Embed Size (px)
Citation preview
LATE COMPLICATIONS OF FRACTURES

LATE COMPLICATIONS
• Delayed union• Non-union• Malunion• Joint stiffness• Myoisitis ossificans• Avascular necrosis• Algodystrophy• Osteoarthritis
• Joint instability• Muscle contracture
(Volkmann’s contracture)
• Tendon lesions• Nerve compression• Growth disturbance• Bed sores
DELAYED UNION
• Fracture that has not healed in the expected time for type of fracture, patient and method of repair
• CausesCauses Inadequate blood supply Severe soft tissue damage Periosteal stripping Excessive traction Insufficient splintage Infection

PERKINS’ TIME TABLE
Upper LimbUpper Limb Lower LimbLower Limb
Callus visibleCallus visible 2-3 wks2-3 wks 2-3 wks2-3 wks
UnionUnion 4-6 wks4-6 wks 8-12 wks8-12 wks
ConsolidationConsolidation 6-8 wks6-8 wks 12-16 wks12-16 wks
Clinical featuresClinical featuresPersistent pain at fracture siteInstability at fracture siteNon weight bearingDisuse muscle atrophy
X-RayX-Ray Visible fracture line Very little callus formation or periosteal reaction

• TreatmentTreatment ConservativeConservative
- To eliminate any possible cause
- Immobilization
- Exercise OperativeOperative
- Indication :
Union is delayed > 6 mths
No signs of callus formation
- Internal fixation & bone grafting

treatment of delayed union fractures
• If alignment is adequate implants are stable but motion exists at fracture sites: apply rigid fixation
• If alignment is poor: straighten and apply rigid fixation
• If reduction is inadequate: treat as nonunion

NON-UNION
• Fracture has not healed and is not likely to do so without intervention
• Healing has stopped.Fracture gap is filled by fibrous tissue (pseudoarthrosis)
causes of nonunion • Instability at fracture site
– inadequate method of stabilization, inadequate postop care
• Inadequate blood supply at fracture– Poor surgical technique following open reduction, following
trauma at time of frature
• Infection• Excessive gap at fracture site
– Bone loss, distracting force not counteracted by method of fixation, bone loss from ischemia or infection
• Excessive postop use of limb• Use of improper metals or combinations of dissimilar
metals• Excessive quantities of implants
Clinical featuresClinical features Painless movement at the fracture site No pain at fracture siteInstability at fracture siteMay be weight bearing with pseudoarthrosis
X-RayX-Ray
Fracture is clearly visibleFracture ends are rounded, smooth and scleroticAtrophic non-unionAtrophic non-union : - Bone looks inactive
(Bone ends are often tapered / rounded) - Relatively avascular Hypertrophic non-unionHypertrophic non-union : - Excessive bone formation
` - on the side of the gap - Unable to bridge the gap

Hypertrophic non-Hypertrophic non-unionunion
Atrophic non-unionAtrophic non-union

treatment of the 2 types of nonunion fractures.
• Vascular nonunion– Rigid immobilization– Open reduction and compression of fracture with
cancellous bone graft
• Avascular nonunion– Surgery required– Open medullary canal, debride sclerotic bone– Apply rigid fixation– Cancellous bone graft

MALUNION
• Condition when the fragments join in an unsatisfactory position (unaccepted angulation, rotation or shortening)
• CausesCauses Failure to reduce a fracture adequately Failure to hold reduction while healing proceeds Gradual collapse of comminuted or osteoporotic
bone.

• Clinical featuresClinical features Deformity & shortening of the limb Limitation of movements
TreatmentTreatment Angulation in a long bone (> 15 degrees)
→ Osteotomy & internal fixation Marked rotational deformity
→ Osteotomy & internal fixation Shortening (> 3cm) in 1 of the lower limbs
→ A raised boot OR Bone operation

JOINT STIFFNESS
• Common complication of fracture Treatment following immobilization
• Common siteCommon site : knee, elbow, shoulder, small joints of the hand
• CausesCausesOedema & fibrosis of the capsule, ligaments, muscle
around the jointAdhesion of the soft tissue to each other or to the
underlying bone (intra & peri-articular adhesions)Synovial adhesions d/t haemarthrosis

• TreatmentTreatmentPrevention :Prevention :
- Exercise- If joint has to be splinted → Make sure in correct position
Joint stiffness has occurred:Joint stiffness has occurred:- Prolonged physiotherapy- Intra-articular adhesions → Gentle manipulation under anaesthesia followed by continuous passive motion- Adherent or contracted tissues → Released by operation

MYOSITIS OSSIFICANS
• Heterotopic ossification in the muscles after an injury
• Usually occurs inDislocation of the elbowA blow to the brachialis / deltoid / quadriceps
CausesCauses (thought to be due to) muscle damageWithout a local injury (unconscious / paraplegic patient)

• Clinical featuresClinical featuresPain, soft tissue tendernessLocal swellingJoint stiffness Limitation of movementsExtreme cases: - Bone bridges the joint
- Complete loss of movement (extra-articular ankylosis)
X-RayX-RayNormalFluffy calcification in the soft tissue

