Embed Size (px)
Citation preview

Federal State Budgetary Educational Institution of Higher Education «Irkutsk State Medical University»
of the Ministry of Healthcare of the Russian Federation
Department of histology, embryology, cytology
L. S. Vasilieva, O. A. Makarova, A. S. Dadueva
Lecture notes on sections «Cytology» and «General histology»
Study guidance
Irkutsk ISMU 2017

2
УДК 611.018(075.8)=111 ББК 28.86я73 V 30
Recommended by the CKMB of the FSBEI HE ISMU MOH Russia as a study guidance for English speaking students trained upon higher education program –
specialist`s degree program in General medicine (record № 5 from 15.06.2017)
Аuthors: L. S. Vasilieva– Dr. of biol. sciences, professor, head of the dep. of histology,
embryology, cytology of the FSBEI HE ISMU MOH Russia O. A. Makarova –Cand. ofbiol. sciences, assistant of professor of the dep. of
histology, embryology, cytology of the FSBEI HE ISMU MOH Russia A. S. Dadueva – senior teacher of the dep. of foreign language with courses of Latin
and Russian for foreignersof the FSBEI HE ISMU MOH Russia
Reviewers : T. I. Shalina– Dr. of med. sciences, professor, head of the dep. of human anatomy of
the FSBEI HE ISMU MOH Russia S. O. Korshunova – Cand. ofphil. sciences, associate professor of dep. humanitarian
and informational disciplines of the Irkutsk Institute of theRSJU (RLA of the Ministry of justice)
V 30 Lecture notes on sections «Cytology» and«General histology» :study
guidance/ L. S. Vasilieva, O. A. Makarova, A. S. Dadueva ; FSBEI HE ISMU MOH Russia, Department of histology, embryology, cytology. –Irkutsk : ISMU, 2017. – 52р.
Study guidance «Lecture notes on sections «Cytology» and «General histology»»is made for classroom and extracurricular work of foreign students. Study guidance contains the text of the lectures on sections«Cytology» and «General histology».
It is intended for foreign students of 1–2 courses of the FSBEI HE ISMU MOH Russia.
УДК 611.018(075.8)=111 ББК 28.86я73 © Vasilieva L. S., MakarovaO. A., Dadueva A.S., 2017
© FSBEI HE ISMU MOH Russia, 2017

3
THE CONTENTS
Introduction ................................................................................................................... 4
Lecture 1.Subject of histology. Histological technique. Cytology .............................. 5
Lecture 2. Differentiation of embryonic material. Life cycle. Differons. Tissue
formation ..................................................................................................................... 12
Lecture 3. Epithelial tissue ......................................................................................... 16
Lecture 4. Leukocytes ................................................................................................ 21
Lecture 5. Hematopoiesis ........................................................................................... 27
Lecture 6. Connective tissues ..................................................................................... 32
Lecture 7. Skeletal connective tissues ........................................................................ 36
Lecture 8. Muscular tissues ........................................................................................ 41
Lecture 9. Nervous tissue ........................................................................................... 46
Recommended literature .............................................................................................. 51

4
INTRODUCTION
The manual «Lecture notes on cytology and general histology» is made up in
accordance with the Federal State Educational Standard of higher education (FSES
HE) and the standard academic program on discipline «Histology, embryology,
cytology». It contains materials of the basic course units. The manual is aimed at
successful studying histology as a compulsory subject in medical education as well as
at the formation of the competencies necessary for future specialists:
1) ability and readiness to analyze socially significant problems and processes,
to use the methods of humanitarian, scientific, biomedical and clinical sciences in
various professional and social activities;
2) ability and readiness to realize ethical and deontological aspects of medical
activities in dealing with colleagues, medical staff and patients;
3) ability and readiness to conduct the morphological analysis of biopsy,
operative and sectional material and interpret the results;
4) ability and readiness to analyze the laws of functioning oforgans and
systems, to use knowledge of Anatomy and Physiology, and the basic methods of
assessing the functional state of the body of adults and teenagers;
5) ability and readiness to studythe scientific and medical information,
domestic and foreign experience on research topic;
6) ability and readiness to participate in mastering modern theoretical and
experimental methods of study with the view of creating new advanced means, in the
organization of works on practical use and implementation of study results.

5
Lecture 1.Subject of histology.Histological technique.Cytology
Histology
Histology is the science on the structure, development and life of tissues. The
course consists of 4 interconnected sections: cytology (the study of cells),
embryology (the study of the organism development), general histology (the study of
tissues), and private histology (the study of the microscopic structure of organs).
The methodological basis depends on one of the 3 approaches:
1. Systemic analysis: each structure is a complex system of interaction with
the systems of its level and with other systems.
2. Comparative evolutionary approach: the formation of the structure and
functions of organs is studied in their evolution.
3. Structural and functional approach: the relationship between the structure
and functions. The main METHOD is study of preparations with light microscopy.
TISSUE PREPARATION for light microscopy. Steps required in preparing
tissues for light microscopy include the following stages: tissue sampling, fixation,
dehydration and clearing, embedding, sectioning, mounting and staining the sections.
Tissue sampling.Tissue blocks (tissue samples cut <1 cm in each dimension)
may be obtained through biopsy (diagnostic sampling), surgical excision, or
postmortem dissection. To avoid misleading structural deterioration, postmortem
samples should be taken as soon as possible, and to minimize tissue distortion,
dissection instruments should be kept extremely sharp. The excised organ (sample)
must be immersed as soon as possible after removal, into a reagent known as a
fixative.
Fixation.Fixatives act to preserve the cells and extracellular substances of
tissues/organs and prevent autolytic (degenerative) changes, fixation refers to
treatment of tissue with chemical agents that not only retard alterations of tissue
subsequent to death (or after removal from the body) but also maintain its normal
structure. The most common fixative agents in light microscopy used in surgical and
general pathology as well as biomedical research is 10 % neutral buffered formalin
(4 % aqueous solution of formaldehyde).

6
Dehydration. The collected tissues, once fixed, are then dehydrated in graded
solutions of alcohol or other dehydrating agents, because a large fraction of the tissue
is composed of water, a graded series of alcohol baths, beginning with 50 % alcohol
and progressing in graded steps to 100 % alcohol, are used to remove water
(dehydration), following removal of the majority of water from the collected
specimen during dehydration, the tissues are cleared.
Clearing is a process of removal of dehydrated agent and replacing it with a
fluid that is miscible both with the dehydrating agent.There are a number of clearing
reagents, the selection of which is dependent largely on the embedding medium
chosen. Xylene is routinely used for clearing tissues. The alcohol-permeated block is
passed through several changes of this solvent to replace alcohol with xylene, in
paraffin embedding tissues are treated with xylene or other clearing reagents.
Embedding. The tissue is placed in a suitable container of melted paraffin until
it is completely infiltrated, once the tissues become completely saturated, melted wax
occupies spaces formerly occupied by water. After the tissue is impregnated with
paraffin, it is placed into a small receptacle, covered with melted paraffin, and allows
hardening, forming a paraffin block containing tissue.
Sectioning. After the formed paraffin blocks together with the contained tissues
are trimmed of excess embedding material, they are mounted for sectioning on a
cutting device called a microtome. Sectioning is performed by a microtome, a
machine equipped with a blade and an armthat advances the tissue block in specific
equal increments. For light microscopy the thickness of each section is about 4 to 7
mcm. In general, the thinner the section, the less is the likelihood that its components
will appear superimposed. The optimal thickness of LM section (5–8 mcm) is less
than the diameter of a typical cell. The edges of the thin shaving (sections) coming
off the microtome knife adhere to one another, producing a long ribbon from which
single sections may readily be detached. The cut sections are then transferred onto the
warm water bath and mounted onto the surface of clean glass microscopic slides.
Paraffin sections mounted (places) on glass slides are then stained by water-soluble
stains that permit differentiation of the various cellular components. Sectioning can
also be performed on specimens frozen either in liquid nitrogen or on the rapid-freeze

7
bar of a cryostat, these sections are mounted by the use of quick-freezing mounting
medium and sectioned at subzero temperatures by means of a precooled steel blade
the sections are placed on precooled glass slides, permitted to come to room
temperature, and stained with specific dyes (or treated for histochemical or
immunocytochemical studies).
Staining.Because many tissue constituents have approximately the same optical
densities, they must be stained for light microscopy: aqueoussolutions are usually
used in staining. Prior to this, the wax must be removed (dissolved) and replaced with
water. This is accomplished by passing the slides together with their mounted
sections through xylene or toluene to remove paraffin. Then through descending
strengths of alcohol solutions to water, as most of the dyes used are in aqueous
solutions. Although various types of stains have been developed for visualization of
many components of cells and tissues, they may be grouped into three classes:
1) stains that differentiate between acidic and basic components of the cell;
2) specialized stains that differentiate fibrous components of the extracellular
matrix;
3) metallic salts that precipitate on tissues forming metal deposits on them.
The most commonly used stains in histology are hematoxylin and eosin
(H & E).Hematoxylin is a base that preferentially colours the acidic components of
the cell a bluish tint, because the most acidic components are deoxyribonucleic acid
(DNA) and ribonucleic acid (RNA).The nucleus and regions of the cytoplasm rich in
ribosomes stain dark blue; these components are referred to as basophilic. Eosin is an
acid that dyes the basic components of the cell a pinkish color, because many
cytoplasmic constituents have a basic pH, regions of the cytoplasm stain pink; these
elements are said to be acidophilic.
After dyeing the tissue is placed a conservative (fir balsam) and the coverslip.
It not only protects the tissue from damage, but also is necessary for viewing the
sections with the microscope. This medium minimizes refraction of the light passing
through the section.
Cytology

8
The cell is an elementary living system and the basis of the structure,
development and life of all living organisms. The cell consists of a nucleus and a
cytoplasm and is covered with the cell membrane (cytolemma).
The nucleus regulates all cell functions. The cytoplasm contains permanent
structures (organelles) and temporary structures (inclusions). The cell form and
structure are adapted to the cell functionto the maximum.
One of the constituents of most cell structures is the elementary cell membrane.
It is a lamellated formation, which has no loose ends and folds into vesicles, cisterns
and tubes. The membrane contains 60 % of proteins, 32 % of phospholipids and 8 %
of lipids.
The phospholipid has a hydrophilic head made of glycerophosphate and two
hydrophobic tails composed of two fatty acids. Therefore, phospholipids always form
a bilipid layer. The bilipid layer has bilipid-associated membrane proteins. There are
three types of them: peripheral (located at the membrane surface), half-integral
(partially incorporated in it) and integral (trans-membrane proteins). According to the
functions there are structural receptor proteins, transporters and enzymes. Proteins
can move and roll, so the membrane surface and function are changed. Elementary
membrane structures of different cells have different properties because they contain
different proteins.
The cytolemma consists of 3 layers:
− the middle layer – elementary (outer) membrane: glycocalyx;
− the submembrane (inner) layer: contains microtubules and microfilaments,
which take part in the cell movement.
The glycocalyx is formed by carbohydrate chains projecting on the outer
surface which are connected with the membrane lipids and proteins. It has a
protective function and is involved in the recognition of external signals. The
glycocalyx limits penetration of water into the cell, regulates intracellular pH and
adsorbs substances to be phagocytosed. Its glycoproteins are the cell receptors and
molecules which recognizethe foreign cells. The glycocalyx thickness, chemical
composition and functions are different in different cells.
The cytolemma functions:

