Embed Size (px)
DESCRIPTION
Late Onset Schizophrenia
Citation preview

VOL 14, NO 1, 1988 Late-Onset Schizophrenia:An Overview
by M. Jackuelyn Harrisand Dillp V. Jeste
Abstract
Onset of schizophrenia after theage of 40 has been a controversialtopic. We reviewed more than 30publications (mainly from Europe)on this subject. Many of thestudies had methodologicalshortcomings, including problemsin precisely dating the onset ofschizophrenia. Nonetheless, itappears that a certain proportionof patients present for the firsttime with diagnosable schizo-phrenia after age 40. Late-onsetschizophrenia is characterized byparanoid symptomatology, a highfemale:male ratio, an elevatedprevalence of hearing loss andocular pathology, schizoid orparanoid traits in premorbidpersonality, a tendency towardchronicity, and symptomaticimprovement with neuroleptics.Family studies suggest that theprevalence of schizophrenia inrelatives of late-onset schizo-phrenic probands is higher thanthat in the general population,but lower than that in relativesof earlier-onset schizophrenicprobands. We believe that late-onset schizophrenia is a validentity (or group of entities).Studies of the course, biologicalassociations, neuropsychologicalperformance, and pharmacologicalcharacterization of late-onsetschizophrenia are wan-anted.
I got the starting point of theline of thought which in 1896led to dementia praecox beingregarded as a distinct disease,on the one hand, from theoverpowering impression of thestates of dementia quite similarto each other which developedfrom the most varied initialclinical symptoms, on the otherhand from the experienceconnected with the observationsof Hecker that these peculiardementias seemed to stand in
near relation to the period ofyouth. . . It has since beenround that the assumptionsupon which the name chosen(dementia praecox) rested are atleast doubtful. As will have tobe explained more in detaillater, the possibility cannot inthe present state of our knowl-edge be disputed, that a certainnumber of cases of dementiapraecox attain to complete andpermanent recovery, and alsothe relations to the period ofyouth do not appear to bewithout exception.—EmitKrnepelm (1919/1971, pp. 3-4).
The onset of schizophrenia in midto late life has been a controversialissue. Kraepelin (1919/1971) usedthe term "dementia praecox" todescribe a state characterized by". .a peculiar destruction of theinternal connections of the psychicpersonality" with the predominanteffects in the "emotional andvolitional spheres of mental life"(p. 3). He observed that most ofthese peculiar dementias developedduring youth. As suggested bythe quote above, however,Kraepelin did go on to questionthe appropriateness of the term"dementia praecox" for describingthis illness since all cases did notresult in a permanent dementia (aterm he used for loss of volitionover thinking, feeling, and acting)nor was the onset found to berestricted to adolescence andyoung adulthood. Yet, Kraepelinoften included patients withpredominantly paranoid symptomsstarting after early adult lifeunder the category "paraphrenia."Followup studies of Kraepelin'sparaphrenic cases by Mayer (1921)and Mayer-Gross (1932) found,
Reprint requests should be sent toDr. M J. Harris, Psychiatry Service,V116A, San Diego Veterans Adminis-tration Medical Center, San Diego, CA92161.
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

40 SCHIZOPHRENIA BULLETIN
however, that many of thosepatients had a course of illnesssimilar to that of patientsKraepelin had called dementiapraecox.
Confusion over terms such aslate-onset schizophrenia, para-phrenia, late paraphrenia, andparanoid states has persisted tothis date. It is intriguing that, inspite of a number of European(especially German and British)investigations reporting that about20 percent of schizophrenicpatients have onset of symptomsafter age 40 (see table 1), Americanresearchers have been relativelyuninterested in the entity oflate-onset schizophrenia or para-phrenia.'
One possible reason may be thehistorical tendency to diagnosesuch patients as having affectiveor organic disorders (Roth andMorrissey 1952). Recently, DSM-III(American Psychiatric Association1980) recommended exclusion ofthe diagnosis of schizophrenia ifsymptoms started after age 45.This age cutoff was not based onany published hard data. Tocorrect this problem and to allowfor a possible diagnosis of schizo-phrenia developing after the ageof 44, the DSM-111 Revised(American Psychiatric Association1987) has introduced the categoryof late-onset schizophrenia.
If schizophrenia does occur inlater life, recognition of this entityis important for clinical as well asresearch purposes. Clinically, theprevalence, symptomatology,course, and prognosis of late-onset
1 There are some notable recentexceptions, including studies byRabins et al. (1984) and Miller et al.(1986) and reviews by Bridge andWyatt (1980a, 1980b), Gold (1984), andVolavka (1985).
schizophrenia must be evaluatedin order to diagnose and provideappropriate treatment for thispatient population. Such data willalso serve as a basis for furtherstudies into the etiology andpathogenesis of this condition.
The purpose of this article is toreview the available literature onlate-onset schizophrenia/para-phrenia critically so as to obtainat least tentative impressionsabout its prevalence and clinicalcharacteristics. We hope that suchan overview will help generateinterest in studies of patients whodevelop schizophrenic symptomslate in life.
Chronology of the Develop-ment of Terminology forLate-Onset Schizophrenia
Historically, the onset of a psy-chotic illness in late life notsecondary to an organic oraffective disorder has been referredto as late-onset schizophrenia,paraphrenia, late paraphrenia, orinvolutional psychotic reaction.The terminology has been useddifferently by different inves-tigators resulting in considerableconfusion. Below is a listing ofsome major milestones in thisarea.
Guislain (19th Century): The term"paraphrenia" was used in theearly part of the 19th century byGuislain, who employed itsynonymously with a clinicalsyndrome then known as "folly";the latter is roughly the equivalentto today's schizophrenia (Hinsieand Campbell 1974).
Kraepelin (1919/1971): Kraepelinused the term "dementia praecox"to describe an illness with onsetusually in youth resulting inchronic deterioration of themental processes responsible foremotion and volition. He also
used the term "paraphrenia" todescribe a group of cases that hadmany points in common withdementia praecox but with lesserdisturbance of emotion andvolition. Kraepelin classifiedparaphrenia into four groups:paraphrenia systematica, para-phrenia expansiva, paraphreniaconfabulans, and paraphreniaphantastica.
Paraphrenia systematica wasdescribed as an extremely insidiousdevelopment of a progressivedelusion of persecution. Later,ideas of exaltation, ideas ofreference, and auditory hallucina-tions appeared. The capacity towork was preserved for a longtime. Sixty percent of Kraepelin'spatients were males. Over halfthe patients had onset ofsymptoms between ages 30 and40, and a little more than 20percent between ages 40 and 50.Only isolated cases began beforethe 25th or after the 50th year.
Paraphrenia expansiva wasdescribed as "exuberantmegalomania with predominatelyexalted mood and slight excite-ment" (p. 3). Hallucinationsappeared fairly early. Later,delusions became somewhat morenonsensical and more discon-nected. There was a lack ofjudgment, a certain incoherence,superficiality of emotions, andweakness of volition but no"disintegration of the psychicpersonality." Unlike mania, thecourse was chronic. Almost all ofKraepelin's patients were women.The onset of symptoms in 75percent of the patients wasbetween 30 and 50 years of age.One patient had onset ofsymptoms at age 64 without anysigns of senile dementia.
Paraphrenia confabulans wascharacterized by delusions ofpersecution and exaltation.
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 14, NO 1, 1988 41
Pseudomemories (i.e., "memories"of impossible events, such ashaving fought in a war twocenturies ago) occurred as well asmegalomania. The mood washappy, yet later became irritable,morose, or indifferent. Manypatients also heard voices overthe course of the illness, and thedelusions became more nonsensicaland incoherent. Both sexes wereequally represented. The age ofonset was evenly distributedbetween the 20th and 50th years.
Paraphrenia phantastica wasdescribed as being characterizedby highly extraordinary, discon-nected, and changing delusions.There were ideas of persecution,auditory hallucinations, delusionsof personal influence, andpseudomemories. The mood wassomewhat exalted or indifferent,but sometimes gloomy or strained.The patients were sometimesinclined to violence. Speech wascharacterized by neologisms orsilly plays on words. Manysentences were incomprehensible.The course was progressive, andthe speech became more confusedand disconnected. Males predomi-nated, accounting for 60 to 70percent of the cases. Twenty-fivepercent of the cases had onsetafter age 40.
There is a great overlap betweenthese clinical pictures of para-phrenia and those of differentpatients with dementia praecox.Although Kraepelin stressed anabsence of personality disintegra-tion in the first two subtypes ofparaphrenia (systematica andexpansiva), he also reported thatsome patients with dementiapraecox (especially paranoid type)also did not have marked deterio-ration of functioning. Indeed,followup studies of Kraepelin'sparaphrenic patients by otherinvestigators found that a number
of them resembled those withdementia praecox (Mayer 1921;Mayer-Gross 1932).
