Embed Size (px)
Citation preview

Learn · Connect · Succeed
JCAHPO Regional Meetings
2017

1
Vikas Chopra, M.D.Health Sciences Associate Professor, Department of Ophthalmology
David Geffen School of Medicine at UCLA
Medical Director, UCLA Doheny Eye Centers – Pasadena
Associate Director, Doheny Image Reading Center, Doheny Eye Institute
pearls and pitfalls of ophthalmic imagingASCRS JCHAPO 2017 Conference
Vikas Chopra, M.D.Financial Disclosure: None
pearls and pitfalls of ophthalmic imagingASCRS JCHAPO 2017 Conference
4
Corneal ImagingFor diagnosis and relevance to refractive and cataract surgery outcomes
• If significant irregularity:
Refractive surgery is contraindicated
Astigmatic keratectomy (AK) may be unpredictable and unstable
Limbal relaxing incisions (LRI) may be unpredictable and unstable
Toric IOLs may be unpredictable
Presbyopia-correcting IOLs will NOT perform well
5
Corneal Imaging Essential to rule-out Irregular AstigmatismCorneal irregularity may lead to poor refractive and cataract surgery outcomes,
thus proper imaging output critical
10
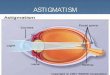
Types of Corneal AstigmatismRegular WTR vs. Regular ATR vs. Irregular
with-the-rule (WTR) regular astigmatism
against-the-rule (ATR) regular astigmatism
Non-symmetric steepeningIrregular astigmatism

2
1. Is astigmatism regular or irregular?
2. How many diopters of astigmatism?
3. How steep is the cornea and in which axis?
4. How does the pachymetry map look?
5. Does posterior corneal surface appear normal and symmetric?
11
Refractive (and Refractive-Cataract) Surgery ScreeningSystematic Approach for Corneal Tomography Interpretation
12
Symmetric anterior and posterior maps?
Symmetric above and below? Centered pachymetry?
Irregularity index @ 3mm
Refractive Surgery Screening with Corneal TomographySymmetric & regular astigmatism, normal pachymetry = Good candidate
13
Symmetric anterior and posterior maps?
Symmetric above and below? Centered pachymetry?
Irregularity index @
3mm
Refractive Surgery Screening with Corneal TomographyAsymmetric and irregular astigmatism, thin pachy = poor candidate ( keratoconus)
14
Astigmatism Correction in Cataract SurgeryAstigmatic Keratotomy (AK) and Limbal Relaxing Incisions (LRIs)
can correct low levels of corneal astigmatism
15
Refractive Cataract Surgery with Acrysof TORIC LensData from Corneal Topography determines Surgical Lens Placement
16
Refractive Cataract Surgery with Tecnis TORIC LensData from Corneal Topography determines Surgical Lens Placement

3
18
• Ensure accurate topography to determine candidacy for
astigmatism management
• Identify steep axis for AKs/LRIs and Toric IOL planning
• Assess post-op astigmatism in unhappy patients
• Investigate causes of decreased final vision
•Residual astigmatism
•Rotated Toric IOL
•Cystoid macular edema
Astigmatism management essential for Refractive Cataract SurgeryProper data acquisition and interpretation improve odds of successful outcome
Poor corneal reflex before artificial tears
Sharp corneal reflex after artificial tears
Instill artificial tears pre-testing to improve image quality
Dry eyes (punctate keratopathy) may affect scan qualityLook at the “sharpness” of the corneal reflex to evaluate corneal surface
Re-scanafter
artificialtears
20
Eyelid & Tear Film ErrorDry eyes can create artifactual corneal flattening &
Tear lake can create artifactual corneal steepening (example below)
22
Retinal ImagingFor diagnosis and management
Evolution of OCT
TD OCT
SD-OCT
SS-OCT
(8-10 µm)
(2-4 µm)
(5-7 µm)
• Changed our understanding of retinal dz
• Allows detection of glaucoma up to 8 years
before perimetric visual field defects seen
• Changed the normal flow in clinic
• Easier for both patient & technician
Optical Coherence Tomography (OCT)Most important imaging technique in Retina (and possibly Ophthalmology)
24
Macular OCTexample: Normal

