Embed Size (px)
Citation preview
Learnings from the ICO Task Force on uncorrected refractive errors and school eye health
Produced by the ICO Task Force on Uncorrected Refractive Errors and School Eye Health
3
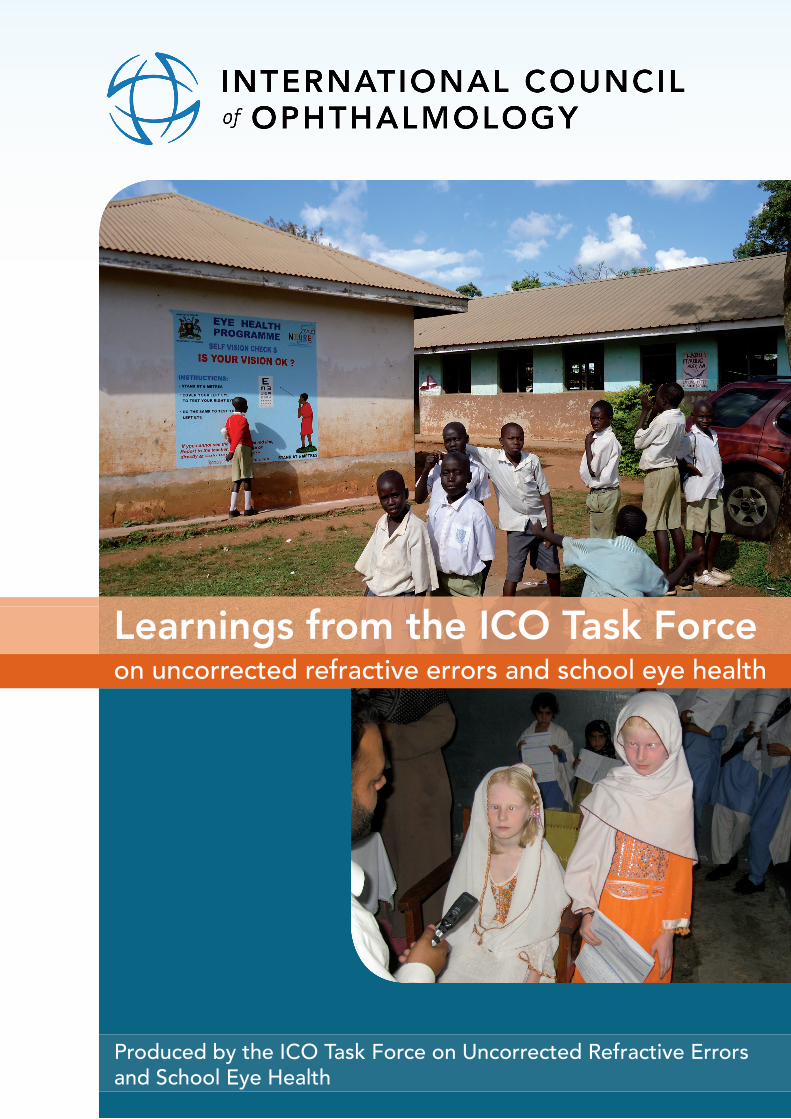
Acronyms and Abbreviations .............................................................................. 3
Foreword by Professor Bruce Spivey .................................................................. 4
Message from the ICO President ........................................................................ 5
Acknowledgements ............................................................................................. 6
Membership of the ICO Task Force..................................................................... 8
Envisaged outcomes of the ICO URE & SEH strategies..................................... 9
Uncorrected Refractive Error – Facts and Figures............................................. 10
Collaboration and Co-operation........................................................................ 12
Strategic Plan 2010 to 2015............................................................................... 15
Managing the lessons learned............................................................................ 17
Key points of learning......................................................................................... 19
Model of successful service provision for NIURE .............................................. 22
Curricula development........................................................................................ 23
Supranational infl uence....................................................................................... 24
Resources and References.................................................................................. 25
Strategic plan and activities of the ICO Task Force on URE & SEH................... 26
Contents
Photographs on front cover courtesy of Wolfgang Gindorfer,NIURE – Uganda (top) and Dr. M. Babar Qureshi (bottom)
Acronyms and Abbreviations
Acronym/abbreviation Description
CBM
CPD
CVC
EMR
HRD
ICO
IJCAHPO
INGDO(s)
MEACO
NIURE
PAAO
PAHO
SEH
URE
UREIG
WCRE
Christoffel-Blindenmission
Continuing professional development
Community vision centre project (Pakistan)
Eastern Mediterranean Region
Human resource development
International Council of Ophthalmology
International Joint Commission for Allied HealthProfessionals in Ophthalmology
International non-government development organisation(s)
Middle Eastern and African College of Ophthalmologists
National Intervention on Uncorrected Refractive Errors(Uganda)
Pan-American Association of Ophthalmologists
Pan-American Health Organization
School eye health
Uncorrected refractive error
Uncorrected refractive error interest group
World Congress on Refractive Error
ICT Information and Communication Technology

54
As the ICO and world ophthalmology began to focus on uncorrected refractive error, Dr. Babar Qureshi was asked to lead the ICO effort in this regard. He quickly put together an outstanding group of colleagues that proceeded to evaluate the provision of refractive and diagnostic services to school children both in Pakistan and Nigeria. Working with Light for the World in a marvellously collaborative manner, this study was confronted with numerous challenges, well described in this report.
The International Council of Ophthalmology is sograteful to Dr. Qureshi and his team for doing this study and carefully and articulately describing learnings from it.
I would also like to thank Johannes Trimmel for his support and partnership during this entire study. Light for the World was an understanding and wonderful partner.
The implications are many, and the challenge in the world remains. This first step by the ICO will be invaluable as we recommend actions for the future to our colleagues.
Foreword by Professor Bruce Spivey
Professor Bruce Spivey
It is with great pleasure that I write to introduce this important work and the report of Dr. Qureshi and the Task Force on Uncorrected Refractive Error.
The Durban Declaration of 2007 recognised the role of uncorrected and under-corrected refractive error as major causes of blindness and vision loss and that it was a problem of global significance.
Prior to that almost all data on vision loss assumed that everyone would already possess their best correction!
To address this important issue the International Council of Ophthalmology established this Task Force. The Task Force has done an outstanding job to develop guidelines and curricula, and to implement some highly successful demonstration training and service delivery programs. From this work have emerged three key principles, the need for integration, coordination and advocacy. All of this work and future work needs to be done in collaboration and we are all most grateful to with partners with whom the current work was performed.
I commend and thank Dr. Qureshi and all the members of the Task Force for this important contribution.
Professor Hugh Taylor AC
Photo courtesy of University of Melbourne
Message from the ICO President
6 7
Dr. Babar Qureshi
Photo courtesy of CBM
The ICO URE & SEH committee would like to thank LIGHT FOR THE WORLD for the generous provision of resources in terms of financing the pilot programmes, provision of time and expertise as well as continued support to the cause of uncorrected refractive errors and school eye health globally.
The committee further likes to thank CBM for its continues technical support as well as chartering new frontiers with ICO in the field of uncorrected refractive errors.
We would like to thank all the people who have contributed to the implementation of the pilot programmes, especially the JOS university teaching hospital Nigeria, the comprehensive health and education forum international CHEF and the LIONS institute of community ophthalmology, Madurai, India.
AcknowledgementsAcknowledgements
On a special note, the committee would like to acknowledge the strong and visionary leadership of Prof. Bruce Spivey and his wholehearted support which led to the formation of this task force and its sustained achievements globally.
