Embed Size (px)
Citation preview

1
Labour & Coping Mechanism’s
Table of contents
Labour………………………………………………………………..2
What is labour? ……………………………………………….2
Signs and symptoms…………………………………………..3
How long is labour?...................................................................7
Fetal monitoring in labour …………………………………….8
Pain relief options…………………………………………………….9
Active birth ………...…………………………………………10
TENS …………………………………………………………16
Entonox………………………………………………………..17
Pethidine………………………………………………………17
Epidural……………………………………………………….18
Alternative pain relief options……………………………………….21

2
LABOUR
You turn up pregnant, you leave with a baby……..
But what really happens in between is the bit we’re all excited about!
It’s been 40 weeks of magic and you are on the home stretch. With your
due date approaching you should ensure that you are informed about
what will happen during labour and birth
Recent years has seen an increase in the number of women requesting a more natural
birth. In response, hospital midwives working in busy labour wards have modified
their practices in order to make the birthing process less medical and clinical. Hence
some outdated practices have been replaced. Women are now encouraged to be active
in labour and deliver in whatever position they choose. In Cavan we have a
Midwifery Led Unit which really adapts this approach while maintaining the highest
of safety standards.
What is labour really like & how do you know it has started?
Everyone’s labour is different, and pinpointing when it begins is not always clear. It’s
more of a process than a single event, when a number of changes in your body work
together to help you give birth. Most people will tell you that you’ll just know! Not
much help if you haven’t been through it before. I know it’s easier said than done, but
it’s important to stay calm during labour and have confidence in your body. Research
shows that a positive mindset can lead to a positive outcome. Familiarising yourself
with the signs & symptoms of labour will help clear up any confusion you may have!
Labour has three stages;
• First stage; when the neck of the womb (cervix) opens to 10 centimetres.
1. Latent Phase (early labour, 0-3cms)
2. Active Phase (established labour, 3-10cms)
• Second stage; when the baby moves down through the vagina and is born.
• Third stage; when the afterbirth (placenta) is delivered.
Labour is a journey, every woman’s labour is different!
Before labour starts, the neck of the womb is long, firm and closed. During the latent
(early) phase, the muscles of the uterus (womb) contract and make the cervix become
flat and soft, at the same time opening it to approximately 3-4cm. This flattening is
called ‘cervical effacement’ or thinning.
The latent phase can last several days or weeks before ‘active’ labour starts. Some
women can feel backache or cramps during this phase. Some women have bouts of
contractions lasting a few hours which then stop and start up again the next day. This
is normal.
Remember – the ‘latent phase’ of labour can last a very long time,
especially for first time mothers. Your body knows how to give birth.
When you understand what helps or hinders the natural process you
can create the right environment around you.

3
Signs and Symptoms of Labour
Pre labour signs; Although the following may indicate that labour is not far off, they are not actually
part of the labour process.
• Braxton Hicks contractions are random practice contractions that occur at
various times throughout pregnancy. They are typically not painful and do not
dilate the cervix as real contractions do. If you have been experiencing
Braxton Hicks contractions these may become stronger in your last month.
Braxton Hicks contractions seldom continue regularly for more than 60
minutes.
• You may be aware of your baby’s head pressing down.
• You may have a bout of diarrhoea and some women also feel nauseated.
• Some women may experience a burst of energy a day or two before they go
into labour.
Classic labour signs; A SHOW;
• A ‘show’ is a white/pinkish/red mucus discharge which comes from the
cervical canal (neck of the womb).
• As the cervix begins to soften and open, the mucus which has been protecting
the entrance to your womb comes away.
• Many women experience a ‘show’.
• Having a ‘show’ means that your body is starting to get ready for labour – but
the actual birth is likely to be some time away.
• Some women have a ‘show’, several days before labour starts.
• If you have an internal examination, you may have a ‘show’ afterwards.
• You do not need to contact the hospital but await events.
WATERS BREAKING;
• During pregnancy, your baby is surrounded by amniotic fluid – the
‘waters’. For some women, the first sign that labour is going to start is
that the waters begin to leak.
• The water leaking/breaking is when the bag of fluid around the baby
breaks and the waters leak.
• There may be a gush of fluid or a slow trickle.
• This may happen before or during labour.
• The fluid is normally a clear colour.
But it can also be;
• Green (Meconium) – the baby has recently had a bowel motion.
• Pink/red (Blood stained) – there is some blood present.
• It is quite common for women to leak a small amount of urine at the end
of pregnancy and it can be difficult to tell if your waters have broken or if
it is urine. If you think your waters have broken, put a sanitary pad on and
lie/sit down and if it is wet/damp after 1 hour, your waters have possibly
broken.

