Embed Size (px)
Citation preview

Lab on a Chip
COMMUNICATION
Cite this: DOI: 10.1039/c8lc00350e
Received 4th April 2018,Accepted 18th May 2018
DOI: 10.1039/c8lc00350e
rsc.li/loc
Label-free, high-throughput detection of P.falciparum infection in sphered erythrocytes withdigital holographic microscopy†
Matthias Ugele, *ab Markus Weniger,a Maria Leidenberger,b Yiwei Huang,a
Michael Bassler,c Oliver Friedrich,b Barbara Kappes,b
Oliver Haydenad and Lukas Richtera
Effective malaria treatment requires rapid and accurate diagnosis
of infecting species and actual parasitemia. Despite the recent
success of rapid tests, the analysis of thick and thin blood smears
remains the gold standard for routine malaria diagnosis in endemic
areas. For non-endemic regions, sample preparation and analysis
of blood smears are an issue due to low microscopy expertise and
few cases of imported malaria. Automation of microscopy results
could be beneficial to quickly confirm suspected infections in such
conditions. Here, we present a label-free, high-throughput
method for early malaria detection with the potential to reduce
inter-observer variation by reducing sample preparation and analy-
sis effort. We used differential digital holographic microscopy in
combination with two-dimensional hydrodynamic focusing for the
label-free detection of P. falciparum infection in sphered erythro-
cytes, with a parasitemia detection limit of 0.01%. Moreover, the
achieved differentiation of P. falciparum ring-, trophozoite- and
schizont life cycle stages in synchronized cultures demonstrates
the potential for future discrimination of even malaria species.
1. Introduction
With over 200 million new cases and more than 400000deaths per year,1 the treatment and elimination of malaria isstill one of the biggest global challenges of today, of whichover 99% of all infections are related to Plasmodiumfalciparum infections.1 For more than 100 years, the micro-scopic analysis of giemsa stained blood smears has been the
gold standard for the routine diagnosis of malaria.2 With adetection limit of 0.0002% parasitemia, thick blood smearsare highly sensitive but only used for the primary detection ofmalaria infections.3,4 Instead, thin blood smears allow thetreatment-relevant determination of malaria species and para-sitemia,4,5 but require time-consuming, accurate sample prep-aration and depend on inter-observer variation.6–8 Qualitativerapid diagnostic tests (RDTs), instead, do not require exten-sive sample preparation, provide detection limits comparableto microscopic thick smear analysis, and provide highly sensi-tive results within 20 minutes.9,10 However, the lack of quanti-tative parasitemia determination and the high costs per testare a significant limitation for diagnostics.10 Last, PCR hasproven to be a superior method for diagnosis of all species ofmalaria parasites and with a detection limit of 20 parasitesper ml clearly exceeds microscopic sensitivity.11–14 Unfortu-nately, time-consuming sample preparation and the requiredtechnical experience limit the application of PCR for routinediagnosis.9
Apart from these conventional methods, alternative label-free approaches for malaria detection and characterizationhave been explored with promising results. Park et al. andKim et al. describe the label-free differentiation of P.falciparum erythrocyte life cycle stages with refracting indexmaps gained by tomographic and diffraction phase micros-copy.15,16 In addition, Chandramohanadas et al. used tomo-graphic phase microscopy to examine the morphology ofinfected erythrocytes after treatment with the inhibitorsE64d, EGTA_AM and chymostatin by the analysis of three di-mensional refractive index distributions.17 Quantitative phasespectroscopy was used to detect a significant decrease inerythrocyte optical volume and hemoglobin mass associatedwith P. falciparum infection.18 Diez-Silva et al. analyzed therole of the parasite protein Pfl55/ring-infected erythocyte sur-face antigen (RESA) on membrane dynamics of P. falciparuminfected erythrocytes by diffraction phase microscopy.19
Moreover, static and dynamic light scattering maps of indi-vidual infected erythrocytes were used to identify and
Lab ChipThis journal is © The Royal Society of Chemistry 2018
a In-Vitro DX & Bioscience, Department of Strategy and Innovation, Siemens
Healthcare GmbH, Günther-Scharowsky-Str. 1, 91058 Erlangen, Germany.
E-mail: [email protected] Institute of Medical Biotechnology, Department of Chemical and Biological
Engineering, Friedrich-Alexander-University Erlangen-Nuremberg, Paul-Gordan-
Str. 3, 91052 Erlangen, Germanyc Analysesysteme und Sensorik, Fraunhofer ICT-IMM, Carl-Zeiss-Str. 18-20, 55129
Mainz, GermanydHeinz-Nixdorf-Chair of Biomedical Electronics, Department of Electrical and
Computer Engineering, TranslaTUM, Campus Klinikum rechts der Isar, Technical
University of Munich, Ismaningerstr. 22, 81675 Munich, Germany
† Electronic supplementary information (ESI) available. See DOI: 10.1039/c8lc00350e
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article OnlineView Journal

Lab Chip This journal is © The Royal Society of Chemistry 2018
distinguish intraerythrocytic P. falciparum life cycle stages.20
Most recently, high-throughput and label-free malaria detec-tion using erythrocyte deformability as a mechanical bio-marker was reported.21
Approaches based on digital holography in microscopeconfiguration (DH) showed a label-free visualization of ma-laria infected erythrocytes,22 the automatic identification ofmalaria-infected erythrocytes using correlation algorithms,23
and the automated detection of P. falciparum infection at thetrophozoite- and schizont stage using machine learning algo-rithms.24 To the best of our knowledge, a label-free micros-copy approach, which enables users to perform erythrocytelife cycle stage differentiation with malaria detection at thering stage, has not been reported so far. Ring stage sensitivityis a critical requirement for the diagnosis of the malaria spe-cies and for therapy monitoring.25 Here, we report an
imaging-based method for label-free, high-throughput earlymalaria detection with minimum sample preparation. Weused a differential digital holographic microscope and two-dimensional hydrodynamic focusing for parallelized detec-tion and differentiation of P. falciparum life cycle stages insphered erythrocytes. With an achieved detection limit of0.01% parasitemia, low sample preparation, and opportunityfor automated analysis, we demonstrate the potential impactof DH even for ring stage analysis.