Bleuler (1943): Bleuler describedlate schizophrenia as having onsetafter age 40 with symptoms notvery different from those ofearly-onset schizophrenia. Bleulerexcluded psychotic symptomscaused by pathologic hrain distur-bances or amnesic syndrome.
DSM-1 (American PsychiatricAssociation 1952): Involutionalpsychotic reaction was a classifica-tion for psychotic reactionsoccurring in the involutionalperiod, with some cases charac-terized chiefly by depression andothers by paranoid ideas. Thecourse was usually long andsymptoms included anxiety,intractable insomnia, guilt, agita-tion, somatic concerns, andsometimes delusions. It waspointed out that differentiationfrom other psychotic reactionswith onset in this age group wasdifficult and patients were not tobe included in this categorymerely because of their age.
Kay and Roth (1950's and 1960's):During the 195CS and early1960's, Kay and Roth investigatedlate-onset paranoid psychosis.Their definitions of paraphreniaand late paraphrenia evolved overthis time period suggest that theirdifferentiation of paraphreniafrom late-onset paranoid schizo-phrenia was blurred. Roth andMorrissey (1952) described 12schizophrenic patients with onsetof symptoms after age 60 charac-terized by prominent "paraphrenicdelusions" occurring in the settingof a well-preserved personalityand "usually associated with thepassivity feelings or other voli-tional disturbances and hallucina-tions in clear consciousnesspathognomonic of schizophrenia."
Hopkins and Roth (1953) used
the term "paraphrenia" to describethose in whom a well-organizedsystem of paranoid delusions,usually with auditory hallucina-tions, existed in the setting of awell-preserved personality andaffective response.
Roth (1955) believed that in themajority of paraphrenic patientsthe illness began after age 60. Henoted that "the clinical picturehas many similarities to theparanoid illness described byKraepelin under the heading ofparaphrenia (later shown to be arelatively late form of schizophre-nia)," and used the name "lateparaphrenia" for this group inplace of schizophrenia.
Kay and Roth (1961) used lateparaphrenia to describe a paranoidsymptom complex with no signsof organic dementia or confusion.From the content of the delusionsand hallucinations, the illness wasjudged not to be a primaryaffective disorder. The patientshad "more or less well-markedschizophrenic symptoms," with asmall proportion having nohallucinations. The investigatorswere able to divide the lateparaphrenic patients into threegroups.
Group 1—Twenty percent ofthe late paraphrenic cases hadabnormal personalities before theonset of the paranoid psychoses.Hallucinations were absent. Theage of admission was often over75. Delusions were confined totheft, poisoning, or ill treatmentby people in contact with them.The symptoms appeared to be anextension of longstanding personal-ity traits.
Group 2—Twenty-five percentof the late paraphrenic patientswere in this group in which thedelusions were said to be some-what understandable in the lightof their circumstances or to have
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

42 SCHIZOPHRENIA BULLETIN
followed prolonged social isolation.Group 3—The majority (55
percent) of late paraphrenicpatients had symptoms that couldnot be attributed either to socialstressors or to long-term personal-ity disorders. These patients wereconsidered to have "endogenous"paraphrenia.
Leonhard (1959): In his classifica-tion of schizophrenia, Leonhardused the term "paraphrenia" torefer to all paranoid schizophrenicswithout distinction as to the ageof onset. Other German authorsalso used the term in this manner(Fish 1960).
Post (1966): Post classifiedpatients who were suffering fromparanoid symptoms that appearedfor the first time after age 50 andwere unrelated to affective illnessinto three categories, according tosymptoms: paranoid hallucinosis,schizophreniform syndrome, andschizophrenic syndrome.
In "paranoid hallucinosis,"auditory hallucinations were theonly type of psychotic experienceassociated with delusions ofpersecution. The "schizo-phreniform syndrome" was char-acterized by paranoid experiencesthat were somewhat more under-standable or psychodynamicallymore comprehensible. Patientslabeled as having "schizophrenicsyndrome" had Schneiderian firstrank symptoms. Post felt thatpatients who met criteria for thislast category would clearly bediagnosed as having paranoidschizophrenia or paraphrenia bypsychiatrists of different schools.After a 3-year followup, Post wasunable to discover any clearetiological differences among thethree syndromes and concludedthat they were merely threedifferent symptom clusters ar-ranged along a continuum.
DSM-U (American PsychiatricAssociation 1968): DSM-U did nothave an age cutoff for making thediagnosis of schizophrenia. Itdescribed a paranoid psychosischaracterized by delusion forma-tion with onset in the involutionalperiod as involutional paranoidstate (involutional paraphrenia).The latter was distinguished fromschizophrenia by the absence ofconspicuous thought disordertypical of schizophrenia.
Feighner et al. (1972): TheFeighner research criteria forschizophrenia required that threeof five items had to be present tomake a definite diagnosis. One ofthese five items was onset beforeage 40.
RDC (1978): The ResearchDiagnostic Criteria (Spitzer et al.1978) had no age specifications forschizophrenia.
1CD-9 (World Health Organization1978): The ninth version of theInternational Classification ofDiseases did not have an agecutoff for schizophrenia. It definedparaphrenia as paranoid psychosiswith conspicuous hallucinations,often in several modalities.Affective symptoms and disorderedthinking, if present, did notdominate the clinical picture andthe personality was well pre-served.
DSM-1II (American PsychiatricAssociation 1980): DSM-HI did notrecognize paraphrenia or involu-tional paranoid disorder asdiagnoses. To make the diagnosisof schizophrenia, the onset ofsymptoms must be before age 45.DSM-III included a separatecategory of "paranoid disorders"to refer to persistent persecutorydelusions without prominenthallucinations or any of the majorsymptoms (criterion A) of schizo-phrenia. There was no age
restriction for diagnosing paranoiddisorders.
DSM-IU-R (American PsychiatricAssociation 1987): The DSM-III-RAdvisory Group recognized theneed to allow a diagnosis ofschizophrenia presenting for thefirst time after the age of 44.Accordingly, the revised versionof DSM-III has specified "lateonset" if the disturbance, includingthe prodromal phase, developsafter age 45.
Thus, it is clear that there is noconsensus about terminology forschizophrenic symptoms appearingfor the first time after 40 or 45years of life. Even worse, theclassification systems used bydifferent researchers have em-ployed arbitrary distinctions orcutoffs, with poor data base. Forinstance, the differentiationbetween paraphrenia and paranoidschizophrenia is not based on theresults of long-term studiescomparing these two entities.Roth (1955) and Post (1966), whoused the term paraphrenia, couldnot find any clear differencesbetween paraphrenia and schizo-phrenia.
Below we will attempt toreview the available data onlate-onset schizophrenia.
Studies of Late-OnsetSchizophrenia
A review of the literature wasdone to look at the prevalence,gender ratio, clinical descriptions,and family studies of late-onsetschizophrenia. We found articlespublished from 1913 to 1986.Most of the studies were Euro-pean. The studies were obtainedby using the Index Medicus andMed-Search. Cross-references fromthese articles were also used toobtain other original articles. In
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 14, NO 1, 1988 43
addition, references from bookson geriatric psychiatry were used.Articles written in a languageother than English were translated.
Before examining the findingsof the studies themselves, we willconsider the generic and specificlimitations of clinical investigationsinto late-onset schizophrenia.
1. There is a conceptual biasdue to the terminology used,leading to circular thinking. Therestriction placed by DSM-1I1(American Psychiatric Association1980) on the age of onset ofschizophrenia prevents cliniciansfrom even considering schizophre-nia in patients with onset ofpsychosis after age 44. Hence ananalysis of chart diagnoses since1980 is not likely to reveal thetrue prevalence of late-onsetschizophrenia. Such data couldthen be used to support the"conceptual basis" of the originaldiagnostic criterion. Similarly, theresults of family studies ofschizophrenia would be expectedto be biased by restricting the riskperiod to < 45 years.
In an ongoing investigation, wehave so far studied 15 patientswho met DSM-IU-R criteria forlate-onset schizophrenia (Jeste etal. 1987). Previously, most of thepatients had been diagnosed,using DSM-IH, as having either"atypical psychosis" or "paranoiddisorder."
2. Defining the age of onset ofschizophrenia is difficult forseveral reasons. The onset ofsymptoms is usually insidiousand therefore hard to pinpoint toa specific time. Premorbid schizoidor paranoid personality traitsfurther complicate determiningthe precise age of onset. Mostpatients do not have insight intothe early symptoms of theirillness. In elderly patients, there
may be age-associated memoryproblems that make it difficult torecall previous psychiatric historyas well as a lack of contemporariesto substantiate the patient'spsychiatric history.
