Embed Size (px)
Citation preview

Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of specific product names does not inferendorsement by Dentistry Today. Information contained in CE articles and courses is not a substitute for sound clinical judgment and acceptedstandards of care. Participants are urged to contact their state dental boards for continuing education requirements.
Authored by Glenn A. van As, BSc, DMD
Upon successful completion of this CE activity, 3 CE credit hours may be awarded
Volume 34 No. 7 Page 134
Lasers in Implant Dentistry,Part 1
CONTINUING EDUCATION

1
CONTINUING EDUCATION
In the past, some in the profession have questioned whetherlasers are a legitimate adjunctive tool for dentistry, or anapplication looking for a purpose.1,2 Lasers have been
slower to gain relevance in our profession, whereas they aremore commonly accepted as staples in the medical professionfor such areas as laser eye surgery;3 ear, nose, and throatsurgery;4 dermatology;5 and urology.6 The development of theuse of lasers in dentistry has grown in the last 5 to 6 years withthe release of soft-tissue diode lasers which were cost effective,portable, lightweight, and reliable. Suddenly, many cliniciansbegan looking to replace their aging electrosurge units withdiode lasers. The growth of diode lasers as soft-tissue handpiecesevolved, in part due to their ability to work safely withpacemakers, and their usefulness in being able to be usedaround implants, crowns, amalgams, and other metalsubstructures while minimizing the risk of creating iatrogenicdamage. In addition, a laser’s ability to be used withinendodontic canals and perio dontal pockets to decrease bacteria,
and for their capability in being able to remove small amountsof tissue with only topical anesthetic, made them increasinglypopular amongst many dentists.7 All of these advantages led tothe popularity of diode lasers as an alternative to electrosurgicalunits world wide.8,9
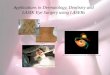
Nd:YAG and carbon dioxide (CO2) lasers were the first soft-tissue laser wavelengths introduced in dentistry in the early1990s. Diode lasers, first introduced in 1995 for soft-tissueprocedures, have impacted many areas of our dental practice,including gingivectomies,10,11 as an alternative to retractioncord in tissue management for crown and bridge,12-14 for soft-tissue surgeries such as frenectomies and fibroma removal,15and for the treatment of vascular lesions such as venous lakes(hemangiomas)16 (Figures 1 to 3).
The erbium family of hard-tissue lasers (Er,Cr:YSGG andEr:YAG wavelengths) made their appearance in dentistry in thelate 1990s and were heralded initially for their ability to cuttooth structure as well as soft tissue. The ability to ablateanything with water in it made it possible to use these “all-tissue” lasers for many purposes, including local anesthetic-freerestorations,17,18 the removal of porcelain veneers, and all-ceramic porcelain restorations in an efficient, safe, andpredictable manner.19-22 In addition, the erbium family of laserscan be used to remove bone for crown lengthening procedures23and have been promoted for their abilities in the field ofendodontics to help with deep disinfection in the dentinaltubules through their antibacterial capabilities.24,25 Morerecently, the Er:YAG laser has been promoted for its role inperiodontics as it possesses suitable characteristics for theeffective elimination of granulation tissue, gingival melaninpigmentation, and gingival discoloration. Furthermore, thecutting and contouring of bone with minimal damage and evenfaster healing can also be performed with this laser. Erbium lasersare antibacterial and can remove both calculus and biofilmaround tooth structure and implant surfaces.26-28
LASERS IN IMPLANTOLOGYThe role of lasers in dental implantology was explored byRomanos et al,29 and they found that soft-tissue lasers could beof benefit for improvements in hemostasis, as an adjunct tosoft-tissue peri-implant re contouring, and for improvingwound healing. Hard-tissue lasers (Er,Cr:YSGG and Er:YAGwavelengths) were valuable for laser-assisted osteotomies, andfor the improvement in early osseointegration af ter fixtureplacement. They29 also mentioned that lasers could be used forthe treatment of peri-implantitis.
Although it is difficult to categorize the role of lasers forimplantology, one method to do so has been developed by the
Lasers in Implant Dentistry,Part 1
About the Author
Dr. van As graduated from the faculty of dentistry atthe University of British Columbia, Vancouver, Cana -da, and was an assistant clinical professor there from1989 to 1999. His memberships include but are notlimited to the British Columbia Dental Association, theCanadian Dental Association, the Academy ofMicroscope Enhanced Dentistry, the Academy of Laser
Dentistry, and the American Academy of Cosmetic Dentistry. He has built ahigh-tech, high-touch, full-time dental practice where the entire dental teamis committed to using the latest technologies available to provide the highestlevel of clinical excellence in dentistry. He has lectured internationally andhas provided hands-on workshops on multiple topics involving dental lasersand microscopes. He is an active member on many web forums dealing withlasers and microscopes in general practice, acts as a consultant for manyhigh-technology companies, and is a reviewer of articles for dentalmagazines. He was honored with the Leon Goldman award in 2006 forworldwide clinical excellence in laser dentistry and has been one of DentistryToday’s Leaders in Continuing Education since 2012. He can be reached viaemail at [email protected], or via the website drvanas.com.
