Embed Size (px)
Citation preview

1
Accomplishing More Together: Collaborative Approaches for Treating Social Communication After
Acquired Brain Injury
Heidi Iwashita, M.S., CCC-SLP
McKay Moore Sohlberg, Ph.D., CCC-SLP
OSHA Fall Conference
October 13, 2018
Disclosures
Heidi Iwashita, M.S., CCC-SLP:• No relevant financial or nonfinancial disclosures related to this talk
• Employed as a Graduate Employee for the Communication Disorders & Sciences (CDS) program at the University of Oregon (UO)
• In the doctoral program of CDS at UO
McKay Moore Sohlberg, Ph.D., CCC-SLP:• No relevant financial or nonfinancial disclosures related to this talk
• A salaried professor in CDS at UO
• Receives grant support from the National Science Foundation and National Institute for Health for projects unrelated to this talk
• Receives book royalties for texts unrelated to the content of this talk
Learning Objectives
After completion of this program, you should be able to:
1. Describe three evidence-based collaborative approaches for treating social communication following acquired brain injury
2. Discuss ways to overcome common obstacles to incorporating collaborative treatment approaches
3. Identify communication partner strategies that foster collaborative communication with a person who has had acquired brain injury
Icebreaker
What is your name?
Where do you work?
What kinds of challenges have you experienced collaborating with clients and others?
What are you hoping to learn from this presentation?
OSHA 2018Strength in Collaboration
• Collaboration– Cooperation– Working together on shared goals– Mutual engagement– Repair of breakdowns
• Complex cognitive and communication skills– May be affected by brain injury
• Reduced processing speed• Reduced ability to repair• Difficulty comprehending complex info• Reduced verbal organization or fluency
(Abreu, Zhang, Seale, Primeau, & Jones, 2002)
Aims of Collaborative Approaches
• Maximize engagement
• Honor autonomy
• Resist the “righting reflex”
• Recognize individual and cultural differences
• Create “buy-in”, leading to
• Greater motivation
• Better outcomes
• Harness strengths of family, peers, others to help recovery
• Create a supportive environment
• Promote open communication

2
• People with ABI may be vulnerable to exclusion
– Interdisciplinary meetings
– Treatment decision making
“At times, it was felt that the professionals were the experts in the client’s life, not the client an expert in his or her own life.”
• When included, may not fully participate
– “OK”, “yes,” “no”
– Minimally engaged, passive
“The role of such clients in supposedly client-centered interdisciplinary meetings is therefore like a ‘ritual ghost’ rather than a full participant” (Abreu, Zhang, Seale, Primeau, & Jones, 2002).
“Ritual Ghosts”
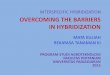
What is social communication?
Social
Interaction
• Culture• Gender• Social
reasoning• Social
tasks• Conflict
resolution• Power
relation-ships
Pragmatics
• Theory of Mind
• Emotional competence
• Joint attention
• Inference• Presup-
position
• Verbal:
– Speech acts
– Prosody
– Discourse
• Nonverbal:
– Body language
– Gesture
– Facial expression
– Proxemics
– Gaze shifts
• Comprehension
• Expression
• Morphology
• Semantics
• Syntax
• Phonological skills
Social Cognition
Language Processing
Source: ASHA.org, Components of Social Communication
Assessment of Social Communication
• Numerous tools have been developed
• No perfect tool measures all aspects
• Should look at communication in natural contexts
• Need to consider
– Culture
– Individual and family preferences, priorities
• Often there is a subjective element
– Can you get alternative perspectives?
– Look at functioning in community, with friends, and with everyday communication partners
Assessment Tool Categories & Examples
Performance-based measures
Receptive
Social cognition, e.g. TASIT
Expressive
e.g. FAVRES
Clinician-reported measures
Pragmatic Rating Scales
PRS (see handout)
Adapted Kagan Scales (Togher et al., 2010)
Self/Other reported measures
La Trobe Communication Questionnaire
Common impairments after ABI
• Losing train of thought – memory and attention• Spoken discourse
– Less coherent and informative– More effortful or disorganized
• Has social knowledge, but has difficulty applying it– Self-regulation– Self-awareness
• Emotion perception– Voice– Facial expression, body language
• Emotion expression• Impulsivity• Reduced initiation

