Embed Size (px)
Citation preview

C
Odnatscsmssm
dM4
M
Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 2, pp. 396–402, 2007Copyright © 2007 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/07/$–see front matter
doi:10.1016/j.ijrobp.2006.11.059
LINICAL INVESTIGATION Head and Neck
LACK OF OSTEORADIONECROSIS OF THE MANDIBLE AFTERINTENSITY-MODULATED RADIOTHERAPY FOR HEAD AND NECK CANCER:
LIKELY CONTRIBUTIONS OF BOTH DENTAL CARE AND IMPROVEDDOSE DISTRIBUTIONS
MERAV A. BEN-DAVID, M.D.,* MAXIMILIANO DIAMANTE, D.M.D,† JEFFREY D. RADAWSKI, B.SC.,*KAREN A. VINEBERG, B.SC.,* CYNTHIA STROUP, M.S., PA.-C.,*
CAROL-ANNE MURDOCH-KINCH, D.D.S., PH.D.,† SAMUEL R. ZWETCHKENBAUM, D.D.S.,†
AND AVRAHAM EISBRUCH, M.D.*Departments of *Radiation Oncology and †Oral and Maxillofacial Surgery/Hospital Dentistry, University of Michigan Medical
School, Ann Arbor, MI
Purpose: To assess the prevalence and dosimetric and clinical predictors of mandibular osteoradionecrosis(ORN) in patients with head and neck cancer who underwent a pretherapy dental evaluation and prophylactictreatment according to a uniform policy and were treated with intensity-modulated radiotherapy (IMRT).Methods and Materials: Between 1996 and 2005, all patients with head-and-neck cancer treated with parotidgland-sparing IMRT in prospective studies underwent a dental examination and prophylactic treatment accord-ing to a uniform policy that included extractions of high-risk, periodontally involved, and nonrestorable teeth inparts of the mandible expected to receive high radiation doses, fluoride supplements, and the placement of guardsaiming to reduce electron backscatter off metal teeth restorations. The IMRT plans included dose constraints forthe maximal mandibular doses and reduced mean parotid gland and noninvolved oral cavity doses. A retro-spective analysis of Grade 2 or worse (clinical) ORN was performed.Results: A total of 176 patients had a minimal follow-up of 6 months. Of these, 31 (17%) had undergone teethextractions before RT and 13 (7%) after RT. Of the 176 patients, 75% and 50% had received >65 Gy and >70Gy to >1% of the mandibular volume, respectively. Falloff across the mandible characterized the dosedistributions: the average gradient (in the axial plane containing the maximal mandibular dose) was 11 Gy(range, 1–27 Gy; median, 8 Gy). At a median follow-up of 34 months, no cases of ORN had developed (95%confidence interval, 0–2%).Conclusion: The use of a strict prophylactic dental care policy and IMRT resulted in no case of clinical ORN. Inaddition to the dosimetric advantages offered by IMRT, meticulous dental prophylactic care is likely an essentialfactor in reducing ORN risk. © 2007 Elsevier Inc.
Intensity-modulated radiotherapy, Osteoradionecrosis, Head and neck cancer.
tiRte
tltdplo
C
A
INTRODUCTION
steoradionecrosis (ORN) of the mandibular bone is a well-ocumented complication of radiotherapy (RT) for head-and-eck cancer (1–4). Generally, bones are resistant to high radi-tion doses and will not sustain any overt damage as long ashe overlying soft tissue remains intact and the bone is notubjected to excessive stress or trauma. Mendenhall (3) re-ently noted that the presentation of ORN after RT varies frommall, asymptomatic bone exposures that can remain stable foronths or years or heal with conservative management to
evere necrosis necessitating surgical intervention and recon-truction. Several risk factors are associated with the develop-ent of ORN, including age, gender, general health, primary
Reprint requests to: Avraham Eisbruch, M.D., Department of Ra-iation Oncology, University of Michigan Medical School, 1500 E.edical Center Dr., Ann Arbor, MI 48109-0010. Tel: (734) 936-
300; Fax: (734) 936-9340; E-mail: [email protected]. A. Ben-David is currently at Department of Oncology, Sheba
edical Center, Tel Hashomer, Israel.396
umor site and stage, proximity of the tumor to bone or itsnvasion, dentition status, treatment type (e.g., external beamT, brachytherapy, surgery, or chemotherapy or combina-
ions), radiation dose, and associated trauma, such as teethxtraction before or after RT or surgery (1–3).
