Embed Size (px)
Citation preview

5 2
©
2 0 0 3 B J U I N T E R N A T I O N A L | 9 2 , S U P P L E M E N T 1 , 5 2 – 5 7
Blackwell Science, LtdOxford, UKBJUBJU International1465-5101BJU International91
Supp Article
LAPAROSCOPY IN PAEDIATRIC UROLOGYC. PETERS
Laparoscopy in paediatric urology: adoption of innovative technology
C. PETERS
Department of Urology, Children’s Hospital, Harvard Medical School, Boston, MA, USA
contrasted with that in paediatric urological laparoscopy. Suggestions as to how this developing field can be evaluated will be proposed for consideration.
BACKGROUND
The early aspects of paediatric urological laparoscopy are well described [1] and preceded applications in adult urology with the use of this technology for diagnostic studies of the undescended testis [2]. This was its principle use from 1976 to 1992, when the first tentative steps towards true surgical laparoscopy were reported [3–7]. These followed adult precedents, e.g. nephrectomy, but diverged with laparoscopic orchidopexy and antireflux surgery, for which there were no common adult counterparts. The initial acceptance was tentative and followed a generalized decline in the reported use of laparoscopic methods in adult urology. This is well illustrated by publication figures for all laparoscopic reports in the urological literature (Fig. 1a). During this time there were a few reports of surgical techniques and small series reports showing the feasibility of differing paediatric procedures, including pyeloplasty [8], antireflux surgery[7], partial nephrectomy [3] and augmentation cystoplasty [9].
Perhaps the most telling pattern can be seen in antireflux surgery, which was approached with enthusiasm, and was technically feasible [7,10,11]. Nonetheless, experienced practitioners felt it was simply too time-consuming and difficult to be considered viable; its use faded rapidly. Pyeloplasty was similarly felt to be the paediatric urologist’s ‘laparoscopic cholecystectomy’, but the technical challenge of efficient suturing effectively limited this procedure to a few experienced, and perhaps obstinate, surgeons. These procedures were clearly meeting a technological barrier, and that was laparoscopic suturing.
Concurrent with these struggles there was steady progress in increasingly complex
extirpative surgery, primarily in the area of laparoscopic and retroperitoneal nephrectomy [12–15]. This progress was made on several fronts, including operative time, safety and decreasing age of the patient. This progress was also supported by improvements in technology, with smaller cannulae for smaller instruments, better tissue-handling devices such as small clip appliers and the harmonic scalpel, all of which are currently available in 5 mm sizes and adaptable to any infant. Partial nephrectomy became a readily performed procedure in experienced centres and this has continued [16].
A major step was the development of techniques to carry out these procedures retroperitoneally. A frequent charge levelled against the early laparoscopic surgeons in paediatric urology was that previously retroperitoneal were being converted into transperitoneal procedures, and that this would inevitably lead to intestinal adhesions and small bowel obstruction [17]. This charge was not always made in a collegial atmosphere of academic discourse, despite the absence of any reports of late intestinal adhesive disease, and the objective reports of the paucity of adhesions after intraperitoneal laparoscopic surgeries in children [18]. Nevertheless, the retroperitoneal approach has always been the natural one for the renal surgeon and as these methods developed in adult practice, they were applied to children with good results. Several reports documented the adaptability of several exposure methods in children of various ages and conditions. There seemed to be no major risks, albeit the case experience was limited. As this experience developed, for the experienced practitioner retroperitoneal exposure was far better than transperitoneal in most cases. At present, the retroperitoneal approach is the standard for all but the very rare situation where an intraperitoneal procedure is needed (e.g. an orchidopexy). Even then, the transperitoneal approach is more difficult because of the exposure and risks of inadvertent bowel injury.
