Embed Size (px)
Citation preview
LECTURE OUTLINE - PHYSIOLOGY OF THE KIDNEYS
KNOW BASIC ANATOMYGROSS STRUCTURE & MICROSCOPIC STRUCTURE
PROCESS OF URINE FORMATION1) GLOMERULUS FILTRATION
(intrinsic and extrinsic controls)2) TUBULAR REABSORPTION
(FROM TUBULES)3) TUBULAR SECRETION
(INTO TUBULES)
STUDY MECHANISM OF EACH
WHAT IS ABSORBED AND IN WHAT PART
COUNTERCURRENT MULTIPLIER SYSTEM
ADH COLLECTING DUCT EFFECT
RENAL CLEARANCE OF INULIN AND CREATINE
CLEARANCE OF UREA
RENAL CONTROL OF ELECTROLYTE BALANCE
RENAL CONTROL OF ACID-BASE BALANCE
LECTURE OUTLINE CONTINUED
Membrane Junctions
Tight junction – impermeable junction that encircles the cell
Desmosome – anchoring junction scattered along the sides of cells
Gap junction – a nexus that allows chemical substances to pass between cells
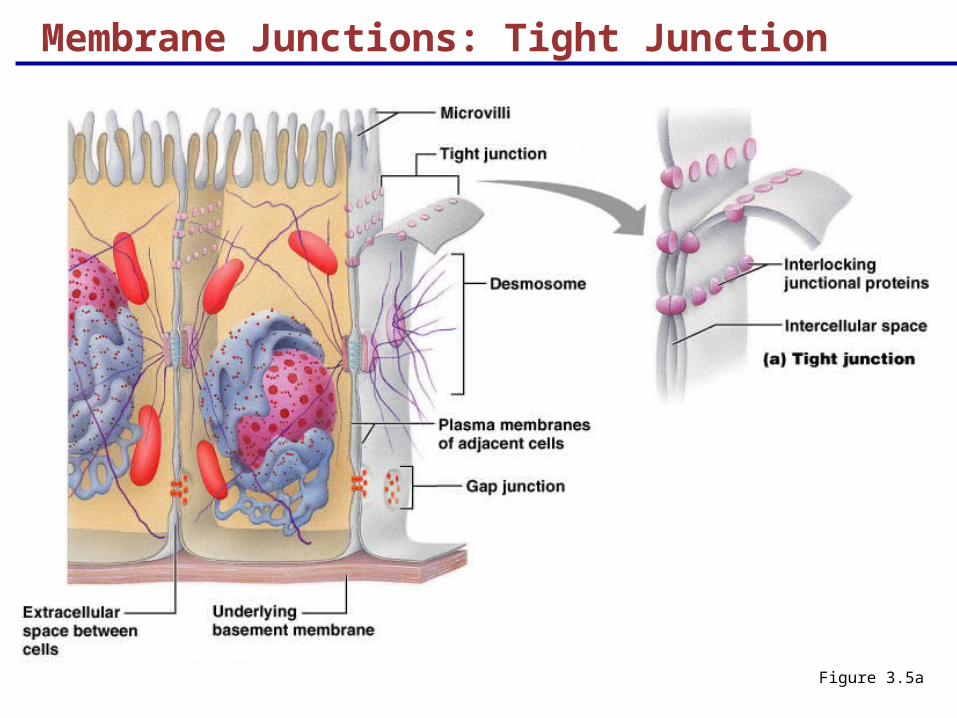
Membrane Junctions: Tight Junction
Figure 3.5a
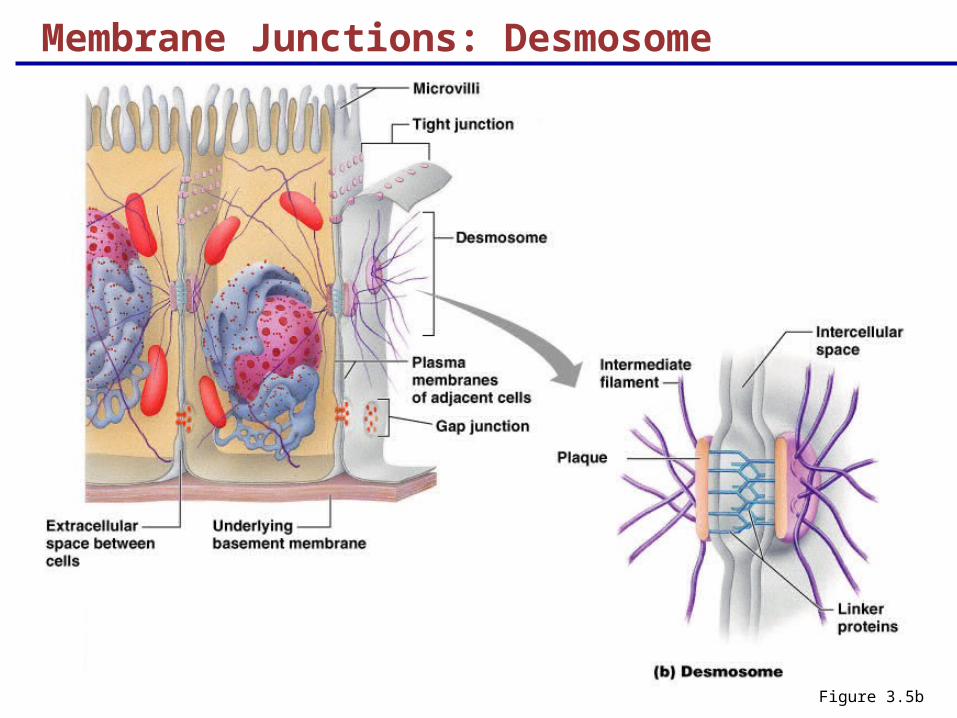
Membrane Junctions: Desmosome
Figure 3.5b
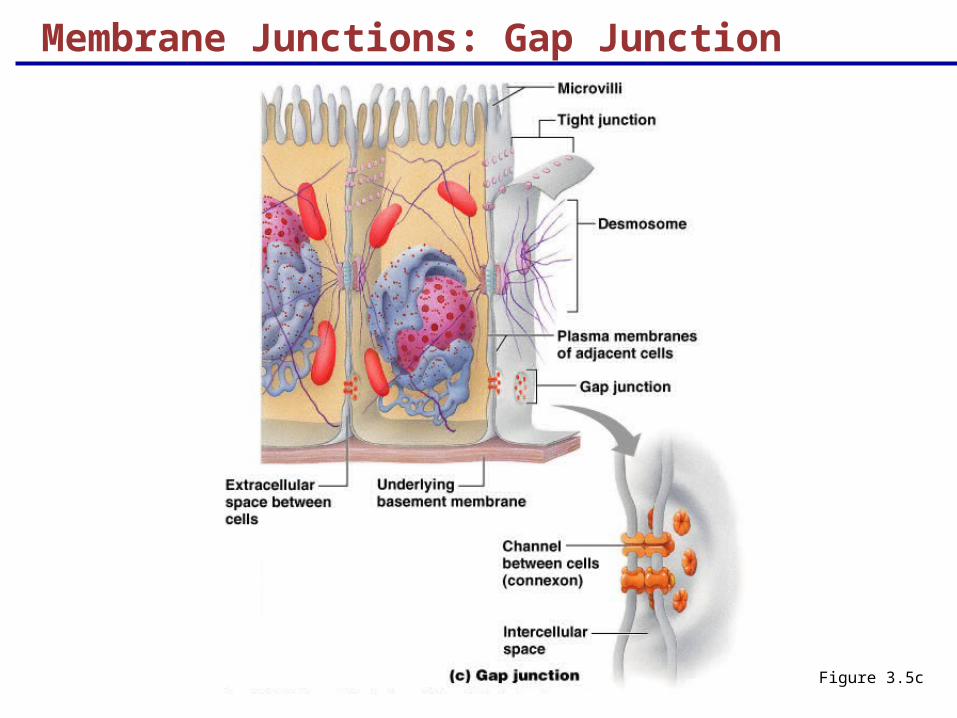
Membrane Junctions: Gap Junction
Figure 3.5c
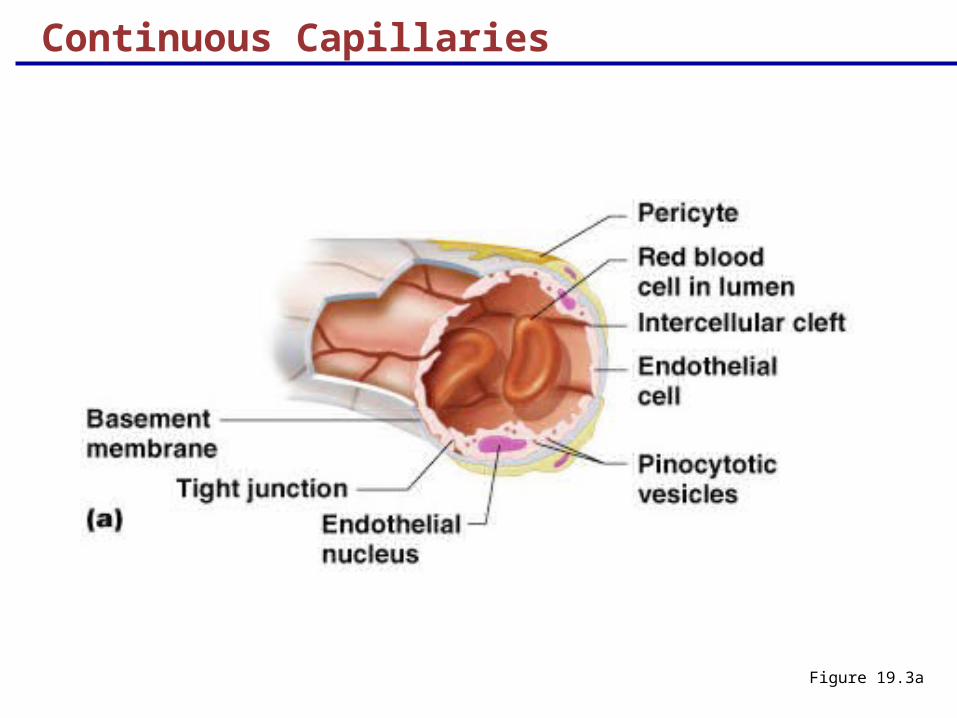
Continuous Capillaries
Figure 19.3a