Disclosure: Dr. van As has received honoraria and equipment and consultingfees from companies including BIOLASE, AMD Lasers, Zolar Lasers, GlobalMicroscopes, and Hiossen Implants.
Effective Date: 07/01/2015 Expiration Date: 07/01/2018

author of this article and looks at the roleof lasers by the timing or stage of theprocedure (Figure 4). This method ofcategorizing the role of lasers looksprimarily at the benefit at a certain stageof the implant treatment cycle. Effectiveuse of laser energy can be beneficial at allstages of implantology, from prior toimplant placement where lasers can beused to remove bacteria and granulationtissue, to during the procedure for flapincision, decortication, and ablation ofexcess soft tissue or bone. After-implantplacement lasers can be beneficial for uncovering and soft-tissuerecontouring during the prosthetic phase. Finally, lasers aregaining an exciting and important role in the growing issue ofperi-implantitis and mucositis during the healing phase.
In the first of this 2-part article series, I will look at the role oflasers prior to, during, and immediately after implant placementin Stage 1—the surgical portion of the procedure. Part 2 willdiscuss the role of lasers after the initial implant surgery and lookat the role of lasers for uncovery, cementation, and in the growingrole of lasers for the treatment of peri-implantitis.
Laser Usage Prior to Implant PlacementAt times, a tooth becomes unsalvageable due to restorative,endodontic, or periodontal concerns, or a combination of thesefactors. Despite heroic attempts, teeth must be at timesextracted, and grafting of the site for preservation of hard andsoft tissue must be undertaken in order to replace missing teethwith dental implants. Kusek30 showed that the use of an erbiumlaser, through photoacoustic streaming, could reduce thebacteria in osteotomy sites that were infected by apicalpathology. The author30 took swabs both immediately afterextracting teeth and subsequently again after the Er,Cr:YSGG
laser was used. The results showed a noticeable reduction ofbacteria and no traces of virulent bacteria.
With the use of the BIOLSE iPlus (Er,Cr:YSGG wavelength),the laser can effectively and safely interact with soft tissue toremove granulation tissue and, in addition, can disinfect theextraction socket without fear of damage to bone prior to socketpreservation procedures (Figures 5 to 10). The effective use ofradially firing tips where 85% of the energy (Figure 11 to 13) fireslaterally, combined with the microexplosive cavitation causedby rapid expansion of water particles when the laser wavelengthinteracts with water, allow for tremendous disinfection andcleaning of the infected extraction socket for prior to the socketgrafting procedure.
All lasers are antibacterial in nature and can be used tovarying degrees to disinfect a site.31-32 Some soft-tissue laserslike diode lasers should be used with caution so as not to heatup the bone, but when used judiciously (power of one W or lesscontinuous wave [CW], uninitiated tip), they can help disinfecta site prior to grafting. There is a growing issue worldwide withbacterial resistance to systemic antibiotics,33 and combinedwith the horrible taste of some of the antibiotics that can becombined with bone grafts (ie, clindamycin), lasers can help
2
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1
Figure 1. Pre-op old veneers requiringreplacement due to caries and discoloration.
Figure 2. Diode laser crown troughing and frenectomy.
Figure 3. Two-week postoperative healing of final results.
Figure 4. Categorization of role of lasers by the stage of the procedure.

lessen the necessity to utilize antibiotics both locally andsystemically for grafting procedures.
Erbium “all-tissue” lasers have been used to ablate bone forlateral sinus lifts in the past,34-35 but one must realize that thelaser is not able to selectively ablate (cut) only bone. The laserenergy is absorbed by water so both bone and soft tissue can beablated. Piezo surgical units are not as likely to cut the sinuslining during their use and the speed of cut with the erbium laseris similar to that of the piezo units. Although lateral windowsinus lifts can be successfully completed with erbium lasers andthe fine mist of water spray can be beneficial to see the surgicalfield compared to a turbine motor with bur, magnification andcaution must be employed when considering lasers in this
procedure in order to prevent tearing of the Schneiderian sinuslining membrane.