3. There are problems infollowing late-onset schizophrenicpatients over time: (a) There maybe social isolation from a combina-tion of schizophrenia and old agewith a loss of important friends,family members, and spouses, sothat there are fewer concernedpeople to help ensure psychiatricfollowup. (b) Medical illnessesand even death interfere withevaluation of the course, treatmentresponse, and prognosis of theschizophrenic illness, (c) Sensorydeficits may complicate thesymptomatology as well asinterfere with driving, making itdifficult for patients to keepappointments, (d) Following thepatient's retirement, financialproblems may limit access tomedical care.
4. There may be a tendency toattribute paranoid symptoms inolder patients to other causessuch as (a) organic mental syn-dromes including medication-in-duced mental status changes, (b)affective disorders, or (c) sensorydeficits.
5. Symptoms of late-onsetschizophrenia may be mixed withage-related difficulties in learningand recent memory.
6. Research protocols forschizophrenia typically excludeolder patients, due to clinical aswell as human subjects considera-tions.
7. It is probable that late-onsetschizophrenia is not a homogene-ous entity, but a combination ofseveral different (and partlyoverlapping) subtypes. Separatingthese subtypes from one another
may need a detailed assessmentof relevant clinical and biologicalvariables.
Critique of Published Studies
The published studies on late-onset schizophrenia have fre-quently been fraught with impor-tant methodological and otherproblems.
Material. 1. Post (1966) attributedlow estimates of late-onset schizo-phrenia in some studies todifficulties in identifying suchpatients in the general population,even when evaluated by experi-enced psychiatrists. For example,he cited a study done by Kay etal. (1964) in which no patientsmeeting Roth's criteria for lateparaphrenia were found among309 persons over age 65 inNewcastle. Yet, a survey revealedthat there were at least eightparaphrenic patients from thatpopulation who had been ininstitutions or mental hospitals.Post believed from his conversa-tions with welfare workers thatseveral other reports of lowprevalence were underestimates.Post also gave an example of afamily setting where mentalillness was not discovered in anelderly man until after his deathwhen a diary was discovered inwhich nothing but paranoidexperiences had been recorded.
2. Most of the early investiga-tions were not conducted withthe goal of studying late-onsetschizophrenia. Rather, they weresurveys either of schizophrenia indifferent age groups or ofpsychosis in the elderly. Hencethey often neglected to givepertinent details of importantvariables, such as gender distribu-tion (e.g., Kraepelin 1919/1971;
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

SCHIZOPHRENIA BULLETIN
Robertson and Mason-Browne1953; Fish 1958, 1960; Herbert andJacobson 1967) or level of educa-tion (no studies gave this informa-tion).
3. Many studies that attemptedto evaluate the prevalence oflate-onset schizophrenia eitheramong schizophrenic patientsfrom various age groups oramong elderly psychiatric patientswere not true prevalence surveys.Their denominator populationusually consisted of series ofunselected patients (instead of,say, all the schizophrenic patientsfrom a specific catchment area).
4. Some investigators did notinclude appropriate controlgroups. For example, familystudies of late-onset schizophrenicpatients often failed to includeage-comparable normal controlsand patients with onset of schizo-phrenia at a younger age fromsimilar populations (Kay and Roth1961; Post 1966; Herbert andJacobson 1967; Larson and Nyman1970; Huber et al. 1975; Rabins etal. 1984).
Methods. 1. Many studies didnot mention the criteria used fordiagnosing schizophrenia, affectivedisorders, or organic mentalsyndromes (Robertson and Mason-Browne 1953; Kay and Roth 1961;Retterstol 1966; Larson andNyman 1970).
2. A number of studies werebased on retrospective chartreviews (Kay and Roth 1961;Larson and Nyman 1970; Rabinset al. 1984) or on assessmentsdone by clinicians other than theinvestigators (Angst et al. 1973;Bland 1977).
3. As noted earlier, there hasbeen considerable confusion inthe terminology used by different
authors; e.g., the term "lateonset" has been used to connoteonset after age 40, 45, 60, or 65.
4. Followup periods werevariable. Some patients werefollowed for only several months(Herbert and Jacobson 1967),while others were followed for 10to 30 years. Kraepelin's para-phrenic cases were followed byMayer (1921) and Mayer-Gross(1932). Other long-term followupswere done by Kay and Roth(1961), Post (1966), and Bleuler(1972).
5. Investigations into specificareas such as sensory loss areespecially difficult to evaluate.Studies looking at sensory loss inlate-onset schizophrenic patientsoften did not give their methodsof evaluating the sensory loss(Kay and Roth 1961; Herbert andJacobson 1967).
6. Most investigations did notdescribe treatment response,neuropsychological performance,or any major biological parameter.
It should be stressed in defenseof the studies in table 1, however,that clinical research into anumber of other psychiatricdisorders during the same timeperiod was methodologicallysimilar—i.e., it focused on clinicaldescriptions instead of on con-trolled studies of specific disorders.Furthermore, when we reanalyzedthe published data to take intoaccount relevant variables, wefound more similarities thandifferences in the results withrespect to late-onset schizophrenia.
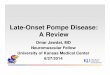
Epidemiology. Table 1 listsstudies that looked at certainepidemiological aspects of late-onset schizophrenia in relativelylarge populations of patients.(Patients said to have late-onset
paraphrenia have been includedin the category of late-onsetschizophrenia.) We excluded casereports.
Prevalence. As stated earlier, amajor drawback in many investiga-tions of the prevalence of late-onset schizophrenia was that thecase samples came from a seriesof unselected patients. Hence, inthe discussion below, we havepreferred the term "proportion"to "prevalence." Eight studiesreported on the occurrence of lateonset (generally defined as onsetafter age 40) among schizophrenicpatients from various age groups(Kolle 1931 [who included twodifferent populations of patients];Fish 1958; Retterstol 1966; Larsonand Nyman 1970; Bleuler 1972;Huber et al. 1975; Bland 1977).The weighted mean proportion(weighted by sample size) oflate-onset schizophrenia in theseeight studies was 23.5 percentwith the range being 15.4 percent(Retterstol 1966) to 32.0 percent(Larson and Nyman 1970). Kraepe-lin (1919) and Schulz (1933)specifically excluded paraphrenicpatients from their populationswith dementia praecox. The meanproportion of late-onset schizo-phrenia in these two reports wasonly 5.6 percent. As discussedearlier, however, the distinctionbetween paraphrenia and schizo-phrenia is unclear.
Robertson and Mason-Browne(1953), Muller (1959), and Larsonand Nyman (1970) examined theproportion of late-onset schizo-phrenia among elderly schizo-phrenic populations. The meanwas 31.0 percent. The remaininginvestigations included eithersurveys of all elderly psychiatricpatients or only late-onset schizo-phrenic patients.
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

Ta
ble
1.
Stu
die
s o
f la
te-o
nset
sch
izo
ph
ren
ia
Aut
hor
Kra
epel
in(1
919/
1971
)
May
er(1
921)
Kol
le (193
1)
Kol
le (193
1)
Sch
ulz
(193
3)
Ble
uler
(194
3,19
72)
Pat
ient
po
pu
lati
on
Pat
ient
s w
ith d
iagn
osis
of d
emen
tia p
raec
oxex
clud
ing
para
phre
nia
Fol
low
up o
f K
raep
elln
'spa
raph
reni
c pa
tient
s
Sch
izop
hren
ic p
atie
nts
Sch
izop
hren
ic p
atie
nts
Sch
izop
hren
ic p
atie
nts,
excl
udin
g pa
raph
reni
a
Late
-ons
et s
chiz
o-ph
reni
c pa
tient
s
To
tal
1,05
4 78 889
182
660
730
Dia
gn
ost
ic c
rite
ria
Par
aphr
enia
-par
anoi
a&
hal
luci
natio
ns,
late
rag
e of
onse
t, no p
ro-
gres
sion
to
dem
entia
,no
affe
ctiv
e bl
untin
g or
thou
ght
diso
rder
Kra
epel
in's
def
initi
onof
par
aphr
enia
Sch
izop
hren
ia—
Sch
neid
er's
firs
t-ra
nksy
mpt
oms
Sch
izop
hren
ia—
Sch
neid
er's
firs
t-ra
nksy
mpt
oms
Late
-ons
et s
chiz
o-ph
reni
a—on
set
afte
r 4
0
Late
-ons
et s
chiz
o-ph
reni
a—on
set
afte
r40
, not
seco
ndar
y to
orga
nic
path
olog
y
nw
ith
late
on
set
61 78 142 33 35 130
Dis
trib
uti
on
of a
ge
of
onse
tA
ge
41
-45
46
-50
51
-55
56
-60
41
-60
>6
0
41
-60
>6
0
40
-^4
45
-49
50
-54
55
-60
>6
0
n 35 13 11 2
?