We are truly grateful to Wolfgang Gindorfer for having supported the task force as the secretary for all this years as well as providing a very high technical input to the task force and to the programmes that we have been able to achieve.
Finally, the task force expresses its sincere appreciation to Dr. Gillian Cochrane for voluntarily developing and formatting the manuscript and Dr. Serge Resnikoff for providing additional information.
Chairman ICO Taskforce on URE and School Eye Health
98
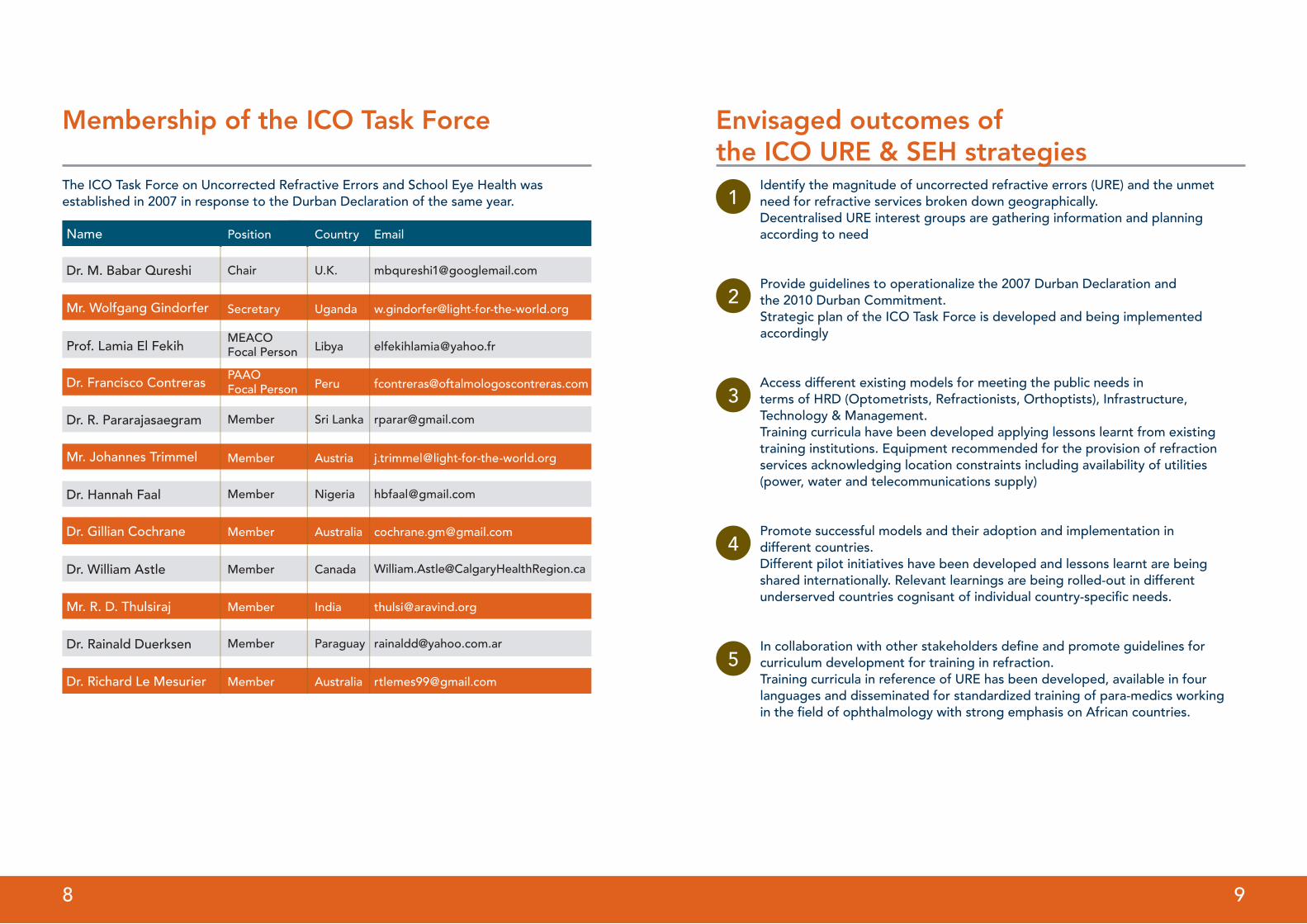
Membership of the ICO Task Force
Name Position Country Email
Dr. M. Babar Qureshi Chair U.K.
The ICO Task Force on Uncorrected Refractive Errors and School Eye Health wasestablished in 2007 in response to the Durban Declaration of the same year.
Mr. Wolfgang Gindorfer Secretary Uganda [email protected]
Prof. Lamia El FekihMEACO Focal Person Libya [email protected]
Dr. Francisco Contreras Peru [email protected] Person
Dr. R. Pararajasaegram Member Sri Lanka [email protected]
Mr. Johannes Trimmel Member Austria [email protected]
Dr. Hannah Faal Member Nigeria [email protected]
Dr. Gillian Cochrane Member Australia [email protected]
Dr. William Astle Member Canada [email protected]
Mr. R. D. Thulsiraj Member India [email protected]
Dr. Rainald Duerksen Member Paraguay [email protected]
Dr. Richard Le Mesurier Member Australia [email protected]
Identify the magnitude of uncorrected refractive errors (URE) and the unmet need for refractive services broken down geographically.Decentralised URE interest groups are gathering information and planningaccording to need
Provide guidelines to operationalize the 2007 Durban Declaration andthe 2010 Durban Commitment.Strategic plan of the ICO Task Force is developed and being implementedaccordingly
Access different existing models for meeting the public needs interms of HRD (Optometrists, Refractionists, Orthoptists), Infrastructure,Technology & Management. Training curricula have been developed applying lessons learnt from existingtraining institutions. Equipment recommended for the provision of refractionservices acknowledging location constraints including availability of utilities(power, water and telecommunications supply)
Promote successful models and their adoption and implementation indifferent countries. Different pilot initiatives have been developed and lessons learnt are being shared internationally. Relevant learnings are being rolled-out in differentunderserved countries cognisant of individual country-specifi c needs.
In collaboration with other stakeholders defi ne and promote guidelines forcurriculum development for training in refraction.Training curricula in reference of URE has been developed, available in fourlanguages and disseminated for standardized training of para-medics workingin the fi eld of ophthalmology with strong emphasis on African countries.
1
2
3
4
5
Envisaged outcomes ofthe ICO URE & SEH strategies
1110
During the first World Congress on Refractive Error (WCRE) in Durban 14 - 16 March 2007, the Durban Declaration on Refractive Error was affirmed and signed in front of key international non-government development organisations (INGDOs) and eye care bodies.
It affirmed that uncorrected refractive error was a public health problem of great social and economic cost especially to developing communities where poverty is rife.
The Declaration states that the following areas need to be preferentially addressed:
1. Create global awareness of the impact of refractive error on sufferers,their families and community and the need for services;
2. Advocate to National Governments and world health care agencies for the policies, services and resources required to meet the needs.