2. Materials and methods2.1. Digital holographic microscopy
Digital holographic microscopy was performed with a cus-tomized differential holographic microscope provided byOvizio Imaging Systems, Belgium (Fig. 1a), which uses
Fig. 1 Optical and microfluidics setup for the detection of P. falciparum infection and differentiation of life cycle stages. (a) Differential DH setupfor high-throughput (105 fps) imaging of blood cells comprising a 528 nm SLED Koehler illumination and a 40×, NA 0.55 objective. A microfluidicsPMMA channel with four sheath flow inlets and one sample inlet was used for two-dimensional hydrodynamic focusing of sphered erythrocytes.(b) Schematics of the hydrodynamic focusing of sphered, P. falciparum-infected erythrocytes. The physical depth of field of ±2.3 μm in combina-tion with a sample flow height of 8 μm resulted in imaging of cell segments which passed the optical field in random positions. (c) P. falciparum in-fection induced a shift in the optical height variance over all life cycle stages in comparison to the negative control. (d) The variation in biconcavityclearly distinguished the trophozoite stage from ring- and schizont stage. The mean value with standard deviation of three samples is displayed. (e)The optical height variance decreased from ring- to schizont stage. The mean value with standard deviation of three samples is displayed. For anoverview of analyzed samples and gating strategy see Fig. S4.† NC, negative control; RS, ring stage; TS, trophozoite stage; SS, schizont stage.
Lab on a ChipCommunication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab ChipThis journal is © The Royal Society of Chemistry 2018
patented ‘double differential digital holographic micros-copy’.26 The microscope comprised a partially coherent trig-gered 528 nm Oslon PowerStar SLED (Osram) Koehler illumi-nation unit in transmission mode and a 40× NA 0.55 NikonCFI LWD 40× Cremove objective. By using a low-coherentlight source, the image degradation caused by the noise of acoherent laser is eliminated and the quality of the image isimproved.27–29 The setup consisted of a differential interfer-ometer of Mach–Zehnder interferometer type, which is lo-cated between the objective and the focusing means, to com-prise a first and a second interferometer arm correspondingto two different optical paths. The microscope is specificallyadapted to implement the phase stepping method30 in orderto extract the optical phase and the intensity informationfrom the interference pattern between the two beams. Theinterference patterns are then recorded by an imaging device.A detailed description of the microscopic setup and workingprinciple is described in ref. 26 and 31. The used light sourceand objective combination resulted in an optical depth offield of ±2.3 μm, which is the half width of the full depth offield range,32 and a lateral resolution of 0.6 μm (Rayleigh). APointGrey Grashopper GS3-U3-32S4 camera was used forhigh-throughput (105 fps, acquisition time 5 μs) imaging oferythrocytes. Reconstruction of phase images from recordedholograms was performed by Poisson integration using thecommercially OsOne software version 5.1 (Ovizio ImagingSystems, Belgium).
2.2. Microfluidics
Two-dimensional hydrodynamic focusing in a microfluidicsPMMA chip with a channel height of 50 μm, a width of 500μm, a total length of 5000 μm and five inlets (purchased fromFraunhofer ICT-IMM, Carl-Zeiss-Str. 18-20, 55129 Mainz, Ger-many) (Fig. 1a and S1†) was used for precise focusing and es-tablishment of a monolayer of sphered erythrocytes. The flowcell consisted of a bottom- and a top-flow inlet (lower/upperz-sheath), two side flow (x/y) inlets and a sample flow inlet.The fluids which entered the channel through the x/y flow in-lets flowed along the sides of the channels to avoid any con-tacts of the cells with the channel side walls. The fluidswhich entered the channel through the bottom and top inletsflowed along the bottom respectively top walls of the chan-nels and the sample fluid was sandwiched between these twoflows, which resulted in a single layer of focused cells.33 Toensure accurate and stable two-dimensional focusing, the vis-cosity of the sheath flow buffer was increased by the additionof 0.9% polyvinylpyrrolidone (PVP, average molecular weight1.3 MDa, Sigma-Aldrich) in autoMACS® Rinsing Solution(Miltenyi Biotec; PBS, 2 mM EDTA, pH 7.2).34 autoMACS®Rinsing Solution without any additives was used as sampleflow buffer. A neMESYS Base120 pump system with five mod-ules (cetoni GmbH) was equipped with 2.5 ml gas tight syrin-ges (VWR). A total flow rate of 0.398 μl s−1 with a sample flowrate of 0.024 μl s−1, an x/y-sheath flow rate of 0.037 μl s−1, anupper z-sheath flow rate of 0.1 μl s−1 and a lower z-sheath
flow rate of 0.2 μl s−1 was used. A six-port injection valve (V-451 Injection Valve Bulkhead 2 Position-6-Port .040 black,IDEX Health & Science) was used for in-flow sample injection.Microfluidics components (tubes, connections) were pur-chased from IDEX Health & Science.
