Embed Size (px)
Citation preview

The diabetic foot: Non-operative care & daily foot care
Dr.Rajiv Shah‘Foot & Ankle Orthopaedics’Foot & Ankle SurgeonPresident, Indian Foot & Ankle Society
Why talk about diabetic foot?
40 million diabetics in India = 80 million feet
What about Mauritius?? India is declared ‘world diabetes capital’!!
‘The load of diabetes is going to get doubled in 2020 & we will need to train family physicians & paramedics to deal with epidemic of diabetes’ -WHO
Why talk about diabetic foot?
20% of diabetics have problem in their foot & ankle
Diabetic patient loses the sensibility of foot & ankle resulting in a condition called ‘Diabetic Neuropathy’
Foot ulcerations are the most common cause of hospital admissions for Diabetics
Why talk about diabetic foot?
Ulcers are expensive to treat, may lead to amputation and need for chronic institutionalized care
Amputation risk increased 8 X Ulcer precedes amputation in 85% of
cases After amputation 30% lose other limb
in 3 years! After amputation 2/3rds die in five
years
Why talk about diabetic foot?
We in developing countries have a high amputation rate among the diabetics : 18% to 20%
Very few truly dedicated diabetic foot care centers
Medical and Para-medical population is not aware about care of diabetic foot
Aim of diabetic foot care
Prevention of foot ulcersPrevention of foot ulcersPrevention of foot ulcersPrevention of foot ulcersPrevention of foot ulcersPrevention of foot ulcers
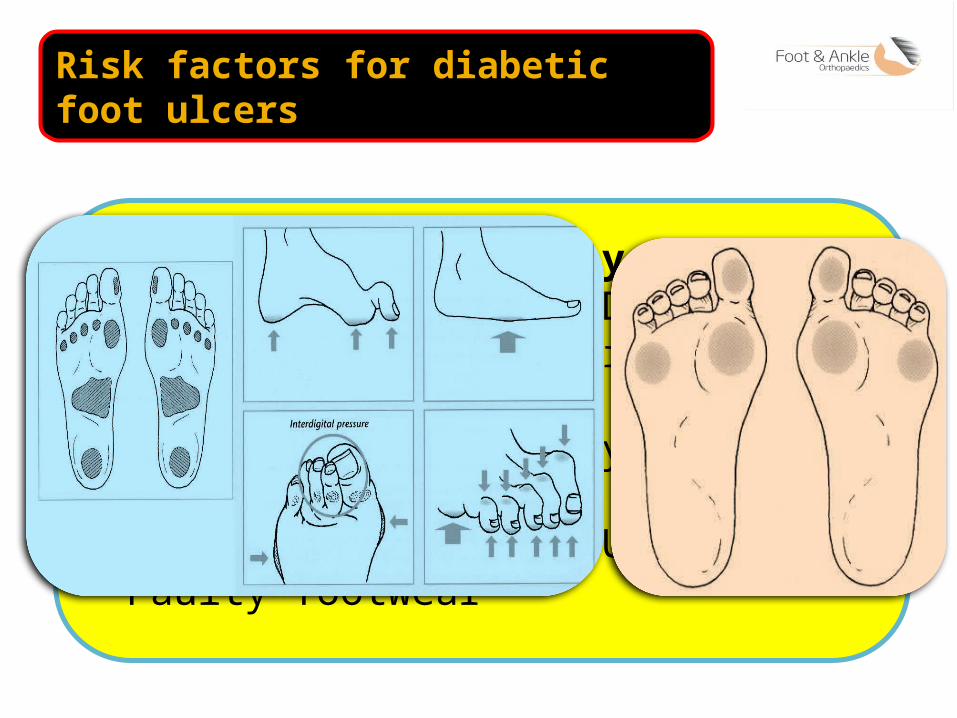
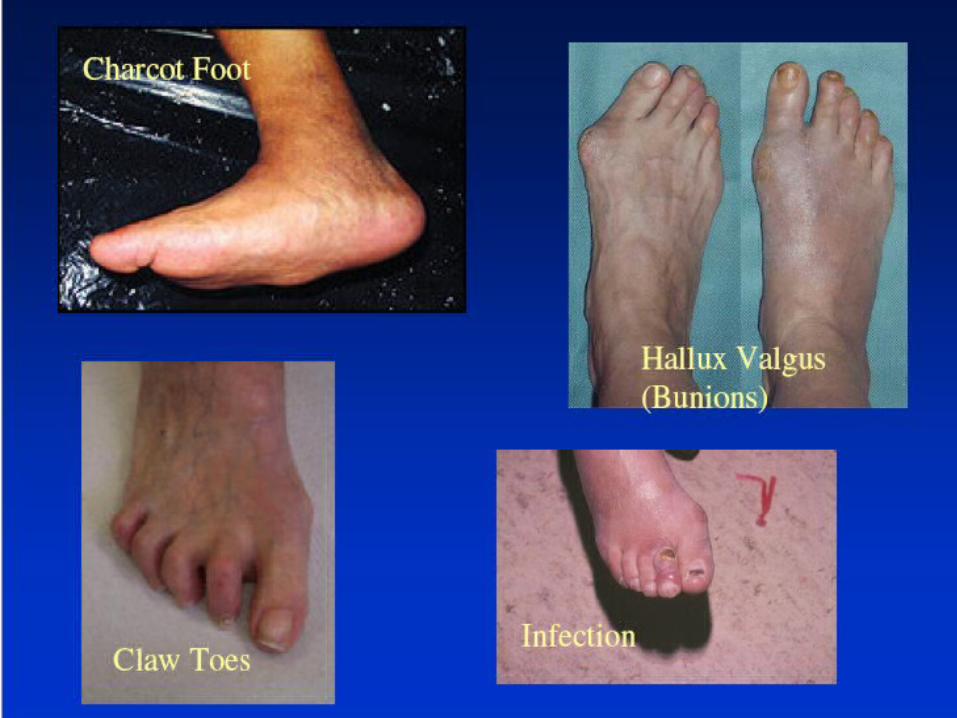
Risk factors for diabetic foot ulcers
Peripheral Neuropathy Peripheral Vascular Disease Deformities like bunion,
