ki67 Index•G2:2-20 Mitosen/10 HPF und /oder 3-20% Ki67 Index•G3:>20 Mitosen/10 HPF und/oder >20% Ki67 Index
gezählt werden mind. 50HPF oder in der Immunhistologie 500-2000 Zellen nach Färbung mit Antikörper Mib1es werden Areale mit der stärksten Färbung(hot spots) gezählt

Update Gastrointestinale Tumoren 2011
Korrelation der WHO Klassifikation
und des Proliferationsindex
mit dem Überleben

Update Gastrointestinale Tumoren 2011

Update Gastrointestinale Tumoren 2011

Neuroendokrine Karzinome- Historische Chemotherapie -

Neuroendokrine Karzinome- Octreotid LAR -
Rinke A et al, J Clin Oncol 27: 4656-66; 2009

Neuroendokrine Pankreastumore- Sunitinib vs. Placebo -
Raymond E et al, NEJM 364(6): 501-13; 2011
PFS 11,4 vs. 5,8 Mo (p=s)

Neuroendokrine Pankreastumore- Everolimus vs. Placebo -
Yao JC. et al, NEJM 364(6): 514-23; 2011
CBR 73 vs. 51% (p=s)

Gastrointestinaler StromatumorGIST

GIST- Imatinib vs. Chemotherapie -

GIST- Imatinib – Response und Prognose -

Test
GIST- Imatinib adjuvant -

GIST- Imatinib adjuvant -

Test
Hepatozelluläres Karzinom - Sorafenib -
Llouvet J.M. et al, NEJM 359: 378-90; 2008
SHARP-Trial
2 x 400mg Sorafenib tgl. p.o. vs. Placebo
06/00 – 06/09
N = 602
Child A
44%
33%

Hepatozelluläres Karzinom - Sunitinib -

Test
Hepatozelluläres Karzinom - Progress nach Sorafenib -

Gallenwegskarzinome- lokal fortgeschritten/metastasiert -
Gemcitabine +/- cisplatin (ABC-02)
Die Ergänzung von cisPlatin zu Gemcitabine verbessert das Überleben ohne die Toxizität zu erhöhen --> neue Referenztherapie
PFS OS
n=410
Valle J. et al, NEJM 362: 1273-81; 2010
∆ 19%

Neuroendokrine Karzinome- Primärtumorlokalisation -

Neuroendokrine Karzinome- Epidemiologie -

Neuroendokrine Karzinome- Lokalisation und Prognose -

Hauttoxizität durchHer-1/EGFR targeted therapy

Metastasiertes Pankreas-Ca - Therapie vs Beobachtung -
*=p <.05
Med. Überleben mit BSC 3,6 Mo. (257 Pat. in 7 Studien)1-Jahres-Überleben 11% (126 Pat. in 4 Studien)
# Pat Med. Ü(Monate)
1-Jahres-Ü.
5-FuCyVcrMtx/5-Fu-Mito Maillison 1980 21 11* 35%
5-Fu/CCNU Frey 1981 65 3 ns
5-Fu/CCNU/VCR Andren-Sandberg 1983 25 5 ns
TamoxifenCyproteronacetat
Keating 1989 3732
5,254,25
20%12%
LHRHSomatostatinSomatostatin + LHRH
Huguler 1992433938
3,85,56
10%25%30%
FAM Palmer 1994 23 8,25 25%
ELF Glimelius 1996 29 6 25%*
Tempero MA, ASCO 2000

Test