2.3. Determination of sample stream height
The sample stream height at different sample flow conditionswas examined by determination of the gray value variationusing 0.1 M methylene blue in autoMACS® Rinsing Solution,as sample. Two-dimensional sheath flow conditionsremained constant, as described above, and the sample flowwas varied from 1 to 0 μl s−1 (1, 0.8, 0.6, 0.4, 0.2, 0.1, 0.08,0.06, 0.04, 0.02, 0.01, and 0 μl s−1). Light microscopy wasperformed using a Leica DM 2500M microscope equippedwith a Baumer HXG20 camera. The gray value for each sam-ple flow condition was quantified at three different positionsinside the channel using ImageJ. For each flow condition, atleast three measurements were performed. For the preferredsample flow of 0.024 μl s−1, a sample flow height of 8 μm wasmeasured (Fig. 1b and S2†). This method was preferably usedinstead of particle tracking35,36 or light scattering ap-proaches,37 which are highly applicable for analyzing the po-sition of objects in microfluidics flows but are unsuitable toabsolutely quantify the sample stream height in the presentmicrofluidics system used for two-dimensional focusing withmultiple sheath flows.
2.4. Data processing and analysis
The floating point phase shift pixel values for each recordedphase image within the interval [0,6] were converted tograyscales. On the resulting grayscale images, a backgroundimage was calculated by determining the pixel by pixel me-dian gray value from the first 11 images. This backgroundimage was subtracted from each phase grayscale image forbackground correction. For each corrected image, a binarypicture was generated by thresholding at the gray level of 28.Resulting holes in binary images were removed. As a singleimage in general contained more than one cell, all objectcontours were segmented out of the resulting images. After-wards, parameters for each object were calculated out of thesegmented contour, based on the phase values inside thecontour and based on a gray level co-occurrence matrix38 (fordetails of calculated parameters see Table S1†). The resultingsegmented object parameters were filtered to eliminate arte-facts and cells out of focus (see Fig. S3†). The following pa-rameter intervals were used to remove invalid segmentations:cell area >30, <12; aspect ratio >1.35; radius variance >1.5;optical height minimum <0.68; optical height mean <2.3;optical height maximum >6.4; sphericity <0.85 and homoge-neity >0.25. The gating strategies for detection of P.falciparum infection and determination of the detection limitwere developed using Kaluza® flow cytometry analysis, ver-sion 1.2 (Beckman Coulter).
Lab on a Chip Communication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab Chip This journal is © The Royal Society of Chemistry 2018
2.5. Parasite cultivation, synchronization and samplepreparation for DH
P. falciparum 3D7 parasites were cultured in type A-positive hu-man erythrocytes at a hematocrit of 5% in RPMI 1640supplemented with 25 mM HEPES, 0.1 mM hypoxanthine, 50μg ml−1 gentamycin and 0.5% albumax I. Cultures were incu-bated at 37 °C under controlled atmospheric conditions of 5%O2, 3% CO2, and 92% N2 at 95% relative humidity.39 Cultureswere synchronized by two sorbitol treatments as described inLeidenberger et al., 2017. In brief, the second synchronizationwas performed 11 h after the first. After the second synchroni-zation step, parasite cultures were subjected to an Easycoll gra-dient to separate ring stages from parasite debris.40 Ring-stageinfected erythrocytes were harvested and allowed to continuegrowth. To obtain ring stages, parasites were further grown for44 h; to gain trophozoites and schizonts, the cultures weregrown for 52 h and 58 h, respectively. For isovolumetric spher-ing41 (Fig. S2(c and d)†), 50 μl cultured erythrocytes were di-luted in 30 ml ADVIA® 120 RBC/PLT sphering buffer (0.035mM sodium dodecyl sulfate (SDS), 109.3 mM sodium chloride,0.11% glutaraldehyde, 4.03 mM Na2EDTA, 3.36 mM Na4EDTA;pH = 7.4; osmolality = 290 mosmol kg−1) followed by centrifuga-tion at 400g for 10 minutes. The cell pellet was resuspended in600 μl autoMACS® Rinsing Solution and used for DH micros-copy without any further labeling or staining.
Erythrocytes for reference measurements were collectedfrom healthy donors with informed consent and proceduresapproved by application 316_14B of the “Ethikkommissionder Universität Erlangen”. All experiments complied with therelevant laws and institutional guidelines of SiemensHealthcare GmbH, Germany.