4
25
Retinal layers as seen on retinal biopsy (or autopsy) specimenExample: Normal
26
OCT provides a non-invasive in-vivo Retinal BiopsyDistinct retinal layers visualized to distinguish normal from pathologic
27
OCT provides very high resolution retinal imagesEven discrete areas of Rods & Cones visualized with high-resolution OCT
28
OCT Retinal Layer Segmentation and LabelingInternationally agreed nomenclature
29
Macular OCT (Cube scan)Allows assessment of multiple scan areas instead of just single printed scan
Pathology (Ellipsoid zone disruption: CSR)
only identified on additional scans
Pathology may be missed (? Normal scan)
if only single scan seen
30
Macular OCTEpiretinal Membrane (ERM)
Normal
ERM
ERM (“retinal wrinkling”) ERM

5
31
Macular OCT“Pseudo”-Macular Hole (due to ERM)
Normal
“Pseudo”-Macular hole ERM
32
Macular OCTVitreo-Macular Traction (VMT)
VMT
Normal
33
Macular OCTMacular Hole (due to vitreo-macular traction [VMT])
VMT pulled off a strip of retinal tissue (= macular hole)
Normal
34
Macular OCTOpen Macular Hole BEFORE surgical repair
and Closed Macular Hole AFTER surgical repair (at Doheny UCLA )
Before repair After repair
35
Macular OCTCystoid Macular Edema (CME) with intra-retinal fluid
(can cause “swelling of retina”)
collections of fluid INSIDE retinal layers
Normal
36
Macular OCTSub-Retinal Fluid (SRF)
can cause “swelling of retina”
collection of fluid UNDER retinal layers
Normal

6
37
Macular OCTGeographic Atrophy (GA)
in dry Age Related Macular Degeneration (ARMD)
Normal 38
Macular OCTDrusen/Drusenoid Pigment Epithelial Detachments (PED)
in dry ARMD
Drusen/Drusenoid
PEDs
Normal
Normal
39
Macular OCTSub-retinal fluid (SRF)
+ hemorrhagic Pigment Epithelial Detachment (PED)- in wet ARMD
SRF PED
Normal
40
Quantitative Macular OCT AssessmentsAllows numerical evaluation for comparison between eyes
OD OS
41
Quantitative Macular OCT AssessmentsAllows numerical evaluation for progression vs. resolution
Re-scan4 weeks
aftertreatment
44
Retinal OCT ImagingImportance of Good Signal Strength

7
45
Evaluating OCT Images: Signal StrengthHigh Signal to Noise Ratio (SNR) essential in improving visualization of retinal layers
Low SNR High SNR
46
Evaluating OCT Images: Anatomical ConstraintsMove focus to area around anatomical constraints (ie corneal opacities)
47
OCT ImagingOld records important
48
Getting previous images can be useful to evaluate for “change”Digital copies (via CD,USB) are ideal
Color printouts of original scans are 2nd best“Faxed” OCTs (ie. example below) are not useful
49
Glaucoma ImagingFor diagnosis and management
Beware of potential obstacles in obtaining ‘interpretable’ OCT scans
Scan Interpretation
• High quality scan?
• Any artifacts?
• Test-retest variability?
• Reproducible?
• vs. normative database?
• Clinical correlation?
Scan Acquisition
• Media opacities
• Punctate keratopathy / corneal edema / scarring
• Dense cataract
• Retinal myopic degeneration
• peripapillary atrophy (PPA)
• Miotic pupil
• Poor vision loss of fixation
• Unable to fixate on target
• Optic disc or retinal abnormalityWu Z, Vazeen M, Varma R, Chopra V, Walsh AC, LaBree LD, Sadda SR. Factors associated with variability in retinal nerve fiber layer thickness
measurements obtained by optical coherence tomography. Ophthalmology 114:1505-1512, 2007.

