Embed Size (px)
Citation preview
Hallux Rigidus
Selene G. Parekh, MD, MBAAssociate Professor of Surgery
Partner, North Carolina Orthopaedic ClinicDepartment of Orthopaedic Surgery
Adjunct Faculty Fuqua Business SchoolDuke University
Durham, NC919.471.9622
http://seleneparekhmd.comTwitter: @seleneparekhmd
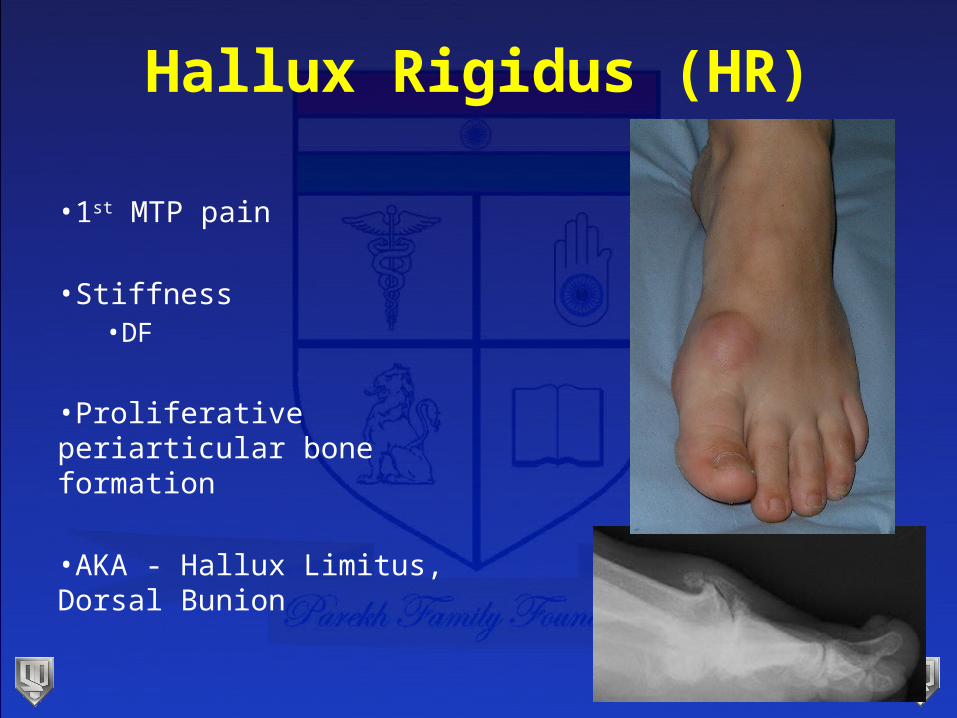
Hallux Rigidus (HR)
•1st MTP pain
•Stiffness•DF
•Proliferative periarticular bone formation
•AKA - Hallux Limitus, Dorsal Bunion
Epidemiology
• One in 40 over age 50 (Gould N, 1980)
• Occurs bilaterally approximately 50% of the time
• Females probably greater than males
• Early onset associated with positive family history
Boney & MacNab, 1952
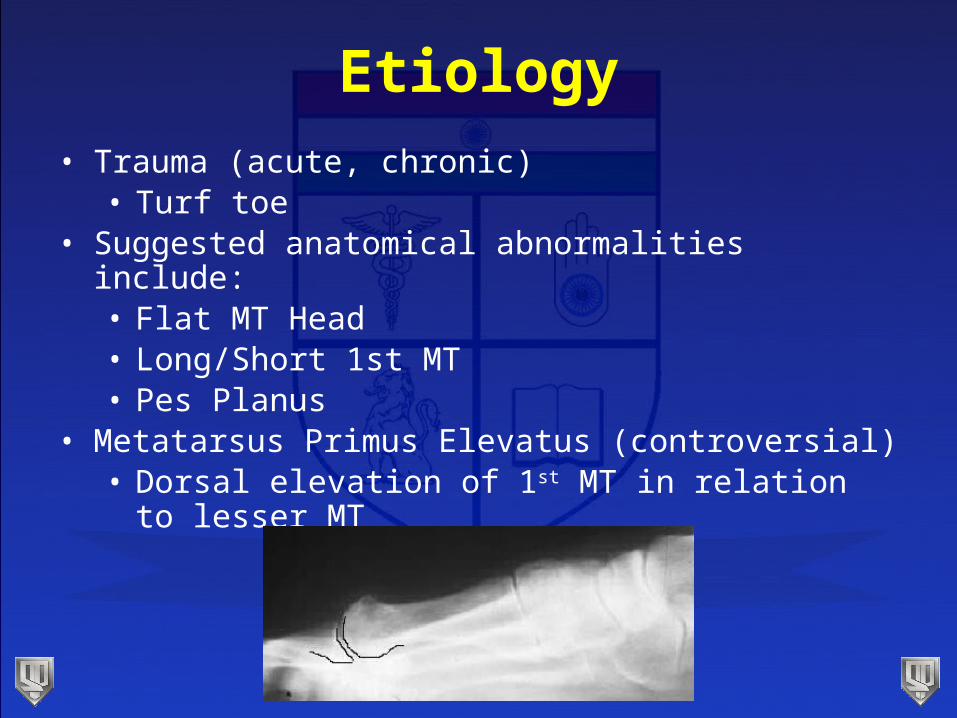
Etiology• Trauma (acute, chronic)