9
1. The barrier function limits free diffusion of substances.
2. The protective function.
3. The receptive function.
4. The synthetic function: membrane proteins have enzymes which catalyze
the synthesis and decomposition of substances.
5. The cell movement function: forms processes to move a cell.
6. The transporting function: transport of substances – passive and active. Gas
and water diffusion occurs passively, without energy. Active transport, with the use
of energy, occurs in three ways: 1) by means of the protein carriers (K-Na-pump), 2)
by endocytosis – transport of the absorbed substance by cytolemma processes (solids
– by phagocytosis; liquids – by pinocytosis), 3) by exocytosis – removal of
substances from the cell.
7. The formation function: formation of special constant structures on the cell
surface.
On the free surfacethe cytolemma forms special organelles, such as cilia and
microvilli. The microvilliincrease the absorption surface. They have a microduct
inside surrounded with the actin filaments which are able to suck different
substances. They can form a striated borderin the small intestine. The cilia are
produced by the cell center and are able to move. They have an axis from
microtubules with the basal body (modified centriole) inside.
On the basal surface there are cells transporting substances through the basal
surface.The basal cytolemma forms deep folds and mitochondrial accumulation
between them. It is called thebasal striation.
On the lateral surfaces of the cells the cytolemma forms 3 groups of cell
junctions:
1) mechanical ones, which firmly connect cells (lock-type junctions,
interdigitations, simple junctions by glycocalyx, desmosome and half-desmosome);
2) isolating junctions which prevent penetration of ions and molecules and are
formed by bonding of the integral proteins of neighboring cells (a tight junction, a
belt clutch);

10
3) chemical, information gap junctions which are of two types: 1 – nexus, in
which integral proteins form interplasm channels and small molecules; ions permeate
through it; 2 – synapse, which is a junction between neurons with unilateral
transmission. Tumor cells have no special structures on the cell surface.
The cell nucleusconsists of nucleolemma, nucleoplasm, chromatin (DNA
genes), enzyme proteins, nucleolus (synthesis of ribosome units). Nucleus
functionsare:
1) to preserve the information about an organism (in genes);
2) to implement this information (by means of the protein synthesis);
3) to reproduce information for a new organism.
The cytoplasmconsists of two parts: 1) the structural part – comprises
organelles and inclusions, and2) thehyaloplasm (cytosol) –it is asolutionwhich
consists of 90 % water and 10 % organic matter and mineral salts. In the cytosol
glycolysis and synthesis of fatty acids, nucleotides and amino acids takes place. All
other metabolic processes take place in the organelles.
The organelles are constant cell structures carrying out certain functions. They
are divided into general and special. General organelles can be membrane and
nonmembrane.
The membrane organelles are the mitochondriа, endoplasmic reticulum, Golgi
complex, lysosomes, peroxisomes.
The nonmembrane organelles are the microtubules, myofilaments, ribosomes,
cytocenter.
The special organelles are on the cell surface (cilia, microvilli) or in the
cytoplasm (myofibrils, tonofibrils, neurofibrils).
Reproduction of cellular structures.The mitochondria and cell center have their
own DNA and ribosomes and can renew their own proteins. The mitochondria are
reproduced by budding. The cell center produces microtubules. All organelle proteins
are synthesized in ribosomes by the nucleus DNA. The ribosomes are formed in the
nucleolus. The endoplasmic reticulum and Golgi complex produce lysosomes and
peroxisomes. Golgi complex produces membrane vesicles to restore all membranes.

11
Inclusions are temporary cell structures; there are four groups of them:
1) secretory – protein, mucous, steroid (lipoid) ones in the glandular cells;
2) excretory – insoluble salts formed during metabolism and then removed
from the cell;
3) trophic – proteins, fats and carbohydrates (in the form of glycogen),
vitamins;
4) pigmentary – products of cell exchange or disintegration (red hemoglobin,
black melanin, brown hemosiderin, red myoglobin).
Noncellular structures. They are cell derivatives. There are 2 groups of them:
supracellular and intracellular substance.
The supracellular structures are symplasts and syncytium. They are formed of
thecomplex of cells, are always multinuclear and much larger than the cell. The
symplastis formed by merging of cells to perform the function. Symplasts are the
skeletal muscle fiber,formed by merging of myosatellites, and osteoclasts (bone
destroyers), formed by macrophage merging. The syncytium isformed in the result of
incomplete cell division, when the affiliate cells remain connected by cytoplasm
bridges (syncytiotrophoblasts in the placenta).
The intracellular substance is produced by the cell: synthesized inside the cell
and secreted into the extracellular environment. It is much simpler than the cell,
consists of fibers and a fundamental amorphous substance.
Questions for self-control:
1. What does histology study?
2. What doescytology study?
3. What are the main components of the cell?
4. What are the functions of cytolemma?
5. What are the membrane and nonmembrane organelles of the cell?
6. What non-cellular structures do you know?
7. What special cell organelles do you know?

12
Lecture 2.Differentiation of embryonic material.Life cycle.Differons. Tissue formation
General Histology
The tissue is a historically developed system of cells and non-cellular
structures possessing the structural generality and performing certain functions.
Tissue development, or histogenesis, is the formation of atissue embryo and its
transformation into the mature tissue. Tissues are formed at the end of embryogenesis
gastrulation as a result of differentiation of embryonic material.
Embryogenesis is preceded by PROGENESIS when male and female gametes
are produced by meiosis: spermatozoa – in the testes, ova – in the ovaries. The sperm
and ovum merging during fertilization produces the zygote, a unicell germ.
EMBRYOGENESIS consists of some stages: fertilization, cleavage,
gastrulation, histogenesis and organogenesis. Embryogenesis stages correspond to 4
periods of differentiationof embryonic material:
1. Ovotypical differentiation is the formation of presumptive germs in the
zygote. The zygote moves cytoplasm parts (ovoplasm segregation). The cytoplasm
with a lot of mitochondria will become a part of the embryo’s body cells. Areas with
a lot of yolk will become provisional organs.
2. Blastomere differentiation (in cleavage) is the formation of
blastomeresdiffering from each other. Cleavage is the mitotic zygote division into the
blastomeres which do not grow; it takes place under the fertilization membrane.
Blastomeres have different cytoplasm contents. At first the embryo is a dense cell
ball – morula. The morula size is not increased and is equal to the zygote size. Then
blastomeres secrete a liquid into the morula and form a single-layer bubble –blastula.
3. Germinal differentiation (in gastrulation) is the formation of tissue embryos
from the same blastomeres. Cells are reproduced by mitosis, differentiate, migrate
and form an embryo of 3 germ layers: ectoderm, entoderm, mesoderm. Gastrulation
has 2 stages. Atthe first stage all blastomeres of thegerminal disc are dividedat the
same time and split into two layers: inner, the hypoblast which is the future entoderm,
and outer, the epiblast which contains the ectoderm material, mesoderm, achord and
aneural tube. At the second stage epiblast cells migrate and form the primary streak
with the groove ending of the primary (Hensen) bundle with theprimary pit. It is the

13
chord and themesoderm germ. The epiblast cells lying before the Hensen bundle form
the head chord and theneural plate. The chord influences the neural plate which turns
into the neural tube. The chord and the neural tube are axial organs.
4. Tissue differentiation(histogenesis) is theformation of tissue from tissue
germs. The germ tissue differentiation is expressed in different cell needs: some
genes are excluded from the transcription process but others remain active.
Differences in the cell and tissue metabolism develop.
The epiblast above the neural tube is called the dermal (skin) ectoderm; it
produces the stratified squamous epithelium of the skin, cornea, oral cavity and anus.
The mesoderm can be dorsal (back) and ventral (abdominal). The dorsal
mesoderm is segmented into somites. The ventral mesoderm splits into 2 layers:
parietal (near the ectoderm) and visceral (near the entoderm). Between them the
celom (thesecondary cavity of the body) is formed. The ventral mesoderm and the
celom form splanchnotom. It is connected with the somites by means of segmented
legs that form nephrogonotom – the germ of the urinary and genital systems. The
ventral mesoderm layers form serosa – peritoneum.
The internal peritoneum layer grows together with the wall of internal
organs.The external layer forms the abdominal wall. The somitesdifferentiate into 3
germs: dermatom– the germ of the skin connective tissue, sclerotom– the skeletal
tissue germ (cartilages, bones), myotom – the skeletal muscle germ.
The cells with processes (expelled from all the germinal layers, basically from
the mesoderm, and filling all intervals between the germinal layers) form the
embryonic tissue – mesenchyme. It is the source of development of the connective
tissue, vessels, blood, lymph and smooth muscle tissue.
The embryo’s body formation begins with the trunk folds which are formed by
the ectoderm and parietal layer of themesoderm. These folds bend under the embryo
and separate the embryo’s body from not embryo’s organs.
Then histogenesis and organogenesis begin – tissues are formed from tissue
germs and organs develop from them. There are 5 groups of tissues: epithelial, blood
and lymph, connective, muscular and nervous.
All processes of embryogenesis pass in thestrict sequence under the influence
of the embryonic induction.

14
The influence of some parts of the embryo (inductors) on other parts (reacting
systems) is called the EMBRYONAL INDUCTION.The inductor determines the
direction of the reacting system.
There are 2 types of induction:
1)homotypic – the development according to the inductor type during the germ
tissue formation;
2)heterotypic – the development according to the type differing from that of
theinductor during organs formation (for example, the chord induces the development
of the nervous tube). The inductor may influence in two ways: by contact with the
reacting system cells, and remotely, secreting substance which activates certain genes
in the reacting system cells.
Cell differentiation is a two-stage process:
1. Determination is determining the direction of differentiation. This phase is
a latent (hidden) and reversible process, the cell changes only its properties and
synthesizes specific proteins. If the inductor is changed, the cell can change the
direction of differentiation.
2. Differentiation is an irreversible stage when the cell acquires special
structural and functional features.
In the process of differentiation of thespecialized cell several cell generations
can replace each other and form a series of differentiation – differons.
The differon consists ofindifferent cells–pluripotential and polipotentialstems,
progenitor cells, adeterminate cell – aunipotential«-BLAST»and adifferentiated cell –
aspecific mature cell«-CYTE».
DESTRUCTION of mature differon cells in embryogenesis occurs due to
apoptosis, in postembryonic period – due to necrosis and apoptosis. NECROSISis
cell destruction under the influence of external factors. In the cell the lysosomes are
activated, after whichcariolysis (nucleus dissolution)and then autolysis occur (cell
dissolution and disintegration). The disintegration products induce inflammation.
APOPTOSIS is the programmed cell destruction under the influence of endocellular
factors. The lysosomes are not activated, and the suicide-programmed genes join. The
Са level in the cell rises, and the cell breaks up into apoptosis bodies surrounded by

15
the membrane. They don’t cause any inflammation, and are entirely phagocytized by
macrophages.
The differons are preserved during all life of the organism and provide tissue
renewal. The induction of cell differentiation occurs in the same way – by contacting
with the reacting systemor distantly.
Under the influence of external factors the regulation of duplication and
differentiation in the tissue can be broken, the cells lose special properties and
multiply infinitely, causes development of tissue metaplasiaand tumors.
Properties of tissues:
1. Organic specificity. Tissues have different needs in oxygen and nutrition.
Different tissues have different metabolism rates.
2. Ability for regeneration. Tissues have ability for physiological regeneration
(renewing) and reparative regeneration (restoration after damage). If differons are
present in tissues, the regeneration occurs quickly and completely. For example the
epithelium, blood, connective tissue are quickly restored, the skeletal muscular tissue
– worse, the nervous tissue – very badly (only processes), the cardiac muscular tissue
is not restored at all.
3. Variability or plasticity of tissues adapts the organism to the changed
conditions and reflects the process of ageing. Adaptation is expressed in the change
of tissue metabolism, sizes of cells and their quantities. If adaptation is impossible,
disadaptation and metaplasia of the tissue take place. Age-related changes of tissues
are expressed in decreased metabolism and regeneration, a reduced quantity of cells
and an increased amount of the intercellular substance (for example, vascular
sclerosis).
Questions for self-control:
1. What is the tissue?
2. What types of tissues do you know?
3. Name 4 periods of embryonic materialdifferentiation.
4. What is gastrulation? Name the stages of gastrulation.
5. What is embryonic induction? Name its types.