Since 1996, patients with head and neck cancer have beenreated at the University of Michigan with intensity-modu-ated RT (IMRT) techniques primarily aimed at reducinghe major salivary gland doses. In addition, they producedose gradients across the mandible. During that period, allatients underwent a pre-RT dental evaluation and prophy-actic care according to uniform policies. The original aimf this retrospective study was to compare the mandibular
Supported in part by National Institutes of Heath GrantsA059827 and K12 RR017607.Conflict of interest: none.Received July 18, 2006, and in revised form Sept 22, 2006.
ccepted for publication Nov 30, 2006.

ddwuct
P
tcoa
D
pmtOstppirdpsac(ehaipsposwtttpae
P
vgbgpNi
A
rfPmrbppbcartMt
Frpc
397Lack of mandibular osteoradionecrosis in IMRT ● M. A. BEN-DAVID et al.
oses and clinical factors in patients receiving IMRT whoid or did not develop ORN. However, because no ORNas found in any of these patients, we present the mandib-lar dose distributions and relevant clinical factors, espe-ially those related to dental care, that may have contributedo the lack of this complication.
METHODS AND MATERIALS
atientsThe patients evaluated in this retrospective study received IMRT to
he bilateral neck with curative intent, participated in prospectivelinical protocols, had not received previous RT, and had �6 monthsf follow-up after RT completion. After institutional review boardpproval, their charts and treatment plans were reviewed.
ental evaluation and treatmentBefore RT, all patients underwent a dental evaluation at the Hos-
ital Dentistry Clinic. During this consultation, the patient’s completeedical, dental, social, and family histories were obtained, and po-
ential oral side effects of RT, including xerostomia, dental caries,RN, mucositis, and trismus, were reviewed with the patient, and
trategies for prevention were discussed. The examination included aooth-by-tooth evaluation, with particular attention to the teeth in thearts of the jaws expected to receive a high dose (�50 Gy). Theeriodontal condition was evaluated, and teeth with mobility, signif-cant pocketing, furcation involvement, or advanced recession wereecommended for extraction. All patients underwent panoramic ra-iographs, which were supplemented in some patients by intraoraleriapical radiographs, if necessary, to evaluate for periapical ab-cesses, caries, and the periodontal condition. Teeth with nonrestor-ble caries or caries that extended to the gum line, teeth with large,ompromised restorations with significant periodontal attachment losspocketing �5 mm), and those with severe erosion or abrasion werextracted if they were in the parts of the jaws expected to receive aigh dose (the posterior mandible and maxilla ipsilateral to the tumornd the posterior mandible contralateral to the tumor). Teeth residingn the anterior mandible were not considered for extraction unless therimary tumor was in the oral cavity. Decisions about extraction wereignificantly affected by the patient’s competence and interest inerforming meticulous oral hygiene and by the patient’s past historyf dental service use. A more aggressive approach was made afterurgical oral reconstructions that inhibit oral hygiene or in patientsith trismus because of their negative impact on the prognosis for the
eeth. Extractions were performed as soon as possible after examina-ion, and primary closure was attempted when possible in the extrac-ion sites. The residual alveolar ridges were prepared for dentures byerforming any needed preprosthetic surgery such as alveoloplastynd torus removal. The start of RT was delayed by �14 days afterxtraction to allow for complete healing of the extraction site.
atient educationOral hygiene, including secular brushing and flossing, was re-
iewed with each patient. Daily use of high-concentrated fluorideel (1.1% neutral sodium fluoride) either in a fluoride carrier or byrush-on technique was also recommended, and a prescription wasiven to the patient. Written information and instructions wererovided, including oral care during and after RT, using theational Institute of Dental and Craniofacial Research (4) and
n-house supplemental material. r
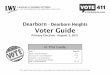
dditional dental proceduresFor all patients with dentitions heavily restored with metallic
estorations, radiation guards were used (Fig. 1). These were maderom polyvinyl siloxane putty (Reprosil, Caulk-Dentsply, York,A) and were intended to provide a 5-mm separation between theetallic restorations and the soft tissue, with the intention of
educing electron backscatter off the metal onto the soft tissue. Thease and catalyst of the putty were hand mixed and placed onosterior quadrant triple trays (Sullivan Schein, Melville, NY) andlaced in the mouth. Four wooden tongue blades were placedetween the upper and lower incisors, and the patient was asked tolose the mouth until the tongue blades were snug between thenterior teeth. After a setting time of about 5 min, the guards wereemoved and disinfected. They were trimmed to achieve a 5 mmhickness. The silicone was polished using a satin wheel (E.C.