3
Profile 1: “Denise”
• Dorsolateral/dorsomesial prefrontal lesions
• Reduced initiation
• Apathy
• Lack of drive
• Lethargy
• Inattentiveness
• Reduced spontaneity
• Reduced emotional reactivity
Profile 2: “Eric”
• Orbitofrontal damage due to MVA
• Lack of inhibition
• Impulsiveness
• Lability
• Reduced anger control
• Aggressiveness
• Poor social judgement
Person-Centered Goalsetting
Audience Poll
When working with adults with ABI, how often does the client themselves bring up and decide on the goal(s) they most want to work on with you?
1) It’s the client’s choice 90-100% of the time
2) It’s the client’s choice 70-89% of the time
3) It’s the client’s choice over half but less than 70%
3) I choose goals for my clients more than half the time
4) I choose goals for my clients over 70% of the time
Collaborative Goalsetting
A key part of assessment:– Get client input
• Current functional challenges• Priorities• Readiness to change• Individual/cultural factors
– Set up a meaningful way to measure progress
As treatment:• Direct the client’s attention and effort towards a
specific functional outcome (Berquist et al., 2012)• Increases satisfaction, enhances outcomes (Plant et
al., 2016)
Motivational Interviewing
• Combines interviewing and counseling techniques
• Honors client autonomy
• Increases readiness to change
• Increases motivation
• Strengthens rapport
• Facilitates selection of goals that have larger impact for the client

4
Five Principles of Motivational Interviewing
1. Express empathy through reflective listening
-OARS
2. Develop discrepancy between clients' values and current behavior
-Develop awareness
-Arguments for change come from the client
3. Avoid argument and direct confrontation
4. Adjust to client resistance rather than opposing it directly
5. Support self-efficacy and optimismMiller & Rollnick, 1991; Medley & Powell, 2010
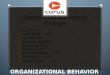
Goal Attainment Scaling (GAS)
• Individualized, objective outcome measure based on client-
centered goals
• Criterion-referenced
• Uses a 5-point scale
• Values range from 2 (most favorable) to -2 (least favorable)
• Can obtain standardized scores such as T-scores to analyze
results across clients
Example of GASLevel of Outcome Statement of Outcome
Best outcome Denise initiates social contact 4+times per week
Better than expectedlevel
Denise initiates social contact 3times per week
Expected level afterworking on it for 2-3months
Denise initiates social contact 2times per week
Baseline level Denise initiates social contactonce per week
Goal Attainment Scaling (GAS)
Key Components: SMARTED
• Specific
• Measurable
• Attainable
• Relevant
• Time-specific
• Equidistant
• uniDimensional
Obstacles to Collaborative Goalsetting
Four themes emerged as barriers to goal-setting (Plant et al., 2016):
1. Mismatch between staff and patients’ perspectives
2. Patient-related barriers
• Communication difficulties, cognitive impairments, fatigue, mood disorders, medical co-morbidities, uncertainty, limited awareness
3. Staff related barriers
4. Organizational/service level barriers
• Time, resources
Overcoming Barrier #1: Mismatchin Perspectives
• Open, early, and frequent communication with patients/families about goals
• Explicit strategies to educate patients/families about goalsetting and enhance participation
• Tailor the process to the individual
– Big goals or small?
– Fewer goals
– Patient-led or therapist-led
• Material to support patients in identifying goals
– Example goals
– Worksheets(Plant et al., 2016)

5
Overcoming Barrier #2: Patient-Related Barriers
• Cognitive-communication barriers
– Provide written materials in simple language
– Pictures/copies of the goals
– Patient-held records, action plans
• Fatigue
– Timing, breaks
• Mood disorders – team approach
• Family involvement may be facilitative or disruptive
• Uncertainty about recovery process
– Clarify expectations, provide education
Barriers to Goal-Setting: Limited Awareness
• “I don’t have a problem”
– Confrontation can make denial stronger
• Align yourself with them, not against them
• Be positive and encouraging
• Allow them opportunities to experience difficulty
• Education on effects of brain injury
• Structured feedback
Self-directed reflection and feedbackVideo feedback
Journal of successes and struggles
Overcoming Barriers #3 and #4
• Staff-related obstacles
– Education, training
• Organizational/service level barriers
– Time• Limited time for evaluation
• Treatment– Individualized, functional goalsetting as a treatment approach
– Periodic revisiting of goals
– Reviewing progress
– Resources• Interdisciplinary team
Facilitators to Goal-Setting
• Individualized goal-setting process
• Strategies to promote communication and understanding
– Visual aids, written materials, active listening
• Avoiding disappointment and unrealistic goals
– Education on realistic goalsetting
• Staff and patients’ knowledge, experience and enthusiasm for goal-setting
(Plant et al., 2016)
Goal-Setting Worksheets
• Provide simple explanation of goals & measurement
• Space to jot down concerns
• Have clients prioritize and discuss
• Ask the client “how would it make sense to measure that goal?” giving examples
– Times per week
– Duration
– Accuracy
– Rating scales
• Frequently confirm understanding, whether this goal gets at what they want to improve
Useful questions for collaborative goalsetting
• If you could wave a magic wand and change one thing—what would it be?
• How motivated are you to change this? (rate 1-10)
• What have you tried so far?
• What seems to help or not help?
• How would it look for you if this problem completely went away? (GAS +2 level)
• How much do you expect it to get better after working on it for a few months? (GAS 0 level)
• Is there anything else I didn’t ask about?