Continuous Capillaries
Continuous capillaries of the brain:
Have tight junctions completely around the endothelium
Constitute the blood-brain barrier
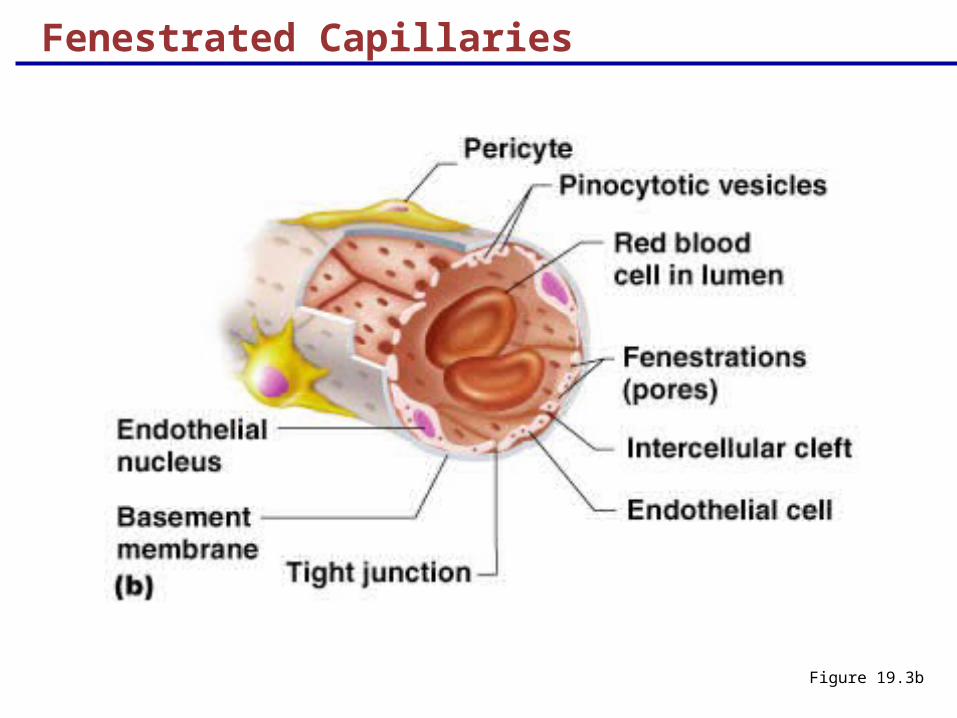
Fenestrated Capillaries
Figure 19.3b
Fenestrated Capillaries
Found wherever active capillary absorption or filtrate formation occurs (e.g., small intestines, endocrine glands, and kidneys)
Characterized by:
An endothelium riddled with pores (fenestrations)
Greater permeability to solutes and fluids than other capillaries
Sinusoids
Highly modified, leaky, fenestrated capillaries with large lumens
Found in the liver, bone marrow, lymphoid tissue, and in some endocrine organs
Allow large molecules (proteins and blood cells) to pass between the blood and surrounding tissues
Blood flows sluggishly, allowing for modification in various ways
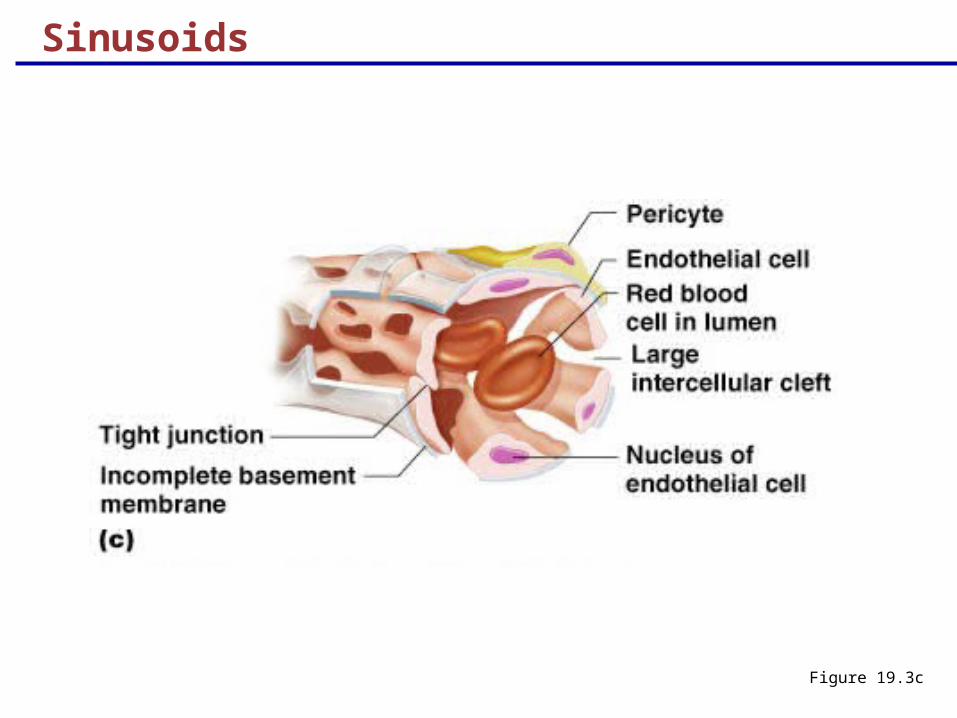
Sinusoids
Figure 19.3c
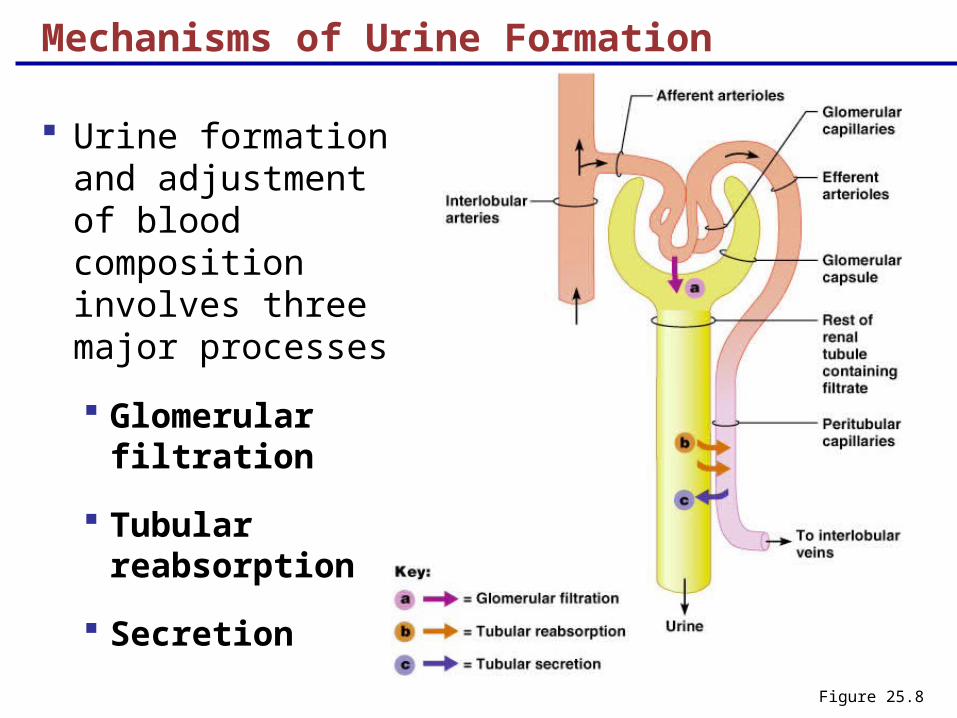
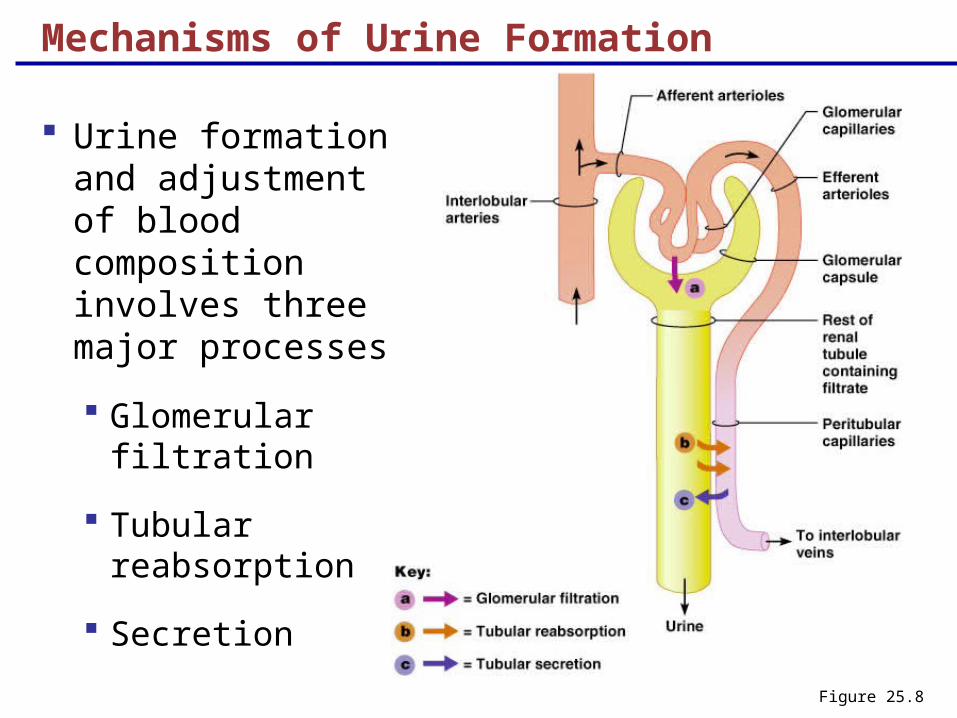
Mechanisms of Urine Formation
Urine formation and adjustment of blood composition involves three major processes
Glomerular filtration
Tubular reabsorption
