Embed Size (px)
Citation preview

Lecture 9Substance Abuse
and Addiction
David Saffen, Ph.D.Principal Investigator
Department of Cellular and Genetic MedicineFudan University, Shanghai, China
Email: [email protected]
Substance abuse
The use of therapeutic drugs or illegal substances with the goal of producing altered psychological states, including hallucinations, euphoria or reduced anxiety.
Substance abuse also includes the use of drugs and other agents to gain unfair advantage in sports or other competitive activities.
Substance abuse often (but not always) results in “addiction” to the drug or illegal substance.
AddictionAddiction is a chronic, often relapsing brain disease that causes compulsive drug seeking and use, despite harmful consequences to the addicted individual and to those around him or her. Although the initial decision to take drugs is voluntary for most people, the brain changes that occur over time challenge an addicted person‟s self control and hamper his or her ability to resist intense impulses to take drugs. (NIDA, NIH)
Drug addition often involves both:
Physical dependence characterized by uncomfortable (and
sometimes) dangerous physiological responses to drug
withdrawal.
Psychological dependence characterized by “craving:” an intense,
urgent „abnormal desire‟ (longing or yearning) for drugs.

Substance abuse and addictionas diseases of the brain
• Until the last half of the 20th century, substance abuse and addiction were primarily considered to be the consequences of “weak personality” or “moral failure” rather than physical/ psychological diseases.
• Research during the last 50-60 years, however, has elucidated many physiological changes brought on by the use of drugs, including physical and neurological adaptations that generate dependence and behavioral and psychological changes that maintain addiction.
• The current hope is that basic research into the molecular and genetic mechanism underlying the substance abuse and addiction will lead to novel strategies for the treatment and prevention of these disorders.

Comorbidities:Substance abuse and addiction are often accompanied
by serious mental and physical illnesses
• Psychotic disorders
• Mood and anxiety disorders
• Physical complaints
• Infectious diseases:
- hepatitis
- HIV/AIDS Source: NIND, NIH

Substance-induced disorders
- intoxication
- withdrawal
- other substance/medication-induced disorders, including:
psychotic disorders
bipolar and related disorders
depressive disorders
anxiety disorders
obsessive-compulsive and related disorders
sleep disorders
sexual dysfunctions
delirium
neurocognitive disorders

Social costs and epidemiology of substance abuse and addiction
Substance abuse-related impact on public health (WHO 2002 survey)
Disability- Adjusted Life Years (DALY),
a measure of the burden of disease; one
DALY = one year of “healthy” life lost.
= no data
= < 40 per 100,000
= 40 – 160 “
= 160 – 320 “
= 320 – 440 “
= > 440 “Nutt D, et al, Lancet, 2007

Substance abuse

DSM-5: 10 classes of abused drugs
• Alcohol
• Caffeine
• Cannabis
• Hallucinogens
(phencyclidine, other hallucinogens)
• Inhalants
• Opioids
• Sedatives, hypnotics and anxiolytics
• Stimulants
(amphetamine-type substances, cocaine, other substances)
• Tobacco/nicotine
• Other substances (e.g. anabolic steroids)

Alcohol (ethanol)
• Alcohol abuse, which can lead to alcoholism, is a pattern of drinking that results in harm to one's health, interpersonal relationships, or ability to work.
• Alcoholism or alcohol dependence is a diagnosable disease characterized by a strong craving for alcohol, and/or continued use despite harm or personal injury.
• “Moderate” drinking: 1 (women) or 2 (men) drinks/day; “heavy” drinking: exceeding the above amounts. 1 drink = 14 grams of ethanol ~ 355 ml beer; 148 ml wine; 44.4 ml 80-proof distilled alcoholic drink or liquor.
Recorded annual alcohol consumption(liters per person; 2004)