• Turf toe• Suggested anatomical abnormalities include:
• Flat MT Head• Long/Short 1st MT• Pes Planus
• Metatarsus Primus Elevatus (controversial)• Dorsal elevation of 1st MT in relation to lesser MT
Evaluation•History
•Pain & swelling
•Physical Exam•Decreased ROM (DF, classically)•Painful ROM
•DF- bony impingement•PF- stretch of EHL, capsule, synovium
•Bony osteophyte •Dorsal •Dorsolateral- Tinel’s sign (1st WS; DPN)
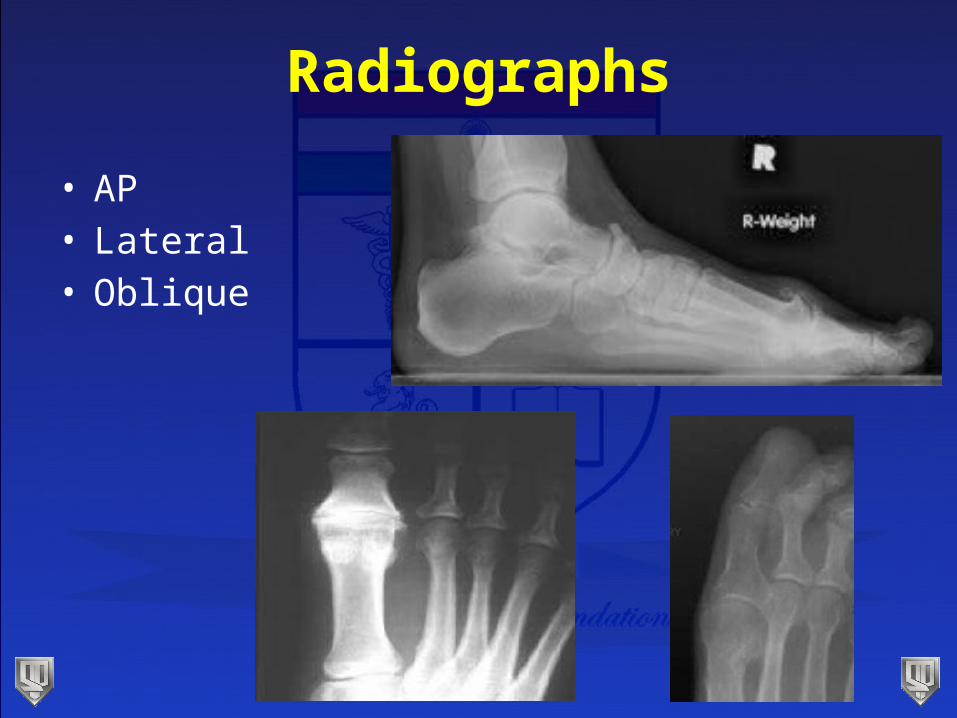
Radiographs
• AP• Lateral• Oblique
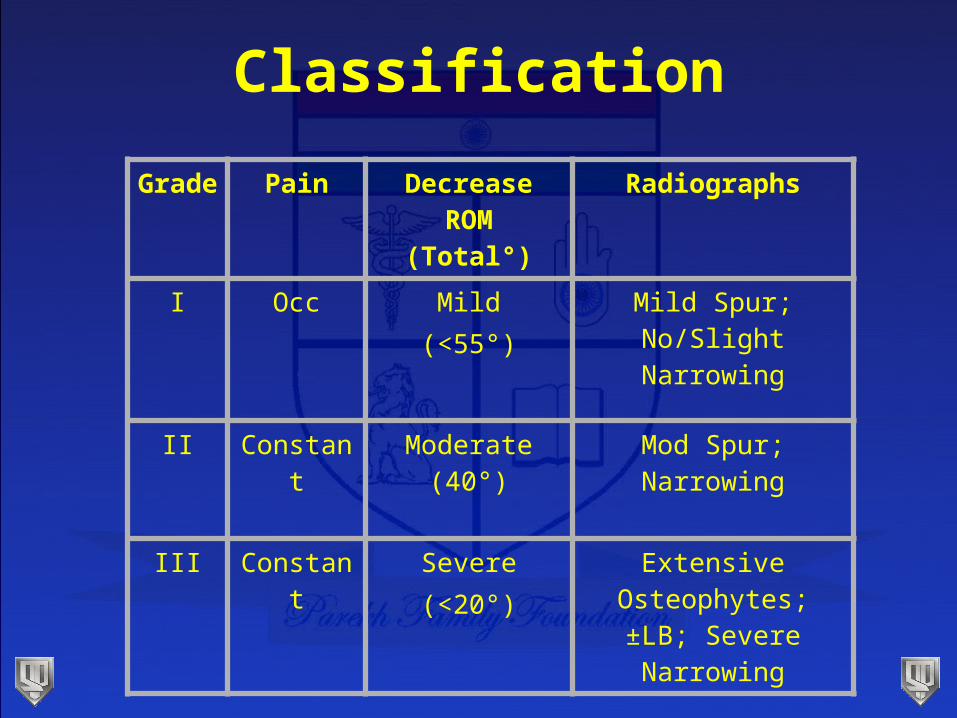
Grade Pain Decrease ROM (Total°)
Radiographs
I Occ Mild(<55°)
Mild Spur; No/Slight Narrowing
II Constant Moderate (40°) Mod Spur; Narrowing
III Constant Severe(<20°)
Extensive Osteophytes; ±LB; Severe Narrowing
Classification
Conservative Treatment