SecretionFigure 25.8
Kidney Functions
Filter 180 liters (45 gallons) of blood daily, allowing toxins, metabolic wastes, and excess ions to leave the body in urine
Regulate volume and chemical makeup of the blood
Maintain the proper balance between water and salts, and acids and bases
Other Urinary System Organs
Urinary bladder – provides a temporary storage reservoir for urine
Paired ureters – transport urine from the kidneys to the bladder
Urethra – transports urine from the bladder out of the body
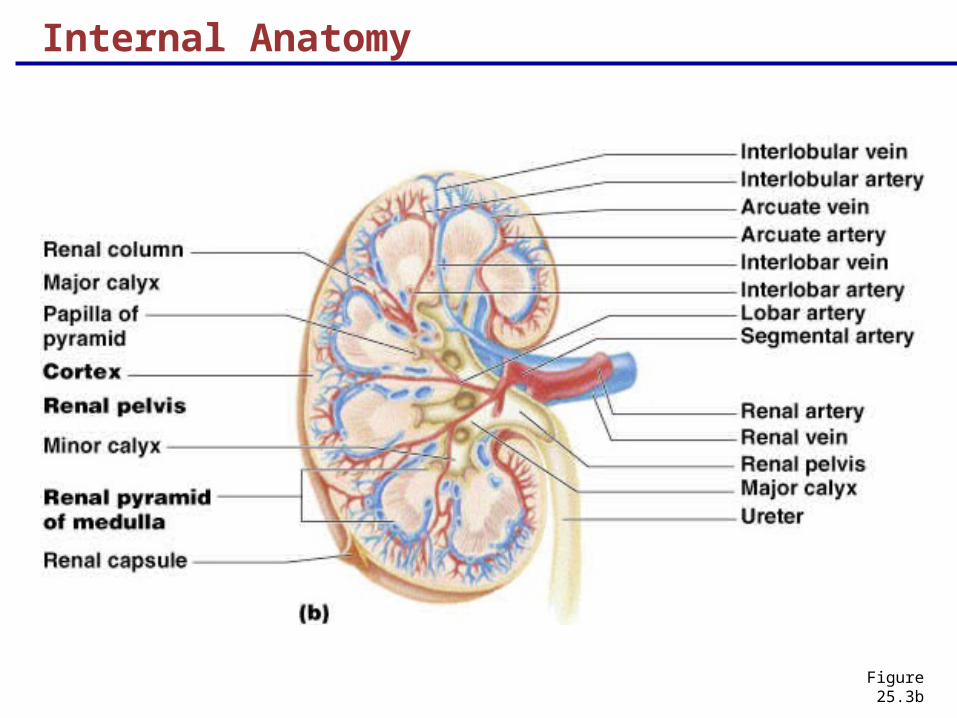
Internal Anatomy
Figure 25.3b
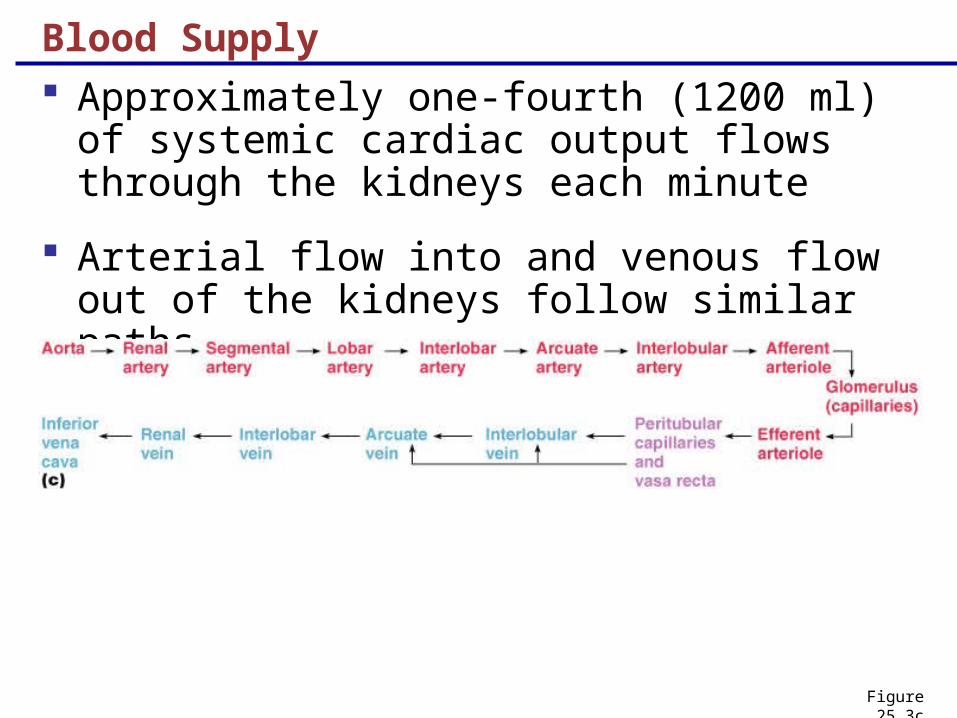
Blood Supply
Approximately one-fourth (1200 ml) of systemic cardiac output flows through the kidneys each minute
Arterial flow into and venous flow out of the kidneys follow similar paths
Figure 25.3c
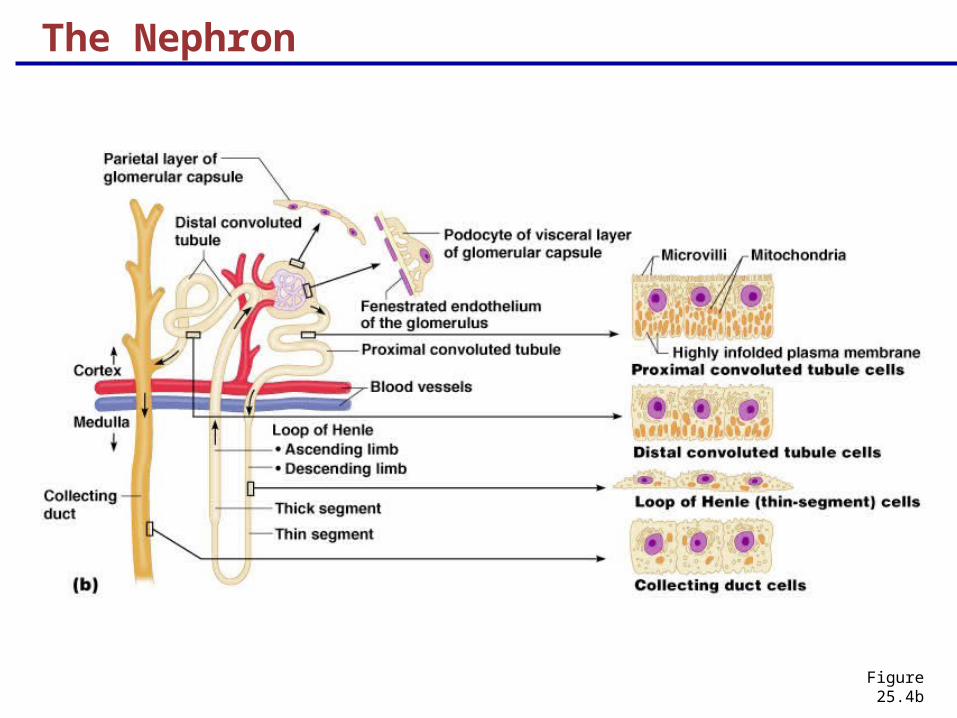
The Nephron
Figure 25.4b
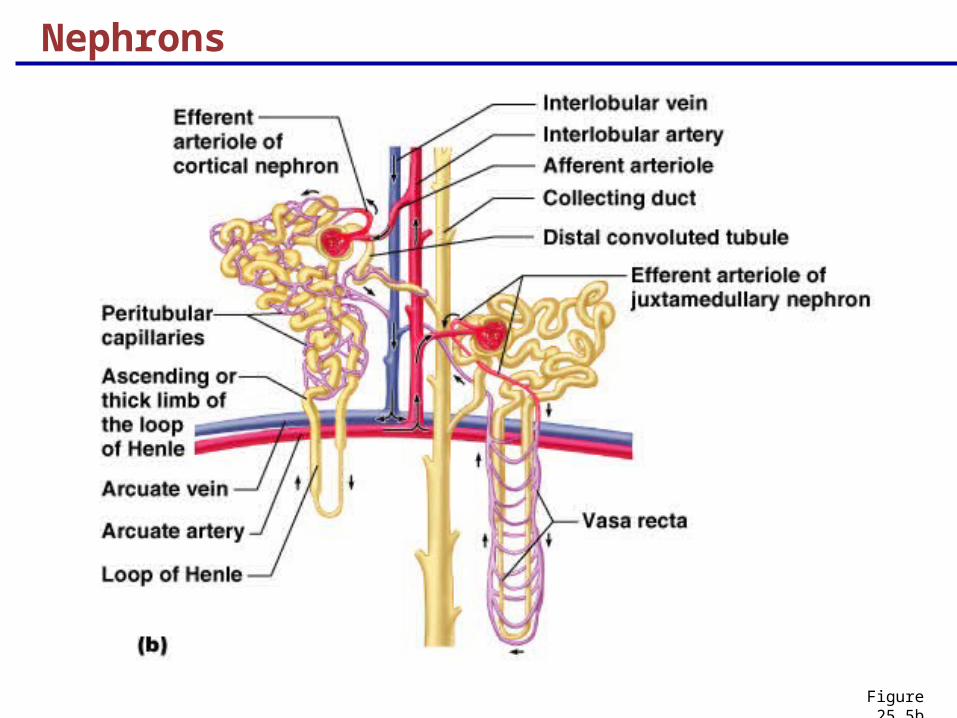
Nephrons
Figure 25.5b
Vascular Resistance in Microcirculation
Afferent and efferent arterioles offer high resistance to blood flow
Blood pressure declines from 95mm Hg in renal arteries to 8 mm Hg in renal veins