3. Strive to overcome the barriers that prevent those with refractive error and low vision from obtaining the same services, rights and opportunities as others;
4. Ensure refractive error services are prioritised in planning and development of National Health Plans;
5. Invest in training of eye care workers and professionals;
6. Support the establishment of global distribution channels to make high quality spectacles available;
7. Encourage research and application of the results to achieving the most effective solutions; and
8. Work to build relationships with private sector and service providers to expand availability of sustainable services
2007
Dur
ban
Dec
lara
tio
n U
RE
The Commitment confirms that participants of the WCRE undertake to promote and support the Call for Action by addressing uncorrected refractive errors in an equitable fashion based on social justice, scientific evidence, training of personnel and effective deployment.
http://icoph.org/downloads/DurbanCommitment2010.pdf
The opening plenary session set the stage for the Congress and placed the meeting and its objectives into context: uncorrected refractive error was not just a public health issue of great social and economic significance, it was also an issue of development.
This message was reinforced by leaders from human rights’ agencies: Greenpeace International, Action Aid International, Amnesty International, African Monitor and the International Council for Adult Education.
The need for inter-sectoral co-operation for poverty alleviation, the impact of poverty on communities (water scarcity, hunger and gender) and the relevance for eye care delivery was highlighted.
2010
Dur
ban
Uncorrected Refractive Error – Facts and Figures
Uncorrected Refractive Error – Facts and Figures
1312
The interdependence of blindness and visual impairment, disability, poverty and gender are now well recognised.
Removing uncorrected refractive error as a public health problem cannot be achieved without addressing the issues of poverty and development. To do so requires a collaborative and co-operative approach within the aid industry: a deliberate effort to tackle the root cause of problems and not just treat the symptoms.
Segregation of eye health from general health is disadvantageous to raising awareness and improving prioritisation of eye health policies and strategies, which can subsequently interfere with providing adequate funding for eye health programs.
Continuing to address eye health as a separate issue will be disadvantageous to those who require it most: the majority of the global population who live in poverty. (GM Cochrane, 2010 World Congress on Refractive Error Report for IAPB Executive)
Collaboration and Co-operation
563 millionpeople globally who have URE for both or either distance and near vision and would benefit from wearing corrective lenses (spectacles or contact lenses) (Holden et al, Arch Ophthalmol. 2008;126(12):1731-1739)
410 millionpeople globally experience significant near vision impairment that reduces their ability to function effectively for near tasks (uncorrected presbyopia) and thereby affecting employment and/or independence. (Holden et al, Arch Ophthalmol. 2008; 126 (12):1731-1739)
81 millionpeople globally live with vision impairment including blindness as a result of uncorrected refractive error that affects their distance vision. (Bourne et al, Lancet Glob Health 2013; 1:e339-49)
US$202 billion each yearare the estimated costs of distance URE in terms of economic impact to society and individuals. (Smith et al, Bull World Health Org 2009; 87:431-437)
US$28 billion over 5 yearsare the estimated costs to resolve the problem for people with URE by enabling them to access appropriate services. (Fricke et al, Bull World Health Org 2012; 90:728-738)
1 Naidoo K. Poverty and blindness in Africa. Clinical and Experimental Optometry 2007;90(6):415-21.
Gilbert CE, Shah SP, Jadoon MZ, et al. Poverty and blindness in Pakistan: results from the Pakistan national
blindness and visual impairment survey. British Medical Journal 2008;336(7634):29-32. DFID. Reducing poverty
by tackling social exclusion, 1 ed. London: Department for International Development, 2005; 31.
48% of global vision impairment – URE Although there is a decrease overall in prevalence of vision impairment globally (Vision Loss Expert Group 2013:Ophthal;1-8), the proportion of vision impairment asa result of uncorrected refractive error has increased from 46% in 1990. The trend is continuing to grow with the recognition of increasing prevalence of myopia and high myopia with associated blinding conditions such as myopic macular degeneration. As such, the forecast of increased human and economic impact because of corrected and uncorrected refractive error is high.
56% - 88% of children (5-15years) with significant RE are UNCORRECTEDExamples from global studies demonstrate that in China :1 where 41% of children aged 5 to 15 years were found to have significant refractive error (causing resultant VA drop to <6/12;<20/40) and 85% of those children were UNCORRECTED. In Nepal2:2, although only 3% of the same aged children were found to have significant refractive error, nearly all were UNCORRECTED (88%); while in Chile2:3 where 15% of children aged 5-15 years had significant refractive error, 56% of those children were UNCORRECTED.
Collaboration and Co-operation
1514
- 22% change to global burden of vision impairmentDespite the heartening decrease in prevalence of vision impairment and blindness in 2010, there is still an increase in the proportion of vision impairment and blindness attributed to URE. (Stevens et al on behalf of the Vision Loss Expert Group 2013: Ophthal;1-8) Partly this can be accounted for by the increasing children age groups which can be over-represented in low resource settings, but also because of populations increasing faster than numbers of trained personnel available to provide appropriate services. The proportional increase to URE is further compounded by the global myopia epidemic.
2% world population with blinding myopia (2010)There is an increasing incidence of associated retinal degenerative conditions including myopic macular degeneration which result in significant vision loss (cause blindness). The population trends indicate that in 35 years this proportion will have risen dramatically to 10%. (Holden et al, 2015 publication in preparation)
28% world population with high myopia (2010)Furthermore, the projected figures indicate that by 2050, 52% of the world’s population will be myopic, if no interventions are applied. High myopia has been defined as ≤-5.00DS. (Holden et al, 2015 publication in preparation). There have been promising results from a number of research projects which indicate possible methods (environmental, optical, and pharmacological) that can statistically and clinically significantly reduce the progression of myopia.
2 1. Zhao J, Pan X, Sui R, Munoz SR, Sperduto RD, Ellwein LB. Refractive error study in children: results from Shunyi
District, China. American Journal of Ophthalmology. 2000;129(4):427-35.
2. Pokharel GP, Negrel AD, Munoz SR, Ellwein LB. Refractive Error Study in Children: results from Mechi Zone, Nepal.
Am J Ophthalmol. 2000;129(4):436-44
3. Maul E, Barroso S, Munoz SR, Sperduto RD, Ellwein LB. Refractive Error Study in Children: results from La Florida,
Chile. Am J Ophthalmol. 2000;129(4):445-54
Three specific objectives were outlined in the URE Strategic Plan for the six-year period 2010 to 2015:
1. Human resource development (education) 2. Service delivery (eye care) 3. Advocacy (society and leadership development)
Within each of these objectives a number of projects were funded to facilitate the desired outcomes.
Strategic Plan 2010 to 2015
Human Resource Development – through improving education tools and opportunities
The focus of this objective has been to develop tools which facilitate the education of adult learners specifically with respect to undertaking refraction skills and working within an ophthalmic team.
Four main outcomes were targeted: to increase the number of training institutions that accept the ICO benchmarked minimum standards and core curriculum for cadres in refraction; increase the number of institutions that can provide trainingand continuous professional development (CPD) for cadres in refraction; ophthalmic team training addressing URE; and, training trainers in andragogy skills for adult learners and assessments.
In addition to actively providing learning materials, advocacy roles to encourage greater recognition of the necessity to prioritise human resources and training to address URE as integrated service provision within health systems were supported.
1
Collaboration and Co-operation
1716
Strategic Plan 2010 to 2015
Service Delivery
In providing eye care services for communities most in need, the implementation of three projects in two countries have been supported by ICO. Refraction training, equipment and resultant services have been provided, as have appropriate community education to raise awareness and acceptability of new service provision. In both countries, the projects have been evaluated to assess the impact caused. Majorlearnings from the evaluation have been analysed and are detailed in the following section ‘Managing the lessons learned’. Additional service provision projects are being planned for regions with scare resources. Currently, negotiations are underway to establish a school eye health program in Ethiopia.