2.6. Determination of P. falciparum infection detection limit
To determine the detection limit of DH, P. falciparum ringstage parasites were used and diluted to a parasitemia of 1,0.1, 0.01, 0.001 and 0.0001% at a hematocrit of 50% withnon-infected erythrocytes. The same non-infected erythro-cytes served as negative controls. In total, the determinationof the detection limit was repeated three times at differentdays with divergent erythrocyte cultures using different donorblood. For DH measurements, sphering of erythrocytes for 1,0.1, 0.01 and 0.001% parasitemia and negative control wasperformed as described above. Dilution accuracy was deter-mined by quantitative PCR (qPCR) (see Fig. S6†), adding 1 mlof the 1, 0.1, 0.01, 0.001 and 0.0001% dilutions as well as anegative control to 9 ml 0.1% glutaraldehyde in autoMACS®Rinsing Solution. DNA extraction was performed with 200 μlof the respective dilutions using a QIAamp DNA blood minikit (Qiagen GmbH, Hilden, Germany) according to the manu-facturer's recommendation. qPCR was performed accordingto Lee et al., 2002.42 Amplification and qPCR measurementswere carried out using the Agilent Mx3005P Real-Time PCRSystem. All analyses, including setting of the threshold andthe quantification of cycle values, were automaticallyestablished using the default settings.
3. Results and discussion3.1. Detection of P. falciparum infection and differentiationof life cycle stages
Sphering of erythrocytes was performed to decrease the proba-bility of imaging infected biconcave erythrocytes in an unfavor-able orientation, where the information about the internal par-asite structure is lost, as only a 4.6 μm section of the cells infocus was analyzed (Fig. 1b). The elimination of orientation ef-fects and the compensation of variabilities in the position ofthe erythrocytes in the microfluidics channel by two-dimensional hydrodynamic focusing, allowed a fast and label-free acquisition of cells without any efforts for continuousautofocusing. Also, the sphering of erythrocytes in hypoosmolarsolution represents an easy preparation step for point-of-careimplementation. In themicrofluidics channel, cells are expectedto have a random orientation,43,44 which could possibly exacer-bate a detection of an infection in sphered erythrocytes. Inter-estingly, it was observed, that even ring stage detection in dif-ferent cellular orientations was possible (see Fig. S4†) andtherefore it can be concluded, that the orientation of the celland thus the random position of parasites had no major influ-ence on the sensitivity with the chosen optical conditions.
First, synchronized P. falciparum infected erythrocytes atdifferent life cycle stages were analyzed to investigate the pos-sibility of label-free detection of infection at high parasitemia(>5%). Perfectly focused cells were segmented out of thereconstructed phase images and used for the calculation ofmorphological parameters (see Methods section 2.4. and Ta-ble S1†). The parameter ‘optical height variance’ (OHV), de-fined as the phase value variance inside the segmented con-tour, was identified as an indicator for P. falciparuminfection. For infected samples, a shift to higher OHV was ob-served over all life cycle stages in comparison to non-infectedcells (Fig. 1c). Additionally, a differentiation of P. falciparumlife cycle stages was achieved by analyzing the distribution ofcells in a biaxial scatter plot on ‘optical height variance’ and‘biconcavity’ (defined as the correlation of phase values on ahorizontal and vertical cut of the cell contour to an idealizedbiconcave cell), by four-quadrant gating (see Fig. S5†).Sphered cells commonly had a low value of the biconcavityparameter as they did not correlate with the biconcave pro-file. However, infected cells did not have a sphered shape inthe phase image and showed a better correlation with the bi-concave profile. Cells in the trophozoite stage revealed signif-icantly higher percentage of biconcavity in quadrant A thancells in the ring- and schizont stage (Fig. 1d and S5†). More-over, a significant decrease in the OHV from ring- to schizontstage in quadrant D allowed a clear differentiation of thering- from trophozoite- and schizont stage (Fig. 1e and S5†).A morphological comparison of life cycle stages revealed sig-nificant differences between the particular stages, which veri-fied the achieved differentiation. Furthermore, multiple/dou-ble P. falciparum infections were observed (Fig. 2).
These results show that label-free, in-flow detection of P.falciparum infection at the clinically relevant ring stage is
Lab on a ChipCommunication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab ChipThis journal is © The Royal Society of Chemistry 2018
achievable in sphered erythrocytes. Additionally, the resultsindicate, that the random orientation of the parasite insidethe sphered erythrocytes, most likely induced by cellular rota-tion in microfluidic channels, did not influence the detectionin the chosen experimental setup, as discussed above (seeFig. S4†). For that reason, also a detection of other malariaspecies (P. vivax, P. malariae, P. ovale and P. knowlesi) seemslikely, since (early) ring stages show similar structures to P.falciparum rings.45,46
For the rapid and proper treatment of malaria, an accuratedifferentiation of P. falciparum, P. vivax, P. malariae, P. ovaleand P. knowlesi is necessary. By conventional blood smearanalysis different ring-, trophozoite- and schizont stages canbe differentiated by morphological characteristics.4,46 Addi-tionally, the occurrence of multiple infections and the lack ofsequestrating stages in peripheral blood smears are charac-teristic for P. falciparum infections.45,47 With the shown dif-ferentiation of P. falciparum schizonts from ring and tropho-zoite stages, also a differentiation of P. vivax, P. malariae andP. ovale life cycle stages, which would allow a differentiationfrom P. falciparum in clinical samples, is likely. The possibledetection of multiple infections at the ring stage could serveas additional discrimination criteria from P. falciparum. It isalso conceivable that a differentiation of P. vivax, P. malariaeand P. ovale is achievable by recognition of significant mor-phological life stage characteristics. Since P. knowlesi infec-tions are difficult to discriminate from other malaria speciesby blood smear analysis,47,48 a potential discrimination fromother species by DH is questionable.