INTRODUCTION
The adoption and widespread application of new technologies in medicine has become increasingly common in recent years. As with so many other technologies, novel medical technologies appear at a rapid pace and demand rapid acceptance or dismissal. Some of this is fuelled by the artificial urgency of commercial forces behind these often-expensive technologies, but it has also become a hallmark of modern life, best typified by the development of computer technology. It is almost as if an idea is not worth serious consideration if it is not being marketed with urgency. It becomes a significant challenge to discern which technologies are truly worthy of the investment of time, money and intellectual commitment. There is strong pressure of priority, ‘being first’, in new areas in medicine, both from academic and commercial perspectives. This challenge can be seen in the adoption of laparoscopic surgical technology in paediatric urology, and practitioners are currently faced with the need to critically assess the current and future role of this technology. The tools to do so are limited as there has been very little in the way of prospective randomized controlled trials (RCTs) in any application of this surgical approach. There has been a steady, if not exponential, growth in publications related to paediatric urology, similar to that being experienced in adult laparoscopic urological surgery. New aspects of the technology will shape its future uses, particularly robotic technology, yet the same questions will apply. How can the value and role of this technology be assessed objectively? What are the responsibilities of the practitioner to his/her patients in terms of interpreting and using these technologies? What should the basic criteria be for acceptance or rejection of a technology in paediatric urology?
In this paper I review the development of paediatric urological laparoscopic surgery and examine the evidence available for assessing its role in this field. Publication patterns of other new technologies in medicine are

L A P A R O S C O P Y I N P A E D I A T R I C U R O L O G Y
©
2 0 0 3 B J U I N T E R N A T I O N A L
5 3
In parallel with the development of retroperitoneal techniques has been the gradual emergence of reconstructive procedures in paediatric urological laparoscopy. In this area a unique concept has appeared that has yet to achieve full application, the intentional integration of open and laparoscopic methods in the same procedure. These might by considered ‘hybrid’
laparo-endoscopic procedures, where laparoscopy is used to mobilize a portion of the gastrointestinal tract, e.g. the appendix, to permit its integration with the reconstructive procedure through a much smaller incision. Jordan and Winslow [19] originally described a case report of this approach, but Docimo
et al.
[20] developed it with a variety of applications. These were generally
mobilizations of the appendix to create a continent catheterizable stoma, or Mitrofanoff, but also included other gastrointestinal segments. Although completely laparoscopic reconstructive procedures were described, including a gastrocystoplasty [9], the practicality was limited because of the difficulty of suturing. The advantages of these methods may be significant by avoiding a large abdominal incision, often in patients with limited pulmonary reserve who would be at greater postoperative pulmonary risk. With the advent of robotically assisted methods, more complex reconstruction may become more practical, including mobilization, harvesting and reconstruction of various elements of the gastrointestinal and urinary tract.
TEACHING AND EDUCATION
An integral aspect of the development and acceptance of new surgical techniques, particularly those that require the acquisition of new skills by the practitioner, is the means by which these technologies may be taught. Laparoscopy in paediatric urology is restricted by the same educational challenges as other laparoscopic fields, e.g. there being relatively little experience to draw from, a lack of similar procedures to use as a starting point, relatively few experienced instructors, and the difficulty of conveying the needed information while the work is being done and viewed through a video screen. These challenges can be met, and to a large extent are being met, but paediatric urological laparoscopy has had some benefit from a unique characteristic that facilitates the learning of more complex skills. The use of laparoscopy for diagnostic purposes provides an excellent introduction to fundamental laparoscopic skills, e.g. port placement, using and interpreting the two-dimensional images in a real patient, and the basic manoeuvres to surgically manipulate tissues. Diagnostic laparoscopy for cryptorchidism provides this experience without needing operative skills in laparoscopy. The diagnostic information may be used before open surgery or for the first step of operative laparoscopic orchidopexy. The transition may be developed at the practitioner’s speed and comfort level. This serves to make learning less difficult and intimidating. Following this, there are procedures of graded complexity. These techniques provide the developing practitioner with increasingly challenging
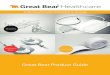
FIG. 1.
a,
Literature citations inthe major urological
publications (
BJU Int
,
J Urol
and
Urology
) relating tolaparoscopy (1985–2001)
showing a biphasic patternof diffusion, with a decline in
apparent activity afteran initial rapid diffusion;
the activity has not yetreached a peak;
b,
Reportsrelating to laparoscopic
cholecystectomy from 1981to 2001. A rapid period of
diffusion followed by aslow decline suggests
maturation of thetechnology. The first RCTs
were not reported untilabout 1991, near the peak
of publication activity;
c,
Published reports of alllaparoscopy (green circles)
and RCTs (red squares)relating to laparoscopy
plotted on a logarithmicscale, from 1985 to 2001.