• NSAID’s• Shoe modifications to decrease motion
• Stiff sole shoe• Morton’s extension• Steel shank w/ rocker bottom
• Taping• Steroid injections
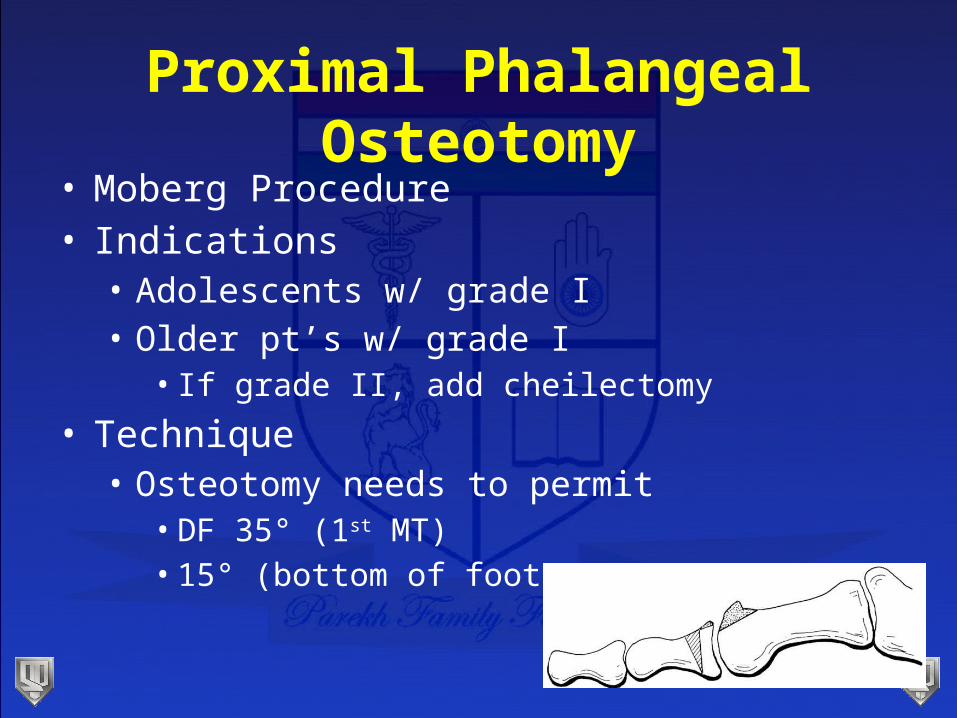
Proximal Phalangeal Osteotomy
• Moberg Procedure• Indications
• Adolescents w/ grade I• Older pt’s w/ grade I
• If grade II, add cheilectomy
• Technique• Osteotomy needs to permit
• DF 35° (1st MT)• 15° (bottom of foot)
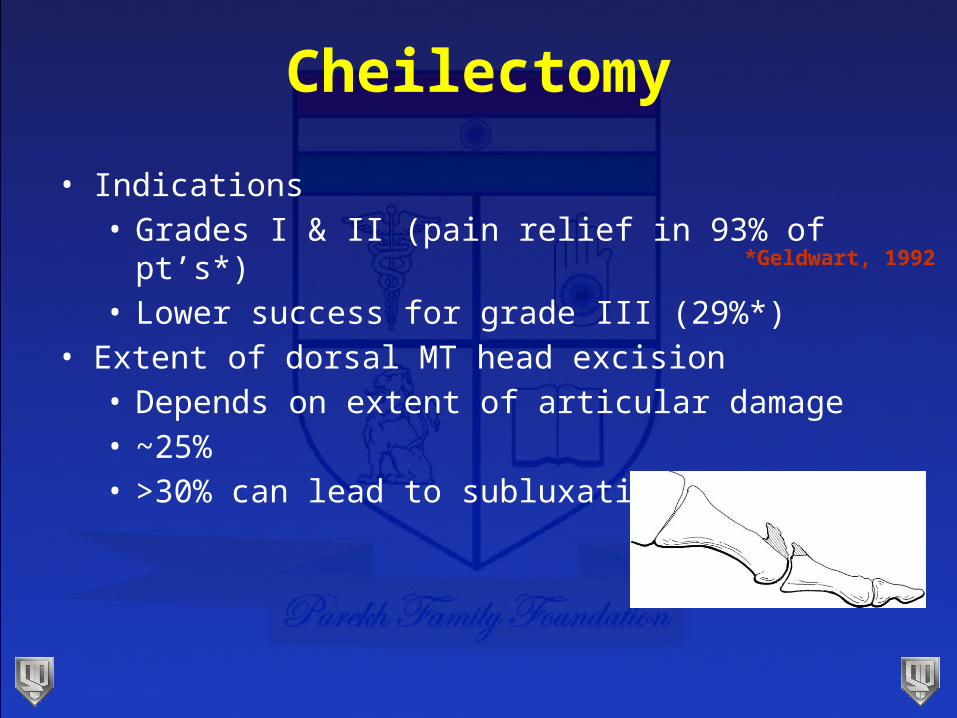
Cheilectomy
• Indications• Grades I & II (pain relief in 93% of pt’s*)• Lower success for grade III (29%*)
• Extent of dorsal MT head excision• Depends on extent of articular damage• ~25%• >30% can lead to subluxation
*Geldwart, 1992
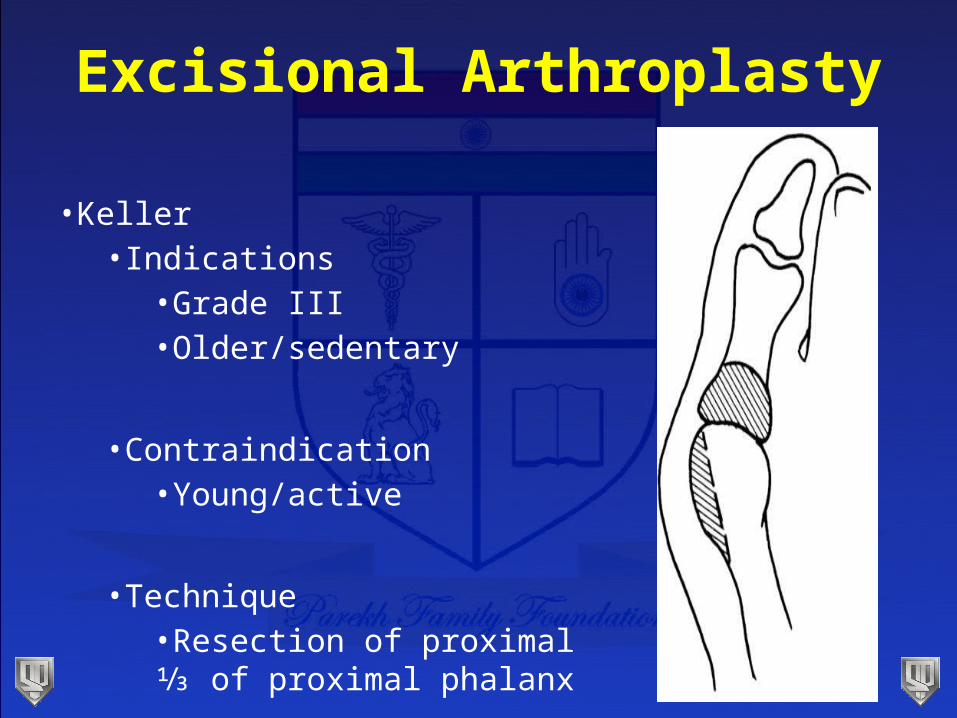
Excisional Arthroplasty
•Keller•Indications
•Grade III•Older/sedentary