oore, Dearborn, MI) and delivered to the patient with instruc-ions in use and care. The guards were in place during the simu-
ig. 1. Stents devised to reduce electron backscatter off dental metalestorations to the adjacent soft tissue. (a) After completion. (b) Inlace. If clinically required, teeth separation and tongue depressionan be achieved by inserting a tongue depressor during stent prepa-
ation or by making separate stents for the mandible and maxilla.
lp
R
ebrst(mIT3p
unifldtpia
rwaam
F
yRFwo
O
(othEtrdCaaGoBm2awe
t9lanyocitwmgawic
mp(OOptetpod
398 I. J. Radiation Oncology ● Biology ● Physics Volume 68, Number 2, 2007
ation to ensure that they were taken into account in the treatmentlanning dosimetry.
adiotherapyThe target definition and radiation techniques have been detailed
lsewhere (5–9). The planning target volumes (PTVs) were createdy uniform expansion of the clinical target volumes by 0.5 cm. Inecent years, the use of on-line imaging and daily correction of theystematic setup errors by the radiation therapists had been foundo reduce the systematic errors to a mean � SD of 1 � 1.5 mmunpublished data), and the PTV expansion has been reduced to 3m. Patients were treated until 2002 using static multisegmental
MRT (7, 8) and afterward by inverse-planned beamlet IMRT (9).he prescribed target dose was 70 Gy to the gross tumor PTV in5 fractions, and low- and high-risk clinical target volumes wererescribed a dose of 56–64 Gy at 1.6–1.8-Gy fractions.The optimization cost functions penalized the maximal mandib-
lar dose (�72 Gy), mean parotid gland (�26 Gy), and meanoninvolved oral cavity dose (�30 Gy). The oral cavity structurencluded the mandible, buccal mucosa, tongue, base of tongue,oor of mouth and palate, and its delineation has previously beenetailed (10). The noninvolved oral cavity was obtained by sub-racting the PTVs from the oral cavity volume. In all patients, thelans strived to address the target prescription goals while reduc-ng target dose inhomogeneity. In recent years, the planning goalslso included reduced doses to the swallowing structures (11, 12).
For the purposes of this study, all available treatment plans wereeviewed (148 plans, 84%). The mandibular dose distributionsere recalculated, and their dose–volume histograms were gener-
ted again for all patients, using the edge/octree model calculationnd the convolution/superposition model for patients treated withultisegmental IMRT and beamlet IMRT, respectively.
ollow-upAll patients were followed every 6–8 weeks during the first 2
ears after therapy and every 3–4 months afterward in both theadiation Oncology and the Head and Neck Surgery Clinics.ollow-up visits at the Hospital Dentistry/Oral Surgery Clinicere used when specific dental problems or suspected ORN werebserved at the other clinics.
RN definitionSeveral staging/grading systems have been suggested for ORN
2, 13, 14), taking into consideration the response to hyperbaricxygen (HBO) (14), the presence of pathologic fractures (13), andhe clinical presentation (2) or a combination of the above (15). Weave elected to use the Common Terminology Criteria for Adversevents, version 3.0 (15) for the grading of ORN in this series and
o retrospectively assign a grade according to the clinical andadiographic findings detailed in the patients’ charts. The ORNefinition and grading according to the Common Terminologyriteria for Adverse Events, version 3.0, is as follows: Grade 1,symptomatic, radiographic findings only; Grade 2, symptomaticnd interfering with function, minimal bone removal indicated;rade 3, symptomatic and interfering with daily life activities,perative intervention or HBO indicated; and Grade 4, disabling.ecause routine radiographs were not performed after therapy inost patients, we sought to identify those patients who had GradeORN or worse, defining Grade 2 as bony exposure observed for
t least two follow-up clinic visits (i.e., persisting for �6–8eeks). The follow-up notes from all clinics were reviewed for
ach patient to capture all possible cases of ORN.
RESULTS
Between March 1996 and March 2005, 188 patients werereated with IMRT in prospective trials. Of the 188 patients,
who had �6 months of follow-up (5 were lost to fol-ow-up at �6 months, 2 had died of pneumonia or trauma,nd 2 had died of lung metastases), and 3 patients who didot complete the RT course, were excluded from this anal-sis (none had ORN at last contact); thus, the total numberf patients evaluated in this study was 176. The patientharacteristics are summarized in Table 1. The large major-ty had oral or oropharyngeal primary tumors. All 20 pa-ients with laryngeal or hypopharyngeal cancer presentedith advanced neck lymphadenopathy and the posteriorandible was within, or close to, the lymphatic nodal tar-
ets. Of the 176 patients, 107 (61%) received primary RTnd 69 (39%) received postoperative RT. Also, 108 patientsere treated with concurrent chemotherapy: cisplatin based
n 22 patients, carboplatin based in 44, and a combination ofarboplatin and paclitaxel in 43 patients.
