Embed Size (px)
Citation preview

Fabio MarraDipartimento di Medicina
Sperimentale e Clinica
Università di Firenze
Le epatiti:
aggiornamento
sulle cure.
Sono per tutti?

Abbvie: consultant fees
Allergan: consultant fees
Alfa-Wassermann: travel grants
AstraZeneca: consultant fees
Bayer: speaker honoraria, consultant fees, travel grants
Gilead: speaker honoraria, consultant fees
Intercept: speaker honoraria
Menarini: consultant fees
Novo Nordisk: consultant fees

Natural history of HCV infection

Natural history of HCV infection:
conflicting views on severity
Worst-case scenario(Tong et al NEJM, 1995)
Best-case scenario(Wiese et al J Hep, 2005)
131 Tx-related
chronic hepatitis C
(followed for 1-15 yr)
2867 women treated
with HCV1b Rh Ig
(followed for 25 yr)
45% cirrhosis
11% HCC
15% HCV-related mortality
7% uninfected
54% spontanous recovery
0.5% cirrhosis
0.1% HCC
0.3% HCV-mortality
How to explain its heterogeneous
and contrasting features ?

Natural History of Hepatitis C
Factors / variables associated with progression
- Age at infection
- Gender
- Race
- HIV – HBV
- HCV genotype
- Alcohol
- Smoking
- Hemochromatosis
- NASH - Obesity
- Genetics
- ALT profile

Scenario 1:
The occasionally diagnosed
patient

Non-specialists’s approach
to a newly diagnosed patient
Recognition and staging of the underlying liver disease
Physical examination, ALT, AST, bilirubin, INR,
albumin, ultrasound
Exposure to other parenterally-transmitted diseases?
HBsAg, anti-HBs, anti-HBc, HIV
Is there an indication to antiviral treatment?
Refer to specialist, HCV-RNA, genotype

Progression of chronic liver diseases
F0 F1 F2 F3 F4
Fibrosis
without septaNo fibrosis Few septa
Numerous
Septa W/O
cirrhosis
Numerous
Septa WITH
CIRRHOSIS
CancerPortal hypertensionDeranged microvascular anatomy

Diagnostic approaches to staging
Biomarkers
Imaging
Elastography HVPG
Biopsy
Biopsy
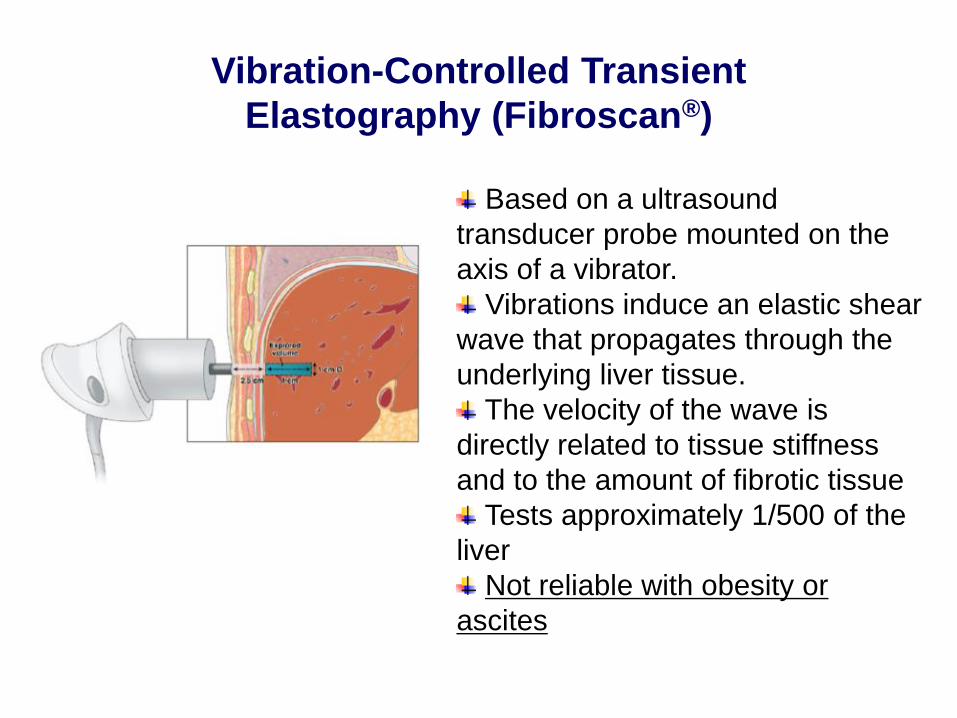
Based on a ultrasound
transducer probe mounted on the
axis of a vibrator.
Vibrations induce an elastic shear
wave that propagates through the
underlying liver tissue.
The velocity of the wave is
directly related to tissue stiffness
and to the amount of fibrotic tissue
Tests approximately 1/500 of the
liver
Not reliable with obesity or
ascites
Vibration-Controlled Transient
Elastography (Fibroscan®)

