Embed Size (px)
Citation preview
William M. Callaghan, MD, MPHActing Chief, Maternal and Infant Health Branch
Division of Reproductive HealthCenters for Disease Control and Prevention
Reproductive Health 2010September 23, 2010
Late Preterm Birth
National Center for Chronic Disease Prevention and Health Promotion
Overview
Burden of preterm birthRecent trends in preterm birth
Early preterm (<32 weeks)Late preterm (34‐36 weeks)
Why is late preterm birth a public health issue?The role of contraceptionResearch for prevention
Leading Causes of Infant Mortality (2006)
• Congenital malformations – 5,850 (20%)• Short gestation/low birthweight (short gestation low
birthweight not elsewhere classified) – 4,843 (17%)• SIDS – 2,327(8%)• Maternal complications – 1,676 (6%)• Accidents – 1,143 (4%)
2005 Linked Birth/Infant Death Data (CDC/NCHS)
An Apparent Paradox
• Over half a million infants born preterm each year
• Preterm birth accounted for 17% of infant deaths in 2006; PTB is the second leading cause of IM
• Two‐thirds of infants who die are born preterm
• Many deaths ascribed to a specific cause almost never occur unless the infant is born preterm
Preterm‐related Infant Mortality
Preterm‐related> 75% of infants who died from a given cause were born <37 weeksCause of death direct consequence of preterm on clinical grounds
36% of infant deaths in 2006 were preterm‐relatedBeing born preterm is the number one reason why infants die
National Vital Statistics Reports, 57 (2), 2008
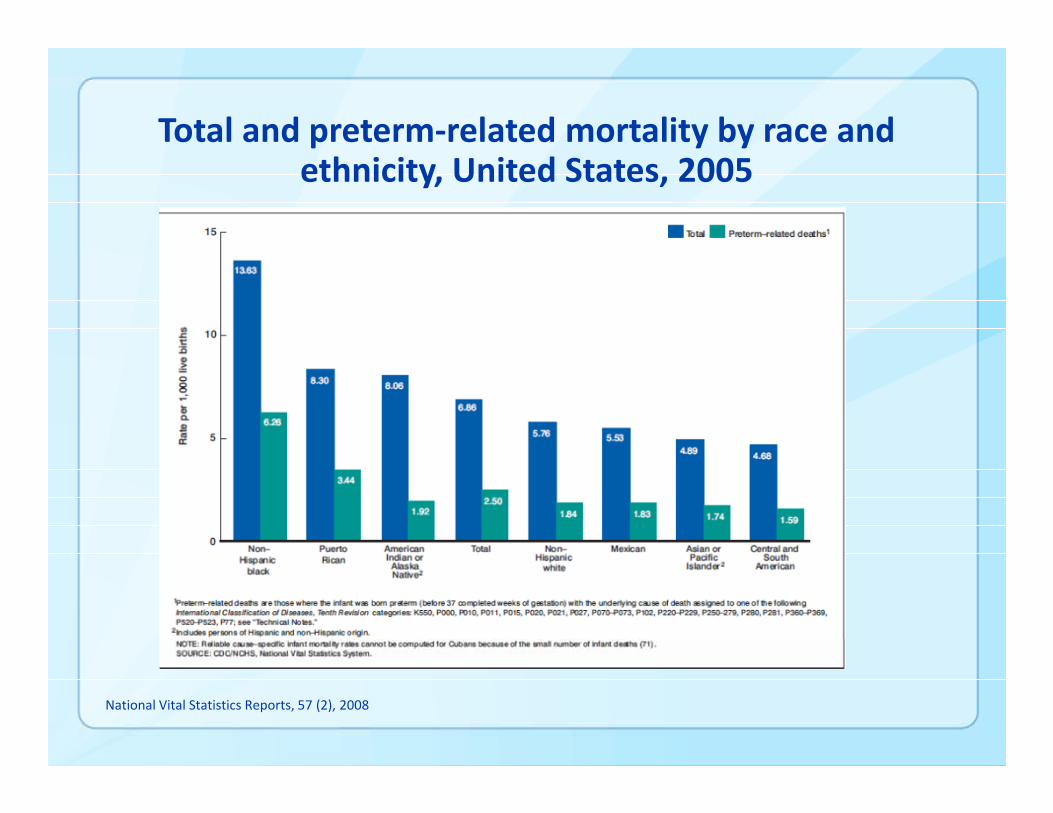
Total and preterm‐related mortality by race and ethnicity, United States, 2005
National Vital Statistics Reports, 57 (2), 2008
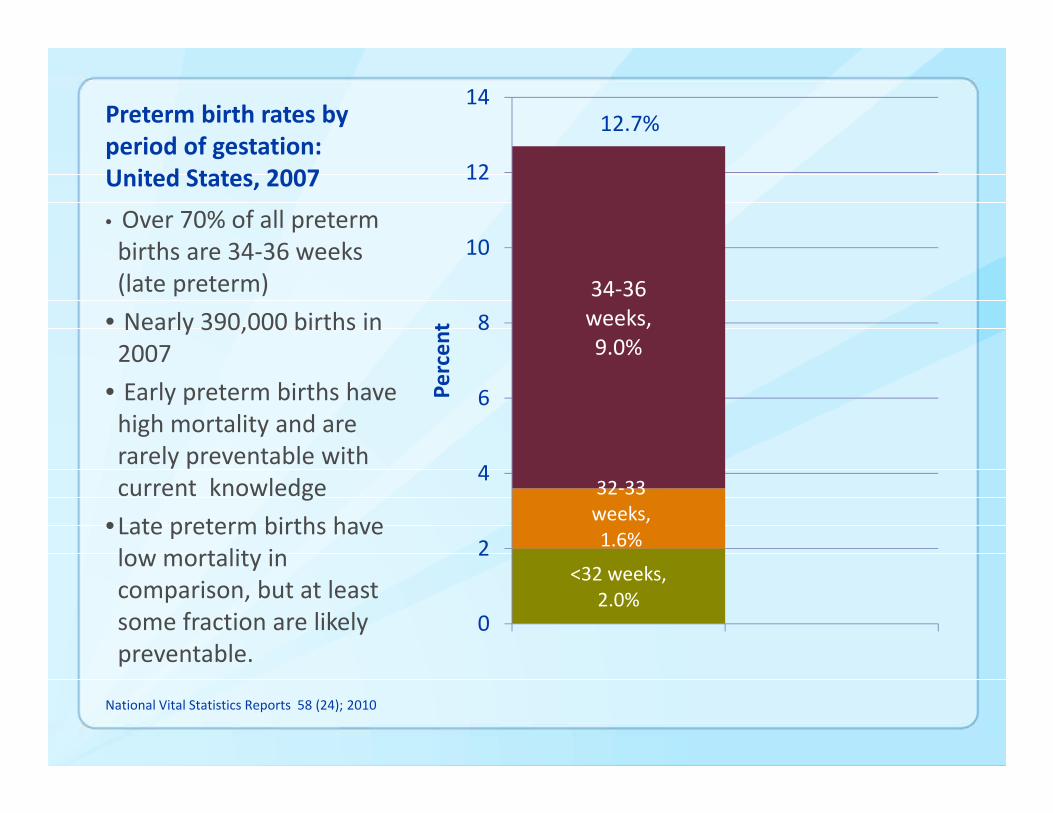
Preterm birth rates by period of gestation: United States, 2007
<32 weeks, 2.0%
32‐33 weeks, 1.6%
34‐36 weeks, 9.0%
0
2
4
6
8
10
12
14
Percen
t
• Over 70% of all preterm births are 34‐36 weeks (late preterm)
• Nearly 390,000 births in 2007
• Early preterm births have high mortality and are rarely preventable with current knowledge
•Late preterm births have low mortality in comparison, but at least some fraction are likely preventable.