4
• Approximately 80% of women will go into labour spontaneously
following their waters breaking.
• You need to make contact with the maternity unit if you think your waters
have broken and come in for assessment.
If there is any bright red bleeding, like that of a period, or greenish
fluid, you should contact the Maternity Unit, 049 4376613.
CONTRACTIONS can be;
• Regular tightening followed by relaxation of the womb.
• Occurring every 5-10 minutes, increasing in strength and duration.
• Aching in the back, moving around to the front lower abdomen.
• Backache that comes and goes in a regular pattern.
• Pains that feel like strong period pains.
In the latent phase of labour, contractions may start and stop. This is normal.
Contractions may continue for several hours but not become longer and stronger.
They stay at about 30-40 seconds. This too is normal.
Remember – a ‘start-stop’ pattern of contractions is common in the
latent phase
In the active phase, contractions should continue until the baby is born. When you are
having regular contractions, which are getting Longer, Stronger & Closer Together,
you are in the active part of labour. The midwife may also describe the active phase as
‘established labour’. It is not possible to say when active labour will begin. It could
start in a couple of hours or in several days, so try and stay as relaxed as you can and
distract yourself from focussing only on the contractions. Even though you’ll be
desperate to get to hospital and finally meet your baby, you’ll be much more
comfortable staying at home unless there is a medical reason to go in, especially as
first labours then to last 12-16 hours (plus some!). There is evidence to suggest that
the further on in labour you are when you come in to hospital, the more likely you are
to have a normal birth.
There are things you can do to help yourself, such as;
• Pottering around the house
• Taking a walk • Watching a DVD/video
• Taking a warm bath or shower
• Having a nap
• Doing some relaxation
• Keeping your breathing quiet and fluid – ‘breath in gently, sigh out slowly’
• Trying massage – ask your partner or labour supporter to do this for you
• Putting a heat pack on any areas that ache – your lower back, your tummy
(under the bump) or between your thighs. Wrap it in a small towel first
• Keeping as mobile as you can, while remembering to save your energy for the
active part of labour

5
• Try out different positions and using a birthing ball to experiment with what
helps
• Drinking plenty of fluids – water, sports (isotonic) drinks, apple juice are all
good
• Eating little and often – carbohydrates (bread, pasta, rice, cereal) for slow –
release energy plus sugary foods for quick-release energy
• You may find it helps to make love – kissing, cuddling and having an orgasm
all cause your body to produce oxytocin. This is the hormone which is also
produced in labour and which makes the uterus contract.
Experiment with positions that you find comfortable. Stay upright and mobile as there
are advantages to staying off the bed and keeping upright in labour, gravity helps your
baby move down through the birth canal. This can mean standing, sitting, squatting,
kneeling and walking around. You may find a birthing ball, a floor mat and a beanbag
useful at this stage.
Some women choose to have the support of more than one person. Your birth
supporters can encourage and reassure you and help to tell your midwife what you
would like.
Partners can help with things such as:
• Massage
• Keeping you active
• Getting you drinks
• Praising and encouraging you
• Giving you cuddles
• Keeping you company and even trying to make you laugh!
MOST IMPORTANTLY
Your birthing supporter/partner should be someone who you can be
totally relaxed and comfortable with.
Remember that you help your labour to carry on smoothly by avoiding stimulating the
‘rational’ part of the brain. You need peace, quiet and a feeling of safety to help you
relax and so increase the levels of your own natural pain relievers – ‘endorphins’.
During labour you can take measures such as avoiding:
• Bright lights
• People asking you questions which you have to think to answer
• People talking to you during contractions
• Feeling as if people are watching or judging you
By having privacy, quiet, being in a darkened room and feeling safe, your ‘rational’
brain can be less stimulated and can allow your body to help you to begin your labour.
Listening to music you have chosen can also help.