8
OCT scan Signal Strength (SS)Adequate SS is necessary for an ‘interpretable’ OCT scan
• SS: intensity level of the signal & uniformity of signal within a scan
• Scale 110
• 1 = poor image quality
• 10 = excellent image quality
• “good” signal strength score : ≥ 7
Wu Z, Vazeen M, Varma R, Chopra V, Walsh AC, LaBree LD, Sadda SR. Factors associated with variability in retinal nerve fiber layer thickness measurements obtained by optical coherence tomography. Ophthalmology 114:1505-1512, 2007.
Zeiss Cirrus® SD-OCT
RNFL and ONH OCT scan analysis
Evaluate3 important
scan parametersbefore interpreting
scan
1. Signal strength2. Centration3. Scan alignment
RNFL & ONHscan
interpretation
OCT Scan Signal PatternScan display should be evenly strong with solid red line extending across the entire scan
Strong OCT scan signal patternallows proper retinal layer segmentation to accurately calculate RNFL thickness
OCT retinal layer Segmentation Errors
Poor differentiation of retinal layerscan lead to erroneous RNFLT measurements
poor Signal Strength (SS) negatively affects RNFLT
Scans with low SS may have falsely low RNFLT
OD: SS=4/10 Avg RNFLT = 77m
OS: SS=6/10 Avg RNFLT = 64m
Re-scan with higher SS yields greater RNFLT
OD: SS=8/10 Avg RNFLT = 87m
OS: SS=9/10 Avg RNFLT = 81m
Wu Z, Vazeen M, Varma R, Chopra V, Walsh AC, LaBree LD, Sadda SR. Factors associated with variability in retinal nerve fiber layer thickness measurements obtained by optical coherence tomography. Ophthalmology 114:1505-1512, 2007.
Re-scan

9
Pupil size may affect scan quality
Pre-Dilation SS = 5/10 Post-Dilation SS = 8/10
Re-scan
Proper centration of scan circle is important for accurate RNFLT measurements with good repeatability and reproducibility
Well-centered scanDe-centered scan
Decentered Scan OS
Same scan OS with proper centration
Poor centration
Centration Errors can lead to “false localized RNFLT defects”
RNFLT decreases withincreasing distance from disc
Good centration
Irregular OCT scan signal pattern can lead to erroneous RNFL thickness measurements
Possible causes of signal dropout or uneven scan
– blinking / eye movement
– PVD / floaters / vitreous debris
– Peripapillary atrophy (PPA)
Eye movement may affect scan quality
Eye Blink Eyes Open
Re-scan
OCT Retinal Layer Segmentation Error due to incomplete scan
67
Re-scan

10
Scan misalignment can lead to a poor quality scandespite “good” signal strength Posterior vitreous detachment (PVD) can interfere with OCT RNFL measurements
Scan circle
over PVD
PVD can lead to OCT signal dropout with “missing data”
Strategies to Improve Scanning
• eye movement to displace floater
• head repositioning
Peripapillary Atrophy (PPA)
• Measurement error due to scanning over area of PPA
• Very difficult to interpret such scans
OCT-based longitudinal glaucoma progression detection
Progression software availablewith serial overlay scanning
Anterior Segment OCT (AS-OCT)
• Excellent resolution of anterior segment
• Technically easy to use and quick
• Requires no contact or immersion
• Provides light and dark measurements
Scleral spur
Cornea
Angle recess
Lens
Anterior chamber
Iris root
Radhakrishnan S, Goldsmith J, Huang D, et al. Arch Ophthalmol 2005;123:1053-9.

11
Anterior Segment OCT (ASOCT): Evaluating treatment outcomes
• Critical to analyze the quality of data from imaging devices
before interpreting the data
•An abnormality on imaging always
requires clinical correlation for correct interpretation
Ocular imaging is now an integral part of ophthalmologyImaging can augment, but does not replace an excellent clinical work-up and exam
by astute technicians and physicians
‘Normal RNFL’ thickness per Normative Databasedoes not always mean normal (non-glaucomatous) optic disc
OD
OS
No cupping with high-normal RNFL
high-normal RNFL low-normal RNFLOS
OS
OD
OD
Vertical cupping with low-normal RNFL
ASYMMETRIC RNFL values
Disc pallor > cupping
Disc pallor > cupping
‘Abnormal RNFL’ thickness per Normative Databasedoes not always correspond with a glaucomatous optic disc
OD
OS
OD - RNFL loss OS - RNFL loss
OPTIC ATROPHY
83
THANK YOU.