FIBROscan or ‘HEPATOscan’?
Confounding factors:
• Inflammation
• Tissue edema
• Extrahepatic cholestasis
• Passive congestion
• Active blood flow (meal)

Scenario 2:
The patient with extrahepatic
manifestations

HCV infection:
Systemic manifestations and associations
• Cryoglobulinemia
• Lymphoma
• Glomerulopathy
• Peripheral neuropathy
• Lichen planus
• Porphyria
• Thyroid diseases
• Diabetes
• CV disease
• Psoriasis
• Rheumatoid arthritis
• Sjogren syndrome
• Behcet’s disease

Scenario 3:
The patient with complications of
cirrhosis

N.M. male, 52 yo
Reports no major problems in the past
No medication, social drinker (60 g/day), obese
Works as a dentist
Presents to the ER during a trip in Spain for massive
hematemesis after taking NSAIDs for back pain
Upper endoscopy shows actively bleeding varices (F3)
Lab test: hyperbilirubinemia, HCV positive

Major complications in HCV-related cirrhosis
6 8 10
Perc
ent
patients
Years0 2 4
Patients
still at risk
12 14 16
155 142 127 118 104 97241 222 209 186 169 79 70 60 51 38 6
156 146 126 116 100 93241 223 206 180 167 78 72 63 54 42 5
158 147 134 126 110 98241 222 208 182 169 80 74 63 53 43 6
165 155 140 132 113 101241 224 212 189 176 87 78 67 57 45 6
HCC
ASCITES
JAUNDICE
BLEEDING
yearly rate: 3.9% HCC
2.8% ascites
1.9% jaundice
0.9% bleeding
4.3% death
100
50
75
25
0
Sangiovanni et al., Hepatology 2005

Portal hypertension
Portal pressure above 6-8 mmHg.
‘Clinically significant’ when >10 mmHg
Major complications:
• ascites
• GI bleeding
• hepatorenal syndrome
• hepatic encephalopathy
• hypersplenism
50% of patients with ‘compensated’ cirrhosis will develop a major
complication within 10 years

Tell the difference between these two patients
571.5 571.5

Towards a new classification of cirrhosis
Arvaniti et al., Gastroenterology 2010;139:1246

Scenario 4:
The patient with hepatocellular
carcinoma

C.G. male, 58 yo
Reports no major problems in the past
No medication, active drinker 120 g/day
Presents to the ER for pain in the RUQ
Ultrasound of the abdomen performed in the ER
reveals a 8-cm nodule in
S5
CT scan: Multiple, diffuse lesions with arterial
enhancement and washout in late phase,
occupying most of the right lobe
Labs: HCV positive