Equally as important as the implementation of service delivery projects is the accurate recording of relevant data for refraction services and also for URE. In the EMR, the recording of URE data within hospital management informationsystems is being explored.
In addition to direct service delivery, information management and analysis, national guidelines for comprehensive refraction services are in the process of being produced. The future potential to manage URE using refractive surgery is further being investigated by the ICO URE & SEH Task Force. Added to this discussion will be the impact of the growing myopia global ‘epidemic’ and the impact it will have on thealready high proportion of people who are unable to access refraction services.
To support eye care service delivery, end-users will benefit by being better informed and supported to know where to go to seek eye care services from eye health professionals. Improved information and communication technology (ICT) tools aswell as improved community engagement through better messaging are still to betested in two regions. However, there has been uptake by two governments (Pakistan and Uganda) and a number of INGDOs to address URE systematically within national eye health policies and programming.
Advocacy
To facilitate the promulgation of the need to address URE and SEH in a co-ordinated and focused manner, the ICO Global Task Force on URE and SEH was conceived in 2007. It is now well established with a quorum whose membership addresses the various disciplines and skillsets required to lead the implementation of the 2010-2015 strategic plan. Two focal persons, one in each of PAAO and MEACO regions have been identified while a further two are being sought to enable URE interest groups (UREIG) in each of four regions.
2
3
ICO in close collaboration with Light for the World, CBM, Brien Holden Vision Institute and Seva Foundation have provided targeted funding and support for three programs to provide improved service delivery and also to develop various models for service delivery. The information resulting from these projects have facilitated analysis and comparison of the key factors that have enabled success and highlighted the different challenges. Management of these lessons learned and appropriate application of the learned principles will enable future modelling to be more effective.
The three target programs are:
1. The National Intervention on Uncorrected Refractive Errors (NIURE) project in Uganda, funded by Light for the World and the Brien Holden Vision Institute Foundation.
Managing the lessons learned
1918
2. The Community Vision Centre (CVC) project in Pakistan, funded by CBM, Light for the World and the Seva Foundation.
3. The School Eye Health Program (SEHP) in Nigeria and Pakistan, funded by Light for the World and the International Council of Ophthalmologist (ICO) Foundation.
The focus of these three programs, which were identified within the first strategic plan for ICO URE 2008-2011, was to support and provide service delivery, education of eye care teams, community awareness and also research. Specifically, a national optical workshop has been developed in both Uganda and Pakistan, as well as a six-week long intensive refraction training course for ophthalmic clinical officers (ten courses completed till date resulting in sixty-two refractionists trained). Additionally, the NIURE project is providing professional refraction equipment to each individual qualified OCO/Refractionist and the CVC project established a logistic base. A school eye health program has been developed in both Uganda and Pakistan.
Managing the lessons learned
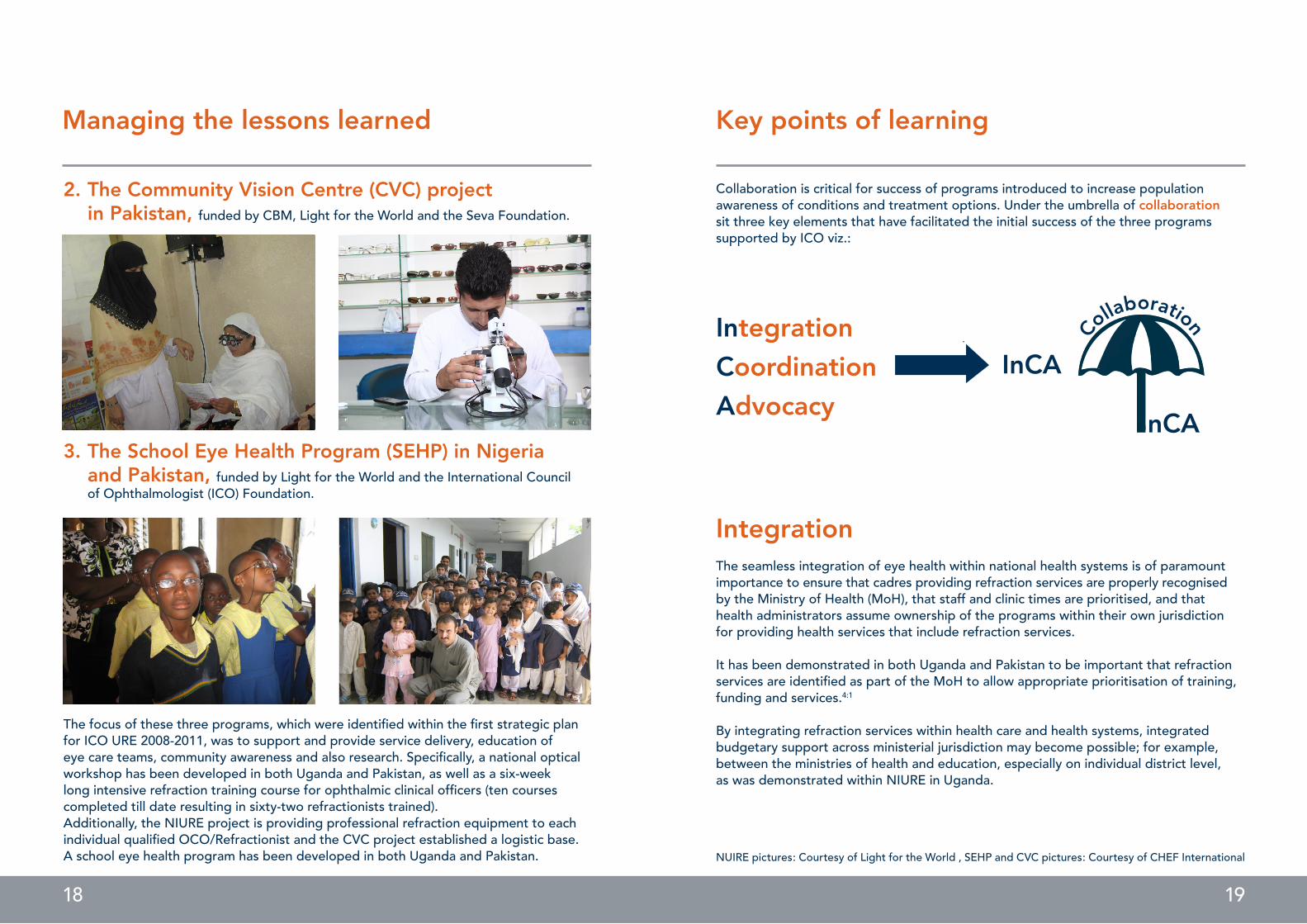
Collaboration is critical for success of programs introduced to increase population awareness of conditions and treatment options. Under the umbrella of collaboration sit three key elements that have facilitated the initial success of the three programs supported by ICO viz.:
Key points of learning
IntegrationCoordinationAdvocacy
nCA
InCA
Collaboration
IntegrationThe seamless integration of eye health within national health systems is of paramount importance to ensure that cadres providing refraction services are properly recognised by the Ministry of Health (MoH), that staff and clinic times are prioritised, and that health administrators assume ownership of the programs within their own jurisdictionfor providing health services that include refraction services.