Caffeine (and derivatives)
• Central nervous system stimulants; promotes wakefulness and alertness
• Antagonize adenosine receptor
(A1 and A2a subtypes)
• Indirectly stimulate the release of dopamine, glutamate and acetylcholine.
• One cup of regular coffee (8 oz = 240 ml) contains 60 - 130 mg caffeine; Tea: 40 -50 mg/8 oz; Colas: (Pepsi and Coca Cola) ~ 40- 50 mg/12 oz can and “energy” drinks: 80 - 120 mg/8 oz serving
• Caffeine withdrawal symptoms include: headaches, depressed mood, irritability, muscle pain and stiffness, lethargy
Psychoactive caffeine metabolites produced in liver
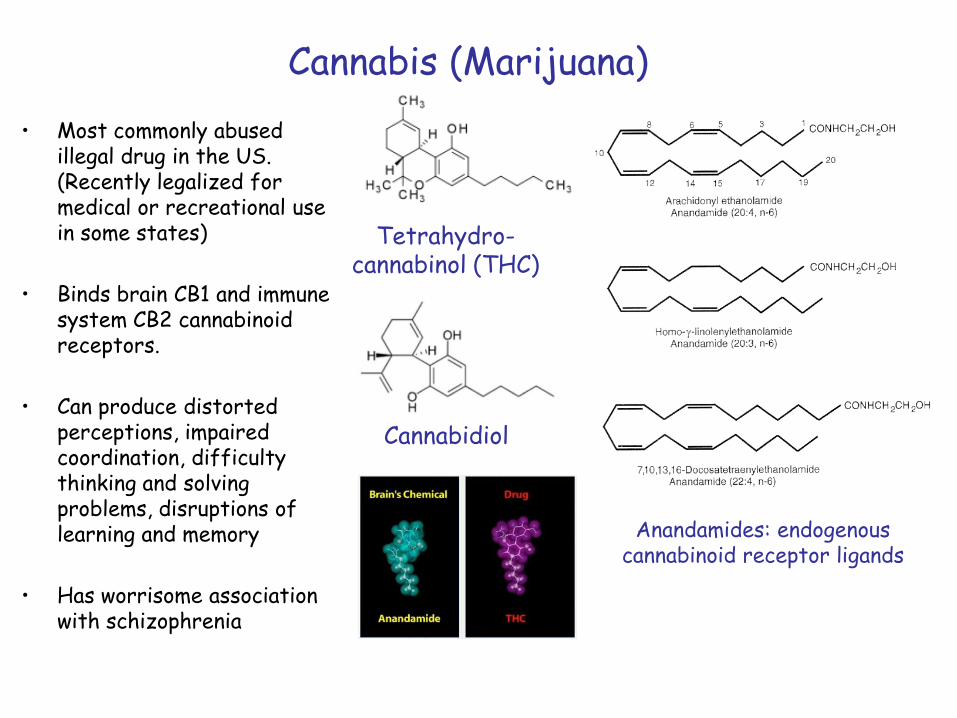
Cannabis (Marijuana)
• Most commonly abused illegal drug in the US. (Recently legalized for medical or recreational use in some states)
• Binds brain CB1 and immune system CB2 cannabinoid receptors.
• Can produce distorted perceptions, impaired coordination, difficulty thinking and solving problems, disruptions of learning and memory
• Has worrisome association with schizophrenia
Tetrahydro-cannabinol (THC)
Anandamides: endogenouscannabinoid receptor ligands
Cannabidiol