16
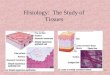
Lecture 3.Epithelial tissue
The epithelial tissue (epithelium) is the cellular tissue that lines the organ
cavities, covers the body surface and forms the glands. The basic features of
epitheliumare as follows:
1. Cells form a continuous layer.
2. The connective tissue always lies under the epithelium. It carries out a
trophic and protective functions.
3. Epithelium is located on the basement membrane which unites all epithelial
cells into a layer, separates the epithelium from the connective tissue.
4. Epithelial cells are differentiated in a polar manner. The basal pole is
attached to the basement membrane. The apical pole is turned to the environment.
The apical surface can have special organoids.
5. Epithelium has ability for regeneration.
The covering (lining) epithelium is the intermediary between the organism
and the environment. It carries out 3 functions:
1) a barrier between the organism and the environment;
2) elimination (pushes foreign particles out of the organism);
3) protection (protects from the mechanical, chemical, thermal, radiation
injuries and microbial invasions). Epithelial cells make a secretion component which
binds the IgA and transfers it onto the epithelial surface where the IgA interferes with
duplication of microbes.
Classification.There are simple and stratified epithelia. In the simple epithelia
all cells are connected with the basement membrane (1 – squamous (flat), cuboidal,
columnar, 2 – pseudostratified (nuclei at different levels)). In the stratified epithelia
(many cell layers) only thebasal layer of cells is connected with the basement
membrane: 1 – stratified, squamous, keratinized (epidermis), 2 – squamous,
nonkeratinized, 3 – transitional (urothelium).
The secretory epithelium synthesizes biologically active substances and
secretes them onto the surface of the covering (lining) epithelium or into the blood.

17
The secretory cycle of the secretory cell consists of 3 phases:
1) absorption of initial substances from the blood for secretion synthesis;
2) synthesis and accumulation of the secretion;
3) removal of the secretion.
The glands remove the secretion in3 ways:
1. The merocrine type – removing the contents of the secretory granules only,
without cytolemma destruction. It is characteristic of the digestive and most sweat
glands.
2. The apocrine type – a part of the cellular top together with the secretory
granule comes off. It is characteristic of the mammary and some sweat glands.
3. The holocrine type – secretory cells are destructed completely, and their
components make up secretion. It is characteristic of the adipose glands of the skin. It
consists of the stratified epithelium: the basal layer contains dividing cells, the middle
layer – the cells accumulating secretion, and in the center of the secretory portion the
destructed cells lie.
Secretory cells may be placed in the epithelium between other cells. Scattered
secretory cells are the unicellular glands, for example the goblet cell secreting mucin.
Many cells comprise specialized exoepithelial glandslying in the connective
tissue under the epithelium. If secretion is discharged from the gland to the surface of
the covering epithelium, the gland is called exocrine. If secretion is discharged from
the gland into the blood, the gland is called endocrine. Glands develop from the
epithelium covering them.
Exocrine glands produce serous and mucous secretion and consist of the
secretory part and the duct. The classification takes into account their structure.
Glands with only one duct are called simple glands. If a gland has a large duct
divided into many small ductules, it is called a complicated gland.Glands with only
one secretory part are called undiverged (unbranched) glands.Glands with many
secretory parts are called diverged (branched) glands.The form of the secretory part
may betubular, alveolar (acinar) ortubuloacinar.

18
Endocrine glands produce special substances, hormones, and discharge them
into the blood, lymph or tissue. These glands have no ducts. The form of the
secretory parts may be of 2 types: 1 – follicular (thyroid gland) and 2 – trabecular
(compact and reticular) constructed from the epithelial trabeculae (hypophysis,
adrenal glands).
TISSUES OF MESENCHYME ORIGIN
Mesenchyme is the embryonic tissue made of mobile cells with processes and
ajellylike intercellular substance. Mesenchymal cells form germs. Germs are
developed in different tissues: blood, lymph, connective tissues, smooth muscular
tissue. They consist of cells and anintercellular substance, have uniform stem cells
and a big variety of cells, and perform the supporting, trophic and protective
functions, possess ahigh variability, as well as ahigh ability for regeneration and
adaptation. In young people they contain more stem cells and water and less fiber,
regeneration proceeds quickly.
BLOOD refers to the blood systemwhich includes 3 parts: 1 – blood producing
organs (the haemopoietic organs make blood cells, the liver – plasma proteins), 2 –
peripheral blood and lymph, as well as blood cells in tissues; 3 – blood destroying
organs (the spleen and the liver). Blood is an intravascular liquid tissue made up of
structural elements and liquid intercellular substance – plasma. In adults blood makes
6–8 % of the body weight, in newborns – 13–15 %, in children till 14 years old –
9 %. Blood functionsare as follows:
1 – trophic (delivery of nutrients),
2 – excretory (excretionof metabolic products),
3 – respiratory (exchange of О2 and СО2),
4 – protective (phagocytosis, immunity),
5 – humoral regulation (delivery of hormones, amines, etc.),
6 – homeostatic (constant concentration of water, gases, ions, temperature).
Blood consist of structural elements and plasma. Blood plasmamakes up 55–
60 %, its рН is 7,36. Plasma contains 90 % of water and 10 % of solids including
6,6–8,5% ofproteins (ofmore than 200 kinds). The main proteins are albumins 4–

19
4,5 %, globulins 2–3 %, fibrinogen, prothrombin 0,2–0,4 % and complement
proteins. All of them, except G-globulin, are synthesized in the liver. Albumins
transfer medicines, bind poisons and can serve as nutrition. α- and β-globulins are
transport proteins, G-globulins (antibodies) are produced by plasmocytes, bind
viruses and other antigens. Fibrinogen and prothrombin are proteins of blood
coagulation. Complement proteins are necessary for phagocytosis, etc.
The structural blood elements include about 99 % of erythrocytes, and about
1 % of leukocytes and platelets (thrombocytes). In the course of blood analysis the
hemogram is made. The hemogram includes the basic parameters: hematocrit (Ht,
the number of formed elements) – 30–35 %, the number of erythrocytes – 4–
5,5*1012/l(=per liter of) blood; leukocytes – 3–10*109/l; platelets – 130–400*109/l;
hemoglobin (Hb) – 130–160 g/l; erythrocyte sedimentation rate (ESR) – 4–20 mm/h.
THROMBOCYTES are not cells, but denuclearized fragments of red bone
marrow cells – megacariocytes. The size of the platelet is 2–3 microns, the form is
oval, may have appendices. A thrombocyte has 2 parts: 1) aperipheral glass-like
hyalomere(contains many microtubules), 2) acentral basophilic granulomere
orchromomerewith many granules containing histamine, serotonine, thromboplastine,
enzymes, regulatory proteins, Са and Mg ions.During activation of blood coagulating
factors thrombocytes stick together (agglutination), discharge the contents of
granules and start up thereactions of blood coagulation. If the number of platelets is
less than 40*109/l blood cannot coagulate. They live for 9–10 days, after whichare
destructed in the spleen and lungs.
ERYTHROCYTES are oxyphilic denuclearized cells without organelles,
containing 60 %of water and 40 % ofpigmentary protein (hemoglobin). In the norm a
person has 2 types of Hb: HbА(in adults – 98 %) and HbF (fetal, in newborns –
80 %). Hb is oxidized into the red oxy-Hb by the air oxygen (it forms the arterial
blood). In tissues lacking oxygen the oxy-Hb dissociates into the free oxygen and
desoxy-Hb of thecherry color (it forms the venous blood). Atpoisoning with
carbonmonoxide the Hb forms proof carboxy-Hb, oxygen does not enter the tissues.
This leads to hypoxia and death. Except for oxygen, erythrocytes transport

20
antibodies, amino acids, medicines, toxins. The Rhesus factor proteins and blood
group are built in the erythrocyte cytolemma as well.
Normal blood contains:
1) 0.2–1 % of young erythrocytes arereticulocytes (in newborns – 3–5 %)
with a low Hb level and a basophilic net from the residues of organelles; they become
mature in 2–3 days in the blood;
2) 80–90 % of erythrocytes are discocyteswhich have the form of a biconcave
disc. The other10–20 % have a different form and are called poikilocytes. An
increase in the number of poikilocytes is called poikilocytosis;
3) 75 % of erythrocytes are normocytes with the diameter of 7–8 microns.
25 % of smaller or larger erythrocytes are called microcytes and macrocytes. An
increase in their number is called anisocytosis. It arises at poisoning and at a blood
loss due to the discharge of large young erythrocytes into the blood from the bone
marrow.
The quantity of erythrocytes depends on the organism’s need in oxygen. In
men it is 3,9–5,5*1012; in women – 3,5–5*1012; in newborns and old people – 6–
8*1012. During a day 1 % of erythrocytes are renewed. These cells live for2–3 months
only in the vessels, are destructed in the spleen. In hypotonic medium they become
dropsical, and hemolysis occurs.
Questions for self-control:
1. Name the types of epithelium.
2. Describe the classification of the covering epithelium.
3. Describe the classification of the glandular epithelium.
4. What types of glandsecretion do you know?
5. Name the tissue of the mesenchyme origin.
6. What main components of blood do you know?

21
Lecture 4.Leukocytes
LEUKOCYTESare colorless and mobile cells with a nucleus and organelles.
Leucocytes move from blood into tissuesand perform theprotective function. In adults
the number of leukocytes is 4–10*109per liter ofblood, in newborns – 10–30*109, in
children 6–22*109. All leukocytes have fine nonspecific basophilic granularity that
are lysosomes. A part of leukocytes called granulocyteshave specific granularity. The
granulocytes cannot be divided. They are definitive forms with a segmented
nucleus.The leukocytes called agranulocytes do not have specific granularity. Some
forms of agranulocytes are able to divide.
The percentage of different leukocytes in blood is called the leukocyte formula.
There are 3 kinds of granulocytes: basophiles – up to 1 %, eosinophiles – 1–5 %,
neutrophiles – 45–75 %. Agranulocytes are of 2 kinds: lymphocytes – 20–35 % and
monocytes – 3–8 %. In newborns the proportion of cells is like in adults. On the
6thday after birth the number of neutrophiles and lymphocytes changes (1stchiasm),
and theblood is lymphocellulartill 5 years of age. Then at the age of 5 the 2ndchiasm
occurs, and the proportion of leukocytes gradually becomes like in adults.
All granulocyteshave a segmented nucleus.
Neutrophileshavea d =10–12 microns, the nucleus forms 3–5 segments, the
cytoplasm consists of a lot of glycogen and has a very small granularity: 10–20 %
nonspecific basophilic, 80–90 % specific oxyphilic. Basophilic granules are
lysosomes. Theycontain acid hydrolyzing enzymes and myeloperoxidase. Specific
granules contain lysocim,lactoferrin, alkaline phosphotase, alkaline proteins –
thusthey are oxyphilic.
Blood contains neutrophiles of different maturity degree: joung – up to 1 %
with a bean-like nucleus, band-nuclear – 1–5 %, segmento-nuclear – 40–70 %. In
women the nucleus chromatin has Barr’s body. It is a sex chromatin shaped like a
drum-stick. The functions of neutrophilesare the following:
1) phagocytosis of microorganisms;
2) destruction of bacteria and damaged tissues due to inflammation by means
of secretion of lysosomal enzymes and oxygen superoxide;