6
Remember – labour is a journey, and the early part of 1st stage
can take a long time. This is normal.
Quick labours are not always the easiest to cope with!
When you are having regular painful contractions (1 every 5 minutes, lasting 40-50
seconds), need pain relief and/or support you can come to the hospital. It is a good
idea to telephone the hospital when you think you may be in labour, the midwives are
always available to offer support and advice, which in turn will give you a better more
positive experience.
Useful telephone numbers;
• Hospital Reception; 049 4361399
• Early Pregnancy Unit; 049 4376060 • Out-patient Clinic Appointments; 049 4376911/6133/6130
• Dr Hussain’s secretary; 049 4376130
• Dr Aziz’z secretary; 049 4376133
• Dr Syeds secretary; 049 4376911
• Dr Essajee’s secretary; 047 4338844
• Cavan Maternity Unit, 049 4376613 • Cavan Labour Ward, 049 4376612
• Midwifery Led Unit, 049 4376059/ 087 9799385
• Special Care Baby Unit; 049 4376323
• Breastfeeding Specialist; 049 4376864
• Parentcraft Co-ordinator; 049 4376541

7
How Long Is Labour?
FIRST
STAGE
Latent
Phase
EARLY
LABOUR
(0-4cm.)
ACCELERATED
LABOUR
(4-8cm.)
TRANSITION
(8-10cm.)
SECOND
STAGE
(10cm-birth)
THIRD
STAGE
Delivery of
the placenta
Thinning
and
opening of
the cervix.
Not
necessarily
painful.
3-5 days.
Contractions
5-30 mins
apart
15-40 secs
long
Mild – feel
like cramps
and back
pain.
4-8 hours
Contractions
2-3 mins apart
45-60 secs long
Stronger and more
intense
4-6 hours
Contractions
1.5-3 mins apart
45-90 secs long
The strongest
ones
2-3 hours
Contractions
3-5 mins apart
45-70 secs
long
More aware
of urge to
push and
fullness in
vagina and
bowel as baby
moves down.
2-3 hours
A feeling of
fullness and
cramping as the
placenta
separates
A time to hold
and enjoy your
baby!
15min-1hour

8
Listening to your baby’s heartbeat during labour
You will be offered an electronic tracing of your baby’s heartbeat for 20 minutes
when you arrive for admission to the maternity unit.
What are we checking for?
We are monitoring your baby’s heartbeat, movements and your contractions. During
contractions the blood flow to the placenta is reduced and your baby may get less
oxygen than usual. This is normal and most babies cope without any problems. But if
the baby is not getting enough oxygen, the pattern of the heartbeat usually changes. In
some case this means that he or she needs to be delivered quickly.
How is it done?
• A small, handheld ultrasound machine caller a ‘Doppler’ or a trumpet
shaped implement called a ‘Pinard Stethoscope’ can be used to monitor
your baby’s heartbeat every 15minutes during the active phase of the first
stage labour and every 5 minutes during the pushing stage. If there are no
complications or risk factors in the labour this is a safe method of monitoring
your baby’s well being which allows you move around.
• If continual monitoring is indicated an Electronic Fetal Monitor
(EFM) can be used. Two receivers held in place by belts around your
waist and hips monitor your baby’s heartbeat and contractions. This
may be done for 20-30 minutes initially and can be continual
throughout labour if indicated.
• EFM can also be recorded by a Fetal Scalp Electrode which is an
electrode fastened to the baby’s head by a very small clip. This
method is used if there is difficulty recording your baby’s heartbeat
abdominally.
Which is best? If you are healthy and have a trouble free pregnancy and labour the
optimal way to listen to your baby’s heartbeat during labour is with a
hand-held Doppler or Pinard.
However, if you have problems in your pregnancy and/or labour your baby
may need to be monitored by the electronic fetal heart monitor.
Some reasons for this include:
o Induction of labour with Syntocinon drip.
o High blood pressure
o Twins
o Previous Caesarean
o Epidural - if you have one
o Pro-longed Labour