National Vital Statistics Reports 58 (24); 2010
12.7%

Trends
Martin JA, et al. NCHS Data Brief. No 39, May 2010
12.8%12.3%
9.1%8.8%
3.7%
3.6%
Risks of Late Preterm Birth
Mortality3‐fold increased risk of death in first year compared to termGreatest discrepancy in first 6 day mortality (early neonatal)Ranking of causes nearly identical to term (congenital malformations, SIDS, accidents, circulatory system diseases, hypoxia/birth asphyxia top 5)
(Tomashek et al., J Ped 2007;151:450‐6)
Newborn Morbidity7‐fold increase in newborn morbidityRisk persists independent of exposure to maternal conditions, but is greater when exposed.Morbidity risk decreases with each increased week of gestation
(Shapiro‐Mendoza et al. Pediatrics 2008;121:e223‐e232)

Morbidity risk by gestational ageShapiro‐Mendoza et al., Pediatrics 2008;121:e223‐e232
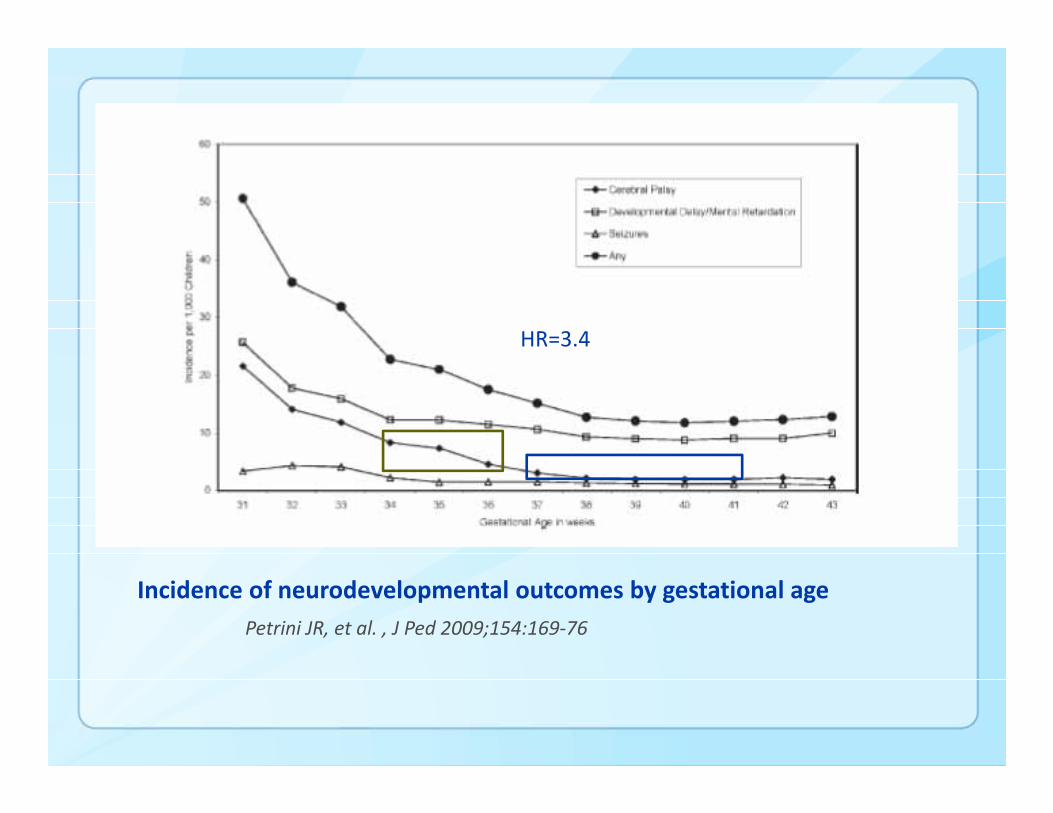
Incidence of neurodevelopmental outcomes by gestational agePetrini JR, et al. , J Ped 2009;154:169‐76