Hallucinogens I(phencyclidine and other arylcyclohexylamines)
• Non-competitive antagonists of the NMDA glutamate receptor: bind within the ion channel
• Produce visual or aural hallucinations; feeling of “dissociation” or being “out of body.”
• Cognitive dysfunctions similar to those observed in schizophrenia.
• At high-doses: psychosis similar to that observed in schizophrenia and bipolar disorder.
(Rolicyclidine)
(Tenocyclidine)
(Eticyclidine)
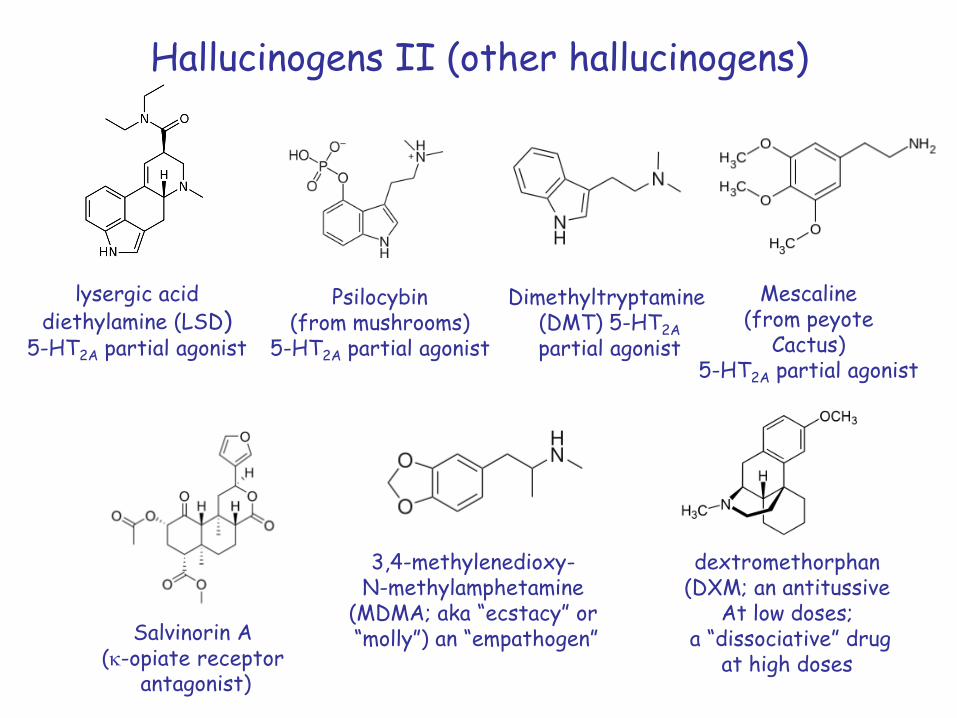
Hallucinogens II (other hallucinogens)
Mescaline(from peyote
Cactus)5-HT2A partial agonist
Dimethyltryptamine(DMT) 5-HT2A
partial agonist
Psilocybin(from mushrooms)
5-HT2A partial agonist
lysergic aciddiethylamine (LSD)
5-HT2A partial agonist
3,4-methylenedioxy-N-methylamphetamine
(MDMA; aka “ecstacy” or“molly”) an “empathogen”
dextromethorphan(DXM; an antitussive
At low doses;a “dissociative” drug
at high doses
Salvinorin A(k-opiate receptor
antagonist)

Intoxicative inhalants
Aliphatic Hydrocarbonse.g., gasoline
Kerosene, butane
Aromatichydrocarbonse.g., toluene
Ketones,e.g., acetone
Nitrites, alkyl nitritese.g., amyl nitrite
nitrous oxide
Haloalkanese.g, tricholoroethyene

Opioids(m-opioid receptor agonists/partial agonists)
Heroin MorphineHydrocodoneaka: Vicodin
MethadoneBuprenorphine(SuboxoneTM)

Sedatives, hypnotics & anxiolytics(including benzodiazepines: non-competitive
agonists of GABAA receptors)
Alprazolam(XanaxTM)
MethaqualoneQuaaludeTM
AmobarbitalAmytalTM
Gamma-hydroxy-butyric acid (GHB)
Diazepam(ValiumTM)
Clonazepam(KlonoponTM)
Lorazopam(AtivanTM)

Stimulants(often agents that rapidly increase extracellular
levels of dopamine, epinephrine and serotonin)
Amphetamine Methamphetamine
Cocaine MephedroneA synthetic stimulant with
structure similar to cathinone. Synthetic cathinones are
collectively known as“bath salts.”
Cathinonefrom Catha edulis
(aka: qat, khat)
2,5-dimethoxy-4-Methylamphetamine
(aka DOM or STP: “Serenity, Tranquility, Peace”)