9
Pain Relief Options
When labour starts you will initially feel tightening of your uterus (womb). These will
gradually become regular and stronger and as labour progresses the pain usually
becomes stronger.
The amount of pain felt during labour can vary. Pain can also occur in the lower back.
Over 90% of women find that they need some sort of pain relief.
It is helpful to attend antenatal classes run by midwives. Understanding what might
happen during labour will make you feel less anxious. At these classes you can also
learn about the types of pain relief that are in use.
Non Pharmacological Pharmacological
Methods Methods
Mobilising/ Positions Entonox (gas & air).
Water Pethidine
Relaxation techniques Epidural
Breathing
Massage
Music
TENS
Heat Packs
Alternative Methods
Aromatherapy
Acupuncture
Reflexology
Homeopathy
Hypnosis
For many women labour = pain. Yes, pain is part of the birth process. However, the
pain of labour is like no other, in that it doesn’t signal that something is wrong, but
that your body is working towards the birth of your baby. Your body is helping you
rather than harming you. Embrace and accept the contractions and your body will
work more efficiently for you. A body that is fit, rested, well hydrated and nourished
will sustain energy levels longer and work more efficiently.
Most women will have experienced varying degrees of pain in their lives and will
have some idea of their pain threshold. Consider what method and/or methods of pain
relief you may like in your labour, but keep an open mind, you may find that you
manage with natural methods much better than you could have hoped.

10
Go with the flow!
Suggestions for coping with the first stage of labour & ways to help yourself;
• Keep moving between contractions, this helps you cope physically with the
pain. During contractions, take up a comfortable position.
• Try to stay as upright as possible, so that the baby’s head sits firmly on the
cervix, making your contractions stronger and more effective.
• Concentrate on your breathing, to calm you and take your mind off the
contraction.
• Relax in between contractions to save your energy for when you need it.
• Sigh, or even moan and groan to release pain.
• Focus on what the contraction is achieving, visualise the cervix opening!
• Take one contraction at a time, and don’t think about the contractions to
follow. Perhaps see each contraction as a wave, which you have to ride over to
reach the baby.
• Pass urine often, so that your bladder doesn’t get in the way of the baby.
• Have a warm bath, for as long as you feel comfortable.
Massage; Massage increases heat to the underlying tissue and is thought to increase the use of
endorphins, which are your body’s naturally produced painkillers. Massage can be
done by your partner, birth partner. During the early stages of labour you may find
general massage of the back and shoulders calming. Later, pressure applied to the
sacral area during a contraction may be useful.
Eat & Drink; Something light and nourishing is best. If labour gets going during the night and you
have to get up, eat a light breakfast even if its 4 am, you probably won’t feel like
eating later. A well nourished and hydrated body will work more efficiently for you in
labour!
Music; Music therapy encourages women to cope with labour and delivery without drugs,
helps them to breathe properly and focus their attention. Using music for some

11
women may make them less anxious during labour. All women are welcome to bring
in their own music, perhaps music they listened to while their babies were in-utero.
Mobilising; Remaining mobile, especially during the early stages of labour, can help reduce
backache as well as acting as a distraction to the pain. Try different positions in labour
using cushions, bean bags or a ‘birthing ball’ for support until you find a position that
suits you best. When you are having a contraction, concentrate on relaxing your
whole body. Active Birth will enable your uterus to contract freely and the baby’s
head to rotate and descend and thereby speeding up labour and assisting in an easier
birth.
Water; There are considerable benefits of using water during labour, including less painful
contractions, less need for pharmacological pain relief and shorter labour. Water
supports the body, and relaxing in the bath may offer welcome relief. The lapping of
the water over your tummy may be very comforting and soothing.
BREATHING FOR LABOUR;
FIRST STAGE BREATHING
o Keep it simple
o Breathing for labour should not be a great conscious effort.
o Start each contraction with a breath
o Then a slow relaxing breath in and out.
o Remain calm and keep your breathing rate as slow as feels comfortable.
o As breathing becomes faster with the intensity of the contraction, take shallow
breaths – ‘candle breathing’.
o At the end of the contraction take a slow relaxing breath in and out.
TRANSITION BREATHING
o Labour partner keeps a continuous eye contact during
contractions
o Distraction such as singing nursery rhymes, counting or
tapping out a rhythm to avoid holding your breath or
involuntary pushing.
SECOND STAGE BREATHING
o You do not need to hold your breath when you are
pushing.
o Pushing with shorter pushes is as effective, take as
many breaths as you need during a contraction.
o Pushing during an out breath is efficient.
o Remember not all contractions are equal.
o Conserve energy by relaxing in between contractions.