22
3) disintoxication: peroxidase decomposes peroxide into water and oxygen
which oxidizes toxins.
Neutrophiles live 3–8 days in tissues and 8–12 hours they spend in blood.
During inflammation neutrophiles absorb much oxygen and form a lot of peroxide
and superoxide oxygen, which destroy bacteria. It is called a respiratory burst.It
happens only 1 time. Then neutrophiles die and form pus, and the bone marrow
intensifies emission of new neutrophiles in blood. The neutrophil (leucocytosis)
arises, the number of band-nuclear cells in blood increases and the leucocyte formula
shifts to the left. It means that the reserves of the red bone marrow are not exhausted,
andthe prognosis is favourable. When hemopoesisisdamaged,bloodneutrophiles
become old, their nuclei become hypersegmented, the reserves are exhausted, and the
prognosis is unfavourable.
Basophileshave a diameter of 11–12 microns. The nucleus is segmented,
andthe cytoplasm has large metachromic (lilac) granules that contain histamine,
heparin, anaphylaxine. Histamine increases permeability of vessels and tissues,
phagocytosis and contraction of smooth myocytes. In allergy basophiles throw out
much histamine; this causes microhypostases and a spasm of smooth myocytes. It
leads to the development of skin hives, rhinitis, conjunctivitis, bronchial asthma or
allergic gastroenteritis. Heparinis the antagonist of histamine. It binds histamine,
reduces allergy and coagulation of blood. Anaphylaxine is a complex of proteins
which causes Quincke’sedema (hypostasis) during allergy.Functions of basophiles
are the following:
1) disintoxication(peroxidase);
2) decrease blood coagulation (heparin);
3) increase vascular and tissue penetration (histamine),
4) development of allergic reactions (histamine, anaphylaxine). Basophiles
spend 1–2 days in blood; their life span is unknown.
Eosinophileshavea d=12–15 microns, the nucleus forms 2–3 segments. In their
cytoplasm there are large acidophil granules with lamellar crystals. These granules
contain some enzymes such as histaminase, collagenase, arilsulfatase, peroxidase.

23
Lamellar crystals are those ofthearginin-rich alkaline protein, the major basic protein
(MBP) which acts to kill parasitic helminthes. Functions of eosinophiles are the
following:
1) antiparasitic (MBP);
2) disintoxication (peroxidase);
3) antiallergic (histaminase);
4) participation in scar formation (collagenase).
Eosinophiles live 8–14 days and 3–8 hours they spendin blood. Atallergy or
parasitic diseases eosinophiliadevelops:the number of eosinophiles in blood
increases. In stress eosinopeniadevelops: eosinophiles get out of blood into a tissue,
their number in blood sharply decreases.
Agranulocytes are monocytes and lymphocytes. They areimmunocompetent
cells and participate in the immune response.
Monocytes are the largest blood cells, 18–20 micronsin diameter. The nucleus
is C-shaped or round. The cell has much weak basophilic cytoplasm and contains
lysosomes. They spend 1,5–4,5 days in blood where they carry out 2 functions:
1) phagocytosis;
2) participation in the immune response.
They move into a tissue and turn into macrophages. Monocytes are precursor
cells of macrophages, bone osteoclasts, microglia of the nervous tissue, and other
cells of the mononuclear phagocyte system.
Due to the ability of cells for phagocytosis the phagocyte theory of immunity
was created. Recently the cloning-selection theory of immunity has been offered. The
immune response is a specific reaction of an organism directed at the destruction of
genetically alien substance – antigen (bacteria, viruses, parasites and mutant cells).
All cells of the organism have identified proteins in their cytolemma which are called
the1st class major histocompartibility complex (MHC). These proteins are unique for
each organism. Immunocompetent cells(macrophages and lymphocytes) have
proteinsof the2nd class MHC. In the immune response monocytes and macrophages
can recognize the antigen by the absence of the1st class MHC. Then they transport the

24
antigen to the lymphocytes; they are called antigen-representing cells or A-cells.
Moreover, A-cells discharge cytokines which activate lymphocytes and other cells.
Some of them,such as interleukins, interferons, the tumor necrosis factor (TNF),
cause a rise in the temperature.
Lymphocytes have a round dense nucleus and basophilic cytoplasm with
ribosomes and lysosomes. In newborns and adults there are 20–35 % lymphocytes, at
the age of 1 year – 55–60 %, at 5 years – 45 %. Lymphocytes differ in size and
functions. By the size they are divided into small (80–90 %), middle (3 %) and large
(5–10 % in adults, up to 20 %in children). Small lymphocytes have a d=4,5–7
microns and a narrow line of basophilic cytoplasm around a very dense nucleus.
Middle lymphocytes have ad=7–10 microns; there are more cytoplasm than in small
lymphocytes, andthe nucleus is lighter. Large lymphocytes have a d=10–16 microns,
much weaker basophilic cytoplasm with well visible basophilic granularity.
According to the modern theory of immunity, clones of lymphocytes
programmed to destroy certain antigens are formedin the organism. There are 2 types
of immune response: 1– humoral immunity –binding antigens by antibodies, 2 –
cellular immunity – destruction of AG-cells.
By function lymphocytes are divided into 3 groups: natural cell-killers (NK),
thymus-dependent Т-lymphocyteswhich create the cellular immunity and bursa-
dependent B-lymphocytes which create the humoral immunity. Т-and B-lymphocytes
are externally identical but have different receptors – clusters of differentiation (CD).
NK (zero and CD-16,56,57)are large granular lymphocytes, formed from stem
cells in the red bone marrow and probably in the liver, whichlive for a long time. The
cytoplasm contains a lot of lysosomes, and sometimes in activation of NK oxyphilic
granules with protein-perforin appear in the cytoplasm. NKs identify and kill cancer
cells.
Т-lymphocytes are divided into 4 types. Т-helpers and Т-suppressors are
constantly formed in the thymus. T-killers and T-memories are formed in the spleen
and lymph nodes from Т-suppressors. Т-helpers (Тh-CD4 +) accept АG from A-cells,
determine the way of its destruction and start the humoral or cellular immune

25
response (when affected with the Human Immunodeficiency Virus, HIV). T-
suppressors (Тs-CD8) suppress the immune reaction. If their number is not enough,
allergy develops. If there are a lot of them, a tumor develops. They move into the
spleen and lymph nodes where under the action of АG they start blasttransformation
– the transformation of lymphocytes to lymphoblasts to multiply and make T-killers
and T-memories. T-memories (Тm-CD8 +) remember AG and identify it during its
secondary appearance in the organism. T-killers (Тk-CD8 +) kill the cells of atumor,
transplants, bacteria, etc. by secreting FNT (lymphotoxin) and perforins.
B-lymphocytes are divided into 3 types. In the bone marrow B-naive (В0, CD-
19–23) ones are formed. They migrate in the spleen and lymph nodes where under
the action of АG they start blast transformation, multiply and form plasmocytes and
B-memories. Plasmocytes secrete antibodies (immunoglobulins, Ig) which bindАG
(viruses). B-memories remember AG and identify it during its secondary appearance.
В-and T-memories live for a long time, T-killers and plasmocytes live some
days. The blood contains more Т-helpers and T-memories (70–80 % of all
lymphocytes) and less B-memories (10–20 %). The number of lymphocytes increases
in blood at chronic infections, intoxications (tuberculosis, chronic inflammation) and
decreases in stress that provokes development of an allergy or a tumor.
The immune response requires cooperation of A-cells and lymphocytes, and
develops in 5 stages:
1. АG Identification –an A-cell (macrophages) meets and captures АG by
means of phagocytosis.
2. Representation of АG to Т-helpers – an A-cell splits АG into fragments
and releases them in the internal environment where they contact receptors of Т-
helpers (СD4+). Тhs-1 are responsible for the cellular immunity, Тhs-2 – for the
humoral immunity. After the contact with АG Тh-1 secretes cytokines which act on
Ts (CD8.) Тh-2 grasps АG, forms AG-receptor complexes and releases them in the
internal environment where B-naive lymphocytes recognize and catch them.

26
3. Blast-transformation – Cytokines and АG-receptor complexes cause the
transformation of Т-suppressors and B-naive lymphocytes intoТ- or B-lymphoblasts
in the peripheral lymphatic organs.
4. Cloning of specific (to certain АG) lymphocytes – Т-lymphoblasts multiply
and make a lot of T-killers and T-memories. B-lymphoblasts multiply and make a lot
of plasmocytes and B-memories.
5. AG Destruction – T-killers kill alien cells (by FTN and perforins), thus
creating the cellular immunity. Plasmocytes secrete Ig (antibodies) to localize АG,
forming immune АG-АB (antigen-antibody) complexes, thus creating the humoral
immunity.
At the repeated appearance ofАG in the organism the secondary immune
response develops, in which the blast transformation is caused by both A-cells and
memory-lymphocytes. NKs don’t participate in cellular cooperation.
Questions for self-control:
1. What types of leukocytes do you know?
2. What are the leukocyte formula and hemogramm?
3. What are the functions of granulocytes?
4. What are the functions of agranulocytes?
5. What is immune response? Name the types of immune response.
6. Name the stages of immune response.

27
Lecture 5. Hematopoiesis
There are 2 types of hematopoiesis:
1) embryonic – it is histogenesis, the formation of blood like a tissue;
2) postnatal – it is physiological regeneration, renewal of blood.
EMBRYONIC HEMATOPOIESIS begins in the yolk sac mesenchyme where
the first stem cells (SC) which originate the blood cells and vessels are formed. Later
SC migrate through the vessels into the embryo`s body – first into the liver and then
into the thymus, spleen, lymph nodes and bone marrow.
During the 2nd–3rd weeks of the development the mesenchymal cells form
blood islets in the wall of the YOLK SAC. In the islet center the cells lose their
processes and differentiate into hematopoietic stem cells. On the islet periphery the
cells are flattened and form vascular walls: theendothelial, smooth muscle and
connective tissue layers.
Hematopoiesis begins intravascularlywithin the blood vessels. The
erythrocytes are the first to appear;theydeliver O2 to the fetus. Some SC differentiate
into primary erythroblasts. They are large cells, 18–20 micronsin diameter, with
basophilic cytoplasm and a light nucleus with large nucleoli. Some of them divide
and differentiate into basophilic erythroblasts accumulating a lot of RNA. They stop
dividing, just differentiate, their size does not change. They begin Hb synthesis. As
Hbis accumulates the cytoplasmic basophilia decreases and oxyphilia increases, the
cytoplasm is stained with azure and eosin. The cells become polychromatic
erythroblasts and then oxyphilic erythroblasts. Their nucleus is wrinkled
(karyopycnosis), and then it is broken down into pieces and pushed out of the cell
(karyorhexis). Sometimes the nucleus remains. Giant primary erythrocytes
(megalocytes) are formed, nuclear and non-nuclear. This is megaloblastic
hematopoiesis – rapid production of erythrocytes which are large anddo not pass
through small blood vessels and die in 2–3 days.
At the same time here is normoblastic hematopoiesis – a longer production of
small long-lived erythrocytes. Some primary erythroblasts give birth to the
secondaryerythroblasts. They are divided and form basophilic normoblasts that give