Tobacco/nicotine
• Nicotine: agonist of nicotinic acetylcholine receptors; a parasympathomimetic and central nervous system agent; stimulates the release of dopamine and norepinephrine at low doses and serotonin and endogenous opiates at higher doses.
• Produces both stimulant and relaxant effects; suppresses appetite
• Highly addictive
• 1 cigarette yields ~ 1 mg absorbed nicotine
Nicotine
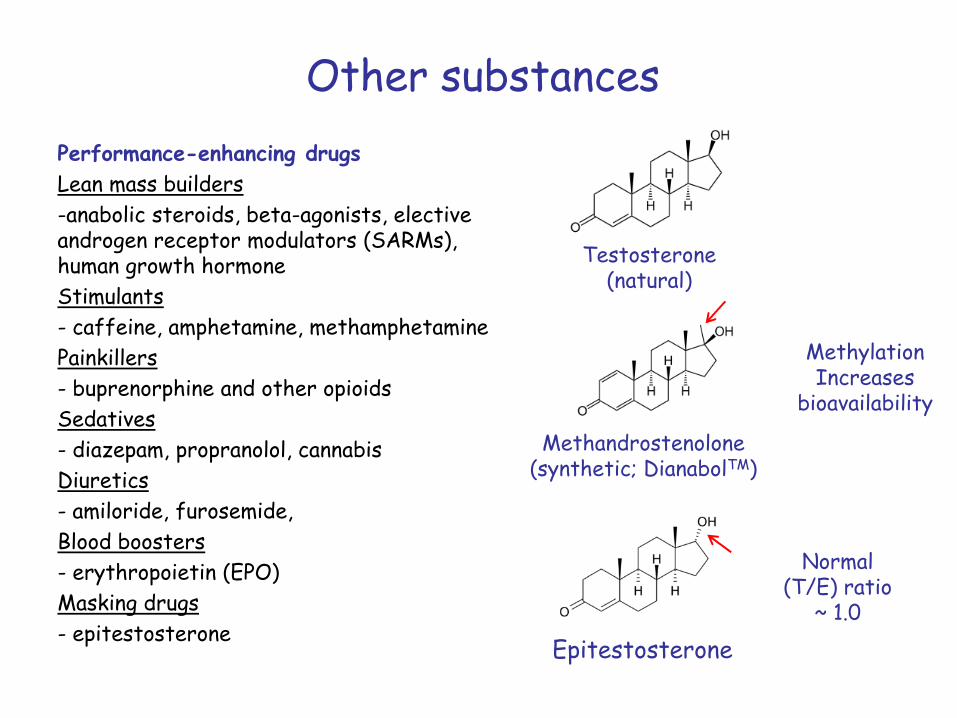
Other substances
Performance-enhancing drugs
Lean mass builders
-anabolic steroids, beta-agonists, elective androgen receptor modulators (SARMs), human growth hormone
Stimulants
- caffeine, amphetamine, methamphetamine
Painkillers
- buprenorphine and other opioids
Sedatives
- diazepam, propranolol, cannabis
Diuretics
- amiloride, furosemide,
Blood boosters
- erythropoietin (EPO)
Masking drugs
- epitestosterone
Testosterone(natural)
Methandrostenolone(synthetic; DianabolTM)
Epitestosterone
Normal(T/E) ratio
~ 1.0
MethylationIncreases
bioavailability

A recent attempt to quantify the relative harm
associated with abuse of different
substances
(Nutt D, et al, Lancet, 2007)
4-MTA: 4-methythioamphetamineA selective serotonin releasing agent (SSRA)
Methylphenidate: A stimulant used in the treatment of ADHD

Addiction

Stage 1: drug exposure stimulates the release of high levels of dopamine in the extended amygdala, ventral pallidum, n. accumbens, and PFC activating D1 dopamine receptors, resulting in increased synthesis of cAMP, activation of PKA and induction of gene expression.
Stage 2: Chronic stimulation of D1 receptors lead to the expression of DFosB, a stable transcription factor that mediates neuroplastic changes in n. accumbens circuitry.
Stage 3: A long-lasting state characterized by craving, relapse, reduced ability to suppress drug-seeking behavior, reduced pleasure
from drug.
Three stages ofdrug addiction
Slightly different definition of 3 stages1. Binge/intoxication2. Withdrawal/negative effects3. Preoccupation/anticipation (craving)