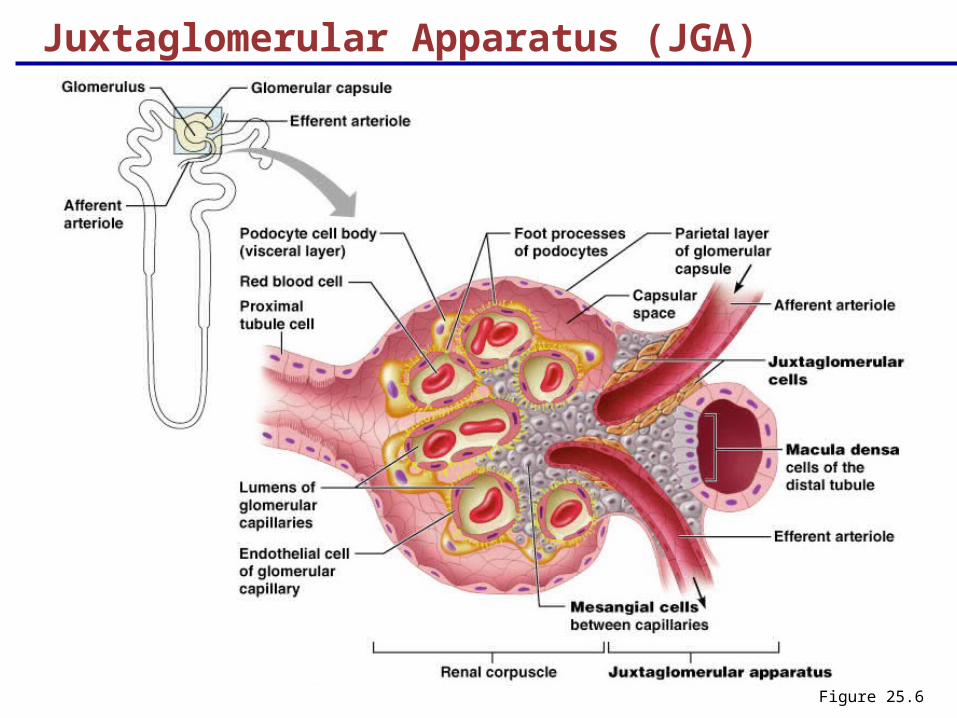
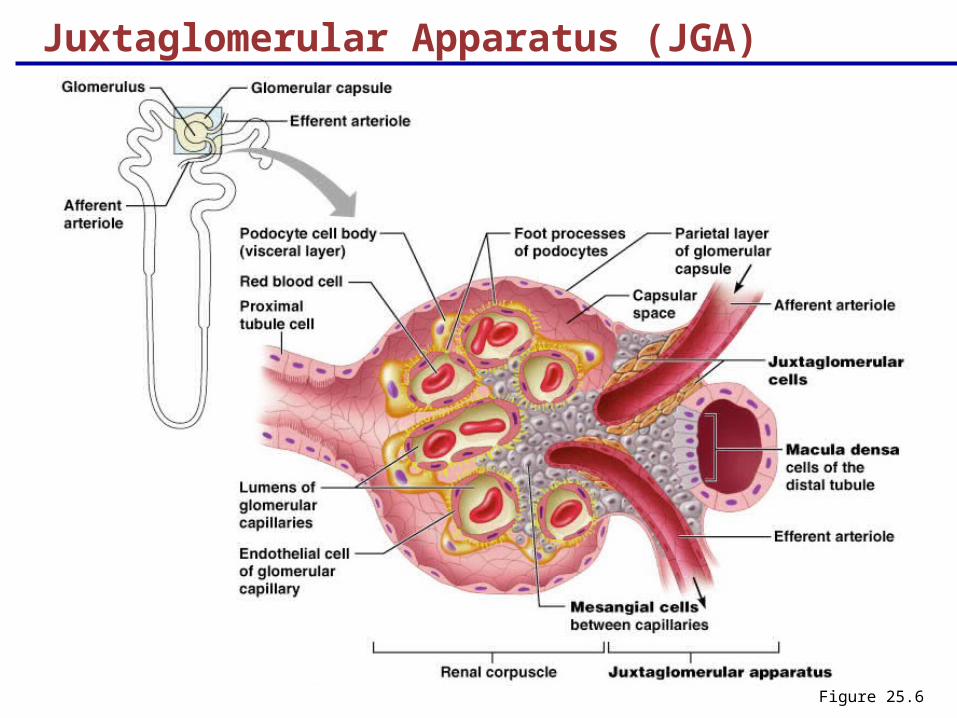
Juxtaglomerular Apparatus (JGA)
Figure 25.6
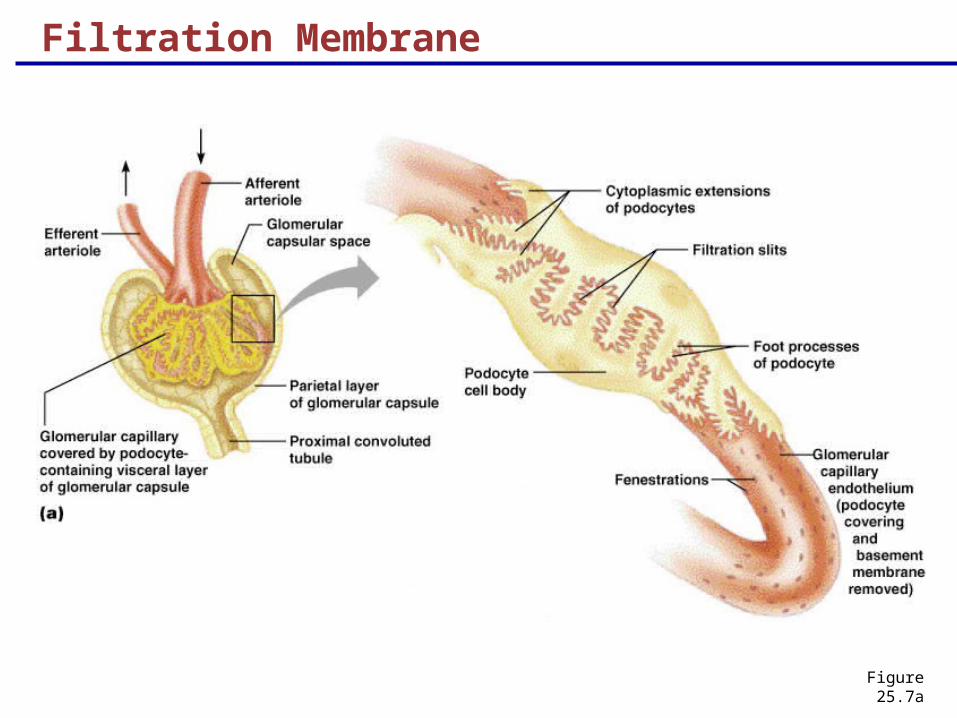
Filtration Membrane
Figure 25.7a
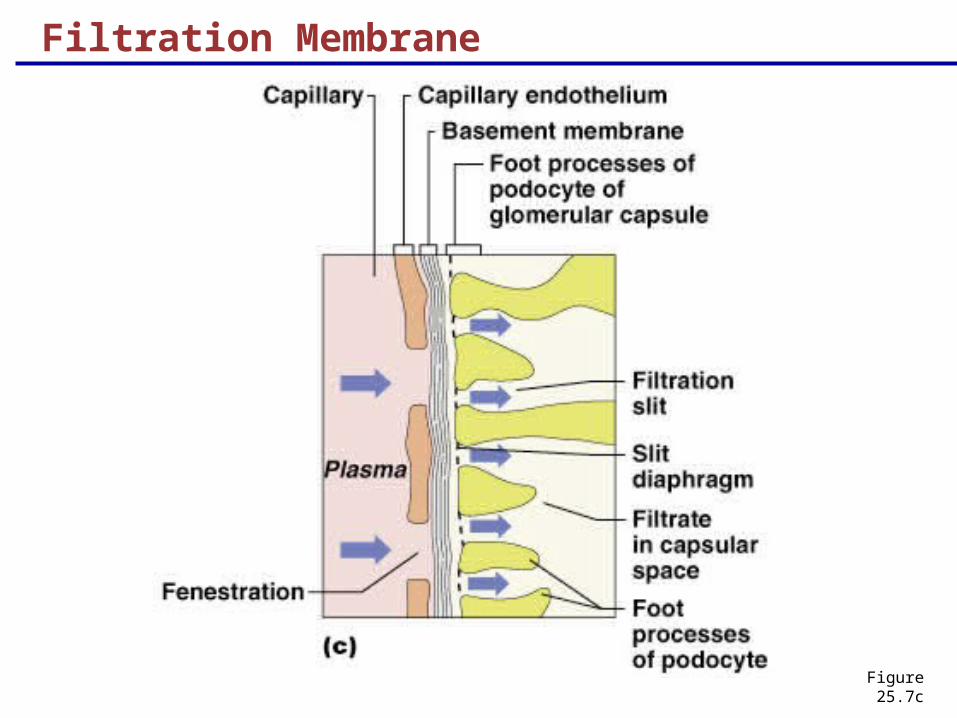
Filtration Membrane
Figure 25.7c
Mechanisms of Urine Formation
Urine formation and adjustment of blood composition involves three major processes
Glomerular filtration
Tubular reabsorption
SecretionFigure 25.8
Glomerular Filtration
Principles of fluid dynamics that account for tissue fluid in all capillary beds apply to the glomerulus as well
The glomerulus is more efficient than other capillary beds because:
Its filtration membrane is significantly more permeable
Glomerular blood pressure is higher
It has a higher net filtration pressure
Plasma proteins are not filtered and are used to maintain osmotic pressure of the blood
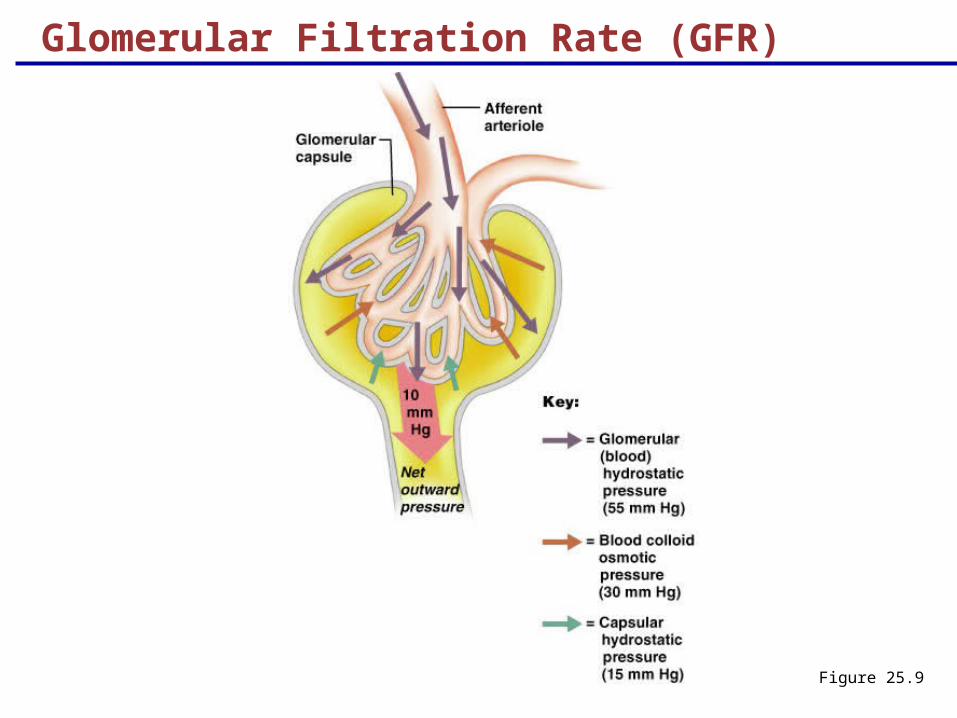
Net Filtration Pressure (NFP)
The pressure responsible for filtrate formation
NFP equals the glomerular hydrostatic pressure (HPg) minus the osmotic pressure of glomerular blood (OPg) combined with the capsular hydrostatic pressure (HPc)
