Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISMVol. 50, No. 9, September 2004, pp 3045–3048© 2004, American College of Rheumatology
CONCISE COMMUNICATIONS
DOI 10.1002/art.20426
Use of sunscreens to protect against ultraviolet-induced lupus erythematosus
Photosensitivity is the leading symptom of cutaneousand systemic lupus erythematosus (LE). The role of sunlight inthe induction of LE lesions has long been recognized, based onthe observation that lesions are predominantly localized tosun-exposed areas of the body, especially the face, but also thehead and neck area. Moreover, LE worsens during the summerperiod or in the weeks following increased sun exposure (1,2).Definite proof for a causative role of ultraviolet (UV) irradi-ation in the induction of LE came from experimental photo-provocation testing in the early 1990s (3). Those studiesunraveled the fact that the UV action spectrum that provokesLE in sensitive individuals includes both the ultraviolet B(UVB; 290–320 nm) and the UVA (320–400 nm) range.Moreover, the studies showed that LE does not developimmediately after UV exposure, but after a delay of 2–3 weeks.
In view of the central role of sunlight in provoking LE,it is important for patients to establish efficient UV protectionthroughout the year. This is a particular challenge for areas ofthe skin that cannot effectively be covered by clothing. Over
the last decade, high-potency sunscreens that protect againstUV-induced sunburn have become widely available. However,the degree to which these sunscreens protect against otherunwanted effects of UV irradiation has been called intoquestion (4,5). Therefore, we have routinely included sun-screens in our diagnostic testing protocol for LE.
A recent study involving 11 patients suggested thatsunscreens protect against UV-induced LE lesions (6). Inorder to obtain a more general assessment of the protectivecapacity of sunscreens in LE in a larger cohort of patients, weperformed a retrospective evaluation of 66 patients who un-derwent photoprovocation testing between 1999 and 2002.After informed written consent had been obtained, testing wasdone (according to a standard protocol) on the upper back,with a field size of 8 � 5 cm (7). The doses applied were 100mJ/cm2 of UVA (from a Dermalight UltrA1 source; HoenleMedizintechnik, Munich, Germany) or the 1.5-fold minimalerythema dose of UVB (from a Waldmann UVB 800 unit;Munich, Germany), or a combination of both, on 3 consecutivedays. An additional field was irradiated with combined UVA/UVB 15 minutes after the application of a commercial sun-screen that efficiently filters UVA (Anthelios W30; La Roche-Posay, La Roche-Posay, France). This sunscreen contained a
Figure 1. Patient with chronic discoid lupus erythematosus, showing a positive reaction to ultraviolet B (UVB) and UVA/UVB2 weeks after photoprovocation, but no reaction to UVA alone (top). No reaction to UVA/UBV was observed in the area towhich sunscreen was applied (bottom).
3045

formulation of different active ingredients shielding predomi-nantly against UVA (parsol 1789), UVB (uvinul N539, uvinulT150), or against UVA and UVB (mexoryl XL, titaniumdioxide).
According to the recommendations of the US Foodand Drug Administration and the European Cosmetic Toiletryand Perfumery Association, 2 mg/cm2 of sunscreen was ap-plied. Readings were performed on days 2, 3, and 4 and again1, 2, and 3 weeks after photoprovocation. Late readings areparticularly important, because cutaneous LE tends to developprimarily 2–3 weeks after irradiation (1). Criteria for a positivereaction were a palpable erythematous infiltrate clinicallyresembling LE that developed with a crescendo time course,becoming most pronounced 2–3 weeks after photoprovocation.
Approximately 75% of our LE patients showed apositive reaction to the UV challenge (Figure 1). Only thosepatients who showed photosensitivity (n � 52) were analyzedfurther. Most of these patients had discoid or tumidus-typeLE. As described previously (2,3), we found the combinedirradiation with UVA and UVB to be most effective intriggering cutaneous LE (98%). In fact, 30% of subjectsreacted to the combined irradiation only and to neither UVAnor UVB when applied alone, suggesting a synergistic effect ofthe combination in some patients. In 19% of the patients, bothUVA and UVB induced LE lesions. UVA alone induced LE inonly 17 patients (33%). UVB induced LE in 48% of thepatients. One patient showed a positive reaction exclusively toUVB and was excluded from further analysis (Table 1). Inselected patients, histologic examination was performed toconfirm the clinical diagnosis.