The number of RCTs barelyregisters compared with the
number of general reports,and has lagged far behind interms of time of occurrence.
0
500
1000
1500
2000
2500
3000
3500
1980 1985 1990 1995 2000
0 100
200
300
400
500
600
700
800
1981 1986 1991 1996 2001Year
0
50
100
150
200
1985 1990 1995 2000
Year
a
b
c
Repo
rts
Repo
rts
Repo
rts
Year

C . P E T E R S
5 4
©
2 0 0 3 B J U I N T E R N A T I O N A L
operations to develop skills but with no substantial risks to the patient. Such a progression would include simple nephrectomy, to partial nephrectomy, to pyeloplasty, to ureteroplasty for VUR, and then to more complex reconstructions. Paediatric urology has a unique advantage in the intrinsic nature of its procedures to facilitate the progressive acquisition of laparoscopic skills.
RCTS
As a new technology is introduced and its applications develop, the issue of its value is inevitably and appropriately raised. This would seem to be a readily examined question, and indeed the assessment of healthcare outcomes is a rapidly developing new technology in and of itself [21,22]. Ideally the new technology would be introduced and pass through a period of early development, with fairly rapid assessment based on objective measurements of comparative outcomes relative to the older technologies being replaced. It would then be deemed of value or not, and if the latter, fade away. This is not the usual pattern, and indeed in surgical areas, this is rarely experienced. In laparoscopic surgery, the use of any real prospective controlled trials is a recent and sparse event. A notable study compared laparoscopic cholecystectomy with mini-cholecystectomy in a truly prospective RCT [23]. That study showed no postoperative benefit for laparoscopic cholecystectomy, even though by this time it was an entrenched surgical technology that was not threatened with obsolescence (Fig. 1b). Challenges to the study were intense [24,25] and included questions as to the high rate of conversion to
open surgical methods, the number of cases undertaken by each practitioner, and various other issues that might suggest the conclusions to be less than valid. Other controlled studies (albeit no other blinded studies) have shown benefits clearly attributable to laparoscopic cholecystectomy. It is difficult to know how to interpret a study that challenges what has become, de facto, the standard of care.
In paediatric urological applications of laparoscopy RCTs are almost unknown. Some attempts have been made to assess the use of diagnostic laparoscopy for cryptorchidism [26] (and Casale A, personal communication, AAP Section on Urology, 1999). Two such studies have been reported and both have shown no benefit for laparoscopic diagnosis in managing the impalpable testis. The outcomes assessed were operative time and cost. This conclusion is inconsistent with a large body of literature and practice, but deserves consideration, as these studies were prospective, with an attempt at randomization. In both there was no attempt to integrate the results of diagnostic laparoscopy with laparoscopic orchidopexy, inherently limiting the value of the mode of diagnosis, as laparoscopic diagnosis intrinsically sets the stage for operative laparoscopic orchidopexy. These studies included few patients and there were no cases of extreme testicular positions that would be difficult, if not impossible, to be diagnosed with open surgical techniques. Such testicular positions have been reported in the larger series of diagnostic laparoscopy and clearly occur, but unusually. The importance of these patients may be difficult to capture in a limited series. Anecdotally, the value of diagnostic laparoscopy is clear, but not
necessarily confirmed objectively. How then should we determine if it offers true clinical value to the patients?