12
Positions; Try a variety of positions in the first stage, as different positions will probably be
comfortable at different times. Practice these before hand, so that you can follow your
body’s natural cues with ease. You may find that you want to lie down at some time
during the first stage. Rest on your side, not on your back, with your head and upper
thigh well supported by cushions.
Staying Upright;
During early contractions, support yourself on a nearby surface,
such as a wall, chair, seat, bed table or the hospital bed.
Kneel down as necessary.
Sitting Forwards; Sit facing the back of the chair, and lean over it on a
pillow or cushion. Rest your head on your folded arms.
Keep your knees apart; you can put a cushion on the seat
of the chair too.
Resting on your Partner; As you move around in early labour, you may like to lean
against your partner during contractions. He can massage
your back or stroke your shoulders.
Kneeling Forwards; Kneel down on a birthing mat with your legs apart, and relax forwards on a pile of
cushions, pillows or a beanbag. Try to be as upright as possible. Sit to one side
between contractions.
On all Fours; Kneel down on your hands and knees on all fours and tilt your pelvis to and fro. Do
not arch your back. Between contractions, relax and rest your head on your arms.
Backache Labour (OP Position);
• When the baby is facing towards your abdomen, instead of away from it, its
head tends to press against your spine, causing backache. To relieve pain:
• During contractions, lean forward with your weight supported, such as on all
fours, to take the baby’s weight off your back, and rock your pelvis to and fro
between contractions.
• Ask your partner to massage your back, or hold a heat pack to the base of your
spine during contractions.

13
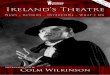
Some Active Positions for Labour

14
A to Z of Natural Pain Relief in Labour.
A is for Active Birth, actively participating in your birth.
B is for Breathing & Body Awareness
C is for Cuddles
D is for Drink plenty of fluids
E is for Eat little & often
F is for Freedom to mobilise around
G is for Getting in tune with your body
H is for Heat; baths, heat packs & hot water bottles
I is for Imagine your baby moving down through your pelvis
J is for Judgement.......... Trusting your own & your midwives
K is for Knowledge & Kisses
L is for Love & Laughter
M is for Massage & Music
N is for Nestle down in a large pile of cushions or a huge bean bag
O is for Opening & allowing your baby to be born
P is for Positive thinking & Praise
Q is for Quiet, enjoy your own space
R is for Relaxation and Rocking
S is for Support & Smiles
T is for Trust your body; ‘you can give birth’
U is for Understanding what's happening & keeping upright
V is for Variety of positions
W is for Water & Walking
X is for Xtra kisses!!
Y is for Your own instincts
Z is for ZZZzzzzzzzzzzz, doze off in between contractions

15
UPRIGHT POSITIONS V’S
RECLINING POSITIONS
SQUATTING, STANDING, KNEELING SUPINE, SEMI-RECLINING
1. GRAVITY EFFECTIVE Weight of baby’s head and body puts even
pressure on the cervix
= faster dilation.
2. UTERUS TILTS FORWARD DURING
CONTRACTIONS WITHOUT
RESISTANCE = more efficient contractions & less pain.
3. LESS PRESSURE ON MAJOR BLOOD
VESSELS = better blood flow to baby and placenta, better
oxygenation, less fetal distress.
4. SACRUM MOBILE = pelvic canal can widen & adjust to descending
head.
5. PELVIC JOINTS CAN EXPAND & MOVE
LESS PRESSURE ON NERVES = less pressure on joints, less pain ( especially
backache), more space, pelvic diameters
increase.
6. SECOND STAGE PELVIS UPRIGHT = baby’s angle of descent easiest (down & out).
Uterus exerts maximum force.
Bearing down more efficient – shortens second
stage.
7. PERINEUM CAN EXPAND EVENLY
DUE TO PRESSURE FROM BABYS
HEAD = less risk of tearing
8. BABY AT BIRTH OPTIMAL CONDITION
9. ACTIVE = less need for painkillers or interventions, no
side effects.
1 .OPPOSES GRAVITY Less pressure on cervix from baby’s weight.
Uneven pressure on cervix
= slower dilation.
2. UTERUS WORKS AGAINST
RESISTANCE FROM GRAVITY
DURING CONTRACTIONS = less efficient contractions
more pain.
3. WEIGHT OF UTERUS RESTS ON
MAJOR BLOOD VESSELS = can affect blood flow - greater risk
of fetal distress.
4. SACRUM IMMOBILE = pelvic canal and outlet narrowed.
5. PELVIS LESS FLEXIBLE MORE
PRESSURE ON NERVES. = more pressure and pain, less space
for baby, pelvic diameters decrease.
6. SECOND STAGE PELVIS HORIZONTAL = baby’s angle of descent more difficult
(up hill). Bearing down force less efficient –
prolongs 2nd stage.
7. DIRECT PRESSURE ON PERINEUM
FORM BABY’S HEAD CANNOT EXPAND
EVENLY = greater risk of tearing.
8. BABY AT BIRTH MAY BE
UNNECESSARILY COMPROMISED
9. PASSIVE = more need for painkillers or interventions,
possible side effects.