•Contraindication•Young/active
•Technique•Resection of proximal ⅓ of proximal phalanx
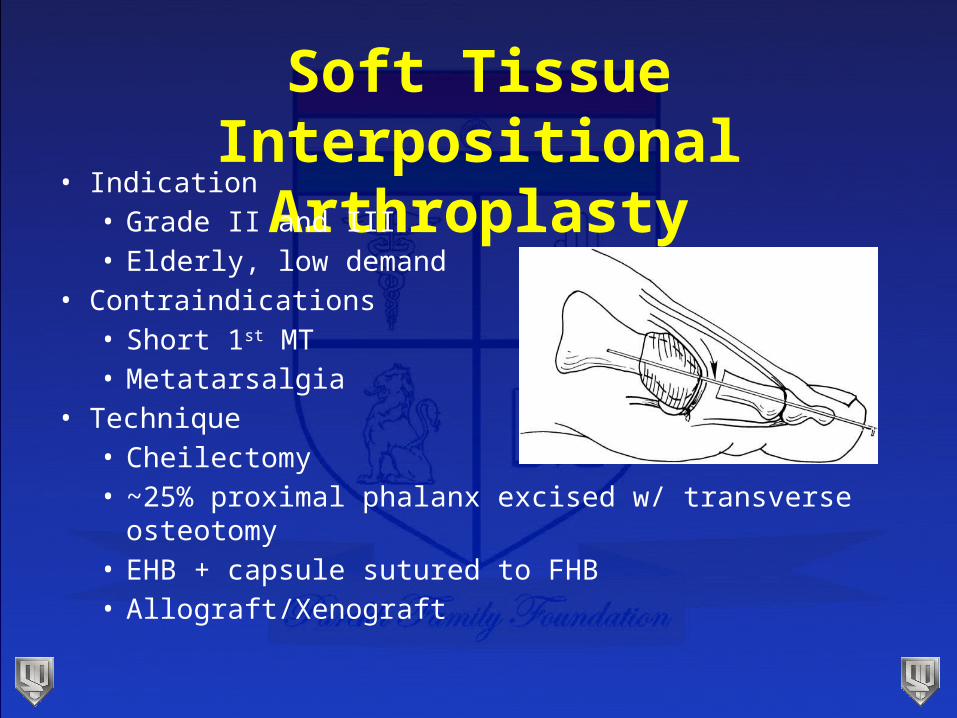
Soft Tissue Interpositional Arthroplasty
• Indication• Grade II and III• Elderly, low demand
• Contraindications• Short 1st MT• Metatarsalgia
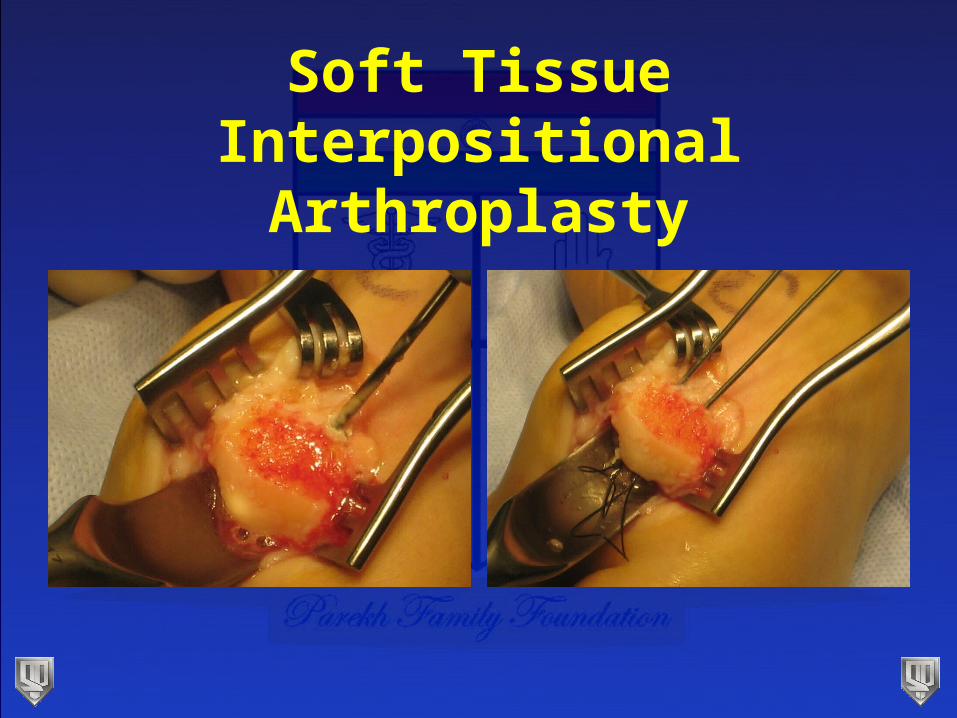
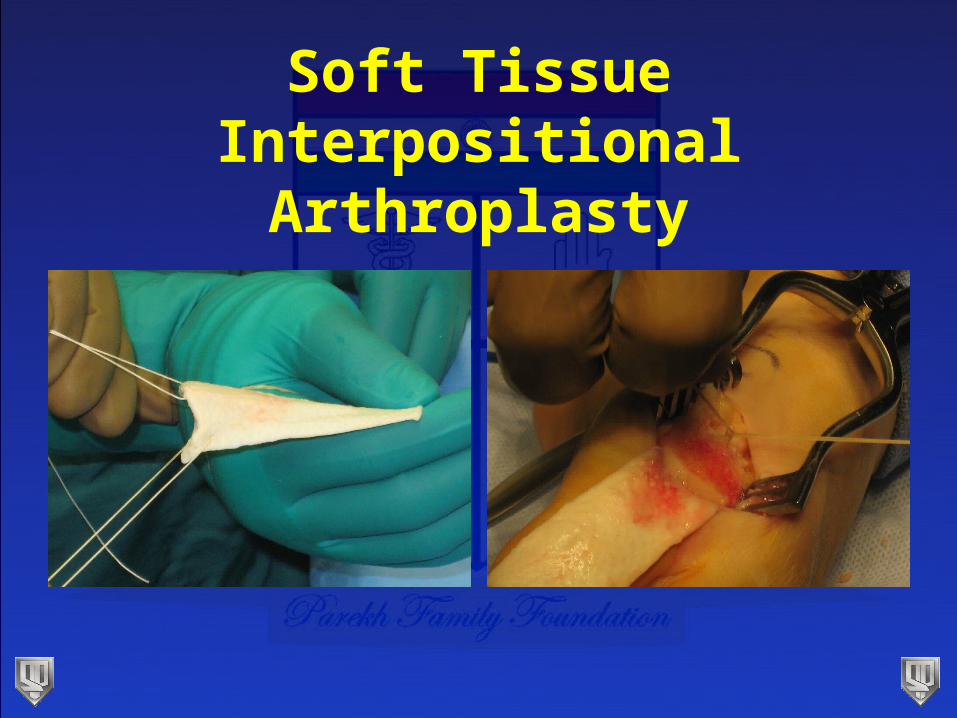
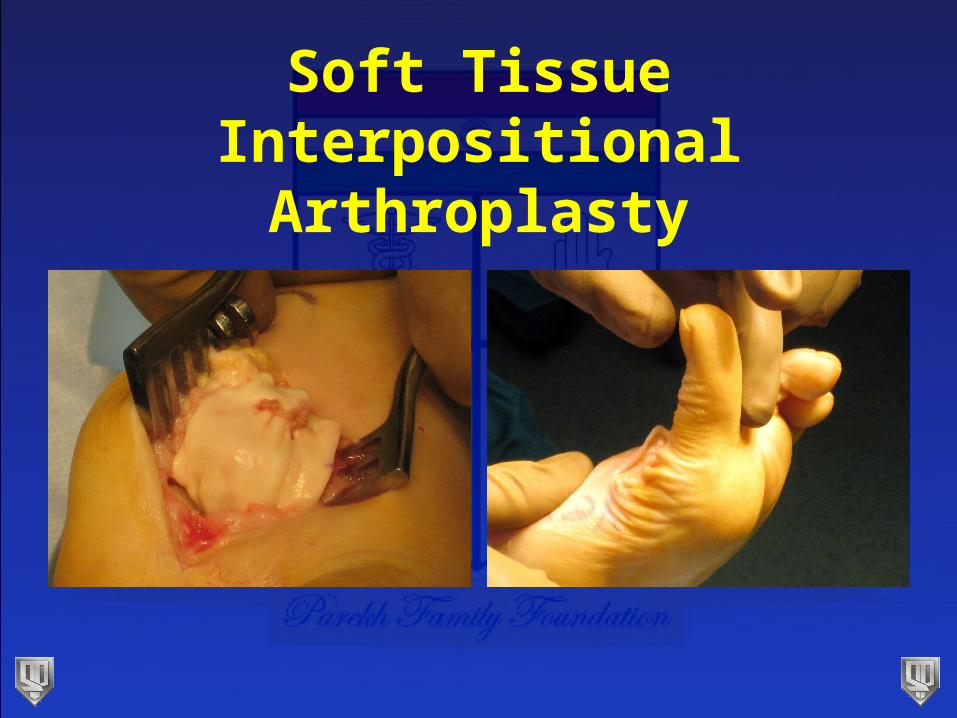
• Technique• Cheilectomy• ~25% proximal phalanx excised w/ transverse osteotomy• EHB + capsule sutured to FHB• Allograft/Xenograft
Soft Tissue Interpositional Arthroplasty
Soft Tissue Interpositional Arthroplasty
Soft Tissue Interpositional Arthroplasty
Soft Tissue Interpositional Arthroplasty
Soft Tissue Interpositional Arthroplasty
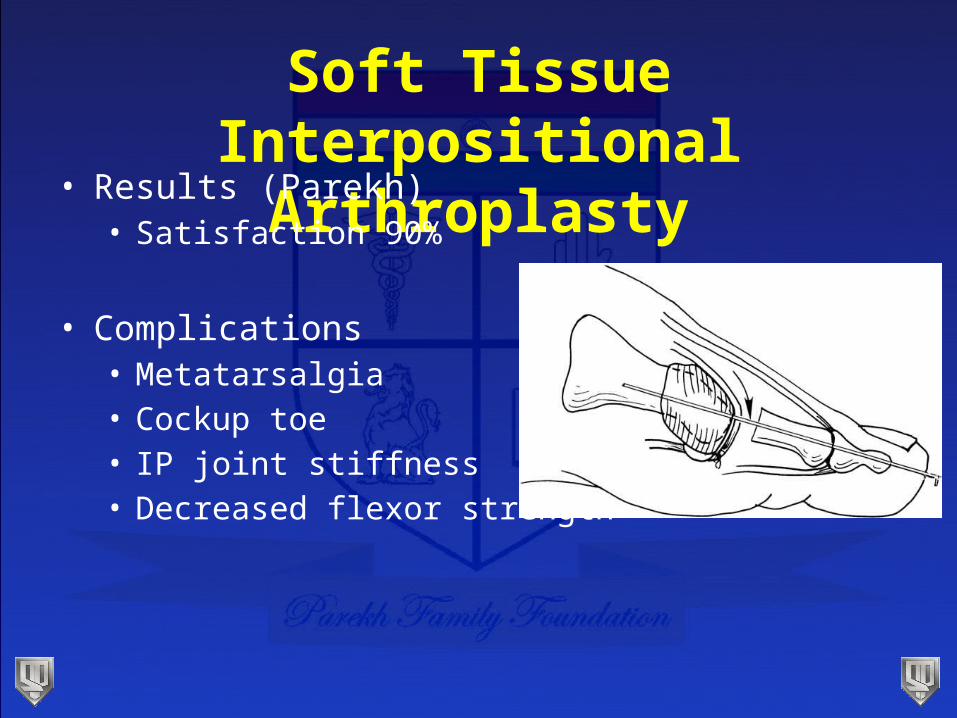