It has been demonstrated in both Uganda and Pakistan to be important that refraction services are identified as part of the MoH to allow appropriate prioritisation of training, funding and services.4:1
By integrating refraction services within health care and health systems, integrated budgetary support across ministerial jurisdiction may become possible; for example, between the ministries of health and education, especially on individual district level, as was demonstrated within NIURE in Uganda.
NUIRE pictures: Courtesy of Light for the World , SEHP and CVC pictures: Courtesy of CHEF International
2120
Key points of learning
CoordinationWorking with the ministries of health and education has facilitated the relatively speedy uptake of school eye health programs wherein teachers are trained to identify visual loss amongst their students. Coordination and cross-ministerial cooperation has enabled the authorisation of vision corridors to be painted on school buildings; to allow teaching staff to have the necessary leave to be trained; and, to allow external refraction staff to access school premises to provide refraction services and the distribution of spectacles to students.
Coordination is key to the success of distribution of spectacles through the use ofnational courier systems such as local bus and taxi companies. Coordination is equally important for the dissemination of appropriate community messaging used to improve community knowledge and awareness of health and related eye conditions and theirmanagement. Furthermore, coordination and cooperation between the private and public sectors have facilitated increased access to refraction services for patients.4:1 However, the three current programs have demonstrated that it is beneficial to improve coordination between service providers and other organisations such asthose for people with disability (DPOs), the elderly, gender-specific groups and impairment-specific groups. 4:1
Lastly, coordination is vital to ensure that advocacy strategies are being implemented most effectively.
AdvocacyAdvocacy by the ICO URE & SEH Task Force has been undertaken at district, national and supranational level.
At the district level, programs jointly supported by ICO, LIGHT FOR THE WORLD and other partner INGDOs have advocated the importance of addressing URE as it relates to school attendance, outcomes and employment opportunities as well as eye health and associated systemic health conditions: for example, cataract, diabetes, glaucoma, trachoma and trauma. Improved community messages that raise awareness of conditions and their management and treatment options benefit individuals and facilitate health practitioners in their ability to improve access and timely intervention, improving outcomes for individuals. Ultimately, by improving awareness of therelationship between general health, lifestyle choices and eye health improves individual understanding of eye conditions and may allow increased personal choice to control individual circumstances.
Key points of learning
At the national level, continuing advocacy for comprehensive eye care service delivery that include refraction and spectacle services have resulted in the inclusion of eye care and refraction services within national health care systems (in Uganda and Pakistan), thus increasing the integral sustainability of such service provision. Moreover, theprovision of clinically viable spectacles through district administration at no cost for children is emphasised at piloted districts, as well as frames and lenses, especially for children, to be highlighted within the appliance policy of the MoH of Uganda becoming a ministerial priority for the line ministries (MoH/MoE) also aiming for tax exemption.In low resource settings, innovative approaches to improve the accessibility of primary eye care are paramount for the change in community expectation and to increase the demand from simply that of refraction to increasing the standards to those expected of optometric provision of primary eye care in high resource settings. National level advocacy has seen the development of a new school of optometry at the University of Makerere in Uganda; the first intake of optometry students occurred in September 2014.
Additionally, the uptake by ministries of education to include eye health as a part of teacher training further enables sustainability of school vision screening. If all teachers are routinely trained in vision screening within their teacher education, the loss of vision screening services within schools when designated vision screening teachers re-locate is prevented.4
The ICO URE & SEH Task Force has increased the profile of URE as a cause of avoida-ble blindness within supranational organisations and detailed the benefits of targeting refraction, its provision and training of cadres as well as embracing that refraction cadres be included within the ophthalmic team. All but one regional supranational organisation have formed URE interest groups (UREIGs).
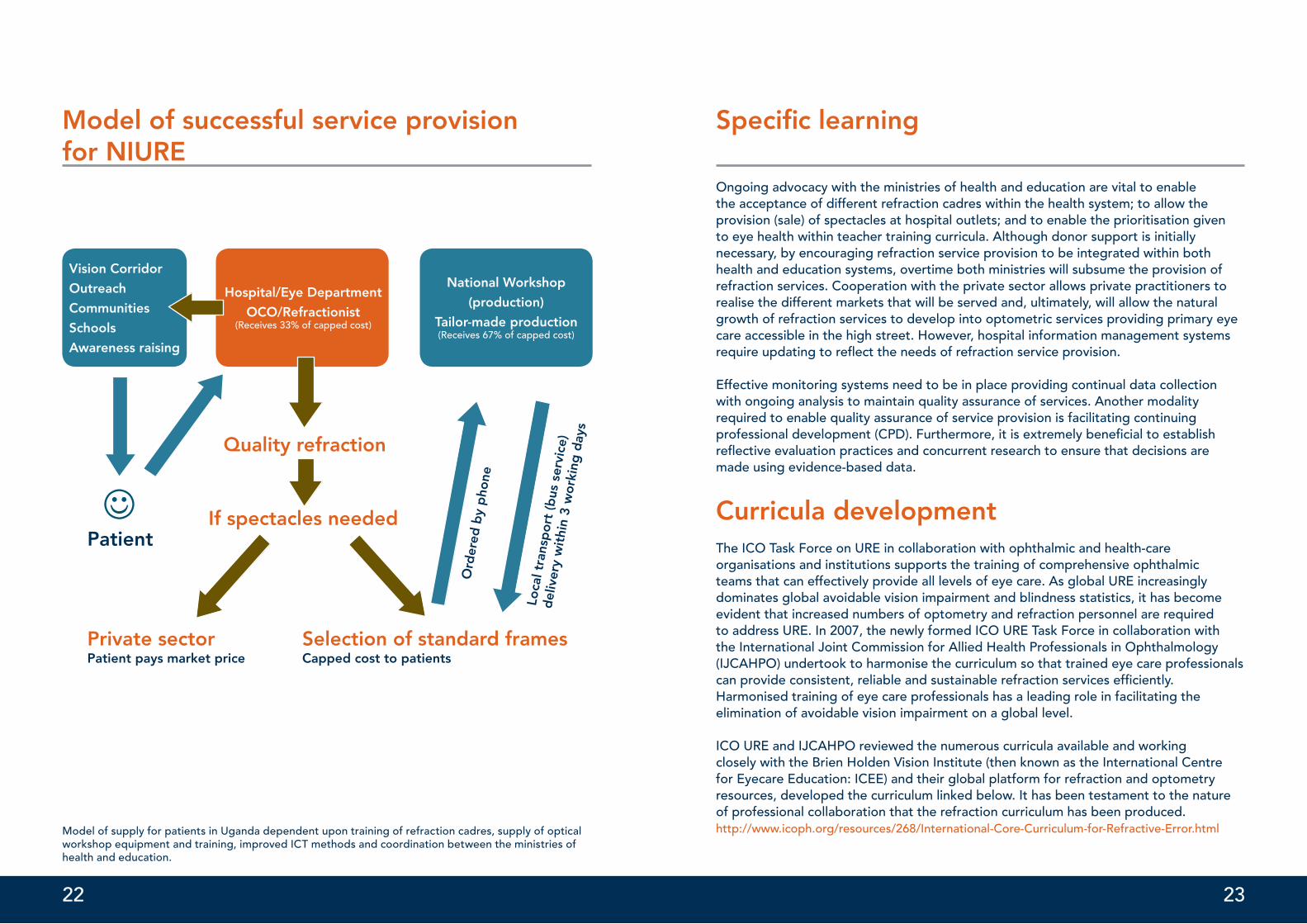
Specific learningWith respect to the program that has been implemented in Uganda, the national intervention on uncorrected refractive errors (NIURE), a model for refractive services and spectacle supply has been identified that links to the training of refractionists and raising community knowledge and awareness. Two activities were key to the refraction service provision: 1. the establishment of a national optical workshop to glaze prescription spectacles, as was identifying a safe, efficient and reliable distribution service using the national bus service network5 and, 2. the establishment of short intensive refraction training courses. A simplified model of successful service provision for NIURE follows:
4 Light for the World. Jan 2014. Impact Evaluation: Finding and Lessons Learned for Universal access to refraction services within the national health system in Uganda.