Of 51 patients who had developed LE in the UVA/UVB field, 49 (96%) were entirely protected by the sunscreenagainst the development of LE or LE-like lesions. Protectedpatients showed either no reaction or pigmentation only(Table 2). Thus, the capacity of the sunscreen to prevent UV-induced LE was higher than the protective action againstUV-induced pigmentation. In a small number of patients, weinvestigated in a third area a high- potency sunscreen basedprimarily on physical protection (TiO2) and obtained similarresults.
Our data show that modern sunscreens that efficientlyprotect against both UVA and UVB are very effective inprotecting against UV-induced LE. Preliminary data suggestthat daily application of high-potency sunscreens also protectspatients against UV-induced LE by natural sunlight. Ourpersonal experience is mainly limited to only 2 sunscreens, butother high-potency sunscreens that protect against UVA and
UVB might be similarly effective. However, a study comparing3 different sunscreen formulations in a set of 11 patients foundthese sunscreens to vary in their protective capacity against LEprovocation, though all of the formulations used containedvarious compounds that filter UVA and UVB (6). The bestprotection was achieved by the only formulation that containedMexoryl XL, a rather novel compound filtering in both theUVA and UVB range. Interestingly, this compound was alsocontained in the sunscreen used in our present study. The factthat our sunscreen protected against LE in 98% of patients butstill allowed for pigmentation in 49% suggests that the effec-tiveness of a compound to shield against LE cannot necessarilybe extrapolated from its capacity to prevent other biologicresponses elicited by sunlight.
Dr. Rocken’s work was supported in part by grant RO764/8-1from the Deutsche Forschungsgemeinschaft.
Thomas Herzinger, MDGerd Plewig, MDLudwig-Maximillian-UniversityMunich, GermanyMartin Rocken, MDEberhard-Karl-UniversityTubingen, Germany
1. Millard TP, Hawk JL, McGregor JM. Photosensitivity in lupus.Lupus 2000;9:3–10.
2. Kuhn A, Sonntag M, Ruzicka T, Lehmann P, Megahed M. His-topathologic findings in lupus erythematosus tumidus: review of 80patients. J Am Acad Dermatol 2003;48:901–8.
3. Lehmann P, Holzle E, Kind P, Goerz G, Plewig G. Experimentalreproduction of skin lesions in lupus erythematosus by UVA andUVB radiation. J Am Acad Dermatol 1990;22:181–7.
4. Haywood R, Wardman P, Sanders R, Linge C. Sunscreens inade-quately protect against ultraviolet-A-induced free radicals in skin:implications for skin aging and melanoma? J Invest Dermatol2003;121:862–8.
5. Poon TS, Barnetson RS, Halliday GM. Prevention of immunosup-pression by sunscreens in humans is unrelated to protection fromerythema and dependent on protection from ultraviolet A in theface of constant ultraviolet B protection. Invest Dermatol 2003;121:184–90.
6. Stege H, Budde MA, Grether-Beck S, Krutmann J. Evaluation ofthe capacity of sunscreens to photoprotect lupus erythematosuspatients by employing the photoprovocation test. PhotodermatolPhotoimmunol Photomed 2000;16:256–9.
7. Walchner M, Messer G, Kind P. Phototesting and photoprotectionin LE. Lupus 1997;6:167–74.
Table 1. Action spectra for the induction of LE lesions*
Patient group UVA UVB UVA � UVB
Chronic discoid LE (n � 33) 9 (27) 16 (48) 32 (97)Systemic LE (n � 4) 3 (75) 3 (75) 4 (100)Subacute cutaneous LE (n � 2) 1 (50) 1 (50) 2 (100)Tumidus-type LE (n � 12) 4 (33) 4 (33) 12 (100)Profound LE (n � 1) 0 (0) 1 (100) 1 (100)
* Values are the number (%) of patients. The ability of differentwavelength spectra to induce lupus erythematosus (LE) on the upperback is described in ref. 3. Only erythematosus infiltrates at week 2 or3 were considered positive. UV � ultraviolet.