6
Role-Play Demonstration
Self-Reflection & Discussion
• Was this helpful?
• What would you need in order to be committed to
consistently using person-centered goal setting?
Communication Partner Training
Audience Poll
How many of you routinely train the communication partners of a person with ABI to communicate with them more effectively?
What might a communication partner do that hinders the communication effectiveness of a person with ABI?
Communication Partner Training
• Impairment participation• Communication
– Context-bound– Interactive
• Everyday Conversation partners (ECP) may unwittingly sabotage communication
• Post-injury changes by ECP in communication style may give people with ABI fewer chances to shine
• ECP can be taught to – Reveal competence of person with ABI– Provide cognitive and emotional support– Provide facilitative contexts
Communication Partner Training
• More effective than when the person with ABI is trained alone (Togher, McDonald, Tate, Power, & Rietdijk, 2013)
• When given a powerful information-giving role, e.g. a guest speaker, the communication of people with ABI approximated matched control participants (Togheret al., 2011).
• Question your assumptions
– Look at context, interaction

7
How Communication Partners maySabotage Communication
• Asking questions they already know the answer to
• Talking down to people with ABI
• Talking too slowly
• Repeatedly checking on accuracy
• Not giving enough opportunities
• Not providing natural consequences
• Failing to follow up on information given by person with ABI
(Togher et al., 2011)
Key Features of Collaboration During Conversation (Ylvisaker et al., 1998; Togher et al., 2011)
• Collaborative intent
“We’re doing this together”
• Cognitive support
“What can help make this easier?”
• Emotional support
“I’m with you, it’s OK”
• Positive question style
“I’m interested in what you have to say”
• Collaborative turn taking
“I’m interested in sharing conversation”
Cognitive Support:Examples
Cognitive Support
• Gives information
• Uses memory aids
• Uses organization supports
• Gives cues
• Gives correct information in a non-punitive manner when correcting errors
Lack of Cognitive Support
• “Quizzes” person with ABI
• Fails to encourage cognitive supports
• No cues
• Corrects in a punishing manner
Togher et al., 2011
Communication Partner Strategy:
Elaboration of Topics
Elaboration of Topics• Topic of interest that can go
further
• Maintain the topic
• Partner contributes information
• Partner asks open-ended questions
Non-Elaborative
• Low-interest topic
• Low potential to elaborate
• Changes topic frequently
• Partner does not add enough information
• Partner does not ask questions
Togher et al., 2011
Communication Partner Strategy:Elaborative Organization(Togher et al., 2011)
Elaborative Organization
• Sequential order
• Causality
• Make connections
• Review organization of information
Non-Elaborative
• Fail to organize information
• Fail to review information
• Fail to make connections clear when topics change
Togher et al., 2011
How to Teach These Strategies
• Group Approach• E.g. TBI Express• Peer support and modeling
• Individualized, family-centered training• Get a baseline with each family member
• Adapted Kagan Scales
• Encourage expression by person with ABI• What’s working, what’s not working• Discuss videos taken outside therapy• Choose one skill to work on at a time• Model skill• Provide frequent opportunities to practice• Family member and person with ABI must demonstrate it
successfully