88 54 33 0 45 43 21 16 5
Fem
ale
mal
e
Pre
dom
-in
ance
of
wom
en ? 7 7 7
1.9:
1
Co
mm
ents
Kra
epel
in s
tate
d th
atat
lea
st 4
0% o
f pa
tient
sdi
agno
sed
as
para
-ph
reni
a w
ould
pro
gres
sto
dem
entia
pra
ecox
>4
0%
dev
elop
edco
urse
of
dem
entia
prae
cox
Dro
p In
inci
denc
e of
late
-ons
et s
chiz
o-ph
reni
a ov
er a
ge 6
0,
acco
rdin
g to
Ble
uler
,w
as d
ue to
cho
osin
a
Lech
ler
Psy
chia
tric
inp
atie
nts
355
(195
0)
over
age 6
5
Rob
erts
on
Fem
ale
patie
nts
over
23
& M
ason
6
0, h
ospi
taliz
ed b
e-
Bro
wne
tw
een
1946 a
nd
195
1,(1
953)
w
ith p
arap
hren
ia o
rsc
hizo
phre
nia
Late
-ons
et s
chiz
o-ph
reni
a—on
set
afte
r 40
Not
sta
ted
30
an i
nvol
utio
nal
diag
-no
sis
in p
refe
renc
e to
para
phre
nic
or
schi
zo-
phre
nic
diag
nosi
s
In t
hose
with
ons
etaf
ter
65
, 14
of
18ca
ses
of
late
-ons
etsc
hizo
phre
nia
mls
diag
-no
sed
as
arte
rio-
scle
rotic
or
seni
lede
men
tia
All
had
age
>6
0A
ll w
omen
by guest on November 20, 2014http://schizophreniabulletin.oxfordjournals.org/Downloaded from

Tab
le 1
. S
tud
ies
of
late
-on
set
sch
izo
ph
ren
ia—
Co
nti
nu
ed
Aut
hor
Fis
h (195
8)
Pat
ien
t p
op
ula
tio
n
Fem
ale
chro
nic
schi
zo-
phre
nic
patie
nts
from
all
war
ds o
f a
men
tal
hosp
ital
exce
ptge
riatr
ic w
ard
To
tal
110
Dia
gn
ost
ic c
rite
ria
Sch
izop
hren
ia w
ithon
set
afte
r 4
0
nw
ith
late
on
set
22
Dis
trib
uti
on
of a
ge
of
on
set
Ag
e n
40-*
9 13
50-5
9 9
>60
1
Fem
ale:
mal
e
All
wom
en
Co
mm
ents
Fis
h fe
lt th
at t
he
num
ber
with
lat
e-on
set
schi
zoph
reni
a m
ay
have
bee
n un
der-
estim
ated
due to
Mul
ler
(195
9)
Fis
h (196
0)
Kay
4 R
oth
(Rot
h19
55;
Kay
& R
oth
1961
; K
ay19
63)
Sjo
gren
(196
4)
Ret
ters
tol
(196
6)
Her
bert &
Jaco
bson
(196
7)
101
elde
rly p
atie
nts
with
sch
izop
hren
ia
All
hosp
italiz
edps
ychi
atric
pat
ient
sov
er 6
0
Hos
pita
lized
pat
ient
sw
ith l
ate
para
phre
ma.
Aut
hors
exa
min
ed 4
2pa
tient
s &
rev
iew
ed 5
7pa
tient
s' c
hart
s
Sw
edis
h m
enta
l hos-
pita
l pa
tient
s ov
er a
ge
70,
with
"fu
nctio
nal"
psyc
hiat
ric d
isor
ders
84 p
aran
oid
schi
zo-
phre
nic
patie
nts
All
hosp
italiz
ed p
a-
tient
s age >
65
exam
ined
& f
ollo
wed
for
seve
ral
mon
ths
Lars
on&
Nym
an(1
970)
All
schi
zoph
reni
cm
ales
adm
itted
to
a m
enta
l w
ard
&
101
Sch
izop
hren
ia w
ith
34
onse
t af
ter
40
264
Sch
izop
hren
ia w
ith
16on
set
over
40
99
Late
par
aphr
enia
- 99
para
noid
sym
ptom
sw
ith c
ompl
ex d
elus
ions
& o
ccas
iona
l ha
llu-
cina
tions
not
seco
nd-
ary
to o
rgan
ic o
raf
fect
ive
dis
ord
er,
age
of
onse
t >
60
649
Late
par
aphr
enia
, 202
as p
er
Kay
& R
oth
(196
1)
84
Late
-ons
et s
chiz
o-
13ph
reni
a—on
set
afte
r40
47
Late
par
aphr
enia
: age
47
>6
5 o
n a
dmis
sion
,sy
stem
ized
del
usio
nsw
ith o
r w
ithou
t ha
llu-
cina
tions
in
cle
arco
nsci
ousn
ess.
Ons
et<
55
, se
nous
dem
entia
& c
hron
ic s
chiz
o-ph
reni
a ex
clud
ed
153
Late
-ons
et s
chiz
o-
49
phre
nia—
age
of
onse
t>
40
Cha
rt r
evie
w
41
-60
>6
0
>50
51-5
961
-71
All
had o
n-
set
afte
rag
e 60
29 5 5 4 7
? ? 7:1
40
-49
>5
0
[Age
at
a65
-69
70-7
475
-79
80-8
485
+
10 3
dmis 9 11 13 10 4
45:2
excl
usio
n of
ger
iatr
icw
ards
. C
linic
al p
ictu
redi
d not
diffe
r fr
ompa
tient
s w
ith o
nset
befo
re a
ge 4
0
No
dist
inct
ive
clin
ical
pic
ture
Par
aphr
enic
s co
n-
stitu
ted
10%
of all
adm
issi
ons
over
age
60.
Aut
hors
con
clud
edth
at s
chiz
ophr
enia
in
old
age
man
ifest
edas
par
aphr
enia
Mos
t had
per
sona
lity
trai
ts t
hat
coul
d be
grou
ped
as
eith
erpa
rano
id o
r sc
hizo
id.
Onl
y 4
con
side
red
chee
rful
, so
cial
&w
arm
41
-50
51
-60
61
-70
28 16 3
All
men
8 i T> I I m z CD c
by guest on November 20, 2014http://schizophreniabulletin.oxfordjournals.org/Downloaded from

VOL 14, NO. 1, 1988 47
COin
•*- O CDC O T 5 LO
£
•a?
I
CO .* i _ COCD f=
ooN-inr-oo *- I-- coo
0 ) 0 ) 0 0 ) •-Q ~ Q —.
' ~"l a 1 <S T S; 6 § C A ;A A
ininin
in
(J) .
I?fca
_J
06
1881
IE
II
rent
esiz
oph
i
$
709
al.
e
nstitui
intri
es
- 8
from
in 5
m
enic
s
1
644
•aCD
2 8
! -
to a
1945
12 c
CD CD
S *
adm
betw
2?
P!
coo's co .5co2-s I D oJ P n o S .2 " » C L.s j u =^<2!f>iJcB<i'
B>CCO
Distribution of Age of Onset:
Ten studies (Kolle 1931 [whoincluded two different populationsof patients]; Fish 1958, 1960;Muller 1959; Larson and Nyman1970; Bleuler 1972; Huber et al.1975; Bland 1977; Rabins et al.1984) reported on the differencesin proportion of schizophreniawith age of onset before and afterage 60. When the numbers fromthese reports are combined, theweighted mean proportion oflate-onset (usually after 40)schizophrenia before age 60 is 86percent and that after age 60 is 14percent.
A further breakdown of thedistribution of age of onset ofschizophrenia is possible on thebasis of data from Bleuler (1972),Fish (1958, 1960), Larson andNyman (1970), Huber et al.(1975), and Bland (1977). In thesefive investigations, the weightedmean proportion of late-onsetschizophrenia in the fifth decadeof life was 57.5 percent, that inthe sixth decade 30.2 percent, andafter age 60 it was 12.3 percent.
Thus, in the studies reviewed,approximately 13 percent of allschizophrenic patients had onsetof symptoms in the fifth decade,7 percent in the sixth decade, and3 percent thereafter. These propor-tions may appear to be muchgreater than those in the commonclinical experience. The reasonsare probably twofold. The above-mentioned reports may haveexaggerated the prevalence oflate-onset schizophrenia, partlybecause of difficulties in preciselydating the onset of schizo-phrenia—i.e., some of the so-calledlate-onset patients might havehad schizophrenic symptomssince earlier in life. On the otherhand, it is highly likely thatschizophrenia tends to be under-
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

48 SCHIZOPHRENIA BULLETIN
diagnosed in patients with lateonset of psychotic symptomsbecause of various factors dis-cussed previously. Well-designedprospective investigations areneeded to establish the exactincidence and prevalence oflate-onset schizophrenia. Nonethe-less, it is fair to suggest thatonset of schizophrenia after age40 is far from rare.