It is logical to ask if formal studies of this sort are valuable in areas of developing surgical technologies [21]. The pattern of experience is that they are generally late in the development of the technology, and may not influence its application. Based upon published reports, the use of RCTs in laparoscopy lags many years behind the application of the technology (Fig. 1c). While this may be appropriate, it is possible that RCTs would have no value in changing practice patterns in an established technology. Similarly, if they are performed too early in the development or maturation of a technology, the relevant issues may not be clear and may be missed by these studies, which may inappropriately condemn valuable procedures. In minimally invasive technology, the constraints against the conduct and clinical application of RCTs are significant and unique. They are not intended to introduce a novel treatment concept, but to reduce the morbidity of a procedure. The differential outcomes, then, are based upon morbidity. Efficacy is required to be identical. Measuring morbidity is inherently difficult; the focus of the measure can influence the outcome. If the principle advantage of a laparoscopic procedure is to shorten recovery time overall, and only the cost of hospital stay is assessed, this benefit will not be detected. In paediatric practice, the issue of returning to work is not directly relevant, but may be applicable to a parent who must care for a convalescing child. In smaller children the effect of a given surgical intervention seems less than in older children, so the relative value of a laparoscopic approach may be age-
TABLE 1
Challenges in assessing paediatric laparoscopic procedures
Challenge Possible solutionsWhen to perform a trial in developing a new technology Use two time-points for the trial and compare differences as a function of timeEffect of return to normal activity Scales including age-appropriate activity assessmentEffect on caregiver Parental assessmentFew patients Multicentred trialsRestrictions on studies in children Work with Institutional Review BoardHow to measure invasiveness during and after surgery Multifactorial assessments: pain, medication, return to normal activityEffect may be age-dependent Age-matched study designDifficulty blinding surgical interventions Uncertain utility and need of single-blind methodsDifficulty randomizing paediatric surgical trials Parental selectionInfluence of specific surgeon Stratified by surgeon

L A P A R O S C O P Y I N P A E D I A T R I C U R O L O G Y
©
2 0 0 3 B J U I N T E R N A T I O N A L
5 5
dependent. The most useful RCTs are blinded, which is extremely difficult in laparoscopic studies. It has been done, in the laparoscopic cholecystectomy vs mini-cholecystectomy study, using identical bandages in all patients. These bandages were large, and one could question whether there might be an effect of such a bandage on the patient, indicating they had a ‘bigger’ operation, leading to a greater sense of surgical impact, i.e. almost a ‘reverse placebo’ effect. In young children this might be less of an effect. The patient’s response to smaller or larger bandages might also be seen as part of the surgical effect. It is indeed a subjective response that is being measured and any practitioner recognises the wide variation in patient response to any surgical event.
A distinction is often drawn between efficacy and effectiveness, which contrasts with the potential efficacy of a new technology in the hands of an expert, with the overall effectiveness of a technology in general use [27]. Early in laparoscopy, there was often the observation that a certain procedure was useful only in the ‘magic hands’ of a few highly focused and experienced surgeons.
ALTERNATIVES TO RCTS
There is recognition that traditional RCTs may not always be completely appropriate to surgical assessment, for a variety of reasons, as suggested above [22]. In place of these, the importance of carefully conducted prospective case-control and observational studies should be recognized and encouraged. These may provide a more secure foundation upon which to establish a formal RCT, and permit adequate recruitment. It may be that in some cases, the beneficial effects of a new technology are sufficiently compelling that a formal RCT is not needed. Expediency cannot be an excuse for scientific laxity, but clinical pragmatism is a relevant factor.