28
birth to polychromatic normoblasts. They can divide as well, and by accumulating
Hb they turn into oxyphilicnormoblasts. With each division the daughter cells
become smaller than the mother cells– that is why the oxyphilicnormoblast is small.
After the nucleus is pushed out the cell turns into the small secondary erythrocyte.
Granulocyte formation in the yolk sac occurs outside the vessels,
extravascularly.Out of the vessels some mesenchymal cells are rounded; they
accumulate nonspecific grains – lysosomes, then some cells accumulate specific
acidophilic grains, the others – neutrophilic grains. In such a wayneutrophiles and
eosinophiles are formed. They pass through the vessel wall into the blood.
Some SC of blood islets are transported with the blood into the hematopoietic
organs of the embryo`s body, there hematopoiesis is performed extravascularlyas
well. By the 4th–5th weeks of embryogenesis the yolk sac is reduced, and the LIVER
becomes the organ of hematopoiesis. It produces blasts from SC. Erythrocytes,
eosinophiles, neutrophiles and megakaryocytes are formed from the blasts passing the
same stages. Megakaryocytes produce platelets. The THYMUSis laid during the 4th–
6th weeks, SC populate,and T-lymphocytes develop from them. In the SPLEENand
LYMPH NODES at first all kinds of blood cells except for basophiles are formed, but
during the 16th week when the T- and B-lymphocytes populate in SC they produce
only lymphocytes. The BONE MARROW is laid at two months of developmentand
SC populate. First they form bone cells forming the bone, and during the 3rd month
hematopoiesis begins in bone cavities. First erythrocytes and granulocytes are
formed, and then other blood cellsdo. From the second half of embryogenesis the
bone marrow becomes the main hematopoietic organ. Thus, from the 2nd–3rd weeks of
embryogenesis the following cells consecutively appear inthe blood: erythrocytes,
eosinophiles and neutrophiles, platelets, monocytes and lymphocytes, and only after
birth – basophiles.
By birth hematopoiesis stopsprocessing in the liver, but other organs retain the
hematopoietic function throughout life.
POST- EMBRYONIC HEMATOPOIESIS. It is physiological regeneration of
blood. The bone marrow is the universal hematopoietic organ, which stores SC

29
reserves. In the thymus the T-cells (helpers and suppressors) are formed. In the
spleen, lymph nodes and lymphoid follicles of the mucosa the final forms of T- and
B-lymphocytes develop.
The stroma, a hematopoietic organ, is a support for hematopoietic cells and
consists of the reticular connective tissue and reticular epithelium in the thymus. The
stromal cells have processes and form a network (reticulum), where loops of
hematopoietic cells are arranged. In different hematopoietic organs stromal cells
create a special microenvironment and direct the development of SC to a certain way.
Stromal cells are able to absorbdefective and dead cells by phagocytosis and to
control the output of mature cells into the bloodstream. Immature blood cells have
antigenic proteins in their cytolemma. Stromal cells recognize immature blood cells
by means of these proteins, bind them and do not release them into the bloodstream.
In the process of maturation of the blood cell the cellular cytolemma is reorganized
and deprived of antigenic properties, so the cell is released into the bloodstream.
When leucosis develops this control is disrupted, so the blasts with antigenic
cytolemma come out into the blood, whichescalates the disease.
The monophyletic theory
The founderof the monophyletic theory, Maksimov, was the first who
suggested that all blood cells are formed from SC morphologically similar to small
lymphocytes. This was confirmed in the experiments that showed that SC form
colonies of various blood cells inthe tissue culture.
SC are pluripotent cells. They proliferate and form two major lineages of
progenitor polypotent cells (half-stem cells, HSC) – lymphoid cells (for
lymphopoiesis) and myeloid cells (for other blood cells). From these, under the action
of colony-stimulating factors (CSF) 7 unipotent progenitor cells are formed; they are
called colony-forming units (CFU):
1) CFU-GM – gives progeny of CFU-M (monocytes) and CFU-Gn
(neutrophiles);
2) CFU-Eo (eosinophiles);
3) CFU-B (basophiles);

30
4) CFU-Meg (megakaryocytes);
5) CFU-E (erythrocytes);
6) pre-T- cell (T-lymphocyte);
7) pre-B-cell (B-lymphocyte).
SC, HSC and GFU are morphologically identical. Under the influence of the
microenvironment and hematopoietins the unipotent cells (CFU) form blasts, which
are morphologically identical as well; they differ only in the set of enzymes. In
several stages blasts mature into the final forms – cytes.
Erythropoiesis is performed around the macrophages which bring Fe into the
bone marrow. The CFU-E reproduction is stimulated by erythrocyte decay products
and erythropoietin produced in the kidneys and liver in response to hypoxia.
Formation of the erythrocyte is performed during 7–10 days in the following stages:
proerythroblast, basophilic erythroblast, polychromatic, oxyphilic erythroblasts,
reticulocyte, and erythrocyte. All blasts except for oxyphilic ones are divided by
mitosis, in each generation to follow the cell size is reduced. 1 % erythrocytes, up to
300 billion cells, are produced per day. There are 2 types of erythropoiesis. The 1st
type – homoblastic erythropoiesis – normal, when new erythrocytes are formed from
oxyphilic erythroblasts. The 2nd type – heteroblastic erythropoiesis – pathological
(after a blood loss or hemolysis), when erythrocytes are formed from different
erythroblasts (oxyphilic and polychromatic).
Granulocytopoiesis (myelopoiesis) is stimulated by granulopoetins (CSF, IL-
3, IL-4 for basophiles, IL-5 for eosinophiles). Development of the granulocyte occurs
within 14 days and progresses in the following stages: myeloblast, promyelocyte, 3
types of myelocytes (basophilic, eosinophilic, neutrophilic), 3 types of
metamyelocytes (basophilic, eosinophilic, neutrophilic), band-nuclear granulocytes,
and segmented-nuclear granulocytes. Promyelocytesaccumulate non-specific
granularity (lysosomes) in the cytoplasm. Myelocytes accumulate specific
granularity. After each division the cells become smaller. Metamyelocytes stop
dividing and then only differentiate. Up to 5 billion granulocytes are produced per
day. In homoblastic (normal)myelopoiesismyelocytes develop from

31
promyelocytesand in heteroblasticmyelopoiesis (after ablood loss) myelocytes
developed from myeloblasts.
Thrombocytopoiesisis stimulated by thrombocytopenia and thrombopoietins
produced in the liver. Within 10 days giant megakaryoblasts are formed in the
promegakaryocyte stage. Megakaryoblasts are up to 40–120 microns in diameter, the
cytoplasm fragments with granules (platelets) are separated from them. During cell
division only nuclei divide, and then merge again in thetelophase. As a result, each
cell grows in size and becomes a polyploid cell.
Monocytopoiesis isstimulated by CFS of monocyte-macrophages.
Monocytopoiesis progresses in 3 stages: monoblast, promonocyte, monocyte. The
promonocyte accumulates lysosomes withnon-specific granularity.
Lymphocytopoiesis. It is a two-stage process. Stage 1 – antigen-independent,
held in the central organs – the bone marrow and thymus. The pre-B-cell remains in
the bone marrow, and the pre-T-cell migrates to the thymus. They form lymphoblasts,
then prolymphocytes, then B-naïve lymphocytes in the bone marrow, and T-helper
and T-suppressor lymphocytes in the thymus. Stage 2 – antigen-dependent, takes
place under the influence of antigens in the peripheral hematogenic organs where T-
suppressor and B- naïve lymphocytes are transformed into T-lymphoblasts and
plasmoblasts. They proliferate and form prolymphocytes and proplasmocytes, from
which T-killer and T-memory, B-memory and plasma cells are formed. Production of
T-lymphocytes is stimulated by IL-2, IL-4, IL-6, and that of B-lymphocytes – by the
same IL and IL-5.
NK cells are presumably produced in the bone marrow and liver.
Questions for self-control:
1. What types ofhematopoiesis do you know?
2. What is megaloblastic hematopoiesis?
3. What is normoblastichematopoiesis?
4. What is the essence of the hematopoiesistheory?

32
Lecture 6.Connective tissues
Connective tissues consist of cells and intercellular substance, the amount of
which is more than that of cells.
Classification.Connective tissues are divided into 2 groups: proper connective
tissues and skeletal ones. Proper connective tissues are divided into fibrous tissues
and those with special properties. A fibrous tissue can be loose and dense. Dense
tissues are divided into regular and irregular. Tissues with special properties can be of
3 types: reticular, adipose, mucoid. Skeletal tissues are divided into cartilage tissues
and bone tissues. Cartilage tissues are of 3 types: hyaline, elastic and fibrous. Bone
tissues are of 2 types: reticulo-fibrous and lamellar.
The functionsof connective tissues:
1. Basic – make capsules of organs, tendons, fascia, and skeleton.
2. Trophic – metabolism between blood and cells.
3. Protective – a mechanical protection, durability of organs, phagocytosis by
macrophages, participation in inflammation and immunity.
4. Hemopoietic – a microenvironment for hemopoietic cells.
5. Plastic – adaptation of the organs at changing conditions due to metabolic
changes, participation in regeneration.
LOOSE FIBROUS CONNECTIVE TISSUE
The loose fibrous connective tissue consists of different cells and intercellular
substance which is developed by cells called fibroblasts. Intercellular substance
consists of basic substance and fibers.
Basic (amorphous) substance is a gel-formed colloid system from water, salts
and organic substances: glycoproteins, glycosaminoglycans (GAG) and
proteoglycans. Glycoproteins are proteins connected with oligosaccharines.
Theyconnect cells with fibersand are divided into soluble and insoluble structural,
species-specific. Proteoglycans areproteins connected with GAG. GAG are sour high-
polymer combinations, synthesized by fibroblasts. 5 groups of GAG are
distinguished. 4 groups are sulfated, connected with proteins,and are constituents of
proteoglycans: chondroitinsulfates A, B, C, dermatansulfates, keratansulfates,
heparansulfates and heparin. The 5thgroup is not sulfated– it ishyaluronic acid. It has
the highest molecular weight, can be free and combined with proteins. GAG
determine permeability ofthe tissue for water and solutions. Hyaluronic acid is

33
hydrophilic, binds much water, and stimulates metabolism, phagocytosis, duplication
and mobility of cells. Its amount is large in young organisms. Chondroitinsulfates are
hydrophobic, inhibit cell duplication and regeneration; with age their quantity
increases. Heparin blocks phagocytosis, metabolism, duplication and mobility of
cells, permeability of tissues, coagulability of blood, but activates disintegration of
fibrin and fats. The breach of theGAG ratio in thetissue leads to the impairment of
fiber formation and development of collagenosis (rheumatism, scleroderma).
Fibers of the connective tissue are presented by 3 kinds: collagenic, elastic and
reticular.
Collagenic fibersare very strong, oxyphilic, tape-like, do not anastomose, lie
freely, slightly twisting. Collagenic fibers are constructed of tropocollagen-protein
which consists of triplets of amino-acids. In each triplet the first amino-acid is
glycine, the second is proline or lysine, the third varies in different types of collagen.
Fibroblasts synthesize tropocollagen and secrete it into the intercellular environment.
Then, with the participation of acidic GAG, it is polymerized into fibrils. Since
tropocollagen molecules being displaced 1/4 of the length relative to each other,
fibrils are cross-striated. Fibrils are combined collagenic fiberswith the thickness of
1–12microns. A fibroblast creeps along the fiber with the help of shoots and
completes it at length and thickness. A young organism has a lot of hyaluronic acid,
so the fibers are thin and long. Anold organism has a lot of heparin,so the fibers are
short and thick. Vitamin C deficiency blocks tropocollagen formation. Defects of the
bones and teethappear. The regenerative process of wounds and broken bones is bad.
Now many types of collagen are known. Despite that, 5 of them are the most
principal. The 1st type collagen forms thick fibers and is present in the connective
tissue, bones and teeth; the 2nd type collagen forms thin fibers in cartilages and
vitreous body of the eye; the 3rd type is found in the reticular and loose collagen
tissue; the 4th type is in basal membrane of the epithelium; the5th type is in the basal
membrane of the endothelium.
Reticular fibers have thickness of 1 micron, arecomposed of the 3rd type
collagen, covered with neutral glycoproteins, not stained by eosin, but impregnated
with silver. They are resistant to acids, alkali and enzymes, branch, anastomose
andtwine the cells. Their amount is large in the stroma of hemopoetic organs, in
thesmooth muscle tissue, mucous layer, basal membranes.