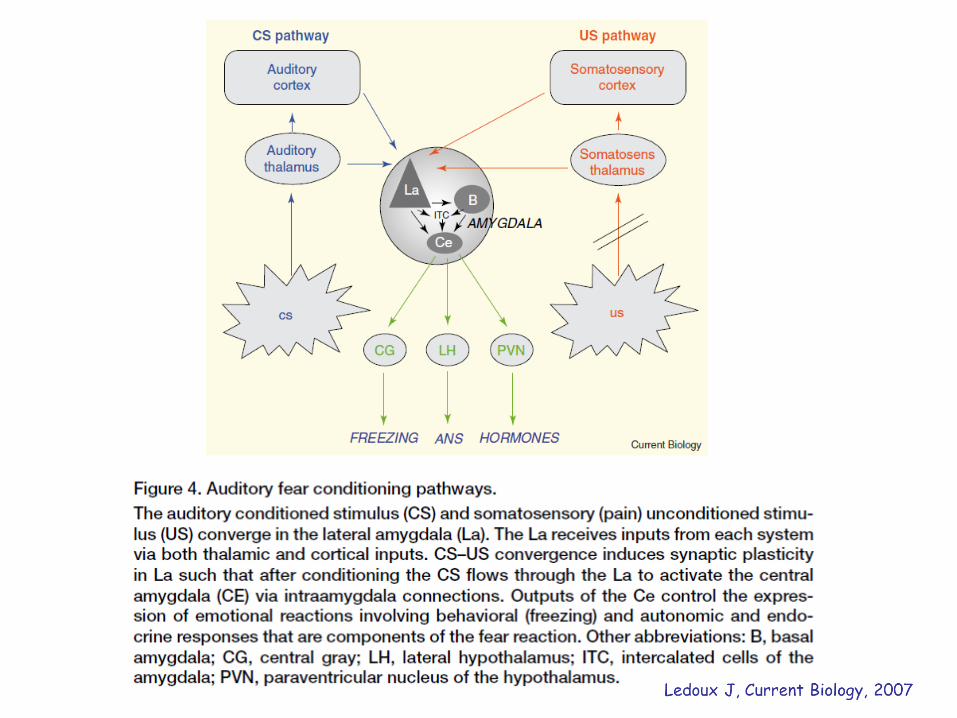
Mesocorticolimbic reward pathway
= midbrain
Limbic system targets(via medial forebrain bundle):- Medial PFC and anterior
cingulate gyrus- Amygdala- Hippocampus- Nucleus accumbens- Ventral globus pallidus

