Embed Size (px)
Citation preview

Laparoscopic Pyloromyotomy
George W. Holcomb, III, M.D., MBAChildren’s Mercy Hospital
Kansas City, Missouri

Preoperative EvaluationPyloric Stenosis
• Non-bilious emesis
• 2-8 wks of age
• Male:Female 4:1
• Dehydration/Metabolic Alkalosis
• Jaundice 10%
• Ultrasound - length - > 14 mm
thickness - > 4 mm

Indications for Surgery
• Presence of pyloric stenosis
• Need to correct electrolyte abnormalities and dehydration

Patient Positioning
• Baby placed across operating table
• Table tilted toward surgeon
• Monitor in front of surgeon
• Assistant/camera holder to right of surgeon
• Scrub nurse opposite assistant
• Red rubber catheter in stomach

Equipment
• 5 mm umbilical cannula – 4 mm, 70o telescope
• Arthroscopy knife (Linvatec)
• Pyloric spreader
• Atraumatic grasping forcep

Tips and Tricks
• Set knife at 2 mm depth
• Incise serosa and muscle to 2 mm
• Sheath knife and use sheath to bluntly separate muscle
• Insert pyloric spreader –Gently separate pyloric muscle fibers as you view the submucosa
• Measure length – know length of stenosis on ultrasound
• Distend stomach with 45-60 cc air
• Place omentum over myotomy

Laparoscopic Pyloromyotomy

Alternative Approaches
• RUQ or upper midline incision
• Circumumbilical incision

Complications
• Incomplete myotomy
• Mucosal perforation
• Wound infection

Post-operative Management
• Advance diet per protocol
• Tylenol for pain
• Feed Like A Pyloric (FLAP) NPO for 2 hours Pedialyte 30cc PO Q 2h X 2, Formula 30cc ½ str Q 2h X 2, Formula 30cc full str Q 2h X 2, Formula 45cc full str Q 3h ad lib

Recent Literature Reports

Retrospective Review – Laparoscopic, Circumumbilical and RUQ Approaches
Intraoperative and Postoperative Data Comparison
Characteristic LAP (n=51)
RUQ (n=190)
UMB (n=49)
p Value
Operating room time (min)
71 ± 13□ 74 ± 14† 83 ± 15‡ <0.0001
Operative time (min) 25 ± 9□ ‡ 32 ± 9† 42 ± 11 <0.0001
Postoperative length of stay (d)
1.8 ± 1 1.6 ± 1 1.8 ± 1 0.26
Time to ad lib feedings (h)
26 ± 22 22 ± 14 26 ± 19 0.07
Conversion rate (%) 2/51 (4)
JACS 201:66-70, 2005JACS 201:66-70, 2005

Retrospective Review – Laparoscopic, Circumumbilical and RUQ
Approaches
Intraoperative and Postoperative Data Comparison
Characteristic LAP (n=51)
RUQ (n=190)
UMB (n=49)
p Value
Complication rate (%) 4 10 14 0.23
Mucosal perforation 0 3 3
Wound infection 0 11 3
Wound dehiscence 1 1 1
Incisional hernia 0 2 0
Persistent emesis 1 2 0
JACS 201:66-70, 2005JACS 201:66-70, 2005

An Effective Pyloromyotomy Length In Infants Undergoing Laparoscopic
Pyloromyotomy
Daniel J. Ostlie, MD, Charles E. Woodall III, MD, Kerri R. Wade, RN, Charles L. Snyder, MD, George K. Gittes, MD, Ronald J. Sharp, MD, Walter S. Andrews, MD, J. Patrick
Murphy, MD, George W. Holcomb III, MD, MBA
Children’s Mercy Hospitals and ClinicsKansas City, Missouri
Surgery 136:827-32, 2004Surgery 136:827-32, 2004

Purpose
To evaluate whether there is an
effective pyloromyotomy length that
can prevent the development of an
inadequate myotomy

ResultsOctober 1999 – October 2003
• 171 infants
• Mean age – 5.2 wks (± 2.8)
• Ultrasound
▲ Mean length– 19.52 ± 2.8 mm
▲ Mean thickness– 4.29 ± 0.7 mm
Surgery 136:827-32, 2004Surgery 136:827-32, 2004

Results• Operative time
• 23.5 (± 8.3) min
• Length of myotomy• 1.94 (± 0.21) cm
• Standardized feeding protocol – 33 pts (19%) experienced at least one feeding setback
• Hospitalization • Postoperative–32.6 (±27.7) hrs
• Total – 53.2 (± 38.7) hrs
Surgery 136:827-32, 2004Surgery 136:827-32, 2004

Results171 Infants
• No mucosal perforations
• No gastric or duodenal injuries
• No inadequate pyloromyotomies
Surgery 136:827-32, 2004Surgery 136:827-32, 2004

Conclusions
• Laparoscopic approach for pyloromyotomy is safe and effective
• The length of the myotomy can be measured effectively
• A pyloromyotomy length of approximately 2 cm is effective in relieving the pyloric obstruction
Surgery 136:827-32, 2004Surgery 136:827-32, 2004