Table 2. Protective effect of sunscreen in patients who developed LElesions at the site of combined UVA/UVB irradiation*
Patient groupLE
lesionNo
reactionPigmentation
only
Chronic discoid LE (n � 33) 2 (6) 15 (47) 15 (47)Systemic LE (n � 4) 0 (0) 2 (50) 2 (50)Subacute cutaneous LE (n � 2) 0 (0) 1 (50) 1 (50)Tumidus-type LE (n � 12) 0 (0) 6 (50) 6 (50)Profound LE (n � 1) 0 (0) 0 (0) 1 (100)
Total 2 (4) 26 (47) 25 (49)
* Values are the number (%) of patients. Sunscreen (2 mg/cm2) wasapplied to a closely adjacent test site 15 minutes before irradiation withultraviolet A (UVA) and UVB. LE � lupus erythematosus.
3046 CONCISE COMMUNICATIONS

DOI 10.1002/art.20475
Lack of linkage of IL1RN genotypes with ankylosingspondylitis susceptibility
The interleukin-1 receptor antagonist gene (IL1RN), anatural modulator existing in the body, can bind IL-1R andblock its effects. Recently, a variable-number tandem repeatpolymorphism in intron 2 of IL1RN was associated withankylosing spondylitis (AS) in 2 European population groups(1,2). Here, we investigated the role of IL1RN genes in ASsusceptibility in North American families with 2 or moresiblings meeting the 1984 modified New York criteria for AS (3).
Informed consent was obtained from each family mem-ber. This study was approved by the Committee for the Protectionof Human Subjects at the University of Texas Health ScienceCenter at Houston. In total, 229 pedigrees with at least 1 affectedindividual were included for family-based association analyses,and 244 affected sibpairs derived from 180 pedigrees wereincluded for linkage analyses after removing the pedigrees inwhich the self-reported relationship was not consistent with thegenetic data. Of these families, 94% were Caucasian, and 97% ofthe probands were HLA–B27 positive.
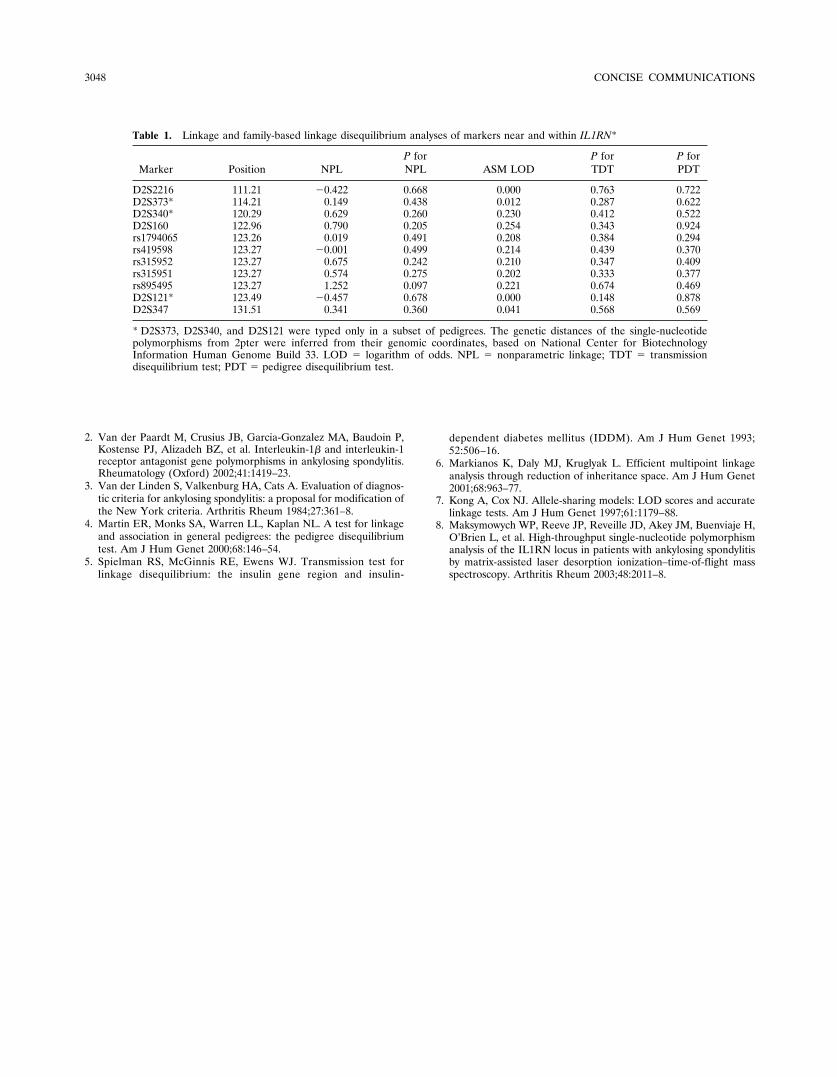
The genetic variation of IL1RN was ascertained bysequencing its complete coding sequence, all intron/exon junc-tion regions, 3�- and 5�-untranslated regions, and the promoterregion in 102 patients and 48 ethnically matched controls. Intotal, 25 single-nucleotide polymorphisms (SNPs) were identi-fied (data not shown). The 5 most informative SNPs(rs1794065, rs419598, rs315952, rs315951, and rs895495) wereselected for further association and linkage studies, along with6 microsatellite markers (D2S2216, D2S373, D2S340, D2S160,D2S121, and D2S347) that are mapped to this region (seeTable 1 for the location of the markers). Family-based associ-ation analyses were performed using the pedigree disequili-brium test (PDT) (4) and the transmission disequilibrium test(TDT) (5). Neither the TDT nor the PDT approach showedsignificant association for individual markers (Table 1) and forthe haplotypes based on 5 SNPs (data not shown).