Limbic system circuitry:mediates the influences of motivation, emotion,
context, affect and information on behavior
mPFC = medialprefrontalcortex
AC = anteriorcingulategyrus
aka: medialdorsal thalamus
dopamine
GABA
glutamate
Aka: ventralglobuspallidus
AC
(ventral striatum)
Medialforebrain
bundle
Amygdala
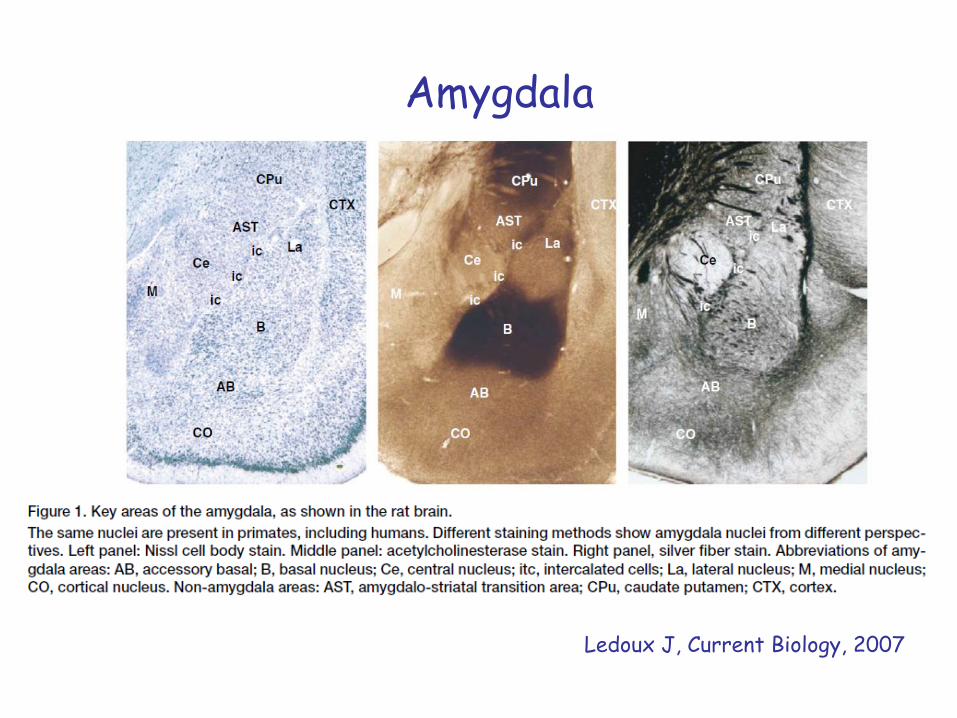
Ledoux J, Current Biology, 2007



Extended amygdala
Comprises: - Central nucleus of the amygdala - Bed nucleus of the stria terminalis (BNST)- Medial shell subregion of the nucleus accumbens
Inputs from limbic structures, including:- basolateral amygdala- hippocampus
Outputs:- medial part of ventral pallidum - lateral hypothalamus
Implicated in the creation of negative states that promote negative-reinforcement mechanisms implicated in addiction (e.g., drug seeking behavior to avoid unpleasant psychological states associated with abstinence).
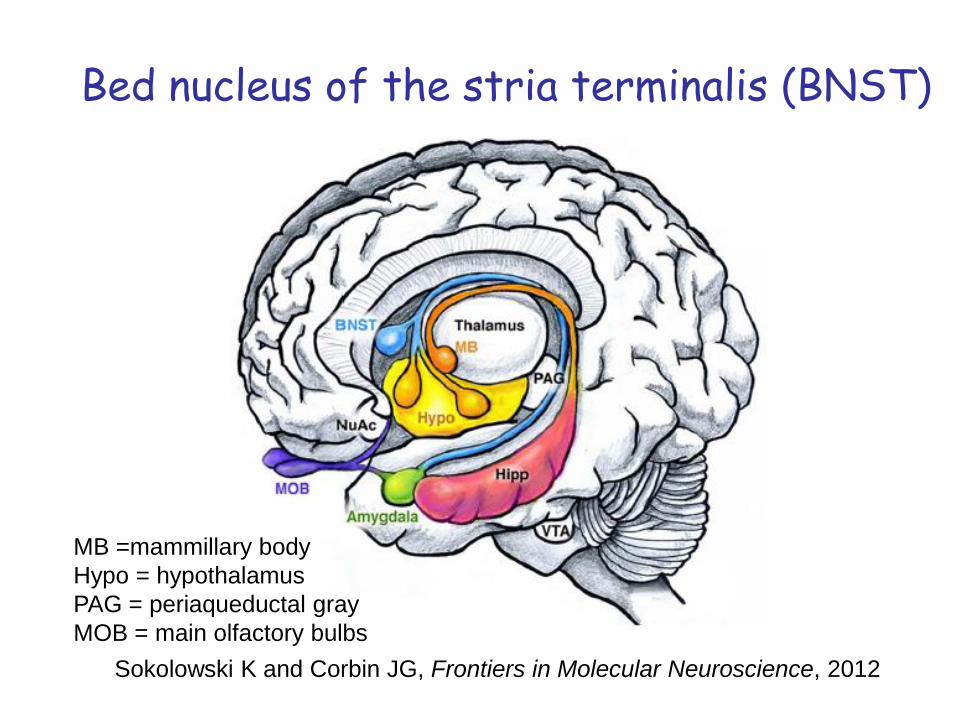
Bed nucleus of the stria terminalis (BNST)
Sokolowski K and Corbin JG, Frontiers in Molecular Neuroscience, 2012
MB =mammillary body
Hypo = hypothalamus
PAG = periaqueductal gray
MOB = main olfactory bulbs