hammertoe, claw toe, mallet toe Prior Lower Extremity Amputation Prior Diabetic Foot Ulcer Faulty footwear
9
10
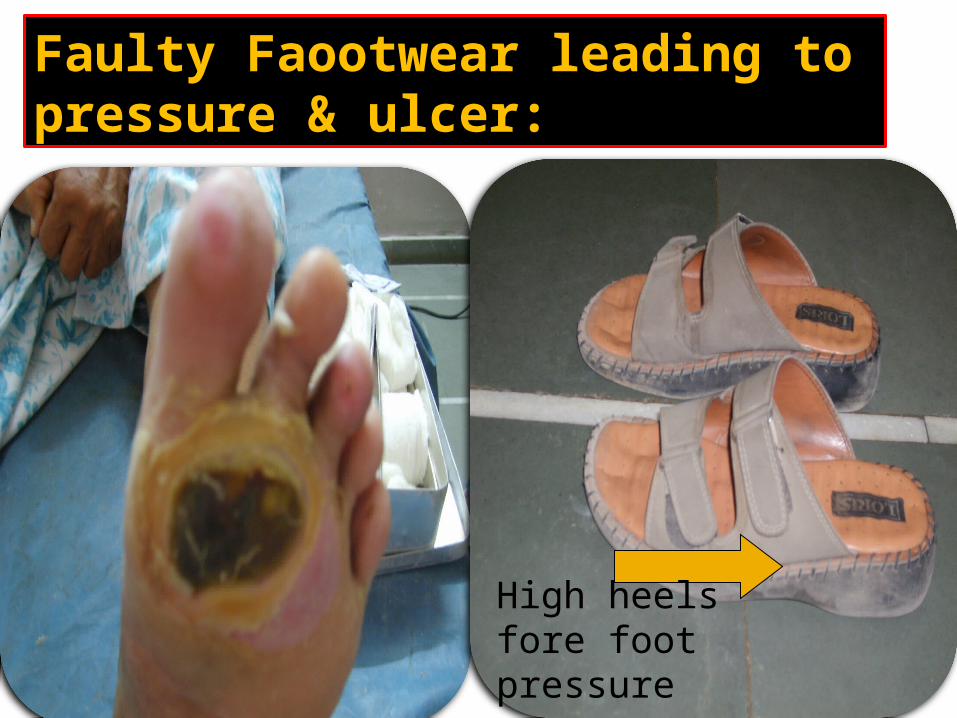
Faulty Faootwear leading to pressure & ulcer:
High heels fore foot pressure
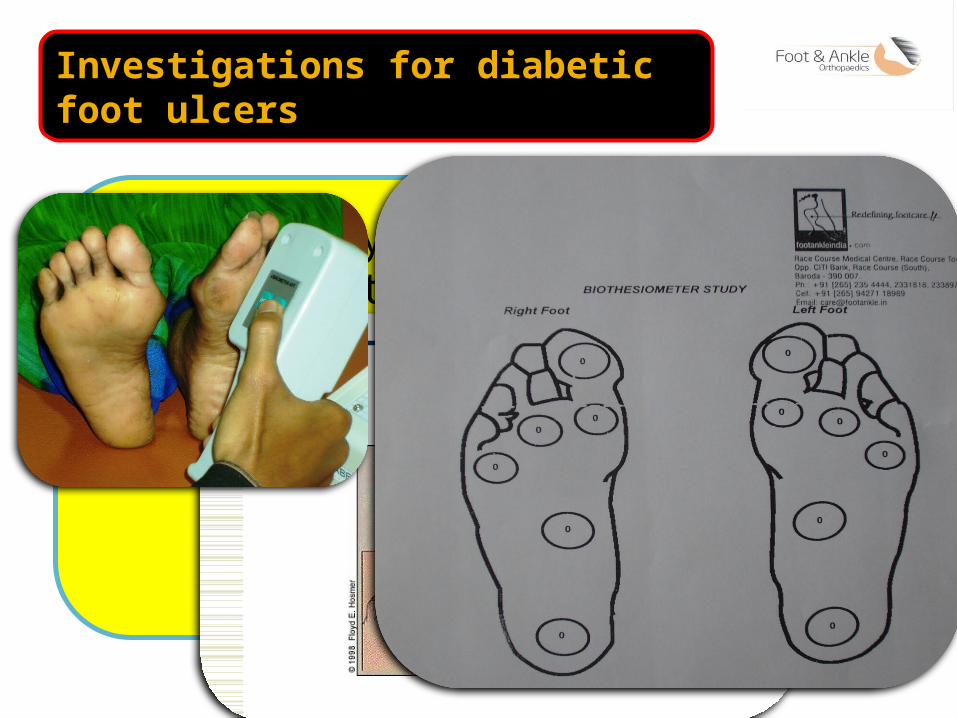
Investigations for diabetic foot ulcers
Neuropathy Assessment by 5.07 monofilament Biothesiometer
Testing Sites
Vascular Doppler
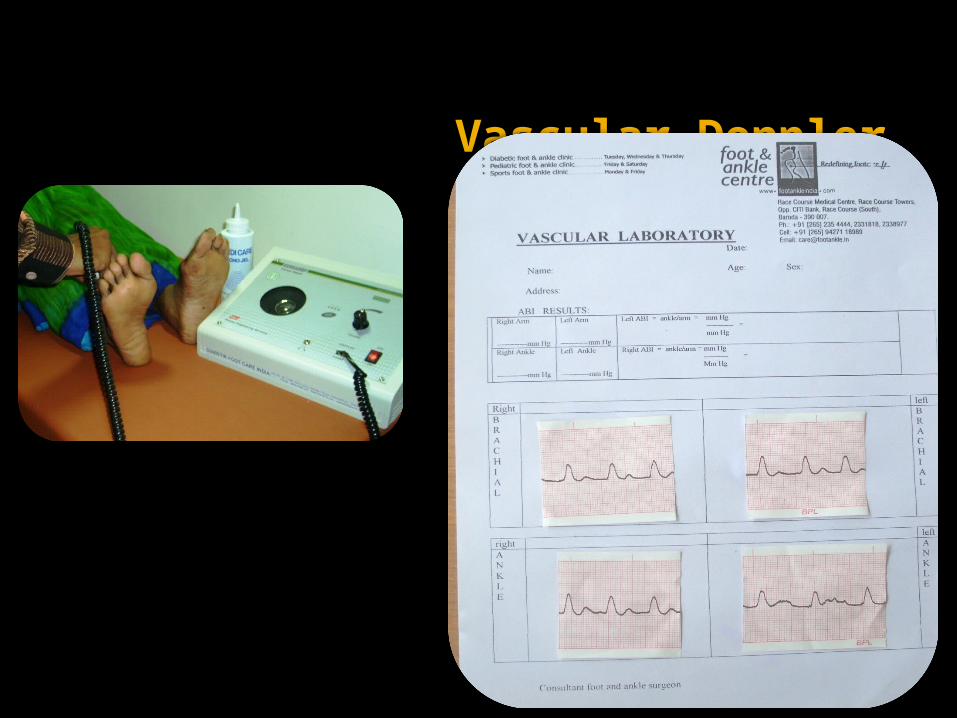
Vascular Doppler
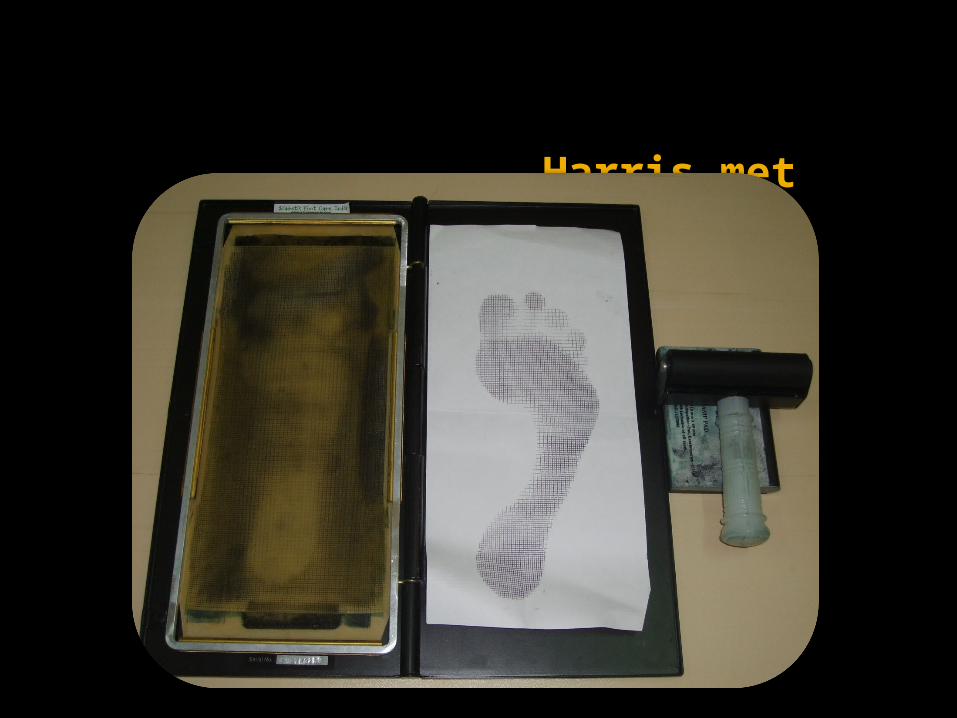
Harris met
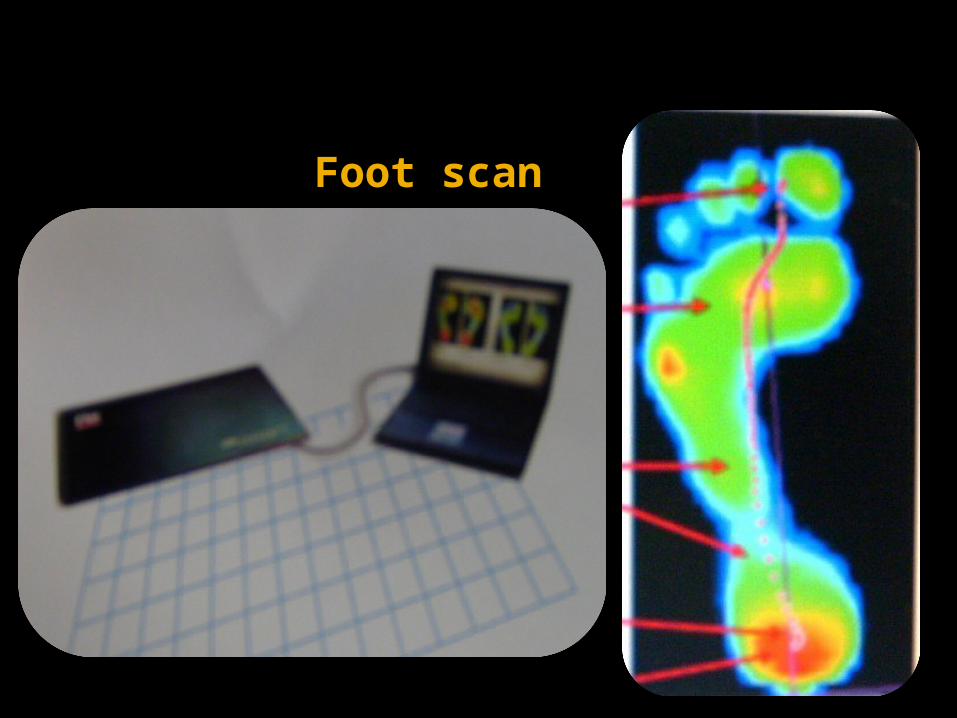
Foot scan
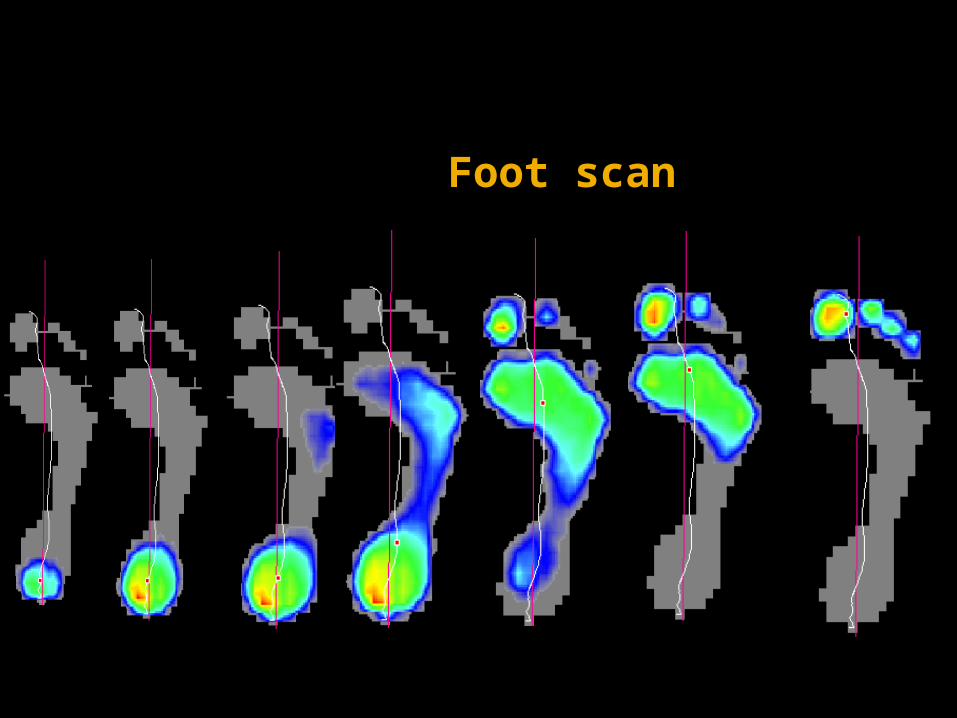