For the verification of this hypothesis clinical samples ofall malaria species are needed. In particular the effects in-duced by sphering of erythrocytes on the complex trophozoiteand schizont morphology, which could possibly exacerbatethe discrimination of the different species, should beaddressed by future work on the study of clinical malariasamples. The clinical relevant detection of species cross in-fection should also be examined. The primary focus of thiswork was to establish the technology and validate it in a de-fined pre-clinical setting. A full random clinical trial is cur-rently planned and subject to future study.
In contrast to morphological parameters used in thisstudy, quantitative phase imaging has been used to charac-terize cells in culture,49–52 erythrocytes53 and P. falciparum
infected erythrocytes15,16,23 by analyzing absolute physicalproperties, such as volume, thickness, refractive index anddry mass. For cell culture monitoring, where analysis time isuncritical, this approach is an accurate tool for precise char-acterization of cellular life cycle stages. The comparative anal-ysis of erythrocytes described by Rappaz et al. showed highconformity with reference methods but did not provide high-throughput capability. Park et al. and Kim et al. describe thelabel-free differentiation of P. falciparum erythrocyte life cyclestages with refracting index maps gained by tomographic anddiffraction phase microscopy. While these approaches pro-duce highly detailed refractive index maps, the computa-tional time is extensive and therefore not high-throughputcompatible. Anand et al. separated erythrocyte populationsbased on the thickness distribution of erythrocytes by the useof correlation algorithms, which resulted in reasonable accu-racies but did not provide sufficient discrimination to enableclinical applicability.
In this work solely morphological parameters were calcu-lated from reconstructed phase images to reduce computa-tional effort and enable high-throughput detection of P.falciparum infection with already clinically relevant detectionlimits. It could be shown, that morphological parameterswere sufficient to detect and discriminate P. falciparum lifecycle stages. Additionally, the characterization of absolutephysical cellular parameters, such as refractive index or drymass, may be of high relevance for cell culture monitoring,but redundant for simply differentiating malaria-infectedfrom non-infected erythrocytes. Furthermore, Park et al. haverecently shown high performance of machine learning algo-rithms for detection of P. falciparum infection beyond thering stage based on morphological parameters only.24 Conse-quently, the implementation of machine learning in the cur-rent setup will be performed in future studies to increase thereliability and performance of even ring-stage detection.
3.2. Determination of P. falciparum infection detection limit
For an accurate clinical valuation of malaria cases, not onlythe species but also the current parasitemia is highly rele-vant. Parasitemia serves as indicator for severity and progressof infections and determines the emergency of clinical treat-ment.5,25 In order to reveal the clinical usefulness of our ap-proach, the P. falciparum infection detection limit was deter-mined as described in the Methods section (see Methods2.6.). To ensure imaging of at least 100 infected cells, 30 000frames were acquired for 1%, 60 000 frames for 0.1% and300 000 frames for 0.01% parasitemia, with resulting mea-surement and analysis times of 5–60 minutes (see Table S2†).We also tried to analyze samples with 0.001% parasitemia,but the necessary acquisition of 107 cells was too time- anddata-consuming for the current experimental setup. Cultiva-tion and measurement procedures did not allow the parallelmeasurement of three replicates from one sample at one day.For that reason three samples with divergent erythrocyte cul-tures were measured at three different days. On the other
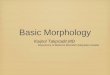
Fig. 2 Morphological analysis of P. falciparum life cycle stages. Toprow: reconstructed phase images of negative control (NC), ring stage(RS), double infection at the ring stage (DI), trophozoite (TS)- andschizont stage (SS). Bottom row: Corresponding height maps of toprow phase images. Scale bars are 5 μm.
Lab on a Chip Communication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab Chip This journal is © The Royal Society of Chemistry 2018
hand, this allowed the examination of inter-sample variationson the infection detection limit.
Again, the differences in OHV were examined, since thisparameter was previously identified as a sensitive indicatorfor P. falciparum infection (Fig. 1c). To ensure a detection ofinfection independent from sample variations, gate E was de-
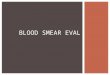
fined by overlaying OHV histograms of the negative controlsfrom day 1–3 (Fig. 3d). Then, the percentage distribution ingate E of negative controls and infected samples were exam-ined. As expected, samples with 1, 0.1 and 0.01% parasitemiaof all three days showed lower percentage in gate E in com-parison to negative controls, which corresponded with a shift
Fig. 3 Detection limit of P. falciparum infection. (a)–(c) Serial dilutions of P. falciparum ring-stage infected erythrocytes were measured at threedifferent days. In comparison to negative controls (NC), samples with 1, 0.1 and 0.01% parasitemia showed lower percentage in gate E, which cor-responds with a shift to higher optical height variance. Total cell numbers varied between individual measurements. (d) Gate E was defined byoverlaying optical height variance histograms of negative controls. Black, NC day 1; red, NC day 2; blue, NC day 3. (e)–(g) Overlaid histograms ofsamples measured at day 1 ((e)), day 2 ((f)) and day 3 ((g)).