HR=3.4
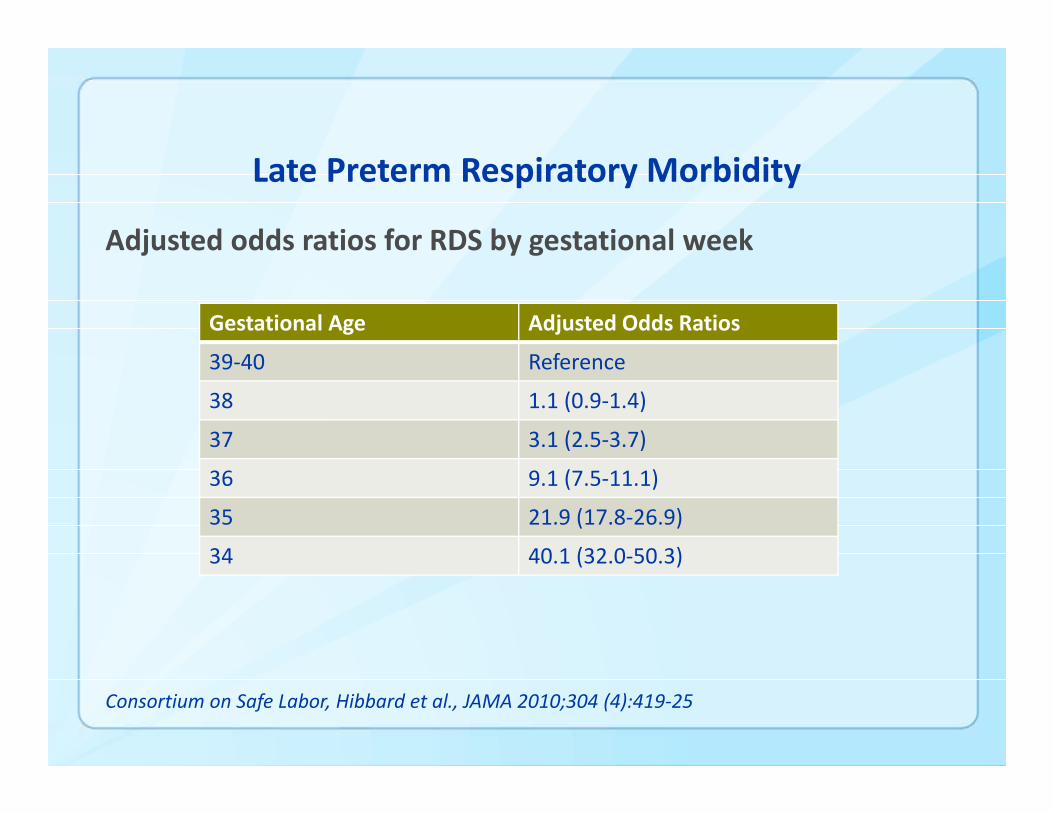
Late Preterm Respiratory Morbidity
Adjusted odds ratios for RDS by gestational week
Consortium on Safe Labor, Hibbard et al., JAMA 2010;304 (4):419‐25
Gestational Age Adjusted Odds Ratios
39‐40 Reference
38 1.1 (0.9‐1.4)
37 3.1 (2.5‐3.7)
36 9.1 (7.5‐11.1)
35 21.9 (17.8‐26.9)
34 40.1 (32.0‐50.3)
Contraception and Preterm Birth: Intendedness and Timing
No study looks specifically at late preterm birthIntention: differences between mistimed and unwanted
Women with mistimed pregnancies have risk profiles more similar to those with wanted pregnancies and unlike women with unwanted pregnancies. (Orr et al. Ann Epidemiol 2008;18:545‐51)Relationship to pregnancy outcomes including preterm birth is inconsistent and largely null when adjusted for maternal risk. (Kost et al. Family Planning Perspect 1998;30:223‐30; Messer et al. Mat Child Health J 2005;9:403‐412).