Foot scan
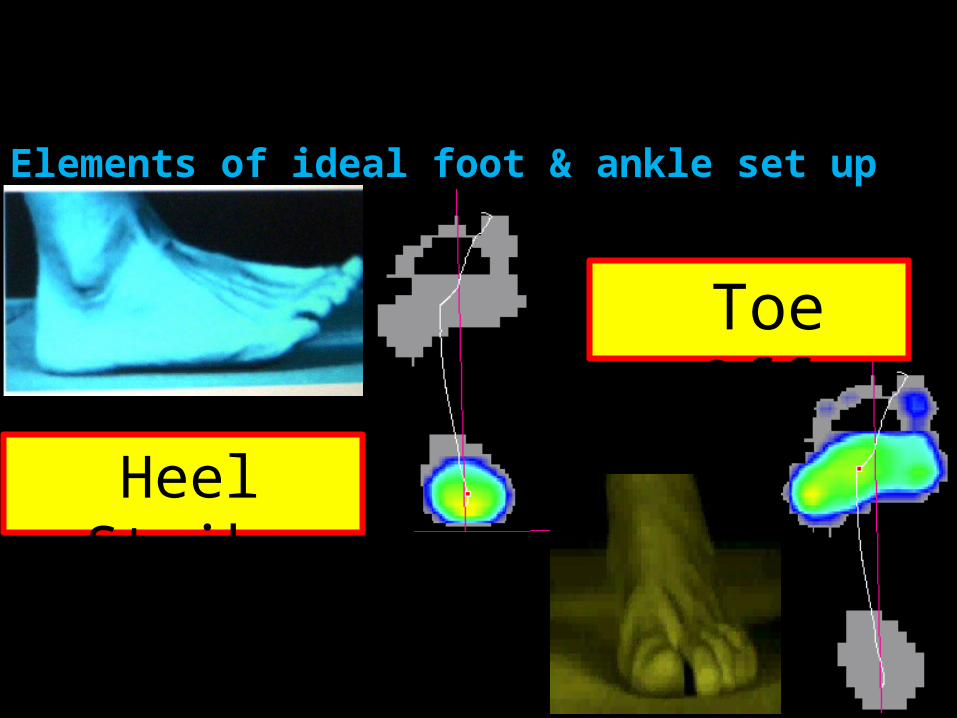
Elements of ideal foot & ankle set upFoot lab –Foot scan
Heel Strike
Toe Off
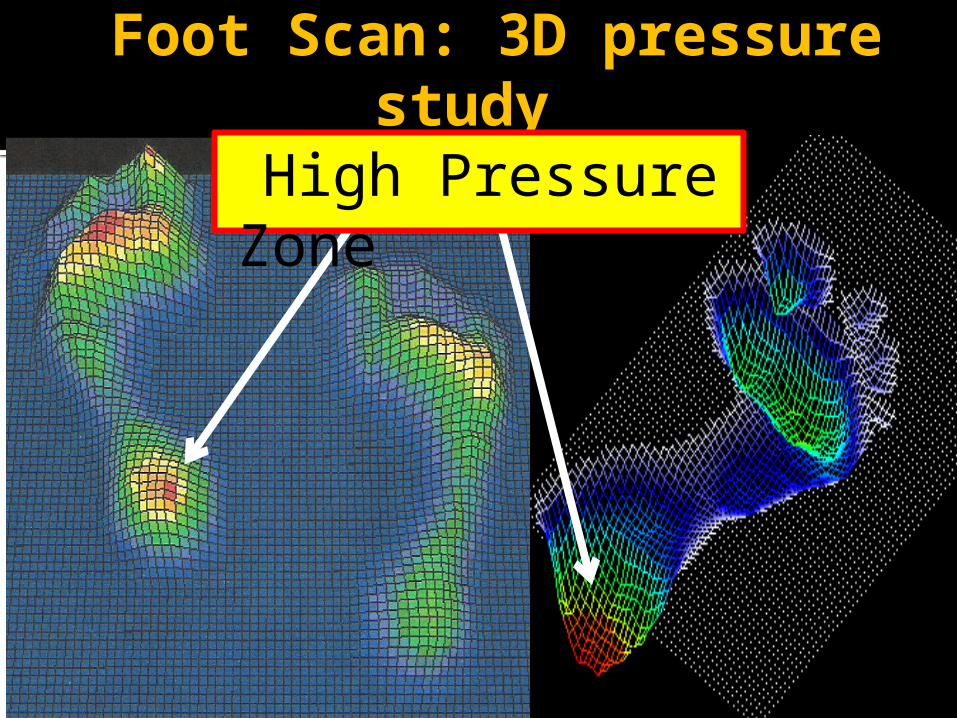
Foot Scan: 3D pressure study
High Pressure Zone
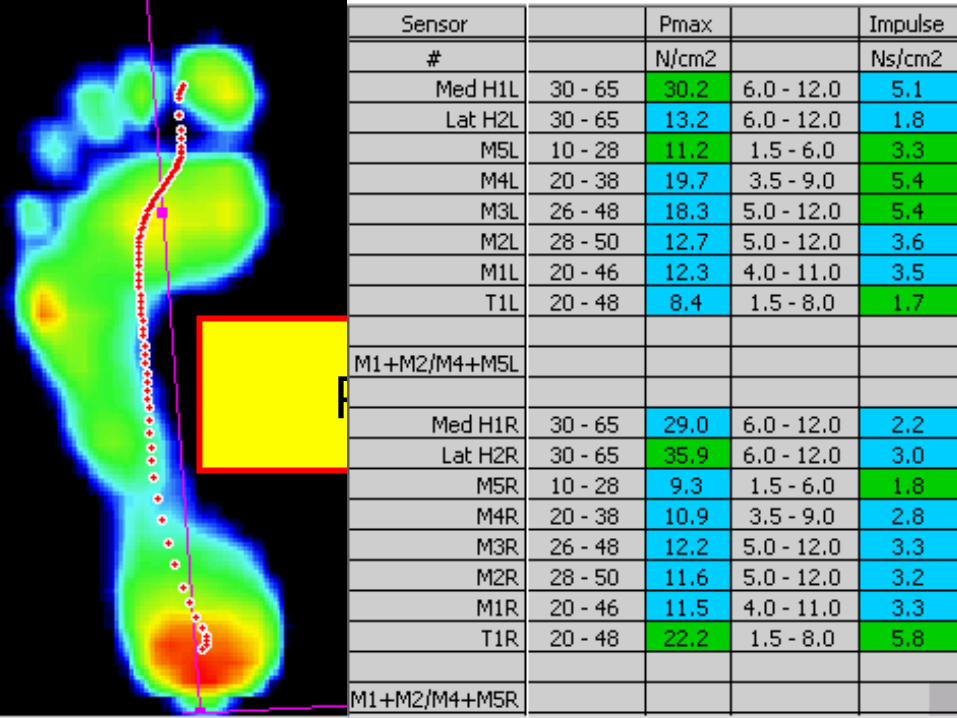
Foot Scan Pressure points analysis
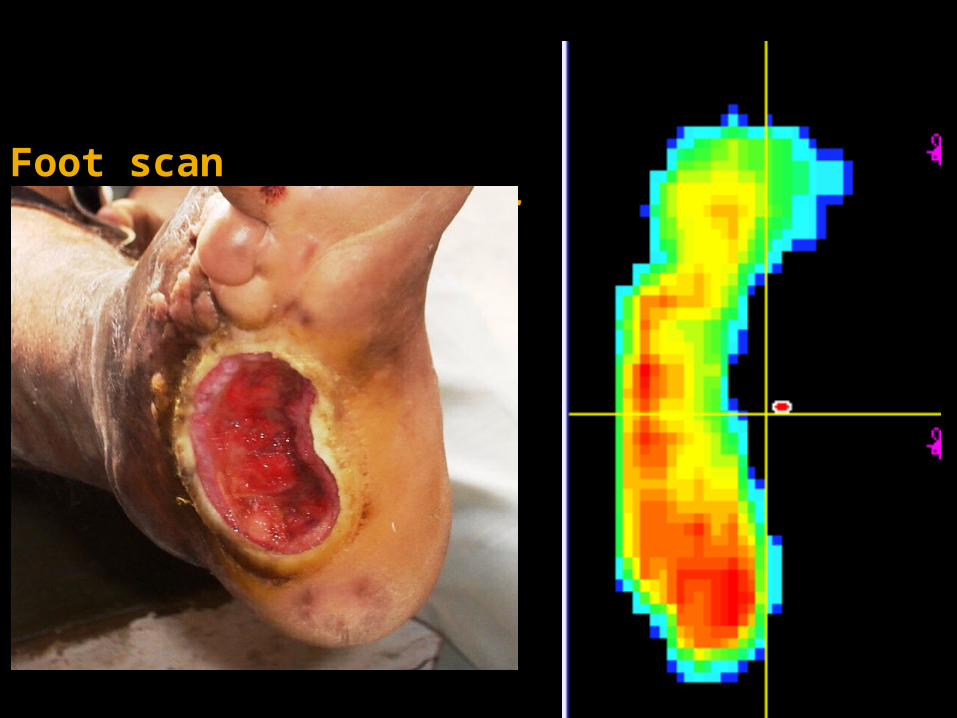
Foot scan14 yrs.non-healing ulcer
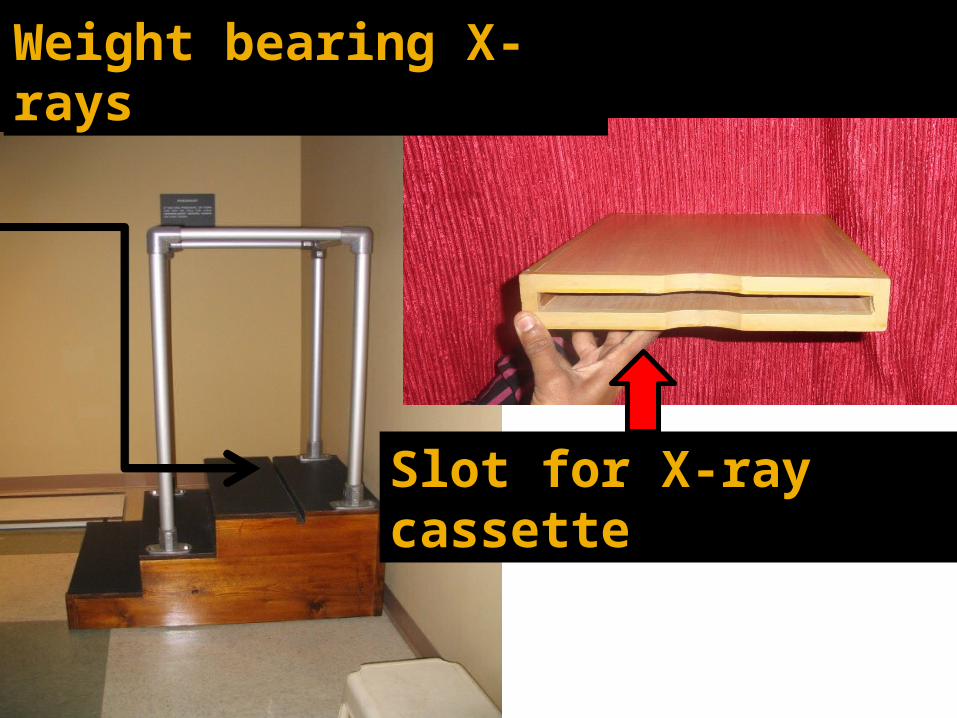
Slot for X-ray cassette
Weight bearing X-rays
Diabetic foot: conservative care
Footwear alteration Orthotics Total contact cast Skin & nail care Medical management Patient education