2322
Model of successful service provisionfor NIURE
Model of supply for patients in Uganda dependent upon training of refraction cadres, supply of optical workshop equipment and training, improved ICT methods and coordination between the ministries of health and education.
Vision Corridor
Outreach
Communities
Schools
Awareness raising
Hospital/Eye Department
OCO/Refractionist(Receives 33% of capped cost)
National Workshop
(production)
Tailor-made production(Receives 67% of capped cost)
Quality refraction
If spectacles needed
Ord
ered
by
pho
ne
Loca
l tra
nsp
ort
(bus
ser
vice
)d
eliv
ery
wit
hin
3 w
ork
ing
day
s
Patient
Private sectorPatient pays market price
Selection of standard framesCapped cost to patients
Ongoing advocacy with the ministries of health and education are vital to enablethe acceptance of different refraction cadres within the health system; to allow theprovision (sale) of spectacles at hospital outlets; and to enable the prioritisation givento eye health within teacher training curricula. Although donor support is initiallynecessary, by encouraging refraction service provision to be integrated within both health and education systems, overtime both ministries will subsume the provision of refraction services. Cooperation with the private sector allows private practitioners to realise the different markets that will be served and, ultimately, will allow the natural growth of refraction services to develop into optometric services providing primary eye care accessible in the high street. However, hospital information management systemsrequire updating to refl ect the needs of refraction service provision.
Effective monitoring systems need to be in place providing continual data collection with ongoing analysis to maintain quality assurance of services. Another modalityrequired to enable quality assurance of service provision is facilitating continuingprofessional development (CPD). Furthermore, it is extremely benefi cial to establishrefl ective evaluation practices and concurrent research to ensure that decisions are made using evidence-based data.
Curricula developmentThe ICO Task Force on URE in collaboration with ophthalmic and health-careorganisations and institutions supports the training of comprehensive ophthalmicteams that can effectively provide all levels of eye care. As global URE increasinglydominates global avoidable vision impairment and blindness statistics, it has become evident that increased numbers of optometry and refraction personnel are requiredto address URE. In 2007, the newly formed ICO URE Task Force in collaboration withthe International Joint Commission for Allied Health Professionals in Ophthalmology(IJCAHPO) undertook to harmonise the curriculum so that trained eye care professionals can provide consistent, reliable and sustainable refraction services effi ciently.Harmonised training of eye care professionals has a leading role in facilitating theelimination of avoidable vision impairment on a global level.
ICO URE and IJCAHPO reviewed the numerous curricula available and workingclosely with the Brien Holden Vision Institute (then known as the International Centrefor Eyecare Education: ICEE) and their global platform for refraction and optometryresources, developed the curriculum linked below. It has been testament to the nature of professional collaboration that the refraction curriculum has been produced. http://www.icoph.org/resources/268/International-Core-Curriculum-for-Refractive-Error.html
Specifi c learning
2524
Curricula development
The core curriculum employs a system that can be used internationally by educators and eye care professionals in academic institutions or for on-the-job training of staff. It is designed to be compatible with local practice and regulations, and to be consistent with ‘best practices’ in eye care and patient care internationally. The curriculum provides learners with content domains and appropriate performance objectives to provide the knowledge, skills, and interpersonal behaviours required to perform their eye care tasks to a satisfactory professional standard. It is in modular format for maximum customisation, focused on three core competencies: patient care; community and health services, and; medical and refraction knowledge. The teaching sequence of the modules can be changed or additional categories added. However, it is not intended that content should be deleted from the training; only the focus or time spent on a topic may be altered. Therefore, the duration for the refraction course varies dependent upon local needs, although it is unlikely that it can be adequately taught in less than six weeks. Furthermore, the curriculum is designed to teach refraction and not intended to be considered as a substitute for the skills required for optometry.
Two key actions will need to occur for the successful implementation of training skilled eye care personnel to appropriate professional standards globally: 1, the adoption by training institutions of the minimum expected professional standards incorporated within the Core Curriculum and 2, training of trainers for allied health personnel is required.
The International Core Curriculum on Refractive Errors was published in 2011 and is also available on the ICO webpage. It has been translated into Portuguese, Spanish and also into French for sub-Saharan Africa. In addition to the curriculum for refraction skills, a curriculum for the training of allied health personnel was previously developed in 2009.http://icoph.org/resources/31/International-Core-Curriculum-For-Ophthalmic-Assistants.html
Supranational influence Tireless advocacy by the lead members of the ICO URE & SEH Task Force to sensitise supranational ophthalmic-orientated organisations to the importance and impact of URE and SEH globally have been successful: all but one regional organisation have acknowledged the growing demand of URE and SEH on their regional capacity. Furthermore, ICO URE & SEH advocacy has influenced strategic interventions at national levels using ICO Task Force initiatives.
The encouraging establishment of URE Interest Groups within supranational organisations has seen a growing dialogue within and between ophthalmic professional organisations. Consequently, the profile of URE and SEH has risen such that there is a growing demand to address URE and SEH from international and national NGDOs and other not-for-profit organisations.
Resources and References
Online linkshttp://www.icoph.org/resources/7/Durban-Declaration-on-Refractive-Error-and-Service-Development-.html
http://icoph.org/downloads/DurbanCommitment2010.pdf
http://www.icoph.org/resources/268/International-Core-Curriculum-for-Refractive-Error.html
http://icoph.org/resources/31/International-Core-Curriculum-For-Ophthalmic-Assistants.html
ReferencesLight for the World. Impact Evaluation: Finding and Lessons Learned for Universal access to refraction services within the national health system in Uganda. Jan 2014.
Bourne et al, Lancet Glob Health 2013; 1:e339-49
Cochrane GM, World Congress on Refractive Error Report for IAPB Executive. 2010 DFID. Reducing poverty by tackling social exclusion, 1 ed. London: Department for International Development, 2005; 31.
Fricke et al, Bull World Health Org 2012;90:728-738
Gilbert CE, Shah SP, Jadoon MZ, et al. Poverty and blindness in Pakistan:results from the Pakistan national blindness and visual impairment survey. British Medical Journal 2008;336(7634):29-32.
Holden et al, Arch Ophthalmol. 2008;126(12):1731-1739
Holden et al, 2015 publication in preparation
ICO Task Force on URE & SEH Report. Sept 2014
Maul E, Barroso S, Munoz SR, Sperduto RD, Ellwein LB. Refractive Error Studyin Children: results from La Florida, Chile. Am J Ophthalmol. 2000;129(4):445-54
Naidoo K. Poverty and blindness in Africa. Clinical and Experimental Optometry2007;90(6):415-21.