The pretherapy dental examination and treatment infor-ation were available for 174 patients (99%). Of these 174
atients, 16 (9%) were edentulous at presentation, and 63%) had had all their remaining teeth extracted before RT.f the 176 patients, 157 (89%) were dentulous during RT.f the 157 dentulous patients, 30 (19%) had undergoneretherapy mandibular teeth extractions (median number ofeeth removed, 2; range, 1–8). In almost all cases, thextractions were from the posterior parts of the mandiblehat were expected to receive high radiation doses. All otheratients (122 patients, 69%) were cleared to start RT with-ut extraction. Thirteen patients underwent post-RT man-ibular teeth extractions at the University of Michigan Den-
Table 1. Patient characteristics
Age (y)Median 55Range 29–86
Race (n)White 172African American 2Asian 2
Gender (n)Male 128Female 48
Tumor site (n)Oral cavity 32Oropharynx 120Larynx 7Hypopharynx 13Other 4
Tumor stage (AJCC) (n)I 2II 7III 40IVA 114IVB 12Recurrent disease 1
Abbreviation: American Joint Committee on Cancer.

tpGppdpwtt
am53drbtu1o�pda(tnpfdP
mw
mgtvccrts
mlh
ed
vbsbdes
h5aOrfsoia0�s
Fbv
Fi
399Lack of mandibular osteoradionecrosis in IMRT ● M. A. BEN-DAVID et al.
al Clinic. Six of these patients had teeth extracted from thearts of the mandible that had received a maximal dose �60y, two of these patients had received HBO before therocedure. Seven other patients had teeth extracted from thearts of the mandible that had received lower maximaloses. The median follow-up after the extractions in theseatients was 26 months. Some patients elected to proceedith post-therapy dental follow-up with their local dentist;
herefore, the information regarding any post-RT extrac-ions was not available for all patients.
The mandibular dose–volume histograms generated forll available treatment plans are summarized in Fig. 2. Theean � SD V50, V60, and V70 (percent volumes receiving
0 Gy, 60 Gy, and 70 Gy, respectively) was 62% � 18%,5% � 20%, and 6.5% � 5%, respectively. No significantifferences were found in the dose–volume histogram pa-ameters between patients treated with multisegmental oreamlet IMRT. The highest doses to �1% of the volume ofhe mandible are summarized in Fig. 3. The mean mandib-lar volume was 58.8 � 14.4 cm3, such that, on average, a% volume represented 0.59 cm3. More than 75% and 50%f the patients had a maximal dose of �65 Gy and 70 Gy to1% of the mandibular volume, respectively. The treatment
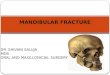
lans were characterized by dose gradients across the man-ible. The average gradient across the mandibular bone, inn axial plane that included the maximal dose, was 11 Gyrange, 1–27 Gy; median, 8 Gy). Figure 4 is of a patientreated with IMRT for Stage T3N1 squamous cell carci-oma of the right tonsil and posterior pharyngeal wall. Therimary PTV prescribed dose was 70 Gy, and the dosealloff across the mandible, perpendicular to the maximalose delivered to the inner mandibular plate adjoining theTV, was 21 Gy (72 Gy through 51 Gy).Dosimetry of the major salivary glands showed that theean doses to the contralateral and ipsilateral parotid glandsere, on average, 22 � 5 Gy and 53 � 7 Gy, respectively. The
ig. 2. Combined cumulative dose–volume histograms of mandi-le for all patients. Thick line represents mean dose volume, and
lertical lines represent standard deviation values.
ean doses to the contralateral and ipsilateral submandibularlands were, on average, 57 � 8 Gy and 65 � 7 Gy, respec-ively. These doses resulted in significant sparing of the sali-ary flows from the contralateral parotid glands, which in-reased continuously during the first 2 years after therapyompletion, as well as in improvements over time in patient-eported xerostomia. The results of the sialometry and xeros-omia-related symptoms in the patients participating in thistudy have been previously published (10, 16–18).
The median follow-up was 35 months (range, 6–129onths). Of the 148 patients still alive, 124 (70%) had at
east 2 years, 82 (55%) had at least 3 years, and 47 (32%)ad at least 5 years of follow-up.Twenty-seven patients (15%) developed locoregional dis-
ase recurrence. Of these 27 patients, 4 also had lungisease, and 4 had metastatic disease only.No case with ORN was identified (95% confidence inter-
al, 0–2%). One patient had a clinical suspicion of ORNecause of local pain; however, no mandibular bone expo-ure was observed and a panoramic X-ray demonstrated noone changes. One patient had asymptomatic transient man-ibular bone exposure diagnosed during routine clinicalxamination, but a panoramic X-ray of the jaws demon-trated no bone changes.