Scenario 5:
The patient with acute-on-
chronic liver failure

P.P. male, 59 yo
CAD with CABG in 2016
Former smoker and drinker
Presents to the ER for diarrhea and fever for 7
days. For this reason he has taken nimesulide and
diclofenac for several days. Previous lab test with
normal bilirubin
At admission: INR 2.9, bilirubin 24 mg/dl, tense
ascites. Labs: HCV positive
Discharge diagnosis: Acute-on-chronic liver failure
grade 1

A syndrome characterized by the acute deterioration of
liver function in a patient with compensated or
decompensated, but hitherto stable, cirrhosis.
It is commonly precipitated by an acute event
(precipitating factor) and associated with failure in the
function of extra-hepatic organs.
Definition of acute-on-chronic liver failure (ACLF)

Different forms of liver failure
associated with cirrhosis
Laleman et al., Expert Rev Gastroenterol Hepatol 2011;5:523
Substantial evolution towards MOF

The liver and other organs in ACLF
Vizzutti et al., Trends Anaest Crit Care 2013

Jalan et al., Gastroenterology 2014
New classification of ACLF


costo
SVR
Guadagno di
salute
(miglioramento
della salute)
determinato
dall’intervento
sanitario
ANNI VITA
GUADAGNATI
LYG - QALYFreccia rossa = entità della spesa per
quell’intervento
Freccia verde = quantità di salute acquistata
o ritorno di salute
“MISSIONE” DEL VALUE FOR MONEY:
massimizzare la salute che si può ottenere
con il finanziamento a disposizione
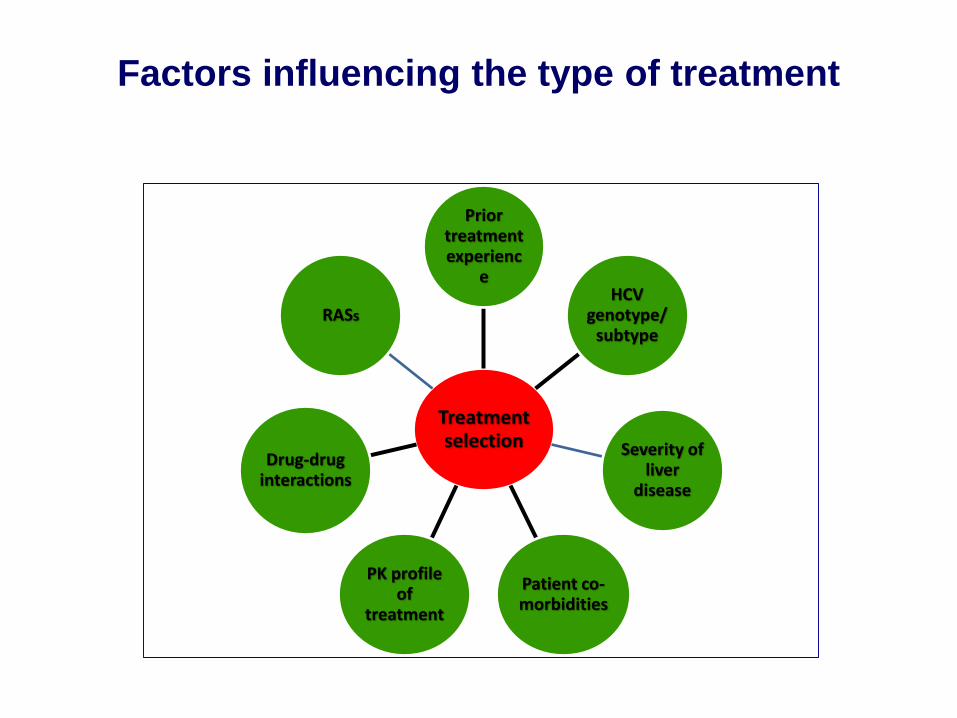
Treatment selection
Prior treatment experienc
eHCV
genotype/subtype
Severity of liver
disease
Patient co-morbidities
PK profile of
treatment
Drug-drug interactions
RASs
Factors influencing the type of treatment