Nucleus accumbens(a component of the “ventral striatum”)
AcbC = accumbens coreAcbSh = accumbens shellCaud = caudate; Put = putamenIc = internal capsule

• Schematic illustrating the connections of the VS. Blue arrows=inputs; gray arrows=outputs;
Amy=amygdala; BNST=bed nucleus stria terminalis; dACC=dorsal anterior cingulate cortex;
Hipp=hippocampus; hypo=hypothalamus; MD=medio-dorsal nucleus of the thalamus; OFC=orbital
frontal cortex; PPT=pedunculopontine nucleus; S=shell; SNc=substantia nigra, pars compacta;
STN=subthalamic nucleus; Thal=thalamus; VP=ventral pallidum; VS=ventral striatum;
VTA=ventral tegmental area; vmPFC=ventral medial prefrontal cortex
Habner SN and Knutsen B, Neuropsychopharmacology Reviews, 2010

Neural circuits central to the three stages of addiction
(1)(2)
(3)
Koob GF and Volkow ND, 2010

Addiction, stage 1 (Binge/intoxication):focal points: ventral tegmental area (VTA),
nucleus accumbens (Acb shell & core), dorsal striatum
SNc = Substantia nigra parscompacta
VGP = ventral globus pallidusDVP = dorsal globus pallidus
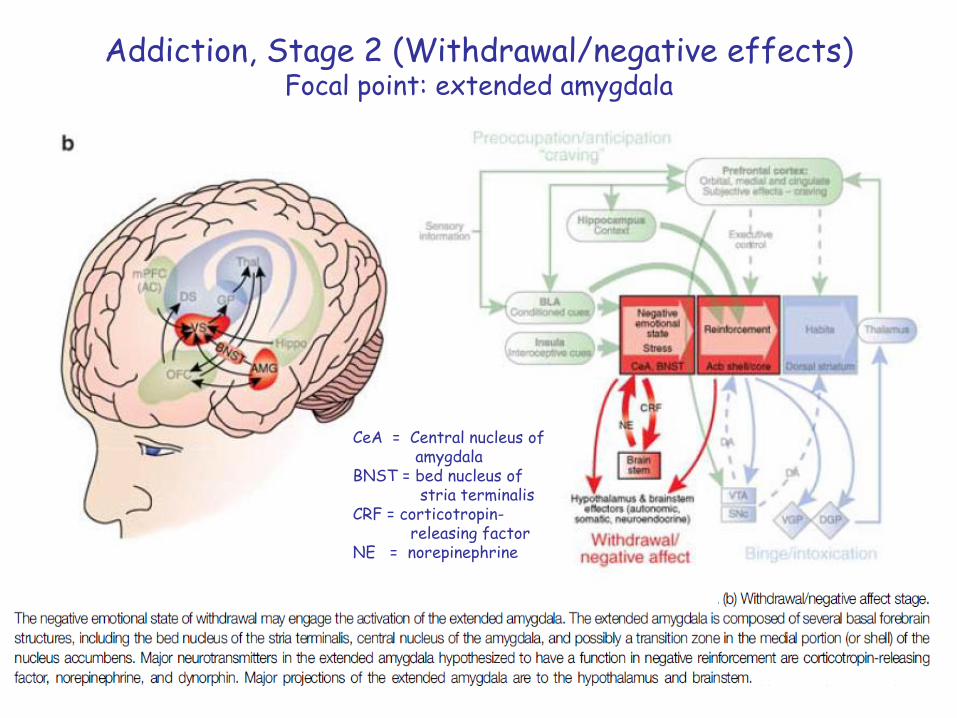
Addiction, Stage 2 (Withdrawal/negative effects)Focal point: extended amygdala
CeA = Central nucleus of amygdala
BNST = bed nucleus of stria terminalis
CRF = corticotropin-releasing factor
NE = norepinephrine