• Results (Parekh)• Satisfaction 90%
• Complications • Metatarsalgia• Cockup toe• IP joint stiffness• Decreased flexor strength
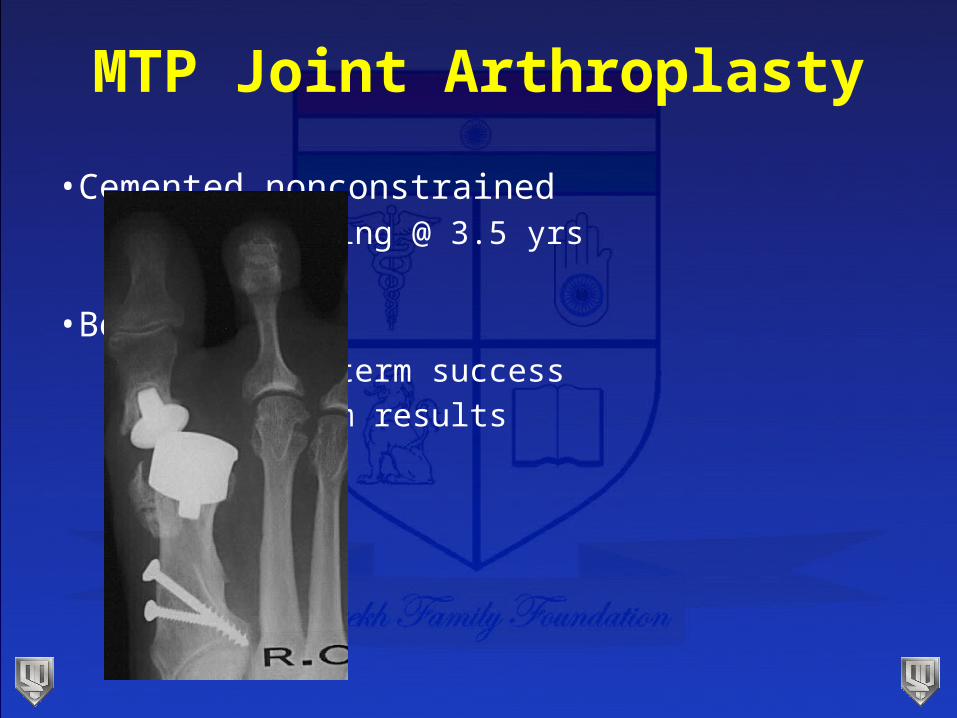
MTP Joint Arthroplasty
•Cemented nonconstrained•>50% loosening @ 3.5 yrs
•Bony ingrowth•Some short term success•No long term results
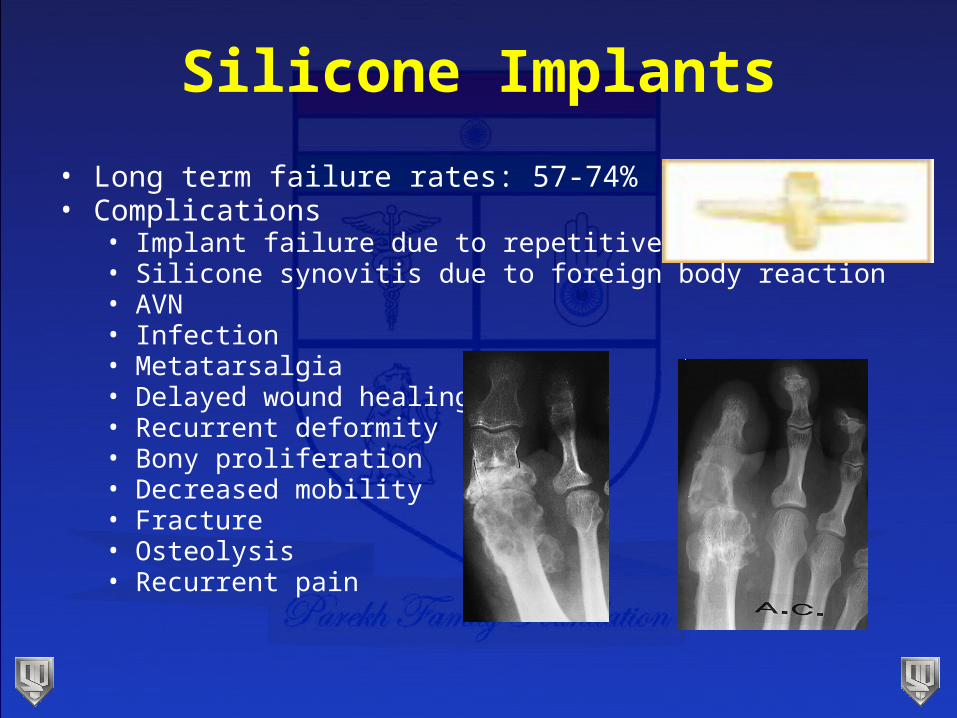
Silicone Implants
• Long term failure rates: 57-74%• Complications
• Implant failure due to repetitive loading• Silicone synovitis due to foreign body reaction• AVN• Infection• Metatarsalgia• Delayed wound healing• Recurrent deformity• Bony proliferation• Decreased mobility • Fracture• Osteolysis• Recurrent pain
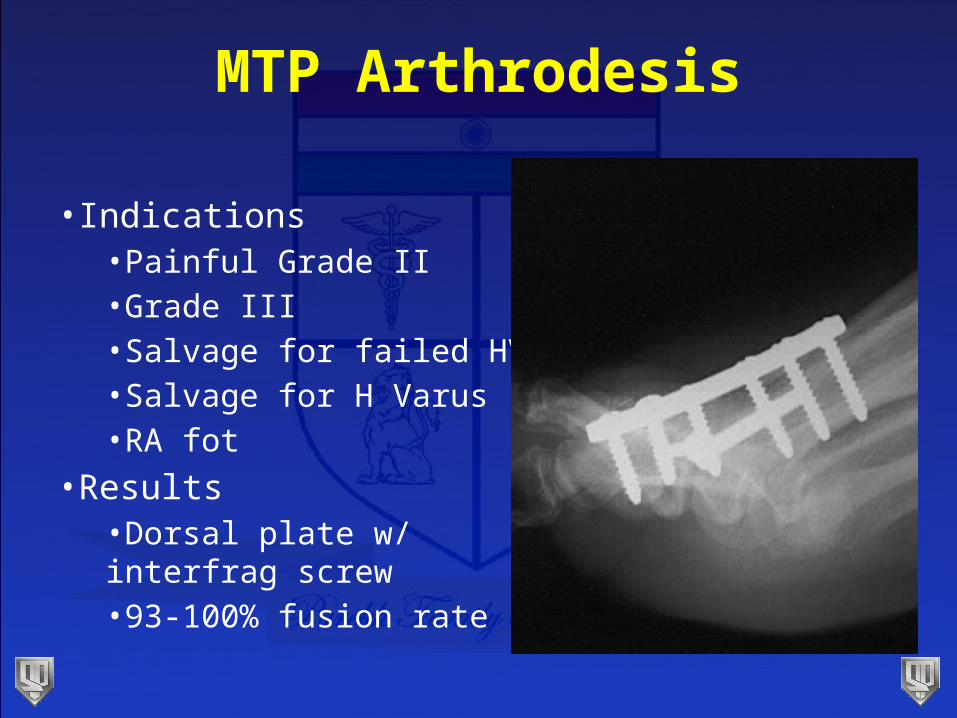
MTP Arthrodesis
•Indications•Painful Grade II•Grade III •Salvage for failed HV•Salvage for H Varus•RA fot