• TreatmentTreatmentEarly stage : Joint should be restedThen : Gentle active movementsWhen the condition has stabilized :
Excision of the bony massAnti-inflammatory drugs may ↓ joint stiffness

AVASCULAR NECROSIS• Circumscribed bone
necrosis
• CausesCauses Interruption of the arterial
blood flowSlowing of the venous
outflow leading to inadequate perfusion
• Common site :Common site : Femoral headFemoral headFemoral condylsHumeral headCapitulum of humerus ScaphoidScaphoid (proximal part) TalusTalus (body)Lunate
• Conditions associated with AVNConditions associated with AVNPerthes’ diseaseEpiphyseal infectionSickle cell diseaseCaisson diseaseGaucher’s diseaseAlcohol abuseHigh-dosage corticosteroid

• Clinical featuresClinical featuresJoint pain, stiffness, swellingRestricted movement
X-RayX-Ray↑ bone densitySubarticular fracturingBone deformity

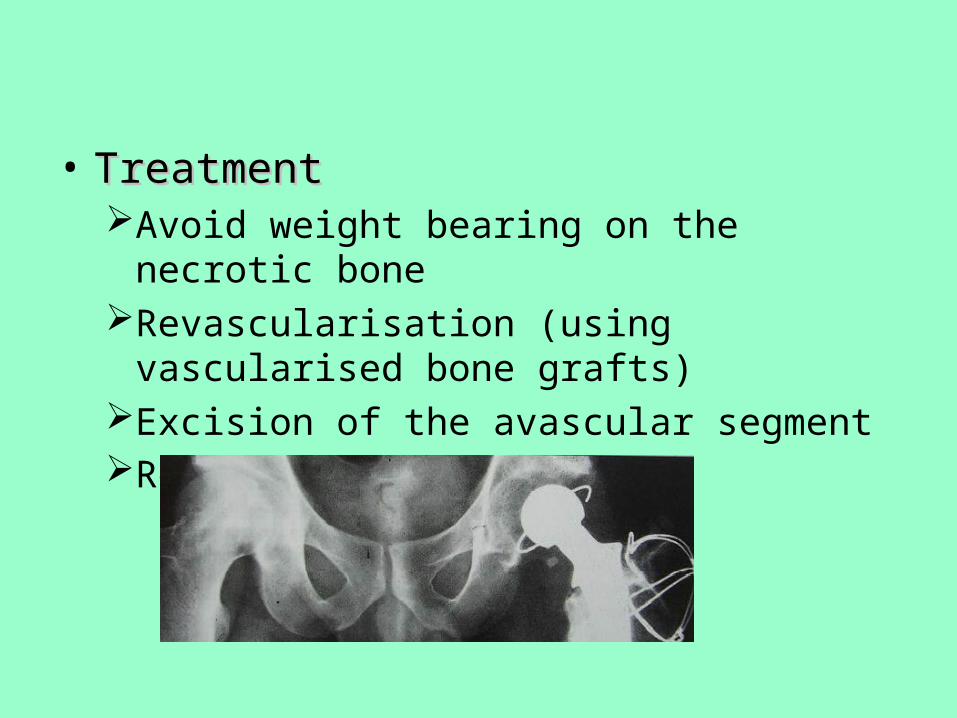
• TreatmentTreatmentAvoid weight bearing on the necrotic boneRevascularisation (using vascularised bone grafts)Excision of the avascular segmentReplacement by prostheses

ALGODYSTROPHY(COMPLEX REGIONAL PAIN SYNDROME)
• Previosly known as Sudeck’s atrophy
• Post-traumatic reflex sympathetic dystrophy
• Usually seen in the foot / hand
(after relatively trivial injury)
• Clinical featuresClinical featuresContinuous, burning painEarly stage : Local swelling, redness, warmthLater : Atrophy of the skin, musclesMovement are grossly restricted

• X-RayX-RayPatchy rarefaction of the bones (patchy osteoporosis)
OsteoporosisOsteoporosis AlgodystrophyAlgodystrophy

TreatmentTreatmentPhysiotherapy (elevation & active exercises)Drugs
- Anti-inflammatory drugs
- Sympathetic block or sympatholytic drugs
(Guanethidine)

OSTEOARTHRITIS
• Post-traumatic OAPost-traumatic OA Joint fracture with severely damaged articular
cartilageWithin period of months
secondary OAsecondary OACartilage healsIrregular joint surface may caused localized stress
→ secondary OAYears after joint injury

• Clinical featuresClinical featuresPainStiffnessSwellingDeformityRestricted movement
• TreatmentTreatmentPain relief : Analgesics
Anti-inflam agent
Joint mobility : PhysiotherapyLoad reduction : wt reductionRealignment osteotomy (young
pt)Arthroplasty (pt > 60yr)

Thank You






![13-02 CRP DM Late Complications.ppt [Read-Only] · Late Complications Navneet Majhail, MD, MS ... App Version • Patient and ... diffuse infiltrat es, ground glass infiltrates, lung](https://img.pdfslide.net/doc/110x75/5c7a8ec409d3f207058c61f6/13-02-crp-dm-late-read-only-late-complications-navneet-majhail-md-ms-.jpg)