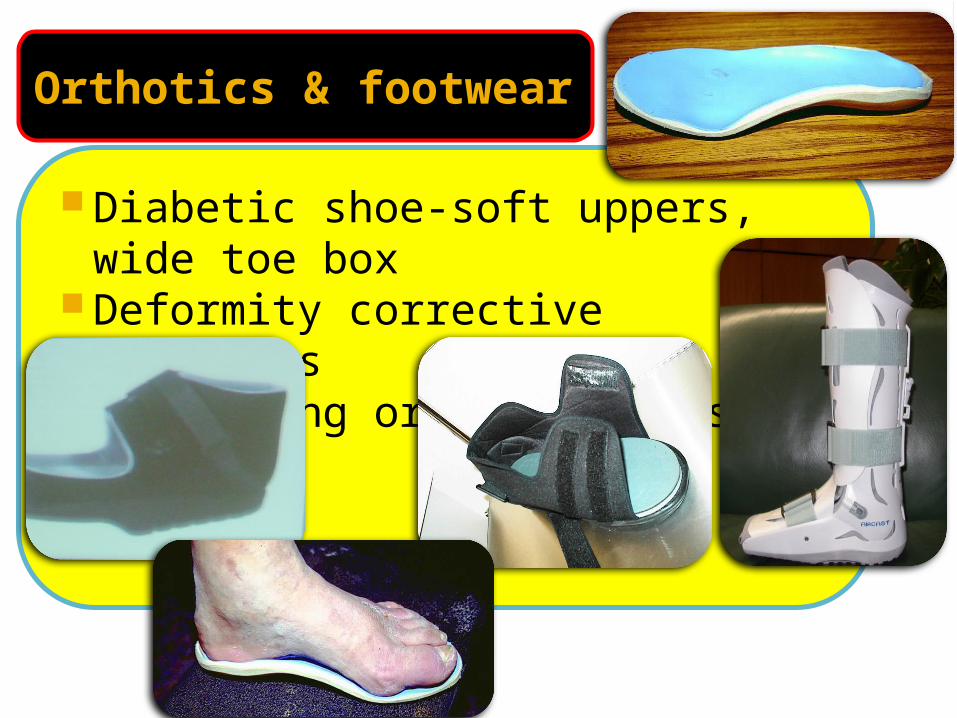
Orthotics & footwear
Diabetic shoe-soft uppers, wide toe box
Deformity corrective orthotics Offloading orthotics or shoe

25
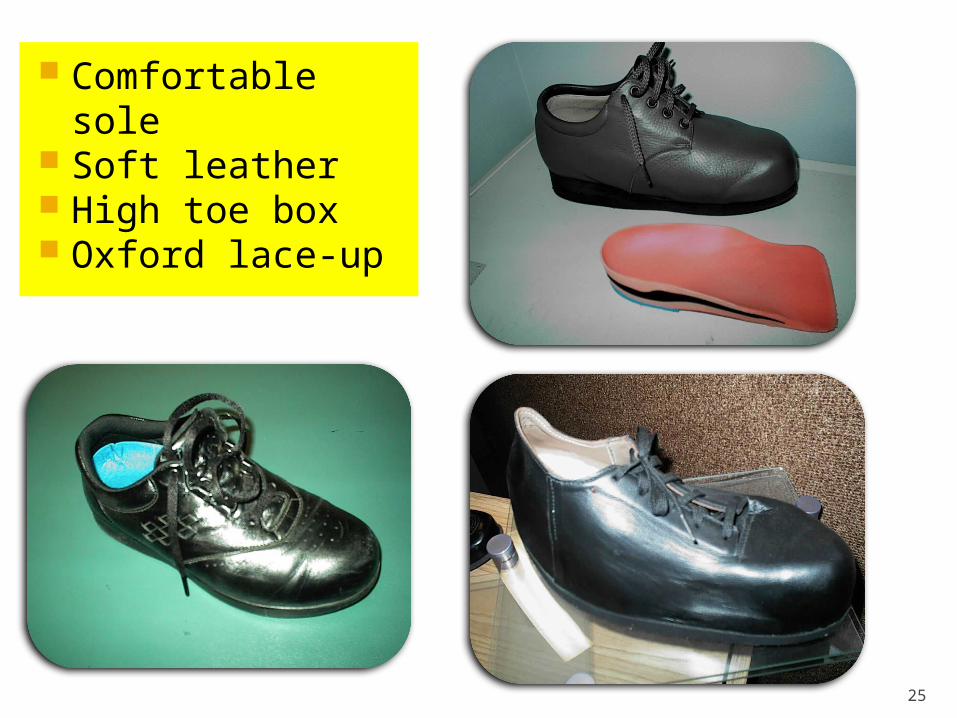
Comfortable sole Soft leather High toe box Oxford lace-up
Total Contact Cast
‘Gold standard’‘Not the material but principles matter’
I follow 6 Mantras
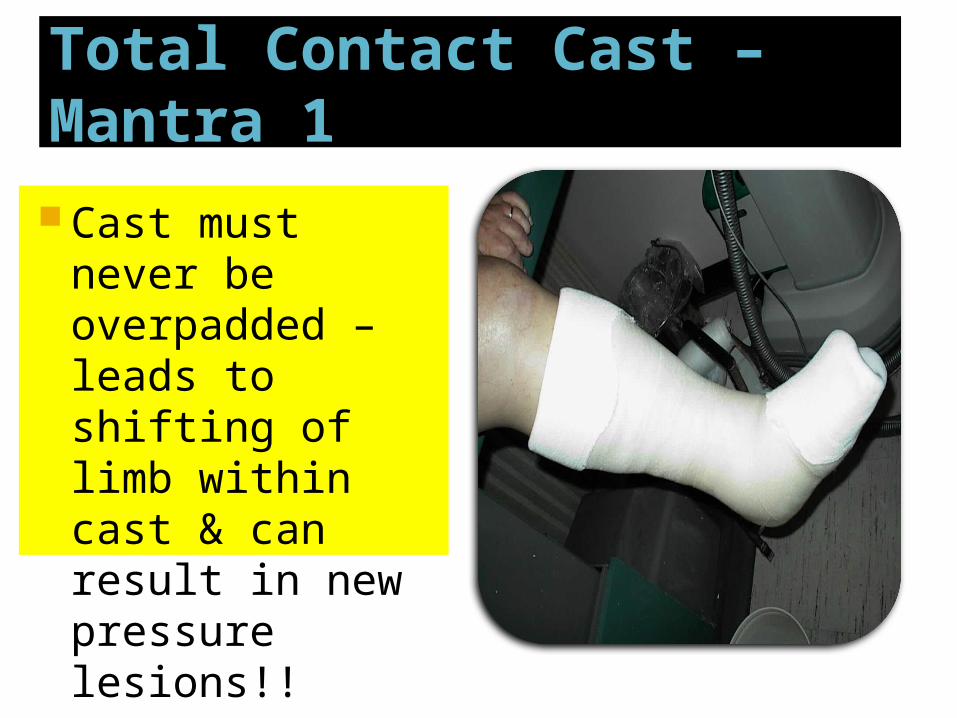
Total Contact Cast – Mantra 1
Cast must never be overpadded – leads to shifting of limb within cast & can result in new pressure lesions!!