Laser Usage During Implant Fixture PlacementLaser usage can be beneficial during the actual implantplacement for creation of the flap incision, for the actualcreation of the osteotomy, and for decortication for guided boneregeneration (GBR), amongst other items.
All lasers can ablate soft tissue and thus can be used to makeincisions in soft tissue. The lasers offer great hemostasiscompared to surgical blades, but do cut a larger incision inwidth due to their larger tip diameter. The wavelengths usedvary in their depth of penetration into the tissue with some soft-
3
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1
Figures 5 to 10. (Figure 5) The extraction of a lower left second molar with retained granulation tissue, and (Figure 6) after epithelium isremoved with the Er,Cr:YSGG laser around the socket, and (Figure 7) the socket is disinfected with the radially firing tips. (Figure 8) Allograftbone, (Figure 9) a resorbable membrane, and (Figure 10) polytetrafluoroethylene sutures complete the socket preservation procedure. Theuse of the laser ensures removal of soft tissue and disinfection without the reliance on antibiotics.
Figures 11 to 13. (Figures 11 and 12) Use of the radially firing tips for the iPlus (BIOLASE) allow for laser energy to fire laterally providing forboth degranulation and disinfection of the extraction socket with tremendous cavitation as evident in Figure 13.
5 6 7
8 9 10
11 12 13

tissue lasers such as diode lasers or Nd:YAGlasers penetrating further compared to CO2lasers.36 Typically, the lateral thermal damagefor lasers is much smaller than for electro-surgery units, but the mechanism of action forsoft-tissue diode lasers is thermal or infrared,which means that light is converted to heatand that is the primary method for ablation.Wavelengths that offer water as a coolingmechanism to the photothermal ablation(erbium lasers and the new CO2 9,300 nmwavelength) may allow for a decrease inunwanted thermal effects due to a low inflam-matory response with minimal resultingdamage to surrounding tissue.37,38
One benefit of using the water-coolederbium lasers is that the fine mist of air andwater that is created helps keep the visual fieldclean and with very little bleeding whencompared to a blade, and the reduction ininflammatory response allows laser incisionsto be comparable to that from a surgical bladein many re spects of healing.39
Lasers that can ablate bone, such as erbiumlasers, have been suggested as potentiallycapable of producing osteotomies in their entirety, with thebenefit being superior bone-to-im plant contact (BIC) andimplant stability measurements at 8 weeks postoperatively.40The laser-produced osteotomy was wider in many areas of thepreparation than a drill osteotomy, but thermal damage to boneis not present in the laser-prepared osteotomies.41 The concernis that similar to using the erbium laser for a lateral sinuswindow, the speed is slow compared to a bur, the depth ofpenetration of the laser energy into surrounding tissues may beminimal, but the inability of the laser to selectively cut onlybone can be an issue if working around key anatomicalstructures such as nerves and blood vessels, where unintentionalablation might lead to severe short- and long-term complicationsof paresthesia or hemorrhage.41 The greatest benefit for usingerbium lasers might be during the initial osteotomy guide hole,where burs might “slip” or “bounce” off irregular or sloped bonysurfaces often seen during immediate implant procedures afterextractions. The ability of the erbium laser to create precisestarting points for the rest of the osteotomy in a noncontactfashion can be of benefit in many instances.42
It has been said that implant dentistry is a prosthetic-driven procedure with a surgical component. In other words,the decision of where to place the implant is formulated by
where the teeth should be ideally positioned, and not wherethe underlying bone is presently located. GBR has become anaccepted procedure in our profession to create adequate bonefor an area if it is deficient in either horizontal43 or vertical44directions. Four basic tenets must be followed for the creationof new bone: primary closure of the wound to promoteundisturbed and uninterrupted healing; angiogenesis toprovide necessary blood supply and undifferentiatedmesenchymal cells; space creation and maintenance tofacilitate space for bone in-growth; and, the stability of thewound to induce blood clot formation, allowing uneventfulhealing.45 To create angiogenesis, most clinicians will use around bur to perforate the cortical plate to allow for the releaseof progenitor cells. An all-tissue laser (erbium family of lasers)can also be utilized to decorticate the bone, and research hasshown that there might be advantages to using the lasercompared to a bur. Kesler et al46 showed that the Er:YAG lasercreated higher levels of platelet-derived growth factorcompared to a bur, and they proposed therefore that laserirradiation would likely en hance and improve the earlyhealing of bone grafted areas when used for decortication.