Lab on a ChipCommunication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab ChipThis journal is © The Royal Society of Chemistry 2018
to higher optical height variance (Fig. 3 and S7(a)†). Surpris-ingly, the expected decrease in the OHV shift with lower para-sitemia was only observed for day 1 samples. For day 2, theOHV shift for 0.1 and 0.01% parasitemia was higher than for1% parasitemia. For day 3, the OHV shift for 0.01% para-sitemia was higher than for 0.1% parasitemia.
Most interestingly, an absolute determination of para-sitemia was not possible for all measured samples. Severalreasons for these observations are possible. For instance, sed-imentation in the microfluidics tubes, induced by the re-quired acquisition time, especially for 0.01% parasitemia, ledto varying cell numbers per frame, which made an absolutedetermination of parasitemia impossible and also explainsthe varying cell numbers per sample. Sedimentation couldalso lead to a loss of infected cells, especially at higher para-sitemia (1%), which could possibly explain the higher OHVshifts at lower parasitemia in day 2 and day 3 samples. Cellsout of focus could be another source of cell loss, which couldinfluence the OHV shifts. It was found that up to 10% of allremoved segmented objects were cells out of focus (Fig. S3†).Additionally, the sphering efficiency of the used ADVIA®RBC/PLT buffer was investigated. An average amount of 11%remaining biconcave erythrocytes was observed after dilutionin the sphering buffer, one sample showed even 17% bicon-cave cells (Table S3†). This sample dependence of erythrocytesphering did possibly contribute to the observed inconsis-tencies. Taken together, these observations could explain theunexpected OHV shifts for day 2 and day 3 samples. Never-theless, all infected samples clearly showed a higher OHVshift than all negative controls (Fig. 3 and S7(a)†), which con-firmed a sample-independent detection of infection down to0.01% parasitemia.
Finally, the parameters homogeneity, optical volume, ra-dius mean, entropy and energy of negative controls andinfected samples were compared to exclude interferences onnon-infected erythrocytes, induced by the different treatmentof added infected cells, which could possibly influence OHVdifferences (Fig. S7IJb)–(e)†). These parameters were chosen toevaluate the size, volume and inner consistency of segmentedcells independently from variances in the optical height. Itwas observed, that mean values were similar within the indi-vidual days and therefore, interferences due to the additionof infected erythrocytes appear unlikely. In contrast, varyingmean values were observed between the three measurementdays, as expected, since different erythrocyte cultures wereused for each day.
Overall, it was shown, that a parasitemia of 0.01% is de-tectable, which is clearly above the detection limits of thickblood film (0.0002% parasitemia3) and RDTs (down to0.0002% parasitemia9). Anyhow, our approach could contrib-ute to overcome the limitations of conventional diagnosistools. Blood smear analysis of thin films is cheap and sensi-tive, but requires time-consuming and error-prone samplepreparation and highly trained experts for accurate speciesand parasitemia determination,8 which is an issue in non-endemic regions with low microscopy expertise due to few
cases of imported malaria. RDTs are sensitive and easy to usebut mainly do not provide sufficient species differentiation,lack parasitemia determination and are relatively expensivecompared to blood smear analysis.8–10 PCR analysis is ultra-sensitive and high-throughput capable,14 but requires rela-tively complex sample preparation and time-consuming DNAamplification. In comparison, with the reduced sample prep-aration and evaluation effort provided by label-free DH basedmalaria diagnosis, a reliable, fast and user-independentworkflow for parasitemia and species determination withprice-competitive costs per test may be within reach.
Conclusions
We have successfully demonstrated label-free detection of P.falciparum infections in sphered erythrocytes using high-throughput, digital holographic microscopy and microfluidicfocusing of cells in a preclinical setting. Additionally, a differ-entiation of P. falciparum life cycle stages was achieved by an-alyzing cellular distributions of synchronized cultures. Theseresults show the potential for the differentiation of P. vivax,P. malariae and P. ovale from P. falciparum with minimumsample preparation. Beyond the distinction of M. tropica, adiscrimination of M. tertiana and M. quartana seems achiev-able. For this issue, the additional implementation of ma-chine learning algorithms24,54 provides a possibility to im-prove the separation efficiency if needed. Since the averageparasitemia of malaria patients is between 5000 parasites perμl (0.1% parasitemia) and 50 parasites per μl (0.001% para-sitemia),9 with a detection of 0.01% parasitemia (equivalentto 500 parasites per μl) obtained within one hour, the com-petitiveness of our DH based approach to clinical thin bloodsmear analysis was demonstrated. Although parasitemias be-low 0.01% could not be resolved with the existing experimen-tal setup, its optimization, e.g. by imaging with up to 1000fps combined with on-the-fly segmentation of cells to reduceoverall acquisition time and data size, is feasible and willcontribute to drastically reduce the detection limit and thusmay provide an opportunity for a reliable, fast and user-independent diagnosis of clinical malaria cases. Recent ad-vances in miniaturization and data analysis for high-throughput analysis without the need for accurate focus con-trol55 provide a further possibility for reducing the complexityof the current setup and improving the overall analysis time.Last, apart from detection of malaria infected cells, our label-free approach offers the potential to assist in the evaluationof potential therapeutics for anti-malarial treatment or moni-toring of treatment success,52 as well as blood transfusionquality control56,57 without the need for time-consumingsample preparation procedures.