We further examined the linkage of the region con-taining IL1RN using the 11 markers. Nonparametric linkage(NPL) analyses were performed with all 5 SNPs and 3 micro-satellite markers (D2S2216, D2S160, and D2S347) using 244affected sibpairs derived from 180 pedigrees. Both parametric(LOD; logarithm of odds) and nonparametric (NPL and ASM)analyses were conducted for linkage analyses, usingGeneHunter-Plus software (6) for LOD, and NPL and ASMfor an allele-sharing–based approach (7) (see Table 1). Threeother markers, including D2S373, D2S340, and D2S121, in thesame region were also typed in a subset of the pedigrees (171affected sibpairs derived from 119 pedigrees). No linkage wasobserved with any of the 11 markers studied.
In a recent collaborative study of a large cohort ofCanadian patients with AS, using 3 SNPs of IL1RN identifiedin this study (rs419598, rs315952, and rs315951), we found anassociation of AS with the SNPs of IL1RN and their haplotypes(8). TDT analysis of a limited sample of AS families fromwestern Canada demonstrated significant differences in trans-mission of an IL1RN SNP haplotype that was disease-associated in the case–control evaluation. In this study, wewere not able to validate the association in our cohort,although our sample size for the TDT and PDT analyses wasmuch larger. The discrepancy may reflect clinical differences inthe patient populations studied, i.e., differences in disease
severity or disease phenotypes (such as uveitis or peripheralarthritis, the frequencies of which were not specified in otherseries) (1,8) due to differing referral patterns between theNorth American Ankylosing Spondylitis Gene Consortiumcenters and other centers where associations have been de-scribed. Variable patterns of association across populationsmay also be attributable to population-specific mechanisms ofgenetic susceptibility. Finally, these data do not exclude aminor role for IL1RN genes. The number of sibpairs thatwould be necessary to detect a gene with a small genetic effect(�s �1.5) would be �1,000. If such a small effect were present,our study would lack power to determine this.
Thus, we present evidence that may lead to the exclu-sion of this region on chromosome 2q and, more specifically,IL1RN as having a significant impact on AS susceptibility.However, an impact on disease severity cannot be ruled out bythis study. This is currently under further investigation.