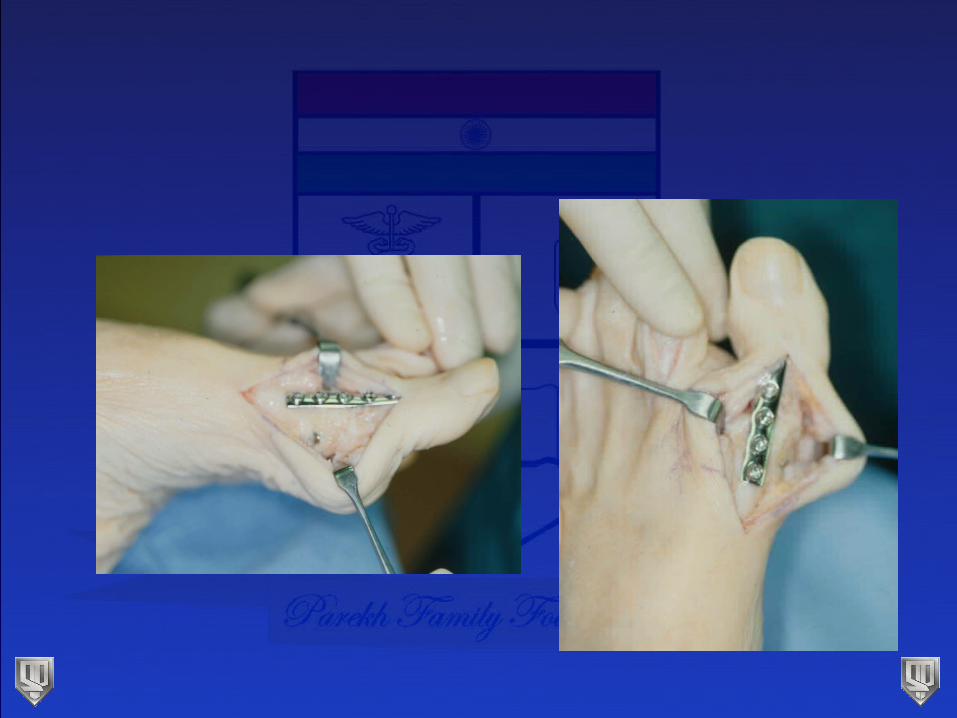
•Results•Dorsal plate w/ interfrag screw•93-100% fusion rate
MTP Arthrodesis
• Few contraindications
• Requires careful explanation to patient,
re: no motion
• Multiple reports in literature ranging from 77 to 100% success
MTP Arthrodesis
• First described by Broca in 1852
• 1940 Thompson & McElveney - 15 cases
• 1952 McKeever successful in 33 patients -- becomes popular
MTP Arthrodesis
•Severe hallux rigidus•Severe hallux valgus•Rheumatoid arthritis•Salvage (Keller, failed implant)
•Post infection•Post traumatic•Neuromuscular disease•Chronic instability
MTP Arthrodesis
•IP joint arthritis
•Active infections
•Vascular deficiency
•Poor skin quality
•Significant neuropathy
•High heeled shoewear
MTP Arthrodesis