SECONDARY EFFECTS OF LAPAROSCOPY ON SURGICAL PRACTICE
A unique effect of the development of laparoscopic surgical techniques has been to modify some open surgical techniques, either in their morbidity or in the selection of approaches. Seemingly in response to laparoscopic cholecystectomy, the mini-cholecystectomy emerged [23] and in a direct, randomized blinded study was compared with laparoscopic cholecystectomy. There
was no demonstrable difference in terms of postoperative analgesia, recovery and return to work between them. In prostate surgery, for example, with the advent of laparoscopic lymphadenectomy, perineal prostatectomy enjoyed a resurgence in popularity. The mini-prostatectomy incision also gained popularity as a consequence of the pressure of laparoscopic techniques. Of course this is all to the benefit of the patient, yet contradicted the basic surgical tenet of effective exposure. In paediatric urology, several authors reported nephrectomy through increasingly smaller incisions, but in one of these reports a disadvantage of this tendency was identified when an inadvertent appendectomy was performed instead of a nephrectomy! [28]. As the concept of laparoscopic antireflux surgery emerged using the Lich-Gregoir approach, our unit, for example, began using this method for open surgery, anticipating its application with laparoscopic methods. That change has only occurred recently [29], in part through the recognition that this open method was of such limited morbidity that it became difficult to justify the challenging laparoscopic approach, despite its advancement in other procedures. The reduced length of stay was also promoted for open surgery, which of course limited the apparent benefits of laparoscopic methods. Laparoscopy has therefore fostered (along with other factors) a reduction in morbidity and hospital stay also for open surgery, a unique benefit.
DEVELOPING TECHNIQUES
During the development of laparoscopic methods in urology, a significant criticism of laparoscopic renal procedures was that formerly retroperitoneal procedures had been converted to transperitoneal ones. This approach incurs risks of injury to intraperitoneal organs and a delayed risk of intestinal adhesive disease with bowel obstruction. In principle this is a real concern, yet the clinical significance is unclear. There have certainly been inadvertent injuries to intraperitoneal organs during laparoscopic surgery, as there have been, e.g. with retroperitoneal procedures such as percutaneous nephrolithotomy. This is probably a product of both the approach and the learning required for laparoscopic surgery. The risk of intestinal adhesive disease is difficult to assess accurately. There is evidence that there is little development of intraperitoneal adhesions with laparoscopic
surgery, particularly in children [18]. There are few, if any, reports of bowel obstruction after laparoscopic procedures that would normally have been open retroperitoneal surgery. The reason for fewer intestinal adhesions is unclear, but has been documented, and immunological mechanisms hypothesized [30]. Renal surgery is naturally retroperitoneal and laparoscopic methods have moved in that direction with adults as well as children.
CURRENT STATUS
Paediatric urological laparoscopy is far from a mature technology, but it is here to stay. Diagnostic laparoscopy for cryptorchidism is a safe and effective method to identify the character and location of the affected organ, and thereby guide subsequent surgical interventions. Its value is comparable with preoperative imaging or endoscopy. It may be difficult to prove in a controlled study that it is indeed beneficial, but those who use it seem convinced, and most were practitioners of previous open surgical methods of exploration. Its significant advantage lies in its integration with the operative laparoscopic management of the testis identified at the time of diagnostic laparoscopy. This can be seamlessly integrated to provide for managing the challenging intra-abdominal testis. Any study of diagnostic laparoscopy must include this aspect to provide a real assessment of the benefits of laparoscopy for cryptorchidism. The outcomes of laparoscopy for the undescended testis are currently being reported, including results for multicentre groups [31]. The results need to be interpreted with caution, as the follow-up is often short and the long-term results unknown. Of course, there are very few data on the outcomes of the alternative, open surgical orchidopexy that are long-term and with objective assessments [32]. There is a suggestion that the outcomes of laparoscopic methods might even be better than open techniques, which may be explained by the increased exposure, magnification and the ability to readily mobilize the testis high into the retroperitoneum. This is preliminary and should be viewed with some scepticism, yet it is intuitively reasonable, and may be true.
Paediatric laparoscopic renal surgery has developed steadily and is now at the stage where there are efficient algorithms for partial nephrectomy and pyeloplasty [33,34].

C . P E T E R S
5 6
©
2 0 0 3 B J U I N T E R N A T I O N A L
There are still few practitioners but the number is increasing. The ability to perform complex reconstructive procedures developed from simpler procedures such as nephrectomy, and then the development of retroperitoneal methods, again with straightforward procedures such as nephrectomy. That progression is a key to the current status and to continued development. With the advent of robotically assisted technology, more complex reconstructive procedures will be readily undertaken, even by those with limited laparoscopic experience. This will permit the widespread application of laparoscopic methods. With robotic technology, any surgeon confident with basic laparoscopic techniques will be able to perform paediatric laparoscopic pyeloplasty. Future use in complex bladder and urinary tract reconstruction is becoming a testable reality.