8
Negotiating Group Rules
Partner Training - Obstacles
1. Difficult family adjustment to injury
➢ Hard to reconcile past vs. presentStill coping with “loss” of valued traits in past loved one
➢ Unrealistic expectations for recoveryMay embrace fad diets, pseudoscience
May try hard to “train” the loved one’s memory
2. No partner available
3. Provider level: SLP not aware of need/materials
4. Organizational/service level barriers
• Time, resources
How to Overcome Obstacles
1. Difficult family adjustment
• Listen & validate differences in perspectives
• Be sensitive to cultural and generational influences
• Promote awareness
• Video reflections
• Journals of successes/failures
• Structured self-rating of their own communication
2. No partner available for intensive program
• Train staff
• Make handouts
• Utilize any brief training opportunities
How to Overcome Obstacles
3. Provider level: SLP not aware of need/materials
• Question assumptions, look at context
• Be flexible, take client’s perspective
• Some videos here: http://sydney.edu.au/health-sciences/tbi-express/
• See References list
4. Organizational/service level barriers
• Time, resources• Group therapy?
• Offer training to community brain injury groups
Context-Sensitive Intervention
Context-Sensitive Intervention
• Away from treating individuals in isolation• Situated in everyday activities• Focus on complex interactions• “Everyday, positive routines”
• Ylivisaker & Feeney, 1998• Involves family, staff, peers • Create successful routines in context
• Collaboration• Coaching• Scaffolding

9
Principles of Ylvisaker’s (2006) “Self-Coaching” Intervention
Automatic self-regulation
Participant Involvement
Specificity of real-world needs
Negotiation of scripts and metaphors
Motivating associations
Self-coaching plays/scripts and communication partner scripts
Practice Monitoring, revisions, and
celebration
Customized Strategies & Scripts
• Self-coaching scripts
– Individualized
– Address obstacles common after ABI
• Emotion control
• Impulsivity
• Difficulty interpreting others’ behavior
• Trouble managing everyday routines
• Metacognitive Strategies
– Developing awareness
– Learning and practicing when to use
Example Self-Regulatory Scripts(Ylvisaker, 2006)
• “Let’s think about that” (impulsivity)
• “What about you?” (egocentrism)
• Respect (boundaries)
– “Is it OK to give this person a hug?”
– “Does that person like that nickname?”
• “Hang in there” - motivating self-talk
• “Am I ready?”
• “Am I sure?”
Positive Metaphors
Individualized
• Sports: self-coaching
• Music: Self-conducting
• Dance: Self-choreographing
• Business: Self-managing; self-supervising
• Film: Self-directing
• Ranching: Self-shepherding
• Hiking: Self-guiding
• Military: Self-commanding
Positive Metaphors
Choosing a personalized positive role model
– The type of person they CAN be
– when effectively self-regulated• Sports, entertainment
• E.g. Clint Eastwood, Wayne Gretsky
Similarly, the person with ABI can choose an example of a negative role model representing how they are when not effectively self-coached
• A “Mike Tyson” kind of person
Ylvisaker, 2006
Obstacles to Context-Sensitive Interventions
• Lack of self awareness– Denial– Overestimating own ability– Rigid thinking– Pessimism
• Passive attitude– Low initiation– Prefers therapist to lead
• Memory deficits– Remembering when to use
strategies

10
Obstacle #1Lack of Self-Awareness
• Inconsistent awareness across domains• Awareness is not unitary
– “Blind spots”– More awareness for motor and sensory deficits than for
cognitive deficits– More awareness for memory, language deficits than
abstract thinking and social deficits• May have good intellectual understanding of deficitsand still be unable to use this knowledge to self-regulate• Cultural component
– Harder to admit deficits in areas more valued by your culture
Toglia & Kirk, 2000
Overcoming Obstacle #1
• Restructuring of one’s beliefs of strengths and limitations
– Pre-injury beliefs New beliefs
– “Getting to know oneself” again
– Learn best from “mastery experiences”
• Guided mastery
Obstacle #3: Memory Deficits
• Remembering when and how to use strategies
– Systematic instruction
– Ample opportunities for practice
– Negotiate partner cueing (Ylvisaker, 2006)
– Negotiate natural, sustainable visual aids
– Daily reminder
• Consider a different approach if memory deficits are severe
– Focus on communication partner training
Awareness Training
• Self-monitoring skills more likely to emerge on familiar tasks that are “just the right amount” of challenge
– Too difficult fail to integrate
– Too easy fail to generalize to real tasks
• Structure experience so person can discover errors themselves
– And feel control and mastery over performance
• Structured methods of self-questioning, self-evaluation
• Video reflection, feedback
Obstacle #2: Apathy“Denise”
• Motivational interviewing– Not a strong evidence base for clients with – apathy (Brett et al., 2015)
• Provide personalized information on injury• Behavioral contracting
– Specific– Written
• Contingent rewards– Token economy
• For non-compliant behaviors– Antecedent management– Barrier reduction
• Reminder call before each session• Modify task demands (unloading vs. loading the dishwasher)
– Graded confrontation (indirect, then direct)Brett et al., 2015
Wrap Up
Three collaborative approaches for treating social communication following ABI are person-centered goalsetting, communication partner training, and context-sensitive intervention.
Common obstacles and ways to overcome them are___
Helpful communication partner strategies are ____
Questions?
Contact: [email protected]