NFP = HPg – (OPg + HPc)
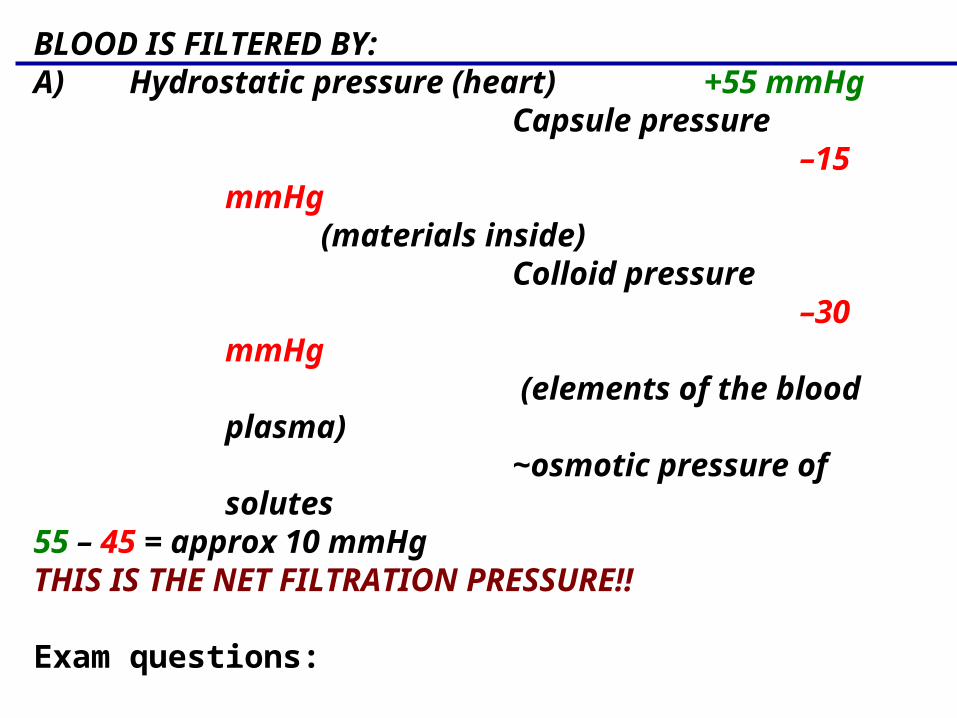
BLOOD IS FILTERED BY:A) Hydrostatic pressure (heart) +55 mmHg
Capsule pressure–15
mmHg(materials inside)
Colloid pressure–30
mmHg (elements of the blood
plasma)~osmotic pressure of solutes
55 – 45 = approx 10 mmHgTHIS IS THE NET FILTRATION PRESSURE!!
Exam questions:
What would an increase in blood pressure do?What effect would this have on urine production?
Glomerular Filtration Rate (GFR)
Figure 25.9
Glomerular Filtration Rate (GFR) inBowmans’s capsule CAPSULE
BOWMAN’S CAPSULE The total amount of filtrate formed per minute by the kidneys
≈ 125 ml of fluid per min (men)
≈ 120 ml of fluid per min (women)
THIS IS CALLED GFR OR
GLOMERULAR FILTRATION RATE
ULTRAFILTRATE
(formed under pressure ≈ 10mmHg)
≈ 125 ml of fluid per min (men) ≈ 7.5 liters per hr OR 180 liters per day ≈ 45 gallons of fluid
Glomerular Filtration Rate (GFR) inBowmans’s capsule continued CAPSULE
BOWMAN’S CAPSULE
TOTAL BLOOD VOLUME IS 5.5 liters
Therefore total blood volume is filtered into the glomerulus (and ends up in Bowman’s capsule) every 40 minutes
PROBLEM??