Author contributions
O. H. conceived the original idea and devised the project. M.U., L. R., B. K., O. F., and O. H. designed the experiments. M.B. and L. R. designed the microfluidic device. M. B. assisted
Lab on a Chip Communication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab Chip This journal is © The Royal Society of Chemistry 2018
with the microfluidic experiments. M. U. conducted the ex-periments. L. R. assisted with the experiments. M. U., L. R.,M. W. and O. H. designed and conducted the data analysis.M. L. performed P. falciparum cultivation. Y. H. performedqPCR experiments. O. H., B. K. and O. F. supervised the re-search and experimental results. M. U. wrote the manuscript.All authors reviewed the experimental results andcommented on the manuscript.
Conflicts of interest
There are no conflicts to declare.
Acknowledgements
The authors thank Professor Thomas Junghanss from the‘Section Clinical Tropical Medicine’ of the Heidelberg Univer-sity Hospital for helpful advice and discussions regardingclinical issues and data interpretation.
References
1 World Health Organization, World Malaria Report 2017,2017.
2 J. J. Barcia, Int. J. Surg. Pathol., 2009, 292–296.3 L. J. Bruce-Chwatt, Lancet, 1984, 323, 751–808.4 D. C. Warhurst and J. E. Williams, J. Clin. Pathol., 1996, 49,
533–538.5 B. Gachot and P. Ringwald, Rev. Prat., 1998, 48, 273–278.6 K. Dunning and A. O. Safo, Biotech. Histochem., 2011, 86,
69–75.7 F. E. McKenzie, J. Sirichaisinthop, R. S. Miller, R. A. Gasser
and C. Wongsrichanalai, Am. J. Trop. Med. Hyg., 2003, 69,372–376.
8 O. E. Lema, J. Y. Carter, N. Nagelkerke, M. W. Wangai, P.Kitenge, S. M. Gikunda, P. A. Arube, C. G. Munafu, S. F.Materu, C. A. Adhiambo and H. K. Mukunza, Am. J. Trop.Med. Hyg., 1999, 60, 177–182.
9 A. Moody, Clin. Microbiol. Rev., 2002, 15, 66–78.10 C. Wongsrichanalai, M. J. Barcus, S. Muth, A. Sutamihardja
and W. H. Wernsdorfer, Am. J. Trop. Med. Hyg., 2007, 77,119–127.
11 J. Nam, Y. Shin, J. K. S. Tan, Y. B. Lim, C. T. Lim and S.Kim, Lab Chip, 2016, 16, 2086–2092.
12 S. Alemayehu, K. C. Feghali, J. Cowden, J. Komisar, C. F.Ockenhouse and E. Kamau, Malar. J., 2013, 12, 1–8.
13 C. C. Hermsen, D. S. Telgt, E. H. Linders, L. a. van de Locht,W. M. Eling, E. J. Mensink and R. W. Sauerwein, Mol.Biochem. Parasitol., 2001, 118, 247–251.
14 M. Imwong, S. Hanchana, B. Malleret, L. Rénia, N. P. J. Day,A. Dondorp, F. Nosten, G. Snounou and N. J. White, J. Clin.Microbiol., 2014, 52, 3303–3309.
15 Y. Park, M. Diez-Silva, G. Popescu, G. Lykotrafitis, W. Choi,M. S. Feld and S. Suresh, Proc. Natl. Acad. Sci. U. S. A.,2008, 105, 13730–13735.
16 K. Kim, H. Yoon, M. Diez-Silva, M. Dao, R. R. Dasari and Y.Park, J. Biomed. Opt., 2014, 19, 011005.
17 R. Chandramohanadas, Y. Park, L. Lui, A. Li, D. Quinn, K.Liew, M. Diez-Silva, Y. Sung, M. Dao, C. T. Lim, P. R. Preiserand S. Suresh, PLoS One, 2011, 6, 1–10.
18 M. T. Rinehart, H. S. Park, K. A. Walzer, J.-T. A. Chi and A.Wax, Sci. Rep., 2016, 6, 24461.
19 M. Diez-Silva, Y. Park, S. Huang, H. Bow, O. Mercereau-Puijalon, G. Deplaine, C. Lavazec, S. Perrot, S. Bonnefoy, M. S.Feld, J. Han, M. Dao and S. Suresh, Sci. Rep., 2012, 2, 1–7.
20 Y. Park, M. Diez-Silva, D. Fu, G. Popescu, W. Choi, I.Barman, S. Suresh and M. S. Feld, J. Biomed. Opt., 2010, 15,020506.
21 X. Yang, Z. Chen, J. Miao, L. Cui and W. Guan, Biosens.Bioelectron., 2017, 98, 408–414.
22 K. W. Seo, Y. R. Ha and S. J. Lee, Appl. Phys. Lett., 2014, 104,1–4.
23 A. Anand, V. K. Chhaniwal, N. R. Patel and B. Javidi, IEEEPhotonics J., 2012, 4, 1456–1464.
24 H. S. Park, M. T. Rinehart, K. A. Walzer, J. T. Ashley Chi andA. Wax, PLoS One, 2016, 11, 1–19.
25 K. Silamut and N. J. White, Trans. R. Soc. Trop. Med. Hyg.,1993, 87, 436–443.
26 F. Dubois and C. Yourassowsky, US Pat. 7,362.449B2, 2004,pp. 1–18.
27 F. Dubois, M. N. Requena, C. Minetti, O. Monnom and E.Istasse, Appl. Opt., 2004, 43, 1131–1139.
28 F. Dubois, C. Yourassowsky, O. Monnom, J.-C. Legros, O.Debeir, P. Van Ham, R. Kiss and C. Decaestecker, J. Biomed.Opt., 2006, 11, 1–5.