Although prolonged use of soft-tissue laser wavelengths canbe damaging to bone, the hard-tissue erbium lasers, due to their
4
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1
Figures 14 to 17. (Figure 14) Decortication with Er,Cr:YSGG Laser (iPlus) for guided boneregeneration (GBR) overexposed threads of ET III dental implants (HIOSSEN), following fractureof buccal plate during ridge split procedure. (Figure 15) Mixture of autogenous and xenograftfor GBR with preformed HIOSSEN Smart Membrane Titanium mesh membranes. (Figure 16)Bone growth at 6 months post-op healing during uncovery and removal of mesh. (Figure 17)Final postoperative appearance of crowns for case.
14 15
16 17

water cooling spray, are safe to use on bone.47-49The Er:YAG and Er,Cr:YSGG lasers provideprecise ablation of bone with minimal thermaldamage that makes them suitable forimplantology. The ability to ablate precisely innoncontact fashion with lasers, and without thevibrations that are felt by the patient whenusing burs, these wavelengths (2,780 and 2,940nm) are wonderful for GBR (Figures 14 to 17).
Laser Usage After Implant Fixture Placement
After the implant fixture has been placed, minoralterations in hard tissue may be needed if thebone is not level around the implant. At times,uneven bone, or sloped overhanging bone mayprevent ideal and complete seating of thehealing abutment in a single-stage procedure,and in addition, the potential of bone to preventideal impression taking, seating of the implant,or final restoration can create chronic dis-comfort, inflammation, or swelling of the finalimplant restoration. Erbium lasers, again due totheir ability to precisely and safely remove bone,can be used at this time to relieve bone for idealplacement of prosthetic components such as thehealing abutment. Research has shown that theerbium family of lasers will not damage the implant itself orcause untoward temperature increases in the surgical site thatcould jeopardize the implant itself (Figure 18).50,51
In addition to ideal hard-tissue contours around theimplants, the erbium laser can be safely used to trim soft tissuearound healing abutments. When adequate soft tissue existsbut the clinician wishes to produce a more ideal emergenceprofile, it can be desirable to choose a larger-diameter healingcap than the im plant fixture diameter. At times it can bedifficult to gain ideal closure of the flap. In these situations,minor soft-tissue refinement can provide a much improvedclosure around the healing abutment. It is important torecognize that adequate attached tissue that is keratinized mustenvelop the implant, so care must be taken to ensure that soft-tissue volume and adequate attached tissue exists prior to itsremoval (Figure 19).
The value of low levels of laser therapeutical energy (LLLT)has gained greater awareness in the last decade as research hasgrown on this topic. Although all laser wavelengths can providesome degree of biostimulation (wound healing) andbioinhibition (pain decrease), the most common wavelengths
for these so-called “cold” or “soft” lasers is in the 655 to 810 nmrange. Thus, diode lasers in the 810 nm range, when used at lowenergies (0.1 to 0.5 W CW) can be used for a variety of benefitsfor patients undergoing implant surgery. When laser energy isused for a therapeutic effect, a diffuse beam of energy size thatis often larger in spot size (larger handpiece) is delivered to thetissue site over a period of time. The level of laser energy is lowenough to have a therapeutic effect without causing any tissuedestruction, and now a very common name for this procedure islaser phototherapy (Figure 20).
The mechanism of action for low levels of near-infraredlaser energy to have either a biostimulatory or bioinhibitoryeffect lies in the energy being absorbed by cell mitochondria,which in turn produces a reactive oxygen species and releasesnitric oxide in the cell. There is a corresponding increase in therelease of ATP within the cell, and this leads to genetranscription that in turn causes the release of growth factors,cell proliferation, and cell motility with an increase inextracellular matrix. The result is that wound healing isimproved through tissue repair, in flammation and edema arereduced, providing pain relief. Finally, neurogenic pain or
5
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1
Figures 18 and 19. (Figure 18). Er,Cr:YSGG laser being used to level the bone on the lingual aspect of the implant fixture which has been placed at the buccal crestal bone level.(Figure 19) Soft-tissue ablation with the same wavelength, allowing for ideal primary closureof soft tissue around the healing abutments through minor recontouring of the lingual keratinized tissue.
Figure 20. Low levels of laser therapeuticalenergy (LLLT) is dispensed through a largerspot beam size handpiece to cover a largerarea when needed.
Figure 21. The handpiece is in actionintraorally after an implant fixture has beenplaced to try to help with initial postoperativediscomfort and to improve the early bone toimplant contact in the initial healing stages.