Timing: robust literature supports association between short inter‐pregnancy interval and preterm birth.
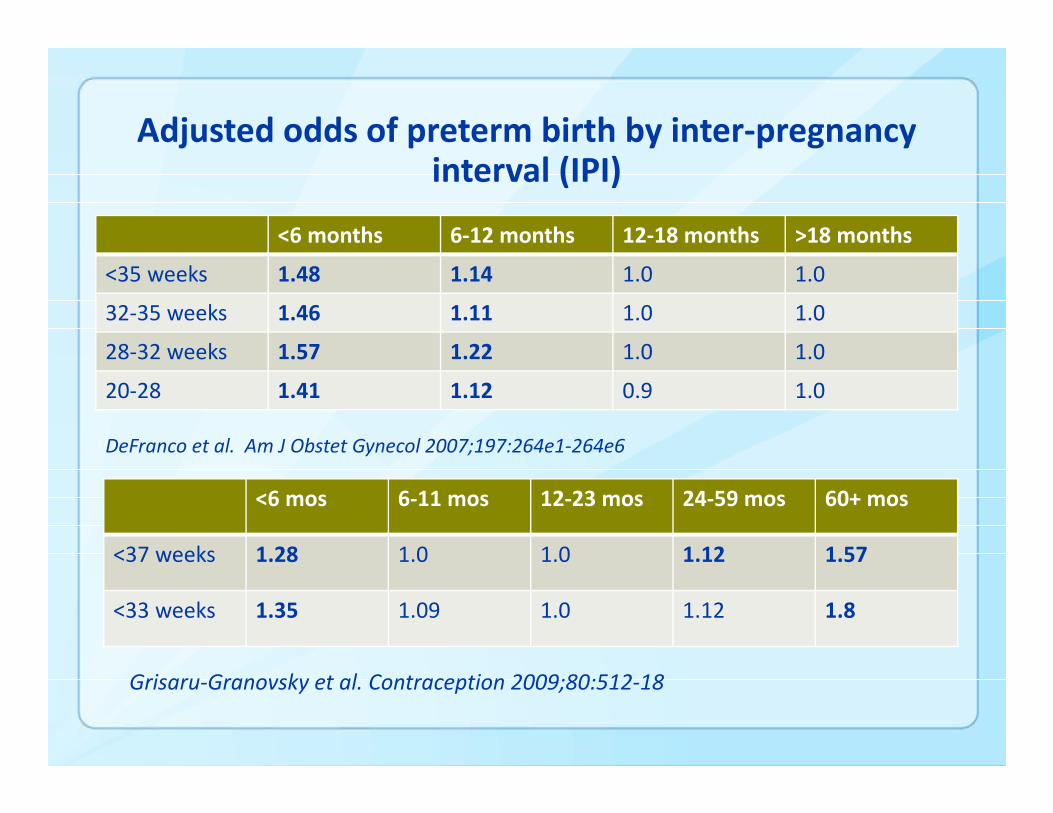
Adjusted odds of preterm birth by inter‐pregnancy interval (IPI)
<6 months 6‐12 months 12‐18 months >18 months
<35 weeks 1.48 1.14 1.0 1.0
32‐35 weeks 1.46 1.11 1.0 1.0
28‐32 weeks 1.57 1.22 1.0 1.0
20‐28 1.41 1.12 0.9 1.0
DeFranco et al. Am J Obstet Gynecol 2007;197:264e1‐264e6
<6 mos 6‐11 mos 12‐23 mos 24‐59 mos 60+ mos
<37 weeks 1.28 1.0 1.0 1.12 1.57
<33 weeks 1.35 1.09 1.0 1.12 1.8
Grisaru‐Granovsky et al. Contraception 2009;80:512‐18
Unanswered Questions
Why are infants born at 34‐36 weeks and why have these births increased?Under what circumstances should delivery at 34‐36 weeks (or anytime prior to 39 weeks) occur?How often does delivery at 34‐36 weeks occur without a medical indication?Does mode of delivery affect neonatal outcome?