16
Transcutaneous Electrical Nerve Stimulation Machine
(TENS)
o Sends weak pulsed electrical current, which feel like ‘pins & needles’, through
your skin via adhesive pads attached to your back
o Stimulates your body’s natural painkillers and blocking pain sensation.
o It can be used with other methods of pain relief.
o The strength or the current is controlled by the mother.
o It is most effective when it is used in early labour.
What are the benefits of TENS machine;
o Drug free
o You are in control
o You can continue to be mobile while using it
o It allows you to use other drugs such as pethidine or gas and air (entonox)
o It is very effective if used from the onset of labour
o No side effects to the baby
o No side effects to you
Please note that Cavan General Hospital does not provide a TENS machine, they may
be hired or bought from local pharmacies.

17
ENTONOX
• This is a mixture of nitrous oxide and oxygen, also known as “gas and
air”. You breathe it in through a mask or mouth piece. It is simple
and quick to act, and wears off in minutes.
• It can be an effective pain killer if used in the correct way,
however, it sometimes makes you feel light headed or a little sick
for a short time. It does not harm your baby.
• It may not take the pain away completely, it dulls the sensation of
the contraction, but it may be helpful through at least part of the
labour. It can be used at any time during labour.
• It can be used in conjunction with other pain relief methods. You
control the amount of gas you use, but to get the best effect timing
is important.
• You should start breathing the gas as soon as you feel a contraction coming on
so that you will get the full effect when the pain is at its peak. You should not
use it between contractions or for long periods as this can make you feel dizzy
and tingly.
PETHIDINE
• Opiates such as Pethidine are strong pain killers. These are given by injection
into a muscle (usually thigh or buttock) by midwives.
• Pethidine is a widely used drug for pain relief in labour.
• It does not completely take the pain of contraction away; it takes the sharp
edge of the pain.
• It takes approx 20 min. to work and usually lasts about 2-3 hrs.
• It is given in the first stage of labour.
• Pethidine works well for some women as it aids relaxation.
• If a woman is tired, Pethidine can provide sedation (and sometimes much
needed sleep).
• It is given with an anti-sickness drug, as Pethidine can sometimes make you
feel sick.
• Pethidine crosses over the placenta and reaches the baby.
• If your baby delivers soon after receiving Pethidine, your baby’s breathing
may be affected and occasionally an antidote needs to be given.
• Most babies are fine, but they may tend to be a little sleepier in the first few
days and may take longer to establish feeding.
• Other side effects include; feeling shaky, light headed and disorientated.

18
EPIDURAL
• An epidural is a method of pain relief which involves numbing the sensations
to your tummy area and womb.
• It involves placing a small plastic tube in a particular part of the spine called
the epidural space.
• It is the most complicated form of pain relief and it is performed by an
anaesthetist, but not all women need this level of pain control. When working
well it is the most effective method of pain relief.
Who can have an epidural?
• Most people can have an epidural, but there are a few women who cannot
have epidurals because of previous back surgery, certain medical conditions
and or bleeding disorders which may make it unsuitable. If you are in doubt,
you can speak with a midwife or one of your team doctors and they can further
advise you.
• If you have a complicated or long labour your midwife or obstetrician may
recommend that you have one.
What does it involve?
• Before inserting an epidural, a drip needs to be set up. This involves putting a
plastic tube into a vein in your hand or arm and running fluid through it (this is
often necessary in labour for other reasons).
• Then you will be asked to curl up on your side or sit bending forwards.
• Your back will be cleaned with antiseptic and a little injection of local
anaesthetic will be given into the skin to numb the area where the epidural
needle will be inserted.
• After the needle is in place a small tube is passed through it into the epidural
space in your back. This is where the nerves carrying pain from the uterus are
located. Care is needed for correct placement of the epidural needle as if it
should go too deep you may get a headache afterwards. It is therefore
important to keep still while the anaesthetist is putting in the epidural, but after
the tube is in place and taped to your back you will be free to move.
• Once the epidural is in place pain relieving drugs can be given as often as is
necessary, sometimes continuously by a pump.
• While the epidural is taking effect, the midwife will take your blood pressure
regularly.
• The anaesthetist and your midwife will also check that the epidural is working
properly. It usually takes between 5-20 minutes for the drugs to take their full
effect, but occasionally it doesn’t work well at first, and some adjustment is
needed.