DISCUSSION
The incidence of ORN after RT for head-and-neck canceras declined in recent decades, from 11.8% before 1968 to.4% from 1968 to 1992, and decreased again after 1997 topproximately 3% (1). The reduction in the incidence ofRN occurred despite an increasing intensity of therapy in
ecent years, such as concurrent chemo-RT and alteredractionated RT, which are characterized by increased acuteide effects of therapy and occasionally by increased ratesf late sequelae (19, 20). The recent reduction in ORN risks reflected in our series, in which no case was observedmong 176 patients, with a 95% confidence interval of–2% (indicating that we cannot exclude a rate of ORN of2% in patient populations similar to the sample we have
tudied). ORN is a late sequel and some cases may require
ig. 3. Distribution of maximal doses to 1% of mandibular volumen individual patients.
ong follow-up; however, the large majority of events have

blfftoctrd
mGsaStcahtodlaNrlerw
mpatGbaoiurht
dtdtddodOfcmdIt
es of m
400 I. J. Radiation Oncology ● Biology ● Physics Volume 68, Number 2, 2007
een reported to occur within 2 years after therapy (21). Theow risk found in our series, in which 70% of patients wereollowed for �2 years, was likely not related to a shortollow-up. The reduction in the ORN rates can be attributedo the more conformal dose distributions, which spared partsf the mandible that would have receive a high dose hadonventional techniques been used, and to better prophylac-ic and on-going dental care. Of these two factors, dosimet-ic improvements and better dental care, it remains to beetermined which is the most important.Although some patients in our series received a highaximal dose to the mandible, with one-half receiving �70y, the mandibular volumes receiving a high dose were
mall (on average, the V70 was 6.5%, which translates tobout 4 cm3 of an average mandibular volume of 60 cm3).maller volumes receiving high doses might have reduced
he risk of bony exposure resulting from severe acute mu-ositis and leading to consequential long-term damage. Inddition to limiting the mandibular volumes receiving aigh dose, the dose distributions in this series were charac-erized by a falloff across the mandible, with the outer platef the mandible across the “hot spot” receiving a lowerose. This dose falloff might have implications regardingong-term effects on the local blood supply and the bone’sbility to withstand future trauma such as teeth extractions.ot only has the total dose been limited, but in patients
eceiving a single IMRT plan, the reduced total doses trans-ated into reduced fraction doses, such that the biologicallyquivalent doses delivered to the parts of the mandibleeceiving �70 Gy were lower than their nominal doses
Fig. 4. Axial computed tomography slices at levels of mademonstrating dose falloff from buccal to lingual surfac
ould imply. For example, in a patient with a maximal i
andibular dose of 70 Gy delivered to the inner mandibularlate and a gradient of 11 Gy across the mandible (theverage gradient in our series), delivered within 35 frac-ions, the nominal dose to the outer mandibular plate was 59y delivered at 1.68 Gy/fraction. This is thought to beiologically equivalent to 55 Gy at 2 Gy/fraction, assuminglow �/� ratio for late effects. In contrast, in a patient withral or oropharyngeal cancer treated with conventional RTn which the final boost is delivered to the gross diseasesing lateral opposed fields, the volume of the mandibleeceiving 70 Gy is expected to be much greater, with theigh dose delivered to the full thickness of the mandible athe same dose fraction prescribed to the tumor.
Parliament et al. (22) examined the mandibular doseistributions in a few IMRT cases and compared them withhose of standard RT. They concluded that IMRT offers aosimetric advantage if sparing the mandible is included inhe plan optimization (22). In our series, reducing the man-ible doses was achieved by constraints on the maximalose to the mandible and the mean dose to the noninvolvedral cavity (which encompassed the mandible). The meanose constraint for the oral cavity was enacted to reduceRN risk and mucositis, as well as xerostomia, which was
ound in an earlier study to be affected by the mean oralavity dose (which represented the potential damage to theinor salivary glands) (10). In addition to reduced mandibular
oses, the partial sparing of the salivary output achieved byMRT might have reduced the ORN risk through reducedeeth decay, a consequence of hyposalivation (23).