Available DAA classes
Pawlotsky, Antivir Ther 2012
NS3/4A protease
inhibitorsNucleotide
analogues
Non-nucleoside
inhibitors
NS5A
inhibitors
NS5A
inhibitors

Principles of HCV therapy
NS5A
inhibitor
Protease
inhibitor
Nucleotide
analogue
Non-
nucleoside
inhibitor

Principles of HCV therapy
Daclatasvir
Ledipasvir
Velpatasvir
Ombitasvir
Elbasvir
Simeprevir
Paritaprevir/r
Grazoprevir
Sofosbuvir
Dasabuvir
RBV RBV

Validated regimens in 2017-18

Criterio 1: Pazienti con cirrosi in classe di Child A o B e/o con HCC
con risposta completa a terapie resettive chirurgiche o loco-
regionali non candidabili a trapianto epatico nei quali la malattia
epatica sia determinante per la prognosi.
Criterio 2: Epatite ricorrente HCV-RNA positiva del fegato
trapiantato in paziente stabile clinicamente e con livelli ottimali di
immunosoppressione.
Criterio 3: Epatite cronica con gravi manifestazioni extra-epatiche
HCV-correlate (sindrome crioglobulinemica con danno d'organo,
sindromi linfoproliferative a cellule B, insufficienza renale).
Criterio 4: Epatite cronica con fibrosi METAVIR F3 (o
corrispondente Ishak).
Criterio 5: In lista per trapianto di fegato con cirrosi MELD <25 e/o
con HCC all'interno dei criteri di Milano con la possibilità di una
attesa in lista di almeno 2 mesi.
Criterio 6: Epatite cronica dopo trapianto di organo solido (non
fegato) o di midollo in paziente stabile clinicamente e con livelli
ottimali di immunosoppressione.
AIFA: fino al 2017

Criterio 7: Epatite cronica con fibrosi METAVIR F2 (o
corrispondente Ishak) e/o comorbilità a rischio di progressione
del danno epatico [coinfezione HBV, coinfezione HIV, malattie
croniche di fegato non virali, diabete mellito in trattamento
farmacologico, obesità (body mass index ≥30 kg/m2),
emoglobinopatie e coagulopatie congenite].
Criterio 8: Epatite cronica con fibrosi METAVIR F0-F1 (o
corrispondente Ishak) e/o comorbilità a rischio di progressione
del danno epatico [coinfezione HBV, coinfezione HIV, malattie
croniche di fegato non virali, diabete mellito in trattamento
farmacologico, obesità (body mass index ≥30 kg/m2),
emoglobinopatie e coagulopatie congenite].
Criterio 9: Operatori sanitari infetti.
Criterio 10: Epatite cronica o cirrosi epatica in paziente con
insufficienza renale cronica in trattamento emodialitico.
Criterio 11: Epatite cronica nel paziente in lista d'attesa per
trapianto di organo solido (non fegato) o di midollo.
AIFA: dal 2017
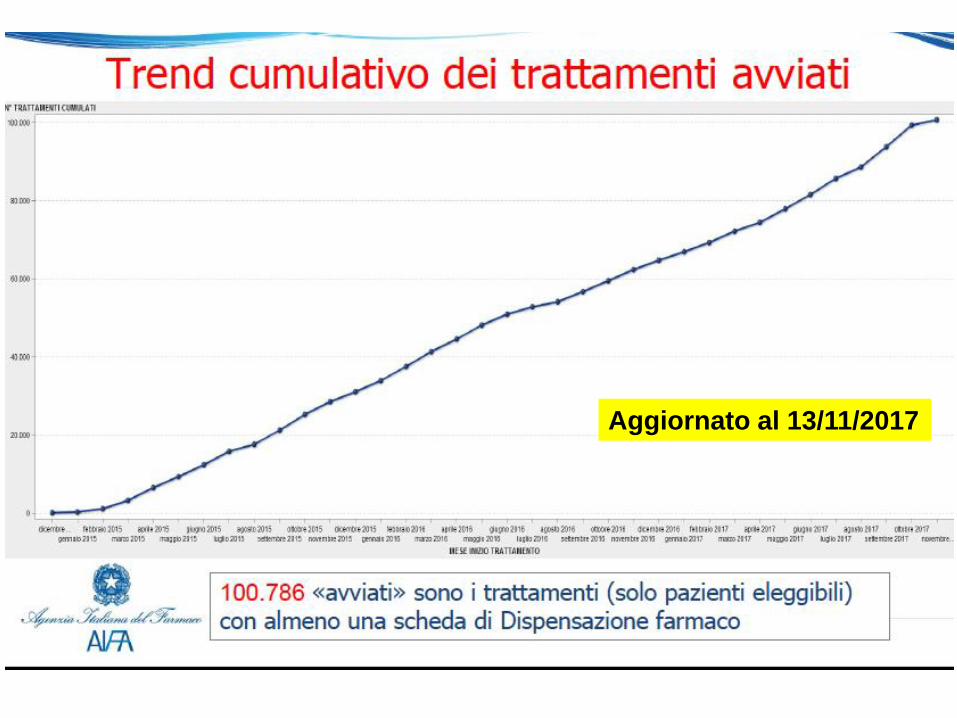
Aggiornato al 13/11/2017