11
References
Abreu, B. C., Zhang, L., Seale, G., Primeau, L. & Jones, J. S. (2002). Interdisciplinary meetings: Investigating the collaboration between persons with brain injury and treatment teams. Brain Injury, 16(8), 691-704. https://doi.org/10.1080/02699050210128942
American Speech Language Hearing Association, n.d. Components of Social Communication. https://www.asha.org/uploadedFiles/ASHA/Practice_Portal/Clinical_Topics/Social_Communication_Disorders_in_School-Age_Children/Components-of-Social-Communication.pdf
Berquist, T. F., Micklewright, J. L., Yutsis, M., Smigielski, J. S., Gehl, C., & Brown, A. W. (2012). Achievement of client-centered goals by persons with acquired brain injury in comprehensive day treatment is associated with improved functional outcomes. Brain Injury, 26(11), 1307-1314. https://doi.org/10.3109/02699052.2012.706355
Brett, C. E., Sykes, C., & Pires-Yfantouda, R. (2015). Interventions to increase engagement with rehabilitation in adults with acquired brain injury: A systematic review. Neuropsychological Rehabilitation 27(6), 1-24. https://doi.org/10.1080/09602011.2015.1090459
Finch, E., Copley, A., Cornwell, P., & Kelly, C. (2016). Systematic review of behavioral interventions targeting social communication difficulties after traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 97, 1352-65. https://doi.org/10.1016/j.apmr.2015.11.005
Gordon, R., G., & Duff, M. C. (2016). Incorporating principles of the collaborative contextualised intervention approach with the empirical study of learning and communication in traumatic brain injury. Aphasiology, 30(12), 1461-1482. https://doi.org/10.1080/02687038.2015.1136050
Grant, M., & Ponsford, J. (2014). Goal Attainment Scaling in brain injury rehabilitation: Strengths, limitations and recommendations for future applications. Neuropsychological Rehabilitation, 24(5), 661-677. https://doi.org/10.1080/09602011.2014.901228
References
MacDonald, S. (2017). Introducing the model of cognitive-communication competence: A model to guide evidence-based communication interventions after brain injury. Brain Injury, 31 (13-14), 1760-1780
https://doi.org/10.1080/02699052.2017.1379613
MacLennan, D.L., Cornis-Pop, M., Picon-Nieto, L., and Sigford, B. (2002). The prevalence of pragmatic communication impairments in traumatic brain injury. Poster presentation from the 2002 Brain Injury Association Conference.
Medley, A. R., & Powell, T. (2010). Motivational interviewing to promote self-awareness and engagement in rehabilitation following acquired brain injury: A conceptual review. Neuropsychological Rehabilitation, 20(4), 481-508. https://doi.org/10.1080/09602010903529610
Miller, W. R. and Rollnick, S. (1991) Motivational interviewing: Preparing people to change addictive behavior. New York: Guilford Press.
Plant, S. E., Tyson, S. F., Kirk, S., & Parsons, J. (2016). What are the barriers and facilitators to goal-setting during rehabilitation for stroke and other acquired brain injuries? A systematic review and meta-synthesis. Clinical Rehabilitation, 30(9), 921-930. https://doi.org/10.1177/0269215516655856
Togher, L. (2013). Improving communication for people with brain injury in the 21st century: The value of collaboration. Brain Impairment, 14(1), 130-138. https://doi.org/10.1017/BrImp.2013.3
Togher, L., McDonald, S., Tate, R., Power, E., & Rietdijk, R. (2013). Training communication partners of people with severe traumatic brain injury improves everyday conversations: A multicenter single blind clinical trial. Journal of Rehabilitation Medicine, 45, 637-545. http://doi.org/10.2340/16501977-1173
Togher, L., McDonald, S., Tate, R., Power, E., & Rietdijk, R. (2009). Training communication partners of people with traumatic brain injury: Reporting the protocol for a clinical trial. Brain Impairment, 10(2), 188-204.
https://doi.org/10.1375/brim.10.2.188
Togher, L., McDonald, S., Tate, R., Power, E., Ylvisaker, M., & Rietdijk, R. (2010). TBI Express: Communication Training Manual. Australian Society for the Study of Brain Impairment, Sydney: Australia
References
Togher, L., Power, E., Tate, R., McDonald, S., & Rietdijk, R. (2010). Measuring the social interactions of people with traumatic brain injury and their communication partners: The adapted Kagan scales. Aphasiology, 24 (6-8), 914-927.
Toglia, J. & Kirk, U. (2000). Understanding awareness deficits following brain injury. Neurorehabilitation, 15 (2000), 57-70
Ylvisaker, M. (2006). Self-coaching: A context-sensitive, person-centered approach to social communication after traumatic brain injury. Brain Impairment, 7(3), 246-258. https://doi.org/10.1375/brim.7.3.246
Ylvisaker, M., & Feeney, T. (1998). Collaborative brain injury intervention: Positive everyday routines. San
Diego: Singular Publishing Group.
Ylvisaker, M. & Feeney, T. (2000). Reflections on Dobermanns, poodles, and social rehabilitation for difficult-to-serve individuals with traumatic brain injury. Aphasiology, 14 (4), 407-431
Graphics from https://pngtree.com, www.pexels.com