A clinical series concentrating on ORN in patients receiv-
lar angle (a) and rami (b) in patient with tonsillar cancerandible. PTV � planning target volume.
ndibu
ng IMRT has recently been reported by Studer et al. (24) In

tbecrncrdoeappGtdhdP
idfipttflpiThprrra
tAbalIhptl
Hbciehaow
ptumbtomocrtthetflarvdni
fturptcwsrd
401Lack of mandibular osteoradionecrosis in IMRT ● M. A. BEN-DAVID et al.
his series, detailed dosimetry of the mandible showed smallone volumes receiving high doses, similar to our experi-nce, and only 1 of 73 patients developed ORN. Otherlinical series of IMRT for head and neck cancer haveeported a very low incidence of ORN (25), and others didot include ORN as one of their late complications. It is notlear whether no cases were observed or ORN was notecorded in these series (26–29). However, IMRT and itsosimetric advantages might not guarantee a negligible riskf ORN. In a recent multi-institutional study of IMRT forarly oropharyngeal cancer conducted by the Radiation Ther-py Oncology Group (RTOG), an ORN rate of 6% (4 of 69atients) was reported (30). In that study (RTOG 00-22), therescribed high-risk PTV dose was 66 Gy in 30 fractions (2.2y/fraction), and the mandibular maximal doses were limited
o 72 Gy (31). No major dosimetric violation of the protocolose constraints occurred in the cases that developed ORN;owever, it is possible that the higher-than-standard fractionoses delivered to the part of the mandible adjacent to theTVs may have played a role in the cases of ORN.Another potential reason for the greater than expected
ncidence of ORN in RTOG 00-22 was the lack of stan-ardized prophylactic dental care in that study. Guidelinesor prophylactic dental care in this protocol were providedn a single sentence (“Any dental repairs must be made androphylaxis instituted before therapy”) (31). Less-than-op-imal prophylactic care was possible, especially in institu-ions treating small number of patients. This issue is re-ected by the lack of any details of protocol dental care inublications that have summarized the results of recentmportant clinical trials in head-and-neck cancer (32–37).his omission has been corrected in the most recent RTOGead-and-neck cancer protocols, which have included ap-endixes detailing the recommended dental care. Theseecommendations, if adhered to, are expected to reduce theates of ORN in multi-institutional studies to the very lowates reported by institutions treating large numbers of headnd neck cancer patients.
Controversy exists regarding some of the traditional den-al care paradigms associated with the prevention of ORN.n extensive discussion of these controversies has recentlyeen provided by Wahl (1). Extraction of healthy or restor-ble teeth before RT starts, practiced in previous years, is noonger recommended and was not practiced in our patients.n contrast, extraction of decaying and nonrestorable teethas been a cornerstone of our prophylactic dental care. Therevention of ORN by HBO in patients requiring post-RTeeth extraction is another contentious issue discussed at
ength by Wahl (1). Randomized studies of HBO vs. no mREFEREN
168–171.
BO before post-RT teeth extractions showed significantenefits for the HBO arms; however, the rates of ORN in theontrol arms seem to be greater than in other, nonrandom-zed studies. In our series, 2 patients requiring post-RT teethxtractions from parts of the mandible that had received aigh dose received HBO before extraction and 4 did not,nd none developed ORN. Another common practice is the usef prophylactic antibiotics before post-RT teeth extractions, forhich no firm evidence of efficacy has been found (1).Apart from these controversies, the principles of pre-RT
rophylaxis include extraction of decaying or nonrestorableeeth, strict dental care, including daily topical fluoride and these of dental protective stents to reduce scattered radiation offetal teeth restorations into the neighboring soft tissue, have
een the cornerstone of the dental preventive care practiced inhis series. We found the latter device (detailed in the “Meth-ds and Materials” section) to be effective in reducing acuteucositis in the soft tissue surrounding the restored teeth. The
verdosage due to backscatter off the high-gold alloy wasalculated to be 30% and 0 at 1 mm and 4 mm off the tooth,espectively (38).Therefore, a thickness of 4 mm is required forhe stent to minimize the increased dose to the soft tissue nearhe tooth. Reducing such “hot spots” around restored teeth mayave contributed to reduced mucosal damage causing bonyxposure and consequent ORN. In addition, the use of dailyopical sodium fluoride gel application by a custom-madeuoride carrier has markedly reduced the risk of caries (39)nd has been a routine practice in our institution. All patientseceived this device, and they were asked during follow-upisits whether they had continued to routinely use it. However,etails regarding the long-term compliance were not available,otwithstanding the costs of the prescribed fluoride and lack ofnsurance coverage of these costs for many patients.