19
The potential disadvantages or complications of epidural.
Complications or adverse effects can occur, even though your anaesthetist takes
special precautions to avoid them. People vary in how they interpret words and
numbers. This scale is provided to help you.
Very
Common
Common Uncommon Rare Very Rare
1 in 10 1 in 100 1 in 1000 1 in 10,000 1 in 100,000
What are the effects and side effects?
• Sometimes it may be technically difficult or even impossible to locate the
epidural space and the procedure may be abandoned (uncommon).
• Occasionally the epidural only partly works leaving you with patches of pain
(uncommon); this can be corrected in most instances and the anaesthetist can
re-site the epidural if necessary. In a small number of women, epidurals do not
work at all (very rare).
• Your blood pressure may drop when the epidural is first put in and whenever
you have a top-up (common). The midwife will check your blood pressure
regularly.
• A sudden drop in your blood pressure can affect your baby and so your baby
will be monitored continuously for the rest of your labour; your baby’s heart
may slow down, usually this just needs watching and will return to normal.
However, if it is severe or persistent indicating that your baby is distressed, the
obstetrician may decide to deliver the baby by Caesarean section (rare).
• You may feel sick and you may be sick (common).
• Some women find they become very itchy; this is harmless and wears off after
the epidural is stopped (common).
• Occasionally epidurals make you shiver. This can be alarming but wears off
quite soon (uncommon).
• You may lose some sensation and it may be difficult to know when you need
to pass urine (common). The midwife will empty your bladder by placing a
catheter (thin tube) put into your bladder to drain out the urine; the insertion of
this tube can sometimes cause a urinary infection (rare).
• An epidural can prolong the second stage of labour and you may find you do
not have the urge to push when it is time for your baby to be born (common);
as a result there is an increased chance that you will need an assisted delivery
with suction or forceps (common).
• You may experience a severe headache. This is caused by a puncture in the
sac that contains the spinal fluid by the hollow needle, causing the fluid to leak
out. It usually disappears in a few days but if symptoms persist a further
epidural may be needed (common).
• Body temperature can rise the longer the epidural is in place. Meningitis, an
infection of the brain, can occur (very rare).
• There is a small risk of the epidural drugs being injected into a blood vessel
which may cause dizziness and seizures that require immediate treatment;
(very rare).
• There is a very small risk of nerve damage producing a weakness or numbness
in one or both legs which may be temporary (rare) or permanent (very rare).