CONCLUSIONS
Laparoscopy in paediatric urology continues its steady development with apparent vigour. There is a steady flow of clinical reports, meetings, workshops and formal discussions relating to its application. The development of effective laparoscopic skills in paediatric urology can be an efficient, progressive process open to any practitioner. Parents are beginning to be aware of this technology and are asking about it. Assessing its value will be challenging but not impossible. There is no simple formula as to how such new technologies should be assessed or at what time in their development that assessment is most appropriate. While RCTs are the ‘gold standard’ for assessing new technologies in medicine, their application, interpretation and relevance is not guaranteed. New technology must be regarded like a child; rich with promise, but unproven. Expecting too much is harmful; not setting standards or limits is harmful and active participation in the developmental process is the key to success.
REFERENCES
1
Clayman RV.
Pediatric laparoscopy: Quo vadis? View from outside.
J Urol
1994;
152
: 730–32
Cortesi N, Ferrari P, Zambarda E, Manenti A, Baldini A, Morano FP.
Diagnosis of bilateral abdominal cryptorchidism by laparoscopy.
Endoscopy
1976;
8
: 33–4
3
Jordan GH, Winslow BH.
Laparoendoscopic upper pole partial nephrectomy with ureterectomy.
J Urol
1993;
150
: 940–34
Jordan GH, Robey EL, Winslow BH.
Laparoendoscopic surgical management of the abdominal/transinguinal undescended testicle.
J Endourol
1992;
6
: 157–61
5
Koyle MA, Woo HH, Kavoussi LR.
Laparoscopic nephrectomy in the first year of life.
J Pediatric Surg
1993;
28
: 693–5
6
Ehrlich RM, Gershman A, Mee S, Fuchs G.
Laparoscopic nephrectomy in a child: Expanding horizons for laparoscopy in pediatric urology.
J Endourol
1992;
6
: 463–5
7
Ehrlich RM, Gershman A, Fuchs G.
Laparoscopic ureteral reimplantation for vesicoureteral reflux: initial case reports.
J Endourol
1993;
7
: S1718
Peters CA, Schlussel RN, Retik AB.
Pediatric laparoscopic dismembered pyeloplasty.
J Urol
1995;
153
: 1962–59
Docimo SG, Moore RG, Adams J, Kavoussi LR.
Laparoscopic bladder augmentation using stomach.
Urology
1995;
46
: 565–910
Atala A, Kavoussi LR, Goldstein DS, Retik AB, Peters CA.
Laparoscopic correction of vesicoureteral reflux.
J Urol
1993;
150
: 748–5111
Janetschek G, Radmayr C, Bartsch G.
Laparoscopic ureteral anti-reflux plasty reimplantation. First clinical experience.
Ann Urol (Paris)
1995;
29
: 101–512
El-Ghoneimi A, Valla JS, Steyaert H, Aigrain Y.
Laparoscopic renal surgery via a retroperitoneal approach in children.
J Urol
1998;
160
: 1138–4113
Kobashi KC, Chamberlin DA, Rajpoot D, Shanberg AM.
Retroperitoneal laparoscopic nephrectomy in children.
J Urol
1998;
160
: 1142–414
Valla JS, Guilloneau B, Montupet P
et al.
Retroperitoneal laparoscopic nephrectomy in children. Preliminary report of 18 cases.
Eur Urol
1996;
30
: 490–3
15
Borer JG, Cisek LJ, Atala A, Diamond DA, Retik AB, Peters CA.
Pediatric retroperitoneoscopic nephrectomy using 2 mm. instrumentation.
J Urol
1999;
162
: 1725–9
16
Horowitz M, Shah SM, Ferzli G, Syad PI, Glassberg KI.
