Embed Size (px)
Citation preview

Disorders of the LarynxWinnie YeungFoundation Year 2

Question 1All of the following muscles are supplied by the recurrent
laryngeal nerve except:
A. Posterior cricoarytenoidB. Lateral cricoarytenoidC. CricothyroidD. ThyroarytenoidE. Mylohyoid

Question 2Which virus is implicated in recurrent respiratory
papillomatosis:
A. EBVB. HPVC. CMVD. VZVE. HIV

Question 3A 37-year old opera singer comes to clinic, complaining of 2-
weeks history of hoarseness which is interfering with her work. On endoscopy, you see normal vibration of the vocal cords, but notice thickened areas at the anterior 1/3 of both cords. The most likely diagnosis is:
A. Vocal cord polypB. Vocal cord nodulesC. Vocal cord synechiaD. Vocal cord paralysisE. Carcinoma of the larynx

Question 4A 5-year old child is brought to A&E by his concerned mother with
high fever and difficulty swallowing. On examination, the child is sat up on the bed, you notice that stridor, quiet shallow breathing and drooling. ‘Thumb-print sign’ is seen on XR. The most likely cause is:
A. EpiglottitisB. CroupC. Peritonsillar abscessD. Retropharygeal abscessE. Foreign body

Question 5A 17-year old comes to see her GP, presenting with a short
history of mild fever, fatigue and sore throat. She has vomited once at home today. On examination, there is splenomegaly. Which of the following treatment should the GP avoid:
A. ClarithromycinB. DoxycyclineC. Co-trimoxazoleD. AmoxicillinE. Aciclovir

Session Overview• Anatomy
• Benign lesions▫ Nodules▫ Polyps▫ Cysts▫ Reinke’s oedema
• Inflammatory conditions▫ Laryngitis
• Degenerative conditions▫ Presbylarynx
• Neoplasia▫Premalignant▫Carcinoma
• Neurological▫Paralysis
• Epiglottitis• Respiratory papillomatosis• Infectious mononucleosis


• Cricothyrodectomy▫ Emergency airway
involves puncturing the cricothyroid membrane.
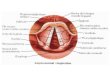
• Larynx skeleton made up of various cartilages:▫ Thyroid cartilage▫ Cricoid cartiage (complete ring)▫ Arytenoid cartilages (pyramid-shaped x2)

Anatomy: Endoscopic view• All muscles of the larynx supplied
by the recurrent laryngeal nerve, from vagus.
• EXCEPT cricothyroid muscle, innervated by the external branch of the superior laryngeal nerve.
• Blood supply: Superior and inferior thyroid arteries.Rima Glottidis

Function of the normal larynx• Appearance: Pearly-white true vocal cords, with surrounding
structure being light pink.• Function: Breathing and phonation.• Movement: Abducts and adducts against each other, meeting
in the midline on phonation. There should be no gaps!

Throat symptoms• Hoarseness
• Stridor: High-pitched noise, in either inspiration or exhalation, due to upper airway obstruction.
• Stertor: Heavy snoring inspiratory sound, occuring in coma or deep sleep, sometimes due to obstruction and upper airways.
• Pain: Not common, even in malignancy, but may be a prominent feature if pathology is inflammatory in nature,

Benign: Nodules• Causes: Microtrauma, gastric
reflux, repeated URTI.
• Findings: Calluses occurs in pairs, preventing cords from meeting in the midline. Hourglass deformity.
• Most commonly occuring in anterior 1/3 of vocal cords.
• Common in children and female patients, singers, teachers.
• Symptoms: Hoarseness, painful phonation, frequent voice breaks, reduced vocal range.
• Formed slowly over time.
• Management: Intensive speech and voice therapy, uncommonly microlaryngeal surgery.

Benign: Polyps• Causes: Isolated trauma, violent
coughing, screaming, LPR (Laryngopharyngeal reflux).
• Findings: Single or paired lesions occuring at phonating margin (edge) of vocal cord.
• Mostly in adult males.
• Symtpoms: Hoarse, breathy voice, tiring easily.
• Management: Voice therapy, voice rest, sometimes surgery.

Benign: Cysts• Causes: Poor draining or blocked
small gland in vocal fold, preventing drainage. Unknown whether vocal cord irritation or excessive voice use contributes.
• Findings: Single or paired lesions, collection of mucous fluid in sac-like structures.
• Management: Poor response to conservative Mx. Surgical removal, followed by voice rest.