34
Elastic fibers are formed from protein elastin and stained withorsein. They are
thinner and lighter than collagenic fibers, less strong, well-stretching, rectilinear,
branching and anastomosing. They are destructed only by elastase, their elasticity is
provided by the derivative amino acids – desmosine and isodesmosine.
THE CELLS of the connective tissue are various and mobile. Main resident
cells (living in a tissue) are fibroblasts, histiocytes and labrocytes. Resident cells
which are small in number are low differentiated cells, lipocytes, melanocytes. There
are endotheliocytes in vessels. Plasmocytes and leucocytes are brought by blood.
During the immune response lymphocytes, plasmocytes, eosinophiles, basophiles
prevail, and at aninacute inflammation –neutrophiles. Plasmocytes have a dense
nucleus and basophilic cytoplasm which contains a light «yard» near the nucleus, that
is the site where Goldgicomplex is located.
Fibroblasts are builders of the connective tissue. Their main function is
synthesis and secretion of basic substance, collagens and elastine. Mature fibroblasts
are large cells, d=40–50 microns, with shoots. The nucleus is light oval witha
nucleolus. The cytoplasm is poorly basophilic; there are well-developed ER and
inclusions. The contours of the cell are indistinct.
Fibroblasts are divided into 5 types:
1) low differentiated(multiples and differentiates) fibroblasts are small (20–25
microns), have few organelles, do not synthesize basic substance and fibers;
2) mature fibroblasts are larger (40 mcm), build fibers and basic substance;
3) fibroclasts which destruct fibers;
4) myofibroblasts have myofilaments and can shorten when a scar is formed;
5) fibrocytes are the final form with a very dense nucleus.
Labrocytes are histobasophiles. The form is oval. The sizes are different,
thenucleus is light, in the cytoplasm there are up to 1000 metachromatic (lilac)
granules with histamine, heparin, etc. (as in basophiles of blood). These cells
influence properties and functions of tissues, regulate permeability of vessels and
tissues, coagulability of blood, synthesis of the basic substance, and participate
indevelopment of allergy.
Histiocytesare macrophages. It is phagocytes formed from blood monocytes.
The form of the cell is oval or extended, the contours are precise, the edges have
irregular short pseudopodia. The nucleus is dense, compact, oval, the cytoplasm is

35
lysosome-rich and poorly basophilic, finely vacuolized (foamy). The functions of
macrophages are: phagocytosis of bacteria (innate immunity), secretion of lysozyme
and the enzymes lyzing diedoff tissues, removing diedoff structures from the
organism, release endogenic water during fat splitting. They are A-cells in the
immune responseand performcytokines secretion.
The inflammatory reaction of the organismis carried out by the loose collagen
tissue together with blood leukocytes.
When the tissue is damaged,labrocytesare the first to react and throw out the
granules intothetissue, histamine increases permeability of capillaries for blood
plasma and leukocytes. Plasma isaccumulated in the tissue and creates inflammatory
edema which separates the inflammatory focus from the healthy tissues and does not
allow the products of disintegration to spread about the organism.
Neutrophilesare the first to come to the focus of thedamage. They throw out
much oxygen superoxide, lysosomal enzymes and contents of specific granules into
the tissue and then die. Oxygen superoxide and lysozyme destroy bacteria, cation-
proteins increase the edema, and lysosomal enzymes destroy the damaged tissue. This
phase of inflammation is calledthe leukocytic phase(or the acute period).
Thenthe macrophagicphase follows. Macrophages come to the focus of the
damage, phagocyte the bacteria and the products of tissue disintegration, completely
clearing the focus of inflammation.
The fibroblastic (reparative) phase begins. Fibroblasts are actively made
multiple copies, they form a fibroblastic capsule around the cleared site of the
damage and secrete basic substance and collagen of the 1st type from which thick
fibers filling the tissue defect are formed. Vessels grow into the capsule, and the
granulation tissue composed of thick, rough collagen fibers and vessels is formed.
Within the next 6 months a rough scar is gradually reconstructed, andthick 1st type
collagen fibers are replaced with thinner 3rd type collagen fibers.
Questions for self-control:
1. What are the connective tissue components?
2. Describe the classification of the connective tissues.
3. Name the connective tissue functions.
4. Name the cell composition of the connective tissue.
5. What types offibers do you know?
6. What types ofcollagen do you know?

36
Lecture 7.Skeletal connective tissues
There are two types of skeletal tissues: cartilage (hyaline, elastic, fibrous) and
bone (reticulo-fibrous, lamellar) tissues.
THE CARTILAGE TISSUEhas no vessels, consists of intercellular substance
and 2 kinds of cells – chondrocytes and chondroblasts. The extracellular matrix
consists of collagen, elastic fibers and basic substance. It easily lets water and
solutions pass through it, provides the cartilage tissue with density and elasticity. Due
to high tissue density chondrocytes lie in cartilage capsules, can multiply, but do not
disperse forming isogeneic groups. Due to it the interstitial growth of the cartilage,or
the growth from within, occurs. Perichondrium contains 2 layers – theexternal fibrous
layer and theinternal chondrogenic layer with chondroblasts. They multiply and make
new young chondrocytes. Due to it the appositional growth of the cartilage, or the
growth from the outside, takes place. The cartilage regenerates slowly through the
connective tissue scar.
According to the structure of the extracellular matrix the cartilages are divided
into 3 types. Hyaline cartilage is glass-like, transparent, and basophilic. The fibers
are so thin that they are not visible andmade up of the 2nd type collagen. It contains
chondroitine sulfates A and C binding Са carbonate, so thatthe cartilage can calcify.
The hyaline cartilage lies on the articular surfaces of bones, in the walls of the
respiratory ways. In theembryo it makes up the entire skeleton. The elastic cartilage
is yellowish, less transparent, weakly oxyphilic, contains many elastic fibers and
chondroitine sulfate B. It does not bind Са, so it does not calcify. The elastic cartilage
is present in the ear auricles, acoustic passages, auditory tube, cartilages of the larynx
and middle bronchi. The fibrous cartilage is present in the intervertebral discs and in
the places of attachment of tendons and bones. It contains thick bundles of collagenic
fibers turning into a tendon or bone.
THE BONE TISSUE is a calcified tissue composed of three major cell types
and calcified bone matrix consisting of 67 % of salts and 33 % of organic substances.
There are collagenic fibers and a little basic substance in organic substances. In
embryos the osteoblasts build bones, and in adults – renew them. They lie on the

37
surface of bone structures. The cells are large, 18–20 microns, have different forms,
thenucleus is light, the cytoplasm is basophilic with well-developed organelles and a
high activity of alkaline phosphatase which forms the insoluble Ca phosphate. The
functions of osteoblastsare:
1) synthesis of basic substance and collagen;
2) calcification of the bone matrix. While forming the bone matrix, they
immure themselves and become osteocytes.
Osteocytes have bodies and processes. Their bodies lie in bone lacunae formed
in the calcified bone matrix. Their processes are in the canaliculi connected by
anastomosis and forming the tissuedrainage system. Osteocytes are low active, the
nucleus is compact, organelles are few in number and the cytoplasm contains
glycogen. The function of the osteocytes is tissue metabolism. Osteoclastsare
multinuclear symplasts. They lie on the bone structure surface. Osteoclasts are
formed by merging of macrophages and have many lysosomes. Their function is bone
destruction, so they appear at the places of reconstruction and regeneration of bones.
All bone cells are formed in the result of division of osteogenic cells of the
periosteum.
Classification. Bone tissuesare divided into reticulo-fibrous (woven bone) and
thin-fibrous (lamellar bone). The woven bone tissue contains thick collagenic fibers.
If collagenic fibers lie in parallel, the tissue is called trabecularor rough-fibrous. If
collagenic fibers lay chaotically, the tissue is called spongy orreticulous. This tissue
is usually temporary and is present in the spongy bones in embryos, in the cranial
bone junctions in adults, at the attachment places of tendons and bones, at places of
bone regeneration. Inthe thin-fibrousor lamellar tissue collagenic fibers are thin and
regulated like plates. This tissue makes up the skeleton of an adult person.
STRUCTURE OF THE BONE. The bone is covered with the periosteum made
up of 2 layers: 1 – outer fibrous, from thedense connective tissue with vessels and
nerves; 2 – innerosteoprogenitor, from theloose collagen tissue with osteoprogenitor
cells. These cells are able to proliferate and are divided into osteoblasts and
osteoclasts for theappositional bone growth or repair.

38
The bone substance from bone plates can be spongy or compact.
The spongy substance forms plane bones and epiphysis of long bones, consists
of bone trabeculae and large bone cavities between them with a red bone marrow. In
the trabeculae bone plates overlap each other like a tile.
The compact substance forms thick walls of the diaphysis of the tubular bones.
It consists of strictly focused bone lamellae, forming 3 layers. The 1stlayer is that of
external general (circumferential) lamellae, the 2nd layer is thick osteon one, the
3rdlayer is that of internal general (circumferential) lamellae which turns into the bone
trabeculae of thespongy substance in the epiphysis. From inside the bone is covered
with thin endosteum composed of the loose tissue with osteogenic cells. The layers of
external and internal general lamellae cover the bone entirely.
The osteon layer is constructed from osteons – Haversian systems. The osteon
is a functional unit of the compact bone, whichconsists of cylindrical bone lamellae,
inserted one inside another. Collagenic fibers of neighboring lamellae lie in
quadrature, they provide the bone with hardness. Between the lamellae in the cavities
there are osteocytes. In the center of the osteon the Haversian canal passes with
vessels and mesosteum composed of theloose tissue with osteogenic cells. From
theoutside every osteon is surrounded with a cement linecomposed of basic
substance. Canaliculi with osteocyte processes do not pass through the cement line,
so the osteon’s nutrition is independent, closed. If the Haversian canal vessels
compress, the osteon dies. The mesosteum cells form osteoclasts destroying this
osteon and osteoblasts which start to build a new osteon from the cement line to the
center. A young osteon has a wide canal,while an old osteon has a narrow one. Then
vessels compress again, and the osteon collapses. Thus, physiological regeneration of
the bone takes place. Between the osteons there are interstitial lamellae, remnants of
lamellae from old osteons. Nutrition of osteons is performed through periosteum
vessels lying in the perforating (Volkmann) canals.
The growth and regeneration of bones depends on vitamins and hormones. The
excess of parathyrin and vitamin A causes bone resorption (fibrous ostitis may
develop). Thyrocalcitonin and sex hormones stimulate calcification, and vitamin D