Pokharel GP, Negrel AD, Munoz SR, Ellwein LB. Refractive Error Study in Children:results from Mechi Zone, Nepal. Am J Ophthalmol. 2000; 129(4):436-44
Smith et al, Bull World Health Org 2009; 87:431-437
Stevens et al on behalf of the Vision Loss Expert Group 2013:Ophthal ;1-8
Vision Loss Expert Group Ophthal;1-8 2013
Zhao J, Pan X, Sui R, Munoz SR, Sperduto RD, Ellwein LB. Refractive error studyin children: results from Shunyi District, China. American Journal of Ophthalmology. 2000; 129(4):427-35.
Stra
teg
ic p
lan
and
act
ivit
ies
of t
he IC
O T
ask
Forc
e on
UR
E &
SEH
Ove
rall
Ob
ject
ive:
All
peo
ple
wit
h U
nco
rrec
ted
Ref
ract
ive
Err
ors
hav
e ac
cess
to
hig
hest
-qua
lity
serv
ices
, in
line
wit
h th
e M
issi
on
of IC
O.
A n
etw
ork
of o
pht
halm
olo
gis
ts t
akin
g
initi
ativ
e in
imp
lem
entin
g t
he S
trat
egic
Pl
an o
n na
tiona
l and
reg
iona
l lev
el is
es
tab
lishe
d (U
RE
IG)
4 U
nco
rrec
ted
Ref
ract
ive
Err
ors
In
tere
st G
roup
s (U
RE
IGs)
are
form
ed o
n a
sup
rana
tiona
l lev
el. F
oca
l per
sons
for
2 R
egio
ns M
EA
CO
(Pro
f. E
l Fek
ih) &
PA
AO
(D
r. C
ont
rera
s)
Enc
our
age
iden
tified
foca
l per
sons
to
fo
rm U
RE
IGs;
iden
tify
activ
e fo
cal p
erso
ns
in n
ot
yet
cove
red
reg
ions
;
Dev
elo
p T
ask
Forc
e St
rate
gic
Pla
n up
to
20
20
3 g
ove
rnm
ents
and
3 N
GD
Os
have
tak
en
up U
nco
rrec
ted
Ref
ract
ive
Err
ors
in t
heir
po
licie
s an
d p
rog
ram
min
g o
n (e
ye) h
ealth
Pa
kist
an, U
gan
da,
Al M
agra
bi i
n E
gyp
t,
LFTW
& o
ther
s
The
lear
ning
fro
m p
ilot
pro
ject
s is
sys
tem
a-tiz
ed, d
ocu
men
ted
and
mad
e av
aila
ble
for
the
ben
efit
of o
ther
and
new
initi
ativ
es t
o
add
ress
Unc
orr
ecte
d R
efra
ctiv
e E
rro
rs.
Go
vern
men
ts in
clud
e ca
dre
s ne
eded
for
refr
activ
e se
rvic
es in
the
ir na
tiona
l hea
lth
wo
rkfo
rce
pla
nnin
g a
nd c
aree
r st
ruct
ure.
An
incr
ease
d n
umb
er o
f tra
inin
g in
stitu
tions
an
d g
ove
rnm
ents
acc
ept
the
ICO
b
ench
mar
ked
Min
imum
Sta
ndar
ds
/ C
ore
C
urric
ulum
for
cad
res
in re
frac
tion.
Sust
aina
bili
ty G
uid
elin
es fo
r tr
aini
ng, C
ME
, an
d re
tain
ing
of c
adre
s in
refr
actio
n ar
e av
aila
ble
.
The
num
ber
of i
nstit
utio
ns t
akin
g u
p
trai
ning
and
co
ntin
uous
med
ical
ed
ucat
ion
(CM
E) o
f cad
res
in re
frac
tion
is s
cale
d u
p.
4 ne
w in
stitu
tions
are
est
ablis
hed
Ban
gla
des
h w
as in
the
focu
s b
ut n
o
fund
ing
has
bee
n se
cure
d
No
pro
activ
e ac
tion
pro
po
sed
Ad
diti
ona
l inf
o t
o b
e o
bta
ined
fro
m
JCA
HPO
1 in
stitu
tion
in e
ach
of t
he 6
reg
ions
ad
op
ts t
he C
ore
Cur
ricul
umE
gyp
t In
stitu
te o
f co
mm
unity
O
pht
halm
olo
gy
(EIC
O)
No
pro
activ
e ac
tion
pro
po
sed
Ad
diti
ona
l inf
o t
o b
e o
bta
ined
fro
m
JCA
HPO
Mas
ter
trai
ners
are
tra
ined
on
new
And
-ra
go
gy
skill
s fo
r le
arni
ng a
nd a
sses
smen
t m
etho
do
log
ies
10 m
aste
r tr
aine
rs in
eac
h o
f the
6
reg
ions
are
tra
ined
Is
lam
abad
& C
airo
car
ried
out
1 tr
aini
ng t
o b
e o
ffere
d t
o C
OE
CSA
No
furt
her
actio
n
Sust
aina
bili
ty G
uid
elin
es a
re p
rod
uced
Incl
ude
resp
ectiv
e el
emen
ts in
to
Nat
iona
l Gui
del
ines
(see
bel
ow
);an
d t
ake
up in
op
erat
iona
l res
earc
h
pro
gre
ss w
ork
in U
gan
da
A k
now
led
ge
man
agem
ent
reso
urce
is
emb
edd
ed in
the
ICO
web
pag
eN
IUR
E le
arni
ng g
uid
e d
one
201
4
Gui
del
ines
/ k
now
led
ge
man
agem
ent
reso
urce
fina
lized
3 ke
y ar
eas
for
epid
emio
log
ical
rese
arch
are
p
riorit
ized
No
t ye
t o
bta
ined
New
ICT
too
ls a
re d
evel
op
ed a
nd
field
-tes
ted
in t
wo
reg
ions
Co
ntin
ue t
o p
ursu
e w
ith g
ove
rnm
ents
and
N
GD
Os
Follo
w P
EE
K t
rials
; dev
elo
p a
co
ncep
t fo
r an
“in
spira
tiona
l” v
iral fi
lm (e
ither
/and
ta
rget
ing
inte
rnat
iona
l co
mm
uniti
es o
r at
p
eop
le’s
leve
l – re
gio
nal a
pp
roac
h)
The
ICO
Tas
k Fo
rce
on
Unc
orr
ecte
d
Ref
ract
ive
Err
ors
co
vers
all
com
pet
enci
es
need
ed t
o t
ake
the
lead
in im
ple
men
ting
th
e St
rate
gic
pla
n.
The
po
tent
ial r
ole
of r
efra
ctiv
e su
rger
ies
(LA
SIK
, etc
.) in
tre
atin
g U
nco
rrec
ted
R
efra
ctiv
e E
rro
rs w
ithin
the
nex
t 10
-15
year
s is
refle
cted
.
A d
iscu
ssio
n p
roce
ss h
as s
tart
ed w
ithin
the
IC
O T
ask
Forc
e
Pres
enta
tion
dur
ing
SO
E/G
äckl
e
Dis
cuss
ion
pro
cess
fina
lized
on
the
role
of
LASI
K in
ad
dre
ssin
g U
RE
for
po
or
peo
ple
Nat
iona
l Gui
del
ines
for
com
pre
hens
ive
refr
activ
e se
rvic
es a
re a
vaila
ble
.
Dat
a o
n U
nco
rrec
ted
Ref
ract
ive
Err
ors
are
in
clud
ed in
the
hea
lth s
yste
m re
po
rtin
g.