Reinke’s Oedema• Aka ‘Polypoid Degeneration’ or
‘Polypoid Corditis’.
• Findings: Enlargement of upper layer of vocal cord covering, ‘Reinke’s space’, with accumulation of gelatinous fluid.
• Causes: Smoking, never seen in non-smokers.
• Symptoms: Lower-pitched voice due to slower vibrations. SOB.
• Management: Surgery. Smoking cessation is key, as may reoccure post-surgery is continued.
• Have some malignant potential.

Inflammatory: Laryngitis • Irritation and swelling of vocal
cords, acute vs. chronic.
• Causes: LPR, infection, smoking and inhalation of noxious fumes.
• Findings: Swollen cords, resulting in limited mucosal waves and incomplete closure. May look dry.
• Management: Seek and treat underlying course. If persists >2 weeks, consider expert advice.

Presbylarynx• Causes: Thicking of vocal cord muscles and
tissues with aging.
• Findings: Reduced bulk, not meeting in midline.
• Symptoms: Hoarse, weak, breathy voice.
• Management: Injection of fat or other material to achieve complete closure.

Malignancy: Carcinoma of the Larynx
• Causes: Smoking, alcohol, LPR.
• Classification: Supraglottic, glottic, subglottic.
• Pre-malignant: Leukoplakia on vocal cords, may develop into cancer if untreated.
• Symptoms: Horaseness, but may be insidious, presenting with acute airway obstruction. SOB, neck lump, blood in spit.
• Management: Surgery, cessation of smoking, alcohol, anti-reflux medication.

Vocal Cord Paralysis• Causes: Iatrogenic, malignant
invasion.
• Findings: Cord abducted on ipsilateral side, no movement/vibration
• Symptoms: Adduction failure results in weak, breathy voice.
• Management: Voice therapy, surgery with sialistic block to displace affect cord medially.

Epiglottitis• CT: ‘Halloween sign’ excludes
acute epiglottitis.
• C-spine XR: ‘Thumb-print’ sign
• Causes: Infection from Haemophilus influenzae.
• Uncommon since Hib vaccine.
• Symptoms: Potentially life-threatening upper respiratory obstruction.
• Young child, anxious, quiet shallow breathing, drooling +++.
• Managment: Protecting and securing airway, antibiotics.

Recurrent papillomatosis• Causes: Associated with HPV,
vertical transmission.
• Symptoms: Wart-like lesions in respiratory tract, causing recurrent obstruction.
• Young patients with stridor.
• Managment: No definitive cure, repeat microdebridement or CO2 laser to manage recurrent lesions.

Infectious mononucleiosis• Glandular fever (aka ‘kissing disease).
• Causes: Epstein-Barr virus.
• Symptoms: Fever, sore throat, malaise, sometimes vomiting and petichiae.
• Signs: Lymphadenopathy in posterior cervical, axillary and inguinal regions. Splenomegaly.
• Investigations: >50% lymphocytes, 10% with enlarged, typical nuclei, Monospot test (heterophile antibody test).
• Differentials: CMV, tonsillitis, flu, leukaemia, diptheria.
• Management: Symptomatic and supportive. Generally self-limiting,
• Avoid penicillins Rash.

Review: Question 1All of the following muscles are supplied by the recurrent
laryngeal nerve except:
A. Posterior cricoarytenoidB. Lateral cricoarytenoidC. CricothyroidD. ThyroarytenoidE. Mylohyoid
Correct answer: C

Review: Question 2Which virus is implicated the development of recurrent
respiratory papillomatosis:
A. EBVB. HPVC. CMVD. VZVE. HIV
Correct answer: B

Review: Question 3A 37-year old opera singer comes to clinic, complaining of 2-weeks history of
hoarseness which is interfering with her work. On endoscopy, you see normal vibration of the vocal cords, but notice thickened areas at the anterior 1/3 of both cords. The most likely diagnosis is:
A. Vocal cord polypB. Vocal cord nodulesC. Vocal cord synechiaD. Vocal cord paralysisE. Carcinoma of the larynx
Correct answer: B

Question 4A 5-year old child is brought to A&E by his concerned mother with high fever
and difficulty swallowing. On examination, the child is sat up on the bed, you notice that stridor, quiet shallow breathing and drooling. ‘Thumb-print sign’ is seen on XR. The most likely cause:
A. EpiglottitisB. CroupC. Peritonsillar abscessD. Retropharygeal abscessE. Foreign body
Correct answer: A

Question 5A 17-year old comes to see her GP, presenting with a short history of mild
fever, fatigue and sore throat. She has vomited once at home today. On examination, there is splenomegaly. Which of the following treatment should the GP avoid:
A. ClarithromycinB. DoxycyclineC. Co-trimoxazoleD. AmoxicillinE. Aciclovir
Correct answer: D


‘ Nothing can surpass the ability of the voice for soulful expression of the human experience.’