39
deficiency inhibits it. Thyroxin and somatotropic hormone activate collagen synthesis
by osteoblasts, and vitamin C deficiency inhibits it.
The bone tissue develops in 2 ways: 1 – direct osteogenesis from mesenchyme
or intramembranous ossification; 2 – indirect osteogenesis at the place of a
bonecartilage model or endochondral ossification. At first the bone tissue is rough
fibrous, then it is reconstructed into thin fibrous (plates) bone tissue.
Direct osteogenesis is characteristic of plane bones and has 4 stages.
Mesenchyme cells form condensation («membranes»).
Stage 1 is the formation of the ossification centers within these membranes,
secretion of intercellular substance.
Stage 2 is differentiation and histogenesis. Within the ossification center the
cells are differentiated into osteocytes, and around the center – into osteoblasts. These
masses grow and form osteoid trabecules.
Stage 3 is mineralization. Osteocytes and osteoblasts secrete alkaline
phosphatase, which provides the formation of insoluble Ca phosphate which is
deposit trabeculae in the bone, and the woven tissue is formed.
Stage 4 is reconstruction.Osteoclasts destroy the woven tissue, and osteoblasts
build osteon plates around the vessels. The lamellar tissue is formed.
Indirect osteogenesis (endochondral ossification)is development of the bone on
the cartilage place. It is characteristic of almost all bones of the skeleton. At the
2ndmonth of embryogenesis blood circulation increases in the cartilage model
diaphysis. Oxygen induces differentiation of chondroblasts into osteoblasts, and the
perichondrium is reconstructed into the periosteum. Osteoblasts build thewoven bone
tissue on the hyaline cartilage which covers the diaphysis and forms a perichondrial
bone collar (kaff). It interferes with feeding of chondrocytes: they become dystrophic
and destruct under the collar. Remnants of the died off cartilage calcify, andthe
diaphysis ossification point (or primary ossification center)is formed. Vessels and
themesenchyme grow into it from the periosteum. Osteoclasts and osteoblasts are
formed from the mesenchyme. Osteoclasts destroy the died off cartilage, thus a cavity
is formed. Osteoblasts build endochondrial bone trabeculae on the cartilage
remnants. The ossificationline between the cavity and the cartilage is formed. Along

40
this line osteoclasts constantly destroy endochondrial bone trabeculae, and
osteoblasts build new trabeculae. Therefore, the ossification line is displaced to the
epiphysis. The bone cavity increases and the red bone marrow fills it. On the border
with the ossification line cartilage continues to collapse, forming the cellular
cartilage zone. Behind this zone the cartilage continues growing, but the bone collar
interferes with its growth to the sides. Therefore, multiplying chondrocytes build
columns, forming thecolumnar cartilage zone. Thereare 3 zones, i.e.the
endochondrial ossification line, the cellular cartilage zone and the columnar cartilage
zone.They form a meta-epiphysial growth plate.Due to this plate the bone grows at
length. The growth of the bone`s thickness occurs due to the increasing thickness of
the perichondrial bone collar.
Due to the growth of the bone collar onto the epiphyses, the epiphysis
ossification points (secondary ossification centers) are laid in them where bone
trabeculae are formed. The epiphysis ossification moves towards diaphysis
ossification. During puberty (under the influence of sex hormones) ossification is
performed more quickly than multiplication of the growth plate cartilage. The plate
soon ossifies, and the bone stops growing (by about 20 years of age). The
endochondrial bone completely collapses, and the perichondrial bone is reconstructed
from the woven bone into the lamellar bone. This process goes especially actively in
the first 3–6 months of life. The osteons appear during the 4th month. The periosteum
is thick and rich with vessels, especially around the growth plate where pathologies
(osteomyelitis, tuberculosis, rickets) often develop.
Questions for self-control:
1. What are the cartilage tissue components?
2. Describe the classification of the cartilage tissue.
3. What are the bone tissue components?
4. Give the classification of the bone tissue.
5. Name thecartilage cells and their functions.
6. Name thebone cells and their functions.
7. What osteogenesis types do you know?

41
Lecture 8.Muscular tissues
The mainfunctionof muscular tissues is to contract, providing the movement.
The structural elements of muscular tissues have some general features:
1) the extended form;
2) special organelles – myofibrils and myofilaments in sarcoplasm, lying
along the cells or fibers;
3) glycogen and myoglobin inclusions (monomer Hb, red, capable to bind and
emit О2);
4) two-layer sarcolemma (cytolemma covered with the basal membrane).
Classification. There are 2 kinds of muscular tissue: smooth and striated (or
cross-striped). The smooth tissue develops from the mesenchyme, except for the
specialized kinds developing from the neuroectoderm (the iris muscles) and ectoderm
(myoepithelial cells of the glands). The striated tissue develops from the mesoderm; it
can be skeletal and cardiac.
CROSS-STRIPED (striated) SKELETAL MUSCULAR TISSUE.It makes up
the muscles of the trunk, extremities and head. It contracts deliberatelyand quickly,
but gets tired quickly. It develops from somite myotomes. Their cells turn into
myoblasts which multiply and merge into the symplasts – muscular tubules. In their
cytoplasm myofibrils are formed, and the basal membrane of sarcolemma is formed
above thecytolemma. A part of the myoblasts turns into low-differentiated cells –
myosatellites. They settle down between the cytolemma and the basal membrane of
sarcolemma. A nerve ending connects with each myosymplast.
The structure of the myosymplast.Its thickness is 20 microns, the length – from
2 to 12 cm, the number of the nuclei – up to ten thousand (they are oval and lie under
sarcolemma). Up to 1000 myofibrils lie in the center along the myosymplast.
Between them there is glycogen, myoglobin, mitochondrions and atubule of
sarcoplasmic reticulum which deposits Ca-ions. The sarcoplasmic reticulum tubules
form circular tanks around the light disks of myofibrils which contact with the
cytolemma tubule. It is necessary for the muscle contraction and is called the T-
system.

42
Myofibrils consist of proteins and myofilaments.
Proteins, constructing the myofibril,include 4 groups:
1) contracting proteins – actin and myosin,
2) regulating proteins – troponin and tropomyosin,
3) structural protein – α-actinin,
4) elastic proteins – titin and nebulin.
Myofilaments, constructing the myofibril, consist of chains from actin and
myosin. Myosin molecules have myosin bridgesmade of lateral chains with the head
composed of ATP (orof the side chains with the head of the ATP). Thin actin
molecules are partially blocked with thick myosin molecules. This creates cross-
striped fibers in the form of altering dark and light disks. The Light disks contain one
kind of proteins – actin, whichdissipates light equally. Therefore, they are called
isotropic or I-disks. In the middle of light disks there is a septum – a telophragmaor
aZ-linecontracted fromα-actininprotein. The Z-line crosses all parallel I-disks and is
attached to the cytolemma. It binds the myofilaments into the myofibril. In dark disks
actin and myosin are blocked. They dissipate light in different ways, so dark disks
possess double refraction and are calledanisotropic or A-disks. In the middle ofan A-
disk there is a light H-band without actin. M-line is amesophragmawhichpasses
through it. The structural and functional unit of themyofibril is SARCOMERE. It is a
section of themyofibril between two Z-lines (an A-disk andtwo halves of I-disks).
The mechanism of muscular contraction is explained by the theory of actin
sliding along myosin. Contraction is regulated by the ATP energy and Са and Mg
ions. Са starts contraction, releasing a site of actin binding. Mg is necessary for
splitting the АТP. From the motor nerve ending excitation passes to the myosymplast
cytolemma, andthen through the T-system to the sarcoplasmic reticulum membranes.
Са leaves it and starts contraction. Myosin contacts with actin by means of myosin
bridges. Theactomyosincomplexis formed,where myosin bridges bend and pull actin
filaments to the A-disk center. So, actin filaments slide along myosin ones to the
sarcomere center, until Са or АТP concentration decreases. Z-lines approach and pull
the sarcolemma. The length of each sarcomere becomes as short as that of the A-disk,

43
and I-disks become invisible. The length of all muscular fibers is reduced. The
myofibrils become anisotropic along their length, andcross stripes disappear.
When nerve impulses stop, Са leaves for the cisterns, and myofibrils relax. It
demands energy. If theАТP is absent, relaxation does not come, anda muscular spasm
develops. Not all muscular fibers contract, but in stress or at physical exertion all of
them can start working.
The structure of the skeletal muscle.Astructural and functional unit of the
skeletalmuscle is amyon. It is amyosymplast with myosatellites, nerve endings and
capillaries. Between myons there is endomysium, around bundles of myons –
perimysium,and the muscle is covered with afascia (epimysium). Skeletalmuscles can
be red, white and mixed. Red muscles are weaker but hardier, contain more
myoglobin and mitochondrions, but less myofibrils and glycogen. White muscles are
strong, but get tired quickly. They have less myoglobin and mitochondrions but more
myofibrils and glycogen. The type of muscles is inherited (in sprinters they are white,
in long-distance runners – red).
Regeneration. At injuries myosatellites are released from the sarcolemma and
turn into myoblasts. Then they multiply and merge into tubules which turn into new
fibers. For complete regeneration it is necessary to join an additional nerve and to
give loading to inhibit scar formation. The sarcolemma basal membrane is formed at
7 years of age, and the whole fiber – at 12.
CROSS-STRIPED (striated) CARDIAC MUSCLE TISSUE. It makes up the
myocardium. It develops from the visceral layer of themesoderm. It consists of cross-
striped muscular cells – cardiomyocytes. These cells can be of 3 types:
1 –typicalcontracting,
2 –atypicalconductive –Purkinje’s cells,
3 – secretory endocrine (in the atrium).
Typical cardiomyocytes are red cells, have anacylindrical form, the length is
50–120 microns, the thickness is 15–20 microns. They have a lot of myoglobin and
mitochondrions. The cell has 1–2 nuclei in the center and myofibrils on theperiphery.
The myofibrils are constructed like those in the skeletal tissue.

44
A typical cardiomyocyte is a structural unit of the cardiac muscle tissue. The
cells are connected together into myofibers by intercalated disks. These are a
complex of cellular contacts; consist of desmosomes, digiform junctions and nexuses.
Digiform junctions bind cells mechanically.Nexuses are between desmosomes.
Myofibers form the cardiac syncytium by means of anastomosis. It is a functional unit
of themyocardium. The syncytium contracts simultaneously and with regular
intervals. Endomysium contains many capillaries and reticular fibers.
Cardiomyocytes have no stem cells; the myocardium is restored by scar formation.
Atypical conductive cardiomyocytes form the nodes and Purkinje’s fibers of
the conductive heart system. The fibers go between the myocardium and the
endocardium. The cells are light and large, contain much sarcoplasm and glycogen.
Myofibrils are thinand disordered. The T-system is absent.
Secretory endocrine cardiomyocytes are in the atriums, have few mitochondria
and myofibrils. These cells secrete atriopeptides into the blood.
SMOOTH MUSCULAR TISSUE. It develops from the mesenchyme in the
walls of the vessels and visceral organs. A structural unit of the smooth
musculartissueis asmooth myocyte. It has a spindle form, the length is from20 to 100
microns, and the thickness is from 2 to 20 microns. In the endocardium and uterus it
can have shoots and reach the length of 500 microns. The nucleus is stretched oval
and lies in the center. The cytoplasm has a lot of myofilaments, mitochondria,
myoglobin, andendoplasmic reticulum. Myofilamentsarethin andsmooth because they
do not form myofibrils. Myofilaments are formed from the chain of actin and myosin.
They are attached to each other and to the sarcolemma by means of dense bodies
from the structural proteins ofα-actinin and vinculin, connectedwith actin).
Contraction is started by Ca ions, but calmodulin protein is necessary in the
formation of the actomyosin complex. Actin filaments slide along myosin ones
towards each other, pull thesarcolemma, and the cell contracts.
The smooth muscle consists of myocyte bundles. Myocytes form bundles by
means of reticular fibers and nexuses. Abundle is a functional unit of smooth
muscles. The wholebundle contracts. The loose tissue layers between bundles form

45
endomysium. Bundles are united into a muscle by perimysium from the loose tissue.
The whole bundle is innervated with vegetative nerves branching in endomysium
and secreting neurotransmitters. They pass into the bundle and excite the cells.
Excitation is slowly transferred from one cell to another by nexuses, so the muscle
contracts slowly and involuntarily, and tiredness is low. There are two sources of
regeneration: 1 – low-differentiated perimysium and endomysium cells; 2 – smooth
myocytes which can multiply by mitotic and amitotic division. Under the increased
functional load (for example in the uterus during pregnancy) myocyte hypertrophy
(anincreased size of the cell)can develop.
Questions for self-control:
1. Describe the classification of the muscle tissue.
2. What groups of protein do myofibrils contain?
3. What is astructural unit of the skeletal muscle?
4. What is astructural unit of the cardiac muscle?
5. What is a structural unit of the smooth muscle?
6. Describe the mechanism of muscle contraction.