12
PRAGMATICS RATING SCALE
D. MacLennan, M.A.
I. Non-Verbal Aspects of Communication
INTELLIGIBILITY
__________________________________________________________
1 2 3 4 5
Frequent distortion of
words. Speech is 0-
5% intelligible.
Moderate distortion
of words. Speech is
36-65% intelligible.
Normal or near-
normal clarity of
words. Speech is
95-100%
intelligible.
FLUENCY
__________________________________________________________
1 2 3 4 5
Communication is
consistently
characterized by
incomplete
utterances, false
starts, and cut-off
words. Normal
fluency occurs 0-5%
of the time.
Communication is
characterized by few
incomplete
utterances, false
starts and cut-off
words. Normal
fluency occurs 36-65%
of the time.
Normal fluency
occurs 95-100% of
the time.
PROSODY
__________________________________________________________
1 2 3 4 5
Severely reduced
variation of
intonation and stress.
Normal prosody 0-5%
of the time.
Moderately reduced
variation of intonation
and stress. Normal
prosody 36-65% of
the time.
Normal variation
of intonation and
stress 95-100% of
the time.

13
FACIAL EXPRESSION
__________________________________________________________
1 2 3 4 5
Severely reduced
variation of facial
expression. Normal
facial expression 0-5%
of the time
Moderately reduced
variation of facial
expression. Normal
facial expression 36-
65% of the time.
Normal variation
of facial
expression
95-100% of the
time.
EYE CONTACT
__________________________________________________________
1 2 3 4 5
Severely reduced eye
contact. Normal eye
contact 0-5% of the
time
Moderately reduced
eye contact. Normal
eye contact 36-65% of
the time.
Normal variation
of eye contact 95-
100% of the time.
GESTURE
__________________________________________________________
1 2 3 4 5
Minimal use of gesture
or unusually frequent
or bizarre gestures that
distract from
conversation. Normal
use of gesture occurs
0-5% of the time.
Limited use of gesture
or moderate
occurrence of bizarre
gestures that distract
from conversation.
Normal use of gesture
occurs 36-65% of the
time.
Normal use of
gesture to support
communication
95-100% of the
time.