18 19

problems can be lessened as well (Figure 21).Although early pioneers in the realm of
LLLT were dismissed, a great deal of researchrecently has shown value in using LLLT forimplant therapy for many areas. A diode laseraround 810 nm, when set to low levels of power,can be an effective modality for reducingpostoperative pain and to promote woundhealing after surgery.50 In addition, LLLT ishighly effective for tissue repair and painrelief.51 Pinheiro et al52 showed that laserphototherapy provided SEM results thatshowed better bone healing after irradiationwith the 830-nm diode laser, and concluded thatLLLT may increase bone repair at early stages of healing. Otherre search53 has shown that LLLT promoted the osseointegrationof im plants with poor initial stability, particularly in the initialstages of bone healing and that using LLLT enhanced peri-implant bone repair, improving stability, BIC, and new boneformation when used every 48 hours for 2 weeks.54
One exciting area of research has looked at the reduction ofneurogenic pain and sensory deficit when using LLLT.Unfortunately, neurosensory deficits can occur after anysurgery, including implants either due to direct contact with aneurovascular bundle (ie, inferior alveolar nerve [IAN], mentalnerve) with an implant, or through contact surgically with theanatomic structure. This can result in transient damage to anarea of the skin or oral cavity. Tradi tionally, the clinician isasked to map out the area to “watch” and see how it heals.Unfortunately, patients want action, and the lasers can thusprovide patients with a solution that often can be “felt”immediately with a significant decrease in neurosensory deficitand the visual analog scale analysis revealing progressive im -provement throughout time.55 Other research concluded thatLLLT is beneficial in patients with an IAN neurosensory deficit.In another study,56 it was seen that LLLT provided clinicaleffects on injured nerves that revealed an increase in nervefunction and improved capacity for myelin production. So,using LLLT can be beneficial in many areas of wound healingand can provide potential options for problems that currentlyare not easy to resolve with traditional methods (Figure 22).
CLOSING COMMENTSIn part one of this 2-part article series, I have attempted to lookat how lasers can provide an adjunctive benefit to the earlystages of implant therapy, namely adding benefits to socketgrafting before the procedure, during the actual implantplacement, and immediately after the surgery is complete. In
part 2, we will see how lasers can be used during implantuncovery, during final prosthesis insertion, and for the excitingbenefit of how lasers may provide a crucial role to thedetoxification and disinfection of ailing and failing implants(peri-implantitis) where many currently used regimens fail toallow for reosseointegration of bone cells to the implant fixture.
Lasers are an application that has found its purpose inimplantology, and hopefully with time, more clinicians willdiscover how vital laser dentistry can be to successful dentalimplantology.�
References1. Christensen GJ. Soft-tissue cutting with laser versus
electrosurgery. J Am Dent Assoc. 2008;139:981-984.2. Christensen G, Child P Jr. New technology: man datory, elective,
or hype? Dent Today. 2011;30:134-138.3. Blumenkranz MS. The evolution of laser therapy in ophthalmology:
a perspective on the interactions between photons, patients,physicians, and physicists: the LXX Edward Jackson MemorialLecture. Am J Ophthalmol. 2014;158:12-25.e1.
4. Kamalski DM, de Boorder T, Bittermann AJ, et al. Capturingthermal, mechanical, and acoustic effects of the diode (980nm) laser in stapedotomy. Otol Neurotol. 2014;35:1070-1076.
5. de Vries K, Prens EP. Laser treatment and its implications forphotodamaged skin and actinic keratosis. Curr Probl Dermatol.2015;46:129-135.
6. Gong YG, Liu RM, Gao R. Photoselective vaporesection of theprostate with a front-firing lithium triborate laser: surgicaltechnique and experience after 215 procedures. Eur Urol.2014 Dec 30. [Epub ahead of print]
7. van As GA. The diode laser as an electrosurgery replacement.Dentaltown. June 2010:56-64.
8. van As GA. Lasers in dentistry: an application that found itspurpose. Oral Health. 2011;101:30-39.
9. van As G. The role of lasers in cosmetic restorative dentistry.PPD (BACD). July 2011:21-25.
6
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1
Figure 22. The mechanism of action for LLLT where near-infrared energy releases reactiveoxygen species and releases nitric oxide, which leads to gene transcription and the release ofgrowth factors, increased cell proliferation, and motility and a growth of extracellular matrixdeposition. The result is a decrease in pain, inflammation, and neurosensory deficits.

10. van As G. Uncovering the tooth: the diode laser to uncoverteeth, brackets and implants. Dent Today. 2012;31:168.
11. de Oliveira Guaré R, Costa SC, Baeder F, et al. Drug-inducedgingival enlargement: biofilm control and surgical therapy withgallium-aluminum-arsenide (GaAIAs) diode laser—a 2-yearfollow-up. Spec Care Dentist. 2010;30:46-52.
12. Gherlone EF, Maiorana C, Grassi RF, et al. The use of 980-nmdiode and 1064-nm Nd:YAG laser for gingival retraction in fixedprostheses. Journal of Oral Laser Applications. 2004;4:183-190.