Laparoscopic partial upper pole nephrectomy in infants and children.
BJU Int
2001;
87
: 514–6
17
Colodny AH.
Laparoscopy in pediatric urology: too much of a good thing?
Seminars Pediatric Surg
1996;
5
: 23–9
18
Moore RG, Kavoussi LR, Bloom DA
et al.
Postoperative adhesion formation after urological laparoscopy in the pediatric population.
J Urol
1995;
153
: 792–519
Jordan GH, Winslow BH.
Laparoscopically assisted continent catheterizable cutaneous appendicovesicostomy.
J Endourol
1993;
7
: 517–2020
Hedican SP, Schulam PG, Docimo SG.
Laparoscopic assisted reconstructive surgery.
J Urol
1999;
161
: 267–7021
Baum M.
Reflections on randomised controlled trials in surgery.
Lancet
1999;
353
(Suppl. 1): S16–822
Reeves B.
Health-technology assessment in surgery.
Lancet
1999;
353
(Suppl. 1): S13–5
23
Majeed AW, Troy G, Nicholl JP
et al.
Randomised, prospective, single-blind comparison of laparoscopic versus small-incision cholecystectomy.
Lancet
1996;
347
: 989–9424
McMahon AJ, O’Dwyer PJ, Baxter JN.
Randomised trial of laparoscopic versus small-incision cholecystectomy.
Lancet
1996;
347
: 162225
Rhodes M, Gompertz H, Armstrong K, Lennard T, Rees B.
Randomised trial of laparoscopic versus small-incision cholecystectomy.
Lancet
1996;
347
: 1621–2
26
Ferro F, Spagnoli A, Zaccara A, De Vico A, La Sala E.
Is preoperative laparoscopy useful for impalpable testis?
J Urol
1999;
162
: 995–627
Pace KT, Honey RJDA.
Unique methodological issues facing randomized controlled trials of endourologic procedures.
J Endourol
2002;
16
: 457–6328
Elder JS, Hladky D, Selzman AA.
Outpatient nephrectomy for nonfunctioning kidneys.
J Urol
1995;
154
: 712–4
29
Lakshmanan Y, Fung LC.
Laparoscopic extravesicular ureteral reimplantation for vesicoureteral reflux: recent technical advances.
J Endourol
2000;
14
: 589–93
30
Gitzelmann CA, Mendoza-Sagaon M, Talamini MA, Ahmad SA, Pegoli W Jr, Paidas CN.
Cell-mediated immune response is better preserved by laparoscopy than laparotomy.
Surgery
2000;
127
: 65–7131
Baker LA, Docimo SG, Surer I
et al.
A

L A P A R O S C O P Y I N P A E D I A T R I C U R O L O G Y
©
2 0 0 3 B J U I N T E R N A T I O N A L 5 7
multi-institutional analysis of laparoscopic orchidopexy. BJU Int 2001; 87: 484–9
32 Docimo SG. The results of surgical therapy for cryptorchidism: a literature review and analysis. J Urol 1995; 154: 1148–52
33 Tan HL. Laparoscopic Anderson-Hynes dismembered pyeloplasty in children. J Urol 1999; 162: 1045–7
34 Yeung CK, Tam YH, Sihoe JD, Lee KH, Liu KW. Retroperitoneoscopic dismembered pyeloplasty for pelvi-
ureteric junction obstruction in infants and children. BJU Int 2001; 87: 509–13
Correspondence: C. Peters, Department of Urology, Children’s Hospital, Harvard Medical School, Boston, MA, USA.e-mail: [email protected]





![LAPAROSCOPY - FIOMEDfiomed.it/wp-content/uploads/2018/12/fiomed-strumentazione-medic… · TELESCOPES FOR LAPAROSCOPY [autoclavable ] X Ø 2.9 mm also for use in Gynecology and Urology]](https://img.pdfslide.net/doc/110x75/5f2d4c4b7830285abf3a8074/laparoscopy-telescopes-for-laparoscopy-autoclavable-x-29-mm-also-for-use.jpg)