WATER, SALTS, GLUCOSE ETC. ALL NEED TO BE REABSORBED!!!
about 99% of the filtrate (formative urine) is
REABSORBED
Glomerular Filtration Rate (GFR)
GFR is directly proportional to the NFP
Changes in GFR normally result from changes in glomerular blood pressure
Regulation of Glomerular Filtration
If the GFR is too high:
Needed substances cannot be reabsorbed quickly enough and are lost in the urine
If the GFR is too low:
Everything is reabsorbed, including wastes that are normally disposed of
Regulation of Glomerular Filtration
Three mechanisms control the GFR
Renal autoregulation (intrinsic system)
Neural controls
Hormonal mechanism (the renin-angiotensin system)
Renal autoregulation (intrinsic system)
REGULATION OF GFR
GFR RATE IS UNDER HOMEOSTATIC CONTROL
VASOCONSTRICTION OR VASODILATION OF AFFERENT ARTERIOLES (intrinsic factors)
KNOWN AS MYOGENIC RENAL AUTOREGULATION
(Myogenic – responds to changes in pressure in the renal blood vessels)
Renal autoregulation (intrinsic system)
FR
LOW BLOOD PRESSURE ——> vasodilation
greater blood flow ——> increased GFR
HIGH BLOOD PRESSURE ——> vasoconstriction
reduced blood flow ———> decreased GFR
MAINTAINS WATER AND SOLUTE FILTRATION
Under normal conditions, renal autoregulation maintains a nearly constant glomerular filtration rate
Extrinsic Controls
When the sympathetic nervous system is at rest:
Renal blood vessels are maximally dilated
Autoregulation mechanisms prevail
Extrinsic Controls
Decrease in blood pressure ----> baroreceptors in aorta