13. van As G. Posterior crown troughing with the AMD Picasso litediode laser. Dent Today. 2011;30:168.
14. Lee EA. Laser-assisted gingival tissue procedures in estheticdentistry. Pract Proced Aesthet Dent. 2006;18(suppl):2-6.
15. Fornaini C, Rocca JP, Bertrand MF, et al. Nd:YAG and diodelaser in the surgical management of soft tissues related toorthodontic treatment and laser surgery. Photomed Laser Surg.2007;25:381-392.
16. Angiero F, Benedicenti S, Romanos GE, et al. Treatment ofhemangioma of the head and neck with diode laser and forceddehydration with induced photocoagulation. Photomed LaserSurg. 2008;26:113-118.
17. van As G. Erbium lasers in dentistry. Dent Clin North Am.2004;48:1017-1059, viii.
18. Olivi G, Genovese MD. Laser restorative dentistry in childrenand adolescents. Eur Arch Paediatr Dent. 2011;12:68-78.
19. van As G. Laser removal of porcelain veneers. Dent Today.2012;31:84-89.
20. Wyatt A. The removal of porcelain veneers using an Er:YAGlaser: a report of two cases. J Laser Dent. 2009;17:37-38.
21. Morford CK, Buu NC, Rechmann BM, et al. Er:YAG laserdebonding of porcelain veneers. Lasers Surg Med.2011;43:965-974.
22. Rechmann P, Buu NC, Rechmann BM, et al. Laser all-ceramiccrown removal—a laboratory proof-of-principle study—phase 2crown debonding time. Lasers Surg Med. 2014;46:636-643.
23. Flax HD. Soft and hard tissue management using lasers inesthetic restoration. Dent Clin North Am. 2011;55:383-402.
24. Olivi G, DiVito E, Peters O, et al. Disinfection efficacy ofphoton-induced photoacoustic streaming on root canalsinfected with Enterococcus faecalis: an ex vivo study. J AmDent Assoc. 2014;145:843-848.
25. Peters OA, Bardsley S, Fong J, et al. Disinfection of root canalswith photon-initiated photoacoustic streaming. J Endod.2011;37:1008-1012.
26. Ishikawa I, Aoki A, Takasaki AA. Potential applications ofErbium:YAG laser in periodontics. J Periodontal Res.2004;39:275-285.
27. Akiyama F, Aoki A, Miura-Uchiyama M, et al. In vitro studies ofthe ablation mechanism of perio dontopathic bacteria anddecontamination effect on periodontally diseased rootsurfaces by erbium:yttrium-aluminum-garnet laser. Lasers MedSci. 2011;26:193-204.
28. Hakki SS, Korkusuz P, Berk G, et al. Comparison of Er,Cr:YSGGlaser and hand instrumentation on the attachment ofperiodontal ligament fibroblasts to periodontally diseased rootsurfaces: an in vitro study. J Periodontol. 2010;81:1216-1225.
29. Romanos GE, Gupta B, Yunker M, et al. Lasers use in dentalimplantology. Implant Dent. 2013;22:282-288.
30. Kusek ER. Immediate implant placement into infected sites:bacterial studies of the Hydroacoustic effects of the YSGGlaser. J Oral Implantol. 2011;37(spec no):205-211.
31. Gokhale SR, Padhye AM, Byakod G, et al. A comparativeevaluation of the efficacy of diode laser as an adjunct tomechanical debridement versus conventional mechanicaldebridement in periodontal flap surgery: a clinical andmicrobiological study. Photomed Laser Surg. 2012;30:598-603.
32. Gutknecht N, Franzen R, Schippers M, et al. Bactericidal effectof a 980-nm diode laser in the root canal wall dentin of bovineteeth. J Clin Laser Med Surg. 2004;22:9-13.
33. Cope AL, Chestnutt IG. Inappropriate prescribing of antibioticsin primary dental care: reasons and resolutions. Prim Dent J.2014;3:33-37.
34. Stübinger S, Nuss K, Sebesteny T, et al. Erbium-doped yttriumaluminium garnet laser-assisted access osteotomy formaxillary sinus elevation: a human and animal cadaver study.Photomed Laser Surg. 2010;28:39-44.
35. Tosun T, Benedicenti S. Usage of Er:YAG lasers in maxillary sinussurgeries: a clinical comparison of VSP vs Gaussian profiles.Journal of the Laser and Health Academy. 2014:29-32.
36. Goharkhay K, Moritz A, Wilder-Smith P, et al. Effects on oralsoft tissue produced by a diode laser in vitro. Lasers SurgMed. 1999;25:401-406.