Delivery Indications for Late Preterm Births
>20,000 late preterm births in DallasSpontaneous labor or PPROM (80%), and fetal complications accounted for all
(McIntire DD and Leveno KJ, Obstet Gynecol 2008;111:35‐41.)
149 late preterm births in CincinnatiSpontaneous labor or PPROM (92%) and maternal/fetal complications accounted for all
(Lubow JM, et al. Am J Obstet Gynecol 2009;200:e30‐e33.)
~Nearly 300,000 late preterm births 2001 United States23% no recorded indication on birth certificate
(Reddy UM et al. Pediatrics 2009;114:253‐60.)
Delivery Indications for Late Preterm BirthsFeasibility Assessment
What are the reasons (maternal and fetal indications) for deliveries at 34‐36 weeks gestation (late preterm)?To what extent do cesarean deliveries or labor inductions that are not medically indicated contribute to rising preterm birth rates?What is the impact of non‐medically indicated preterm delivery on neonatal and maternal morbidity?What role does medical liability play in the decision to perform a cesarean section delivery before term?
Delivery Indications for Late Preterm BirthsFeasibility Assessment
90 late preterm births at 3 metro‐Atlanta hospitalsMaternal and infant chart abstractionsKey informant (physician and nurse) interviewsResults ?????
Should Term be Re‐defined?
ACOG guidelines : In absence of clinical indications, elective delivery should not occur prior to 39 weeks.37‐38 week infants suffer higher morbidity than infants at later gestation.
Birth 2010;37:169‐71
Obstet Gynecol 2010;116:136‐9.
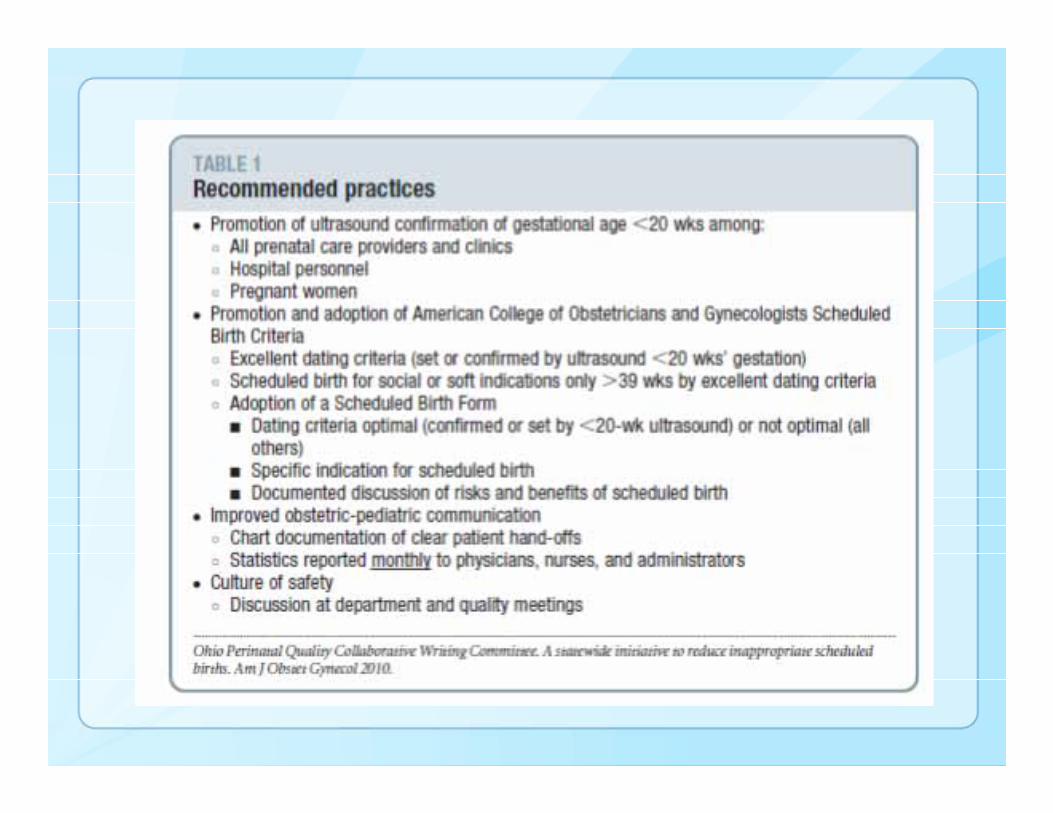
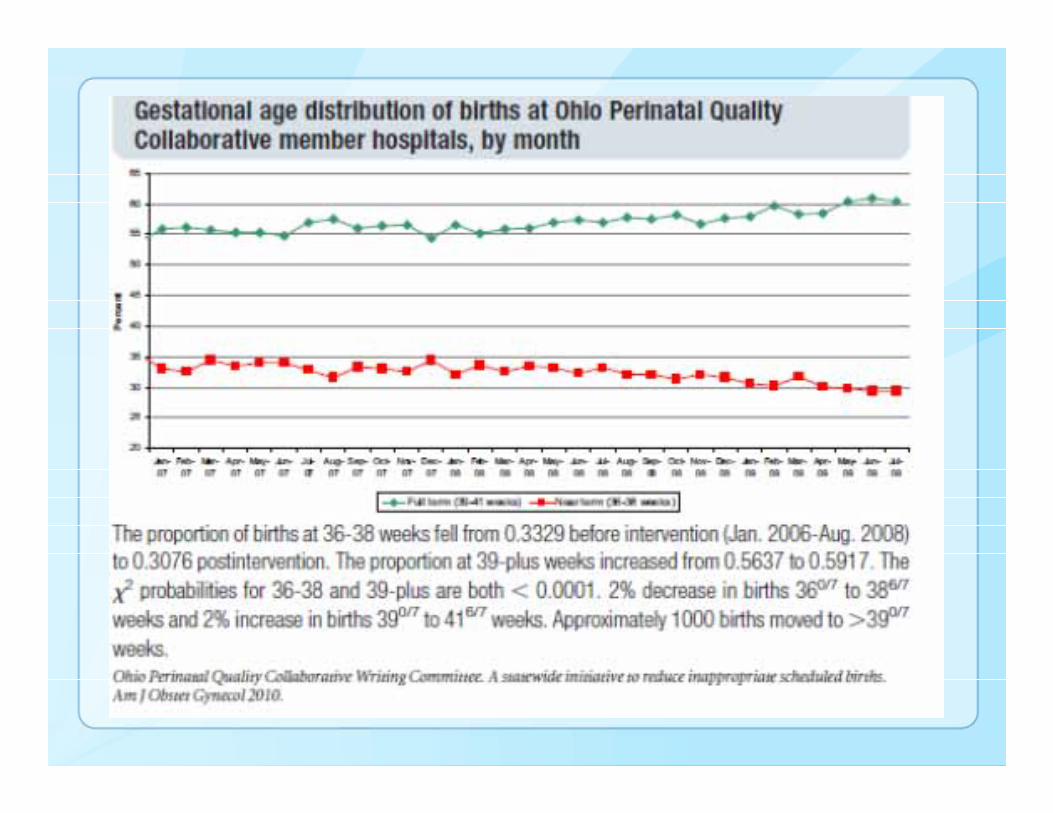
Prevention of Late Preterm: It’s not easy
Ohio Perinatal Quality Collaborative (OPQC)Statewide20 maternity/neonatal hospitals6 metropolitan areas
Data sharing to inform rapid adoption of evidence‐based quality improvementsOPQC Scheduled Birth Initiative: Reduce scheduled deliveries between 36‐38 weeks without clinical indications