Prospective Randomized Trial of Laparoscopic vs Open
Fundoplication

Open Versus Laparoscopic Pyloromyotomy For Pyloric Stenosis: A Prospective
Randomized Trial
The Center for Prospective Clinical Trials
Children’s Mercy Hospital Kansas City, MO
Shawn D. St. PeterGeorge W. Holcomb III
Casey M. CalkinsWalter S. AndrewsJ. Patrick Murphy Charles L. SnyderRonald J. Sharp George K. GittesDaniel J. Ostlie

We conducted the first large prospective
randomized controlled trial investigating the
role of laparoscopy in treating pyloric stenosis
Introduction
Ann Surg 244:363-370, 2006Ann Surg 244:363-370, 2006

MethodsSample Size
• Mean operative times were utilized from retrospective data within our institution
• Power = 0.80 and α = 0.05
• 60 patients in each arm
• Potentially significant complications occur infrequently
• Therefore, a recruitment goal of 100 patients in each arm was established

Assignment
• Individual unit randomization sequence
• Non-stratified
• Blocks of 10
• Allotment obtained from randomization sequence after permission form signed

Interventions
• Operations were performed by 7 pediatric surgeons at a single institution
• The surgical resident (fellow) or on-call surgeon performed the operation
• Allotment had no influence on which surgeon performed the operation

InterventionsOpen Pyloromyotomy
• 2-3 cm incision, transverse right upper quadrant or upper midline
• Pylorus exteriorized through incision
• Incision in pylorus with #15 blade
• Muscle spreader used to complete myotomy

InterventionsLaparoscopic Pyloromyotomy
• 5 mm port in umbilicus
• 2 stab incisions • right and left upper quadrants
• 3 mm instruments • Grasper in surgeon’s left hand• Blade followed by spreader in surgeon’s right
hand

ManagementDiet Orders
• Standard diet order sets for both groups• 2 feedings of Pedialyte® • 2 feedings of ½ strength formula/breast milk• 2 feedings of full strength formula/breast
milk• Resume home regimen
• Criteria for stopping feeds outlined in order set
• Discharged when home diet tolerated

ManagementPain Control
• Acetaminophen (10mg/kg) PO/PR every 4 hours as needed for pain
• No patients received narcotics

Data Collection
• Age• Weight• Electrolytes on presentation• Ultrasound measurements of the pylorus• Operating time• Time to complete advancement of diet• Number of episodes of post-operative emesis• Number of doses of tylenol (10mg/kg)• Length of post-operative hospitalization• Complications

Statistics
• Continuous variables were compared using an independent sample, 2-tailed Student’s t- test
• Discrete variables were analyzed with Fisher’s exact test
• Significance was defined as P value < of 0.05
• All measures evaluated on intention-to-treat basis

ResultsUpon Presentation
OPEN (n = 100) LAP LAP ((n = 100))
Age (weeks) 5.24 +/- 0.25 5.33 +/- 0.22
P ValueP Value
Thickness (mm) 4.17 +/- 0.08 4.16 +/- 0.09 Length (mm) 19.51 +/- 0.27 19.38 +/- 0.27
Cl - (mmol/L) 99.36 +/- 0.78 99.76 +/- 0.79
HCO3 -(mmol/L) 28.18 +/- 0.51 27.86 +/- 0.49
(Mean +/- S.E.) (Mean +/- S.E.)
0.77
0.88
0.74
0.72
0.65

ResultsOutcomes
OPEN OPEN ((n = 100)) LAP (n = 100) P ValueP Value
OR time (mins) 19:28 +/- 0.60 19:34 +/- 0.78
Emesis (#) 2.61 +/- 0.27 1.84 +/- 0.23 Full Feeds (hrs) 21:01 +/- 2.16 19:30 +/- 1.46
LOS (hrs) 33:10 +/- 1.63 29:38 +/- 1.69
Tylenol (doses) 2.23 +/- 0.18 1.59 +/- 0.16
(Mean +/- S.E.) (Mean +/- S.E.)
0.93
0.05
0.43
0.12
0.01

ResultsComplications
• 1 mucosal perforation in the open group
• 1 incisional hernia in the open group
• 1 laparoscopic case was converted to open
• 4 wound infections in the open group compared to 2 wound infections in the laparoscopic group (P = 0.68)

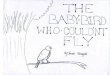
ResultsCosmetic Outcome
OPENOPEN LAPLAP

Conclusions
• Operative approach for pyloromyotomy has no significant influence on operating time or length of recovery
• Laparoscopic pyloromyotomy results in significantly less post-operative discomfort
• Fewer episodes of emesis and doses of tylenol
• Laparoscopic pyloromyotomy results in obvious cosmetic benefits

Conclusions
• All surgeons confirmed they will perform the pyloromyotomy with the laparoscopic approach

? ? ?