Gender Difference. Withoutexception, all the studies thatincluded both male and femalepatients with late-onset schizophre-nia reported a predominance ofwomen (table 1). The lowestfemale:male ratio was 1.9:1(Bleuler 1943, 1972), and thehighest ratio was 45:2 (Herbertand Jacobson 1967). The study byBland (1977) suggested that thefemale:male ratio increased withan increase in age at first hospitali-zation for schizophrenia. This isin contrast to the consistentlyhigher treated incidence rates forearly-onset schizophrenia in malesthan in females, particularlybetween the ages of 15 and 34(Babigian 1985).
It is very unlikely that the smalldifference (of about 2 years) inthe mean longevity of men andwomen provides an adequateexplanation for the female pre-dominance in late-onset schizo-phrenia. Seeman (1982) givesseveral alternative hypotheses: (1)There may be two forms ofschizophrenia—a juvenile-onsetform with a higher incidence inmen, and a late-onset form with ahigher incidence in women. (2)There is commonly an accumula-tion of nonspecific stressors thatmainly affect males during adoles-cence. (3) There may be specificbiological protective factors in thefemale, such as relatively bilateralrepresentation of left-hemispherefunctions or relative dopaminergic
inhibition by estrogens. Carefulresearch into this important areais necessary.
Family Studies. Some specificdifficulties are encountered instudying the families of late-onsetschizophrenic patients. For exam-ple, migration of family membersmay make it difficult to locateand evaluate them. It is not ofteneasy to find contemporaries toprovide information about familymembers. The risk period forpossible development of a late-onset schizophrenic disorder islong, requiring that family mem-bers ideally be followed untildeath. If death occurs earlier inlife, there is no way to determineif a schizophrenic disorder wouldhave developed. There are alsodifficulties in the diagnosis oflate-onset schizophrenia in relativeswithout personal and carefulevaluation. As mentioned earlier,such patients frequently carry adiagnosis other than schizophrenia.
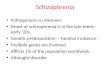
Table 2 summarizes familystudies of probands with late-onsetschizophrenia. The study byFunding (1961) was excludedbecause schizophrenic patientswere not separated from affectivedisorder patients among theirlate-onset psychotic probands.Two limitations of most of thesestudies are that they did notdescribe their method of identify-ing family members; nor did theygive the number of family mem-bers on whom information wasnot available (e.g., due to deathat a young age or migration).
Findings. Four studies (Bleuler1943; Kay and Roth 1961; Herbertand Jacobson 1967; Larson andNyman 1970) looked at the overallprevalence of schizophrenia insiblings of probands. With theexception of Larson and Nyman(1970), they also included parents
of late-onset schizophrenic pro-bands. The combined meanprevalence was 7.2 percent insiblings and 2.9 percent in parents.Huber et al. (1975) and Rokhlina(1975) looked at the prevalence ofschizophrenia among all relatives.The mean prevalence was 15.1percent. Rokhlina (1975) found a10.8 percent prevalence of schizo-phrenia in relatives of late-onsetschizophrenic patients comparedwith a 17.7 percent prevalence inrelatives of early-onset schizo-phrenic patients. Affective disor-ders were rare in relatives oflate-onset schizophrenic patients(Huber et al. 1975; Rokhlina 1975;Rabins et al. 1984), except in thestudies by Klages (1961) and Post(1966).
The data on the age of onset ofillness in schizophrenic relativesof late-onset schizophrenic pro-bands are sparse. According toBleuler (1943), such probandshave comparable numbers ofrelatives with early- and late-onsetschizophrenia.
The results of family studies oflate-onset schizophrenia, despitetheir limitations, may be comparedto those of schizophrenia ingeneral. According to Weiner(1985), the risk of schizophreniain siblings of schizophrenicprobands in different studiesranges from 3 percent to 14percent, while that in parents is0.2 percent to 12 percent. Thus, itappears that the prevalence ofschizophrenia in the first-degreerelatives of late-onset schizophrenicprobands is greater than that inthe general population, but lowerthan that in the first-degreerelatives of earlier-onset schizo-phrenic patients.
Other Characteristics ofLate-Onset Schizophrenia
Main Symptoms. According to
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 14, NO 1, 1988 49
most studies, the symptoms oflate-onset schizophrenia aresimilar to those of earlier-onsetschizophrenia, especially theparanoid type. Fish (1960) notedthat the clinical picture of 23middle-aged and elderly schizo-phrenic patients did not differfrom the clinical picture in patientswith onset before age 40. In
seven out of nine patients withonset between 50 and 59 years,auditory hallucinations were aprominent feature.
Kay and Roth (1961) reportedthat delusions were more or lesssystematized and "fantastic."They were usually persecutory,but also exotic, hypochondriacal,or grandiose. In 28 percent of the
cases, feelings of mental orphysical influence were found.Auditory hallucinations developedin 75 percent of the cases. Visual,tactile, and olfactory hallucinationsalso occurred. Incoherence of talkand even neologisms were seenin cases of long duration. Verbos-ity, circumstantiality, or irrelevancewas found in about 30 percent of
Table 2. Family studies of late-onset schizophrenic patients
Investigators
Bleuler (1943)
Kay (1959);Kay & Roth (1961)
Klages (1961)
Herbert & Jacobson(1967)
Larson & Nyman(1970)
Huber et al.(1975)
Rokhlina (1975)
Number ofprobands
65
99(including 57 fromSweden & 42 fromU.K.)
53
45 women
153 male schizo-phrenic patients(including 49 withlate-onset)
110
65
Prevalence ofschizophrenia in
first-degreerelatives
9.8% in sibs; 4.4% inparents (6 of 24 affectedrelatives had "probableschizophrenia")
Risk for schizophreniabetween ages 18 & 50:2.1% in parents4.9% in sibs6.3% in children(of 57 Swedish probands)
8 first-degree relatives
2 2% in parents2.3% in sibs
Overall risk in sibs 11.6%16 out of 64 schizo-phrenic sibs developedsymptoms after 40
19.4% among all relatives
10.8% in relatives of
Prevalence ofother psychiatric
disorders infamily
?
?
7 depressives
6 fathers psychopathic2 alcoholic
?
None with affectivedisorders
2% relatives of late-
Risk of late-onsetschizophrenia
9 relatives had late-onset(& 15 early-onset)schizophrenia
8 relatives of 99 late-onset schizophrenicprobands (but only 2relatives of 200 affectivedisorder patients)
Risk much greater in femalethan male relatives
Post (1966)
Rabins et al.(1984)
93
35
late-onset schizophrenics& 17.7% in relatives ofearly-onset schizophrenics
5 relatives with schizo-phrenia (including 2 withlate onset)
5 probands (vs. 3 of 35depressed controls) had afamily history of schizo-phrenia
onset & 6.6% of early-onset schizophrenicshad affective psychoses
16 affective disorders;27 personality disorders& alcoholism; 8 organicdisorders (includingepilepsy)
No probands (vs. 12 of35 depressed controls)had family history ofaffective disorder
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

50 SCHIZOPHRENIA BULLETIN
the cases. Some emotional blunt-ing, mild incongruity, or euphoriawas quite common in chronicpatients. Kay and Roth (1961) feltthat over time the clinical picturebecame indistinguishable fromthat seen in chronic schizophrenia.In 25 percent of cases, markedfluctuations in behavior continuedfor years. Sometimes, the illnesseventually became "burnt out,"leaving residual defects.
Post (1966) found that 60percent of his 65 treated patientshad "depressive admixtures." Inlongstanding cases, negativesymptoms similar to those ofother forms of schizophrenia werecommon.
Rabins et al. (1984) observedthat the symptoms in paraphrenicpatients were similar to thosesuffered by patients diagnosed ashaving schizophrenia. Of the 35paraphrenic patients, 24 sufferedfrom hallucinations and 22 hadSchneiderian first-rank symptoms.These numbers were significantlyhigher than those for affectivedisorder controls. Of 35 patients,21 met the DSM-III criteria forschizophrenia, and 11 for schizo-phreniform disorder if the criterionrequiring onset before age 45 wasdisregarded.
In our (Jeste et al. 1987) pilotstudy of 15 patients who metDSM-HI-R criteria for late-onsetschizophrenia, 14 patients werenoted to have paranoid delusionswhile 6 patients also had auditoryhallucinations.