37. Ryu SW, Lee SH, Yoon HJ. A comparative histological andimmunohistochemical study of wound healing following incisionwith a scalpel, CO2 laser or Er,Cr:YSGG laser in the guinea pigoral mucosa. Acta Odontol Scand. 2012;70:448-454.
38. Sawabe M, Aoki A, Komaki M, et al. Gingival tissue healingfollowing Er:YAG laser ablation compared to electrosurgery inrats. Lasers Med Sci. 2015;30:875-883.
39. Freemont AJ, Charlton A, Wannop NM, et al. Post-operativehealing of erbium YAG laser incisions. Lasers Med Sci.1992;7:449-453.
40. Schwarz F, Olivier W, Herten M, et al. Influence of implant bedpreparation using an Er:YAG laser on the osseointegration oftitanium implants: a histomorphometrical study in dogs. J OralRehabil. 2007;34:273-281.
41. Stübinger S, Landes C, Seitz O, et al. Er:YAG laser osteotomy forintraoral bone grafting procedures: a case series with a fiber-opticdelivery system. J Periodontol. 2007;78:2389-2394.
42. Ozdemir F, Demir HB, Oztoprak MO, et al. A report on the useof Er:YAG laser for pilot hole drilling prior to miniscrewinsertion. Lasers Med Sci. 2015;30:605-609.
43. Urban IA, Nagursky H, Lozada JL, et al. Horizontal ridgeaugmentation with a collagen membrane and a combination of
7
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1

particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 25 patients. Int JPeriodontics Restorative Dent. 2013;33:299-307.
44. Urban IA, Lozada JL, Jovanovic SA, et al. Vertical ridgeaugmentation with titanium-reinforced, dense-PTFEmembranes and a combination of particulated autogenousbone and anorganic bovine bone-derived mineral: aprospective case series in 19 patients. Int J Oral MaxillofacImplants. 2014;29:185-193.
45. Wang HL, Boyapati L. “PASS” principles for predictable boneregeneration. Implant Dent. 2006;15:8-17.
46. Kesler G, Shvero DK, Tov YS, et al. Platelet derived growthfactor secretion and bone healing after Er:YAG laser boneirradiation. J Oral Implantol. 2011;37(spec no):195-204.
47. Aoki A, Mizutani K, Takasaki AA, et al. Current status of clinicallaser applications in periodontal therapy. Gen Dent.2008;56:674-687.
48. Kimura Y, Yu DG, Fujita A, et al. Effects oferbium,chromium:YSGG laser irradiation on canine mandibularbone. J Periodontol. 2001;72:1178-1182.
49. Wang X, Zhang C, Matsumoto K. In vivo study of the healingprocesses that occur in the jaws of rabbits followingperforation by an Er,Cr:YSGG laser. Lasers Med Sci.2005;20:21-27.
50. Mohammadi F, Hasheminasab M, Jahandide PP, et al.
Effectiveness of low level laser in minimizing edema andpromoting wound healing after third molar surgery: arandomized clinical trial. Journal of Cranio maxillofacialResearch. 2014;1:58-62.
51. Enwemeka CS, Parker JC, Dowdy DS, et al. The efficacy of low-power lasers in tissue repair and pain control: a meta-analysisstudy. Photomed Laser Surg. 2004;22:323-329.
52. Pinheiro A, Oliveira MG, Martins PP, et al. Biomodulatory effects ofLLLT on bone regeneration. Laser Ther. 2000;13:73-79.
53. Campanha BP, Gallina C, Geremia T, et al. Low-level lasertherapy for im plants without initial sta bility. Photomed LaserSurg. 2010;28:365-369.
54. Gomes FV, Mayer L, Massotti FP, et al. Low-level laser therapyimproves peri-implant bone formation: resonance frequency,electron microscopy, and stereology findings in a rabbit model.Int J Oral Maxillofac Surg. 2015;44:245-251.
55. Bozkaya S, Cakir M, Peker E, et al. Effect of low-level lasertherapy on neurosensory recovery after dental procedures.Poster presented at: American Association of Oral andMaxillofacial Surgeons 96th Annual Meeting, ScientificSessions & Exhibition; September 11, 2014; Honolulu, HI.
56. Miloro M, Repasky M. Low-level laser effect on neurosensoryrecovery after sagittal ramus osteotomy. Oral Surg Oral MedOral Pathol Oral Radiol Endod. 2000;89:12-18.