----> increased sympathetic nerve activity ------>
1) vasoconstriction of GI tract and skin
2) heart rate increased (therefore cardiac output)
-----> BOTH raise systemic blood pressure
Extrinsic Controls
Under stress:
Norepinephrine/epinephrine is released by the sympathetic nervous system
Epinephrine is also released by the adrenal medulla
Afferent arterioles constrict and filtration is inhibited
Juxtaglomerular Apparatus (JGA)
Figure 25.6
Renin Release
Renin release is triggered by:
1) Reduced stretch of the granular JG cells
Stimulus (low blood pressure; therefore
reduced blood flow to kidneys)
2) Direct stimulation of the JG cells via
noreepinephrine/epinephrine by renal nerves
Renin Release
WHICH STIMULATES CELLS IN JUXTAGLOMERULUS APPARATUS
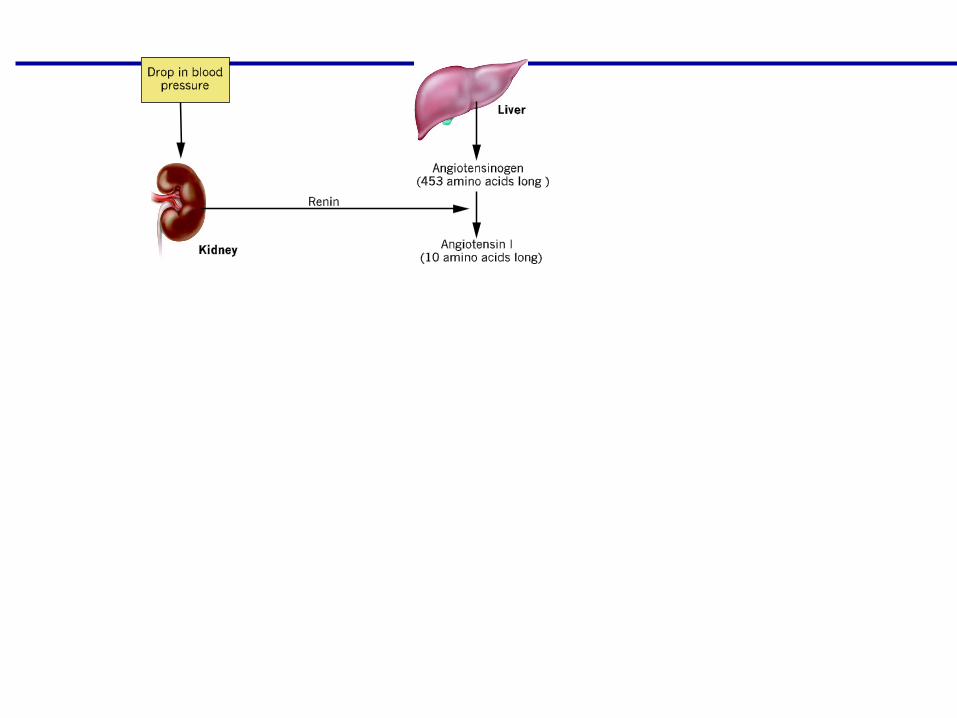
——> RELEASES RENIN ——>
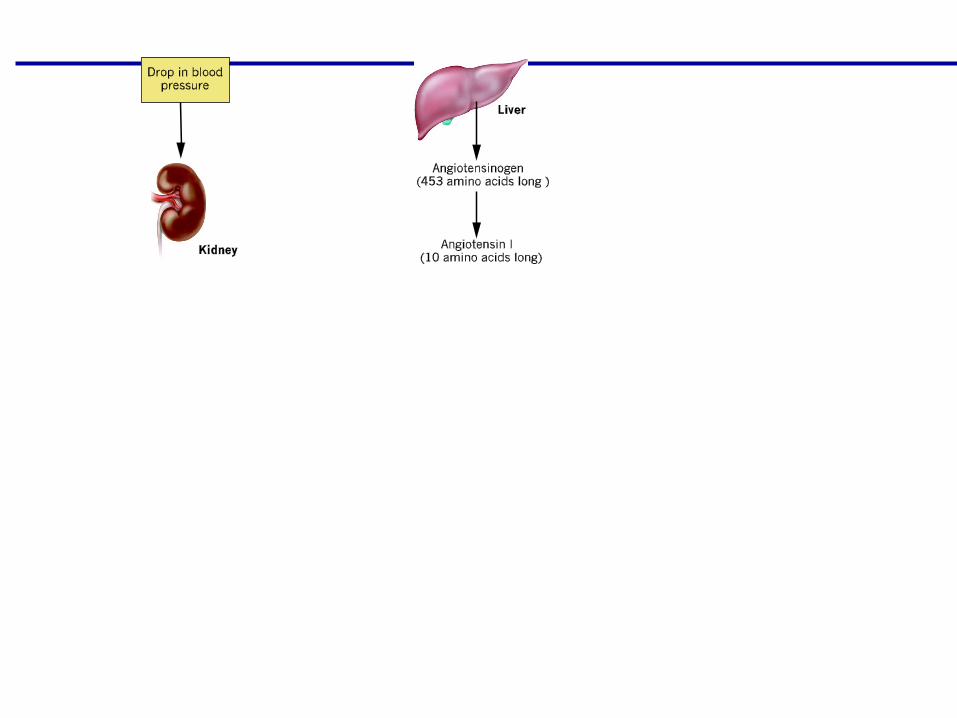
TRAVELS TO LIVER ——>
STIMULATES RELEASE OFANGIOTENSINOGEN ——>
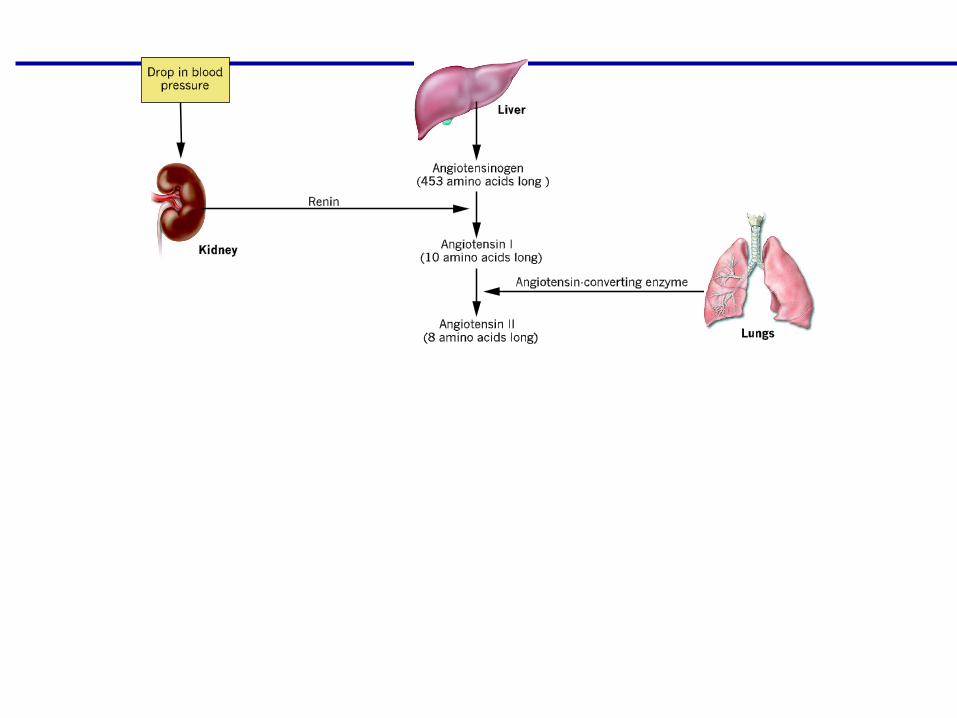
TRAVELS IN BLOOD TO LUNGS ——>
CONVERTS ANGIOTENSIN I TO ANGIOTENSIN II
Renin-Angiotensin Mechanism
Is triggered when the JG cells release renin
Travels to liver
Renin releases angiotensinogen
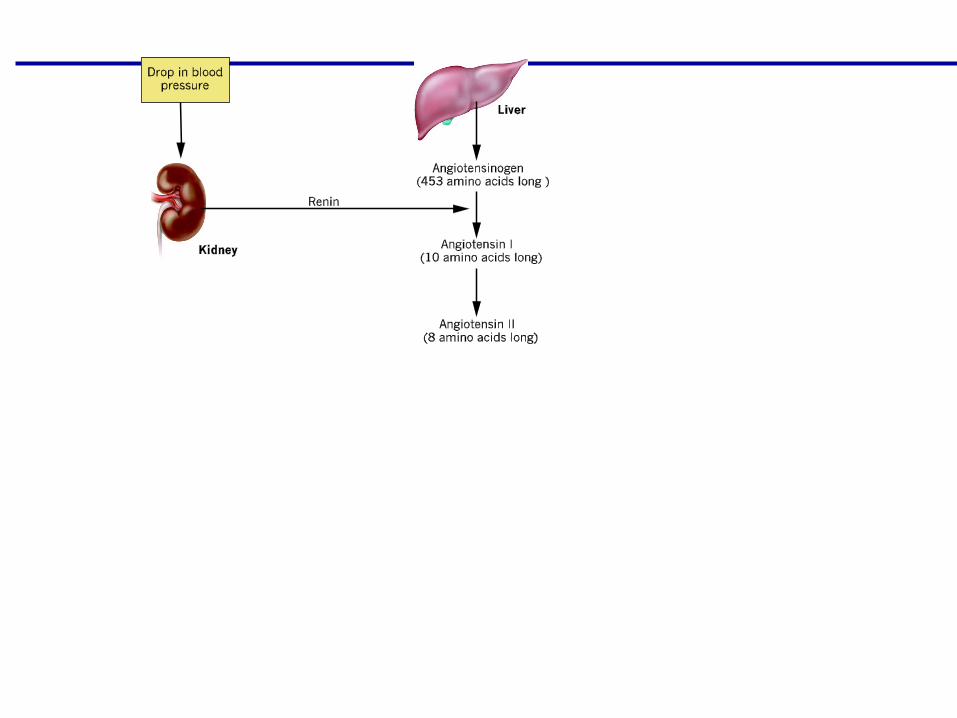
Angiotensinogen converted to angiotensin I
Angiotensin I travels in blood to lungs and is converted to angiotensin II
Angiotensin II action (s):
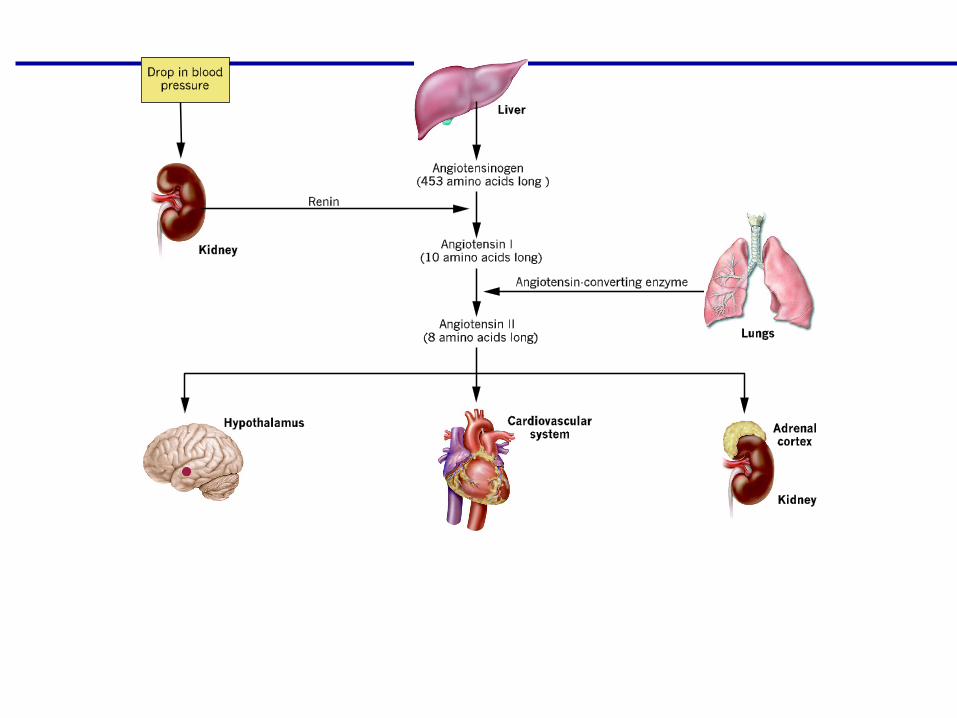
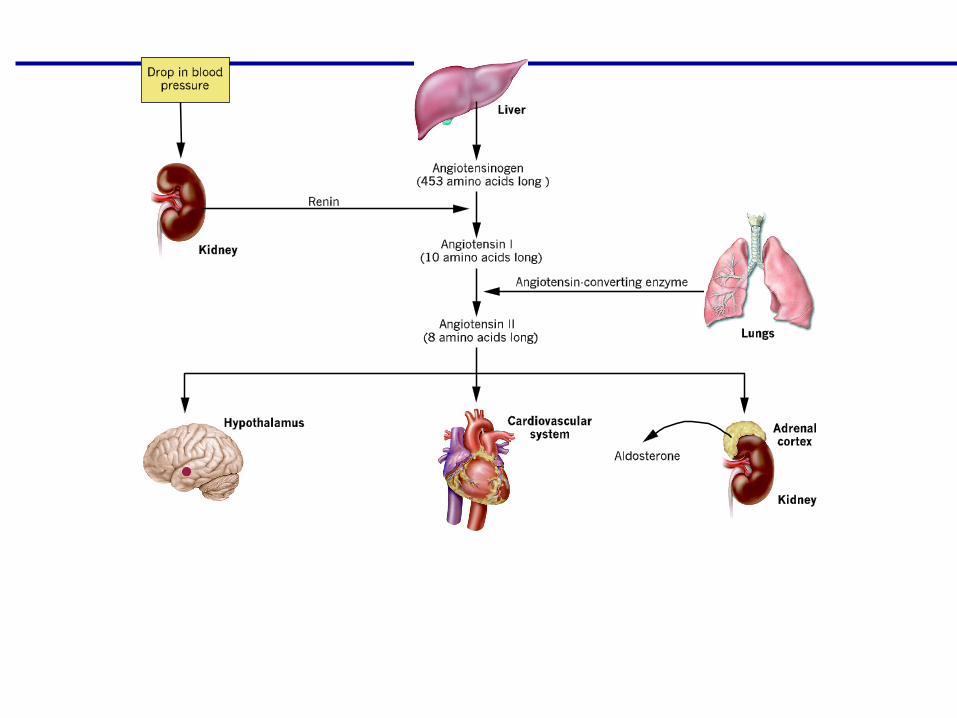
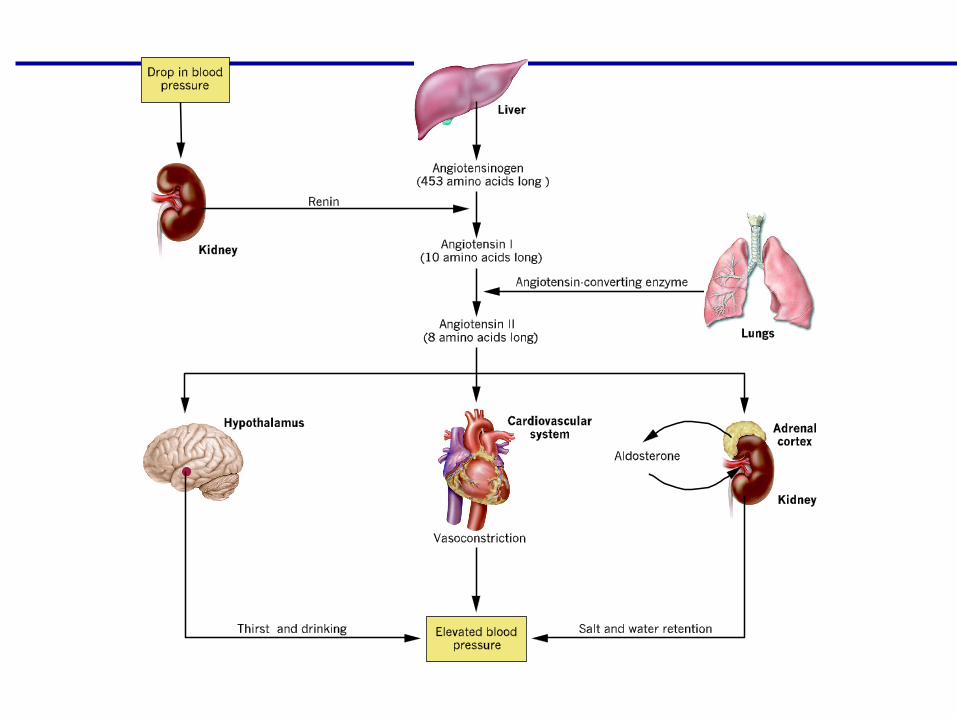