46
Lecture 9.Nervous tissue
The nervous tissue unites the organism into the whole. It consists of neurons
and theneuroglia. Neurons accept irritation, form a nervous impulse and transfer it to
other cells. Theneuroglia creates conditions for the neuron’s life.
Development.The nervous plate rolls over into the neural grooveabove the
chord. Its margins form the neural crest. Under it there is the neural tube. It is a germ
for the spinal cord and the brain. Above the neural tube the ectoderm closes, the crest
cells form the ganglion plate which is segmented into the spinal ganglions. Some of
its cells move and are differentiated forming:
1) sympathoblasts(vegetative neurons);
2) chromaffinoblasts (cells of the adrenal glands medulla and APUD-cells);
3) melanoblasts (melanocyte precursors).
In the lateral walls of the neural tube the cells form 3 layers: the internal
ependymal layer from ependymoblasts, the middle mantle layer – neuroblasts and
spongioblasts (astrocytes, oligodendrocytes), and the external layer– a marginal layer
from cell processes. After birth neurons do not multiply, died-off neurons are not
restored, but neuron processes can be restored.
The NEURON has a body and processes. The body (perikaryon) contains a
large light nucleus with nucleoli. The processes are of 2 kinds: dendrites and axons.
Dendrites can be numerous; they transfer impulses to the neural body. There is only
one axon (neurit) which transfers impulses from the neural body. The cytoplasm has
organelles and inclusions of melanin and lipofuscin. The granular endoplasmic
reticulum forms basophilic masses called Nissl substance(basophilic, chromatophilic,
tigroid substance); it is present in the body and dendrites, but never in the axon. It
synthesizes enzymes for synapsis. Disintegration of thetigroidsubstance is called
tigrolysis; it occurs when the neuron is overexcited. Special neuron organelles are
neurofibrils, a complex composed of neurotubules and neurofilaments. Their function
is bidirectional intracellular transport of substances. Anterograde transport moves
substances from the perikaryon to the synaptic terminals. Retrograde transport returns
substances from the processes to the cell body for the control of their integrity.

47
Atpathology neurofibrils are not revealed. The function of neurons is transferring
nerve impulses. The resting potential of the cytolemma is -60 mV. At excitation the
cytolemma changes the polarity, and its action potential is +50 mV. So the nerve
impulse appears and moves along the neuron processes as a wave of membrane
depolarization. The nerve impulse goes only in one direction: first along the dendrite,
then through the neuron body and along the axon.
Classification of neurons
By number of processesneurons are divided into 4 types:
1) unipolar, having only an axon (neuroblasts in an embryo);
2) bipolar, having one dendrite and one axon (in the olfactory organ, eye
retina, ganglions of the internal ear);
3) pseudo-unipolar, having a uniform basis for the dendrite and the axon
(sensory neurons in the spinal ganglion;
4) multipolar, having one axon and a lot of dendrites.
By function neurons are of 4 kinds:
1) sensory (afferent);
2) effectory (efferent) (motor and secretory);
3) associative (interneurons) (between sensory and motor neurons);
4) neurosecretory neurons (synthesis of neurosecretion and discharging it
through the axon terminals into the tissue, liquor or blood). There is a lot of them in
the hypothalamus nuclei.
The NEUROGLIA consists of micro- and macroglia.
The microgliais small macrophages with multibranch short processes. When
the tissue is damaged they are involved, and the cells become ordinary macrophages
(called granular spheres).
The macroglia includes 3 kinds of cells:
1) ependymocytescover the central canal of the spinal cord and brain
ventricles. The cells have cilia in the apical part for the brain liquor circulation and
long processes in the basal part to support the brain cells;

48
2) astrocytes are small cells with processes and a light nucleus, whose
functions are supporting, trophic and protective. Plasmatic astrocytes are placed in
the grey matter of the brain and have short branchy processes. Fibrous astrocytes are
placed in the white matter and have long smooth processes. The astrocytes contact
with the capillaries by processes and form thehemato-encephalon barrier possessing
selective permeability;
3) oligodendrocytesform sheaths of neurons on the periphery. Satellite
gliocytes form capsules around the neuron bodies in the ganglions. Lemmocytesform
Schwann sheaths around the neuron processes in the nerves. These cells carry out 5
functions: trophic, protective, phagocytosis of disintegration products, participation in
the transfer of the nerve impulse and in nerve regeneration.
The NERVE FIBER is a neuron process (the axialone), surrounded
withlemmocytes which form the Schwann sheath around the process. It acts as an
electrical isolator and protects the process from damages. The Schwann sheath can be
myelinated and non-myelinated.
Non-myelinated fibers are thin, 1–2 microns, the impulse passes slowly, 1–2
m/s. Lemmocytes cover the axial cylinder by means of their processes which close
and form mesaxon (the dual membrane). Lemmocytes often form arope likethe fibers
covering some axial cylinders which are separated only by a thin layer of the
lemmocyte cytoplasm. So, the non-myelinated Schwann sheath does not create
electrical isolation. Therefore, distribution of the nerve impulse on the neighboring
fibers and its generalization are possible.
The myelinated fiber is thick, up to 20 microns;there is only one axial cylinder.
The lemmocyte processes grow, extend, and the mesaxon is wound spirally on the
axial cylinder, forming the myelinated layer. The lemmocyte cytoplasm and
thenucleus are pushed aside to the periphery forming the neurilemma. The axial
cylinder and lemmocytes grow with different rates, and slanting fissures are visible in
the myelinated layer. These are the sites of myelin stratification; they are called
myelin clefts (Schmidt – Lantermann’sincisures). On impregnating with osmium
myelin is black. The myelin layer has small parts lacking myelin where the

49
lemmocytes connect witheach other; these parts are called Ranvier`s nodes (or nodal
gaps). The myelin consists of fat (phospholipids) and creates good electrical
isolation; the impulse is transferred precisely to destination. Under the myelin the
acting potential cannot arise. The impulse arises only in Ranvier`s nodes jumping
through the myelin. Therefore, the rate of its movement is high – 100 km/s.
The STRUCTURE of the NERVE. The nerve consists of bundles of
myelinated and non-myelinated nerve fibers. Large nerves unite many bundles of
fibers and are covered with the epineurium made of the connective tissue with
vessels. Each bundle of fibers is covered with dense perineurium. Inside the bundle
thin fibers of theloose connective tissue with capillaries form the endoneurium.
Under the perineurium there is a fissure with liquid called the perineural space. It
communicates with the brain liquor and can be «the infectiongate» which can invade
the brain.
Nerve REGENERATIONis possible. When damaged, the peripheral part of the
neuron process dies. Myelin breaks up forming myelin spheres. The lemmocytes
multiply and form a long compact cord – Biungner’s cord which reaches the nerve
endings. On the intact end of the process the thickening (the growth flask) is formed.
It grows into the lemmocyte cord and moves along it to the nerve endings building on
the neuron process with the rate of 0,5–5 mm/day.
The neural impulse is transferred from the neural receptor to organs by means
of the REFLEX ARCH. It is a chain of neurons. The first link of thereflex arch is the
sensory neuron, the second link is one or many interneurons, the third one is the
motor (or secreting) neuron. Reflex arches can be simple, made up of 2–3 neurons,
and complicated, composed of hundreds of neurons. The whole nervous system
consists of reflex arches. In the reflex arch the nervous impulse is transferred by
synapses.
SYNAPSEScan be axodendritic (transfer the impulse from the axon to the
dendrite), axosomatic (to the neuron body), axoaxonic (to the axon) or neural-
muscular(between the neuron and other effector cells in the organs). In humans
synapses are chemical, of theopen type, with a wide intracellular space (20

50
nanometers) calledasynaptic cleft.The impulse is transferred only in one direction by
means of chemical neurotransmitters. The synapse is surrounded with lemmocytes
heath and has 2 poles separated with the synaptic cleft. The presynaptic pole is the
thickening of the axon terminal; it contains a lot of mitochondrions and vesicles with
neurotransmitters. The postsynaptic pole is formed from the neuron cytolemma
accepting excitation and having receptors to the neurotransmitter and the enzymes
destroying it. The action potential stimulates discharge of one portion of
neurotransmitter from the axon into the synaptic cleft. It depolarizes the postsynaptic
membrane; the nerve impulse arises on it. The used neurotransmitter is destroyed by
the synaptic enzymes at once. That allows dosing the intensity of excitation.
The synapses can be excitatory and inhibitory. The excitatory synapses have
neurotransmitters: noradrenalin, dophamin, acetylcholin. They depolarize the
postsynaptic membrane, and the nerve impulse goes further. The inhibitory synapses
have neurotransmitters: glycine, GABA, opioid peptides. They hyperpolarize the
postsynaptic membrane up to the membrane potential of ˗90 mV, so the action
potential (+50 mV) cannot develop and the impulse does not go further. The
synapses are formed throughout the humanlife.
Questions for self-control:
1. What are the nervous tissue components?
2. Describe the classification of the neuroglia.
3. What are the functions of the neuroglia?
4. What neuron types do you know?
5. What kinds of nerve fibers do you know?
6. What synapses kinds do you know?

51
Recommended literature
Basic:
1. Wheaterʼs Functional histology:a textbook and colour atlas/ Ed. Barbara
Young, Geraldine OʼDowd, Phillip Woodford.–Ssixth edition. –Printed in the USA,
2014. –452 p.
2. Histology, Cytology and embryology: textbook / Ed. Y. I. Afanasiev. –
Public., add. andproces. – M.: Medicine, 2006. – 768 p.
3. Atlas of microscopic and submicroscopic structure of cells, tissues and
organs: Study guidance/ V. G. Eliseev, Y. I. Afanasiev, E. F. Kotovski, A. N.
Jackowski.– 5th publ., add. andproces. – M.: Medicine, 2004. – 448 p.: ill.
Additional :
1. Bykov V. L. Cytology and General histology. Functional morphology of
cells and tissues of human origin: a textbook /V. L. Bykov. – St. Petersburg: SOTIS
2007. – 520 p.
2. Garstukova L. G. Visual histology (General and private): textbook /L. G.
Garstukova, S. L. Kuznetsov, G. V. Derevyanko. – M.: MIA, 2008. – 204 p.
3. Histology: Atlas for practical exercises: textbook /N. V.Boychuk, R. R.
Islamov, S. L. Kuznetsov, Y. A. Chelyshev. – M.: GEOTAR-MEDIA, 2008. – 160 p.
4. Kuznetsov S. L. Atlas of histology, cytology and embryology: Atlas:
textbook/ S. L. Kuznetsov, N. N. Mushkambarov, L. V. Goryachkina. – 2 public.,
add. andprocess – M.: MIA, 2006. – 376 p.
5. Kuznetsov S. L. Histology, Cytology and embryology: textbook /S. L.
Kuznetsov, N.N. Mushkambarov. – M.: MIA 2007. – 600 p.

52
Educational edition
VasilievaLudmilaSergeevna Makarova Olga Alexandrovna DaduevaAlexandra Sokratovna
Lecture notes on sections «Cytology» and «General histology»
Study guidance