8
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1

POST EXAMINATION QUESTIONS
1. The growth of diode lasers as soft-tissue handpiecesevolved, in part due to their ability to work safely withpacemakers, and their usefulness in being able to beused around implants, crowns, amalgams, and othermetal substructures while minimizing the risk ofcreating iatrogenic damage. a. True b. False
2. The erbium family of hard-tissue lasers (Er,Cr:YSGGand Er:YAG wavelengths) made their appearance indentistry in the late 1990s and were heralded initiallyfor their ability to cut only tooth structure. a. True b. False
3. The ability to ablate anything with water in it, made itpossible to use these “all-tissue lasers” for the
removal of porcelain veneers and all ceramicporcelain restorations in an efficient, safe andpredictable manner. a. True b. False
4. More recently, the Er:YAG laser has been promotedfor its role in periodontics as it possesses suitablecharacteristics for the effective elimination ofgranulation tissue, gingival melanin pigmentation,and gingival discoloration. a. True b. False
5. The role of lasers in dental implantology was exploredby Romanos et al, and they mentioned that laserscould be used for the treatment of peri-implantitis. a. True b. False
6. Kusek showed that the use of an erbium laser throughphotoacoustic streaming could reduce the bacteria inosteotomy sites that were infected by apicalpathology. a. True b. False
9
CONTINUING EDUCATION
POST EXAMINATION INFORMATION
To receive continuing education credit for participation in this educational activity you must complete the program post examinationand receive a score of 70% or better.
Traditional Completion Option:You may fax or mail your answers with payment to Dentistry Today (see Traditional Completion Information on following page). Allinformation requested must be provided in order to process the program for credit. Be sure to complete your “Payment,” “PersonalCertification Information,” “Answers,” and “Evaluation” forms. Your exam will be graded within 72 hours of receipt. Upon successfulcompletion of the post-exam (70% or higher), a letter of completion will be mailed to the address provided.
Online Completion Option:Use this page to review the questions and mark your answers. Return to dentalcetoday.com and sign in. If you have not previously purchased the program, select it from the “Online Courses” listing and complete the online purchase process. Oncepurchased the program will be added to your User History page where a Take Exam link will be provided directly across from theprogram title. Select the Take Exam link, complete all the program questions and Submit your answers. An immediate grade reportwill be provided. Upon receiving a passing grade, complete the online evaluation form. Upon submitting the form, your Letter of Completion will be provided immediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time in the future to access previously purchased programs and view or printletters of completion and results.
Lasers in Implant Dentistry, Part 1
This CE activity was not developed in accordance with AGDPACE or ADA CERP standards. CEUs for this activity will notbe accepted by the AGD for MAGD/FAGD credit.

7. Some lasers are not antibacterial in nature and cannotall be used to varying degrees to disinfect a site. a. True b. False
8. All lasers can ablate soft tissue, and thus can be usedto make incisions in soft tissue. a. True b. False
9. The greatest benefit for using erbium lasers might beduring the initial osteotomy guide hole, where bursmight “slip” or “bounce” off irregular or sloped bonysurfaces often seen during immediate implantprocedures after extractions. a. True b. False
10. The erbium laser cannot be safely used to trim softtissue around healing abutments. a. True b. False
11. The mechanism of action for low levels of nearinfrared laser energy to have either a biostimulatoryor bioinhibitory effect lies in the energy beingabsorbed by cell mitochondria, which in turnproduces a reactive oxygen species and releasesnitric oxide in the cell. a. True b. False
12. Studies have shown that low levels of lasertherapeutical energy provided clinical effects oninjured nerves that revealed an increase in nervefunction and improved capacity for myelinproduction. a. True b. False
10
CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1

CONTINUING EDUCATION
Lasers in Implant Dentistry, Part 1PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activity traditionally (mail or fax) rather than online, you must provide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer at least 9 of the 12 questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $60.00 Credit Hours: 3
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additional questions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved. Content was useful and benefited your clinical practice. Review questions were clear and relevant to the editorial. Illustrations and photographs were clear and relevant.Written presentation was informative and concise.
How much time did you spend reading the activity and completing the test?What aspect of this course was most helpful and why?
What topics interest you for future Dentistry Today CE courses?
ANSWER FORM: VOLUME 34 NO. 7 PAGE 134Please check the correct box for each question below.
1. o a. True o b. False 7. o a. True o b. False 2. o a. True o b. False 8. o a. True o b. False 3. o a. True o b. False 9. o a. True o b. False 4. o a. True o b. False 10. o a. True o b. False 5. o a. True o b. False 11. o a. True o b. False 6. o a. True o b. False 12. o a. True o b. False
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
11
This CE activity was not developed in accordance with AGDPACE or ADA CERP standards. CEUs for this activity will notbe accepted by the AGD for MAGD/FAGD credit.