DAA in non-Gt3 cirrhosis

Van der Meer et al., JAMA 2014
Impact of sustained virologic response
in patients with advanced fibrosis

218 Pts
Treated
n= 149
Non-SVR
n= 115
SVR prevents de-novo development of esophageal varices in compensated HCV cirrhosis
21
30,4
46
40,0
0
0
Varices (n)
Varices (%)
Untreated
n= 69
SVR
n= 34Median
follow-up:
11,4 years
p=ns
p = 0,0001
Vs “Untreated” and“Non-
SVR”
7,5 years 10,7 years 15,9 years
Bruno et al., Hepatology 2010

Etiological treatment of underlying liver disease may
reduce portal hypertension and prevents complications in
patients with established cirrhosis (A1).
Baveno VI considerations

A.Z, male, age 65
2006: Diagnosed with compensated HCV-related cirrhosis
Starts IFN/Ribavirin SVR
2010: Persistently normal liver panel. Discharged from active
follow-up
2014: Admitted to the ER for RUQ pain HCC nodule of S4,
5 cm CPS A5. Undergoes resective surgery
2015: Early HCC relapse. Starts sorafenib
Deceased after 2 months on sorafenib
A case of HCV-related cirrhosis

SVR
No SVR
HCC
Surveillance with
biannual ultrasound
must be continued

No evidence of de novo HCC
in patients treated with DAA

What changes in decompensated patients?
Ribavirin

To treat or not to treat decompensated cirrhosis

Outcomes in decompensated patients


2017: what is still needed?
• Pts with decompensated cirrhosis would benefit
from more effective, RBV-free options
• Truly pangenotypic regimens
• Effective options for DAA-experienced pts with
RAVs
• Pts with renal failure and GT2, 3, 5, or 6 HCV
infection still lack IFN- and RBV-free options

WHO definition of control, elimination and
eradicationControl of disease
•Reduction of disease incidence, prevalence, morbidity or mortality to a locally
acceptable level
➢ Continued intervention measures are required to maintain the reduction
Elimination of disease
•Reduction to zero of incidence of a specified disease in a defined geographic
area as a result of deliberate effort.
➢ Continued intervention measures are required to maintain the reduction
Elimination of infection
•Reduction to zero of incidence of infection caused by a specific agent in a
defined geographic area as a result of deliberate effort
➢ Continued intervention measures to prevent reestablishment of
transmission are required.
Eradication of infection
•Permanent reduction to zero of the wordwide incidence of infection caused by
a specific agent as result of deliberate efforts:
➢ Intervention measures are no longer required





