29 J. Dohet-Eraly, C. Yourassowsky, A. El Mallahi and F.Dubois, Opt. Lett., 2016, 41, 111–114.
30 T. Zhang and I. Yamaguchi, Opt. Lett., 1998, 23, 1221–1223.31 F. Dubois, L. Joannes and J. Legros, Appl. Opt., 1999, 38,
7085–7094.32 S.-H. Lu and H. Hua, Opt. Express, 2015, 23, 10714–10731.33 O. Hayden, L. Richter and M. Ugele, WO2017/045703A1,
2017, 1–31.34 R. C. Moore and A. Ferrante, US Pat., 2004/0070757A1, 2004,
1–6.35 L. Miccio, P. Memmolo, F. Merola, S. Fusco, V. Embrione, A.
Paciello, M. Ventre, P. A. Netti and P. Ferraro, Lab Chip,2014, 14, 1129–1134.
36 P. Memmolo, L. Miccio, M. Paturzo, G. Di Caprio, G.Coppola, P. A. Netti and P. Ferraro, Adv. Opt. Photonics,2015, 7, 713.
37 D. Dannhauser, D. Rossi, F. Causa, P. Memmolo, A. Finizio,T. Wriedt, J. Hellmers, Y. Eremin, P. Ferraro and P. A. Netti,Lab Chip, 2015, 15, 3278–3285.
38 R. M. Haralick, K. Shanmugam and I. Dinstein, IEEE Trans.Syst. Man. Cybern., 1973, SMC-3, 610–621.
39 C. Lambros and J. P. Vanderberg, J. Parasitol., 1979, 65, 418.40 M. Leidenberger, C. Voigtländer, N. Simon and B. Kappes, in
Methods in Molecular Biology, 2017, vol. 1601, pp. 97–110.41 Y. R. Kim and L. Ornstein, Cytometry, 1983, 3, 419–427.42 M. Lee, C. Tan, L. Aw, M. Singh, S. Lee, H. Chia, P. Eric, H.
Yap, C. Tang and E. P. H. Yap, J. Clin. Microbiol., 2002, 40,4343–4345.
Lab on a ChipCommunication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online

Lab ChipThis journal is © The Royal Society of Chemistry 2018
43 M. M. Villone, P. Memmolo, F. Merola, M. Mugnano, L.Miccio, P. L. Maffettone and P. Ferraro, Lab Chip, 2018, 18,126–131.
44 F. Merola, P. Memmolo, L. Miccio, R. Savoia, M. Mugnano,A. Fontana, G. D'Ippolito, A. Sardo, A. Iolascon, A. Gambaleand P. Ferraro, Light: Sci. Appl., 2017, 6, e16241.
45 M. Poostchi, K. Silamut, R. Maude, S. Jaeger and G. Thoma,Transl. Res., 2018, 1–20.
46 World Health Organization, in Basic Malaria microscopy Part1. Learner's guide, 2nd edn, 2010.
47 B. Singh and C. Daneshvar, Clin. Microbiol. Rev., 2013, 26,165–184.
48 J. Cox Singh, T. M. E. Davis, K. S. Lee, S. S. G. Shamsul, A.Matusop, S. Ratnam, H. A. Rahman, D. J. Conway and B.Singh, Clin. Infect. Dis., 2008, 46, 165–171.
49 P. Girshovitz and N. T. Shaked, Biomed. Opt. Express,2012, 3, 1757–1773.
50 B. Rappaz, P. Marquet, E. Cuche, Y. Emery, C. Depeursingeand P. J. Magistretti, Opt. Express, 2005, 13, 9361–9373.
51 L. Kastl, M. Isbach, D. Dirksen, J. Schnekenburger and B.Kemper, Cytometry, Part A, 2017, 91, 470–481.
52 D. Bettenworth, P. Lenz, P. Krausewitz, M. Brückner, S.Ketelhut, D. Domagk and B. Kemper, PLoS One, 2014, 9, 1–10.
53 B. Rappaz, A. Barbul, Y. Emery, R. Korenstein, C.Depeursinge, P. J. Magistretti and P. Marquet, Cytometry,Part A, 2008, 73, 895–903.
54 Y. Rivenson, Z. Göröcs, H. Günaydin, Y. Zhang, H. Wangand A. Ozcan, Optica, 2017, 4, 1437–1443.
55 B. Mandracchia, V. Bianco, Z. Wang, M. Mugnano, A.Bramanti, M. Paturzo and P. Ferraro, Lab Chip, 2017, 17,2831–2838.
56 A. D. Kitchen and P. L. Chiodini, Vox Sang., 2006, 90, 77–84.57 S. Abdullah and K. Karunamoorthi, Parasitol. Res.,
2016, 115, 35–47.
Lab on a Chip Communication
Publ
ishe
d on
22
May
201
8. D
ownl
oade
d by
Tec
hnic
al U
nive
rsity
of
Mun
ich
on 2
4/05
/201
8 13
:04:
27.
View Article Online