CONCLUSION
No cases of ORN were observed in this series of IMRTor head and neck cancer. The potential factors contributingo the lack of this complication included reduced mandib-lar volumes receiving high doses, improved salivary flowates and associated improved oral health, and uniformrophylactic dental care. We do not know which factor washe most important. However, because of the reported oc-urrences of ORN in a multi-institutional study of IMRT inhich a uniform dental care protocol was not applied, we
uspect that the dental prophylactic care, as detailed in oureport, was a major factor in reducing ORN risk. Meticulousental care policies should be an integral part of the treat-
ent of head and neck cancer.CES
1. Wahl MJ. Osteoradionecrosis prevention myths. Int J RadiatOncol Biol Phys 2006;64:661–669.
2. Schwartz HC, Kagan AR. Osteoradionecrosis of the mandible:Scientific basis for clinical staging. Am J Clin Oncol 2002;25:
3. Mendenhall WM. Mandibular osteoradionecrosis. J Clin On-col 2004;22:4867–4868.
4. Sciubba JS, Goldenberg D. Oral complications of radiother-apy. Lancet Oncol 2006;7:175–183.
5. Eisbruch A, Foote RL, O’Sullivan B, et al. Intensity-modu-

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
33
3
3
3
3
3
3
3
402 I. J. Radiation Oncology ● Biology ● Physics Volume 68, Number 2, 2007
lated radiation therapy for head and neck cancer: Emphasis onthe selection and delineation of the targets. Semin RadiatOncol 2002;12:238–249.
6. Eisbruch A, Marsh LH, Dawson LA, et al. Recurrences nearbase of skull after IMRT for head-and-neck cancer: Implica-tions for target delineation in high neck and for parotid glandsparing. Int J Radiat Oncol Biol Phys 2004;59:28–42.
7. Eisbruch A, Marsh LH, Martel MK, et al. Comprehensiveirradiation of head and neck cancer using conformal multiseg-mental fields: Assessment of target coverage and noninvolvedtissue sparing. Int J Radiat Oncol Biol Phys 1998;41:559–568.
8. Fraass BA, Kessler ML, McShan DL, et al. Optimization andclinical use of multisegment intensity-modulated radiationtherapy for high-dose conformal therapy. Semin Radiat Oncol1999;9:60–77.
9. Vineberg KA, Eisbruch A, Coselmon MM, et al. Is uniformtarget dose possible in IMRT plans in the head and neck? IntJ Radiat Oncol Biol Phys 2002;52:1159–1172.
0. Eisbruch A, Kim HM, Terrell JE, et al. Xerostomia and itspredictors following parotid-sparing irradiation of head-and-neck cancer. Int J Radiat Oncol Biol Phys 2001;50:695–704.
1. Eisbruch A, Schwartz M, Rasch C, et al. Dysphagia and aspira-tion after chemoradiotherapy for head-and-neck cancer: Whichanatomic structures are affected and can they be spared byIMRT? Int J Radiat Oncol Biol Phys 2004;60:1425–1439.
2. Feng F, Kim HM, Lyden T, et al. IMRT aiming at reducingdysphagia: Early dose-volume-effect relationships for the swal-lowing structures. Int J Radiat Oncol Biol Phys 2007; In press.
3. Epstein JB, Wong FL, Stevenson-Moore P. Osteoradionecro-sis: Clinical experience and a proposal for classification.J Oral Maxillofac Surg 1987;45:104–110.
4. Marx RE. Osteoradionecrosis: A new concept of its patho-physiology. J Oral Maxillofac Surg 1983;41:283–288.
5. http://ctep.canchttp://ctep.cancer.gov/forms/CTCAEv3.pdf.http://ctep.cancer.gov/forms/CTCAEv3.pdf.
6. Lin A, Kim HM, Terrell JE, et al. Quality of life followingparotid-sparing IMRT of head and neck cancer: A prospectivelongitudinal study. Int J Radiat Oncol Biol Phys 2003;57:61–70.
7. Jabbari S, Kim HM, Feng M, et al. Quality of life andxerostomia following standard vs. intensity modulated irradi-ation: A matched case-control comparison. Int J Radiat OncolBiol Phys 2005;63:725–731.
8. Meirovitz A, Murdoch-Kinch CA, Schipper M, et al. Scoringxerostomia by physicians vs. patients after IMRT of head andneck cancer. Int J Radiat Oncol Biol Phys. 2006;66:445–453.
9. Starr S, Rudat V, Stuetzer H, et al. Intensified hyperfraction-ated accelerated radiotherapy limits the additional benefit ofsimultaneous chemotherapy: Results of a multicentric ran-domized German trial in advanced head-and-neck cancer. IntJ Radiat Oncol Biol Phys 2001;50:1161–1171.