20
• The needle or fine tube can break in the body tissues or the epidural space
which may require surgical removal (very rare).
• Epidurals do not cause long-term backache but can cause local tenderness
around the needle site. This will only last a few days (common).
Although extremely rare, life threatening conditions can occur such as low blood
pressure, respiratory or cardiac arrest, severe allergic reaction or convulsion. These
will require emergency treatment to save the lives of mother and baby. However, the
use of epidural during labour and delivery has been well researched and proven to be
safe.
What if I need an operation?
• If you need an operation (such as a caesarean section or removal of a retained
placenta after delivery) the epidural and or spinal can be used instead of a
general anaesthetic.
• A mixture of strong local anaesthetic and painkiller can be used to “top up”
your epidural to provide enough numbness and pain relief for your operation.
• However, under certain circumstances, if the epidural is less than adequate, or
if there is no time to “top up” the epidural you may need a general anaesthetic.
• Occasionally, (1 in 20 chance) it is necessary to convert to using a general
anaesthetic part way through an operation if the epidural becomes less
effective.
What are the pros and cons of having a spinal anaesthetic compared with a
general anaesthetic?
• Spinals are generally safer for you and your baby.
• They enable you and your partner to share in the birth experience.
• You will not feel as drowsy afterward after a spinal as you would after a
general anaesthetic.
• They allow for earlier feeding and contact with your baby.
• You will have good pain relief for longer after the operation.
• Your baby will be born more alert.
• Rarely spinals do not work properly, so a general anaesthetic is required (1 in
100 chance).
• Itching can occur during or after the operation but this can be treated.
• Severe headache can occur (less than 1 in 100 chance) but this can be treated.
• Local tenderness in your back may occur for a few days. Spinals do not cause
long term backache.
You will have a choice of different methods for pain relief during labour and delivery.
If you need a caesarean section, be reassured it is safe and can be a very rewarding
experience. Most women will remain awake, but others will need to go to sleep for
the reasons discussed.
We hope that the information provided will enable you to make informed choices for
pain relief and anaesthesia. If you need further information please speak to your
midwife. She will discuss any issues or concerns that you may have and may
recommend that you make an appointment to see the anaesthetist.

21
Alternative Pain Relief Methods
If you are considering using any of the following alternative methods
of pain relief such as Aromatherapy, Acupuncture, Reflexology, Homeopathy or
Hypnosis, please be aware that as midwives we may not be qualified in that area, so it
would be recommended that you consult with a qualified person in that area for
guidance and support.
Aromatherapy; Aromatherapy is... the skilled and controlled use of essential oils for physical and
emotional health and well being. “Aromatherapy is a caring, hands-on therapy which
seeks to induce relaxation, to increase energy, to reduce the effects of stress and to
restore lost balance to mind, body and soul.” Robert Tisserand.
Aromatherapy can be very useful in pregnancy, but great care should be taken and
consultation with a qualified Aroma therapist would be advised. As the essential oils
are easily absorbed through the skin and inhaled into the lungs, they then enter
the bloodstream and cross the placenta and the fetal circulation.
Acupuncture; Ancient Chinese therapy that involves the insertion of fine needles into specific points
on your body. It relieves pain by stimulating endorphins. Acupuncture is a method of
encouraging the body to promote natural healing and to improve functioning.
Acupuncture should only be carried out by someone qualified in that area.
Reflexology; Often mistaken for a foot massage, this involves applying pressure to specific points
on the foot, which are linked to every organ and system of the body, to help relieve
pain. Through skilful manipulation a reflexologist can help to unblock the flow of
energy in organs and rebalance entire systems. It is particularly useful for stress
related conditions as it helps to discharge the negative effects of stress and stimulate
the body’s own healing. This should only be carried out by someone qualified in this
area.
Homeopathy; Homeopathy is a gentle, yet highly effective system of medicine which involves
treating the individual with highly diluted naturally occurring substances, in the form
of remedies, with the aim of triggering the body's natural system of healing, which
assists the natural tendency of the body to heal itself. Based on their individual
symptoms, a homeopath will match the most appropriate medicine to each patient. It
recognises that all systems of ill health are expressions of disharmony within the
whole person and it is the patient who needs treatment not the disease. Different
people react in different ways to the same disease. In order to select the correct
remedy, your homeopath will need to know not only your physical symptoms but also
as much as possible about yourself and how your symptoms affect you. This should
only be carried out by someone qualified in this area.

22
Hypnosis/Hypnobirthing;
Hypnosis is a form of deep physical and mental relaxation. Hypnobirthing is a unique
antenatal programme that teaches simple but specific self-hypnosis and relaxation
techniques for an easier, gentler birth. Hypnobirthing is about training your mind to
relax so your body can easily do what it was designed for. It works by the power of
suggestion, which can reduce the intensity of labour pains. You are able to relax your
body and release some of the tension and anxiety which exacerbates pain. If you
believe you can control the pain you may be less frightened or disturbed by it and
therefore be more able to cope with it. It is not a form of sleep and you have full
control over yourself. You can come out of hypnosis any time you want. This should
only be carried out by someone qualified in this area.
YOUR MIDWIFE ON LABOUR WARD WILL HELP AND GUIDE
YOU IN YOUR PAIN RELIEF OPTIONS
~~ SO ASK HER ADVICE.