Li Jin, PhDGe Zhang, MSJoshua M. Akey, PhDJingchun Luo, MMJuwon Lee, PhDUniversity of CincinnatiCincinnati, OHMichael H. Weisman, MDCedars–Sinai Medical CenterLos Angeles, CAJane Bruckel, BSNSpondylitis Association of AmericaSherman Oaks, CARobert D. Inman, MDMillicent A. Stone, MDUniversity of TorontoToronto, Ontario, CanadaMuhammad A. Khan, MDCase Western Reserve UniversityCleveland, OHH. Ralph Schumacher, MDUniversity of PennsylvaniaPhiladelphia, PAWalter P. Maksymowych, MDUniversity of AlbertaEdmonton, Alberta, CanadaMaren L. Mahowald, MDUniversity of MinnesotaMinneapolis, MNAllen D. Sawitzke, MDUniversity of UtahSalt Lake City, UTFrank B. Vasey, MDUniversity of South FloridaTampa, FLDavid T. Y. Yu, MDUniversity of California, Los AngelesJohn D. Reveille, MDUniversity of Texas Health Science Center at Houston
1. McGarry F, Neilly J, Anderson N, Sturrock R, Field M. A poly-morphism within the interleukin 1 receptor antagonist (IL-1Ra)gene is associated with ankylosing spondylitis. Rheumatology (Ox-ford) 2001;40:1359–64.
CONCISE COMMUNICATIONS 3047
2. Van der Paardt M, Crusius JB, Garcia-Gonzalez MA, Baudoin P,Kostense PJ, Alizadeh BZ, et al. Interleukin-1� and interleukin-1receptor antagonist gene polymorphisms in ankylosing spondylitis.Rheumatology (Oxford) 2002;41:1419–23.
3. Van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnos-tic criteria for ankylosing spondylitis: a proposal for modification ofthe New York criteria. Arthritis Rheum 1984;27:361–8.
4. Martin ER, Monks SA, Warren LL, Kaplan NL. A test for linkageand association in general pedigrees: the pedigree disequilibriumtest. Am J Hum Genet 2000;68:146–54.
5. Spielman RS, McGinnis RE, Ewens WJ. Transmission test forlinkage disequilibrium: the insulin gene region and insulin-
dependent diabetes mellitus (IDDM). Am J Hum Genet 1993;52:506–16.
6. Markianos K, Daly MJ, Kruglyak L. Efficient multipoint linkageanalysis through reduction of inheritance space. Am J Hum Genet2001;68:963–77.
7. Kong A, Cox NJ. Allele-sharing models: LOD scores and accuratelinkage tests. Am J Hum Genet 1997;61:1179–88.
8. Maksymowych WP, Reeve JP, Reveille JD, Akey JM, Buenviaje H,O’Brien L, et al. High-throughput single-nucleotide polymorphismanalysis of the IL1RN locus in patients with ankylosing spondylitisby matrix-assisted laser desorption ionization–time-of-flight massspectroscopy. Arthritis Rheum 2003;48:2011–8.
Table 1. Linkage and family-based linkage disequilibrium analyses of markers near and within IL1RN*
Marker Position NPLP forNPL ASM LOD
P forTDT
P forPDT
D2S2216 111.21 �0.422 0.668 0.000 0.763 0.722D2S373* 114.21 0.149 0.438 0.012 0.287 0.622D2S340* 120.29 0.629 0.260 0.230 0.412 0.522D2S160 122.96 0.790 0.205 0.254 0.343 0.924rs1794065 123.26 0.019 0.491 0.208 0.384 0.294rs419598 123.27 �0.001 0.499 0.214 0.439 0.370rs315952 123.27 0.675 0.242 0.210 0.347 0.409rs315951 123.27 0.574 0.275 0.202 0.333 0.377rs895495 123.27 1.252 0.097 0.221 0.674 0.469D2S121* 123.49 �0.457 0.678 0.000 0.148 0.878D2S347 131.51 0.341 0.360 0.041 0.568 0.569
* D2S373, D2S340, and D2S121 were typed only in a subset of pedigrees. The genetic distances of the single-nucleotidepolymorphisms from 2pter were inferred from their genomic coordinates, based on National Center for BiotechnologyInformation Human Genome Build 33. LOD � logarithm of odds. NPL � nonparametric linkage; TDT � transmissiondisequilibrium test; PDT � pedigree disequilibrium test.
3048 CONCISE COMMUNICATIONS









![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://img.pdfslide.net/doc/110x75/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)