Addiction, Stage 3 (preoccupation/anticipation “craving”)craving: orbitofrontal cortex-dorsal striatum, prefrontal cortex, basolateral
amygdala (BLA), hippocampus, insula; inhibitory control: cingulate gyrus, dorsolateral prefrontal cortex and inferior frontal cortex

Hypothesized sequential cascade of neuroplasticity underling addiction

Summary• Addiction is a disease caused by maladaptive neuroplastic changes in
brain circuitry
• Neuroplasticity occurs in distinct neuronal systems during three (partially overlapping) phases of addiction.
1) Stage 1 (Binge/intoxication): VTA and ventral and dorsal striatum
2) Stage 2 (Withdrawal/negative effects): Extended amygdala
3) Stage 3 (Craving): OFC-dorsal striatum, PFC, BLA, Hipp, insula;
(Inhibitory control deficits): cingulate gyrus, dlPFC,
inferior frontal cortex
• The overall shift in motivation to take addicting drugs is from positive rewards (e.g. euphoria) to avoidance of the negative effects of abstinence.
• Knowledge of the neuronal networks underlying addiction opens the door to novel pharmacologic and behavioral therapies and preventive strategies.
References (1)• Nutt D, et al, Development of a rational scale to assess the harm of drugs of
potential misuse, Lancet 369, 1047-53, 2007
• Sinha R, The clinical neurobiology of drug craving, Current Opinion in Neurobiology 23, 649 – 654, 2013
• Kalivas PW and Volkow ND, The neural basis of addiction : a pathology of motivation and choice, American Journal of Psychiatry 162, 1403 - 1413, 2005
• Koob GF and Volkow ND, Neurocircuitry of Addiction , Neuropsychopharmacology Reviews 35, 217 – 238, 2010
• Pierce RC and Kumaresan V, The mesolimbic dopamine system: the final common pathway for the reinforcing effect of drugs of abuse?, Neuroscience and Biobehavioral Reviews 30, 215-239, 2006
• LeDoux J, The amygdala, Current Biology 17, R868 – R874, 2007
• Robinson AJ and Nestler EJ, Transcriptional and epigenetic mechanisms of addiction, Nature Reviews Neuroscience 12, 623-637, 2012

References (2)
• Kreek MJ et al., Opiate addiction and cocaine addiction: underlying molecular neurobiology and genetics, Journal of Clinical Investigations 122, 3387-3393, 2012
• Mazei-Robison MS and Nestler EJ, Plasticity of ventral tegmental area and locus ceruleus catecholamine neurons, Cold Spring Harbor Perspectives in Medicine 2, a012070, 1-16, 2012
• Zhang L et al, Src Phosphorylation of mu-receptor is responsible for the receptor switching from an inhibitory to a stimulatory signal, Journal of Biological Chemistry 284, 1990-2000, 2009
• Zhang L et al, a novel noncanonical signaling pathway for the mu-opioid receptor, Molecular Pharmacology 84, 844-853, 2013
• Monfils MH et al, Extinction-reconsolidation Boundaries: Key to persistent attenuation of fear memories, Science 324, 951-955, 2009
• Hutton-Bedbrook K and McNally GP, The promises and pitfalls of retrieval-extinction procedures in preventing relapse to drug seeking, Frontiers in Psychiatry 4, article 4, 1-4, 2013

Journal Presentations,
• Milton AL and Everitt BJ, Wiping Drug Memories, Science336, 167-168, 2012
• Xue YX, et al, A memory retrieval-extinction procedure to prevent drug craving and relapse, Science 336, 241-245, 2012
Internet resources
• National Institute on Drug Abuse (NIDA) http://www.drugabuse.gov/
• National Institute on Alcohol Abuse and Alcoholism (NIAAA)
http://www.niaaa.nih.gov/

Additional Slides