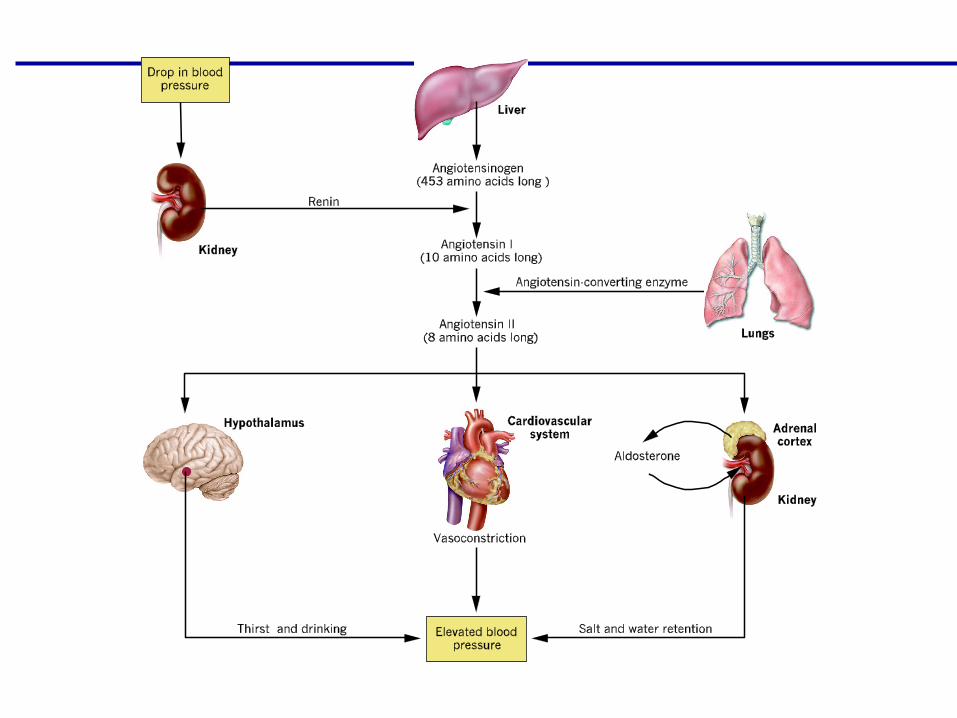
ANGIOTENSIN II
ACTS ON FOUR (4) DIFFERENT EFFECTORS
1. VASOCONSTRICTION OF SYSTEMIC ARTERIOLES (INCREASES BLOOD PRESSURE)
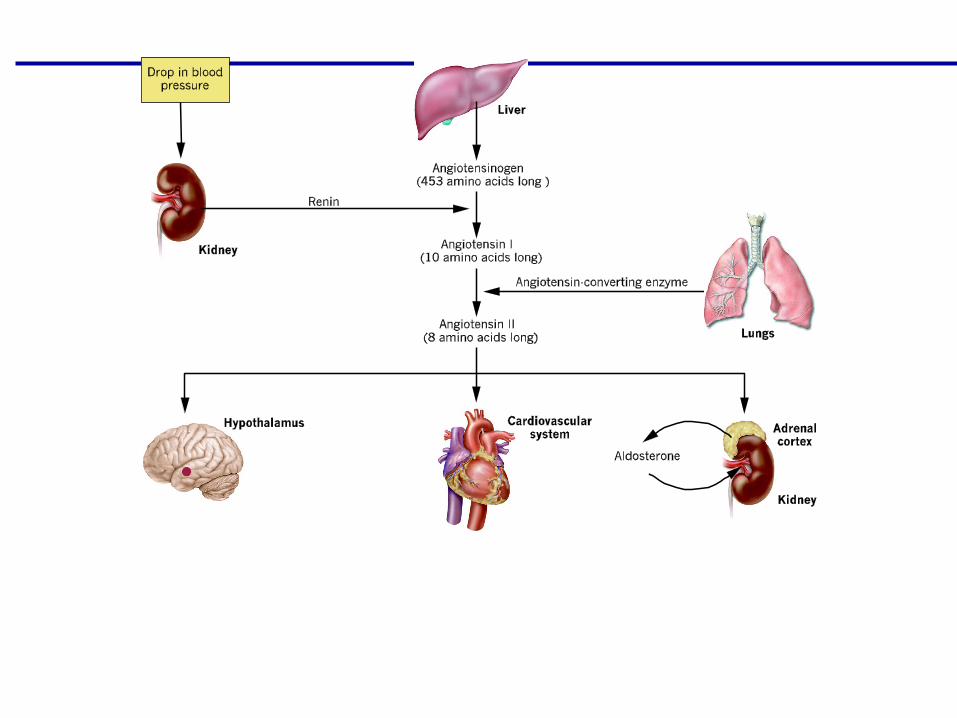
2. STIMULATES ALDOSTERONE SECRETION FROM ADRENAL CORTEX
ALDOSTERONE ————> INCREASES WATER RETENTION OF SODIUM, CHLORIDE AND WATER BY KIDNEYS ————> INCREASES BLOOD VOLUME ————> INCREASES BLOOD PRESSURE
3. STIMULATION OF THIRST CENTERS IN HYPOTHALAMUS
(CAUSES INCREASED WATER INTAKE ———> INCREASES BLOOD VOLUME ——> INCREASES BLOOD PRESSURE!!
4. STIMULATION OF ADH FROM POSTERIOR PITUITARY GLAND
ADH PROMOTES WATER RETENTION BY KIDNEYS
(makes distal tubule and collecting ducts more permeable to water) ———> INCREASES BLOOD VOLUME ———> INCREASES BLOOD PRESSURE!!
(ALL 4 EFFECTORS WILL RETURN GFR BACK TO “NORMAL”)
ATRIAL NATRIURETIC PEPTIDE (ANP)
(cells discovered in left and right atria in 1983)
Stretching of cells due to INCREASED BLOOD VOLUME
(INCREASED BLOOD PRESSURE)
PROMOTES EXCRETION OF WATER (DIURESIS)
AND EXCRETION OF SODIUM (NATRIURESIS)
HOW??
1. DILATES AFFERENT ARTERIOLES (INCREASES GFR)
2. INCREASES PERMEABILITY OF GLOMERULUS (INCREASES GFR)
3. DECREASES ADH
4. DECREASES ALDOSTERONE
5. DECREASES RENIN
(a decrease in blood volume as a result of 1 through 5 inhibits
Cells in Left and Right Atria)
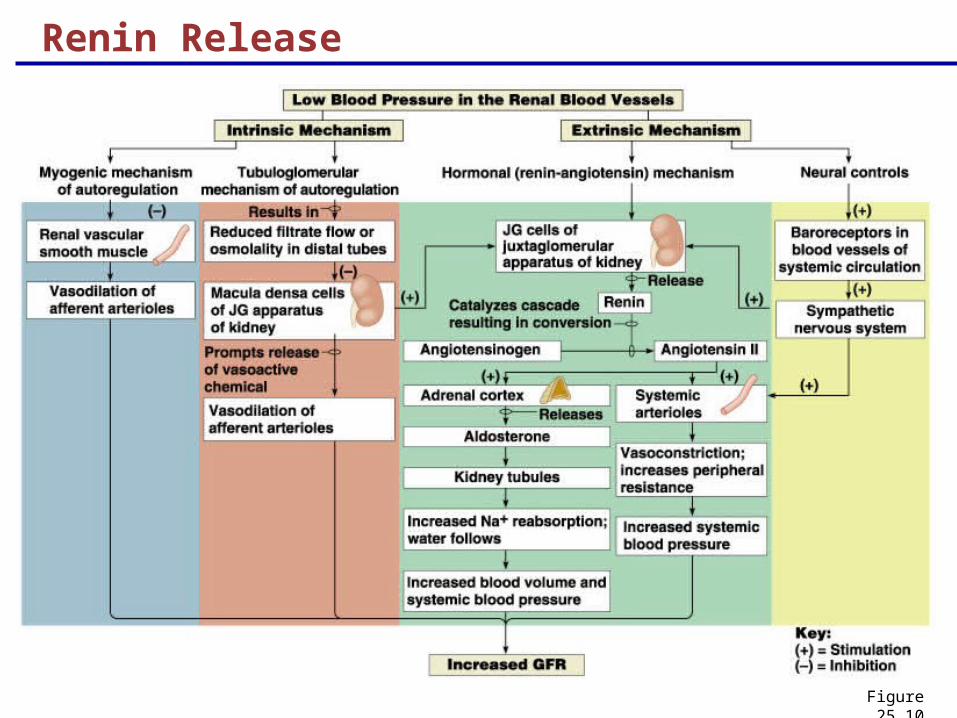
Renin Release
Figure 25.10
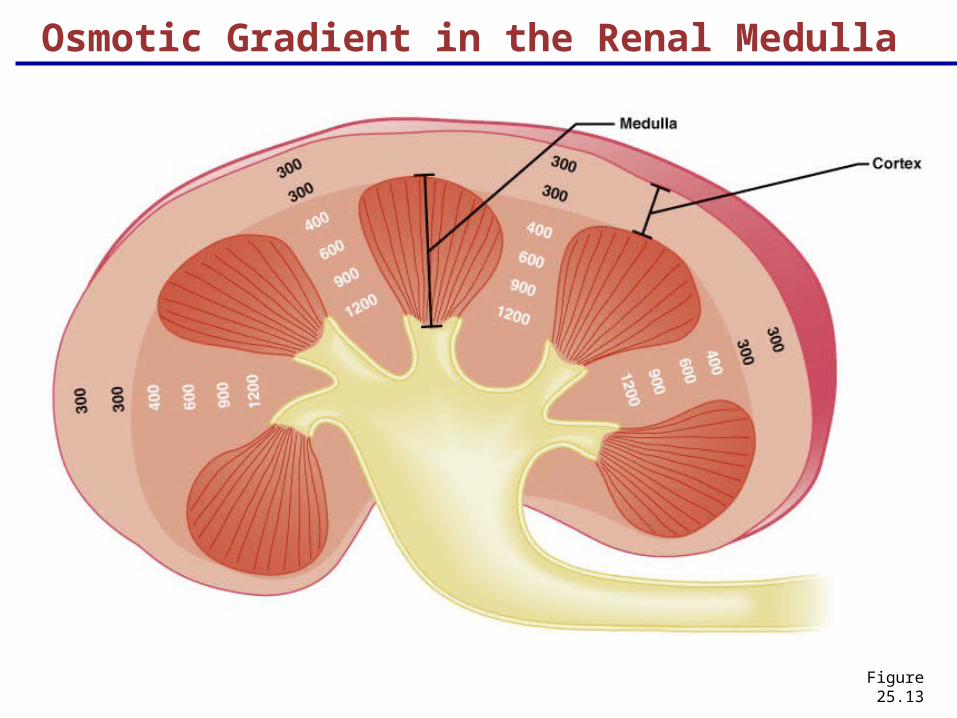
Osmotic Gradient in the Renal Medulla
Figure 25.13