Embed Size (px)
Citation preview
What are ketones? Why should we measure β–OHB?
Ketone bodies are energy-rich molecules, derived from fat, Beta–OHB and AcAc are normally produced in a 1:1 ratio. which can be utilized by tissues during periods of glucose However, this ratio increases according to the redox potential deficiency. They are short-chain organic acids that can freely in the hepatic mitochondria. During DKA, the highly reduced move across cell membranes, even the bloodbrain barrier state of the mitochondria results in higher production of β–OHB (BBB). Therefore, ketones play a crucial role in providing and the ratio increases, sometimes to as high as 10:1. In the energy to the brain, which unlike other tissues cannot use fatty event of sudden insulin deficiency, blood levels of β–OHB acids. therefore increases rapidly, while the urinary excretion of AcAc
is not only decreased, but also delayed, as it is dependent on 4renal function and hydration status. During recovery, the At physiologic pH, these organic acids dissociate completely
redox potential changes and relatively more AcAc is produced and when present in large quantities, may lead to a metabolic and excreted.acidosis with high anion gap.
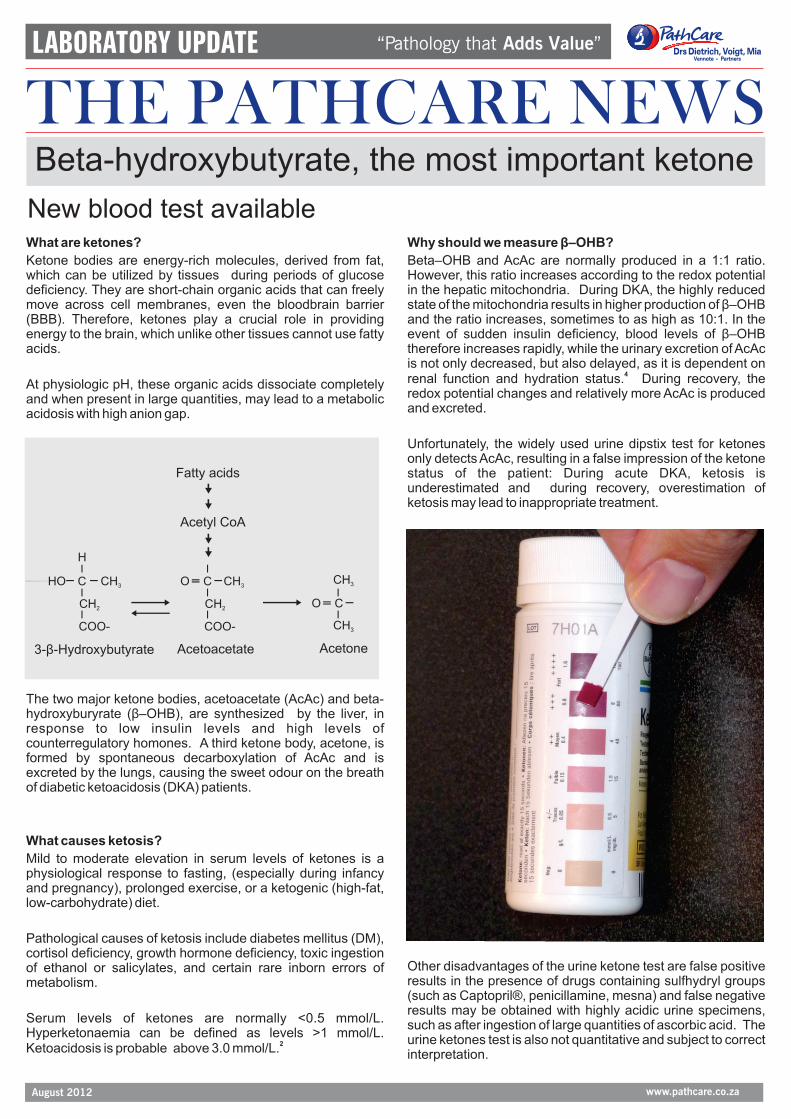
Unfortunately, the widely used urine dipstix test for ketones only detects AcAc, resulting in a false impression of the ketone status of the patient: During acute DKA, ketosis is underestimated and during recovery, overestimation of ketosis may lead to inappropriate treatment.