• Technique
• Planar coaptation vs. convex-concave
• Threaded Steinmann pins
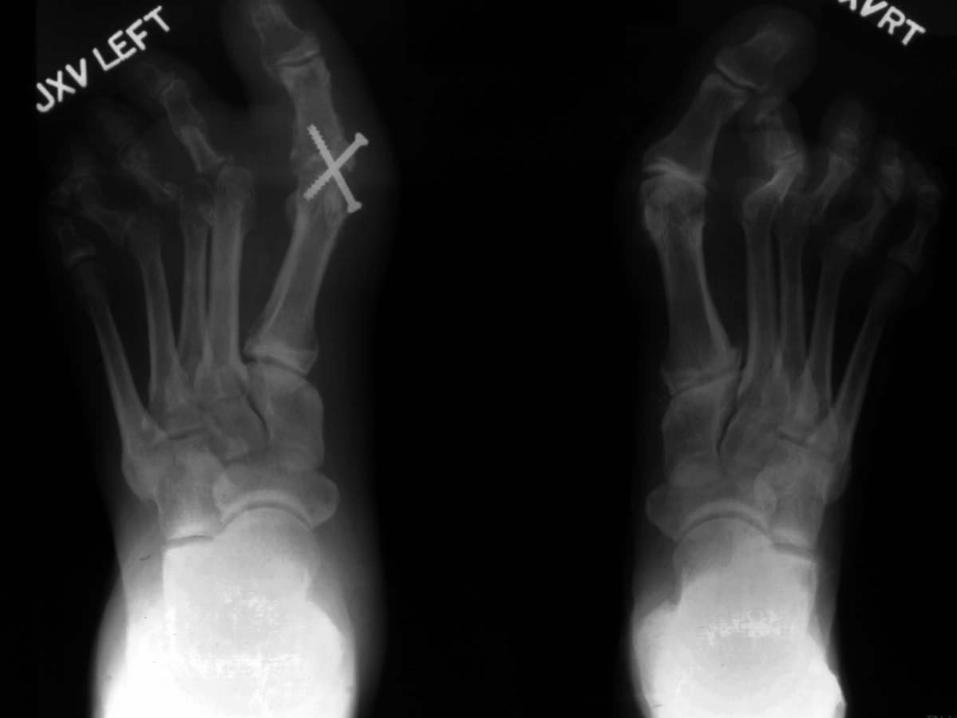
• Screw or plate or screw & plate
Biomechanics - Shortening
• 1987, Turan and Lindgren • Planar cuts: 1.0 to 1.5 cm
• 1994, Coughlin • Cone shaped reamers: 7.7 mm• Cup shaped reamers: 3.8 mm
• 2006, Parekh• No statistical difference 7.1mm v 5.7mm
Fixation Strength: Biomechanic Studies
• 1986, Sykes & Hughes - Planar surfaces with single cancellous screw gave best fixation
• 1993, Curtis - Conical surfaces with lag screw was best





Position
• 10-15o DF above the horizontal• 25o from 1st metatarsal axis
• 15-20o abduction in the transverse plane - avoid 2nd toe impingement
• 0o rotation

Fusion Rates with Plates
• Coughlin & Abdo:
98% fusion with 93% success.