In 2
co
untr
ies
mo
del
s fo
r re
po
rtin
g a
re
exp
lore
dFo
llow
up
with
in E
MR
Ug
and
a to
incl
ude
esse
ntia
ls in
HM
IS
Nat
iona
l Gui
del
ines
are
pro
duc
edW
ill b
e fin
aliz
ed
Info
rmat
ion
and
Co
mm
unic
atio
n Te
chno
log
y to
ols
are
use
d t
o c
reat
e p
ublic
aw
aren
ess
and
ad
dre
ss ig
nora
nce
on
Unc
orr
ecte
d R
efra
ctiv
e E
rro
rs (e
.g. s
ms
mes
sag
ing
, vira
l film
s, in
tera
ctiv
e p
rese
ntat
ions
, sm
artp
hone
ap
ps,
etc
.)
Kno
wle
dg
e g
aps
on
pre
vale
nce
and
in
cid
ence
of U
nco
rrec
ted
Ref
ract
ive
Err
ors
are
ad
dre
ssed
by
Ep
idem
iolo
gic
al
Res
earc
h, t
o e
nhan
ce u
nder
stan
din
g a
nd
assi
st p
rog
ram
me
pla
nnin
g o
n p
rovi
ncia
l an
d n
atio
nal l
evel
.
The
effe
ctiv
enes
s o
f the
on-
go
ing
pilo
t p
rog
ram
mes
on
com
mun
ity le
vel i
s kn
own
and
anal
ysed
- b
y co
nduc
ting
op
erat
iona
l re
sear
ch a
nd im
pac
t ass
essm
ents
- to
info
rm
furt
her d
evel
opm
ent o
f the
se p
rog
ram
mes
as
wel
l as
to id
entif
y le
arni
ng a
reas
.
Team
trai
ning
s on
ad
dre
ssin
g u
ncor
rect
ed
refr
activ
e er
rors
, inc
lud
ing
Op
htha
lmol
o-g
ists
, Op
tom
etris
ts, R
efra
ctio
nist
s an
d o
ther
al
lied
hea
lth p
erso
nnel
, are
sca
led
up
.
4 in
stitu
tions
pra
ctic
e te
am tr
aini
ngPI
CO
, Pak
ista
n In
stitu
te o
f Reh
abili
tatio
n Sc
ienc
es, E
gyp
t Ins
titut
e O
f Com
mun
ity
Op
htha
lmol
ogy,
Col
leg
e of
Op
htha
lmol
ogy
and
Alli
ed V
isio
n Sc
ienc
es
Hum
an R
esou
rces
to d
etec
t and
m
anag
e U
ncor
rect
ed R
efra
ctiv
e Er
rors
ar
e an
intr
insi
c p
art o
f hea
lth s
yste
ms.
Wel
l tra
ined
Hum
an R
esou
rces
ar
e av
aila
ble
to d
etec
t and
man
age
Unc
orre
cted
Ref
ract
ive
Erro
rs.
Syst
emat
ized
info
rmat
ion
on
effe
ctiv
e st
rate
gie
s to
ad
dre
ss
Unc
orre
cted
Ref
ract
ive
Erro
rs is
av
aila
ble
for i
nter
este
d s
take
hold
ers.
(1) I
mp
act A
sses
smen
ts in
pilo
t pro
ject
s ha
ve
bee
n un
der
take
n
CVC
& S
EHP
Nig
eria
201
2
NIU
RE 2
013
/ w
ay fo
rwar
d 2
014
(2) 4
are
as
for o
per
atio
nal r
esea
rch
are
iden
tified
3 g
over
nmen
ts in
clud
e ca
dre
s in
refr
actio
n in
to th
eir h
ealth
wor
kfor
ce p
olic
yPa
kist
an a
chie
ved
U
gan
da
form
alis
atio
n in
pro
gre
ss
pub
lish
scho
ol e
ye h
ealth
dat
a (L
AIC
O);
take
up
op
erat
iona
l res
earc
h on
sus
tain
able
p
rovi
sion
of r
efra
ctiv
e se
rvic
es to
poo
r p
eop
le (L
ions
fund
ing
?)
New
inte
rven
tion
stra
teg
ies
on
prim
ary/
com
mun
ity le
vel i
n ad
diti
on
to C
om
mun
ity
Vis
ion
Cen
ters
and
Sch
oo
l Eye
Hea
lth P
ro-
gra
mm
es a
re p
ilote
d fo
r sc
arce
ly re
sour
ced
re
gio
ns (e
.g. S
out
h Su
dan
), to
ad
dre
ss
Unc
orr
ecte
d R
efra
ctiv
e E
rro
rs a
s an
ent
ry
po
int
to c
om
pre
hens
ive
prim
ary
eye
care
in
the
fram
e o
f nat
iona
l hea
lth s
trat
egie
s.
1 ad
diti
ona
l pilo
t p
roje
ct is
est
ablis
hed
SEH
pro
gra
mm
e in
Eth
iop
ia h
as b
een
earm
arke
d, d
iscu
ssio
ns a
re u
nder
way
but
ha
ven’
t b
een
able
to
sec
ure
fund
ing
till
d
ate
SEH
P p
ilot
initi
ativ
e in
Eth
iop
ia h
as s
tart
ed,
pro
vid
ed a
po
sitiv
e fe
asib
ility
che
ck;
Star
t a
pilo
t o
n U
RE
in N
ort
hern
Mo
zam
-b
ique
on
pro
vinc
ial l
evel
(Cab
o D
elg
ado
) to
cre
ate
lear
ning
on
po
ssib
le a
pp
roac
hes
in s
carc
ely
reso
urce
d s
ettin
gs;
Und
erta
ke a
qua
litat
ive
anal
ysis
on
bar
riers
to
sp
ecta
cle
upta
ke, d
isag
gre
gat
ed b
y g
end
er, a
ge
and
dis
abili
ty;
NG
DO
s an
d o
ther
rele
vant
sta
keho
lder
s ad
dre
ss s
yste
mat
ical
ly U
nco
rrec
ted
R
efra
ctiv
e E
rro
rs in
the
ir p
olic
ies
and
p
rog
ram
min
g o
n (e
ye) h
ealth
.
With
in IC
O w
ell-f
unct
ioni
ng s
truc
ture
s ar
e in
pla
ce t
o d
rive
the
Stra
teg
ic P
lan
on
add
ress
ing
Unc
orr
ecte
d R
efra
ctiv
e E
rro
rs.
The
pub
lic h
as b
ette
r ac
cess
to
re
frac
tive
serv
ices
by
incr
easi
ng
resp
ectiv
e p
rog
ram
mes
and
usi
ng
mo
der
n IC
T
The
ICO
Tas
k Fo
rce
on
Unc
orr
ecte
d R
e-fr
activ
e E
rro
rs is
wel
l est
ablis
hed
Stra
teg
ic w
ork
pla
n fo
r 20
15/1
6
SOC
IETY
AN
D L
EA
DER
SHIP
DE
VEL
OPM
ENT
EYE
CA
RE D
ELIV
ERY
Educ
atio
n
Spec
ific
Obj
ectiv
esRe
sults
Targ
et 2
015
Wor
kpla
n 20
15/2
016
28
ICO Headquarters:711 Van Ness Ave.San Francisco, California 94102United States of AmericaFax: +1 415 521 1649Phone: +1 415 521 1651Email: [email protected]
www.icoph.orgbuilding a world alliance for sight