0. Robbins K. Barriers to winning the battle with head-and-neckcancer. Int J Radiat Oncol Biol Phys 2002;53:4–5.
1. Reuther T, Schuster T, Mende U, et al. Osteoradionecrosis ofthe jaws as a side effect of radiotherapy of head and necktumour patients—A report of a thirty year retrospective re-view. Int J Oral Maxillofac Surg 2003;32:289–295.
2. Parliament M, Alidrisi M, Munroe M, et al. Implications ofradiation dosimetry of the mandible in patients with carcino-mas of the oral cavity and nasopharynx treated with intensitymodulated radiation therapy. Int J Oral Maxillofac Surg 2005;34:114–121.
3. Kielbassa AM, Hinkelbein W, Hellwig E, et al. Radiation-
related damage to dentition. Lancet Oncol 2006;7:326–335.4. Studer G, Studer SP, Zwahlen RA, et al. Osteoradionecrosis ofthe mandible: Minimized risk profile following intensity-mod-ulated radiation therapy (IMRT). Strahlenther Onkol 2006;182:283–288.
5. de Arruda FF, Puri DR, Zhung J, et al. Intensity-modulatedradiation therapy for the treatment of oropharyngeal carci-noma: The Memorial Sloan-Kettering Cancer Center experi-ence. Int J Radiat Oncol Biol Phys 2006;64:363–373.
6. Lee N, Xia P, Fischbein NJ, et al. Intensity modulated radia-tion therapy for head and neck cancer: The UCSF experiencefocusing on target volume delineation. Int J Radiat Oncol BiolPhys 2003;57:49–60.
7. Chao KSC, Ozygit G, Blanco AI, et al. Intensity modulatedradiation therapy for oropharyngeal carcinoma: Impact on tumorvolume. Int J Radiat Oncol Biol Phys 2004;59:43–50.
8. Kam MKM, Teo PML, Chau RMC, et al. Treatment of naso-pharyngeal carcinoma with intensity modulated radiotherapy:The Hong Kong experience. Int J Radiat Oncol Biol Phys2004;60:1440–1450.
9. Lauve A, Morris M, Schmidt-Ullrich R, et al. Simultaneousintegrated boost intensity modulated radiotherapy for locallyadvanced head and neck squamous cell carcinoma: II—Clin-ical results. Int J Radiat Oncol Biol Phys 2004;60:374–387.
0. Eisbruch A, Harris J, Garden, et al. Phase II multi-institutionalstudy of IMRT for oropharyngeal cancer (RTOG 00-22): Earlyresults. [Abstract]. Int J Radiat Oncol Biol Phys. 2006;66(suppl.):546.
1. www.rtog.org/members/active.html.2. Fu KK, Pajak TF, Trotti A, et al. A Radiation Therapy
Oncology Group (RTOG) phase III randomized study to com-pare hyperfractionation and two variants of accelerated frac-tionation to standard fractionation radiotherapy for head andneck squamous cell carcinomas: First report of RTOG 9003.Int J Radiat Oncol Biol Phys 2000;48:7–16.
3. Dische S, Saunders M, Barrett A, et al. A randomised multi-centre trial of CHART versus conventional radiotherapy inhead and neck cancer. Radiother Oncol 1997;44:123–136.
4. Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concur-rent radiotherapy and chemotherapy for high-risk squamous-cellcarcinoma of the head and neck. N Engl J Med 2004;350:1937–1944.
5. Brizel DM, Albers ME, Fisher SR, et al. Hyperfractionatedirradiation with or without concurrent chemotherapy for lo-cally advanced head and neck cancer. N Engl J Med 1998;338:1798–1804.
6. Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradia-tion with or without concomitant chemotherapy for locally ad-vanced head and neck cancer. N Engl J Med 2004;350:1945–1952.
7. Ang KK, Trotti A, Brown BW, et al. Randomized trial ad-dressing risk features and time factors of surgery plus radio-therapy in advanced head-and-neck cancer. Int J Radiat OncolBiol Phys 2001;51:571–578.
8. Reitemeier B, Reitemeier G, Schmidt A, et al. Evaluation of adevice for attenuation of electron release from dental restora-tions in a therapeutic radiation field. J Prosthet Dent 2002;87:323–327.
9. Horiot JC, Schraub S, Bone MC, et al. Dental preservation inpatients irradiated for head and neck tumours: A 10-year expe-rience with topical fluoride and a randomized trial between two
fluoridation methods. Radiother Oncol 1983;1:77–82.