Total Contact Cast – Mantra 2
Cast must limit toe movements & prevent hyperextension of MTP joints
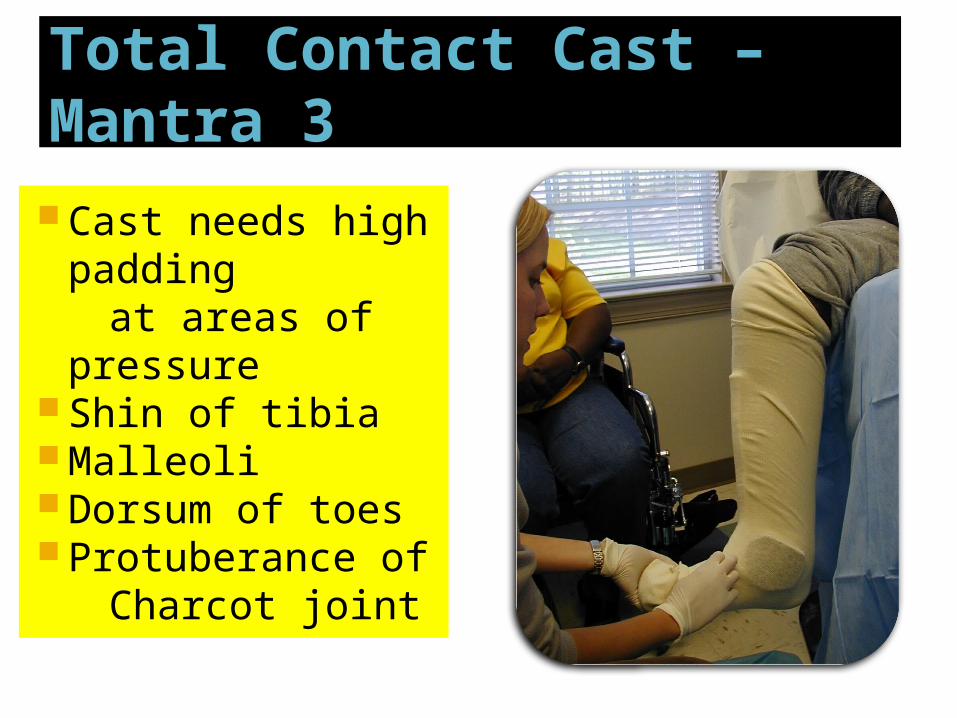
Total Contact Cast – Mantra 3 Cast needs high
padding at areas of
pressure Shin of tibia Malleoli Dorsum of toes Protuberance of Charcot joint
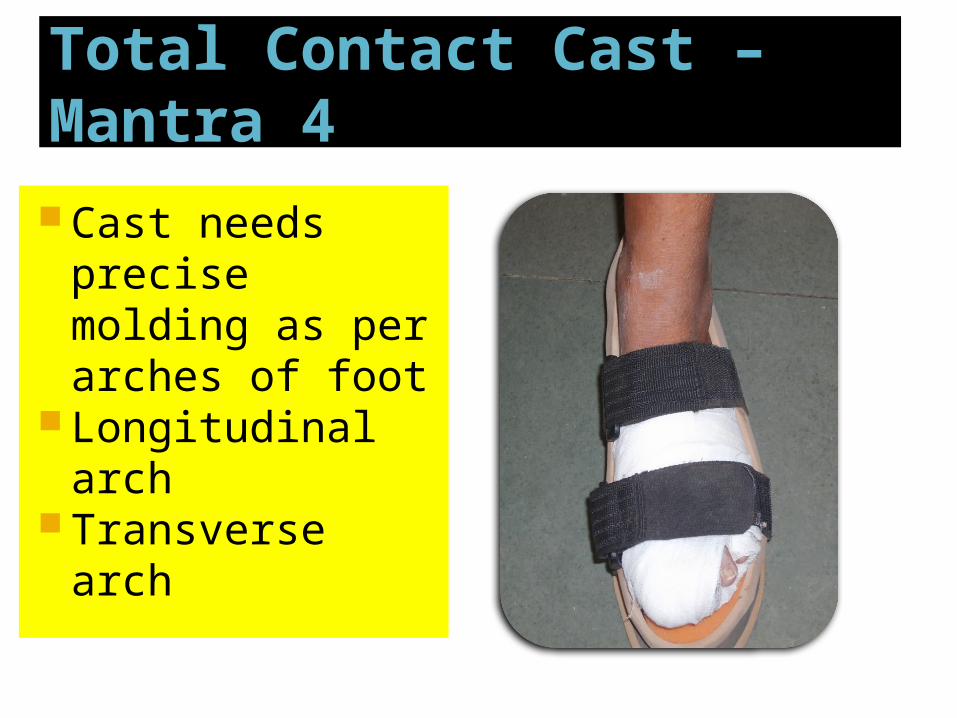
Total Contact Cast – Mantra 4
Cast needs precise molding as per arches of foot
Longitudinal arch
Transverse arch
Total Contact Cast – Mantra 5
First cast needs to be changed within 5 to 7 days
Loose cast is more dangerous then no cast!!
Subsequent cast may be at the interval of 2 to 4 weeks

Total Contact Cast – Mantra 6
If the cast is not helping the healing Check & recheck Stiffen the plantar walking
surface Wooden platform Sole of a sleeper You might have to resort to surgical
offloading or shifting of loads

Foot ulcer of long duration

Typical foot ulcer of long duration

Foot ulcer

36
Treatment: Nail Care
Trim transversely Rounded corners
can lead to infected ingrown toenails
Treatment: Skin Care
Diabetic foot: Prevention is better than cure!
Common foot care advices given to diabetic patients

Daily examination of foot with magnifying mirror
Strict control of blood sugar
Serial periodic examination by expert for diagnosis of ‘foot at risk’
Wash foot daily & clean with dry & smooth cloth
Clean the web spaces between toes
Take bath first with hands then with foot
Wear footwear first in hands then in feet!