• Salis-Soglio & Thomas: 92%
• Mankey & Mann: 92%
• Coughlin: 100%
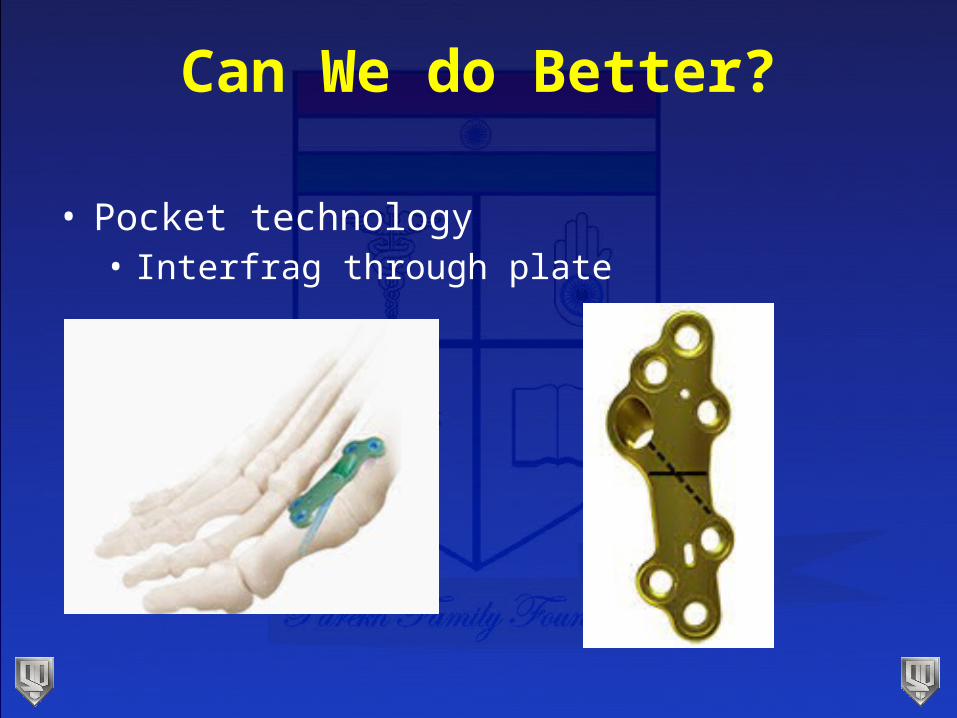
Can We do Better?
• Pocket technology• Interfrag through plate
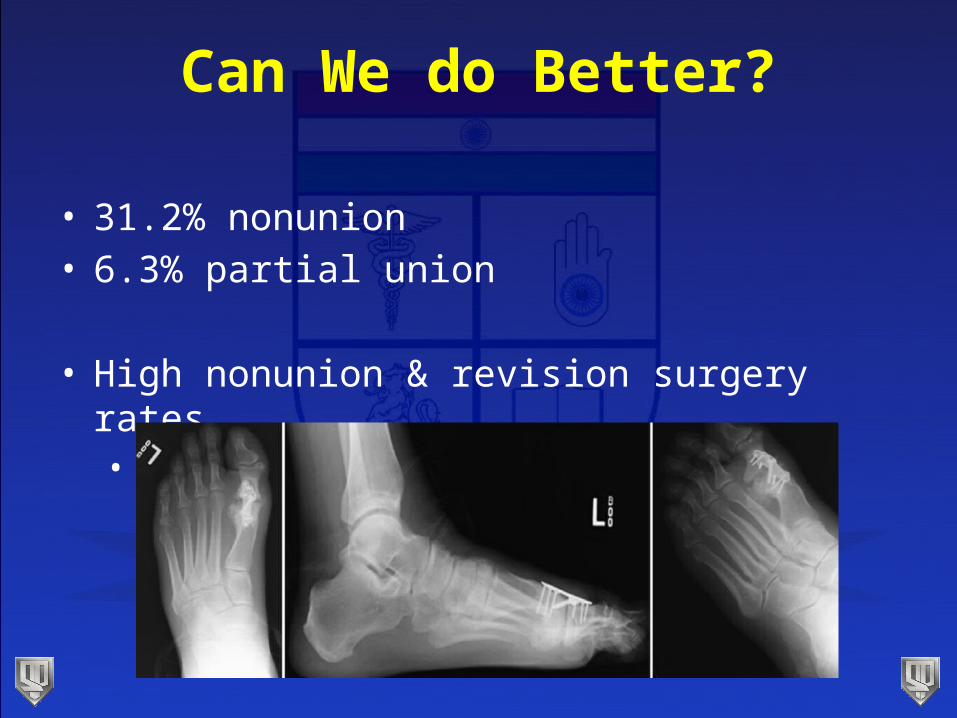
Can We do Better?
• 31.2% nonunion • 6.3% partial union
• High nonunion & revision surgery rates• Use w caution
Results: Reports of union > 90%
• 1994, Coughlin: Cup & cone surfaces with mini
fragment plate & K-wire• 35 cases with 98% union
• 1992, Holmes: Interfragmentary screw added to above with good results
Complications of Arthrodesis
• Malalignment: Varus-valgus, DF-PF, or rotation
• Nonunion: 0-7% with plate and interfragmentary screw
• IP arthritis increases with less than 20o valgus position
Complications
• IP arthrosis (progression in 6% )*• Decrease in IP joint motion - 22o*• Nonunion• Callus formation• Malposition• Infection• Subsequent plate removal: 7% to 46%
*Coughlin, 1994
RE ECT
the ankle
the foot