Sensory Deficits. Auditory andvisual deficits have been noted byEnglish investigators in a sizableportion of the paraphrenic popula-tion. Cooper (1976) reviewed theliterature concerning the relation-ship between deafness andpsychiatric disorders in general.He concluded that the prevalence
of schizophrenia in the prelin-gually deaf was not significantlydifferent from that in the normalpopulation, whereas the postlin-gually deaf were overrepresentedamong samples of patients suffer-ing from paranoid psychoses inlater life. The following studiesspecifically looked at sensorydeficits in the patients withlate-onset paranoid psychosis.
Kay and Roth (1961) studied 42patients with late paraphreniafrom a British hospital and 57comparable patients from aSwedish hospital. Visual defectswere found in approximately 15percent of cases, about half ofthose being severe. According tothe authors, this percentage didnot differ significantly from thatin control groups of comparableage. (The control group was notclearly defined; it probably in-cluded affective disorder patients.)Some impairment of hearing wasfound in 40 percent of the Britishpatients; in 15 percent, it was ofmarked degree. In Sweden onlythe most severe cases of hearingloss had been recorded, and theirprevalence was 16 percent. Thefrequency in patients with affectivedisorders, on the average 3 yearsyounger, was only 7 percent. Thepresence of visual or hearing lossdid not seem to modify thesymptomatology of paraphreniagreatly. Kay and Roth (1961)considered that deafness, alongwith abnormalities of personalityand loss of many relatives,contributed to more social isolationin the paraphrenic populationthan in affective disorder patients.(The method of assessing visualand hearing loss was not stated.)
Post (1966) found that deafnesswas present in 25 percent of 72elderly paranoid disorder patients,compared to only 11 percent ofelderly depressives. The method
used to assess hearing loss wasnot specified.
Herbert and Jacobson (1967)studied 45 late-paraphrenicpatients and found moderate tosevere visual loss in one or botheyes in 47 percent of the patients.In 12 cases (27 percent), criticalvisual defects in both eyes werepresent. Forty percent of thepatients had moderate to severeauditory loss. No controls wereused in this study.
Cooper and Porter (1975)examined the association betweenocular pathology and functionalpsychoses in 54 paranoid and 57affective elderly patients. Appreci-able ocular pathology was foundin 30 paranoid and 21 affectivedisorder patients. Significantlymore cataracts were detectedamong the paranoid patients thanamong the affective disorderpatients.
Cooper and Curry (1976)studied 27 paranoid and 18affective disorder patients whowere deaf before the onset oftheir psychosis. A significantassociation emerged betweenparanoid illness and bilateralconductive deafness which had anearlier age of onset, longerduration, and greater severitythan the forms of sensorineuraldeafness found in affectivedisorder patients.
In sum, there is some suggestiveevidence for a higher-than-normalprevalence of visual and, espe-cially, auditory deficits in late-onset schizophrenic patients.Important methodological problemsin the published studies make itdifficult, however, to draw anyeriopathological inferences.
Abnormal Personality Traits.Abnormal personalities werenoted in the late-paraphrenicpopulation by the following
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 14, NO 1, 1988 51
groups of investigators.Kay and Roth (1961) reported
that paraphrenic patients withouthallucinations (20 percent of thetotal patient sample) hadlongstanding personality abnor-malities that interfered withinterpersonal relationships. Theonset of psychosis in thesepatients was difficult to date, andrelatives tended to regard it as acaricature of the premorbidpersonality. Another third weredescribed as explosive or sensitive.In 45 percent of the cases, thepersonality traits found werepredominantly of paranoid andschizoid type (jealousy, suspicious-ness, arrogance, egocentricity,emotional coldness, and extremesolitariness). The authors con-cluded that abnormalities ofpersonality were present in alarge proportion of the patientsand were probably related to thefrequent failure to marry, the lowfertility, and the social isolation.
Herbert and Jacobson (1967)excluded from their paraphreniccategory patients with premorbidpersonality traits that had beendisabling enough to prevent themfrom coping with their environ-ment. Out of 45 patients with lateparaphrenia so diagnosed, only 4were considered to have beenlacking abnormal personalitytraits. The others were mostlyschizoid or paranoid.
Kay and Roth (1961) andHerbert and Jacobson (1967)reported that a large number oftheir paraphrenic patients wereunmarried and childless. Theseinvestigators did not provide dataon age-matched controls, however.
Rabins et al. (1984) found that10 of 35 paraphrenic patientswere married, compared to 17 of35 age- and sex-matched affectivedisorder controls. These research-ers also noted that 22 of 35
paraphrenic patients, comparedwith 28 of 35 affective disorderedcontrols, had children. Neither ofthese differences was significant.
Brain Lesions. Miller et al. (1986)found evidence of an "occult"neurological disorder in fivelate-onset schizophrenic/para-phrenic patients. We (Jeste et al.1987) have been studying late-onset schizophrenic patients witha neuropsychological battery andmagnetic resonance imaging(MRI). Our preliminary resultssuggest that a subset of thesepatients has neuropsychologicalimpairment and structural brainabnormalities on MRI, whileanother subset is normal (for age)on neuropsychological performanceand MRI scans.
Course and Prognosis. All fourinvestigations of the course andprognosis of late-onset schizophre-nia concluded that the coursetended to be chronic, and prog-nosis unfavorable. Kay and Roth(1961) found prognosis to bepoor. In Graylingwell, recoverywas reported to be very rare. Allbut 4 of the 24 cases known to bealive after 5 years were stillhospitalized. Of the 14 deaths,only 2 took place after dischargeand neither of these patients wasdischarged under supervision.About half the remaining lifespanwas spent in mental hospitals orsimilar institutions. Post (1966)reported that life expectancy wasnormal, but prognosis with regardto loss of symptoms was poor.Herbert and Jacobson (1967)found that prognosis in their 45late-paraphrenic patients was poorand the course was chronic. Ofthe 45 patients admitted, 29 weredischarged. Fourteen of thesewere readmitted, but eight weredischarged again after a short
stay. Within 1 year, two patientswere readmitted and, within 2years, one more patient wasreadmitted. Of the 16 patientswho remained in the hospital, 10were over age 75 and showedintellectual deterioration. Therewere eight deaths (length offollowup is not given). Fish (1960)was able to discharge only 3 of110 senile schizophrenic patientsbetween 6 and 12 months afteradmission. One patient hadrelapsed, one was lost to followup,and another patient claimed thatshe was doing well in a letter tothe author, which he felt was notvery reliable information.
Treatment. Only a few recentstudies of late-onset schizophreniahave looked at the treatmentresponse of these patients. Janzarik(1957), as cited by Post (1966),studied 50 elderly schizophrenicpatients with onset of symptomsafter age 60 and noted thatelecrroconvulsive therapy (ECT)and medications (chlorpromazinewas mentioned in one case; othermedications used were notspecified) produced temporaryremissions. Kay and Roth (1961)reported temporary remissionsoccurring spontaneously, withECT or with "tranquilizers" (thesewere not identified) in about 25percent of the patients treated atGraylingwell. Twelve of 43patients received ECT; seven ofthem improved and were dis-charged. On followup, only onepatient remained symptom free.The authors felt that the smallnumber of patients consideredappropriate for ECT and the poorresponse to it were furtherevidence that late paraphreniawas not a primary affectivedisorder.
Post (1966) followed 93 late-onsetschizophrenic patients who were
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

52 SCHIZOPHRENIA BULLETIN
divided into two groups accordingto phenothiazine treatment.Twenty-two patients had receivedeither no neuroleptic treatment orinadequate dosage. Only one ofthese patients had remissionduring the 16-month followupperiod. Seventy-one patientsreceived at least short-termadequate treatment, usually withtrifluoperazine (10-30 mg/day) orthioridazine (50-400 mg/day). Sixof these patients had no response,22 had moderate improvement,and 43 had complete remission.Sixty-five patients were followedfor 12—41 months. Twenty-twopatients remained free of allpsychotic symptoms after initialtreatment; 25 patients hadsymptoms for periods of varyinglength; and 18 remained psychoticthroughout the followup period,though in most cases there wassome improvement.
The long-term outcome withregard to the number of patientsspending greater than 25 percentof their time in the hospitaldiffered similarly with treatment.The numbers were as follows: 7of 19 patients without neuroleptictreatment, 4 of 16 patients giveninitial adequate treatment but notmaintained on medication, andonly 2 of 21 patients maintainedon medication remained hos-pitalized greater than 25 percentof the time. Treatment alsoresulted in significant improvementin psychotic symptoms (comparedto no treatment). Neuroleptics didnot, however, produce an im-provement equal to the premorbidlevel of social adjustment. Theyalso had little effect on thedevelopment of insight in amajority of patients.
Herbert and Jacobson (1967)treated 38 patients diagnosed ashaving late paraphrenia withtrifluoperazine. Pharmacotherapy
was considered "impressive" incontrolling aggression and irritabil-ity, and therefore helped inpromoting discharge and keepingpatients out of the hospital. (Thelength of followup, symptomsthat responded to medication,dosage, and length of treatmentwere not given.)