The two major ketone bodies, acetoacetate (AcAc) and beta-hydroxyburyrate (β–OHB), are synthesized by the liver, in response to low insulin levels and high levels of counterregulatory homones. A third ketone body, acetone, is formed by spontaneous decarboxylation of AcAc and is excreted by the lungs, causing the sweet odour on the breath of diabetic ketoacidosis (DKA) patients.
What causes ketosis?
Mild to moderate elevation in serum levels of ketones is a physiological response to fasting, (especially during infancy and pregnancy), prolonged exercise, or a ketogenic (high-fat, low-carbohydrate) diet.
Pathological causes of ketosis include diabetes mellitus (DM), cortisol deficiency, growth hormone deficiency, toxic ingestion
Other disadvantages of the urine ketone test are false positive of ethanol or salicylates, and certain rare inborn errors of results in the presence of drugs containing sulfhydryl groups metabolism.(such as Captopril®, penicillamine, mesna) and false negative results may be obtained with highly acidic urine specimens,
Serum levels of ketones are normally <0.5 mmol/L. such as after ingestion of large quantities of ascorbic acid. The
Hyperketonaemia can be defined as levels >1 mmol/L. urine ketones test is also not quantitative and subject to correct 2Ketoacidosis is probable above 3.0 mmol/L. interpretation.
“Pathology that Adds Value ” LABORATORY UPDATE
THE PATHCARE NEWS
www.pathcare.co.zaAugust 2012
Beta-hydroxybutyrate, the most important ketone
Acetone
CH3
CH3
H
HO C CH3
CH2
COO-
3- -Hydroxybutyrateβ
O C CH3
CH2
COO-
Acetoacetate
Acetyl CoA
Fatty acids
O C
New blood test available
Ketone measured
Assay type
Specimen
Dx & management
Interference
Blood ketones
β-OH-Butyrate
Quantitative
Blood
Correlates with course of disease
None
Urine ketones
Acetoacetate
Qualitative, operator dependent
Urine – may be difficult to obtain
May underestimate ketones in acute phase. May overestimate ketones during recovery.
False positives with sulfhydryl medications. False negatives with highly acidic urine
“Pathology that Adds Value ” LABORATORY UPDATE
THE PATHCARE NEWS
www.pathcare.co.zaAugust 2012
How can β–OHB be used? episodes, compared to ketonuria guidelines, especially in
children with Type 1 DM.
Criteria for diagnosing DKA include serum bicarbonate≤ 18 Specimen requirementsmmol/L, pH ≤ 7.3, anion gap >10 mmol/L, plasma glucose Laboratory assay:Serum (SST tube)
>13.9 mmol/L and the presence of ketonuria or ketonaemia. EDTA- or heparin plasma is also acceptable
However, these criteria have limitations, as the bicarbonate, P.O.C instrument:Capillary or venous whole blood
pH and anion gap may be affected by co-existing acid-base (EDTA- or heparin tube)
disturbances, e.g. chronic renal disease, respiratory disease,
vomiting, lactic acidosis.In summary:
Measurement of β–OHB, on the other hand, directly reflects
the rate of ketone body production, which is accompanied by 1an equimolar production of hydrogen ions.
A β–OHB level of ≥3 mmol/L predicts the presence of DKA with
a likelihood ratio of 15. In contrast, the best predictive value 3with urine dipstix of 3+ ketones, is a likelihood ratio of 6.
βOHB levels correlate better with the changes in acid-base
status during the course of treatment for DKA. It was found
that when insulin therapy adjustment was based on β–OHB
instead of glucose levels, the resolution of ketosis occurred 14 2hours earlier. References:
1.Sheikh-Ali, M. Diabetes Care 2008; 31(4):643-647
2.Laffel, L. Diabetes Metab Res Rev 1999; 15:412-426
3.Meas, T. Diabetes Metab 2005;31:299-303An instrument is also available for measurement of capillary 4.Taboulet, P. Diabetes & Metabolism 2007; (33):135-139(finger-prick) blood β–OHB, which can be used by patients at
home. Monitoring β–OHB, with adequate supplemental Compiled by Dr Esmé Hitchcock, Chemical Pathologist,insulin, may reduce or even prevent the occurrence of DKA PathCare Cape Town
Diagnosis and treatment of DKA:
Home-monitoring:
A new blood test is now available for quantitative measurement of β–OBH





