Do not immerse feet for longer time in water
Apply oily substance to foot after bath
Do not apply oil in between toes
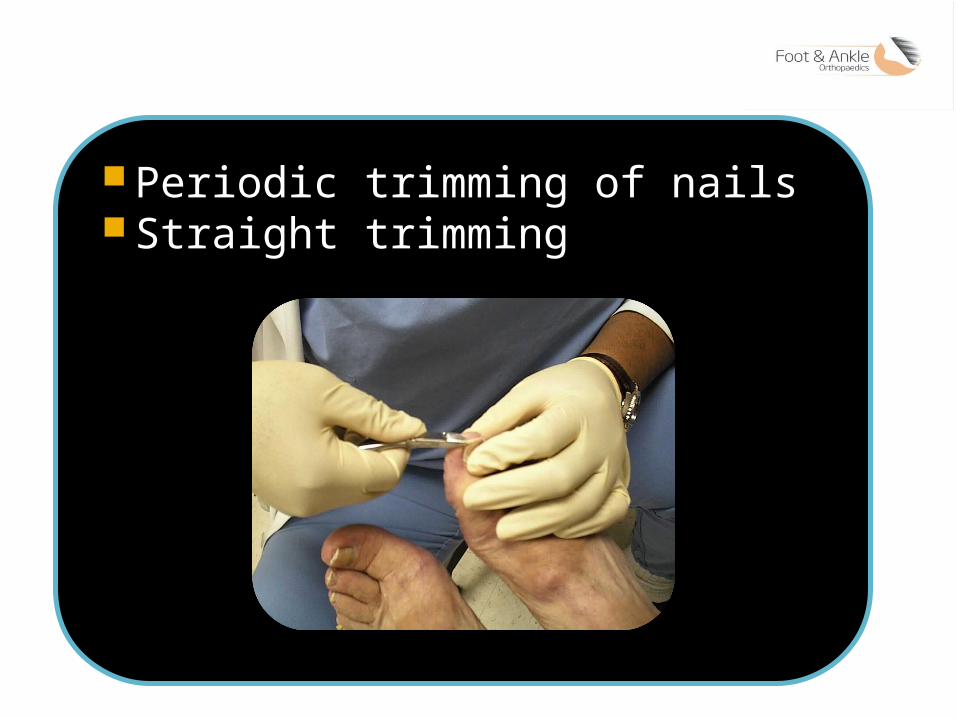
Periodic trimming of nails Straight trimming
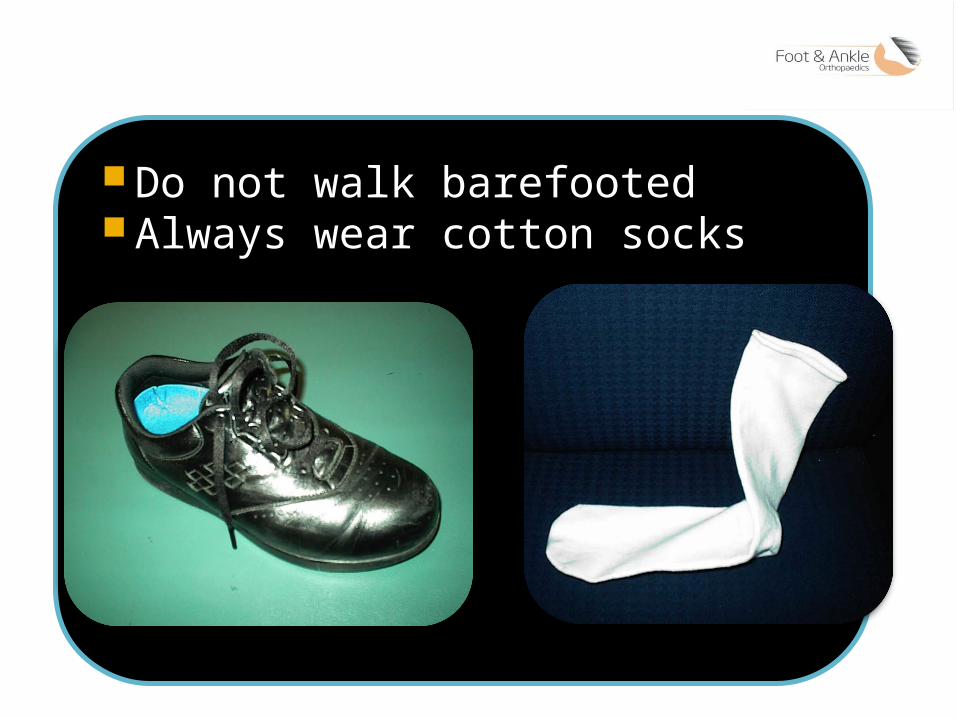
Do not walk barefooted Always wear cotton socks

Always report to doctor for warning signs like swelling, discoloration or discharge

Education is the need of the day !
Foot School
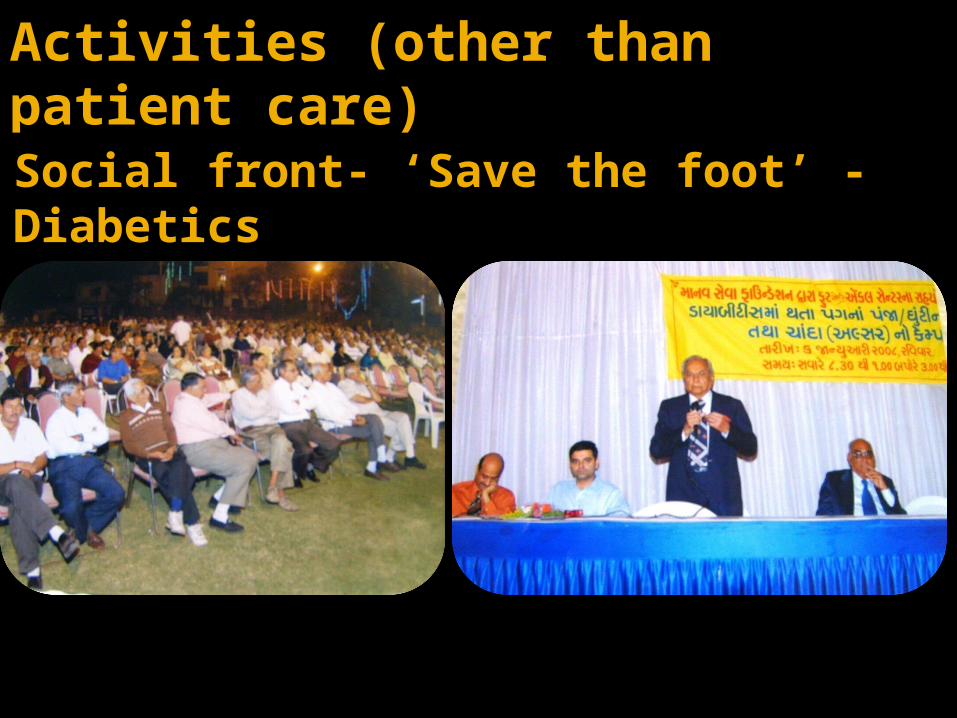
Activities (other than patient care)Social front- ‘Save the foot’ -Diabetics
That’s all…Thank you all..