Rabins et al. (1984) reportedthat 35 patients with a diagnosisof late-onset schizophrenia orparaphrenia were treated withneuroleptics and psychosocialtherapies. (The types of neurolep-tic, dosage, and length of treat-ment were not given.) On dis-charge, 20 patients were symptomfree, 10 symptomatic but im-proved, and 5 symptomaticallyunchanged. A 2-year followupwas done on 14 patients over age60. Four patients remainedsymptom free, six patients hadrelapses with symptom-freeperiods, and three patients hadchronic symptoms. With theexception of one patient who hadsuffered a stroke, all patientswere living at home. (Whetherthese patients over age 60 werecontinued on neuroleptics afterdischarge is not known.)
In summary, a sizable propor-tion of late-onset schizophrenicpatients improved with neuro-leptic treatment. Aspects such astype of neuroleptic, dosage,blood levels, side effects, anddegree of improvement in spe-cific symptoms have not beensufficiently investigated. Also,there have been no double-blind,controlled studies similar tothose conducted in youngerpatients. Nonetheless, the clin-ical impression that a numberof late-onset schizophrenic pa-tients are helped by neurolepticsis comparable to the experiencewith younger schizophrenicpatients.
Clinical and ResearchImplications
There is little debate about thefact that schizophrenia-likesymptoms can develop for thefirst time in middle and lateadulthood. In some of thesecases, the patients clearly havemajor affective disorders, organicmental syndromes, or paranoiddisorders. The main question iswhether a syndrome that may becalled "schizophrenia" occurs withany regular frequency after age 40(or 44). In this regard, twospecific problems must be recog-nized: (1) The validity of psychi-atric diagnoses is often moredifficult to establish than that ofmost other medical diagnosesbecause of an absence of suitablelaboratory procedures (Rosenhan1973). (2) Schizophrenia is, in allprobability, not a single diseasebut a syndrome with multiplesubtypes (see Jeste et al. 1982).
The literature we have reviewedsuggests that investigators havediagnosed new-onset schizophreniaor paraphrenia after age 40 in asizable proportion of patients.Furthermore, a number of re-searchers have failed to find anydistinctive differences in course ofillness between schizophrenia andparaphrenia. Late-onset schizo-phrenia is characterized byparanoid symptomatology, premor-bid personality traits of schizoidor paranoid type, a tendencytoward chronicity, and symptomat-ic improvement with neuroleptics.
Spitzer and Williams (1985)have discussed certain relativelyobjective methods for demonstrat-ing validity other than facevalidity (which requires onlyconsensus among observers).These include (1) descriptivevalidity, in which the characteristicfeatures are unique; (2) predictive
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL. 14, NO 1, 1988 53
validity, in which followupstudies indicate a homogeneouscourse, complications specific tothat disorder, and a differentialtreatment response; and (3)construct validity in which afamilial pattern, biological abnor-mality, or relationship to environ-mental variables helps to explainetiology of a disorder.
It will obviously be difficult toquantify the validity of late-onsetschizophrenia, or even of theoverall schizophrenic syndrome,using these criteria. Nevertheless,the general similarities betweenlate-onset and early-onset schizo-phrenia (including the results offamily studies) suggest that thelate-onset form is probably no lessvalid than the early-onset variety.Whether late-onset and early-onsetschizophrenia are distinct subtypes(biologically or otherwise) or aremerely forms of the same schizo-phrenic spectrum differing in ageis unclear.
A number of important ques-tions related to late-onset schizo-phrenia remain unanswered.What are the factors that protectthese patients from a schizophrenicbreakdown until later in life? Whyis there a high preponderance ofwomen in this group? How dothese patients compare with age-and education-matched normalcontrols as well as earlier-onset(18-44 years) schizophrenicpatients in their neuropsychologicalperformance, structural brainabnormalities, psychosocial srres-sors, and family constellation?The treatment-response patternsof the late-onset schizophrenicpatients also deserve a specialstudy. Several reports indicatethat elderly subjects have signifi-cantly higher blood levels ofneuroleptics than younger patientsgiven similar dosages (MSrtenssonand Roos 1973; Jeste et al. 1981;
Yesavage et al. 1982). Similarly,the risk of tardive dyskinesia hasbeen noted to be higher inschizophrenic patients with laterage of onset of psychosis. (Yassaet al. 1986; Waddington andYoussef 1986).
Suggestions for FutureResearch
There is a great need for carefulresearch into late-onset schizo-phrenia. Among the methodologi-cal improvements that might bemade in this area are the following:
• To reduce confusion interminology, a single set ofdiagnostic criteria should be used.We prefer the nomenclature inthe DSM-M-R (American Psychiat-ric Association 1987), which offersan operational definition oflate-onset schizophrenia. Termssuch as paraphrenia, which havebeen employed inconsistently,should be avoided.
• Diagnostic assessment shouldgive special consideration toruling out major affective disor-ders, organic mental syndromes,and delusional (paranoid) disor-ders. This will entail obtainingdetailed past and family history(of possible affective disorder),and use of appropriate laboratoryevaluations (e.g., thyroid functiontests) to exclude "organic" causesof late-onset psychosis.
• Special efforts need to bemade to ascertain the age ofonset of schizophrenia. Athorough review of past medicalrecords and interviews of "signifi-cant others" are necessary to ruleout the possibility of an undiag-nosed schizophrenic disorderbefore age 45.
• Prevalence surveys of late-onset schizophrenia shouldinclude the entire predefinedpopulation base (e.g., all the
schizophrenic patients from agiven catchment area).
• Prospective, long-term fol-lowup investigations are necessaryto determine the course of theillness.
Hypothesis-oriented clinical,neuropsychological, and biologicalevaluations of this patient popula-tion are indicated.
• The likelihood that late-onsetschizophrenia is not a homogene-ous entity but is a syndrome withclinically and biologically relevantsubtypes should be considered inresearch in this field.
• It is important to determinethe relative risk:benefit ratio withneuroleptics (as well as othertreatments) in late-onset schizo-phrenic patients.
• Appropriate control groups,such as normal subjects matchedfor age, gender, level of education,and socioeconomic status, andadult-onset (18—44 years) schizo-phrenic patients matched forseverity of psychopathology, areessential for interpreting anyobserved "abnormalities" inlate-onset schizophrenic patients.
Research into late-onset schizo-phrenia promises to improve ourunderstanding of schizophrenia ingeneral.
References
American Psychiatric Association.DSM-l: Diagnostic and StatisticalManual of Mental Disorders.Washington, DC: The Association,1952.American Psychiatric Association.DSM-11: Diagnostic and StatisticalManual of Mental Disorders. 2nded. Washington, DC: The Associa-tion, 1968.American Psychiatric Association.DSM-I1I: Diagnostic and StatisticalManual of Mental Disorders. 3rd ed.
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

54 SCHIZOPHRENIA BULLETIN
Washington, DC: The Association,1980.American Psychiatric Association.DSM-HI-R: Diagnostic and StatisticalManual of Mental Disorders. 3rded., revised. Washington, DC:The Association, 1987.Angst, J.; Baastrupp, P.; andGrof, P. Statistical aspects of theonset and course of schizophrenicpsychoses. (In German) In:Huber, G., ed. Verlauf und AusgangSchizophrener Erkrankungen.Stuttgart-New York: F.K. Schaut-tauer, 1973. pp. 67-78.