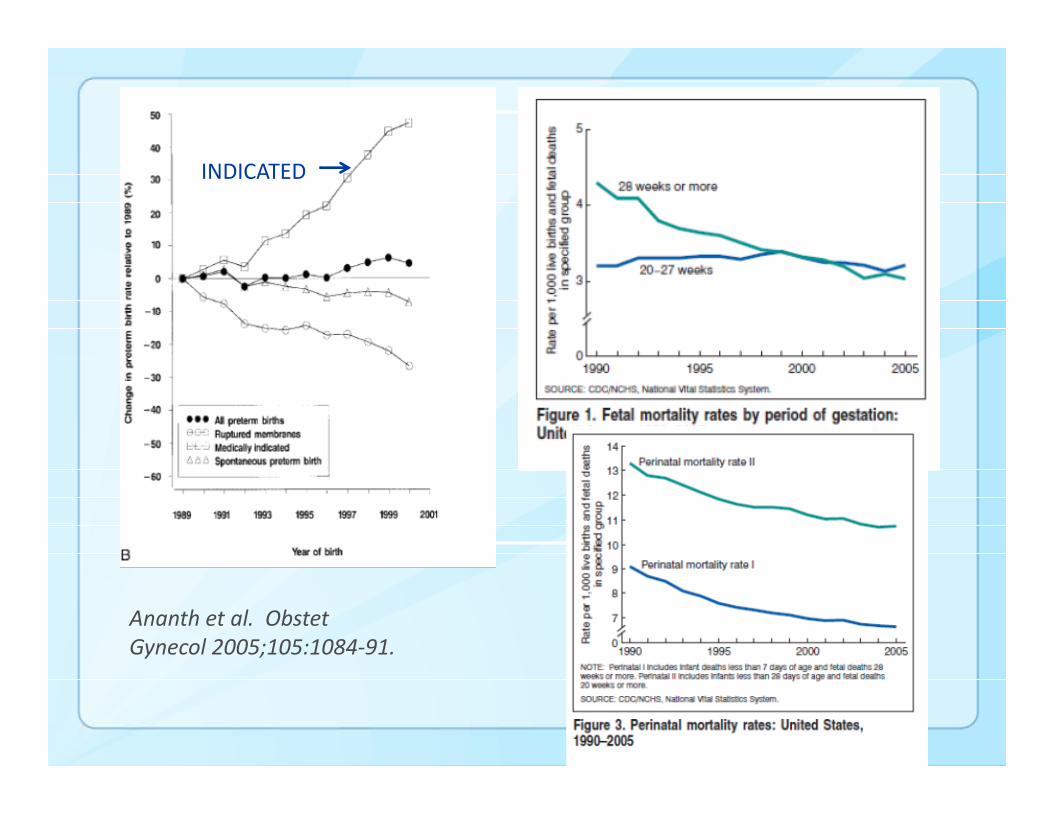
Ananth et al. Obstet Gynecol 2005;105:1084‐91.
INDICATED
Can we prevent late preterm birth?
To the extent that pregnancies at 34‐36 weeks can be safelyprolonged and intervention avoided, some late preterm deliveries can be avoided.There is a critical gap in nuanced clinical information and understanding about decision‐making regarding timing of delivery.It is critical that all pregnancies have the most accurate estimates of gestational age.We still do not have strategies to prevent most spontaneous preterm labor, preterm rupture of membranes, and most maternal/fetal complications leading to preterm birth.Family planning services likely an important prevention intervention
For more information please contact Centers for Disease Control and Prevention
1600 Clifton Road NE, Atlanta, GA 30333Telephone, 1‐800‐CDC‐INFO (232‐4636)/TTY: 1‐888‐232‐6348E‐mail: [email protected] Web: www.cdc.gov
Thank [email protected]