14
II Propositional Aspects of Communication
COHESION
__________________________________________________________
1 2 3 4 5
Communication is
consistently vague
and lacks adequate
information or clear
referents 95-100% of
the time.
Communication is
moderately vague and
lacks adequate
information or clear
referents 36-65% of
the time.
Communication is
consistently clear
with ample
information for
understanding
and clear
referents 0-5% of
the time.
RELEVANCE (topic maintenance)
__________________________________________________________
1 2 3 4 5
Communication
is consistently
irrelevant to topic.
Conversation is
relevant 0-5% of the
time.
Communication is
moderately irrelevant
to topic.
Conversation is
relevant 36-65% of
the time.
Communication is
consistently
relevant to topic
95-100% of the
time.
ELABORATION (topic maintenance)
__________________________________________________________
1 2 3 4 5
Severely reduced
topic elaboration.
Produces consecutive
utterances related to
a given topic or
responds to
communication
partner’s comments
0-5% of the time.
Moderately reduced
topic elaboration.
Produces consecutive
utterances related to
a given topic or
responds to
communication
partner’s comments
36-65% of the time.
Normal
elaboration of
topic. Produces
consecutive
utterances related
to a given topic or
responds to
communication
partner’s
comments 95-
100% of the time.

15
INITIATION (quantity/conciseness)
__________________________________________________________
1 2 3 4 5
Severely reduced
initiation of new
topics. Initiates new
topic where
appropriate 0-5% of
the time.
Moderately reduced
initiation of new
topics. Initiates new
topic where
appropriate 36-65%
of the time.
Normal initiation
of new topics.
Initiates new
topics where
appropriate 95-
100% of the time.
VERBOSITY (quantity/conciseness)
__________________________________________________________
1 2 3 4 5
Communication is
consistently
characterized by
excessive detail or
unnecessary
repetition of
information.
Appropriate detail
and repetition 0-5%
of the time.
Communication is
characterized by
moderately excessive
detail or unnecessary
repetition of
information.
Appropriate detail
and repetition 36-65%
of the time.
Communication
has appropriate
amount of detail
and repetition of
information 95-
100% of the time.
III Interactional Aspects of Communication
APPROPRIATENESS (topic management)
__________________________________________________________
1 2 3 4 5
Severe impairment in
selecting topics
appropriate to
context. Topic is
appropriate to
situational context 0-
5% of the time.
Moderate impairment
in selecting topics
appropriate to
context. Topic is
appropriate to
situational context
36-65% of the time.
Topics introduced
in conversation
are appropriate to
situational context
95-100% of the
time.

16
RESPONSIVENESS (turn-taking)
__________________________________________________________
1 2 3 4 5
Severely increased
response latency.
Normal response
latency occurs
0-5% of the time
Moderately increased
response latency.
Normal response
latency occurs 36-65%
of the time.
Normal response
latency occurs
95-100% of the
time.
INTERRUPTION (turn-taking)
__________________________________________________________
1 2 3 4 5
Consistent
interruption of
communication
partner. Interruption
occurs
95-100% of the time.
Moderate
interruption of
communication
partner. Interruption
occurs
36-65% of the time.
Minimal
interruption of
communication
partner.
Interruption
occurs 0-5% of the
time.
FEEDBACK
__________________________________________________________
1 2 3 4 5
Severe reduction of
verbal or non-verbal
response to
communication
partner. Appropriate
feedback occurs 0-5%
of the time
Moderately reduced
verbal or non-verbal
response to
communication
partner. Appropriate
feedback occurs 36-
65% of the time.
Normal verbal or
non-verbal
response to
communication
partner.
Appropriate
feedback occurs
95-100% of the
time.

17
REPAIR
__________________________________________________________
1 2 3 4 5
Severely reduced
repair of
conversational
breakdown.
Conversational repair
occurs 0-5% of the
time where
appropriate
Moderately reduced
repair of
conversational
breakdown. Repair
occurs 36-65% of the
time where
appropriate.
Normal repair of
conversational
breakdown.
Conversational
repair occurs 95-
100% of the time
where appropriate

18
Priorities
We’ve talked about several things you might be interested in
working on with us. What seems to be most important?
______________________________________
______________________________________
______________________________________
______________________________________
______________________________________
______________________________________

19
Measurement
• How often?
o In a week, in a day, in an hour, in 15
minutes?
• How well?
o Accuracy
o Performance
• How much time does it take to do something?
o Efficiency
• Self-rating, 1-5
o Rate your effort (when you do the task)
o Rate your confidence (in
o being able to do the task)
• Who will measure this?
• How will you measure this?

20
Goal #1 At this level, I would
consider this
problem solved
Where I hope to be
after ____
weeks/months
Where I hope to be
after ____
weeks/months
Where I am now
Goal #2
At this level, I would
consider this
problem solved
Where I hope to be
after ____
weeks/months
Where I hope to be
after ____
weeks/months
Where I am now