Babigian, H.M. Schizophrenia:Epidemiology. In: Kaplan, H.I.,and Sadock, B.H., eds. Comprehen-sive Textbook of Psychiatry. Balti-more: Williams & Wilkins Com-pany, 1985. pp. 643-650.Bland, R.C. Demographic aspectsof functional psychoses in Canada.Ada Psychiatrica Scandinavica,55:369-380, 1977.Blessed, G., and Wilson, I.D. Thecontemporary natural history ofmental disorder in old age. Britishjournal of Psychiatry, 141:59-67,1982.Bleuler, M. Late schizophrenicclinical pictures. (In German)Forschritte der Neurologw-Psychtatrie,15:259-290, 1943.Bleuler, M. The SchizophrenicDisorders: Long-term Patient andFamily Studies. Translated by S.M.Clemens. New Haven and Lon-don: Yale University Press, 1978.Bridge, T.P., and Wyatt, R.J.Paraphrenia: Paranoid states oflate life. I. European research.journal of the American GeriatricsSociety, 28:193-200, 1980a.Bridge, T.P., and Wyatt, R.J.Paraphrenia: Paranoid states oflate life. II. European research.journal of the American GeriatricsSociety, 28:201-205, 1980b.Cooper, A.F. Deafness and
psychiatric illness. British journalof Psychiatry, 129:216-226, 1976.Cooper, A.F., and Curry, A.R.The pathology of deafness in theparanoid and affective psychosesof later life, journal of PsychosomaticResearch, 20:97-105, 1976.Cooper, A.F., and Porter, R.Visual acuity and ocular pathologyin the paranoid and affectivepsychoses of later life, journal ofPsychosomatic Research, 20:107-114,1975.Feighner, J.P.; Robins, E.; Guze,S.B.; Woodruff, R.A.; Winokur,G.; and Munoz, R. Diagnosticcriteria for use in psychiatricresearch. Archives of GeneralPsychiatry, 26:57-63, 1972.Fish, F. A clinical investigation ofchronic schizophrenia, journal ofMental Science, 104:34-54, 1958.Fish, F. Senile schizophrenia.journal of Mental Science, 106:938-946, 1960.Funding, T. Genetics of paranoidpsychoses of later life. AdaPsychiatrica Scandinavica, 37:267-282,1961.Gold, D.D. Late age of onsetschizophrenia: Present but unac-counted for. Comprehensive Psychi-atry, 25:225-237, 1984.Herbert, M.E., and Jacobson, S.Late paraphrenia. British journal ofPsychiatry, 113:461^69, 1967.Hinsie, L.E., and Campbell, R.J.Psychiatric Dictionary. 4th ed. NewYork: Oxford University Press,1974.Hopkins, B., and Roth, M.Psychological test performance inpatients over sixty: II. Paraphrenia,arteriosclerotic psychosis andacute confusion. Journal of MentalScience, 99:451^163, 1953.Huber, G.; Gross, G; and Schut-tler, R. Spatschizophrenie. Archivfur Psychiatrie und Nervenkrankheiten,221:53-66, 1975.
Janzarik, W. Zur problematikschizophrener psychosen inhoheren lebensalter. Nervenarzt,28:535-542, 1957.Jeste, D.V.; DeLisi, L.E., Zalcman,S.; Wise, CD.; Phelps, B.H.;Rosenblatt, J.E.; Potkin, S.G.;Bridge, T.P.; and Wyatt, R.J. Abiochemical study of tardivedyskinesia in young male patients.Psychiatry Research, 4:327-331, 1981.Jeste, D.V.; Harris, M.J.; Cullum,CM.; Zweifach, M.; Thai, L.J.;and Grant, I. "Late Onset Schizo-phrenia: Neuropsychology andMRI." (New Research AbstractNo. NR76) Presented at the 140thAnnual Meeting of the AmericanPsychiatric Association, May 9-14,1987.Jeste, D.V., Kleinman, J.E.;Potkin, S.G.; Luchins, D.; andWeinberger, D.R. Ex Uno Multi:Subtyping the schizophrenicsyndrome. Biological Psychiatry,17:199-222, 1982.Kay, D.W.K. Late paraphreniaand its bearing on the aetiologyof schizophrenia. Ada PsychiatricaScandinavica, 39:159-169, 1963.Kay, D.W.K.; Beamish, P.; andRoth, M. Old age mental disordersin Newcastle Upon Tyne. Britishjournal of Psychiatry, 110:146-158,1964.
Kay, D.W.K., and Roth, R.Environmental and hereditaryfactors in the schizophrenias ofold age ("late paraphrenia") andtheir bearing on the generalproblem of causation in schizo-phrenia, journal of Mental Science,107:649-686, 1961.
Klages, W. Die Spatschizophrenie.Stuttgart: Enke, 1961.Kolle, K. Die Preimare Verrucktheit.Leipzig: Thieme, 1931.Kraepelin, E. Dementia Praecox andParaphrenia. (1919) Translated byR.M. Barclay. New York: Robert
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from

VOL 14, NO 1, 1988 55
E. Krieger Publishing Co., Inc.,1971. pp. 282-329.Larson, C.A., and Nyman, G.E.Age of onset in schizophrenia.Human Heredity, 20:241-247, 1970.Lechler, H. Die Psychosen derAltan. Archiv fur Psychiatrie undNervenkrankheiten, 185:440-465,1950.
Leonhard, K. Die Aufteilung derendogenen Psychosen. Berlin:Akademie Verlag, 1959.Martensson, E., and Roos, B.E.Serum levels of thioridazine inpsychiatric patients and healthyvolunteers. European Journal ofClinical Pharmacology, 6:181-186,1973.
Mayer, W. On paraphrenicpsychoses. (In German) Zeitschriftfur die Gesamte Neurologie undPsychiatrie, 71:187-206, 1921.Mayer-Gross, W. Die Schizo-phrenic (IV. Die Klinik; V.Erkennung und Differentialdiagnose). In: Bumke, O. BumkesHandbuch der Geiskrankheiten. Spez.5. Berlin: Springer, 1932.Miller, B.L.; Benson, F.; andCummings, J.L. Late-life para-phrenia: An organic delusionalsyndrome. Journal of ClinicalPsychiatry, 47:204-207, 1986.Miiller, C. Uber das Senium derSchizophrenen. Basle: Karger, 1959.Post, F. Persistent Persecutory Statesof the Elderly. Oxford: PergamonPress, 1966.
Rabins, P.; Pauker, S.; andThomas, J. Can schizophreniabegin after age 44? ComprehensivePsychiatry, 25:290-293, 1984.Retterstol, N. Paranoid andParanoiac Psychoses. Springfield, IL:Bannerstone House, 1966.Robertson, E.E., and Mason-Browne, N.L. Review of mentalillness in the older age gTOup.British Medical Journal, 2:1076-1079,1953.
Rokhlina, M.L. A comparativeclinico-genetic study of attack-likeschizophrenia with late and earlymanifestations with regard to age.(In Russian) Zhurnal Nevropatologiii Psiikhiatrii Imeni S.S. Korsakova,75:417-424, 1975.
Rosenhan, D.L. On being sane ininsane places. Science, 179:250-258,1973.Roth, M. The natural history ofmental disorder in old age. Journalof Mental Science, 101:281-301, 1955.
Roth, M., and Morrissey, J.D.Problems in the diagnosis andclassification of mental disorder inold age; with a study of casematerial. Journal of Mental Science,98:66-80, 1952.
Schulz, B. Zur Erbpathologie derSchizophrenic. Zentralblatt fiir dieGesamte Neurologie und Psychiatrie,143:175-293, 1933.Seeman, M.V. Gender differencesin schizophrenia. Canadian Journalof Psychiatry, 27:107-111, 1982.
Sjogren, H. Paraphrenic, melan-cholic and psychoneurotic statesin the presenile-senile period oflife. Ada Psychiatrica Scandinavica,40:1-63, 1964.
Spitzer, R.L.; Endicott, J.; andRobins, E. Research DiagnosticCriteria for a Selected Group ofFunctional Disorders. 3rd ed. NewYork: New York State PsychiatricInstitute, 1978.Spitzer, R.L., and Williams,J.B.W. Classification of mentaldisorders. In: Kaplan, H.I., andSadock, B.H., eds. ComprehensiveTextbook of Psychiatry. Baltimore:Williams & Wilkins Company,1985. pp. 591-613.Volavka, J. Late-onset schizophre-nia: A review. ComprehensivePsychiatry, 26:148-156, 1985.Waddington, ]., and Youssef, H.Involuntary movements and
cognitive dysfunction in late onsetschizophrenic outpatients. IrishMedical Journal, 79:347-350, 1986.Weiner, H. Schizophrenia: Etiol-ogy. In: Kaplan, H.I., and Sadock,B.H., eds. Comprehensive Textbookof Psychiatry. Baltimore: Williams& Wilkins Company, 1985.pp. 650-680.
World Health Organization.Mental Disorders: Glossary andGuide to Their Classification inAccordance With the Ninth Revisionof the International Classification ofDiseases. Geneva: The Organiza-tion, 1978.Yesavage, J.A.; Becker, J.; Werner,P.D.; Mills, M.J.; Holman, C.A.;and Cohn, R. Serum levelmonitoring of thiothixene inschizophrenia: Acute single-doselevels at fixed doses. AmericanJournal of Psychiatry, 139:174-178,1982.
Acknowledgments
The research was supported, inpart, by the Veterans Administra-tion. We thank Ingrid Lewin fortranslating German articles intoEnglish. We also appreciate theexpert assistance by Linda Barnettand Karen Bruno.
The Authors
M. Jackuelyn Harris, M.D., isAssistant Professor of Psychiatry,and Dilip V. Jeste, M.D., isProfessor of Psychiatry andNeurosciences and Director of theNeuropsychiatry/GeropsychiarryProgram and NeuropathologyResearch Laboratory, San DiegoVeterans Administration MedicalCenter and Department of Psychi-atry, University of California, SanDiego.
by guest on Novem
ber 20, 2014http://schizophreniabulletin.oxfordjournals.org/
Dow
nloaded from